![COMPUTATIONAL COMPARISON OF FLUID-DYNAMICS IN …€¦ · the Carotid Artery Stenosis Consensus conference [20] for grading carotid stenoses. In particular, stenosis estimate (% diameter](https://static.fdocuments.us/doc/165x107/5f070b947e708231d41b06ac/computational-comparison-of-fluid-dynamics-in-the-carotid-artery-stenosis-consensus.jpg)
Guidelines in the management of carotid stenosis
65
Guidelines in the Management of Carotid Stenosis Professor Alun H Davies Academic Section of Vascular Surgery, Imperial College, Charing Cross & St Mary’s Hospital, London
-
Upload
uvcd -
Category
Presentations & Public Speaking
-
view
245 -
download
1
Transcript of Guidelines in the management of carotid stenosis

Guidelines in the Management of Carotid Stenosis
Professor Alun H DaviesAcademic Section of Vascular Surgery,
Imperial College,Charing Cross & St Mary’s Hospital,
London
Stroke
• Each year 120,000 people suffer 1st stroke• Within 1 year 33% dead• 3rd most common cause of death (UK)
Symptoms due to:- Critical Stenosis- Occlusion- Unstable plaque

Aetiology of Stroke
• Ischaemic (80%)- 75% Carotid territory
- 50% thrombo-embolism of ICA or MCA- 25% small vessel disease- 15% cardiac embolus,- 10% other: Takayasu’s arteritis, FMD
- 15% Vertebrobasillar features- 10% unknown
• Haemorrhagic (20%) Under-perform by 2-3 fold CEA/CAS
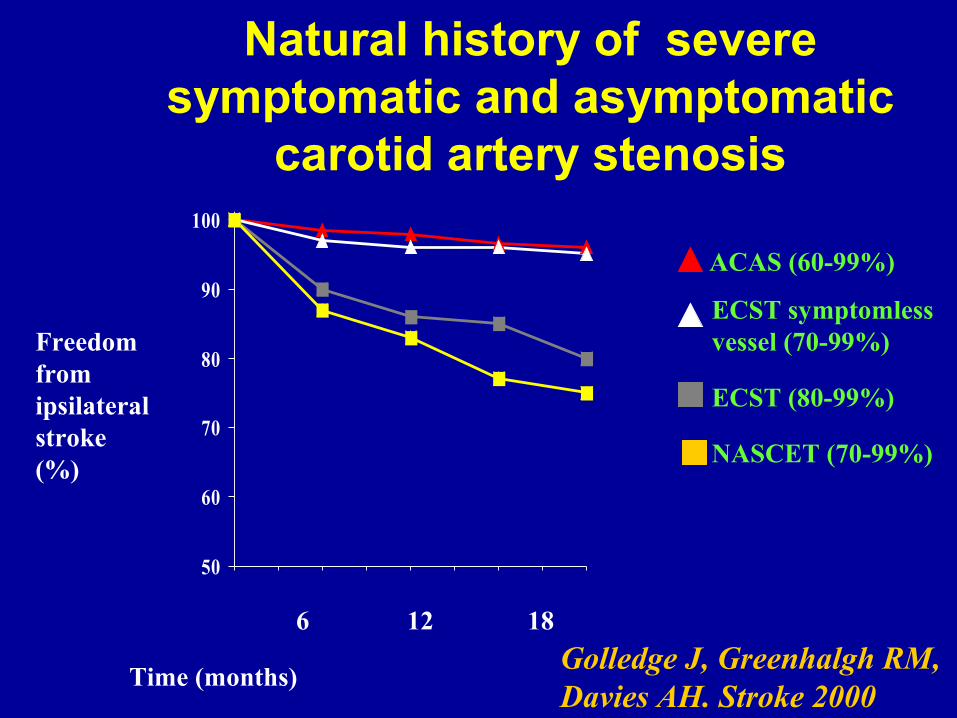
Natural history of severe symptomatic and asymptomatic
carotid artery stenosis
50
60
70
80
90
100
Golledge J, Greenhalgh RM, Davies AH. Stroke 2000
6 12 18
Time (months)
Freedom from ipsilateral stroke (%)
ACAS (60-99%)
ECST symptomless vessel (70-99%)
ECST (80-99%)
NASCET (70-99%)

Life-table analysis of stroke related to presentation
0102030405060708090
100
0 6 12 18 24 30 36
AmaurosisTIATransient strokeEstablished strokeProgressive strokeCrescendo TIA
Avoidance of stroke (%)
Time (months)
Golledge J, Cuming R, Beattie DK,
Davies AH, Greenhalgh RM JVS 1996

Life-table analysis of survival related to presenting symptom
0102030405060708090
100
0 6 12 18 24 30 36
AmaurosisTIATransient strokeEstablished strokeProgressive strokeCrescendo TIA
Survival (%)
Time (months)
Golledge J, Cuming R, Beattie DK, Davies AH, Greenhalgh RM
JVS 1996
Stroke Risk: NASCET and ECST
• 13.1% major ipsilateral stroke at 2 years
• 13%/yr for ANY ipsilateral stroke
• ECST - 16.2% for ANY ipsilateral stroke at 3 years
• Most strokes occur within first year of signal event
• Risk is directly proportional to degree of stenosis
Stroke, 1999
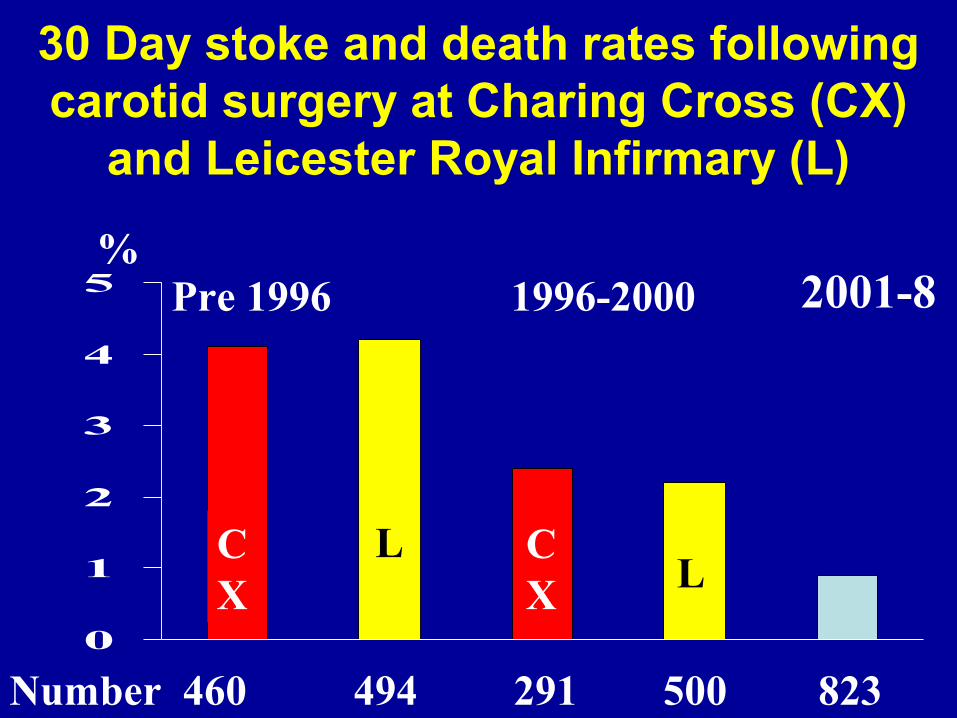
30 Day stoke and death rates following carotid surgery at Charing Cross (CX)
and Leicester Royal Infirmary (L)
0
1
2
3
4
5 Pre 1996 1996-2000
CX
CX
LL
Number 460 494 291 500 823
% 2001-8

Risk of Stroke
Naylor 2007

Number of stokes saved at 5 yearsPer 1000 CEAs in 50-99% stenosis
Naylor 2007

Benefit of Urgent Treatment
Naylor 2007

Natural history - stroke rate in asymptomatic carotid artery
stenosis
Patients with <75% stenosis - annual stroke rate 1.3%
Patients with >75% stenosis - annual stroke rate 3.3%
Chambers BR, Norris JW Stroke 1991

Asymptomatic Disease• Stroke risk with asymptomatic stenosis
(NASCET)> 60% is 9.9% at 5 yrs < 60% risk stroke 5.4% at 5 yrs
• ACST : DEGREE OF STENOSIS 60%-80% = 9.5% risk stroke at 5 yrs 80%-99% = 9.6% risk stroke at 5 yrs
• NO INCREASE IN STROKE WITH INCREASE IN STENOSIS
• THEREFORE There is NO high risk subgroup of asymptomatic patients based on degree of stenosis

Asymptomatic stenosis
0
1
2
3
4
5
6
7
8
9
VA ACAS ACE ACST
Trial
% risk of stroke
% medical risk
% surgical risk 2004
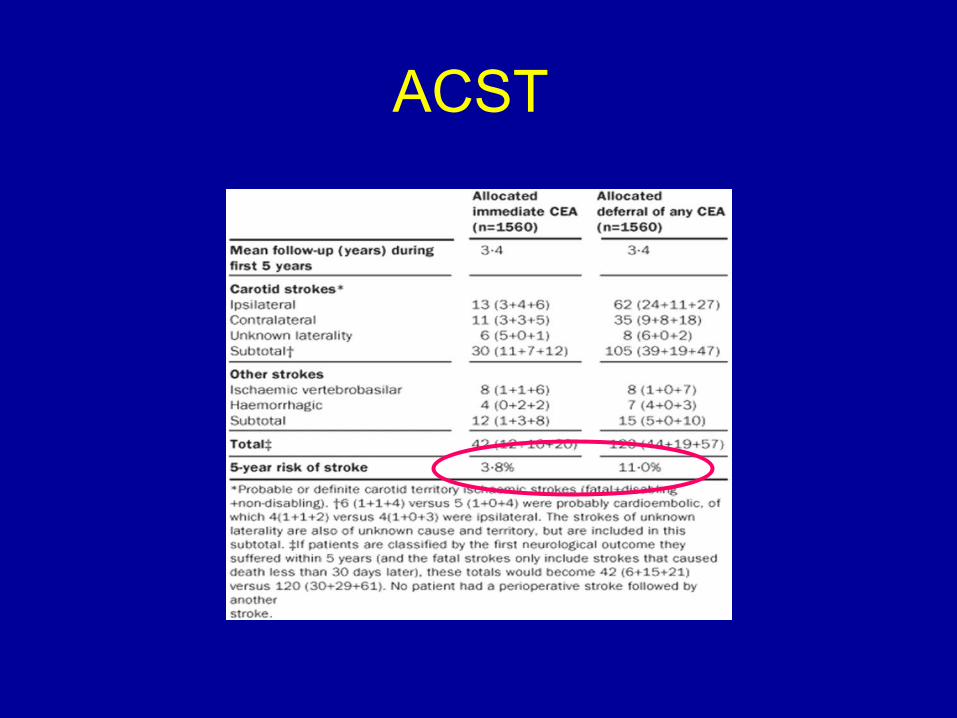
ACST

Carotid angioplasty

Single center studies 1990-1999
Studies Number of arteries
PTA 13 714
Endarterectomy 20 6970
Stent used in 44% of patients with cerebral
protection in 11%
Technical failure in 37 Cases (7%)
Golledge J, Mitchell A, Greenhalgh RM, Davies AH Stroke 2000
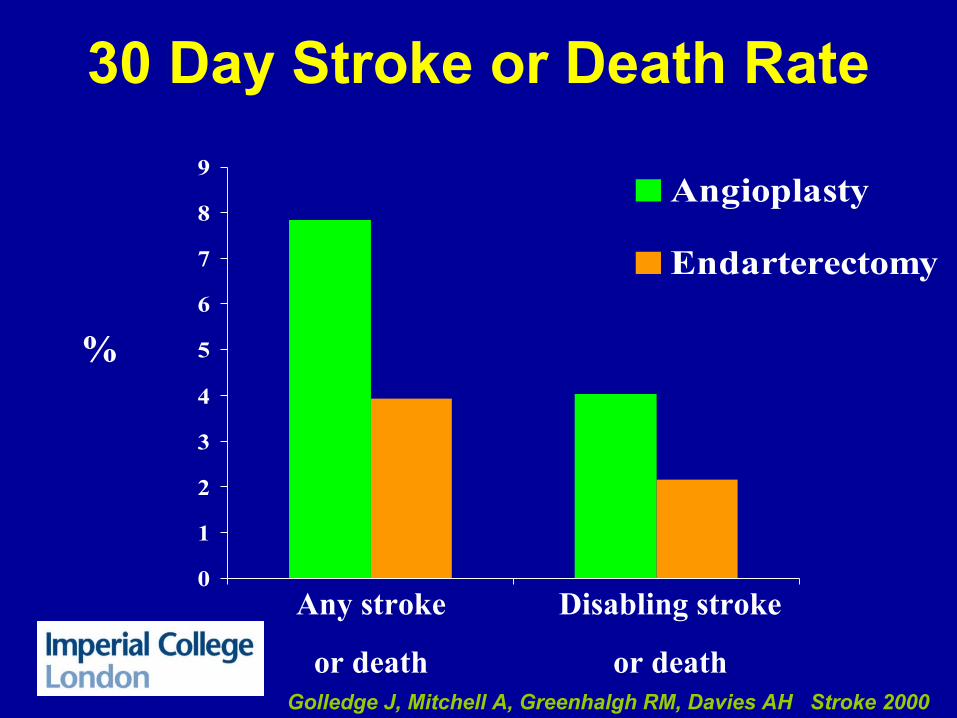
30 Day Stroke or Death Rate
0
1
2
3
4
5
6
7
8
9Angioplasty
Endarterectomy
Any stroke
or death
Disabling stroke
or death
%
Golledge J, Mitchell A, Greenhalgh RM, Davies AH Stroke 2000

Odds ratio for outcome
Any stroke
Disabling or fatal stroke
TIA
Death
Any stroke or death
Disabling stroke or death
1 2 3 4 5 6 70
Relative odds
2.22
2.09
4.02
0.68
Surgery Angioplasty
Golledge J, Mitchell A, Greenhalgh RM, Davies AH Stroke 2000
CAVATAS
CAVATAS trial compared carotid
endarterectomy with carotid angioplasty.
The rate of any stroke lasting more than
7 days, or death were 9.9% and
10% respectively. CAVATAS investigators Lancet June 2001

Sapphire
Archer
Crest
Caress
“High Risk”
The Rest

EVAS -3
• RCT• N=527
Stoke/Death Rates• 30 day CEA 1.5 % vs CAS 3.4% RR 2.2• 6/12 CEA 6.1% vs CAS 11.7% p<0.02• 4 yrs CEA 6.2% vs CAS 11.1% RR 1.97
p<0.03
Mas et al, 2006 ,2008
SPACE Trial
• n=1200
• CAS n=605 or CEA n=595
• 30 days CAS 6.84% vs CEA 6.34% SPACE failed to prove non-inferiority of CAS compared
to CEA. Results do not justify the widespread use in the short term of CAS for treatment of carotid- artery
stenosis. Reingleb et al 2006 The incidence of recurrent carotid stenosis at 2 years,
as defined by ultrasound, is significantly higher after carotid artery stenting. Older patients do worse with CAS.
Eckstein et al 2008
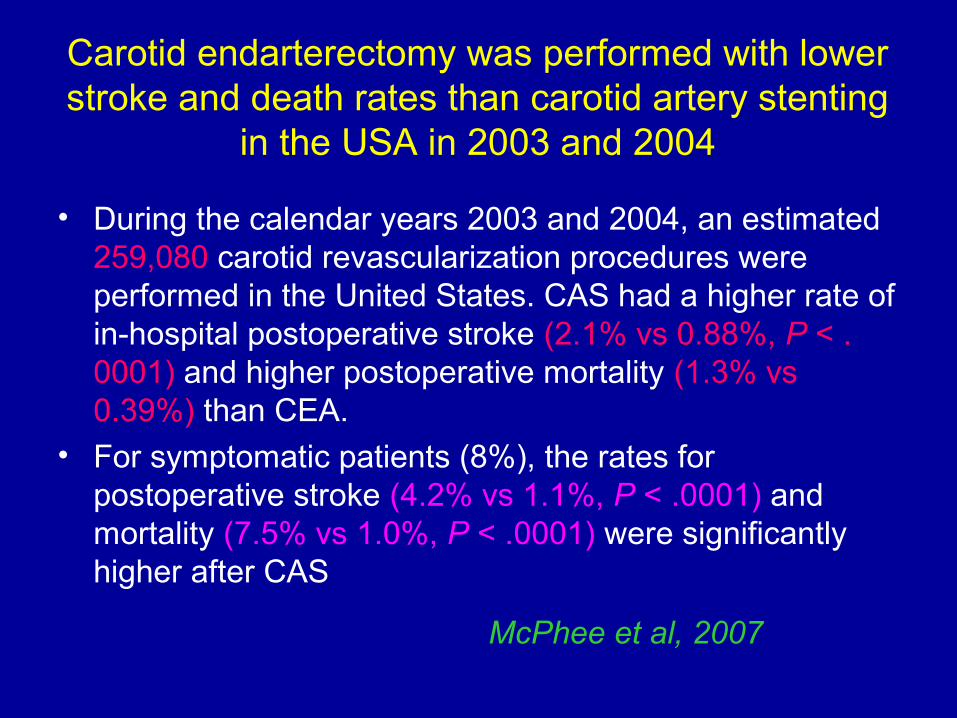
Carotid endarterectomy was performed with lower stroke and death rates than carotid artery stenting
in the USA in 2003 and 2004
• During the calendar years 2003 and 2004, an estimated 259,080 carotid revascularization procedures were performed in the United States. CAS had a higher rate of in-hospital postoperative stroke (2.1% vs 0.88%, P < .0001) and higher postoperative mortality (1.3% vs 0.39%) than CEA.
• For symptomatic patients (8%), the rates for postoperative stroke (4.2% vs 1.1%, P < .0001) and mortality (7.5% vs 1.0%, P < .0001) were significantly higher after CAS
McPhee et al, 2007

Clinical results of carotid artery stenting
compared with carotid endarterectomy
• Ten trials encompassing 3580 patients were analyzed. Patients who underwent CAS had a higher risk of 30-day stroke/death relative to patients who underwent CEA (risk ratio [RR], 1.30; 95% CI, 1.01-1.67).
• Subgroup analysis of trials enrolling only symptomatic patients showed higher risk of 30-day stroke/death (RR, 1.63; 95% CI, 1.18-2.25), but trials enrolling both symptomatic and asymptomatic patients showed no significant differences (RR, 0.89; 95% CI, 0.59-1.35).
Brahmandam et al 2008

Risk-adjusted 30-day outcomes of carotid stenting and endarterectomy: results from the
SVS Vascular Registry.
• When CAS and CEA were compared in the treatment of atherosclerotic disease only, the difference in outcomes between the two procedures was more pronounced, with death/stroke/MI
6.42% after CAS vs 2.62% following CEA, P < .0001.
• Following best possible risk adjustment of these unmatched groups, symptomatic and asymptomatic CAS patients had significantly higher 30-day postprocedure incidence of death/stroke/MI when compared with CEA patients.
Sidway et al 2009

Further on Going Trials
• Various RCTs on CEA vs PTA + Stent
CAVATAS IIACST IITACITSPACE II
Equipoise!
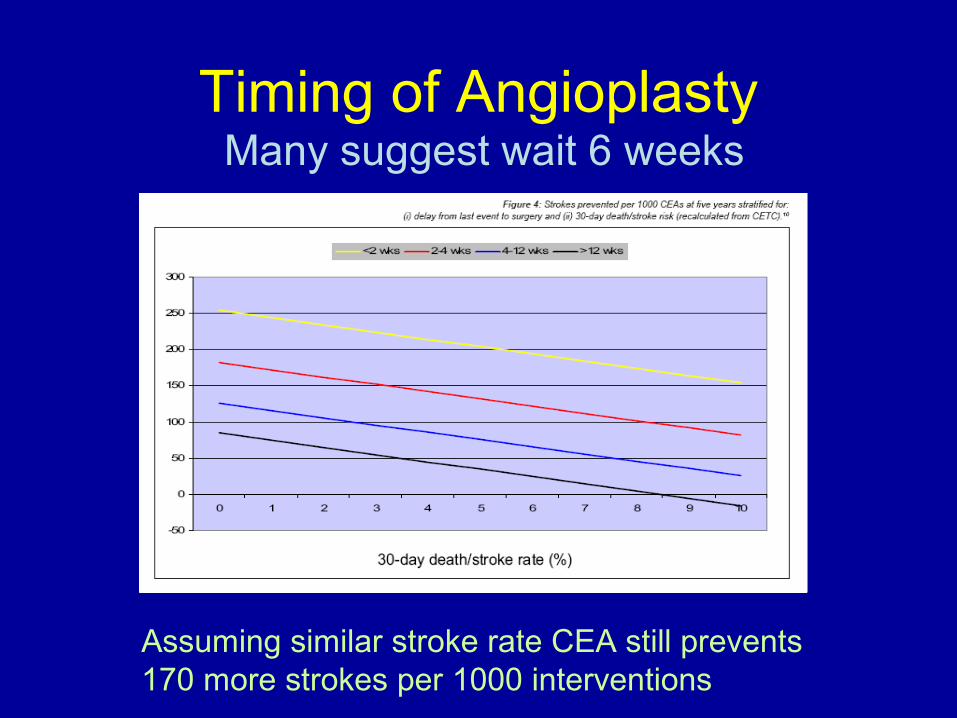
Timing of Angioplasty Many suggest wait 6 weeks
Assuming similar stroke rate CEA still prevents 170 more strokes per 1000 interventions

Better out than in !
Candidates for PTA

30 Day Stroke Rate
0
1
2
3
4
5
6
7
8
Angioplasty
Endarterectomy
Any stroke Disabling/
fatal stroke
TIA Death
%
Golledge J, Mitchell A, Greenhalgh RM,
Davies AH Stroke 2000
2009
CREST Study Design
• RCT of CAS vs CEA• 1:1 randomisation, stratified by centre and
symptomatic status• Lead-in credentialing for CAS
– N=20 CAS– 427 applicants, 224 (52%) approved to randomise
• Primary end-point – composite:– Any stroke, MI (including biochemical) or death within
30 days– Ipsilateral stroke to 4 years
• Target recruitment 2,500• Industry sponsored

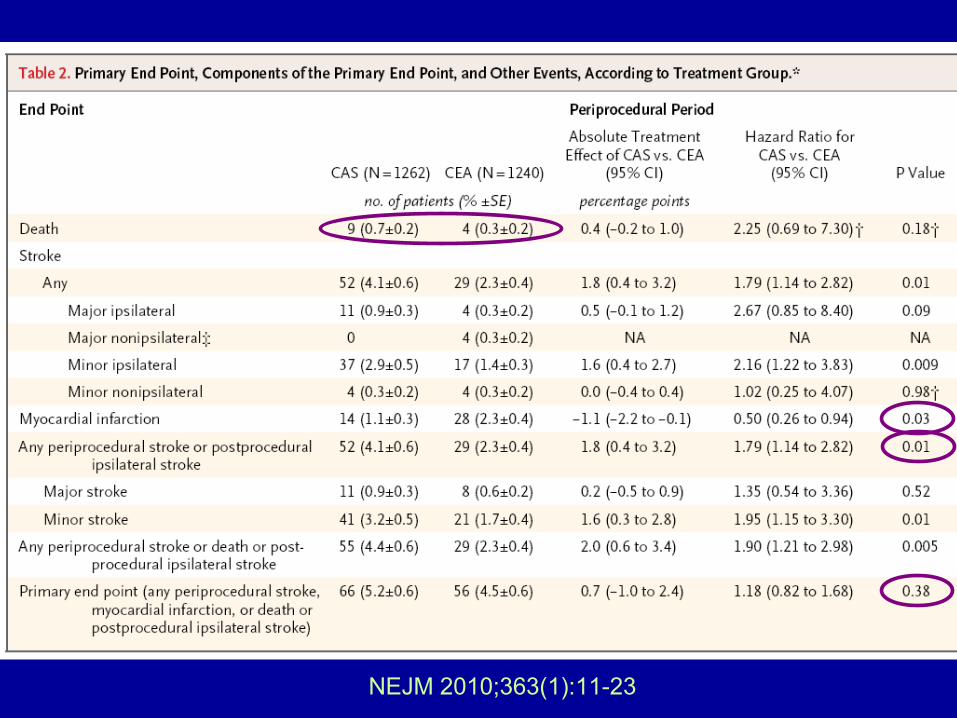
NEJM 2010;363(1):11-23
p=0.51
NEJM 2010;363(1):11-23
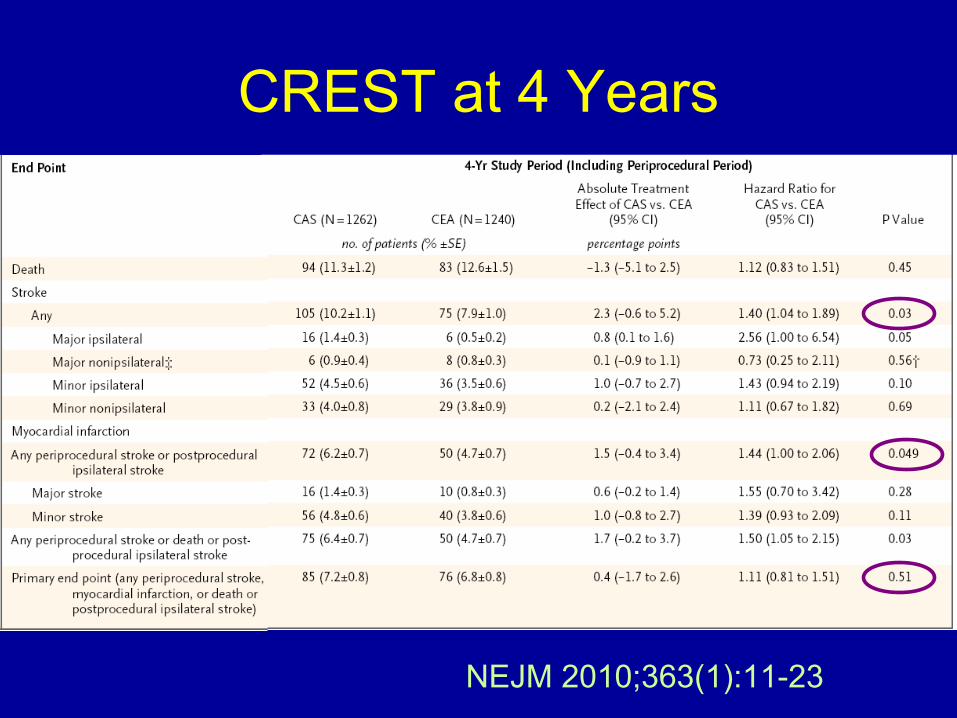
NEJM 2010;363(1):11-23
CREST at 4 Years

CREST• symptomatic (n=1,321) or asymptomatic (n=1,181)
• At 30 days, the rate of stroke was significantly higher with stenting, at 4.1% vs. 2.3% with surgery.
• Myocardial infarction was higher with carotid endarterectomy, at 2.3% vs. 1.1% with stenting.
• when death and stroke are considered alone, there are almost twice as many events with carotid stenting/angioplasty as there are with carotid endarterectomy.
“I do not believe the results of CREST should alter the conclusion that endarterectomy remains the treatment of choice for symptomatic patients”
Moore 2010, PI CREST
CREST Limitations
• Composite endpoint• Biochemical MI• Underpowered to show difference in death and major
ipsilateral stroke• Heterogeneity of symptomatic and asymptomatic patients• Not all patients on statins • More lipid lowering in CEA• More anti-platelets in CAS• Advances in BMT, CEA stent and embolic protection
since CREST commenced in 2000• Can CREST CAS results be reproduced in wider
practice?• Left to interpretation based on personal bias?

Identify at risk asymptomatic patients
• NNT
• Degree of stenosis
• Plaque type
Is asymptomatic carotid endarterectomy a good use of
resources?

Are stroke rates changing over time?
SMART
ASED
Johnson
ACAS
VA
CHS
ACBS

To estimate the lifetime cost-effectiveness of early endarterectomy in the UK based on the Asymptomatic
Carotid Surgery Trial
ACST, Lancet 2010

Markov transition state model
HenrikksonBJS 2005
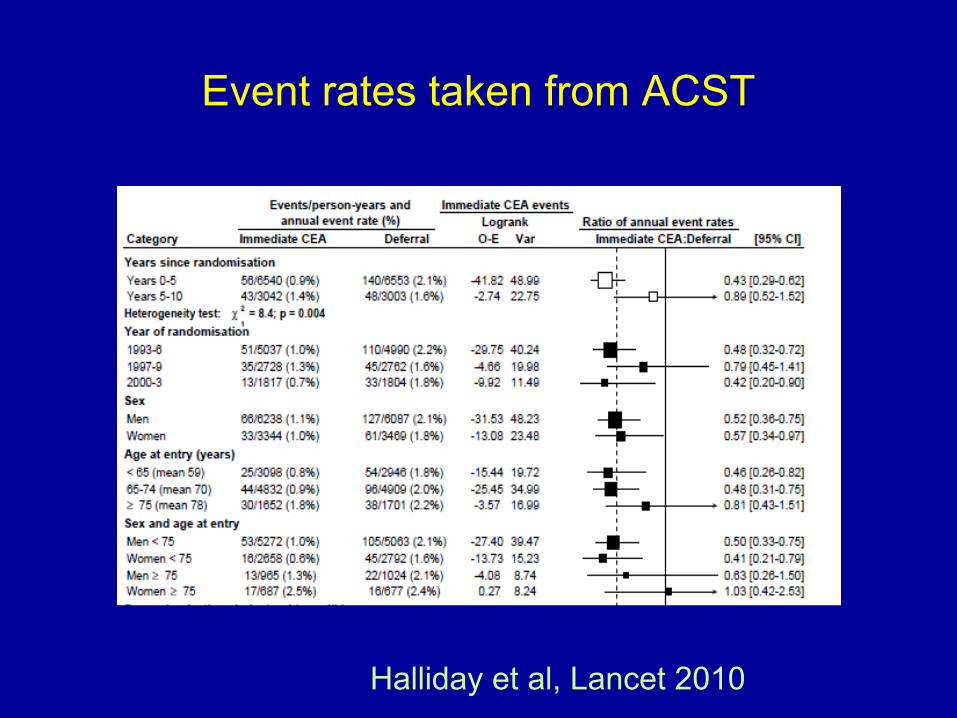
Event rates taken from ACST
Halliday et al, Lancet 2010
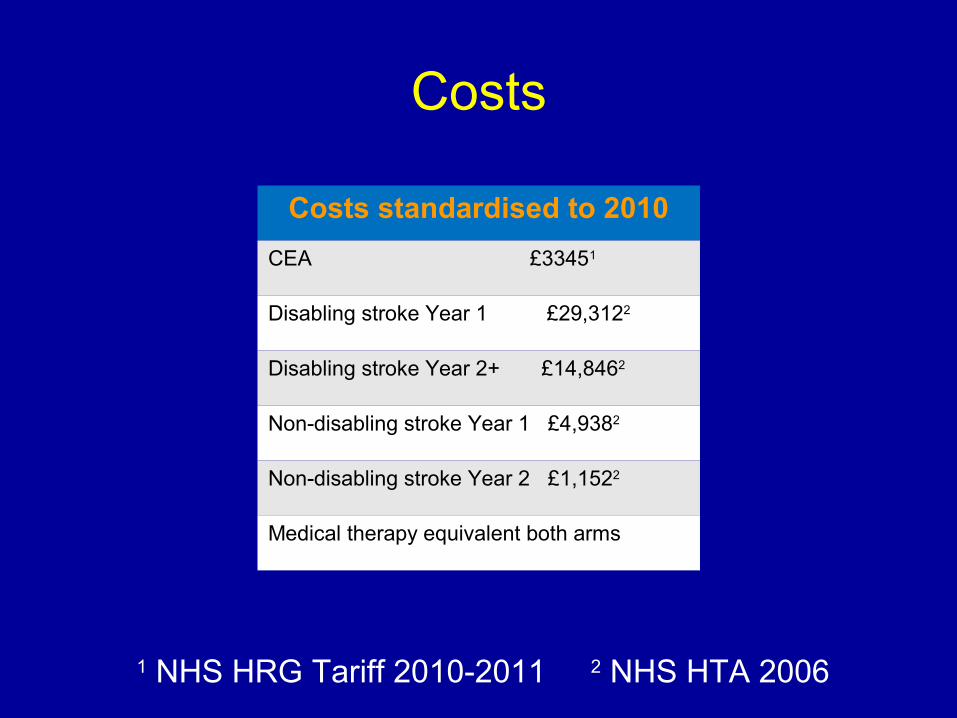
Costs standardised to 2010
CEA £33451
Disabling stroke Year 1 £29,3122
Disabling stroke Year 2+ £14,8462
Non-disabling stroke Year 1 £4,9382
Non-disabling stroke Year 2 £1,1522
Medical therapy equivalent both arms
Costs
1 NHS HRG Tariff 2010-2011 2 NHS HTA 2006

?
?
Assessing cost-effectiveness
Additional cost (£)
Additional effect (QALYs)
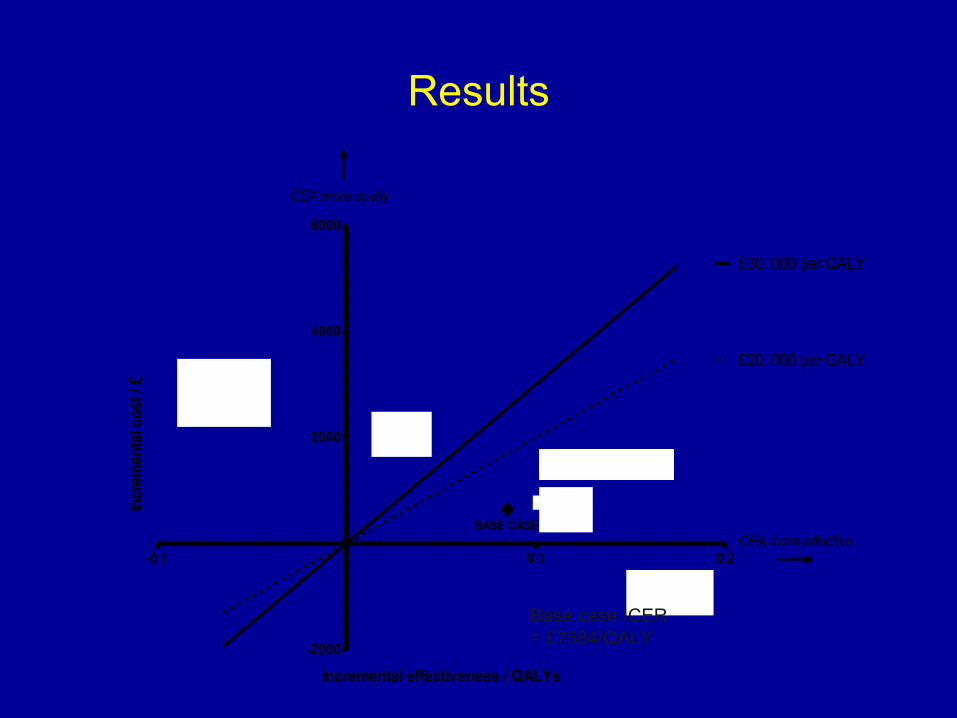
Results
-0.1 0.1 0.2
-2000
2000
4000
6000
£20, 000 per QALY
£30, 000 per QALY
Women > 75y
Men > 75y
Men < 75y
Women < 75y
BASE CASE
CEA more costly
CEA more effective
Restriction of crossovers
Incremental effectiveness / QALYs
Incr
emen
tal c
ost /
£
Base case ICER = £7584/QALY

Reduced stroke rates

Limitations
• Previous US trials with higher stroke rates, shorter follow up and fewer patients excluded
• TIA not included as endpoint• Loss of productivity from stroke not included in costs• Informal care not included in costs• Stenting not considered following interim guidance from
NICE

Interpretation
• Endarterectomy was likely to be cost-effective in under 75s• Especially so in young women• Late crossovers to endarterectomy did not improve cost-
effectiveness• With lower background stroke rates, endarterectomy may soon
become borderline cost-effective, even if it becomes safer
• Maintaining cost-effectiveness relies on:• Identification of patients with high risk carotid plaque• Maintaining low rates of operative stroke• Prevention of cardiac death for men in their 70s

X
XX
?

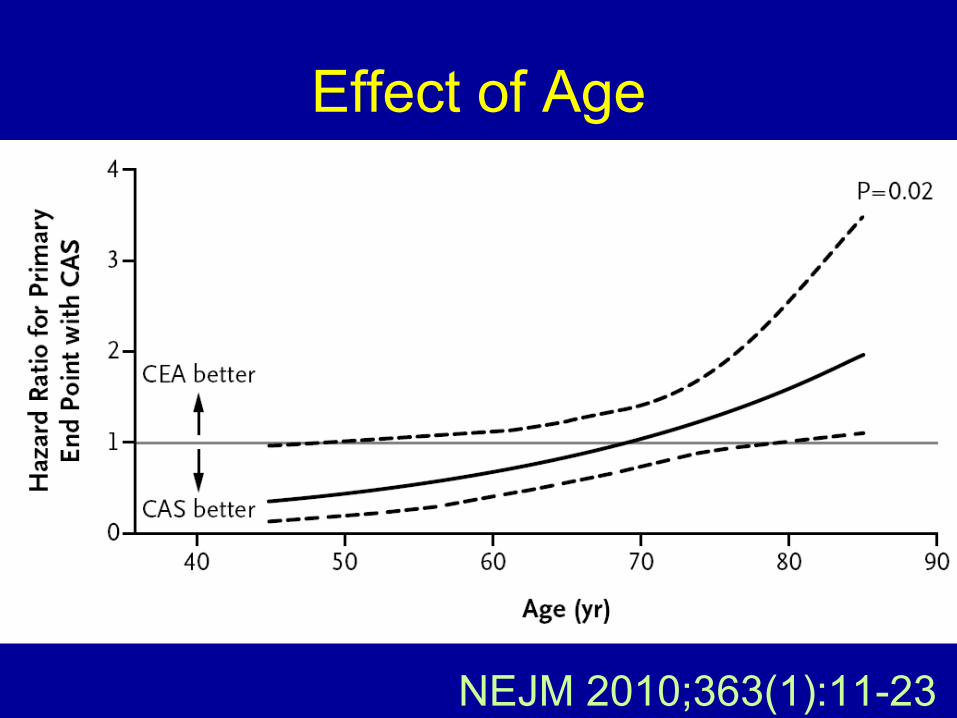
NEJM 2010;363(1):11-23
Effect of Age

NEJM 2010;363(1):11-23

Lancet Neurol 2011;10:530-537
Effect of Gender

Impact at 1 Year
JACC 2011;58:1557-1565
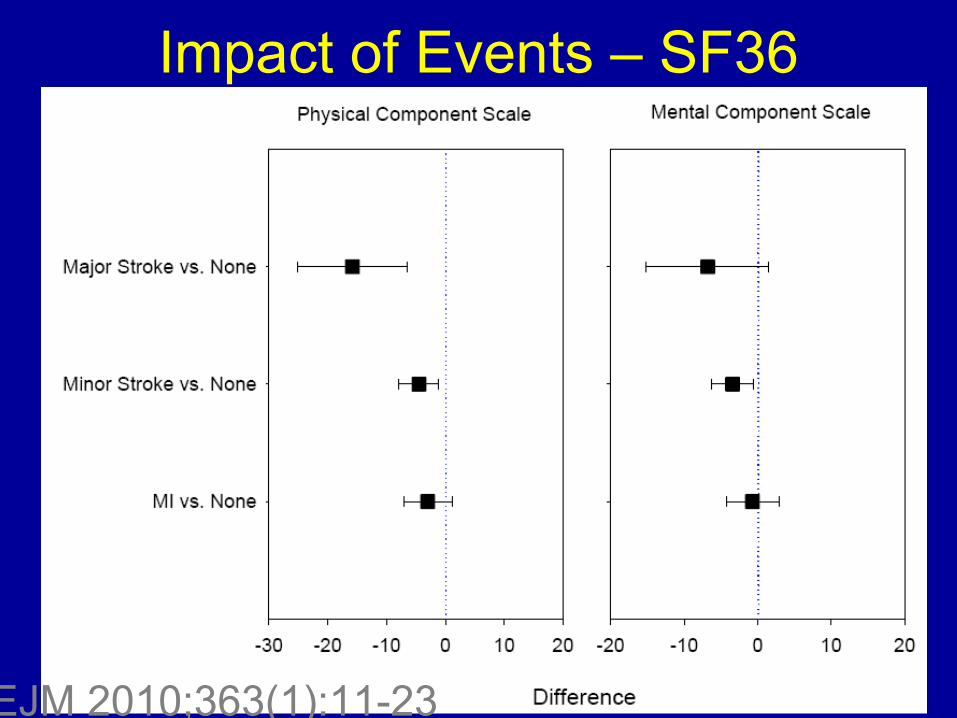
Impact of Events – SF36
NEJM 2010;363(1):11-23

Time from Symptoms to Surgery
Naylor 2007

ACST
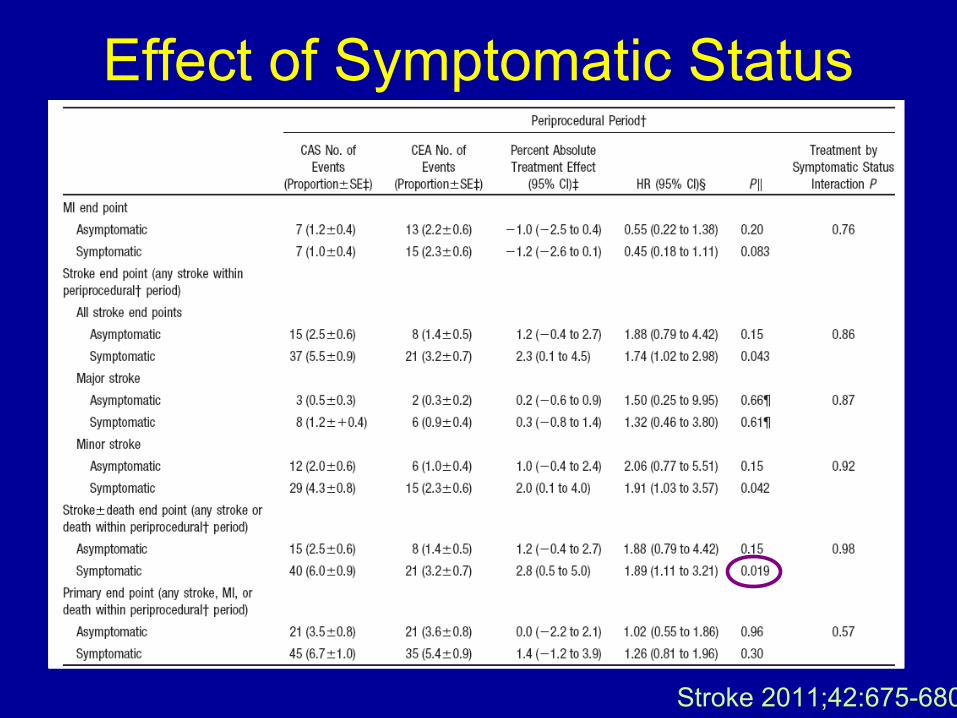
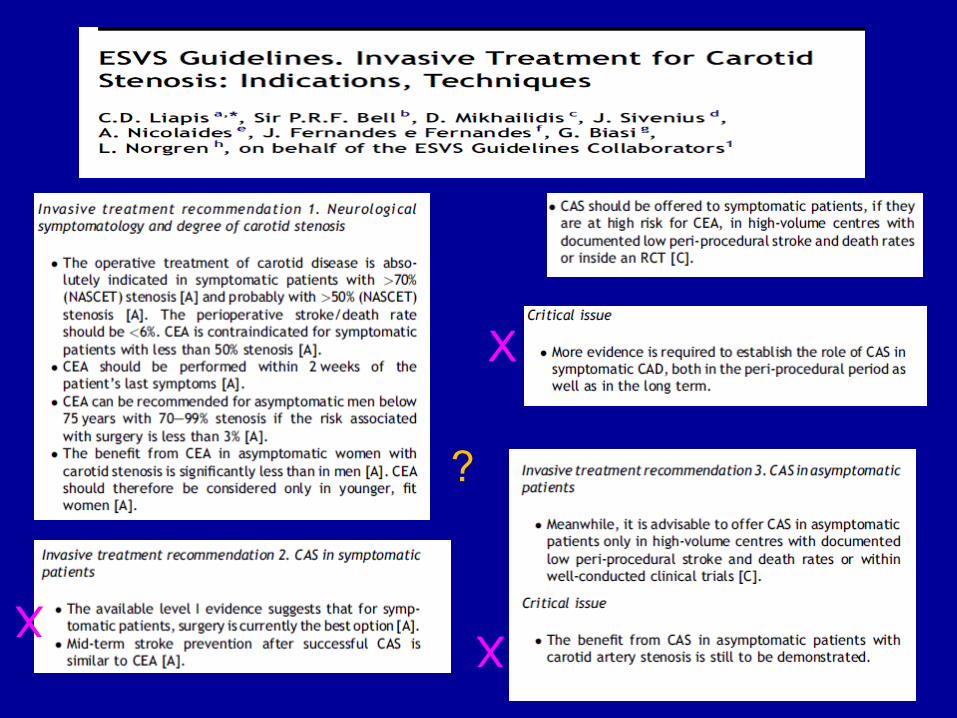
Effect of Symptomatic Status
Stroke 2011;42:675-680


















