Hablemos de mantenimiento Después de la RC: ¿cómo y hasta ... · Hablemos de mantenimiento...
86
Hablemos de mantenimiento Después de la RC: ¿cómo y hasta cuando? Rosario García Campelo Servicio de Oncología Médica Hospital Universitario A Coruña, INIBIC
Transcript of Hablemos de mantenimiento Después de la RC: ¿cómo y hasta ... · Hablemos de mantenimiento...

Hablemos de mantenimiento
Después de la RC: ¿cómo y hasta cuando?
Rosario García Campelo
Servicio de Oncología Médica
Hospital Universitario A Coruña, INIBIC

LA TAREA DE LA MEJOR NARRATIVA ES RELAJAR AL INQUIETO E INQUIETAR AL
RELAJADO
David Foster Wallace

The message…

The message…
Good things come from good science


Rapid
development of
molecular
targeting agents

Rapid
development of
molecular
targeting agents
Availability of IO

Rapid
development of
molecular
targeting agents
Availability of IOClinical application of
plasma and tissue
based genomic
testing

Treatment Duration in Oncology
Early Stage goal: Treat to Achieve Cure• Limited duration
Stage IV goals: Extend OS, reduce burden/symptoms/ QoL• Duration often limited by toxicity• Maintenance therapy and targeted TKIs changed paradigm• What about IO? Is the same concept?



Ongoing Phase 3 Adjuvant Studies in Early Stage NSCLC
• ANVIL- ECOG-ACRIN – Adjuvant nivolumab versus observation
• BR 31- CCTG – Adjuvant durvalumab versus placebo
• PEARLS – EORTC – Adjuvant pembrolizumab versus placebo
• IMpower 010 – Adjuvant atezolizumab versus observation
8

Open questions regarding IO and TKI in early-locally
advanced disease
• Duration of treatment: one year….enough, too short, too long?
• Is duration of treatment the same for all tumor types?
• The dose…lower than in stage IV?
• Toxicity…the same in early than in advanced disease?

Stav I et al. Med Oncol 2018

WHAT DO PATIENTS AND WE WANT?
TO BE CURE…
To relieve a person of the symptoms of a
disease of condition
To eliminate a diseaseor condition with
medical treatment
SURVIVAL ≠
CURE


What did we need in advanded disease to prolong
treatments?
3 strong arguments

What did we need in advanded disease to prolong
treatments?
3 strong arguments
▪ Active drugs

What did we need in advanded disease to prolong
treatments?
3 strong arguments
▪ Active drugs
▪ Drug with few cumulative toxicities

What did we need in advanded disease to prolong
treatments?
3 strong arguments
▪ Active drugs
▪ Drug with few cumulative toxicities
▪ Scientific evidence…


Would you stop 1st line treatment after 4 cycles of
therapy in a metastatic breast, CCR or prostate cancer
patient without progression or significant toxicity?

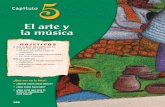
2 YEARS SURVIVAL RATE NSCLC (non-squamous)
Schiller J, N Engl J Med 2002; Scagliotti, G. V. et al. J Clin Oncol 2008; Cappuzzo F et al.
Lancet Oncol 2010; Ciuleanu TE et al. Lancet 2009; Paz Ares L et al. J Clin Oncol 2013; Barlesi
et al. Ann Oncol 2014

2 YEARS SURVIVAL RATE NSCLC (non-squamous)
0%
5%
10%
15%
20%
25%
30%
35%
40%
ECOG1594 JMBD ECOG4599 PARAMOUNT AVAPERL
11%
19%23%
32%
39%
Schiller J, N Engl J Med 2002; Scagliotti, G. V. et al. J Clin Oncol 2008; Cappuzzo F et al.
Lancet Oncol 2010; Ciuleanu TE et al. Lancet 2009; Paz Ares L et al. J Clin Oncol 2013; Barlesi
et al. Ann Oncol 2014

2 YEARS SURVIVAL RATE NSCLC (non-squamous)
0%
5%
10%
15%
20%
25%
30%
35%
40%
ECOG1594 JMBD ECOG4599 PARAMOUNT AVAPERL
11%
19%23%
32%
39%
Schiller J, N Engl J Med 2002; Scagliotti, G. V. et al. J Clin Oncol 2008; Cappuzzo F et al.
Lancet Oncol 2010; Ciuleanu TE et al. Lancet 2009; Paz Ares L et al. J Clin Oncol 2013; Barlesi
et al. Ann Oncol 2014

2 YEARS SURVIVAL RATE NSCLC (non-squamous)
0%
5%
10%
15%
20%
25%
30%
35%
40%
ECOG1594 JMBD ECOG4599 PARAMOUNT AVAPERL
11%
19%23%
32%
39%
Schiller J, N Engl J Med 2002; Scagliotti, G. V. et al. J Clin Oncol 2008; Cappuzzo F et al.
Lancet Oncol 2010; Ciuleanu TE et al. Lancet 2009; Paz Ares L et al. J Clin Oncol 2013; Barlesi
et al. Ann Oncol 2014

2 YEARS SURVIVAL RATE NSCLC (non-squamous)
0%
5%
10%
15%
20%
25%
30%
35%
40%
ECOG1594 JMBD ECOG4599 PARAMOUNT AVAPERL
11%
19%23%
32%
39%
Schiller J, N Engl J Med 2002; Scagliotti, G. V. et al. J Clin Oncol 2008; Cappuzzo F et al.
Lancet Oncol 2010; Ciuleanu TE et al. Lancet 2009; Paz Ares L et al. J Clin Oncol 2013; Barlesi
et al. Ann Oncol 2014

2 YEARS SURVIVAL RATE NSCLC (non-squamous)
0%
5%
10%
15%
20%
25%
30%
35%
40%
ECOG1594 JMBD ECOG4599 PARAMOUNT AVAPERL
11%
19%23%
32%
39%
Schiller J, N Engl J Med 2002; Scagliotti, G. V. et al. J Clin Oncol 2008; Cappuzzo F et al.
Lancet Oncol 2010; Ciuleanu TE et al. Lancet 2009; Paz Ares L et al. J Clin Oncol 2013; Barlesi
et al. Ann Oncol 2014

2 YEARS SURVIVAL RATE NSCLC (non-squamous)
0%
5%
10%
15%
20%
25%
30%
35%
40%
ECOG1594 JMBD ECOG4599 PARAMOUNT AVAPERL
11%
19%23%
32%
39%
Schiller J, N Engl J Med 2002; Scagliotti, G. V. et al. J Clin Oncol 2008; Cappuzzo F et al.
Lancet Oncol 2010; Ciuleanu TE et al. Lancet 2009; Paz Ares L et al. J Clin Oncol 2013; Barlesi
et al. Ann Oncol 2014

2 YEARS SURVIVAL RATE NSCLC (non-squamous)
0%
5%
10%
15%
20%
25%
30%
35%
40%
ECOG1594 JMBD ECOG4599 PARAMOUNT AVAPERL
11%
19%23%
32%
39%
Schiller J, N Engl J Med 2002; Scagliotti, G. V. et al. J Clin Oncol 2008; Cappuzzo F et al.
Lancet Oncol 2010; Ciuleanu TE et al. Lancet 2009; Paz Ares L et al. J Clin Oncol 2013; Barlesi
et al. Ann Oncol 2014

2 YEARS SURVIVAL RATE NSCLC (non-squamous)
0%
5%
10%
15%
20%
25%
30%
35%
40%
ECOG1594 JMBD ECOG4599 PARAMOUNT AVAPERL
11%
19%23%
32%
39%
Schiller J, N Engl J Med 2002; Scagliotti, G. V. et al. J Clin Oncol 2008; Cappuzzo F et al.
Lancet Oncol 2010; Ciuleanu TE et al. Lancet 2009; Paz Ares L et al. J Clin Oncol 2013; Barlesi
et al. Ann Oncol 2014

2 YEARS SURVIVAL RATE NSCLC (non-squamous)
0%
5%
10%
15%
20%
25%
30%
35%
40%
ECOG1594 JMBD ECOG4599 PARAMOUNT AVAPERL
11%
19%23%
32%
39%
Schiller J, N Engl J Med 2002; Scagliotti, G. V. et al. J Clin Oncol 2008; Cappuzzo F et al.
Lancet Oncol 2010; Ciuleanu TE et al. Lancet 2009; Paz Ares L et al. J Clin Oncol 2013; Barlesi
et al. Ann Oncol 2014

2 YEARS SURVIVAL RATE NSCLC (non-squamous)
0%
5%
10%
15%
20%
25%
30%
35%
40%
ECOG1594 JMBD ECOG4599 PARAMOUNT AVAPERL
11%
19%23%
32%
39%
Schiller J, N Engl J Med 2002; Scagliotti, G. V. et al. J Clin Oncol 2008; Cappuzzo F et al.
Lancet Oncol 2010; Ciuleanu TE et al. Lancet 2009; Paz Ares L et al. J Clin Oncol 2013; Barlesi
et al. Ann Oncol 2014

2 YEARS SURVIVAL RATE NSCLC (non-squamous)
0%
5%
10%
15%
20%
25%
30%
35%
40%
ECOG1594 JMBD ECOG4599 PARAMOUNT AVAPERL
11%
19%23%
32%
39%
Schiller J, N Engl J Med 2002; Scagliotti, G. V. et al. J Clin Oncol 2008; Cappuzzo F et al.
Lancet Oncol 2010; Ciuleanu TE et al. Lancet 2009; Paz Ares L et al. J Clin Oncol 2013; Barlesi
et al. Ann Oncol 2014

EL EFECTO DIFERENCIAL DE LA
QUIMIOTERAPIA Y LAS TERAPIAS DIRIGIDAS

EL EFECTO DIFERENCIAL DE LA
QUIMIOTERAPIA Y LAS TERAPIAS DIRIGIDAS
QUIMIOTERAPIA

EL EFECTO DIFERENCIAL DE LA
QUIMIOTERAPIA Y LAS TERAPIAS DIRIGIDAS
QUIMIOTERAPIA
TERAPIAS DIRIGIDAS

Finally we can talk about long term survivors in
advanced melanoma
Presented By Christian Blank at 2018 ASCO Annual Meeting

January 2014…PS 3, EVA 8
• 51 years old female
• HBP, Obesity
• Ex-smoker: 8 Pack/year
• January 2014: LungAdenocarcinoma pT1bN0M1b
• PS 3
• Exon 21 L858R mut
• Clinical trial: afatinib
TKIs in NSCLC…how long should we treat?

January 2014…PS 3, EVA 8
November 2018…PS 0, EVA 0
• 51 years old female
• HBP, Obesity
• Ex-smoker: 8 Pack/year
• January 2014: LungAdenocarcinoma pT1bN0M1b
• PS 3
• Exon 21 L858R mut
• Clinical trial: afatinib
TKIs in NSCLC…how long should we treat?

How many of you would stop EGFR TKI right now?

Rational to sustain TKI inhibition: Disease Flare-Up
Chaft J.E, CCR 2011
• Flare after EGFR TKI cessation in 23% (n=14/61) leading to
hospitalization or death
• The median time to disease flare after TKI discontinuation was 8 days
(range 3–21).


What do patients want?

Patient preference
Blinman et al. Lung Cancer 2010

Sadfer T, NEJM 2018
Gilligan J Clin Oncol 2018

INNOVATION CHANGES THE GAME…

The classic approach…

Disease
Take pill
Killsomething
The classic approach…

Disease
Take pill
Killsomething
The classic approach…

Disease
Take pill
Killsomething
Disease
Geneticalteration
Targetedtherapy
The classic approach…

The new approach….
Disease
Take pill
Kill something
Disease
Genetic alteration
Targeted therapy

The new approach….
Disease
Take pill
Kill something
Disease
Genetic alteration
Targeted therapy
Organ/Disease
Microenviroment
Inmune System

UNIQUE ACTIVITY PATTERNS…
Ascierto AL, Frontiers in Oncol 2015

61 years old male
Active smoker 50 paq/year
May 2014: Stage IV squamous Cell Lung Cancer
cT4NxM1b (bilateral adrenal metastasis)
1st line: Platinum-Gem 6 cycles :PD
January 2015:
2nd line Docetaxel: severe acute infusion reaction
PS 1-2
June 2015: Clinical trial IO
THE PATIENT
CTLA-4, cytotoxic T-lymphocyte associated protein 4; PD-L1, programmed death
ligand 1

02/11/2018
PR after 24 minutes of anti PD-1 infusion….and more than 3 years without active treatment……

02/11/2018
PR after 24 minutes of anti PD-1 infusion….and more than 3 years without active treatment……

3 years after stopping IO…

Why would you want to stop ICI?

Why would you want to stop ICI?
• Do we have enough evidence for prolonged treatment?

Why would you want to stop ICI?
• Do we have enough evidence for prolonged treatment?
• Is the treatment working? PR, CR, SD…

Why would you want to stop ICI?
• Do we have enough evidence for prolonged treatment?
• Is the treatment working? PR, CR, SD…
• Patient choice (remember…the name of the dog)
– Inconvenience
– Toxicity (>gr 3), prolonged low grade toxicity

Why would you want to stop ICI?
• Do we have enough evidence for prolonged treatment?
• Is the treatment working? PR, CR, SD…
• Patient choice (remember…the name of the dog)
– Inconvenience
– Toxicity (>gr 3), prolonged low grade toxicity
• Economic resources

THE EVIDENCE…
SCARCE

Duration: Pivotal Advanced IO Lung Trials
First Line Advanced NSCLC Second LineKN-024 2 yrs (35 cycles) KN-010 2 yrsKN-189 2 yrs CM-057 IndefiniteKN-407 2 yrs CM-017 IndefiniteKN-042 2 yrs OAK IndefiniteCM 227 2 yrsIM150 IndefiniteIM132 Indefinite
Reck, NEJM 2016 Herbst, Lancet 2015Gandhi, NEJM 2018 Borghaei, NEJM 2015Paz-Ares, ASCO 2018 Brahmer, NEJM 2015Lopes, ASCO 2018 Rittmeyer, Lancet 2017Hellman, NEJM 2018Socinski, NEJM 2018
Spigel WCLC 2018

aConventional systemic therapies, excluding immuno-oncology therapies; bTreatment until PD, unacceptable toxicity or withdrawal of consent; treatment beyond investigator-assessed PD permitted; cAll patients on treatment at 1 year were randomized regardless of response status; dPrimary endpoint was incidence of high-grade select treatment-related AEs1,2
Exploratory endpointsd: safety/efficacy with continuous vs 1-year treatment, efficacy, other (eg, biomarkers, PK)
Key eligibility criteria
• Advanced/ metastatic NSCLC
• ≥1 prior systemic therapya
• ECOG PS 0−2
• Treated CNS metastases allowed
Stop nivolumab
Continuous nivolumab
Nivolumab3 mg/kg IV Q2W
Treatment for 1 yearb
Rc
Nivolumab retreatment allowed at PD
Spigel, ESMO 2017
Checkmate 153Continuous vs 1-Year Fixed-Duration

36
aPatients who did not have PD at randomization; minimum/median follow-up time post-randomization, 10.0/14.9 monthsbWith optional retreatment allowed at PDtx = treatment
Median, months(95% CI)
PFS rate, %
6-month 1-year
Continuous tx NR (NR) 80 65
1-year txb 10.3 (6.4, 15.2) 69 40
HR: 0.42 (95% CI: 0.25, 0.71)
No. at risk
1-year tx
Continuous tx
87 50 43 33 21 16 5 1 0
76 60 53 49 35 22 10 3 0
No. at risk
1-year tx
Continuous tx
87 50 43 33 21 16 5 1 0
76 60 53 49 35 22 10 3 0
Time post-randomization (months)
PF
S (
%)
0
20
40
60
80
100
0 3 6 9 12 15 18 21 24
Spigel, ESMO 2017
Checkmate 153PFS from Randomization

37
Median, months(95% CI)
Continuous tx NR (NR)
1-year txb,c 10.6 (4.8, NA)
HR: 0.45 (95% CI: 0.24, 0.85)
Median, months(95% CI)
Continuous tx NR (5.6, NA)
1-year txb 9.6 (4.5, 12.6)
HR: 0.44 (95% CI: 0.17, 1.09)
CR/PR SD
1-year tx 49 29 26 20 14 11 3 1 0
Continuous tx 53 45 41 39 28 17 7 2 0
No. at risk
0
20
40
60
80
100
PF
S (
%)
0 3 6 9 12 15 18 21 24
Time post-randomization (months)
38 21 17 13 7 5 2 0 0
23 15 12 10 7 5 3 1 0
0
20
40
60
80
100
PF
S (
%)
0 3 6 9 12 15 18 21 24
Time post-randomization (months)
Spigel, ESMO 2017
Checkmate 153PFS by Response

38
Median, months(95% CI)
OS rate, %
6-month
1-year
Continuous tx NR (NR) 97 88
1-year txb 23.2 (23.2, NA) 88 81
HR: 0.63 (95% CI: 0.33, 1.20)
74 72 67 62 41 29 7 2 0
79 74 70 61 38 23 4 0 0
No. at risk
1-year tx
Continuous tx
87
76
Time post-randomization (months)
0
20
40
60
80
100
OS
(%
)
0 3 6 9 12 15 18 21 24 27
Spigel, ESMO 2017
Checkmate 153OS from Randomization

5-Year Estimates of OS <br />Phase 1 nivolumab
Presented By Solange Peters at 2018 ASCO Annual Meeting

CM 003: heavily pretreated NSCLC population
Nivolumab up to 96 weeks
Gettinger S, et al. J Clin Oncol 2018
▪ 12/16 p who achieved a reponse on Nivolumab therapy
▪ 12 5-year survivors (75%) received no subsequent
therapy and were without evidence of progressive
disease at last follow-up.

KN 010: Pembrolizumab in previously treated advanced
NSCLC
Herbst R, et al. ESMO 2018
▪ 79 patients completed 35 cycles or 2
years of pembrolizumab
▪ 75 of 79 (95%) patients had a complete
response or partial response
▪ Response was ongoing in 48 patients
(64%)

Ipilimumab in melanoma: association
of response with survivalKN006. Pembrolizumab in melanoma:
association of response with survival

Relapse by PET response in melanoma patients receiving
checkpoint inhibition
Tan AC, et al. Ann Oncol 2018

PET and rebiopsy predictive value
Christainsen et al ASCO 2018

Long term toxicity…

¿PODEMOS CORRELACIONAR EL DESARROLLO DE
EFECTOS ADVEROS IR CON EL BENEFICIO A LA IO?
Weber et al. J Clin Oncol 2016

Los pacientes con CNMP que desarrollaron efectos adversos IR
alcanzaron mayor SG (13.2 vs 5.8 meses, p = 0.018). Owen et al, ASCO 2017
¿PODEMOS CORRELACIONAR EL DESARROLLO DE
EFECTOS ADVEROS IR CON EL BENEFICIO A LA IO?
Weber et al. J Clin Oncol 2016

Los pacientes con CNMP que desarrollaron efectos adversos IR
alcanzaron mayor SG (13.2 vs 5.8 meses, p = 0.018). Owen et al, ASCO 2017
¿PODEMOS CORRELACIONAR EL DESARROLLO DE
EFECTOS ADVEROS IR CON EL BENEFICIO A LA IO?
Weber et al. J Clin Oncol 2016Von Pawel J, et al. ESMO 2017

Slide 13
¿Cómo “de seguro” es retratar a los pacientes con IO
tras EA inmunorelacionados?

▪ 62 years old male
▪ Active smoker 45 pack/year
▪ Stage IV SCC in April 2014
▪ OAK trial: Atezolimumab 2nd
line since September 2014 to
April 2018, 62 cycles
▪ Gr 3 pneumonitis
▪ Stop therapy
▪ Ongoing complete response
▪ 55 years old female
▪ Active smoker 35 pack/year
▪ Stage IV Non-SCC January
2013
▪ OAK trial: Atezolimumab 2nd
line since February 2015: 66
cycles
▪ No significant toxicity
▪ Treatment ongoing

▪ 62 years old male
▪ Active smoker 45 pack/year
▪ Stage IV SCC in April 2014
▪ OAK trial: Atezolimumab 2nd
line since September 2014 to
April 2018, 62 cycles
▪ Gr 3 pneumonitis
▪ Stop therapy
▪ Ongoing complete response
▪ 55 years old female
▪ Active smoker 35 pack/year
▪ Stage IV Non-SCC January
2013
▪ OAK trial: Atezolimumab 2nd
line since February 2015: 66
cycles
▪ No significant toxicity
▪ Treatment ongoing

▪ 62 years old male
▪ Active smoker 45 pack/year
▪ Stage IV SCC in April 2014
▪ OAK trial: Atezolimumab 2nd
line since September 2014 to
April 2018, 62 cycles
▪ Gr 3 pneumonitis
▪ Stop therapy
▪ Ongoing complete response
▪ 55 years old female
▪ Active smoker 35 pack/year
▪ Stage IV Non-SCC January
2013
▪ OAK trial: Atezolimumab 2nd
line since February 2015: 66
cycles
▪ No significant toxicity
▪ Treatment ongoing

Presented By Sarah Goldberg at 2018 ASCO Annual Meeting

Take Home Message
Optimal duration of therapy in advanced cancer is still an issue to debate…overall talking about IO
Duration should be based on regimen data from pivotal trials• Two years can be an option for IO…• But care must be individualized for efficacy, QoL, toxicity, and patient choice
Future research is needed to study:• Shorter durations• Alternative schedules• Redosing / Repriming• Biomarkers to predict benefit

TENDIENDO PUENTES….THE WAY TO MOVE FORWARD