Halina Matsumoto Medical University of Warsaw Chair...
29
Seminarium 1 Halina Matsumoto Medical University of Warsaw Chair and Department of Psychiatry Laboratory of Psychopharmacology Granada, LLP ERASMUS, June 5, 2013
Transcript of Halina Matsumoto Medical University of Warsaw Chair...

Seminarium 1
Halina Matsumoto
Medical University of Warsaw
Chair and Department of Psychiatry
Laboratory of Psychopharmacology
Granada, LLP ERASMUS, June 5, 2013

Deante Toscano


Possible consequences of CYP2D6
genotype on treatment effect


Dose adjustment depending on
CYP2D6 genotype
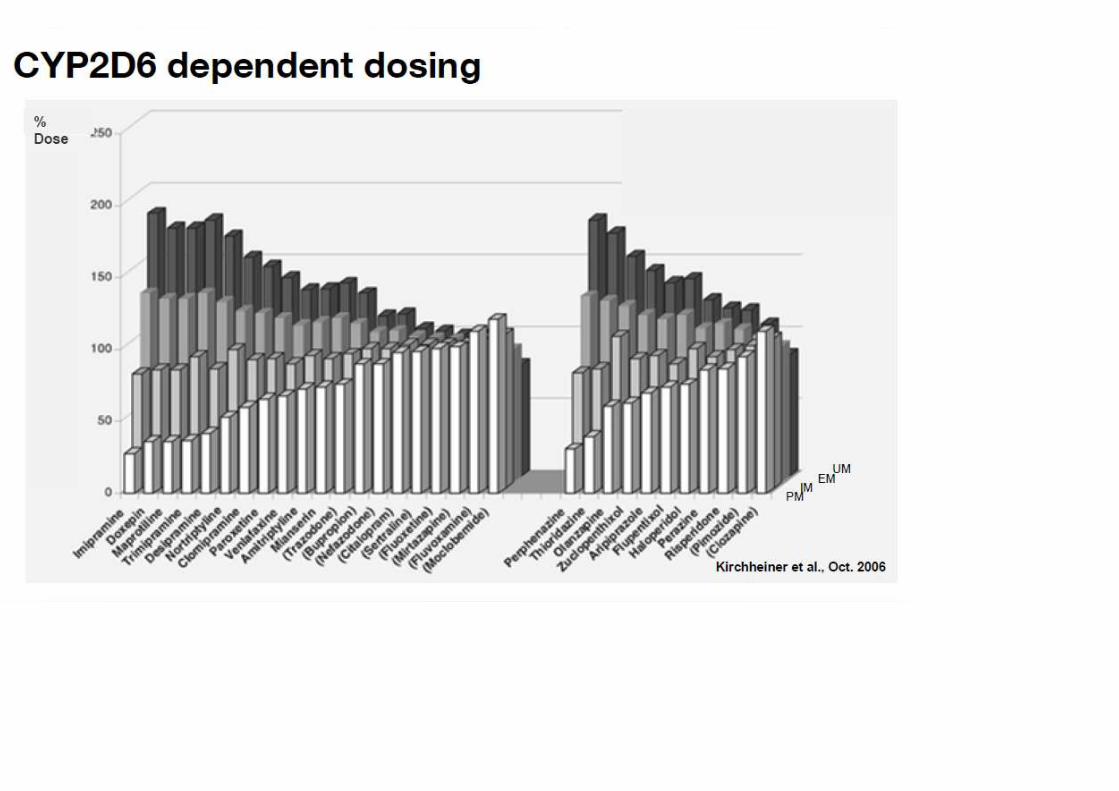


Different drugs require different level of
dose adjustment (depending on
genotype).





CYP2D6 and Clinical Outcome



Targeted interventions – clozapine
response
• Clozapine: approximately 60% efficacy for
schizophrenia
• Works through dopaminergic and
serotonergic mechanisms
• In some studies:
– Response predicted by polymorphisms at 5HT2A
and 5HT2C receptors, 5-HTT
– Predict response in 78% of patients (female)

Clozapine in treatment resistant
schizophrenia• Approximately one third of patients fail to antipsychotic medication and are said to suffer from
treatment resistant schizophrenia (TRS)
• The only drug with proven efficacy in this group of patients is clozapine and NICE (The National
Institute for Health and Clinical Excellence) has recommended that: „In individuals with evidence of
TRS, clozapine should be introduced at the earliest opportunity”.
• However, clozapine has potentially serious side effects and its use is often accompanied by
apprehension from clinicians, patients and carers.
• In addition, only approximately half of clozapine treated patients will show meaningful
symptomatic improvement.
• The genetic test provides clinicians with an indication of a patient’s probability of response to
clozapine. Reassuring the clinician and the patient that exposure to clozapine is merited, based on
the likelihood of response, can stop clozapine being used only as a last resort, thus allowing
patients to benefit from the proven efficacy of the drug at the earliest possible opportunity. For
patients on longterm clozapine treatment who are ahowing equivocal response, the test may
guide the clinician as to the merit of continuing treatment.

Clozapine response – side effects
• Risk of agranulocytosis is a prominent reason for not prescribing clozapine
• Clozapine can be associated with a drop in white blood cell count even with blood monitoring
• Incidence of clozapine-induced leukopenia is 2.95%
• Incidence of clozapine-induced agranulocytosis (CIA) is 0.38%
• The risk of CIA rises steeply the first 2 months of therapy and peaks during month 3-4
• Prescribing clozapine requires mandatory blood monitoring to help reduce the incience of CIA


TDM STANDARDS IN PSYCHIATRY ACCORDING TO AN INTERNATIONAL GROUP OF
EXPERTS FROM GERMAN SPEAKING COUNTRIES ( AGNP= ger. Arbeitsgeeinschaft für
Neuropsychopharmakologie und Pharmakopsychiatrie) Baumann et al., 2004
• GENERAL INDICATIONS FOR TDM METHOD DURING PHARMACOTHERAPY OF PSYCHIATRIC DISEASES:
• Noncompliance
• Therapy with drugs that routinely require TDM (lithium salts)
• No clinical improvement of insufficient efficacy of treatment, despite using adequate doses of medicaments
• Adverse side effects during treatment with therapeutic doses
• Suspicion of drug interactions
• Pharmacovigilance
• Combined pharmacotherapy with a drug with hight interaction potential, while treating „comorbidities”, „potentialisation” of pharmacotherapy
• Prophylaxis of psychiatric disease reccurences in longterm treatment
• Reccurence of disease despite compliance and using adequate doses of drugs
• Genetic polymorphism in drug metabolism, genetic deficiency or amplification of genes involved in the drug metabolism
• Population of children (up to 12 years) and adolescents (12-18 years)
• Elderly patients
• Patietns with renal/liver failure, cardiovascular diseases
• Forensic psychiatry
• Changing original drug to a generic
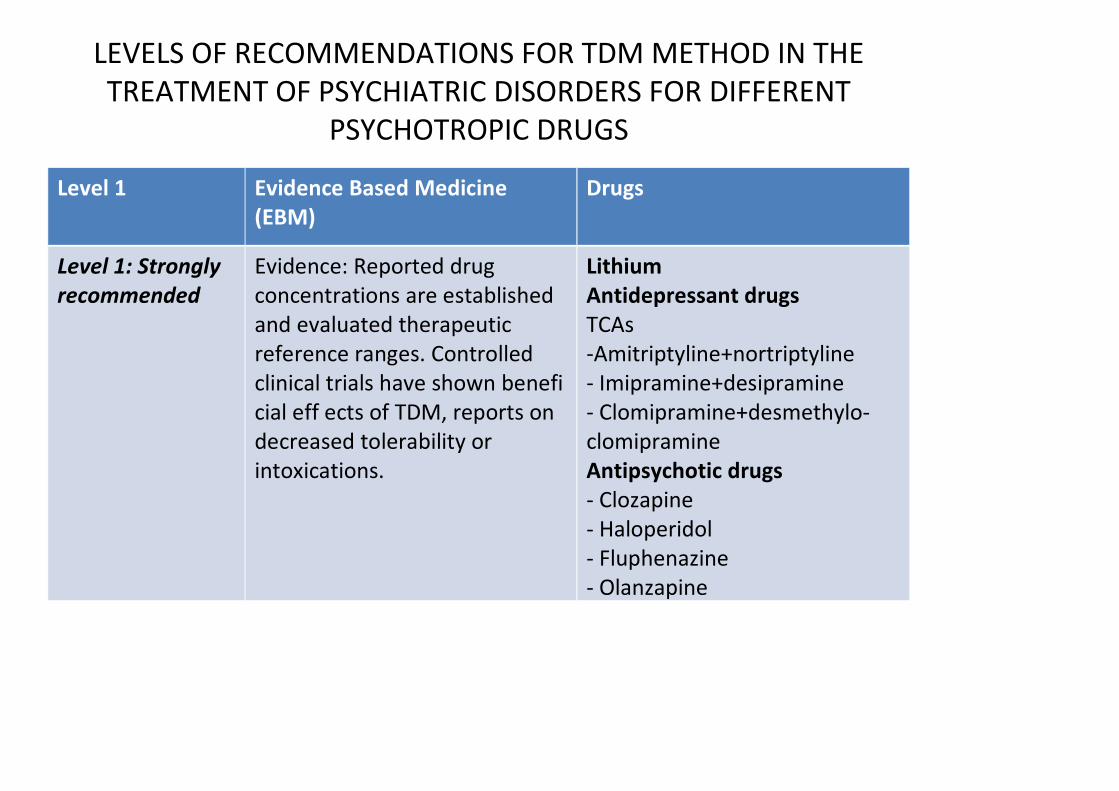
LEVELS OF RECOMMENDATIONS FOR TDM METHOD IN THE
TREATMENT OF PSYCHIATRIC DISORDERS FOR DIFFERENT
PSYCHOTROPIC DRUGS
Level 1 Evidence Based Medicine
(EBM)
Drugs
Level 1: Strongly
recommended
Evidence: Reported drug
concentrations are established
and evaluated therapeutic
reference ranges. Controlled
clinical trials have shown benefi
cial eff ects of TDM, reports on
decreased tolerability or
intoxications.
Lithium
Antidepressant drugs
TCAs
-Amitriptyline+nortriptyline
- Imipramine+desipramine
- Clomipramine+desmethylo-
clomipramine
Antipsychotic drugs
- Clozapine
- Haloperidol
- Fluphenazine
- Olanzapine

Level 2: Recommended Evidence: Reported drug
concentrations were
obtained from
plasma concentrations at
therapeutically eff ective
doses and
related to clinical eff ects;
reports on decreased
tolerability or
intoxications at
“supratherapeutic” plasma
concentrations.
Recommendation: TDM is
recommended for dose
titration
and for special indications
or problem solving.
Antidepressant drugs:
- Desipramine
- Venlafaxine +
Desmethylvenlafaxine
Antipsychotic drugs
- Chlorpromazine
- Flupentixol
- Perazine
- Risperidone + 9-
hydroxyrisperidone
Other
- Carbamazepine
- Valproic acid
- Donepezil
- Taurine
- Methadone

Level 3: Useful Evidence: Reported drug
concentrations were calculated
from plasma concentrations at eff
ective doses obtained from
pharmacokinetic studies. Plasma
concentrations related to
pharmacodynamic eff ects are
either not yet available or
based on retrospective analysis of
TDM data, single case
reports or non-systematic clinical
experience.
Recommendation: TDM is useful for
special indications or
problem solving.
Antidepressant drugs:
- Citalopram
- Dexepine + Nordoxepine
- Fluoxetine +
Norfluoxetine
- Mianserin
- Mirtazapine
- Paroxetine
- Sertraline
- Trazodone
- Trimipramine
- Viloxazine
Antipsychotic drugs:
- Amisulprid
- Chlorprothixen
- Levomepromazine
- Quetiapine
Benzodiazepines
- Alprazolam
Other
- Galantamine
- Acamprosate

Level 4:
Potentially useful
Evidence: Plasma concentrations do
not correlate with clinical
eff ects due to unique
pharmacology of the drug, e. g.,
irreversible
blockade of an enzyme, or dosing
can be easily
guided by clinical symptoms, e. g.,
sleep induction by a hypnotic
drug.
Antidepressant drugs:
- Escitalopram
- Moclobemide
- Reboxetine
Antipsychotic drugs:
- Melperone
- Pimozide
- Ziprasidone
Anxiolytic drugs
- Buspiron
- Lorazepam
- Midazolam
Other
- Bupropion
- Memantine
- Naltrexone

Level 4: Not
recommended
TDM is not recommended in cases
of unique pharmacology of a drug.
i.e. irreversible enzyme inhibition or
diversed drug dosing depending on
diagnosis and clinical symptoms
Tranylcypromine
Zolpidem
Zopiclone
Clomethiazole
Disulphiram

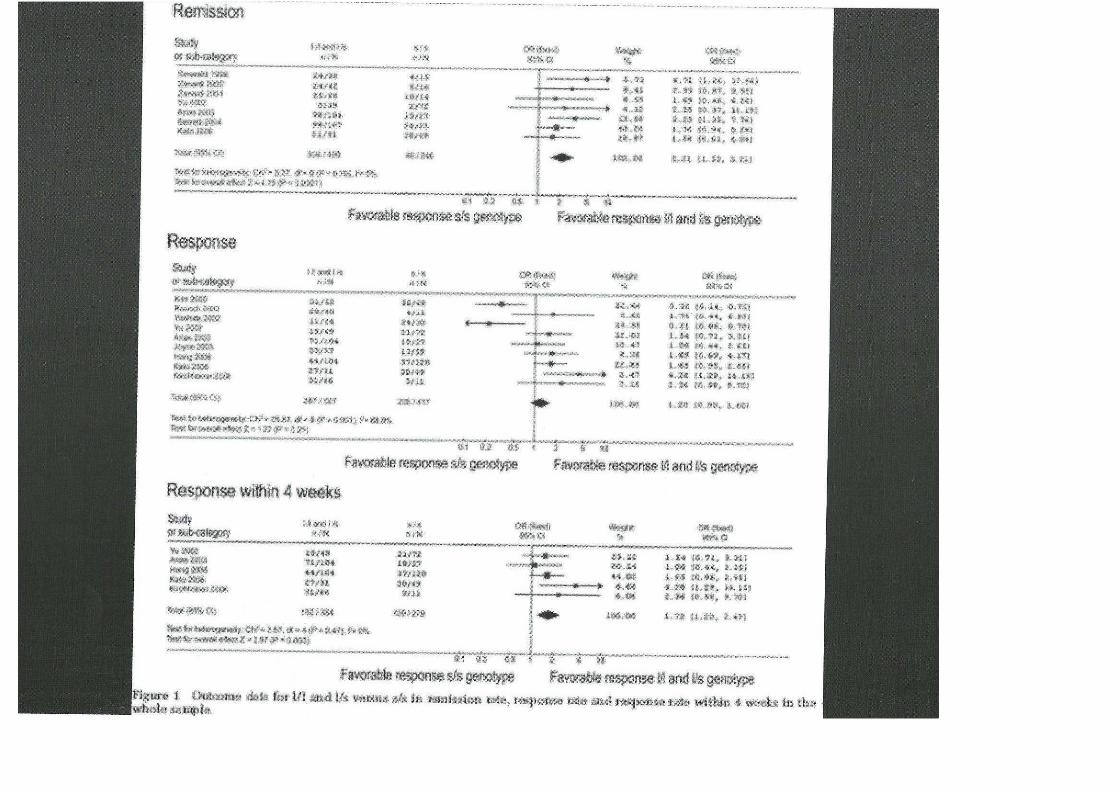
ANTIDEPRESSANT TREATMENT
RESPONSE ENDOPHENOTYPESLeuchter i wsp.:A new paradigm for the prediction of antidepressant
treatment response. Dial Clin Neurosci, 2009,11,435-446
1. RE – response endophenotypes – a class of predictors consisting of clinical symptoms or neurobiological reaction present at the beginning of the treatment with high predictive value for response of individual treatment
2. Implementation of response endophenotype strategy in pharmacological treatment consists a new paradigm in clinical trials. A drug that will probably be inefficient could be stopped after 1-2 weeks and replaced with a new, more efficient drug (based on specific markers)
3. Potential predictors of response to treatment”– Early changes is symptoms severity
– Results of QEEG
– Gene expression examiantions.