
Going beyond Meaningful Use with GE...
12
GE Healthcare Going beyond Meaningful Use with GE Healthcare 0 1 1 0 1 0 1 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 1 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 1 0 1 0 1 0 1 1 0 1 1 1 0 0 1 1 0 1 0 0 1 0 1 0 1 0 0 1 0 1 0 1 0 1 1 0 1 0 0 1 0 1 01 0 1 0 0 0 1 0 1 0 0 1 0 1 0 1 0 1 0 1 1 0 0 1 1 0 1 0 0 1 0 1 1 0 0 1 1 0 1 0 1 1 0 1 0 1 0 1 0 1 0 1 0 1 0 1 1 0 0 0 1 0 0 1 0 1 1 0 1 0 1 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 1 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 1 0 1 0 1 0 1 1 0 1 1 1 0 0 1 1 0 1 0 0 1 0 1 0 1 0 0 1 0 1 0 1 0 1 1 0 1 0 0 1 0 1 0 1
-
Upload
vuongkhanh -
Category
Documents
-
view
220 -
download
0
Transcript of Going beyond Meaningful Use with GE...

GE Healthcare
Going beyond Meaningful Use with GE Healthcare
1 0 1 1 0 1 0 1 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 1 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 1 0 1 0 1 0 1 1 0 1 1 1 0 0 1 1 0 1 0 0 1 0 1 0 1 0 0 1 0 1 0 1 0 1 1 0 1 0 01 0
1 01 0
1 00 0
1 01 0
0 10 1
0 10 1
0 11 0
0 11 0
1 00 1
0 11001101011010101010101011000100100001
1 0 1 1 0 1 0 1 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 11 0
1 01 0
1 10 1
0 10 1
0 10 1
1 01 0
1 01 0
1 01 0
1011011100110100101010010101011010010101

2
Today, the U.S. leads the world in pharmaceutical and medical device innovation. At the beginning of the 21st century, analysis showed that “many important medical innovations in the past 30 years arguably originated in the United States.”1 Since 1975, American researchers have collected more Nobel Prizes in medicine or physiology than researchers in all other countries combined.1,2
Innovation in healthcare goods and services has improved the quality of life and life expectancy for Americans. Life expectancy increased from 68.2 years in 1950 to 77.2 years in 20011, and medical advances have improved quality of life in terms of mobility, sight, and hearing. But some would argue Americans spend too much for healthcare relative to other countries. The U.S. expends a higher fraction of Gross Domestic Product on healthcare than any other industrialized country, but health outcomes such as longevity and infant mortality are not markedly different than in other advanced economies that spend substantially less. For all of our innovation, Americans receive only 55% of recommended care.3
Deployment of evidence-based medicine guidelines to caregivers will, it is broadly believed, drive superior outcomes. But the lag between innovation and accepted practice is long, taking on average, 17 years for clinical trial results to become a standard of care in the clinical arena.4,5 The current fragmented, paper-based U.S. healthcare delivery model inhibits knowledge transfer and the spread of best practices at the point of care; complicates effective continuity of care, especially around care transitions; and exacerbates redundancy and ineffi ciency.
The widespread adoption of electronic medical records (EMRs) is an essential element of enhanced healthcare delivery. But this is only a start. Even in communities with strong EMR adoption, many providers still cannot share data meaningfully. They may be digitized, but they are still “siloized.”
1. Council of Economic Advisors. Economic Report of the President. Report H. Doc. 108-145. Washington: United States Government Printing Offi ce, 2004. (accessed September 8, 2010).
2. Fuchs, Victor , Sox, Harold. “Physicians’ Views of the Relative Importance of Thirty Medical Innovations”, Health Affairs: Volume 20, Number 5; 30-42.
3. McGlynn et al. “The Quality of Health Care Delivered to Adults in the United States”, NEJM 2003; 348:2635-45.
4. Porter, Michael E, and Elizabeth Olmsted Teisberg. Redefi ning Health Care: Creating Value-Based Competition on Results. Boston: Harvard Business School Press, 2006. Page 27.
5. Balas, E.A., Boren, S.A. “Managing Clinical Knowledge for Health Care Improvement,” Yearbook of Medical Informatics 2000; 65-70.
6. The National Ambulatory Medical Care Survey.
Electronic Medical Records: A foundation for improved healthcare delivery and outcomes
3
Adoption of Electronic Medical Records
Research shows that only a minority of providers has adopted full EMR functionality. According to a 2009 study by the National Center for Healthcare Statistics,6 20.5% of U.S. clinicians reported that they have basic functionality, defi ned by use of patient demographic information, patient problem lists, clinical notes, prescription ordering, laboratory, and imaging results. A much lower percentage of users, 6.3%, reported using electronic systems with comprehensive capabilities, which include basic functionality plus medical history and follow-up, warnings of drug interactions or contraindications, and evidence-based medicine.
EMR adoption is an important component of a truly interoperable health information ecosystem that enables the delivery of value-added information to providers, at the right place and time. The two other critical components are personal health records and health information exchange. This health information ecosystem will empower patients to become better consumers of healthcare products and services, while encouraging providers to raise performance expectations.
The HITECH Act
The American Recovery and Reinvestment Act of 2009 (or ARRA), commonly known as the “Economic Stimulus Package,” is a comprehensive package for economic recovery in the United States. On February 17, 2009, President Barack Obama signed the fi nal package of $787 billion into law. The HITECH Act refers to the $30+ billion set aside in this package for Health IT infrastructure and EHR adoption.
The ARRA HITECH Act specifi es incentive payments for hospitals, clinicians, and other eligible healthcare professionals. The incentive programs require that the provider demonstrate “Meaningful Use” of a certifi ed EHR product. The Offi ce of the National Coordinator (ONC) for Healthcare IT (HIT) is responsible for Standards and Certifi cation; it defi nes the criteria by which EHR technology will be certifi ed and whom will be accredited to certify such technology.

4
Financial incentives and eligibility for Meaningful Use
Through its Centers for Medicare and Medicaid Services (CMS), the Department of Health and Human Services will provide fi nancial incentives to Meaningful Users through either its Medicare or Medicaid programs. Unlike hospitals, eligible professionals (EPs) can only participate in one of these incentive programs, but not both. Medicaid eligible professionals with 30% of their volume attributable to Medicaid (20% for pediatricians) can receive up to $63,750 over a six-year period. Medicare incentive recipients can receive up to $44,000 over a fi ve-year period. For Meaningful Users whose fi rst payment year is 2011, Medicare incentive payments can be disbursed as early as May 2011 if all requirements are met (payments made in a lump sum). States will begin their Medicaid incentive programs on a rolling basis starting in 2011, subject to CMS approval of the state Medicaid HIT plans. It is likely that not all states will have Medicaid programs operational by the start of 2011.
For additional information and a list of frequently asked questions about eligibility and fi nancial incentives, go to: gehealthcare.com/meaningfuluse.
Program priorities and care goals
To receive incentives, EPs must demonstrate progress toward fi ve healthcare policy priorities and corresponding goals as outlined on the next page (see Table 2). They will do this by meeting specifi c Meaningful Use objectives and measures fl owing from these priorities and goals. A full list of Stage 1 Meaningful Use objectives and measures can be viewed at: http://www.cms.gov/EHRIncentivePrograms/Downloads/MU_Stage1_ReqSummary.pdf.
Financial Incentives
Table 2 delineates the Medicare fi nancial incentives for 2011 through 2015 to Eligible Professionals (EPs). Medicare eligible professionals can receive a maximum award of $44,000 dollars over a fi ve-year payment period. To maximize the award, the Medicare qualifying physicians will need to begin Meaningful Use reporting by 2011 or 2012. If the Medicare qualifying professional also practices in a Health Professional Shortage Area, they are eligible for an additional 10% incentive payment for each year that they qualify. Thus, eligible Medicare professionals
Medicare EP Medicaid EP
Doctor of Medicine or Doctor of Osteopathy Clinicians
Doctor of Dental Surgery or Dental Medicine Dentists
Doctor of Podiatric Medicine Nurse Practitioners
Doctor of Optometry Certifi ed Nurse-Midwives
Chiropractor Physician Assistants (working in a Federally Qualifi ed Health Center or rural health clinic that is also led by a Physician Assistant)
Table 1. Eligible professionals by program

5
Calendar yearFirst calendar year in which the
Eligible Professional receives an incentive payment
2011 2012 2013 2014 2015+
2011 $18,000
2012 $12,000 $18,000
2013 $8,000 $12,000 $15,000
2014 $4,000 $8,000 $12,000 $12,000
2015 $2,000 $4,000 $8,000 $8,000 $0
2016 $2,000 $4,000 $4,000 $0
Total $44,000 $44,000 $39,000 $24,000 $0
Health Professional Shortage Area
$48,400 (+10%)
$42,900(+10%)
$42,900(+10%)
$26,400(+10%) $0
Table 2. Medicare Incentive Payments
Adoption year
First calendar year in which the qualifyingEligible Professional receives an incentive payment
2011 2012 2013 2014 2015 2016
2011 $21,250
2012 $8,500 $21,250
2013 $8,500 $8,500 $21,250
2014 $8,500 $8,500 $8,500 $21,250
2015 $8,500 $8,500 $8,500 $8,500 $21,250
2016 $8,500 $8,500 $8,500 $8,500 $8,500 $21,250
2017 $8,500 $8,500 $8,500 $8,500 $8,500
2018 $8,500 $8,500 $8,500 $8,500
2019 $8,500 $8,500 $8,500
2020 $8,500 $8,500
2021 $8,500
Total $63,750 $63,750 $63,750 $63,750 $63,750 $63,750
Table 3. Medicaid Incentive Payments
in such shortage areas, whose fi rst incentive year is 2011 or 2012 and receives all fi ve payments, can receive $48,400. Eligible Professionals who begin their reporting in 2013 and 2014 can still qualify for incentives; however, the longer one waits to qualify, the less incentive funding is available. Medicaid Eligible Professionals can receive up to $63,750 over six payment periods. As long as the qualifying profes-sional receives the fi rst incentive payment by 2016, they will receive the maximum funding. The fi rst payments for the Medicare Incentive program are expected to be made in May of 2011 based on meaningful use for the fi rst three months of 2011. Payments for the Medicaid Incentive program are expected to be available during or after May 2011 depending on when a given state is ready to initiate the Medicaid EHR incentive program, which will be administered by the each state’s Medicaid Offi ce. States are expected to start on a rolling basis beginning January 2011.

6
Qualifying for Incentives
Eligible Professionals can participate in either the Medicare program or the Medicaid program. If an eligible professional qualifi es under both programs, they must select the program in which they want to participate. It is important to note that eligibility is determined on a per Eligible Professional basis, not at a practice level. For instance, if a there are four Eligible Professionals in a practice, all four Eligible Professionals can qualify for the stimulus funding, and meaningful use reporting requirements are based on the status of each Eligible Professional. In this scenario, it is possible that only two of the four physicians in the practice would elect to participate or meet the qualifying criteria. Table 3 highlights the criteria required for participating in the Medicare or Medicaid program, in addition to delineating the Meaningful Use reporting timeframes.
Under the Medicare incentive program, Eligible Professionals must bill under the Medicare Fee for Service program and have 90 days of consecutive Meaningful Use reporting in their fi rst year of the program, and a full year of Meaningful Use in each payment year beyond the fi rst.
Medicaid offers more fl exibility in achieving Meaningful Use. For providers with a minimum of 30% Medicaid volume (20% for pediatricians), the First Year incentive payment does not require Meaningful Use. Rather, the First Year Incentive payment will be available for Eligible Professionals who Adopt, Implement, or Upgrade an HHS certifi ed electronic health record (EHR). The guideline for Adopt, Implement or Upgrade is defi ned broadly to include purchase, installation or upgrade to a certifi ed EHR technology. There is no specifi ed waiting period or demonstration period for a Medicaid Eligible Professional to demonstrate that they have Adopted, Implemented or Upgraded. Thus, once a state receives approval to begin administering payments, qualifying Medicaid Eligible Professionals can submit the required reporting to the state for a payment. CMS has indicated that state incentive payments will start in May 2011. For many qualifying Medicaid providers, the fi rst Medicaid payment of $21,250 provides a signifi cant funding vehicle to support the purchase of a qualifi ed EHR. It is not until the second year of the incentive that providers must report on Meaningful Use for a period of 90 days. In the remaining incentive years, Medicaid Eligible Professionals must have a full year of MU report-ing to receive the incentives.

7
Meaningful Use Stages
First Payment Year 2011 2012 2013 2014 2015
2011 Stage 1 Stage 1 Stage 2 Stage 2 TBD
2012 Stage 1 Stage 1 Stage 2 TBD
2013 Stage 1 Stage 1 TBD
2014 Stage 1 TBD
2015+ TBD
Table 5. Meaningful Use stages
Table 4. Qualifying for Incentives
Qualifying for Incentive Programs
Medicare Medicaid
Bill Medicare fee for service and have allowed charges for covered professional services
Have a minimum of 30% Medicaid volume as measured by patient encounters (20% for Pediatricians)
Year 1: 90 consecutive days of MU
Year 2 and on: Full Year of MU
Year 1: (1) Acquire, purchase, or secure access to certifi ed EHR technology;2) Install or commence utilization of certifi ed EHR technology capable of meeting meaningful use requirements; or(3) Expand the available functionality of certifi ed EHR technology capable of meeting meaningful use requirements at the practice site, including staffi ng, maintenance, and training, or upgrade from existing EHR technology to certifi ed EHR technology per the ONC EHR certifi cation criteria.
Year 2: 90 consecutive days of MU
Year 3: Full Year of MU
Stages of Meaningful Use
The HITECH Act creates a gradual approach to achieving increasingly rigorous Meaningful Use, with three distinct stages, expected to be updated every two years. Stage I objectives and measures have been fully defi ned. Proposed rules for Stage II and Stage III criteria are targeted for completion by the end of 2011 and 2013 respectively with fi nalization during 2012 and 2014.
Each stage incorporates additional reporting and information exchange require-ments, and practices will have to adjust their workfl ows accordingly. The planned Meaningful Use progression is highlighted by Table 5.

8
Demonstrating Meaningful Use
CMS has devised two reporting sets of functional measures to demonstrate Meaningful Use: Core Set and Menu Set.
Core Set –All Required
The Core Set includes fi fteen objectives and corresponding measures. The majority of the measures require a calculation based on a numerator and a denominator, while a few require a Yes/No attestation.
15 Core Measures—All Apply
1. Use CPOE—at least one medication order for 30% unique patients
2. Implement drug-drug and drug-allergy interaction checks—Enabled 3. E-Prescribing—40% of all permissible prescriptions are transmitted 4. Record demographics—50% of all unique patients have in structured data 5. Maintain an up-to-date problem list—80% of all unique patients 6. Maintain active medication list—80% of all unique patients
7. Maintain active medication allergy list—80% of all unique patients 8. Record and chart changes in vital signs—50% of all unique patients over
the age of two 9. Record smoking status—50% of all unique patients over the age of 13 10. Implement one clinical decision support rule—One rule and track progress 11. Report 6 Clinical Quality Measures to CMS—Attest 2011, report 2012 12. Electronically exchange key clinical information—Perform one test 13. Provide electronic copy of their health information—50% requesting,
within three days 14. Provide clinical summaries for patients for each offi ce visit—50%, within
three days 15. Protect electronic health information for EHR—Perform risk analysis
Menu Set—Select Five
The Menu Set includes ten objectives and measures. EPs are required to report on fi ve measures of their choosing (one must include a population and public health measure). As with previous objectives, the corresponding Menu Set measures are reported with both “yes/no” attestations and numerators and denominators.
9
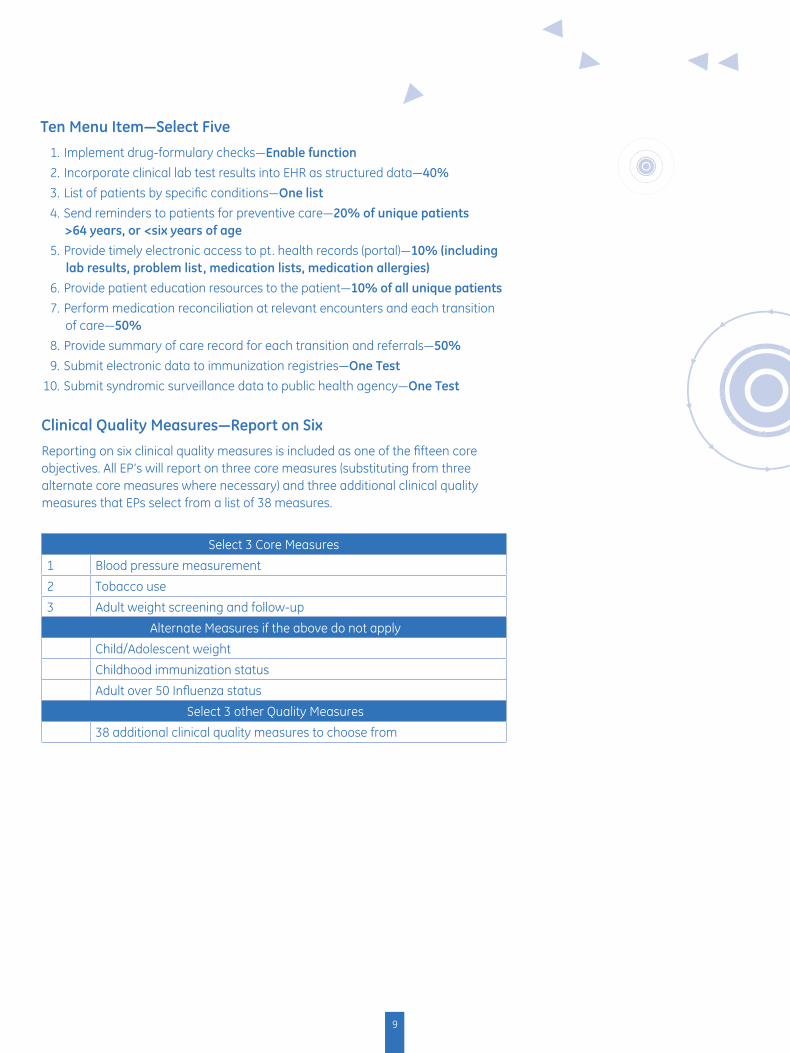
Ten Menu Item—Select Five
1. Implement drug-formulary checks—Enable function 2. Incorporate clinical lab test results into EHR as structured data—40%
3. List of patients by specifi c conditions—One list 4. Send reminders to patients for preventive care—20% of unique patients
>64 years, or <six years of age 5. Provide timely electronic access to pt. health records (portal)—10% (including
lab results, problem list, medication lists, medication allergies) 6. Provide patient education resources to the patient—10% of all unique patients 7. Perform medication reconciliation at relevant encounters and each transition
of care—50%
8. Provide summary of care record for each transition and referrals—50% 9. Submit electronic data to immunization registries—One Test 10. Submit syndromic surveillance data to public health agency—One Test
Clinical Quality Measures—Report on Six
Reporting on six clinical quality measures is included as one of the fi fteen core objectives. All EP’s will report on three core measures (substituting from three alternate core measures where necessary) and three additional clinical quality measures that EPs select from a list of 38 measures.
Select 3 Core Measures
1 Blood pressure measurement
2 Tobacco use
3 Adult weight screening and follow-up
Alternate Measures if the above do not apply
Child/Adolescent weight
Childhood immunization status
Adult over 50 Infl uenza status
Select 3 other Quality Measures
38 additional clinical quality measures to choose from
10
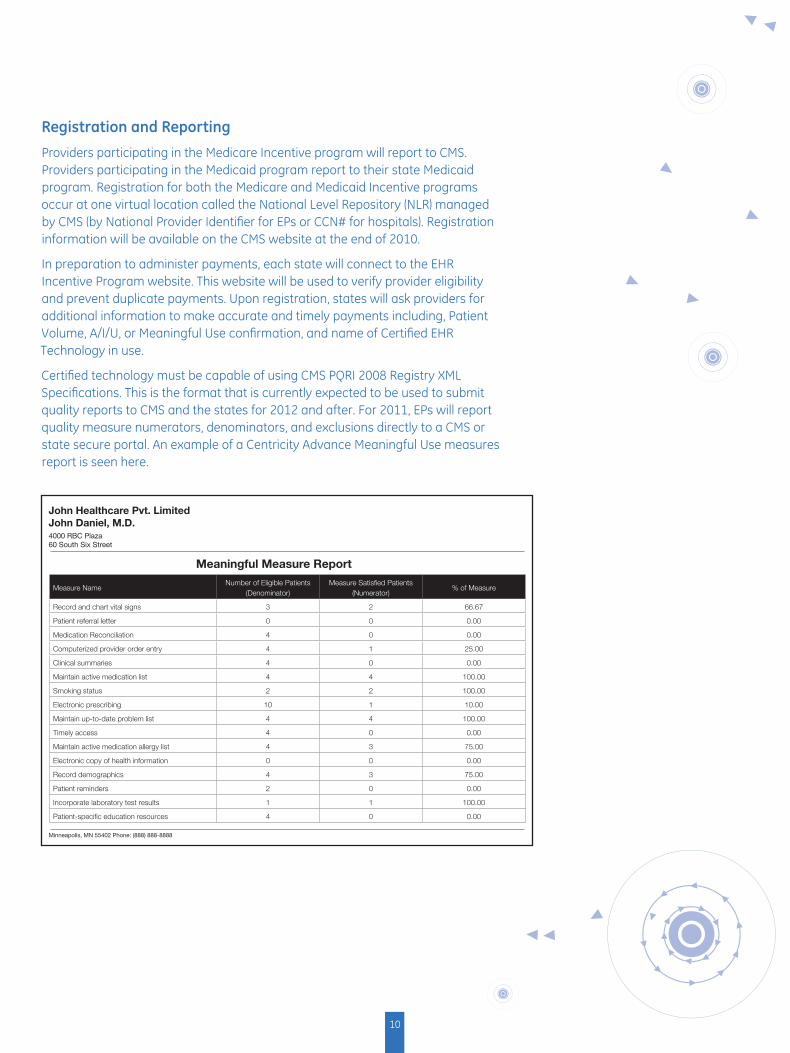
Registration and Reporting
Providers participating in the Medicare Incentive program will report to CMS. Providers participating in the Medicaid program report to their state Medicaid program. Registration for both the Medicare and Medicaid Incentive programs occur at one virtual location called the National Level Repository (NLR) managed by CMS (by National Provider Identifi er for EPs or CCN# for hospitals). Registration information will be available on the CMS website at the end of 2010.
In preparation to administer payments, each state will connect to the EHR Incentive Program website. This website will be used to verify provider eligibility and prevent duplicate payments. Upon registration, states will ask providers for additional information to make accurate and timely payments including, Patient Volume, A/I/U, or Meaningful Use confi rmation, and name of Certifi ed EHR Technology in use.
Certifi ed technology must be capable of using CMS PQRI 2008 Registry XML Specifi cations. This is the format that is currently expected to be used to submit quality reports to CMS and the states for 2012 and after. For 2011, EPs will report quality measure numerators, denominators, and exclusions directly to a CMS or state secure portal. An example of a Centricity Advance Meaningful Use measures report is seen here.
Measure NameNumber of Eligible Patients
(Denominator)Measure Satisfi ed Patients
(Numerator)% of Measure
Record and chart vital signs 3 2 66.67
Patient referral letter 0 0 0.00
Medication Reconciliation 4 0 0.00
Computerized provider order entry 4 1 25.00
Clinical summaries 4 0 0.00
Maintain active medication list 4 4 100.00
Smoking status 2 2 100.00
Electronic prescribing 10 1 10.00
Maintain up-to-date problem list 4 4 100.00
Timely access 4 0 0.00
Maintain active medication allergy list 4 3 75.00
Electronic copy of health information 0 0 0.00
Record demographics 4 3 75.00
Patient reminders 2 0 0.00
Incorporate laboratory test results 1 1 100.00
Patient-specifi c education resources 4 0 0.00
John Healthcare Pvt. LimitedJohn Daniel, M.D.4000 RBC Plaza60 South Six Street
Meaningful Measure Report
Minneapolis, MN 55402 Phone: (888) 888-8888

11
Meaningful Use Health Outcomes Policy Priorities
Meaningful use is structured around fi ve health outcomes policy priorities: care coordination; engage patients and families; improve quality, safety, effi ciency, and reduce health disparities; ensure privacy and security protections for personal health information; and improve population and public health. The diagram below highlights the fi ve health outcomes policies and some of the functionalities that certifi ed EHRs, such as Centricity Advance, possess to support Meaningful Use.
• Send Continuity of Care documet to other providers• Provide patients with clinical summaries for office visits• Perform medication reconciliationCare
Coordination
Engage Patientsand Families
Improve Qualityand Efficiency
Protect Privacy
Improve PublicHealth
• Provide patient portal access• Communicate results securely
• Perform ePrescribing with drug interaction checking• Monitor and report quality measures
• Track and monitor access to electronic health records• Use secure messaging for exchange of patient information
• Submit information to immunization registry• Recieve electronic laboratory results• Provide information to public health agencies
Centricity Advance Meets the Challenge
To achieve these priorities, communication and interoperability will occur across multiple points in the healthcare ecosystem. This requires electronic information exchange and improved communication about patient status and outcomes among providers, patients, and care facilities. As one of the fi rst products to be certifi ed by an Offi ce of the National Coordinator Authorized Testing and Certifi cation Body (ONC-ATCB), Centricity Advance provides the tools needed to accomplish these goals. Table 6 highlights Centricity Advance’s capabilities.

imagination at workITP-0192-09.10-EN-US
GE Healthcare 540 West Northwest Highway Barrington, IL 60010 U.S.A.
www.gehealthcare.com
©2011 General Electric Company – All rights reserved.
General Electric Company reserves the right to make changes in specifications and features shown herein, or discontinue the product or service described at any time, without notice or obligation. Contact your GE representative for the most current information.
GE, the GE Monogram, Centricity and imagination at work are trademarks of General Electric Company.
General Electric, by and through its GE Healthcare division.
For the most current CCHIT certification information for Centricity EMR and Centricity Practice Solution, visit www.cchit.org
Final thought
Transformation is an overused word, but is nonetheless what is required to reposition a healthcare system that is fundamentally focused more on what is delivered than what is achieved. Dr. Brandon Savage, Chief Medical Officer of GE Healthcare IT, comments on the sheer exasperation experienced by healthcare professionals that want more for patients: “Physicians with the healthcare delivery team want to do the right thing, but they are consistently challenged by a lack of process automation and decision support. As leaders in healthcare we need to redouble our efforts to provide an always-ready, easy-to-access array of tools to maximize insight and ease decision making. We must make these tools as commonplace in medicine as the stethoscope. With these we can spark a new age in medicine—the age of performance, the age of results.” With Centricity Advance from GE Healthcare, your practice can have the proficiency and tools needed to accomplish these goals.
Quality metrics and reporting
In 2011, reporting will be by attestation, and all customers will have access to Centricity Advance reporting tools that comply with the proposed reporting requirements. For 2012, CMS has proposed to require electronic submission from the EHR through the PQRI XML format, with which GE has extensive experience. GE plans to have the ability to submit electronically according to these guidelines.
ePrescribing The latest release of Centricity Advance includes sophisticated eRx at no additional monthly charge to meet all currently defined ARRA requirements for eRx.
Interfaces Centricity Advance supports the standards-based lab and immunization registry interfaces and will continue to remain compliant as standards evolve. GE Healthcare will work with customers to identify their specific connectivity needs.
Interoperability Centricity Advance uses standards-based interoperability approaches that rely on such standards as HL7 and CCD, and will continue to expand these capabilities to support evolving certification and Meaningful Use requirements.
Patient and family engagement
Customers have multiple options for sharing health information with patients. In addition to the ability to generate Continuity of Care Documents, GE Healthcare offers Internet-based Patient Portal and secure messaging email solutions as two options that can increase patient access and satisfaction while improving communication with staff and providers.
Computerized Physician Order Entry
Centricity Advance provides CPOE functionality for ease of order submission and tracking of test results.
Clinical decision support
Centricity Advance provides functionality for clinical decision support rules and can customize rules to meet any specialty.
Table 6.


















