
GUIDANCE ON DEATH, STILLBIRTH & CREMATION · PDF fileGUIDANCE ON DEATH, STILLBIRTH &...
57
GUIDANCE ON DEATH, STILLBIRTH & CREMATION CERTIFICATION RF Preliminary - DHSSPS 315-008-001
Transcript of GUIDANCE ON DEATH, STILLBIRTH & CREMATION · PDF fileGUIDANCE ON DEATH, STILLBIRTH &...

GUIDANCE ONDEATH,STILLBIRTH& CREMATIONCERTIFICATION
RF Preliminary - DHSSPS 315-008-001

RF Preliminary - DHSSPS 315-008-002
4
2
3
5
6
7
8
9
10
1
11
RF Preliminary - DHSSPS 315-008-003

Produced by:Department of Health, Social Servicesand Public Safety
Telephone: (028) 9052 2359Textphone: (028) 9052 7668www.dhsspsni.gov.uk
August 2008 Ref: 20/2008
RF Preliminary - DHSSPS 315-008-004

RF Preliminary - DHSSPS 315-008-005
M.C.C.D.
Why do we have certification relating to death?
Who can complete the Medical Certificate of Cause of Death?
Deaths and the coroner
Registrar’s extra-Statutory list of diagnoses which should be referred to the coroner
Who Reports a death to the coroner?
When to Contact the coroner?
Sample Pro-forma
A step-by-step to completing a MCCD. Before you start - Rules for Good Practice.
CREMATION
Cremation Forms
Reasons for cremation certification
Who should complete cremation forms?
How to complete cremation Form B side 1
How to complete cremation Form B side 2
How to complete cremation Form C – confirmatory medical certificate
STILLBIRTH
Stillbirth certificate
What is a stillbirth?
3
5
7
8
15
17
19
21
37
39
41
43
45
47
50
51
Contents
RF Preliminary - DHSSPS 315-008-006

RF Preliminary - DHSSPS 315-008-007

Why do we have certification relating to death? Page 3
For the Family
So that:
• a deceased’s family will be able toregister the death or stillbirth;
• the register can provide apermanent legal record of the factof death or stillbirth;
• the registrar can provide a burialcertificate to enable the family toarrange for burial;
• the registrar can provide copies ofthe entry in the register commonlyknown as the death certificate,which enables the family to settlethe deceased’s estate.
The death certificate includes an exactcopy of the cause of death informationfrom the Medical Certificate of Causeof Death (MCCD) or stillbirthcertificate. This provides anexplanation of how and why theirrelative died. It also gives them apermanent record of information about
their family medical history, which maybe important for their own health andthat of future generations.
For Society
Statistical information on deaths andstillbirths by underlying cause isimportant as it is used for:
• monitoring the health of thepopulation;
• designing and evaluating publichealth interventions;
• recognising priorities for medicalresearch and health services;
• planning health services; and
• assessing the effectiveness ofservices.
Why do we have certification relatingto death?
RF Preliminary - DHSSPS 315-008-008

RF Preliminary - DHSSPS 315-008-009

Who can complete the Medical Certificate of Cause of Death? Page 5
Registered Medical Practitioners havea legal duty to provide, without delay, acertificate of cause of death if, to thebest of their knowledge, that persondied of natural causes for which theyhad treated that person in the last 28days.
This is a statutory legal duty on alldoctors based on Births and DeathsRegistration (Northern Ireland) Order1976, independent of any employmentcontract.
In hospital, there may be severaldoctors in a team caring for thepatient who will be able to certify thecause of death. It is ultimately theresponsibility of the consultant incharge of the patient's care to ensurethat the death is properly certified.Foundation level doctors should notcomplete medical certificates of causeof death unless they have receivedtraining. Discussion of a case with a
senior colleague may helpclarify issues about completionof an MCCD or referral to acoroner.
In general practice, morethan one GP may havebeen involved in thepatient’s care and sobe able to certify thecause of death.
A doctor who had notbeen directly involvedin the patient’s careat any time during theillness from which theydied cannot certify thecause of death, but heshould provide thecoroner with anyinformation thatmay help todetermine thecause of death.
Who can complete the Medical Certificateof Cause of Death?
RF Preliminary - DHSSPS 315-008-010
Before you proceed with completing a Medical Certificateof Cause of Death ask yourself this question -
Does this Death have to be reported to the coroner?
RF Preliminary - DHSSPS 315-008-011
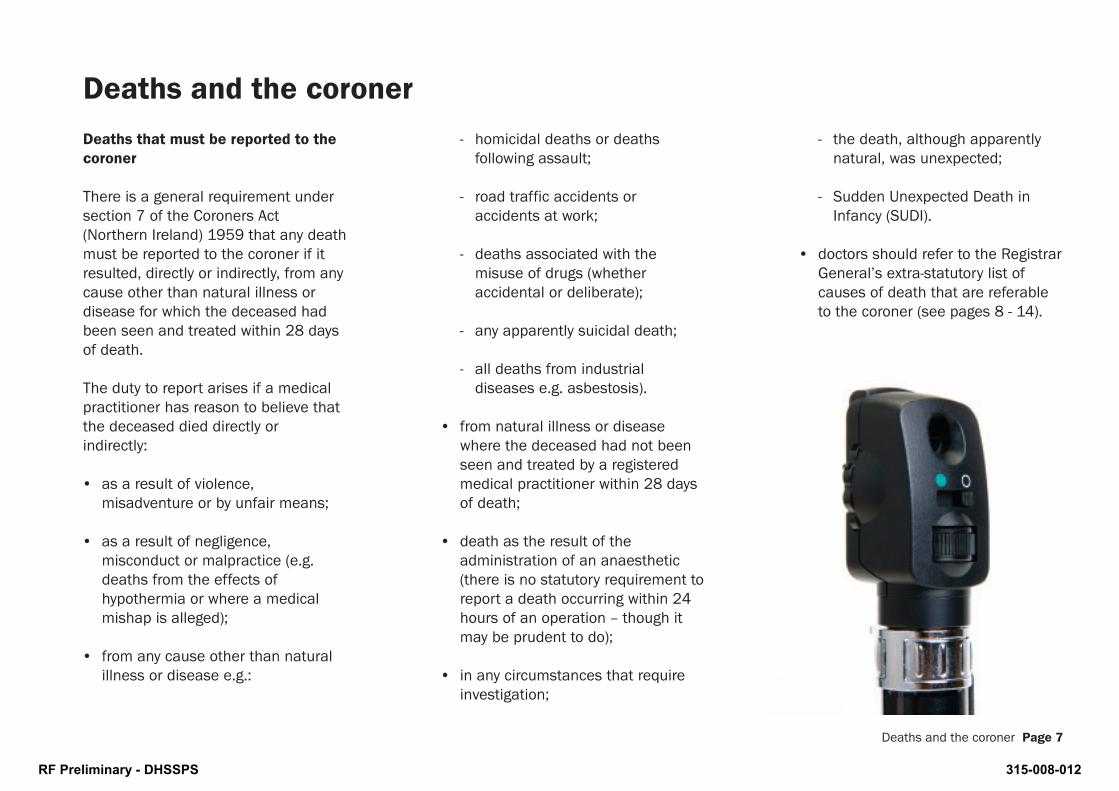
- homicidal deaths or deathsfollowing assault;
- road traffic accidents oraccidents at work;
- deaths associated with themisuse of drugs (whetheraccidental or deliberate);
- any apparently suicidal death;
- all deaths from industrialdiseases e.g. asbestosis).
• from natural illness or diseasewhere the deceased had not beenseen and treated by a registeredmedical practitioner within 28 daysof death;
• death as the result of theadministration of an anaesthetic(there is no statutory requirement toreport a death occurring within 24hours of an operation – though itmay be prudent to do);
• in any circumstances that requireinvestigation;
- the death, although apparentlynatural, was unexpected;
- Sudden Unexpected Death inInfancy (SUDI).
• doctors should refer to the RegistrarGeneral’s extra-statutory list ofcauses of death that are referableto the coroner (see pages 8 - 14).
Deaths and the coroner Page 7
Deaths that must be reported to thecoroner
There is a general requirement undersection 7 of the Coroners Act(Northern Ireland) 1959 that any deathmust be reported to the coroner if itresulted, directly or indirectly, from anycause other than natural illness ordisease for which the deceased hadbeen seen and treated within 28 daysof death.
The duty to report arises if a medicalpractitioner has reason to believe thatthe deceased died directly orindirectly:
• as a result of violence,misadventure or by unfair means;
• as a result of negligence,misconduct or malpractice (e.g.deaths from the effects ofhypothermia or where a medicalmishap is alleged);
• from any cause other than naturalillness or disease e.g.:
Deaths and the coroner
RF Preliminary - DHSSPS 315-008-012
Page 8 Deaths and the coroner
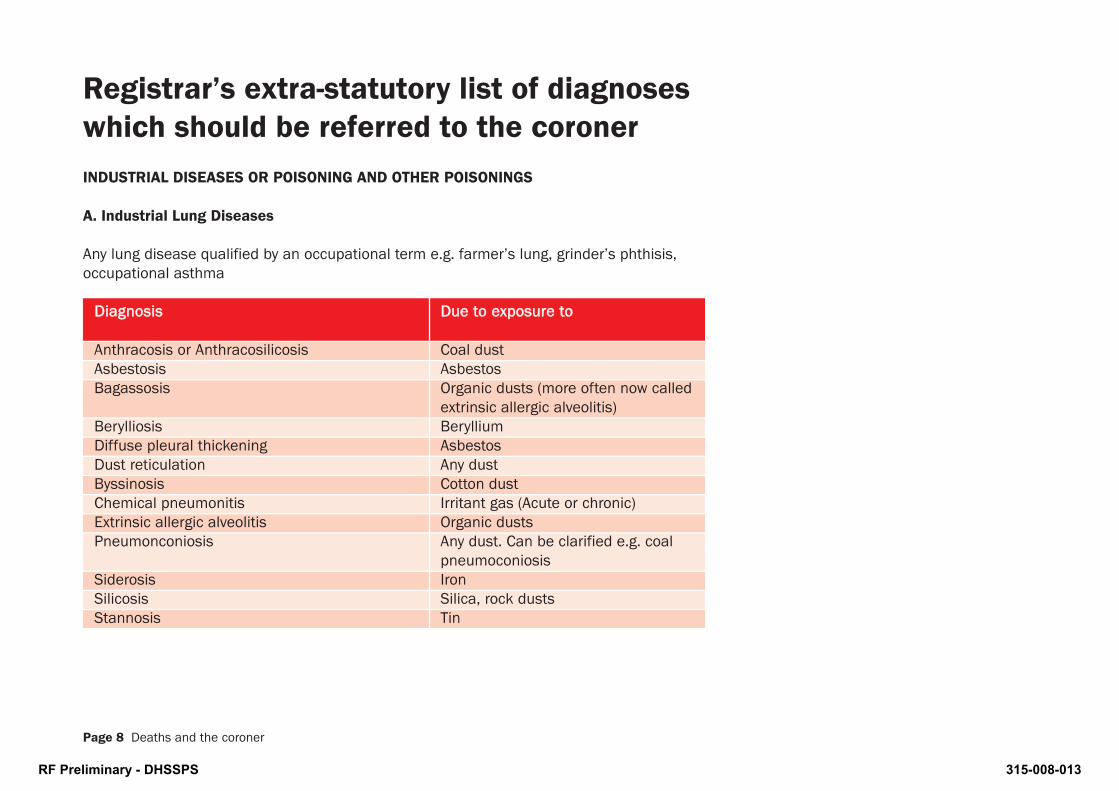
INDUSTRIAL DISEASES OR POISONING AND OTHER POISONINGS
A. Industrial Lung Diseases
Any lung disease qualified by an occupational term e.g. farmer’s lung, grinder’s phthisis,occupational asthma
DDiiaaggnnoossiiss DDuuee ttoo eexxppoossuurree ttoo
Anthracosis or Anthracosilicosis Coal dustAsbestosis AsbestosBagassosis Organic dusts (more often now called
extrinsic allergic alveolitis)Berylliosis BerylliumDiffuse pleural thickening AsbestosDust reticulation Any dust Byssinosis Cotton dustChemical pneumonitis Irritant gas (Acute or chronic)Extrinsic allergic alveolitis Organic dustsPneumonconiosis Any dust. Can be clarified e.g. coal
pneumoconiosisSiderosis IronSilicosis Silica, rock dustsStannosis Tin
Registrar’s extra-statutory list of diagnoseswhich should be referred to the coroner
RF Preliminary - DHSSPS 315-008-013
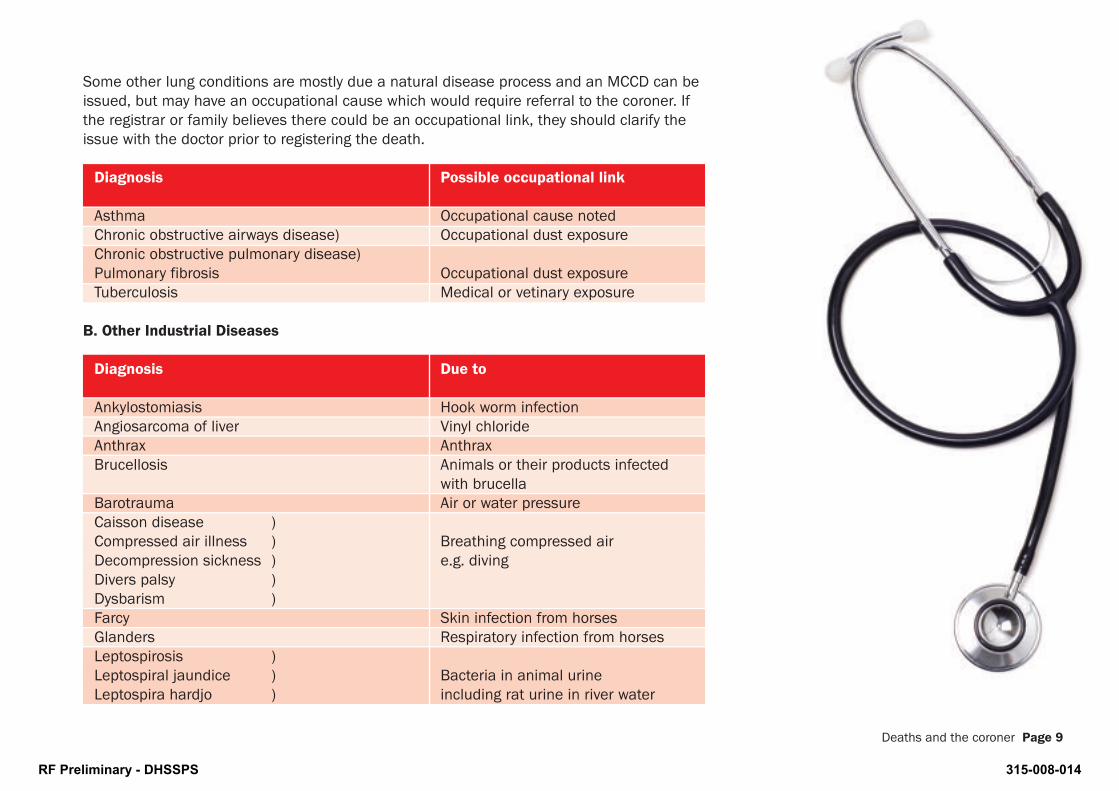
Some other lung conditions are mostly due a natural disease process and an MCCD can beissued, but may have an occupational cause which would require referral to the coroner. Ifthe registrar or family believes there could be an occupational link, they should clarify theissue with the doctor prior to registering the death.
Diagnosis Possible occupational link
Asthma Occupational cause notedChronic obstructive airways disease) Occupational dust exposureChronic obstructive pulmonary disease)Pulmonary fibrosis Occupational dust exposureTuberculosis Medical or vetinary exposure
B. Other Industrial Diseases
Diagnosis Due to
Ankylostomiasis Hook worm infectionAngiosarcoma of liver Vinyl chlorideAnthrax AnthraxBrucellosis Animals or their products infected
with brucellaBarotrauma Air or water pressureCaisson disease )Compressed air illness ) Breathing compressed airDecompression sickness ) e.g. divingDivers palsy )Dysbarism )Farcy Skin infection from horsesGlanders Respiratory infection from horsesLeptospirosis )Leptospiral jaundice ) Bacteria in animal urineLeptospira hardjo ) including rat urine in river water
Deaths and the coroner Page 9
RF Preliminary - DHSSPS 315-008-014

Page 10 Deaths and the coroner
B. Other Industrial Diseases (continued)
Diagnosis Due to
Malignant pustule AnthraxMesothelioma AsbestosNon-cirrhotic portal fibrosis Vinyl chlorideOrnithosis Chlamydia psittaci from birdsOsteolysis of terminal phalanges of the fingers Vinyl chlorideOsteonecrosis Compressed air or injury Psittacosis Chlamydia psittaci from birdsSpirochaetal jaundice Bacteria in animal urine
(also called leptospirosis)Streptocosccus suis Bacteria from pigsWeil’s disease Bacteria in animal urine
(also called leptospirosis)
Some cancers are mostly due a natural disease process and an MCCD can be issued, butmay have an occupational cause which would require referral to the coroner. If the registraror family believes there could be an occupational link, they should clarify the issue with thedoctor prior to registering the death.
Diagnosis Possible occupational link
Cancer of skin Tar, oil, soot, arsenicCancer of nose, nasopharynx or sinuses Nickel fumes used in making leather,
fibre board, woolCancer of bladder, ureter or urethra Industrial chemicals and dyes
RF Preliminary - DHSSPS 315-008-015

C. Industrial Poisoning
*If MCCD indicates toxic anaemia or jaundice is due to natural causes the case does notneed referred to the coroner.
Diagnosis Due to
Toxic anaemia* ) Metals and chemicals Toxic Jaundice* )Plumbism ) LeadSaturnism )
D. Other Poisonings
*If MCCD indicates blood poisoning, septicaemia or hepatitis is due to natural causes thecase does not need referred to the coroner.
Diagnosis Comments
Alcohol Acute alcohol poisoning, or alcohol as a contributory factor
Blood poisoning* If due to injury or following an operation (also called septicaemia)
Food poisoning e.g. salmonella, botulismHepatitis* If due to occupation or drug abuse
(usually Hepatitis B)Septicaemia* If due to injury or following an
operation (also called blood poisoning)Tetanus Usually related to an injury
Deaths and the coroner Page 11
RF Preliminary - DHSSPS 315-008-016

DEATH RESULTING FROM AN INJURY ETC
A. Injury
The term injury includes:
Diagnosis Comments
Asphyxia *Unless MCCD indicates underlying natural cause e.g. Cerebro-Vascular accident, stroke.
*Neonatal Asphyxia or Birth Asphyxia are acceptable if MCCD indicates underlying natural cause
Aspiration Pneumonia ) *Unless MCCD indicates underlyingInhalation Pneumonia ) natural cause e.g. Cerebro-VascularVomitus Pneumonia ) accident, stroke causing swallow
problemsBurnsChoking (or other effects of foreign bodies)ConcussionContusionCutDrowningElectricity, Electric ShockFracture Except pathological fractures e.g.
bone cancer, severe osteoporosisGunshot WoundsHyperthermia Hypothermia Ill treatment
Page 12 Deaths and the coroner
RF Preliminary - DHSSPS 315-008-017

Deaths and the coroner Page 13
A. Injury (continued)
Diagnosis Comments
LightningMalnutrition Unless MCCD indicates underlying
natural cause e.g. Anorexia NervosaScaldsStarvationSubdural Haemorrhage ) *Unless MCCD indicates underlyingSubdural Haematoma ) natural cause e.g.SuffocationSunstrokeTrauma or Traumatic
* The coroners have requested that all cases of asphyxia, aspiration or subdural bleedshould be referred to the coroner before completing an MCCD. If the coroner agrees theunderlying cause was natural an MCCD can be completed indicating the underlying naturalcause, and a note can be attached informing the registrar that the case has beendiscussed with the coroner.
RF Preliminary - DHSSPS 315-008-018
B. INDIRECT INJURY
As well as obvious injury, registrarsshould also be watchful for deathswhich have been caused indirectly asa result of an injury received whichshould be reported to the coroner, forexample, where a medical certificateshows death due to:
I (a) hypostatic pneumonia due to
I (b) immobility due to
I (c) fractured femur.
C. BIRTH INJURY
The death of any newborn child whichis certified by a doctor as due to birthinjury should be referred to thecoroner.
There are natural causes of neonataldeath including asphyxia (asphyxianeonatorum, asphyxia pallida,asphyxia livida) or bleeding (tentorialtear, intracranial haemorrhage).
Such cases should be referred to thecoroner only if:-
a. the coroner has requested that theyshould be;
b. it is represented to the Registrarthat death resulted from accident,violence or neglect; or
c. there are suspicious circumstances.
D. OPERATION / ANAESTHETIC
Deaths occurring during an operationor before recovery from the effect ofan anaesthetic should be reported tothe coroner.
Deaths following an operationnecessitated by injury should bereported to the coroner becausethe underlying cause of death wasan injury.
Deaths which follow an operationnecessitated by a natural illness neednot be reported unless the cause of
death is attributable to an unrelatedincident which arose during theoperation or because of theadministration of the anaesthetic.
Operations are often referred to byterms ending in –tomy (e.g.osteotomy,colonostomy, splenectomy)
Page 14 Deaths and the coroner
RF Preliminary - DHSSPS 315-008-019
Whenever a patient dies a doctor whois familiar with their medical historyand who is able to give an explanationof why death occurred should speak tofamily members. This will provide anopportunity for the family to expressany concerns before a MedicalCertificate of Cause of Death (MCCD)is completed. If the family is unhappywith the care and treatment thedeceased received it is advisable toreport the death to the coroner withparticulars of the family’s concerns. Awritten record of these concernsshould always be made and retainedwith the medical records.
Deaths and the coroner Page 15
Who reports a deathto the coroner?
position in England and Wales where only the Registrar of Deaths is under astatutory duty to report such deaths tothe coroner.
A foundation level doctor shouldnormally consult a more seniorcolleague before reporting a death tothe coroner.
The family should be advised if thedeath is being referred to the coronerwith an explanation why.
The doctor who assumes responsibilityfor dealing with the death shouldalways view the body before reportingthe death to the coroner.
The duty to report is imposed also onregistrars of deaths, funeral undertakers and every occupier of ahouse or mobile dwelling and everyperson in charge of any institution orpremises in which a deceased personwas residing. This contrasts with the
RF Preliminary - DHSSPS 315-008-020

RF Preliminary - DHSSPS 315-008-021
If a death which needs to be reportedto the coroner occurs in thecommunity, the coroner or the policeshould be contacted before the body ismoved. The coroner will direct wherethe body is to be taken.
A death occurring in hospital duringthe night does not usually need to beimmediately reported to the coroner.The body should be moved to themortuary for overnight storage and thecoroner’s office contacted promptlythe following morning.
However, if the death follows acriminal assault the death should bereported to the coroner as soon aspossible.
In coroner’s cases where thedeceased or their family have agreedto donation of organs fortransplantation there is a need toobtain the consent of the coronerbefore the removal of organs.
The office of the Coroners Service forNorthern Ireland is at:
• May’s Chambers, 73 May Street, BelfastBT1 3JL.
• Tel: 028 9044 6800;Fax 028 9044 6801.
• Website: www.coronersni.gov.uk
• E-mail: [email protected]
• the office is staffed weekdays 9.00am –5.00pm, weekends and public holidays 9.30am– 12.30pm(except Christmas Day when the officeis closed)
• outside normal office hours a recordedmessage will provide contact details forthe duty coroner or messages may be lefton the telephone answering machine.
The Coroner’s Decision
Following the report of a death the coronermay adopt one of three courses:
1. Direct that the doctor should issuea Medical Certificate of Cause ofDeath (MCCD).
After discussion the coroner anddoctor may agree that the cause ofdeath does not need investigatedand the MCCD can be completed.You should record the dicussion inthe patient's notes.
2. Allow the death to be processedunder the “pro-forma” system.
Coroner’s Pro-forma
This is a special form for stating thecause of death and providing briefparticulars of the backgroundcircumstances. Normally, thecoroner will agree to use the “pro-forma” system where:
• it is a natural death and theonly reason a death certificatecannot be issued is that thedoctor has not seen and
When to contact the coroner? Page 17
When to contact the coroner?
RF Preliminary - DHSSPS 315-008-022

treated the deceased for thecondition from which they diedwithin 28 days of death;
• the cause of death is not anatural one but there are nosuspicious circumstances e.g. asimple fall by an elderly personresulting in a fractured neck offemur and leading to the onsetof bronchopneumonia as theterminal event;
• the cause of death is not anatural one but a post-mortemexamination is unnecessary as adefinite diagnosis had alreadybeen made eg asbestosis in ashipyard worker.
A doctor should not proceed to usethe “pro-forma” system for a deathwithout having first agreed thatcourse with the coroner.
The pro-forma should be sentimmediately by fax and followed byhard copy to the Coroner’s Service. Itshould not be given to the family asthey may confuse it with an MCCDand try to take it to the registrar.
If the special ”pro-forma” form isnot available the doctor shouldinstead forward to the coroner’soffice a completed but unsignedMCCD and an accompanying letterbriefly setting out the backgroundcircumstances and explaining thecause of death given on the MCCD.
3. Direct a post-mortem examination.
Clinical Summary for a Coroner’sPost-Mortem Examination
If the coroner directs a post-mortemexamination, the doctor whoreported the death should preparea clinical summary for thepathologist. This should accompanythe body to the mortuary (Mostcoroner’s post-mortemexaminations are carried out in theState Pathology Department on theRoyal Hospital site in Belfast). Theabsence of a clinical summary maylead to a delay in the post-mortemexamination being carried out.Where the deceased’s medicalhistory is complex the consultant orGP who lead their care shouldassume personal responsibility forthe content of the clinical summary.
Coroner’s Investigations
When a coroner directs a post-mortem examination a police officerwill act on behalf of the coroner inmaking the necessaryarrangements, and investigations.All medical staff should facilitatethe police officer in these duties.GMC guidance Good MedicalPractice paragraph 32 states “youmust assist the coroner orprocurator fiscal, by responding toinquiries, and by offering allrelevant information to an inquestor inquiry into a patient’s death.Only where your evidence may leadto criminal proceedings being takenagainst you are you entitled toremain silent.”
In relation to hospital deaths, thepolice officer will require a memberof staff to formally identify the bodyand to provide brief particulars ofthe background to the death.
Page 18 When to contact the coroner?
This pro-forma is available forphotocopying if required
RF Preliminary - DHSSPS 315-008-023

To:
H.M
. C
oron
er f
or t
heD
octo
r’s A
dd
ress
:C
oron
er’s
Dis
tric
t of
Tel N
o
Fax
No
Dat
e
Dea
r S
ir,
Nam
e of
Dec
ease
d
Dat
e of
Birt
h of
Dec
ease
d/
/
Ad
dre
ss
Occ
upat
ion
The
abov
e w
as a
pat
ient
of
min
e fo
r th
e p
ast
year
s, a
nd h
ad a
med
ical
his
tory
of:
I las
t sa
w h
im/h
er o
nat
whe
n he
/she
was
suf
ferin
g fr
om
He/
She
die
d o
n th
eat
in t
he f
ollo
win
g ci
rcum
stan
ces:
Dea
th w
as c
onfir
med
by
me/
Dr.
and
I am
sat
isfie
d t
hat
he/s
he d
ied
fro
m:
I(a
)d
ue t
o(b
)d
ue t
o(c
)
II Your
s fa
ithfu
lly,
N.B
.T
his
form
sho
uld
no
t b
e us
ed u
nles
s th
e co
rone
r ha
s co
nfir
med
tha
t he
do
es n
ot
req
uire
an
auto
psy
. It
need
no
t b
e ac
com
pan
ied
by
an
unsi
gne
d c
erti
ficat
e, b
ut s
houl
d a
s fa
r as
po
ssib
le c
ont
ain
the
follo
win
g in
form
atio
n:
1.N
ame,
D.O
.B.,
add
ress
and
occ
upat
ion
of d
ecea
sed
.2.
How
long
a p
atie
nt a
nd a
ny r
elev
ant
med
ical
his
tory
.3.
Whe
n la
st s
een
and
con
diti
on t
hen.
4.Ti
me,
dat
e, p
lace
and
circ
umst
ance
s of
dea
th,
givi
ng a
ny f
inal
sym
pto
ms.
5.N
ame
of d
octo
r w
ho s
aw b
ody
and
con
firm
ed d
eath
.6.
The
caus
e of
dea
th,
spec
ifyin
g sa
me
as o
n a
dea
th c
ertif
icat
e, a
nd n
ot in
clud
ing
anyt
hing
whi
ch d
id n
ot c
ontr
ibut
e to
the
dea
th.
Ple
ase
ensu
re t
hat
this
fo
rm is
ful
ly c
om
ple
ted
.
RF Preliminary - DHSSPS 315-008-024

Ensuring Accurate Certification Relating to Death
IndividualsAll doctors completing medical certificates of cause of death or cremation forms and doctors and midwifescompleting stillbirth forms should be aware of when and how to complete the forms and when deathsshould be referred to the coroner. They should ensure they are competent by updating their knowledge andreflecting on their practice.
OrganisationsOrganisations should provide induction and update training on certification and coroners referrals forrelevant staff. They should promote good practice by monitoring or regular audit of certification.
RF Preliminary - DHSSPS 315-008-025
A step-by-step to completing a MCCD. Page 21
General
Doctors are expected to state thecause of death to the best of theirknowledge and belief.
Any alterations to the MCCD must beinitialled by the doctor.
Registrars sometimes need to contactthe doctor to clarify issues beforeregistering the death. Difficultycontacting the doctor can lead to delayin funeral arrangements and distressfor families. Incorrectly completedforms can cause difficulties for thedoctor, registrar and relatives.
It is good practice to either make anote of the details recorded on theMCCD or keep a copy of the MCCD inthe patient’s records.
Legibility and spelling
Ensure the form is readable. Considerwriting in BLOCK CAPITALS.
Abbreviations or symbols
Do not use abbreviations such as MIinstead of myocardial infarction or (L)instead of left or medical symbolssuch as 1° instead of primary or #instead of fracture on deathcertificates.
The only abbreviations which theregistrar can accept are HIV for HumanImmunodeficiency Virus infection, AIDSfor Acquired Immune DeficiencySyndrome and MRSA for MethicillinResistant Staphylococcus Aureus.
A step-by-step guide to completing a MCCD.Before you start - Rules for Good Practice.
RF Preliminary - DHSSPS 315-008-026
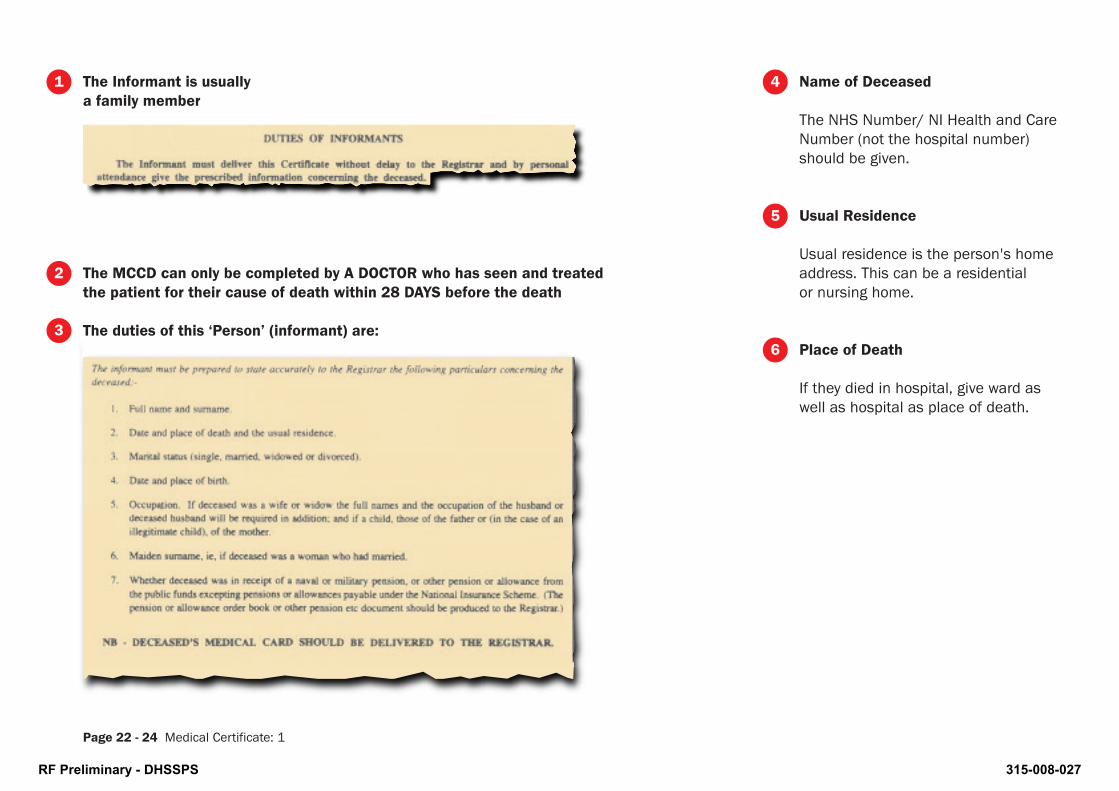
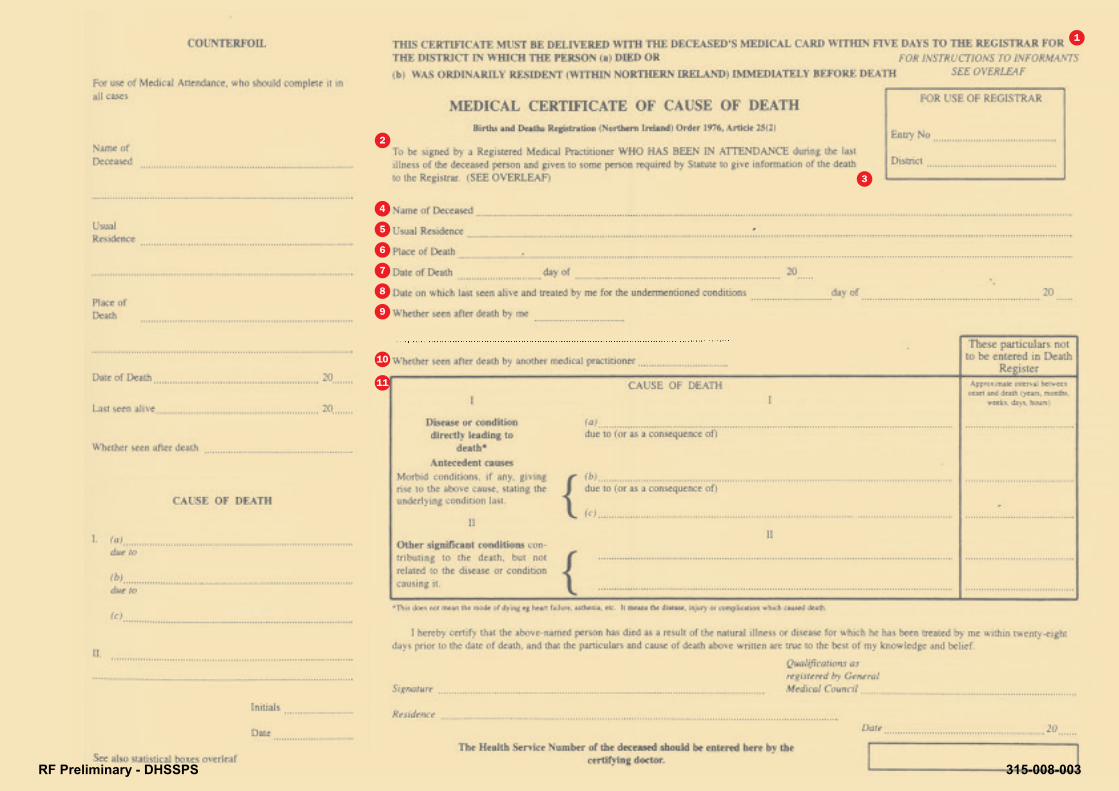
Name of Deceased
The NHS Number/ NI Health and CareNumber (not the hospital number)should be given.
Usual Residence
Usual residence is the person's homeaddress. This can be a residentialor nursing home.
Place of Death
If they died in hospital, give ward aswell as hospital as place of death.
Page 22 - 24 Medical Certificate: 1
1
2
3
4
5
6
The Informant is usuallya family member
The MCCD can only be completed by A DOCTOR who has seen and treatedthe patient for their cause of death within 28 DAYS before the death
The duties of this ‘Person’ (informant) are:
RF Preliminary - DHSSPS 315-008-027
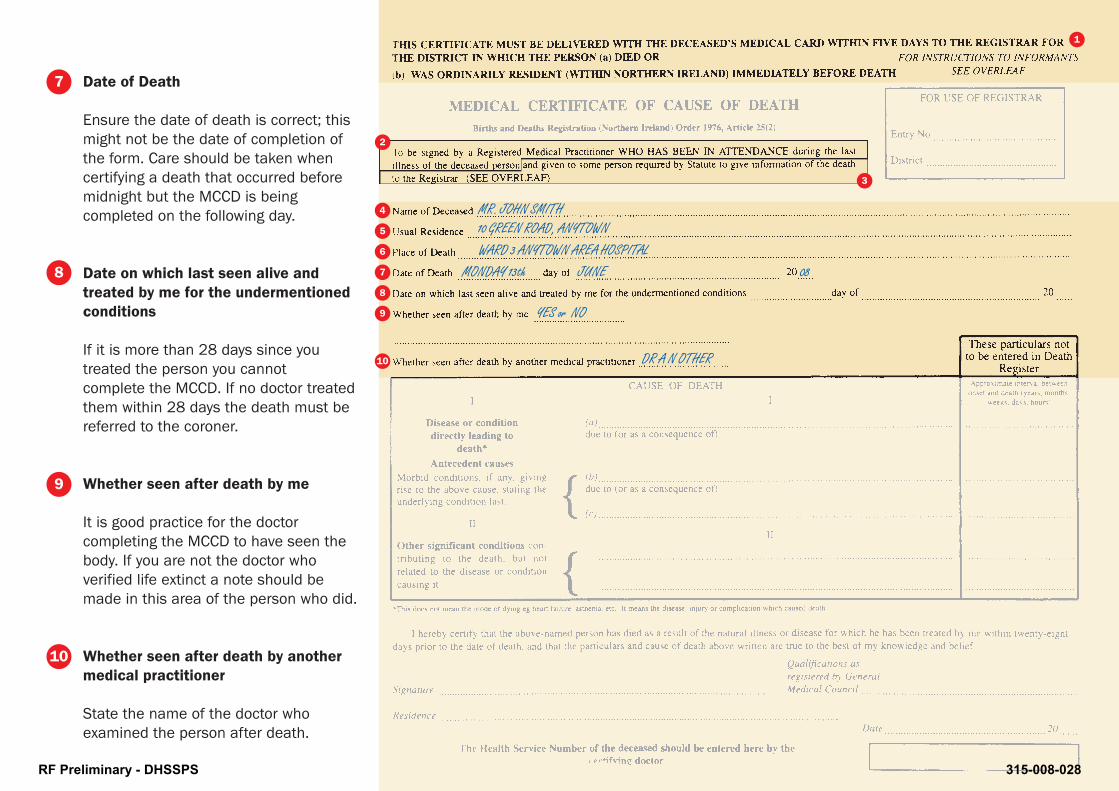
Date of Death
Ensure the date of death is correct; thismight not be the date of completion ofthe form. Care should be taken whencertifying a death that occurred beforemidnight but the MCCD is beingcompleted on the following day.
Date on which last seen alive andtreated by me for the undermentionedconditions
If it is more than 28 days since youtreated the person you cannotcomplete the MCCD. If no doctor treatedthem within 28 days the death must bereferred to the coroner.
Whether seen after death by me
It is good practice for the doctorcompleting the MCCD to have seen thebody. If you are not the doctor whoverified life extinct a note should bemade in this area of the person who did.
Whether seen after death by anothermedical practitioner
State the name of the doctor whoexamined the person after death.
4
2
3
5
6
7
8
9
MR. JOHN SMITH10 GREEN ROAD, ANYTOWNWARD 3 ANYTOWN AREA HOSPITAL
MONDAY 13th JUNE 08
YES or NO
10
1
7
8
9
10
DR A N OTHER
RF Preliminary - DHSSPS 315-008-028

RF Preliminary - DHSSPS 315-008-029

Recording the Cause of Death
The Cause of Death section of theMCCD is set out in two parts, inaccordance with World HealthOrganisation (WHO) recommendationsin the International StatisticalClassification of Diseases and RelatedHealth Problems (ICD).
Part I - Sequence leading to death,underlying cause
You have to start with the immediate,direct cause of death on line I (a), thento go back through the sequence ofevents or conditions that led to deathon subsequent lines, until you reachthe one that initiated the fatalsequence. If the certificate has beencompleted properly, the condition onthe lowest completed line of part I willhave caused all of the conditions onthe lines above it.
Part II - Contributory causes
You should enter any other diseases,injuries, conditions, or events thatcontributed to the death, but were notpart of the direct sequence, in part IIof the certificate.
INTRA-PERITONEAL HAEMORRHAGE
Example >Page 25
RUPTURED METASTATIC DEPOSIT IN LIVER
NON-INSULIN DEPENDANT DIABETES MELLITUS
PRIMARY ADENOCARCINOMA OF ASCENDING COLON
11
11
MR. JOHN SMITH10 GREEN ROAD, ANYTOWNWARD 3 ANYTOWN AREA HOSPITAL
MONDAY 13th JUNE 08
YES or NO
DR A N OTHER
RF Preliminary - DHSSPS 315-008-030
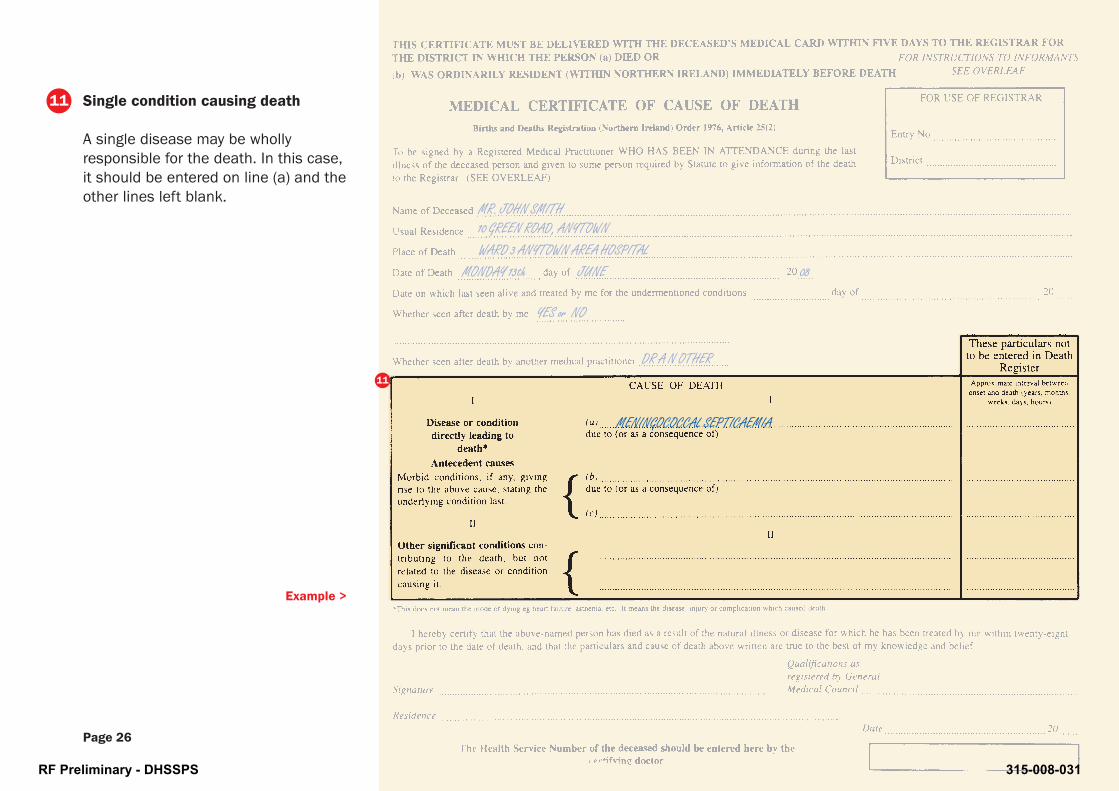
Single condition causing death
A single disease may be whollyresponsible for the death. In this case,it should be entered on line (a) and theother lines left blank.
MENINGOCOCCAL SEPTICAEMIA
Example >
Page 26
11
11
MR. JOHN SMITH10 GREEN ROAD, ANYTOWNWARD 3 ANYTOWN AREA HOSPITAL
MONDAY 13th JUNE 08
YES or NO
DR A N OTHER
RF Preliminary - DHSSPS 315-008-031
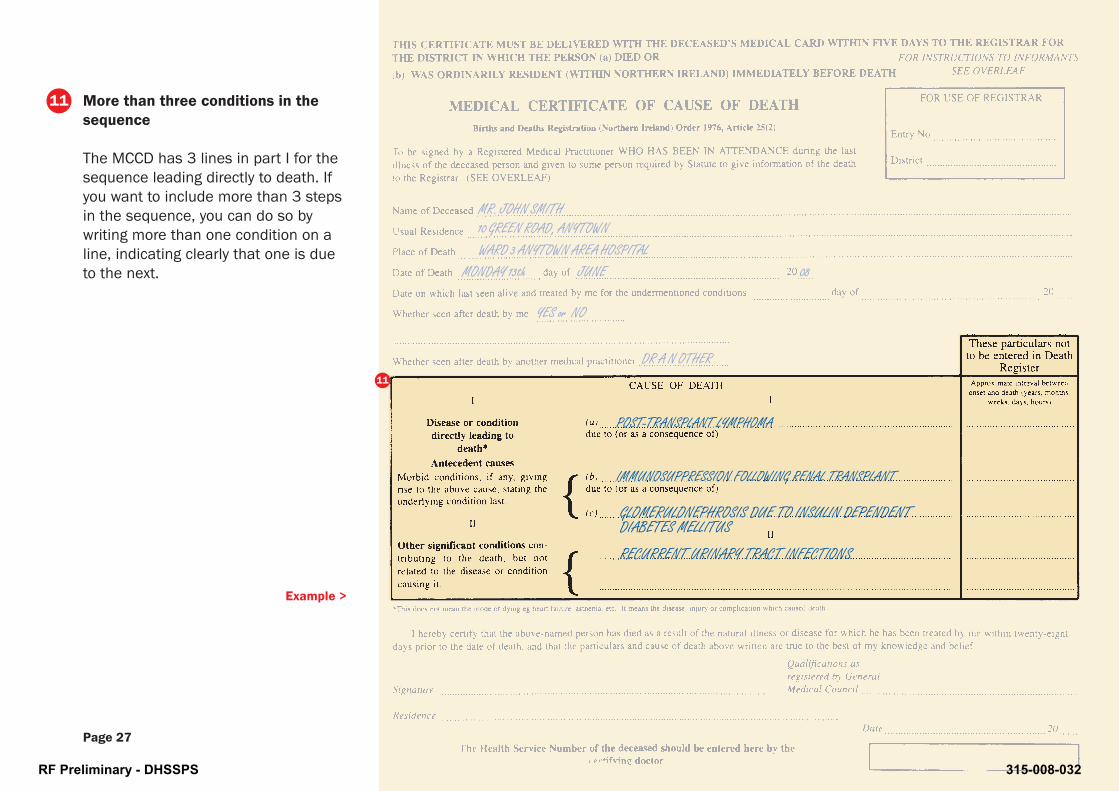
More than three conditions in thesequence
The MCCD has 3 lines in part I for thesequence leading directly to death. Ifyou want to include more than 3 stepsin the sequence, you can do so bywriting more than one condition on aline, indicating clearly that one is dueto the next.
POST-TRANSPLANT LYMPHOMA
Example >
Page 27
IMMUNOSUPPRESSION FOLLOWING RENAL TRANSPLANT
RECURRENT URINARY TRACT INFECTIONS
GLOMERULONEPHROSIS DUE TO INSULIN DEPENDENTDIABETES MELLITUS
11
11
MR. JOHN SMITH10 GREEN ROAD, ANYTOWNWARD 3 ANYTOWN AREA HOSPITAL
MONDAY 13th JUNE 08
YES or NO
DR A N OTHER
RF Preliminary - DHSSPS 315-008-032
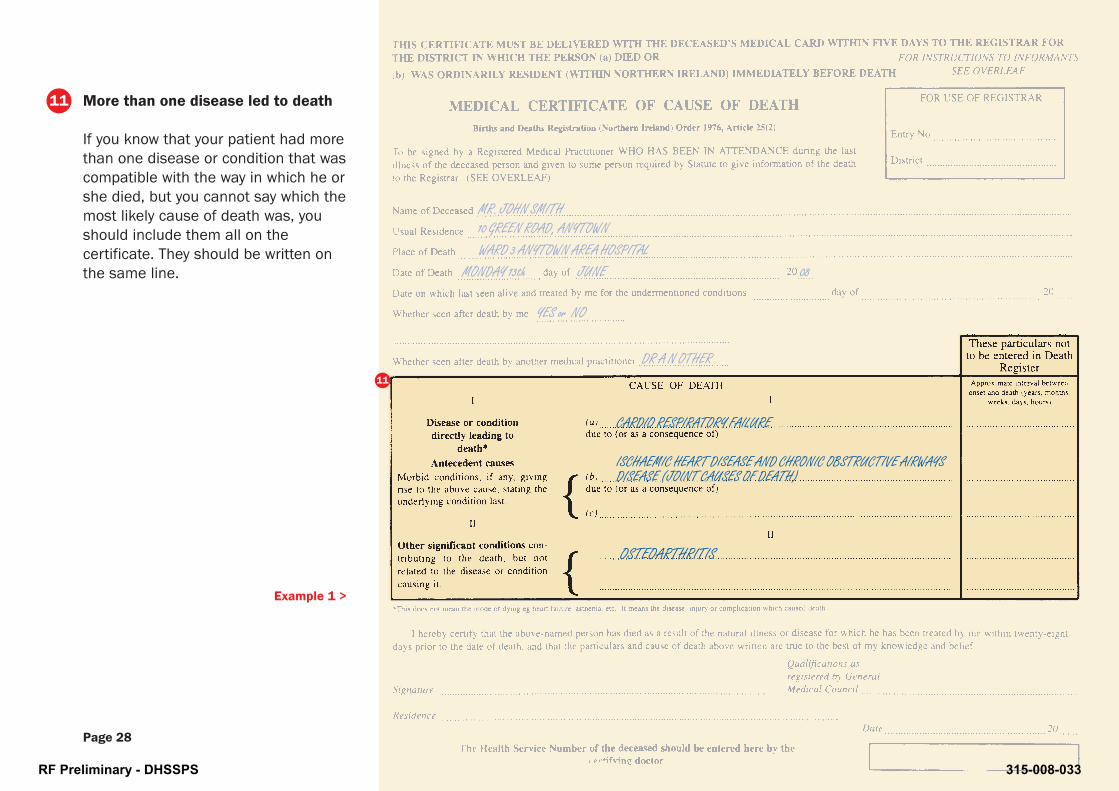
More than one disease led to death
If you know that your patient had morethan one disease or condition that wascompatible with the way in which he orshe died, but you cannot say which themost likely cause of death was, youshould include them all on thecertificate. They should be written onthe same line.
CARDIO RESPIRATORY FAILURE
Example 1 >
Page 28
ISCHAEMIC HEART DISEASE AND CHRONIC OBSTRUCTIVE AIRWAYSDISEASE (JOINT CAUSES OF DEATH)
OSTEOARTHRITIS
11
MR. JOHN SMITH10 GREEN ROAD, ANYTOWNWARD 3 ANYTOWN AREA HOSPITAL
MONDAY 13th JUNE 08
YES or NO
DR A N OTHER11
RF Preliminary - DHSSPS 315-008-033

More than one disease led to death(continued)
HEPATIC FAILURE
Example 2 >
Page 29
LIVER CIRRHOSIS
CHRONIC HEPATITIS C INFECTION AND ALCOHOLISM
11
MR. JOHN SMITH10 GREEN ROAD, ANYTOWNWARD 3 ANYTOWN AREA HOSPITAL
MONDAY 13th JUNE 08
YES or NO
DR A N OTHER11
RF Preliminary - DHSSPS 315-008-034
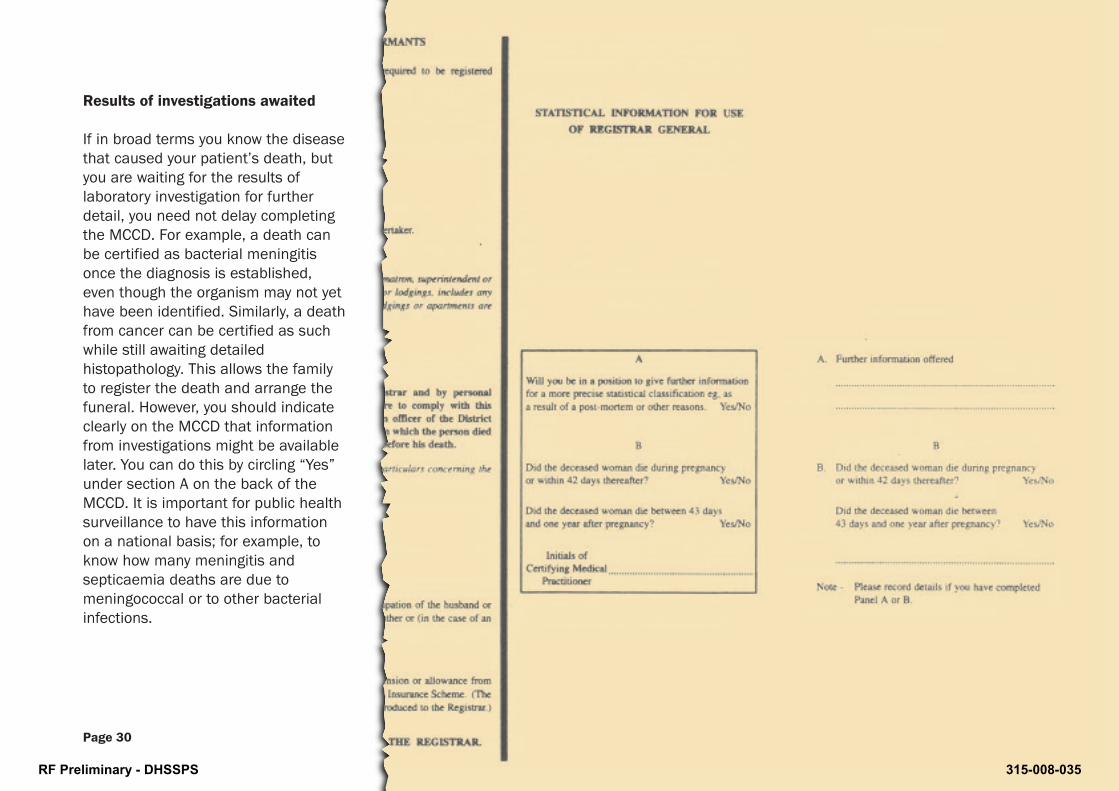
Results of investigations awaited
If in broad terms you know the diseasethat caused your patient’s death, butyou are waiting for the results oflaboratory investigation for furtherdetail, you need not delay completingthe MCCD. For example, a death canbe certified as bacterial meningitisonce the diagnosis is established,even though the organism may not yethave been identified. Similarly, a deathfrom cancer can be certified as suchwhile still awaiting detailedhistopathology. This allows the familyto register the death and arrange thefuneral. However, you should indicateclearly on the MCCD that informationfrom investigations might be availablelater. You can do this by circling “Yes”under section A on the back of theMCCD. It is important for public healthsurveillance to have this informationon a national basis; for example, toknow how many meningitis andsepticaemia deaths are due tomeningococcal or to other bacterialinfections.
Page 30
RF Preliminary - DHSSPS 315-008-035

Deaths during pregnancy or withinone year after pregnancy
Section B on the back of the MCCDform asks if the deceased woman diedduring or after pregnancy. This isstatistical information for the RegistrarGeneral. The pregnancy did not haveto result in a live birth. The death doesnot have to be related to thepregnancy.
Page 31
RF Preliminary - DHSSPS 315-008-036

Recording Healthcare AssociatedInfections
The level of Healthcare AssociatedInfections remains a matter of concernto clinicians and the public.
The Health Service depends onaccurate information gained fromdeath certificates to record changes inmortality associated with infections.Trends which are identified canhighlight new areas of concern, ormonitor changes in deaths associatedwith certain infections.
Families may be surprised if aninfection the patient was being treatedfor such as MRSA or clostridiumdifficile is not mentioned on a deathcertificate.
CLOSTRIDIUM DIFFICILE PSEUDO MEMBRANOUS COLITIS
Example 1 >
Page 32
MULTIPLE ANTIBIOTIC THERAPY
POLYMYALGIA RHEUMATICA
COMMUNITY ACQUIRED PNEUMONIA WITH SEVERE SEPSIS
OSTEOPOROSIS
11
11
MR. JOHN SMITH10 GREEN ROAD, ANYTOWNWARD 3 ANYTOWN AREA HOSPITAL
MONDAY 13th JUNE 08
YES or NO
DR A N OTHER
RF Preliminary - DHSSPS 315-008-037

Recording Healthcare AssociatedInfections (continued)
It is a matter of clinical judgement if aHealthcare Associated Infection wasthe disease directly leading to thedeath [record at part I (a), was anantecedent cause [record at part I (b)or I (c) or was a significant conditionnot directly related to the cause ofdeath [record at part II].
Where infection does follow treatment,including surgery, radiotherapy, anti-neoplastic, immunosuppressive, andantibiotic or other drug treatment foranother disease, remember to specifythe treatment and the disease forwhich it was given.
Example 2 >
Page 33
BRONCHOPNEUMONIA (HOSPITAL ACQUIRED MRSA)
MULTIPLE MYELOMA
CHRONIC OBSTRUCTIVE AIRWAYS DISEASE
11
MR. JOHN SMITH10 GREEN ROAD, ANYTOWNWARD 3 ANYTOWN AREA HOSPITAL
MONDAY 13th JUNE 08
YES or NO
DR A N OTHER
11
RF Preliminary - DHSSPS 315-008-038

Recording Healthcare AssociatedInfections (continued)
CARCINOMATOSIS AND RENAL FAILURE
Example 3 >
Page 34
ADENOCARCINOMA OF THE PROSTATE
CATHETER ASSOCIATED ESCHERICHIA COLI URINARYTRACT INFECTION
CHRONIC OBSTRUCTIVE AIRWAYS DISEASE
11
11
MR. JOHN SMITH10 GREEN ROAD, ANYTOWNWARD 3 ANYTOWN AREA HOSPITAL
MONDAY 13th JUNE 08
YES or NO
DR A N OTHER
RF Preliminary - DHSSPS 315-008-039

Terms to avoid on MCCD
Coroner’s cases
Any diagnosis which might indicate anindustrial disease, trauma, unnaturaldeath or where the widercircumstances may requireinvestigation. The registrars have anextra-statutory list of diagnoses thatmust be referred to the coroner seepages 8 - 14). Doctors should beaware that any case where the causeof death is included in this list shouldbe referred to the coroner.
Organ failure alone
Do not certify deaths as due to thefailure of any organ, without specifyingthe disease or condition that led to theorgan failure. Examples which needfurther information: Liver Failure,Renal Failure, Heart Failure.
Example >
Page 35
RENAL FAILURE
NECROTISING-PROLIFERATIVE NEPHROPATHY
SYSTEMIC LUPUS ERYTHEMATOSUS
11
11
MR. JOHN SMITH10 GREEN ROAD, ANYTOWNWARD 3 ANYTOWN AREA HOSPITAL
MONDAY 13th JUNE 08
YES or NO
DR A N OTHER
RF Preliminary - DHSSPS 315-008-040
Cancer alone
The terms cancer, neoplasm or tumourshould all have detail of thehistological type, primary site andmetastatic spread.
Pneumonia alone
Chest signs and symptoms arecommon terminal findings, not alwaysdue to significant infection contributingto the death. If pneumonia is a causeof death, try to give details about:
• type of pneumonia (lobar,bronchopneumonia);
• organism;
• whether hospital or communityacquired;
• sequence of conditions leading topneumonia, including use ofventilation.
Infections alone
Where possible give details about:
• site ( meningitis, peritonitis, woundsite etc);
• organism;
• antibiotic resistance;
• route of infection (needle sharing,food poisoning etc).
Terminal events, modes of dying,clinical signs and other vague terms
Terms that do not identify a disease orpathological process clearly are notacceptable as the cause of death.Description of terminal events such ascardiac or respiratory arrest, syncopeor shock describe modes of dying notcauses of death. Signs such asoedema, ascites, haemoptysis,haematemesis and vague statementssuch as debility or frailty are equallyunacceptable.
Natural causes
There is no ICD code equivalent to“natural causes”, and registrars willseek clarification from the doctor, orrefer the case to the coroner. If you donot know what disease caused yourpatient's death, you should discussthe case with the coroner.
Old age or general debility of age
It is possible that families, registrarsand cremation referees may requestfurther explanation of your opinionthat old age was the only cause ofdeath.
It may be acceptable as the only causeof death in some cases of patientsover 80 years of age. In these casesyou need to be confident the deathwas expected following gradual declinein health due to natural causes, butnot to any identifiable disease.
Page 36
RF Preliminary - DHSSPS 315-008-041

CremationForms
RF Preliminary - DHSSPS 315-008-042
Reasons
RF Preliminary - DHSSPS 315-008-043

Reasons for Cremation Certification Page 39
Once a body has been cremated there is no possibility of further examination ifquestions arise about the death. When a body is to be cremated there are aseries of medical forms to be completed, by different, independent doctors, toprovide reassurance that the death does not require further investigation. Thelaw governing cremation in Northern Ireland is the Cremation (Belfast)Regulations (Northern Ireland) 1961. If the death has not been referred to thecoroner, and a certificate of cause of death has been completed, the medicalforms are:
Reasons for cremationcertification
Form B Certificate of Medical Attendant
Form C Confirmatory Medical Certificate
Form F Authority to Cremate
RF Preliminary - DHSSPS 315-008-044
Forms: B C F
RF Preliminary - DHSSPS 315-008-045

Form B
This should be completed by a registered medical practitioner who has attendedthe deceased during his last illness. It is often the same doctor who completedthe MCCD.
Foundation level doctors should NOT complete cremation Form B unless they havebeen trained to do so.
Form C
The doctor completing cremation Form C should:
• be a registered medical practitioner of not less than 5 years standing (overseasdoctors who has a primary medical qualification in an EEA member state for 5years will be eligible to sign cremation Form C);
• be independent of the doctor who completed Form B. The legal requirement isthat the doctor completing Form C should not be a relative, partner or assistantof the doctor who completed Form B. It would be good practice that the doctorcompleting Form C should not have been directly involved in the patient’s care;
• not be related to the deceased.
Form F
This is completed by the Medical Referee for the Cremation Authority.
Who should complete cremation forms? Page 41
Who should complete cremation forms?
RF Preliminary - DHSSPS 315-008-046

RF Preliminary - DHSSPS 315-008-047
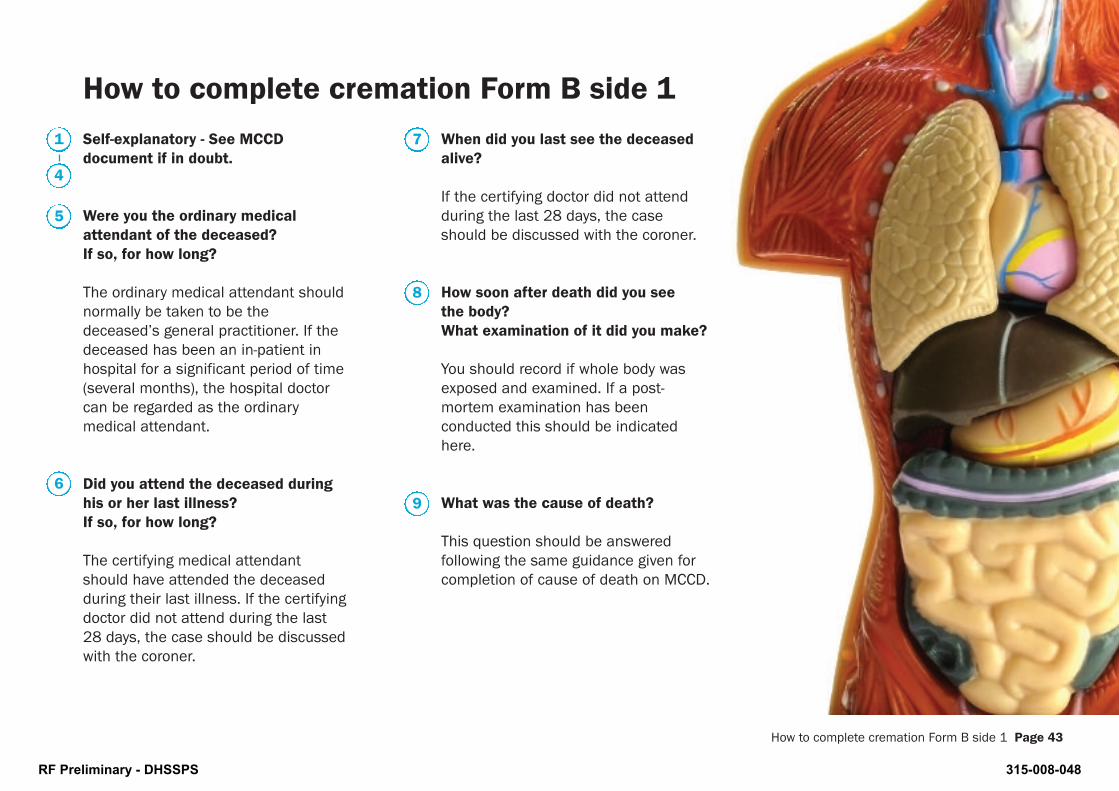
Self-explanatory - See MCCDdocument if in doubt.
Were you the ordinary medicalattendant of the deceased?If so, for how long?
The ordinary medical attendant shouldnormally be taken to be thedeceased’s general practitioner. If thedeceased has been an in-patient inhospital for a significant period of time(several months), the hospital doctorcan be regarded as the ordinarymedical attendant.
Did you attend the deceased duringhis or her last illness?If so, for how long?
The certifying medical attendantshould have attended the deceasedduring their last illness. If the certifyingdoctor did not attend during the last28 days, the case should be discussedwith the coroner.
When did you last see the deceasedalive?
If the certifying doctor did not attendduring the last 28 days, the caseshould be discussed with the coroner.
How soon after death did you seethe body?What examination of it did you make?
You should record if whole body wasexposed and examined. If a post-mortem examination has beenconducted this should be indicatedhere.
What was the cause of death?
This question should be answeredfollowing the same guidance given forcompletion of cause of death on MCCD.
How to complete cremation Form B side 1 Page 43
How to complete cremation Form B side 1
1
4
5
6
7
8
9
RF Preliminary - DHSSPS 315-008-048
21
RF Preliminary - DHSSPS 315-008-049
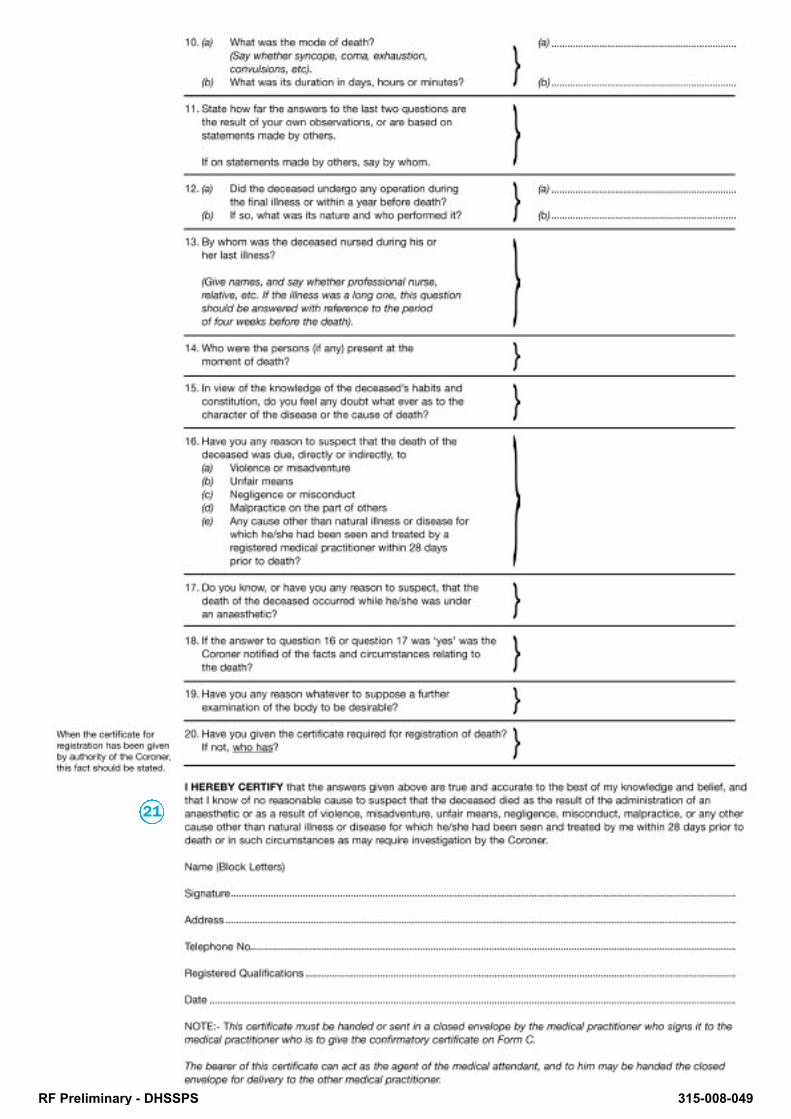
How to complete cremation Form B side 2 Page 45
What was the mode of death? What wasits duration in days, hours or minutes?
Syncope implies a sudden deathoccurring in minutes, but not necessarilyunexpectedly, with a history of ischaemicheart or cerebrovascular disease.Convulsions may indicate an unnaturaldeath unless adequately explained by thecause of the death.
State how far the answers to the lasttwo questions are the result of your ownobservations, or are based onstatements made by others.
If your answers to Q 9 & 10 have beeninformed by other sources, state who.
Did the deceased undergo any operationduring the final illness or within a yearbefore death?
Any failure to include operativeprocedures which are of potentialsignificance may call into question thereliability of the certificate.
By whom was the deceased nursedduring his or her last illness?
Who were the persons (if any) present at themoment of death?
Specific names (and contact details) willassist both the doctor completing theconfirmatory certificate and the medicalreferee.
In view of the knowledge of the deceased’shabits and constitution, do you feel anydoubt whatever as to the character of thedisease or the cause of death?
Have you any reason to suspect that thedeath of the deceased was due, directly orindirectly
Do you know, or have you any reason tosuspect, that the death of the deceasedoccurred while he/she was under ananaesthetic?
Have you any reason whatever to supposea further examination of the body to bedesirable?
These questions confirm that there were nocircumstances surrounding the death whichmight require further investigation. Any “yes”answers should prompt referral to the coroner.
How to complete cremation Form B side 2
Have you given the certificate requiredfor registration of death? If not, who has?
Give the name and contact details of thedoctor who completed the MCCD, if it was adifferent doctor.
Identification of the doctor
Doctor should:
• print their name beside their signature;
• give their GMC number beside theirqualifications;
• doctors should be contactable by theMedical Referee, who is required tosatisfy themselves that Forms B and Chave been completed satisfactorily.Medical Referees will usually completetheir enquiries and forms on Saturdaysand some Bank Holidays so that formsare usually processed within two calendardays, to allow for funeral arrangements tobe finalised. Ideally doctors should give adaytime contact (e.g. bleep number,mobile phone number) for the two daysafter completing the forms.
10
11
12
13
14
15
17
19
20
21
16
RF Preliminary - DHSSPS 315-008-050
9
10
RF Preliminary - DHSSPS 315-008-051
How to complete cremation Form B side 2 Page 47
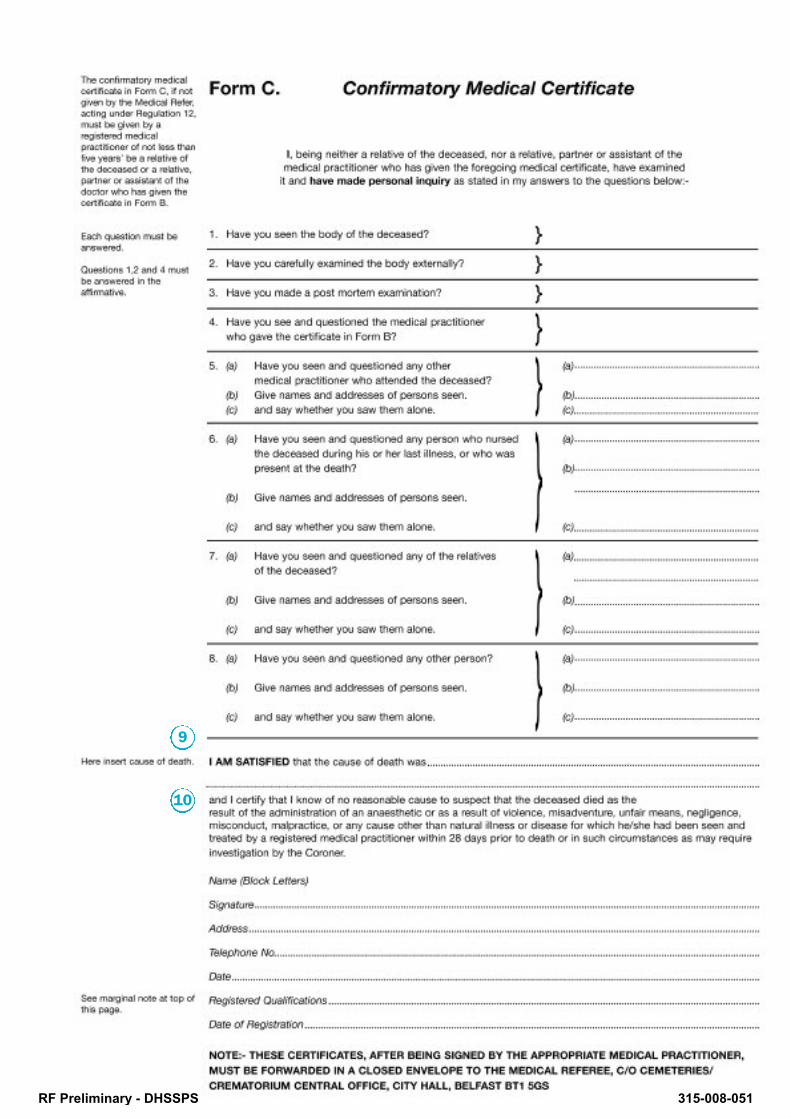
Form C should only be completedwhere one is required under theCremation Regulations. Form C is notrequired where:
a. A post-mortem examination hasbeen carried out by a medicalpractitioner appointed by theCremation Authority and who hasissued a Form D;
b. A post mortem examination hasbeen carried out and the cause ofdeath certified by the coroner(Form E).
Have you seen the body of thedeceased?
Have you carefully examined thebody externally?
Have you made a post mortemexamination?
The doctor completing Form C isexpected to have seen and examinedthe body.
Have you see and questioned themedical practitioner who gave thecertificate in Form B?
If the medical practitioners have notseen each other, Form C should becompleted to show that the enquirieshave been ‘adequate’, for example bytelephone conversation.
Have you seen and questioned anyother medical practitioner whoattended the deceased?
Have you seen and questioned anyperson who nursed the deceasedduring his or her last illness, or whowas present at the death?
Have you seen and questioned any ofthe relatives of the deceased?
You should have questioned a doctorother than the one who completedFrom B, a nurse or a relative i.e. beable to answer “Yes” to at least one ofquestions 5, 6 or 7.
How to complete cremation Form C – confirmatorymedical certificate
Have you seen and questioned anyother person?
Form C doctors should speak toanother doctor or nurse who attendedthe deceased, or a relative or otherperson (i.e. they should be able toanswer “Yes” to one of questions 5-8on Form C). This will support theirstatement that they know of noreasonable cause to refer the case forinvestigation by the coroner.
The cause of death This does not need to be the same asthe one given on the Form B, but anydiscrepancy should be explained. Medical referees will expect that the evidence offered on the certificatesdemonstrates sound clinical groundsfor the cause of death given, andForms B and C should be completedwith this in mind.
Continue over page >
4
5
8
1
2
9
6
7
3
RF Preliminary - DHSSPS 315-008-052

10
How to complete cremation Form B side 2 Page 48
Identification of the doctor
Doctor should:
• print their name beside theirsignature;
• give their GMC number beside theirqualifications;
• Doctors should be contactable bythe Medical Referee, who isrequired to satisfy them selves thatForms B and C have beencompleted satisfactorily. MedicalReferees will usually complete theirenquiries and forms on Saturdaysand some Bank Holidays so thatforms are usually processed withintwo calendar days, to allow forfuneral arrangements to befinalised. Ideally doctors shouldgive a daytime contact (e.g. bleepnumber, mobile phone number)for the two days after completingthe forms.
How to complete cremation Form C – confirmatorymedical certificate (continued)
RF Preliminary - DHSSPS 315-008-053

Form for Certificates of:
Stillbirth
RF Preliminary - DHSSPS 315-008-054

2
FETAL ANOXIA
PROLONGED LABOUR
BREECH PRESENTATION
HYPERTENSION (ARISING DURINGPREGNANCY)
RF Preliminary - DHSSPS 315-008-055

The stillbirth register is separate from the Register of Births and theRegister of Deaths.
Northern Ireland (Births and Deaths Registration Order 1976 asamended by the Stillbirth Definition Northern Ireland Order 1992),requires that any ‘child’ expelled or issued forth from its mother afterthe 24th week of pregnancy that did not breathe or show any othersigns of life be registered as a stillbirth.
Fetuses born dead before 24 weeks of pregnancy are not registeredas stillbirths. No statutory forms need to be completed, and the familydo not need to attend the registrar.
A fetus which is delivered after 24 weeks, but which was dead by the24th week are not registered as stillbirths. Further guidance on thesecases can be found on the websites of the Royal College ofObstetricians & Gynaecologists www.rcog.org.uk and the nursing &midwifery council www.nmc-uk.org.
A child who breathed or showed other signs of life is considered live-born for registration purposes, irrespective of the number of weeksduration of the pregnancy. In these cases either a doctor involvedmust complete an MCCD or the death must be referred to the coroner.
What is a stillbirth? Page 51
What is a stillbirth?
The coroner’s role in stillbirths
The coroner does not investigatestillbirths, unless there is doubtabout whether or not the childwas stillborn.
RF Preliminary - DHSSPS 315-008-056
Page 52 What is a stillbirth?
Who should complete the stillbirthform
Stillbirth forms can be completed by amedical practitioner who was presentat the birth, or who examined thebody. Foundation level doctors shouldnot complete stillbirth forms withoutdiscussion with a more seniorcolleague.
A registered midwife who was presentat the birth or examined the body canalso complete the stillbirth certificate.
How to complete the stillbirth form
Part I - Sequence leading to death,underlying cause
You have to start with the immediate,direct cause of stillbirth, then to goback through the sequence of eventsor conditions that led to death onsubsequent lines, until you reach theone that initiated the fatal sequence. Ifthe certificate has been completedproperly, the condition on the lowestcompleted line of part I will havecaused all of the conditions on thelines above it.
Avoid using general terms such asprematurity, anoxia, intra-uterine deathor maternal haemorrhage withoutclarifying the cause of the condition. In maternal conditions e.g.hypertension, diabetes state if thecondition existed before pregnancy orarose during pregnancy.
Part II - Contributory causes
You should enter any other diseases,injuries, conditions, or events thatcontributed to the stillbirth, but werenot part of the direct sequence, inpart II of the certificate.
Identification of the doctor ormidwife
The doctor or midwife should:
• print their name beside theirsignature;
• give their GMC/NMC number besidetheir qualifications;
• ensure the residence given willallow the registrar to contact them ifneeded (e.g. in hospital should giveward or bleep number, incommunity give practice or mobilenumber).2
1 3
RF Preliminary - DHSSPS 315-008-057


















