Goldstein atrial fibrillation1
28
2/13/2015 1 Atrial Fibrillation It Doesn’t Have to Be Irregular Anymore Edward Goldstein PA-C Lead Electrophysiology PA. UCVA Cardiology Rochester,NY Disclosure • None LEARNING POINTS What is Atrial Fibrillation? Why do we care? Treatment Options:Rate vs Rhythm Anticoagulation: Coumadin vs NOACs
Transcript of Goldstein atrial fibrillation1
2/13/2015
1
Atrial FibrillationIt Doesn’t Have to Be Irregular
Anymore
Edward Goldstein PA-C
Lead Electrophysiology PA.
UCVA Cardiology
Rochester,NY
Disclosure
• None
LEARNING POINTS
What is Atrial Fibrillation?
Why do we care?
Treatment Options:Rate vs Rhythm
Anticoagulation: Coumadin vs NOACs
2/13/2015
2
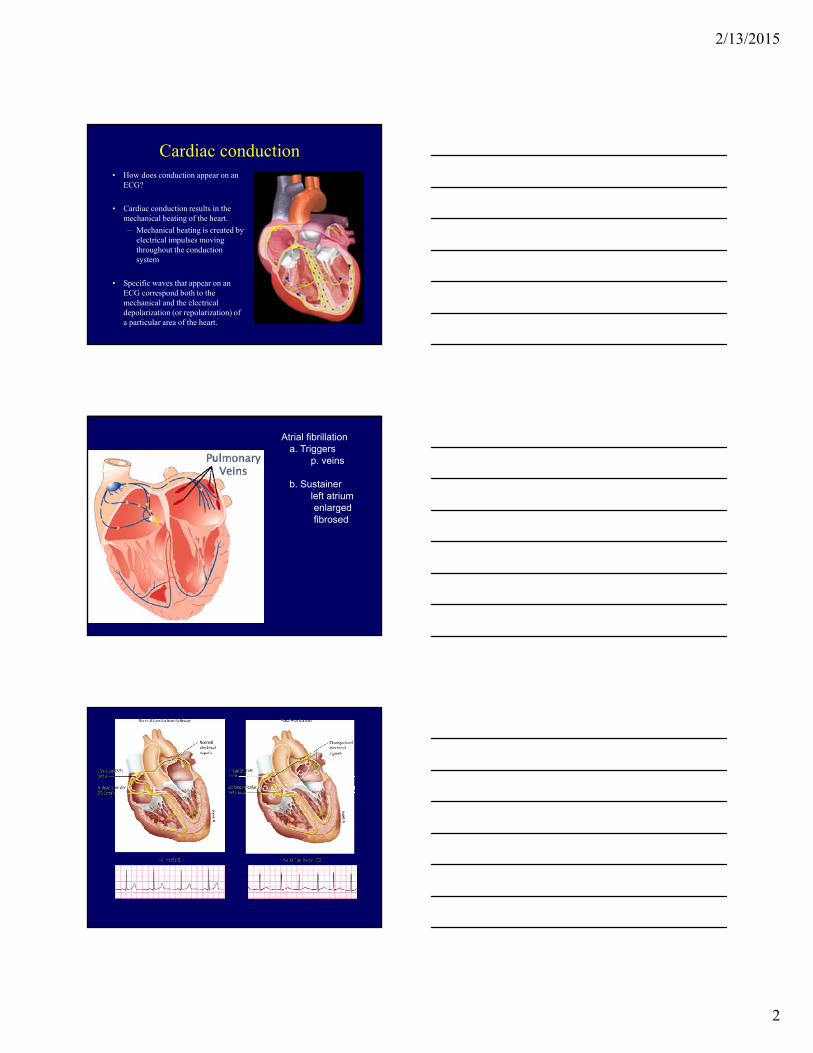
Cardiac conduction• How does conduction appear on an
ECG?
• Cardiac conduction results in the mechanical beating of the heart.
– Mechanical beating is created by electrical impulses moving throughout the conduction system
• Specific waves that appear on an ECG correspond both to the mechanical and the electrical depolarization (or repolarization) of a particular area of the heart.
Atrial fibrillationa. Triggers
p. veins
b. Sustainerleft atriumenlargedfibrosed
2/13/2015
3
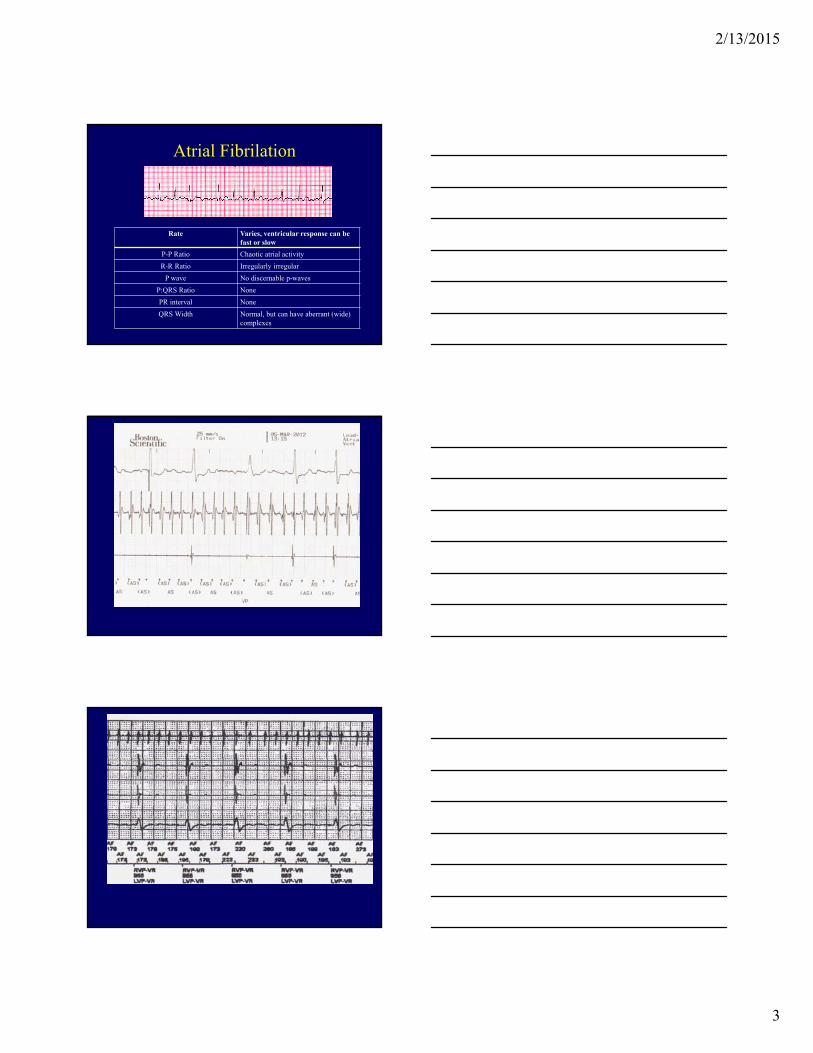
Atrial Fibrilation
Rate Varies, ventricular response can be fast or slow
P-P Ratio Chaotic atrial activity
R-R Ratio Irregularly irregular
P wave No discernable p-waves
P:QRS Ratio None
PR interval None
QRS Width Normal, but can have aberrant (wide) complexes
2/13/2015
4
Is Atrial Fibrillation Important?
• 2.5 million Americans with Atrial Fib
• 88,000 deaths per year
• $16 billion dollars cost to health care per year
Estimated Number of Atrial Fib Cases by 2030
• A) 3 million
• B) 5 million
• C) 7 million
Atrial fibrillation treatment
2/13/2015
5
Atrial fibrillation
April 2010:March 2010: 1,980,000 hits
March 2011: 2,550,000 hits
January 2012: 9,500,000 hits
Stroke Prevention in Atrial Fibrillation-
2/13/2015
6
Background
• 30% of ischemic strokes are of unknown mechanism (cryptogenic stroke)
• Detection of AF usually prompts long-term anticoagulation instead of antiplatelet therapy
• Optimal monitoring duration to detect AF is currently undetermined
Objectives of CRYSTAL AF
• To assess whether a long-term monitoring strategy with an insertable cardiac monitor (ICM) is superior to standard medical care for the detection of AF in patients with a cryptogenic stroke at 6 months (primary end point) and 12 months follow-up (secondary end point)
• Determine the proportion of patients with cryptogenic stroke that have underlying AF.
Comparison of Monitoring Strategies
Minimally invasive outpatient procedure
Local anesthetic and no leads orfluoroscopy
15-30 minute procedure
Device can be followed remotely
MRI conditional
3 year device longevity
Continuous Monitoring Arm: Insertion of REVEAL® XT
Standard Monitoring Arm
Cardiac monitoring performed according to local standards, after mandated testing completed
Symptoms consistent with AF were evaluated by study physicians
Reveal LINQ InsertionAnimation-hi-res.mp4
Reveal LINQ InsertionAnimation-hi-res.mp4
2/13/2015
7
Reveal LINQ InsertionAnimation-hi-res.mp4
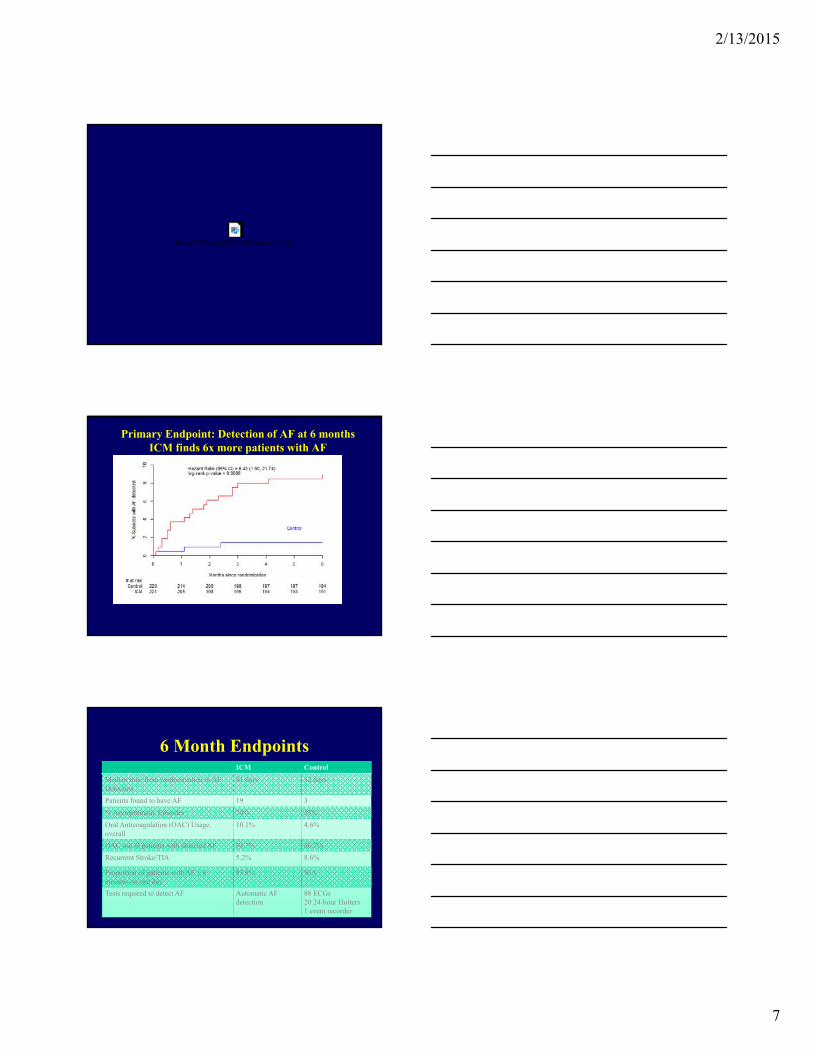
Primary Endpoint: Detection of AF at 6 monthsICM finds 6x more patients with AF
Rate of detection in ICM arm was 8.4% vs 1.4% in control arm
6 Month EndpointsICM Control
Median time from randomization to AF Detection
41 days 32 days
Patients found to have AF 19 3
% Asymptomatic Episodes 74% 33%
Oral Anticoagulation (OAC) Usage, overall
10.1% 4.6%
OAC use in patients with detected AF 94.7% 66.7%
Recurrent Stroke/TIA 5.2% 8.6%
Proportion of patients with AF ≥ 6 minutes on one day
93.8% N/A
Tests required to detect AF Automatic AF detection
88 ECGs20 24-hour Holters 1 event recorder
2/13/2015
8
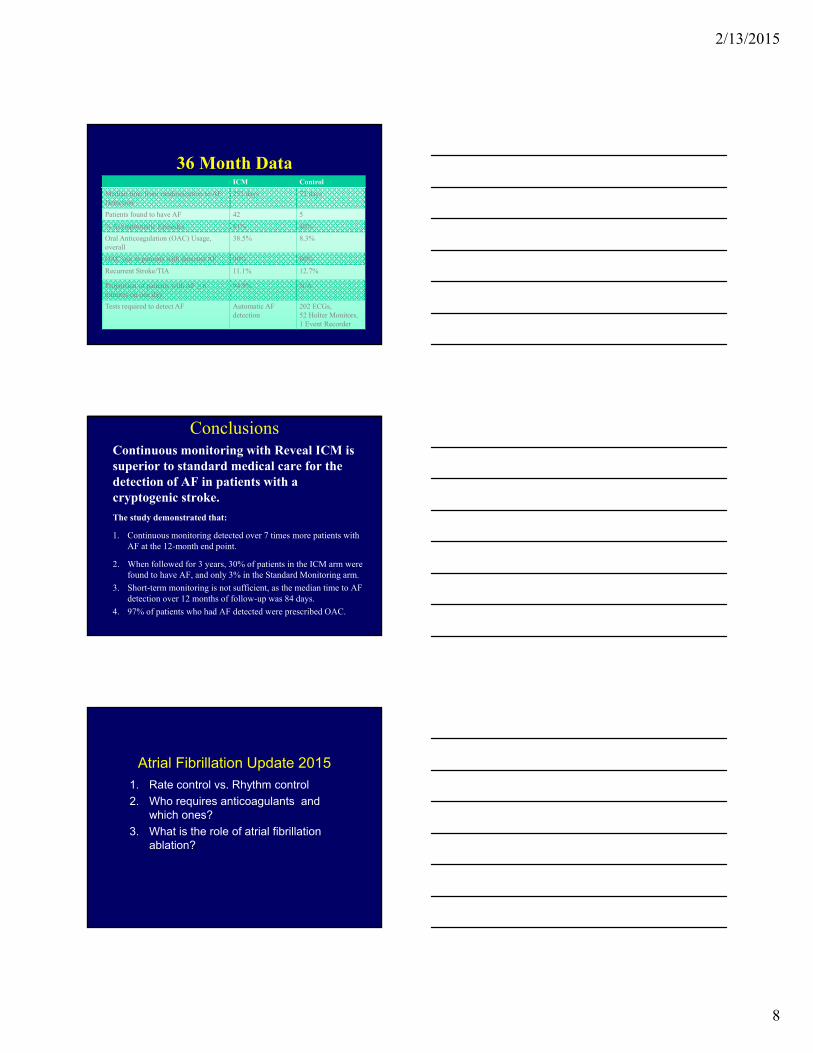
36 Month DataICM Control
Median time from randomization to AF Detection
252 days 72 days
Patients found to have AF 42 5
% Asymptomatic Episodes 81% 40%
Oral Anticoagulation (OAC) Usage, overall
38.5% 8.3%
OAC use in patients with detected AF 90% 80%
Recurrent Stroke/TIA 11.1% 12.7%
Proportion of patients with AF ≥ 6 minutes on one day
94.9% N/A
Tests required to detect AF Automatic AF detection
202 ECGs, 52 Holter Monitors, 1 Event Recorder
ConclusionsContinuous monitoring with Reveal ICM is superior to standard medical care for the detection of AF in patients with a cryptogenic stroke.
The study demonstrated that:
1. Continuous monitoring detected over 7 times more patients with AF at the 12-month end point.
2. When followed for 3 years, 30% of patients in the ICM arm were found to have AF, and only 3% in the Standard Monitoring arm.
3. Short-term monitoring is not sufficient, as the median time to AF detection over 12 months of follow-up was 84 days.
4. 97% of patients who had AF detected were prescribed OAC.
Atrial Fibrillation Update 2015
1. Rate control vs. Rhythm control
2. Who requires anticoagulants and which ones?
3. What is the role of atrial fibrillation ablation?
2/13/2015
9
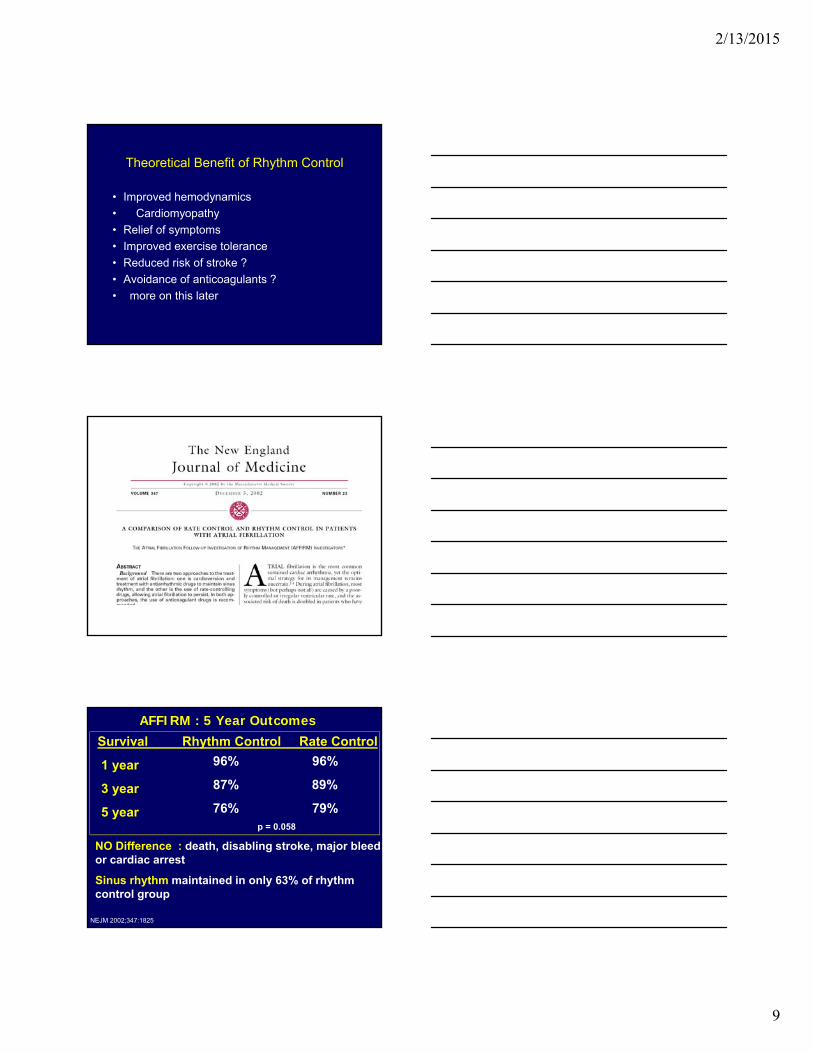
Theoretical Benefit of Rhythm Control
• Improved hemodynamics
• Cardiomyopathy
• Relief of symptoms
• Improved exercise tolerance
• Reduced risk of stroke ?
• Avoidance of anticoagulants ?
96% 96%
87% 89%
76% 79%p = 0.058
NO Difference : death, disabling stroke, major bleed,or cardiac arrest
Sinus rhythm maintained in only 63% of rhythm control group
AFFIRM : 5 Year Outcomes
NEJM 2002;347:1825
Survival Rhythm Control Rate Control
1 year
3 year
5 year
2/13/2015
10
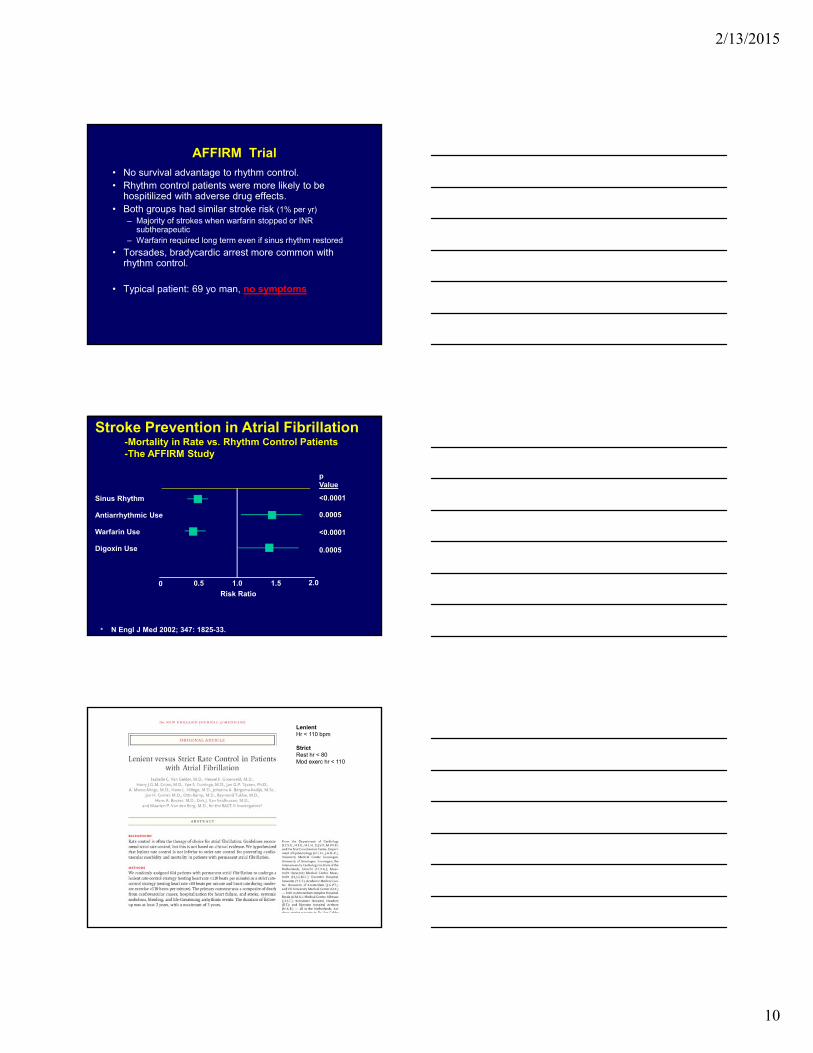
AFFIRM Trial
• No survival advantage to rhythm control.• Rhythm control patients were more likely to be
hospitilized with adverse drug effects.• Both groups had similar stroke risk (1% per yr)
– Majority of strokes when warfarin stopped or INR subtherapeutic
– Warfarin required long term even if sinus rhythm restored
• Torsades, bradycardic arrest more common with rhythm control.
• Typical patient: 69 yo man, no symptoms
Sinus Rhythm
Antiarrhythmic Use
Warfarin Use
Digoxin Use
0.5 1.0 1.5
Risk Ratio0
pValue
<0.0001
0.0005
<0.0001
0.0005
• N Engl J Med 2002; 347: 1825-33.
Stroke Prevention in Atrial Fibrillation-Mortality in Rate vs. Rhythm Control Patients -The AFFIRM Study
2.0
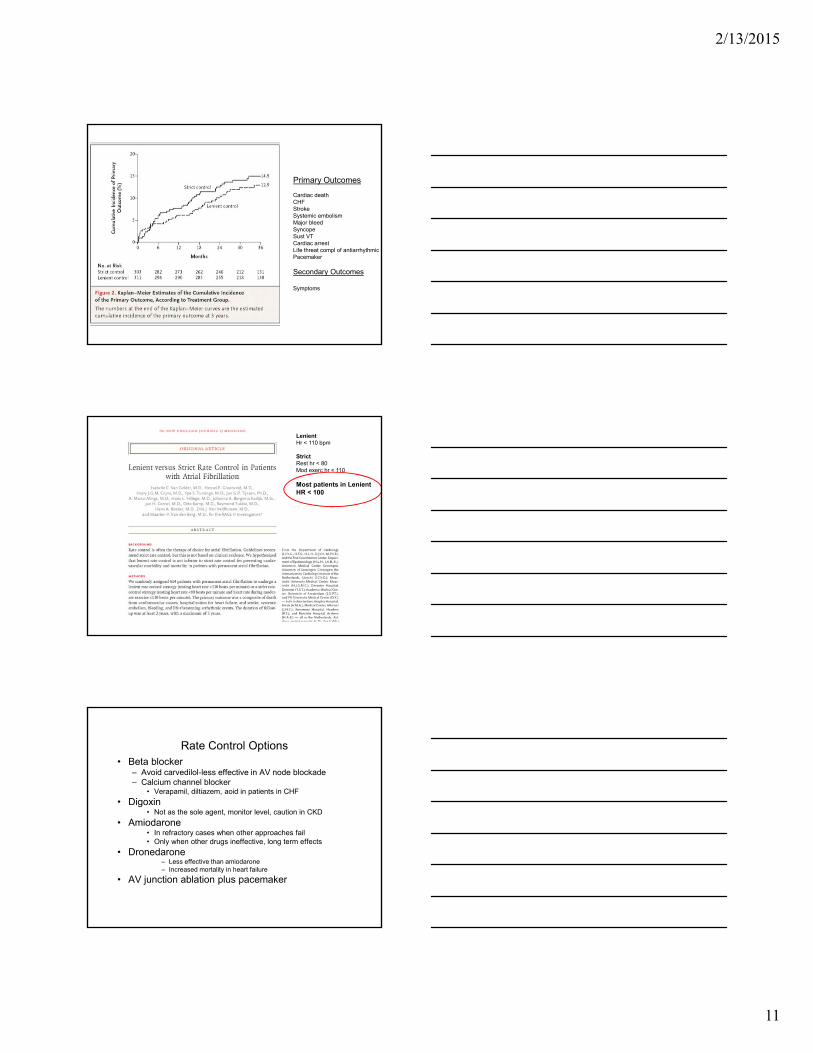
LenientHr < 110 bpm
StrictRest hr < 80Mod exerc hr < 110
2/13/2015
11
Primary Outcomes
Cardiac deathCHFStrokeSystemic embolismMajor bleedSyncopeSust VTCardiac arrestLife threat compl of antiarrhythmicPacemaker
Secondary Outcomes
Symptoms
LenientHr < 110 bpm
StrictRest hr < 80Mod exerc hr < 110
Most patients in Lenient HR < 100
Rate Control Options• Beta blocker
– Avoid carvedilol-less effective in AV node blockade– Calcium channel blocker
• Verapamil, diltiazem, aoid in patients in CHF
• Digoxin• Not as the sole agent, monitor level, caution in CKD
• Amiodarone• In refractory cases when other approaches fail• Only when other drugs ineffective, long term effects
• Dronedarone– Less effective than amiodarone– Increased mortality in heart failure
• AV junction ablation plus pacemaker
2/13/2015
12
Date of download: 2/12/2015
Copyright © The American College of Cardiology. All rights reserved.
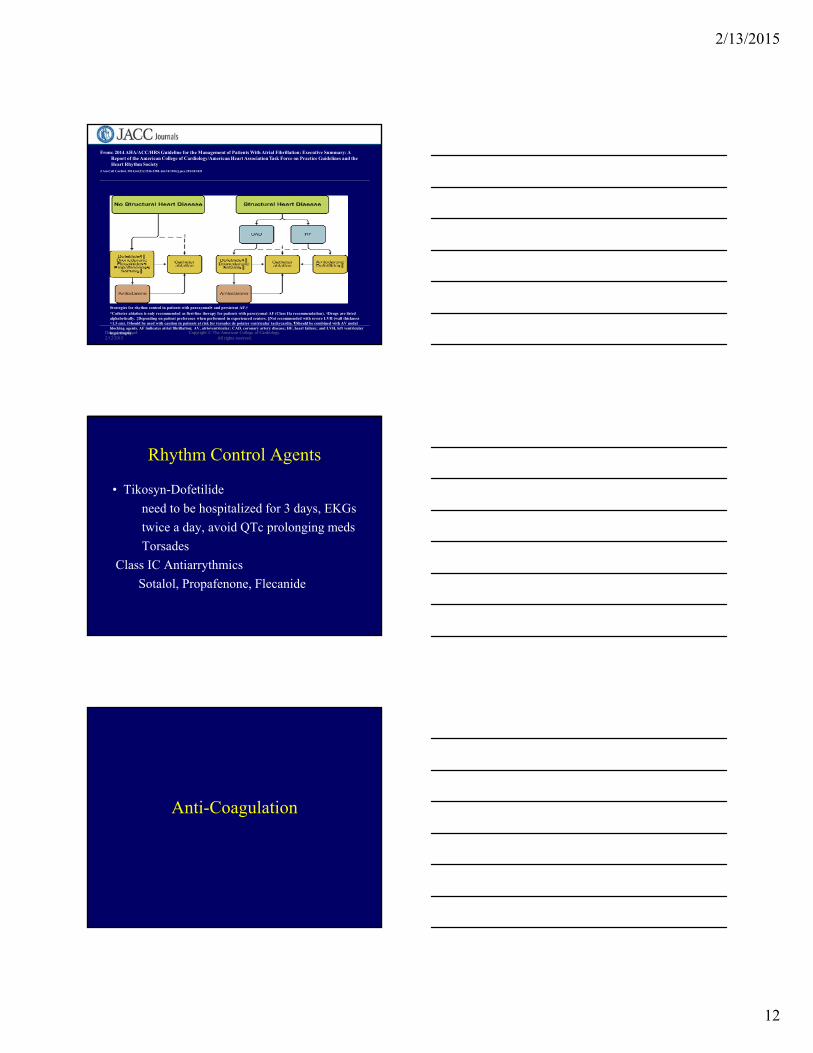
From: 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society
J Am Coll Cardiol. 2014;64(21):2246-2280. doi:10.1016/j.jacc.2014.03.021
Strategies for rhythm control in patients with paroxysmal∗ and persistent AF.†
*Catheter ablation is only recommended as first-line therapy for patients with paroxysmal AF (Class IIa recommendation). †Drugs are listed alphabetically. ‡Depending on patient preference when performed in experienced centers. §Not recommended with severe LVH (wall thickness >1.5 cm). ‖Should be used with caution in patients at risk for torsades de pointes ventricular tachycardia. ¶Should be combined with AV nodal blocking agents. AF indicates atrial fibrillation; AV, atrioventricular; CAD, coronary artery disease; HF, heart failure; and LVH, left ventricular hypertrophy.
Figure Legend:
Rhythm Control Agents
• Tikosyn-Dofetilide
need to be hospitalized for 3 days, EKGs
twice a day, avoid QTc prolonging meds
Torsades
Class IC Antiarrythmics
Sotalol, Propafenone, Flecanide
Anti-Coagulation
2/13/2015
13
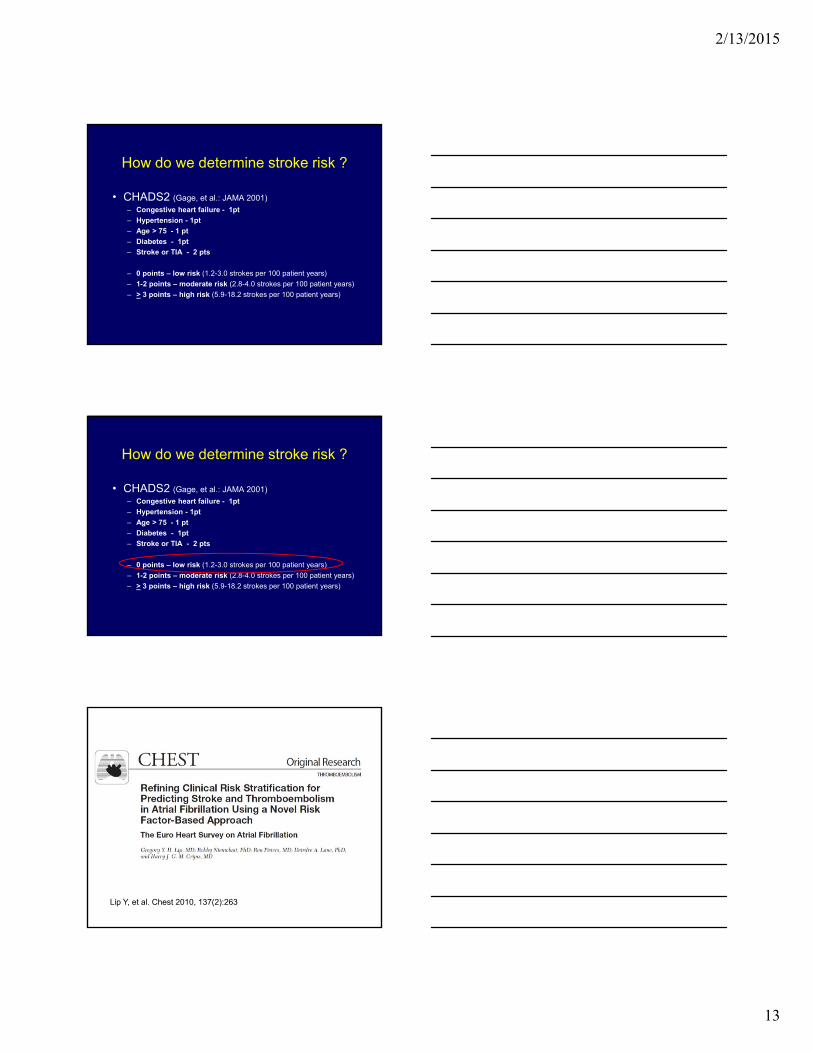
How do we determine stroke risk ?
• CHADS2 (Gage, et al.: JAMA 2001)
– Congestive heart failure - 1pt
– Hypertension - 1pt
– Age > 75 - 1 pt
– Diabetes - 1pt
– Stroke or TIA - 2 pts
– 0 points – low risk (1.2-3.0 strokes per 100 patient years)
– 1-2 points – moderate risk (2.8-4.0 strokes per 100 patient years)
– > 3 points – high risk (5.9-18.2 strokes per 100 patient years)
How do we determine stroke risk ?
• CHADS2 (Gage, et al.: JAMA 2001)
– Congestive heart failure - 1pt
– Hypertension - 1pt
– Age > 75 - 1 pt
– Diabetes - 1pt
– Stroke or TIA - 2 pts
– 0 points – low risk (1.2-3.0 strokes per 100 patient years)
– 1-2 points – moderate risk (2.8-4.0 strokes per 100 patient years)
– > 3 points – high risk (5.9-18.2 strokes per 100 patient years)
Lip Y, et al. Chest 2010, 137(2):263
2/13/2015
14
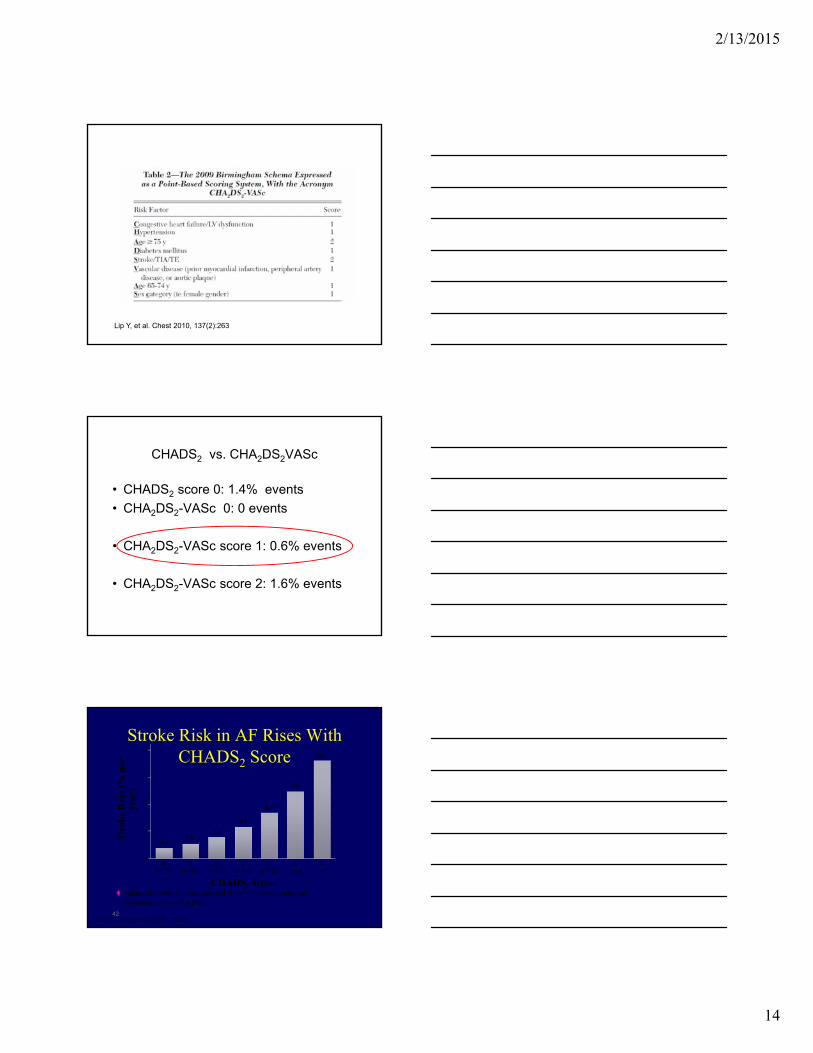
Lip Y, et al. Chest 2010, 137(2):263
CHADS2 vs. CHA2DS2VASc
• CHADS2 score 0: 1.4% events
• CHA2DS2-VASc 0: 0 events
• CHA2DS2-VASc score 1: 0.6% events
• CHA2DS2-VASc score 2: 1.6% events
Stroke Risk in AF Rises With CHADS2 Score
42Fuster V et al. J Am Coll Cardiol. 2011;57(11):e101-e198.
20
5
15
10
0
1.92.8
4.0
5.9
8.5
12.5
18.2
0n=120
1n=463
2n=523
3n=337
4n=220
5n=65
6n=5
CHADS2 Score
Str
oke
Rat
e (%
per
ye
ar)
♦ Adjusted stroke rate was derived from multivariate analysis assuming no use of aspirin
2/13/2015
15
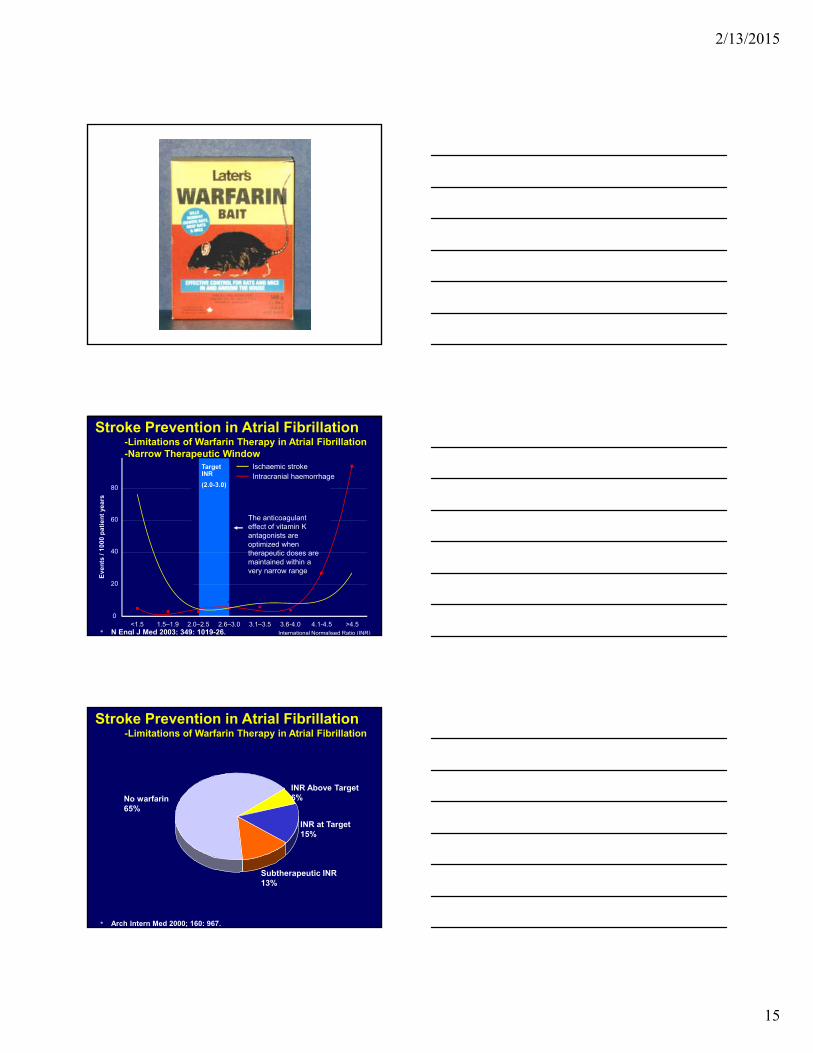
International Normalised Ratio (INR)
Target INR
(2.0-3.0)
<1.5 1.5–1.9 2.0–2.5 2.6–3.0 3.1–3.5 3.6-4.0 4.1-4.5 >4.50
20
40
60
80
Ev
en
ts /
10
00
pa
tie
nt
yea
rs
Intracranial haemorrhageIschaemic stroke
The anticoagulant effect of vitamin K antagonists are optimized when therapeutic doses are maintained within a very narrow range
• N Engl J Med 2003; 349: 1019-26.
Stroke Prevention in Atrial Fibrillation-Limitations of Warfarin Therapy in Atrial Fibrillation-Narrow Therapeutic Window
INR Above Target6%
Subtherapeutic INR 13%
INR at Target15%
No warfarin65%
• Arch Intern Med 2000; 160: 967.
Stroke Prevention in Atrial Fibrillation-Limitations of Warfarin Therapy in Atrial Fibrillation
2/13/2015
16
Meta-Analysis to Assess the Quality of Warfarin Control in
AF in the United States
In the United States, AF patients spend only about one-half the time within therapeutic INR. Anticoagulation clinic services are associated with somewhat better INR control compared with standard community care. 55% therapeutic range, “coumadin clinc” 11% better contol
• Analyzed 323 patients with a second ischemic stroke who had known atrial fibrillation at the time of their first stroke, and who had no known contraindications to anticoagulation
• Stroke 2009; 40: 235-40.
Stroke Prevention in Atrial Fibrillation-Limitations of Warfarin Therapy in Atrial Fibrillation-2o Prevention of Strokes in Patients with A Fib
Subtherapeutic INR 39%
INR at Target18%
No warfarin43%
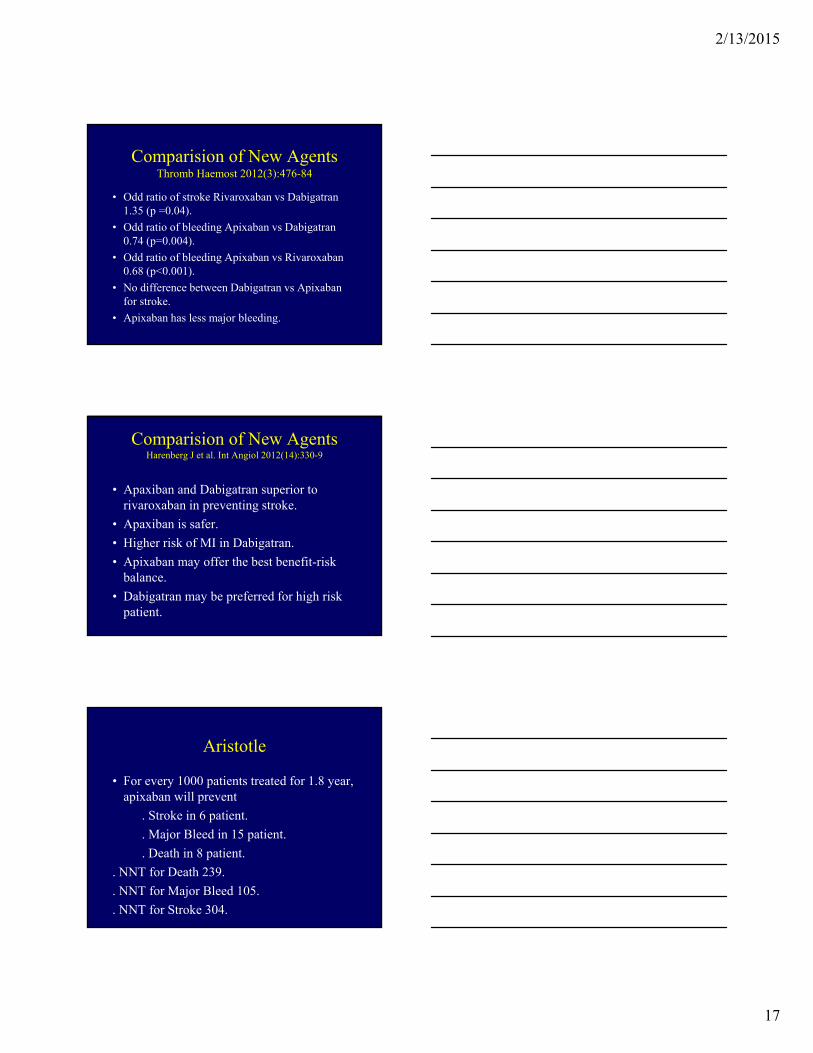
New Anticoagulation Agents
Dabigatran Warfarin Rivaroxaban Warfarin Apixaban Warfarin
Stroke 1.11% 1.69% 1.7% 2.2% 1.27% 1.6%
Major Bleed
3.11% 3.36% 3.6% 3.4% 2.13% 3.09%
HS 0.1% 0.38% 0.5% 0.7% 0.24% 0.47%
Mortality 3.64% 4.13% 4.9% 4.5% 3.52% 3.94%
2/13/2015
17
Comparision of New AgentsThromb Haemost 2012(3):476-84
• Odd ratio of stroke Rivaroxaban vs Dabigatran 1.35 (p =0.04).
• Odd ratio of bleeding Apixaban vs Dabigatran 0.74 (p=0.004).
• Odd ratio of bleeding Apixaban vs Rivaroxaban 0.68 (p<0.001).
• No difference between Dabigatran vs Apixaban for stroke.
• Apixaban has less major bleeding.
Comparision of New AgentsHarenberg J et al. Int Angiol 2012(14):330-9
• Apaxiban and Dabigatran superior to rivaroxaban in preventing stroke.
• Apaxiban is safer.
• Higher risk of MI in Dabigatran.
• Apixaban may offer the best benefit-risk balance.
• Dabigatran may be preferred for high risk patient.
Aristotle
• For every 1000 patients treated for 1.8 year, apixaban will prevent
. Stroke in 6 patient.
. Major Bleed in 15 patient.
. Death in 8 patient.
. NNT for Death 239.
. NNT for Major Bleed 105.
. NNT for Stroke 304.
2/13/2015
18
Who should remain on warfarin?
• Patient already receiving warfarin and stable whose INR is easy to control
• If dabigatran, rivaroxaban, apixaban not available
• Cost
• If patient not likely to comply with twice daily dosing (Dabigatran, Apixaban)
• Chronic kidney disease (GFR < 30 ml/min)
How about Clopidogrel + Aspirin ?
N Engl J Med online publication March 31, 2009
How about Clopidogrel + Aspirin ?
N Engl J Med online publication March 31, 2009
Aspirin: stroke 3.4% per yearmajor bleed 1.27% per year
Aspirin + clopidogrel:stroke 2.4% per yearmajor bleed 2.0% per year
2/13/2015
19
What is new in atrial fibrillation ablation?
2/13/2015
20
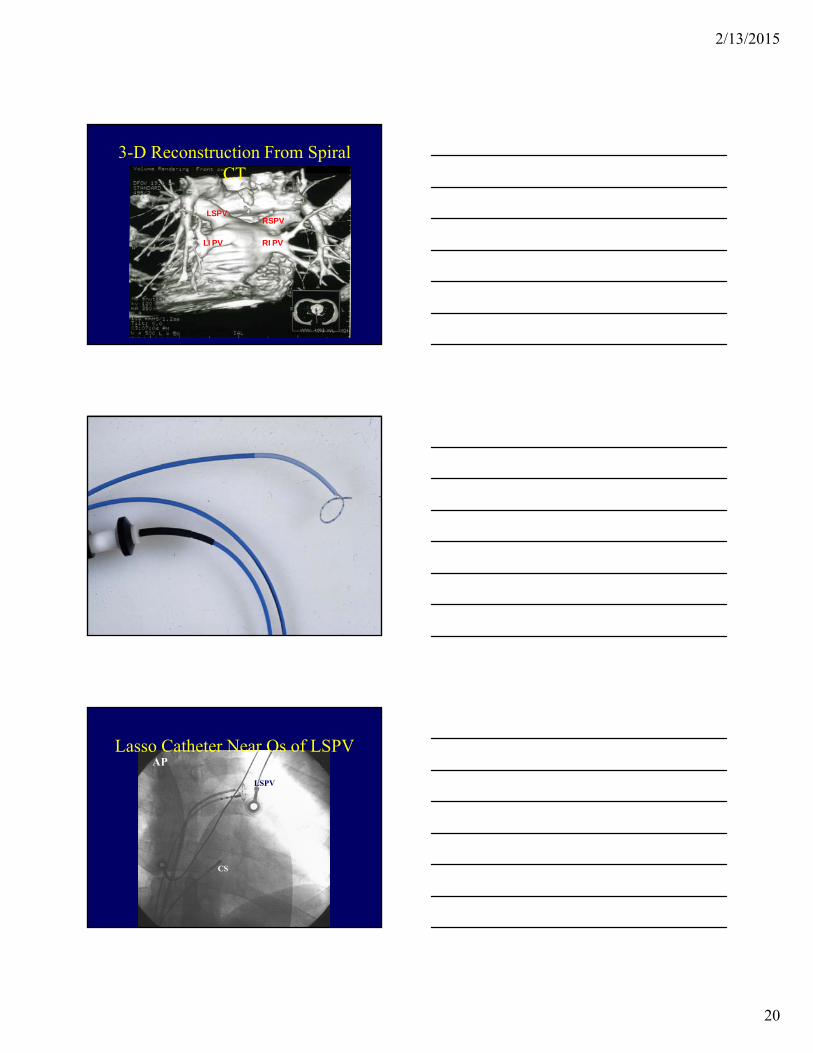
RSPV
RIPV
LSPV
LIPV
3-D Reconstruction From Spiral CT
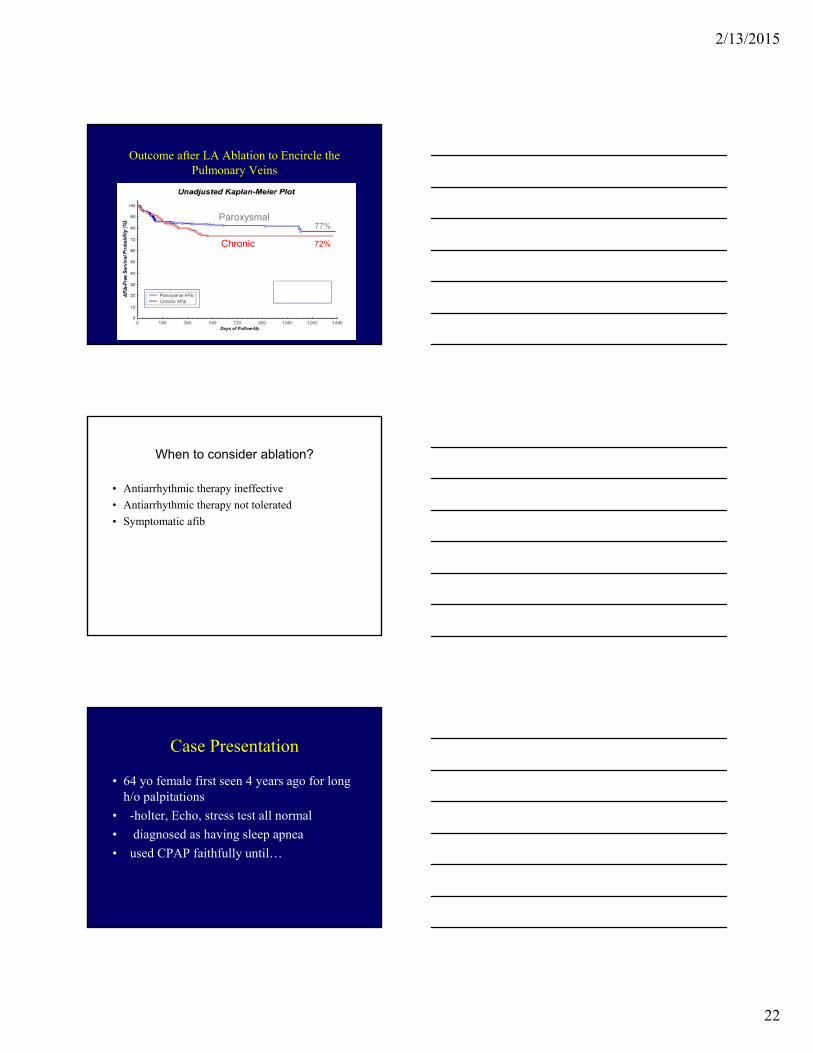
AP
CS
LSPV
Lasso Catheter Near Os of LSPV
2/13/2015
21
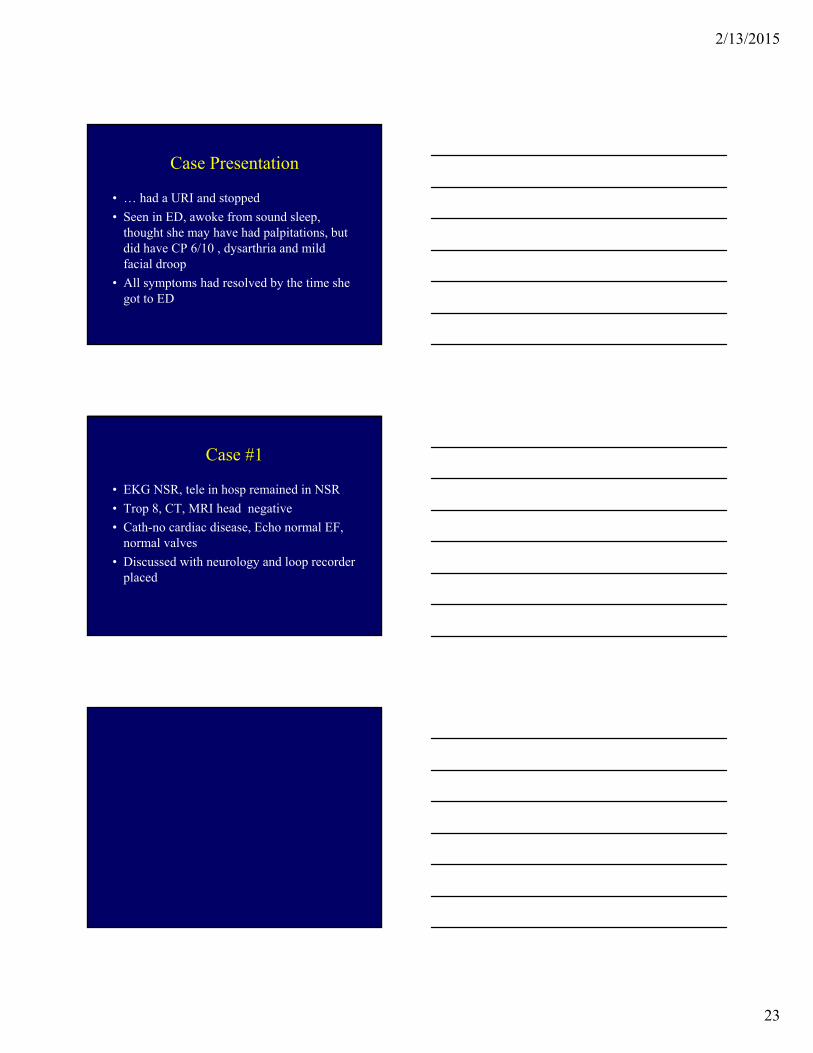
Anatomic Carto Map of Let atrium – ablation points
From: Dong et al.: Nature Clinical Practice Cardiovacular Medicine 2005, 2, 159-166
Left Atrial Ablation to Encircle the Pulmonary Veins
• 8 mm tip catheter
• 70 watts, 55°C
• Left & right PV’s encircled
• Mitral isthmus
• Line in posterior LA
2/13/2015
22
Outcome after LA Ablation to Encircle the Pulmonary Veins
72%
77%Paroxysmal
Chronic
When to consider ablation?
• Antiarrhythmic therapy ineffective
• Antiarrhythmic therapy not tolerated
• Symptomatic afib
Case Presentation
• 64 yo female first seen 4 years ago for long h/o palpitations
• -holter, Echo, stress test all normal
• diagnosed as having sleep apnea
• used CPAP faithfully until…
2/13/2015
23
Case Presentation
• … had a URI and stopped
• Seen in ED, awoke from sound sleep, thought she may have had palpitations, but did have CP 6/10 , dysarthria and mild facial droop
• All symptoms had resolved by the time she got to ED
Case #1
• EKG NSR, tele in hosp remained in NSR
• Trop 8, CT, MRI head negative
• Cath-no cardiac disease, Echo normal EF, normal valves
• Discussed with neurology and loop recorder placed

2/13/2015
24
Case Presentation #2
• 62 yo male, no cardiac history, only history is BPH on Flomax
• Retiring as chief of police, small city outside Philadelphia, got his PHD, teaching small college upstate NY, going for a routine physical for D1 baseball umpire
2/13/2015
25
Case Presentation #2
• What would you do?
• Aspirin started
Case Presentation #2
• What did we do?
• Started Xarelto
• Scheduled Echo, stress test, scheduled TEE, CV
• Told him he may eventually need a pacemaker

2/13/2015
26
Case Presentation #2
• TEE
• since hadn’t been on anti-coagulation, even though low risk, R/O thrombus
• Xarelto
• after Cardioversion, atria are “stunned” may not contract, raises risk for thrombus formation
• If no recurrent AF after 4 weeks change to ASA
2/13/2015
27
2/13/2015
28





![Dysrhythmias (002) [Read-Only] - Aventri · Atrial AV node Ventricular Classification of Rhythm Abnormalities Supraventricular Atrial origin Atrial fibrillation Atrial flutter Atrial](https://static.fdocuments.us/doc/165x107/5f024baa7e708231d4038f22/dysrhythmias-002-read-only-aventri-atrial-av-node-ventricular-classification.jpg)