
Group D: Team Project Paper HIE Exchange in an...
15
Group D: Team Project Paper HIE Exchange in an Emergency Room Environment Wade Astin, Tracy V. Nunnery, Biljana Spasic, John Stoudenmire MED INF 405 DL Sec 55 Summer 2012 Northwestern University
Transcript of Group D: Team Project Paper HIE Exchange in an...

Group D: Team Project Paper
HIE Exchange in an Emergency Room Environment
Wade Astin, Tracy V. Nunnery, Biljana Spasic, John Stoudenmire
MED INF 405 DL Sec 55
Summer 2012
Northwestern University

Group D 2
Contents
What is an HIE? ............................................................................................................................................................. 3
Benefits of a HIE ....................................................................................................................................................... 3
Types of HIE ............................................................................................................................................................. 4
Examples of existing HIE ......................................................................................................................................... 4
Stakeholders .................................................................................................................................................................. 5
Functional Requirements ............................................................................................................................................... 7
Clinical Functionality .................................................................................................................................................... 8
Use of Standards ............................................................................................................................................................ 8
Technical Design ........................................................................................................................................................... 9
Data Flow Example ................................................................................................................................................. 10
Barriers to Implementing HIE ..................................................................................................................................... 11
Conclusion ................................................................................................................................................................... 12
References ................................................................................................................................................................... 13

Group D 3
What is an HIE?
While it is widely accepted that use of the electronic medical record can improve the quality and safety of healthcare
delivery, the EMR is itself part of a much larger vision of a unified network of health information exchange across
multiple providers. However, adoption of the electronic medical record (EMR) – a fundamental building block of
this vision - has been slow. In 2009, Bluementhal, described that “…only 17% of U.S. physicians and 8 to 10% of
U.S. hospitals have at least a basic electronic health record system. Far fewer have — and routinely use — the types
of comprehensive systems that would allow them to fully realize the potential of the technology” (Blumenthal
2009). While the Bush Administration initially tried to jump start more widespread development of the EMR by
creating in 2004 the Office of the National Coordinator (ONC) for Health Information Technology, the Obama
Administration gave a more decisive push in 2009 with the Health Information Technology for Economic and
Clinical Health Act (HITECH), part of the American Recovery and Reinvestment Act. This legislation codifies the
ONC, and charges it with developing not only widespread use of EMR but also a system of governance for a
nationwide health information network.
A Health Information Exchange (HIE) is defined as the “electronic movement of health-related information among
organizations according to nationally recognized standards” The Healthcare Information and Management Systems
Society (HIMMS) definition develops this idea further by adding that health information is to be exchanged, “… in
an authorized and secure manner.” (HIMSS, 2012) The participants of a HIE can include many entities such as
hospitals, doctor groups, labs, pharmacies, and payers. As use of the electronic medical record expands, more
specialized caregivers can also join HIEs, including rehabilitation and long-term care facilities. The most common
type of data shared include lab results, clinical summaries, medication lists, and medical image reports. Below is a
graphic from GE’s eHealth that helps illustrate the concept of a HIE.
Figure 1. HIE Concept map
(GE eHealth)
Benefits of a HIE
The ONC provides several benefits for the establishment of a HIE. (healthit.gov, 2012)

Group D 4
Provides a vehicle for improving quality and safety of patient care
Provides a basic level of interoperability among EHRs maintained by individual physicians and
organizations
Stimulates consumer education and patients' involvement in their own health care
Helps public health officials meet their commitment to the community
Creates a potential loop for feedback between health-related research and actual practice
Facilitates efficient deployment of emerging technology and health care services
Provides the backbone of technical infrastructure for leverage by national and State-level initiatives
The North Carolina Health Information Exchange (NCHIE) is an example of an active HIE. The NCHIE provides a
list of the benefits they have experienced:
Emergency Departments with connectivity to an HIE have improved productivity by more than 20%
Across all insurance types, EHR sites were associated with significantly higher achievement of care and
outcome standards and greater improvement in diabetes care.
By reducing their dependence on paper records, a practice seeing 3,000 patients annually could save
$24,000.
At the highest level of health IT adoption, only 0.001% of prescriptions would require a phone call between
a pharmacist and physician (NCHIE, 2012)
Types of HIE
HIMSS provides descriptions of the three common HIE types: the Centralized, the Decentralized (Federated), and
the Hybrid. (HIMSS, 2012)
Centralized: A typical centralized architecture is implemented as a logical, single database that aggregates
identified data from multiple sources in one location. All data exists in a single warehouse. Participants
send their data to a central repository.
Decentralized (Federated): A federated architecture model provides organizational control of the health
information and provides the framework for data-sharing capability to organizations widely distributed
across regions. This model allows the data source organizations to manage and store the patient health
information and indices. When requested, data is queried from the data source organization and not stored
centrally.
Hybrid: A hybrid architecture model uses a system where some health information and data is physically
stored and managed in a central location and other data is stored and managed by data source organizations
with a common framework for data-sharing capability. When requested, data is queried from either the
central repository or the source organizations depending on use cases.
According to HIMSS the Hybrid model is described as the “best of both worlds” from setup, socio-economic,
political and management perspectives. HIMSS also describes the Hybrid model as the most flexible. HIMMS
shows that the Hybrid model has only medium risks, but also a high amount of benefits. (HIMSS, 2012)
Examples of existing HIE
There are several examples of HIEs already in use, both public and private. For example, the Indiana Health
Information exchange network claims to be the largest Health Information Exchange in the nation. The IHIE
explains that they are “providing a secure and robust statewide health information technology network that
connects over 90 hospitals, long-term care facilities, rehabilitation centers, community health clinics and other
healthcare providers in Indiana. This network serves more than ten million patients and over 20,000 physicians
throughout the country. ” (Indiana Health Information Exchange, 2012) While the Indiana Health Information
Exchange is the largest, the Delaware Health Information Exchange Network (DHIN), launched in 2007, describes
themselves as the first operational statewide information exchange, and currently celebrated their fifth anniversary
since HIE “go live”. (DHIN, 2012) As stated above, North Carolina also has a mature HIE.
An example of a private vendor supplying a HIE is “eHealth” a Health Information Exchange product offered by GE
healthcare. It is interesting to note the GE’s Health Information Exchange (HIE) solution states that it’s framework

Group D 5
supports all three models of HIE. GE advertises that, “Data can be stored in several ways, as dictated by business
and security requirements including federated, centralized or hybrid systems.” (GE Healthcare, 2012)
Stakeholders
The successful implementation of an HIE depends heavily on a number of different stakeholders. Stakeholder
support and buy-in can be critical in determining whether a project succeeds or fails. “Data accessibility, reliability,
and accuracy are critical factors in obtaining the trust of stakeholders, including consumers, and in sustaining long-
term data exchange on a large scale” (Acker, 2007). Ideally, projects should have stakeholders who are informed of
the goals, represent the needs of the organization, committed to the project and also authorized to make decisions
(Rozanski, 2005). In an emergency room setting, these primary stakeholders include patients, providers and the
hospital in which it operates. Secondary stakeholders also exist including payers of health care services, employers,
providers of health care plans and the community which the HIE serves. Overall, a successful HIE requires “a
coordinated set of behavior changes on the part of providers, insurers, and payers” (Wagner, 2006).
In a business sense, some stakeholders rely on an HIE to “look like, act like, and operate like a business when in fact
the stakeholders come from many different industry sectors and are sometimes competitors” (Middleton, 2010). For
physicians, patients, researcher and the community at large, the measure of success may be quite different. For these
constituents, an efficient and functioning HIE system translates into increased access and speed for services, a
higher quality of care, an increase in patient safety, lower costs for health care as well as improved collaboration,
measurement of evidence-based medicine initiatives and expedited coordination of care among providers of health
care services.
Involving stakeholders in the early phases of a project can have a number of benefits. Stakeholders can actively
support the project and encourage confidence in others and influence resources. Stakeholders can also be critical in
gauging the reaction of others and helping shape approaches, anticipating criticism or adjusting the project as
needed. Because of their importance in the success of a project, their input should be a determining factor in the
architecture of the system. “The first step in Stakeholder Analysis is to identify who your stakeholders are. The next
step is to work out their power, influence and interest, so you know who you should focus on. The final step is to
develop a good understanding of the most important stakeholders” (Mind Tools, 2012). After the stakeholders are
identified, it is also important to understand their motivations, communications patterns, influences as well as the
nature of their investment in the project. The needs of the stakeholders can then be clarified and prioritized and
included as a part of the overall project design. “A very good way of answering these questions is to talk to your
stakeholders directly – people are often quite open about their views, and asking people's opinions is often the first
step in building a successful relationship with them” (Mind Tools 2012).
Improvements to a system of care which include HIE can have a positive impact on the overall health of the
community and can also improve the accessibility of coordination of services for the under-served. In an ER
environment, the most obvious stakeholder of an optimally-functioning HIE is the patient. The advantages to
patients can include reduced wait times to receive services, improved engagement with the physicians and nursing
staff, greater access to their personal health information, reduced medical error rates and duplicative lab testing or
medication administrations. All of these factors can provide an overall improvement of the quality of care they
receive. “Research conducted by the eHealth Initiative suggests that the more consumers learn about the creation of
secure HIEs, the more they support these initiatives. The HIE message that tends to resonate the most with
consumers is that of having access to information in an emergency medical situation, followed by access to medical
records when out of state and access to medical records when visiting a doctor” (Wiegand, 2007).
Physicians, nursing and staff can also clearly benefit from the advantages provided by HIE. The data physicians use
to guide their decisions and formulate care plans can be based upon more reliable, accurate and up-to-date patient
information. The availability of accurate past medical histories is especially important in an ER, since information is
needed quickly and patients may be incapacitated or unable to communicate. “From the physician stakeholder
perspective, the goal of reduced costs and improved revenues will be achieved through savings in time, overhead,
human resources and materials, as well as through the ability to see more patients” (Fleming, 2010). Physicians are
also able to more easily and accurately document patient encounters, electronically order clinical labs or prescribe
medications or collaborate and follow-up with other members of the care team.

Group D 6
From a financial perspective, an HIE can increase revenues by increasing the number of patient encounters per
provider, per day. Malpractice insurance rates can also be lessened as a result of the higher quality of care and
potential reduction in error rates. “For hospital stakeholders, goals might be defined as a reduction in time spent on
patient intake and shorter wait times in Emergency Departments. The HIE could result in a reduction in medication
errors due to more complete information at the point of care, and streamlined communications of orders and results
that can lead to earlier discharges, when medically appropriate, which save the hospital money in payment models
that are based on per episode vs. length of stay” (Fleming, 2010).
Another positive impact of an HIE is the reduced storage footprint as compared to paper-based record keeping. In
the ER where space may be constrained and records rooms inconveniently located, an HIE can provide ready-access
to information and paper storage areas can be otherwise repurposed - - This results in reduced waiting times for ER
patients, an increased throughput of patients and potentially increased revenue from improved claims management
and capture of services rendered to patients.
Figure 2. HIE stakeholders

Group D 7
(Middleton, 2010)
Research, quality of care and public health initiatives can also be important stakeholders in health information
exchanges. “Local health information exchanges (HIEs) hold the promise of collecting patient clinical data across
sites of care to provide more complete and timely information for treatment, as well as supporting quality
improvement and reporting, public health activities, and clinical research” (Grossman, 2008). Especially when
integrated as a part of an emergency room, HIE is positioned to support population heath and quality assurance
initiatives. Using discretely coded patient data, patients who exhibit common characteristics or sharing a common
condition can be easily identified and managed. This can be leveraged to assist with quality of care initiatives by
providing a means to assess the quality of care for patients with a within a disease or symptom-specific cohort. Data
which is coded and shared within an HIE can be critical in identifying potential candidates for clinical research and
also be used to detect sentinel events and syndromic surveillance efforts. Information from an ER or group of ERs
can create a repository of data which can be monitored for specific symptoms or conditions. When shared within the
context of an HIE, the presence or occurrence of a significant of environmental, bioterror or epidemiological event
can be detected over a large region.
There are also secondary stakeholders who can be beneficiaries of an HIE-enabled system. For payers of service
such as insurance companies, an HIE can improve the capability to determine the use of quality measures as well as
utilization rates and provide efficiencies in the review of claims and resolution of disputes. Employers can also
realize similar benefits and cost reductions improving preventative medicine and management or chronic disease,
improving employee attendance and reducing worker’s compensation claims. Employer stakeholders will realize a
positive “through a reduction in the amount of time spent managing claims appeals, reductions in Emergency
Department visits by employees with chronic conditions—which also results in costs related to lost productivity—
and improved management of workers compensation claims” (Fleming, 2010).
Functional Requirements
An emergency department has unique HIE and EHR needs, with functional requirements being met by an
Emergency Department Information Systems (EDIS). The environment is high-speed and dynamic. The ED needs to
have rapid and accurate access to records already in the hospital’s system as well as communication and sharing of
patient information from and to other medical organizations including the primary physician. Rothenhaus, T.,
Kamens, D., Keaton, B. F., Nathanson, L., Nielson, J., Mcclay, J. C., Taylor, T. B. & Villarin, A. (2009) offer

Group D 8
suggestions on emergency department-specific functional requirements. These are broken into clinical functionality,
administrative functions and other considerations.
Clinical Functionality
Patient Entry: Rothenhaus, T., Kamens, D., Keaton, B. F., Nathanson, L., Nielson, J., Mcclay, J. C., Taylor, T. B. &
Villarin, A. (2009) define this as the process of uniquely identifying a patient in the EDIS. The process can begin at
triage, entering the patient into the EDIS and assigning a unique identifier.
Patient tracking: Tracking consists of patient-centered and department-centered tracking. Patient- centered tracking
includes a clinical course which follows the patient through the ED process and patient-location tracking which
tracks all phases of the hospital process from pre-arrival through discharge.
Department dashboards: These are administrative tools which monitor key performance indicators. Examples
include the number of patients: waiting to be seen, in waiting room and awaiting inpatient bed assignment.
Clinical Documentation: The system must be able to provide quick, efficient, accurate and complete patient
information. Having the ability to utilize already gathered patient information can reduce time and redundancy. The
system must also be able to link documentation to medical billing.
Computer Provider Order Entry (CPOE): A requirement of HIE as well as an EDIS is that a physician should be
able to order laboratory, radiology, medications, nursing tasks and medical equipment. In order to complete orders
and prioritize tasks, physicians benefit from a task management system and order acknowledgement replies.
Result Reporting: Rothenhaus, T., Kamens, D., Keaton, B. F., Nathanson, L., Nielson, J., Mcclay, J. C., Taylor, T.
B. & Villarin, A. (2009) state that key features are easy access and review within the context of each EDs particular
workflow. The system should be easily customizable for the specific needs of the ED.
Discharge Management: An HIE and EDIS should be able to exchange data to both medical organizations for
follow-up as well as patients. Examples of functions can include prescriptions, discharge education and instructions
and follow-up information.
Administrative Functions: Billing and financial management are key functions required for an EDIS. A function of
an HIE and EDIS should be auditing and logging data for reporting. Another function could be the reporting of
mandated public health diseases.
Other Considerations: HIE and particularly an EDIS should have directory services as a component to the system.
Types of directories can include users or individuals, organizations and locations, data services by organizations or
service providers and semantics or terminology as well as translation services, (HLN Consulting, LLC). Also,
emergency departments require an HIE which can communicate data between disparate computer systems. These
should be in compliance with HL7 standards as well.
Use of Standards
Standards provide a framework or format for which information systems, EHRs and medical providers can work
together. A standard is a recognized, approved and adopted way of doing things in the industry. Standards are
critical in creating interoperability among varying systems. Most official IT standards are set by ANSI (American
National Standards Institute), IEEE (Institute of Electrical and Electronic Engineers) and VESA (Video Electronics
Standards Association), (Webopedia). In HIE, other standards apply as well. Although no emergency department-
specific standards were noted, ED utilizes many standards implemented throughout HIE.
Meaningful Use: The Health Information Technology for Economic and Clinical Health (HITECH) Act
was created to improve healthcare quality, safety and efficiency through the use of HIE/EMR and private
and secure electronic information exchange, (Office of the National Coordinator for Health Information
Technology). Medical professionals who are in compliance with the meaningful use objectives can be
eligible for Medicaid and Medicare incentives.
LOINC: LOINC (Logical Observation Identifiers Names and Codes) is a database and standard for
measuring laboratory results. Vreeman, D. (2010) states LOINC was developed to provide a definitive
standard for identifying clinical observation in electronic reports. This standard has been designated for use
in the U. S. Federal Government systems for the exchange of clinical health information, (U.S. National
Library of Medicine).
SNOMED-CT: SNOMED-CT (Systemized Nomenclature of Medicine-Clinical Terms), according to the
International Health Terminology Standards Development Organization, is the most comprehensive,
Group D 9
multilingual healthcare terminology in the world . This standard is able to cross-map to other international
standards and is used in more than fifty countries. SNOMED can assist in recording, storing and retrieving
data within the EMR as well.
RxNorm: According to the National Library of Medicine, RxNorm provides normalized names for clinical
drugs and links its names to many of the drug vocabularies commonly used in pharmacies. NLM adds that
RxNorm now includes the National Drug File-Reference Terminology (NDF-RT) from the Veterans Health
Administration, (National Library of Medicine).
DICOM: “DICOM is a global Information-Technology standard that is used in virtually all hospitals
worldwide,” states DICOM (Digital Imaging and Communications in Medicine). Among other functions,
DICOM is designed to create interoperability of systems used to produce, store, retrieve and view medical
images. This standard ensures interoperability among many medical departments and units. Examples
include radiology, cardiology and neurology.
HL-7: HL-7 provides a comprehensive framework and related standards for the exchange, integration,
sharing, and retrieval of electronic health information (Health Level 7 International). HL-7 standards define
how information is packaged and communicated from one party to another, setting the language, structure
and data types required for seamless integration between systems.
CCD: A continuity of care document is an electronic summary of all of a patient’s clinical information.
This standard provides physicians with the ability to share a patient’s medical history and current condition
in a comprehensive representation. CCD is typically used in among other capacities, emergency
departments. CCD is one of two formats required by the government to achieve meaningful use.
Technical Design
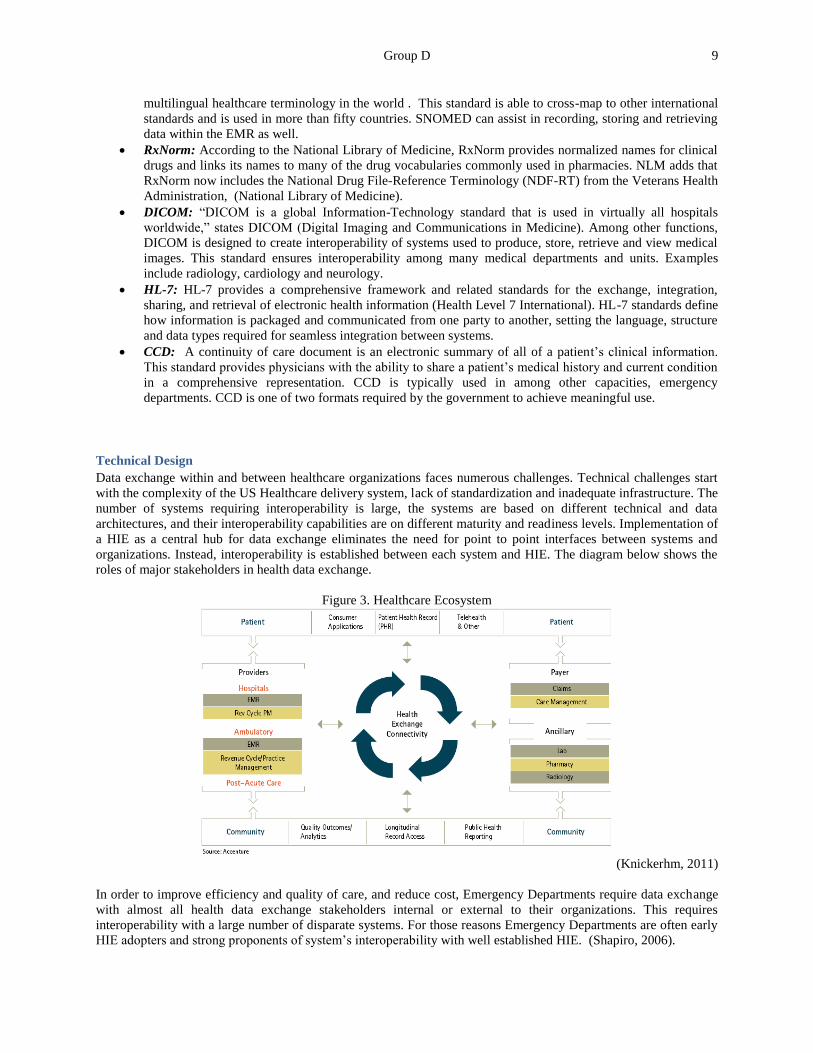
Data exchange within and between healthcare organizations faces numerous challenges. Technical challenges start
with the complexity of the US Healthcare delivery system, lack of standardization and inadequate infrastructure. The
number of systems requiring interoperability is large, the systems are based on different technical and data
architectures, and their interoperability capabilities are on different maturity and readiness levels. Implementation of
a HIE as a central hub for data exchange eliminates the need for point to point interfaces between systems and
organizations. Instead, interoperability is established between each system and HIE. The diagram below shows the
roles of major stakeholders in health data exchange.
Figure 3. Healthcare Ecosystem
(Knickerhm, 2011)
In order to improve efficiency and quality of care, and reduce cost, Emergency Departments require data exchange
with almost all health data exchange stakeholders internal or external to their organizations. This requires
interoperability with a large number of disparate systems. For those reasons Emergency Departments are often early
HIE adopters and strong proponents of system’s interoperability with well established HIE. (Shapiro, 2006).

Group D 10
The quality of patient care in ED benefits from easy and fast access to complete patient record and the most current
health information. The required information includes problem lists, diagnoses, allergies, medications and diagnostic
results, as well as a summary of patient health history, chronic conditions, etc. To take full advantage of HIE, ED
system’s interoperability requires data exchange that supports Continuity of Care Document (CCD) standard and
unrestricted access. Where there is no CCD interface available, interoperability via other standard HL7 messages is
a substitute. In cases of limited interoperability, HIE should provide a contact information for the healthcare
provider in support of two way data exchange via secure email.
Major concerns with making data available to many providers via HIE are related to security, such as controlled
access to all data and in particular restricted data, sharing with authorized providers only, ensuring patient privacy,
and maintaining confidentiality of personal health information. Security and access control are addressed by
implementing strict policies and procedures, and maintaining master provider directory with the appropriate
credentials. Unique identification of patients across all data sources that utilize HIE is managed via the master
patient index.
Figure 4. HIE architecture/tech design
Data Flow Example
HIMSS provides interoperability use cases to illustrate data exchange scenarios. The case referenced in the diagram
below illustrates clinical and data flow in a Emergency Department encounter, and exchange of restricted data with
other healthcare organizations and their systems, PCP and patient via HIE. In this use case HIE processes utilize
provider profiles to authorize appropriate access, enable required high level of interoperability and maintain integrity
of restricted data. The use case support Meaningful Use requirements of improving quality, efficiency and
coordination of care, enabling increased patients’ involvement, and protecting privacy. (HIMSS, 2012)

Group D 11
Figure 5. HIMSS Interoperability Showcase, EMS and ED Encounter
(HIMSS, 2012)
Barriers to Implementing HIE
Cost can be a limiting factor for adoption of healthcare information technology, and especially in the case of an HIE.
Since participation in system of electronic data exchange is highly dependent on the existence of an electronic
medical record system, this cost must also be considered as a part of any financial evaluation. “The cost of
implementing an EHR [is] estimated at $5,500 to $36,000 per physician” (Burton, 2004). Hardware, software and
maintenance needs are responsible for a portion of these costs but there are other costs relating to loss of
productivity during implementation, training and reduced number of patients which can be accommodated. In
addition to these expenses, there are also costs associated with the integration with external systems as well as fees
to access the HIE network. Federal programs have provided financial support to fund systems to share health
information. These funds are time-limited, with no assurances of future funding. “Failure to come up with a
sustaining financial model has doomed regional data-sharing organizations in the past; participants often don't see
the value in funding the exchanges out of their own pockets once the initial support dries up” (McGee, 2010).
In a system which is designed to share sensitive patient data, concerns regarding security and privacy must be fully
considered. “Because the United States has a large, private data collection industry governed by a conflicting
patchwork of federal and state laws and agencies, federal regulations will need to be modified to encourage secure
data exchange in the Nationwide Health Information Network” (Fontaine, 2010). Ensuring the security of sensitive
patient information is collective responsibly and includes protections for sharing, storage, transmission, archive and
dissemination. Although “there is scant legal precedent to offer guidance about the liability of a physician who acts
on clinical information made available in such situations” (Fontaine, 2010), legal and liability issues are important
considerations since physicians could act upon incorrect data or fail to act on correct data which is provided by an
HIE.
Interoperability is significant barrier to HIE implementation and may also be one of the most persistent since
“getting data in front of doctors and other clinicians is one of the biggest challenges HIEs face” (McGee, 2010).
Many proprietary commercial and home-grown EHR systems lack the necessary functionality to be able to exchange
data with other systems in a meaningful way. If a physician’s EMR is unable to directly interface with an external

Group D 12
system, there are other options such as portals which can provide the necessary information. “The problem with
portals is that they force doctors to take an extra step to view data--to remember to check the portal for new
information every time they're about to treat a patient. Doctors often end up using the HIE less as a result, and some
provider groups decide the exchange isn't worth the investment if their clinicians aren't using it” (McGee, 2010). A
primary reason for the lack of interoperability is the variability of coding systems used by organizations and EHR
vendors. A fully-interoperable HIE structure requires systems to be able to communicate with each other using a
known and agreed-upon lexicon for medications, laboratory values, conditions and other health care parameters.
Although standards for medical codes have been encouraged at the national level, interoperability continues to be a
significant technical barrier to HIE participation.
An International Journal of Medical Informatics article from 2007 reports that “almost two thirds of primary care
physicians surveyed in 2006 cited the lack of a strategic plan as a barrier to health IT implementation” (Anderson,
2007). These issues are coupled with physician who may be reluctant to use technology or who see electronic
systems as the cause for an increased workload. Physicians may also be concerned that new systems will interfere
with their established workflow and that training and learning new systems is both time-consuming and difficult.
Some organizations may also lack the necessary in-house technical staff or expertise to effectively support an HIE.
As reported in an article in from The Commonwealth Fund, “if careful consideration goes into developing policies
that address these challenges, the exchanges will be able to accomplish what they are intended to do: expand access
to affordable health insurance coverage, improve the quality of coverage, and reduce costs. These are outcomes that
will benefit the health system overall” (Jost, 2010).
Some organizations or agencies may have concerns with sharing information and potentially collaborating with
competing organizations. Participation in an HIE “requires competing and adversarial parties to collaborate and
share their most valued asset: patients and their data” (Grossman, 2006). The “fragmented and competitive US
health care system [provides] few offsetting incentives for sharing clinical data” (Anderson, 2007). This loss of
competitive advantage, either real or perceived, is certainly a factor which may impede willingness to participate in
a data-sharing system.
Conclusion
An emergency department has unique needs and has much to gain from access to a HIE. While access to the HIE
may occur outside the EMR workflow, an HIE offers a relatively easy insight into a patient’s scenario, Information
regarding historical problems, past procedures, allergies, active medications, etc. saves both time and resources upon
each ED visit. In fact, the NCHIE reports that “Emergency Departments with connectivity to a HIE have improved
productivity by more than 20%.” The claim is also supported by research by Frisse et al (2012), where Emergency
Room encounters in Tennessee were studied over a 13 month period. They reported that HIE access for the ED
resulted in a decrease in hospital admissions and cost savings primarily through reductions in duplicative CT and
Lab tests (Frisse, 2012). Through the use of standard terminologies, such as LOINC, SNOMED-CT, RX Norm, even
the complex barriers to semantic interoperability can be reduced; however, there is still much work to do in these
realms. Barriers such as software and hardware costs, ensuring security and privacy, staffing shortages, and the
Clinician perception of a disruption to clinical workflow also remain a challenge.

Group D 13
References
Acker, B. (2007, September). HIM Principles in Health. Retrieved from AHIMA:
http://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_035095.hcsp?dDocName=bok1_035095.
Anderson, J. (2007). Social, ethical and legal barriers to e-health. International Journal of Medical Informatics, 480-
3.
Aratow, M.. Navigating the Electronic medical records (EMR) terrain: A guide for emergency departments. CEP
America white paper. CEP America. Retrieved from http://www.healthleadersmedia.com/content/272577.pdf
DICOM general information brochure. Digital Imaging and Communications in Medicine. Retrieved from
http://medical.nema.org/dicom/geninfo/brochure.pdf.
Burton, L. (2004). Using electronic health records to help coordinate care. Milbank Quarterly, 457-81.
DICOM general information brochure. Digital Imaging and Communications in Medicine. Retrieved from
http://medical.nema.org/dicom/geninfo/brochure.pdf
Electronic health records and meaningful use. The Office of the National Coordinator for Health Information
Technology. Retrieved from http://healthit.hhs.gov/portal/server.pt?open=512&objID=2996&mode=2
DHIN. (2012). Delaware Health Information Network. Retrieved August 6, 2012, from http://www.dhin.org/
Fontaine, P. (2010). Systematic Review of Health Information Exchange in Primary Care Practices. Journal of
the American Board of Family Medicine, 655-670.
Fleming, M. (2010). Common Goals for the Community HIE: Building a Roadmap. Center for Community Health
Leadership. Retrieved from www.allscriptscenter.com.
Frisse ME, Johnson KB, Nian H, et al . The financial impact of health information exchange on emergency
department care. J Am Med Inform Assoc 2012;19:328–33.
GE Healthcare. (2012). eHealth Information Exchange. Retrieved August 6, 2012, from
http://ehealth.gehealthcare.com/ehealth-products/ehealth-info-exchange/.
Grossman, J. (2006). Hospital-physician portals: the role of competition in driving clinical data exchange. Health
Affairs, 1629-36.
Grossman, J. (2008). Creating sustainable Local Health Information Exchanges: Can Barriers to Stakeholder
Participation be Overcome? Center for Studying Health System Change. Retrieved from
http://www.hschange.org/CONTENT/970/.
Guilford-Blake, Roxanna. (2010). 8 HIE Implementation Barriers Detailed. Health Leaders Media. Retrieved from
http://www.healthleadersmedia.com/page-1/TEC-257277/8-HIE-Implementation-Barriers-Detailed. HIMSS,
(2012). HIMSS Interoperability Show Case. 2012. Retrieved August 6, 2012 from
http://himss.myweeverapp.com/?paged=3.
Indiana Health Information Exchange. (n.d.). Retrieved August 6, 2012, from IHIE: http://www.ihie.com/.
International Health Terminology Standards Development Organisation. (2012). SNOMED-CT. International
Health Terminology Standards Development Organisation website. Retrieved from
http://www.ihtsdo.org/snomed-ct/.
Jost, T. (2010). Health Insurance Exchanges: Overcoming Implementation Barriers. The Commonwealth Fund.
Retrieved from http://www.commonwealthfund.org/Blog/2010/Sep/Health-Insurance-Exchanges.aspx.

Group D 14
Knickerhm, M., Ficery, K. (2011). Secrets of Success on the EMR Journey to Meaningful Use: Leading
HospitalCIOs Reveal Key Lessons Learned. Accenture, 2011. Retrieved August 6, 2012 from
http://www.accenture.com/SiteCollectionDocuments/PDF/Secrets_to_Success_on_the_Journey_to_Meaningful
_Use.pdf#zoom=50.
McGee, M. (2010). Health Information Exchanges’ Tech Challenges. Information Week. Retrieved from
http://www.informationweek.com/news/healthcare/interoperability/228800047.
Middleton, B. (2010). Best Practices for Community Health Information Exchange. Center for Community Health
Leadership. Retrieved from www.allscriptscenter.com.
Mindtools. (2012). Stakeholder Analysis: Winning Support for Your Projects. Mind Tools website. Retrieved from
http://www.mindtools.com/pages/article/newPPM_07.htm.
NCHIE. (2012). NC Health Information Exchange. Retrieved August 6, 2012, from http://nchie.org/?page_id=187.
ONC. (2012). Department of Human Services . Retrieved August 6, 2012, from Office of the national Coordinator
for Health Information Technology: http://www.healthit.gov/providers-professionals/health-information-
exchange.
The Office of the National Coordinator for Health Information Technology (ONC). (2011). Electronic health
records and meaningful use. The Office of the National Coordinator for Health Information Technology.
Retrieved from http://healthit.hhs.gov/portal/server.pt?open=512&objID=2996&mode=2.
Rothenhaus, T. C., Kamens, D., McClay, J. & Coonan, K. (2007). Emergency department information systems
(EDIS) functional profile. EDIS Functional Profile Working Group Emergency Care Special Interest Group
Health Level 7. Draft Version 1.02. 2/15/2007. Retrieved from
http://www.providersedge.com/ehdocs/ehr_articles/HL7_2007_EHR-
S_FM_R1Example_Functional_Profile_EDIS.pdf.
Rozanski, N. (2005). Software Systems Architecture. Prentice Hall. Upper Saddle River, NJ.
Shapiro, J., Kannry, J., Lipton, M., Goldberg, E., Conocenti, P., Stuard, S., Wyatt, B., Kuperman, G. (2006).
Approaches to Patient Health Information Exchange and Their Impact on Emergency Medicine. Annals of
Emergency Medicine 2006. Retrieved August 6, 2012 from
http://www.sciencedirect.com.ezproxy.galter.northwestern.edu/science/article/pii/S0196064406004884.
U.S. National Library of Medicine. (2012). Introduction to HL7 standards. Health Level Seven International.
Retrieved from http://www.hl7.org/implement/standards/index.cfm?ref=nav.
U.S. National Library of Medicine. (2011). Logical observation identifiers names and codes (LOINC). Retrieved
From http://www.nlm.nih.gov/research/umls/loinc_main.html.
U.S. National Library of Medicine. (2012). RxNorm. U.S. National Library of Medicine, National Institutes of
Health. Retrieved from http://www.nlm.nih.gov/research/umls/Snomed/snomed_main.html.
Vermont (Government Site). (2011). The CCD: Continuity of care document. VITL.5 Jan 2011. Retrieved from
http://hcr.vermont.gov/sites/hcr/files/4_-_Fundamentals_of_HIE_-_CCD.pdf.
Vreeman, D. (2010). LOINC overview. LOINC: Logical Observation Identifiers Names and Codes. 2010-12-21.
Retrieved from http://loinc.org/faq/getting-started/getting-started/.
Wagner, E. (2006). It Takes a Region: Creating a Framework to Improve Chronic Disease Care. California
HealthCare Foundation. 2006.
Webopedia. (2012). Definition. Webopedia website. Retrieved from

Group D 15
http://www.webopedia.com/TERM/S/standard.html.
Wiegand, T. (2007). Staying on Track: Facilitating an Ongoing Discourse Among Stakeholders. Center for
Community Health Leadership. Retrieved from www.allscriptscenter.com.


















