
Granulomatous Rosacea or Rhinophyma
8
ONLINE FIRST OBSERVATION Cutaneous B-Cell Neoplasms Mimicking Granulomatous Rosacea or Rhinophyma Aviv Barzilai, MD, MSc; Hana Feuerman, MD; Pietro Quaglino, MD; Michael David, MD; Meora Feinmesser, MD; Marisa Halpern, MD; Edit Feldberg, MD; Carlo Tomasini, MD; Hilla Tabibian-Keissar, PhD; Ninette Amarilgio, PhD; Emmilia Hodak, MD Background: Unlike T-cell neoplasms, B-cell lympho- proliferative disorders have a limited clinical spectrum of skin involvement. Cutaneous B-cell neoplasms mim- icking rosacea or rhinophyma are rare. Observations: We described 12 patients with B-cell lymphoproliferative neoplasms presenting with a facial eruption clinically mimicking rosacea or rhinophyma. Eleven patients were women; ages ranged from 36 to 81 years. The clinical presentation included small papules on the nose and cheeks and around the eyes mimicking granulomatous rosacea; nodules on the nose, cheeks, chin, or forehead mimicking phymatous rosacea; or a combination of both. Three patients had preexisting erythematotelangiectatic rosacea and 1 had rhino- phyma. Based on a clinicopathologic correlation and B-cell clonality analysis, the diagnosis was primary cutaneous follicular center B-cell lymphoma in 4 cases, primary cutaneous marginal zone lymphoma in 6, and skin involvement of chronic lymphocytic leukemia in 2. All patients had an indolent course as expected for their disease. Conclusions: Cutaneous involvement of B-cell neo- plasms may mimic granulomatous rosacea or rhino- phyma. This unusual clinical presentation is more com- mon in women and appears in the setting of preexisting rosacea or as a new eruption. Proliferative B-cell disor- ders should be added to the differential diagnosis of sym- metric papular or papulonodular eruptions of the face. Arch Dermatol. 2012;148(7):824-831. Published online April 16, 2012. doi:10.1001/archdermatol.2011.3575 B -CELL NEOPLASMS CAN IN- volve the skin as a primary cutaneous lymphoma or as a secondary process, includ- ing specific infiltrates of nodal or extranodal lymphoma or leuke- mia. 1 When involving the skin, both B- cell neoplasms, lymphoma and leuke- mia, have a distinct clinical appearance, presenting as isolated, grouped, or mul- tiple erythematous to violaceous pap- ules, plaques, or nodules, usually in an asymmetric distribution. B-cell lympho- proliferative diseases simulating rosacea are extremely rare. 2-8 In this report, we de- scribe 12 patients who presented with ro- sacea or rhinophymalike lesions and dis- cuss various aspects of this rare clinical manifestation of low-grade B-cell lym- phoma/leukemia involving the face. METHODS We performed a retrospective case analysis of 12 patients with cutaneous B-cell neoplasms who were referred to our tertiary dermatology clinics from January 1, 1996, through Decem- ber 31, 2010, for a persistent facial rash. The differential diagnoses included rosacea and rhinophyma. We retrieved clinical history, clinical findings, laboratory results, and follow-up data from the medical files and reviewed the biopsy specimens. Final diagno- sis was made according to the criteria of the World Health Organization or the European Organization for Research and Treatment of Cancer. 1 The study was approved by the local ethics committees. RESULTS The patients’ clinical data and final diag- noses are described in Table 1. The study group included 11 women and 1 man with a mean age of 57 (range, 36-81) years. The time elapsed from the initial presentation to the final diagnosis varied from a few months to 10 years (mean time, 23 months). The distin- guishing features of the clinical presenta- tion included nonpustular granuloma- Author Affiliations are listed at the end of this article. ARCH DERMATOL/ VOL 148 (NO. 7), JULY 2012 WWW.ARCHDERMATOL.COM 824 ©2012 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ on 12/07/2021
Transcript of Granulomatous Rosacea or Rhinophyma

ONLINE FIRST
OBSERVATION
Cutaneous B-Cell Neoplasms MimickingGranulomatous Rosacea or RhinophymaAviv Barzilai, MD, MSc; Hana Feuerman, MD; Pietro Quaglino, MD; Michael David, MD;Meora Feinmesser, MD; Marisa Halpern, MD; Edit Feldberg, MD; Carlo Tomasini, MD;Hilla Tabibian-Keissar, PhD; Ninette Amarilgio, PhD; Emmilia Hodak, MD
Background: Unlike T-cell neoplasms, B-cell lympho-proliferative disorders have a limited clinical spectrumof skin involvement. Cutaneous B-cell neoplasms mim-icking rosacea or rhinophyma are rare.
Observations: We described 12 patients with B-celllymphoproliferative neoplasms presenting with a facialeruption clinically mimicking rosacea or rhinophyma.Eleven patients were women; ages ranged from 36 to 81years. The clinical presentation included small papuleson the nose and cheeks and around the eyes mimickinggranulomatous rosacea; nodules on the nose, cheeks,chin, or forehead mimicking phymatous rosacea; or acombination of both. Three patients had preexistingerythematotelangiectatic rosacea and 1 had rhino-phyma. Based on a clinicopathologic correlation andB-cell clonality analysis, the diagnosis was primary
cutaneous follicular center B-cell lymphoma in 4 cases,primary cutaneous marginal zone lymphoma in 6, andskin involvement of chronic lymphocytic leukemia in 2.All patients had an indolent course as expected for theirdisease.
Conclusions: Cutaneous involvement of B-cell neo-plasms may mimic granulomatous rosacea or rhino-phyma. This unusual clinical presentation is more com-mon in women and appears in the setting of preexistingrosacea or as a new eruption. Proliferative B-cell disor-ders should be added to the differential diagnosis of sym-metric papular or papulonodular eruptions of the face.
Arch Dermatol. 2012;148(7):824-831.Published online April 16, 2012.doi:10.1001/archdermatol.2011.3575
B -CELL NEOPLASMS CAN IN-volve the skin as a primarycutaneous lymphoma or asa secondary process, includ-ing specific infiltrates of
nodal or extranodal lymphoma or leuke-mia.1 When involving the skin, both B-cell neoplasms, lymphoma and leuke-mia, have a distinct clinical appearance,presenting as isolated, grouped, or mul-tiple erythematous to violaceous pap-ules, plaques, or nodules, usually in anasymmetric distribution. B-cell lympho-proliferative diseases simulating rosacea areextremely rare.2-8 In this report, we de-scribe 12 patients who presented with ro-sacea or rhinophymalike lesions and dis-cuss various aspects of this rare clinicalmanifestation of low-grade B-cell lym-phoma/leukemia involving the face.
METHODS
We performed a retrospective case analysis of12 patients with cutaneous B-cell neoplasms
who were referred to our tertiary dermatologyclinics from January 1, 1996, through Decem-ber 31, 2010, for a persistent facial rash. Thedifferential diagnoses included rosacea andrhinophyma. We retrieved clinical history,clinical findings, laboratory results, andfollow-up data from the medical files andreviewed the biopsy specimens. Final diagno-sis was made according to the criteria of theWorld Health Organization or the EuropeanOrganization for Research and Treatment ofCancer.1 The study was approved by the localethics committees.
RESULTS
The patients’ clinical data and final diag-noses are described in Table 1. Thestudy group included 11 women and 1man with a mean age of 57 (range,36-81) years. The time elapsed from theinitial presentation to the final diagnosisvaried from a few months to 10 years(mean time, 23 months). The distin-guishing features of the clinical presenta-tion included nonpustular granuloma-
Author Affiliations are listed atthe end of this article.
ARCH DERMATOL/ VOL 148 (NO. 7), JULY 2012 WWW.ARCHDERMATOL.COM824
©2012 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 12/07/2021

tous rosacea-like lesions and rhinophyma/phymatousplaques (Table 1, Figure 1, and Figure 2). Fourpatients (patients 1-3 and 10) had a history of preexist-ing rosacea manifesting as erythematotelangiectaticrosacea (in 3 patients) and rhinophyma (in 1 patient)(Figure 3). Two of these patients developed rhinophy-malike lymphoma on the nose. Half the patients weretreated for rosacea with topical or systemic antibioticsor both, without any benefit (Table 1).
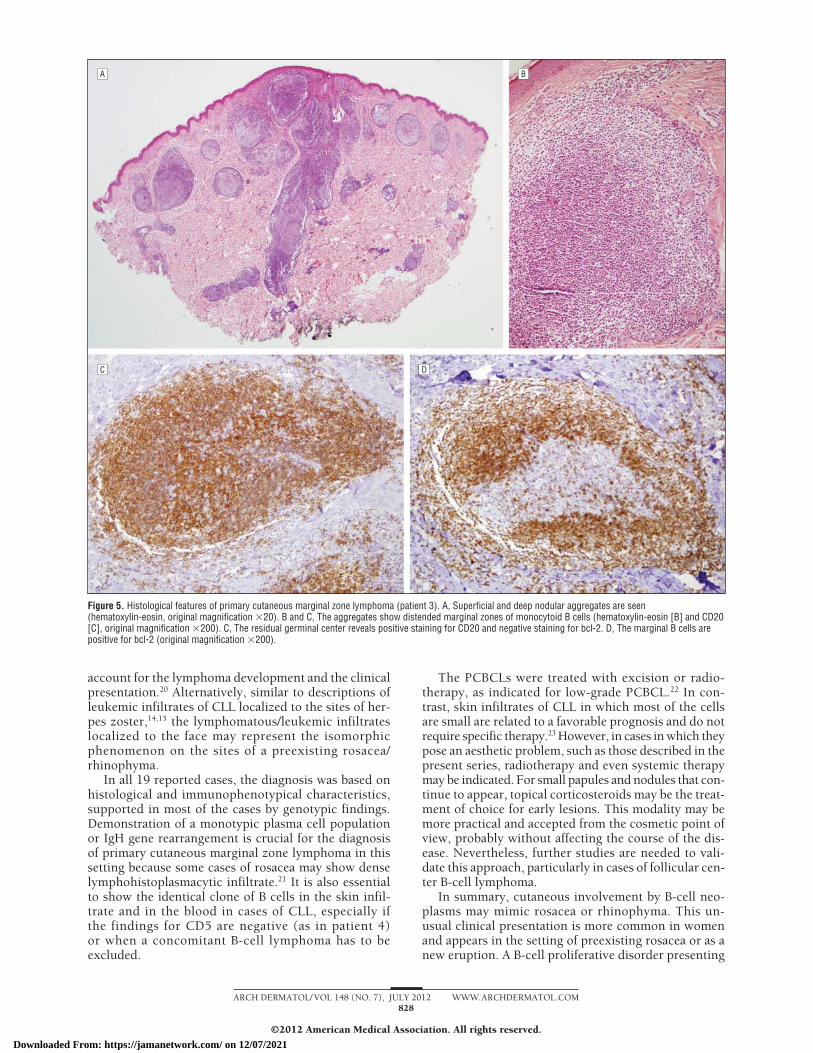
The histological and immunophenotypical featuresof the cases and the results of molecular studies aredescribed in Table 2. Four cases revealed superficialand deep nodular aggregates of centrocytes and centro-blasts, features of follicular-center cell lymphoma(Figure 4). Six cases showed superficial and deepnodular aggregates of small irregular B lymphocytes,some with a monocytoid or plasmacytoid appearance
Table 1. Clinical Data and Final Diagnosis in Patients With B-Cell Neoplasms Mimicking Rosacea or Rhinophyma
Patient No./Sex/Age, y
Duration BeforeDiagnosis Clinical Presentation Initial Diagnosis Early Therapy
FinalDiagnosis
1/F/51 3 y Papulonodular eruption on thecheeks; erythematous infiltratedplaque on the nose
Rosacea and rhinophyma Minocycline hydrochloride,topical metronidazole
PCFCL
2/F/48 4 mo Erythematous infiltrated plaque on thenose on top of rosacea
Rhinophyma None PCFCL
3/F/36 3 y Facial erythematous and skin-coloredpapules with erythema andtelangiectasia
Rosacea Erythromycin, minocycline PCMZL
4/F/67 6 mo Nodular eruption on nose, cheeks,and chin
Rosacea and rhinophyma Topical clindamycinphosphate
CLL, leukemiacutis
5/F/81 3 y Erythematous infiltrated plaque on thenose
Rhinophyma None PCMZL
6/F/60 4 mo Erythema on the distal part of thenose with 3 small nodules
Sebaceous hyperplasia,basaliomas;granulomatous rosacea
None PCMZL
7/F/52 6 mo Small erythematous papules oncheeks but also on neck, nape, andchest
Granulomatous rosacea None PCMZL
8/F/57 6 mo Small skin-colored to erythematouspapules on cheek, sides of thenose, eyebrows, helices, and upperback
Granulomatous rosacea,basaliomas, sebaceoushyperplasia
None PCFCL
9/F/36 6 mo Erythematous papules around themouth, including the chin and onthe nose
Granulomatous rosacea,sarcoidosis, andmolluscum
Liquid nitrogen PCMZL
10/M/74 10 y Erythematous infiltrated nodularlesion on the nose
Rhinophyma Azithromycin, topicalmetronidazole
CLL, leukemiacutis
11/F/70 1 y Erythematous plaques on the noseand cheeks
Granulomatous rosacea,sarcoidosis
Topical metronidazole PCMZL
12/F/49 6 mo Erythematous infiltrated plaque on theleft ala nasi
Granulomatous rosacea Topical metronidazole PCFCL
Abbreviations: CLL, chronic lymphocytic leukemia; PCFCL, primary cutaneous follicular center cell lymphoma; PCMZL, primary cutaneous marginal zonelymphoma.
Figure 1. Erythematous (granulomatous rosacea-like) papules on the rightcheek in a patient with primary cutaneous follicular center B-cell lymphoma(patient 1).
Figure 2. Rhinophymalike lesion in a patient with primary cutaneousmarginal zone lymphoma (patient 11).
ARCH DERMATOL/ VOL 148 (NO. 7), JULY 2012 WWW.ARCHDERMATOL.COM825
©2012 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 12/07/2021

and residual fragmented germinal centers, features of mar-ginal cell lymphoma (Figure 5). Two cases had diffusedermal infiltrates of mostly small regular B cells(Figure 6), consistent with skin involvement by chroniclymphocytic leukemia (CLL). Furthermore, in patient 4,results of an IgH rearrangement study showed an iden-tical clone in the blood and skin (Figure 6), establishingthe diagnosis of leukemia cutis. Demodex folliculorum wasnot present in any of the biopsy specimens.
Based on a full workup including clinicopathologic cor-relation and analysis of B-cell clonality, the diagnosis re-tained was primary cutaneous follicular center B-cell lym-phoma in 4 of 12 cases (33%), primary cutaneous marginalzone lymphoma in 6 (50%), and skin involvement of CLLin 2 (17%) (Table 2). All the patients had an indolentcourse as expected for their disease. Initial therapy, whichincluded radiotherapy and/or excisions for 8 patients withprimary cutaneous B-cell lymphoma (PCBCL), led to com-plete remission. However, in patients 3 and 8, new le-sions developed at sites not previously treated. Intral-esional or potent topical corticosteroids applied to these
Figure 3. Papular/granulomatous rosacea-like lesions on the background ofpreexisting erythematotelangiectatic rosacea. Small erythematous papulesthat were determined to be primary cutaneous marginal zone lymphomawere found on erythema and telangiectasia (patient 3). This patient hadpapules on both cheeks and also on the submental areas.
Table 2. Histological, Immunophenotypical, and Molecular Characteristics of Cases of B-Cell Neoplasms Mimicking Rosaceaand Rhinophyma
PatientNo.
Histological Features
ImmunophenotypeIgH Gene
RearrangementFinal
DiagnosisArchitecture Cells
1 Superficial and deep nodular Small and large (centrocytes,centroblasts)
Positive for CD20 and CD10 in germinal center–likestructures; negative for bcl-2
ND PCFCL
2 Superficial and deep, nodularand diffuse
Small and large, regular andirregular
Positive for CD20, bcl-6, and CD10 in follicularcenter cells; CD23 in nonfollicular center cells; andCD3 small cells between aggregates
Monoclonal PCFCL
3 Superficial and deep, nodularand diffuse, follicularcolonization, prominentmarginal zone
Small irregular and monocytoidin marginal areas andbetween germinal centers
Positive for CD20 and bcl-2 in T cells and marginalareas, bcl-6 and CD10 in germinal centers, andCD3 in small cells
Monoclonal PCMZL
4 Diffuse infiltrate involving thewhole dermis, with areas ofproliferation centers
Small regular and slightlyirregular, prolymphocytesand paraimmunoblasts inproliferation centers
Positive for CD20 and CD23; negative for CD5 Same clone inthe skin andperipheralblood
Cutaneouslocalizationof B-CLL
5 Superficial and deep nodular,small remnants of germinalcenters
Irregular small lymphocytes,also at the periphery of thenodules, few plasma cells
Positive for CD20 and bcl-2 in the small irregularlymphocytes, bcl-6 in remnants of germinalcenters, and CD3 in T cells at the periphery of thenodules; some plasma cells, lambda predominates
Monoclonal PCMZL
6 Superficial and deep nodularaggregates, few smallgerminal centers
Small irregular, somemonocytoid
Positive for CD20(��) and CD3(�) at theperiphery, bcl-2 in small B and T cells, and CD10in germinal centers
Monoclonal PCMZL
7 Superficial and deep nodular,residual germinal centers
Small irregular cells, plasmacells
Positive for CD20 and bcl-2 in most of the cells,bcl-6 and CD10 in residual germinal centers, andCD3 in small T cells
Polyclonal PCMZL
8 Superficial and deep nodularaggregates, focallyfragmented germinal centers
Small and large, regular andirregular
Positive for CD20, CD45RA, bcl-6, and CD10 infollicle center cells; bcl-2 in some of the B cellsand in T cells; and CD3
Monoclonal PCFCL
9 Diffuse infiltrate involving thewhole dermis
Small irregular lymphocytes,plasmacytoid and plasmacells
Positive for CD20 (approximately 50%) and bcl-2 inB and T cells; negative for bcl-6; many plasmacells, lambda predominates
Polyclonal PCMZL
10 Diffuse infiltrate involving thedeep dermis andsubcutaneous tissue
Small and medium lymphoidcells, reactive T lymphocytes,few histiocytes
Positive for CD5, CD20, and bcl-2; negative for bcl-6;clonal expression of � light chain
Monoclonal Cutaneouslocalizationof B-CLL
11 Nodular infiltrate involving thewhole dermis with a grenzzone toward the epidermis
Small lymphocytes, reactiveT cells, some histiocytes
Negative for CD10; positive for CD20 and bcl-2; afew bcl-6–positive follicle center cells; no lightchain restrictions
Monoclonal PCMZL
12 Nodular infiltrate involving thewhole dermis with a grenzzone toward the epidermis,focally germinal centers
Small and medium lymphoidcells, reactive T cells, fewhistiocytes and plasmocytes
Positive for CD20 and bcl-6; negative for CD10;no light chain restriction
Polyclonal PCFCL
Abbreviations: B-CLL, B-cell chronic lymphocytic leukemia; ND, testing not performed; PCFCL, primary cutaneous follicular center cell lymphoma; PCMZL, primarycutaneous marginal zone lymphoma.
ARCH DERMATOL/ VOL 148 (NO. 7), JULY 2012 WWW.ARCHDERMATOL.COM826
©2012 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 12/07/2021

small lesions led to complete remission. The cutaneouslesions of CLL resolved completely after a course of pred-nisone and chlorambucil therapy in patient 4 and ritux-imab and radiotherapy in patient 10. Two patients hadonly received the diagnosis at the time of this report, andfollow-up was not available.
COMMENT
B-cell lymphoproliferative diseases clinically mimickingrosacea are extremely rare and have been previously
reported in only 7 cases detailed in Table 3. The find-ings of the present case series of 12 patients with B-celllymphoproliferative diseases simulating granulomatousrosacea, rhinophyma, or both are comparable to thosereports. Likewise, most of our patients were women.However, our patients were somewhat younger thanthose described in the previous reports (mean age, 57vs 76 years), making the initial diagnosis of rosaceamore plausible. Clinically, all our patients presentedwith phymatous lesions (mostly rhinophyma), granulo-matous rosacea-like lesions, or both. In contrast, allpreviously described patients who had PCBCL had phy-matous lesions.3-7 Three patients described herein and 1described previously6 had preexisting rosacea present-ing as facial flushing, erythema, and telangiectasia.Therefore, the development of papules or rhinophymain these patients was considered part of the preexistingrosacea. Two patients described in the literature alsohad pustules,2,8 and both of them had CLL. In one ofthose patients, earlier biopsy findings showed polymor-phonuclear leukocytes, which probably representedpreexisting rosacea.2 In the other patient, histologicalfeatures of the pustules were not described. Thus, pus-tules might have formed secondary to occlusion of thefolliculosebaceous unit by the leukemic infiltrate.8 Incontrast, none of the patients described herein had apustular eruption.
This unique clinical presentation of B-cell neoplasminvolving the skin and simulating rosacea led to a diag-nosis delay that ranged from months to years. Half thepatients in the present series (6 of 12) and most of thepatients described in the literature (6 of 7)2-7 had beeninitially treated with topical or systemic antibiotics forat least a few months without any benefit before abiopsy specimen was obtained. Thus, rosacea and rhi-nophyma should be added to the list of the unusualmanifestations of B-cell neoplasms simulating otherskin diseases (Table 4). The clinical differential diag-nosis of these lesions does not include only rosacea. Forthe papular/granulomatous rosacea-like lesions, the dif-ferential diagnosis would include mostly adnexaltumors, such as basal cell carcinoma, trichoepithelioma,or sebaceous hyperplasia, and cutaneous sarcoidosis.For the phymatous lesions, granulomatous diseases (in-fectious or noninfectious) and T-cell lymphoma shouldbe considered.
Fifteen of the 19 total patients (10 in the present se-ries and 5 in previously reported cases) had PCBCL,with the marginal zone lymphoma being the most com-mon (10 of 19 patients, including 1 with immunocy-toma, currently considered a type of marginal zonelymphoma) followed by follicular center cell lymphoma(5 of 19 patients). In 4 patients, the skin infiltrative le-sions represented leukemia cutis of CLL. In general, pri-mary cutaneous marginal zone lymphoma is uncom-monly located on the face.1 One may therefore speculatethat chronic antigenic stimulation caused by a residentorganism such as D folliculorum leads to the developmentof the lymphoma similar to the relation between Helico-bacter pylori and gastric lymphoma.19 Although we didnot observe Demodex organisms in any of the biopsy speci-mens, such a mechanism is plausible because it would
A
B
C
Figure 4. Histological features of primary cutaneous follicular center B-celllymphoma (patient 8). A, Superficial and deep nodular aggregates showirregular lymphoid germinal center–like areas (hematoxylin-eosin, originalmagnification �20). B and C, The areas are composed of small and large Blymphocytes (hematoxylin-eosin [B] and CD20 [C], original magnification�400).
ARCH DERMATOL/ VOL 148 (NO. 7), JULY 2012 WWW.ARCHDERMATOL.COM827
©2012 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 12/07/2021
account for the lymphoma development and the clinicalpresentation.20 Alternatively, similar to descriptions ofleukemic infiltrates of CLL localized to the sites of her-pes zoster,14,15 the lymphomatous/leukemic infiltrateslocalized to the face may represent the isomorphicphenomenon on the sites of a preexisting rosacea/rhinophyma.
In all 19 reported cases, the diagnosis was based onhistological and immunophenotypical characteristics,supported in most of the cases by genotypic findings.Demonstration of a monotypic plasma cell populationor IgH gene rearrangement is crucial for the diagnosisof primary cutaneous marginal zone lymphoma in thissetting because some cases of rosacea may show denselymphohistoplasmacytic infiltrate.21 It is also essentialto show the identical clone of B cells in the skin infil-trate and in the blood in cases of CLL, especially ifthe findings for CD5 are negative (as in patient 4)or when a concomitant B-cell lymphoma has to beexcluded.
The PCBCLs were treated with excision or radio-therapy, as indicated for low-grade PCBCL.22 In con-trast, skin infiltrates of CLL in which most of the cellsare small are related to a favorable prognosis and do notrequire specific therapy.23 However, in cases in which theypose an aesthetic problem, such as those described in thepresent series, radiotherapy and even systemic therapymay be indicated. For small papules and nodules that con-tinue to appear, topical corticosteroids may be the treat-ment of choice for early lesions. This modality may bemore practical and accepted from the cosmetic point ofview, probably without affecting the course of the dis-ease. Nevertheless, further studies are needed to vali-date this approach, particularly in cases of follicular cen-ter B-cell lymphoma.
In summary, cutaneous involvement by B-cell neo-plasms may mimic rosacea or rhinophyma. This un-usual clinical presentation is more common in womenand appears in the setting of preexisting rosacea or as anew eruption. A B-cell proliferative disorder presenting
A B
C D
Figure 5. Histological features of primary cutaneous marginal zone lymphoma (patient 3). A, Superficial and deep nodular aggregates are seen(hematoxylin-eosin, original magnification �20). B and C, The aggregates show distended marginal zones of monocytoid B cells (hematoxylin-eosin [B] and CD20[C], original magnification �200). C, The residual germinal center reveals positive staining for CD20 and negative staining for bcl-2. D, The marginal B cells arepositive for bcl-2 (original magnification �200).
ARCH DERMATOL/ VOL 148 (NO. 7), JULY 2012 WWW.ARCHDERMATOL.COM828
©2012 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 12/07/2021

Table 3. Reports of B-Cell Neoplasms Mimicking Rosacea or Rhinophyma: Review of the Literature
Patient No./Sex/Age, y Clinical Presentation/Initial Diagnosis Early Therapy Final Diagnosis Source
1/F/69 Erythematous papules and pustules on the cheeks,forehead, and chin/rosacea
Tetracycline hydrochloride CLL Thomson and Cochran,2
19782/F/50 Multiple erythematous infiltrated nodules and plaques
over face and ears/granulomatous rosaceaTopical metronidazole,
minocyclinehydrochloride
PCMZL(immunocytoma)
Colvin et al,3 2003
3/F/86 Indurated, well-demarcated, erythematous toviolaceous nodule extending from the midnasalbridge to the nasal tip/rhinophyma
Topical metronidazole PCFCL Seward et al,4 2004
4/F/83 Erythema and swelling of the nose/rhinophyma (alsonodule on pinna of the ear and nail fold swelling)
Minocycline PCMZL Stanway et al,5 2004
5/F/78 Nontender erythematous nodules and plaques at tip ofnose/rhinophyma
Erythromycin, acyclovirsodium
PCMZL Ogden and Coulson,6
20086/F/80 Slightly infiltrated painless erythematous plaque
localized on tip of nose/rhinophymaMinocycline PCMZL Rosmaninho et al,7
20107/F/83 Infiltrated nodules and plaques on nose, cheeks, and
periorbitally; papules and pustules; sebaceoushyperplasia; and telangiectasia/rosacea andrhinophyma
None CLL Bennett et al,8 2010
Abbreviations: CLL, chronic lymphocytic leukemia; PCFCL, primary cutaneous follicular center cell lymphoma; PCMZL, primary cutaneous marginal zonelymphoma.
A B
C D
Figure 6. Leukemia cutis of chronic lymphocytic leukemia mimicking phymatous rosacea (patient 4). A, Erythematous plaques and nodules on the nose, cheeks,and chin. B, Diffuse lymphocytic infiltrate involving the dermis (hematoxylin-eosin, original magnification �40). C, The infiltrate is composed of small roundlymphocytes and larger cells (prolymphocytes and paraimmunoblasts) (hematoxylin-eosin, original magnification �400). D, Results of the IgH study showidentical clones (dark filled peaks marked by arrows at 125 kilobase) in the skin biopsy specimen (top) and in the peripheral blood (bottom). The y-axes showpeak intensity, measured in arbitrary units; the x-axes show DNA fragment size, measured in kilobases.
ARCH DERMATOL/ VOL 148 (NO. 7), JULY 2012 WWW.ARCHDERMATOL.COM829
©2012 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 12/07/2021

in the skin should be added to the long list of diseasesaffecting the face manifested by rhinophyma or papulo-nodular rosacea-like eruptions.
Accepted for Publication: December 29, 2012.Published Online: April 16, 2012. doi:10.1001/archdermatol.2011.3575Author Affiliations: Departments of Dermatology (Dr Bar-zilai) and Pathology (Drs Barzilai and Tabibian-Keissar)and Hematology Institute (Dr Amarilgio), Sheba Medi-cal Center, Tel-Hashomer, Israel; Departments of Der-matology (Drs Feuerman, David, and Hodak) and Pa-thology (Drs Feinmesser and Halpern), Beilinson Hospital,Rabin Medical Center, Petach-Tikva, Israel; Sackler Fac-ulty of Medicine, Tel-Aviv University, Tel-Aviv, Israel(Drs Barzilai, Feuerman, David, Feinmesser, Halpern, andHodak); Department of Pathology, Kaplan Medical Cen-ter, Rehovot, Israel (Drs Barzilai and Feldberg); and De-partment of Biomedical Sciences and Human Oncology,Dermatologic Clinic (Dr Quaglino) and Laboratory of Cu-taneous Pathology (Dr Tomasini), University of Turin,Turin, Italy.
Correspondence: Aviv Barzilai, MD, MSc, Departmentof Dermatology, Sheba Medical Center, 52621 Tel-Hashomer, Israel ([email protected]).Author Contributions: Drs Barzilai, Feuerman, Qua-glino, and Hodak had full access to all the data in thestudy and take responsibility for the integrity of thedata and the accuracy of the data analysis. Study conceptand design: Barzilai, Feuerman, and Hodak. Acquisitionof data: Barzilai, Feuerman, Quaglino, and Hodak.Analysis and interpretation of data: Barzilai, Feuerman,Quaglino, David, Feinmesser, Halpern, Feldberg, To-masini, Tabibian-Keissar, Amarilgio, and Hodak. Draft-ing of the manuscript: Barzilai. Critical revision of themanuscript for important intellectual content: Barzilai,Feuerman, Quaglino, David, and Hodak. Administrative,technical, and material support: Feinmesser, Tabibian-Keissar, and Amarilgio. Study supervision: Barzilai andHodak.Financial Disclosure: None reported.
REFERENCES
1. Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneouslymphomas. Blood. 2005;105(10):3768-3785.
2. Thomson J, Cochran RE. Chronic lymphatic leukemia presenting as atypical ro-sacea with follicular mucinosis. J Cutan Pathol. 1978;5(2):81-87.
3. Colvin JH, Lamerson CL, Cualing H, Mutasim DF. Cutaneous lymphoplasmacy-toid lymphoma (immunocytoma) with Waldenstrom’s macroglobulinemia mim-icking rosacea. J Am Acad Dermatol. 2003;49(6):1159-1162.
4. Seward JL, Malone JC, Callen JP. Rhinophymalike swelling in an 86-year-old wom-an: primary cutaneous B-cell lymphoma of the nose. Arch Dermatol. 2004;140(6):751-756.
5. Stanway A, Rademaker M, Kennedy I, Newman P. Cutaneous B-cell lymphomaof nails, pinna and nose treated with chlorambucil. Australas J Dermatol. 2004;45(2):110-113.
6. Ogden S, Coulson IH. B-cell lymphoma mimicking rhinophyma. Clin Exp Dermatol.2008;33(2):213-214.
7. Rosmaninho A, Alves R, Lima M, Lobo I, Amorim I, Selores M. Red nose: pri-mary cutaneous marginal zone B-cell lymphoma. Leuk Res. 2010;34(5):682-684.
8. Bennett M, Higgins E, Curran S, Marren P. Leukaemia cutis mimicking florid rhi-nophymatous rosacea [abstract 13]. Br J Dermatol. 2010;163:443. doi:10.1111/j.1365-2133.2010.09921.x.
9. Hodak E, Feuerman H, Barzilai A, David M, Cerroni L, Feinmesser M. Anetoder-mic primary cutaneous B-cell lymphoma: a unique clinicopathological presen-tation of lymphoma possibly associated with antiphospholipid antibodies. ArchDermatol. 2010;146(2):175-182.
10. Dasgupta S, Mitra D, Bhattacharya A, Sur PK. B cell lymphoma with unusual clini-cal cutaneous presentation. J Cancer Res Ther. 2006;2(4):203-205.
11. Paulli M, Arcaini L, Lucioni M, et al. Subcutaneous “lipoma-like” B-cell lym-phoma associated with HCV infection: a new presentation of primary extra-nodal marginal zone B-cell lymphoma of MALT. Ann Oncol. 2010;21(6):1189-1195.
12. Garbea A, Dippel E, Hildenbrand R, Bleyl U, Schadendorf D, Goerdt S. Cutane-ous large B-cell lymphoma of the leg masquerading as a chronic venous ulcer.Br J Dermatol. 2002;146(1):144-147.
13. Roglin J, Boer A. Skin manifestations of intravascular lymphoma mimic inflam-matory diseases of the skin. Br J Dermatol. 2007;157(1):16-25.
14. Wakelin SH, Young E, Kelly S, Turner M. Transient leukaemia cutis in chroniclymphocytic leukaemia. Clin Exp Dermatol. 1997;22(1):37-40.
15. Claeys A, Pouaha J, Christian B, Froment N, Truchetet F. Zosteriform cutaneouslocalizations of B-cell chronic lymphocytic leukaemia. Eur J Dermatol. 2008;18(1):101-102.
16. Freiman A, Muhn CY, Trudel M, Billick RC. Leukemia cutis presenting with fin-gertip hypertrophy. J Cutan Med Surg. 2003;7(1):57-60.
17. Chui CT, Hoppe RT, Kohler S, Kim YH. Epidermotropic cutaneous B-cell lym-phoma mimicking mycosis fungoides. J Am Acad Dermatol. 1999;41(2, pt 1):271-274.
18. Chiang S, DiCaudo DJ, Valdez R, Swanson DL. Cutaneous B-cell lymphoma with
Table 4. Unusual Clinical Manifestations of CutaneousB-Cell Neoplasms
B-Cell Neoplasm Clinical Appearance Selected Source
CLL Papules in adermatomaldistribution (afterherpes zoster)
Wakelin et al,14
1997Claeys et al,15
2008CLL Fingertip
hypertrophyFreiman et al,16
2003MZL/FCC/CLL Rosacea/rhinophyma Present series
Thomson andCochran,2
1978Colvin et al,3
2003Seward et al,4
2004Stanway et al,5
2004Ogden and
Coulson,6
2008Rosmaninho et
al,7 2010Bennett et al,8
2010FCC/MZL Anetoderma Hodak et al,9
2010MZL Lipoma
(subcutaneous)Paulli et al,11
2010Large B-cell lymphoma Cutaneous horns Dasgupta et al,10
2006Large B-cell lymphoma,
leg typeChronic venous
ulcerGarbea et al,12
2002Intravascular
lymphomaLivedo reticularis
and livedovasculitis
Roglin andBoer,13 2007
Secondary involvementof the skin by MZL
Mycosis fungoides Chui et al,17 1999Chiang et al,18
2010
Abbreviations: CLL, chronic lymphocytic leukemia; FCC, follicular center cell;MZL, marginal zone lymphoma.
ARCH DERMATOL/ VOL 148 (NO. 7), JULY 2012 WWW.ARCHDERMATOL.COM830
©2012 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 12/07/2021

histologic features of mycosis fungoides. J Am Acad Dermatol. 2010;62(2):320-323.
19. Sagaert X, Van Cutsem E, De Hertogh G, Geboes K, Tousseyn T. Gastric MALTlymphoma: a model of chronic inflammation-induced tumor development. NatRev Gastroenterol Hepatol. 2010;7(6):336-346.
20. Yamasaki K, Gallo RL. The molecular pathology of rosacea. J Dermatol Sci. 2009;55(2):77-81.
21. Aroni K, Tsagroni E, Lazaris AC, Patsouris E, Agapitos E. Rosacea: a clinico-pathological approach. Dermatology. 2004;209(3):177-182.
22. Senff NJ, Noordijk EM, Kim YH, et al; European Organization for Research andTreatment of Cancer; International Society for Cutaneous Lymphoma.European Organization for Research and Treatment of Cancer and Interna-tional Society for Cutaneous Lymphoma consensus recommendations forthe management of cutaneous B-cell lymphomas. Blood. 2008;112(5):1600-1609.
23. Kaddu S, Smolle J, Cerroni L, Kerl H. Prognostic evaluation of specific cutane-ous infiltrates in B-chronic lymphocytic leukemia. J Cutan Pathol. 1996;23(6):487-494.
Notable Notes
Morbus Europaeus: Europeans Naming Syphilis for Their Enemies
The Spanish physician Rodrigo Ruiz Diaz de Isla attributed theentryofsyphilisinEuropetoChristopherColumbus,whobroughtit fromtheNewWorld(1493).1AfterKingCharlesVIIIconqueredthe Neapolitan kingdom, the French called syphilis maladie deNaples or mal napolitain. Interestingly, Italians Luca Ghini andNicola Massa used the name morbus neapolitanus in the titles oftheir 2 works, respectively.2 After the battle of Fornovo, with avictory by the Italian League over the French army commandedbyCharlesVIII, syphiliswascalledmale italianoormorbo italico.3
Syphilisbecamethesymbolof shamethatwasusedbypeopleto cast aspersion on their enemies. It was named morbo lusitanobytheCastiliansandmalcastiglianobytheLusitans, showingtheancient acrimony between them. Castilians also called syphilismal di Galizia, referring to both Catholic kings Isabella of Cas-tile and Ferdinand of Aragon. Turks used the name mal dei cris-tiani,underscoringthenever-endinghostilitybetweenTurksandChristians.Intheearly16thcentury,theDutchandFlemishcalledsyphilis morbo spagnolo, in commemoration of the Spanish in-vasion. Russians used the synonyms mal dei Polacchi and malpolacco as they expanded into Poland, but the Polish, who didnot insult the Russians, used the synonym mal dei Tedeschi.4
Morbus europaeus was justified because syphilis spreadthrough all of Europe and beyond. Pietro Rostino used theterm male indiano, referring to the New World; Antonio Sca-naroli more precisely used mal d’America; and Francois XavierSwediaur used mal de la baia di St Paul.5 Syphilis was namedmalattia del Portogallo in India because of the undesirable pres-ence of the Portuguese Vasco de Gama in 1498 and Pedro Al-varez in 1500 and their men. Firanga was the name used inCalcutta, in remembrance of the Carlovingian empire. TheJapanese called syphilis mal portoghese as an affront to the Por-tuguese and ulcera della Cina or veleno di susino to offend theChinese. Finally, the Chinese named syphilis ulcera di susinoor eruzione di Canton, after the first Chinese city where syphi-lis spread.6 Chinese poets compared syphilis to the buddingof a flower without fear of winter, meaning that the appear-ance of syphilis is both abrupt and startling.
Antonio Tagarelli, MDGiuseppe Tagarelli, PhDPaolo Lagonia, PhDAnna Piro, MD
Author Affiliations: National Research Council of Italy, Institute of Neurological Sciences, Mangone, Cosenza, Italy.Contact Dr A. Tagarelli at the National Research Council of Italy, Institute of Neurological Sciences, Contrade Burga, Man-gone, Cosenza 87050, Italy ([email protected]).
1. Diaz de Isla R, ed. Tractado llamado fructo de todos los santos contra el mal serpentine venido de la isla Espanola hecho y ordenado en el grande y famosohospital de todos los santos. Seville, Spain: A Burgos; 1539.
2. Astruc J, ed. De morbis venereis libri sex. In quibus disseritur tum de origine, propagatione & contagione horumce affectuum in genere: tùm de singulorumnaturà, aetiologia & therapeia, cum brevi analisi & epicrisi operum plerorumque quae de eodem argomento scripta sunt. Paris, France: G Cavelier; 1736.
3. Rondelet G, ed. Methodus curandorum omnium morbum corpis humani. De morbo gallico. Paris, France: C Maceo; 1754.4. Pernotti di Cigliano P, ed. Storia generale e ragionata dell’origine, dell’essenza e specifica dell’infezione venerea. Turin, Italy: Stampa Reale; 1788.5. Swediaur F, ed. Traite complet sur les symptomes, les effets, la nature et le traitment des maladies syphilitiques. Paris, France: Cellot; 1817.6. Wang N, ed. Dermatologia in medicina tradizionale cinese. Milan, Italy: Ambrosiana; 1997.
ARCH DERMATOL/ VOL 148 (NO. 7), JULY 2012 WWW.ARCHDERMATOL.COM831
©2012 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 12/07/2021


















