1. 2 Spore-forming Bacilli Genus Bacillus Genus Clostridium.
Upload
clementine-snowCategory
view
235download
2
Gram + Bacilli: Spore-forming
(Bacillus & Clostridium), andNon-spore forming
(Listeria, Corynebacterium, Mycobacteria)
Nestor T. Hilvano, M.D., M.P.H.
Learning Objectives You should be able to: 1. Describe three clinical manifestations of Bacillus anthracis and
identify its diagnosis and prevention. 2. Identify the mechanisms of pathogenicity, diagnosis, treatment, and
prevention of Clostridium perfringens. 3. Contrast three manifestations of botulism poisoning and its treatment
and prevention.4. Describe the epidemiology, treatment, and prevention of tetanus. 5. Discuss Listeria monocytogenes as to its pathogenicity, infections,
diagnosis, treatment, and prevention.6. Characterize Corynebacterium as to morphology, transmission,
disease, diagnosis, treatment, and prevention. 7. Characterize mycobacteria in terms of cell wall composition, growth
rate, and resistance to antimicrobial drugs. 8. Describe the transmission of Mycobacterium tuberculosis and
discuss diagnosis, treatment, and prevention of tuberculosis. 9. Compare and contrast tuberculoid leprosy with lepromatous leprosy. 10. Discuss the diagnosis, treatment, and prevention of leprosy.
Bacillus anthracis• Facultative anaerobe; gm + rod, central endospore;
peritrichous• Transmission= endospore from infected animals
• 3 Clinical manifestations
1. Cutaneous anthrax – solid, painless
nodule; eschar (crusty ulcer); 20% fatal
2. Inhalation anthrax – airborne
endospores; produce toxemia
(fever, labored breathing, shock);
100% die untreated; 50% fatal (even w/ Rx)
3. GIT anthrax – rare in human; intestinal bleeding• Prevention – vaccination of livestock• Does steaming of mails suspected with anthrax contamination
prevents the spread of infection?
Clostridium • Soil, water, sewage, and GIT of humans and animals;
anaerobes; gm + rod• Pathogenicity- endospore survive; vegetative cells secrete
toxins (histolytic toxins, enterotoxins, & neurotoxins)• C. perfringens – isolated from clinical specimens; toxins lyse
blood cells; common cause of food poisoning in U.S. and gas gangrene; over 40% fatal even w/ Rx; Prevention = refrigeration and reheating, proper cleaning of wound
• C. difficile - opportunistic pathogens in patients Rx w/ broad spectrum antibiotics; release toxins and enzyme hyaluronidase; hemorrhagic necrosis of intestine; pseudomembranous colitis (antibiotic -associated diarrhea)
Clostridium botulinum • soil and water; improper canning of food• Exotoxin = neurotoxin, blocks acetylcholine release in cholinergic synapses (CNS/PNS)- muscle weakness (muscles can’t contract)
• Food-borne botulism – ingestion of contaminated food, exotoxin absorbed into blood (incubation less than 24 hrs., 10 ug fatal), death within few hours to 1 week (60-70% fatal); recovery of 6 to 8 months
- Symptoms = vomiting, constipation, double vision, thirst, thick saliva, paralysis of pharynx/diaphragm - Prevention: strict hygienic canning
- Rx: Antitoxin
• Infant botulism from ingestion of endospores (paralysis & death rare)
• Wound botulism - endospores germinate in wounds
Clostridium tetani• Gm +, anaerobic,with terminal endospore
• in soil, dust, feces
• tetanus toxin (neurotoxin) – affects AHC of spinal cord, interferes w/ inhibitory signal to muscles causing sustained contract →rigidity of muscles (locked jaw, bend back)
• tetanolysin = hemolytic

Causes, Prevention, & Rx of Tetanus• Common in non-immunized children, after
abortions, septic deliveries, infection of umbilical cord
• Prevention
– tetanus toxoids (deactivated tetanus toxins;
immunogenic to prevent tetanus);
- DPT vaccines
• Treatment
- antitoxin; antibiotics
Listeria monocytogenes • Listeriosis • Gm +, non-endospore forming coccobacilli• Intracellular in macrophages• MOT: human to human; transfer of agent from pregnant
woman to fetuses• Pathogenicity
- From animal/human feces, soil, water, food
- rarely symptomatics or mild flulike illness
- sepsis/ meningitis in immunocompromised
- spontaneous abortion, stillbirth, or meningitis in newborn
(lead to brain damage or death, 60%)
• Rx – penicillin
Corynebacterium diptheria • Gm + rod, V shaped/ palisade, non-endospore-
forming, aerobic• Droplets inhalation• Toxin = resp. for S/Sx
- necrosis of epithelium, leakage of exudates, pseudomembrane formation (necrotic epith. + C. d. + proteins)- swelling, dislodged pseudomembrane- obstruction, suffocation
• Complication affect kidney, heart, and nerves • Dx. – Immunodiffusion assay (Elek test)• Rx. – antitoxin (horse serum), penicillin or
erythromycin• Prev. – DPT shots (2,4,6 months; booster every 10
yrs.)
Mycobacterium tuberculosis • Waxy lipid (mycolic acid) cell wall; slender rods (AFB)• >50,000 new cases/yr.; 10,000 deaths/yr.• Deep inhalation of organisms; droplet (5um) w/ 1-3 bacilli • Tubercle/granuloma formation
- phagocytosis by macrophages
- intracellular multiplication
- macrophage bursting
- ingestion of TB by macrophages
- fibroblast proliferation,
recruitment of lymphocytes, walling off by fibroblasts
- caseous necrosis (cheeselike due to release of proteins + fats from
dying cells) → cavity formation; macrophage fusion
- calcification
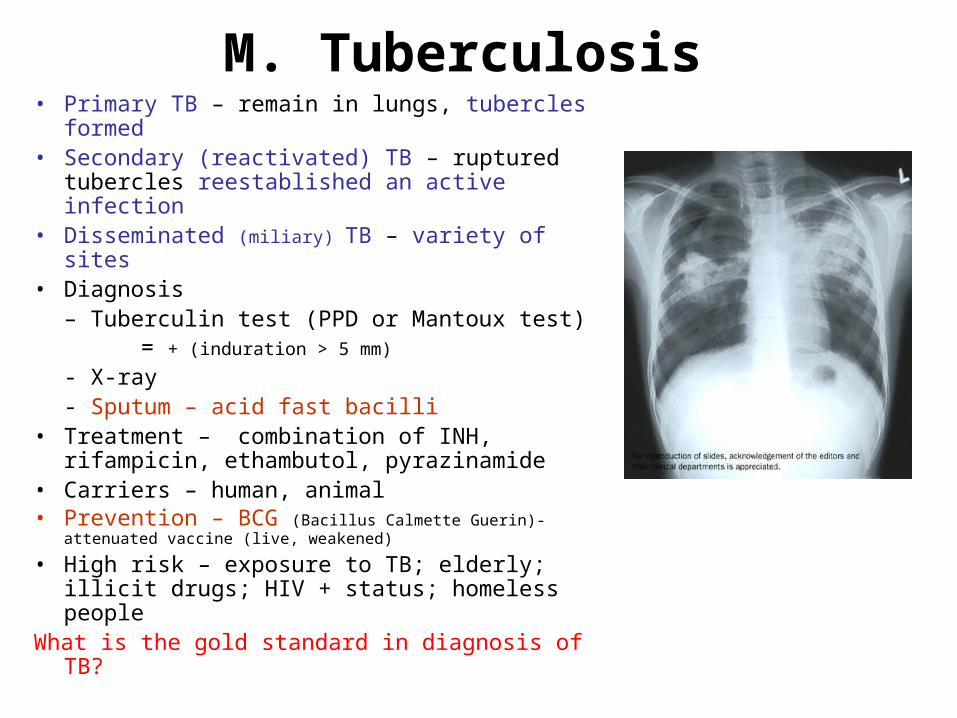
M. Tuberculosis • Primary TB – remain in lungs, tubercles
formed• Secondary (reactivated) TB – ruptured
tubercles reestablished an active infection• Disseminated (miliary) TB – variety of sites • Diagnosis
– Tuberculin test (PPD or Mantoux test) = + (induration > 5 mm)
- X-ray - Sputum – acid fast bacilli
• Treatment – combination of INH, rifampicin, ethambutol, pyrazinamide
• Carriers – human, animal• Prevention – BCG (Bacillus Calmette Guerin)-
attenuated vaccine (live, weakened)
• High risk – exposure to TB; elderly; illicit drugs; HIV + status; homeless people
What is the gold standard in diagnosis of TB?
Mycobacterium leprae • Hansen’s disease• Grow best at 30˚C (peripheral nerve endings;
skin cells in ear lobes, lips, fingers, toes)• Human and Armadillos hosts• Transmission – direct contact; inhalation of
droplets; breaks in skin (only after years of intimate social contact)
• 2 forms – tuberculoid and lepromatous • Tuberculoid leprosy – nonprogressive
destruction of body; loss of sensory in affected nerve (pain, temp., proprioception)
Lepromatous leprosy • Virulent form• 1990, 12 million cases worldwide; 2004, decreased to
457,792 (only 81 cases in US)
• Incubation take years before S/Sx• Progressive disfigurement • Dx - + skin test with leprosy antigen
or direct AFB smear • Rx – multiple drug (clofazidime, rifampicin, dapsone for
atleast 2 yrs. or lifelong for some)• Prevention – BCG; prophylactic antibiotics
Exotoxin • Produced by both gram + and gram –
bacteria
• Released from cell
• Protein chemical unit
• Heat labile
• Specific receptors on target cells
• Specific effects in host
• Toxoids (Antibodies) can be made by treating with formalin
Homework
1. Define terms – tuberculin test, BCG, lepromatous leprosy, tuberculoid leprosy, gas gangrene, Elek test, primary tuberculosis
2. Describe the 3 clinical manifestations of anthrax diseases and its prevention.
3. Discuss pathogenicity (causative agent) and prevention of gas gangrene, food-borne botulism, and tetany.
4. What diagnostic test is confirmative of an active case of tuberculosis?