
Guideline for Acute Malnutrition · MSF - Holland Muslim Aid Oxfam Novib Relief International Save...
132
Guideline for Management of Acute Malnutrition 1 Somali Guidelines for Management of Acute Malnutrition 2010 UNICEF/BANNON/2005
Transcript of Guideline for Acute Malnutrition · MSF - Holland Muslim Aid Oxfam Novib Relief International Save...

Guideline for Management of Acute Malnutrition
1
Somali Guidelines for Management of Acute Malnutrition
2010UNICEF/BANNON/2005

2
Important Warning
These Guidelines are based on international standards. However, some changes have been introduced to adapt them to Somali specific working conditions and environment.
These adaptations are identified in the text, along with the international recommendations: Whenever possible, the international recommendations should be followed.The adaptations should NOT be implemented in any other circumstances.
Whenever one of these adaptations needs to be applied, agencies should consider investing their efforts in changing the working conditions, through lobbying and mobilisation of resources in an effort to eliminate the extreme situation.

Guideline for Management of Acute Malnutrition
3
Foreword
In Somalia, acute malnutrition has become a chronic problem. In many areas, prevalence consistently exceeds emergency thresholds. While levels of acute malnutrition fluctuate over seasons and among livelihood zones, a meta-analysis of surveys taken over the past ten years shows a national median rate of 16.7% global acute malnutrition and 4.4% for severe acute malnutrition in the overall population, with slightly higher levels in IDPs. The underlying causes of acute malnutrition include a lack of access to health care services, poor hygiene and sanitation facilities, high incidence of morbidity, sub-optimal childcare practices, poor or irregular access to nutritious food stuffs including milk. These underlying causes are perpetuated by poverty, low education levels, a lack of infrastructure and public services, livelihood systems eroded by destructive climatic events, as well as ongoing conflict and displacement. The management of acute malnutrition is a vital link in reducing mortality and promoting optimal nutrition and development for Somali children.
There is considerable regional variation in the burden of acute malnutrition. Children in the south and central zone, the area most at risk of conflict, displacement, and a lack of access to basic services typically experiences a chronic nutrition crisis. Apart from IDPs, the populations of Somaliland and Puntland generally experience lower incidence of acute malnutrition but a high vulnerability to nutritional shocks characterized by episodic peaks in acute malnutrition. Despite these challenges, many partners strive to provide access to quality programs for the management of acute malnutrition. Nutrition partners are diverse including communities, local authorities, government ministries, local NGOs, international NGOs, and UN agencies. Over the past few years, the geographical coverage of malnutrition management programs has grown considerably. In 2009, nutrition partners reached over 190,548 children, which is over 60% of the estimated case load of acutely malnourished children. This is a significant achievement in a context where partners encounter problems of access in much of the country. In 2010 and beyond, nutrition actors wish to work together to improve the quality, access, and utilization rates of services they provide. One part of this includes implementation of standardized guidelines for the management of acute malnutrition which are based on international standards and which take into account the unique context of supporting nutrition programs in Somalia. The IMAM package (guidelines, field cards, and training aides) was produced in a collaborative way, supported by the Nutrition Cluster, and with input from a wide variety of partners. Use of the IMAM package will help to streamline management protocols and improve the quality of the services provided. In addition, they will facilitate a more harmonized capacity building program for IMAM and assist in improving monitoring.

4
Acknowledgements
The IMAM package was facilitated by the IASC Nutrition Cluster through a consultative process. We are grateful for ECHO funds which made the development of the package possible. The following organizations participated in meetings to review the guidelines.
Action contre la faim AFRECANPPCANCEC NutriCISPConcern WorldwideCOSVDIALERDFSNAUGTZHEALIMCMedairMerlinMinistry of Health – PuntlandMinistry of Health – SomalilandMSF - HollandMuslim AidOxfam NovibRelief InternationalSave the Children UKSCDFSOLNARDOSRCSTrocaireUNICEFWFPWHOWorld Vision International

Guideline for Management of Acute Malnutrition
5
Contents
Somali Guidelines for Management of Acute Malnutrition Foreword 3 Acknowledgements 4List of Field Cards 7Using these guidelines - 1 8Using these guidelines - 2 9Introduction 10 The challenge of managing acute malnutrition in Somalia 11Section 1 – Malnutrition: an overview 13 Components of Nutrition 14 Causes of Malnutrition 15 Types of Malnutrition: definitions 16 Acute malnutrition: types and classification 17Section 2 – Programme Overview 19 Components of Management of Acute Malnutrition programmes: 20 Usual programme set-ups in Somalia 21 Key elements for programme quality 22Section 3 – Diagnosis of Acute Malnutrition and Admission criteria 23 Diagnosis of acute malnutrition 24Section 4 – Supplementary Feeding: Management of MAM 43 Overview 44 Admission criteria to targeted SFP 45 Nutrition support: Diet and frequency. 46 Routine Medication 47Section 5 – Outpatient Therapeutic Programme (OTP): Management of Uncomplicated SAM 51 Overview 52 Admission Criteria 53 Nutrition Support: Diet and Frequency 54 Routine Medication 56 Complicated SAM in the OTP 64Section 6 – Inpatient care – Management of complicated SAM in Children 6 to 59 months 65 Overview 66 Admission Criteria for Inpatient Care 68 Discharge criteria 68 Criteria of return to Phase 1 69 Nutritional Treatment 70 Phase 1 (Stabilisation) 70 Transition Phase 70 Phase 2 71Section 7 – Management of Acute Malnutrition in Infants 77 Overview 78 Infants that cannot be admitted to SC 78 Discharge Criteria for children less than six months (or less than 3 kg) 79 Infants Less Than Six Months with a Prospect of Being Breastfed 79 Routine Medication 79 Care for the Mother 82 Infants Without a Prospect of Being Breastfed 83 Routine Medication 83 Follow-Up after discharge 83Section 8 – Treatment of medical complications 85 Hypoglycaemia 86 Hypothermia 87

6
Dehydration 88 Septic (or Toxic) Shock for All Malnourished Patients 94 Absent Bowel Sounds, Abdominal Distension 95 Heart Failure 96 Severe Anaemia 97 Administration of Medication 98Section 9 – Community involvement in Management of Acute Malnutrition 99 Overview 100 Phases of Community involvement 100Section 10 – Nutrition information, education and communication 105 Nutritional topics and key messages 108Section 11 – Management of centres and routine work 113 Management of the centre (SFP and OTP) 114 Flow of patients (SFP, OTP): 115 Organisation of work in the SFP / OTP 119Section 12 – Patient’s cards and reporting system 121

Guideline for Management of Acute Malnutrition
7
List of Field Cards
FC 1 – Taking measurementsFC 2 – Determining weight-for-height (W/H)FC 3 – The appetite testFC 4 – Clinical presentation of SAMFC 5 – SAM history and examinationFC 6 – Pathophysiology of SAMFC 7 – Admission criteria for children 6 to 59 monthsFC 8 – Complicated and non-complicated malnutritionFC 9 – Admission criteria for other age groupsFC 10 – How to prepare CSB at homeFC 11 – Routine medication in SFPFC 12 – Surveillance/follow-up of patients in SFPFC 13 – Discharge criteria from SFPFC 14 – Failure to respond to treatment in SFPFC 15 – Amounts of RUTF to distributeFC 16 – Taking RUTF at home – messages for the carerFC 17 – Routine medication for OTP and SC admissionsFC 18 – Specific medicationsFC 19 – Surveillance/follow-up of patients in OTPFC 20 – Discharge criteria from OTPFC 21 – Failure to respond to OTP treatment. Definition.FC 22 – Failure to respond. Causes and actionsFC 23 – Transfer to SC. Criteria and procedure.FC 24 – SC – Promotion between phasesFC 25 – Quantities of milk and RUTF in SCFC 26 – Preparation of F75 and F100FC 27 – Feeding techniqueFC 28 – Routine medicines in SC (to be used with FC17 & FC 29)FC 29 – Systematic antibiotics in SC FC 30 – Patient follow-up in SCFC 31 – Infants – criteria for admission and dischargeFC 32 – F100 diluted – preparation and distributionFC 33 – Supplementary suckling techniqueFC 34 – Infants less than 6 months without prospect of being breastfedFC 35 – Treatment of dehydration for the marasmic patientFC 36 – Active screening for acute malnutrition FC 37 – Home visit check-listFC 38 – Routine work at OTP – check-listFC 39 – Discharge procedures

8
Using these guidelines - 1
Components of the package:
The Package of the Somali Guidelines for Management of Acute Malnutrition is formed of three components:
• these Guidelines• the Field Cards (FC)• the Training materials.
The guidelines present the main body of the recommendations for the management of acute malnutrition, with explanations and following a logical order. In the relevant sections of the guideline, a “field card” (FC) is inserted with the explanation of a particular procedure, treatment or protocol. These “field cards” will be detached and presented as a stand-alone document, the field guide.
Several field guides are prepared, selecting different “field cards”, so that the relevant material is available for each level of care. In this way, the field guide for OTPs does not need to include the field cards for Stabilisation Centres and vice-versa. Some field cards are relevant for all levels of care.
The field cards are intended as a reference to be used in daily activities in the field. For this reason, they are printed in resistant materials, so that they can be checked while consulting the patient. They can take the form of figures, to remind the practitioner of the correct way of taking anthropometry measurements; tables for checking the correct dosage of a food product or drug; summaries of the messages that need to be transmitted to the carers; check lists of steps to follow when consulting each patient; and many others.
The training materials are constructed around the field cards. They are meant to be used in consultation with the field cards – the objective is to learn how to use them and encourage their use, rather than to rely solely on memorization.

Guideline for Management of Acute Malnutrition
9
Using these guidelines - 2
Distribution of chapters:
After the Introduction on the specificities of managing malnutrition in Somalia, these guidelines present an overview of malnutrition (Chap. 1) and of the different programmes (Chap. 2). These three sections are intended for all readers, including non-technical readers that want to have a general understanding of programmes to manage acute malnutrition. Chapter 3 presents the anthropometric and medical procedures to diagnose malnutrition, as well as a presentation of malnutrition from the medical point of view. It also presents the criteria for admission to all components of the programme, so that those making the diagnose have the criteria for admission summarized in a single place and can decide to which service the patient should be referred. Some basic procedures to follow during the admission process are presented as well. This first part of the guideline is addressed to all staff working on the management of acute malnutrition, with specific parts focusing on those in charge of taking anthropometric measurements, those organizing the diagnosis or those making clinical consultations.
Subsequent chapters present the management of Moderate Acute Malnutrition (MAM) in Supplementary Feeding Programmes (SFP) (Chap. 4), uncomplicated Severe Acute Malnutrition (SAM) in Oupatient Therapeutic Programmes (OTP) (Chap. 5) and complicated Acute Malnutrition in Stabilization Centers (SC) (Chap. 6). Each of these chapters follows the same logic:
• overview• recall of admission and discharge criteria• dietary treatment• routine medicines• surveillance / follow up of the patient
Each of these chapters is completed with additional materials, as required for each service. Each of these chapters is intended for staff working in those facilities, as well as for their supervisors.
The following two chapters present the special case of children under 6 months of age (Chap. 7) and the diagnosis and treatment of acute complications in SC (Chap. 8). These are addressed mainly to senior nurses and doctors working in SC, but their reading would be useful for those working in OTP that do not have access to transfer to SC.
Chapter 9 addresses how to organise community mobilisation, and gives some practical suggestions. This is completed by advice on how to organise nutrition information, education and communication (Chap. 10), with a summary of the main health and nutrition messages. This can be used, not only during community mobilisation, but as well in education and counseling sessions at the SFP, OTP or SC. Finally, chapter 11 gives some advice on how to organise the routine work at the centres, and chapter 12 presents the standard cards for the patients and reporting materials.

10
Introduction
Acute malnutrition is a deadly disease. It arrives as the consequence of insufficient or inappropriate feeding and as a consequence of disease. Without appropriate treatment, acute malnutrition may result in the death of the child. Even the children that survive may remain vulnerable to other episodes of malnutrition and disease and present lower intellectual and psycho-motor abilities, which will in turn reduce their chances later in life.
In the second half of 2009, 1 in 6 children were estimated to have acute malnutrition in Somalia, 25 % of which were severe1. This critical situation, particularly in areas of the centre and south, is related to a high disease burden, lack of access to health services and to safe water and sanitation, as well as suboptimal infant and young child feeding (IYCF) practices. This chronic crisis is addressed through a variety of programmes, including food distributions, water and sanitation, blanket feeding, livelihood programmes and the direct management of acute malnutrition. To further address this problem, a scale-up of preventative nutrition programmes, such as IYCF, also needs to be considered.
At the time of writing these guidelines there were numerous SFP sites for treating moderate acute malnutrition and about 250 outpatient units (OTPs) for the treatment of uncomplicated severe acute malnutrition in Somalia. Most of them have been opened or re-opened in the last 2 years – a great achievement. There were as well, around 20 inpatient stabilisation centres, all but four integrated into health structures. Despite this remarkable effort to increase the number of facilities, only a part of the needs for treatment of acute malnutrition in Somalia are covered. Great distances, spread of the population, lack of access to existing facilities and the lack of a stable and solid health network cause many areas to remain uncovered. This situation also means that outpatient facilities are often disconnected from stabilisation centres, limiting transfer opportunities for patients with complicated malnutrition.
The spread of activities and diversity of actors in Somalia has given place to a number of differences in the way malnutrition is managed in centres, as well as to important differences in programme quality. These current guidelines, initially promoted by UNICEF and the Somali Nutrition Cluster, have been written in consultation with all organisations, departments and agencies implementing programmes to manage acute malnutrition in Somalia. This was done with the intention of capitalizing on best-practices and experiences, so that lessons learnt by one can be applied by all partners. They intend as well to facilitate the process of training new staff and to help with the opening of new centres, so that we approach the objective of ensuring the right to treatment of every child with malnutrition, through ever increasing rates of coverage.
Managing malnutrition in certain parts of Somalia is difficult. The number of obstacles for quality management and good coverage are endless, and the situation is often volatile, preventing standard and sometimes consistent service implementation. These guidelines try to take these constraints into account, whenever possible, and with the hope that the current exceptional adaptations will become irrelevant and a new set of standard guidelines written.
1 FSNAU Post Dyer 2009/10 Nutrition Technical Series Report. February 22, 2010.

Guideline for Management of Acute Malnutrition
11
The challenge of managing acute malnutrition in Somalia
Some of the specific challenges that Management of Acute Malnutrition faces in Somalia are:
• Conflict,• High insecurity,• High mobility of population (including health staff),• Spread of the population, with long distances and isolation,• Difficult transport and communications,• Population displacement (and the inability for IDPs to access services in some host areas),• Regular migration among pastoralists,• Difficult social environment related to complex clan structure,• Specific conflicts between clans,• Rigid traditional family structures that relies heavily in women’s work,• Lack of health infrastructure,• Lack of training infrastructure, and therefore chronic lack of qualified health staff,• And, in some areas, the need to pay fees to access the health system (and, as a consequence a lack of access for services)
These problems result in, amongst others:
• Lack of enough centres to have good geographical coverage of programmes,• Low coverage even in areas that are theoretically served by a centre,• Lack of referral of complicated cases to stabilisation centres for life-saving treatment,• Frequent and unpredictable breakdowns in the supply chain,• Discontinuity of programmes in some areas, with regular closure and re-opening of programmes,• Irregular and often inconsistent community mobilisation,• Overall fragmentation of aid and of other interventions to prevent malnutrition,• Low qualification of staff and difficulties to hire new health staff when needed,• High turn-over of staff,• Difficulty of supervision, on-site monitoring or on-the-job training,• Costs for families attending health and nutrition services regularly,• Fear of mothers to attend due to insecurity and volatility of the situation,
These guidelines take into consideration the specific challenges of implementing the management of acute malnutrition in Somalia and the adaptations that programmes have made as a consequence. The usual set-up of services seen in Somalia is presented in Chapter 2.
In order to increase coverage, promote early diagnosis and reduce the need for transfers, these guidelines promote the use of intense community mobilisation as the first priority in all programmes. When possible, protocols are adapted for the eventuality of a complicated case that cannot be transferred to a SC.

12

Guideline for Management of Acute Malnutrition
Section 1Malnutrition
an overview
13

14
Components of Nutrition
People eat foods that contain the nutrients necessary for life. Nutrients may be divided into categories:
Macronutrients
Protein, fat and carbohydrates are macronutrients that make up the bulk of a diet and supply the body’s energy.
In resource-poor populations, carbohydrates (i.e. starches and sugars) are often a large part of the diet (80%) and the main source of energy. Fats are also important in cell formation. Proteins are required to build new tissue and are derived mostly from animal origin such as milk, meat and eggs, and from cereals and pulses. Animal by-products contain essential amino acids that cannot be produced by the body but must be eaten to promote growth and good health.
Micronutrients
There are around forty different micronutrients that are essential for good health. From a functional point of view, micronutrients can be divided into two classes: Type I and Type II.
Type I micronutrients, or functional nutrients, include nutrients that are required for the hormonal, immunological, biochemical and other processes of the body. They include iodine, iron, vitamins A and C among others. Deficiencies in Type I micronutrients do not affect growth directly (i.e. the individual can have normal growth with appropriate weight and still be deficient in micronutrients) and thus a deficiency in Type I micronutrients cannot be identified by anthropometric measurements. Deficiencies in Type I micronutrients will cause major illness such as anaemia, scurvy and impaired immunity.
Type II micronutrients, or growth nutrients, include magnesium, sulphur, nitrogen, essential amino-acids, phosphorus, zinc, potassium, sodium and chloride. They are essential for growth and tissue repair. Type II micronutrients are required only in small quantities by every cell and system, but the correct balance is essential for good health. A deficiency in any of the Type II micronutrients will lead to growth failure, measured by stunting and/or wasting. Replenishment of all these nutrients, in the correct balance, is essential for recovery from malnutrition and convalescence from acute illness.
Water
Most of the body is water. Water is necessary for good nutrition as well as for maintaining hydration. Only half of the body’s water is obtained through drinks, the rest being absorbed from foods and produced by the body. Water often needs to accompany foods in order to provide good dilution and absorption of nutrients.
Causes of Malnutrition
Malnutrition, whether acute or chronic, has multiple causes that usually work in conjunction, reinforcing each other to the point that no single action or intervention can prevent it. Only exceptionally, a single cause can be found. Managing acute malnutrition implies having an understanding of the causes of malnutrition and how they interact. The immediate causes are usually easier to observe, but they cannot be addressed unless their underlying causes are understood and addressed. Sustainable eradication of malnutrition can only be based in the elimination of its basic causes.
The division of the causes of malnutrition into different levels facilitates understanding and analysis of a given context, and can be used for planning of programmes.
Immediate Causes of Malnutrition
Inadequate dietary intake and disease are immediate causes of malnutrition and create a vicious cycle in which

Guideline for Management of Acute Malnutrition
15
disease and malnutrition exacerbate each other. Thus, food intake and disease must both be addressed to support recovery from malnutrition.
Underlying Causes of Malnutrition
Three major underlying causes of malnutrition include:
• Food: Inadequate household food security (limited access or availability of food).• Care: Inadequate social and care environment in the household and local community, especially with regard to women and children.• Health: Limited access to adequate health services and/or inadequate environmental health conditions (including access to safe water and sanitation facilities).
All underlying causes of malnutrition are usually the consequence of poverty.
Basic Causes of Malnutrition
The basic causes of malnutrition in a community originate at the regional and national level, where strategies and policies that affect the allocation of resources (human, economic, political and cultural) influence what happens at community level. Geographical isolation and lack of access to markets or services due to poor infrastructure, displacement or conflict can have a huge negative impact on food security and health.
CAUSES OF MALNUTRITION: UNICEF CONCEPTUAL FRAMEWORK.
Short-term consequences:Mortality, morbidity, disability
Inadequate dietary intake
Household foodinsecurity Inadequate care
Unhealthy household environment and lack of
health services
Income poverty:employment, self-
employment, dwelling, assets, remittances,
pensions, transfers etc
Disease
Maternal and child undernutrition
Long-term consequences:Adult size, intellectual ability,
economic productivity, reproductive performance,
metabolic and cardiovascular disease
Social, economic and political context
Basic causes
Immediate causes
Underlying causes
Lack of capital: financial, human, physical, social and
natural

16
Types of Malnutrition: definitions
Malnutrition refers to all deviations from adequate nutrition, including undernutrition and overnutrition, resulting from inadequacy of food relative to need and/or disease. Malnutrition also encompasses specific deficiencies (or excesses) of essential nutrients such as vitamins and minerals. In the context of these guidelines, the term malnutrition always makes reference to undernutrition, and more particularly to the syndrome called Acute Malnutrition.
Undernutrition is caused primarily by an inadequate intake of dietary or food energy, whether or not that is deficiency of any specific nutritient present. It encompasses stunting, wasting, nutritional oedema and deficiencies of essential vitamins and minerals (micronutrient deficiencies). Different forms of undernutrition may co-exist within the same individual.
Stunting / Chronic malnutrition: Stunting is a retardation of linear growth and is indicated by a low height-for-age. It can occur when a child suffers from chronic (long-term) nutrient deficiencies, and/or if the child suffers from repeated episodes of disease or acute malnutrition.
Acute Malnutrition occurs when a person suffers from a severe nutritional restriction. It can present in the form of wasting or kwashiorkor. Acute malnutrition is measured as either moderate (MAM) or severe (SAM)2.
Wasting as a clinical sign means visible loss of subcutaneous fat and skeletal muscles (severe thinness). It is also known as Marasmus. Anthropometric wasting refers strictly to low weight-for-height, which is usually observed in cases of clinical wasting.
Kwashiorkor is a form of severe acute malnutrition characterized by the accumulation of liquid (swelling or oedema) in the legs and sometimes arms and face. It may be accompanied by wasting, in which cases it is called Marasmaic Kwashiorkor.
Underweight refers to a child who has a low weight-for-age. This concept does not distinguish between wasting and stunting as it does not indicate if the deficit is in weight (with normal height) or in height itself. Weight-for-age is used in health programmes for growth monitoring.
2 The term “protein-energy malnutrition” is no longer used as it is not thought anymore that protein or energy deficiency are causes of acute malnutrition.
MALNUTRITION
OVER-NUTRITION
ObesityWasting, Stunting, Underweight, MDD
micronutrient deficiencies
UNDER-NUTRITION

Guideline for Management of Acute Malnutrition
17
Acute malnutrition: types and classification
The term acute malnutrition makes reference to two different medical entities with different clinical and pathological characteristics: Marasmus (or wasting) and Kwashiorkor. Each of them is the consequence of different metabolic disturbances. Despite these differences, the standard protocols to treat them are similar, with small – but important – differences.
Acute malnutrition is also categorised into Moderate acute malnutrition (MAM) and Severe acute malnutrition (SAM), depending on the patient’s degree of wasting and/or the presence of kwashiorkor. Severe acute malnutrition is often the result of Moderate acute malnutrition that has not been treated. All cases of kwashiorkor are categorized as SAM. Moderate acute malnutrition and severe acute malnutrition are treated in different programmes, reflecting their different level of severity and their different nutritional and medical needs. These programmes are most often based in the community.
The metabolism of individuals with complicated severe acute malnutrition is seriously disturbed, and the immune system seriously impaired. The patient develops severe complications (i.e. hypoglycaemia, hypothermia, electrolyte imbalance, micronutrient deficiencies and severe infections) that are difficult to diagnose for the untrained doctor (i.e. often the only sign present may be anorexia). In order to survive and recover, these patients need more advanced treatment in specific hospital units called Stabilisation Centres (SC).

18

Guideline for Management of Acute Malnutrition
Section 2Programme
an overview
19

20
Components of Management of Acute Malnutrition programmes:
The objectives of programmes for the Management of Acute Malnutrition are:• to save the lives of individuals that have developed severe acute malnutrition• to prevent the development of severe acute malnutrition.
Well run programmes can obtain this through the combination of their different components, particularly when they are well coordinated and integrated.
Community mobilisation:
Objective: To sensitize the population to the problem of malnutrition and how to identify it, in order to reach more children and at an earlier stage in their development of acute malnutrition, therefore increasing programme coverage and recovery.
Intervention: Screening of children through assessment of MUAC and nutritional oedema; mobilisation of key leaders and associations; education and sensitization; promotion of acceptance of the programme by the community; follow up of patients in programmes that default or present a problem.
Targeted Supplementary Feeding Programme - SFP:
Objective: To treat patients with Moderate Acute Malnutrition (MAM) and prevent the development of Severe Acute Malnutrition (SAM).
Intervention: Weekly, biweekly, or monthly distributions of take home rations in the form of Fortified Blended Flours (e.g. CSB or UNIMIX) or Ready to Use Supplementary Foods (RUSFs) (e.g. Supplementary Plumpy) and routine medicines; nutritional monitoring of the patient; programmes implemented as stand alone by fixed or mobile teams, or from Health Centres.
Outpatient Therapeutic Programme (Outpatient care) - OTP:
Objective: To treat patients with SAM who have a good appetite and no medical complications. Intervention: Weekly or biweekly distributions of Ready to Use Therapeutic Foods (RUTFs) and routine
medicines; medical and nutritional monitoring of the patient; programmes implemented as stand alone by fix or mobile teams, or in Health Centres. After recovery and discharge he/she can be admitted in SFP to prevent relapse through supplementary food.
Stabilisation Centre (Inpatient care) - SC:
Objective: To treat patients with SAM who have poor appetite or medical complications. Intervention: Daily therapeutic milk and medical treatment in inpatient care centre (Hospital or stand alone
centre, run as daycare or as a 24h care centre). A child with complicated SAM will start treatment at SC (inpatient), when the child improves he/she can continue treatment as an outpatient at the OTP. After recovery and discharge he/she can be admitted in SFP to prevent relapse through supplementary food.
A referral system must be in place to transfer patients from one component to the next (when the patient condition worsens), or to return to the previous one if the evolution of treatment is satisfactory.Refer to respective chapters for more information on each of the programme components presented here.

Guideline for Management of Acute Malnutrition
21
Usual programme set-ups in Somalia:
Ideally, all programmes for the management of acute malnutrition should implement the four components, presented in the previous page, in an integrated way. This is not always possible in places like Somalia. Currently, these are the usual programme set-ups that are implemented in Somalia:
OTP and SC services available
Usually one SC -attached to a Hospital or on its own- that can receive children with SAM and complications from several OTPs. Patients starting treatment in the SC can complete it at the OTP as soon as they recover from complications (usually after one week). Only those patients that live in an area that is not covered by an OTP will complete the treatment at the SC (usually lasting one month). Patients presenting SAM without complications can follow treatment at the OTP from the start.
This is the ideal set up that all programmes should follow. In Somalia, it is usually seen only in towns.
Only OTP services available (with no SC)
A network of several OTPs with little or no possibility of referring the complicated cases to SC. The patient receives all the treatment at the OTP, from diagnosis to discharge, regardless of whether or not there are medical complications.
The lack of SC services may be due to distance to the nearest facility, or due to lack of access for other reasons (ex. transport, clan issues, inability to leave the family for a full week or insecurity). The mortality and default rates in these programmes are usually high. Although there may be no alternative, this set-up is not ideal for children presenting complications since the OTP cannot provide the specialised treatment they need, including therapeutic milks or continuous surveillance of the patient.
SFP for moderate malnutrition In Somalia, each of the previous two set-ups can be found with or without SFP. When no SFP is available, children with MAM cannot be treated and they are at risk of developing SAM. As well, children that complete treatment at the OTP cannot be referred to the SFP, and therefore they can relapse more easily.
Isolated SFP
In some areas, SFPs are implemented in the absence of OTP or SC. In these cases, the centres will admit all malnourished children regardless of their severity. High mortality and defaulting are usual in these cases.
Seasonal centres
Given the seasonality of malnutrition and the difficulties to maintain centres open throughout the year, some agencies prefer to open the centres only during the season when malnutrition is high. This requires less resources, but endangers the continuity of services and demands a bigger effort of training and supervision each time that the centres are reopened.
Only the first of these scenarios is desirable, particularly if supported by SFP. All others set-ups should be upgraded when possible. This upgrade may not be realistic in many parts of Somalia, at least in the short term. These guidelines take this into account and provide specific advice adapted to the current situation.

22
Key elements for programme quality:
The implementation of programmes to manage acute malnutrition requires a series of elements to ensure their quality and success. Some of these elements are particularly important in the Somalia context. Each of them needs to be given careful attention and dedication during the duration of the programme. The main elements are:
Integration of the different components of the programme. Integration consists of referral of patients from one level of care to the next level, as needed and without interruption in the continuity of treatment. It also includes coordination and exchange of information to monitor and improve programme results.
Community mobilisation, Supplementary Feeding, Outpatient care and Inpatient care need to be understood as the components of the same programme, rather than different programmes. This needs to be particularly stressed when each of the facilities is managed by a different organisation. In this case, regular meetings and exchange of information are mandatory.
Training of all staff involved in the management of acute malnutrition is of radical importance. This includes all levels of staff, from the community volunteers to the doctors in hospitals. The modern protocols for the management of acute malnutrition were developed in the last 10 years. Most health staff currently working in the health system have therefore not been trained on the protocols during their formative years. Therefore, continuous training should be in place in all programmes in order to train new staff, incorporate new developments, and to learn from experiences.
Supervision is key to maintaining and improving the quality of the programmes. It also allows for quick reaction to specific problems and for adapting to changing circumstances. Supervision should be implemented in a systematic way and be an opportunity for learning from your own work, rather than just an inspection of duties.
In the Somalia context, training and supervision are often difficult or challenging, given the limited access of senior (and particularly international) staff to the centres. Innovative ways of training and supervising staff need to be developed for this purpose. These rely extensively in communication technology – usually available at district or regional level in most parts of Somalia. Some ideas may include:
• emailing of weekly/monthly statistics, reports, supplies requests, etc.• scan-and-email or faxing of centre register books and/or patient’s cards (including, for example, some randomly
selected cards, or those of patients that presented a specific problem or died),• telephone or Skype conferences to discuss a specific issue or to update on a protocol,• taking pictures of a particular case and sharing with colleagues for discussion,
Community mobilisation and early diagnosis. Regardless of the set-up of the programme, community mobilisation and early diagnosis are the most important components. When properly implemented, they will contribute to increased coverage of the programme, and will identify children at an early stage of malnutrition before the development of complications that can result in the death of the patient if he/she cannot be transferred to the SC. Community mobilisation will help as well to develop good relationships and understanding with the local community.
All programmes should have dedicated staff and resources for community mobilisation, and develop a proper strategy for its implementation. It should never be left as an additional activity to be done “when times allows” or be left only in the hands of volunteers or community leaders, however committed they are.

Guideline for Management of Acute Malnutrition
Section 3Diagnosis of Acute Malnutrition
and Admission criteriadiagnosis
23

24
Diagnosis of acute malnutrition
The diagnosis of acute malnutrition can be done in different ways:
• Weight for height (W/H): Calculated from patient’s weight, height and sex, using WHO Growth Standards (Z-scores). The weight and the height of the child are compared to those of a standard population of the same sex.
• Middle Upper Arm Circumference (MUAC): Using a band around the mid-point of the upper left arm of the patient.
• Bilateral Oedema: bilateral pitting oedema, for identification of Kwashiorkor and Marasmic kwashiorkor.• Severe Wasting and other clinical signs of SAM and its complications.
The raw measurements (weight, height, MUAC and oedema) are of radical importance. Mistakes in these measurements will result in a wrong diagnosis and unnecessary treatment or, worst, in a malnourished child not being treated.
The process of diagnosis has, therefore, three steps:
1. Measure the child’s oedema, MUAC, weight and height, and calculate W/H.2. Decide if the child presents acute malnutrition, and if it is moderate (MAM) or severe (SAM).3. If the child has SAM, run an appetite test and observe presence of complications, to decide if the child needs treatment at the SC.
The role of each of this possible diagnosis is different:
• MUAC and oedema are used for screening of malnutrition at the community.• W/H, MUAC and oedema are used for screening of malnutrition at the centre and to classify the patient as
normal, MAM or SAM, in order to decide on the admission of the patient to the programmes. Depending on the level of severity of these indicators, the patient will be admitted to a different type of programme (TSFP, OTP or SC).
• A series of clinical signs, and above all the lack of appetite (anorexia), are used to identify complicated SAM, which requires treatment at the SC.
• Weight, oedema and presence of clinical signs (ex. appetite) are used to monitor the evolution of the patient under treatment.
An individual is malnourished when he/she meets AT LEAST one diagnostic criteria of malnutrition (W/H, MUAC or oedema). For this reason, the patient cannot be declared cured after treatment until he/she has recovered for ALL the criteria).
See FC-7 for criteria of admission in the programme and FC 13 and FC 20 for discharge criteria.

Guideline for Management of Acute Malnutrition
25
Field Card 1. Taking measurements
1. Taking a child’s weight
Children are weighed with a 25 kg hanging sprint scale, graduated to 0.100 kg. Do not forget to re-adjust the scale to zero before each weighing.
A plastic wash basin should be supported by four ropes that attach (are knotted) underneath the basin. The basin is close to the ground in case the child falls out and to make the child feel secure during weighing. If the basin is soiled, first clean it with disinfectant. The basin is comfortable and familiar for the child, can be used for ill children, and is easily cleaned. In the absence of a basin, weighing pants can be used although are sometimes inappropriate for very sick children. When the pant is soiled, it can be cleaned and disinfected to reduce the risk of passing an infection to the next patient.
When the child is steady in the basin or pant, record the measurement to the nearest 100 grams, recording with the frame of the scale at eye level. The scales must be checked for accuracy by using a known weight on a regular basis, i.e. weekly.
Taking a child’s weight
Instructions on Taking the Weight
• Before weighing the child, take all his/her clothes off. If possible, provide privacy for girls.
• Zero the weighing scale (i.e. make sure the arrow is on 0 after placing the empty basin or the weighing pants).
• Ensure that the weighing scale is at eye level.
• Place the child in the basin or the weighing pans.
• Make sure the child is not holding onto anything.
• Read the child’s weight. The arrow must be steady.
• Record the weight in kg to the nearest 100 g e.g. 6.6 kg.
• Do not hold the scale when reading the weight.
Source: How to Weigh and Measure Children: Assisting the Nutritional Status of Young Children, United Nations, 1986
1 2
3
4
5

26
2. Using the electronic scale.
Controls and displays
Mother-and-baby key

Guideline for Management of Acute Malnutrition
27
If several children are to be weighed consecutively, it is important that it is always the same adult who performs the measurement and that this person’s weight does not change (e.g due to a piece of clothing being removed).
The mother-and-baby function remains switched on until
• you press the mother-and-baby key again (total weight is displayed).
• the scale swtiches off automatically.

28
3. Taking a Child’s Length or Height
Taking a child’s length
For children less than 87 cm the measuring board is placed on the ground.
• You will need two people to take a good measurement. If there is no assistant, the mother may help by holding the head straight.
• The child is placed lying down along the middle of the board.
• The assistant holds the sides of the child’s head and positions the head until it firmly touches the fixed headboard with the hair compressed.
• The measurer places her hands on the child’s legs, gently stretches the child and then keeps one hand on the thighs to prevent flexion.
• While positioning the child’s legs, the sliding foot-plate is pushed firmly against the bottom of the child’s feet.
• To read the length measurement, the foot-plate must be perpendicular to the axis of the board and vertical.
• The length is read to the nearest 0.1 cm.
Taking a child’s height
For children taller than 87 cm the measuring board is fixed upright on level ground.
• The child stands, upright against the middle of the measuring board.
• The child’s head, shoulders, buttocks, knees, and heels are held against the board by the assistant.
• The measurer positions the head and the cursor.• The height is read to the nearest 0.1 cm.• Measurement is recorded immediately.
1111111
7
8
9
23
4
5
6
Source: How to Weigh and Measure Children: Assisting the Nutritional Status of Young Children, United Nations, 1986
Source: How to Weigh and Measure Children: Assisting the Nutritional Status of Young Children, United Nations, 1986
Measurer on knees
Assistant on knees
Questionnaire and pencil on clipboard on fl oor or ground
Headpiece fi rmly on head
Hand on chin
Shoulder level
Child’s handsand arms at side
Left hand on knees; knees together against board
Right hand on child’s heels against back andless on board
Line of sight
1
2
3
4
5
6
7
8
9
10
12
13
15
16
11

Guideline for Management of Acute Malnutrition
29
How to Measure MUAC
• Ask the mother to remove any clothing covering the child’s left arm.
• Calculate the midpoint of the child’s left upper arm: first locate the tip of the child’s shoulder with your finger tips.
• Bend the child’s elbow to make the right angle.
• Place the tape at zero, which is indicated by two arrows, on the tip of the shoulder and pull the tape straight down past the tip of the elbow.
• Read the number at the tip of the elbow to the nearest centimetre. Divide this number by two to estimate the midpoint. As an alternative, bend the tape up to the middle length to estimate the midpoint.
• Mark the midpoint with a pen on the arm.• Straighten the child’s arm and wrap the
tape around the arm at the midpoint. Make sure the numbers are right side up. Make sure the tape is flat around the skin.
• Inspect the tension of the tape on the child’s arm. Make sure the tape has the proper tension and is not too tight or too loose. Ensure that there is no bulging (the tape sits well on the skin and cannot be moved). Repeat any step as necessary.
• When the tape is in the correct position on the arm with correct tension, read and call out the measurement to the nearest 0.1cm.
• Immediately record the measurement.
4. Taking a Child’s Middle Upper Arm Circumference (MUAC)
MUAC is especially used for children six months old to five years old to measure thinness.
The colours in the MUAC tapes used in most centres in Somalia do not reflect current criteria to define malnutrition. Until these are replaced, DO NOT FOLLOW THE COLOUR CODES.
Instead, just note the number of mm and follow the guidelines: < 115 mm : Severe acute malnutrition >=115 and < 125 mm : Moderate acute malnutrition > 125 mm: No malnutrition
Source: How to Weigh and Measure Children: Assisting the Nutritional Status of Young Children, United Nations, 1986

30
5. Diagnosing Bilateral Oedema
• Oedema is the swelling of the body or one of its parts.• Oedema is an indication of Kwashiorkor.• Kwashiorkor oedema should be in both feet (bilateral). It is noticed when the bilateral oedema is pitting on both
feet after pressing for a few seconds. “Pitting” means that when you press on the top of the feet or the leg the finger leaves a pit in the skin for some seconds.
• Any oedemas which appear only in one foot or leg are not Kwashiorkor. Oedema that is not pitting is not Kwashiorkor either. However these patients still need to be seen by a medical person, in order to do a proper diagnosis.
Steps of diagnosing oedema
• Oedema is evaluated first on the top of the feet.• Press gently with your thumbs on each foot, while you count: 121, 122, 123 (approx 3 seconds).• After removing the thumb, there is kwashiorkor oedema if a pit stays for some seconds.• Do the same thing for the leg (above the knee) and for the back of the hands and the face (around the eyes).
Oedema is coded in the following way: Oedema in both feet: + Oedema in both feet plus legs: + + Oedema in both feet, legs and hands or face: + + +
@ Get picture for “bilateral” and for other parts of the body
Pitting oedema on dorsum of foot. After applying pressure for a few seconds, a pit remains after the fi nger is removed.
1
2

Guideline for Management of Acute Malnutrition
31
Field Card 2. Determining Weight-for-height (W/H)
Most children who are healthy have weight in a normal range. When children weight less than the normal, they are malnourished. This can be measured and classified into Z-scores. Z-scores are used to see if the children are moderately or severely malnourished and admit then in the different programmes.
Use the charts in the following two pages of this Field Card to understand how they work.
This is the process to follow for each patient:
1. Write down the weight, height and sex of the child.2. Select the chart that corresponds to the child’s sex (there is one for boys and one for girls).3. Select the column to use: 1. Length: If the child was measured lying down (less than 87 cm), use the chart in the left. 2. Height: If the child was measured standing (more than or equal to 87 cm), use the chart in the right.4. Follow the column to the left of the chart you just selected. Scroll down through the numbers until you reach a
number higher than the height of the child. Select the height value that is closest to the height of the child: 1. Example: If the height of the child was 55.7, choose 55.5; 2. Example 2: If the height of the child was 55.8, choose 56.5. Now you have selected the line that is going to be used to check the child’s weight.6. Follow this line to the right (it is recommended to use a ruler, to be sure that you do not move to a different
line). When you reach a weight that is above the weight of the child, stop. 7. Check the colour of the column where you have stopped, or the heading of the column, to obtain the W/H group
of the patient. 8. Write the result.9. Using the W/H, MUAC and oedema findings, decide if the child needs admission, and to which programme.
The groups of weight for height are:
< -3 -----------------> Severe acute malnutrition. < -2 -----------------> Moderate acute malnutrition. 0 -----------------> Normal
For interpretation,
< - 3 means that the patient’s W/H is below -3 Z-scores. < - 2 means that the patient’s W/H is between -3 and - 2 Z-scores. 0 means that the patient’s W/H is between -2 and 0 Z-scores.

32

Guideline for Management of Acute Malnutrition
33

34
Field Card 3. The appetite test
Once the child has been diagnosed as presenting SAM, you need to decide if the patient can be treated at the OTP or if he/she needs to be transferred to the SC. This is done by looking for the presence of complications and through the appetite test.
Why do we do the appetite test?
The appetite test is the most important step to decide if a child has complicated malnutrition and should go to the SC. A poor appetite means that the child is ill and requires treatment in a SC or hospital.
A poor appetite means that the child has a significant infection or a major metabolic abnormality such as liver dysfunction, electrolyte imbalance, and cell membrane damage or damaged biochemical pathways. These are the patients at immediate risk of death. Often, the child with SAM does not present any other signs of these complications.
Furthermore, a child with a poor appetite will not take the diet at home and will continue to deteriorate or die. As the patient does not eat the special therapeutic food (RUTF) the family may take the surplus and become habituated to sharing.
How to do the appetite test
1. The appetite test should be conducted in a separate quiet area. 2. Explain to the carer the purpose of the appetite test and how it will be carried out. 3. The carer should wash her hands and the child’s hands. 4. The carer should sit comfortably with the child on her lap and either offer the RUTF from the packet or put a
small amount on her finger and gives it to the child.5. The carer should offer the child the RUTF gently, encouraging the child all the time. If the child refuses then the
carer should continue to quietly encourage the child and take time with the test. The test usually takes a short time but may take up to one hour. The child must not be forced to take the RUTF.
6. The child needs to be offered plenty of safe water to drink from a cup as he/she is taking the RUTF.
The test can be done with a table spoon (if the size of the sachet is not practical). Take the amount of one spoon and put it in a plate or cup, and let the child eat it with the fingers. When the child has completed one spoon, add a second one – until he/she does not eat any more. Count the number of spoons to see the result of the test.
This is the minimum amount that malnourished patients should take to pass the appetite test. If the child does not take at least the amount in the table, in sachets or in spoons, then he/she should be sent to the nearest SC.
If you think that the child did not pass the test because he/she was frightened or didn’t like the product, try repeating it in a calmer environment. This test can be done with other products other than Plumpy’nut, following the amounts in spoons.
RUTF (Plumpy’nut)
Body Weight (kg) Sachets Spoons
Less than 4kg 1/8th 1/3rd
4 - 6.9 1/4th 2/3rd
7 - 9.9 1/3rd 1
10 - 14.9 1/2th 1 1/2th
15 - 29 3/4th 2
Over 30kg 1 3

Guideline for Management of Acute Malnutrition
35
Field Card 4. Clinical presentation of SAM
These are the main clinical characteristics of Marasmus and Kwashiorkor, the two manifestations of SAM.
• Severe weight loss and wasting• Ribs prominent• Limbs emaciated• Muscle wasting• May have good appetite• With correct treatment, good prognosis
• Bilateral pitting oedema • Loss of appetite• Brittle thinning hair• Hair colour change • Apathetic and irritable• Face may seem swollen• High risk of death
Marasmus Kwashiorkor

36
Field Card 5. SAM History and examination
The usual signs and symptoms that are recorded on these patients are the following (see OTP card and SC card):
History: Ask the carer if the child presented any of the following in the last few days:
Physical examination: Explore the patient for any of the following:
Diarrhoea (Yes, No) If yes, ask for more details
Stools per day (1-3, 4-5, >5) Diarrhoea is only when there are more than 3 watery stools/day
Vomiting (Yes, No) If yes, ask for more details
Cough (Yes, No) If yes, ask for more details. Consider respiratory distress
Appetite (Good, Poor, None) Ask the mother. Do not report the appetite test here!
If oedema, how long swollen (number of days) Longer duration of oedema implies severity
Breastfeeding (Yes, No) If the child is less than 1 year and not breastfeed, ask why, and give counseling
Respirations per minute (<30, 30-39, 40-49, 50-59, 60+)
Respiratory distress if: >60 (children <2mths); >50 (2 – 12 mths); >40 (1-5 yrs); >30 (over 5 yrs).
Chest retractions (Yes, No) This is always a sign of respiratory distress
Temperature (number in ºC) Remember, SAM children may not have fever
Conjunctiva/palms (Normal, Pale) If pale, consider anaemia. Check chapter 8 to decide if it is real anaemia or hemodilution
Eyes (Normal, Sunken, Discharge)
If eyes sunken, consider dehydration. Check chapter 8. If discharge, treat for conjunctivitis
Dehydration (None, Moderate, Severe)
Always check Chapter 8 for diagnosis of dehydration. Malnutrition and dehydration are very similar and can be confused!
Ears (Normal, Discharge) If discharge, treat for otitis
Mouth (Normal, Sores, Candida)
If sores or candida, treat as in FC 18
Lymph nodes (None, Neck, Axilla, Groin)
If lymph nodes are swollen consider local infections
Disability (Yes, No) Consider what special help the child may need.
Skin changes (None, Scabies, Peeling, Ulcers/Abscesses)
Treat according to findings, check FC 18
Hands/feet (Normal, Cold) If cold, consider dehydration and septic shock. Check chapter 8.

Guideline for Management of Acute Malnutrition
37
Field Card 6. Pathophysiology of Severe Acute Malnutrition
This section has been specifically written for doctors attending patients with complicated SAM at the Stabilisation Centre or in the Paediatric Ward of a Hospital. It is important to understand as the characteristics of children with SAM are so different from other sick children.
Severe acute malnutrition can result in profound metabolic, physiological and anatomical changes. Virtually all physiological processes are altered due to severe acute malnutrition. Every organ and system is involved in reductive adaptation.
Reductive adaptation is the physiological response of the body to undernutrition i.e. systems slowing down to survive on limited macro and micro-nutrient intake. The system reduces activity, to adapt to the lack of nutrients and energy.
Reductive adaptation results in profound physiological and metabolic changes, some of which can be observed by the clinician and others which are not. The initial reductions will not alter normal functioning of the body BUT will affect its capacity to adapt to any other new situation (an infection, cold, or even to an IV infusion or excessive oral liquids). For example, the circulatory system may still be working correctly, with no signs or symptoms of presence of a problem... BUT it may not be able to adapt to a sudden increase of circulatory volume (after an infusion or a transfusion, for example). Since the adaptive mechanisms to increased volume cannot be mobilised, a simple infusion may result in cardiac overload and lethal pulmonary oedema. Similar situations occur with: digestive system, and the amount of proteins and other nutrients that can be absorbed in one meal; immune system, and its ability to respond to infection; the liver’s ability to detoxify; and the kidney’s ability to excrete, etc.
In addition, some of the changes mentioned result in unusual signs and symptoms. For example, a child with severe acute malnutrition may not be able to present fever in face of an infection. In fact, very often the infection will present with hypothermia! You can see other examples in the following page.
These are the reasons why it is so important to follow standard protocols for the treatment of severe acute malnutrition and its complications (like this one). The changes in metabolic and physiological responses in the malnourished child are so important that therapeutic decisions which are lifesaving in a well nourished child can be potentially deadly in a malnourished child.
The following page presents some of the main alterations in each of the body systems. Knowing them can help understand the evolution and therapy of severe acute malnutrition and its complications.

38
Cardiovascular system Gastro-intestinal system
• Cardiac output and stroke volume are reduced.• Infusion of saline may cause an increase in venous
pressure.• Any increase in blood volume can easily produce
acute heart failure.• Any decrease will further compromise tissue
perfusion.• Blood pressure is low.• Renal perfusion and circulation time are reduced.• Plasma volume is usually normal and red cell volume
is reduced.
• Production of gastric acid is reduced.• Intestinal motility is reduced.• Pancreas is atrophied and production of digestive
enzymes is reduced.• Small intestinal mucosa is atrophied; secretion of
digestive enzymes is reduced.• Absorption of nutrients is reduced.
Liver function Genitourinary system
• Synthesis of all proteins is reduced.• Abnormal metabolites of amino acids are produced.• Capacity of liver to take up, metabolize and excrete
toxins is severely reduced.• Energy production from galactose and fructose is
much slower than normal.• Gluconeogenesis is reduced, with high risk of
hypoglycemia during infection.• Bile secretion is reduced.
• Glomerular filtration is reduced.• Capacity of kidney to excrete excess acid or a water
load is greatly reduced.• Urinary phosphate output is low.• Sodium excretion is reduced.• Urinary tract infection is common.
Circulatory system Endocrine system
• Basic metabolic rate is reduced by about 30%.• Energy expenditure due to activity is very low.• Both heat generation and heat loss are impaired.• The child becomes hypothermic in a cold environment
and hyperthermic in a hot environment.
• Insulin levels are reduced and the child has glucose intolerance.
• Insulin growth factor 1 (IGF-1) levels are reduced.• Growth hormone levels are increased.• Cortisol levels are usually increased.
Immune system
• All aspects of immunity are diminished.• Lymph glands, tonsils and thymus are atrophied • Ig-A levels in secretions are reduced.• Complement components are low.• Phagocytes do not kill ingested bacteria efficiently.• Tissue damage does not result in inflammation or migration of white cells to the affected area.• Acute phase immune response is diminished and cell-mediated immunity is severely depressed.• Typical signs of infection, such as an increased white cell count and fever, are frequently absent.• Hypoglycaemia and hypothermia are signs of severe infection usually associated with septic shock.
Guideline for Management of Acute Malnutrition
39
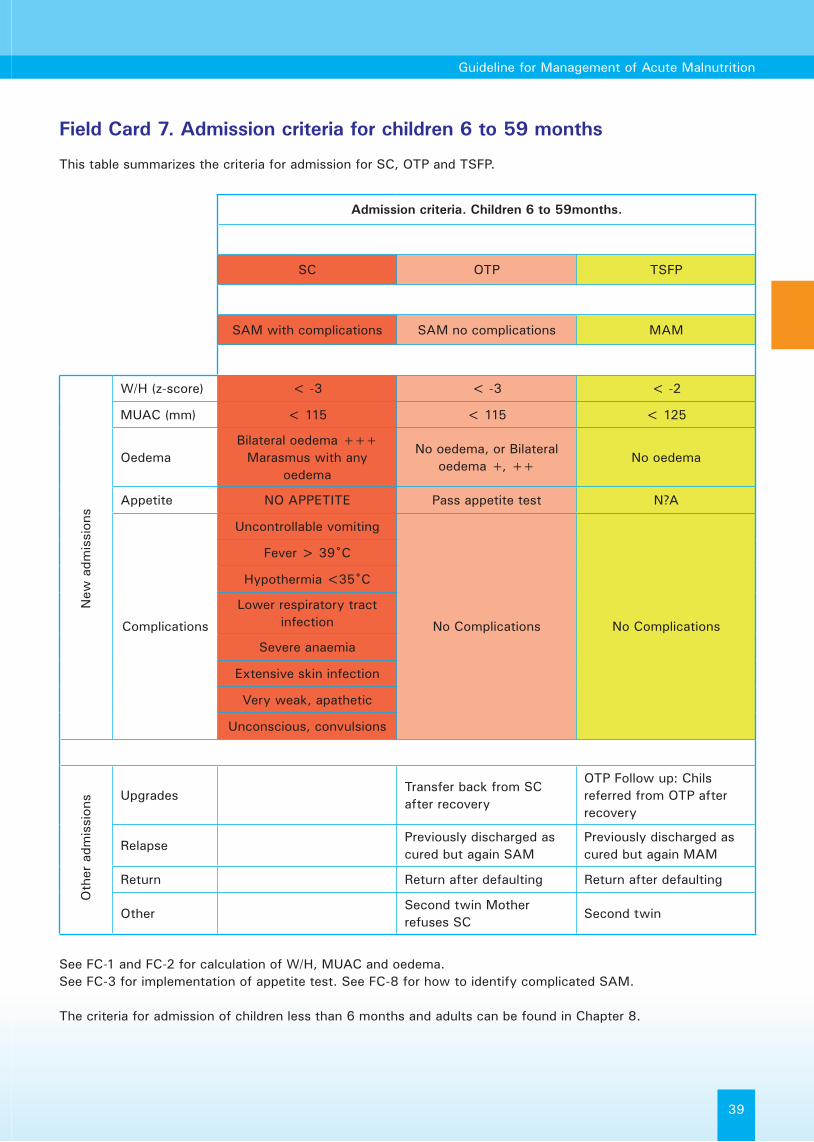
Field Card 7. Admission criteria for children 6 to 59 months
This table summarizes the criteria for admission for SC, OTP and TSFP.
See FC-1 and FC-2 for calculation of W/H, MUAC and oedema.See FC-3 for implementation of appetite test. See FC-8 for how to identify complicated SAM.
The criteria for admission of children less than 6 months and adults can be found in Chapter 8.
Admission criteria. Children 6 to 59months.
SC OTP TSFP
SAM with complications SAM no complications MAM
W/H (z-score) < -3 < -3 < -2
MUAC (mm) < 115 < 115 < 125
OedemaBilateral oedema +++
Marasmus with any oedema
No oedema, or Bilateral oedema +, ++
No oedema
Appetite NO APPETITE Pass appetite test N?A
Complications
Uncontrollable vomiting
No Complications No Complications
Fever > 39˚C
Hypothermia <35˚C
Lower respiratory tract infection
Severe anaemia
Extensive skin infection
Very weak, apathetic
Unconscious, convulsions
UpgradesTransfer back from SC after recovery
OTP Follow up: Chils referred from OTP after recovery
RelapsePreviously discharged as cured but again SAM
Previously discharged as cured but again MAM
Return Return after defaulting Return after defaulting
OtherSecond twin Mother refuses SC
Second twin
New
adm
issi
ons
Oth
er a
dmis
sion
s

40
Field Card 8. Complicated and non-complicated malnutrition
A child with severe acute malnutrition will be treated in the OTP if he/she has good appetite and no complications, but will be admitted to the SC if there are complications or appetite is poor.
It is important to be familiar with the complications of malnutrition in order to identify them and refer the child when necessary. Ask your supervisor for advice if you are not sure that you can identify each of these complications.
On admission:
This table is used for deciding who needs to be sent to SC, but as well to identify failure to respond to treatment. It should be present in ALL consultations, and each item in the list should ALWAYS be checked.
On children that are already under treatment:
Severe complication How to identify it
Oedema +++ Bilateral pitting oedema. See FC-1
Anorexia (lack of appetite) Perform appetite test
Intractable (uncontrolled) vomiting The child presents sudden vomiting, and he cannot retain it (ex. He can't wait to do it outside)
Fever > 39 oC or hypothermia < 35 oC Use thermometer and measure for at least 1 minute.
Lower respiratory tract infection Always count respirations for at least 1 minute. 60 resp/min for under 2 months 50 resp/min for 2 – 12 months 40 resp/min for 1 – 5 yearsOR any chest in-drawing.
Severe anaemia Check palms are very pale– compare with a healthy child. If unclear, check conjunctiva or nail beds.
Extensive skin infection Examine the child without clothes for skin infection or lesions and ask the mother for any other severe infection.
Very weak, apathetic, unconscious, convulsions Observe child's attitude. Ask the mother about convulsions (fitting – absences).
Hydration status Recent history of diarrhoea or vomiting, and RECENT appearance of clinical signs of dehydration reported by the carer
Failure to gain weight Weight loss for 3 consecutive visitsStatic weight for 5 consecutive visits
Increase or new oedema Increase of oedema, or new oedema in a child that did not have it on admission.

Guideline for Management of Acute Malnutrition
41
Field Card 9. Admission criteria for other age groups
This table summarizes the criteria for admission for MAM (STFP) and SAM (OTP, and SC if severe complications).
To decide if the patient needs to be transferred to the SC, use the same criteria as for children (FC8).ALL infants with SAM should be treated in the SC. These children cannot take RUTF (see Chapter 7).
Indicator SAM MAM Normal
Infants less than 6 months
W/H (W/L Z-scores) < - 3Static weight or losing weight at home
Gains weight at home
Oedema Present Absent Absent
Clinical presentation To weak to suckle breast Poor feeding Normal feeding
Adolescents (10 – 18 years)
W/H (Z-scores) < - 3 < - 2 Above - 2
MUAC (mm) < 160 N/A N/A
Oedema Present Absent Absent
Adults (older than 18 years)
BMI and clinical signs< 16 with weight loss in the last 4 weeks
< 16 but no weight loss
Oedema Present Absent Absent
Pregnant and lactating women
MUAC (mm)< 210 with weight loss in the last 4 weeks
< 210 with no weight loss in the last 4 weeks
No weight loss

42

Guideline for Management of Acute Malnutrition
Section 4Supplementary Feeding
Management of MAM
43

44
Overview
The main objective of Supplementary Feeding Centres (SFPs) is to treat Moderate Acute Malnutrition (MAM) and prevent individuals with MAM from becoming severely malnourished (SAM).
Supplementary programmes are usually separated into two types:
Blanket SFP: Blanket feeding is addressed to all members of a particular group, like children below 5 years or pregnant or lactating women, and is independent of their nutritional status. The distribution is usually intended for all the family. Supplementary food distributions are typically done once a month, but other frequencies are possible. Blanket feeding is usually implemented only during short periods of time, coinciding with existing or expected peaks in malnutrition.
Possible groups (more than one of these groups can be addressed at the same time):• All children under 5 years (or under 110 cm) or• All children under 10 years (or under 130 cm) or• All pregnant and lactating women or• The chronically ill, as defined by a diagnosis of HIV or TB or Kala-Azar, or other, or• The disabled, or• The elderly (over 60 years old, for example),• etc.
Targeted SFP: Targeted feeding is addressed only to those that present MAM. These can be children below 5 years, older children and adults, pregnant and lactating women, etc. Targeted feeding is offered as well to children discharged fromOTP or SC, after recovering from SAM.
Targeted feeding can be implemented weekly, bi-weekly or even less often. Patients are followed up at each visit, and discharged when they recover from malnutrition.
Both types of SFPs are related to other services, as follows:
Community mobilisation: Patients with MAM are identified at the community level and referred to SFP. Patients that are already following treatment in the SFP and that are absent for one or two weeks can be followed up at their homes by the community mobilisation teams, to ensure that they return to the programme before they become defaulters (in the third week of absence).
OTP/SC: Patients that do not recover or deteriorate while in treatment in SFP are referred to OTP for evaluation and treatment. Patients screened at the SFP that present SAM are sent directly to the OTP. When a patient recovers in OTP/SC he is sent to SFP in order to consolidate his nutritional status and prevent relapses.
Take home / wet rations:
During emergencies, food rations can be distributed as either “wet” (i.e. on-site) or “dry” (i.e. take-home) rations. The ideal dry ration supplementary food provides, per day, 1000 to 1200Kcal; 35g to 45g of protein; and fat supplying 30% of required energy. On-site supplementary feeding provides 500 to 700Kcal per beneficiary per day; including 15g to 25g of protein; and with fat supplying 30% of required energy.

Guideline for Management of Acute Malnutrition
45
Admission criteria to targeted SFP
See Chapter 3 for information on how to diagnose Severe Acute Malnutrition (check Field Cards 1 to 9).Admission criteria to targeted SFP are in yellow (far right column) of this table (FC -7). The criteria for other services are presented as well in order to properly refer the children presenting with SAM.
Admission criteria. Children 6 to 59months.
SC OTP TSFP
SAM with complications SAM no complications MAM
W/H (z-score) < -3 < -3 < -2
MUAC (mm) < 115 < 115 < 125
OedemaBilateral oedema +++
Marasmus with any oedema
No oedema, or Bilateral oedema +, ++
No oedema
Appetite NO APPETITE Pass appetite test N?A
Complications
Uncontrollable vomiting
No Complications No Complications
Fever > 39˚C
Hypothermia <35˚C
Lower respiratory tract infection
Severe anaemia
Extensive skin infection
Very weak, apathetic
Unconscious, convulsions
UpgradesTransfer back from SC after recovery
OTP Follow up: Chils referred from OTP after recovery
RelapsePreviously discharged as cured but again SAM
Previously discharged as cured but again MAM
Return Return after defaulting Return after defaulting
OtherSecond twin Mother refuses SC
Second twin
New
adm
issi
ons
Oth
er a
dmis
sion
s
The patient is discharged cured from SFP when W/H and MUAC are above the admission criteria for two consecutive visits. See FC 13 for more details on discharge criteria.There are no specific admission criteria for Blanket SFP. All members of the group selected for supplementation are included in the programme, regardless of their nutritional status.

46
Nutrition support: Diet and frequency
The following products can be distributed as take-home rations or taken on-site by the beneficiary. The choice of the product to distribute is done at the coordination level, not in the centre. Refer to the instructions given by your supervisors for the amounts to distribute and the target group.
In the majority of programmes, the amount of supplementary food given to each beneficiary is THE SAME.Weight of the patient is usually not taken into consideration for SFP distributions. These amounts may change from one programme to the other, or even within the same programme at different periods. No matter what product is given, ALWAYS recommended that the child breast-feeds before taking it, if the child is still breast feeding.
Food commodities for Supplementary Feeding Programmes:
Food commodity Quantity/person/day Comments
Recommended food commodities for supplementary feeding programmes
CSB/UNIMIX Dry Ration: 200-250gWet Ration: 100-150g
PREMIX:Dry Ration: 200g CSB + 25g oil + 20g sugarWet Ration: 125g CSB +10g oil + 10g sugar
• Maize-soya blend flour.• Fortified with micronutrients.• Suitable for children, pregnant
and lactating women.• Oil and/ or sugar may be
distributed separately.• Premix MUST be done under
hygienic conditions. Premix should not be kept past 2 weeks.
Supplementary Plumpy® 1 sachet (92g) per child per day • ALWAYS give with clean drinking water
• High energy density• Does not contaminate• No need of mixing or packaging• Better nutrient profile than CSB
Other products are being made available, and may be used in Somalia. Check with your supervisor for specific guidelines whenever a new product is sent, and at the start of a new programme.
Non-food items
Non- food items such as mosquito nets, soap, blankets, tents, and buckets can also be distributed depending on availability and the needs of the beneficiaries. Most non- food items are distributed on admission, except for consumable items such soaps that can be provided to beneficiary at each visit.
Storage and handling of food items
Food items must be stored and handled following strict guidelines. • Record any food item entering or leaving the store with stock control cards and report monthly, • Maintain store security (lock, guards). • Check for damaged or expired food items and separate them.

Guideline for Management of Acute Malnutrition
47
Field Card 10. How to prepare CSB at home
• Ensure that the water being used for cooking is safe before starting to cook
• Wash your hands with soap before you start to prepare the porridge.
• Mix CSB (or UNIMIX) with part of the cold water to make a paste
• Add the rest of the water and bring to boil for no longer than 10 minutes
• Add (if available), oil, sugar, seasonal fruits and or local nuts to increase the energy density and taste
• Serve on a clean plate or bowl• Wash the child’s face and hands with water and soap
before they eat • Use a separate plate for the child
Storage of CSB at home:• Keep CSB covered to prevent flies and other dirt getting into it • Keep CSB in the coolest part of the house• Use the CSB within 2 weeks to prevent it from spoiling
Method 2 - Thick Porridge
1 cup - CSB
2 cups - water
Routine Medication
Field Card 11. Routine medication in SFP
In the SFP, a nurse should check medical conditions, immunization status, anaemia and common infections then record the information on the beneficiary card.
All beneficiaries must receive systematic treatment to cure any current infection, as well as to minimize chance of catching others. Record all treatment in the register and beneficiary card.
For details on usage of each of the drugs in this list, refer to FC 17 in the OTP chapter.
Systematic Medicine for Moderate Malnutrition in SFP
Name of Product When Age / Weight Prescription Dose
VITAMIN A* AT ADMISSION
6 months to < 1 year≥ 1 year
100 000 IU
200 000 IU Single dose on admission
DO NOT GIVE TO CHILDREN WITH OEDEMA
MEASLES VACCINATION
AT ADMISSION From 9 months (standard)Single dose on
admission
ALBENDAZOLE AT ADMISSION
< 1 year DO NOT GIVE NONE
12 - 23 months 200 mg (1/2 tablet) Single dose on second visit≥ 2 years 400 mg (1 tablet)
IRON FOLATE ** AT ADMISSION
24 - 59 months 20 - 30mg
Daily for one month6 - 11 years 30 - 60mg
adults 60 mg
* VITAMIN A: do not give if child has already received within last 3 months** IRON: DO NOT give in malaria endemic areas. In this areas give only to children with anaemia.
48
Special medication:
Treatment of sick moderately malnourished patients should be in line with the WHO/IMCI protocols. There are common illnesses that can be treated in a supplementary feeding site. These include diarrhoea, vomiting, malaria and other common infections such as ears, eyes and skin infections. In the absence of a nurse/ clinician, all beneficiaries with common ailments should be referred to the nearest health facility.
Field Card 12. Surveillance / Follow up of patients in SFP
Patients may attend the SFP every week, every other week, or monthly. Check with your supervisor for the modality implemented in your centre.
Follow up at the Targeted SFP:
At each visit:• Measurement of oedema.• Measurement of weight.• Measurement of MUAC.• Medical checks and treatment if necessary.• Give routine medicines if necessary.• Assess evolution of the patient: organise home visit or refer if no evolution.• Distribute food items.• Update ration card and SFP card.• Give health education.
Monthly:• Measure height/length.• Recalculate W/H.
When necessary:• Refer to medical facility for health problems that cannot be treated at the SFP.
Follow up at the Blanket SFP:
No individual monitoring is required in Blanket SFPs. There is no registration of beneficiaries.A general report on geographic location, date of distribution, number of beneficiaries and ration composition is required for logistical purposes and evaluation.All beneficiaries should remain in the programme for the duration of the blanket feeding operation (often around 4 months).

Guideline for Management of Acute Malnutrition
49
Field Card 13. Discharge criteria from SFP
There are several ways of discharging a beneficiary from a targeted SFP program, these are;
DISCHARGE CRITERIA for SFP
CuredW/H > -2 Z-score, andMUAC > 125 mm, andFor 2 consecutive visits
Default Absent for 3 consecutive visits
Death Died during time registered in SFP
Non-cured Has not reached target weight within 4 months
Transfer to OTP/SCCondition has deteriorated and requires transfer to OTP or SC
A child that is sent to a different SFP to continue treatment is not discharged from the programme. He/she should take the card with him/her.
These children need to be taken into account in the statistics in order to calculate the number of children in charge in the centre at the end of the month (to calculate food needs for the centre).
Field Card 14. Failure to respond to treatment in SFP
A child that does not gain weight or develops complications is defined as a failure to respond to treatment. A special procedure should be implemented to identify these children and provide appropriate action (improvement of treatment follow up or transfer). This should be always done before the child reaches the 4 months of treatment and is discharged as “non-cured”.
Criteria for failure to respond to treatment
• Failure to reach discharge criteria after 4 months in the program• No weight gain after 6 weeks in the program• Weight loss over 4 weeks in the program• Weight loss exceeding 5% of body weight at any time.
The reasons for failure to respond can be classified as:
• Problems with the application of the protocol (when many children are not recovering)• Nutritional deficiencies that are not being corrected by the diet supplied in the SFP• Home/ Social circumstances of the patient (ex. Sharing or selling of the food)• An underlying physical condition/ illness (to be examined by an experienced nurse)• Other causes.
Transfer to OTP/SC:
All children that meet the criteria of Severe Acute Malnutrition should be transferred to the OTP or SC depending on their condition. Additionally, those that present a failure to respond to treatment that cannot be corrected in the SFP (after having checked through the list above and tried all options) should also be transferred for further investigation.

50

Guideline for Management of Acute Malnutrition
Section 5Outpatient Therapeutic
Programme (OTP)Management of Uncomplicated SAM
51
52
Overview
Patients with severe acute malnutrition (SAM) with present with appetite and no medical complications can be treated as outpatients in the community, through OTPs. The patient attends the OTP once per week, or once every two weeks, to assess treatment evolution and to receive therapeutic foods and drugs until the next visit. The carer provides the treatment for the patient everyday at home, following indications from OTP staff.
The objective of outpatient management of severe acute malnutrition is to increase access to treatment, establishing the appropriate facilities within or closer to more communities. A system of community mobilisation must always be organised in order to screen, monitor and follow-up malnourished children in the community. A good community mobilization program will help identify children at an early stage in their progression towards malnutrition and will reduce the number requiring transfer to SC.
The intervention in the OTP is not limited to distributing RUTF. Other parts are as important, including the education to the carer on how to follow the treatment, the follow up, and the identification of medical conditions and their treatment.
Working in a OTP is not reduced either to visiting patients. The duties of the staff at the OTP include monitoring the number of admissions and their evolution, keeping and sending statistics, keeping the stores of foods and drugs, and preparing requests of foods and drugs, etc.
Fixed or Mobile teams:
The OTP should ideally be organised as part of MCH activities in a Health Centre. However in some areas with low access to health facilities, it is implemented independently. In both cases, the team of the OTP may be fixed (they always work in the same centre) or mobile.
Weekly or Bi-weekly visits:
In most centres the child is seen weekly, while in others they are seen every other week. Weekly centres have the advantage that the child’s follow up is better (which is particularly important for complicated cases that are treated in OTP instead of in the SC), and they do not have to care so much RUTF home. This can be more manageable and easier to organize for the mother. Where visits are biweekly this allows a single mobile team to cover a wider area and reduces the amount of displacement for mothers and children. In general, both systems can obtain good recovery rates in a similar amount of time.OTP centres do not operate in isolation in the management of acute malnutrition. They have relationships with the other services, as follows:
Targeted SFP (SFP): • The OTP receives patients whose nutrition status deteriorates in SFP. • Children that recover in OTP are sent to the TSFP for 3 months, to consolidate nutrition status and prevent
relapses.
SC: • The OTP can refer to the SC those patients that present on admission with anorexia or medical complications,
as well as those that present them after having started treatment and those that present failure to respond to treatment in the OTP.
• Once the children treated in the SC regain appetite and their medical complications are under control, the OTP receives them to complete the treatment in the community.
Community mobilisation: • As all programmes, the key for success consists of a good community mobilisation programme that will
ensure early diagnosis of cases before they develop the complications that would require treatment at the SC, and to increase coverage of the programme.

Guideline for Management of Acute Malnutrition
53
• Community mobilisation activities help to identify and refer patients to the OTP for assessment of their status and the need of treatment (early case finding).
• The patients that do not evolve correctly in the OTP, or who default from treatment are visited at their homes by the community mobilisation teams. The first visit is done after 2 visits of absence, without waiting for the child to be declared defaulter (which is done after 3 absences).
These relationships are not always possible in the working environment of Somalia, due to lack of SC or TSFP services. In these cases, the following may be needed:
• The children with complicated SAM need to be treated at the OTP from the beginning of treatment.• The children that recover in OTP cannot be transferred to TSFP to consolidate treatment.• In both cases, community mobilisation should be reinforced, to reduce the need for SC.
Admission Criteria
See Chapter 3 for information on how to diagnose Severe Acute Malnutrition (check Field Cards 1 to 9).In particular, check Field Card 7 for the criteria of admission for OTP.
Criteria of admission for OTP and SC:
SC OTP
SAM with complications SAM no complications
W/H (z-score) < -3 < -3
MUAC (mm) < 115 < 115
OedemaBilateral oedema +++
Marasmus with any oedema
No oedema, or Bilateral oedema +, ++
Appetite NO APPETITE Pass appetite test
Complications
Uncontrollable vomiting
No Complications
Fever > 39˚C
Hypothermia <35˚C
Lower respiratory tract infection
Severe anaemia
Extensive skin infection
Very weak, apathetic
Unconscious, convulsions
UpgradesTransfer back from SC after recovery
RelapsePreviously discharged as cured but again SAM
Return Return after defaulting
OtherSecond twin Mother refuses SC
New
adm
issi
ons
Oth
er a
dmis
sion
s

54
Nutrition Support: Diet and Frequency
Nutrition rehabilitation in OTP can be done with take home Ready-to-Use Therapeutic Food (RUTF). This is a specialized food developed specifically for the recovery of severe malnutrition at home. It is an energy-dense, mineral/vitamin-enriched product that is equivalent to F100 with added iron. It contains the required energy and micronutrients to meet the nutritional needs of the severely malnourished child. RUTF is an oil-based, ready-to-use product that has a low risk of contamination.
The RUTF most commonly used in Somalia at the time of writing these guidelines is Plumpy’nut. This product is presented as a peanut paste in metallic sachets that contain 500 kcal (92 g). The child can easily eat the product directly from the sachet (after tearing one corner). The child can eat it with the fingers only if enough hygiene has been ensured (i.e. hands and face washing).
It is of radical importance to provide the correct amounts of RUTF and ensure that the carer understands how and when it has to be given to the child. During monitoring visits medical staff will check that the RUTF is being taken correctly, and will explore with the mother any potential problems with following the recommendations at home.
Information on RUTF for health professionals.
• RUTF (Plumpy’nut) is made from ground nuts, oil, sugar, milk powder and vitamin and minerals. It requires no further cooking or preparation and can be eaten directly from the packet.
• It provides approximately 530Kcal per 100g. The ration given to a severely malnourished child is based on the intake requirement of between 150-200 kcal/kg/day.
• Due to its low moisture (water) content it is safe for home use – a packet can be opened and folded over and reused – the contents do not have to be finished all at one time.
• RUTF should always be given with safe drinking water, to improve absorption.• The amount prescribed to a child is based on their weight and should be adjusted at subsequent OTP visits when
there is weight gain (see FC 15).• For the first week encourage the child to take mainly RUTF, afterwards other family foods can be introduced as
long as the entire RUTF ration per day has been consumed.• Breast feeding should be continued during treatment, and given always before the RUTF, to avoid filling the child
with RUTF so that he/she will not be hungry for breast feeding.• The carer should be advised to provide clean water with the RUTF.• RUTF should never be used in children below 6 months (i.e. they can’t suckle well, which may produce chocking,
and their digestive system cannot process RUTF correctly).
Preparation of RUTF
RUTF is pre-cooked thus does not require preparation. It can be eaten directly from the container or packet.
Field Card 15. Amounts of RUTF to distribute
The child is usually given a week or a two week supply of RUTF at each visit to the OTP. The carer is informed on how much to give daily and how to do it (see FC 16). Learn carefully the instructions to give to the mother, and repeat them at each occasion. In particular, remember the importance of recommending to continue breast feeding if the mother was doing so.
This card presents the amounts of RTUF to give, depending on the body weight of the child.

Guideline for Management of Acute Malnutrition
55
This table refers specifically to Plumpy’nut, the RUTF most commonly used in Somalia. If your project is using a different RUTF, check the specific table for that product.
Some programmes add to this amounts an extra ration, to be kept in stock by the family. This may be useful if they cannot come to the OTP at the normal time – but make sure that they understand that it is only for that purpose, and it is not consumed, shared, or used as an excuse not to come to visit the centre regularly!
If there is a problem with food security or in an emergency situation, a “protection” ration (usually CSB Premix or equivalent) can be given to the family both to assist the family of the malnourished child and to prevent sharing of the RUTF with other family members. The carer must be told that this ration is not for the patient but for the rest of the family only.
Plumpy’nut Dosage
(average of 200 kcal/kg/day)
Weight of the child (kg) Packets per day Packets per 1 week Packets per 2 weeks
3.5 - 3.9 1.5 11 22
4.0 - 5.4 2 14 28
5.5 - 6.9 2.5 18 36
7.0 - 8.4 3 21 42
8.5 - 9.4 3.5 25 50
9.5 - 10.4 4 28 56
10.5 - 11.9 4.5 32 64
>=12 5 35 70
Field Card 16. Taking RUTF at home - messages for the carer.
When delivering these messages, replace the name RUTF for the local name of the product you use.You should know these messages by heart. Always check this Field Card to be sure that you didn’t forget anything.
• Breastfeeding is best – and first. For infants and young children, continue to put the child to the breast regularly.
• RUTF should not be shared. It is a food and a medicine for the malnourished child only.• Give small amounts and often. Sick children often do not like to eat. Give small regular meals of RUTF and
encourage the child to eat often (if possible 8 meals a day). RUTF can be left for later if not finished, and be eaten during the course of the day.
• Give RUTF before other foods (except for breast-milk). RUTF is the only food the child needs in order to recover. Other foods should only be offered after RUTF.
• Offer safe water. Always offer plenty of clean water to drink while he or she is eating the RUTF.• Wash before eating. Use soap for children’s hands and face before feeding if possible. • Keep food clean and covered. • Give RUTF even if child is ill or has diarrhoea. When taking RUTF, the stools of the child may change. This is
normal. When a child has diarrhoea, never stop feeding. Give extra food and extra clean water and breastmilk.• Come to the OTP. Continue coming to the OTP even if the child has problems, or if he/she starts participating
in another programme.

56
Repeat the same messages at each visit, and ask the mother to repeat them as well, in order to check that she has understood them. If the child is having problems gaining weight, you can use this list to ask the mother to explain to you how she used the RUTF at home. Check one point at a time and don’t forget any of them.
In addition to these recommendations, it is important to train carers on how to feed their child with available local foods. Each programme and centre should know what the availability of local foods is, and how they can be used to improve the child’s diet – and transmit this information to the carers.
Routine Medication
Field Card 17. Routine Medication for OTP and SC admissions
The next page presents a summary of the routine medication to be given to ALL children admitted directly into OTP and to SC, even if they do not present clinical signs of infection. Children transferred from one centre to another while undergoing treatment have already received their routine medications, and do not need to receive them again.
Medications are given as a single-dose treatment so that the health worker can observe administration and avoid problems with compliance. The one exception is the first-line antibiotic (Amoxycillin): the first dose should be given in front of the health worker who explains to the carer how to continue treatment at home.
Vitamin A
Give ONLY to wasted patients. DO NOT give on admission to patients with oedema.Check if the child has already received Vitamin A during a vaccination campaign or a health day in the last three months. In this case, do not give Vitamin A again, to avoid overdose.Vitamin A deficiency in Somalia is very prevalent. The amounts of Vitamin. A in RUTF are enough to manage mild deficiencies, but not to treat a child with important Vitamin A deficiency.Vitamin A can be given as well at the 4th week of treatment, including those that have been transferred from Inpatient care and those that did not receive it on admission because they had oedema.
Antibiotic
Most severely malnourished children have several infections, but they cannot be diagnosed due to diminished inflammatory response (which hides the signs of infection). Treat all children admitted to the OTP.First line choice is Amoxycillin for 7 days, as it is effective against small bowel overgrowth, usually associated with malnutrition. See below for dosages based on child’s weight.If a child is receiving Cotrimoxazole prophylaxis due to a chronic disease, this should continue at the same dose throughout the duration of treatment. You still need to give the Amoxycillin to these children.
Malaria treatment
First line treatment in Somalia is with Artesonate (3 day) and Sulphadoxine Pyrimethamine(1 day). See the table below for dosages based in child’s weight. Malaria treatment is give treatment if a rapid diagnostic check and/or microscopy is positive or the child has clinical signs (particularly if fever persists after completing antibiotics),
Measles vaccination
Standard treatment includes measles vaccination to all children admitted to OTP. Measles vaccination is not usually done in Somalia, due to lack of cold chain in many centres, except in the presence of a measles epidemic. As soon as your centre is equipped with a cold chain, start vaccinating all children admitted to OTP.
De-worming
Albendazole is the only routine medicine that is given only on the second visit of the child and only for children above 1 year. In case of doubt on age, give only to children who can walk. In some programmes, Albendazole can be replaced with Mebendazole (but check dosages: they are different).

Guideline for Management of Acute Malnutrition
57
Iron and Folic Acid
Not to be given routinely, since there is enough in RUTF. Where anaemia is identified, treatment should begin after 14 days of care and NEVER before, following standard guidelines. For severe anaemia, refer to inpatient care.
Other nutrients
RUTF already contains all the other nutrients required to treat the malnourished child. Additional potassium, magnesium or zinc should not be given – even if they present diarrhoea! -, as far as the child takes the RUTF, as an additional micronutrients may cause excesses.
AMOXYCILLIN DOSAGES
ROUTINE MEDICINES FOR SAM IN OTP and SC
Systematic Medicine for Severe Malnutrition in OTP
Name of Product When Age / Weight Prescription Dose
VITAMIN A* AT ADMISSION
6 months to < 1 year≥ 1 year
100 000 IU
200 000 IU Single dose on admission
DO NOT GIVE TO CHILDREN WITH OEDEMA
AMOXYCILLIN AT ADMISSION All beneficiaries See protocol 3 times a day for 7
days
MEASLES VACCINATION
AT ADMISSION From 9 months (standard)Single dose on
admission
ALBENDAZOLE SECOND VISIT
< 1 year DO NOT GIVE NONE
12 - 23 months 200 mg (1/2 tablet) Single dose on second visit≥ 2 years 400 mg (1 tablet)
* VITAMIN A: do not give if child has already received within last 3 months
Dosage of Amoxicillin
Weight range Amoxycillin (50 – 100 mg/kg/d)Dosage – twice per day
Kg in mg capsules
<5kg 125 mg * 2 ½ cap.*2
5 – 10 250 mg * 2 1 cap * 2
10 – 20 500 mg * 2 2 cap * 2
20 - 35 750 mg * 2 3 cap * 2
> 35 1000 mg * 2 4 cap * 2
*2 implies that the dosage needs to be taken twice per day

58
Malaria Treatment
Patients with severe acute malnutrition may have an asymptomatic malaria infection. With the new recommendation from WHO that all suspected cases of malaria be confirmed parasitological (using either microspy or with a malaria rapid diagnostic test - RDTs) before administration of antimalarials, the procedure for these children is now the same irrespective of whether they live in an endemic or non-endemic malarial zone.
Endemic malarial zone and Non-endemic malarial zone
All children admitted for SAM should be systematically tested for malaria using either microscopy or RDTs irrespective of the presence or not of symptoms and /or signs of malaria and all positive cases treated with an antimalarial, regardless of clinical signs. If the patient tests negative (especially with RDT) but remains persistently symptomatic for malaria, give full treatment for malaria. This is especially true if fever persists once the patient has started antibiotics.
Treatment dosages are based on weight. Follow the dosages below.
• Give Artesunate (50mg) & Sulphadoxine/Pyrimethamine (500mg/25mg) as a combination on Day 1• Continue with Artesunate (50mg) on Day 2 and 3 as per the schedule below:
ARTESUNATE & SULPHADOXINE/PYRIMETHAMINE
Dose
Weight of child in kgArtesunate
Day1, Day2, Day3SP
Day 1 tablets
< 5 ¼ ¼
5.0 – 7 ½ ½
7.1 – 12 1 ½
12.1 – 20 2 ¾
20.1 – 30 2 1
30.1 – 40 3 1 ½
40.1 – 50 4 2
50.1 – 60 4 2 ½
> 60 5 3

Guideline for Management of Acute Malnutrition
59
Field Card 18. Specific Medication
Additional medication may be prescribed to treat other medical problems as required, following the indications in this table.
Supplemental Medicines for Severe Malnutrition OTP
Name of Product When to Give Prescription Special Instructions
Chloramphenicol
To be given as a second line antibiotic for children
not responding to amoxycillin i.e continued fever that is not due to
malaria
See separate protocol Continue for 7 days
Tetracycline eye ointment
For treatment of eye infection. Systematic
treatment for malnourished children
with measles
Apply 3 times a day, morning, afternoon and
at night before sleep
Wash hands before and after use. Wash
eyes before application. Continue for 2 days after infection has
gone.
Nystatin Drop For treatment of candida
100,000 units (1ml) 4 times a day after food (use dropper and show the carer how to use it)
Continue for 7 days
ParacetamolFor children with fever
over 38.5˚C See separate protocolSingle dose only - DO NOT give to take home
Benzyl Benzoate For treatment of scabies
Apply over whole body. Repeat without bathing on following day. Wash
off 24 hours later
Avoid eye contact. Do NOT use on broken or
secondary infected skin
Whitfields
For treatment of ringworm or other fungal infections
of the skinApply twice a day
Continue treatment until condition has
completely resolved
Gentian Violet
For treatment of minor abrasions of fungal
infections of the skinApply on lesion
Can be repeated at next visit and continued until condition resolved
Ferrous Sulphate & Folic Acid
Treatment for anaemia identified according to
IMCI guidelinesAccording to IMCI
ONLY to be given after 14 days in the
programme (dangerous before and RUTF contains enough)

60
CHLORAMPHENICOL DOSAGES
PARACETAMOL DOSAGES
Use for second line antibiotic for those children who have not responded to amoxycillin
Give 3 times a day for 7 days
SYRUP 125mg/5ml
Weight Dose
2.0 - 6.0 kg 6.25 mg (2.5ml) three time per day
6.0 - 10.0 kg 125 mg (5ml) three time per day
10.0 - 30.0 kg Give capsule
CAPSULES 250mg
Weight Dose
2.0 - 6.0 kg give syrup
6.0 - 10.0 kg 125 mg (1/2 capsule) three time per day
10.0 - 30.0 kg 250 mg (1 capsule) three time per day
NOTE: Always check label on bottles for dosages and dilution of syrups as this can change between different manufacturers
PARACETAMOL 125mg/5ml (syrup)
Weight Dose
<4.0kg 25 mg (1ml) stat
4.0 - 8.0 kg 60 mg (2.5ml) stat
8.0 - 15.0 kg 120 mg (5ml) stat
>15kg 240 mg (10ml) stat
Warning on Paracetamol
Paracetamol can be dangerous in malnourished children because of poor liver function. It should be given only when there is high fever. Combine always with natural methods to reduce fever (damp clothes, tepid sponge) and start as soon as possible antibiotics or antimalarials. Refer the child to SC if possible. Monitor the child carefully. Never give Paracetamol for use at home.

Guideline for Management of Acute Malnutrition
61
Field Card 19. Surveillance / Follow up of patients in OTP
Patients attend the OTP each week or every other week.
The frequency of follow up of the main variables are:
At each visit:• Measurement of oedema.• Measurement of weight.• Measurement of MUAC.• Repeat appetite test in the second and third visits, and again later if the child is not gaining weight.• Check of vital signs (temperature, respiratory rate, etc.)• Medical check and history (stools, vomiting, etc. See FC 5).• Assess evolution of the patient: organise home visit or refer if no evolution.• Receives RUTF.• Update of ration card and OTP card.• Give health education.
Monthly:• Measurement of height / length.• Recalculate W/H.
When necessary:• Measurement of height / length (if you suspect that the child has been substituted for a different child).• An appetite test (unless it is done for every visit). Do a complete medical evaluation and consider transfer to
Inpatient if the patient fails the appetite test and weight is not increasing. Consider a home visit if the child is not gaining weight but his appetite is normal (it could be the consequence of family sharing of RUTF).
• A complete medical examination, if the child presents a condition that requires further investigation. The objective will be: 1) to evaluate if the condition can be treated at the OTP, 2) to evaluate if the child needs transfer to the SC.
The best way not to forget any measurements is to follow the OTP card point by point, from the beginning to the end, at every visit.
Field Card 20. Discharge Criteria from OTP
A child is discharged when he/she reaches the criteria to be declared cured (well nourished), or when the treatment is interrupted for other reasons.
DISCHARGE CRITERIA for OTP
Cured
W/H > -2 Z-scoreMUAC > 125 mmNo oedema For 2 consecutive visits
Default Absent for 3 consecutive visits
Death Died during time registered in OTP
Non-cured Has not reached target weight within 3 months
Transfer to Stabilization Centre* Condition has deteriorated and requires Stabilization Centre/hospital care
*this child is not discharged from the OTP; his card is kept at OTP but the transfer noted on the tallysheet

62
In order to identify the patients that become defaulters or non-cured, you need to check the information in the register and the OTP card.
Most children who die while in OTP treatment, do so at home. As a consequence, they may appear in the statistics as “Defaulters”. If the defaulter tracing finds out that the child had died, you need to correct the reason for discharge in the OTP card and the register book, so that this will be taken into account when calculating statistics.
When the only criteria of admission is MUAC, some agencies impose a minimum of 2 months of treatment before discharge.
Children discharged from OTP should be sent to TSFP for consolidation of their nutrition status and to avoid relapse. When no TSFP is available, advise the mother to bring the child back to the OTP if his/her status deteriorates.
Field Card 21. Failure to respond to OTP treatment. Definition.
Failure to respond to treatment necessitates either further investigation or transfer to SC.
See FC-8 for the full list of complications that represent failure to respond to treatment (the list is the same as for the criteria to be sent directly to SC, plus the addition of the following:
• Failure to gain any weight or weight loss during 3 consecutive weeks of treatment• No improvement in clinical condition.• Increase of oedema and/or no resolution of oedema by 3 weeks. Development of oedema in a child who previously
did not have any.• Child has not reached discharge criteria by month 3.• Development of complicated SAM (Loss of appetite or development of complications in the list)
Do not wait until the end of the third month to take action. Failure to properly respond to treatment should be investigated and dealt with as soon as the child shows any sign of not progressing.
Recovery syndrome
As the immune and inflammatory systems recover, the child may present symptoms of infection or other pathology. This happens when the illness was asymptomatic, and the child only expresses symptoms after nutritional start of recovery. The child may present fever, increased respirations and increased pulse rate. The majority of these conditions can be diagnosed and treated at the OTP. Otherwise refer to Inpatient care. As a general rule, the rehabilitation syndrome presents accompanied with weight gain.It is, in fact, a sign of recovery – rather than a symptom of failure of treatment!
Field Card 22. Failure to respond. Causes and actions.
Problems with the OTP:
Consider this issue when many children present failure to respond at the same time or when there is a low recovery rate.
• Inappropriate selection of patients to go directly to Outpatient care, • Poor assessment of presence of appetite• Inadequate instructions given to mother/carer.• Wrong amounts of RUTF dispensed to children (not enough)• Excessive time between distributions• Poor follow up of evolution of patients - to address problems early enough

Guideline for Management of Acute Malnutrition
63
Actions: Review all procedures of the OTP and organise a supervision visit. Reconsider protocols. Re-calibrate scales and measuring boards. Reassess knowledge of health staff and organise training.
Problems with the individual child:
Social problems:
• Sharing with the family (siblings, parents/carer,..). • Child eating too much of family food instead of the RUTF.• Sibling rivalry (other children taking the diet).• Unwilling carer.• Carer overwhelmed with other work and responsibilities.• Important change in home circumstances.• Administration of traditional medicine.
Actions: In depth interview with the carer to investigate possible causes. If necessary, complete with a home visit. Education at the centre and during the home visit. Feed back to nurse on the possible cause of failure to respond.
Medical problems:
• Specific vitamin or mineral deficiency.• Malabsorption of nutrients.• Psychological trauma / Deficient mother-child bounding.• Infections, especially: diarrhoea, dysentery, pneumonia, tuberculosis, urinary infection, otitis media, malaria,
schistosomiasis / leishmaniasis, hepatitis / cirrhosis.
Actions: Complete medical history and detailed examination. Treat possible causes. Refer to Inpatient care. This will be necessary for most patients with medical failure to respond.
While investigating the causes for failure to respond, ask the carer to explain in detail how she gives the RUTF to the child at home, or ask her to do it in front of you. An appetite test may orient you to the type of problem: if the child who is not responding to treatment has appetite, it is more likely that the problem is social; if the child has no appetite, consider first medical causes. Always be polite and respectful of the carer’s response.
Field Card 23. Transfer to SC. Criteria and procedure.
A child presenting failure to respond to treatment, or any complication in Field Card – 8, should be transferred to the SC.
When transferring the child, always do the following:
• Write a transfer form (Chapter 12), with details of the evolution of the child, medication given and reason for transfer,
• Give the child sugared water, and• Discuss with the carer how they are going to proceed to the SC – assess if it is realistic that they will arrive
to the SC, taking into account the severity and urgency of the condition of the child. In some instances, the only option for you may be to arrange transport for the transfer.

64
Complicated SAM in the OTP
All cases of complicated severe acute malnutrition should be treated as inpatients in Stabilisation Centres (SC). Currently, there are many OTPs in Somalia that cannot refer patients to SC, due to distance, insecurity lack of programmes or other factors (see Introduction).
Two actions are necessary at the planning level:• to consider the implementation of SC in the area, and• to increase community mobilisation and ensure maximum early diagnosis, so that the proportion of children with
complicated SAM that arrive to the centre are reduced.
An OTP that cannot refer children to SC should give very high priority to active screening and early diagnosis – with most of its resources geared towards it.
Despite these efforts, there will be children with complicated SAM that arrive to the OTP.
What to do?
There is little that can be done to adapt the protocols for these patients: The types of drugs that are used in the field cannot be adapted to this circumstance, as this would generate problems. In particular, most facilities where OTP is implemented cannot use IV medication.
Explain to the carer that her child has medical complications and needs more advanced care. Explore with her the possibility of transfer. If this is totally not possible, spend extra time with her to explain all the details of the treatment at home and be sure that she understands the treatment and the risks involved. Ask her to refer to the clinic if the child’s status worsens.
Ask the community mobilisation team to prioritize this family for home visits, and visit them several times during the week if possible. Ask them to report the evolution of the child to the OTP nurse and reconsider transfer to SC if that is an option.
Ensure that the antibiotic treatment is being taken correctly. Use second line antibiotics if the first line does not work in one week. If necessary and possible, ask the mother to come every day (only for those that do not live far from the centre), to observe the feeding and to take the antibiotic.
Rehydration should always be done with safe clean water. Do not use ReSoMal or ORS in the OTPs, as the diagnosis of dehydration must be done by an expert and there is an important risk of complications. These children usually have an excess of sodium in their body, which makes it more medically advisable to give them plain water than to give ORS or even ReSoMal, particularly if there are no means to supervise intake or signs of potential fluid overload.
Reporting Complicated-SAM at the OTP:
Monitor the proportion of complicated to non-complicated SAM that arrives to the centre, as an indicator of the quality of early diagnosis (and community mobilisation). Additionally, this will give an indication of how well the community is identifying SAM and what is the importance of the problem of non-referral in the area.Attention! There may be an increase in complicated cases as a consequence of increased mobilisation.

Guideline for Management of Acute Malnutrition
65
Section 6Inpatient care
Management of complicated SAM in Children 6 to 59 months

66
Overview
Most cases of severe acute malnutrition (SAM) do not need to be admitted to a hospital ward in order to follow treatment and recover. They can be treated at the OTP and follow the treatment from home. However, those cases that present complicated SAM, and in particular anorexia, need to be admitted in order to stabilise their metabolism and treat the complications. After this has been accomplished (in average one week), they can continue treatment at the OTP.
Complicated severe acute malnutrition is a life-threatening condition. These patients are very fragile, often with a serious electrolyte imbalance. They do not always present with the typical symptoms of an illness (e.g. fever, rapid pulse or rapid respirations). Also, it can be very difficult to diagnose dehydration or anaemia however it is extremely important to do so accurately. A misdiagnosis can lead to a high risk of mortality (see Management of SAM complications).
The child with complicated SAM does not usually present the same symptoms and signs of complications that other children do. They react differently to the same inputs: for example, an IV infusion that may be life saving for a well-nourished child could be lethal for a child with SAM. For this reason, these children should ONLY be treated by health staff that have been specifically trained to diagnose and treat severe acute malnutrition. This includes assistants, nurses and doctors. When admitted to the hospital, children with severe acute malnutrition should not be attended in the emergency ward or casualty department for the first 24 – 48 hours, as the staff in these departments are usually not familiar with the management of SAM – and a wrong decision taken during this period could be fatal.
Despite these complexities, the correct application of the protocols presented in this section results in the recovery of the child in the majority of cases. The use of specialised therapeutic foods (ex. F75) in combination with antibiotics and the use of appropriate differential diagnosis and treatment that is adapted to the condition of severe acute malnutrition, have shown that mortality in the SC may be as low as 5 % when these protocols are respected by dedicated and careful medical staff.
The management of severe acute malnutrition in the inpatient setting is divided into three phases:
• Phase 1 covers nutrition and medical stabilization, treatment of medical complications, and commences nutritional rehabilitation.
• Transition Phase covers a gradual increase in diet leading to some weight gain while preventing complications of over-feeding.
• Phase 2 is a rapid weight-gain phase (catch-up growth). It is most often implemented at the OTP but can be done at the in-patient facility under some circumstances.
The inpatient treatment of acute malnutrition can be done in a section of the paediatric ward, but it is preferable to do it in a separate ward to avoid cross-infection with other children and allow total dedication of medical staff. The facility can offer 24 h care, or work as a daycare (ex. from 6am to 9pm). In the last case, the patients and their carers can return home or stay in the ward overnight, although no specific care is offered during the night.
Phase 1: Nutrition and Medical Stabilization
Patients without an adequate appetite and/or a major medical complication are initially admitted to an in-patient facility for Phase 1 treatment.
The formula used during this phase (F75) promotes recovery of normal metabolic function and nutrition-electrolytic balance. In Phase 1, the patient receives F75 formula at 100kcal/kg/day. Rapid weight gain at in Phase 1 is dangerous, and that is why the quantities and formula are formulated so that patients do not gain weight during this stage.
A routine systematic medical treatment is commenced in Phase 1, and medical complications are treated. It is important in Phase 1 that oedema, if present, reduces. When oedema is reduced from +++ to ++, only then can these patients graduate from Phase 1 to Transition Phase. Patients who initially require intravenous (IV) therapy or

Guideline for Management of Acute Malnutrition
67
naso-gastric (NG) feeding must have completed these therapies before transfer to Transition Phase.The patient remains in Phase 1 until the medical complications stabilize, appetite improves, and the patient completes the designated quantity of F75 or equivalent diet at each mealtime.
Phase 1 treatment is always given in an inpatient setting for children with complicated SAM. This phase of the treatment is intended to:
a. Stabilise patients with complicationsb. Restore metabolic functionsc. Prevent and/or treat associated conditions and complications and,d. Intensively monitor patients
Transition Phase: Increase Diet and Prevent Complications
Patients normally remain in Transition Phase for two to three days. This phase is designed to slowly increase the diet and prevent complications of over-feeding. F75 is replaced with F100 or a locally made-up milk of the equivalent nutritional value. The patient’s diet is increased from 100kcal/kg/day to 130kcal/kg/day for children. The quantity of milk remains the same, but the calorie content changes by changing milk formulas from 75kcal to 100kcal per 100ml of milk.
The patient in Transition Phase receives around 30% more calories than when in Phase 1. Daily weight gain can be expected at about 6g/kg/day. For patients qualified and willing to be discharged from Transition Phase to Outpatient Therapeutic Care for the remainder of nutrition treatment, the equivalent calories are given to the patient in the form of Ready-to-Use-Therapeutic Food (RUTF).
Phase 2: Catch-up Growth and Discharge
Patients move from Transition Phase into Phase 2 when they have a good appetite; are tolerating the diet given; have no major medical complications; and oedema is resolved. The objective is to achieve catch-up growth and resolve micronutrient deficiencies. In Phase 2, the patient receives F100 at 200kcal/kg/day or the equivalent in the form of RUTF. These formulas are designed for patients to rapidly gain weight (more than 8g/kg/day). Recovered patients are discharged for supplementary feeding if available at the nearest health facility.
Staff Roles:
The mother is the primary carer. She is the one actually giving the feeds to the child, as well supervising any changes in the child’s condition as instructed by the nurses.
Auxiliary or Nurse aide do most of the actual “nursing”. They weight, measure, mix and dispense feeds, give the oral drugs, assess the clinical signs and fill the patient’s chart with all the routine information.
The nurse functions as a teacher and supervisor of the assistants to ensure that they are performing these functions correctly and accurately. The nurses also need to give or supervise any intravenous or unusual treatment.
The doctor’s main duty is to support the nurses and to concentrate on any patients that fail to respond to treatment or present diagnostic difficulty. This role can be effectively done by the Senior Nurse in most SC.
Staff turnover should be minimised and any new staff must be specifically trained in the management of SAM and work for a period under supervision before they are allowed to take charge and work alone or at night with these patients. This recommendation affects doctors in particular as they are more likely to take the most important decisions.

68
Admission Criteria for Inpatient Care
See FC 7 for a complete explanation on how to identify Complicated – SAM and admission criteria to SC.
In order to be admitted to SC, the child needs to present Severe Acute Malnutrition (SAM), as identified by W/H, MUAC or bilateral oedema, AND at least one complication and/or lack of appetite (measured through the appetite test).
SC
SAM with complications
W/H (z-score) < -3
MUAC (mm) < 115
OedemaBilateral oedema +++
Marasmus with any oedema
Appetite NO APPETITE
Complications
Uncontrollable vomiting
Fever > 39˚C
Hypothermia <35˚C
Lower respiratory tract infection
Severe anaemia
Extensive skin infection
Very weak, apathetic
Unconscious, convulsions
Other Child referred from OTP due to complications or
lack of weight gain
Choice of the carer
New
adm
issi
ons
Discharge criteria:
Children admitted to SC (Phase 1) are usually sent to OTP to complete treatment, after moving through Transition Phase. See next page for criteria for being promoted to OTP.
In the exceptional cases that a child needs to stay in Phase 2, the discharge criteria are the same as for OTP (see FC 20). In this case, the child is sent to TSFP, if possible.

Guideline for Management of Acute Malnutrition
69
Field Card 24. SC - Promotion between phases
The patient must meet the following criteria to transfer from Phase 1 to Transition Phase and from Transition to OTP or Phase 2:
All patients are sent to OTP to complete treatment. If the patient is from an area with no OTP services, or if he/she presents a chronic complication (ex. tuberculosis, clef palate) he/she may stay in Phase 2 at the hospital.
Criteria of return to Phase 1
Some patients develop complications when promoted from one phase to the next, usually related to fluid retention or development of new complications. This can happen in Transition phase and during the first week of Phase 2. These patients need to re-start the treatment in Phase 1.
Criteria From Ph1 to Transition Phase From Transition Phase to OTP/Ph2
Appetite and intake Appetite improved. Child taking all quantity of milk prescribed
Appetite is good.Child is taking at least 75 % of RUTF or all F100 prescribed
Oedema (if present) Reduced to moderate++ Reduced to low +Absent, if patient stays in Ph2
Medical complications Treatment has commenced and patient is recovering
All medical complications must be resolved, treatment completed
IV fluids and NG feeding They are not needed any more IV or NG feeding
Criteria From Transition Phase or Ph2 to Ph1
Appetite and intake Patient presents anorexia or cannot complete meals
Oedema (if present) Increase of oedemaChild without oedema that develops it during treatment
Medical complications Child develops any of the medical complications in FC-8, and in particular:reduced consciousness (ex. hypoglycaemia), hypothermia, hyperthermia, acute vomiting, as well as dehydration or septic shock
Fluid overload Signs of rapid increase in liver sizeDevelopment of tense abdominal distensionWeight gain is too fast >10g/kg/d (fluid retention)Any signs of heart failure: increased respiratory rate, crepitants, ...Other signs of fluid overload: increased venous pressure, new oedema...
Other complications Re-feeding diarrhoea WITH weight loss (if child gains weight, continue treatment).
IV fluids and NG feeding Any condition that needs IV or NG tube
Some of the conditions that result in return to Phase 1 need specific treatment. See chapter 8 “treatment of complications” for advice. It is common for some change in stool frequency when there is a change in diet. This does not need to be treated unless the child loses weight. Several loose stools without weight loss are not a criterion to move back to Phase 1.

70
Nutritional Treatment
Phase 1 (Stabilisation):
Nutritional treatment in Phase 1 is given through a F75 therapeutic milk diet only.
The quantity of milk a child needs to receive in phase one is equivalent to 130ml/kg/day.
For older children and adults, the quantity of milk per kg of body weight is different than for children younger than five years. If you are treating children above 5 years or adults, please refer to international guidelines for the amounts to give per kg of body weight.
The milk diet is given at regular intervals throughout the day (approximately every two to three hours). The quantity required for each 24 hour period is determined by the child’s weight. To determine the amount per feed, divide the 24-hour required quantity by the number of feeds per day. Give 6 meals per day (ex. every three hours from 6am to 9pm). If conditions allow feeding overnight (i.e. enough and well trained staff and possibility to prepare milk at night) then you can divide the intake in 8 meals (every 3 hours), see FC-25 for the appropriate amounts.
Special situations:
In rare cases where a child has severe vomiting or refuses adequate diet quantities, it may be necessary to give the diet continuously by NG tube. Occasionally, a patient may have osmotic diarrhoea and may require more frequent feeds (feed every two to three hours, and overnight).
For severely malnourished patients with severe oedema (+++), reduce the quantity of F75 by up to 20% until the oedema begins to subside.
Breastfed children from 6 months up to 24 months should always be offered breast milk before the therapeutic milk, and always on demand.
Transition Phase: Nutrition Support: Diet and Frequency
The ONLY change in the diet when transferring from Phase 1 to Transition Phase is that F75 is replaced by either F100 or RUTF. In some situations, the child can receive one product or the other at alternate meal times (for example, RUTF during the night and F100 during the day, or you can alternate the product given in each meal).
The number of feeds, the timing, and the volume of the diet remains exactly the same in Transition Phase as in Phase 1 (130ml/kg/day). The child is fed 6 times per day, usually between 6am and 9 pm.
Ideally, in transition phase there should be a progressive increase in the amount of feed perscribed. A slow progression is particularly important for children that have a tendency to develop cardiac overload, or that have already developed it during treatment.
If RUTF is given, you need to explain its use to the mother, following the indications in FC 16. When on RUTF, the child should be given as much safe water as possible, to ensure good absorption and child’s hydration.
If the child is going to be discharged to the OTP the child should receive RUTF during Transition phase, so that he/she starts getting used to it. In some occasions, RUTF can be alternated with F100 (ex. F100 during the day and RUTF during the evening, the weekends or when there is not enough staff). If both F100 and RUTF are given, they can be substituted on the basis that about 100ml of F100 is equivalent to 20g of RUTF.

Guideline for Management of Acute Malnutrition
71
Some patients initially refuse the RUTF. In this case, give the F100 diet for one or two days and then reintroduce the RUTF. Other children prefer the RUTF. It is good practice to give the diet that the children prefer. Particularly small or weak children (those between 6 months and 1 year) usually prefer a milk diet.
As in Phase 1, the breastfeeding children should always be breastfed before taking F100 or RUTF, and on demand. This is because human breast-milk is better than any product. If the child takes the products first then he/she will not be hungry enough to demand the breast, and if the mother does not breastfeed then breast-milk production will stop. Giving the breast first ensures that breastfeeding is maintained despite the treatment, and can be continued at home.
Phase 2: Nutrition Support: Diet and Frequency
Most children will move directly from Transition phase to the OTP. Only a few will complete Phase 2 at the inpatient setting. For example, when the child lives in an area where there are no OTP services, if the child presents a chronic condition that requires him/her to stay in the hospital (i.e. tuberculosis, HIV, Kala-azar), or if there are other social circumstances that makes it advisable for the child to stay (ex. non-accompanied children).
The objective of Phase 2 is to achieve weight gain and promote growth. Phase 2 inpatient care can be managed using F100 or RUTF (see tables).
In Phase 2 the main change in the diet is an increase in the amount of F100 or made-up milk formulas. The volume of milk is increased from 130ml/kg/day to 200ml/kg/day (equivalent to 200kcal/kg/day). If the child remains hungry after completing a feed, more milk can be offered. This is usually given in 6 meals per day.
One porridge meal may be given to patients who weigh more than 8kg (approximately 24 months of age); it is not necessary to give porridge unless the patient asks for it.
In general, RUTF is preferred to F100, even at the hospital level because it does not need preparation. However, weak children and those that have mild disease may prefer F100. Always respect the preference of the child.
Never give F100 to be used at home, only use RUTF.

72
Field Card 25. Quantity of milk and RUTF in SC
Quantity of Therapeutic milk and RUTF to give in each phase of treatment, according to child’s weight.
Phase 1F75
Transition PhaseF100
Transition Phase
Plumpy’nut
Phase 2F100
Class of Weight (kg)
8 feeds per day
6 feeds per day
8 feeds per day
6 feeds per day
6 feeds per day
6 feeds per day
ml per feed ml per feedsachets per
dayml per feed
2 - 2.1 40 50
F100 diluted F100 diluted F100 diluted F100 diluted2.2 - 2.4 45 60
2.5 - 2.4 50 65
2.8 - 2.9 55 70
3.0 - 3.4 60 75 60 75 1 ¼ 110
3.5 - 3.9 65 80 65 80
1 ½
120
4.0 - 4.4 70 85 70 85150
4.5 - 4.9 80 95 80 95
5.0 - 5.4 90 110 90 110
2180
5.5 - 5.9 100 120 100 120
6.0 - 6.9 110 140 110 140 210
7.0 - 7.9 125 160 125 160
3
240
8.0 - 8.9 140 180 140 180 270
9.0 - 9.9 155 190 155 190 300
10 - 10.9 170 200 170 200
4
35011 - 11.9 190 230 190 230
12 - 12.9 205 250 205 250450
13 - 13.9 230 275 230 275
14 - 14.9 250 290 250 290
15 - 19.9 260 300 260 300 5 550
20 - 24.9 290 320 290 3206
650
25 - 29.9 300 350 300 350 750
30 - 39.9 320 370 320 370 7 850
40 -60 350 400 350 400 8 1000

Guideline for Management of Acute Malnutrition
73
Field Card 26. Preparation of F75 and F100
Prepare enough milk for the next three hours, not longer, to assure that it will not spoil.
If five or less children are being treated for severe acute malnutrition, smaller quantities of milk are necessary. In this case, prepare small amounts by using the red scoop that comes with the package.
1. Decide on the amount of milk to prepare, by adding how much each child needs for the meal.2. Boil the water.3. Let the water cool down.4. Add the milk powder WHILE THE WATER IS STILL WARM following this table:
Product Water quantities Product quantities
F75
Large packet of F75 (410 g) 2 litres of water 2.4 litres of F75
1 scoop (4.1 g) 20 ml of water 24 ml of F75
F100
Packet of F100 (456 g) 2 litres of water 2.4 litres of F100
1 scoop (4.1 g) 18 ml of water 22 ml of F100
• Mix• Distribute to each child according to the amount needed for that meal.
Field Card 27. Feeding Technique
Never force-feed a malnourished child and also ensure that the mothers do not force-feed their children. This can distress the child and can lead to aspiration pneumonia. Teach the mother how to sit the child in her lap, with an arm behind the child’s back and the child sitting straight (vertical), and how to offer the cup with the other hand.
All feeds should be controlled by a feeding assistant. The mother or carer must be actively involved in the feeding and the daily care of the child. They should be informed and sensitized to the importance of not introducing other foods until the child is stabilised. Feeding is carried out with a cup (never from a bottle or with a spoon). Feeding assistants should alert carers to the signs of acute danger so that they can call a nurse when necessary (see section on complications).
The following information lessens the risk of aspiration pneumonia.
The child sits straight up (vertical) on the mother’s lap, leaning against her chest with one arm behind her back. The mother’s arm encircles the child. She holds a saucer under the child’s chin.
74
• The milk feed is given by cup. Any dribbles that fall into the saucer are returned to the cup.• The child is never force fed, never has his/her nose pinched, and never lies back and has the milk poured into
the mouth.• Meal times are best to be social. The mothers can sit together in a semi-circle around an assistant who encourages
the mothers, talks to them, corrects any faulty feeding technique, and observes how the children are taking the milk.
• Carers do not take their meals beside the patient. The child is likely to demand some of the mother’s meal and this sharing is not recommended as the child’s appetite will reduce and then the milk will be refused.
Naso-gastric Feeding
Naso-Gastric (NG) tube feeding is required only when a patient is not taking a sufficient diet orally, which is less than 75% of the prescribed diet per day . NG tube feeding is required when one or more of the following is true:• The patient takes less than 75% of the prescribed diet per 24 hours in Phase 1• The patient presents with pneumonia with a rapid respiration rate• The patient has painful lesions of the mouth• The patient has a cleft palate or other physical deformity• The patient is experiencing disturbances of consciousness
IMPORTANT: Each day, try patiently to give the patient F75 by mouth before using the NG tube. NG tube feeding should not exceed three days, and is only used in Phase 1.
Field Card 28. Routine Medicines in SC (to be used with FC 17 and FC 29)
See FC 17 for a complete explanation of Routine medicines given to children on admission to OTP or SC. This page only reflects what is different in SC.
Phase 1.
Vitamin A: As in OTP.Measles vaccination: As in OTP.Malaria treatment: As in OTP.Folic acid: As in OTP.Other Nutrients: As in OTP.
Systemic antibiotics: See next page.
Transition Phase:
Routine antibiotic therapy should be continued for four days after Phase 1 or until the patient is transferred to OTP or Phase 2. This is to ensure that any infection is treated. Patients arriving to OTP after the SC do not need to be given antibiotics again. Their transfer slip should clearly indicate what systematic treatment they received at the SC.
Phase 2.
Iron
For inpatients receiving entire treatment of acute malnutrition in the inpatient health facility: Add iron to the F100 in Phase 2. RUTF already contains the necessary iron.
Iron is added to the F100 diet:

Guideline for Management of Acute Malnutrition
75
Crush an iron tablet and add to 4mls of water and mix well (Iron Solution).• For one sachet of F100 (makes 2.4 litres of F100), add one (1) crushed tablet of ferrous sulphate (200mg) in
the 4mls of water (Iron Solution).• For half a sachet of milk (1200ml of F100), add 2mls of the iron solution.• For 600ml of F100, add 1ml of the iron solution.
If severe anaemia is identified, see “Treatment of Medical Complications”.
De-worming
De-worming is necessary for malnourished children being treated as inpatients, but should be delayed until they are recovering in Phase 2 or discharged to OTP.
Use Albendazole as in OTP, with the same dosages (see FC 17).
Field Card 29. Systematic Antibiotics in SC
All severe acute malnourished children receive antibiotic treatment upon admission, regardless of if they have clinical signs and symptoms of systemic infection or not. Nearly all these children have infections even if they are not symptomatic.
Small bowel bacterial over-growth occurs in all SAM children. Enteric bacteria are frequently the source of systemic infection by translocation across the bowel wall. This can also cause mal-absorption of nutrients and failure to eliminate the substances excreted in the bile, fatty liver, intestinal damage, and can cause chronic diarrhoea. The antibiotic administered for routine treatment must be active against small bowel bacterial overgrowth.
Children with Kwashiorkor have free iron in their blood: this can lead to bacteria that are not normally invasive, such as Staphylococcus epidermidis, and “exotic bacteria” to cause systemic infection or septicaemia.
Antibiotic Regime
First line antibiotic treatment:
Oral Amoxycillin. (If not available, doctor to decide appropriate alternative). See FC 17.
Second line antibiotic treatment:• Add Chloramphenicol (FC 18) (do not stop Amoxycillin) OR• Add Gentamycin 5 mg/kg IM daily (do not stop Amoxycillin) OR• Switch to Amoxycillin/clavulinic acid (Augmentin®).
In inpatient settings where severe infection is common, this may sometimes be considered as the first line antibiotic combination.
Third line antibiotic treatment:Third line treatment is at the discretion of the medical doctor and is dependent on each patient’s medical condition or complication. Frequently, a systemic anti-fungal (fluconazole) is added for patients who have signs of severe sepsis or systemic candidiasis.
Important note: Co-trimoxazole is not active against small bowel bacterial overgrowth and is not adequate for the severely malnourished child. If Co-trimoxazole is administered as a prophylaxis against pneumocystis pneumonia in HIV-positive patients, the above recommended antibiotics should be administered in addition.

76
Duration of Antibiotic Treatment:
Antibiotics are administered every day of Phase 1 plus an additional four days or until transfer to OTP or Phase 2.Whenever possible, antibiotics should be given orally or by NG tube. No CANULA PLEASE.
IV antibiotics should not be used with intravenous infusion because of the danger of fluid overload. Venous access point are often colonised by resistant organisms and may give rise to bacteraemia or even systemic fungal infection. Infusions containing antibiotics should not be used because of the danger of inducing heart failure. Indwelling cannula should rarely be used. Additionally, never give intravenous infusions of quinine to a severely malnourished patient in the first two weeks of treatment. Impregnated bed nets should always be used in malaria endemic regions.
Field Card 30. Patient Follow Up in SC
See Chapter 12 for examples of patients’ cards.Use the patient card as a guide for the information that needs to be collected and as a guide for your consultation and decision making. All fields in the chart have a purpose and should be filled by the nurses or the doctor visiting the patient.
Phase 1 and Transition phase:Obtain the following information and record it in the chart...
Each day (in the morning):• Weight. Plot weight on the chart.• Oedema (0, +, ++, +++).• Body temperature (twice a day).• Key clinical sings (stools, vomiting, dehydration, cough, respiration, etc.)• Record patient’s feeds and fluid intake: record if the patient takes each feed, or if the patient refuses, vomits or
is absent during the meal. Once a week: measure MUAC.On admission and after 21 days (if the child is still in the centre): measure length / height.
Phase 2:Patient surveillance in Phase 2 is less intensive and less frequent than during Phase 1 and Transition Phase. However, it is important to routinely monitor progress.
Each day (in the morning):• Body temperature (twice a day).• Key clinical sings (stools, vomiting, dehydration, cough, respiration, etc.)• Record patient’s feeds and fluid intake: record if the patient takes each feed, or if the patient refuses, vomits or
is absent during the meal. Every other day:• Weight. Plot weight on the chart.• Oedema (0, +, ++, +++).Once a week: measure MUAC.Every month: measure length / height.
IMPORTANTDuring Phase 1, you should not expect any increase in weight. The amount of energy given is not enough to promote weight gain. If the child gains weight during this phase, suspect fluid retention and be careful with further treatment and fluid overload. It is more frequent to observe weight loss, due to elimination of fluid retained inside the cells.
During Transition Phase some weight gain is expected (around 6 g/kg/d), if there is no malabsorption and if the patient is not loosing oedema. Once the patient is in Phase 2, expect rapid weight gain (up to 20 g/kg/d).

Guideline for Management of Acute Malnutrition
Section 7Management of Acute Malnutrition in Infants
77
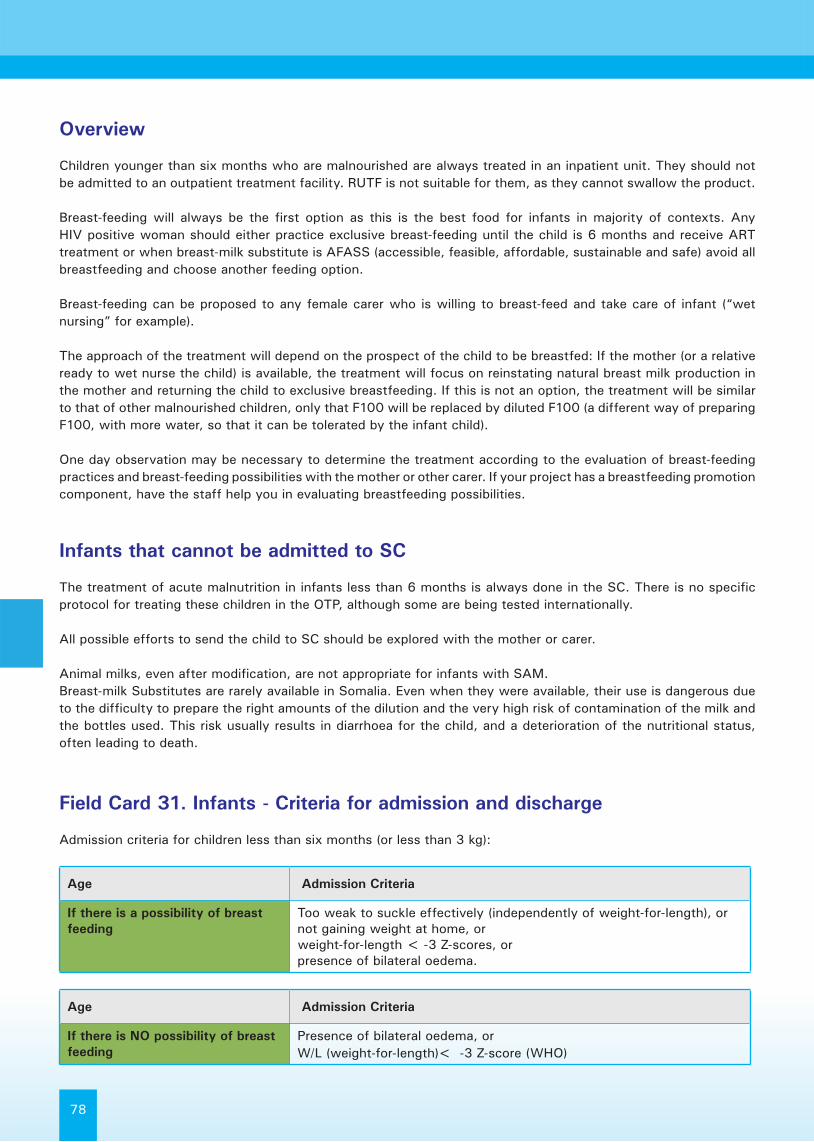
78
Overview
Children younger than six months who are malnourished are always treated in an inpatient unit. They should not be admitted to an outpatient treatment facility. RUTF is not suitable for them, as they cannot swallow the product.
Breast-feeding will always be the first option as this is the best food for infants in majority of contexts. Any HIV positive woman should either practice exclusive breast-feeding until the child is 6 months and receive ART treatment or when breast-milk substitute is AFASS (accessible, feasible, affordable, sustainable and safe) avoid all breastfeeding and choose another feeding option.
Breast-feeding can be proposed to any female carer who is willing to breast-feed and take care of infant (“wet nursing” for example).
The approach of the treatment will depend on the prospect of the child to be breastfed: If the mother (or a relative ready to wet nurse the child) is available, the treatment will focus on reinstating natural breast milk production in the mother and returning the child to exclusive breastfeeding. If this is not an option, the treatment will be similar to that of other malnourished children, only that F100 will be replaced by diluted F100 (a different way of preparing F100, with more water, so that it can be tolerated by the infant child).
One day observation may be necessary to determine the treatment according to the evaluation of breast-feeding practices and breast-feeding possibilities with the mother or other carer. If your project has a breastfeeding promotion component, have the staff help you in evaluating breastfeeding possibilities.
Infants that cannot be admitted to SC
The treatment of acute malnutrition in infants less than 6 months is always done in the SC. There is no specific protocol for treating these children in the OTP, although some are being tested internationally.
All possible efforts to send the child to SC should be explored with the mother or carer.
Animal milks, even after modification, are not appropriate for infants with SAM.Breast-milk Substitutes are rarely available in Somalia. Even when they were available, their use is dangerous due to the difficulty to prepare the right amounts of the dilution and the very high risk of contamination of the milk and the bottles used. This risk usually results in diarrhoea for the child, and a deterioration of the nutritional status, often leading to death.
Field Card 31. Infants - Criteria for admission and discharge
Admission criteria for children less than six months (or less than 3 kg):
Age Admission Criteria
If there is a possibility of breast feeding
Too weak to suckle effectively (independently of weight-for-length), ornot gaining weight at home, orweight-for-length < -3 Z-scores, orpresence of bilateral oedema.
Age Admission Criteria
If there is NO possibility of breast feeding
Presence of bilateral oedema, or W/L (weight-for-length)< -3 Z-score (WHO)

Guideline for Management of Acute Malnutrition
79
Age Admission Criteria
If the child is breast feeding • Child is gaining weight on breast-milk alone after the Supplementary Suckling technique has been stopped, and
• There is no medical problem, and• The mother has been adequately supplemented with vitamins and
minerals. (there are no anthropometric criteria for discharge)
Age Admission Criteria
If the child is not breast feeding • The mother has been adequately supplemented with vitamins and minerals, and
• When they reach -1 Z-Score, and• An appropriate breast-milk substitute for the child is defined
considering the family’s possibilities and is sustainable, and• Child is used to milk substitute, gaining weight and carer education
on preparing and dispensing the milk substitute is done.
Discharge Criteria for children less than six months (or less than 3 kg):
Infants Less Than Six Months with a Prospect of Being Breastfed
Infants who are malnourished are weak and do not suckle strongly enough to stimulate adequate production of breast milk. The mother often thinks that she herself has insufficient milk and is apprehensive about her ability to adequately feed her child. The low output of milk is due to inadequate stimulation by the feeble infant. Breast milk supply is demand-led, the more the baby breastfeeds, the more breast-milk the mother will produce.
The objective of treatment of these patients is to return them to full exclusive breastfeeding.
Nutrition Support: Diet, Frequency and Suckling TechniqueThe objective is to supplement the child with therapeutic milk (F100-diluted) while stimulating production of breast milk until it is sufficient enough alone to allow the child to grow properly. This is achieved through the supplementary suckling (SS) technique (see FC 33). If the infant presents with oedema, start treatment with F75 instead of F100 diluted. After resolution of oedema, change to F100 diluted.
There are no separate phases in the treatment of infants with the SS technique. There is no need to start with F75 and then switch to F100 Diluted unless the infant has severe oedema. NEVER use normal F100 with an infant!
Infants should be nursed in a separate space from the older malnourished children. This can be in a “breast feeding corner”. It is important not to admit infants into the inpatient facility where the severely complicated cases are admitted. It is important that these infants are not put at high risk of cross infection from older sick children.
Routine Medication
Folic acid: 2.5mg (1/2 tab) in one single dose
Ferrous sulphate: when the child suckles well and starts to gain weight, start adding iron to the milk. The easiest way is to add iron to normal F100, following explanations for older children, and then dilute it with 1/3 water to obtain the correct dilution.
Antibiotics: First line: Amoxycillin (from 2kg): 30mg/kg two (2) times a day (60mg/day).

80
Second line if required: Gentamycin for severe infections (do not use Chloramphenicol in young infants).SurveillanceSurveillance is the same as for other patients in Phase 1 (see FC 30).
Follow-Up after dischargeThe follow-up for these children is very important. The mother should be enrolled for a supplementary feeding programme if it exists and receive a high quality food ration to improve the quantity and quality of breast milk. It is also important to monitor the infant’s progress, support exclusive breast feeding and inform the mother on when to introduce appropriate complementary food at the age of six months.
Field Card 32. F100 diluted – preparation and distribution
Preparation of F100 Diluted
Dilute F100 (one packet) into 2.7l litres of water (instead of 2 litres) to make F100 Diluted.
To make small quantities of F100 Diluted:1. Use 100ml of F100 already prepared and add 35ml of water, then you will get 135ml of F100 diluted. Discard
any excess waste. Don’t make smaller quantities.2. If you need more than 135ml, use 200ml of F100 and add 70ml of water, to make 270ml of F100 diluted and
discard any excess waste.
If F100 Diluted is not readily available, the infant can be fed with the same quantities of commercial infant formula, diluted according to the instructions on the tin. However, infant formula is not designed to promote rapid catch up growth. Unmodified powdered whole milk should not be used.
Quantity of F100 Diluted and Timing of Feeds
It is important to feed these children often as they are small and will only take small quantities. The quantity of F100 diluted to give to a malnourished infant is calculated depending on the body weight. As opposed to the older children, the quantity is NOT increased as the infant starts to gain weight.1. Breast feed every three hours for at least 20 minutes (more if the child cries or demands more)2. Between 30 minutes and one hour after a normal breast feed, give maintenance amounts of F100-diluted using
the SS technique.3. F100-diluted is given at 130 ml/kg/day, distributed in 8 meals.4. If the child has oedema, use F75 instead of diluted F100.
Quantity of F100 Diluted to give to infants with a prospect of being breastfed, per Kg of body weight:
Class of Weight (kg)ml of F100 diluted per feed
(8 feeds/day)Diluted F100
<=1.2 25 ml per feed
1.3 - 1.5 30
1.6 – 1.7 35
1.8 – 2.1 40
2.2 - 2.4 45
2.5 - 2.7 50
2.8 – 2.9 55
3.0 - 3.4 60
3.5 – 3.9 65
4.0 – 4.4 70

Guideline for Management of Acute Malnutrition
81
Field Card 33. Supplementary Suckling Technique
The supplementation is given using a tube the same size as n°8 NG tube. Cut the tip of the NG tube back beyond the side ports on the tube, if these ports exist
• F100 Diluted or formula milk is put in a cup. The mother holds it.• The end of the tube is put in the cup.• The tip of the tube is put on the breast at the nipple and the infant is offered the breast in the normal way so that
the infant attaches properly. This way the infant will both get milk from the cup and at the same time stimulate the breast and the mother’s milk production. Sometimes at the beginning the mothers find it better to attach the tube to the breast with a piece of tape.
• When the infant suckles on the breast with the tube in his mouth, the milk from the cup is sucked up through the tube and taken by the infant. It is like taking a drink through a straw.
• At first an assistant needs to help the mother by holding the cup and the tube in place. She encourages the mother confidently. Later the mother nearly always manages to hold the cup and tube without assistance.
• At first, the cup should be placed at about 5 to 10cm below the level of the nipple so the milk does not flow too quickly and distress the infant, and so the weak infant does not have to suckle excessively to take the milk. As the infant becomes stronger the cup should be lowered progressively to about 30cm below the breast.
• The mother holds the tube at the breast with one hand and uses the other for holding the cup.
Notes
• It may take one or two days for the infant to get used of the tube and the taste of the mixture of milks (F100 diluted and breastmilk), but it is important to persevere.
• By far the best person to show the mother the technique is another mother who is using the technique successfully. Once one mother is using the SS technique successfully the other mothers find it quite easy to copy her.
• The mother should be relaxed. Excessive or officious instructions about the correct positioning or attachment positions often inhibit the mother and make her think the technique is much more difficult than it is. Any way in which the mother is comfortable and finds that the technique works is satisfactory.
• If the formula diet is changed then the infant normally takes a few days to become used to the new taste. It is preferable to continue with the same supplementary diet throughout the treatment.
Cleaning the tube
After feeding is completed the tube is flushed through with clean water using a syringe. It is then spun (twirled) rapidly to remove the water in the lumen of the tube by centrifugal force. If convenient, the tube is then left exposed to direct sunlight. For optimal hygiene replace tubes often.

82
Regulating Quantity of F100 Diluted
The child’s progress is monitored by his/her daily weight:
• If the child loses weight over three consecutive days yet seems hungry and is taking all the F100 Diluted, add 5mls to each feed.
• In general the supplementation is not increased during the stay in the centre. If the child grows regularly with the same quantity of milk, it means the quantity of breast milk is increasing.
• If, after some days, the child does not finish all the supplemental milk, but continues to gain weight, it means that the breast milk is increasing and that the child has enough.
• Weigh the child daily with a scale graduated to within 10g or 20g. When a baby is gaining weight at 20g per day (whatever his weight):
• Decrease the quantity of F100 Diluted to one half of the maintenance intake. • If the weight gain is maintained (10g per day whatever his weight) then stop supplemental suckling completely. • If the weight gain is not maintained then increase the amount given to 75% of the maintenance amount for
two to three days and then reduce it again if weight gain is maintained.• If the mother is agreeable, it is advisable to keep the infant in the centre for a further few days on breast milk
alone to make sure that the infant continues to gain weight. If the mother wishes to go home as soon as the child is taking the breast milk greedily then they should be discharged.
• When it is certain that the child is gaining weight on breast milk alone he should be discharged, no matter what his current weight or weight-for-length.
Care for the Mother
Since the aims of the treatment are to increase breast milk and for the mothers learn from each other, and because the treatment is different from older patients, the infants should be together in a specific room that can be monitored and kept quiet.
• Check mother’s MUAC and the presence of oedema.• Explain to the mother what the aim of treatment is and what is expected of her.• Do not make the mother feel guilty for the state of her child or blame her for giving other foods. Discourage
self-criticism for the lack of milk.• Strongly reassure the mother that the technique works and that she will produce enough milk to make her baby
better.• Be attentive to her and introduce her to the other mothers in the centre.• She should drink at least two (2) litres of fluids per day.• She must eat enough - about 2500kcal/day (one porridge in the morning, one or two family meals, one porridge
in the afternoon).• The mother who is admitted in the centre with her child receives Vitamin A (200,000 IU): If the child is below
1 month old (there should be no risk of pregnancy)• Micronutrient supplementation must also be given to the mother. The quality of the milk depends upon the
mother’s nutritional status. It is critical that the mother receives meals while the child is an inpatient. The breast feeding mother’s diet is important for the recovery of the infant from malnutrition.
• The length of stay in the inpatient facility should be as short as possible.
Field Card 34. Infants Less Than Six Months without Prospect of Being Breastfed
There are special circumstances where a child less than six months cannot be exclusive breastfed (these include abandonment, a child being orphaned, medical conditions or when a mother who is HIV positive meets the criteria for, and chooses, exclusive replacement feeding).

Guideline for Management of Acute Malnutrition
83
When there is no prospect of being given breast milk, then severely malnourished infants less than six month old are treated according to the standard protocols of management of severe acute malnutrition in Phase 1, Transition and Phase 2. However, the following dietary modifications explained here must be applied.
Nutrition Support: Diet and Frequency
Follow the same phases as for older children (see FC 24 for criteria to move from one phase to the next).Use ONLY F100 diluted for children without oedema. Give F75 for children with oedema (at the same amounts) and switch to F100 dilute once oedema resolves.
Phase 1 Transition PhasePhase 2F100
Diluted F100 or F75 (kwash) Dilute F100 Diluted F100
Class of Weight (kg)
8 feeds per day 8 feeds per day 6 feeds per day
ml per feed ml per feed ml per feed
Below 1.5 30 45 60
1.6 - 1.8 35 53 70
1.9 – 2.1 40 60 80
2.2 - 2.4 45 68 90
2.5 - 2.7 50 75 100
2.8 – 2.9 55 85 110
3.0 - 3.4 60 90 120
3.5 – 3.9 65 98 130
4.0 – 4.4 140
Routine Medication
Routine medicine is the same as for infants under six months who are breastfed.
Surveillance
Surveillance is the same as for phase 1, inpatient care. See FC 30.
Follow – up after discharge
Follow-up for these children is very important and needs to be organized between the carer and the health staff. With the absence of breastmilk, other milks need to be included in the diet to prevent relapse. Nutrition counselling for the mother or caregiver is essential. If the child has been exposed to HIV, refer to appropriate clinics for diagnosis and treatment.

84
Guideline for Management of Acute Malnutrition
Section 8Treatment of medical
complications
85

86
Hypoglycaemia
Though uncommon, severely malnourished patients can develop hypoglycaemia. All children who have travelled long distances to attend a health centre should be given sugar-water as soon as they arrive ( 1 heaped teaspoon of sugar in 50ml of water). Children who have hypothermia or septic shock should be given 50-100ml of sugar water, whether or not they have low blood glucose.
A child who has taken the prescribed quantity of F75 diet each day (with 5-6 feedings per day) will not develop hypoglycaemia overnight and does not need to be woken for night-time feeding. If the diet is not completely taken during the day (due to vomiting or refusal of milk), the health worker should encourage the caregiver to give at least one prescribed quantity of F75 during the night.
Clinical Signs of Hypoglycaemia
• Low body temperature• Lethargy or limpness• Possible loss of consciousness• Eyelid retraction is one sign of an over-active sympathetic nervous system, which starts before actual
hypoglycaemia develops. If a child is sleeping with his eyes slightly open, wake the child up and give sugar-water to drink. Health staff and carers should be taught to look for this sign during the night.
Treatment of Hypoglycaemia
• Patients who are conscious and able to drink are given about 50ml (approximately 5-10ml/kg) of sugar-water. Or they can be given F75 diet or F100 (depending on what is immediately available) orally. The actual amount given is not critical.
• Patients losing consciousness are given 50ml (or 5-10ml/kg) of sugar-water by NG tube immediately. When consciousness is regained, give milk feed frequently.
• Unconscious patients are given sugar-water by NG tube. They should also be given glucose as a single intravenous injection (5ml/kg of a sterile 10% glucose solution).
• All severely malnourished patients with suspected hypoglycaemia should be treated with second-line antibiotics. Also keep the child warm and monitor for hypothermia.
Preparation of sugar water (10% dilution):
Quantity of Water Quantity of Sugar
100 ml 10g 2 heaped teaspoons
200 ml (average cup) 20g 4 heaped teaspoons
500 ml (small bottle) 50g 10 heaped teaspoons
1 litre 100 g 20 heaped teaspoons
Notes:
• Take clean drinking water (slightly warm if possible to help dilution). Add required amount of sugar and shake or stir vigorously.
• Give immediately to ALL ADMISSIONS IF MILK CANNOT BE GIVEN IMMEDIATELY.

Guideline for Management of Acute Malnutrition
87
Hypoglycaemia in the OTPIf a child presents with signs of hypoglycaemia in the OTP you can implement the treatment protocol as indicated here.
Always consider starting second line antibiotics, if the patient is not taking them already.Always try to transfer the child to SC – AFTER starting treatment with sugared water and antibiotics!
If transfer is possible, give sugared water to the carer to administer during the transfer.
If transfer is not possible, provide sugared water at the centre and give small amounts of RUTF as soon as the patient is able to eat. Instruct the mother/carer to do the same when they return home, and to continue to give small meals throughout the day to avoid relapse.
Monitoring Hypoglycaemia
The patient’s response to treatment should be dramatic and rapid. If a very lethargic or unconscious patient does not respond, it indicates a different cause for the clinical condition such as an infection. The different source of the lethargy must be determined and treated. If consciousness drops or temperature falls, re-test the blood glucose level and give another dose of glucose 50ml by NG tube or IV (10% glucose as above).
Prevention of Hypoglycaemia
Make sure that the severely malnourished patient receives sugar water on admission if it is not close to a feed time or if the patient is waiting in the casualty/emergency department for over one hour. For patients at risk of hypoglycaemia (very sick children with poor appetite, with vomiting or diarrhoea), give frequent, regular feeds every three (3) hours.
“Kangaroo Care”Kangaroo care means keeping an infant in continuous skin-to-skin contact with the mother or adult caregiver. The infant is kept near the mother’s breast.1. The mother removes inner clothing2. The infant only wears a nappy and head covering3. The infant is held close against the mother’s bare chest by wrapping a culturally appropriate cloth4. The mother wears enough outer clothing to keep warm, adjusting so that the infant’s face is exposed to the
air and the mother can see the infant.
Hypothermia
Clinical signs of Hypothermia
Severely acutely malnourished patients are highly susceptible to hypothermia. Hypothermia is indicated by a rectal temperature below 35.5ºC, or an under-arm temperature below 35ºC.
Treatment of Hypothermia
• Do not bathe severely malnourished patients on admission. Later, when the patient is stabilized, bathe patient only during the warmest part of the day with warm water. Dry patients quickly and gently after washing.
• Use the “kangaroo technique” for children with a carer.• Put a hat on the child and wrap mother and child together.• Offer hot drinks for the mother to drink to keep her skin warmer (plain water, tea or any other hot drink).

88
Hypothermia in the OTPIf a child presents with signs of hypothermia in the OTP follow treatment as indicated here. Protect the child from air currents, cover head and body. If it is not too windy encourage carer and child to sit outside – but not directly under the sun. Use “Kangaroo care” technique and explain the mother/carer that she/he needs to do the same when home, particularly at night.
Always consider transferring the child to inpatient care and ensure that the child eats – even if small amounts at the beginning, as this will be the main source of energy and heat.Ensure that antibiotic treatment is started and followed up correctly.
Monitoring Hypoglycaemia
• Monitor a patient’s body temperature during re-warming.• The room should be kept warm, especially at night (between 280C and 320C). A maximum-minimum thermometer
should be on the wall in the Phase 1 area to monitor the temperature.• Treat for hypoglycaemia and give second-line antibiotic treatment.
Note: The thermo-neutral temperature range for malnourished patients is 280C to 320C. This is often uncomfortably warm for the staff and carers who may want to adjust the room to suit them. Staff and caregivers should not reduce the room temperature as it will be too cold for severely malnourished children. Children should sleep with their mothers or caregivers and not in the traditional hospital child-cots. There should be adequate blankets and a thick sleeping mat or adult bed. Most heat is lost through the head; hats should be worn by malnourished children.
During treatment of severe acute malnutrition, be aware of the following: The standard protocol for the dehydrated child (who is not malnourished) should not be used.
Dehydration
Misdiagnosis and inappropriate treatment for dehydration is the most common cause of death of the severely malnourished patient. It is difficult to diagnose dehydration in these patients. The signs of dehydration - such as non-elastic skin and sunken eyes - are often present in the severely malnourished patient regardless of hydration status. It is important to take a detailed medical history and determine if there was a recent fluid loss from acute diarrhoea or vomiting.
A severely malnourished dehydrated child has a different protocol.
• With severe malnutrition, the “therapeutic window” is narrow: even dehydrated children can quickly go from having a depleted circulation to experiencing over-hydration with fluid overload and cardiac failure.
• In malnutrition, both marasmus and to a greater extent kwashiorkor, IV infusions are rarely used because there is a particular renal problem that makes the children sensitive to salt (sodium) overload and at high risk of fluid overload.
• To prevent overuse of oral rehydration salts i.e. ReSoMal, do not leave these products accessible in the ward for the carers to give freely to children. Over consumption of ReSoMal can lead directly to heart failure in the severely malnourished patient. Additionally, it may aggravate oedema.
• If there is no dehydration, do not treat diarrhoea with rehydration fluids with the intention to prevent the onset of dehydration. This will again lead to over-hydration and heart failure.

Guideline for Management of Acute Malnutrition
89
The diagnosis is determined by the patient’s history rather than by examination.
There needs to be:• A definite history of significant and recent fluid loss. Usually this is a watery diarrhoea (not just soft or mucus),
frequent, and with a sudden onset within the past few hours or days.• There should also be a history of a recent change in the child’s appearance.• If the eyes are sunken, the carer must be able to report that the eyes have become sunken since the diarrhoea
started.• The child must not have any oedema.
Children with persistent or chronic diarrhoea (without an acute watery exacerbation) are not considered dehydrated.
Field Card 35. Treatment of Dehydration for the Marasmic Patient
When possible and feasible, re-hydrate the patient orally with ReSoMal. Intravenous infusions are dangerous and NOT recommended unless there is: 1) severe shock with 2) loss of consciousness from 3) confirmed dehydration.
The management of dehydration is based on the accurate measurement of a patient’s weight which is the best measurement of fluid balance. The patient should be weighed without any items of clothing on (naked).
Before starting any re-hydration treatment:
1. Weigh the child;2. Take and record the child’s pulse;3. Record the child’s respiration rate and;4. Mark the edge of the liver and the costal margin on the skin with an indelible marker pen (skilled staff only).5. f the staff is qualified to do so, record the patient’s heart sounds (presence or absence of gallop rhythm).
The marasmic malnourished dehydrated child is managed entirely by:
• Weight changes• Clinical signs of improvement such as alertness• Clinical signs of over-hydration (engorged veins, rapid pulse, respiratory distress)
Step 1: Determine 5% of patient’s body weight
For the severely malnourished dehydrated child, a maximum of 5% of the child’s body weight is replaced in the form of fluids during the rehydration process. To determine 5% of body weight, equate: body weight in grams/100 x 5.Therefore, 5% body weight of a 4kg child equals: 4000g/100 x 5 = 200gm which then equates to 200ml of re-hydration fluid.It is estimated that a severely dehydrated marasmic child will lose a maximum of 5% of body weight so it is important to only replace this amount otherwise there is a danger of over-hydration.
Step 2: Administer re-hydration fluid
The fluid must be given slowly over time to prevent complications such as overload or heart failure.• Give ReSoMal orally or by NG tube• Give: 5ml/kg every 30 minutes for first two (2) hours• Give 5-10mls hourly until weight gain has been achieved

90
Case Study
For a 4kg child, over the first two hours give the following orally or by NG tube: • 5ml/kg ReSoMal every 30 minutes for two hours = 20ml x four (there are four 30 minute intervals in two hours)
= 80ml. (This is 2% of a 4kg child’s body weight).• Over the next few hours give 5 to 10ml/kg/hour ReSoMal until weight gain is achieved and the patient shows
improvement. Therefore for a 4kg child, give 20 to 40ml per hour after the initial two hours.
It is important to re-assess frequently to make sure that the patient does not become over-hydrated. Fluid balance is measured at frequent intervals by weighing the child.
Step 3: Complete the re-hydration
Give re-hydration fluid until the weight deficit (measured or estimated) is corrected (maximum of 5% body weight). Stop as soon as the child is re-hydrated, having reached the target re-hydrated weight. As the child gains weight during re-hydration, definite clinical improvement should be obvious. The signs of dehydration should disappear. If there is no improvement with weight gain, the initial diagnosis of dehydration was wrong and re-hydration therapy must be stopped, and the child should be reassessed for another medial diagnosis.
Treatment of dehydration- assessment
Step 4: After rehydration
After rehydration, usually no further treatment is given. However, for severe acutely malnourished children from 6 to 24 months, 30ml of ReSoMal can be given for each incidence of a watery stool. The standard instructions to give 50-100ml for each stool should not be applied. It may cause fluid overload which is dangerous.
ONLY rehydrate until the weight deficit (measured or estimated) is
correct and then STOP – Do not give extra fluid to prevent “recurrence”
CONSCIOUS UNCONSCIOUS
ReSoMal
• 5 ml/30 min first 2 hours• 5 to 10 ml/kg/hour, 12 hours
IV Fluid
Darow’s solution or½ saline & 5% glucose orRinger lactate & 5% dextrose at 15 ml/kg the first hour & reasses
• If improving, 15 ml/kg 2nd hour• If conscious, NasoGastric tube: Resomal• If not improving ==> Septic Shock

Guideline for Management of Acute Malnutrition
91
Two hours after commencing re-hydration therapy, make a major medical reassessment.
• Check all vital signs such as body temperature, pulse and respiration rate.• Check heart sounds.• Check for clinical signs of respiratory distress.• Check level of consciousness and weight gain.• Check for vomiting and/or diarrhoea.
If there is:
• Continued weight loss: Increase ReSoMal by 10ml/kg/hour and re-assess the patient in one hour.• No weight gain: Increase ReSoMal by 5ml/kg/hour and re-assess the patient in one hour.• Weight gain and... ...deterioration of the child’s condition with the re-hydration therapy: • The diagnosis of dehydration was definitely wrong. (Even senior clinicians make mistakes in the diagnosis
of dehydration in malnutrition.) • Stop the ReSoMal and start the child on F75 diet. ...no improvement in the mood and look of the child, or no reversal of the clinical signs: • The diagnosis of dehydration was probably wrong. • Change to F75. ...clinical improvement, but signs of dehydration: • Continue with treatment until the appropriate weight gain is achieved. • Continue with ReSoMal alone. Or F75 and ReSoMal can be alternated. ...resolution of the signs of dehydration: • Stop re-hydration treatment and start the child on F75 diet.
During re-hydration, breast-feeding should not be interrupted.
Begin to give F75 as soon as possible after re-hydration has been completed. The F75 can be given orally or by NG tube. ReSoMal and F75 can be alternated each hour in the case of a patient with mild dehydration and continuing diarrhoea. The introduction of F75 is usually achieved within two to three hours after starting the re-hydration process when the patient should be improving. The re-commencement of F75 will also help to prevent development of hypoglycaemia
Treatment of dehydration- monitoring
Monitor weight
Stable
Clinically improved
Clinically not improved
Continue
LossGain
Target weight
F75
• STOP ALL re-hydration fluid• Give F75• Re-diagnose &
assess
• Increase Resomal by 5 ml/kg/hour
• Reassess every hour
• Increase Resomal by 10 ml/kg/hour
• Reassess every hour

92
Monitoring Re-hydration
Re-hydration (oral or intravenous) therapy must immediately stop if any of the following are observed:
• The target weight for re-hydration is achieved (start F75).• Visible veins are full (start F75).• The development of oedema (indicates over-hydration: start F75).• The development of prominent neck veins.• The neck veins engorge when the abdomen (liver) is pressed.• An increase in the liver size by more than one centimetre.• The development of tenderness over the liver.• An increase in the respiration rate by 5 breaths per minute or more.• The development of a “grunting” respiration (this is a noise on expiration not inspiration). This sign indicates
that the child has fluid overload, an over-expanded circulation, and is going into heart failure.• The development of râles or crepitations in the lungs.• The development of a triple rhythm.
Dehydration in the OTPAt the OTP, only well trained nurses will be able to differentiate true dehydration from marasmus. Those not trained, should not recommend SAM children for transfer just because they appear dehydrated. A full history and assessment should take place first.
If dehydration is confirmed and the child is conscious, start treating as in these guidelines: NEVER use ORS! If ReSoMal is not available, use normal safe drinking water (water is less dangerous for the malnourished child than ORS). The treatment may last for several hours, but it may work. Transfer the child as soon as possible.
If the child is unconscious, then transfer as an emergency. Mobilise local resources (transport, etc.) to get to the SC as fast as possible. Unfortunately, OTPs cannot be equipped with the material for the treatment of re-hydration, due to the complexities of its treatment and the risks of complications of treatment that can only be addressed at the Hospital.
Diagnosis of Shock from Dehydration for the Marasmic Patient
The marasmic patient is going into shock when:• There is definite dehydration determined by the patient’s history and the medical examination, AND• There is a weak or absent radial or femoral pulse, AND• The patient has cool or cold hands and feet (check with back of hand gently for five seconds).
The patient is going into severe shock when, in addition to the above signs, there is a decrease in the level of con-sciousness, the patient is semi-conscious or cannot be roused. The treatment of cardiogenic shock or liver failure is not the same as shock due to dehydration. With cardiogenic shock or liver failure, fluid given is severely restricted or it can cause serious deterioration and the treatment itself could lead to death. Treatment of Shock from Dehydration for the Marasmic Patient
If the patient is definitely dehydrated (a history of fluid loss, a change in the appearance of the eyes), and shows all of the following three bullets, then the patient should be treated with intravenous fluids:• Semi-conscious or unconscious and• Rapid weak pulse and• Cold hands and feetThe amount of IV fluid given is half or less of the amount used for nourished, dehydrated children.

Guideline for Management of Acute Malnutrition
93
Use one of the following solutions:• Half strength Darrow’s solution• Ringer-Lactate with 5% dextrose• Half strength saline with 5% dextrose
Re-hydration needs to be done slowly and monitored closely to prevent over-hydration. Administer 15 ml/kg IV over the first hour and reassess the child.• If there is continued weight loss, or the weight is stable, repeat the 15ml/kg IV over the next hour. Continue
until there is weight gain with the infusion. (15mg/kg is 1.5% of body weight, so the expected weight gain after two (2) hours is up to 3% of body weight.)
• If the child has gained weight but there is no improvement, assume that the child has toxic, septic or cardiogenic shock or liver failure. Stop re-hydration treatment. Look and assess for other causes of loss of consciousness.
As soon as the child regains consciousness, or the pulse rate drops to a normal level, then stop the intravenous fluids and treat the child orally or by NG tube with 10ml/kg/hour of ReSoMal. Continue with the protocol above for re-hydration of the child orally, using weight change as the main indicator of progress.
Note: Other Causes of Shock
Apart from the shock related to dehydration, there are four other causes of shock in the severe acutely malnour-ished child.
1) Toxic shock2) Septic shock3) Liver failure4) Cardiogenic shock.
Toxic shock may be caused by traditional medicines, self-treatment with other medication such as aspirin,paracetamol, or metronidazole, etc.
Septic shock is a specific type of toxic shock where the damage is caused by overwhelming sepsis.This is frequently associated with liver failure.
Diagnosis of Dehydration for the Kwashiorkor Patient
Patients with bi-lateral oedema are over-hydrated and have increased total body water and increased sodium levels. Oedematous patients thus cannot be dehydrated, although they are frequently hypovolaemic.
The hypovolaemia (relatively low circulating blood volume) is due to a dilatation of the blood vessels with a low cardiac output. The treatment of hypovolaemia in kwashiorkor is the same as the treatment for septic shock (see below). If a child with kwashiorkor has watery diarrhoea, and the child is deteriorating clinically, then the fluid lost can be replaced on the basis of 30ml of ReSoMal per watery stool.

94
Septic (or Toxic) Shock for All Malnourished Patients
Septic shock is a serious medical condition. It is caused by decreased tissue perfusion and oxygen delivery as a result of infection and sepsis. It can cause multiple organ failure and death. Children, immuno-compromised individuals, and the elderly are most susceptible as their immune systems cannot cope with infection as well as healthy adults do. The mortality rate from septic shock can be as high as 50%.
Septic shock presents with some of the signs of true dehydration and also of cardiogenic shock. The differential diagnosis is often very difficult. Children who appear very ill may have septic shock, cardiogenic shock, liver failure, poisoning with traditional medicines, malaria, acute viral infection or other severe conditions. All “very ill” children should not be automatically diagnosed as having septic shock; the true reason for the condition should be sought.
If septic shock develops after admission, treatment must be carefully reviewed to determine if the treatment is the cause of the clinical deterioration. Any unnecessary drugs should be stopped.
Diagnosis of Septic Shock
To diagnose septic shock, signs of hypovolaemic shock are present. There is a fast, weak pulse with all three of the following:
• Cold peripheries• Disturbed consciousness• Absence of signs of heart failure Treatment of Septic Shock
All patients with signs of early or developed septic shock should immediately:• Be given broad-spectrum antibiotics – therefore continue first-line antibiotic and add a second-line antibiotic.
For incipient (early) septic shock, give the standard F75 diet by NG tube.
For developed septic shock: Consider third-line antibiotics, antifungal treatment and antistaphylococcal treatment.• Keep the patient warm to prevent or treat hypothermia.• Give patient sugar-water (1 teaspoon sugar in 50ml water) by mouth or NG tube as soon as the diagnosis is
made (to prevent hypoglycaemia).• Do not physically disturb the patient (no washing, excess examination, investigations in other departments, etc.)• Do not transport patient to another facility. The stress of transport leads to dramatic deterioration.
If the patient is unconscious because of poor brain perfusion, then a slow IV infusion of one of the following can be given:• Whole blood of 10ml/kg over at least three hours. Nothing is given orally during the blood transfusion.• Or 10ml/kg/hour for two hours of the following (do not give if there is a possibility of cardiogenic shock): Half-strength Darrow’s solution with 5% glucose Ringer’s lactate solution with 5% glucose Half-normal (0.45%) saline with 5% glucose
Use of antibiotics in septic shock
Make sure the child already received Ampicilin/ GentamicinWhen there is no improvement after 24H hours of this treatment, switch to:
When origin of infection is unknown:Continue Ampicillin and Gentamicin AND addCloxacillin IV: Children: 100mg/kg/d by 3 injections every 8 hours.

Guideline for Management of Acute Malnutrition
95
When gastro-intestinal, or gynaecological origin:Gentamycin IM: 5 mg/kg/day by 1 injection for 7 days ANDCeftriaxone slow IV: Children: 100mg/kg/d in 1 dose the 1st day, then, 50mg/kg/d the following days ANDMetronidazole IV: Children: 20-30mg/kg/d by 3 infusions every 8 hours.
When of cutaneous origin:Cloxacillin IV: Children: 100mg/kg/d by 3 infusions every 8 hours AND Gentamycin IM: 5 mg/kg/day by 1 injection for 7 days.
When of pulmonary, urinary and other origin:Ceftriaxone slow IV: Children: 100mg/kg/d in 1 dose the 1st day, then, 50mg/kg/d the following days ANDCiprofloxacin PO: Children: 15-30mg/kg/d in 2 doses.
Also add oral anti-fungal drugs if necessary. Fluconazole: 6 mg / kg / day once daily for 14 days.
Treatment Monitoring
Monitor the patient every ten minutes for signs of deterioration. Especially watch for overhydration and heart failure indicated by signs such as:• Increasing respiratory rate,• Development of grunting respiration,• Increasing liver size,• Vein engorgement.
As soon as the patient improves (stronger radial pulse, regain of consciousness), stop all IV intake. Continue with F75 diet.
Absent Bowel Sounds, Abdominal Distension
Bowel sounds in the severe acute malnourished patient may be reduced or absent. The severe acute malnourished patient will often experience impaired bowel functions, mainly as a result of bowel infections.
Signs and symptoms of impaired bowel function:• Abdominal distension• Loss of bowel sounds• Vomiting
Treatment
• Give first-line and second-line antibiotic treatment by intra-muscular injection.• Consider adding third-line antibiotics, at doctor’s discretion.• Stop all other drugs that may be causing toxicity (such as metronidazole).• Give a single IM injection of magnesium sulphate (2ml of 50% solution).• Pass an NG tube, and aspirate the contents of the stomach. Then “irrigate” the stomach with isotonic clear fluid
(5% dextrose or 10% sucrose. The solution does not need to be sterile). Do this by introducing 50ml of solution into the stomach and then gently aspirating all the fluid back again. This should be repeated until the fluid that returns from the stomach is clear.
• Put 5 ml/kg of sugar-water (10% sucrose solution) into the stomach and leave it for one hour. Then aspirate the stomach and measure the volume that is retrieved. If the volume is less than the amount that was introduced, either give a further dose of sugar-water or return the fluid to the stomach.
• There is frequently gastric and oesophageal candidiasis: give oral Nystatin suspension or Fluconazole• Keep the child warm. If the child’s level of consciousness is poor given intravenous glucose:

96
• Do not put up a drip at this stage. Monitor the child carefully for six (6) hours without giving any other treatment.• Improvement is measured first by a change in intestinal function: a decrease in the distension of the abdomen,
visible peristalsis seen through the abdominal wall, return of bowel sounds, and decreasing size of gastric aspirates. Second, there should also be improvement in the child’s general condition.
If there is intestinal improvement, begin to give small amounts of F75 by NG tube (half the quantities given per kg in dehydration. Subsequently adjust by the volumes of gastric aspirated).
If there is no improvement after six (6) hours:
• Consider putting up an IV drip. It is crucial that the administered fluid contains adequate amounts of potassium. Add Sterile Potassium Chloride (20mmol/l) to all solutions that do not contain potassium. If it is available, use one-fifth normal saline in 5% dextrose, otherwise use Ringer-Lactate in 5% dextrose or half-strength saline in 5% dextrose. The drip should be run VERY SLOWLY. The amount of fluid that is given should be NO MORE THAN 2 to 4 ml/kg/hour.
• Start to give the first and second line antibiotics intravenously.• When the gastric aspirates decrease so that one half of the fluid given to the stomach is absorbed, discontinue
the IV treatment and continue with oral treatment only.
Heart Failure
For the severely malnourished patient, congestive heart failure is usually a complication of over-hydration (when IV fluids or standard ORS solution is given). It can also manifest when there is very severe anaemia; after a blood or plasma transfusion; or with a diet high in sodium. It is important to differentiate heart failure from respiratory infection and septic shock.
Signs and Symptoms of Heart Failure
Heart failure is diagnosed when the patient has a few of the following symptoms (do not wait for all symptoms to occur, as the patient will continue to deteriorate):• An increase in respiration rate: - An acute increase in respiration rate of more than 5 breaths per minute (particularly during rehydration
treatment). - More than 50 breaths/minute in infants (0-12 months) - More than 40 in children one to five years old.• Physical deterioration with a gain in weight.• A sudden increase in liver size with tenderness developing over the liver. (The liver is marked before starting any
infusion to determine change in size).• Respiration that has or develops a “grunting” sound during each expiration• Crepitations or râles in the lungs.• Prominent superficial and neck veins.• Engorgement of the neck veins when the abdomen (liver) is pressed.• Increasing oedema or reappearance of oedema during treatment.• An acute fall in haemoglobin concentration (Requires laboratory).
If heart failure progress, and the patient further deteriorates, there is either1) Marked respiratory distress progressing to a rapid pulse, cold hands and feet, oedema and cyanosis; or2) Sudden, unexpected death.
This is cardiogenic shock. Severely malnourished patients are fragile and can go from dehydration to over-hydration quickly after treatment has started. Patients can be admitted with heart failure: it is important that it’s differentiated from shock due to dehydration or sepsis because the treatment is quite different.

Guideline for Management of Acute Malnutrition
97
For patients who have already been admitted, there is usually also weight gain. As heart failure usually starts after treatment, there is nearly always a record of the weight of the patient that was taken before the onset of heart failure.
Heart failure and pneumonia are clinically similar, and very difficult to tell apart:• If there is an increased respiratory rate and any gain in weight, then heart failure is the first diagnosis.• If there is an increased respiratory rate with a loss of weight, then pneumonia is diagnosed.• If there is no change in weight (fluid balance) then the differentiation has to be made using the other signs of
heart failure.• Pneumonia is NOT diagnosed if there has been any weight gain before the onset of respiratory distress.
Heart Failure and Oedema
• Children with oedema can go into heart failure without a gain in weight, when the expanded circulation is due to oedema fluid moving from the tissues to the vascular space.
• During the initial treatment of severe acute malnutrition, any fluid containing sodium given will have to be safely excreted later. Initial over-treatment can lead to death from heart failure several days later, when intracellular sodium (marasmus and kwashiorkor) and oedema fluid are being mobilised.
• As oedema fluid is mobilised (kwashiorkor) and the sodium is coming out of the cells (both kwashiorkor and marasmus), the plasma volume expands and there is a fall in haemoglobin concentration. This dilutional anaemia happens to some extent in nearly all children as they recover. A substantial fall in haemoglobin, as a sign of an expanding circulation, is also a sign of impending or actual heart failure. These children should never be transfused.
Treatment of Heart Failure
When heart failure is diagnosed:• Stop all intakes of oral or IV fluids. No fluid or food is given to the patient until signs of heart failure are improved
which may take 24 to 48 hours. Small amounts of sugar-water can be given orally to prevent hypoglycaemia.• Administer frusemide (1mg/kg) stat, as a single dose.• Digoxin can be given in a single dose of 5 micrograms/kg. Note that this is lower than the normal dose of digoxin.
A loading dose is not given. Use the paediatric preparation, not small quantities of the adult preparation.• If the heart failure is associated with severe anaemia, treatment of the heart failure takes precedence over the
treatment of the anaemia.• A patient with heart failure should never be transfused (unless there are facilities and experience with exchange-
transfusion).
Severe Anaemia
Diagnosis of Anaemia
If the haemoglobin concentration is less than 40g/l, or the packed-cell volume is less than 12% in the first 24 hours after admission, the child has very severe anaemia which can cause heart failure.All children have a fall in Hb during the early phase of treatment. This ‘dilutional anaemia’ is due to the sodium coming of the cells and mobilization of oedema – it must not be treated. That is why it is important to check Hb on admission for any child suspected of having severe anaemia.
Treatment of Anaemia
• Give 10ml per kg body weight of packed red cells or whole blood, slowly over three hours.• The patient fasts during blood transfusion and for at least three hours after blood transfusion.• After the start of nutritional rehabilitation with F75, do NOT transfuse a child after 48 hours and up to 14 days.• Do NOT give iron during Phase 1 and Transition Phase of treatment.

98
• If the facilities and staff expertise exist (i.e. neonatal units), it is preferable to give an exchange transfusion to SAM children with severe anaemia.
Heart failure due to anaemia is clinically different from “normal” heart failure. With anaemia there is “high output” failure with an over-active circulation.
Increasing anaemia and heart failure or respiratory distress, is a sign of fluid overload and an expanding plasma volume. The heart failure is not being “caused” by the anaemia; these patients should never be given a straight transfusion of blood or even packed cells.
Diagnosis and treatment of anaemia
AnaemiaCheck Hb at admission if any clinical
suspicion of anaemia
Hb>= 40 g/l or Packed cell vol> = 12 %
Hb < 40 g/l or Packed cell vol < 12 %
Between 2 to 14 days after admission: NO ACUTE TREATMENTIron during phase 2
ONLY during the first 48 hours after admission:Give 10 ml/kg whole or packed cells 3 hours – No food for 3 to 5 hours.
Administration of Medication
Great care should be exercised in prescribing drugs to severely malnourished patients. Severely malnourished pa-tients have: abnormal kidney and liver function; changed levels of the enzymes that metabolise and excrete drugs; excess enterohepatic circulation (reabsorption) of drugs that are excreted in the bile; a decreased body fat which increases the concentration of fat-soluble drugs; and, in kwashiorkor, a possible defective blood-brain barrier. Few drugs have been examined for pharmocokinetics, metabolism or side effects in SAM patients.
It is strongly advised that severe malnutrition is treated first, before standard doses of drugs are given (with the exception of the routine medicines). Drugs used for HIV and TB can damage the liver and pancreas. HIV and TB are not considered rapidly fatal (except military TB and TB meningitis) so treatment can be delayed for up to one week. During that time, nutritional treatment returns the patient’s metabolism to normal.
Common drugs such as Paracetamol do not work for most severely malnourished children during Phase 1, and can cause serious hepatic damage.
Any required drugs can usually be given in standard doses to patients who are Phase 2 and those in OTP.

Guideline for Management of Acute Malnutrition
Section 9Community involvement in
Management of Acute Malnutrition
99

100
Overview
Community involvement is a multi-functional approach that highly contributes to successful implementation of nutrition programs in both emergency and development contexts. This means placing the affected population at the centre of decision making for how protection and assistance will be provided when setting up the response program.
In Somalia, community involvement and mobilisation is of radical importance, for the following reasons:• The need to provide early diagnosis, since many patients cannot be transferred to SC (and therefore, they should
be identified in the community before they develop complications)• The need to obtain maximum programme coverage, through identification of the children at their homes and
involvement of more peripheral communities that have low access to the centres• The need to develop good relationships with the elders and representatives from clans and sub-clans, to ensure
that the purpose and objectives of the programme are well understood, and to prevent potential misunderstandings or problems.
• The need to have good relationships with all partners and local leaders to ensure security and continuity of the programmes.
There is no easy way to do community mobilisation. Each area and organisation will require its own techniques and approaches. The following pages summarize a number of steps to be taken into account, which may be helpful.
In ALL CASES, it is fundamental that ALL PROGRAMMES take community mobilisation very seriously.Community mobilisation is a MAJOR part of the programme and not just an extra activity that is implemented “when time allows” or only through volunteers without proper supervision or training.
Phases of Community involvement
Programmes for the Management of Acute Malnutrition usually involve large numbers and types (SFPs, OTPs, SC) of sites that are near or associated with health facilities.
The members of the community play a major role in assisting health workers to assess the needs, identify and diagnose children with malnutrition, as well as to plan the programmes or participate to deliver distributions or follow up patients.
To have a successful programme, community members must understand the objectives and structure of the feeding programmes. In addition, the local community must be involved in the early stages of programme implementation to avoid common problems such as absenteeism, misuse of rations (like selling or sharing), mishandling of routine medications and defaulting.
Community mobilisation is challenging in Somalia. However, some agencies have gained experience in implementing nutrition interventions that heavily involve the community. This strategy is comprised of three phases:
1: Initial stage - Planning and Participatory assessment
Involving the community at the initial stage will greatly improve the effectiveness of the programme. Where this is not possible, the agency may have to undertake the actual implementation of the programme with minimal community consultation.
During the needs assessment and planning sessions, the leaders may be involved in identifying appropriate sites as well as creating awareness about the intervention. Where community involvement is possible, the agency should first conduct a participatory assessment. Sources of information may include national and local media, need assessment reports, local experts, community leaders, religious leaders, host community members in the case of a refugee or IDP camp, community based organizations (CBOs), UN agencies and international NGOs and government departments (where the government is operational). During the participatory assessment the agency will gather information on;

Guideline for Management of Acute Malnutrition
101
• Inventory of services most needed by the community to help manage malnutrition (water and sanitation, health education programs, transport and communication channels, roads, health facilities, schools, marketing systems of food products)
• Feeding program sites – based on proximity to households/villages/health facility • Components of the feeding program that community can undertake/implement• Community resources ( storage space, money, time, religious and cultural values)• Human capacity (type of skilled personnel and level of involvement)• Existing community based organizations and learning institutions working on food and nutrition related issues• Most appropriate motivational factors to enhance participation of community volunteers and carers.
Analysis of information obtained will determine the level of community involvement. In addition, selecting a community for partnership will also depend on whether the agency is already working in that particular community and the potential openness of the community to participate in the programme.
2: Collaboration stage (Partnership)
At this stage, the implementing agency needs to decide on the modalities of working with the community based on the information obtained in the assessment (initial stage). The agency can decide to work with individual community outreach workers and/or with existing community based organisations (CBOs).
Individual outreach workers may require training and skills to assist with programme activities whereas the CBOs may need some bit of technical support and additional resources to implement programme. Both options need close monitoring in the initial stages of involvement. It is important that the rest of the community members understand the criteria used for selecting specific individuals or CBOs to avoid misunderstandings that can lead to conflicts.
Elements of partnership vary and depend on the type of nutrition interventions being implemented. When setting up feeding programmes that involve the community, the following factors should be taken into consideration;
• Recruit and train individual community members – have some kind of an agreement between the individual and implementing agency. During recruitment it is very important that the community members understand their duties, programme objectives, target groups, and type of remuneration (if any) or motivational elements.
• Identify additional resources needed to support participation e.g. incentives for community members.• Design an outreach system by mapping out areas where services are most needed and can be provided though
collaboration. Allocate health workers, community workers and resources accordingly.• Establish links with CBOs and agree on the role of each partner, levels of collaboration, resources needed (who
will provide what), time frame, entry and exit criteria of each partner and sign a memorandum of understanding to formalize the agreement.
• Formulate health and nutrition educational messages that can be used for counselling target groups. • Mobilize the community members and involve them in actual programme activities. Mobilization is the process
of bringing men and women together to discuss common problems and establishing community responses with the support of humanitarian workers.
• Keep a continual dialogue with target population to build trust and confidence and to ensure active participation in planning, implementation and monitoring of service delivery.
Actual partnership in program implementation happens at two levels, at programme level and community level. In these two levels, the outreach workers team up with the technical staff to perform various activities:
At programme level- • Assist in taking anthropometric measurement of beneficiaries• Assist in making pre-mix and distributing to beneficiaries• Communicate or interpret education messages into local languages during community education sessions.

102
At community level -
Community sensitization;
• The technical staff with the help of the outreach workers will formulate appropriate messages and where possible translate to the local language e.g. define malnutrition and describe characteristics of a malnourished individual as perceived by community members.
• Identify best channel to pass messages to local leaders and target group• Plan and have sessions with community leaders and announce schedule of trainings and programme activities
to community members. • The outreach worker identifies barriers to the work and provides timely solutions, as well as enhances dialogue
between the community and the implementing agency.
Case-finding
A team of outreach workers may actively be involved in screening children at community level in order to find the malnourished individuals (severe, moderate or at risk) and refer them to the most appropriate programme. If a child is found to be severely malnourished without any medical complications, then they should be referred to the nearest OTP site. If a pregnant mother in 2nd or 3rd trimester or a child 6 -59 months is moderately malnourished, they should be referred to nearest SFP site. Sometimes, community sensitization alone may stimulate self-referrals by families and communities to selective feeding programme sites. Case finding is very essential to increase programme coverage and treat children before they develop life threatening complications.
Follow-up visits
Sometimes beneficiaries are absent or default from the programme. In such instances, the community outreach worker should follow-up the individual cases to investigate reasons for absence or defaulting and encourage return to programme. A follow-up can also be done for those individuals that do not respond to treatment; the outreach worker investigates the potential causes and provides information to the implementing agency for additional support and care. In short term emergencies, specific outreach workers can be hired to work together with the implementing agency staff. For longer term activities, trained community volunteers (supported through a health facility or with some incentives) can assist in follow-up activities.
3: Final stage and ongoing process
In this final stage the programme is operational with active involvement of the community. The community has access and takes control of the services whereas the partner agency takes the supervisory role and, where need be, continues providing technical support and resources.
Community sensitization is an on-going process. Community members, by attending meetings, can regularly voice their views and suggest alternative courses for action. The volunteers/outreach workers and other community workers maintain regular contact with the community to identify problems and work together to provide timely solutions. A regular means of maintaining contact with the community should be established as soon as the programme becomes operational. During design stage, information collected on appropriate channels, individuals and forums in which to conduct this dialogue can be useful to the process.
Guideline for Management of Acute Malnutrition
103
Field Card 36. Active Screening of Acute Malnutrition
Active screening is a tool to rapidly estimate the general health and nutritional status of a child. It is part of the community mobilisation activities.
The objectives of active screening are:• to identify all children in the community that have malnutrition, and• to diagnose malnutrition before the child develop complications.
Good active screening should therefore lead to better coverage and to less children needing inpatient care at SC, which should translate in turn into better recovery rates and programme statistics.
This is particularly important in Somalia, where there are many OTPs that do not have the possibility to transfer children with complicated SAM to a SC. When a child presents complicated SAM and cannot be treated accordingly, his/her chances of survival are much lower.
Identify children to be screened (case finding):
Use the techniques presented in Chapter 9 (Community involvement) to organise activities.
There are many ways of organising case-finding. In general, it consists of sending volunteers/outreach workers to their communities in order to visit families door to door, or to gather all children in a central place (door to door is usually preferred to ensure that no child is missed) for screening.
Children identified as malnourished may be referred directly to the programme with a referral slip (SFP, OTP or SC), or be told to present themselves at the next distribution. The outreach workers and the communities should have a good understanding of the target groups for the different programmes, in order to reduce in appropriate referrals and rejections at the distribution site.
Screening method at the community:
• Measure child’s MUAC• Assess presence of bilateral oedema.• Clinical status (wasting and weakness, particularly in children below 6 months)
Use criteria of admission as the threshold to decide if the child needs transferring. W/H will be assessed at the centre, but the child may be admitted to the centre because of W/H, MUAC or bilateral oedema.
Follow up of activity:
Volunteers and/or outreach workers should meet regularly with programme staff (from the SFP or OTP) and provide a report of their activities (places visited, number of children screened, number of children referred, etc.). They should report as well, on their activities to sensitize community leaders, local organisations, etc.
This meeting can be used to help evaluate outreach activities, and make plans of areas to visit in the following weeks.

104
Field Card 37. Home Visit Check-list
The following are some issues to focus on during a home visit. The questions selected depend on the child’s individual circumstances.
Feeding
• Is the Premix/RUTF eaten only by the sick child?• Is food other than Premix/RUTF given to the sick child? If yes, what food?• Is Premix/RUTF finished before other food is given? What about breastmilk?• How is the child given the Premix/RUTF? (eg. mixed with other food, with water)• How much Premix/RUTF does the child eat each day?• How many times per day is the sick child given food/RUTF to eat?• Does anyone encourage/help the sick child to eat?• What does the parent/caregiver do if the sick child does not want to eat?• Observe child eating one meal of Premix/RUTF.
Caring
• Does the parent/caregiver feel that their child is improving? If not, why?• Have they visited the traditional healer to help this child?• Who cares for the sick child during the day?• Is the sick child clean?• Is anyone in the household sick or has recently died? How does this affect the caring of the child?• Any other household circumstances that affect how the child is cared for?
Health
• What is the household’s main source of water?• Do they use soap in the household?• Does the parent or caregiver and the sick child wash hands and face before feeding?• Is Premix/RUTF, other food and water covered and free from flies?• Does the parent or caregiver know what causes diarrhoea?• What action does the parent or caregiver take when the sick child suffers from diarrhoea? (Include any action
involving foods, medicines, fluids)• If any medicines have been prescribed, are they being given correctly?• If there is a particular medical problem that has been identified by the outpatient care team, how is the child
progressing? Is there a need for an extra clinic visit?• Observation of diarrhoea or vomiting.
Food Security
• What is the most important source of food for the household?• What is the most important source of income for the household?• Is the family currently receiving General Food Rations? And if so, for how many people?

Guideline for Management of Acute Malnutrition
Section 10Nutrition information,
education and communication
105

106
One way of managing acute malnutrition is through addressing the improper behaviours and practices of community members that contribute to malnutrition. It is imperative to educate members of the community on causes of malnutrition and best practices to manage and prevent malnutrition at household level. Involvement of the community in designing and developing education materials is essential and contributes largely towards behaviour change. Distribution sites and demonstration sessions are good opportunities to deliver appropriate messages focusing on proper child care practices, household and personal hygiene, use of safe drinking water, hygienic preparation and protection of foods, and use of nutritious local ingredients for complementary feeding.3
Nutrition information refers to knowledge, such as information about new foods that are being introduced in an emergency situation. Nutrition education refers to training or orientation for a particular purpose such as support for breast feeding. Nutrition communication refers to the method by which information is imparted.
Steps for conducting effective community nutrition education sessions:
Step 1 At the community level, identify the problems affecting the target population. The problem is best identified through conducting a needs assessment.
Step 2 List down the problems and prioritize them. The most pressing problems should take up the first position and the least important ones should come last.
Step 3 Identify the target group. The target group is defined as that group that is most affected by the problems.
Step 4 Build consensus about the problem with the community. The involvement of the community in this step is crucial and will assist in providing relevant information for the next steps.
Step 5 Based on the problems agreed upon in step 4, select relevant nutrition topics e.g. if the problem is poor child care practices- select topics such as optimal breast feeding and complementary feeding.
Step 6 Identify possible factors that may impede communicating the nutritional messages e.g. language barriers and beliefs, and seek for the most appropriate ways of addressing the identified barriers
Step 7 Assess and select appropriate communication channels such as demonstrations, songs, drama, poems, and counseling sessions
Step 8 Conduct the education session: Prepare educational materials, agree on appropriate dates, time and venue and inform the target group accordingly.
Step 9 After conducting the education sessions, inform individuals or target group of next sessions and evaluate your work. The educator must know what was useful, what channels were most effective, how was the message received by the audience? And adapt accordingly.
Step 10 Write a training report and submit to supervisor.
3 This chapter is adapted from Guidelines on Management of Moderate Acute Malnutrition – Somalia - January 2009.

Guideline for Management of Acute Malnutrition
107
4 Nutrition and HIV/AIDS guidelines
Counseling sessions
Carers and family members need to understand the need for proper care and nutritional support of malnourished children or individuals discharged from a nutrition program. The counselor, in this case the nurse or nutrition educator, has the responsibility of giving appropriate information to the caregiver. Below is the process of conducting a counselling session. All counsellors must be adequately trained on the processes of conducting counseling sessions and ethical matters. The GATHER4 approach is currently being used by counselors for conducting effective counseling sessions. This involves;
• Greet the patient and offer them a seat, make introductions and assess their well being• Ask their feeling about their nutritional status, symptoms, nutritional problems and concerns.• Tell patient of different options that can be used to address the nutritional problems- communicate key messages• Help patient make informed choices and together develop an action plan / approaches to address the problem • Explain fully the choices and actions and possible barriers• Reassure and give the Return date for the next visit
General guidance in counseling sessions
1. The individuals to be counseled include; acutely malnourished patients (especially if pregnant and lactating mothers), caregivers (parents or guardian) of children under 10 years, and for the chronically ill and community groups.
2. Counseling can be undertaken by nutritionists, nurses, clinicians, Community Health Workers, or extension workers
3. Counseling can be conducted during actual management, discharge, and follow-up of malnourished individuals4. The kind of materials to be used will depend on problems identified and topics selected. In the absence of national
guidelines, counselors can use other available materials such as nutrition and health guidelines, integrated management of child hood illnesses, guidelines on IYCF, Nutrition and HIV/AIDS.
Nutritional education topics
Nutrition counseling and education is crucial for management of moderate malnutrition and prevention of severe malnutrition, because knowledge on the causes of malnutrition enables a patient or carer to be able to control and prevent further deterioration in nutritional status. It is also recommended that whenever such sessions are conducted, they should be considered as opportunities and as such should be well utilized in order to deliver key messages about the health of women and children.
Focus of such messages depends on context but often includes the following:• proper child care practices• household and personal hygiene• use of safe drinking water• hygienic preparation of food• protection of foods, • use of nutritious local ingredients for complementary feeding• Utilization of ready-to-use food commodities.

108
Topic Target audience
Key messages/ action points
Optimal breast feeding
1. Breast feeding women
2. Pregnant mothers in the 3rd trimester
• Timely initiation of BF (within 1 hr of delivery) and giving of colostrums • Importance of continuing to breast feed for at least 2 years• Importance of ensuring proper hygiene in food preparation and feeding • Give appropriate information to mothers to support exclusive and continued
breast feeding. • Children 0-6 months should be exclusively breast fed: No feeds (including
water) other than breast milk. • Breast feeding should be on demand (as long as the infant wants). • Encourage breast feeding during illness. If child is not able to breast feed,
encourage expression of breast milk and feed by cup.
Optimal complementary feeding
Mothers with children 6 months and above
• Encourage continued breast feeding beyond 6 months together with appropriate complementary feeding.
• Explain body building, energy giving, and protective foods. Body building foods responsible for building and repairing our body (e.g. Meat, beans, milk eggs).
• Explain energy giving foods, they provide energy to our body to enable us to carry out daily activities like, working, thinking, running, playing etc (sorghum, maize, oil,).
• Explain protective foods that enable the body to protect against infection and fight diseases (e.g. Green vegetables, Mangoes, Carrots).
• Encourage increased fluid intake, including breast feeding, day and night for children with diarrhea or vomiting.
• Discourage withholding of feeds during illness and instead encourage intake of small frequent enriched feeds or give an extra meal above child ’ s usual daily feeds.
• Encourage mothers to bring all their children below 5 years old to the nearest health facility for regular monitoring as well as for vitamin A supplementation every 6 months.
Feeding of the sick and or malnourished children
Carers/mothers with sick children that are malnourished
• If the child is still breast feeding, encouraged mother to continue. • The child at this stage requires: 1. High energy intake (150 -200 kcal/kg body
weight) 2. Sufficient protein 4-5g/kg body weight/day 3. Micronutrients especially potassium, iron, zinc and vitamins
• The feeds must be easy to eat and digest. • To achieve high energy intakes: 1. Feed the child frequently, at least six times a
day 2. Add oil, honey, margarine, butter, sugar 3. Use fat-rich foods like ground nuts, avocado, animal milk.
• To achieve high protein intakes: Use milk, or locally available staple mixed with legumes, meat or fish
Maternal nutrition
1. Pregnant and lactating mothers
• Take the weight (in kg) of all pregnant women and record it on the maternal clinic card.
• Counsel mothers on appropriate diet for pregnant women using locally available foods.
• Encourage consumption of a balanced diet rich in vitamins and minerals. • Encourage mother to ensure that all children aged five years and below and
pregnant women sleep under insecticide treated mosquito nets, for preventing anemia because malaria is often a major underlying factor.
• Counsel mothers on diet during lactation as well as consuming enough water (2L per day). Emphasize the importance of extra food while lactating using the list of locally affordable foods.
Nutritional topics and key messages

Guideline for Management of Acute Malnutrition
109
Vitamin A supplementa-tion
1. Carers of children 6-59 months
2. Lactating mothers
Children• All children aged 6 to 59 months need a vitamin A capsule every 6 months. • Vitamin A supplementation is safe for children and protects them from diseases
such as diarrhea, acute respiratory infections and also reduces deaths. • Children should be fed as often as possible with vitamin A rich foods (mangoes,
green leafy vegetables, wild red and orange fruits, egg yolk, liver, milk, etc.) • Children sick with measles, certain eye problems, severe diarrhoea or severe
malnutrition should visit health centres because they may need additional Vitamin A according to the treatment schedule.
Mothers• Give mothers a dose of 200,000 IU of vitamin A if baby is 8 weeks old or less. • Ensure that the capsule is swallowed on site.• Encourage the mother to consume a balanced diet using locally available foods
and a variety of foods rich in vitamin A such as liver, eggs, oranges, yellow sweet potatoes, pumpkins, dark green leafy vegetables.
• Record in register mother who have received high dose vitamin A supplementation. Also indicate in Child Card that mother has been supplemented with vitamin A.
Iron and folate 1. Carers of children 6-59 months
2. Pregnant and Lactating mothers
Children• Give one dose at 6 mg/kg of iron daily for 14 days.• Avoid iron in a child known to suffer from sickle cell anemia• Avoid folate until 2 weeks after child has completed the dose of sulfa based
drugs (malaria treatment)Mothers• Give all pregnant women a standard dose of 200mg iron (Feso4) tablets three
times a day + 5 mg folate once daily OR offer multiple micronutrients• Promote use of anti-malarial interventions such as bed nets for preventing
anemia because malaria is often a major underlying factor. • Provide advice on food items and medicines that should not be taken together
with iron supplements since they may inhibit absorption such as milk, antacids, tea, and coffee.
• Treat anemia with treatment doses of iron for 3 months.• Refer severe cases of anemia to the nearest higher level of care if they are
in the last month of pregnancy, have signs of respiratory distress or cardiac abnormalities such as oedema.
• Provide advice on a balanced diet and emphasize on consumption of iron rich foods such as liver, red meats, eggs, fish, whole-grain bread, legumes and iron fortified foods.
• Promote consumption of vitamin C rich foods such as oranges, green vegetables, as they enhance the absorption of iron.
Hygiene and sanitation
1. Carers of children under five years.
2. General Community members
3. Household members
• Store uncooked food in a safe dry place • Protect food from insects, rodents and other animals • Avoid contact between raw food stuffs and cooked food • Keep areas where children are fed, or play, free from human and animal faeces • Keep all food preparation premises clean • Wash hands before preparing food for feeding children • Wash cooking utensils and wash fruits and vegetables • Use clean water • Cook food thoroughly • Avoid storing cooked food, instead, prepare food often. If cooked food is saved,
keep it as cool as possible. If previously cooked food is to be eaten, reheat it thoroughly before eating
• Wash the child’s hands before feeding • Use open feeding cups • Feed actively, that is supervise the child and continue offering food until the
child has enough
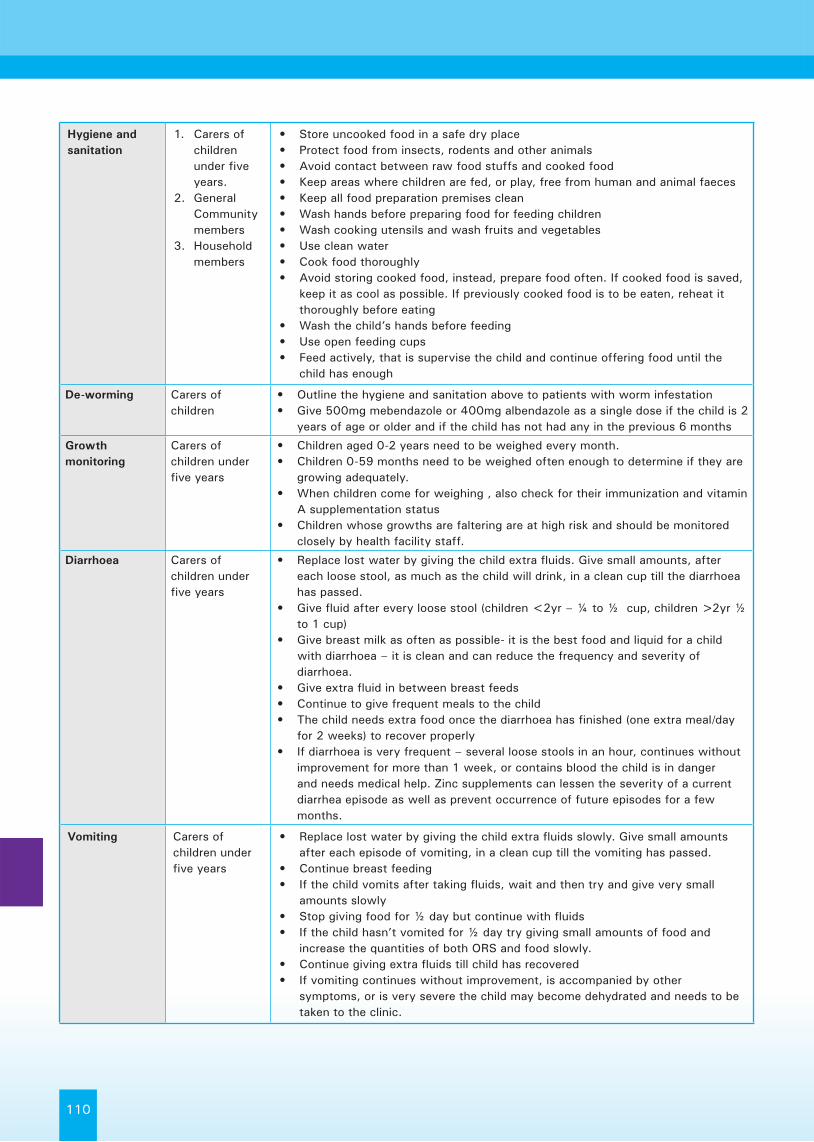
110
Hygiene and sanitation
1. Carers of children under five years.
2. General Community members
3. Household members
• Store uncooked food in a safe dry place • Protect food from insects, rodents and other animals • Avoid contact between raw food stuffs and cooked food • Keep areas where children are fed, or play, free from human and animal faeces • Keep all food preparation premises clean • Wash hands before preparing food for feeding children • Wash cooking utensils and wash fruits and vegetables • Use clean water • Cook food thoroughly • Avoid storing cooked food, instead, prepare food often. If cooked food is saved,
keep it as cool as possible. If previously cooked food is to be eaten, reheat it thoroughly before eating
• Wash the child’s hands before feeding • Use open feeding cups • Feed actively, that is supervise the child and continue offering food until the
child has enough
De-worming Carers of children
• Outline the hygiene and sanitation above to patients with worm infestation• Give 500mg mebendazole or 400mg albendazole as a single dose if the child is 2
years of age or older and if the child has not had any in the previous 6 months
Growth monitoring
Carers of children under five years
• Children aged 0-2 years need to be weighed every month. • Children 0-59 months need to be weighed often enough to determine if they are
growing adequately. • When children come for weighing , also check for their immunization and vitamin
A supplementation status• Children whose growths are faltering are at high risk and should be monitored
closely by health facility staff.
Diarrhoea Carers of children under five years
• Replace lost water by giving the child extra fluids. Give small amounts, after each loose stool, as much as the child will drink, in a clean cup till the diarrhoea has passed.
• Give fluid after every loose stool (children <2yr – ¼ to ½ cup, children >2yr ½ to 1 cup)
• Give breast milk as often as possible- it is the best food and liquid for a child with diarrhoea – it is clean and can reduce the frequency and severity of diarrhoea.
• Give extra fluid in between breast feeds• Continue to give frequent meals to the child • The child needs extra food once the diarrhoea has finished (one extra meal/day
for 2 weeks) to recover properly• If diarrhoea is very frequent – several loose stools in an hour, continues without
improvement for more than 1 week, or contains blood the child is in danger and needs medical help. Zinc supplements can lessen the severity of a current diarrhea episode as well as prevent occurrence of future episodes for a few months.
Vomiting Carers of children under five years
• Replace lost water by giving the child extra fluids slowly. Give small amounts after each episode of vomiting, in a clean cup till the vomiting has passed.
• Continue breast feeding• If the child vomits after taking fluids, wait and then try and give very small
amounts slowly• Stop giving food for ½ day but continue with fluids • If the child hasn’t vomited for ½ day try giving small amounts of food and
increase the quantities of both ORS and food slowly.• Continue giving extra fluids till child has recovered• If vomiting continues without improvement, is accompanied by other
symptoms, or is very severe the child may become dehydrated and needs to be taken to the clinic.

Guideline for Management of Acute Malnutrition
111
Dehydration Carers of children under five years
What causes dehydration?• Dehydration may be as a result of excessive vomiting and/or diarrhea How is dehydration diagnosed?• Child becomes lethargic (tired), thirsty, miserable, refuses to eat, eyes may
become sunken What are appropriate drinks for children with diarrhoea or vomiting?• Breast milk – the best fluid for the treatment of diarrhoea• Clean water (or boiled)• Oral Rehydration Salts from the clinic (made up with clean water) – helps to
replace lost salts• Homemade ORS (4 tsp sugar, ½ tsp salt, squeeze of lemon – in 1 litre of water) How to prepare and give ORS?• Add 1 sachet to 1litre clean (boiled and cooled) water (do not add to milk or
other fluids)• prepare in a clean bottle• give with a clean cup• children <2yr – ¼ to ½ cup, children >2yr ½ to 1 cup after each loose stool• continue until diarrhoea stops• Keep ORS cool and covered and use within 24hrs.
Community Sensitization
Community membersCommunity health workers,Community Volunteers
• What are the different terms used to describe malnutrition? • Is there a perceived difference between malnutrition and general sickness?• What are the perceived signs of malnutrition? These may include skinny legs/
arms and loose skin. Remember to include swollen children as oedema is not always associated with malnutrition
• What are the perceived causes of malnutrition? Is it food related? • How has the community traditionally dealt with malnutrition? Is knowledge of
treatment available to all? Are there specific people in charge of it? • Are there many cases of malnutrition in the community? How can these be
identified? Services and Other outreach activities• Explain what services are available for malnutrition (Outpatient Therapeutic
Program/OTP) for uncomplicated severe cases and inpatient hospital care for complicated cases of severe malnutrition and supplementary feeding for moderate cases
• Talk about the other outreach activities that are being carried out – immunisation, preventative services, health education, curative services as sickness can lead to weight loss and weight loss/malnutrition makes it more likely for the child to get an infection and to link with services for malnutrition
Utilization of Ready-to-eat foods (RUFs)
Carers of 6-59 months children
• RUFs are a food and medicine for very thin children (under 5 years) only. • RUFs should NOT be shared• RUFs are for children 6 – 59 months only • Give the child the RUF amount prescribed by the health worker • Always offer the child plenty of clean water or breast milk to drink while he or
she is eating the RUF• Wash children’s hands and face before feeding• Use soap for washing children’s hands and face • Keep the open sachet of RUF clean and covered and give to the child whenever
he/she demands for it.• Breastfeeding the child should continue when they are on RUF • CHILDREN BELOW SIX MONTHS SHOULD ONLY BE EXCLUSIVELY
BREASTFED and should not be given RUFs or any other foods or liquids• Before giving to the child to eat, knead the unopened sachet gently (do not apply
too much force) to allow for flow of the content.• Open the sachet using a clean device and then give to the child to eat.• RUFs should not be shared with other members of the family

112

Guideline for Management of Acute Malnutrition
Section 11Management of centres
and routine work
113

114
Management of the centre (SFP and OTP)
The protocols for treatment in the centres have been developed in order to be able to provide an adequate level of care, even in times of large influx of new admissions. By implementing the protocols correctly, the number of children who recover is very high and the number of those who die is generally low.
Individual care is important, but a good organization of the activities in the centre is key for the success of the programme. This includes having a good relation with patients, taking time and care to talk to the mothers, promoting a fluid flow of patients in the centre, and as well a good control of stock of drugs and food commodities and a good relationships with the community.
The minimum responsibilities of the centre manager are: Ensuring correct weight and height measurement by measurement team Ensuring correct registration in the registration book Ensuring all cards are filled in completely and correctly Ensuring correct weekly statistical update on admissions and discharges (tally sheets) Ensuring adequate medical check-up for all patients. Ensure correct follow up of treatment protocols, using Field Cards; this ranges from provision of the correct
drugs to the provision of adequate amounts of food and correct delivery of information to mothers on how to use the drugs or food.
Providing specific care for those who do not gain weight and/or develop medical complications. Adequate additional care and advice need to be given.
Ensuring adequate implementation of admission and discharge criteria Ensuring adequate stock management of drugs and food provided. Ensuring adherence to hygienic standards and make suggestions for improvements where needed Ensuring early identification of new malnourished children in the community and inclusion of these children in
the program Ensuring follow-up home visits during the week for those children requiring extra attention Ensuring all absentees and defaulters are followed up by outreach workers, and are accounted for Ensuring community involvement in all centre facilities
Flow of patients (SFP, OTP):
The basic flow of patients is standard (see schema) but you can adapt it to the situation in your clinic. This is an example of patient and activity flow in an OTP. Each of them is explained in more detail in this section:
Waiting area: Screening Sugared water Promotion activities
Exit
Medical check-up. Drug and nutrition prescription
Drug and RUTF delivery
Vaccination
Measurements W/H, MUAC, Oedema
Counselling
Register

Guideline for Management of Acute Malnutrition
115
Organising each of the steps of the flow:
1. The waiting area:
These recommendations are valid for any type of facility (SFP, OTP, SC).
• The waiting area should be a comfortable place for the children and their carers. It should always be shaded.• Ensure that water is available for those waiting.• Provide sugared water to patients that look tired (see section on Hypoglycaemia for preparation).• Inform them of the waiting time before they will be seen.• Make water and soap available for mothers to wash their hands and child’s hands.• Visit the waiting area regularly, and identify those children that are ill or very weak. Examine them first!• Avoid accumulation of people next to the measurement or the examination areas.• In OTP and SC, you can start the appetite test of those patients that do not look very ill while they wait.
It is important that the parent or caregiver who attends the health facility with a child is acknowledged for the visit. This is particularly important when the child is not considered malnourished by the weight and height anthropometry taken at the health centre. Otherwise, the community can become disgruntled with the service, particularly if mothers travel a long distance. It can seriously affect uptake of the services and negatively impact on coverage. Every mother should be congratulated for taking good care of her child.
2. Measurement area:
• Always ensure that there is enough room to work, and people waiting to be measured are at a reasonable distance.
• Ask the mother of the child and/or a volunteer to help with measurements (remember: height and weight measurements need two people to be done correctly!).
• Check every day that the measurement equipment is in good shape, and order replacements with enough time if you think that something is not working correctly.
• Keep the measurement area tidy. Always write the measurements in the right form – do not write them on just any piece of paper, as these may be lost and create confusion!
3. Registration and admission:
Admit the child according to the admission criteria, issue with an identification wrist-band. Fill in the Register book. Fill in the OTP chart for new admissions. Take the card from the file for the follow ups!
Give explanations concerning the functioning of the OTP to the caregiver:
Ensure that the carer understands:• Why the child is admitted• What the treatment will consist of (medication and therapeutic food)• Frequency and duration of visits (weekly, expected length of stay in the program etc).• Hygiene rules• Discuss any problem the carer might have concerning the treatment so that a solution can be found• Importance of continued breastfeeding• Feed the child at regular intervals during the day and also at night, especially if they do not finish
Some of these explanations will be repeated to the mother when they receive the food. It is important that they understand everything and that all questions are answered before they leave the centre.

116
Children who are not admitted:
• Explain carefully to the mother that the child is not malnourished.• Make it clear that there are no other reasons why the child is not admitted (for example: show them that
other people from their same clan have been admitted, to avoid misinterpretation).• Check if there is any medical complaint that needs treatment in the clinic.• Tell the carer to come back if the child has any problems in the future.• Vaccinate the child (if feasible).• If possible, give in addition a piece of soap or other products supplied by your organisation.
4. Medical consultation (check other parts of this protocol for detail):
Check other sections of these guidelines for details on how to run a medical consultation (FC 5).
• ALWAYS examine every child (new admissions and follow-ups) for nutrition and medical history.• Information should be recorded in the card. In OTP, follow the patient’s card as a guide for the information that
needs to be collected, and write the answer to every box.• ALWAYS ask the mother for any complaints that the child may have, even if not related to malnutrition.• In OTP, CHECK APPETITE on the day of admission and for the next few distributions. Thereafter, appetite need
only be checked if the child presents a problem (see FC 3)• ALWAYS ask how the child is taking the food at home, ask the carer to explain how she/he organises the feeds.• Ask for treatments that the child may be taking for other conditions.• ALWAYS make a judgement about the evolution of the child: is the child’s health and nutritional status improving?
Is it not evolving or is it deteriorating? What actions should be taken? TAKE A DECISION!• Evaluate if the child needs to be discharged, if the child presents signs of failure to respond (FC 14 and FC 21),
if the child needs transfer to other centre, etc.
5. Distribution of drugs and foods
Check appropriate sections of the guidelines for amounts of foods to be distributed and routine medication.
At the start of the day, and before starting the visits: • Be sure to have all the forms with the dosage for the drugs and foods in the table • Prepare all the drugs, water, foods, cards, etc.
• Start systematic treatment for new admissions (Vitamin A, Amoxicillin, etc.)• Supervise how the child takes the treatments that need to be taken in the OTP (Vitamin A, Albendazole, first
dose of antibiotics, ….)• Give Albendazole for children on the second visit (OTP).• Give Malaria treatment if the test was positive.• Vaccinate for Measles new admissions (unless they have been already vaccinated or the centre has no vaccines).• Check in the card if the child has been prescribed other drugs and give them.• Collect empty sachets from the previous week and count them (OTP).• Ask the mother if she had any problem when giving the RUTF/CSB to the child, or with the drugs.• Give the appropriate amount of RUTF/CSB sachets to the mother.• Explain the mother how to prepare CSB or how to take RUTF at home (FC 10 and FC 16)• Explain the mother how to give the drugs at home (antibiotics).
Check that the mother has understood everything by asking her to repeat the messages that you have given to her. Respond any question of doubts from the mother before letting her go.
CHECK that the patient card is correctly filled.CHECK the OTP card. If it is not complete, ask your colleagues to complete it.File the OTP card for the next session!

Guideline for Management of Acute Malnutrition
117
Organising the cards:
At the beginning of the session, all the OTP cards of the children in treatment should be in the Registration area – classified by registration number. After the child has been seen, the card is filed again.
At the end of the session, check the OTP cards that have not been used. These are those for the children that did not come. Write “Absent” in the column corresponding to that day. If a child is in the third week “Absent”, discharge the child and file the OTP card with the other discharges.File the cards of the children that have been discharged, to be used in supervision.
Field Card 38. Routine work at the OTP – check list
This card summarizes the main actions to take for each patient during OTP activities. Use it as a check list, to be sure that everything has been done correctly.
Routine work for new admissions (first visit):
Assessment:1. Give priority to cases that look bad and urgent cases.2. Welcome the child and the carer and explain that you need to measure the child to know if he can be in the
programme.3. Check for oedema4. Measure and record MUAC.5. Take the patient’s weight and height, and calculate weight-for-height (Z-scores).6. DECIDE if the patient is malnourished or not. If MAM, send to TSFP (if available). 1. If not malnourished, congratulate for taking care of the child, explain why the child was not admitted,
and encourage them to come if the situation changed.7. Do the Appetite test. Write down the results. 1. If the child could have complications, send the patient to the nurse for assessment.8. DECIDE if the patient should be admitted at OTP or SC.9. Explain the diagnosis to the carer. Tell him/her the consequences of the diagnosis. 1. If admitted to OTP, explain what will be the following steps of the visit for today and for the following
visits. 2. If the child needs SC, explore with the carer the possibility of transfer. Explain the situation to the carer,
and if transfer not possible, follow instructions about complicated SAM in OTP.
Registration:9. Assign registration number and prepare a card.10. Register the child in the registration book, including all necessary information to identify the patient’s residence.
Write down in the registry the information provided by the assessment.11. Write all the necessary information in the patient’s OTP card.
Medical consultation and distribution of drugs/RUTF:12. Welcome the mother and resolve any questions that she has at this point.13. Do the consultation following the steps in the OTP card:14. Check that all the identification information and the anthropometry section are complete. If not, ask the
registration to provide the details.15. Complete History section by asking the mother.16. Examine the patient and complete the Physical examination section. 1. Go through the list of complications that require SC treatment. If the child presents complicated
SAM, consider transfer to SC with the mother.17. Prescribe Routine medicines.

118
18. Calculate the amounts of RUTF to be given to the carer until the next visit.19. Fill in the Ration card that the carer will take home.20. Explain to the mother what are your conclusions and the treatment that you are going to give.21. Send the patient to the assistant, to give the single dose of each drug, and first dose of antibiotics. Give the
RUTF.22. Provide explanations on how to take the drugs and the RUTF, using Field Card 16.23. Check that the carer understands well all the instructions, and that she knows the date of next visit.24. Ask the mother if she has questions, and resolve them. Assure her that the child will get better soon.
Routine work for all patients (in following visits):
Assessment and Registration:1. Welcome the child and the carer and explain that you need to measure the child to see what is his/her evolution.2. Check for oedema3. Measure and record MUAC.4. Take the patient’s weight and height, and calculate weight-for-height (Z-scores).5. Do the Appetite test if needed (necessary for visits 1 and 2, and afterwards if the patient is not gaining weight
or presents with another problem). Write down the results.6. Write down all the information in the Register book and in the patient’s card.
Medical consultation:7. Welcome the mother and resolve any questions that she has at this point.8. Do the consultation following the steps in the OTP card:9. Check that all the identification information and the anthropometry section are complete. If not, ask the
registration to provide the details.10. Complete History section by asking the mother.11. Explore the patient and complete the Physical examination section.12. Prescribe Routine medicines if still needed (week 2).13. Check the evolution of weight, oedema and the clinical status of the patient. 1. If child is not gaining weight, do the Appetite test, and explore what may be reasons with carer. 2. Go through the list of complications that require SC treatment. If the child presents complicated SAM
or failure to respond to treatment, consider transfer to SC with the mother.14. Calculate the amounts of RUTF to be given to the carer until the next visit.15. Fill in the Ration card that the carer will take home.16. DECIDE if the patient needs to be classified as Cured or Non-response, or continue treatment.17. Explain to the mother what are your conclusions and the treatment that you are going to give.18. Send the patient to the assistant to give the RUTF. 1. Collect the empty sachets from previous week. If they don’t have them, explain the importance of
bringing them every week, but do not threaten the mother if she can’t do it.19. Remind the explanations on how to take the drugs and the RUTF, using Field Card 16.20. Check that the carer understands well all the instructions, and that she knows the date of next visit.21. Ask the mother if she has any questions, and resolve any doubts. Reassure her that the child will get better
soon.

Guideline for Management of Acute Malnutrition
119
Organisation of work in the SFP / OTP
Here are some basic tips on how to organise the work on the SFP or OTP, and the main tasks that need to be accomplished. Each centre and organisation may have a different way of organising these.
Flow of patients:
It is important to organise a smooth flow of patients which limits waiting time and ensures that all patients are seen and properly looked after. This chapter presents a suggestion of flow of patients and routine activities for each of the stations.
Health and nutrition education:
Health and nutrition education is usually provided for all patients and carers while waiting to be seen.
Reporting statistics – Monitoring:
Reviewing the activity is part of daily activity. It is usually done when all patients have left the centre.It includes: checking the register book to check if all information is written correctly for patients (for example, that no patients are left without an exit criteria, and there is no missing information from the admission day), checking the cards of the patients that were absent that day, to see which of them needs to be classified as defaulter and those absent who require a home visit. See chapter 9 for more information.
Stock control:
The stocks of RUTF and routine drugs need to be checked weekly in order to avoid running out of any key item and to ensure accountability for these expensive items. This needs to be done as well for stocks of cards and other essential material. Each centre should designate a working day to check supplies and to make reports, as well as to prepare the next stock request according to actual figures of the week.
Home visiting and monitoring:
Some patients may need to be monitored through visits by outreach workers at their homes. This may be necessary when there is an unexplained lack of weight gain. The outreach worker can discuss issues with the carer, assess home environment and adapt messages to improve treatment.
Defaulter tracing:
All absences from outpatients should be followed up at their homes by outreach workers, volunteers, key community figures or other carers. It is important to gain an understanding of the reason for absence and to encourage return, without reprimanding the absentee. Information on the reasons for absence can be used to improve the organisation of the programme and make it more accessible and appropriate. When resources for community outreach are limited, the nurse may decide which patients need to be traced back to their homes, based on their absence or on their lack of evolution under treatment.

120
FIELD CARD 39: Discharge Procedures
It is important to complete the discharge procedures, both for patients that have completed the treatment as cured and for those that are discharged as non-respondents or transferred to a different centre.
• Give feedback to the parent/caregiver on the patient’s final outcome. Make sure that the carer understands why the child is being discharged.
• Refer the patient to the appropriate centre (from SC to OTP and from OTP to SFP). Ensure the parent/caregiver understands the importance of continuing treatment at the other centre, and knows when and where they need to attend it.
• In OTP, give a final ration of seven (7) packets as a weaning off ration.• Fill in date and reason of discharge on the register.• Store the patient’s card with the other exits, for future reference (monthly reports or supervision).• Advise parent/caregiver to return to the centre if child becomes sick or is losing weight again.
If the child was cured: Congratulate the carer. Some carers will receive the discharge as bad news, because they appreciated receiving the food distributions. Explain that the child is cured and needs to return to eating normal food – or continue treatment in the other centre. Let them know that they are not being “expelled” from the programme for a bad reason, and that they are very welcome to come back if the child needs it.
If the child was non-response: Do not be judgemental with the carer. Explain that the child was not evolving correctly, and that the centre has made the necessary medical and social investigations but could not find a reason for the lack of weight gain. Encourage them to come back if the state of the child deteriorates again, or to go to an Inpatient centre.

Guideline for Management of Acute Malnutrition
Section 12Patient’s cards and reporting system
121

122
SFC RATION CARD
Serial Number: Name of partner/Centre:
Region: District: Village:
REGISTRATION
WEIGHT FOLLOW-UP
Date
Weight
MUAC
Date of Admission:
Weight(kg): Height(cm): Z-score Weight/Height:
MUAC(cm): Oedema: Weight to Reach (Kg):
Name of Mother/Caregiver:
Name of Child: Age: Sex:
Address:
SYSTEMATIC TREATMENT
Measles Vaccination date:
Vitamin A dose:
Date:
Albendazole dose:
Date:
Other (Specify):

Guideline for Management of Acute Malnutrition
123
Magac canuga (name of child) DIW. No
Tuuladda (village)
Da'da (bilo) (age:mths)
Jinsi (sex)
M F
Sababta loo qaatey(admission)
Toos uga yimid bulshada ka SFP ka TFC/SC
Dib u seexin (sib u soo celin)
(relapse)
Tirada guud ee guri-guri masuulka (#HH)
Mataano (twin)
haa mayaFogaanta guriga
(saacado) (distance:hrs)
Magaca daryeelaha guud ee bukaaanka
(name of carer)
Daryeelaha labaad ee bukaanka
(2nd carer)
Guud ahaan rashiinka: masuulka guriga diwaan
gashanhaa maya
Miisaanka (kg) Dheerer (cm) WH z-score MUAC (cm)
Nooca jufinta (admission criteria) Barar/oedema <3 z-score MUAC
<11.5cmKale: cadeey (other: specify)
Shuban (diarrhoea)
haa maya 1-3 .4-5 >5
Matag (vomiting)
haa maya haa maya
Qufac (cough)
haa maya
Cunta qaadasho (appetite)
fiican(good)
liito(poor)
midnaba(none)
Naas-nuujin (breastfeeding)
haa maya
dhibaatooyinka kale (problems)
Heerka Neefsashada (# min)
<30 30 - 39 40 - 49 50+ haa maya
Heerka kulka 0C (temp.) caadi cadaan
Indhaha(eyes) caadi godan Soo baxsan ma jiro dhex-
dhexaad daran
Dhagaha (ears) caadi Soo baxsan Afka
(mouth) caadi nabro cad-cadaan
Qanjirada (lymph nodes) ma jiro luqunta kilkisha laabato Awood daro
(disability)haa maya
Isbedelada Maqaarka (skin changes) ma jiro cadho xubka Gacmaha/ciribta
(hands/feet) caadi qaboow
Bukaanka: daawa taariikh daawa taariikh
Vitamin A
Amoxycillin AS (artesunate)
Aragtida labaad (2nd visit):
Mebendazole
taariikh
Measles haa maya
taarikh qaadasho taarikh qaadashoDaaweeynta Kale (Other Medication)
daawa daawa
Talaal buuxo (fully immunised)
lab-dox / barar
Daaweeynta Bukaan socodka iyo daaweynta u socota (Routine Admission Medication)qaadasho qaadasho
Antimalarials: SP
Haddii barar jiro, intee le'eg yahay? ( if oedema, how long swollen?)
Baaris Guud (Physical Examination)
Noqashada xabadka (chest retractions)
Xirib/calaacalaha (conjunctiva/palms)
Fuuq bax (dehydration)
Diiwan gelinta & Cabiraad (Admission Anthropometry)
Taarikh (History)
Saxaro/maalin (stools/day)
Socodka Kaadida (passing urine)
Taariikhda la diiwaangeliyey/la qaatey
TFC/SC diidmo(refused transfer)
Cunto Qeybnta Guud (General Ration)Haddii ay Haa tahay,
goormaa u danbeeysay in raashin ay helaan
(If yes, when last received ration)
FAAHFAAHINTA : BARNAAMIJKA DAWEEYNTA iyo DIIWAAN GELINTA BUKAAN SOCODKA
/ /
Aaga (area)

124
OTP KAAR - LA SOCOD
Magaca (name)
Usbuuc (week) Diiwangelinta 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17Taariikh (date)
Culeys (kg) (weight)
Culeys lumay * (H/M) (weight loss) * *
Dherer (cm)(height)
W / H z-score
MUAC (cm)
Barar (+ ++ +++)(oedema)
Shuban (# maalmo) (diarrhoea)
Matag (# maalmo) (vomiting)
Qando/xumad(# maalmo) (fever)
Qufac (# maalmo) (cough)
Heerka kulka (0C) (temp.)
Heerka neefsashada(# / min) (RR)
Fuuqbax(H/M) (dehydrated)
Dhiigla'aan (H/M) (anaemia)
Maqaarka oo jirado (H/M) (skin infection)
P'nut itixaan Fiican /Liito/Diiday
Plumpynut/ tirada baakada (# units)
Howsha loo baahan yahay in la qabto **
(H/M) (sida hoose) (action needed)
Daaweeyn kale(eega kaarka hortiisa) (other
medication)Magaca baaraha
(name examiner)WAXA SOO BAXA **
(OUTCOME)
Baaris Guud (Physical Examination)
** A=Maqan D=Fakaday (3 maqnaasho oo xirir ah) T=Badel TFC/SC X=Dhintay C=Daawoobay RT=Diiday Badol HV=Booqasho guri NC=Ma daaweeysmin (A=absent D=default T= transfer TFC/SC X=died C=cured RT= refused transfer HV= home visit NC=noncured)
** Talaabadii laga qaaday markii lala socday (taariikhda) (Action taken during follow-up: include date)
DIW No
Cabiraad (Anthropometry)
* Isbedelida culeys: MARASMICS: haddii uu ka hooseeyo miisanka seexinta ee usbuuc 3 la xariri shaqaalaha dibada. Haddii uu soo kordheeyn miisaanka usbuuca 5 aad la xariiri TFC/SC
Taarikh (History)

Guideline for Management of Acute Malnutrition
125
Goobta OTPga
Magaca Ilmaha Ciwaanka
Magaca masuulka Ilmaha
Tarikh Miisan (KG) Dherer (CM) CWCG Barar(+ ++ +++)
Plumpynut(# units)
Tarikh Miisan (KG) Dherer (CM) CWCG Barar(+ ++ +++)
Plumpynut(# units)
Faalo
Cunto kale
KAARKA RAASHINKA OTPNambarka Diiwaanka
Cunto kale

126
Age Sex
1 2 3 4 5 6 7 8 9 10 11 12
11/22/10
1 2 3 4 5 6 7 8 9 10 11 12
7-10 days
TESTS
on discharge TYPE
RESULTS
Com
men
ts /
NG
tu
be
/Res
omal
Temperature
Respirations
Stools
Vomit
Date of Discharge OTP of Discharge
Milk/RUTF
Amount per meal (6 meals per day)
Total per day
MEA
L TI
MES
07:00 AM
10:00 AM
01:00 PM
04:00 PM
07:00 PM
10:00 PM
SPEC
IAL
MED
ICIN
ES
Measles Vaccine
RO
UTI
NE
MED
ICIN
ES
DATE
Amoxycillin
Fansidar
Artesunate
Vitamin A
Albendazole or Mebendazole
AN
THR
OP
OM
ETR
IC C
HA
RT
DATE
Height (cm)
Weight (kg)WHZ
(z-score)MUAC (mm)
Oedema (+ ++ +++)
STABILISATION CENTRE CARD
Stabilisation Centre Registration Number Referred From
NameAdmission Criteria

Guideline for Management of Acute Malnutrition
127
MED
ICA
L FO
LLO
W U
P F
OR
M S
CN
AM
E:
N
UM
BER
:DATE
SIGNATURE
DATE
SIGNATURE

128
Feeding Programme Referral CardKAARKA GUDBINTA BARNAAMIJKA QUUDINTA
Date: Partner Program:
Name of the beneficiary:
Reason for Referral:
SEVERELY MALNOURISHED (MUAC<11.5cm)
MODERATELY MALNOURISHED (MUAC <12.5)
NEED MEASLES VACCINATION
PREGNANT/ LACTATING WOMEN
Other (Specify):
To be refer to (Goobta Barnaamijka)
Remarks:

Guideline for Management of Acute Malnutrition
129
1.
C
OO
PER
ATIN
G P
AR
TN
ER
INFO
RM
ATIO
N
1.1
Reg
ion
1.2
Dis
tric
t1.
3 C
oope
ratin
g Pa
rtne
r 1.
4 W
FP S
ub-o
ffic
e
1.5
Fina
l D
istr
ibut
ion
Poin
t1.
6 R
epor
ting
Mon
th1.
7 R
epor
t Su
bmis
sion
Dat
e
2.
B
EN
EFI
CIA
RY
INFO
RM
ATIO
N
2.1.
2A
dmis
sion
s
1.8
CP
Staf
f Mem
ber
Nam
e an
d Ti
tle
1.9
CP
Staf
f Mem
ber
Pho
ne N
umbe
r1.
10 C
P St
aff M
embe
r E
mai
l
Chi
ldre
n (6
-59
mon
ths)
Wom
en (P
regn
ant a
nd
Lac
tatin
g)To
tal
Gir
lsB
oys
2.1
Ben
efic
iari
es
2.1.
1 Fr
om la
st m
onth
2.1.
2A N
ew A
dmis
sion
s 2.
1.2B
Rea
dmis
sion
s2.
1.2C
Ref
erre
d fr
om o
ther
TSF
P2.
1.2D
Tra
nsfe
r fr
om O
TP/
SC2.
1.2E
Tot
al A
dmis
sion
s
2.1.
3 D
isch
arge
s
2.1.
3A C
ured
2.1.
3B N
on-R
espo
nse
2.
1.3C
Tra
nsfe
r ou
t2.
1.3D
Def
aulte
rs2.
1.3E
Dea
ths
2.1.
3F T
otal
Exi
ts
2.1.
4 To
tal e
nd o
f the
mon
th
2.2
Adm
issi
ons
Cri
teri
a us
ed a
t the
fa
cilit
y
2.2.
1 C
hild
ren:
MU
AC
(ti
ck o
ne)
>
=11.
0 cm
, < 2
1.5
cm
>=
11.5
cm
, <1
2.5
cm
2.2
.2 C
hild
ren:
W
eigh
t for
Hei
ght
(tick
one
)
W
eigh
t for
Hei
ght %
Med
ian
W
eigh
t for
Hei
ght Z
Sco
re W
HO
W
eigh
t for
Hei
ght Z
Sco
re N
CH
S(s
peci
fy u
pper
and
low
er th
resh
olds
)
2.2.
3 W
omen
: (ti
ck o
ne)
M
UA
C<2
1 cm
othe
r (s
peci
fy)
M
UA
C<2
3 cm
2.3
Perf
orm
ance
In
dica
tors
2.3.
1 Av
erag
e w
eigh
t gai
n (c
hild
ren
who
rec
over
ed in
g/k
g bo
dy w
eigh
t/day
)2.
3.2
Aver
age
stay
(day
s)2.
3.3
% C
ured
2.3.
4 %
Def
aulte
d2.
3.5
% D
eath
Not
e: T
he S
PHE
RE
stan
dard
s are
Cur
ed: >
75%
, def
ault
<15%
, dea
th<3
%

130
IMPL
EMEN
TIN
G A
GEN
CYRe
port
pre
pare
d by
OTP
SCM
ON
TH /
YEA
R
FRO
M -
---
TO
OTP
- re
fers
to
out
pati
ent
or a
mbu
lato
ry c
entr
es;
SC-
refe
rs t
o st
abili
sati
on c
entr
es o
r in
-pat
ient
fac
iliti
es
G
rey
cells
con
tain
for
mul
ae,
DO
NO
T FI
LLPL
EASE
, re
ad c
aref
ully
exp
lana
tion
s be
fore
fill
ing
the
form
OU
TRe
adm
iss
afte
r de
faul
t (D
1)
Tran
sfer
fr
om T
FC
or f
rom
O
TP (
D2)
Tran
sfer
to
OTP
or
to T
FC
(E1)
< 6
mon
ths
00
0
6-59
mon
ths
00
0
>5 y
ears
00
0
TOTA
L0
00
00
00
00
00
00
0
#DIV
/0!
#DIV
/0!
#DIV
/0!
#DIV
/0!
F =
A +
B -
C +
D1
+ D
2 -
E1
OTH
ER IN
DIC
ATO
RS(o
nly
for
child
ren
6-59
mon
ths
cure
d)
010
0%#D
IV/0
!#D
IV/0
!Av
erag
e w
eigh
t ga
ing/
kg/d
ayg/
kg/d
ay
Aver
age
leng
th o
f st
ayda
yda
y
AD
DIT
ION
AL
INFO
RMA
TIO
N (
for
6-59
mon
ths-
old
only
)
RELA
PSES
MO
NTH
LY S
TATI
STIC
S RE
PORT
- T
HER
APE
UTI
C PR
OG
RAM
MES
SITE
DIS
TRIC
TTY
PE O
F PR
OG
RAM
ME
OPE
NIN
G D
ATE
Esti
m.
U5
pop.
Gro
up a
ge
Tota
l be
ginn
ing
of
the
mon
th
(A)
New
Adm
issi
ons
(B)
Dis
char
ges
(C)
TOTA
L D
ISCH
ARG
E (C
)
Oth
er m
ovem
ents
Tota
l end
of
the
m
onth
(F)
W/H
<-3z
-sc
ore,
M
UAC
<115
mm
OR
MU
AC <
16
0mm
OED
EMA
(B2)
OTH
ER
ADM
ISS
(B3)
TOTA
L N
EW
AD
MIS
SIO
N (
B)
CURE
D(C
1)D
EATH
(C2)
DEF
AULT
ER
(C3)
NO
N-
CURE
D
(C4)
IN
ADM
ISSI
ON
SM
ALE
FEM
ALE
Ave
rage
wei
ght
gain
and
ave
rage
leng
th o
f st
ayM
aras
mus
Kw
ashi
orko
rN
b:N
b:
Nb:
Nb:
num
ber
of R
UTF
sac
hets
us
edba
lanc
e of
RU
TF in
sto
ck
DIR
ECT
ADM
ISSI
ON
S IN
SC
/TFC

Guideline for Management of Acute Malnutrition
131
Notes
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________



















