Granulomatous Meningoencephalomyelitis inDogs · form,representingthefocalformofGME.3,4,11,17 Focal...
13
a Dr. Adamo is now affiliated with Bay Area Veterinary Specialists, San Leandro, California. ranulomatous meningoencephalomye- litis (GME) is a nonsuppurative inflam- matory disease of the canine central nervous system (CNS). 1–7 Its cause is unknown. This devastating disease was first called reticulo- sis by Koestner and Zeman in 1962. 8 The term GME was proposed by Braund and colleagues in 1978. 9 GME has a worldwide distribution and accounts for 5% to 25% of all CNS disor- ders in dogs. 3,10 PATHOLOGY GME is thought to account for most lesions previously described as reticulosis. 5,11,12 The term reticulosis refers to an abnormal increase in cells derived from, or related to, monocyte macrophages (i.e., histiocytes). 3 Because GME lesions contain histiocytes, GME may, by definition, represent a form of reticulosis. 3 In 1972, reticulosis was divided into three categories: inflammatory (granulomatous) reticulosis, neoplastic reticulo- sis, and microgliomatosis. 13 More recently, 9 the inflammatory form has been referred to as GME, 2,4–6,9,10,14,15 and neoplastic reticulosis has been reclassified as lymphoma or malignant histiocytosis. 11 At necropsy, gross lesions of GME are evi- dent if the angiocentric inflammatory reaction is sufficient to produce changes of the normal brain symmetry (i.e., falx deviation or compres- sion of surrounding structures). 5 Lesions are seen as areas of swelling and yellow to gray dis- coloration and are predominantly found in white matter; however, gray matter and lep- tomeninges also may be affected. 4,5 Meninges may appear thickened and cloudy. In some cases, optic nerves are grossly enlarged. 2 COMPENDIUM 678 November 2007 Granulomatous Meningoencephalomyelitis in Dogs P. Filippo Adamo, DVM, DECVN a William M. Adams, DVM, DACVR (Radiology, Radiation Oncology) Howard Steinberg, VMD, PhD, DACVP University of Wisconsin ABSTRACT: Granulomatous meningoencephalomyelitis (GME) is a nonsuppurative inflammatory disease of unknown origin that affects the central nervous system of dogs. GME is characterized histologically by large perivascular cuffs of mononuclear cells in the parenchyma and meninges of the brain and spinal cord. If left untreated, it is usually fatal. Immunosuppressive doses of glucocorticosteroids have been the mainstay of treatment for GME; however, new and more effective therapies have recently been proposed.This article reviews the pathology, origin, clinical signs, therapeutic response, and outcome of GME in dogs. • Take CE tests • See full-text articles CompendiumVet.com Article # 2 CE G
Transcript of Granulomatous Meningoencephalomyelitis inDogs · form,representingthefocalformofGME.3,4,11,17 Focal...

aDr. Adamo is now affiliated withBay Area Veterinary Specialists,San Leandro, California.
ranulomatous meningoencephalomye-litis (GME) is a nonsuppurative inflam-matory disease of the canine central
nervous system (CNS).1–7 Its cause is unknown.This devastating disease was first called reticulo-sis by Koestner and Zeman in 1962.8 The termGME was proposed by Braund and colleaguesin 1978.9 GME has a worldwide distributionand accounts for 5% to 25% of all CNS disor-ders in dogs.3,10
PATHOLOGYGME is thought to account for most lesionspreviously described as reticulosis.5,11,12 The
term reticulosis refers to anabnormal increase in cellsderived from, or related to,monocyte macrophages (i.e.,
histiocytes).3 Because GME lesions containhistiocytes, GME may, by definition, representa form of reticulosis.3 In 1972, reticulosis wasdivided into three categories: inflammatory(granulomatous) reticulosis, neoplastic reticulo-sis, and microgliomatosis.13 More recently,9 theinflammatory form has been referred to asGME,2,4–6,9,10,14,15 and neoplastic reticulosis hasbeen reclassified as lymphoma or malignanthistiocytosis.11At necropsy, gross lesions of GME are evi-dent if the angiocentric inflammatory reactionis sufficient to produce changes of the normalbrain symmetry (i.e., falx deviation or compres-sion of surrounding structures).5 Lesions areseen as areas of swelling and yellow to gray dis-coloration and are predominantly found inwhite matter; however, gray matter and lep-tomeninges also may be affected.4,5 Meningesmay appear thickened and cloudy. In somecases, optic nerves are grossly enlarged.2
COMPENDIUM 678 November 2007
GranulomatousMeningoencephalomyelitisin DogsP. Filippo Adamo, DVM,DECVNaWilliam M.Adams, DVM,DACVR (Radiology, Radiation Oncology)Howard Steinberg, VMD, PhD,DACVPUniversity of Wisconsin
ABSTRACT: Granulomatous meningoencephalomyelitis (GME) is a nonsuppurative inflammatory
disease of unknown origin that affects the central nervous system of dogs. GME is characterized
histologically by large perivascular cuffs of mononuclear cells in the parenchyma and meninges
of the brain and spinal cord. If left untreated, it is usually fatal. Immunosuppressive doses of
glucocorticosteroids have been the mainstay of treatment for GME; however, new and more
effective therapies have recently been proposed.This article reviews the pathology, origin, clinical
signs, therapeutic response, and outcome of GME in dogs.
•Take CE tests• See full-text articles
CompendiumVet.com
Article #2CE
G

November 2007 COMPENDIUM
Granulomatous Meningoencephalomyelitis in Dogs 679CE
Microscopically, lesions of GME are characterized byperivascular cuffs of lymphocytes, varying numbers ofmacrophages, and plasma cells in the parenchyma andmeninges of the brain and spinal cord3,4,9,11,12,14,16 (Figure 1).Sometimes the cells are arranged in a whorled patternaround the central vessels, a feature that is emphasized byreticulin stain17 (Figure 1). In some areas, the perivascularcells are predominantly lymphocytes; in other regions,macrophages predominate.14 Lymphocytes are predomi-nantly CD3 antigen positive, and nearly all lymphocytesand macrophages express major histocompatibility com-plex class II antigen.15 Macrophages may differentiate intoepithelioid cells, which often form a discrete nest withinthe cuff.5 Infiltration of all these cells into the CNSparenchyma is typically minimal; however, as the perivas-cular population around several vessels expands and coa-lesces, the intervening parenchyma is progressivelycompressed and obliterated. Such cases are grossly evidentat necropsy.5 The neuropil surrounding GME lesionsshows modest glial cell reaction and edema.4,5 Prolongedcases have lesion confluence, vascular proliferation, andreparative changes.2,9,14–16Based on the site and distribution of lesions, GME isclassified as one of three morphologic forms: dissemi-nated, focal, or ocular.3–5,10,12 In disseminated GME, the
white matter of the cerebrum, caudal brainstem, cerebel-lum, and cervical spinal cord is primarily affected; how-ever, vascular lesions may also be found in gray matter,leptomeninges, and choroid plexus.4,5 If multipleperivascular cuffs coalesce, a solitary granuloma mayform, representing the focal form of GME.3,4,11,17 Focallesions most commonly occur in the brainstem, espe-cially in the pontomedullary region, and in cerebralwhite matter.3,4,11,17 A focal form of GME associatedwith multifocal, smaller lesions throughout the neuraxishas been reported.18 The focal form of GME should bedifferentiated from CNS malignant histiocytosis andprimary CNS lymphosarcoma.11,19,20 The ocular form ofGME affects the retinal or postretinal portions of theoptic nerve.5 Dogs with ocular GME may subsequentlydevelop the disseminated or focal form of the disease.10
ORIGINThe cause of GME is unknown.3–6,12,21 Autoimmune,infectious, and neoplastic causes have been theorized; anautoimmune cause is considered most likely.15 Recent dataindicate that the inflammatory lesions in GME consist ofa T-cell–mediated delayed-type hypersensitivity reactionwith organ-specific autoimmune disease.15 Lesions of theoptic nerve also support this hypothesis. An antiastrocyte
Figure 1. Histopathology section of a canine brain with disseminated GME. (Courtesy of Dr. A. Armien)
Hematoxylin and eosin stain shows tightly aggregated whorls oflymphocytes, spindle-shaped phagocytes, and collagen depositionaround demonstrated (arrow ) or presumed vascular structures(asterisks).The lesions consist of single or clustered aggregates ofperivascular inflammatory cell accumulation.The presumedvessels are occluded by eosinophilic amorphous material, withscarce spindle cells (fibroblasts). Original magnification ×10.
Reticulin stain shows that the spindle cells are rich inextracellular reticular fibrin deposition. Original magnification×20.
* **

COMPENDIUM November 2007
Granulomatous Meningoencephalomyelitis in Dogs680 CE
autoantibody was recently identified in the cerebrospinalfluid (CSF) of dogs with GME or necrotizing menin-goencephalitis (NME), indicating a possible relationshipbetween these two diseases and the autoantibody.22 How-
ever, it remains unclear whether the autoantibody is thecause or the consequence of the inflammation.22Pathologic features and lesion distribution distinguishGME from idiopathic encephalitides of small-breeddogs, such as NME of young pugs and Maltese terriersand the necrotizing leukoencephalitis of Yorkshire terri-ers and Chihuahuas.12,16,23,24 NME of pugs and Malteseterriers is histopathologically characterized by inflamma-tory changes with lymphocytic, plasmacytic, and histio-cytic infiltration and extensive parenchymal necrosisrestricted to the cerebral hemispheres.24–26 Necrotizingleukoencephalitis of Yorkshire terriers has similarnecrotic lesions on histopathologic evaluation, but brain-stem lesions occur in addition to cerebral lesions.23,26,27
INCIDENCE AND PREDISPOSITIONThe disease has been described more commonly insmall-breed dogs, especially in toy breeds and terriers;
however, other breeds have been affected.14,16,21 The dis-ease frequently affects young to middle-aged dogs, witha mean age around 5 years (range: 6 months to 12years).5,21 A female predisposition has been observed,with a female:male ratio ranging from 1.8:1 to 3:1.4,15,21,28One study (21 dogs) reported a higher incidence inmales, with a male:female ratio of 1.5:1.6
CLINICAL SIGNSGME usually has an abrupt onset and an inexorablyprogressive course. If left untreated, it is usually fatal in afew days or weeks.4–6,21 Clinical signs are variable andreflect the morphologic type of GME and the site ofthe lesion in the neuraxis.
Disseminated (Multifocal) FormIn dogs with disseminated GME, several areas of theCNS are damaged and any combination of clinical signsreflecting lesions in multiple CNS areas is likely. Dogs aredetermined to have multifocal involvement if they displaysigns referable to at least two of the following structuresof the nervous system: optic nerve, forebrain, cerebellum,brainstem, spinal cord, or meninges21 (Figure 2). Occa-sionally, fever may accompany neurologic signs.14 Cervical
hyperesthesia may be associated with disseminated orfocal GME.3
Focal FormThe focal form of GME causes clinical signs sugges-tive of a single, space-occupying lesion. If the lesion isin the forebrain, the clinical signs are usually seizures,behavior and mental status change, ataxia, circling, pac-ing, head pressing, and central visual impairment withnormal pupillary reflexes.14 If the lesion involves themidbrain, mental depression and mydriasis unrespon-sive to light with normal vision are typical clinicalsigns.14 If the lesion involves the pons or medullaoblongata, clinical signs may include hemiparesis rang-ing to tetraplegia; multiple cranial nerve deficits, suchas depressed palpebral, corneal, and gag reflexes; facialand trigeminal nerve paralysis; and central vestibularsyndrome.14 If the lesion involves the cerebellum, spas-
Figure 2. Postcontrast sagittalT1-weighted MRI imageof a dog with necropsy-confirmed disseminated GME.Note the multiple irregularly shaped, contrast-enhanced foci inthe ventral brainstem (yellow arrow), caudal cerebellum (greenarrow), and C1–C2 spinal cord (white arrow).
The cause of GME is unknown. Autoimmune, infectious, and neoplastic causeshave been theorized; an autoimmune cause is considered most likely.
November 2007 COMPENDIUM
Granulomatous Meningoencephalomyelitis in Dogs 681CE
ticity, goose-stepping gait, and intention tremor arecommon clinical signs.14
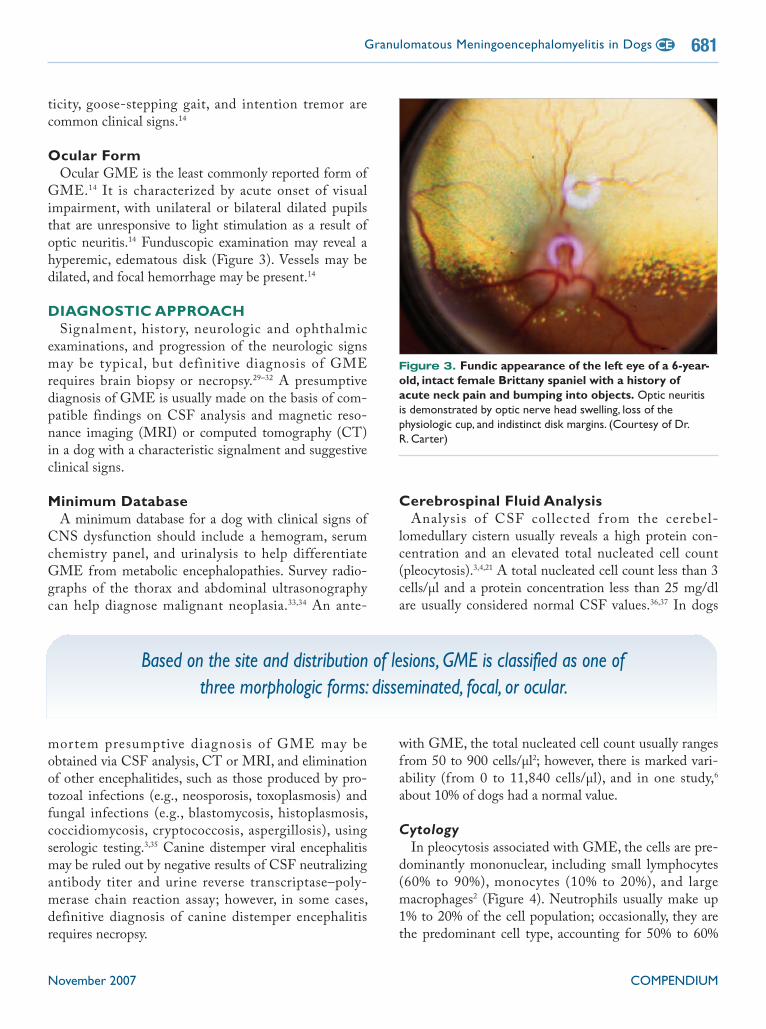
Ocular FormOcular GME is the least commonly reported form ofGME.14 It is characterized by acute onset of visualimpairment, with unilateral or bilateral dilated pupilsthat are unresponsive to light stimulation as a result ofoptic neuritis.14 Funduscopic examination may reveal ahyperemic, edematous disk (Figure 3). Vessels may bedilated, and focal hemorrhage may be present.14
DIAGNOSTIC APPROACHSignalment, history, neurologic and ophthalmicexaminations, and progression of the neurologic signsmay be typical, but definitive diagnosis of GMErequires brain biopsy or necropsy.29–32 A presumptivediagnosis of GME is usually made on the basis of com-patible findings on CSF analysis and magnetic reso-nance imaging (MRI) or computed tomography (CT)in a dog with a characteristic signalment and suggestiveclinical signs.
Minimum DatabaseA minimum database for a dog with clinical signs ofCNS dysfunction should include a hemogram, serumchemistry panel, and urinalysis to help differentiateGME from metabolic encephalopathies. Survey radio-graphs of the thorax and abdominal ultrasonographycan help diagnose malignant neoplasia.33,34 An ante-
mortem presumptive diagnosis of GME may beobtained via CSF analysis, CT or MRI, and eliminationof other encephalitides, such as those produced by pro-tozoal infections (e.g., neosporosis, toxoplasmosis) andfungal infections (e.g., blastomycosis, histoplasmosis,coccidiomycosis, cryptococcosis, aspergillosis), usingserologic testing.3,35 Canine distemper viral encephalitismay be ruled out by negative results of CSF neutralizingantibody titer and urine reverse transcriptase–poly-merase chain reaction assay; however, in some cases,definitive diagnosis of canine distemper encephalitisrequires necropsy.
Cerebrospinal Fluid AnalysisAnalysis of CSF collected f rom the cerebel-lomedullary cistern usually reveals a high protein con-centration and an elevated total nucleated cell count(pleocytosis).3,4,21 A total nucleated cell count less than 3cells/µl and a protein concentration less than 25 mg/dlare usually considered normal CSF values.36,37 In dogs
with GME, the total nucleated cell count usually rangesfrom 50 to 900 cells/µl2; however, there is marked vari-ability (from 0 to 11,840 cells/µl), and in one study,6about 10% of dogs had a normal value.
CytologyIn pleocytosis associated with GME, the cells are pre-dominantly mononuclear, including small lymphocytes(60% to 90%), monocytes (10% to 20%), and largemacrophages2 (Figure 4). Neutrophils usually make up1% to 20% of the cell population; occasionally, they arethe predominant cell type, accounting for 50% to 60%
Figure 3. Fundic appearance of the left eye of a 6-year-old, intact female Brittany spaniel with a history ofacute neck pain and bumping into objects. Optic neuritisis demonstrated by optic nerve head swelling, loss of thephysiologic cup, and indistinct disk margins. (Courtesy of Dr.R. Carter)
Based on the site and distribution of lesions, GME is classified as one ofthree morphologic forms: disseminated, focal, or ocular.

COMPENDIUM November 2007
Granulomatous Meningoencephalomyelitis in Dogs682 CE
of the cell type differential.2,21,28 Fewer lymphocytes thanmonocytes are reported in some cases.38 Mononuclearpleocytosis is more common in the disseminated formof GME, although in one report,21 17% of dogs had apredominantly neutrophilic inflammation, emphasizingthe variability in CSF findings that can be encounteredwith GME. CSF pleocytosis can develop in dogs withfocal disease if lesions are close to the ventricular systemor meninges.3,21
ProteinThe protein concentration in the CSF may increasebecause of the breakdown of the blood–brain barrier withsubsequent extravasation of serum protein and intrathecalantibody production.4,39 Protein levels are variable in dogswith GME, usually ranging from 40 to 400 mg/dl.2
ImagingMagnetic Resonance ImagingMagnetic resonance features of GME consist of sin-gle or multiple lesions that are hyperintense on T2-weighted and fluid-attenuated inversion recovery(FLAIR) images and mildly to moderately hypointenseon T1-weighted images, relative to adjacent brain tis-sue40 (Figure 5). Meningeal enhancement may also beevident.41 If affected, optic nerves and the optic chiasmmay be more identifiable than usual (Figure 6).
Computed TomographyAlthough not as sensitive as MRI in imaging brainand meningeal lesions, CT can provide evidence ofGME. Both focal and disseminated forms of GMEshow contrast enhancement, and the mass effect may beindirectly observed by displacement of surroundingbrain tissue.42–45 Meningeal and optic nerve contrastenhancement may also be seen on high-quality images.GME lesions in the forebrain may show contrastenhancement42,43 (Figure 7), but brainstem lesions aremore difficult to see due to beam-hardening artifactsfrom the petrous temporal bones.34,46
Brain BiopsyAlthough infrequently performed, brain biopsy can bea very useful diagnostic test in an animal with GME.21
Figure 4. Cytocentrifugation preparation of CSF.Thereis a predominance of small lymphocytes (black arrows), withsmaller proportions of vacuolated macrophages (red arrows) andnondegenerate neutrophils (green arrows). (Courtesy of Dr. R.Dickinson)
Figure 5. Two sets of brain MRI images, taken 49 daysapart, of a 13-year-old spayed dachshund. First study: (A)A postcontrastT1-weighted image shows an area of hypointensityin the ventral temporal lobe (between arrows); note the lack ofcontrast enhancement. (B) On a FLAIR image, there is diffusehyperintensity in the white matter of the left cerebral cortex.Thisdog was treated for presumed infarction. In the weeks followingtapering of corticosteroid therapy, clinical signs progressed. Secondstudy: (C) On a postcontrastT1-weighted image, there are nowbilateral foci of marked contrast enhancement in the cerebralcortex. (D) On a FLAIR image, multiple bilateral hyperintense fociare seen in the cerebral cortex.These findings are consistent withprogressive GME, distemper, or fungal granulomas. GME wasconfirmed by CT-guided needle biopsy (Figure 8) and 17 monthslater at necropsy. (The dog was treated with a combination ofcorticosteroids and cyclosporine.)
A B
C D

November 2007 COMPENDIUM
Granulomatous Meningoencephalomyelitis in Dogs 683CE
Brain biopsy can be performed via stereotactic CT-guided technique (Figure 8) or by open surgical resec-tion.29–32
TREATMENT PROTOCOLS ANDPROGNOSISVarious treatment protocols have been suggested forGME, including glucocorticosteroids, radiation therapy,cytosine arabinoside, procarbazine, leflunomide, andcyclosporine. Common adverse effects, median survivaltime, and approximate cost of therapy are summarizedin Table 1.
GlucocorticosteroidsAdministration of immunosuppressive doses of glu-cocorticosteroids, particularly prednisone (2 mg/kg/dayPO) tapered with response over the following monthsto achieve the lowest dose possible to control signs,47 isthe traditional primary treatment. Response is variable;clinical signs often recur quickly with tapering doses;and the prognosis for permanent recovery is poor,causing overall results to be unsatisfactory.9,21,48 Long-term, high-dose corticosteroid treatments predisposepatients to gastrointestinal ulceration, pancreatitis, andiatrogenic hyperadrenocorticism.9,21,48 A median sur-
vival time for 15 dogs with focal clinical signs treatedwith corticosteroids alone was 41 days in one report(range: 3 to >1,215 days).21 In this report, a differencein survival was noticed on the basis of clinical signs:dogs with multifocal signs had a median survival timeof 8 days.
Figure 6. T1-weighted, contrast-enhanced MRI images of a 9-year-old spayed dachshund that presented with acuteblindness and absent pupillary reflexes in both eyes.
On this sagittal view, there is an ill-defined area of hyperintensity(arrow) at the rostral base of the brain, extending just cranial tothe hypophysis (asterisk), corresponding to the area of the opticchiasm.
On this axial view, the area of hyperintensity extends just caudalto the optic chiasm (asterisk) and dorsolaterally and bilaterally inthe optic tract region of the pyriform lobe. A presumptivediagnosis of ocular GME was made. Clinical signs and CSFabnormalities resolved with cyclosporine therapy.
CSF analysis showed increased protein concentration andlymphocytic pleocytosis. On this dorsal view, both optic disks areenlarged and hyperintense (arrows) and extend into the vitreous.

COMPENDIUM November 2007
Granulomatous Meningoencephalomyelitis in Dogs684 CE
RadiationTherapyRadiation has been proposed as an alternative treat-ment for focal GME on the basis of the assumptionthat the focal form may actually be primary B-cell lym-phoma of the CNS.21,49 Although this assumptionremains unproven, in one study,21 six dogs treated withradiation therapy for focal forebrain signs had signifi-cantly longer survival times (median: >404 days) than 15dogs with the focal form treated with steroids only(median: 41 days). In the same study, 12 of 21 dogs withmultifocal signs died before any therapy could be initi-ated, and eight of the remaining nine dogs had suchdebilitating neurologic signs that they were not consid-ered suitable candidates for radiotherapy.Acute radiation reactions of incidentally irradiatednormal tissue are self-limiting and generally well toler-ated. Such reactions include epilation, otitis, and (whenthe eyes are included in the treatment field) conjunctivi-tis, keratoconjunctivitis, and corneal ulcers. Acute radia-tion side effects subside within 3 to 5 weeks aftercompletion of therapy.50 An important consideration inthe use of radiation therapy is delayed adverse radiation
effects. Early delayed effects can occur from 2 weeks to3 months after treatment and may be due to transientdemyelination. Animals with early delayed effects maypresent with signs similar to those of the initial presen-tation, or they may be generally stuporous. These effectsare infrequently encountered, are usually transient, andrespond to systemic corticosteroids.50 Late delayedeffects can occur 6 months to years after treatment; themost serious is brain necrosis.50,51 The risk for latedelayed effects increases with the size of each radiationfraction and with a higher total dose.
Cytosine ArabinosideCytosine arabinoside (cytarabine) is an antineoplasticdrug with immunosuppressive effects. In conjunctionwith prednisone or as a sole agent, it has been reportedto be effective in some dogs with GME.35,52 Cytarabineacts on mitotically active cells by inserting itself intoDNA molecules, causing premature chain termination.Due to the ability of the drug to cross the blood–brainbarrier and its effect on immunosuppression, it has beentheorized that cytarabine may be useful in treating GMEin dogs.35 The drug is administered as a subcutaneousinjection of 50 mg/m2 twice a day for 2 consecutivedays.35,53 This regimen is initially repeated every 3weeks.35,53 Gloves should be worn during the administra-
Figure 7. CT image of an 8-year-old female Chihuahuathat presented with acute onset of blindness 1 monthpreviously, episodic cervical pain, and recent progressionto right-sided head tilt, pacing, and right circling. Leftfacial sensation and left limb conscious proprioception weredecreased. Neurologic signs were consistent with multifocallesions involving optic tracts and the right forebrain. On thisimage of the brain following administration of intravenouscontrast medium, there is enhancement in the right parietal lobe(arrow) and left shift of the falx cerebri with compression of theright lateral ventricle (mass effect).
Figure 8. CT-guided needle brain biopsy of the dog inFigure 5.Histopathology of the collected sample confirmed thediagnosis of GME.

November 2007 COMPENDIUM
Granulomatous Meningoencephalomyelitis in Dogs 685CE
Table 1.VariousTherapies for Granulomatous Meningoencephalomyelitis in DogsMedianSurvival Survival
Number Time Range Cost ofStudy of Dogs Therapy Side Effects (days) (days) Dose Therapya
Coates et al54 11 No treatment — 18 — — —
Coateset al54,b
20 Procarbazine ±prednisone
Myelosuppression,hemorrhagicgastroenteritis
450 NA 25–50 mg/m2/day PO
$60–$120/moc
MunanaandLuttgen21
15 Prednisone Gastrointestinalulceration, pancreatitis,iatrogenic Cushing’ssyndrome
41d 3–>1,215
0.25–2 mg/kgPO bid
$3–$7/mo
MunanaandLuttgen21
7 Radiationtherapy +prednisone
Demyelination (earlydelayed); brain necrosis(late delayed)
404d NA Total 40–49.5Gy, divided in2.4- to 4.0-Gyfractions
$4,000 for fullcycle
Zarfosset al53,e
10 Cytarabine ±prednisone
Myelosuppression 531 45–1,025
50 mg/m2bid SCfor 2 consecutivedays, repeatedinitially q3wk,then onceq2–3mo
$10 for eachdrug per cycle f+ professionalfee for the twoinjections percycle
Adamoet al63,g
10 Cyclosporine ±corticosteroids
Gingival hyperplasia,hypertrichosis,excessive shedding,vomiting, diarrhea
930d 60–>1,290
Starting dose: 6mg/kg PO bid;adjust to obtainblood troughcyclosporinelevel of 200–400ng/ml
$60/moh +serial CSF andcyclosporineblood level
Adamoet al63,g
10 Cyclosporine +ketoconazole
Gingival hyperplasia,hypertrichosis,excessive shedding,vomiting, diarrhea
930d 60–>1,290
Cyclosporine(5 mg/kg) +ketoconazole(8 mg/kg) sid
~$28/moh +serial CSF andcyclosporineblood level
NA: not available.aCost of therapy is approximated for a 13.2-lb (6-kg) dog.bIn this study, the prednisone dose was reduced or discontinued in 17 dogs.cProcarbazine is available as 10- to 80-mg capsules; the approximate price is $2 for a 10- or 20-mg capsule and $3 for a 30-mg capsule;the price increases progressively to $8 for an 80-mg capsule.The drug is also available as an aqueous solution or oil-based suspension(Diamondback Drugs, Scottsdale, AZ); the price for these formulations is the same as for the capsules.dAs calculated by Kaplan-Meier analysis.eInitially in combination with prednisone (1 mg/kg q12h); after the second round of cytosine injections, prednisone therapy is reducedand, in some cases, discontinued. In this study, 8 dogs received long-term prednisone (0–1.7 mg/kg bid) treatment, and 2 dogs receivedtertiary immunosuppressive chemotherapeutics (procarbazine and leflunomide) in addition to the prednisone–cytarabine regimen.fCytarabine is supplied as a 20 mg/ml injectable solution in 5-ml (100-mg) vials ($10/vial).gIn this study, 7 dogs were treated with cyclosporine alone or in combination with ketoconazole, and 3 dogs were treated withcyclosporine and corticosteroids. Because of the small total number of cases in the study, all data were grouped together.hCyclosporine is available in 10-, 25-, 50-, and 100-mg capsules; it may also be reformulated in capsules from oral solution (Neoral;Novartis).The approximate price is $1 for a 25-mg capsule and $6 for a 100-mg capsule. A generic formulation could cost approxi-mately one-third to one-half of the wholesale price.

COMPENDIUM November 2007
Granulomatous Meningoencephalomyelitis in Dogs686 CE
tion of this agent because it can be absorbed through theskin.35 A complete blood count (CBC) is conducted 10to 14 days after the first course of cytarabine therapy andperiodically throughout the course of treatment (usuallyonce every 2 to 3 months).35 To increase treatment effi-cacy, cytarabine is usually used initially in combinationwith prednisone (1 mg/kg bid); after the second round ofcytarabine injection, prednisone therapy is reduced.35 Themost significant side effect is myelosuppression. Otherside effects include vomiting, diarrhea, and hair loss.35 Inone study,53 the use of cytarabine was investigated in 10dogs with suspected GME. Eight dogs received long-term prednisone (0 to 1.7 mg/kg bid) treatment, andtertiary immunosuppressive chemotherapeutics (pro-carbazine and leflunomide) were added to the pred-nisone–cytarabine regimen in two dogs (Table 1).53 Inthis study, the median survival time was 531 days (range:46 to 1,025 days), and five of the 10 dogs were alive atthe time of the study’s conclusion.
ProcarbazineProcarbazine, an antineoplastic drug with multiplesites of action, has been used as an adjunct therapy toprednisone or as a single agent.35,54 It inhibits incorpora-tion of small DNA precursors as well as RNA and pro-tein synthesis. Procarbazine can also directly damageDNA through an alkylation reaction.35,55 Procarbazine islipid soluble and crosses the blood–brain barrier.35,55 Inone study,54 procarbazine and prednisone were investi-gated in 20 dogs with suspected GME, and the resultswere compared with those of an untreated control group(11 dogs) with histopathologically confirmed GME(Table 1). In this study, the prednisone dose was reducedor discontinued in 17 dogs, and the median survivaltime was 15 months.54 Procarbazine has been used orallyat a dose of 25 to 50 mg/m2/day.35,54 The main sideeffect associated with procarbazine therapy (usuallyassociated with the higher dose) is myelosuppression(30% in one study).54 The CBC should be monitored
After contrast injection.Before contrast injection.
Figure 9. Brain CT studies of the dog in Figure 7 after 7 months of cyclosporine treatment.Absence of contrastenhancement indicates resolution of the previous lesion. CSF analysis confirmed resolution of the previous abnormalities.

November 2007 COMPENDIUM
Granulomatous Meningoencephalomyelitis in Dogs 687CE
once weekly for the first month, then monthly there-after.35 Other side effects include hemorrhagic gastroen-teritis (15% in one study54), nausea, vomiting, andhepatic dysfunction.35,54
CyclosporineThe rationale for using cyclosporine in GME arosef rom recent data suggesting that GME is a T-cell–mediated, organ-specific, autoimmune disease.15Cyclosporine has profound immunosuppressive proper-
ties and suppresses T-cell–mediated immune responsesthrough inhibition of synthesis of interleukin (IL)-2and other cytokines.56,57 Cyclosporine also suppressesactivation of macrophages and monocytes and the pro-duction of other cytokines (IL-3, IL-4, IL-5, tumornecrosis factor-α, and γ interferon), thus indirectlyinhibiting antigen presentation by class I and II majorhistocompatibility complex, mononuclear cell function,mast cell and eosinophil production, and growth anddifferentiation of B cells.58 The blood–brain barrier per-meability of cyclosporine is poor; however, becauseGME is a perivascular disease and the blood–brain bar-rier is disrupted during inflammation, therapeutic
cyclosporine concentration is most likely present inaffected areas of the CNS.44 In addition, as the T-cellresponse is initiated in the peripheral lymphoid organsin autoimmune disease,59 there may not be a need forcyclosporine to cross the blood–brain barrier to suppressthe pathological immune repsonse to the CNS. In dogs,it is recommended to administer cyclosporine either 1hour before or 2 hours after feeding to guarantee consis-tent and best absorption.60 Cyclosporine is not nephro-toxic or hepatotoxic in dogs and cats unless extremely
high blood concentrations (>3,000 ng/ml) are main-tained.61,62In a retrospective study63 of 10 dogs with presumptiveGME treated with cyclosporine alone or in combinationwith corticosteroids and/or ketoconazole, cyclosporineeither alone or in combination with ketoconazole wasfound to be effective (Table 1). In this study, no significantabnormalities were detected on serial CBC and serumchemistry panel in any dog. Serial CSF analysis showed amarked improvement in inflammation in all dogs (Figure9). Side effects of cyclosporine therapy at the therapeuticdose included excessive shedding, gingival hyperplasia, andhypertrichosis (Figure 10); signs of overdose included gas-
Figure 10. Adverse effects of cyclosporine in the treatment of GME.
Hypertrichosis after 7 months of cyclosporine therapy in the dogin Figure 7.
Gingival hyperplasia after 2 years of cyclosporine therapy.
GME usually has an abrupt onset and an inexorably progressive course. If left untreated,it is usually fatal in a few days or weeks.

COMPENDIUM November 2007
Granulomatous Meningoencephalomyelitis in Dogs688 CE
trointestinal signs (e.g., vomiting, diarrhea, anorexia). Theoverall median survival time for all dogs in the study was930 days (range: 60 to >1,290 days), and five dogs werestill alive at the time of the study’s conclusion. Based onthe results of this study, we recommend cyclosporine asmonotherapy at a starting dose of 6 mg/kg PO q12h, witha blood cyclosporine trough level target of 200 to 400ng/ml. The blood cyclosporine trough level should betested after 5 to 7 days and reevaluated together with CSFafter 1 month and every 4 or 6 months thereafter, or anytime the patient neurologically deteriorates.
Cyclosporine and KetoconazoleIf cyclosporine monotherapy is cost prohibitive, coad-ministration of cyclosporine and ketoconazole has beensuggested.44 Ketoconazole has been shown to decreasethe systemic clearance of cyclosporine in dogs throughinhibition of hepatic cytochrome P450 3A microsomalenzymes.64 We found the coadministration of ketocona-zole and cyclosporine clinically effective using a startingdose of 5 mg/kg PO q24h of cyclosporine and 8 mg/kgof ketoconazole. The target trough blood cyclosporinelevel and serial monitoring are similar to the protocoldescribed for cyclosporine used as monotherapy. Thiscombined treatment has the advantage of being givenonly once daily. No significant side effects from keto-conazole were observed after 2 years in one dog and 14months in two other dogs after receiving this combinedtherapy. This combination protocol is not recommendedif liver enzyme levels are elevated or any other medicalcondition that might exacerbate liver insufficiency ispresent at the time of diagnosis or during treatment.
LeflunomideLeflunomide is an immunomodulator used in a pre-liminary clinical study in three dogs with inflammatoryor malacic brain lesions of unknown cause.65 In thisstudy, leflunomide replaced an effective treatment withimmunosuppressive doses of glucocorticosteroids, whichhad to be discontinued due to the onset of iatrogenicCushing’s syndrome. This study indicated a favorableresponse in all three dogs that survived more than 12months after starting leflunomide therapy.
SurgerySurgical removal of brain GME lesions has also beenreported.1 Surgical intervention is not a typical treatmentmodality for inflammatory or infectious brain disorders;however, it is suggested that the mass removal and the
decrease in intracranial pressure afforded by craniotomymay benefit the patient.1 Surgical removal may alsoenable histologic confirmation of GME, which then maybe followed by the most appropriate medical treatment.1
CONCLUSIONUntreated GME is invariably fatal, and the dissemi-nated form carries the worst prognosis.21 Radiation ther-apy combined with corticosteroids has been shown tosignificantly increase survival time in dogs with the focalform presenting with forebrain signs. Leflunomide ther-apy is promising; however, prospective evaluations of alarger treatment group with a longer follow-up to sub-stantiate these initial findings is warranted. Cytarabine,procarbazine, and cyclosporine treatment for GME mayresult in better long-term outcomes than those previ-ously reported with glucocorticosteroid treatment alone.
ACKNOWLEDGMENTSThe authors thank Drs. R. Carter, A. Armien, and R. Dickinson for pro-viding the images of the fundus of the eye, the histopathology of brain sec-tion, and the cytology of CSF, respectively.
REFERENCES1. Dewey C: Surgical disorders of the brain. Proc 23rd ACVIM Forum:324–326,2005.
2. Braund K: Granulomatous meningoencephalomyelitis, in Vite C (ed): Clini-cal Neurology in Small Animals—Localization, Diagnosis and Treatment. Ithaca,NY, International Veterinary Information Service, 2005.
3. Cuddon PA, Smith-Maxie L: Reticulosis of the central nervous system in thedog.Compend Contin Educ Pract Vet 6:23–32, 1984.
4. Sorjonen DC: Clinical and histopathological features of granulomatousmeningoencephalomyelitis in dogs. JAAHA 26:141–147, 1990.
5. Summers BA, Cummings JF, de Lahunta A: Granulomatous meningoen-cephalomyelitis, in Veterinary Neuropathology. St Louis, Mosby, 1995, pp110–114.
6. Thomas JB, Eger C: Granulomatous meningoencephalomyelitis in 21 dogs.J Small Anim Pract 30:287–293, 1989.
7. Schatzberg J, Haley N, Barr S, et al: Polymerase chain reaction screening forDNA viruses in paraffin embedded brains from dogs with necrotizingmeningoencephalitis, necrotizing leukoencephalitis, and granulomatousmeningoencephalitis. J Vet Intern Med 19:553–559, 2005.
8. Koestner A, Zeman W: Primary reticulosis of the central nervous system indogs.Am J Vet Res 23:381, 1962.
9. Braund KG, Vandevelde M, Walker T: Granulomatous meningoencephalitisin six dogs. JAVMA 172:1195–1200, 1978.
10. Braund KG: Granulomatous meningoencephalomyelitis, in Braund KG (ed):Clinical Syndrome in Veterinary Neurology, ed 2. St Louis, Mosby, 1994, pp135–139.
11. Vandevelde M, Fatzer R, Fankhauser R: Immunohistological studies on pri-mary reticulosis of the canine brain. Vet Pathol 18:577–588, 1981.
12. Vandevelde E: Neurologic diseases of suspected infectious origin, in GreeneCE (ed): Infectious Diseases of the Dog and Cat, ed 2. Philadelphia, WB Saun-ders, 1998, pp 530–539.
13. Fankhauser R, Fatzer R, Luginbuhl H: Reticulosis of the central nervous sys-tem (CNS) in dogs.Adv Vet Sci Comp Med 16:35–72, 1972.
14. Braund KG: Granulomatous meningoencephalomyelitis. JAVMA 18:138–141, 1985.

November 2007 COMPENDIUM
Granulomatous Meningoencephalomyelitis in Dogs 689CE
15. Kipar A, Baumgartner W, Vogl C, et al: Immunohistochemical characteriza-tion of inflammatory cells in brains of dogs with granulomatous meningoen-cephalomyelitis. Vet Pathol 35:45–52, 1998.
16. Cordy DR: Canine granulomatous meningoencephalomyelitis. Vet Pathol16:325–333, 1979.
17. Russo ME: Primary reticulosis of the central nervous system in dogs. JAVMA174:492–500, 1979.
18. Gearhart M, de Lahunta A, Summer B: Cerebellar mass in a dog due togranulomatous meningoencephalomyelitis. JAAHA 22:683–686, 1986.
19. Koestner A, Bilzer T, Fatzer R, et al: Histological classification of the tumorsof the nervous system of domestic animals, in American Registry of Pathology,World Health Organization, ed 2.Washington, DC, Armed Forces Institute ofPathology, 1999, pp 11–15.
20. Suzuki M, Uchida K, Morozumi M, et al: A comparative pathological studyon canine necrotizing meningoencephalitis and granulomatous meningoen-cephalitis. J Vet Med Sci 65:1233–1239, 2003.
21. Munana KR, Luttgen PJ: Prognostic factors for dogs with granulomatousmeningoencephalomyelitis: 42 cases (1982–1996). JAVMA 212:1902–1906,1998.
22. Matsuki N, Fujiwara K, Tamahara S, et al: Prevalence of autoantibodies incerebrospinal fluids from dogs with various CNS diseases. J Vet Med Sci66:295–297, 2004.
23. Tipold A, Fatzer R, Jaggy A, et al: Necrotizing encephalitis in Yorkshire ter-riers. J Small Anim Pract 34:623–628, 1993.
24. Stalis I, Chadwick B, Dayrell-Hart B, et al: Necrotizing meningoencephalitisof Maltese dogs. Vet Pathol 32:230–235, 1995.
25. Cordy DR, Holliday T: A necrotizing meningoencephalitis of pug dog. VetPathol 26:191–194, 1989.
26. Summers BA, Cummings JF, de Lahunta A: Inflammatory diseases of thecentral nervous system, in Veterinary Neuropathology. St Louis, Mosby, 1995,pp 402–501.
27. Jull B, Merryman J, Thomas W, et al: Necrotizing encephalitis in a Yorkshireterrier. JAVMA 211:1005–1007, 1997.
28. Bailey CS, Higgins RJ: Characteristic of cerebrospinal fluid associated withcanine granulomatous meningoencephalomyelitis: A retrospective study.JAVMA 188:418–421, 1986.
29. Moissonier P, Blot S, Devauchelle P, et al: Stereotactic CT-guided brainbiopsy in the dog. J Small Anim Pract 43:115–123, 2002.
30. Koblik P, LeCouteur RA, Higgins R, et al: CT-guided brain biopsy using amodified Pelorus Mark III stereotactic system: Experience with 50 dogs. VetRadiol Ultrasound 40:434–440, 1999.
31. Adamo P, Lang A: Frameless stereotactic CT-guided needle brain biopsy indogs. Proc 23rd ACVIM Forum:857, 2005.
32. Flegel T, Podell M, March P, Chakeres D: Use of disposable real-time CTstereotactic navigator device for minimally invasive dog brain biopsy througha mini-burr hole.Am J Neuroradiol 23:1160–1163, 2002.
33. Fenner WR: Diseases of the brain, in Ettinger SJ, Feldman EC (eds): Text-book of Veterinary Internal Medicine: Diseases of the Dog and Cat, ed 5. Philadel-phia, WB Saunders, 2000, pp 552–602.
34. LeCouteur R: Tumors of the nervous system, in Withrow SJ, MacEwen EG(eds): Small Animal Clinical Oncology, ed 3. Philadelphia,WB Saunders, 2001,pp 500–531.
35. Cuddon P, Coates J, Murray M: New treatment for granulomatous menin-goencephalitis. Proc 20th ACVIM Forum:319–321, 2002.
36. Chrisman C: Cerebrospinal fluid analysis, in Moore M (ed): Diseases of theSpine. Philadelphia,WB Saunders, 1992, pp 781–809.
37. Bailey C, Vernau W: Cerebrospinal fluid, in Clinical Biochemistry of DomesticAnimals, ed 5. San Diego, Academic Press, 1997, pp 785–827.
38. Bailey C, Higgins R: Characteristic of cisternal cerebrospinal fluid associatedwith primary brain tumors in the dog: A retrospective study. JAVMA188(4):414–417, 1986.
39. Sojonen D: Total protein, albumin quota, and electrophoretic pattern in cere-brospinal fluid of dogs with central nervous system disorders. Am J Vet Res48:301–305, 1987.
40. Cherubini G, Anderson T, Rusbridge C, et al: MRI findings in 7 dogs withconfirmed GME. J Vet Intern Med 19:284, 2005.
41. Mellena L, Samii V, Vernau K, et al: Meningeal enhancement of magnetic res-onance imaging in 15 dogs and 3 cats.Vet Radiol Ultrasound 43:10–15, 2002.
42. Speciale J, Van Winkle TJ, Steinberg SA, et al: Computed tomography in thediagnosis of focal granulomatous meningoencephalitis: Retrospective evalua-tion of three cases. JAAHA 28:327–332, 1992.
43. Dzyban L, Tidwell A: Imaging diagnosis—Granulomatous meningoen-cephalitis in a dog.Vet Radiol Ultrasound 37:428–430, 1996.
44. Adamo P, O’Brien R: Use of cyclosporine to treat granuloma meningoen-cephalitis in three dogs. JAVMA 225:1211–1226, 2004.
45. Plummer S,Wheeler S, Thrall D, Kornegay J: Computed tomography of pri-mary inflammatory brain disorders in dogs and cats. Vet Radiol Ultrasound33:307–312, 1992.
46. Tipold A: Diagnosis of inflammatory and infectious diseases of the central nerv-ous system in dogs: A retrospective study. J Vet InternMed 9:304–314, 1995.
47. Platt S: Recommendations for corticosteroid use in neurological diseases.Proc 20th ACVIM Forum:370–372, 2002.
48. Thomas WB: Inflammatory diseases of the central nervous system in dogs.Clin Tech Small Anim Pract 13:167–168, 1998.
49. Sisson AF, LeCouteur RA, Dow SW, et al: Radiation therapy of granuloma-tous meningoencephalomyelitis of dogs. Proc 7th ACVIM Forum:1031, 1989.
50. LaRue S, Gillette E: Radiation therapy, in Withrow SJ, MacEwen EG (eds):Small Animal Clinical Oncology. Philadelphia,WB Saunders, 2001, pp 119–137.
51. Theon A, LeCouteur RA, Carr E, et al: Influence of tumor cell proliferationand sex hormone receptors on effectiveness of radiation therapy for dogs withincompletely resected meningiomas. JAVMA 216:701–707, 2000.
52. Nuhsbaum MT, Powell CC, Gionfrido JR, et al: Treatment of granulomatousmeningoencephalomyelitis in a dog. Vet Ophthalmol 5:29–33, 2002.
53. Zarfoss M, Schatzberg S, Venator K, et al: Combined cytosine arabinosideand prednisone therapy for meningoencephalitis of unknown aetiology in 10dogs. J Small Anim Pract 47(10):588–595, 2006.
54. Coates J, Barone G, Dewey C, et al: Procarbazine for treatment of suspectedgranulomatous meningoencephalomyelitis: 20 cases (1998–2004). Proc 23rdACVIM Forum:912, 2005.
55. Oliverio V, Denham C, Devita V, Kelly M: Some pharmacologic propertiesof a new antitumor agent N-isopropyl-(2-methylhydrazino)-p-toluamidehydrochloride (NSC-77213).Cancer Chemother Rep 42:1–7, 1964.
56. Daigle JC: More economical use of cyclosporine through combination drugtherapy. JAAHA 38:205–208, 2002.
57. Gorman NT: Immunology, in Feldman E (ed): Textbook of Veterinary InternalMedicine. Philadelphia,WB Saunders, 1995, pp 1978–2002.
58. Bennet WM, Norma DJ: Action and toxicity of cyclosporine. Ann Rev Med37:215–224, 1986.
59. Janeway C, Travers P, Walport M, Shlomchik M: T-cell–medicated immu-nity, in Janeway C (ed): Immunobiology, ed 6. New York, Garland Science,2005, pp 319–366.
60. Steffan J, Strehlau G,Maurer M, Rolphs A: Cyclosporin A pharmacokineticsand efficacy in the treatment of atopic dermatitis in dogs. J Vet PharmacolTher 27:231–238, 2004.
61. Gregory CR: Immunosuppressive agents, in Kirk RW, Bonagura JD (eds):Current Veterinary Therapy. XIII. Small Animal Practice. Philadelphia, WBSaunders, 2000, pp 509–513.
62. Ryffel B: Experimental toxicological studies with cyclosporine A, inWhite DJG(ed):Cyclosporine A. Amsterdam,Elsevier Biomedical Press, 2003, pp 45–75.
63. Adamo PF, Rylander H, Adams WM: Ciclosporin use in multi-drug therapyfor meningoencephalomyelitis of unknown aetiology in dogs. J Small AnimPract 48(9):486–496, 2007.

COMPENDIUM November 2007
Granulomatous Meningoencephalomyelitis in Dogs690 CE
64. D’mello A, Venkataramanan R, Satake M, et al: Pharmacokinetics of thecyclosporine-ketoconazole interaction in dogs. Res Commun Chem PatholPharmacol 64:441–454, 1989.
65. Sturges B, LeCouteur RA, Gregory C, et al: Leflunomide for treatment ofinflammatory or malacic lesions in three dogs: A preliminary clinical study.Proc 16th ACVIM Forum:40, 1998.
1. The histopathologic appearance of GME is char-acterized bya. necrotic changes in the brainstem.b. necrotic changes in the cerebral cortex.c. perivascular cuffs composed of lymphocytes, a vary-
ing number of macrophages, and plasma cells in theparenchyma and meninges of the brain and spinalcord.
d. diffuse brain necrotic changes with perivascular accu-mulation of polymorphonucleated cells.
2. Which statement regarding the signalment forGME is most correct?a. Pugs, Maltese, and Yorkshire terriers appear to be
predisposed.b. Large-breed dogs appear to be predisposed.c. Any breed of dog of any age and either sex may be
affected; however, older dogs appear to be predis-posed.
d. Any breed of dog of any age and either sex may beaffected; however, young to middle-aged, female,small-breed dogs appear to be predisposed.
3. Based on the site and distribution of the lesions,GME is classified intoa. two morphologic forms: disseminated and focal.b. three morphologic forms: disseminated, focal, and
ocular.c. four morphologic forms: disseminated, focal, ocular,
and cerebellar.d. none of the above
4. What is the most likely cause proposed for GME?a. virus c. neoplasiab. autoimmune disease d. protozoa
5. Definitive diagnosis of GME requiresa. viral isolation.b. detection of a histopathologic lesion on brain biopsy
or necropsy.c. detection of inclusion bodies in lymphocytes in the
CSF.d. detection of unidentified protozoa in macrophages in
the CSF.
6. CSF analysis in dogs with GME is characterized bya high total protein concentration and an elevatedtotal nucleated cell count with a predominance ofa. macrophages. c. small lymphocytes.b. neutrophils. d. eosinophils.
7. Characteristic MRI features of GME consist ofa. single or multiple lesions, primarily involving the white
matter, that are hyperintense on T2-weighted andFLAIR images and hypointense onT1-weighted images.
b. single or multiple lesions, primarily involving the whitematter, that are hypointense on T2-weighted andFLAIR images and hypointense onT1-weighted images.
c. single or multiple lesions, primarily involving the whitematter, that are hyperintense on T2-weighted andFLAIR images and hyperintense on T1-weightedimages.
d. No characteristic MRI features have been describedfor GME.
8. The following new alternative therapies havebeen proposed for GME:a. cytarabine, procarbazine, radiation therapy, lefluno-
mide, and cyclosporine.b. cytarabine, amphotericin B, radiation therapy, and
cyclosporine.c. cytarabine, cyclophosphamide, procarbazine, and radi-
ation therapy.d. cytarabine, itraconazole, radiation therapy, and
cyclosporine.
9. _________ is the most significant side effect ofcytarabine when used in the treatment of GME.a. Myelosuppression c. Renal failureb. Papillomatosis d. Hepatic failure
10. The most common side effects of cyclosporine inthe treatment of GME area. gingival hyperplasia and hypertrichosis.b. lymphopenia and anemia.c. hepatic and renal failure.d. gingival hyperplasia and hepatic failure.
ARTICLE #2 CETESTThis article qualifies for 2 contact hours of continuingeducation credit from the Auburn University Collegeof Veterinary Medicine. Subscribers may purchaseindividual CE tests or sign up for our annualCE program. Those who wish to apply this credit tofulfill state relicensure requirements should consult theirrespective state authorities regarding the applicabilityof this program. CE subscribers can take CE tests onlineand get real-time scores at CompendiumVet.com.
CE