
Hand Transplantation - Hand...
9
Hand Transplantation Scott M. Tintle, MD Benjamin K. Potter, MD River M. Elliott, MD L. Scott Levin, MD Investigation performed at the University of Pennsylvania, Philadelphia, Pennsylvania COPYRIGHT © 2014 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED » Upper extremity limb loss is catastrophic. It affects nearly every activity of daily living, leaving patients with substantial disability. » Despite high rates of rejection of upper extremity prostheses, hand transplantation remains controversial. » The indications for hand transplantation remain relatively ill defined. » The American Society for Reconstructive Transplantation (ASRT) and the International Registry on Hand and Composite Tissue Transplan- tation (IRHCTT) have been founded to advance the science, to educate, to report outcomes, and to define the indications for vascularized composite allotransplantation. U pper extremity loss repre- sents a life-changing, often devastating event, affecting nearly every activity of daily living and subsequently leaving a patient with substantial disability 1,2 . The potential immediate dependency and despair result- ing from the loss of one or both hands cannot be overstated. Promising techno- logical advances in upper extremity pros- theses include improved neural-control interfaces, multiple-degrees-of-freedom terminal devices, and prototype haptic feedback mechanisms 3,4 . However, the available literature still demonstrates high prosthesis rejection rates for upper ex- tremity amputees 5-12 , suggesting that prostheses continue to inadequately repli- cate the complex, prehensile functions of the native hand and arm. The most com- monly cited reasons for upper extremity prosthesis rejection remain limited useful- ness, weight, and residual limb discomfort 5,13 . Pioneers of hand transplantation rec- ognized that prosthetic devices probably would never completely satisfy the upper extremity amputee for these very reasons. Even if the prehensile function and dex- terity of the human hand could be restored, these would do little to restore patient body image or hand sensibility, both traits coveted by amputees. Rather, they postu- lated that these could only be replaced with “like” human tissue 14 . The field of vascu- larized composite allotransplantation has grown from this basic desire to fully restore both the functional and emotional aspects of the human hand, building on the foundations developed by solid organ transplantation, hand surgery, and recon- structive microsurgery. The concept of using composite tissue allograft was first suggested in 1960 by Peacock, when he utilized cadaveric flexor tendons along with their synovial sheaths in order to reconstruct end-stage tendon incarcerations that otherwise would have Disclosure: None of the authors received payments or services, either directly or indirectly (i.e., via his or her institution), from a third party in support of any aspect of this work. One or more of the authors, or his or her institution, has had a financial relationship, in the thirty-six months prior to submission of this work, with an entity in the biomedical arena that could be perceived to influence or have the potential to influence what is written in this work. No author has had any other relationships, or has engaged in any other activities, that could be perceived to influence or have the potential to influence what is written in this work. The complete Disclosures of Potential Conflicts of Interest submitted by authors are always provided with the online version of the article. Disclaimer: The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the United States Army, United States Navy, Department of Defense, or the US Government. | JBJS REVIEWS 2014;2(1):e1 · http://dx.doi.org/10.2106/JBJS.RVW.M.00063 1
Transcript of Hand Transplantation - Hand...

Hand Transplantation
Scott M. Tintle, MD
Benjamin K. Potter, MD
River M. Elliott, MD
L. Scott Levin, MD
Investigation performed at theUniversity of Pennsylvania,Philadelphia, Pennsylvania
COPYRIGHT © 2014 BY THEJOURNAL OF BONE AND JOINTSURGERY, INCORPORATED
» Upper extremity limb loss is catastrophic. It affects nearly everyactivity of daily living, leaving patients with substantial disability.
» Despite high rates of rejection of upper extremity prostheses, handtransplantation remains controversial.
» The indications for hand transplantation remain relatively ill defined.
» The American Society for Reconstructive Transplantation (ASRT) andthe International Registry on Hand and Composite Tissue Transplan-tation (IRHCTT) have been founded to advance the science, to educate,to report outcomes, and to define the indications for vascularizedcomposite allotransplantation.
Upper extremity loss repre-sents a life-changing, oftendevastating event, affectingnearly every activity of daily
living and subsequently leaving a patientwith substantial disability1,2. The potentialimmediate dependency and despair result-ing from the loss of one or both handscannot be overstated. Promising techno-logical advances in upper extremity pros-theses include improved neural-controlinterfaces, multiple-degrees-of-freedomterminal devices, and prototype hapticfeedback mechanisms3,4. However, theavailable literature still demonstrates highprosthesis rejection rates for upper ex-tremity amputees5-12, suggesting thatprostheses continue to inadequately repli-cate the complex, prehensile functions ofthe native hand and arm. The most com-monly cited reasons for upper extremityprosthesis rejection remain limited useful-ness, weight, and residual limbdiscomfort5,13.
Pioneers of hand transplantation rec-ognized that prosthetic devices probablywould never completely satisfy the upperextremity amputee for these very reasons.Even if the prehensile function and dex-terity of the human hand could be restored,these would do little to restore patientbody image or hand sensibility, both traitscoveted by amputees. Rather, they postu-lated that these could only be replaced with“like” human tissue14. The field of vascu-larized composite allotransplantation hasgrown from this basic desire to fullyrestore both the functional and emotionalaspects of the human hand, building on thefoundations developed by solid organtransplantation, hand surgery, and recon-structive microsurgery.
The concept of using composite tissueallograft was first suggested in 1960 byPeacock, when he utilized cadaveric flexortendons along with their synovial sheathsin order to reconstruct end-stage tendonincarcerations that otherwise would have
Disclosure: None of the authors received payments or services, either directly or indirectly (i.e., via his
or her institution), from a third party in support of any aspect of this work. One or more of the
authors, or his or her institution, has had a financial relationship, in the thirty-six months prior to
submission of this work, with an entity in the biomedical arena that could be perceived to influence
or have the potential to influence what is written in this work. No author has had any other
relationships, or has engaged in any other activities, that could be perceived to influence or have the
potential to influence what is written in this work. The complete Disclosures of Potential Conflicts of
Interest submitted by authors are always provided with the online version of the article.
Disclaimer: The opinions and assertions contained herein are the private views of the authors and are
not to be construed as official or as reflecting the views of the United States Army, United States
Navy, Department of Defense, or the US Government.
|
JBJS REVIEWS 2014;2(1):e1 · http://dx.doi .org/10.2106/JBJS.RVW.M.00063 1

required amputation15-18. Shortly afterthis early success with composite tissueallografts, and likely inspired by therapid growth of the solid organ trans-plantation community, the world’s firsthand transplantation was performed inSouth America in 19641,19,20. Unfor-tunately, probably because of the rela-tively primitive immunosuppressionas well as a lack of basic-science prepa-ration, acute rejection predictablyoccurred and the transplanted limbwas amputated about three weekslater15,21. Perhaps reflecting the scien-tific hazards of reaching too far, toofast, the next attempt at hand trans-plantation did not occur until thirty-four years later in Lyon, France, in199815,22,23. Technically, this secondprocedure succeeded; however, thissuccess was not functionally realizedand sustained because the patient didnot adapt psychologically to the newhand and discontinued the use ofimmunosuppressive medications. Thetransplanted limb was eventuallyamputated1. The first hand transplan-tation in the United States was per-formed the following year in Louisville,Kentucky. At the time of writing, thisthird patient still had the transplantedhand, nearly fourteen years later15,24.
The early success of hand trans-plantation in the late 1990s was madepossible by advances in solid organtransplantation. Specifically, the devel-opment of new medications suchas cyclosporine, tacrolimus, andmycophenolate mofetil made theavoidance of rejection possible. In ad-dition, animal models of vascularizedcomposite allotransplantation providedthe basic and translational science evi-dence that successful composite tissueallotransplantation without rejectionwas possible with use of thesemedications15,25-27. Since that time, thefield of vascularized composite allo-transplantation has grown dramatically.Eighty-nine hand transplantationshave been performed worldwide to date,and there are at least seven centers inthe United States at which hand trans-plantation has been performed.
Indications for Transplantation andEthical Considerations“Primum non nocere”—“first do noharm”—remains a paramount principleas the field of vascularized compositeallotransplantation progresses. In the2002 position statement of the Ameri-can Society for Surgery of the Hand,Cooney and Hentz echoed this senti-ment when they recommended “greatcaution and a measured approach to thepatient requesting a limb transplant.”28
This caution, along with appropriateethical considerations, have temperedthe growth of vascularized compositeallotransplantation as compared withsolid organ transplantation. Handtransplantation is very different frommost solid organ transplantations inthat the candidate for hand transplan-tation is not faced with a life-or-deathdecision29. For this reason, developingwidely accepted indications for subject-ing a physiologically healthy person tothe risks of life-long immunosuppres-sion remains a challenge for the allo-transplantation community30.
In 2009, Hollenbeck et al. indi-cated that there were no current, well-defined indications for vascularizedcomposite allotransplantation of thehand or face14. Unfortunately, thisremains the case today31,32—the indi-cations remain open to interpretationby individual vascularized compositeallotransplantation centers. While thisautonomy to develop indications toaccompany slightly different approachesis ostensibly important in a developingfield, the vascularized composite allo-transplantation community is attempt-ing to develop universally acceptedindications for hand transplantationbased on the evidence available. Havingrecognized the need for defined andaccepted indications for hand trans-plantation, the allotransplantationcommunity founded the AmericanSociety for Reconstructive Transplan-tation (ASRT) in 2008. The goalof the ASRT is to provide a platformfor the advancement of education, sci-ence, and the practice of compositetissue allotransplantation as relevant to
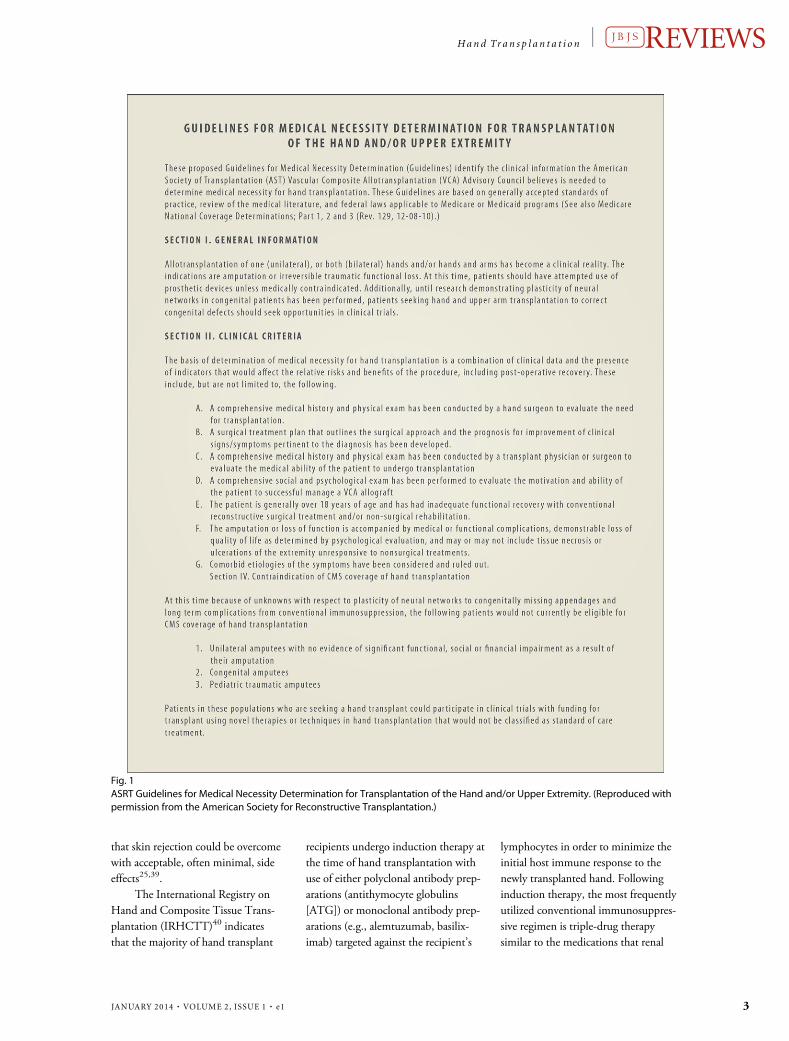
reconstructive and transplant surgery.Last year, the ASRT published guide-lines for medical necessity determina-tion for transplantation of the hand and/or upper extremity (Fig. 1).
Psychological ScreeningThe majority of amputee patients areafflicted by a psychological disorder33.This consideration complicates handtransplantation in that the outcome ofa hand transplantation is very muchdependent on the participation, coop-eration, and compliance of a patientwith hand therapy, medications, andfollow-up screening appointments.A kidney, liver, or heart transplantdepends only on compliance withmedications, and even still there arerelatively high rates of medication non-compliance in this population34,35. Ina combined heart and heart/lung trans-plant population, it was found thatthe only risk factor for graft loss betweensix and twelve months was beingunmarried or not living in a stablerelationship34,35. It is therefore impera-tive that all patients who are to beconsidered for hand transplantationundergo extensive psychological andpsychiatric screening prior to selectionfor hand transplantation. In addition,the social support for an individualcandidate must be identified, and atransplantation should not occur ifthe surgeon is not comfortable withthe patient’s support system.
ImmunosuppressionConventional ImmunosuppressionAside from the ethical issues surround-ing hand transplantation, perhaps themost critical reason that vascularizedcomposite allotransplantation has lag-ged behind solid organ transplantationis the skin. Skin is the most antigenictissue of the composite tissues thatconstitute a hand transplant, and pre-venting the immune system fromrejecting the skin was necessary prior tosuccessful hand transplantation1,36-38.In the 1990s, the aforementionedpharmacologic discoveries and subse-quent animal testing provided evidence
| Han d Tr a n s p l a n t a t i o n
2 JANUARY 2014 · VOLUME 2, ISSUE 1 · e1
that skin rejection could be overcomewith acceptable, often minimal, sideeffects25,39.
The International Registry onHand and Composite Tissue Trans-plantation (IRHCTT)40 indicatesthat the majority of hand transplant
recipients undergo induction therapy atthe time of hand transplantation withuse of either polyclonal antibody prep-arations (antithymocyte globulins[ATG]) or monoclonal antibody prep-arations (e.g., alemtuzumab, basilix-imab) targeted against the recipient’s
lymphocytes in order to minimize theinitial host immune response to thenewly transplanted hand. Followinginduction therapy, the most frequentlyutilized conventional immunosuppres-sive regimen is triple-drug therapysimilar to the medications that renal
Fig. 1ASRT Guidelines for Medical Necessity Determination for Transplantation of the Hand and/or Upper Extremity. (Reproduced withpermission from the American Society for Reconstructive Transplantation.)
Han d Tr a n s p l a n t a t i o n |
JANUARY 2014 · VOLUME 2, ISSUE 1 · e1 3
transplantation patients receive, gener-ally consisting of tacrolimus, mycophe-nolate mofetil, and prednisone30,41.
While conventional, this immu-notherapy has been extremely effectivein the field of hand transplantation: nohand transplant has been lost becauseof acute rejection when conventionaltriple-drug immunosuppression hasbeen used30. This 100% rate of graftsurvival at one year after transplantationhasnotbeenachieved todate inanyotherfield of transplantation30. Despite thisimpressive statistic, however, 85% to90% of these twenty-four transplantedextremities were associated at least oneepisode of acute rejection within the firstyear following transplantation30,40,41.
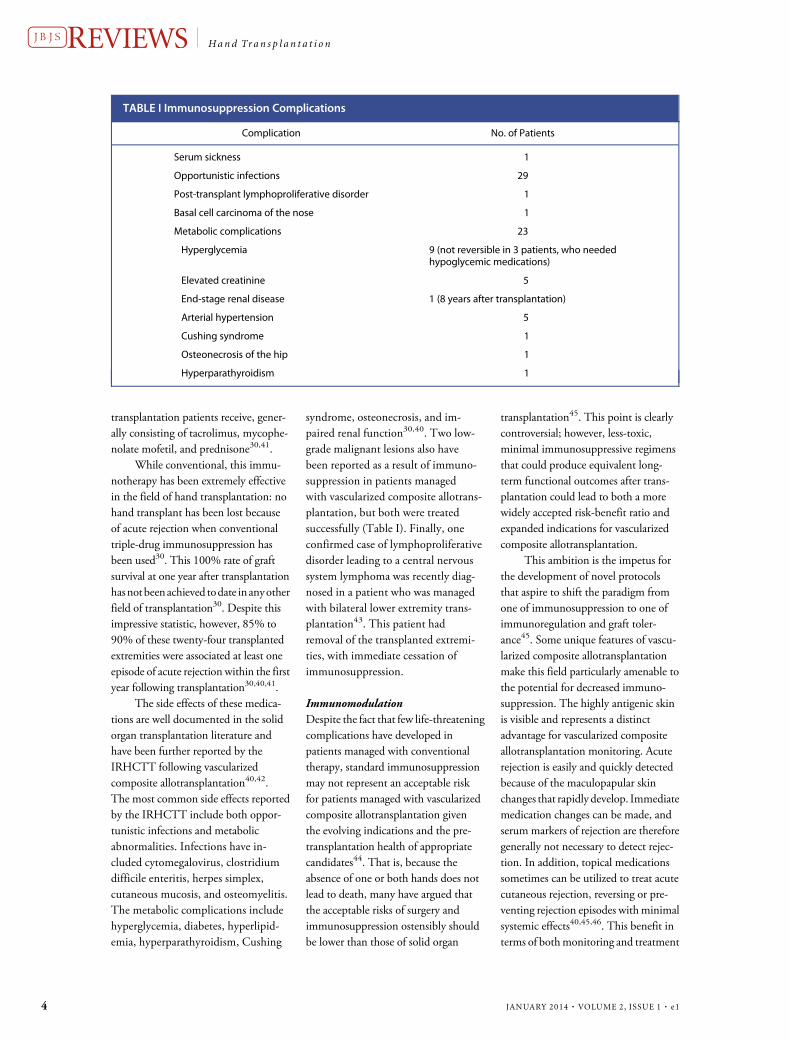
The side effects of these medica-tions are well documented in the solidorgan transplantation literature andhave been further reported by theIRHCTT following vascularizedcomposite allotransplantation40,42.The most common side effects reportedby the IRHCTT include both oppor-tunistic infections and metabolicabnormalities. Infections have in-cluded cytomegalovirus, clostridiumdifficile enteritis, herpes simplex,cutaneous mucosis, and osteomyelitis.The metabolic complications includehyperglycemia, diabetes, hyperlipid-emia, hyperparathyroidism, Cushing
syndrome, osteonecrosis, and im-paired renal function30,40. Two low-grade malignant lesions also havebeen reported as a result of immuno-suppression in patients managedwith vascularized composite allotrans-plantation, but both were treatedsuccessfully (Table I). Finally, oneconfirmed case of lymphoproliferativedisorder leading to a central nervoussystem lymphoma was recently diag-nosed in a patient who was managedwith bilateral lower extremity trans-plantation43. This patient hadremoval of the transplanted extremi-ties, with immediate cessation ofimmunosuppression.
ImmunomodulationDespite the fact that few life-threateningcomplications have developed inpatients managed with conventionaltherapy, standard immunosuppressionmay not represent an acceptable riskfor patients managed with vascularizedcomposite allotransplantation giventhe evolving indications and the pre-transplantation health of appropriatecandidates44. That is, because theabsence of one or both hands does notlead to death, many have argued thatthe acceptable risks of surgery andimmunosuppression ostensibly shouldbe lower than those of solid organ
transplantation45. This point is clearlycontroversial; however, less-toxic,minimal immunosuppressive regimensthat could produce equivalent long-term functional outcomes after trans-plantation could lead to both a morewidely accepted risk-benefit ratio andexpanded indications for vascularizedcomposite allotransplantation.
This ambition is the impetus forthe development of novel protocolsthat aspire to shift the paradigm fromone of immunosuppression to one ofimmunoregulation and graft toler-ance45. Some unique features of vascu-larized composite allotransplantationmake this field particularly amenable tothe potential for decreased immuno-suppression. The highly antigenic skinis visible and represents a distinctadvantage for vascularized compositeallotransplantation monitoring. Acuterejection is easily and quickly detectedbecause of the maculopapular skinchanges that rapidly develop. Immediatemedication changes can be made, andserum markers of rejection are thereforegenerally not necessary to detect rejec-tion. In addition, topical medicationssometimes can be utilized to treat acutecutaneous rejection, reversing or pre-venting rejection episodes withminimalsystemic effects40,45,46. This benefit interms of bothmonitoring and treatment
TABLE I Immunosuppression Complications
Complication No. of Patients
Serum sickness 1
Opportunistic infections 29
Post-transplant lymphoproliferative disorder 1
Basal cell carcinoma of the nose 1
Metabolic complications 23
Hyperglycemia 9 (not reversible in 3 patients, who neededhypoglycemic medications)
Elevated creatinine 5
End-stage renal disease 1 (8 years after transplantation)
Arterial hypertension 5
Cushing syndrome 1
Osteonecrosis of the hip 1
Hyperparathyroidism 1
| Han d Tr a n s p l a n t a t i o n
4 JANUARY 2014 · VOLUME 2, ISSUE 1 · e1

represents an advantage that cannotcurrently be exploited in the field of solidorgan transplantation.
Attempts to minimize immuno-suppression following solid-organtransplantation by infusing bonemarrow from donors into recipientshave successfully led to decreasedimmunosuppressive medicationrequirements47-51. The goal of such aninfusion is to create chimerism, inwhichthe host does not attack the graft and,vice versa, there is no graft-versus-hostdisease52-54. Studies have demonstratedthat as little as 1% “microchimerism”
has been sufficient to allow for thedevelopment of tolerance55,56. Theresulting chimerism, as well as the use ofcell-based therapies, may lead to hosttolerance for the grafted hand, resultingin potentially lower immunosuppressiverequirements and subsequently fewertreatment-related morbidities andsequelae.
Since 2009, one group in theUnited States has been utilizing abone-marrow-cell-based treatment pro-tocol (the so-called Pittsburgh protocol)in efforts to minimize maintenanceimmunosuppression47. This protocolincludes standard induction followedby tacrolimus monotherapy. On thefourteenth day after transplantation,the patients receive an infusion ofdonor bone-marrow cells isolated fromnine vertebral bodies of the donorpatient47. The authors had performeda successful trial of a similar regimen ina swine model prior to implementingthis method in humans44,47. In thisminiature swine model of hindlimballotransplantation across a majorhistocompatibility complex barrier, theauthors were able to induce toleranceto the musculoskeletal elements of thetransplanted hindlimb in two of threeswine treated with bone marrow cellsalong with enteral cyclosporine formonotherapy immunosuppression.The third animal died early (on theforty-second day after transplantation)as a result of an upper gastrointestinalbleed44. The authors did not demon-strate chimerism in the animal recipients
and, unfortunately, tolerance to skinwasnot achieved.
Schneeberger et al.47 reported ontheir cell-based protocol to minimizeimmunosuppression in human trialsinvolving five patients. All patients hadsuccessful hand/arm transplantationwith use of tacrolimus monotherapyfor maintenance immunosuppression.Two patients had three episodes ofrejection each, whereas the other threepatients had one episode each. All epi-sodes were treated with steroid bolustherapy and/or topical tacrolimus andclobetasol. These episodes of rejectionare consistent with the world experiencewith hand transplantation40. Donor-specific alloantibodies were detectedin four of the five patients and wereassociated with skin rejection in mostinstances. However, the authors dem-onstrated that their protocol involvingtacrolimus monotherapy followingbone-marrow-cell infusion was suc-cessful for maintaining viability of ahand/arm transplant. They concludedthat larger and/or randomized con-trolled trials with long-term follow-upwere needed to confirm their earlyfindings47.
OutcomesThe IRHCTT was founded in May200240, with the aim of the registrybeing to combine international clinicalexperiences so that state-of-the-artknowledge can be shared among thosealready working in or approachingthe field of composite tissue allotrans-plantation. According to the IRHCTTitself, one of the main limitations thatcurrently exists with the registry is thatsome international and even someUnitedStates vascularized composite allotrans-plantation programs had not submittedtheir patients’ data at the time of the lastpublication from the IRHCTT40.
The IRHCTT reported on thirty-three patientswhohadundergone upperextremity transplantation in 201040.One death has been reported among thepatients from the registry who weremanaged with vascularized compositeallotransplantation of the hand. The
patient was managed in France andunderwent bilateral hand transplanta-tion as well as face transplantation. Thispatient sustained cerebral anoxia as aresult of an obstructed airway and diedon the sixty-fifth postoperative day.Two additional deaths have now beenreported in Turkey57-59. These twodeaths represent substantial concernin that they occurred following triple andquadruple limb transplantations. Thesequestionably indicated lower extremitytransplantations are reminiscent of thefirst hand transplantation that was per-formed in1964withpoor indications andlittle or no basic-science preparation.
In China, at least seven graftshave been removed. The indicationsfor graft removal in these patientsincluded noncompliance with medica-tions, a lack of appropriate immuno-suppressive therapy, the long distancefrom the patient homes to the transplantcenters, and/or unreported episodesof rejection that were discovered oneventual follow-up. InWestern countries,therehavebeen threepublished reportsofgraft losses. One patient with bilateralinvolvement lost one hand transplantforty-five days postoperatively as a resultof infection, one patient lost a graft 275days postoperatively because of intimalhyperplasia (potentially representingchronic rejection), andonepatient lost thetransplanted limb twenty-nine monthspostoperatively as a result of noncompli-ance with immunosuppressive medica-tions and poor function.
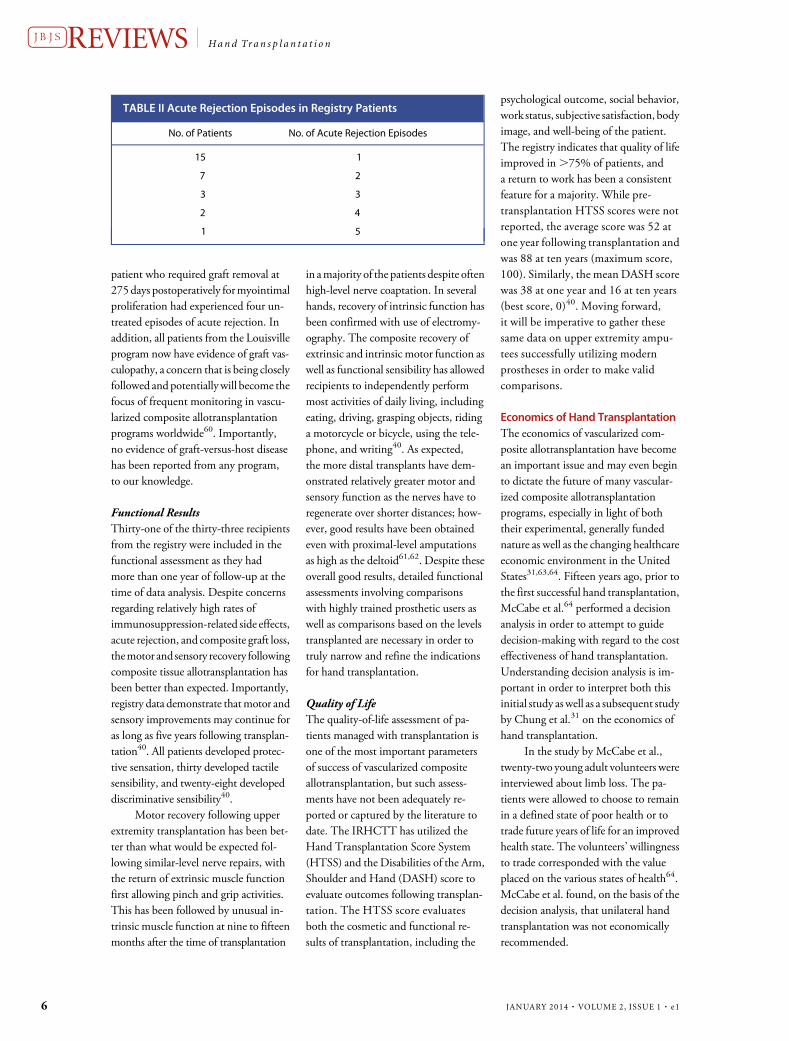
To date, 85% of the thirty-threepatients in the registry have experienced atleast one episode of acute rejection, andmany have had multiple episodes (TableII). These rejection events frequentlycorrelated with short-term noncompli-ance with medications and/or a decreasein immunosuppression as ordered by thevascularized composite allotransplanta-tion team for various reasons. However,all episodes of rejectionwere reversedwithshort-term increases in medication dos-ing, the use of topical agents, and/or in-travenous steroid boluses.
While nodefinite chronic rejectionhas been reported to our knowledge, the
Han d Tr a n s p l a n t a t i o n |
JANUARY 2014 · VOLUME 2, ISSUE 1 · e1 5
patient who required graft removal at275days postoperatively formyointimalproliferation had experienced four un-treated episodes of acute rejection. Inaddition, all patients from the Louisvilleprogram now have evidence of graft vas-culopathy, a concern that is being closelyfollowed andpotentiallywill become thefocus of frequent monitoring in vascu-larized composite allotransplantationprograms worldwide60. Importantly,no evidence of graft-versus-host diseasehas been reported from any program,to our knowledge.
Functional ResultsThirty-one of the thirty-three recipientsfrom the registry were included in thefunctional assessment as they hadmore than one year of follow-up at thetime of data analysis. Despite concernsregarding relatively high rates ofimmunosuppression-related side effects,acute rejection, and composite graft loss,themotor andsensory recovery followingcomposite tissue allotransplantation hasbeen better than expected. Importantly,registry data demonstrate thatmotor andsensory improvements may continue foras long as five years following transplan-tation40. All patients developed protec-tive sensation, thirty developed tactilesensibility, and twenty-eight developeddiscriminative sensibility40.
Motor recovery following upperextremity transplantation has been bet-ter than what would be expected fol-lowing similar-level nerve repairs, withthe return of extrinsic muscle functionfirst allowing pinch and grip activities.This has been followed by unusual in-trinsic muscle function at nine to fifteenmonths after the time of transplantation
in amajority of the patients despite oftenhigh-level nerve coaptation. In severalhands, recovery of intrinsic function hasbeen confirmed with use of electromy-ography. The composite recovery ofextrinsic and intrinsic motor function aswell as functional sensibility has allowedrecipients to independently performmost activities of daily living, includingeating, driving, grasping objects, ridinga motorcycle or bicycle, using the tele-phone, and writing40. As expected,the more distal transplants have dem-onstrated relatively greater motor andsensory function as the nerves have toregenerate over shorter distances; how-ever, good results have been obtainedeven with proximal-level amputationsas high as the deltoid61,62. Despite theseoverall good results, detailed functionalassessments involving comparisonswith highly trained prosthetic users aswell as comparisons based on the levelstransplanted are necessary in order totruly narrow and refine the indicationsfor hand transplantation.
Quality of LifeThe quality-of-life assessment of pa-tients managed with transplantation isone of the most important parametersof success of vascularized compositeallotransplantation, but such assess-ments have not been adequately re-ported or captured by the literature todate. The IRHCTT has utilized theHand Transplantation Score System(HTSS) and the Disabilities of the Arm,Shoulder and Hand (DASH) score toevaluate outcomes following transplan-tation. The HTSS score evaluatesboth the cosmetic and functional re-sults of transplantation, including the
psychological outcome, social behavior,work status, subjective satisfaction, bodyimage, and well-being of the patient.The registry indicates that quality of lifeimproved in.75% of patients, anda return to work has been a consistentfeature for a majority. While pre-transplantation HTSS scores were notreported, the average score was 52 atone year following transplantation andwas 88 at ten years (maximum score,100). Similarly, the mean DASH scorewas 38 at one year and 16 at ten years(best score, 0)40. Moving forward,it will be imperative to gather thesesame data on upper extremity ampu-tees successfully utilizing modernprostheses in order to make validcomparisons.
Economics of Hand TransplantationThe economics of vascularized com-posite allotransplantation have becomean important issue and may even beginto dictate the future of many vascular-ized composite allotransplantationprograms, especially in light of boththeir experimental, generally fundednature as well as the changing healthcareeconomic environment in the UnitedStates31,63,64. Fifteen years ago, prior tothe first successful hand transplantation,McCabe et al.64 performed a decisionanalysis in order to attempt to guidedecision-making with regard to the costeffectiveness of hand transplantation.Understanding decision analysis is im-portant in order to interpret both thisinitial study aswell as a subsequent studyby Chung et al.31 on the economics ofhand transplantation.
In the study by McCabe et al.,twenty-two young adult volunteers wereinterviewed about limb loss. The pa-tients were allowed to choose to remainin a defined state of poor health or totrade future years of life for an improvedhealth state. The volunteers’ willingnessto trade corresponded with the valueplaced on the various states of health64.McCabe et al. found, on the basis of thedecision analysis, that unilateral handtransplantation was not economicallyrecommended.
TABLE II Acute Rejection Episodes in Registry Patients
No. of Patients No. of Acute Rejection Episodes
15 1
7 2
3 3
2 4
1 5
| Han d Tr a n s p l a n t a t i o n
6 JANUARY 2014 · VOLUME 2, ISSUE 1 · e1

In the similar study recently per-formed by Chung et al.31, 100 medicalstudent volunteers were utilized to as-sign utilities. The investigators foundthat, in the setting of unilateral handamputation, prosthesis use was favoredover hand transplantation. They foundthat bilateral hand transplantation wasfavored over prosthesis use in the settingof bilateral limb loss; however, theincremental cost-utility ratio of bilateraltransplantation was $381,961 perquality-adjusted life year (QALY),which greatly exceeds the traditionallyaccepted cost-effectiveness thresholdof $50,000 per QALY31. Nonetheless,the authors concluded that prosthesisadoption was the dominant strategyfor unilateral hand amputation andthat bilateral hand transplantationexceeds the societal acceptable thresholdfor general adoption.
Despite the importance of viewingthe success and feasibility of an inter-vention financially, there are inherentflaws in decision analysis, which bothMcCabe et al.64 and Chung et al.31
brought to light in their discussions.Perhaps the biggest problem with suchdecision analysis lies in the fact that theassigning of utilities will vary amongdifferent populations of people andcritically affects the outcome of theanalysis64. While assessing the generalpublic is important to determine thesocietal perspective, surrogate patientsfrom the general public and even medi-cal students may not be able to trulyassess the benefit of a transplantedhand or to comprehend the complica-tions associated with long-termimmunosuppression29,31.
Future of Hand TransplantationReconstructive surgeons have madeconsiderable progress over the last fifteenyears and can now offer functionalrestorative surgery to patients with up-per extremity limb loss that cannot betreated with conventional techniques.The lingering question at this point iswhether this trend can and will con-tinue. Recent reports have describedlimb loss after transplantation due to
progressive vasculopathy, patient non-compliance with immunosuppression,failure of functional recovery despitea living transplant, and substantial psy-chiatric pathology adversely affectingfunctional outcomes40. In addition, twocases of perioperative failure resultingin reamputation have occurred in theUnited States. Even more concerning,however, are the reports of perioperativemortality that have occurred followingquestionably indicated and undoubt-edly aggressive triple and quadruplelimb allotransplantations performedoutside of theUnited States57. Similarly,potentially premature implementationof lower extremity vascularized com-posite allotransplantation has led someto conclude that “just because you can,does not mean that you should.”65
Rather than accelerating the advance-ment and acceptance of composite tissueallotransplantation, ill-advised and po-tentially reckless utilization of the tech-nique threatens to endanger the field.
The risk-benefit ratio guides us assurgeons and influences our decision tooffer various procedures. This is no dif-ferent in the case of hand transplanta-tion, except that the risks and benefits ofthe procedure have yet to be clearly de-fined29.However, the intermediate risksof hand transplantation are relativelywell defined in the literature40, and thelong-term risks of immunosuppressioncan be extrapolated from the data onsolid-organ transplantation. We nowhave evidence that a patient who has hada leg transplantation will likely die of animmunosuppression-related centralnervous system tumor in the near future.It is critical to the future of this fieldthat appropriate indications for trans-plantation are established and that ourpatients are counseled about the com-plications of immunosuppression, in-cluding potential death.
Moving forward, it is imperativethat the physical and mental benefitsof hand transplantation are carefullyreported and evaluated66. In this regard,attempts to better understand the socialand psychological impact of upper ex-tremity limb loss and then to document
the change in these factors after trans-plantation will need to be closely scru-tinized in order for the risk-benefit ratioto be defined accurately. In addition,objective sensory andmotor testingwithbreakdown by the level of transplanta-tion as well as the use of accepted func-tional assessments (e.g., the Carroll test)need to be embraced andwidely utilized.Last, rapid and transparent reportingof complications to the IRHCTT isnecessary in order to both quantify andqualify both failures and successes.Only then can an accurate assessmentof the risk-benefit ratio be performed,indications be refined, immunosup-pression and immunomodulation regi-mens be adjusted, and candidatepatients be appropriately screened andcounseled. As physicians and surgeons,we can accept nothing less for ourpatients, and doing so ostensibly mayjeopardize the entire field of compositetissue allotransplantation.
While the field remains in its in-fancy, hand transplantation has dem-onstratedmany successes, and the futureappears promising for this restorativetreatment.Webelieve that it is now timeto step back and reevaluate what has andhas not worked and to reassess thecurrent public and medical field accep-tance of allotransplantation. Manyobstacles remain, among them contin-ued funding, immunology, candidateselection, and long-term assessmentof outcomes, in addition to the contin-ued refinement of indications. Weshould approach the future with cau-tious optimism and continue to evaluateall that we do with bench science, peerreviewof both favorable andunfavorableclinical outcomes, and ethical treatmentof our patients. Video 1 demonstrateshand function following bilateral prox-imal forearm transplantation withcomplete flexor-pronator and extensormuscle transfers with coaptation of theradial, median, and ulnar nerves at theelbow.
Source of FundingNo external fundingwas received for thepresent study.
Han d Tr a n s p l a n t a t i o n |
JANUARY 2014 · VOLUME 2, ISSUE 1 · e1 7
Scott M. Tintle, MD1,Benjamin K. Potter, MD1,River M. Elliott, MD2,L. Scott Levin, MD3
1Department of Orthopaedic Surgery,Walter Reed National Military MedicalCenter, 8901 Wisconsin Avenue,Bethesda MD 20889
2Division of Plastic and ReconstructiveSurgery, University of PennsylvaniaHealth System, 3400 Spruce Street,10 Penn Tower, Philadelphia, PA 19106
3Department of Orthopaedic Surgery,University of Pennsylvania Health System,3400 Spruce Street, 10 Penn Tower,Philadelphia, PA 19106.E-mail address for L.S. Levin:[email protected]
References1. Errico M, Metcalfe NH, Platt A. History andethics of hand transplants. JRSM Short Rep.2012 Oct;3(10):74. Epub 2012 Oct 26.
2. Grob M, Papadopulos NA, Zimmermann A,Biemer E, Kovacs L. The psychologicalimpact of severe hand injury. J Hand SurgEur Vol. 2008 Jun;33(3):358-62. Epub 2008May 01.
3. Kuiken TA, Li G, Lock BA, Lipschutz RD, MillerLA, Stubblefield KA, Englehart KB. Targetedmuscle reinnervation for real-time myoelectriccontrol of multifunction artificial arms. JAMA.2009 Feb 11;301(6):619-28.
4. Harvey ZT, Loomis GA, Mitsch S, Murphy IC,Griffin SC, Potter BK, Pasquina P. Advancedrehabilitation techniques for the multi-limbamputee. J SurgOrthopAdv. 2012 Spring;21(1):50-7.
5. Wright TW, Hagen AD, Wood MB.Prosthetic usage in major upper extremityamputations. J Hand Surg Am. 1995 Jul;20(4):619-22.
6. Pinzur MS, Angelats J, Light TR, Izuierdo R,Pluth T. Functional outcome followingtraumatic upper limb amputation andprosthetic limb fitting. J Hand Surg Am. 1994Sep;19(5):836-9.
7. Sturup J, Thyregod HC, Jensen JS, Retpen JB,Boberg G, Rasmussen E, Jensen S. Traumaticamputation of the upper limb: the use of body-powered prostheses and employmentconsequences. Prosthet Orthot Int. 1988 Apr;12(1):50-2.
8. Millstein SG, Heger H, Hunter GA. Prostheticuse in adult upper limb amputees: a comparisonof the body powered and electrically poweredprostheses. Prosthet Orthot Int. 1986 Apr;10(1):27-34.
9. Bhaskaranand K, Bhat AK, Acharya KN.Prosthetic rehabilitation in traumatic upperlimb amputees (an Indian perspective). ArchOrthop Trauma Surg. 2003 Sep;123(7):363-6.Epub 2003 Jun 25.
10. Raichle KA, Hanley MA, Molton I, Kadel NJ,Campbell K, Phelps E, Ehde D, Smith DG.Prosthesis use in persons with lower- andupper-limb amputation. J Rehabil Res Dev.2008;45(7):961-72.
11.Dudkiewicz I,GabrielovR, Seiv-Ner I, ZeligG,Heim M. Evaluation of prosthetic usage inupper limb amputees. Disabil Rehabil. 2004Jan 7;26(1):60-3.
12. Tintle SM, Baechler MF, Nanos GP 3rd,Forsberg JA, Potter BK. Traumatic and trauma-related amputations: Part II: Upper extremityand future directions. J Bone Joint Surg Am.2010 Dec 15;92(18):2934-45.
13. McFarland LV, Hubbard Winkler SL,Heinemann AW, Jones M, Esquenazi A.Unilateral upper-limb loss: satisfaction andprosthetic-device use in veterans andservicemembers from Vietnam and OIF/OEFconflicts. J Rehabil ResDev. 2010;47(4):299-316.
14. Hollenbeck ST, Erdmann D, Levin LS.Current indications for hand and faceallotransplantation. Transplant Proc. 2009 Mar;41(2):495-8.
15. Foroohar A, Elliott RM, Kim TWB,BreidenbachW, Shaked A, Levin LS. The historyand evolution of hand transplantation. HandClin. 2011 Nov;27(4):405-9: vii. Epub 2011Sep 21.
16. Peacock EE Jr. A review of composite tissueallografts of the digital flexor mechanism.Transplant Proc. 1976 Jun;8(2)(Suppl 1):119-27.
17. Peacock EE Jr. Homologous compositetissue grafts of the digital flexor mechanismin human beings. Transplant Bull. 1960 Apr;7:418-21.
18. Peacock EE Jr, Madden JW. Humancomposite flexor tendon allografts. Ann Surg.1967 Oct;166(4):624-9.
19. Gilbert R. Transplant is successful with acadaver forearm. Med Trib Med News. 1964;5:20-2.
20. Goldwyn RM. Joseph E. Murray, M.D.,Nobelist: some personal thoughts. PlastReconstr Surg. 2013 Apr;131(4):918-20.
21. Dubernard JM, Petruzzo P, Lanzetta M,Parmentier H, Martin X, Dawahra M, Hakim NS,Owen E. Functional results of the first humandouble-hand transplantation. Ann Surg. 2003Jul;238(1):128-36.
22. Dubernard JM, Owen E, Lefrançois N,Petruzzo P, Martin X, Dawahra M, Jullien D,Kanitakis J, Frances C, Preville X, Gebuhrer L,Hakim N, Lanzetta M, Kapila H, Herzberg G,Revillard JP. First human hand transplantation.Case report. Transpl Int. 2000;13(Suppl 1):S521-4.
23. Jones JW, Gruber SA, Barker JH,Breidenbach WC; Louisville Hand TransplantTeam. Successful hand transplantation. One-year follow-up. N Engl J Med. 2000 Aug 17;343(7):468-73.
24. Breidenbach WC, Gonzales NR, Kaufman CL,KlaphekeM, TobinGR, Gorantla VS. Outcomes ofthe first 2 American hand transplants at 8 and 6years posttransplant. J Hand Surg Am. 2008 Sep;33(7):1039-47.
25. Benhaim P, Anthony JP, Lin LY, McCalmontTH, Mathes SJ. A long-term study of allogeneicrat hindlimb transplants immunosuppressedwith RS-61443. Transplantation. 1993Oct;56(4):911-7.
26. Ustuner ET, Zdichavsky M, Ren X, EdelsteinJ,MaldonadoC, RayM, JevansAW, BreidenbachWC, Gruber SA, Barker JH, Jones JW. Long-termcomposite tissue allograft survival in a porcinemodel with cyclosporine/mycophenolatemofetil therapy. Transplantation. 1998 Dec 27;66(12):1581-7.
27. Jones JW Jr, Ustuner ET, Zdichavsky M,Edelstein J, Ren X, Maldonado C, Ray M, JevansAW, Breidenbach WC, Gruber SA, Barker JH.Long-term survival of an extremity compositetissue allograft with FK506-mycophenolatemofetil therapy. Surgery. 1999 Aug;126(2):384-8.
28. CooneyWP, Hentz VR; American Society forSurgery of the Hand. Hand transplantation—primumnon nocere. J Hand Surg Am. 2002 Jan;27(1):165-8.
29. Chang J, Mathes DW. Ethical, financial, andpolicy considerations in hand transplantation.HandClin. 2011Nov;27(4):553-60: xi. Epub2011Sep 21.
30. Brandacher G, Gorantla VS, Lee WP. Handallotransplantation. Semin Plast Surg. 2010 Feb;24(1):11-7.
31. Chung KC, Oda T, Saddawi-Konefka D,Shauver MJ. An economic analysis of handtransplantation in the United States. PlastReconstr Surg. 2010 Feb;125(2):589-98.
32.Manske P. The sound of one hand clapping.J Hand Surg Am. 2008 Sep;33(7):1037-8.
33.Melcer T, Walker GJ, GalarneauM, Belnap B,Konoske P. Midterm health and personneloutcomes of recent combat amputees.Mil Med. 2010 Mar;175(3):147-54.
34. Shores JT. Recipient screening andselection: who is the right candidate for handtransplantation. Hand Clin. 2011 Nov;27(4):539-43: x. Epub 2011 Oct 06.
35.Dobbels F, Vanhaecke J, Dupont L, NevensF, Verleden G, Pirenne J, De Geest S.Pretransplant predictors of posttransplantadherence and clinical outcome: an evidencebase for pretransplant psychosocialscreening. Transplantation. 2009 May 27;87(10):1497-504.
36. Murray JE. Organ transplantation (skin,kidney, heart) and the plastic surgeon. PlastReconstr Surg. 1971 May;47(5):425-31.
37. Thaunat O, Badet L, El-Jaafari A, Kanitakis J,Dubernard JM, Morelon E. Composite tissueallograft extends a helping hand to transplantimmunologists. Am J Transplant. 2006 Oct;6(10):2238-42. Epub 2006 Aug 01.
38. Brouha P, Naidu D, Cunningham M, Furr A,Majzoub R, Grossi FV, Francois CG, MaldonadoC, Banis JC,Martinez S, Perez-Abadia G,WigginsO, Kon M, Barker JH. Risk acceptance incomposite-tissue allotransplantationreconstructive procedures. Microsurgery. 2006;26(3):144-9, discussion :149-50.
39. Tobin GR, Breidenbach WC 3rd, Ildstad ST,MarvinMM, Buell JF, Ravindra KV. The history ofhuman composite tissue allotransplantation.Transplant Proc. 2009 Mar;41(2):466-71.
40. Petruzzo P, Lanzetta M, Dubernard JM,Landin L, Cavadas P, Margreiter R,Schneeberger S, Breidenbach W, Kaufman C,Jablecki J, Schuind F, Dumontier C. TheInternational Registry on Hand and CompositeTissue Transplantation. Transplantation. 2010Dec 27;90(12):1590-4.
41. Petruzzo P, Lanzetta M, Dubernard JM,Margreiter R, Schuind F, Breidenbach W,Nolli R, Schneeberger S, van Holder C,Kaufman C, Jablecki J, Landin L, Cavadas P.The international registry on hand andcomposite tissue transplantation.Transplantation. 2008 Aug 27;86(4):487-92.
42. Lanzetta M, Petruzzo P, Dubernard JM,Margreiter R, Schuind F, BreidenbachW, Nolli R,Schneeberger S, van Holder C, Gorantla VS,
| Han d Tr a n s p l a n t a t i o n
8 JANUARY 2014 · VOLUME 2, ISSUE 1 · e1
Pei G, Zhao J, Zhang X. Second report (1998-2006) of the International Registry of Handand Composite Tissue Transplantation.Transpl Immunol. 2007 Jul;18(1):1-6. Epub2007 Apr 09.
43. Levin LS, Cavadas PC. Reconstructivesurgery – the evolution of VC. Symposiumsession at the World Society for ReconstructiveMicrosurgery; 2013 Jul 11-13; Chicago, IL.
44. Hettiaratchy S, Melendy E, Randolph MA,Coburn RC, Neville DM Jr, Sachs DH, Huang CA,Lee WP. Tolerance to composite tissueallografts across a major histocompatibilitybarrier in miniature swine. Transplantation.2004 Feb 27;77(4):514-21.
45. Shores JT, Imbriglia JE, Lee WP. The currentstate of hand transplantation. J Hand Surg Am.2011 Nov;36(11):1862-7.
46. Hautz T, Brandacher G, Zelger B, GorantlaVS, Lee AW, Pratschke J, Schneeberger S.Immunologic aspects and rejection insolid organ versus reconstructivetransplantation. Transplant Proc. 2010 Nov;42(9):3347-53.
47. Schneeberger S, Gorantla VS, BrandacherG,Zeevi A, Demetris AJ, Lunz JG, Metes DM,Donnenberg AD, Shores JT, Dimartini AF, KissJE, Imbriglia JE, Azari K, Goitz RJ, Manders EK,NguyenVT, CooneyDS,WachtmanGS, Keith JD,Fletcher DR, Macedo C, Planinsic R, Losee JE,Shapiro R, Starzl TE, Lee WP. Upper-extremitytransplantation using a cell-based protocol tominimize immunosuppression. Ann Surg. 2013Feb;257(2):345-51.
48. Starzl TE, Zinkernagel RM. Antigen localizationandmigration in immunity and tolerance. N EnglJ Med. 1998 Dec 24;339(26):1905-13.
49. Starzl TE, Murase N, Abu-Elmagd K, Gray EA,Shapiro R, Eghtesad B, Corry RJ, Jordan ML,Fontes P, Gayowski T, Bond G, Scantlebury VP,Potdar S, Randhawa P, Wu T, Zeevi A, NalesnikMA,Woodward J,Marcos A, TruccoM, DemetrisAJ, Fung JJ. Tolerogenic immunosuppressionfor organ transplantation. Lancet. 2003 May 3;361(9368):1502-10.
50. Fontes P, Rao AS, Demetris AJ, Zeevi A,TruccoM, Carroll P, RybkaW, RudertWA, RicordiC, Dodson F, et al Bone marrow augmentationof donor-cell chimerism in kidney, liver, heart,andpancreas islet transplantation. Lancet. 1994Jul 16;344(8916):151-5.
51. Ciancio G, Miller J, Garcia-Morales RO,Carreno M, Burke GW 3rd, Roth D, Kupin W,Tzakis AG, Ricordi C, Rosen A, Fuller L,Esquenazi V. Six-year clinical effect of donorbone marrow infusions in renal transplantpatients. Transplantation. 2001 Apr 15;71(7):827-35.
52. Siemionow M, Nasir S. Impact of donorbone marrow on survival of composite tissueallografts. Ann Plast Surg. 2008 Apr;60(4):455-62.
53. Foster RD, Fan L, Neipp M, Kaufman C,McCalmont T, Ascher N, Ildstad S, Anthony JP,Niepp M. Donor-specific tolerance induction incomposite tissue allografts. Am J Surg. 1998Nov;176(5):418-21.
54. Prabhune KA, Gorantla VS, Maldonado C,Perez-Abadia G, Barker JH, Ildstad ST. Mixedallogeneic chimerism and tolerance tocomposite tissue allografts.Microsurgery. 2000;20(8):441-7.
55. Shores JT, Brandacher G, Schneeberger S,Gorantla VS, Lee WPA. Composite tissueallotransplantation: hand transplantation andbeyond. J Am Acad Orthop Surg. 2010 Mar;18(3):127-31.
56.Wu S, Xu H, Ravindra K, Ildstad ST.Composite tissue allotransplantation: past,present and future-the history and expandingapplications of CTA as a new frontier intransplantation. Transplant Proc. 2009 Mar;41(2):463-5.
57. Gann C. Quadruple limb transplant patientdies. http://abcnews.go.com/blogs/health/2012/02/28/quadruple-limb-transplant-patient-dies/. Accessed 2013 Jun 18.
58. Adams Sheets C. Atilla Kavdir deadmonthsafter receiving triple-limb transplant in Turkey.
ABC News. http://www.ibtimes.com/atilla-kavdir-dead-months-after-receiving-triple-limb-transplant-turkey-694734. Accessed 2013Oct 22.
59. Man, 27, who had world’s first quadruplelimb transplant dies days after operation. DailyMail. http://www.dailymail.co.uk/health/article-2107533/Quadruple-limb-transplant-fails-patient-dies-days-operation.html.Accessed 2013 Oct 22.
60. Kaufman CL, Ouseph R, Blair B, Kutz JE,Tsai TM, Scheker LR, Tien HY, Moreno R,Ozyurekoglu T, Banegas R, Murphy E, Burns CB,Zaring R, Cook DF, Marvin MR. Graftvasculopathy in clinical hand transplantation.Am J Transplant. 2012 Apr;12(4):1004-16. Epub2012 Feb 11.
61. Cavadas PC, Ibañez J, Thione A, Alfaro L.Bilateral trans-humeral arm transplantation:result at 2 years. Am J Transplant. 2011 May;11(5):1085-90.
62. Stangl MJ. 3 year immunological follow upof the first bilateral arm transplant world wide:1817. Transplantation. 2012;94:346.
63. Concannon MJ. Discussion: An economicanalysis of hand transplantation in the UnitedStates. Plast Reconstr Surg. 2010 Feb;125(2):599-600.
64. McCabe S, Rodocker G, Julliard K,Breidenbach W, Marcel C, Shirbacheh MV,Barker J. Using decision analysis to aidin the introduction of upper extremitytransplantation. Transplant Proc. 1998 Sep;30(6):2783-6.
65. Vicente D, Potter BK, Elster E. “Just becauseyou can, does not mean that you should”. Am JTransplant. 2013 May;13(5):1123-4. Epub 2013Mar 08.
66. Schuind F. Hand transplantation andvascularized composite tissue allografts inorthopaedics and traumatology. OrthopTraumatol Surg Res. 2010 May;96(3):283-90.Epub 2010 Apr 18.
Han d Tr a n s p l a n t a t i o n |
JANUARY 2014 · VOLUME 2, ISSUE 1 · e1 9


















![Kidney Transplantation (Renal Transplantation) Auto Saved]](https://static.fdocuments.us/doc/165x107/577d22b31a28ab4e1e9807d7/kidney-transplantation-renal-transplantation-auto-saved.jpg)