Glutamate and capsaicin effects on trigeminal nociception II: Activation and central sensitization...
12
Research Report Glutamate and capsaicin effects on trigeminal nociception II: Activation and central sensitization in brainstem neurons with deep craniofacial afferent input David K. Lam, Barry J. Sessle, James W. Hu ⁎ Faculty of Dentistry, University of Toronto, 124 Edward Street, Toronto, Ontario, Canada M5G 1G6 ARTICLE INFO ABSTRACT Article history: Accepted 17 November 2008 Available online 28 November 2008 We examined the effect of the peripheral application of glutamate and capsaicin to the temporomandibular joint (TMJ) in influencing the activation and central sensitization of TMJ-responsive nociceptive neurons in the trigeminal subnucleus caudalis/upper cervical cord (Vc/UCC). The activity of single neurons activated by noxious mechanical stimulation of the TMJ was recorded in the Vc/UCC of 49 halothane-anesthetized male rats. Cutaneous mechanoreceptive field (RF), cutaneous mechanical activation threshold (MAT), and TMJ MAT of each neuron were assessed before and after injection of 0.5 M glutamate (or vehicle) and 1% capsaicin (or vehicle) into the TMJ. A total of 49 nociceptive neurons (37 nociceptive- specific, 12 wide-dynamic-range) that could be activated by blunt noxious mechanical stimulation of the TMJ were studied. When injected alone, glutamate and capsaicin activated and induced central sensitization (reflected in cutaneous RF expansion and cutaneous and/ or TMJ MAT reduction) in most Vc/UCC neurons. Following glutamate injection, capsaicin evoked greater activity and less cutaneous/TMJ MAT reduction compared with capsaicin alone, whereas capsaicin abolished all subsequent glutamate-evoked activity and depressed cutaneous RF expansion in most neurons. Glutamate effects on deep afferents and Vc/UCC neurons were analogous since glutamate sensitized afferent and neuronal responses to capsaicin but the desensitizing effects of capsaicin on glutamate-evoked excitability of Vc/ UCC neurons contrast with the lack of capsaicin-induced modulation of glutamate-evoked afferent excitability [Lam, D.K., Sessle, B.J., Hu, J.W., 2008a. Glutamate and capsaicin effects on trigeminal nociception I: activation and peripheral sensitization of deep craniofacial nociceptive afferents. Brain Res. doi:10.1016/j.brainres.2008.11.029], suggesting that peripheral and central sensitization may be differentially involved in the nociceptive effects of glutamate and capsaicin applied to deep craniofacial tissues. © 2008 Published by Elsevier B.V. Keywords: Excitatory amino acid TRPV1 Pain Temporomandibular joint 1. Introduction Peripheral excitatory amino acid (EAA) and vanilloid (TRPV1) receptor mechanisms may interact to modulate nociceptive processing of deep craniofacial tissues (Lam et al., 2005a,b, 2008a). In the companion paper (Lam et al., 2008a), we demonstrate that peripheral application of glutamate to deep craniofacial tissues can modulate activation and peripheral sensitization in BRAIN RESEARCH 1253 (2009) 48 – 59 ⁎ Corresponding author. Fax: +1 416 979 936. E-mail address: [email protected] (J.W. Hu). 0006-8993/$ – see front matter © 2008 Published by Elsevier B.V. doi:10.1016/j.brainres.2008.11.056 available at www.sciencedirect.com www.elsevier.com/locate/brainres
-
Upload
david-k-lam -
Category
Documents
-
view
220 -
download
0
Transcript of Glutamate and capsaicin effects on trigeminal nociception II: Activation and central sensitization...

B R A I N R E S E A R C H 1 2 5 3 ( 2 0 0 9 ) 4 8 – 5 9
ava i l ab l e a t www.sc i enced i rec t . com
www.e l sev i e r. com/ loca te /b ra in res
Research Report
Glutamate and capsaicin effects on trigeminal nociception II:Activation and central sensitization in brainstem neurons withdeep craniofacial afferent input
David K. Lam, Barry J. Sessle, James W. Hu⁎
Faculty of Dentistry, University of Toronto, 124 Edward Street, Toronto, Ontario, Canada M5G 1G6
A R T I C L E I N F O
⁎ Corresponding author. Fax: +1 416 979 936.E-mail address: [email protected] (J.W
0006-8993/$ – see front matter © 2008 Publisdoi:10.1016/j.brainres.2008.11.056
A B S T R A C T
Article history:Accepted 17 November 2008Available online 28 November 2008
We examined the effect of the peripheral application of glutamate and capsaicin to thetemporomandibular joint (TMJ) in influencing the activation and central sensitization ofTMJ-responsive nociceptive neurons in the trigeminal subnucleus caudalis/upper cervicalcord (Vc/UCC). The activity of single neurons activated by noxiousmechanical stimulation ofthe TMJ was recorded in the Vc/UCC of 49 halothane-anesthetized male rats. Cutaneousmechanoreceptive field (RF), cutaneous mechanical activation threshold (MAT), and TMJMAT of each neuron were assessed before and after injection of 0.5 M glutamate (or vehicle)and 1% capsaicin (or vehicle) into the TMJ. A total of 49 nociceptive neurons (37 nociceptive-specific, 12 wide-dynamic-range) that could be activated by blunt noxious mechanicalstimulation of theTMJwere studied.When injected alone, glutamate and capsaicin activatedand induced central sensitization (reflected in cutaneous RF expansion and cutaneous and/or TMJ MAT reduction) in most Vc/UCC neurons. Following glutamate injection, capsaicinevoked greater activity and less cutaneous/TMJ MAT reduction compared with capsaicinalone, whereas capsaicin abolished all subsequent glutamate-evoked activity and depressedcutaneous RF expansion in most neurons. Glutamate effects on deep afferents and Vc/UCCneurons were analogous since glutamate sensitized afferent and neuronal responses tocapsaicin but the desensitizing effects of capsaicin on glutamate-evoked excitability of Vc/UCC neurons contrast with the lack of capsaicin-induced modulation of glutamate-evokedafferent excitability [Lam, D.K., Sessle, B.J., Hu, J.W., 2008a. Glutamate and capsaicin effectson trigeminal nociception I: activation and peripheral sensitization of deep craniofacialnociceptive afferents. Brain Res. doi:10.1016/j.brainres.2008.11.029], suggesting thatperipheral and central sensitization may be differentially involved in the nociceptiveeffects of glutamate and capsaicin applied to deep craniofacial tissues.
© 2008 Published by Elsevier B.V.
Keywords:Excitatory amino acidTRPV1PainTemporomandibular joint
1. Introduction
Peripheral excitatory amino acid (EAA) and vanilloid (TRPV1)receptor mechanisms may interact to modulate nociceptive
. Hu).
hed by Elsevier B.V.
processingofdeepcraniofacial tissues (Lametal., 2005a,b, 2008a).In the companion paper (Lam et al., 2008a), we demonstrate thatperipheral application of glutamate to deep craniofacial tissuescan modulate activation and peripheral sensitization in

49B R A I N R E S E A R C H 1 2 5 3 ( 2 0 0 9 ) 4 8 – 5 9
trigeminal nociceptive primary afferents. However, previousstudies have also suggested a role for central sensitization inmediating glutamate-evoked pain in craniofacial tissues.Glutamate injection into the rat jaw muscle or temporoman-dibular joint (TMJ) also evokes reflex increases in jaw muscleactivity that can be antagonized by centrally administered EAAreceptor antagonists (Cairns et al. 2001a). Furthermore, gluta-mate injection into the humanneck (Ge et al., 2005; Svensson etal., 2005) or jaw (Cairns et al., 2001b, 2003a,b, 2006; Svensson etal., 2003, 2005) muscles causes referred as well as local pain.
The vanilloid type 1 receptor, TRPV1, is another peripheralreceptor involved in craniofacial nociceptive mechanisms. Inthe companion paper (Lam et al., 2008a), peripheral applica-tion of capsaicin to deep craniofacial tissues was shown tomodulate activation and peripheral sensitization in trigeminalnociceptive primary afferents. However, central sensitizationmechanisms may also be involved in mediating capsaicin-evoked pain in craniofacial tissues. Peripheral application ofcapsaicin to craniofacial tissues reflexly evokes a dose-dependent increase in jaw muscle activity (Tang et al., 2004;Lam et al., 2005a) and activates brainstemnociceptive neurons(Carstens et al., 1998; Zanotto et al., 2007) and studies inhumans have shown that injection of capsaicin into cranio-facial regions can induce secondary hyperalgesia as well asallodynia and jawmuscle pain associated with changes in jawmotor function (Sohn et al., 2000, 2004; Wang et al., 2002;Gazerani and Arendt-Nielsen 2005; Gazerani et al., 2006).
Although peripheral glutamate and capsaicin receptormechanisms may interact to modulate deep craniofacialafferent nociceptive responses (Lam et al., 2008a), there is noknowledge of how these peripheral effects might influencecentral neurons involved in processing of deep nociceptiveinformation such as those found in the trigeminal subnucleuscaudalis/upper cervical spinal cord (Vc/UCC) an important sitefor processing of nociceptive afferent inputs from TMJ andother deep craniofacial tissues (for review, see Bereiter et al.,
Fig. 1 – The unit recording sites reconstructed from histology we1997). Coronal sections at 3 different rostrocaudal levels of the V(WDR) neurons; opened symbols nociceptive-specific (NS) neuroinjection followed by capsaicin injection and capsaicin injectionlabels 2(a), 2(b), and 3 represent the NS neurons shown in Figs. 2
2000; Sessle 2005; Hu et al., 2005). Therefore, the aim of thepresent study was to examine the effects of the peripheralapplication of glutamate and capsaicin to theTMJ in influencingthe activation and central sensitization of TMJ-responsivenociceptive neurons in the Vc/UCC. A portion of this data hasbeen previously presented in abstract form (Lam et al., 2003).
2. Results
2.1. Neuronal properties
The properties of 49 nociceptive neurons (37 nociceptive-specific (NS), 12 wide dynamic range (WDR)) that responded tonoxious mechanical stimulation of the TMJ region and thatwere recorded primarily in the deep laminae (III–V) of the Vc/UCC region were studied (Fig. 1). Examples of typical neuronalmechanoreceptive field (RF) and response propertiesare shown in Figs. 2 and 3 and their histologically con-firmed recording sites are shown in Fig. 1. Less than 5% (2/49,1 NS, 1WDR) of these neuronswere spontaneously active (0.22±0.15 spikes/second) prior to injection of receptor agonists. All37 NS neurons and 12WDR neurons had at baseline (i.e. beforeagonist injection) an ipsilateral cutaneous RF involving theskin overlying the TMJ and extending into the maxillary andmandibular divisions aswell as an ipsilateral deepRF involvingthe TMJ region. There were no differences in baselinespontaneous activity, laminae location (i.e. superficial vs.deep), or responses to glutamate and capsaicin (i.e. responsemagnitude (Rmag), response duration (Rdur), response latency(Rlat) and peak frequency (Pfreq); cutaneous RF expansion andcutaneous/TMJ MAT reduction) between the WDR and NSneurons (pN0.05, Mann–Whitney U test; pN0.05, Fisher's exacttest) (data not shown); thus, the data from NS and WDRneurons were pooled together for analysis of glutamate andcapsaicin-induced activation and sensitization.
re plotted on diagrams of the brainstem (Paxinos andWatsonc/UCC region. Filled symbols represent wide dynamic rangens. The dot and triangle symbols represent the glutamatefollowed by glutamate injection subgroups, respectively. Thea, b and 3, respectively.

Fig. 2 – Examples of typical cutaneous mechanoreceptive field (RF) and response properties of NS TMJ-responsive nociceptiveneurons in the Vc/UCC region. (a) Cutaneous RF of a NS neuron involving the TMJ region and its lack of neuronal responsefollowing injection of glutamate vehicle into the TMJ as well as its neuronal response evoked by injection of capsaicin followingglutamate vehicle into the TMJ. Note: histologically confirmed lesioned NS neuronal recording site is shown in Fig. 1. (b)Cutaneous RF of a NS neuron involving the TMJ region and neuronal response evoked by injection of glutamate into the TMJ aswell as its enhanced neuronal response evoked by injection of capsaicin following glutamate into the TMJ. Note: histologicallyconfirmed lesioned NS neuronal recording site is shown in Fig. 1.
50 B R A I N R E S E A R C H 1 2 5 3 ( 2 0 0 9 ) 4 8 – 5 9
2.2. Glutamate effects
2.2.1. ActivationInjection of glutamate alone (but not vehicle alone, 0/5) acti-vated 86% (12/14) of the neurons tested (p<0.001, Fisher exacttest), with the activation response properties outlined inTable 1. Glutamate-evoked neuronal activation began approx-imately 5 s from injection (Rlat=4.3 [2.6] s) and lasted about2 min (Rdur=98.6 [49.1] s).
Similarities and differences in response properties ofVc/UCC neurons and afferents (Lam et al., 2008a) to glutamateand capsaicin injection are summarized in Table 2.
2.2.2. MAT reductionThe post-incision cutaneous MAT values remained un-changed from baseline and remained stable prior to glutamate(or vehicle) injection (pN0.05, RM ANOVA-on-ranks) (Lam etal., 2008b). The spontaneous neuronal activity returned tobaseline level prior to determination of MAT post-injection ofglutamate in all 14 neurons tested. Injection of glutamatealone (but not vehicle alone, 0/5) induced TMJ MAT reduction(≥50% threshold reduction from baseline MAT score) in 57%(8/14) and cutaneous MAT reduction in 64% (9/14) of theneurons tested (p<0.05, Fisher exact test) at 10–20 min post-injection. However, for the neuronal population as whole, thebaseline median TMJ and cutaneous MAT values were 67.9[56.1] grams (g) and 63.0 [53.0] g, respectively, and injection of
glutamate alone (or vehicle alone, n=5) produced a non-significant reduction in TMJ (41.8 [33.6] g) and cutaneous (56.7[48.1] g) MAT values at 10–20 min post-injection relative totheir pre-injection baseline (pN0.05, RM ANOVA-on-ranks)(Fig. 4). Some neurons activated by glutamate injection alonedid not show cutaneous [33% (4/12)] or TMJ [42% (5/12)] MATreduction, and the two neurons not activated by glutamateinjection alone also did not display cutaneous or TMJ MATreduction.
2.2.3. Cutaneous RF expansionThe post-incision cutaneous RF size remained unchangedfrom baseline and remained stable prior to glutamate (orvehicle) injection (pN0.05, Fisher exact test) (Lam et al., 2008b).Injection of glutamate alone (but not vehicle alone, 0/5)induced cutaneous RF expansion at 10–20 min post-injectionin 93% (13/14) of the neurons tested (p<0.05, Fisher exact test).All 12 neurons activated by glutamate injection alone showedcutaneous RF expansion, whereas there was no cutaneous RFexpansion following glutamate injection alone in one neuronthat showed no prior activation by glutamate.
2.3. Capsaicin effects
2.3.1. ActivationInjection of capsaicin alone (but not vehicle alone, 0/5) acti-vated 88% (14/16) of the neurons tested (p<0.001, Fisher exact

Fig. 3 – Example of capsaicin and glutamate-induced central sensitization in a NS TMJ-responsive nociceptive neuron in theVc/UCC region. (a) Neuronal activity at baseline and responses evoked by injection of capsaicin and glutamate into the TMJ, (b)Cutaneous mechanoreceptive field (RF) of NS neuron at baseline and following injection of capsaicin and glutamate into theTMJ, (c) Cutaneous mechanical activation threshold (MAT) of NS neuron at baseline and following injection of capsaicin andglutamate into the TMJ. Note: histologically confirmed lesioned NS neuronal recording site is shown in Fig. 1.
51B R A I N R E S E A R C H 1 2 5 3 ( 2 0 0 9 ) 4 8 – 5 9
test), with the activation response properties outlined in Table1. Capsaicin-evoked neuronal activation began approximately20 s from injection (Rlat=16.4 [10.5] s) and lasted about 2–3min(Rdur=112 [201] s). The incidence of Vc/UCC neuronal activa-tion (pN0.05, Fisher exact test) and response properties (Rmag,Rlat, Rdur and Pfreq) (pN0.05, Mann–Whitney U test) inducedby injection of capsaicin alone was similar to that induced byglutamate alone (Table 1).
2.3.2. MAT reductionThe post-incision cutaneous MAT values remained unchangedfrom baseline and remained stable prior to capsaicin (orvehicle) injection (pN0.05, RM ANOVA-on-ranks) (Lam et al.,2008b). The spontaneous neuronal activity returned to baselinelevel prior to determination of MAT post-injection of capsaicinin all 16 neurons tested. Injection of capsaicin alone (but notvehicle alone, 0/5) induced TMJMAT reduction (≥50% thresholdreduction from baseline MAT score) in 63% (10/16) andcutaneous MAT reduction in 56% (9/16) of the neurons tested
(p<0.05, Fisher exact test) at 10–20 min post-injection. Simi-larly, for the neuronal population as a whole, the baselinemedian TMJ and cutaneous MAT values were 80.5 [63.1] g and74.6 [56.9] g, respectively, and capsaicin alone (but not vehiclealone, n=5) injected into the TMJ produced a significantreduction in TMJ (38.6 [18.1] g; p<0.01) and cutaneous (33.6[14.8] g; p<0.05) MAT values relative to their pre-injectionbaseline (RM ANOVA-on-ranks, Dunn's method) at 10–20 minpost-injection (Fig. 4). However, some neurons activated bycapsaicin injection alone did not show cutaneous [36% (5/14)]or TMJ [36% (5/14)] MAT reduction, whereas the two neuronsnot activated by capsaicin injection alone displayed bothcutaneous and TMJ MAT reduction (pN0.05, Fisher exact test).
There was no significant difference between the incidenceof reductions in TMJ MAT and cutaneous MAT induced byinjection of capsaicin alone compared to those induced byglutamate alone (pN0.05, Fisher exact test).
An example of a neuron manifesting capsaicin-induced RFexpansion and MAT reduction is shown in Fig. 3.

Table 1 – Properties of responses of TMJ-responsive Vc/UCC nociceptive neurons to injection of glutamate (or vehicle) andcapsaicin (or vehicle) into the TMJ (⁎⁎⁎p<0.001, glutamate vehicle vs. glutamate alone or glutamate alone vs. glutamatepost-capsaicin or capsaicin vehicle post-glutamate vs. capsaicin post-Glutamate; †††p<0.001, capsaicin vehicle vs. capsaicinalone or glutamate vehicle post-capsaicin vs. glutamate post-capsaicin;‡p<0.05, capsaicin alone vs. capsaicinpost-glutamate; Mann–Whitney U test)
Glutamate CapsaicinMedian [Interquartile range]
Capsaicin Glutamate medianMedian [Interquartile range]
Responseproperty
Glutamatealone (n=14)
Capsaicinpost-Glutamate
(n=13)
Capsaicin alone(n=16)
Glutamatepost-Capsaicin
(n=10)
Rmag (spikes) 833 [1186] 2915 [4079]‡ 161 [942] 0⁎⁎⁎Rlat (s) 4.3 [2.6] 5.3 [2.5]‡ 16.4 [10.5] 0⁎⁎⁎Rdur (s) 98.6 [49.1] 377 [283]‡ 112 [201] 0⁎⁎⁎Pfreq (Hz) 31.7 [39.2] 45.1 [43.7]‡ 16.6 [35.6] 0⁎⁎⁎
Responseproperty
Glutamatevehicle (n=5)
Capsaicinpost-Glutamatevehicle (n=5)
Capsaicinvehicle (n=5)
Glutamatepost-Capsaicinvehicle (n=5)
Rmag (spikes) 0⁎⁎⁎ 131 [718] 0††† 643 [1396]Rlat (s) 0⁎⁎⁎ 15.1 [14.4] 0††† 4.3 [2.6]Rdur (s) 0⁎⁎⁎ 111 [153] 0††† 108 [50.6]Pfreq (Hz) 0⁎⁎⁎ 13.3 [29.8] 0††† 33.5 [41]
Responseproperty
Glutamatealone (n=5)
Capsaicin vehiclepost-Glutamate
(n=5)
Capsaicinalone (n=4)
Glutamate vehiclepost-Capsaicin
(n=4)
Rmag (spikes) 472 [1253] 0⁎⁎⁎ 131 [718] 0†††
Rlat (s) 3.6 [4.7] 0⁎⁎⁎ 15.1 [14.4] 0†††
Rdur (s) 126 [103] 0⁎⁎⁎ 111 [153] 0†††
Pfreq (Hz) 21.7 [46.9] 0⁎⁎⁎ 13.3 [29.8] 0†††
52 B R A I N R E S E A R C H 1 2 5 3 ( 2 0 0 9 ) 4 8 – 5 9
2.3.3. Cutaneous RF expansionThe post-incision cutaneous RF size remained unchangedfrom baseline and remained stable prior to capsaicin (orvehicle) injection (pN0.05, Fisher exact test) (Lam et al., 2008b).Injection of capsaicin alone (but not vehicle alone, 0/5)induced cutaneous RF expansion at 10–20 min post-injection
Table 2 – Comparison of response properties of WDR and NScraniofacial nociceptive afferents (Lam et al., 2008a) to injection
Glutamate Capsaicin
Responseproperty
Glutamate alone Capsaicin posGlutamate
Afferent Vc/UCC Afferent Vc
Activation + ++‡ ++† +Deep MAT + + +†† +Cutaneous MAT N/A + N/A +Cutaneous RF N/A + N/A +
In general, both glutamate and capsaicin-evoked responses were greateincidence, Rmag or Rdur).+ Sensitized— increased excitability (↑Rmag, ↑Pfreq, ↑Rdur, ↓Rlat or ↓MAT- Desensitized— decreased excitability (↓Rmag, ↓Pfreq, ↓Rdur, ↑Rlat or ↑MN/A: Not applicable.† increased excitability compared to capsaicin alone.†† decreased excitability compared to glutamate/capsaicin alone.‡ increased excitability compared to afferents tested.‡‡ glutamate-evoked activity abolished.
in 63% (10/16) of the neurons tested (p<0.05, Fisher exact test).However, some neurons activated by capsaicin [36% (5/14)]injection alone did not show cutaneous RF expansion,whereas one neuron displaying cutaneous RF expansionfollowing capsaicin injection alone showed no prior activationby capsaicin.
TMJ-responsive Vc/UCC nociceptive neurons and of deepof glutamate and/or capsaicin into deep craniofacial tissues
Capsaicin Glutamate
t- Capsaicin alone Glutamate post-Capsaicin
/UCC Afferent Vc/UCC Afferent Vc/UCC
++†‡ + ++‡ + −‡‡
†† + + + −N/A + N/A +N/A + N/A +††
r in Vc/UCC neurons COMPARED to afferents (i.e. increased activation
).AT).

Fig. 4 – The time courses of glutamate (GLU) and capsaicin (CAP)-induced cutaneous mechanical activation threshold (MAT)and TMJ MAT reduction in Vc/UCC nociceptive neurons. Arrow indicates time point for injection of GLU (black) and CAP(grey) into the TMJ. Circles indicate median normalized cutaneous MAT (black) and TMJ MAT (white) following injection ofGLU and CAP. Triangles indicate GLU or CAP-induced median normalized cutaneous MAT and TMJ MAT before or afterinjection of vehicle controls for GLU or CAP. Raw MAT threshold values were normalized to the initial baseline pre-injectionvalue of the first agonist. Lines: interquartile range. Note that injection of CAP following GLU vehicle control or CAP aloneinto the TMJ significantly reduced both the (a, c) cutaneous (⁎p<0.05) and (b, d) TMJ MAT (⁎⁎p<0.01); whereas injection of (a)CAP following GLU, or (c) GLU following CAP significantly reduced the cutaneous MAT (⁎p<0.05; RM ANOVA-on-ranks,Dunn's method).
53B R A I N R E S E A R C H 1 2 5 3 ( 2 0 0 9 ) 4 8 – 5 9
The incidence of cutaneous RF expansion induced byinjection of capsaicin alone was similar to the incidence ofcutaneous RF expansion induced by glutamate alone (pN0.05,Fisher exact test).
2.4. Glutamate and capsaicin interactions
2.4.1. ActivationThere were only two types of agonist-responsive Vc/UCCneurons found in the glutamate followed by capsaicin sub-group, as summarized in Fig. 5: (1) glutamate-sensitive andcapsaicin-sensitive [92% (12/13)] and (2) glutamate-insensi-tive and capsaicin-sensitive [8% (1/13)]. Following glutamateinjection, capsaicin (but not vehicle, 0/5) evoked responses
in all 13 neurons tested and neuronal activation occurredapproximately 5–6 s from injection (Rlat=5.3 [2.5] s) andlasted about 6–7 min (Rdur=377 [283] s). Moreover, followingglutamate injection, capsaicin produced significantlygreater (2–18 fold) increases in Rmag, Pfreq, and Rdur anda decrease in Rlat compared with capsaicin alone (p<0.05,Mann–Whitney U tests) (Table 1). There were also only twotypes of agonist-responsive Vc/UCC neurons found in thecapsaicin followed by glutamate subgroup (see Fig. 5): (1)capsaicin-sensitive and glutamate-insensitive [90% (9/10)]and (2) capsaicin-insensitive and glutamate-insensitive[10% (1/10)]. Injection of glutamate following capsaicinfailed to evoke any activity in the Vc/UCC neurons [0% (0/10)] tested (Table 1).
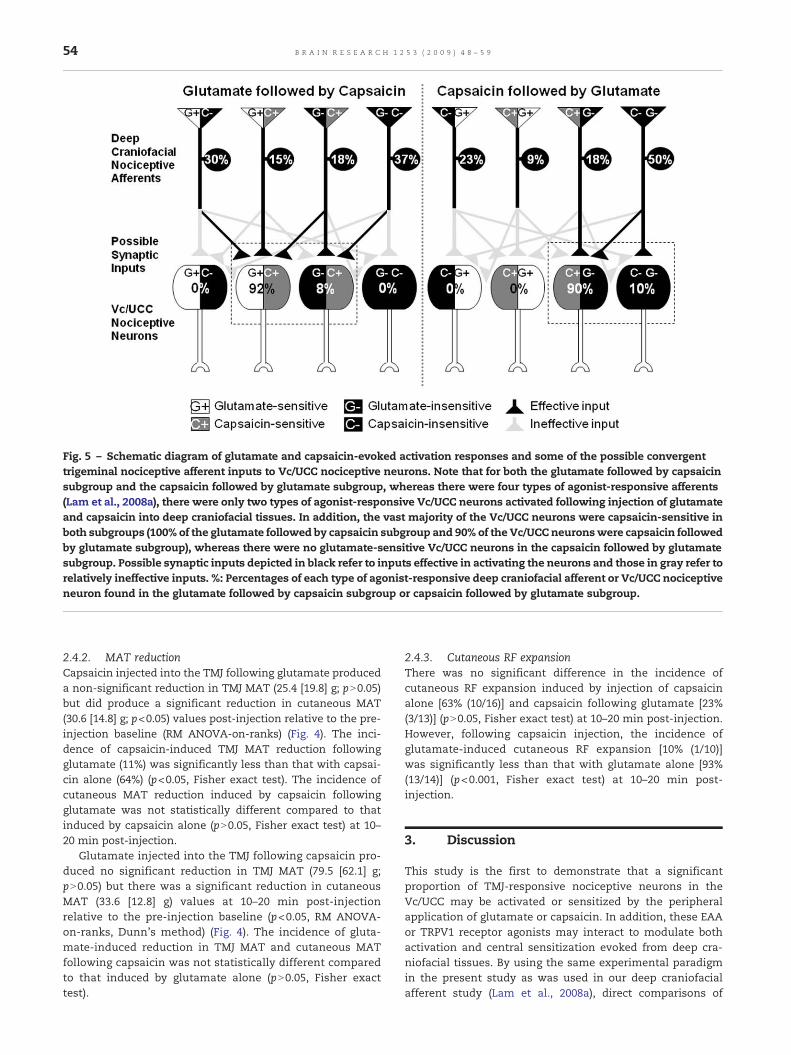
Fig. 5 – Schematic diagram of glutamate and capsaicin-evoked activation responses and some of the possible convergenttrigeminal nociceptive afferent inputs to Vc/UCC nociceptive neurons. Note that for both the glutamate followed by capsaicinsubgroup and the capsaicin followed by glutamate subgroup, whereas there were four types of agonist-responsive afferents(Lam et al., 2008a), there were only two types of agonist-responsive Vc/UCC neurons activated following injection of glutamateand capsaicin into deep craniofacial tissues. In addition, the vast majority of the Vc/UCC neurons were capsaicin-sensitive inboth subgroups (100% of the glutamate followed by capsaicin subgroup and 90% of the Vc/UCC neuronswere capsaicin followedby glutamate subgroup), whereas there were no glutamate-sensitive Vc/UCC neurons in the capsaicin followed by glutamatesubgroup. Possible synaptic inputs depicted in black refer to inputs effective in activating the neurons and those in gray refer torelatively ineffective inputs. %: Percentages of each type of agonist-responsive deep craniofacial afferent or Vc/UCC nociceptiveneuron found in the glutamate followed by capsaicin subgroup or capsaicin followed by glutamate subgroup.
54 B R A I N R E S E A R C H 1 2 5 3 ( 2 0 0 9 ) 4 8 – 5 9
2.4.2. MAT reductionCapsaicin injected into the TMJ following glutamate produceda non-significant reduction in TMJ MAT (25.4 [19.8] g; pN0.05)but did produce a significant reduction in cutaneous MAT(30.6 [14.8] g; p<0.05) values post-injection relative to the pre-injection baseline (RM ANOVA-on-ranks) (Fig. 4). The inci-dence of capsaicin-induced TMJ MAT reduction followingglutamate (11%) was significantly less than that with capsai-cin alone (64%) (p<0.05, Fisher exact test). The incidence ofcutaneous MAT reduction induced by capsaicin followingglutamate was not statistically different compared to thatinduced by capsaicin alone (pN0.05, Fisher exact test) at 10–20 min post-injection.
Glutamate injected into the TMJ following capsaicin pro-duced no significant reduction in TMJ MAT (79.5 [62.1] g;pN0.05) but there was a significant reduction in cutaneousMAT (33.6 [12.8] g) values at 10–20 min post-injectionrelative to the pre-injection baseline (p<0.05, RM ANOVA-on-ranks, Dunn's method) (Fig. 4). The incidence of gluta-mate-induced reduction in TMJ MAT and cutaneous MATfollowing capsaicin was not statistically different comparedto that induced by glutamate alone (pN0.05, Fisher exacttest).
2.4.3. Cutaneous RF expansionThere was no significant difference in the incidence ofcutaneous RF expansion induced by injection of capsaicinalone [63% (10/16)] and capsaicin following glutamate [23%(3/13)] (pN0.05, Fisher exact test) at 10–20 min post-injection.However, following capsaicin injection, the incidence ofglutamate-induced cutaneous RF expansion [10% (1/10)]was significantly less than that with glutamate alone [93%(13/14)] (p<0.001, Fisher exact test) at 10–20 min post-injection.
3. Discussion
This study is the first to demonstrate that a significantproportion of TMJ-responsive nociceptive neurons in theVc/UCC may be activated or sensitized by the peripheralapplication of glutamate or capsaicin. In addition, these EAAor TRPV1 receptor agonists may interact to modulate bothactivation and central sensitization evoked from deep cra-niofacial tissues. By using the same experimental paradigmin the present study as was used in our deep craniofacialafferent study (Lam et al., 2008a), direct comparisons of

55B R A I N R E S E A R C H 1 2 5 3 ( 2 0 0 9 ) 4 8 – 5 9
peripheral versus central nociceptive neuronal responses toperipherally applied glutamate and capsaicin obtained undersimilar experimental conditions could be made. Similar toour companion study (Lam et al., 2008a), the nociceptiveafferent inputs activated by glutamate applied to the TMJsensitized TMJ-responsive Vc/UCC nociceptive neurons, andproduced more immediate, larger and more prolongedresponses to noxious stimulation of the TMJ by capsaicin.However, in contrast to our afferent findings (Lam et al.,2008a), the nociceptive afferent inputs activated by capsaicinapplied to the TMJ desensitized the Vc/UCC nociceptiveneurons to subsequent noxious stimulation of the TMJ byglutamate. As depicted in Fig. 5, these findings suggest thatconvergent signaling pathways are involved in glutamateand capsaicin-evoked activation of deep craniofacial afferentinputs to Vc/UCC nociceptive neurons.
The RF properties, lamina loci and convergence of TMJ andcutaneous afferent inputs of TMJ-responsive neurons areconsistent with previous findings (Yu et al., 1993; Hu et al.,2005; Mørch et al., 2007). This is the first study to docu-ment capsaicin-induced activation and central sensitizationin Vc/UCC nociceptive neurons with deep craniofacial RFs. Incontrast to previous studies (Takeshita et al., 2001; Bereiteret al., 2005; Tashiro et al., 2007) that required extensive ex-posure and retraction of muscle and connective tissue tostimulate the TMJ, the less invasive small skin incision over-ying the TMJ in the present study allowed us to bypass super-ficial (i.e. cutaneous) afferent inputs and directly assess deep(i.e. TMJ) RF sites. As such, the present findings combinedwith those of our companion paper (Lam et al., 2008a) suggestthat both peripheral and central sensitization mechanismsmay contribute to the enhanced responses to glutamate andcapsaicin (e.g. increase in Rmag, Rdur or Pfreq and/or adecrease in Rlat) and TMJ MAT reduction. However, the ob-served cutaneous RF expansion and cutaneous MAT reduc-tion in Vc/UCC nociceptive neurons induced by injection ofglutamate and capsaicin cannot simply be explained by peri-pheral sensitization and likely reflect central sensitizationsince glutamate and capsaicin were applied to a deep tissueRF site (TMJ) remote from the cutaneous RF sites assessed.
Thepresent findings of glutamate-induced central sensitiza-tion in Vc/UCC nociceptive neurons are consistent withtrigeminal (Cairns et al., 1998, 2001a,b, 2003a,b, 2006; Svenssonet al., 2003, 2005) and spinal (Lawand et al., 1997; Wang et al.,1997;Warncke et al., 1997) findings in animals andhumans thatsuggest a role for central sensitization inglutamate-evokedpain(e.g. secondary hyperalgesia). However, glutamate did notinduce a significant reduction in cutaneous MAT for the Vc/UCCneuronal population as awhole but did significantly reduceMAT in the deep craniofacial afferents (Lam et al., 2008a), whichsuggests that peripheral sensitizationmay play a greater role inglutamate-evoked mechanical hypersensitivity.
In the case of capsaicin, the findings that capsaicin producedno significant reduction in deep craniofacial afferent MAT (Lamet al., 2008a) compared with its significant reduction incutaneous MAT for the Vc/UCC neuronal population as awhole is consistent with previous studies suggesting thatcentral sensitizationmayplaya greater role incapsaicin-evokedmechanical hypersensitivity (Baumann et al., 1991; LaMotte etal., 1991, 1992; Simone et al., 1991). In addition, the significant
reduction in MAT directly at the deep (TMJ) site of capsaicininjection for the Vc/UCC neuronal population as a wholecontrasts with the desensitized RF site of superficial (intrader-mal) capsaicin injection in previous studies (Baumann et al.,1991; LaMotte et al., 1991, 1992; Simone et al., 1991) and suggestsdifferences in central nociceptive processing of deep versuscutaneous tissues to peripherally applied capsaicin.
3.1. Glutamate and capsaicin receptor interactions in deepcraniofacial tissues
Capsaicin-evoked activation of TMJ-responsive Vc/UCC neu-rons following glutamate injectionwas significantly enhancedcompared to capsaicin alone. These results are consistentwithfindings in deep craniofacial afferents (Lam et al., 2008a), aswell as the finding that pre-injection of NMDA receptorantagonists into the TMJ region attenuates jawmuscle activityevoked by capsaicin (Lam et al., 2005a). Taken together, thesefindings suggest that the activation and/or sensitization ofperipheral EAA receptors may be important in the mechan-isms whereby capsaicin evokes nociceptive trigeminalresponses.
The interactions between peripheral glutamate and capsai-cin receptors on deep craniofacial afferent inputs to Vc/UCCnociceptive neurons suggest a convergent nociceptive signalingpathway (see Fig. 5). That is, the nociceptive signaling pathwaysare not separate; the glutamate and capsaicin-activated deepcraniofacial afferents converge on Vc/UCC neurons. In theglutamate followed by capsaicin subgroup, the activation offour possible combinations of agonist-responsive afferentinputs (Lam et al., 2008a) converge centrally to result in theactivation of only two agonist-responsive Vc/UCC neurons thatare both capsaicin-sensitive following glutamate, whereas inthe capsaicin followed by glutamate subgroup, the activation offour possible combinations of agonist-responsive afferentinputs converge centrally to result in the activation of onlytwo agonist-responsive Vc/UCC neurons that are both gluta-mate-insensitive following capsaicin. Glutamate-evoked acti-vation and cutaneous RF expansion in the Vc/UCC nociceptiveneurons following capsaicin injection were abolished or sig-nificantly reduced. These findings suggest that capsaicin maydesensitize Vc/UCCneurons to subsequent noxious stimuli (e.g.to glutamate) which is consistent with previous evidenceshowing that capsaicin may desensitize central nociceptiveneurons to subsequent noxious stimuli applied to craniofacialand other tissues (Baumann et al., 1991; LaMotte et al., 1991,1992; Simone et al., 1991; Carstens et al., 1998). Capsaicin-induced activation of the Ca2+-dependent phosphatase calci-neurin may not only mediate dephosphorylation and desensi-tization of peripheral TRPV1 (Docherty et al., 1996; Jung et al.,2004) but it may also desensitize central NMDA and non-NMDAreceptors (Swope et al., 1999; Rycroft and Gibb, 2004) to subse-quent noxious stimulation. However, our findings in Vc/UCCneurons contrast with our afferent data where many of theafferents remained responsive to glutamate following capsaicininjection (Lam et al., 2008a). This difference in peripheral andcentral nociceptive processing of glutamate-evoked responsesfollowing capsaicin injection is difficult to explain. However,since deep craniofacial afferents remain responsive to gluta-mate following capsaicin injection, the peripheral contribution

56 B R A I N R E S E A R C H 1 2 5 3 ( 2 0 0 9 ) 4 8 – 5 9
to the mechanisms behind capsaicin's desensitizing effect onVc/UCC neurons appears to be minimal.
Nociceptive afferents may use glutamate, neuropeptides andproteinsasneurotransmittersor synapticmodulators (Woolf andSalter, 2000; Dubner, 2005; Woolf and Ma, 2007) and it is possiblethat there may be differences in the types of presynapticreceptors, neurotransmitters or modulators released from thecentral terminals of capsaicin-sensitive versus glutamate-sensi-tive afferents that may account for the differential sensitizing ordesensitizing effects on Vc/UCC neurons. The variety of theseneurotransmitters may result in considerable spatial andtemporal summation capabilities that are subject to bothexcitatory and inhibitory influences. In the companion study(Lam et al., 2008a), capsaicin-evoked activation was lower thanthat evoked by glutamate alone in the afferents tested. Incontrast, capsaicin-evoked activation was analogous to thatevoked by glutamate in the Vc/UCC neurons. These findingssuggest that a greater proportion of convergent capsaicin-sensitive afferent inputs on Vc/UCC neurons may contribute tothe enhanced capsaicin-evoked responses as well as thedesensitizingeffectsonsubsequent glutamate-evokedresponsesin Vc/UCC neurons. Since the majority of capsaicin-sensitiveafferents were very slowly conducting afferents (Lam et al.,2008a) projecting to the Vc/UCC region and the vast majorityof Vc/UCC neurons were capsaicin-sensitive, the findingssuggest that these very slowly conducting afferents may bemainly responsible for the activation of Vc/UCC neurons byperipherally applied capsaicin. These capsaicin-sensitiveafferent inputs may activate segmental and/or descendinginhibitory influences on Vc/UCC neurons (for review, seeDubner and Bennett, 1983; Sessle et al., 1992; Dubner and Ren,2004) that in the case of the capsaicin-induced desensitizingeffects, might involve increased inhibitory GABAergic synap-tic transmission through alterations in cation-chloridecotransporters such as NKCC1 or KCC2 on nociceptiveneurons (Galan and Cervero, 2005; Karlsson et al., 2005; Priceet al., 2005, 2006; Garcia-Nicas et al., 2006; Pitcher et al., 2007).The present findings are consistent with recent evidence ofother peripheral TRP receptors participating in the activationof central inhibitory circuits, such as the attenuation of theincreased excitability of spinal nociceptive neurons followingactivation of TRPA1-related nociceptive afferent inputs(Kosugi et al., 2007; Merrill et al., 2008). Thus it is possiblethat the capsaicin-induced desensitization in the presentstudymay occur despite subsequent glutamate-evoked activ-ity in afferent inputs on Vc/UCC neurons via the activation ofsimilar central inhibitory circuits. Further studies are neces-sary to clarify the mechanisms involved.
4. Experimental procedures
4.1. Animal preparation
The animal preparation in this study was the same as the oneoutlined in the companion paper (Lam et al., 2008a). Adultmale (n=49, 250–400 g) Sprague–Dawley rats were preparedfor acute in vivo recording activity of TMJ-responsive noci-ceptive neurons in the Vc/UCC region under halothanesurgical anesthesia. A tracheal cannula was inserted, the
rat's head placed in a stereotaxic frame, a C1 laminectomyperformed, and the dura reflected to expose the Vc/UCC andfacilitate placement of a recording microelectrode in the leftVc/UCC (Hu, 1990; Hu et al., 2005). To ensure that an adequateanesthesia level was maintained during the experiment, thehalothane was reduced to a level that was sufficient toproduce reflex suppression of the hindlimb to noxiouspressure application to the hindpaw. Heart rate and bodycore temperature were continuously monitored and keptwithin the physiological range of 330–430/min and 37–37.5 °C,respectively. All procedures were approved by the Universityof Toronto Animal Care Committee in accordance with theregulations of the Ontario Animal Research Act (Canada).
4.2. Recording and stimulating procedures
One hour after completion of surgery, an epoxy-resin-coatedtungsten microelectrode was slowly lowered into the ex-posed Vc/UCC region under stereotaxic control (3–6 mmcaudal to obex, 0.5–3 mm lateral to the midline) until theextracellular activity of a single TMJ-responsive nociceptiveneuron was isolated and identified (Hu, 1990). When a neuronwas found that responded to direct, blunt noxious mecha-nical stimulation of the TMJ, the nociceptive neuron wasconsidered TMJ-responsive. Mechanical (brush, pressure, andpinch) stimuli were applied to the craniofacial cutaneoustissues to classify each TMJ-responsive nociceptive neuron asWDR or NS Mechanical (pinch) stimuli were also applied tocontralateral skin as well as to selected spinally innervatedtissues (e.g. paws). Baseline spontaneous neuronal activity(spikes/second) was recorded for a 10-minute period prior tomechanical and chemical stimulation. The cutaneous RF sizeand MAT of the TMJ-responsive nociceptive neurons wereassessed at the time intervals specified under the experi-mental paradigm (see below). The cutaneous RF of eachneuron was determined through the use of a brush, bluntprobe, and a pair of nonserrated forceps. The extent of theneuron's cutaneous RF was also outlined on a life-sizedrawing of the rat's head. The MAT of the neuronal RF wasdetermined with an electronic von Frey device (Model 735, 1.0-mm diameter probe tip, Somedic Sales AB, Sweden) appliedto the center of the cutaneous RF or the TMJ region and wasdefined as the force (g) required to evoke the first spike, or afiring rate of greater than 2 standard deviations abovebaseline neuronal activity when the neuron was sponta-neously active, measured at the neuronal RF site with aramp of gradually increasing force.
4.3. Receptor agonists
Glutamate (0.5 M; 10 μL; Sigma Chemical Company, St. Louis,MO), 1% capsaicin (10% capsaicin in ethanol:Tween-80: sterilenormal saline in a 1:1:8 ratio by volume; 10 μL; Calbiochem,La Jolla, CA) or vehicle (isotonic saline as control for gluta-mate or ethanol:Tween 80:sterile normal saline in a 1:1:8ratio by volume as control for capsaicin; 10 μL) was injectedinto the left TMJ at 30 min intervals in both experimentalsubgroups of rats. The above solutions were adjusted tophysiologic pH (7.2–7.6).

57B R A I N R E S E A R C H 1 2 5 3 ( 2 0 0 9 ) 4 8 – 5 9
4.4. Experimental paradigm
The experimental paradigm used in this study was the sameas the one outlined in the companion paper (Lam et al.,2008a). Study animals were divided into two subgroups: TMJ-responsive nociceptive neuronal response properties of ratswith glutamate (or vehicle) injection followed by capsaicin (orvehicle) injection in one subgroup of rats were compared withproperties of neurons in a second subgroup of rats withcapsaicin (or vehicle) injection followed by glutamate (orvehicle) injection. A similar experimental paradigm wasapplied to both subgroups: 10 min after a TMJ-responsivenociceptive neuronwas identified as aWDR or NS neuron, theneuronal cutaneous RF and cutaneous MAT were determinedand served as baseline values. A short-acting local anesthetic(2% Lidocaine in 10 μL) was infiltrated subcutaneously 15 minprior to incision of the skin overlying the left TMJ to reducethe effects of the incision-induced afferent barrage onneuronal excitability (Lam et al., 2008b). The skin overlyingthe TMJ was then raised with tissue forceps to avoid damageto the TMJ and deep tissues, and a surgical incision (<2 mmlong) was made with a 16-gauge needle through skin andfascia overlying the left TMJ to facilitate later injection ofreceptor agonists (or vehicle) into the TMJ and allow directassessment of the TMJ MAT before and after receptor agonistinjection. Neuronal cutaneous RF and MAT were reassessedat 10 and 20 min post-incision to ensure there were nochanges from baseline values (Lam et al., 2008b). In addition,the TMJ MAT was determined at 10 and 20 min post-incision.The tip of a catheter was then carefully inserted into the leftTMJ through the incision site. It was observed that subse-quent insertion of the catheter used to inject receptoragonists or vehicle control into the TMJ evoked a spikedischarge in all TMJ-responsive neurons identified in order toconfirm that the injection site was within the neuronal RF.Baseline neuronal activity was recorded for 10 min prior toinjection of the first receptor agonist or vehicle control intothe left TMJ. The receptor agonist or vehicle control was thenslowly injected into the left TMJ (over a 5-second period) andfour response properties were assessed: (1) Rmag: the totalnumber of evoked spikes, or a firing rate of greater than 2standard deviations above baseline neuronal activity whenthe neuron was spontaneously active, following agonist orvehicle injection, (2) Rdur: the total time (seconds) from thefirst spike following agonist or vehicle injection to the lastspike, (3) Rlat: the total time (seconds) from agonist or vehicleinjection to the first spike following agonist injection, and (4)Pfreq: the highest firing rate in a one second period (Hz) duringthe Rdur. At 10 min post-injection of the receptor agonist orvehicle control, the needle was withdrawn and an assess-ment was made at this 10 min time point and again at 20 minafter injection to determine if any changes in cutaneous RF,cutaneous MAT and TMJ MAT from baseline had occurred.The same protocol described above was used for injection ofthe second receptor agonist (or vehicle) 30 min post-injectionof the first receptor agonist (or vehicle). In each animal, onlyone TMJ-responsive neuron was tested with the aboveprotocol.
Cutaneous RF expansionwas defined as expansion in RF sizeto include a predetermined point lying 5 mm outside the
perimeter of the baseline cutaneous RF. This methodologyfor assessment of RF reduces the possibility of iatrogenicallyinduced sensitization by avoiding multiple sites of noxiousstimulation. In a small number of neurons, the border of thecutaneous RF was mapped in detail for illustration purposes(e.g. Figs. 2 and 3). Cutaneous MAT reduction was defined as≥50% threshold reduction from baseline MAT score mea-sured at the center of the cutaneous RF site. TMJ MATreduction was defined as ≥50% threshold reduction frombaseline MAT score measured at TMJ RF sites. Raw MATthreshold values measured post-injection were normalizedto the initial baseline pre-injection value to illustratepopulation responses. At the end of each experiment,electrolytic lesions were made in the Vc/UCC recording siteof rats by applying amonopolar, monophasic current pulse of10 μA for 10 s to identify the recording site. Rats werethen euthanized with the agent T61 (Hoechst, Canada). Theunit recording sites confirmed histologically by H & E stain-ing were subsequently reconstructed and plotted on stan-dardized diagrams of the brainstem (Paxinos and Watson,1997).
4.5. Data analysis
Recorded neuronal activity was stored electronically andanalyzed off-line. Most of the population data are reportedas mean±SE. However, if not normally distributed, populationdata are reported as median values with interquartile rangesindicated in square brackets; median [IQR]. Mann–Whitney Utest, t-test, Fisher exact test, and RM ANOVA-on-ranks wereused as appropriate (p<0.05 considered to reflect statisticalsignificance).
Acknowledgments
Support contributed by CIHR MOP-43905 and NIH DE15420.
R E F E R E N C E S
Baumann, T.K., Simone, D.A., Shain, C.N., LaMotte, R.H., 1991.Neurogenic hyperalgesia: the search for the primary cutaneousafferent fibers that contribute to capsaicin-induced pain andhyperalgesia. J. Neurophysiol. 66, 212–227.
Bereiter, D.A., Hiraba, H., Hu, J.W., 2000. Trigeminal subnucleuscaudalis beyond homologies with the spinal dorsal horn. Pain88, 221–224.
Bereiter, D.A., Okamoto, K., Bereiter, D.F., 2005. Effect ofpersistent monoarthritis of the temporomandibular jointregion on acute mustard oil-induced excitation of trigeminalsubnucleus caudalis neurons in male and female rats. Pain117, 58–67.
Cairns, B.E., Sessle, B.J., Hu, J.W., 1998. Evidence that excitatoryamino acid receptors within the temporomandibular jointregion are involved in the reflex activation of the jaw muscles.J. Neurosci. 18, 8056–8064.
Cairns, B.E., Sessle, B.J., Hu, J.W., 2001a. Temporomandibular-evoked jaw muscle reflex: role of brain stem NMDA andnon-NMDA receptors. NeuroReport 12, 1875–1878.
Cairns, B.E., Hu, J.W., Arendt-Nielsen, L., Sessle, B.J., Svensson, P.,2001b. Sex-related differences in human pain and rat afferent

58 B R A I N R E S E A R C H 1 2 5 3 ( 2 0 0 9 ) 4 8 – 5 9
discharge evoked by injection of glutamate into the massetermuscle. J. Neurophysiol. 86, 782–791.
Cairns, B.E., Svensson, P., Wang, K., Hupfeld, S., Graven-Nielsen,T., Sessle, B.J., Berde, C.B., Arendt-Nielsen, L., 2003a. Activationof peripheral NMDA receptors contributes to human pain andrat afferent discharges evoked by injection of glutamate intothe masseter muscle. J. Neurophysiol. 90, 2098–2105.
Cairns, B.E., Wang, K., Hu, J.W., Sessle, B.J., Arendt-Nielsen, L.,Svensson, P., 2003b. The effect of glutamate-evoked massetermuscle pain on the human jaw-stretch reflex differs in menand women. J. Orofac. Pain 17, 317–325.
Cairns, B.E., Svensson, P., Wang, K., Castrillon, E., Hupfeld, S.,Sessle, B.J., Arendt-Nielsen, L., 2006. Ketamine attenuatesglutamate-induced mechanical sensitization of the massetermuscle in human males. Exp. Brain Res. 169, 467–472.
Carstens, E., Kuenzler, N., Handwerker, H.O., 1998. Activation ofneurons in rat trigeminal subnucleus caudalis by differentirritant chemicals applied to oral or ocular mucosa. J.Neurophysiol. 80, 465–492.
Docherty, R.J., Yeats, J.C., Bevan, S., Boddeke, H.W., 1996. Inhibitionof calcineurin inhibits the desensitization of capsaicin-evokedcurrents in cultured dorsal root ganglion neurones from adultrats. Pflugers Arch. 431, 828–837.
Dubner, R., 2005. Plasticity in central nociceptive pathways. In:Merskey, H., Loeser, J.D., Dubner, R. (Eds.), The Paths of Pain1975–2005. IASP Press, Seattle, WA, pp. 101–115.
Dubner, R., Bennett, G.J., 1983. Spinal and trigeminal mechanismsof nociception. Annu. Rev. Neurosci. 6, 381–418.
Dubner, R., Ren, K., 2004. Brainstem mechanisms of persistentpain following injury. J. Orofac. Pain 18, 299–305.
Galan, A., Cervero, F., 2005. Painful stimuli induce in vivophosphorylation and membrane mobilization of mouse spinalcord NKCC1 co-transporter. Neuroscience 133, 245–252.
Garcia-Nicas, E., Laird, J.M., Cervero, F., 2006. GABAA-receptorblockade reverses the injury-induced sensitization ofnociceptor-specific (NS) neurons in the spinal dorsal horn ofthe rat. J. Neurophysiol. 96, 661–670.
Gazerani, P., Arendt-Nielsen, L., 2005. The impact of ethnicdifferences in response to capsaicin-induced trigeminalsensitization. Pain 117, 223–229.
Gazerani, P., Staahl, C., Drewes, A.M., Arendt-Nielsen, L., 2006. Theeffects of Botulinum Toxin type A on capsaicin-evoked pain,flare, and secondary hyperalgesia in an experimental humanmodel of trigeminal sensitization. Pain 122, 315–325.
Ge, H.Y., Madeleine, P., Arendt-Nielsen, L., 2005. Genderdifferences in pain modulation evoked by repeated injectionsof glutamate into the human trapezius muscle. Pain 113,134–140.
Hu, J.W., 1990. Response properties of nociceptive andnon-nociceptive neurons in the rat's trigeminal subnucleuscaudalis (medullary dorsal horn) related to cutaneous and deepcraniofacial afferent stimulation and modulation by diffusenoxious inhibitory controls. Pain 41, 331–345.
Hu, J.W., Sun, K.Q., Vernon, H., Sessle, B.J., 2005. Craniofacialinputs to upper cervical dorsal horn: implications forsomatosensory information processing. Brain Res. 1044,93–106.
Jung, J., Shin, J.S., Lee, S.Y., Hwang, S.W., Koo, J., Cho, H., Oh, U.,2004. Phosphorylation of vanilloid receptor 1 by Ca2+/calmodulin-dependent kinase II regulates its vanilloid binding.J. Biol. Chem. 279, 7048–7054.
Karlsson, U., Sundgren-Andersson, A.K., Johansson, S., Krupp, J.J.,2005. Capsaicin augments synaptic transmission in the ratmedial preoptic nucleus. Brain Res. 1043, 1–11.
Kosugi, M., Nakatsuka, T., Fujita, T., Kuroda, Y., Kumamoto, E.,2007. Activation of TRPA1 channel facilitates excitatorysynaptic transmission in substantia gelatinosa neurons of theadult rat spinal cord. J. Neurosci. 27, 4443–4451.
Lam, D.K., Sessle, B.J., Hu, J.W., 2003. Trigeminal nociceptive
neuronal activity modulated by glutamate and capsaicinapplication to rat TMJ. ProgramNo. 1178. 2003 Abstract Viewer/Itinerary Planner. International Association for DentalResearch.
Lam, D.K., Sessle, B.J., Cairns, B.E., Hu, J.W., 2005a. PeripheralNMDA receptor modulation of jaw muscle electromyographicactivity induced by capsaicin injection into thetemporomandibular joint of rats. Brain Res. 1046, 68–76.
Lam, D.K., Sessle, B.J., Cairns, B.E., Hu, J.W., 2005b. Neuralmechanisms of temporomandibular joint and masticatorymuscle pain: a possible role for peripheral glutamate receptormechanisms. Pain Res. Manag. 10, 145–152.
Lam, D.K., Sessle, B.J., Hu, J.W., 2008a. Glutamate and capsaicineffects on trigeminal nociception I: activation and peripheralsensitization of deep craniofacial nociceptive afferents. BrainRes. doi:10.1016/j.brainres.2008.11.029.
Lam, D.K., Sessle, B.J., Hu, J.W., 2008b. Surgical incision can altercapsaicin-induced central sensitization in rat brainstemnociceptive neurons. Neurosci. 156, 737–747.
LaMotte, R., Shain, C.N., Simone, D.A., Tsai, E.F., 1991. Neurogenichyperalgesia: psychophysical studies of underlyingmechanisms. J. Neurophysiol. 66, 190–211.
LaMotte, R.H., Lundberg, L.E., Torebjork, H.E., 1992. Pain,hyperalgesia and activity in nociceptive C units in humansafter intradermal injection of capsaicin. J. Physiol. 448, 749–764.
Lawand, N.B., Willis, W.D., Westlund, K.N., 1997. Excitatory aminoacid receptor involvement in peripheral nociceptivetransmission in rats. Eur. J. Pharmacol. 324, 169–177.
Merrill, A.W., Cuellar, J.M., Judd, J.H., Carstens, M.I., Carstens, E.,2008. Effects of TRPA1 agonists mustard oil andcinnamaldehyde on lumbar spinal wide-dynamic rangeneuronal responses to innocuous and noxious cutaneousstimuli in rats. J. Neurophysiol. 99, 415–425.
Mørch, C.D., Hu, J.W., Arendt-Nielsen, L., Sessle, B.J., 2007.Convergence of cutaneous, musculoskeletal, dural and visceralafferents onto nociceptive neurons in the first cervical dorsalhorn. Eur. J. Neurosci. 26, 142–154.
Paxinos, G., Watson, C., 1997. The Rat Brain in StereotaxicCoordinates, Compact Third Edition. Academic Press, Toronto.
Pitcher, M.H., Price, T.J., Entrena, J.M., Cervero, F., 2007. SpinalNKCC1 blockade inhibits TRPV1-dependent referred allodynia.Mol. Pain 3, 17.
Price, T.J., Cervero, F., de Koninck, Y., 2005. Role ofcation-chloride-cotransporters (CCC) in pain and hyperalgesia.Curr. Top. Med. Chem. 5, 547–555.
Price, T.J., Hargreaves, K.M., Cervero, F., 2006. Protein expressionand mRNA cellular distribution of the NKCC1 cotransporter inthe dorsal root and trigeminal ganglia of the rat. Brain Res.1112, 146–158.
Rycroft, B.K., Gibb, A.J., 2004. Inhibitory interactions of calcineurin(phosphatase 2B) and calmodulin on rat hippocampal NMDAreceptors. Neuropharmacology 47, 505–514.
Sessle, B.J., 2005. Orofacial pain. In: Merskey, H., Loeser, J.D.,Dubner, R. (Eds.), The Paths of Pain 1975–2005. IASP Press,Seattle, pp. 131–150.
Sessle, B.J., Chiang, C.Y., Dostrovsky, J.O., 1992. Interrelationshipsbetween sensorimotor cortex, anterior pretectal nucleus andperiaqueductal gray in modulation of trigeminal sensorimotorfunction in the rat. In: Inoki, R., Shigenaga, Y., Tohyama, M.(Eds.), Processing and inhibition of nociceptive information.Elsevier, Amsterdam, pp. 77–82.
Simone, D.A., Sorkin, L.A., Oh, U., Chung, J.M., Owens, C., LaMotte,R.H., Willis, W.D., 1991. Neurogenic hyperalgesia: centralcorrelates in responses of spinothalamic tract neurons.J. Neurophysiol. 66, 228–246.
Sohn, M.K., Graven-Nielsen, T., Arendt-Nielsen, L., Svensson, P.,2000. Inhibition of motor unit firing during experimentalmuscle pain in humans. Muscle Nerve 23, 1219–1226.
Sohn, M.K., Graven-Nielsen, T., Arendt-Nielsen, L., Svensson, P.,

59B R A I N R E S E A R C H 1 2 5 3 ( 2 0 0 9 ) 4 8 – 5 9
2004. Effects of experimental muscle pain on mechanicalproperties of single motor units in human masseter. Clin.Neurophysiol. 115, 76–84.
Svensson, P., Cairns, B.E., Wang, K., Hu, J.W., Graven-Nielsen, T.,Arendt-Nielsen, L., Sessle, B.J., 2003. Glutamate-evoked painand mechanical allodynia in the human masseter muscle.Pain. 101, 221–227.
Svensson, P., Wang, K., Arendt-Nielsen, L., Cairns, B.E., Sessle, B.J.,2005. Pain effects of glutamate injections into human jaw orneck muscles. J. Orofac. Pain 19, 109–118.
Swope, S.L.,Moss, S.J., Raymond,L.A.,Huganir,R.L., 1999.Regulationofligand-gated ion channels by protein phosphorylation. Adv.Second Messenger Phosphoprot. Res. 33, 49–78.
Takeshita, S., Hirata, H., Bereiter, D.A., 2001. Intensity coding by TMJ-responsive neurons in superficial laminae of caudal medullarydorsal horn of the rat. J. Neurophysiol. 86, 2393–2404.
Tang, M.L., Haas, D.A., Hu, J.W., 2004. Capsaicin-induced jointinflammation is not blocked by local anesthesia. Anesth. Prog.51, 2–9.
Tashiro, A., Okamoto, K., Milam, S.B., Bereiter, D.A., 2007.Differential effects of estradiol on encoding properties of TMJunits in laminae I and V at the spinomedullary junction infemale rats. J. Neurophysiol. 98, 3242–3253.
Wang, H., Liu, R.J., Zhang, R.-X., Qiao, J.-T., 1997. Peripheral NMDAreceptors contribute to the activation of nociceptors: a c-fosexpression study in rats. Neurosci. Lett. 221, 101–104.
Wang, K., Arendt-Nielsen, L., Svensson, P., 2002.Capsaicin-induced muscle pain alters the excitability of thehuman jaw-stretch reflex. J. Dent. Res. 81, 650–654.
Warncke, T., Jørum, E., Stubhaug, A., 1997. Local treatment withN-methyl-D-aspartate receptor antagonist ketamine inhibitsdevelopment of secondary hyperalgesia inman by a peripheralaction. Neurosci. Lett. 227, 1–4.
Woolf, C.J., Salter, M.W., 2000. Neuronal plasticity: increasing thegain in pain. Science 288, 1765–1769.
Woolf, C.J., Ma, Q., 2007. Nociceptors—noxious stimulus detectors.Neuron 55, 353–364.
Yu, X.M., Sessle, B.J., Hu, J.W., 1993. Differential effects ofcutaneous and deep application of inflammatory irritanton mechanoreceptive field properties of trigeminalbrain stem nociceptive neurons. J. Neurophysiol. 70,1704–1707.
Zanotto, K., Merrill, A.W., Carstens, M.I., Carstens, E., 2007.Neurons in superficial trigeminal subnucleus caudalisresponsive to oral cooling, menthol and other irritant stimuli.J. Neurophysiol. 97, 966–978.