HAND – FOOT – MOUTH DISEASE Prepared by: Dr. NGUYEN QUANG DIEN Emergency Department.
24
HAND – FOOT – MOUTH DISEASE Prepared by: Dr. NGUYEN QUANG DIEN Prepared by: Dr. NGUYEN QUANG DIEN Emergency Emergency Department Department
-
Upload
dora-poole -
Category
Documents
-
view
236 -
download
3
Transcript of HAND – FOOT – MOUTH DISEASE Prepared by: Dr. NGUYEN QUANG DIEN Emergency Department.

HAND – FOOT – MOUTH DISEASE
Prepared by: Dr. NGUYEN QUANG DIEN Prepared by: Dr. NGUYEN QUANG DIEN Emergency Department Emergency Department

HAND – FOOT – MOUTH DISEASE
HFM disease is a viral syndrome with a distinct exanthem – enanthem.
This clearly recognizable syndrome is characterized by vesicular lesions on the mouth and an exanthem on the hands and feet (and buttocks) in association with fever.
HAND – FOOT – MOUTH DISEASE
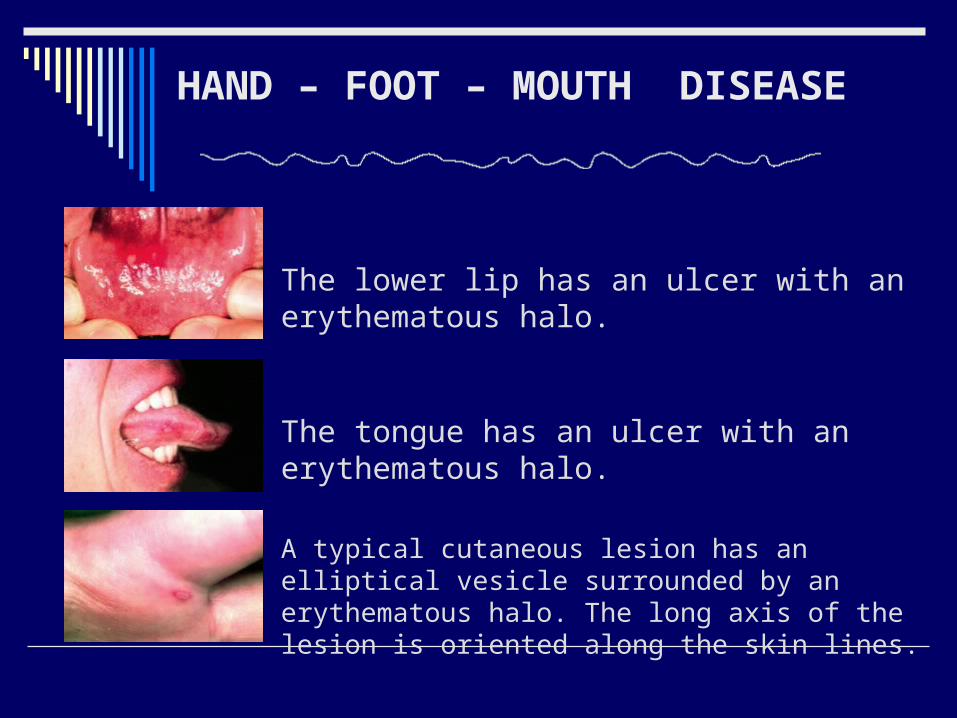
The lower lip has an ulcer with an erythematous halo.
The tongue has an ulcer with an erythematous halo.
A typical cutaneous lesion has an elliptical vesicle surrounded by an erythematous halo. The long axis of the lesion is oriented along the skin lines.

HAND – FOOT – MOUTH DISEASE

Pathophysiology
Hand-foot-and-mouth disease is caused by a group of
RNA viruses called enteroviruses. The most commonly
implicated enterovirus is coxsackievirus A16.[1] However,
coxsackieviruses A5, A9, A10, A16, B1, and B3; human
enterovirus 71 (HEV71); as well as herpes simplex viruses
(HSV) can cause the illness. HEV71 is of the most care
because HEV71 has been recently implicated in several
large outbreaks with severe complications and deaths.

Pathophysiology
Cases are commonly spread via the fecal-oral or oral-oral
route. Respiratory droplet transmission also may occur but
is less likely. Typically, the virus seeds the GI tract via the
buccal mucosa or the ileum. Over the next 72 hours
(accounting for the incubation period), a viremia is
established via spread through nearby lymph nodes.
In Vietnam , the peak incident is in April & May .
HAND – FOOT – MOUTH DISEASE
Mortality/ Morbidity
Severe complications may occur when CNS or
cardiopulmonary involvement is present .
Age
More common among infants and children younger
than 5 years.

History
The usual incubation period of hand-foot-and-mouth (HFM) disease is 4-6 days.
The prodrome is associated with the following: Low-grade fever Malaise Anorexia Abdominal pain Sore mouth
The prodrome precedes the development of oral lesions, followed shortly by skin lesions, primarily on the hands and feet and occasionally on the buttocks.

Physical
Hand-foot-and-mouth disease is the most common cause of mouth sores in
pediatric patients.

Physical
These primarily occur on the labial and buccal mucosal surfaces but may be observed on the tongue, palate, uvula, anterior tonsillar pillars, or gums. Unlike herpetic gingivostomatitis, perioral lesions are uncommon. Coxsackie A virus also causes herpangina, mostly described as palatal and posterior oropharyngeal lesions without any associated exanthem.
The oral ulcers are painful. Children younger than 5 years are predominately more symptomatic than older patients.
Yellow ulcers surrounded by red halos characterize the oral lesions

Physical
These lesions may be asymptomatic or pruritic.
They usually begin as erythematous macules that rapidly progress to thick-walled grey vesicles with an erythematous base.
In young infants, these lesions may also be observed on the trunk, thighs, and buttocks.
The rash is usually self-limited, lasting approximately 3-6 days.
Case reports have documented subacute, chronic, and recurring skin lesions.
The exanthem typically involves the dorsal surfaces but frequently may include the palmar, plantar, and interdigital surfaces of the hands and feet.

Complications Neurologic complications :
1. Encephalitis aseptic : Wake up with a start
Myoclonal jerk
Limbs trembling
Nystagmus
Cerebellar ataxia
Transverse myelitis >> limbs weakness
2. Cranial nerves paralysis
3. Convulsion , coma coupled with respiratory failure ,
cardiovascular failure .

Complications Cardiopulmonary complications:
Pulse > 150 bpm , mottled skin , capillary refill > 2s
BP : normal or increasing
RR increasing , laboured breathing , rose froths , wet rales
Cyanosis
Diagnosis
Positive :
Clinical exam. is the cornerstone with Exanthem – Enanthem
( oral ulcers & skin lesions )

DiagnosisSeverity degrees :
1. Buccal ulcers +/- skin lesions : recovery in 01 week , no sequelae
2. Encephalomyelitis risk: Myoclonal jerk , restlessness , hands reaching up repeatedly , flounder .

DiagnosisSeverity degrees :
2a/. Less starts : not found on exam.
2b/. More starts : > 2times / min or found on exam,
frequent starts coupled with : Hands reaching up repeatedly
Trembling
Flounder
Somnolence
P> 150bpm
Fever > 39 dC not relieved
Limbs weakness / paralysis
DiagnosisSeverity degrees :
3. Diaphoresis , RR increasing , P > 170bpm ,
BP increasing , convulsion , coma
(glasgow <10)
4. Respiratory failure , Cardiovascular failure.

TREATMENT :
Symptomatic treatment
Close monitoring
Complications treatments
Early sedations >> decreasing irritation
>> treat increased ICP

TREATMENTI – Outpatient: (stage 1st and 2nd a )
Fever relief
Oral higiene
Rest and prevent irritation
Recs everyday or every
other day in 7 days
Recs immediately if :
Fever >39dC
Laboured breathing
Starts , trembling , crying ,
hands reaching up repeatedly
Convulsion , coma
Limbs weakness
Mottled skin

TREATMENTII – Admission: ( Degree 2b backwards ) if meet one of following criteria:
Fever : < 3yos : > 38dC w/o time mentioned
>=3yos : > 38dC and > 3 days
HR : < 3yos : > 150 bpm
>= 3yos : > 120bpm
RR : < 3yos : >40 / min
>= 3yos : > 30/min

TREATMENTII – Admission: ( Degree 2b backwards ) if meet one of following criteria:
Any of :
○ Refuse to eat
○ Vomiting all the time
○ Fatigue
○ Mottled skin
○ Look bad .
Signs of :
○ Meningitis
○ Myocarditis
○ Encephalitis
○ Acute limbs weakness /
paralysis

Indications for Immunoglobulin at Peadiatric N.1 Hospital:
Neurologic Complications:
Mental status disorder : Glasgow<10.
Frequent starts , restlessly exciting .
Neurologic deficit (limbs weakness /
paralysis, cranial nerves paralysis).
Convulsion (febrile convulsion ruled out).

Indications for Immunoglobulin at Peadiatric N.1 Hospital:
Cardiorespiratory complications :
Abnormal RR (rapid RR , Irregular RR , and no pneumonia
signs / chest Xray ).
Pulmonary Edema .
Tachycardia, HR >150 bpm, Capillary refill > 2 s.
HTN.
Immunoglobulin is not effective in severe shock, deep
coma

THANKS FOR YOUR ATTENTION!
Dr NGUYEN QUANG DIEN




![[Quang Nguyen] Performance Test in Best Practices](https://static.fdocuments.us/doc/165x107/554f41f3b4c905423f8b45e5/quang-nguyen-performance-test-in-best-practices.jpg)