Gynecology 5th year, 5th & 6th lectures (Dr. Sallama Kamil)
47
م ي ح ر ل ا ن م ح ر ل ه ا ل ل م ا س ب م ي ح ر ل ا ن م ح ر ل ه ا ل ل م ا س بOvarian tumours Ovarian tumours By Dr. Sallama kamel By Dr. Sallama kamel
-
Upload
college-of-medicine-sulaymaniyah -
Category
Health & Medicine
-
view
3.413 -
download
5
description
The lecture has been given on May 16th & 18th, 2011 by Dr. Sallama Kamil.
Transcript of Gynecology 5th year, 5th & 6th lectures (Dr. Sallama Kamil)

الرحمن الله الرحمن بسم الله بسمالرحيمالرحيم
Ovarian Ovarian tumourstumours
By Dr. Sallama kamelBy Dr. Sallama kamel

The classification of ovarian cysts and The classification of ovarian cysts and tumourstumours::A.Non-neoplastic functional cystsA.Non-neoplastic functional cysts::
--Follicular cystsFollicular cysts..--Leuteal cystsLeuteal cysts..
--Theca- lutein and granulosa lutein cystsTheca- lutein and granulosa lutein cysts..--Endometriotic cystsEndometriotic cysts..
B.Primary ovarian neoplasmsB.Primary ovarian neoplasms::11 . .Epithelial tumours ( benign, borderline or malignant)Epithelial tumours ( benign, borderline or malignant)::
--Serous tumourSerous tumour..--Mucinous tumourMucinous tumour..
--Endometrioid tumourEndometrioid tumour-.-.--Clear cell ( mesonephroid ) tumourClear cell ( mesonephroid ) tumour..
--Brenner tumourBrenner tumour..--Undifferentiated carcinomaUndifferentiated carcinoma..

22..Sex cord stromal tumoursSex cord stromal tumours::
--Granulosa cell tumourGranulosa cell tumour..--Theca cell tumourTheca cell tumour..
--FibromaFibroma..--Androblastoma: sertoli-leydig cell tumourAndroblastoma: sertoli-leydig cell tumour..
--GynandroblastomaGynandroblastoma..
33..Germ cell Germ cell tumourtumour::a. Benigna. Benign::
--cystic Teratoma andcystic Teratoma and --solid teratomasolid teratoma..
b.Malignantb.Malignant::--DysgerminomaDysgerminoma..
--Malignant change in cystic teratomaMalignant change in cystic teratoma..--Malignant solid teratomaMalignant solid teratoma..
--Non-gestational choriocarcinomaNon-gestational choriocarcinoma..--Yolk sac tumour (endodermal sinus tumour)Yolk sac tumour (endodermal sinus tumour)..
C. Metastatic tumoursC. Metastatic tumours::

Physiological cystPhysiological cyst--They are simply large versions of the cysts They are simply large versions of the cysts
that forms in the ovary during the normal that forms in the ovary during the normal ovarian cycleovarian cycle..
--Most are asymptomatic and found incidentally Most are asymptomatic and found incidentally on pelvic examination or ultrasoundon pelvic examination or ultrasound..
--They are most common in young womenThey are most common in young women..--They may be a complication of ovarian They may be a complication of ovarian
inductioninduction..--They also occur in women with trophoblastic They also occur in women with trophoblastic
diseasedisease..

11..Follicular cystsFollicular cysts::it result from the non-rupture of a dominant follicle or the failure of atresia it result from the non-rupture of a dominant follicle or the failure of atresia in a non-dominant folliclein a non-dominant follicle..
22..Luteal cystsLuteal cysts : :
Less common than follicular cystLess common than follicular cyst..Are more likely to present with intra-peritoneal bleedingAre more likely to present with intra-peritoneal bleeding..They may also ruptureThey may also rupture..This is usually happens on day 20-26 of the cycleThis is usually happens on day 20-26 of the cycle . .
33..Theca-lutein and granulosa lutein cystsTheca-lutein and granulosa lutein cysts..--These occurs in association with Hydatidiform moles orThese occurs in association with Hydatidiform moles or
choriocarcinomachoriocarcinoma . .They are usually bilateral and usually resolve spontaneously afterThey are usually bilateral and usually resolve spontaneously afterevacuation of the moleevacuation of the mole..
- - Similar cysts may formed if excessive doses of gonadotrophins or Similar cysts may formed if excessive doses of gonadotrophins or ofof clomiphines are given to induce ovulation causing hyperstimulationclomiphines are given to induce ovulation causing hyperstimulation syndromesyndrome..

--In most of the cases physiological In most of the cases physiological cysts resolve spontaneously and cysts resolve spontaneously and does not need any surgical does not need any surgical interference unless they cause an interference unless they cause an acute symptoms or their size exceed acute symptoms or their size exceed 10cm10cm..

Epithelial tumoursEpithelial tumours::--These tumours arise from the ovarian surface epitheliumThese tumours arise from the ovarian surface epithelium..--So they arise from the Coelomic epithelium overlying the So they arise from the Coelomic epithelium overlying the
embryonic gonadal ridgeembryonic gonadal ridge..Since the epithelial covering of the ovary and the mullerianSince the epithelial covering of the ovary and the mullerian duct ( from which the tubal, endometrial and cervicalduct ( from which the tubal, endometrial and cervical epithelium are derived ) are both from coelomic epitheliumepithelium are derived ) are both from coelomic epithelium , ,
comparable metaplastic transformation into different types comparable metaplastic transformation into different types ofof epithelium is possibleepithelium is possible..
--So the cells may differentiate to endocervical cells giving rise So the cells may differentiate to endocervical cells giving rise to to mucinous cystadenomamucinous cystadenoma..
--Differentiation into endometrial cells give rise to Differentiation into endometrial cells give rise to Endometrioid tumourEndometrioid tumour..
--Differentiation to tubal epithelium give rise to Differentiation to tubal epithelium give rise to serous serous cystadenomacystadenoma..
--Differentiation along uro-epithelium give rise to Differentiation along uro-epithelium give rise to Brenner Brenner tumourtumour..They are most common in women over 40 years oldThey are most common in women over 40 years old..

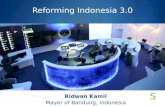
11..Serous cystadenomaSerous cystadenoma::
--These are the most common epithelial tumours These are the most common epithelial tumours with a range from benign to the highly with a range from benign to the highly malignantmalignant. .
--The benign form are called The benign form are called benign serous cystbenign serous cyst..--It is unilocular cyst with papilliferous processes It is unilocular cyst with papilliferous processes
on the inner surface and occasionally on the on the inner surface and occasionally on the outer surfaceouter surface..
--The lining epithelium is cuboidal or columnar and The lining epithelium is cuboidal or columnar and may be ciliatedmay be ciliated..
--The cyst contain thin serous fluidThe cyst contain thin serous fluid..--They are usually smaller than the mucinous They are usually smaller than the mucinous
tumourtumour..--They are often bilateralThey are often bilateral
--They occur most commonly in late reproductive They occur most commonly in late reproductive and early postmenopausal lifeand early postmenopausal life..

Serous cyst adenomaSerous cyst adenoma

The malignant form called Serous The malignant form called Serous papilliferous carcinomapapilliferous carcinoma::
--This is the commonest primary ovarian carcinomaThis is the commonest primary ovarian carcinoma..--It is bilateral in 50%It is bilateral in 50%..
-The growth often penetrates the capsule and -The growth often penetrates the capsule and project on the external surface with project on the external surface with dissemination of the cells into the peritoneal dissemination of the cells into the peritoneal cavity giving multiple seedling metastases and cavity giving multiple seedling metastases and ascites.ascites.
-The cyst contains many papillary processes which -The cyst contains many papillary processes which have proliferated so much that they almost fill have proliferated so much that they almost fill the cavity and there may be exophytic papillary the cavity and there may be exophytic papillary growth on the surface.growth on the surface.
-The lining cells are multilayer and may invade -The lining cells are multilayer and may invade normal tissues.normal tissues.

Serous papilliferous Serous papilliferous carcinomacarcinoma::

22..Mucinous cystadenomaMucinous cystadenoma::
--The 2The 2ndnd most common epithelial tumour most common epithelial tumour..--They are large, unilateral , multilocular cysts with smooth They are large, unilateral , multilocular cysts with smooth
inner surfaceinner surface..--The lining epithelium is columnar mucous-secreting cellsThe lining epithelium is columnar mucous-secreting cells..
--The cyst contain thick glutinous fluidThe cyst contain thick glutinous fluid..
Malignant mucinous cyst (Mucinous Malignant mucinous cyst (Mucinous carcinoma)carcinoma) : :
Constitute 10% of ovarian cancersConstitute 10% of ovarian cancers..--On histological examination, 5% of mucinous cysts found to On histological examination, 5% of mucinous cysts found to
be malignantbe malignant . .
Epithelial tumours of borderline malignancyEpithelial tumours of borderline malignancy:: - -mean that the tumour carry some of the features of mean that the tumour carry some of the features of
malignancy( e.g. multilayering of cells and nuclear atypia)malignancy( e.g. multilayering of cells and nuclear atypia)..--But there is no stromal invasionBut there is no stromal invasion..

33..Endometrioid cystadenomaEndometrioid cystadenoma::
--These are very similar to ovarian endometriosisThese are very similar to ovarian endometriosis..
--They may be associated with pelvic pain and They may be associated with pelvic pain and dyspareunia due to adhesionsdyspareunia due to adhesions..
44..Clear cell tumours( mesonephroid)Clear cell tumours( mesonephroid)::
--They arise from serosal cells showing little They arise from serosal cells showing little differentiation, and are only rarely benigndifferentiation, and are only rarely benign..
--The typical histological appearance is of clear or The typical histological appearance is of clear or hobnail cellshobnail cells

55..Brenner tumoursBrenner tumours::
Macroscopically: Macroscopically: a Brenner tumour resembles a a Brenner tumour resembles a fibroma, being a solid tumour with a white cut fibroma, being a solid tumour with a white cut surfacesurface..
Histologically: Histologically: -It consists of islands of round -It consists of islands of round transitional-like epithelium in a dense fibrotic transitional-like epithelium in a dense fibrotic stroma giving a solid appearancestroma giving a solid appearance..

Germ cell tumoursGerm cell tumours::• •• •It is among the commonest ovarian tumours seen in women of less It is among the commonest ovarian tumours seen in women of less
than 30years oldthan 30years old..
●●Amongst women under 20 years ,up to 80% of ovarian malignancies Amongst women under 20 years ,up to 80% of ovarian malignancies are due to germ cell tumoursare due to germ cell tumours..
••Overall only 2-3 percent are malignantOverall only 2-3 percent are malignant. .
••These tumours arise from a totipotential germ cellThese tumours arise from a totipotential germ cell
••Thus they contain element of all three germ layer( embryonic Thus they contain element of all three germ layer( embryonic differentiation)differentiation)..Differentiation into embryonic tissues result in teratomaDifferentiation into embryonic tissues result in teratoma
((dermoid cystdermoid cyst .) .)
••Differentiation into Differentiation into extra-embryonic tissuesextra-embryonic tissues results in results in ovarian ovarian choriocharcinoma or endodermal sinus tumourchoriocharcinoma or endodermal sinus tumour..
••When neither embryonic nor extra-embryonic differentiation occurs, When neither embryonic nor extra-embryonic differentiation occurs, dysgerminoma resultsdysgerminoma results..

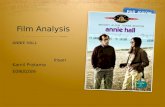
Dermoid cyst (mature cystic teratoma)Dermoid cyst (mature cystic teratoma)--This is the commonest germ cell tumour and it is benignThis is the commonest germ cell tumour and it is benign..
--It results from differentiation into embryonic tissuesIt results from differentiation into embryonic tissues..
--It account for about 40% of all ovarian neoplasmIt account for about 40% of all ovarian neoplasm..
--It is most common in young women and the median age of It is most common in young women and the median age of presentation is 30 years oldpresentation is 30 years old..
--it contain a variety of tissues derived from the two or more of the it contain a variety of tissues derived from the two or more of the primary germ layersprimary germ layers....
--The dermoid cyst is usually unillocular cystThe dermoid cyst is usually unillocular cyst..--Less than 15cm in diameterLess than 15cm in diameter
--It is often lined by epithelium like the epidermis and contain skin It is often lined by epithelium like the epidermis and contain skin appendages, teeth , sebaceous material , hair and nervous appendages, teeth , sebaceous material , hair and nervous tissues, cartilage bone and thyroid tissuestissues, cartilage bone and thyroid tissues . .
--The cavity of the cyst contain yellow greasy materialThe cavity of the cyst contain yellow greasy material..

--The majority of dermoid cysts (60%) are asymptomaticThe majority of dermoid cysts (60%) are asymptomatic..
--However it may undergo torsionHowever it may undergo torsion..
--Less commonly it may rupture spontaneously, either Less commonly it may rupture spontaneously, either suddenly causing an acute abdomen and chemical suddenly causing an acute abdomen and chemical peritonitis, or slowly causing chronic granulomatous peritonitis, or slowly causing chronic granulomatous peritonitisperitonitis..
--During pregnancy, rupture is more common due to During pregnancy, rupture is more common due to external pressure from expanding gravid uterus or to external pressure from expanding gravid uterus or to trauma during deliverytrauma during delivery..
Mature solid teratomaMature solid teratoma::
--These are tumours contain mature tissues just like the These are tumours contain mature tissues just like the dermoid cyst but are soliddermoid cyst but are solid..

Mature cystic teratomaMature cystic teratoma

Malignant germ cell tumoursMalignant germ cell tumours::
These are rare tumours accounting for only These are rare tumours accounting for only 3% of ovarian cancers3% of ovarian cancers..
11..DysgerminomaDysgerminoma::
2.Yolk sac tumour ( endodermal sinus tumour). Secret alpha feto protein
33..Immature Solid teratomaImmature Solid teratoma::
44..Non gestational choriocarcinoma: secret Non gestational choriocarcinoma: secret HCGHCG..

sex cord stromal tumourssex cord stromal tumours::
--These account for only 4% of benign ovarian tumoursThese account for only 4% of benign ovarian tumours..--They occur at any age from prepubertal children to They occur at any age from prepubertal children to
elderly, postmenopausal womenelderly, postmenopausal women..--They secrete hormones and present with the results of They secrete hormones and present with the results of
inappropriate hormone effectsinappropriate hormone effects..
11..Granulosa cell tumours: secret estrogenGranulosa cell tumours: secret estrogen..
22..Theca cell tumours: also secret estrogenTheca cell tumours: also secret estrogen..
33..FibromaFibroma : :--MeigMeig’’s syndromes syndrome ( ascites , pleural effusion in association ( ascites , pleural effusion in association with a fibroma of the ovary) is seen in only 1% of caseswith a fibroma of the ovary) is seen in only 1% of cases . .
44..Sertoli- leydig cell tumoursSertoli- leydig cell tumours::

Clinical presentation of ovarian Clinical presentation of ovarian tumourstumours
--AsymptomaticAsymptomatic..--PainPain..
--Abdominal swellingAbdominal swelling..--Pressure effectsPressure effects..
--Menstrual disturbancesMenstrual disturbances..--Hormonal effectsHormonal effects..
--Abnormal cervical smearAbnormal cervical smear..

11..AsymptomaticAsymptomatic::Many benign ovarian tumours are found incidentally in the Many benign ovarian tumours are found incidentally in the course of investigating another unrelated problem or course of investigating another unrelated problem or during a routine examinationduring a routine examination..
22..PainPain:: --Acute pain from an ovarian tumour may result fromAcute pain from an ovarian tumour may result from
complication e.g. torsion, rupture, haemorrhage or infectioncomplication e.g. torsion, rupture, haemorrhage or infection..
--TorsionTorsion give rise to a sharp, constant pain caused by give rise to a sharp, constant pain caused by ischaemia of the cyst and areas may become infarctedischaemia of the cyst and areas may become infarcted..
--HaemorrhageHaemorrhage into the cyst may cause pain as the capsule is into the cyst may cause pain as the capsule is stretchedstretched..
--RuptureRupture of the cyst causes intraperitoneal bleeding of the cyst causes intraperitoneal bleeding mimickingmimicking
ectopic pregnancy (this happens mostly with a luteal cyst )ectopic pregnancy (this happens mostly with a luteal cyst )..

33..Abdominal swellingAbdominal swelling::
--Patients seldom note abdominal swelling until the Patients seldom note abdominal swelling until the tumour is very largetumour is very large. .
--A benign mucinous cyst may occasionally fill the entire A benign mucinous cyst may occasionally fill the entire abdominal cavityabdominal cavity..
44 . .pressure effectspressure effects.. --Gastro-intestinal or urinary symptoms may result from Gastro-intestinal or urinary symptoms may result from
pressure of large tumourpressure of large tumour..--In extreme cases, oedema of the legs, varicose veins In extreme cases, oedema of the legs, varicose veins
and haemorrhoids may resultand haemorrhoids may result..
-55..menstrual disturbancesmenstrual disturbances:: -Occasionally the patient will complain of menstrual Occasionally the patient will complain of menstrual
disturbances but this may coincidence rather than disturbances but this may coincidence rather than due to the tumourdue to the tumour..

66..hormonal effectshormonal effects: :
--rarely Sex cord tumours may present with rarely Sex cord tumours may present with oestrogens effects such as precocious oestrogens effects such as precocious puberty, menorrhagia and glandular puberty, menorrhagia and glandular hyperplasia, breast enlargement and hyperplasia, breast enlargement and postmenopausal bleedingpostmenopausal bleeding..
--Secretion of androgens may cause hirsuitism Secretion of androgens may cause hirsuitism and acne initially progressing to frank and acne initially progressing to frank virilism with deepening of the voice or virilism with deepening of the voice or clitoral hypertrophyclitoral hypertrophy..

DiagnosisDiagnosis::11..Full historyFull history::
--Details of the presenting symptoms and a full gynaecological historyDetails of the presenting symptoms and a full gynaecological history should be obtained with particular reference to the date of the lastshould be obtained with particular reference to the date of the last menstrual period , the regularity of the cycle, any previousmenstrual period , the regularity of the cycle, any previous pregnancies , contraception, medication and family historypregnancies , contraception, medication and family history
( (particularly of ovarian, breast and bowel cancerparticularly of ovarian, breast and bowel cancer.) .)
22..Examination ( abdominal and pelvic examination)Examination ( abdominal and pelvic examination)::--If the patient presented with acute abdomen look for evidence ofIf the patient presented with acute abdomen look for evidence of
hypovolaemiahypovolaemia..
--The neck , axilla and groins should be examined for lymphadenopathyThe neck , axilla and groins should be examined for lymphadenopathy..
--A malignant ovarian tumour may cause a pleural effusionA malignant ovarian tumour may cause a pleural effusion..--This is much less commonly found with benign tumourThis is much less commonly found with benign tumour..
--Also some patient may have ankle oedemaAlso some patient may have ankle oedema..--The abdomen should be inspected for distension by fluid (ascites) orThe abdomen should be inspected for distension by fluid (ascites) or
by the tumour itselfby the tumour itself..--A male distribution of hair may suggest a rare androgen-producingA male distribution of hair may suggest a rare androgen-producing
tumourstumours..

Bimanual examinationBimanual examination::
--This is an essential part of assessmentThis is an essential part of assessment..
--To palpate the mass , its mobility, To palpate the mass , its mobility, consistencyconsistency..
--Presence of nodules in the pouch of Douglas Presence of nodules in the pouch of Douglas and the degree of tendernessand the degree of tenderness..
--A cystic mobile mass is mostly benignA cystic mobile mass is mostly benign , ,
while a hard, irregular fixed mass is likely to while a hard, irregular fixed mass is likely to be malignantbe malignant..

InvestigationsInvestigations::
11..UltrasoundUltrasound--Trans-abdominal and trans-vaginal ultrasound can Trans-abdominal and trans-vaginal ultrasound can
demonstrate the presence of an ovarian mass with demonstrate the presence of an ovarian mass with reasonable sensitivity and specificityreasonable sensitivity and specificity..
--However it can not distinguish reliably between However it can not distinguish reliably between benign and malignant tumours but solid masses are benign and malignant tumours but solid masses are more likely to be malignant than the purely cystic more likely to be malignant than the purely cystic massmass..
--The use of colour- flow Doppler may increase the The use of colour- flow Doppler may increase the reliability of ultrasoundreliability of ultrasound . .
--CT scan and MRICT scan and MRI can be used but are more expensive can be used but are more expensive..

22..Radiological investigationsRadiological investigations::
--A chest X- ray is essential to detect metastatic disease A chest X- ray is essential to detect metastatic disease in the lungs or a pleural effusionin the lungs or a pleural effusion. .
--Occasionally an abdominal X-ray may show Occasionally an abdominal X-ray may show calcification, suggesting the possibility of a benign calcification, suggesting the possibility of a benign teratomateratoma..
--A barium enema is indicated only if the mass is A barium enema is indicated only if the mass is irregular or fixed, or if there are bowel symptomsirregular or fixed, or if there are bowel symptoms..
33..Blood test and serum markersBlood test and serum markers::--Elevated WBCElevated WBC count may indicate infection count may indicate infection..
--CaCa125125
Raised serum CaRaised serum Ca125125 is strongly suggestive of ovarian is strongly suggestive of ovarian carcinoma, especially in postmenopausal womencarcinoma, especially in postmenopausal women . .

- -B-HCGB-HCG level is elevated in women with level is elevated in women with choriocarcinomachoriocarcinoma..
--OestradiolOestradiol levels may be elevated in some levels may be elevated in some women with physiological follicular cysts women with physiological follicular cysts and sex cord stromal tumoursand sex cord stromal tumours..
--AndrogensAndrogens are increased with Sertoli-lydig are increased with Sertoli-lydig tumourstumours..
--Raised alpha-fetoproteinRaised alpha-fetoprotein levels suggest a levels suggest a yolk sac tumouryolk sac tumour..

Management of benign ovarian Management of benign ovarian tumourstumours::
This will depend upon theThis will depend upon the --Severity of the symptomsSeverity of the symptoms..
--Age of the patientAge of the patient. . --The risk of malignancyThe risk of malignancy..
--Her desire for future pregnancyHer desire for future pregnancy..
The asymptomatic womenThe asymptomatic women::The older womenThe older women::
--Women over 50 years of age are more Women over 50 years of age are more likely to have a malignancy so likely to have a malignancy so surgery is usually indicatedsurgery is usually indicated..

In pre-menopausal womenIn pre-menopausal women:: --Young women of less than 35 years are Young women of less than 35 years are
both more likely to wish to have further both more likely to wish to have further children and are less likely to have children and are less likely to have malignant epithelial tumourmalignant epithelial tumour..
--A clear unilocular cyst of 3-10 cm identifiedA clear unilocular cyst of 3-10 cm identified by ultrasound should be re- examined afterby ultrasound should be re- examined after
1212 weeks for evidence of diminution in sizeweeks for evidence of diminution in size. .

- -If the cysts persists, such women may be followed If the cysts persists, such women may be followed with a six-monthly ultrasound and Ca125 estimationswith a six-monthly ultrasound and Ca125 estimations..
--If the cyst does enlarge , laparoscopy or laparotomy may If the cyst does enlarge , laparoscopy or laparotomy may be indicatedbe indicated..
..A cyst of more than 10 cm is unlikely to be physiological A cyst of more than 10 cm is unlikely to be physiological or to resolve spontaneously and operation indicatedor to resolve spontaneously and operation indicated . .
--The use of combined oral contraceptive pills is unlikely The use of combined oral contraceptive pills is unlikely to accelerate the resolution of a functional cystto accelerate the resolution of a functional cyst..
The patient with symptomsThe patient with symptoms::
If the patient present with severe acute pain or signs ofIf the patient present with severe acute pain or signs of
intraperitoneal bleeding an emergency laparoscopy orintraperitoneal bleeding an emergency laparoscopy or
laparotomy will be requiredlaparotomy will be required..

The pregnant patientThe pregnant patient::
--An ovarian cyst in pregnant women may undergo torsion or An ovarian cyst in pregnant women may undergo torsion or may bleedmay bleed..
--The pregnant women with an ovarian cyst is a special case The pregnant women with an ovarian cyst is a special case because of the risk of surgery to the fetusbecause of the risk of surgery to the fetus..
--Thus if the patient present with acute painThus if the patient present with acute pain due to due to torsion or haemorrhage into an ovarian cyst or if torsion or haemorrhage into an ovarian cyst or if appendicitis is a possibility, the correct course is to appendicitis is a possibility, the correct course is to undertake undertake a laparotomy regardless the stage of the a laparotomy regardless the stage of the pregnancypregnancy..
--The operation should be covered with by tocolytic drugs and The operation should be covered with by tocolytic drugs and performed in a center with intensive neonatal careperformed in a center with intensive neonatal care..
--If asymptomatic cyst is discovered during the 1If asymptomatic cyst is discovered during the 1stst trimestertrimester, it is prudent to wait until after 14 weeks, it is prudent to wait until after 14 weeks’’ gestation before removing itgestation before removing it . .

--This avoids the risk of removing a corpus luteal cyst This avoids the risk of removing a corpus luteal cyst upon which the pregnancy might still be dependentupon which the pregnancy might still be dependent..
--In the 2In the 2ndnd and 3 and 3rdrd trimesters , the management of an trimesters , the management of an asymptomatic ovarian cyst may be either asymptomatic ovarian cyst may be either conservative or surgicalconservative or surgical..
--Cysts < 10cm , which have simple appearance on U/S , Cysts < 10cm , which have simple appearance on U/S , are unlikely to be malignant or to result in cyst are unlikely to be malignant or to result in cyst accident and may therefore be followed by U/Saccident and may therefore be followed by U/S..
--Many may resolve spontaneouslyMany may resolve spontaneously. .
--If the cyst unresolved 6 weeks postpartum , surgery If the cyst unresolved 6 weeks postpartum , surgery indicatedindicated..

--Malignancy is uncommon in pregnancy occurring in Malignancy is uncommon in pregnancy occurring in less than 3% of the cystsless than 3% of the cysts..
--However a cyst with a features suggestive of malignancy onHowever a cyst with a features suggestive of malignancy on U/S , or one that is growing, should be removed surgicallyU/S , or one that is growing, should be removed surgically..
--The tumour marker C 125 is not useful in pregnancy since it The tumour marker C 125 is not useful in pregnancy since it may bemay be elevated in normal pregnancieselevated in normal pregnancies..
Prepupertal girlPrepupertal girl::--Ovarian cysts are uncommon and often benignOvarian cysts are uncommon and often benign..
--Teratoma and follicular cysts are the most commonTeratoma and follicular cysts are the most common..--Presentation may be abdominal pain, distension or precocious Presentation may be abdominal pain, distension or precocious
pubertypuberty..--Management depends onManagement depends on : :
--relief of symptomsrelief of symptoms . .--exclusion of malignancy andexclusion of malignancy and
--conservation of maximum ovarian tissue without depressing fertilityconservation of maximum ovarian tissue without depressing fertility..

Types of surgery for apparently benign Types of surgery for apparently benign ovarian tumoursovarian tumours::
For young women less than 35 yearsFor young women less than 35 years::
11..Cystectomy ( removal of the cyst only)Cystectomy ( removal of the cyst only)..
22..Oophorectomy( removal of the ovary with the Oophorectomy( removal of the ovary with the cyst)cyst)..
For woman more than 45 yearsFor woman more than 45 years with ovarian with ovarian cyst more than 6cm in diameter it is advisable to cyst more than 6cm in diameter it is advisable to do total abdominal hysterectomy and bilateral do total abdominal hysterectomy and bilateral salpingo-oopgorectomysalpingo-oopgorectomy..

Malignant disease of the ovaryMalignant disease of the ovary::
--Most ovarian tumours are of epithelial originMost ovarian tumours are of epithelial origin..
--They are rare before the age of 35 years, but the incidence They are rare before the age of 35 years, but the incidence increases with age to a peak in the 50-70 yearsincreases with age to a peak in the 50-70 years..
--Most epithelial tumours are not discovered until they have Most epithelial tumours are not discovered until they have spread widelyspread widely..
--Surgery and chemotherapy forms the main stay of treatmentSurgery and chemotherapy forms the main stay of treatment..
The results are poorThe results are poor..
--The 5 year survival is less than 25%The 5 year survival is less than 25%..
--Only 3 % of ovarian cancers are seen in women younger than Only 3 % of ovarian cancers are seen in women younger than 35 years and most are non-epithelial cancers such as germ 35 years and most are non-epithelial cancers such as germ cell tumourscell tumours..

Risk factors predisposing for ovarian cancerRisk factors predisposing for ovarian cancer::Continuous ovulation increase the risk as inContinuous ovulation increase the risk as in::
11..NulliparityNulliparity..22..Early menarche and Late menopauseEarly menarche and Late menopause , both of these are , both of these are
associatedassociated with long estimated numbers of years of ovulationwith long estimated numbers of years of ovulation . .
33..increasing age at first birthincreasing age at first birth..44..The prolonged use of drugs for induction of ovulationThe prolonged use of drugs for induction of ovulation..
55..Exposure to environmental substances e.g. Talc and Exposure to environmental substances e.g. Talc and asbestosesasbestoses..
66..Family history of ovarian cancerFamily history of ovarian cancer::There is a family history in 5-10 % of women with epithelial There is a family history in 5-10 % of women with epithelial cancerscancers..A woman with one affected close relative has risk of 2.5%A woman with one affected close relative has risk of 2.5%With two affected close relatives the risk increase to 30-40%With two affected close relatives the risk increase to 30-40%..
--Breast feeding reduce the riskBreast feeding reduce the risk..--Also Oral contraceptive use reduces the risk by 50% after Also Oral contraceptive use reduces the risk by 50% after
5years of use5years of use..

Staging of ovarian cancer (FIGO staging )Staging of ovarian cancer (FIGO staging )::The staging of ovarian cancer is a clinical stagingThe staging of ovarian cancer is a clinical stagingStage 1Stage 1 growth limited to the ovariesgrowth limited to the ovaries..
IaIa growth limited to one ovarygrowth limited to one ovary..No ascites, no tumour on external surfaces ; capsule intactNo ascites, no tumour on external surfaces ; capsule intact..
Ib tumour limited to both ovariesIb tumour limited to both ovaries..No ascites, no tumour on external surfaces; capsule intactNo ascites, no tumour on external surfaces; capsule intact..
Ic either stage 1a or 1b with ascites contain malignant cells or tumour on Ic either stage 1a or 1b with ascites contain malignant cells or tumour on the surface of one or both ovariesthe surface of one or both ovaries..
Stage IIStage II: growth involving one or both ovaries with pelvic extension: growth involving one or both ovaries with pelvic extension..
Stage III:Stage III: growth involving one or both ovaries with peritoneal implants growth involving one or both ovaries with peritoneal implants outside the pelvis or positive retroperitoneal or inguinal lymph nodes or outside the pelvis or positive retroperitoneal or inguinal lymph nodes or superficial liver metastasissuperficial liver metastasis
Stage IV :Stage IV :growth involving one or both ovaries with distantgrowth involving one or both ovaries with distant metastasis,parenchymal liver metastasis equal stage 1Vmetastasis,parenchymal liver metastasis equal stage 1V..

Spread of ovarian malignanciesSpread of ovarian malignancies::
- -direct spread:direct spread: usually to the pelvic peritoneum and usually to the pelvic peritoneum and other pelvic organs ( uterus and broad ligament )other pelvic organs ( uterus and broad ligament )..
--Lymphatic spreadLymphatic spread commonly involves the pelvic and commonly involves the pelvic and the para-aortic nodesthe para-aortic nodes..
Spread may also involves the nodes of the neck or Spread may also involves the nodes of the neck or inguinal regioninguinal region . .
--Haematogenous spreadHaematogenous spread
--usually occurs late and involves mainly the liver, and usually occurs late and involves mainly the liver, and lunglung..
--Bone and brain metastasis sometimes seenBone and brain metastasis sometimes seen..

Presentation and diagnosisPresentation and diagnosis::
- -Vague abdominal pain or discomfort is the commonest Vague abdominal pain or discomfort is the commonest presenting complaintpresenting complaint..
--Distension or feeling a lump is the next most frequentDistension or feeling a lump is the next most frequent..--The patient may complain ofThe patient may complain of::
* * IndigestionIndigestion..* * Urinary frequencyUrinary frequency . .
* * Weight lossWeight loss..--Or rarely abnormal menses or postmenopausal bleedingOr rarely abnormal menses or postmenopausal bleeding..
A hard abdominal mass arising from the pelvis is highly A hard abdominal mass arising from the pelvis is highly suggestive especially with ascitessuggestive especially with ascites..
- - A fixed, hard, irregular pelvic mass is usually felt best by A fixed, hard, irregular pelvic mass is usually felt best by combined vaginal and rectal examinationcombined vaginal and rectal examination..The neck and groin should also be examined for enlarged The neck and groin should also be examined for enlarged nodesnodes..

InvestigationsInvestigations::
11..full blood countfull blood count..
22..Urea, electrolyte and liver function testUrea, electrolyte and liver function test..
33..Chest x-rayChest x-ray..
44..Sometimes, barium enema and colonoscopy is needed to Sometimes, barium enema and colonoscopy is needed to differentiate between an ovarian and a colonic tumour or to differentiate between an ovarian and a colonic tumour or to assess bowel involvementassess bowel involvement..
55..IVP (intravenous urography)IVP (intravenous urography)..
66..Ultrasonography may help to confirm the presence of a Ultrasonography may help to confirm the presence of a pelvic .mass and detect ascitespelvic .mass and detect ascites..
77..Tumour markers e.g. Ca 125Tumour markers e.g. Ca 125..
88..In most women the diagnosis is uncertain before laparotomy is In most women the diagnosis is uncertain before laparotomy is undertakenundertaken..

SurgerySurgery::--Surgery is the mainstay of both the diagnosis and the treatment of ovarian Surgery is the mainstay of both the diagnosis and the treatment of ovarian
cancercancer..
--A vertical incision is required for an adequate exploration of the upper A vertical incision is required for an adequate exploration of the upper abdomenabdomen..
--A sample of ascitic fluid or peritoneal washings with normal saline should be A sample of ascitic fluid or peritoneal washings with normal saline should be taken for cytologytaken for cytology..
--The pelvis and upper abdomen are explored carefully to identify metastatic The pelvis and upper abdomen are explored carefully to identify metastatic diseasedisease..
--The therapeutic objective of surgery for ovarian cancer is the removal of all The therapeutic objective of surgery for ovarian cancer is the removal of all tumour tissuestumour tissues..
--This is usually possible in the majority of stage I and stage II, but impossible This is usually possible in the majority of stage I and stage II, but impossible in advanced casesin advanced cases..

To resect all visible tumour requiresTo resect all visible tumour requires a total a total hysterectomy, bilateral salpingo-hysterectomy, bilateral salpingo-oophorectomy and infra-colic omentectomyoophorectomy and infra-colic omentectomy..
--However , in a young , nulliparous woman with However , in a young , nulliparous woman with unilateral tumour and no ascites ( stage Ia ), unilateral tumour and no ascites ( stage Ia ), unilateral salpingo-oophorectomy may be done after unilateral salpingo-oophorectomy may be done after careful exploration to exclude metastatic disease , careful exploration to exclude metastatic disease , and curettage of the uterine cavity to exclude a and curettage of the uterine cavity to exclude a synchronous endometrial tumoursynchronous endometrial tumour..
--If the is subsequently found to be poorly differentiated If the is subsequently found to be poorly differentiated or if the washings are positive, a second operation to or if the washings are positive, a second operation to clear the pelvis will be necessaryclear the pelvis will be necessary..

--For older women who complete her family a total For older women who complete her family a total hysterectomy and bilateral salpingo-oophorectomy hysterectomy and bilateral salpingo-oophorectomy is usually doneis usually done..ChemotherapyChemotherapy::
--Women with stage Ia or Ib and well or moderately Women with stage Ia or Ib and well or moderately differentiated tumours will not require further differentiated tumours will not require further treatmenttreatment..
--All other patient with invasive ovarian carcinoma All other patient with invasive ovarian carcinoma require chemotherapy (stage II-IV require chemotherapy (stage II-IV ––possibly stage possibly stage Ic )Ic )..
--There is no evidence that adjuvant therapy affects There is no evidence that adjuvant therapy affects the outcome in women with borderline tumourthe outcome in women with borderline tumour..
--Drugs used are Carboplatin, cisplatin and taxolDrugs used are Carboplatin, cisplatin and taxol . .

PrognosisPrognosis::
Borderline tumourBorderline tumour::
Long term prognosis excellent in most casesLong term prognosis excellent in most cases..
Invasive tumours- 5 year survival ratesInvasive tumours- 5 year survival rates..---90%90% for Stage Ia and 1b ( well or moderately for Stage Ia and 1b ( well or moderately
differentiated )differentiated )..
--1010 % % for stage IIIfor stage III..
--23%23% overalloverall..

THANK THANK YOUYOU