
GLOBAL PROSTATE CANCER OUTCOMES REGISTRY · healthcare, designed to engender “competition”...
65
PCOR AND THE DELPHI PROJECT GLOBAL PROSTATE CANCER OUTCOMES REGISTRY
Transcript of GLOBAL PROSTATE CANCER OUTCOMES REGISTRY · healthcare, designed to engender “competition”...

P C O R A N D T H E D E L P H I P R O J E C T
GLOBAL PROSTATE CANCER OUTCOMES REGISTRY

• Provide an overview of the registry/timeline
• Describe the dataset development
• Discuss the Delphi consensus quality indicator project
• Outline the next steps
Objectives

P C O R - V I C P C O R - A N Z T R U E N T H G L O B A L P C O R

PCOR-Vic
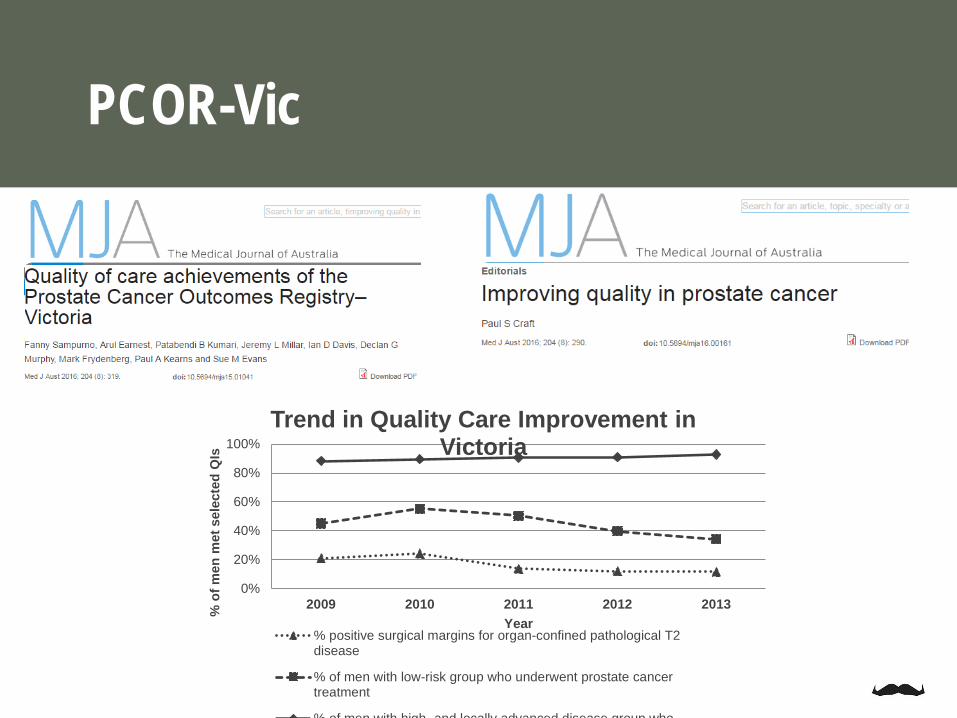
Prostate Cancer Outcome Registry-Victoria (PCOR-VIC)• Established 2009 to test feasibility of clinician-led registry to monitor quality of care• 6 sites• Extended to two regional areas with additional funding• Currently captures 75% of cases in Victoria

PCOR-Vic

Hospital volumePositive marginsDocumented cTAS for low-risk diseaseHigh-risk disease having RxRisk adjusted CaP-specific survival and recurrencePRO-sexual, bowel and urinary bother and functionIn-hospital death from major complicationsTime from biopsy to treatment for men with pT2 disease
PCOR-Vic
PCOR-Vic
0%
20%
40%
60%
80%
100%
2009 2010 2011 2012 2013% o
f men
met
sel
ecte
d Q
Is
Year
Trend in Quality Care Improvement in Victoria
% positive surgical margins for organ-confined pathological T2disease
% of men with low-risk group who underwent prostate cancertreatment
% of men with high and locally advanced disease group who
0%
20%
40%
60%
80%
100%
2010(n=2428)
2011(n=2422)
2012(n=2496)
2013(n=2186)
2014(n=2147)
2015(n=2221)
To 1/7/2016(n=1033)
Low Intermediate High Very high/mets
Low risk
Intermediate
High risk
Very high risk/ metastatic
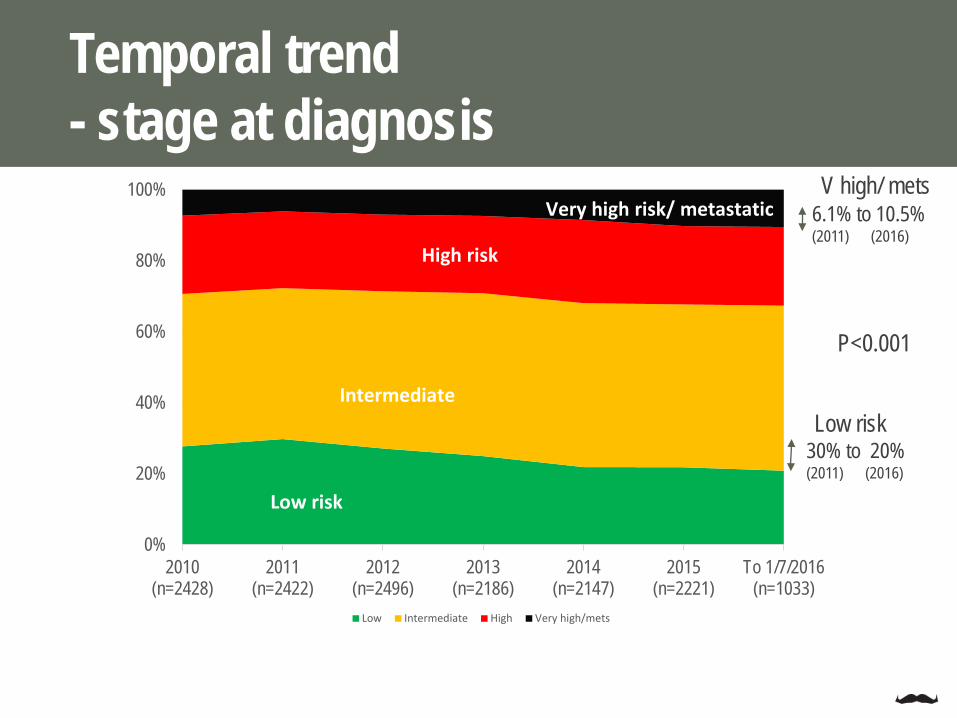
Temporal trend- stage at diagnosis
P<0.001
30% to 20%(2011) (2016)
6.1% to 10.5%(2011) (2016)
Low risk
V high/ mets

Temporal trend- Method of diagnosis
0%
20%
40%
60%
80%
100%
2010(n=2428)
2011(n=2422)
2012(n=2496)
2013(n=2186)
2014(n=2147)
2015(n=2221)
To 1/7/2016(n=1033)
TRUS
Transperineal
Clinical/otherTURP
P<0.001

Temporal trend-low risk disease management
0%
20%
40%
60%
80%
100%
2010(n=640)
2011(n=710)
2012(n=660)
2013(n=529)
2014(n=454)
2015 (n=468) To 1/7/2016(n=208)
Surg EBRT Brachy AS/WW
AS/WW
BRACHYEBRT
SURGERY
P<0.001
52% to 75%(2011) (2016)
AS/WW
Surg 35% to 20%(2011) (2016)

Temporal trend-intermediate risk disease management
0%
20%
40%
60%
80%
100%
2010(n=1021)
2011(n=1016)
2012(n=1085)
2013(n=980)
2014(n=961)
2015 (n=984)
To 1/7/2016 (n=463)
Surg AS/WW EBRT Surg+EBRT Brachy Other
AS/WW
EBRT
SURGERY
P<0.001
16% to 11%(2011) (2016)EBRT
13% to 18%(2011) (2016)
AS/WW
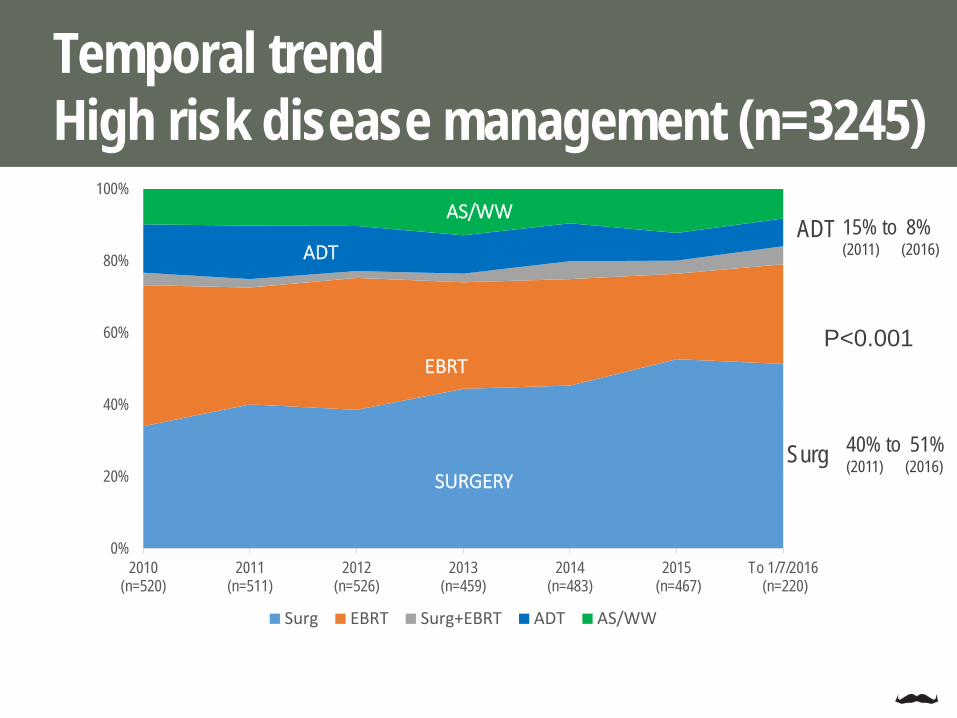
Temporal trendHigh risk disease management (n=3245)
0%
20%
40%
60%
80%
100%
2010(n=520)
2011(n=511)
2012(n=526)
2013(n=459)
2014(n=483)
2015 (n=467)
To 1/7/2016 (n=220)
Surg EBRT Surg+EBRT ADT AS/WW
SURGERY
EBRT
AS/WW
ADT
P<0.001
40% to 51%(2011) (2016)Surg
15% to 8%(2011) (2016)
ADT

Very high risk/ metastatic disease (n=1153)
0%
20%
40%
60%
80%
100%
2010(n=174)
2011(n=145)
2012(n=171)
2013(n=157)
2014(n=178)
2015 (n=215)
To 1/7/2016 (n=104)
Surg EBRT Chemo ADT Other
SURGERY
EBRT
CHEMO
ADT
OTHER
3% to 14%(2011) (2016)Chemo

PCOR-ANZ
Prostate Cancer Outcome Registry-Aust and NZ
• Progressively rolled out• National indicators developed through
Delphi panel
Data• Cancer registries
• Mandatory hospital and pathology notifications• Demographic details• Diagnosing clinician/hospital
• Hospital databases• Procedures (electronically where possible)• Pathology (PSA levels)/ histopathology
• Consulting rooms• Treatment• PSA level
• Patients• Treatment confirmation• PROMs• Comorbidities (no ICD complications)
PCOR-ANZ

TrueNTH Global Prostate Cancer Registry
Prostate Cancer Outcome Registry-Global registry

Largest international prostate cancer cohort study to date.
It provides the ability to make a large contribution to our knowledge of how prostate cancer can best be managed to provide the best possible outcomes for men, their partners and their families.
TrueNTH Global Prostate Cancer Registry
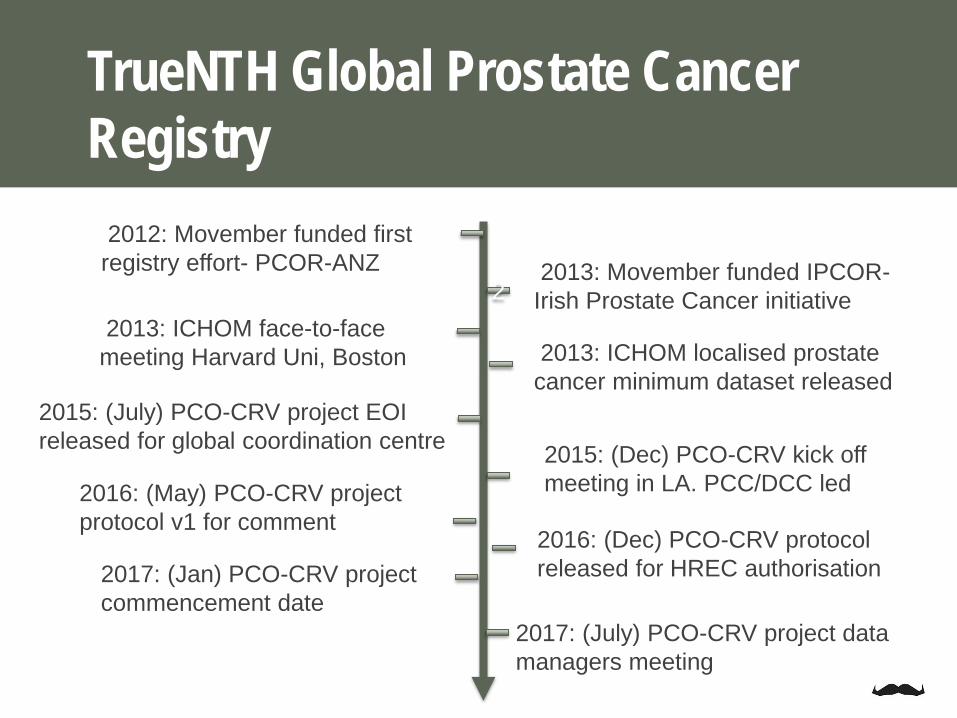
2012: Movember funded first registry effort- PCOR-ANZ
22013: Movember funded IPCOR-
Irish Prostate Cancer initiative2013: ICHOM face-to-face
meeting Harvard Uni, Boston 2013: ICHOM localised prostate cancer minimum dataset released
2015: (July) PCO-CRV project EOI released for global coordination centre
2016: (May) PCO-CRV project protocol v1 for comment
2017: (July) PCO-CRV project data managers meeting
2017: (Jan) PCO-CRV project commencement date
2015: (Dec) PCO-CRV kick off meeting in LA. PCC/DCC led
2016: (Dec) PCO-CRV protocol released for HREC authorisation
TrueNTH Global Prostate Cancer Registry
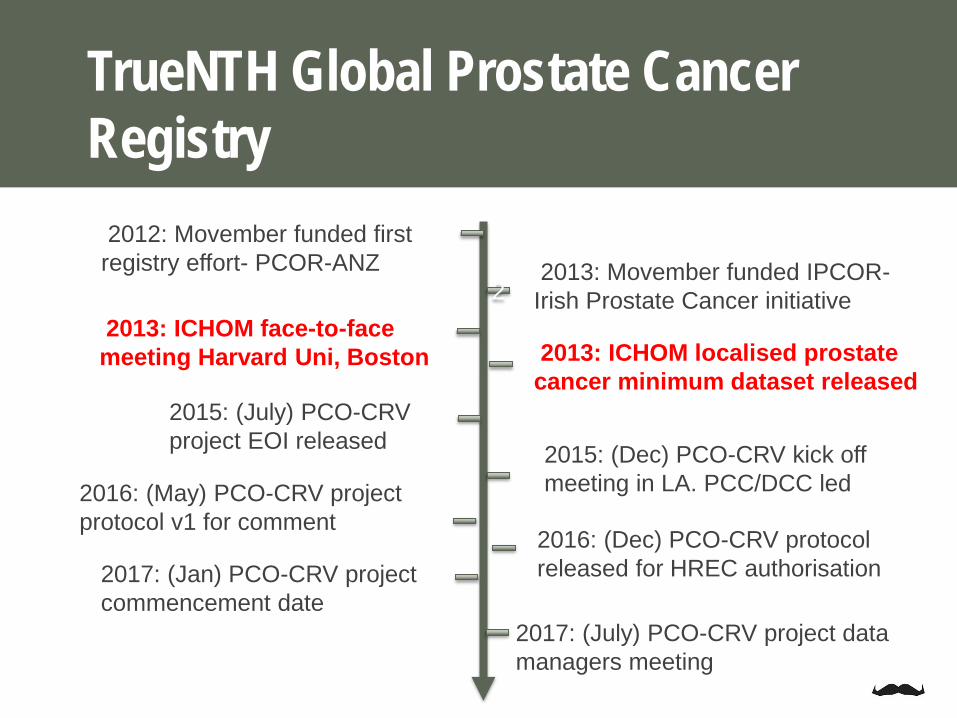
2012: Movember funded first registry effort- PCOR-ANZ
22013: Movember funded IPCOR-
Irish Prostate Cancer initiative2013: ICHOM face-to-face
meeting Harvard Uni, Boston 2013: ICHOM localised prostate cancer minimum dataset released
2015: (July) PCO-CRV project EOI released
2016: (May) PCO-CRV project protocol v1 for comment
2017: (July) PCO-CRV project data managers meeting
2017: (Jan) PCO-CRV project commencement date
2015: (Dec) PCO-CRV kick off meeting in LA. PCC/DCC led
2016: (Dec) PCO-CRV protocol released for HREC authorisation
TrueNTH Global Prostate Cancer Registry
• Develop consensus standardised minimum dataset
• Facilitate comparative effectiveness research and foster value-based healthcare, designed to engender “competition” between high-quality entities to achieve better outcomes for patients and simultaneously optimize cost of this care
• .
• Facilitate international collaborations to combine data, allow comparisons, insight into high value and high quality features of care, and action to adopt these more widely
• Mechanism to do this was not described
Goals
ICHOM

• Develop consensus standardised minimum dataset
• Facilitate comparative effectiveness research and foster value-based healthcare, designed to engender “competition” between high-quality entities to achieve better outcomes for patients and simultaneously optimize cost of this care
• .
• Facilitate international collaborations to combine data, allow comparisons, insight into high value and high quality features of care, and action to adopt these more widely
• Mechanism to do this was not described
Goals
ICHOM

Study schema

• Develop consensus standardised minimum dataset
• Facilitate comparative effectiveness research and foster value-based healthcare, designed to engender “competition” between high-quality entities to achieve better outcomes for patients and simultaneously optimize cost of this care
• .
• Facilitate international collaborations to combine data, allow comparisons, insight into high value and high quality features of care, and action to adopt these more widely
• Mechanism to do this was not described
Goals
ICHOM

The theory of “positive deviance”
Identify organisations consistently
achieving high performance in area of interest
Study this organisation using qualitative methods
to generate hypotheses about
why this is occurring
Test hypotheses in larger
representative sample
Disseminate evidence about
newly characterised best practice

Timeline
2012: Movember funded first registry effort- PCOR-ANZ
22013: Movember funded IPCOR-
Irish Prostate Cancer initiative2013: ICHOM face-to-face
meeting Harvard Uni, Boston 2013: ICHOM localised prostate cancer minimum dataset released
2015: (July) PCO-CRV project EOI released
2016: (May) PCO-CRV project protocol with proposed dataset
2017: (July) PCO-CRV project data managers meeting
2017: (Jan) PCO-CRV project commencement date
2015: (Dec) PCO-CRV kick off meeting in LA. PCC/DCC
2016: (Dec) PCO-CRV protocol released for HREC authorisation
Participating Sites contribute to data governance, dataset development and evolution, analysis, dissemination of identified “best practice”, and monitoring change
Data Coordination Centre: • hosts the clinical quality registry providing high security, highly reliable, flexible
controlled storage and data manipulation services • Coordinates activities of the Participating Sites.• Conducting principal data analyses under the guidance of the project Steering
Committee
EOI released mid-2015 for Participating Sites and Data Coordination Centre
Task 1: Identify participating sites and coordination centre

DCC and PCC appointed
DCC
PCC

Data discovery project-DCC
Task 2: is ICHOM data collection feasible?

Task 2: is ICHOM data collection feasible?
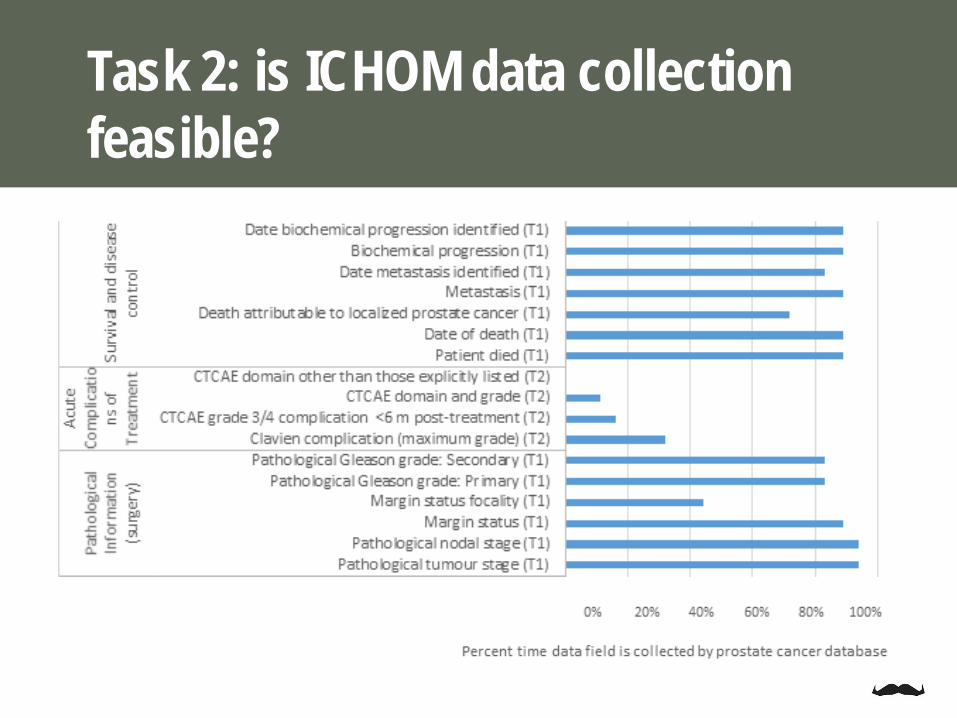
Task 2: is ICHOM data collection feasible?
Task 2: is ICHOM data collection feasible?
Not straight away…….
…. Concept of Tier 1 (T1) and Tier 2 (T2) introduced
…. By the PCO-CRV Executive Committee
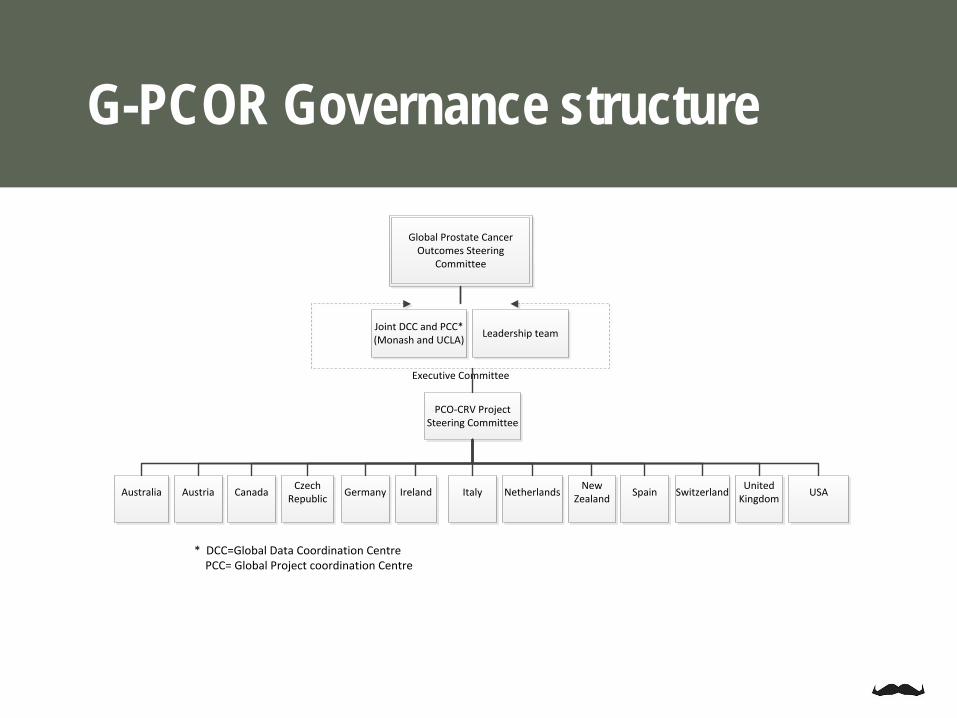
G-PCOR Governance structure
Global Prostate Cancer
Outcomes Steering Committee
Joint DCC and PCC* (Monash and UCLA)
Leadership team
Executive Committee
PCO-CRV Project
Steering Committee
Australia
Austria
Canada
Germany
Ireland
Italy
Spain
United Kingdom
USA
Switzerland
Czech Republic
Netherlands
New Zealand
* DCC=Global Data Coordination Centre PCC= Global Project coordination Centre
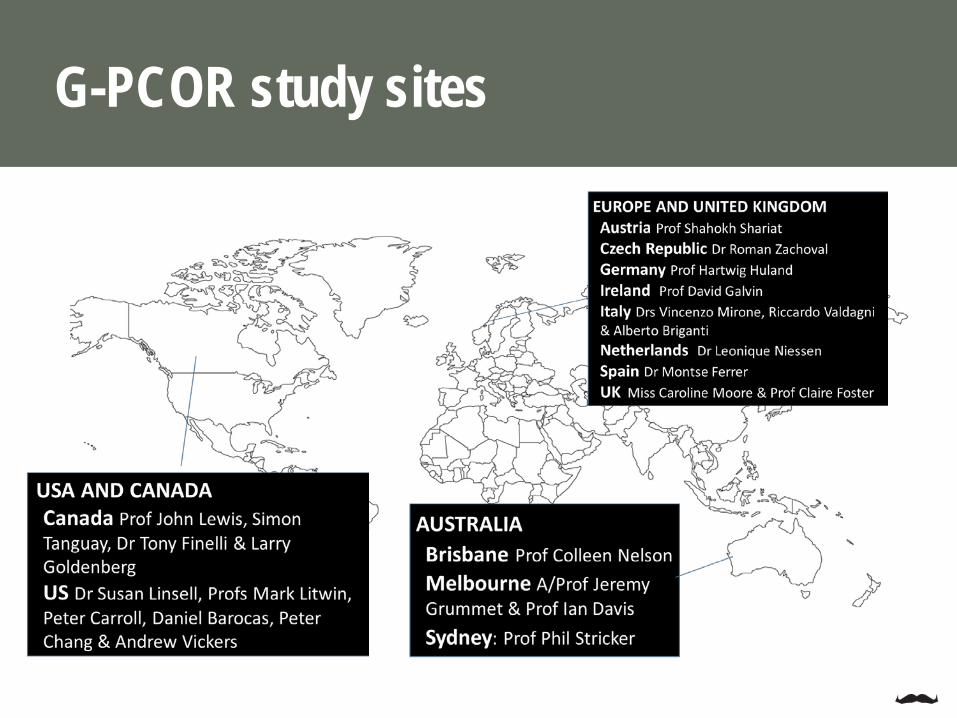
G-PCOR study sites
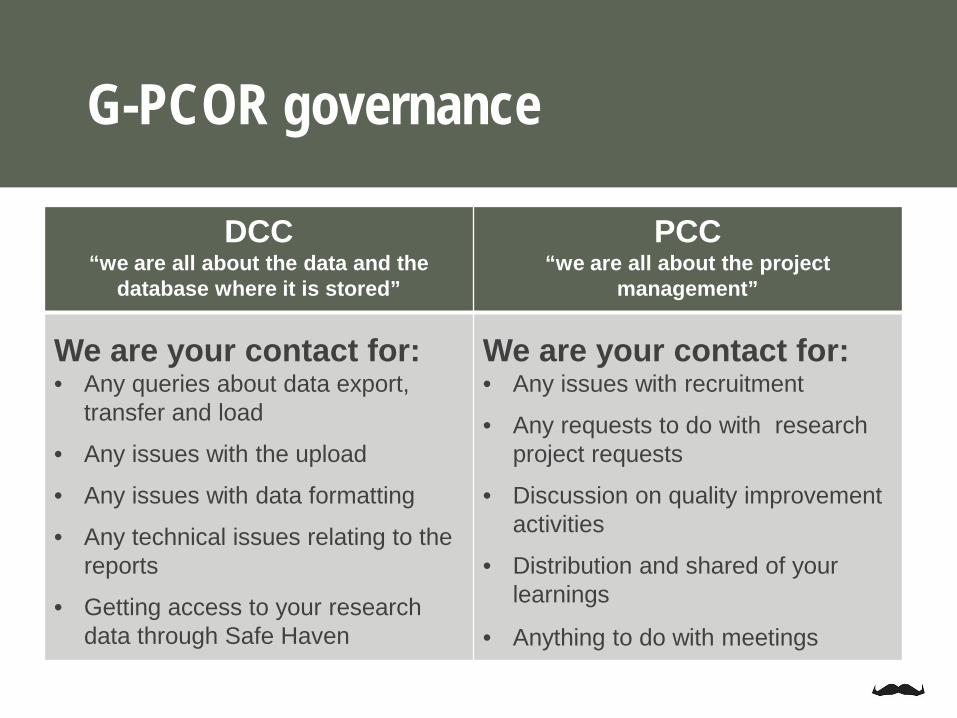
G-PCOR governance
DCC“we are all about the data and the
database where it is stored”
PCC“we are all about the project
management”
We are your contact for:• Any queries about data export,
transfer and load
• Any issues with the upload
• Any issues with data formatting
• Any technical issues relating to the reports
• Getting access to your research data through Safe Haven
We are your contact for:• Any issues with recruitment
• Any requests to do with research project requests
• Discussion on quality improvement activities
• Distribution and shared of your learnings
• Anything to do with meetings
M O D I F I E D D E L P H I P R O C E S S TO D E V E L O P G L O B A L Q U A L I T Y I N D I C ATO R S
Modified Delphi panel
Select a reasonable number of indicators that can measure thequality of prostate cancer management worldwide.
Refine and reduce the number of quality-of-care indicators thatwere derived from the clinical guideline literature review.
Disclaimer: We acknowledge that there are many important indicators that have not been considered in this panel discussion. Many indicators had to be excluded after the literature review due to the limitations of the PCOR-CRV dataset.

A process for determining consensus on something…It is iterative (one round builds on the next) 3 roundsBegins with an open ended questionnaire to solicit information about a subject Often a large group participate
**The modified Delphi technique is similar to the full Delphi in terms of procedure (i.e., a series of rounds with selected experts) and intent (i.e., to predict future events and to arrive at consensus).
Modified Delphi
What is a Delphi panel?
Delphi Not part of the original Delphi processIt is an iterative process with 3 rounds including a face-to-face meetingBegins with a set of carefully selected items for discussionOnly 9-14 people participateAllows for expert interaction to provide clarification on matters and to present arguments in order to justify their point of viewStudies show it is can be superior to Delphi 3,4

The Delphi panel
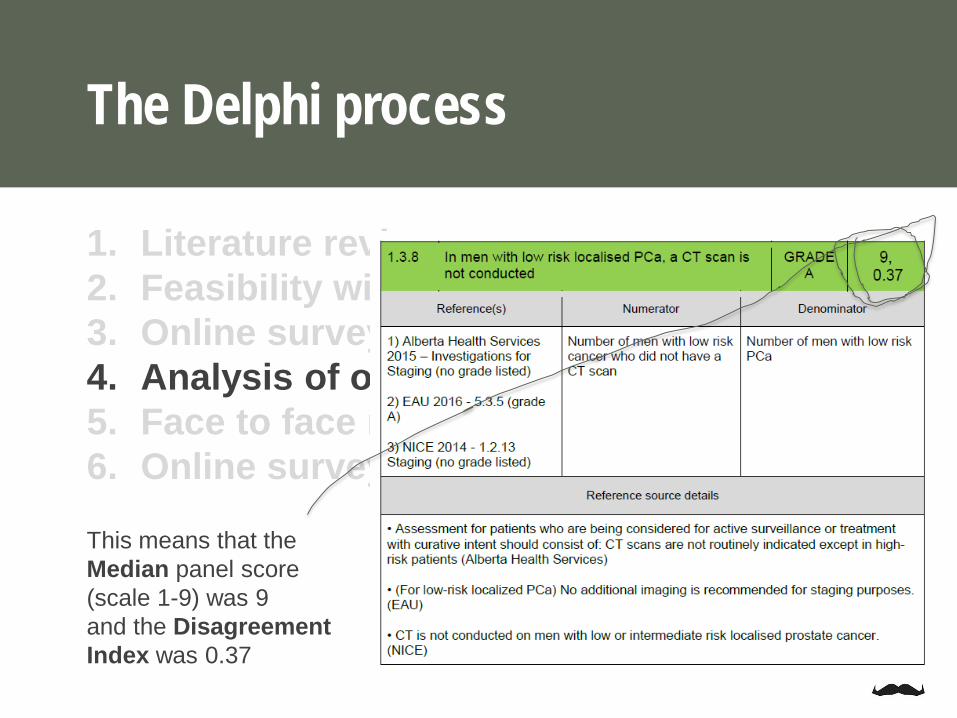
1. Literature review2. Feasibility with existing data3. Online survey 14. Analysis of online survey5. Face to face panel meeting6. Online survey 2
The Delphi process

1. Literature review2. Feasibility with existing data3. Online survey 14. Analysis of online survey5. Face to face panel meeting6. Online survey 2
The Delphi process
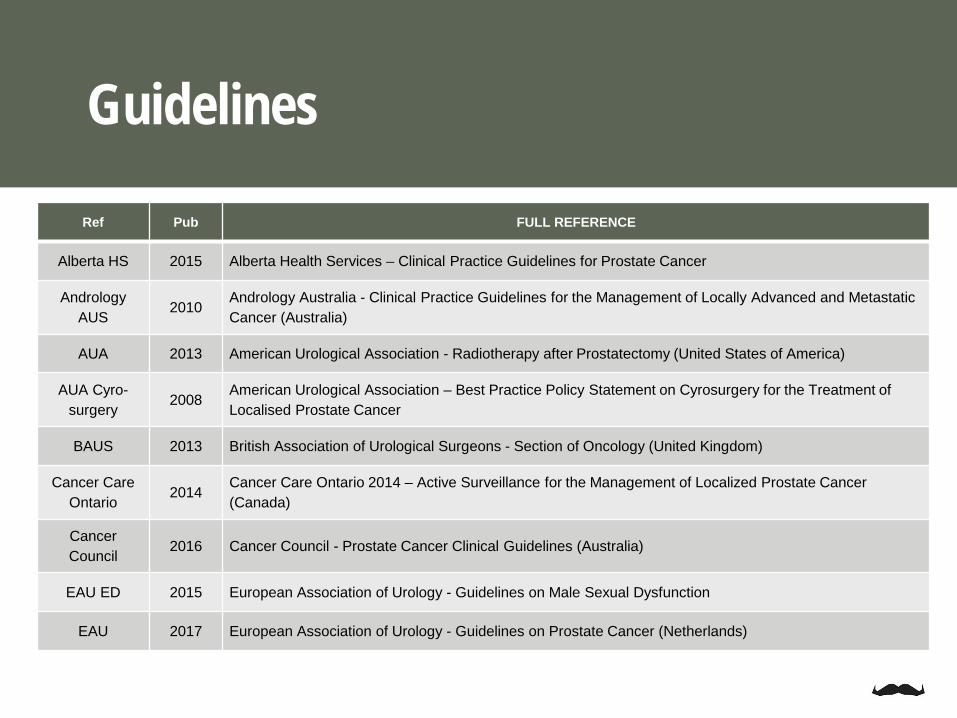
Guidelines
Ref Pub FULL REFERENCE
Alberta HS 2015 Alberta Health Services – Clinical Practice Guidelines for Prostate Cancer
Andrology AUS
2010Andrology Australia - Clinical Practice Guidelines for the Management of Locally Advanced and Metastatic Cancer (Australia)
AUA 2013 American Urological Association - Radiotherapy after Prostatectomy (United States of America)
AUA Cyro-surgery
2008American Urological Association – Best Practice Policy Statement on Cyrosurgery for the Treatment of Localised Prostate Cancer
BAUS 2013 British Association of Urological Surgeons - Section of Oncology (United Kingdom)
Cancer Care Ontario
2014Cancer Care Ontario 2014 – Active Surveillance for the Management of Localized Prostate Cancer (Canada)
Cancer Council
2016 Cancer Council - Prostate Cancer Clinical Guidelines (Australia)
EAU ED 2015 European Association of Urology - Guidelines on Male Sexual Dysfunction
EAU 2017 European Association of Urology - Guidelines on Prostate Cancer (Netherlands)

Guidelines
Ref Year Guideline/ Reference
EAU 2017 European Association of Urology - Guidelines on Prostate Cancer (Netherlands)
ESMO 2015European Society for Medical Oncology - Cancer of the Prostate: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up (Switzerland)
KCE 2014Belgian Health Care Knowledge Centre - National Practice Guideline on the Treatment of Localized Prostate Cancer (Belgium)
NCI 2016 National Cancer Institute - Prostate Cancer Treatment (United States of America)
NCCN 2017National Comprehensive Cancer Network - Clinical Practice Guidelines in Oncology: Prostate Cancer (United States of America)
NCCP 2015 National Cancer Control Programme - Diagnosis, Staging and Treatment of Patients with Prostate Cancer (Ireland)
NCCS 2013 National Cancer Centre Singapore - Guidelines on Management of Prostate Cancer (Singapore)
NICE 2016 National Institute for Health and Care Excellence - Prostate Cancer: Diagnosis and Management (United Kingdom)
NZ PCT 2013 Prostate Cancer Taskforce (New Zealand)
VIC-OCP 2015 Optimal Care Pathway for Men with Prostate Cancer (Victoria, Australia)

ArticlesRef (et al) Year FULL REFERENCE
Ahmadi 2014 Androgen Deprivation Therapy for Prostate Cancer Patient Relat Outcome Meas., 5:63-70
Ahmed 2014Comparison of biochemical failure rates between permanent prostate brachytherapy and radical retropubic prostatectomy as a function of posttherapy PSA nadir plus ‘X’, Radiation Oncology, 9:171
Chin 2015Magnetic Resonance Imaging-Guided Transurethral Ultrasound Ablation or Prostate Tissue in Patients with Localized Prostate Cancer: A Prospective Phase 1 Clinical trial, European Urology, 70:447-455
Loeb 2013 Systematic review of complications of prostate biopsy Eur.Urol., 64 (6), pp. 876–892
Nag 2016 Development of Indicators to Assess Quality of Care for Prostate Cancer. Eur Urol Focus
Punnen 2015Long-Term Health-Related Quality of Life after Primary Treatment for Localized Prostate Cancer: Results from the CaPSURERegistry, European Urology, 68(4):600-608
Ramsay 2015Ablative therapy for People with Localized Prostate Cancer: A Systematic Review and Economic Evaluation - Chapter 4: The Comparative Effectiveness of Cryotherapy, Health Technology Assessment, No. 19.49
Resnick 2013 Long-Term Functional Outcomes after Treatment for Localized Prostate Cancer, N Engl J Med Jan 31;368(5):436-45
Robinson 2009A Randomized Trial of External Beam Radiotherapy versus Cryoblation in Patients with Localized Prostate Cancer Quality of Life Outcomes, Cancer, 115 (20)
Wegner 2014 Laser Ablation as Focal Therapy for Prostate Cancer, Curr Opin Uro, 24(3):236-240
Yap 2016The Effects of Focal Therapy for Prostate Cancer on Sexual Function: A Combined Analysis of Three Prospective Trials, European Urology, 69(5):844-851

1. Literature review2. Feasibility with existing data3. Online survey 14. Analysis of online survey5. Face to face panel meeting6. Online survey 2
The Delphi process

Which indicators to include
1. Those where there is a high level of agreement among the panel that it is a good indicator
• = Median score
2. Those where there is little disagreement (dispersion) among the panel that it is a good indicator
• = Disagreement Index (DI)

The Delphi process
Median score 7-9 and no disagreement (DI<1)
Any disagreement regardless of median score (DI≥1)
Median score 1-6 and no disagreement
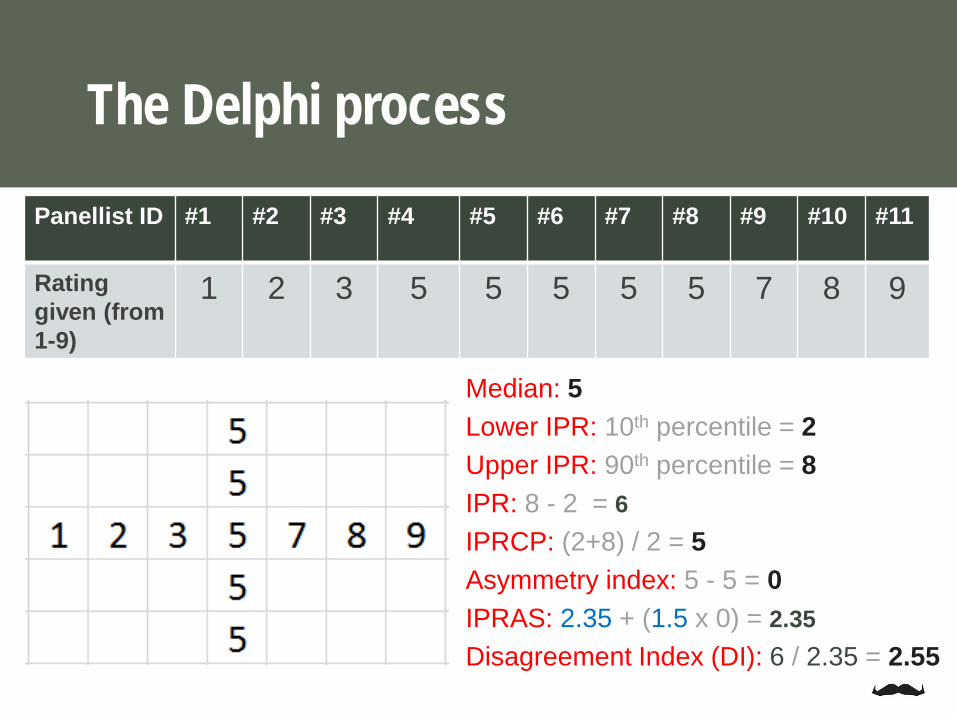
Panellist ID #1 #2 #3 #4 #5 #6 #7 #8 #9 #10 #11
Ratinggiven (from 1-9)
1 2 3 5 5 5 5 5 7 8 9
Median: 5Lower IPR: 10th percentile = 2 Upper IPR: 90th percentile = 8IPR: 8 - 2 = 6IPRCP: (2+8) / 2 = 5Asymmetry index: 5 - 5 = 0IPRAS: 2.35 + (1.5 x 0) = 2.35Disagreement Index (DI): 6 / 2.35 = 2.55
The Delphi process
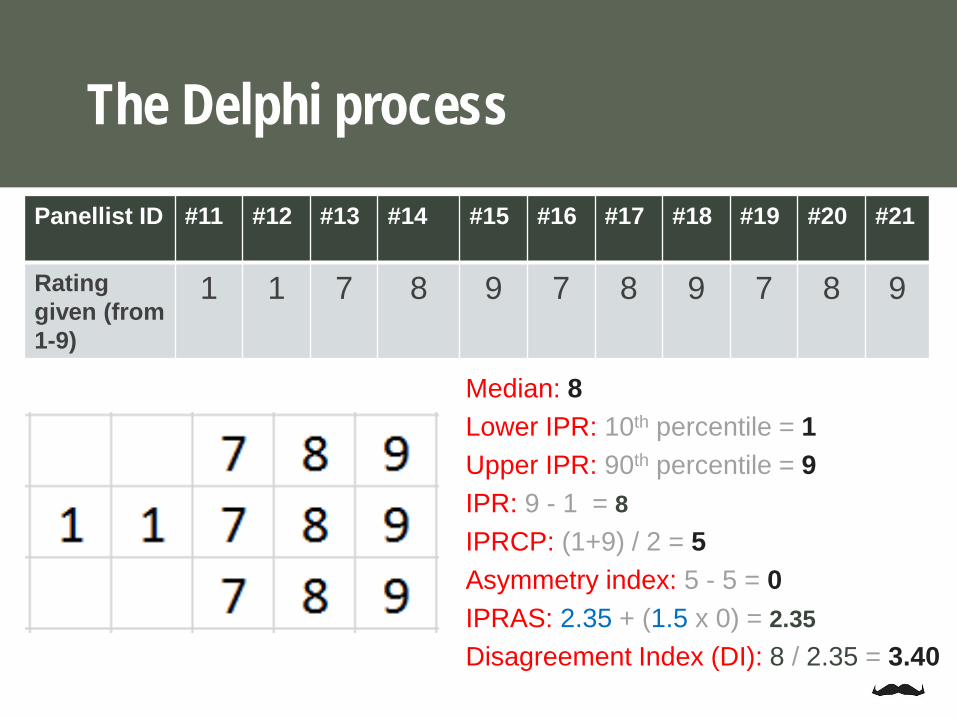
Panellist ID #11 #12 #13 #14 #15 #16 #17 #18 #19 #20 #21
Ratinggiven (from 1-9)
1 1 7 8 9 7 8 9 7 8 9
Median: 8Lower IPR: 10th percentile = 1 Upper IPR: 90th percentile = 9IPR: 9 - 1 = 8IPRCP: (1+9) / 2 = 5Asymmetry index: 5 - 5 = 0IPRAS: 2.35 + (1.5 x 0) = 2.35Disagreement Index (DI): 8 / 2.35 = 3.40
The Delphi process
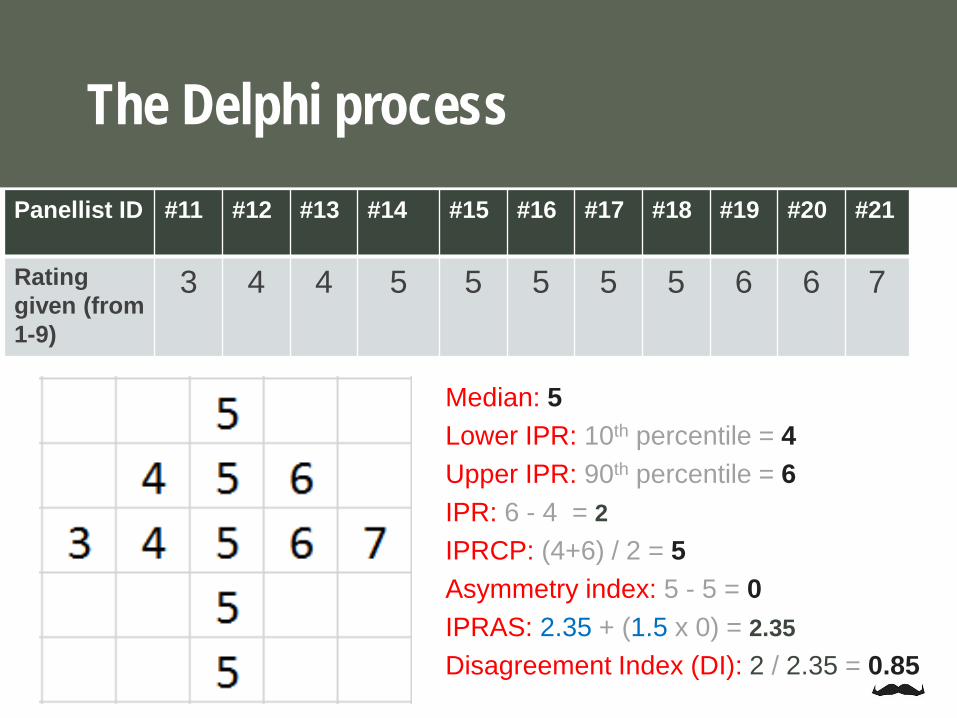
Panellist ID #11 #12 #13 #14 #15 #16 #17 #18 #19 #20 #21
Ratinggiven (from 1-9)
3 4 4 5 5 5 5 5 6 6 7
Median: 5Lower IPR: 10th percentile = 4 Upper IPR: 90th percentile = 6IPR: 6 - 4 = 2IPRCP: (4+6) / 2 = 5Asymmetry index: 5 - 5 = 0IPRAS: 2.35 + (1.5 x 0) = 2.35Disagreement Index (DI): 2 / 2.35 = 0.85
The Delphi process
1. Literature review2. Feasibility with existing data3. Online survey 14. Analysis of online survey5. Face to face meeting6. Online survey 2
The Delphi process
This means that the Median panel score (scale 1-9) was 9 and the Disagreement Index was 0.37
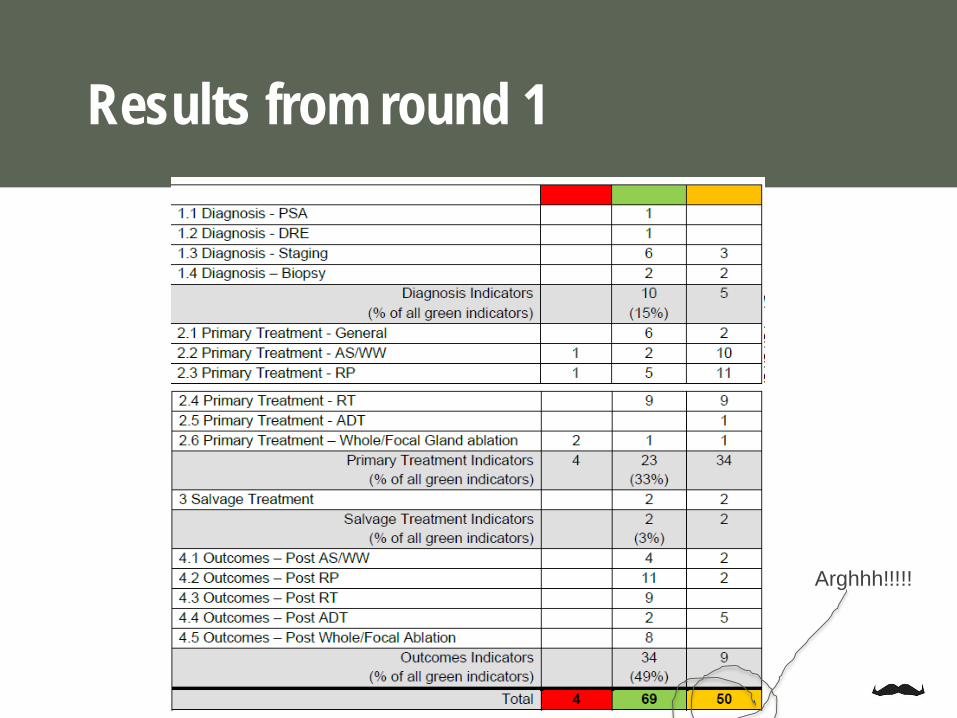
Results from round 1
Arghhh!!!!!

1. Literature review2. Feasibility with existing data3. Online survey 14. Analysis of online survey5. Face to face panel meeting6. Online survey 2
The Delphi process
Vancouver

Rated importance AND feasibility (scale 1-9)
Face to face meeting
The Delphi process

The Delphi process

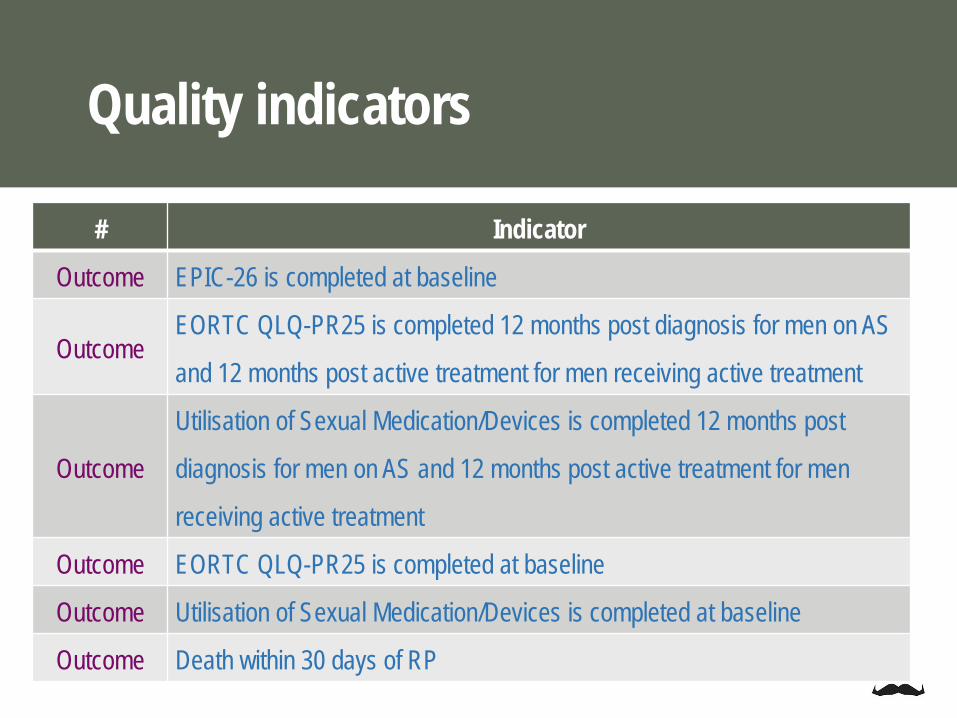
Quality indicators
# Indicator
DiagInitial investigations of a male with PCa include measurement of
PSA level
DiagT category/stage (DRE or MRI) is documented prior to treatment for
localised PCa
DiagIn men with high risk localised PCa, nodal staging using CT, MRI or
PET/CT is performed
DiagIn men with high risk localised PCa, perform metastatic screening
using a CT/MRI and a bone scan
DiagIn men with intermediate risk localised PCa, a bone scan is not
conducted

# Indicator
Diag In men with low risk PCa, a bone scan is not conducted
Diag In men with low risk localised PCa, a CT is not conducted
Primary Rx Men with high risk localised PCa receive active treatment
Primary Rx Men with high risk localised PCa do not receive AS
Primary Rx PSA is taken within 3 months post RP
Primary Rx For pN0 men undergoing RP, adjuvant ADT is not given
Quality indicators
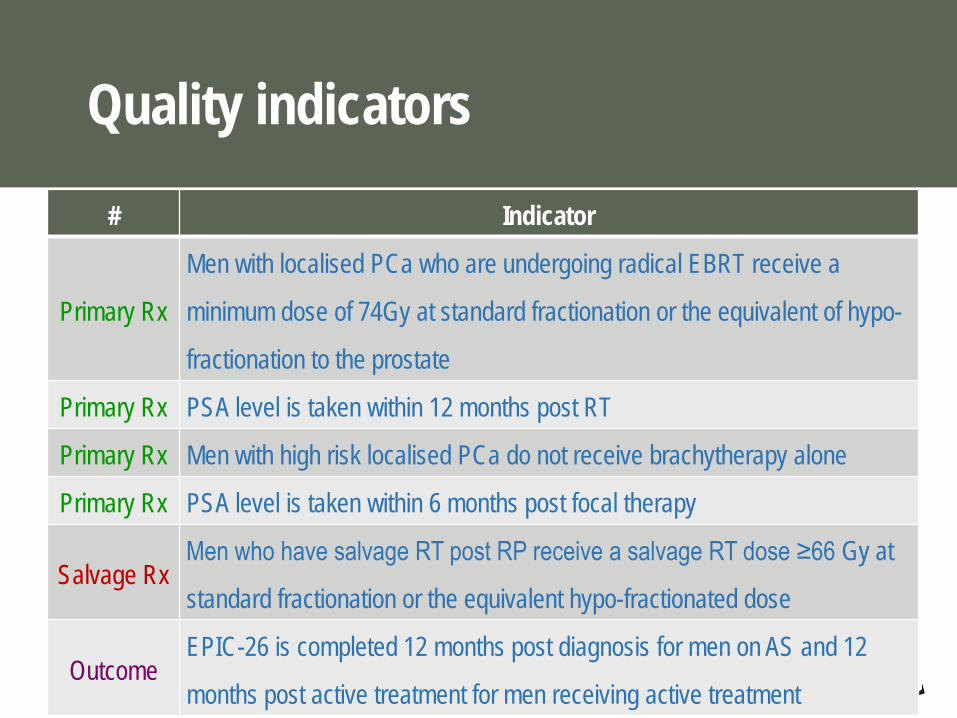
# Indicator
Primary Rx
Men with localised PCa who are undergoing radical EBRT receive a
minimum dose of 74Gy at standard fractionation or the equivalent of hypo-
fractionation to the prostate
Primary Rx PSA level is taken within 12 months post RT
Primary Rx Men with high risk localised PCa do not receive brachytherapy alone
Primary Rx PSA level is taken within 6 months post focal therapy
Salvage RxMen who have salvage RT post RP receive a salvage RT dose ≥66 Gy at
standard fractionation or the equivalent hypo-fractionated dose
OutcomeEPIC-26 is completed 12 months post diagnosis for men on AS and 12
months post active treatment for men receiving active treatment
Quality indicators
# Indicator
Outcome EPIC-26 is completed at baseline
OutcomeEORTC QLQ-PR25 is completed 12 months post diagnosis for men on AS
and 12 months post active treatment for men receiving active treatment
Outcome
Utilisation of Sexual Medication/Devices is completed 12 months post
diagnosis for men on AS and 12 months post active treatment for men
receiving active treatment
Outcome EORTC QLQ-PR25 is completed at baseline
Outcome Utilisation of Sexual Medication/Devices is completed at baseline
Outcome Death within 30 days of RP
Quality indicators

# Indicator
Outcome Men with low risk PCa who had a positive margin post-RP
Outcome Men with pT2 disease who had a positive margin post-RP
Outcome Men with pT3 disease who had a positive margin post-RP
Outcome Biochemical recurrence at 1 year post RP
OutcomeRadical or systemic treatment at 18 months post focal-gland or
whole-gland ablation therapy
Quality indicators

1. Publish findings2. Build the reports3. Test and refine the indicators 4. Develop reports 5. Distribute reports to LDCs 6. LDCs will distribute reports to participating sites
Next steps…
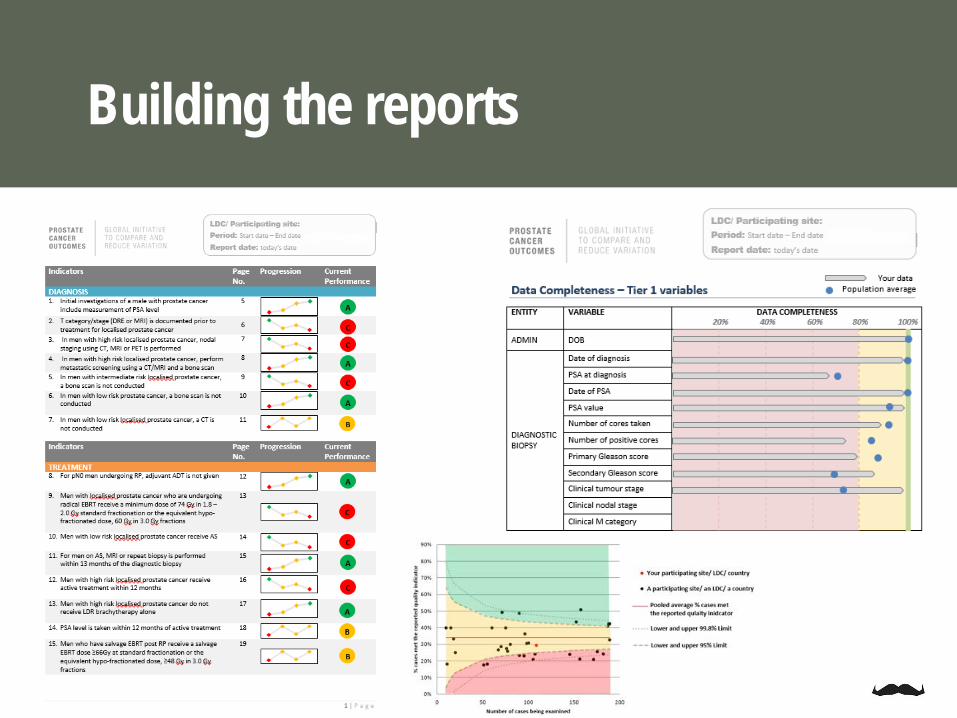
Building the reports

PCO-CRV Monash/Movember teamFanny SampurnoJeremy MillarJia ZhengEllie JamesAshwini KannonHarvey Goh
Acknowledgement
PCO-CRV UCLA teamSarah ConnorMark LitwinEmily Pearman
Delphi panel
TrueNTH Steering Committee
Contributors to the registry
PCOR-Vic and ANZ teamMelanie EvansGabriella TikellisData collector and follow up team

Funding bodies
Acknowledgement
Endorsing groups
Thank youPCOR-Vic Steering Committee
Contributing clinicians and hospitals
Participating men
PCOR-Vic data collectors and researchers

Questions?


















