Guz trzustki- rms - WordPress.com · Male-to-female ratio 4:1, in long segment 1,5-2:1 Incidence -...
62
Przemysław Gałązka, MD, PhD Clinical Ward of General and Oncological Surgery for Children and Adolescents CM UMK Bydgoszcz, Poland Head of the Department: Irena Daniluk-Matraś, MD, PhD
-
Upload
nguyenminh -
Category
Documents
-
view
213 -
download
0
Transcript of Guz trzustki- rms - WordPress.com · Male-to-female ratio 4:1, in long segment 1,5-2:1 Incidence -...

Przemysław Gałązka, MD, PhD
Clinical Ward of General and Oncological Surgery
for Children and Adolescents
CM UMK Bydgoszcz, Poland
Head of the Department: Irena Daniluk-Matraś, MD, PhD

Hirschsprung`s disease
One of the most common causes of
intestinal obstruction in newborns.
Absence of ganglion cells in the distal
bowel and extending proximally for
varying distances.
First description - 1691 r Frederick
Ruysch, 1886 r. Harold Hirschsprung

Male-to-female ratio 4:1, in long segment 1,5-
2:1
Incidence - 1 in 5000 live births
Distance of aganglionosis:
- 75% rectosigmoid
- 17% sigmoid, splenic flexure or transverse
colon
- 8% total colon along with a short segment of
terminal ileum
Cases of total intestinal aganglionosis or skip
lesions

Neural crest-derived neuroblasts first
appear in the developing esophagus at
5 weeks, and then migrate down to the
anal canal in a cranio-caudal direction
during 5th to 12th weeks of gestation
The ealier the arrest of migration, the
longer the aganglionic segment
Other theories: changes in
microenvironment (matrix proteins),
disturbing of migration or maturation of
the ganglion cells

3,6-7,8% reported incidence
of familial cases
15-21% incidence in TCA
Dominant gens with
incomplete penetration in
TCA. Recessive gens with low
penetration for recto-sigmoid
disease

4,5-16% of all cases of HD – Down
syndrome
Other genes: RET (mutation in 50% of
familial cases, 20% of sporadic cases)
Hereditary syndromes with association
of HS: Waardenburg syndrome, Smith-
Lemli-Opitz, von Recklinghausen`s
syndrome

HD
Impaired
process of
neuroblasts
migration
IND
Impaired
process of
neuroblasts
maturation

IND type A (5%) - congenital aplasia or
hypoplasia of the sympathetic innervation
(neonatal period: obstruction, diarrhoea,
bloody stools)
IND type B – hyperganglionosis of the
submucous and myenteric plexuses , giant
ganglia (usually
Hypoganglionosis
Internal Sphincter Achalasia
Smooth Muscle Cell Disorders (MMIHS-
megacystis microcolon intestinal hypoperistalsis
syndrome)
Neonatal bowel obstruction:
- colonic atresia, - meconium ileus, -
meconium plug syndrome, - small left
colon syndrome, - malrotation, - low
anorectal malformation, - intestinal
motility disorder / pseudo-obstruction, -
necrotizing enterocolitis, medical
causes: sepsis, electrolyte abnormalities,
drugs, hypothyroidism

Aganglionic bowel:
* Absence of ganglion cells in submucosal and myenteric plexus.
* Marked increase in acetylcholinesterase positive fibers in lamina propria and hypertrophic nerve trunks in the submucosa
Hypoganglionic bowel:
* Sparse and small myenteric ganglia with no- or low ACHE activity in lamian propria or muscularis mucosae.

80-90% are diagnosed during the
neonatal period
Over 90% of affected patients fail to
pass the meconium in the first 24 hours
of life
1/3 of babies with HD present with
diarrhoea

constipation
abdominal distension
vomiting
diarrhoea
Enterocolitis (life threatening condition!)

Clinical features
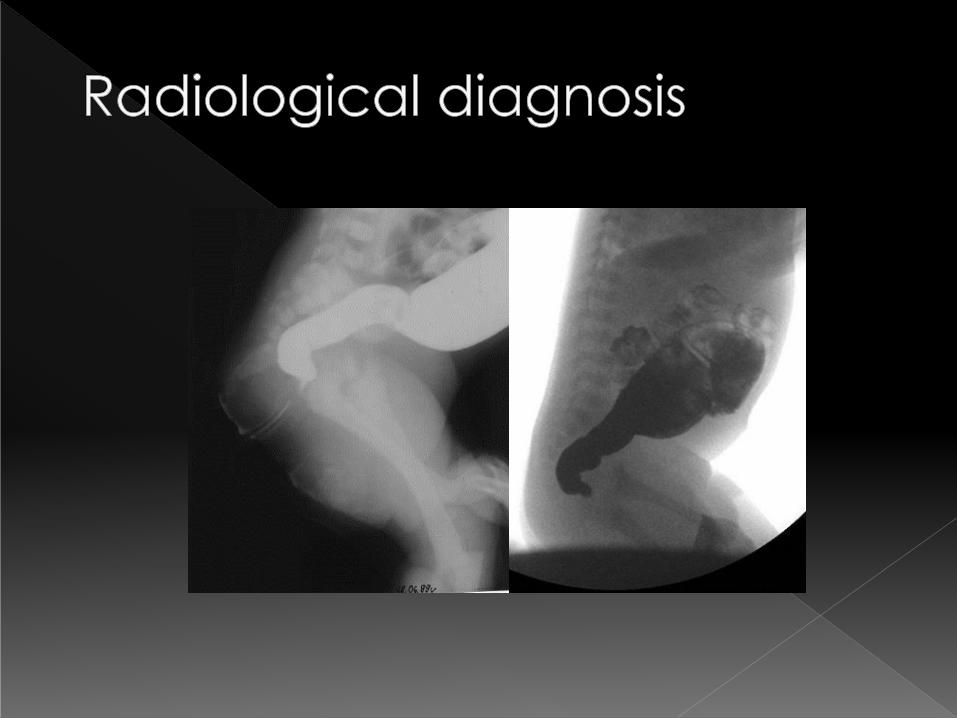
Radiological diagnosis
Anorectal manometry
Rectal biopsy

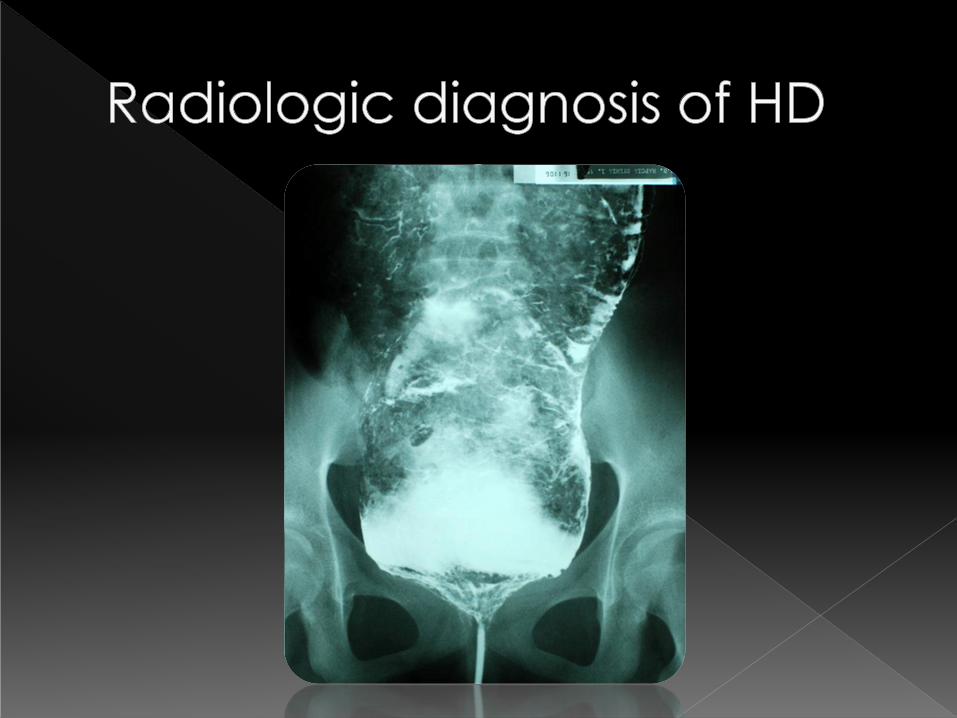
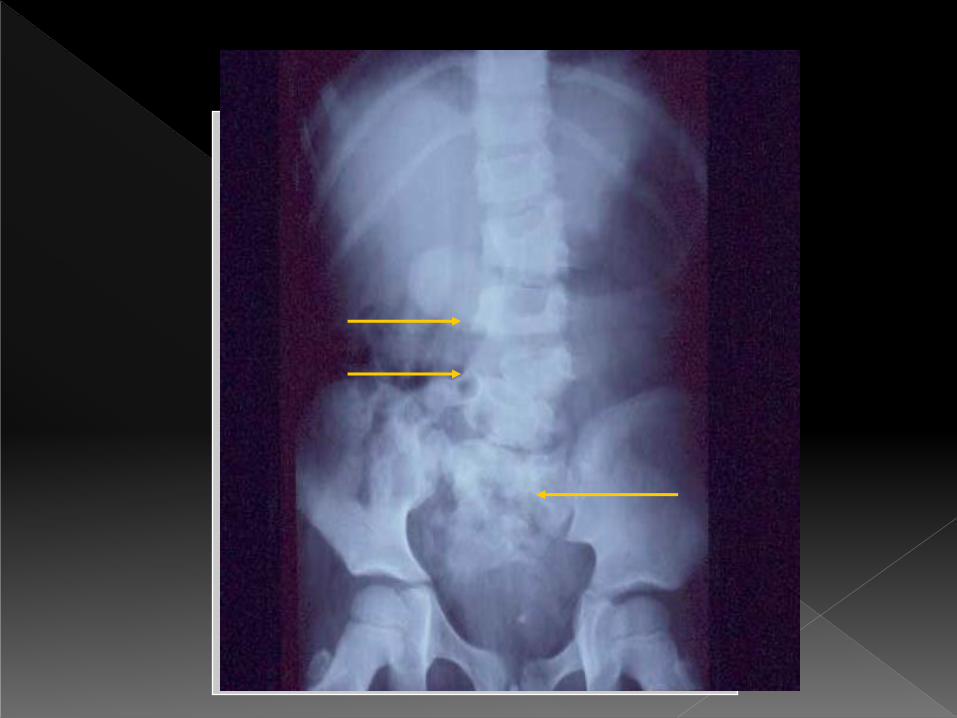
Dilated bowel loops with fluid levels
Airless pelvis
In patients with enterocolitis:
thickening of the bowel wall with
mucosal irregularity or grossly dilated
colon loop
Pneumoperitoneum (spontaneous
perforation)





Infant should not have rectal washouts or
digital examinations prior to barium
enema
Baby in the lateral position
Demonstration of transitional zone- flow of
barium from undilated rectum through a
cone-shaped zone into dilated proximal
colon
Retained barium and transitional zone at
24 hours delayed film


…of Total Colonic Aganglionosis

Suction- or full-thickness rectal biopsy
H&E staining
Histochemic examination for ACHE
Immunohistochemistry (NSE, S-
100,CD56)
Conservative
Surgical One-stage
Two- or Three-stage
Colostomy
Place of stoma formation
Surgical technique of definitive treatment



Swenson
Duhamel
Soave

Swenson Duhamel
Soave Rehbein

Anastomosis is performed after
intraoperative histopathologic
examination – confirmation of
colon level with normal
ganglion cells in ganglia.


Enterocolitis – commonest cause of
death !
Resolving with adequate therapy or !!!
!!! Toxic megacolon- sudden onset of
marked abdominal distension, bile
stained vomiting, fever, signs of
dehydratation, sepsis and shock

- Anastomotic leak
- Retraction of the pullthrough
- Perianal excoriation
- Enterocolitis
- Constipation
- Soiling

Inflammatory Bowel Disease
(IBD)

Ulcerative Colitis
• UC is an IBD of unknown etiology
• Confined to rectum and colon
• males and females equally affected
• highest incidence >10/100 000 in Nordic
countries, British Isles and North America
• 5% of cases have onset before the age of
of 10 years, and 20% before the age of 20
years
• the incidence has remained unchanged
after 1980`s

UC
• Etiology – multifactorial: environmental, infections,
psychosiocial, immunological and genetic factors (…some
inherited defects in the immunoregulation may lead to
clinical manifestation of the disease in certain
environmental conditions including infective agents).
• Pathology – chronic inflammatory disease of the rectum
and colon affecting mucosa and submucosa of the bowel
wall. Rectum affected in more than 95% and the
inflammation extends contiguously to the more proximal
large bowel.
• Specificity in pediatric cases: pancolitis more often than in
adult patients, backwash ileitis (suggests Crohn`s disease)

UC
• Characteristic histological appearance:
diffuse superficial unspecific inflammation,
neutrophilic epithelial invasion, crypt
abscesses, crypt deformity, mucosal
ulceration, epithelial regeneration with
pseudopolyp formation, atrophic and
dysplastic mucosa
• Risk of colon cancer in pediatric patients: 1-
3% - 10 years after onset of the disease,
• risk is increased by 1-1,5% after every year

UC
• Clinical Fatures: bloody mucous diarrhoea, abdominal pain, tenesmus,
fever, weight loss, poor apetite, growth retardation, malnutrition,
delayed sexual maturation, iron deficiency anemia secondary to
chronic intestinal bleeding, increased blood sedimentation rate and
fecal calprotectin concentration.
• Extraintestinal manifestations: joints (arthralgias, arthritis), skin
(erythrema nodosum, pyoderma gangrenosum), skeleton (decreased
bone density), eyes (uveitis) and hepatobiliary system (primary
sclerosing cholangitis, autoimmune hepatitis)
• Endoscopic diagnosis – findings and histological examination of the
biopsy specimen
• Differential diagnosis: Crohn`s disease, up to 5-15% of children with
UC diagnosis is changed to Crohn`s disease.
• 10-15% of children with IBD – initially: indeterminate colitis.

UC
• Medical management: intensive nutritional support,
corticosteroids – control of initial disease,
sulfasalazine and 5-aminosalicylic acid – maintaining
of remission, in selected cases: immunomodulatory
drugs (azathioprine, methotrexate, cyclosporine,
tacrolimus, infliximab)
• Surgical management (not the first-line treatment):
40-70% of children with UC
• Indications for operative treatment: chronic
persisting symptoms despite optimal medical therapy
and corticosteroid dependency, risk for colonic
dysplasia and carcinoma.

UC
• Emergency operation: toxicmegacolon, fulminant colitis
and persistent colonic bleeding.
• Procedure: restorative proctocolectomy with ileoanal
anastomosis (mucosectomy 5mm above dentate line, J-
pouch, with/without ileostomy)
• Postoperative function: 10-12 stools per 24 h, within 6
months: 2-7 per 24 h.
• Protective pads for nigh-time soiling.
• 20-50%- pouchitis (metronidazole and cyprofloxacin),
5-15%- wound infection (anastomotic leakage, fistula
formation), 15-45%- repeat operation

Crohn`s disease
• CD – chronic inflammation of the bowel with
unknown etiology
• In children is reported to be more common then
UC
• Males ad females equally affected
• 20-25% of patients with CD have the onset of
the disease before 15 yrs of age
• occurs more often in white population
• there are some hereditary risk factors for CD
• Etiology: genetic, immunological,
microbiological and environmental factors

Crohn`s disease
• Pathology: CD involves terminal ileum and colon in 60%
of cases, small bowel only in 30% and colon only in
10% of cases.
• Involved bowel and mesentery are thickened, fat
migrates into antimesenteric border, stricturising in the
segmet of bowel.
• Histologically: mucosa extensively ulcerated and the
inflammation is transmural. Inflammation often
interspersed with almost normally appearing mucosal
areas.
• Transmural inflammatory changes may develop to
fistulas: to bowel, bladder, vagina, perineum and
abdominal wall.

Simple classification of CD`s
location and behaviour = Vienna
classification:
Age at diagnosis A1, <40 years
A2, >40 years
Location L1, Terminal ileum
L2, Colon
L3, Ileocolon
L4, Upper gastrointestinal
Behaviour B1, Non-stricturing, non-
penetrating
B2, Stricturing
B3, Penetrating

Crohn`s disease
onset most often after the age of 10 years
typical early symptom: non-specific abdominal
pain
other symptoms: diarrhea, weight loss and fever,
growth failure, delayed onset of puberty
perianal disease (first presentation in 20% of CD): chronic anal fissures and skin tags and chronic
fitula in ano,
extraintestinal manifestations (may present years before the onset of CD): arthritis, erythrema
nodosum, pyoderma gangrenosum, iritis and
uveitis

Crohn`s disease
– medical management
more complex and more aggressive than in
UC
corticosteroids, aminosalicylates, antibiotics:
metronidazole and ciprofloxacin for colonic
disease
Elemental or semi-elemental enteral nutrition
Immunosupression: azathioprine, 6-
merkaptopurine, cyclosporine
TNF-alpha antibodies for fistulizing or refractory
CD

Crohn`s disease
– surgical management
There is no definitive curative treatment
for Crohn`s disease !
Indications for surgery-
Acute: toxic megacolon, acute bleeding,
GI perforation
Subacute or chronic conditions: refractory
strictures, internal or external fistula and
intra-abdominal abscesses

Crohn`s disease
– surgical management
MAIN PRINCIPLE: TO SAVE BOWEL
LENGHT !
Surgical procedures:
strictureplasty, colectomy and
ileorectal anastomosis, perianal
fistula resection, temporary or
permament stoma.

Anorectal Anomalies

• The term „anorectal anomalies” encompasses a series
of congenital defects that represent a wide spectrum.
• In the past: „high” and „low”, subsequently „high”,
„intermediate” and „low”.
• Actually: practical classification with therapeutic and
prognostic implication.
Anorectal Anomalies

• MALES:
1. Rectobladder neck fistula
2. Rectourethral prostatic fistula
3. Rectourethral bulbar fistula
4. Imperforate anus with no fistula
5. Perineal fistula
6. Complex defects
• FEMALES
1. Cloaca with a common channel longer than 3 cm
2. Cloaca with a common channel shorter than 3 cm
3. Rectovestibular fistula
4. Imperforate anus with no fistula
5. Perineal fistula
6. Complex malformations
ARM - Classification

Males
1 2

Females
1 2 3

Questions:
• Does the baby have a serious
associated defect ?
• Does the baby need a colostomy or
should we perform a primary repair of
the malformation?
Anorectal Anomalies –
- Neonatal Approach

Frequency of associated defects
in cases of anorectal anomalies :
urologic defects (50%)
spinal and sacral defects (30%)
tethered cord and other cord
abnormalites (25%)
cardiovascular malformations (30%, but
only 10% have important hemodynamic
repercussions)
esophageal atresia (5-10%)


• Descending colostomy with separated stomas
• distal stoma = mucous fistula
• High pressure distal colostogram before
definitive repair
Anorectal Anomalies - colostomy


Voluntary bowel movements in:
• 15% with rectobladder neck fistula
• 60% with recto-prostatic fistula
• 70% with cloaca (depending on the quality of the sacrum)
• 85% with recto-bulbar fistula
• 95% with vestibular fistula
• 100% for perineal fistula
• Occasional soiling
• Constipation
• Incapacity to empty bladder after cloaca repair (80%/20%)
• in case of fecal incontinence – bowel management
program is implemented
Anorectal Anomalies - Results

The end…