
Bacon Spring 2014 Brochure Landscape V3.indd - Bacon Theatre

MULTIPLE MALIGNANT TUMORS, WITH INVOLVEMENT OF THE LOWER BOWEL
REPORT OF MULTIPLE PRIhlARY AND CONTACT GROWTHS *
HARRY E. BACON, M.D., F.A.C.S., F.A.P.S.
(From the Proctologic Departments of the Temple University Hospital, the Graduate Hospital, University of Pennsylvania, and the Radiologic Department of the Philadelphia
General Hospital)
The existence of one or more malignant growths occurring independently of each other has been recognized since Billroth published his first report in 1869. His postulates for the identification of multiple carcinomata as inde- pendent lesions are well known but bear repetition: (1) The two growths should differ histologically to a degree which excludes the possibility of an identical origin, but should be in different stages of development. ( 2 ) Each growth must spring from its parent epithelium. ( 3 ) Each growth must be held responsible for its separate group of metastases. Mercanton added a further evidence of independent growth: (( If, after removal of two carcinomas, the patient remains free from the disease, the two growths must have been independent, else there should have been other metastasis.”
Bunting is of the opinion that Billroth’s postulates were intended to apply only to malignant growths arising in different organs. It is evident that in carcinomas arising from the intestinal epithelium the first of them, at least, cannot well be satisfied, since, as Thompson has said, carcinomatous degen- eration of multiple intestinal polypi is entirely likely.”
What then are the criteria to be employed. What actually constitutes multiple primary malignancy? Neoplasms arising independently of anteced- ent tumor growth are known as primary. Whereas a mutation for tumor usu- ally occurs in a single group of cells-so-called unicentric origin-it cannot be denied that occasionally several groups of cells are involved, giving rise to more than one malignant growth-multicentric or pluricentric origin. For this there are excellent examples, as polyposis of the large bowel and stomach, lymphosarcoma, and multiple myeloma. Multiple malignancy superimposed on an intestinal polyposis, while a distinct entity, is excluded from the present discussion.
The question arises, should these multiple growths be histologically distinct and heterogeneous? It is generally agreed that two tumors which are dis- tinctly different histologically are independent, but it does not necessarily fol- low that histologic similarity implies a single parent tumor from which the other has sprung.
In order to obviate a falsely low incidence of multiple primary malignancy, there has been a tendency to liberalize the original requirements. Those sug- gested by Warren and Gates seem logical and are here cited: ‘(Each of the
1 Read before the American Proctologic Society, San Francisco, June, 1938.
243

244 HARRY E. BACON
TABLE I: Sarcoma and Carcinoma in Diferent Systems
Author
Warren and Gates Landau Werner Nehrkorn Dij kstra Bargen and Rankin (cited also in Table 11)
Type and Organ
Adenocarcinoma, rectum Carcinoma, rectum Adenocarcinoma, rectum Melanotic sarcoma, rectum Spindlecell sarcoma, rectum Adenocarcinoma, sigmoid
Type and Organ
Lymphosarcoma, rectum Fibrosarcoma, breast Fibromyosarcoma, uterus Carcinoma, uterus Carcinoma, gallbladder Sarcoma, uterus
Type and
Organ -- Osteoma, jaw
TABLE I1 : Double Malignancy in the Anus, Rectum and Sigmoid Colon
Author Site Site
Graham Rectum Rectum Kraske Rectum Anus Bargen and Rankin Rectum Sigmoid Morton Rectum Sigmoid Bargen and Rankin Sigmoid Sigmoid Bargen and Rankin Rectum Rectum Bargen and Rankin Rectum Rect um Bargen and Rankin Rectum Sigmoid Bargen and Rankin Rectum Sigmoid Hochenegg Rectum Rectum Robson and Knaggs Rectum Rectum Abel Rectum Pelvic colon Abel Rectum Rectum Lockhart-Mummery Rectum Sigmoid Lockhart-Mummery Rectum Sigmoid Norbury Rectum Rectum Miller Sigmoid Sigmoid Morgan Rectum Sigmoid Papin Rectum Rectum Rotter Rectum Rectum Rotter Rectum Rectum Rotter Rectum Rectum Rotter Rectum Rectum Rotter Rectum Rectum Graham Rectosigmoid Sigmoid Graham Rectum Rectosigmoid Cole Rectum Pelvic sigmoid
tumors must present a definite picture of malignancy; each must be distinct, and the possibility of one being a metastasis of the other must be excluded.” In other words, as Cokkins has said, a good rule to follow is that if two ma- lignant tumors coexist, or follow each other, and it can be definitely established that one is not a metastasis of the other, they must be regarded as primary growths.
The incidence of multiple primary malignancy is variously estimated be- tween 0.6 (Bilello and Montanini) and 4.3 (Medwedjew) per cent of cancer autopsies. We shall, however, consider this subject only in relation to growths in the anus, rectum, and sigmoid colon. The proved cases from the literature are presented in Tables I-VI and seven additional cases axe reported.

Author
Sigmoid Sigmoid Sigmoid Sigmoid
Lane Norbury Dowden Maingot Bargen and Rankin Bargen and Rankin Schmidt Angevine Zimmermann Doering Wulf Miller Bunting Gotting v. Mielecki Jentzer Bargen and Rankin Lauda Goetze Bargen and Rankin Klingenstein
Breast Transverse colon Small intestine Anus
MULTIPLE MALIGNANT TUMORS
TABLE I1 I : Three or More Malignant Lesions
Site 1 Site 1 Site
Rectum Rectum Rectum Rectum
Three sep, Rectosigmoic Rectum Rectum Rectum Rectum Rectum Rectum Sigmoid Rectum Rectum Rectum Sigmoid Rectum Rectum Sigmoid Sigmoid
Rectum Rectum Rectum Sigmoid Rectum Hepatic flexure Hepatic flexure Cecum Stomach Stomach Stomach Ascending colon Esophagus Stomach Cecum Ascending colon
- Rectum Sigmoid Anus Left adrenal Hepatic flexure Splenic flexure Transverse colon Ileum Larynx Larynx Orbit Splenic flexure Bile duct Prostate Transverse colon Transverse colon
245
Site
Uterus (sa.) Tonsil Colon Splenic flexure Uterus
In multiple growths limited to a small portion of the bowel and of the same histologic type, a multicentric origin may be difficult or impossible of proof. Such growths may occur by direct contact, a detached fragment of the pri- mary lesion being engrafted elsewhere. Three cases (VIII, IX, and X) are reported here.
CASE I. G. S., a white man aged thirty-seven, was admitted to Temple University Hos- pital Jan. 18, 1937, because of epigastric pain, increasing constipation, and loss of weight. His illness had begun late in 1935 with abdominal discomfort, especially after meals, and at- tacks of belching. There had been no nausea or vomiting, but the patient had lost 20 pounds in weight in eight months and more recently there had been some bleeding from the rectum. Gastric analysis a t another hospital in July 1936 had shown a low content of free and total hydrochloric acid and the presence of occult blood; it was negative for lactic acid, bile and starch. Roentgen examination a t the same time showed an hour-glass appearance a t the pyloric end of the stomach and an old ulcer was suspected. A second x-ray study about two months later showed the stomach to be normal, though emptying fairly rapidly. The head of the barium at that time was in the descending colon, with a spastic transverse colon. No six-hour retention was demonstrable a t either examination. I n the early part of January 1937, the patient was seized with violent pain in the abdomen, which was unrelieved by medication or enemas. His stools were described as " ribbon-like."
On admi?sion the abdomen was greatly distended. Rectal palpation revealed a cauli- flower mass three inches above the anal margin. The diagnosis was intestinal obstruction due to a malignant growth in the rectum.
On Jan, 19, 1937, an appendicostomy was performed under spinal analgesia, and three weeks later an exploratory operation revealed a hard, constricting annular mass in the mid- stomach, in addition to the rectal growth. The patient was discharged in February to the diagnostic clinic, where he was re-examined a t weekly intervals. On March 3 he was referred to the Radiologic Department of the Philadelphia General Hospital because of chronic in- testinal obstruction. X-ray examination on April 6, by Dr. H. Ostrum, showed the stomach to be contracted, fibrosed, rigid, and fixed. I t emptied rapidly into the dilated small in- testine. No peristalsis was demonstrable, and a two-hour study showed only a trace of

246 HARRY E. BACON
TABLE IV: Dual Malignancy of the Gastro-intestinal Tract
Author Site Site
Junghanns Rectum Colon Klister Rectum Colon Lockhart-Mummery Rectum Colon Lockhart-Mummery Rectum Colon Norbury Rectum Colon Warren and Gates Rectum Colon Norbury Rectum Transverse colon Handford Rectum Splenic flexure Eliot Sigmoid Splenic flexure Bargen and Rankin Rectum Cecum Bargen and Rankin Sigmoid Ascending colon Abel Pelvic colon ’ Descending colon Karsner and Clark Sigmoid Descending colon Behrend Rectum Ascending colon Lockhart-Mummery Rectum Transverse colon Littlewood Rectum Splenic flexure Littlewood Rectum Ascending colon Cokkins Pelvic sigmoid Transverse colon Cokkins Pelvic sigmoid Descending colon Cokkins Rectosigmoid Transverse colon Goriainowa and Schabad Sigmoid Stomach Hauser Sigmoid Stomach Pemberton and Waugh Sigmoid Stomach Hauser Rectum Stomach Orr Rectum Stomach Rau Rectum Stomach Judd and Phillips Rectum Stomach Feilchenfeld Rectum Stomach Hanlon Rectum Stomach v. Hansemann Rectum Stomach Orr Rectum Stomach Lockhart-Mummery Rectum Stomach Kr6ger Rectum Stomach Devic and Gallavardin Rectum Pylorus Robson and Knaggs Rectum Jejunum Lockhart-Mummer y Rectum Pylorus deVries Rectum Stomach Deetz Rectum Gallbladder Brandt and Jekabson Rectum Pancreas Nicholls Rectum Pancreas Mliller Rectum Pancreas Maingot Sigmoid Stomach
barium in the stomach; both the small and large bowel were distended, and a portion of the small bowel, probably the mid-ileum, was distended by barium. A twenty-hour study showed a good outline of the entire colon, distended but with no gross defects. The diagnosis was scirrhous carcinoma of the stomach with metastasis to the peritoneum and generalized car- cinomatosis of the abdomen.
A biopsy report on the rectal growth, by Dr. R. P. Custer, April 30, was as follows: ‘‘ The hyperplastic rectal mucosa is markedly edematous but seems intact over the surface. The submucosa, however, is infiltrated by groups and strands of hyperchromatic epithelium which is markedly anaplastic and distinctly invasive. Adenocarcinoma.” Partial decom- pression was obtained by cecostomy and Wangensteen’s suction technic. Beginning March 26 roentgen therapy was given, 1100 t being administered through four portals, but the weak- ened condition of the patient precluded further therapy. Death occurred June 14, 1937.
Autopsy disclosed a primary adenocarcinoma of stomach grade IV; primary adeno- carcinoma of the rectum grade 11; secondary carcinoma of the peritoneum, diaphragm, small and large intestine (subserosal), bladder, sacrum, and coccyx.

Stomach Rectum
FIG. 1. CASE I: CARCINOMA OF STOMACH AND RECTUM The roentgenograms show the narrowing of the gastric lumen and the irregular filling defect,
particularly in the region of the cardia and pars media. produced by extensive infiltration of the stomach walls by carcinoma.
The photomicrograph to the left shows a small portion of the gastric mucosa, submucosa and muscle coat. Note the extension of malignant tumor composed of tall, columnar cells with hyper- chromatic nuclei arranged to form atypical glands. Other parts of the tumor show pleomorphism with numerous giant cells, some of which can be seen near the center. There is some degeneration with inflammatory infiltration. In other portions of the muscle, small nests of relatively undiffer- entiated, rapidly growing pleomorphic epithelial cells can he seen. Mitotic figures are numerous.
The photomicrograph to the right shows a portion of rectal mucosa with its hyperchromatic glands and secondary reaction in the submucosa and muscular layer, which is being invaded by cords of epithelial cells that occasionally show a tendency toward glandular arrangement. The nuclei are large and hyperchromatic; cells are epithelial in origin but rather undifferentiated. The stroma is abundant and has undergone myxomatous degeneration. The rapid invasive qualities of the tumor may be recognized by the diffuse infiltration.
247

TABLE V: Multiple Malignancy of the Lower Iwtestinal Tract and the Genito-urinary System
Author Intestinal Site Genito-urinary Tumor
Bilz Sigmoid Carcinoma, uterus Hanlon Sigmoid Adenocarcinoma, uterus Lockhart-Mummery Rectum Carcinoma, uterus Fried Anus Epid&poid carcinoma, cervix Warren and Gates Rectum Epidermbid carcinoma, cervix Warren and Gates Rectum Epidermoid carcinoma, cervix Hanlon Rectum Papillary carcinoma, fallopgn tube Scharlieb Rectum Papillary ckrcinoma, both aiar ies Gouillioud Sigmoid Cylindric-cell carcinoma, ovary Rau Rectum Carcinoma, ovary Tanberg Rectum Adenocarcinoma, kidney I*
Hanlon Rectum Tubular carcinoma, kidney Hanlon Sigmoid Tubular carcinoma, kidney Bilz Rectum Carcinoma, kidney Hanlon Rectum Tubular carcinoma, kidney Hanlon Rectum Carcinoma, kidney Hanlon Anus (basal-cell) Adenocarcinoma, prostate Junghanns Rectum Carcinoma, prostate Miiller S i g m o i d Adenocarcinoma, prostate Hanlon Rectum Epidermoid carcinoma, penis Hanlon Sigmoid Epidermoid carcinoma, penis Nehrkorn Anus (squamous-cell) Carcinoma, bladder
TABLE VI: Miscellaneous Cases
Author Intestinal Site Other Tumor
Junghanns Bile110 and Montanini Carnevale-Ricci Ophiils Rau Rau Rau Kaufmann Hanlon Klebs de Besche Hanlon deVries Gottstein Eliot Lockhart-Mummery Norbury Norbury Kesteven Lockhart-Mummery Eliot Hanlon Williams Seecof Lockhart-Mummery MIiller v. Volkmann Warren and Gates Hibshman
Rectum Rectum Rectum Rectum Rectum Rectum Rectum Rectum Sigmoid Rectum Rectum Rectum Rectum Rectum Sigmoid Rectum Rectum Rectum Rectum Anus Rectum Rectum Rectum Rectum Rectum Rectum Rectum Rectum Rect,um
Carcinoma, esophagus Carcinoma, esophagus Epidermoid, esophagus Carcinoma, esophagus Carcinoma, esophagus Carcinoma, esophagus Carcinoma, esophagus Carcinoma, orbit Basal-cell carcinoma, face Carcinoma, eyelid Carcinoma, lip Epidermoid carcinoma, lip Epidermoid carcinoma, tongue Epidermoid carcinoma, tongue Carcinoma, breast Breast Breast Breast Breast Breast Breast Breast Breast Carcinoma, lung Carcinoma, bronchus Epidermoid carcinoma, bronchus Carcinoma, skin of buttocks Basal-cell carcinoma, skin Tongue
248

2 49 MULTIPLE MALIGNANT TUMORS
FIG. 2. CASE 11: ADENOCARCINOMA OF THE COLON AM) SQUAMOUS-CELL EPITHELIOMA OF THE LIP The roentgenogram shows the filling defect at the junction of the descending and sigmoid colon. The photomicrograph to the left shows a portion of the intestinal wall with masses of tumor
cells which are arranged in a glandular pattern. Many of the cells are tall columnar and appar- ently line spaces. There is, however, no basement membrane. Occasional mitotic figures are seen. In other areas the cells form solid masses.
The photomicrograph to the right shows the superficial layers of the lip. The epidermis shows hyperplasia with marked keratinization ; the epithelial pegs are irregular with definite extension as a malignant tumor into the subcutaneous tissue. Note transition from the stratified squamous epithelium to definite epidermal carcinoma.
CASE 11: J. D., a white male aged sixty-one, was referred to the Proctologic Clinic of Temple University Hospital Dec. 15, 1937, because of rectal bleeding and abdominal pain. The patient stated that during the past year he had suffered from constipation, which had be- come progressively worse, necessitating the use of laxatives once or twice daily. During the past few weeks he had experienced a griping pain in the left lower abdomen, which was not relieved by medication. A past history of gonorrhea and syphilis was mentioned. For the latter he had received intensive therapy. H e had been treated for cancer of the lip in April 1935, with extensive radium therapy to the local and cervical node region. The biopsy re- port was cornifying squamous-cell carcinoma.

250 HARRY E. BACON
Sigmoidoscopic examination was negative but palpation of the abdomen showed the presence of a hard, sausage-shaped mass in the left lower quadrant, its upper border ex- tending to the crest of the left ilium. Roentgen examination by Dr. W. E. Chamberlain demonstrated a partial obstruction of the lower descending portion of the colon, a t which point there was a palpable mass apparently fixed to the inner surface of the left ileum. This was believed to be a carcinoma.
The patient was admitted to Temple University Hospital Dec. 18, 1937. Two days fol- lowing admission he was seized with cramps in the abdomen. A diagnosis was made of par- tial obstruction, and exploration, Dec. 30, revealed an annular, scirrhous growth at the junc- tion of the descending and sigmoid colon. A three-stage Mikulicz procedure was performed. The subsequent course was uneventful and the patient was discharged Jan. 20, 1938. The microscopic report, by Dr. E. E. Aegerter, is as follows: ‘ I The mucosal glands show malig-
f
I
FIG. 3A. CASE Iv: CARCINOMA OF THE SICMOD ASSOCIATED WITH ESOPHAGEAL CARCINOMA SHOWN IN FIG. 3B: MUSCLE COAT OF THE SIGMOUJ SHOWING INFILTRATION BY MALIGNANT
ADENOCARCINOMA Note imitation of the normal glandular structure made up of rather gigantic feathery columnar
cells, ,in which deep hyperchromatic nuclei are seen. No basement membrane; many mitotic figures. No evidence of degeneration or softening with inflammatory reaction.
nant hyperplasia and extension downward into the mucosa to form pseudo-acini of carcinoma- tous tissue. The two polyps do not show neoplastic change. Diagnosis : adenocarcinoma.”
CASE 111: H. B., a white man aged seventy-nine, was admitted to the Philadelphia Gen- eral Hospital in March 1922, because of a small keratotic patch at the junction of the nose and cheek, which had been present for two years. Its dimensions were 2.5 cm. a t the nose, 2 cm. a t the center of lesion, and 4 cm. at the outer edge. The biopsy report, by Dr. Joseph McFarland, was as follows: ‘I One edge of the specimen shows very much thickened skin with surface cells hornified. At the opposite edge is normal skin. At one point on the thickened skin the basal cells have broken through these confines and are invading the corium. The corium and subcutaneous tissue show irregularly arranged groups of epithelial cells of the basal type; these cells vary in size, shape, and staining qualities and show mitotic figures. One pearl is seen. Diagnosis: Basal-cell carcinoma.” Radium therapy was given: a total of 1304 mc. hr. of radium, with 1 mm. aluminum filter.
MULTIPLE MALIGNANT TUMORS 251
Four years later the patient was referred to the Radiologic Department by his family physician because of bleeding from the rectum. He gave a history of passing blood for a period of thirteen months, change in bowel habit, incomplete evacuation, discomfort a t stool, and some loss of weight. On examination a large, spongy mass involving the lower portion of the rectum was found. The histologic report, by Dr. J. Golforth, was as follows: “ E x - tensive invasion of malignant cells reproducing gland-like structures ; many mitoses ; sec- ondary infection with ulceration-adenocarcinoma.” Operation and roentgen therapy were refused. Death occurred two years later. No autopsy was performed.
CASE IV: J. R., a white male aged seventy-two, was referred to the Philadelphia Gen- eral Hospital, April 6, 1938, with a diagnosis of ‘ I organic lesion of the esophagus, probably carcinoma.” He complained of difficulty in swallowing, which had begun three months pre- viously. Regurgitation occurred approximately one-half hour after ingestion of solid food.
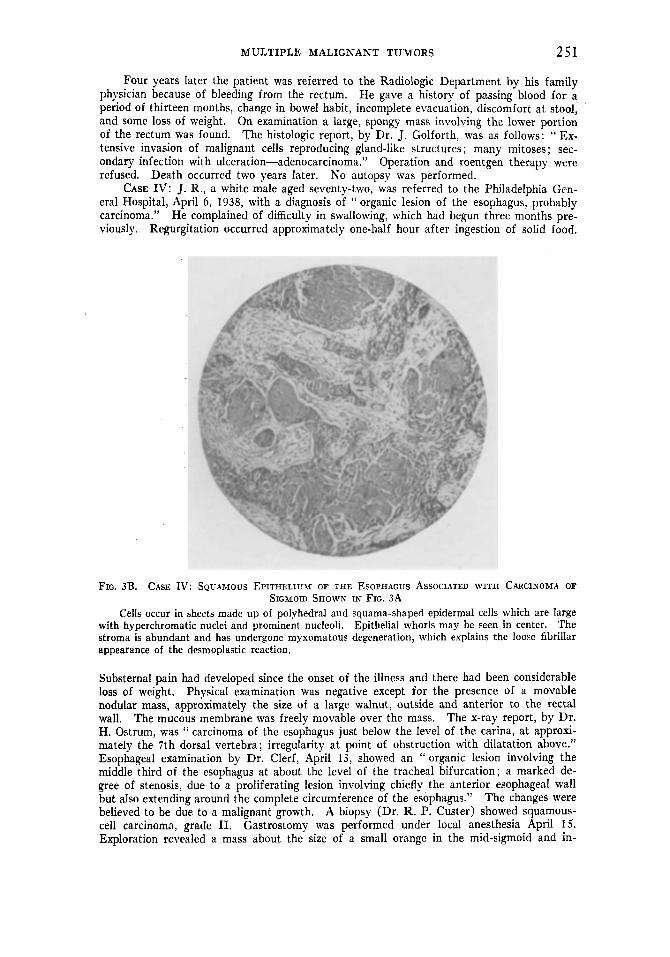
FIG. 3B. CASE IV: SQUAMOUS EPITHELIUM OF THE ESOPHAGUS ASSOCIATED WITH CARCINOMA OF
Cells occur in sheets made up of polyhedral and squama-shaped epidermal cells which are large with hyperchromatic nuclei and prominent nucleoli. Epithelial whorls may be seen in center. The stroma is abundant and has undergone myxomatous degeneration, which explains the loose fibrillar appearance of the desmoplastic reaction.
SIGMOID SHOWN IN FIG. 3A
Substernal pain had developed since the onset of the illness and there had been considerable loss of weight. Physical examination was negative except for the presence of a movable nodular mass, approximately the size of a large walnut, outside and anterior to the rectal wall. The mucous membrane was freely movable over the mass. The x-ray report, by Dr. H. Ostrum, was ‘‘ carcinoma of the esophagus just below the level of the carina, a t approxi- mately the 7th dorsal vertebra; irregularity a t point of obstruction with dilatation above.” Esophageal examination by Dr. Clerf, April 13, showed an “ organic lesion involving the middle third of the esophagus at about the level of the tracheal bifurcation; a marked de- gree of stenosis, due to a proliferating lesion involving chiefly, the anterior esophageal wall but also extending around the complete circumference of the esophagus.” The changes were believed to be due to a malignant growth. A biopsy (Dr. R. P. Custer) showed squamous- cell carcinoma, grade 11. Gastrostomy was performed under local anesthesia April 15. Exploration revealed a mass about the size of a small orange in the mid-sigmoid and in-

252 HARRY E. BACON
volving the mesosigmoid. Autopsy, twelve days later, disclosed an extensive carcinoma of the esophagus and a large adenocarcinoma, grade 111, of the sigmoid approximately 35 cm. above the anal margin. The growth had prolapsed into the rectovesical pouch.
CASE V : S. L., a white male, aged eighty, was admitted to the Graduate Hospital July 6, 1934, complaining of intractable itching about the anus, for which he had consulted a num- ber of physicians without relief. The itching had been present for about a year and seemed to be getting worse. There had been occasional bleeding and protrusion at the time of stool. No change of bowel habit was mentioned. Examination revealed a large cauliflower mass in the rectum, biopsy of which showed adenocarcinoma. The abdomen was explored and a double-barreled colostomy established. The rectal growth was later fulgurated. Radium, 150 mg. filtered through 2.0 mm. of platinum, was given for forty-eight hours. The patient
FIG. 4. CASE VI: ADENO~ARCINOMA OF THE RECTUM AND OF THE STOMACH There is evidence of a marked degree of obstruction in the lower sigmoid colon and upper
The cuff-like enclosure of the pars media of the stomach just below the cardia is very charac- rectum.
teristic of neoplastic growth.
was subsequently discharged but continued to have attacks of diarrhea. Following extensive roentgen therapy he improved and gained weight. One year later the rectum was smooth in outline and showed no evidence of the malignant process. The patient was so dissatisfied, however, with the abdominal anus, that the bowel was closed by the extraperitoneal method. In 1937 a “ s o r e ” appeared on the tongue, subsequent biopsy of which was reported squamous-cell carcinoma, grade IV.
CASE VI: D. D.. a white male forty-one years of age, was admitted to the Temple Uni- versity Hospital April 21, 1938, because of difficulty in swallowing of five months’ duration, indigestion for five years, gaseous distention, progressive constipation, and rectal bleeding. An annular growth almost occluding the lumen of the ampulla was palpable per rectum. Biopsy showed this to be an adenocarcinoma of the rectum. Gastro-intestinal studies re- vealed a cuff-like enclosure of the pars media of the stomach just below the cardia, very characteristic of a neoplasm, and a marked degree of obstruction in the lower sigmoid colon
Extensive radium therapy was given.

MULTIPLE MALIGNANT TUMORS 253
and upper rectum. Exploratory laparotomy performed by Dr. W. W. Babcock disclosed a nodular growth in the rectosigmoid; in addition there was a large mass involving the greater curvature and anterior wall of the stomach, extending close to the cardia. The more massive growth was located in the stomach.
CASE VII: S. Q., a physician aged fifty, was admitted to the service of Dr. W. W. Bab- cock at Temple University Hospital Feb. 16, 1938, because of pain in the right upper quad- rant. For a period of three months the attacks occurred in the epigastrium but radiated to the right upper abdomen. They were associated with fever, 101' to 102" F. There was no jaundice and the stools were not clay-colored. The patient had had an appendicostomy in 1911, and a perineal proctectomy in 1929, a t which time the diagnosis had been adeno- carcinoma.
With a clini- cal diagnosis of cholecystitis, the abdomen was opened through a transverse muscle-splitting incision and a carcinoma involving the ampulla of the gallbladder found. A cholecystectomy was performed.
The diagnosis was adenocarcinoma of the stomach.
On examination, a hard mass was palpable in the region of the gallbladder.
The three cases of possible contact malignancy are as follows
CASE VIII: J. S., a white male aged seventy-seven, was admitted to the Philadelphia General Hospital March 11, 1937, because of pain in the abdomen. H e had enjoyed good health until the previous January, when he experienced distress in the upper abdomen, oc- curring usually fifteen minutes to half an hour after eating. Medication afforded no relief. There was no nausea or vomiting. For the past month the stools, numbering one or two daily, had been liquid; for almost a year they had been of small caliber. No bleeding or tarry stools were reported, although occasionally there was some discomfort a t defecation. Two years ago the patient had weighed 122 pounds and he was sure that he had lost no weight. One brother had died of bowel trouble; age unknown.
The patient was moderately emaciated, with evidence of arteriosclerotic cardiovascular disease. Rectal examination disclosed a circular ridge in the lower rectum, which would not permit entrance of the finger. Gastro-intestinal x-ray study following a barium meal showed the left lobe of the liver enlarged, producing a smooth depression on the lesser curvature of the stomach. There was considerable distention of the jejunum and upper ileum, seen best a t the end of three hours. The distribution of barium in the small in- testine was suggestive of a metastatic process in the abdomen and liver.
Under nitrous oxide anesthesia the stenosis was dilated and a large fungating mass encountered on the anterior rectal wall, 3 inches above the sphincter. The biopsy report, by Dr. R. P. Custer, was as follows: I ' The fragments are composed of tumor which shows rough tubular gland formation and the presence of slender feathering villi on the surface. The epithelium is of fairly well differentiated columnar type in pseudo-stratified arrangement, mitotic figures averaging less than one per high-power field. Adenocarcinoma, grade 11." I t was decided to transfer the patient to the Radiologic Department, but bronchopneumonia developed and he died seven days following admission to the hospital.
Autopsy revealed three separate carcinomas : one circumferential growth at the recto- sigmoid junction; another of approximately the same size in the rectum, involving the ante- rior and lateral walls; one in the lower rectum immediately above the anorectal line, in- volving approximately half the circumference. Histologically all were adenocarcinoma, grade 11. Serial section of the bowel wall between the growths showed no malignant growth. Ex- tensive secondary involvement was found in the liver. Examination of the entire large bowel disclosed no evidence of polyposis.
CASE IX: T. S., a white male aged eighty-three, was admitted to the Radiologic Depart- ment of the Philadelphia General Hospital Jan. 7, 1937, because of diarrhea, the stools num- bering about nine per day. For a period of twelve months he had been passing blood a t defecation. During the past nine months constipation had alternated with diarrhea, and more recently complete evacuation had been impossible. The caliber of the stools had changed in character, but no pain nor discomfort had been experienced at any time. Exam- ination of the rectum revealed a large fungating mass on the right lateral wall, approximately

254 HARRY E, BACON
10 cm. above the anorectal line. In the lower rectum was a moderate degree of hemorrhoidal tissue, with definite nodule formation. Microscopically the upper specimen showed a hyper- plastic rectal mucosa undergoing abrupt transition to tumor, which formed tubular glands in some areas’and solidly cellular sheets in others. The cells were of poorly differentiated co- lumnar epithelial type, averaging one mitotic figure per high-power field. The lower tumor was of the same variety, the cells being perhaps slightly better differentiated. Both were di- agnosed adenocarcinoma, grade 111. Another description of the lower growth was as follows: “ The section consists of a portion of rectal mucosa in the center of which is a circumscribed collection of large tumor cells with pale vesicular nuclei arranged in perpendicular layers and forming moderately well differentiated glands. Mitotic figures average 1 per high-power field.” Roentgen study following a barium enema showed no evidence of disease in the colon. Because of the poor condition of the patient, operation was not advised, but roentgen therapy
Case VIII Case IX Case X
FIG. 5 . C ~ S E S VIII, IX AND X: SO-CALLED CONTACT MALIGXANCY The specimen from Case VIII shows three lesions: one at the rectosigmoid junction; another,
the largest, in the lower ampulla; a third immediately above the anorectal line. The proctoscopic view, from Case IX, shows two malignant neoplasms, The specimen from Case X shows two crater-like ulcerations in the rectum, separated distinctly
from each other. Both are adenocarcinoma, Grade 11.
was instituted, a total of 3600 r being given to the tumors through four portals. Autopsy disclosed two lesions in the lower rectum. The colon was free of polyposis.
CASE X : H. F., a white male aged fifty-three, was admitted to the Temple University Hospital March 23, 1938, because of chronic constipation, “ spotting,” pain on sitting, and frequency of urination. He stated that he had been in good health until six months before, a t which time he noticed blood following defecation, usually bright red in color. Constipa- tion, present for many years, had become worse during the past twenty-four months. There had been a dull aching pain for three months and frequency of urination for two. Physical examination was negative except as it revealed two separate and distinct growths-one on the posterior wall of the rectum and another on the left lateral wall a t a slightly lower level. On March 29 a one-stage abdominoperineal excision was performed with a perineal colostomy. The report by Dr. Aegerter described the specimen as consisting of approximately 22 cm. of the lower intestine including the anal region. About 3 cm. from the anal sphincter was a cauliflower-like lesion 3.5 cm. X 4 cm. in diameter, the edges of which were raised, firm, and

MULTIPLE MALIGNANT TUMORS 255
partly ulcerated. Above and to the side of this was another similar lesion, measuring 4 X 3.5 cm., the edges of which were not quite as prominent as the other though the central part was inore ulcerated. These lesions were separated by about 2.5 cm. of normal-appearing mucosa. Microscopic sections taken from the border of the rectal tumors revealed a characteristic adenocarcinomatous lesion. The acini and granular structures were considerably distorted and many were greatly enlarged. The cells were fairly characteristic and showed a few mi- totic figures. There was a fairly marked desmoplastic reaction in the region of the tumor growth. Diagnosis : Adenocarcinoma of rectum. The patient made an uneventful recovery.
SUMMARY
The literature on the occurrence of multiple primary malignant lesions with involvement of the anus, rectum, or sigmoid (omitting malignant polypo- sis) has been reviewed. There are reported 145 cases with one or more of multiple growths in this locality. These include 2 7 instances of dual car- cinomata and 5 instances of triple carcinomata confined to the anus, rectum and sigmoid colon. In a somewhat greater number other portions of the gastro-intestinal tract were involved and in a few instances growths were pres- ent in systems unrelated to the rectum and sigmoid.
Seven additional cases are presented, and three others (Cases VIII, IX and X) in which there was no absolute proof of a multicentric origin, are re- ported as possible examples of " contact " cancer.
Carcinoma and sarcoma in the same individual appear prone to occur in systems unrelated to each other (see Table I ) .
The following conclusions are reached: (1) it must be recognized that ma- lignancy, excluding cancerous alteration in intestinal polyposis, may be multi- centric in origin; further, that this is by no means a rarity; ( 2 ) in cases where two or three malignant and apparently primary growths are confined to a relatively small segment of bowel, approximately the same size and showing the same histologic characteristics as well as grade, multicentric origin may be, and often is, as is Cases VIII, IX and X, extremely difficult to determine.
BIBLIOGRAPHY
ABEL. A. L.: Proc. Roy. SOC. Med. 22 (Sect. Surg.): 1330, 1928-29. ANGEVINE, D. M.: Canadian M. A. J. 23: 38, 1930. BARGEN, J. A., AND RANKIN, F. W.: Ann. Surg. 91 : 583, 1930. BEHREND, M.: Surg., Gynec. & Obst. 65: 505, 1937. BILELLO, A., AND MONTANINI, N.: Tumori 5: 369, 1931. BILLROTH, T. : Chirurgische Klinik, Berlin, A. Hirschwald, 1869, p. 142. BILZ, G.: Ztschr. f . Krebsforsch 19: 282, 1923. BRANDT, M., AND JEKABSON, K.: Ztschr. f . Krebsforsch. 32: 280, 1930. BUNTING, C. H. : Bull. Johns Hopkins Hosp. 15 : 389, 1904. CARNEVALE-RICCI, F.: Arch. ital. di otol. 42: 265, 1931. COKKINS, A. J.: Brit. J. Surg. 21 : 570, 1934. COLE, P. P.: Brit. M. J. 1 : 431, 1913. DE BESCHE, A.: Norsk. mag. f . laegevidensk. 5: 533, 1908. DEETZ, E.: Virchows Arch. f . path. Anat. 164: 381, 1901. DEVIC, E., AND GALLAVARDIN: Bull. SOC. mCd. d. h8p. de Lyon 2 : 242, 1903. DE VRIES, W. M.: Nederl. tijdschr. v. geneesk. 1: 961 and 2 : 1258, 1912. DIJKSTRA, 0. H.: Nederl. tijdschr. v. geneesk. 2 : 270, 1926. DOERING, H.: Arch. f . klin. Chir. 83: 194, 1907. DOWDEN, J. W.: Edinburgh M. J. 19: 1S1, 1917.

256 HARRY E. BACON
ELIOT, E., JR.: Tr. Am. Surg. Assoc. 40: 115, 1922. FEILCHENFELD: Inaug. Diss., Berlin, 1901. FRIED, B. M.: Arch. Path. 5: 565, 1928. GOTTING: Ztschr. f. Krebsforsch. 7: 675, 1909. GOETZE, 0.: Ztschr. f . Krebsforsch. 13: 281, 1913. GOTTSTEIN: Quoted by Warren and Gates. GORIAINOWA, R. W., AND SCHABAD, L. M.: Ztschr. f . Krebsforsch. 33: 594, 1931. GOUILLIOUD, C.: Zentralbl. f . Gynak. 31 : 1426, 1907. GRAHAM, S.: Personal communication, Dec. 10, 1937. HANDFORD, H.: Tr. Path. SOC. London 41 : 133, 1890. HANLON, F. R.: Am, J. Cancer 15: 2001, 1931. v. HANSEMANN : Ztschr. f . Krebsforsch. 1 : 183, 1904. HAUSER, G. : Das Cylinderepithelcarcinom des Magens und Dickdarms, G. Fischer, Jena,
HIBSHMAN, H. Z. : Personal communication. HOCHENEGG, J.: Wien. med. Wchnschr. 5: 241, 1900. JENTZER, A.: Rev. mCd. de la Suisse Rom. 40: 236, 1920. JUDD, E. S., AND PHILLIPS, J. R.: Surg. Clin. North America 14: 525, 1934. JUNGHANNS, H.: Ztschr. f . Krebsforsch. 29: 623, 1929. KARSNER, H. T., AND CLARK, B., JR.: Am. J. Cancer 16: 958, 1932. KAUFMANN, C.: Virchows Arch. f . path. Anat. 75: 317, 1879. KESTEVEN, W. B.: Tr. Clin. SOC. London 9: 77, 1876. KLEBS, E. T. A.: Handbuch der path. Anat. 2 : 190, 1869. KLINGENSTEIN, P.: Ann. Surg. 102: 1079, 1935. KRASKE, P.: Zentralbl. f . Chir. 11: 801, 1884. KROGER: Cited by Rieder in Arch. f . klin. Chir. 135: 719, 1925. KUSTER: Ein chirurgisch Triennium, 1882, p. 161. Centralbl. f . d. Krankh. d. Harn-u. Sex.-
LANDAU, H. : Munchen. med. Wchnschr. 52 : 650, 1905. LANE, W. A.: Lancet 2: 1184, 1920. LAUDA, E.: Wien. med. Wchnschr. 75: 1890, 1925. LITTLEWOOD: Cited by Yeomans, F. C., in Proctology, D. Appleton 8z Co., New York, 1929. LOCKHART-MUMMERY, J. P.: Diseases of the Rectum and Colon, Wm. Wood & Co., Balti-
LOCKHART-MUMMERY, J. P.: Proc. Roy. SOC. Med. 24: 198, 1930. MAINGOT, R.: Tr. Med. SOC. London 50: 121, 1927. MAINGOT, R.: Brit. M. J. 1: 118, 1938. MEDWEDJEW: Mediz. d. Gegenwart No. 9, 1924. MERCANTON, F.: ThCse de Lausanne, 1893; also in Rev. m6d. de la Suisse Rom. 13: 173,
v. MIELECKI, W.: Ztschr. f . Krebsforsch. 13: 505, 1913. MILLER, R. T.: Ann. Surg. 80: 456, 1924. MORGAN, C. N.: Proc. Roy. SOC. Med. 24: 207, 1930. MORTON, C. A.: Lancet 1: 1245, 1895. MULLER, R. F.: Ztschr. f . Krebsforsch. 31: 339, 1930. NEHRKORN: Munchen. med. Wchnschr. 48: 581, 1901. NICHOLLS, A. G.: Montreal M. J. 32: 326, 1903. NORBURY, L. E.: Proc. Roy. SOC. Med. 24: 198, 1930. OPHULS, W.: A Statistical Survey of 3,000 Autopsies, Stanford Univ. Press, 1926, p. 316. ORR, J. W.: J. Path. & Bact. 33: 283, 1930. PAPIN, F.: Gaz. hebd. sc. mCd. de Bordeaux 52: 41, 1931. PEMBERTON, J. DE J., AND WAUGH, J. M.: Surgery 2 : 211, 1937. RAU, W.: Ztschr. f . Krebsforsch. 18: 141, 1922. ROBSON, A. w. M., AND KNAGGS, R. L.: Lancet 1 : 640, 1905. ROTTER, J.: in v. Bergmann and Bruns: Handbuch der prakt. Chir., F. Enke, Stuttgart, 3:
SCHARLIEB, M. A,: Proc. Roy. SOC. Med. 4: 358 (Obstet. & Gynaec. Sect.), 1911.
1890; Beitr. z. path. Anat. u. z. allg. Path. 33: 1, 1903.
Org. 8: 583, 1897.
more, 2nd ed., 1934, pp. 314, 534.
1893.
580, 1903. Arch. f . klin. Chir. 58: 357, 1899.

MULTIPLE MALIGNANT TUMORS 257
SCHMIDT: Inaug. Diss., Kiel, 1901. SEECOF, D. P.: J. Cancer Research 8: 213, 1924. TANBERG, A.: Norsk. mag. f . laegevidensk. 4: 983, 1906.
v. VOLKMANN, R.: Beitrage zur Chirurgie, Leipzig, Breitkopf & Hartel, 1875, pp. 358, 359. WARREN, S., AND GATES, 0.: Am. J. Cancer 16: 1358, 1932. WERNER, J. L.: Tr. Am. Proc. SOC. 1937, p. 64. WILLIAMS, C.: Virginia M. Month. 58: 24, 1931. WULF: Inaug. Diss., Kiel, 1892. ZIMMERMAN, R. : Canadian J. M. Sc. 7 : 390, 1882.
THOMPSON, J. W.: J. A. M. A. 107: 1688, 1936.


















