Harvard Alumni Day Address June 2006 Dr Kinnunen
32
Tobacco Dependence and Its Treatment Taru Hannele Kinnunen, PhD Harvard Medical School Harvard School Dental Medicine Department of Oral Health Policy and Epidemiology Harvard Medical School Alumni Day Plenary June 2006
-
Upload
taru-kinnunen -
Category
Documents
-
view
100 -
download
0
Transcript of Harvard Alumni Day Address June 2006 Dr Kinnunen

Tobacco Dependence and Its Treatment
Taru Hannele Kinnunen, PhDHarvard Medical School
Harvard School Dental Medicine
Department of Oral Health Policy and Epidemiology
Harvard Medical School Alumni Day PlenaryJune 2006
Tobacco Use and Oral Cavity
TOBACCO USE
Pre-cancerous Lesions
Oral Cancers
•Gingivitis•Periodontitis•Acute Ulcero-Necrotic Gingivitis
•Teeth colorations•Halitosis•Sense of taste/smell•Chronic Sinusitis
Consequences in implantology
Consequences in wound healing

Tobacco Dependence –a Chronic Syndrome
ICD-10: 17 Mental and behavioral disorders due to use of tobacco17.1 Harmful use 17.2 Dependence syndrome 17.3 Withdrawal state
DSM-IV-TR: Nicotine Use Disorder305.1 Nicotine Dependence 292.0 Nicotine Withdrawal
Dental codeD1320 Tobacco counseling for the control
and provision of oral disease
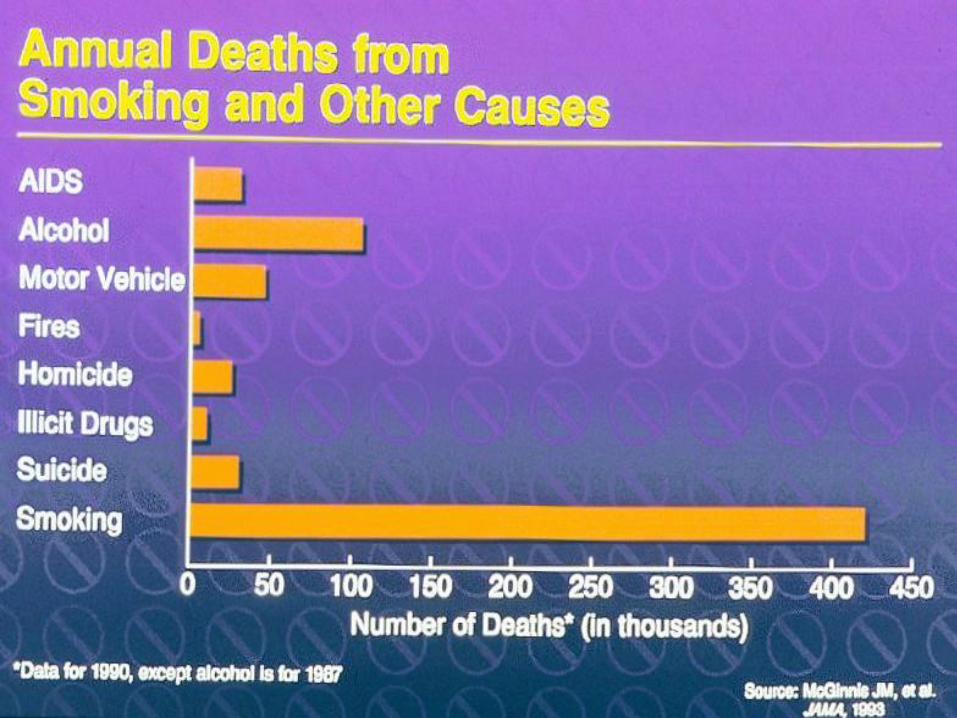
Smoking in Perspective• Kills more than 430,000 Americans each year
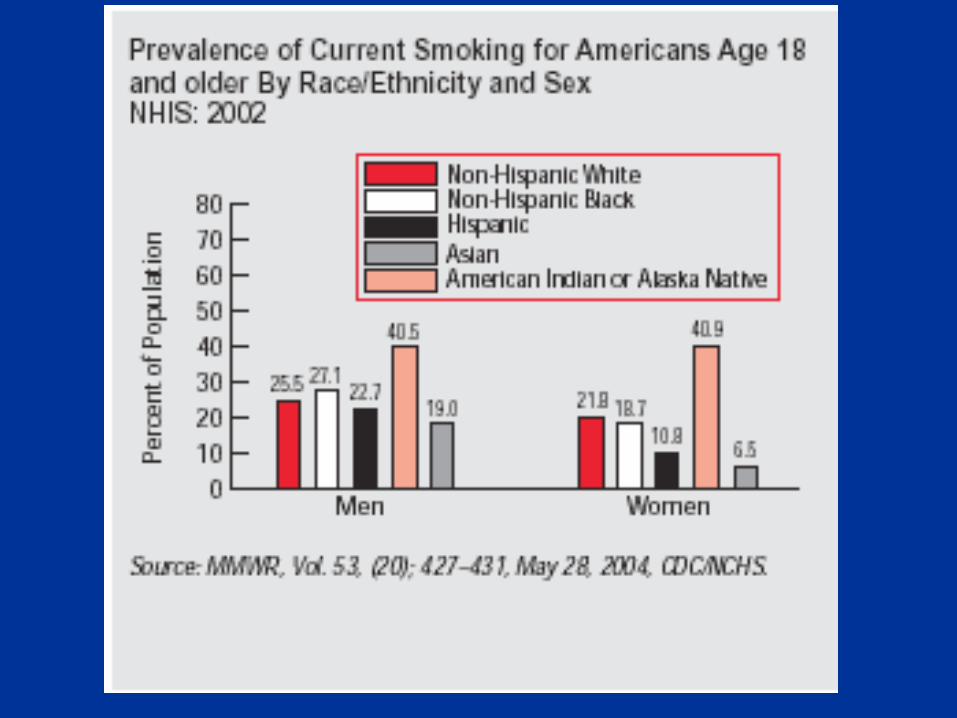
• 25% of adult Americans smoke
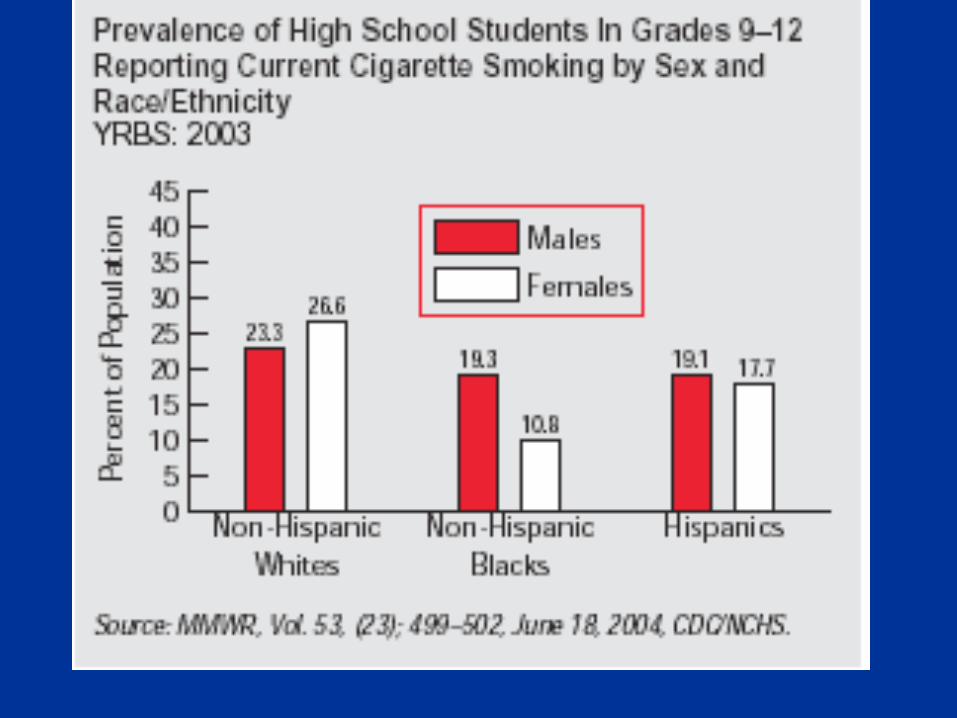
• 3,000 children and adolescents become regular tobacco users every day
• Causes cancer, heart disease, stroke, pulmonary disease, and adverse pregnancy outcomes
• Adds $50 billion in direct health costs each year
• One-third of all tobacco users in U.S. will die prematurely

Health Consequences of Smoking Cessation
• Smoking is number 1 preventable cause of death
• Treating tobacco dependence– cost-effective– significant measure in primary and secondary
prevention• Smoking cessation results in many positive
health consequences– most immediately and substantially coronary
heart disease and other cardiovascular diseases (CVD)(USDHH. Women and smoking: A report of the Surgeon General 2001.), (Benowitz 2003, Kinnunen Mustonen 2004)

Treatment after CHD: Reduction of the Mortality Risk
39%
29%
23%
23%
15%
0% 5% 10% 15% 20% 25% 30% 35% 40% 45%
Smoking Cessation
Statins
Beta-blockers
ACE-Inhibitors
Aspirin
JAMA, 2003
BMJ, 2000
BMJ, 1999
Lancet, 2000
BMJ, 2002
Difficulty in Quitting
• 70% of tobacco users would like to quit
• Less than 10% succeed in a given year
• Long term or permanent abstinence may be achieved after several attempts.
• Only 5-10% tobacco users are not nicotine dependent
Nicotine Dependence
Copyright © 2002, TK. All rights reserved.
• Physiological dependence neurobiology:
neuromodulation and neuroadaptation
genetics
positive and negative reinforcment
withdrawal
• Conditioning/Learning highly conditioned behavior
20 cigarettes x 10 puffs= 200 repetitions
slips, relapse
• Sensory aspect of smoking
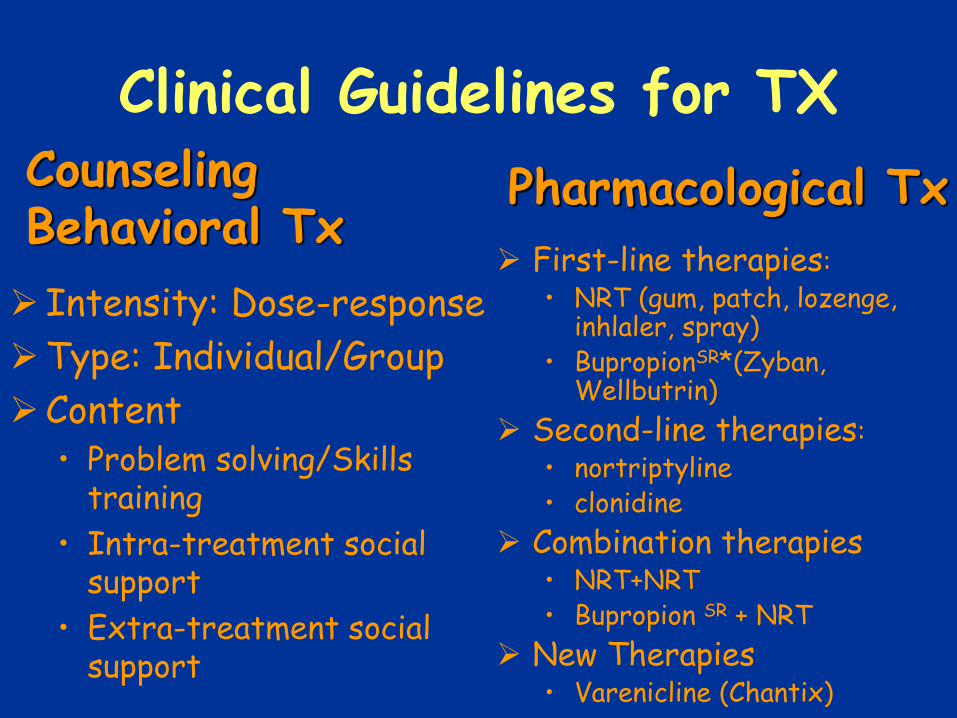
Clinical Guidelines for TX
Intensity: Dose-response
Type: Individual/Group
Content• Problem solving/Skills
training
• Intra-treatment social support
• Extra-treatment social support
First-line therapies:
• NRT (gum, patch, lozenge, inhlaler, spray)
• BupropionSR*(Zyban, Wellbutrin)
Second-line therapies:
• nortriptyline• clonidine
Combination therapies• NRT+NRT• Bupropion SR + NRT
New Therapies• Varenicline (Chantix)
CounselingBehavioral Tx
Pharmacological Tx

1-year Abstinence in Studies with NRT and Behavioral Counseling
0
20
40
60
80
100
% A
bst
inen
t
1-week 16-weeks 1-year
Ex_NicGum CG_NicGum NicGum0
10
20
30
40
50
60
70
80
90
100
1-week 16-week 1-year
NicGum
1992-1995
1999-2002
(Garvey & Kinnunen, NIDA)
(Kinnunen, NIDA)
From Tobacco Plant to Cigarettes
Nicotine Dependenceself-administrationwithdrawal symptoms
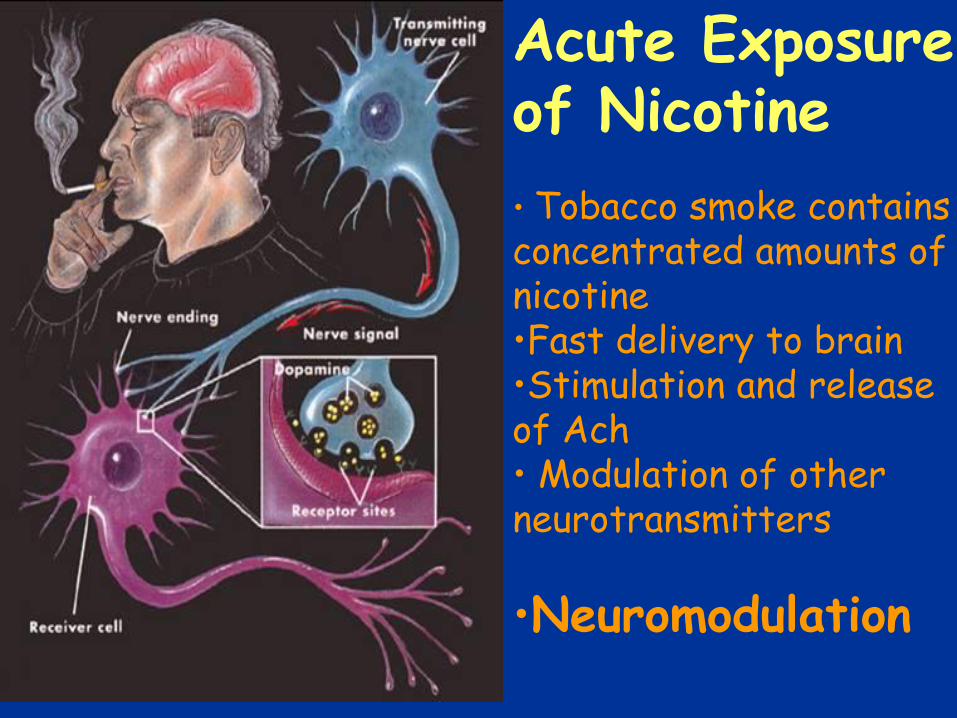
Acute Exposure of Nicotine
• Tobacco smoke contains concentrated amounts of nicotine•Fast delivery to brain•Stimulation and release of Ach• Modulation of other neurotransmitters
•Neuromodulation

nicotine receptornAChR
nicotine molecules from
tobacco smokeAcetylcholine
ACh
Synapse
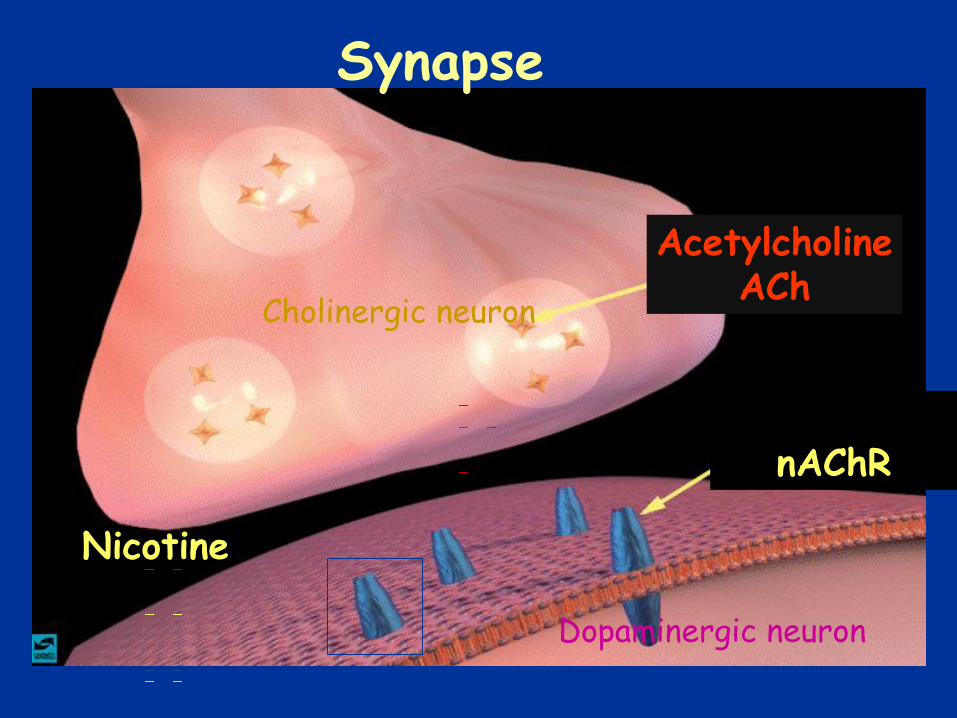
AcetylcholineACh
nAChR
Nicotine
Synapse
Cholinergic neuron
Dopaminergic neuron

Most Effects are Mediated by Nicotinic Receptors
(nAChRs)
Subtype α4β2
17 subtypes (α4β2, α7)
Minutes
Incre
ase i
n n
ico
tin
e c
on
cen
trati
on
( n
g/m
l )
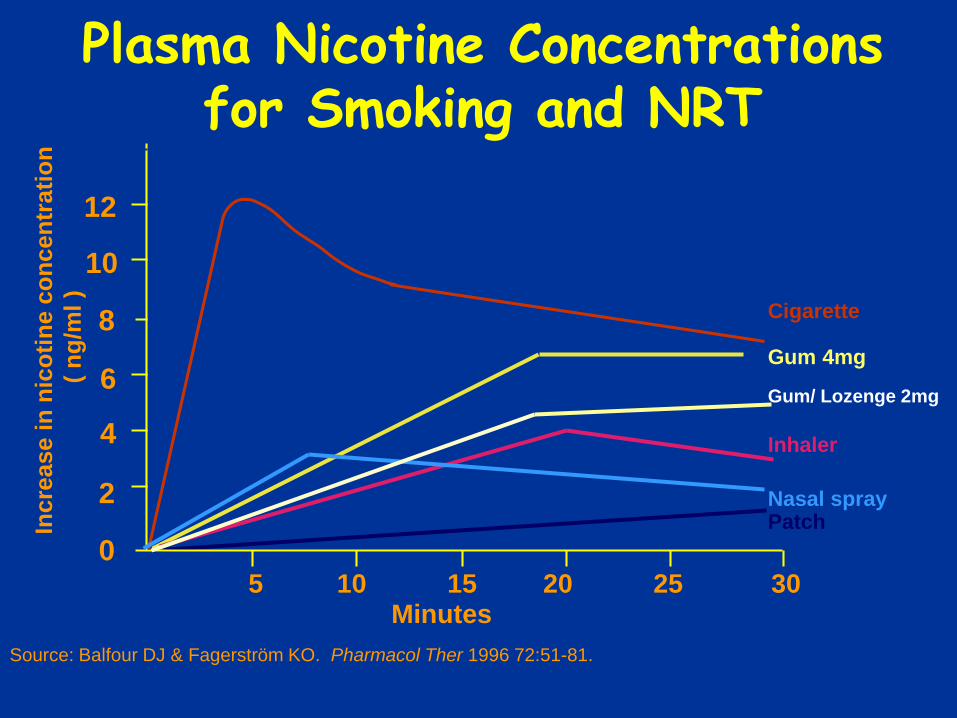
Cigarette
Gum 4mg
Gum/ Lozenge 2mg
Inhaler
Nasal sprayPatch
5 10 15 20 25 30
0
2
4
6
8
10
12
14
Plasma Nicotine Concentrations for Smoking and NRT
Source: Balfour DJ & Fagerström KO. Pharmacol Ther 1996 72:51-81.
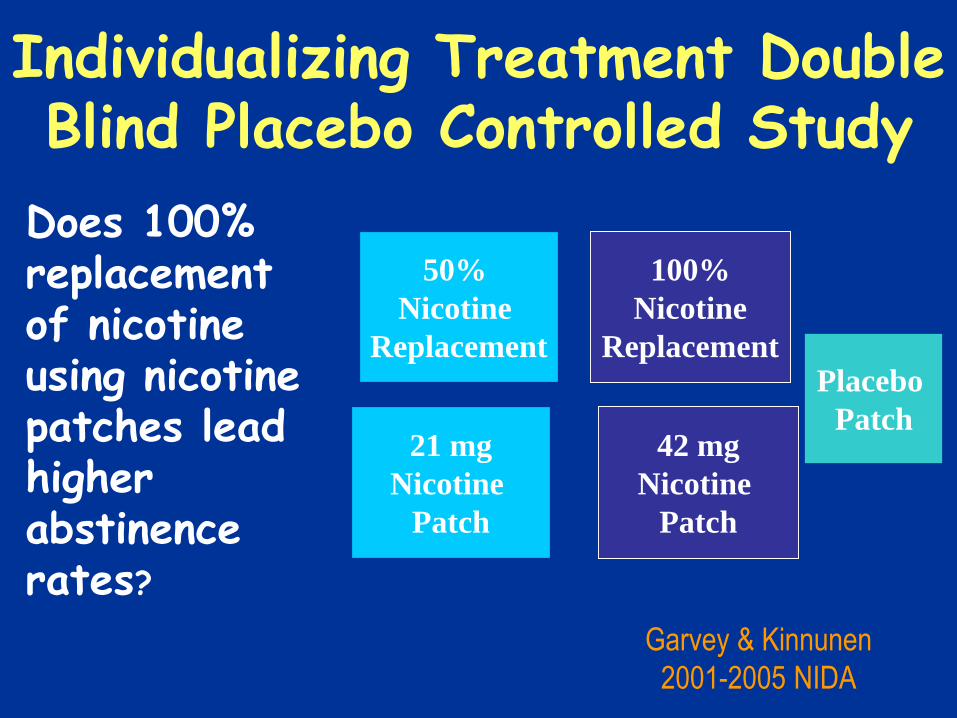
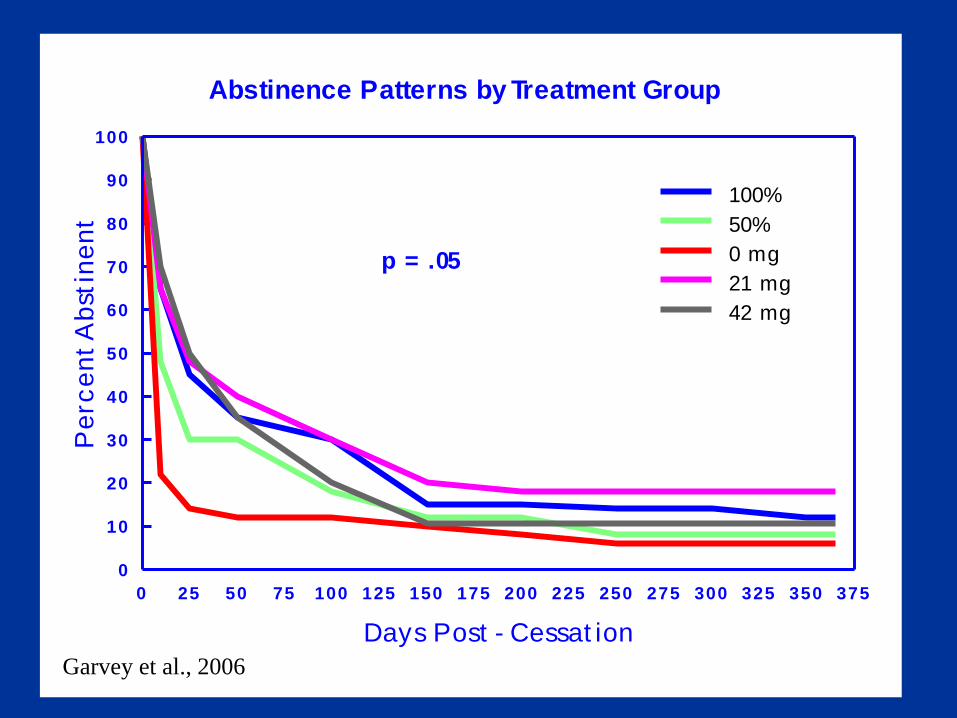
Individualizing Treatment Double Blind Placebo Controlled Study
Individualized Treatment
50%
Nicotine
Replacement
21 mg
Nicotine
Patch
42 mg
Nicotine
Patch
100%
Nicotine
ReplacementPlacebo
Patch
Garvey & Kinnunen
2001-2005 NIDA
Does 100% replacement of nicotine using nicotine patches lead higher abstinence rates?
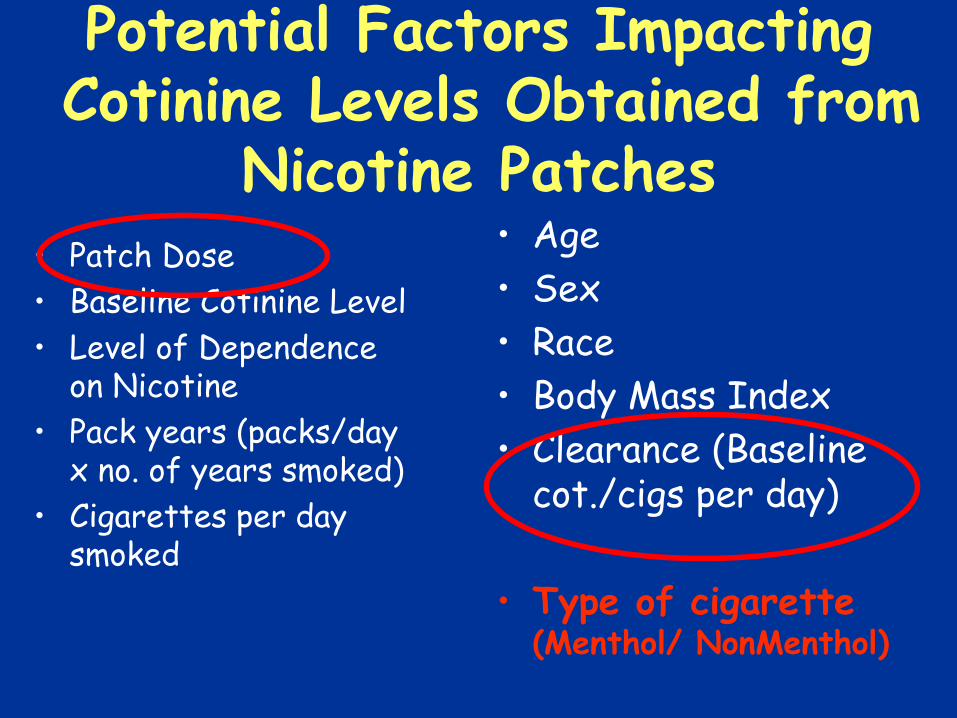
Potential Factors ImpactingCotinine Levels Obtained from
Nicotine Patches• Patch Dose
• Baseline Cotinine Level
• Level of Dependence on Nicotine
• Pack years (packs/day x no. of years smoked)
• Cigarettes per day smoked
• Age
• Sex
• Race
• Body Mass Index
• Clearance (Baseline cot./cigs per day)
• Type of cigarette (Menthol/ NonMenthol)
0 25 50 75 100 125 150 175 200 225 250 275 300 325 350 375
Days Post - Cessat ion
0
10
20
30
40
50
60
70
80
90
100
Pe
rce
nt
Ab
stin
en
tAbstinence Patterns by Treatment Group
100%
50%
0 mg
21 mg
42 mg
p = .05
Garvey et al., 2006
Improving Treatment
• Adjuncts to behavioral and pharmacological treatments may be one solution
• Tailoring treatments to specific population– > WOMEN– Women more fearful of gaining weight– Women report more often negative affectivity
and stress after quitting– Depression and smoking cessation have a
strong association and depression is more common among women

Aerobic Exercise and NRT for Female Smokers - Study
DA12503-01_04 Kinnunen (1999-2003)
•sedentary smokers•ages 18-55•no cardiac Hx•over 5 cigarettes/day
Equal Contact Group (n=56)Wellness Counseling (2 x week)3 wks prequit 16 wks postquitNicotine gumBrief Counseling
Experimental Group (n=92)Aerobic Exercise (2-3 x week)3 wks prequit 16 wks postquitNicotine gumBrief Counseling
Standard Care Control Group (n= 34)_Nicotine gumBrief Counseling
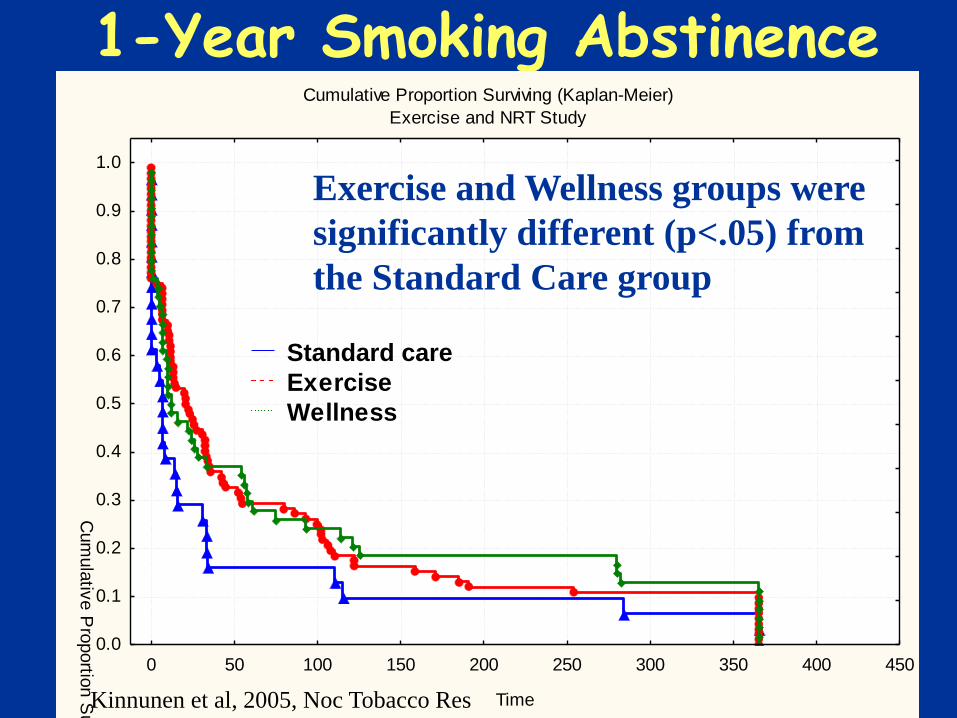
1-Year Smoking AbstinenceCumulative Proportion Surviving (Kaplan-Meier)
Exercise and NRT Study
0 50 100 150 200 250 300 350 400 450
Time
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Cum
ula
tive P
roportio
n S
urv
ivin
g
Standard care
Exercise
Wellness
Exercise and Wellness groups were
significantly different (p<.05) from
the Standard Care group
Kinnunen et al, 2005, Noc Tobacco Res

Conclusions• Exercise promoted smoking cessation beyond
standard care• Exercise had favorable impact on mood • Poor adherence to exercise regimen among
those who had:
Higher nicotine dependence
Higher body mass index
Higher depression level
Higher stress level
Lower education
Korhonen, Kinnunen et al., 2005, Tob Induced Dis
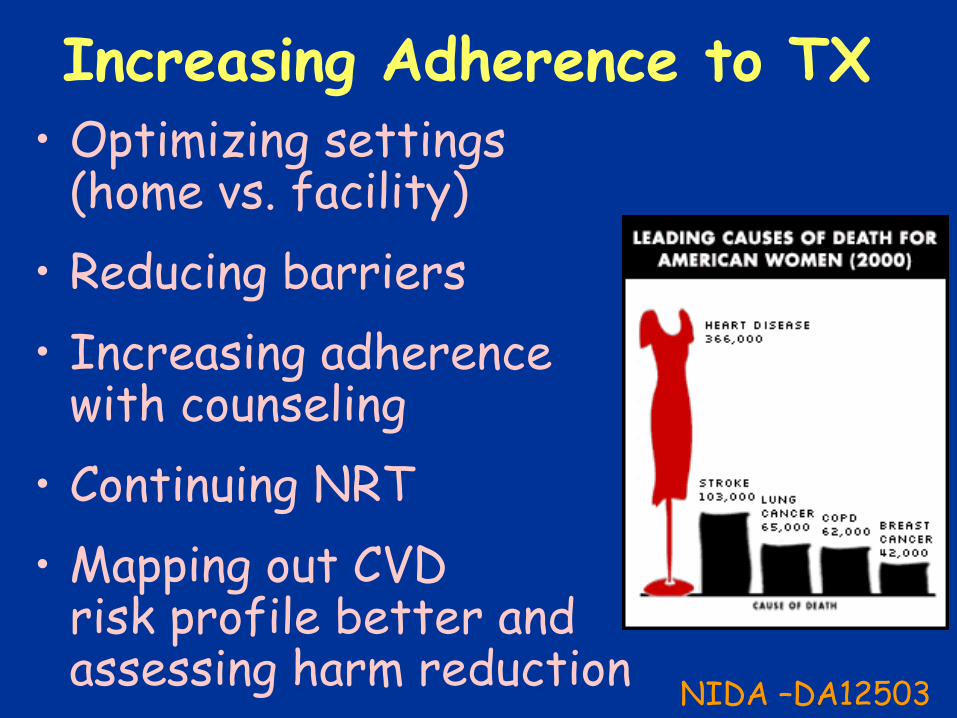
Increasing Adherence to TX• Optimizing settings
(home vs. facility)
• Reducing barriers
• Increasing adherence with counseling
• Continuing NRT
• Mapping out CVD risk profile better and assessing harm reduction
NIDA –DA12503

Future Directions
• Expanding and enhancing behavioral treatments
– (Front-loaded counseling Garvey & Kinnunen, NIDA)
• Discovering new and new combinations of pharmacotherapy
• Immunotherapy – Nicotine vaccine
• Harm reduction

Nicotine Vaccine
• Nicotine vaccine is designed to elicit the production of nicotine antibodies.
If someone smokes after being immunized, the antibodies bind with nicotine molecules in the bloodstream and prevent them from entering the brain where nicotine receptors are located.
Previous research has shown that, since antibody levels rise slowly, smokers lose the nicotine reward gradually, avoiding withdrawal symptoms.
"Quitting smoking is easy.
I've done it a thousand times.“- Mark Twain