
GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG...
49
GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE (GOLD) TEACHING SLIDE SET 2019 This slide set is restricted for academic and educational purposes only. Use of the slide set, or of individual slides, for commercial or promotional purposes requires approval from GOLD. © 2019 Global Initiative for Chronic Obstructive Lung Disease
Transcript of GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG...

GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE (GOLD)
TEACHING SLIDE SET 2019
This slide set is restricted for academic and educational purposes only. Use of the slide set, or of individual slides, for commercial or promotional purposes
requires approval from GOLD.
© 2019 Global Initiative for Chronic Obstructive Lung Disease

Perubahan
Wanita prevalensi banyak indoor
Kemiskinan
HIV risk factor
Electronic health record
Active case finding
Eosinofil
Vacin
LABA/LAMA low exacerbation
Individualized

Reasses
Eskalasi dan deeskalasi
Budesonid monoterapi untuk eksaserbasi
GOLD 2017 Report: Chapters
© 2017 Global Initiative for Chronic Obstructive Lung Disease
1. Definition and Overview
2. Diagnosis and Initial Assessment
3. Evidence Supporting Prevention
& Maintenance Therapy
4. Management of Stable COPD
5. Management of Exacerbations
6. COPD and Comorbidities

GOLD 2017 Report: Chapters
© 2017 Global Initiative for Chronic Obstructive Lung Disease
1. Definition and Overview
2. Diagnosis and Initial Assessment
3. Evidence Supporting Prevention
& Maintenance Therapy
4. Management of Stable COPD
5. Management of Exacerbations
6. COPD and Comorbidities

Definisi dan overview
© 2018 Global Initiative for Chronic Obstructive Lung Disease
► Penyakit paru obstruktif kronik (PPOK) adalah
penyakit yang umum, dapat dicegah dan diobati
ditandai dengan gejala respirasi yang persisten
dan obstruksi saluran napas (SN) disebabkan
karena kelainan pada SN dan/atau alveolar yang
biasanya akibat dari pajanan partikel atau gas
berbahaya yang signifikan

Definisi and Overview
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Gejala respirasi yang paling sering
adalah sesak, batuk dan/atau produksi
sputum
►Faktor risiko utama adalah rokok akan
tetapi bisa bahan bakar biomass

PPOK, Etiologi, Patobiologi & Patologi
© 2017 Global Initiative for Chronic Obstructive Lung Disease

Definisi dan Overview
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Faktor individual-host : genetik,
pertumbuhan paru dan penuaan
►PPOK ditekankan pada eksaserbasi
►Ko-morbid meningkatkan risiko
morbiditas dan mortalitas

Progresivitas PPOK
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Genetik
►Umur dan jenis kelamin
►Tumbuh kembang paru
►Pajanan partikel
►Status sosioekonomik
►Asma & airway hyper-reactivity
►Bronkitiskronik dan infeksi

Patologi, patogenesis & patofisiologi
© 2017 Global Initiative for Chronic Obstructive Lung Disease
► Patologi
Inflamasi kronik dan Perubahan struktur
► Patogenesis
Stres oksidatif
Imbalans protease-antiprotease
Sel-sel inflamasi
Fibrosisi peribronkiolar & interstisiel
► Patofisiologi
Obstruksi SN dan gas trapping
Abnormal pertukaran
Hipersekresi mukus
Hipertensi pulmonal

GOLD 2017 Report: Chapters
© 2017 Global Initiative for Chronic Obstructive Lung Disease
1. Definition and Overview
2. Diagnosis and Initial Assessment
3. Evidence Supporting Prevention
& Maintenance Therapy
4. Management of Stable COPD
5. Management of Exacerbations
6. COPD and Comorbidities

Diagnosis dan Asesmen awal
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Curigai PPOK : sesak, batuk kronik/produktif
sputum , dan/atau terpajanan faktor risiko
►Spirometri diagnosis; FEV1/FVC < 0.70 pasca BD
memastikan airflow limitation yang persisten
►Tujuan penilaian PPOK : derajat , status kesehatan,
dan risiko kejadian tidak diinginkan
Diagnosis dan Asesmen Awal
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Ko-morbid : disfungsi otot skeletal, sindrom
metabolik, osteoporosis, depresi,
kecemasan osteoporos, dan kanker paru
►Ko-morbid harus proaktif dan diobati
dengan tepat

Diagnosis dan Asesmen Awal
© 2017 Global Initiative for Chronic Obstructive Lung Disease

Diagnosis dan Asesmen Awal
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Simtom PPOK
Sesak kronik dan progresif
Batuk
Produksi sputum
Wheezing dan chest tightness
Lain-lain- kelelahan, penurunan
BB, anoreksia, edema tungkai,
depresi, kecemasan

Anamnesis
© 2017 Global Initiative for Chronic Obstructive Lung Disease
► Pasien terpajan faktor risiko
► Riwayat medis yang lalu
► Riwayat PPOK keluarga atau penyakit resprasi kronik
► Pola simtom pasien
► Riwayat eksaserbasi atau rawat inap sebelumnya karena
kelainan respirasi
► Riwayat komorbiditas
► Dampak pada kehidupan sehari-hari
► Dukungan sosial dan keluarga

Classification of severity of airflow limitation
© 2017 Global Initiative for Chronic Obstructive Lung Disease
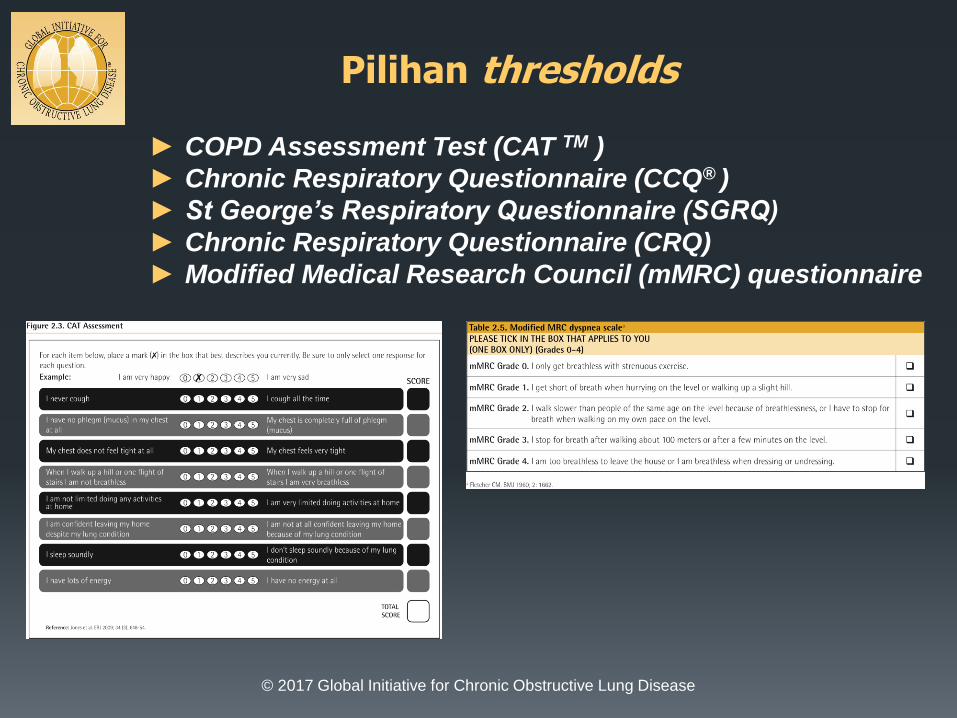
Pilihan thresholds
© 2017 Global Initiative for Chronic Obstructive Lung Disease
► COPD Assessment Test (CAT TM )
► Chronic Respiratory Questionnaire (CCQ® )
► St George’s Respiratory Questionnaire (SGRQ)
► Chronic Respiratory Questionnaire (CRQ)
► Modified Medical Research Council (mMRC) questionnaire

Asesmen Risiko Eksaserbasi
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Definisi eksaserbasi: perburukan akut atas
simtom sehingga penambahan terapi .
►Kllasifikasi eksaserbasi :
Ringan (cukup hanya dengan SABDs )
Sedang (SABDs plus antibiotik dan/atau
kortikosteroids oral) atau
Berat (harus mrs atau ke IGD). Eksaserbasi
berat mungkin disertai gagal napas akut
►Eosinofil darah memrediksi eksaserbasi (pada
LABA tanpa ICS)

Asesmen ABCD
© 2017 Global Initiative for Chronic Obstructive Lung Disease

Asesmen ABCD
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Contoh
►Ada 2 pasien (I dan II):
FEV1 < 30% predikted
Skor CAT 18
Pasien I tanpa eksaserbasi setahun yang
lalu, dan pasien II 3 x eksaserbasi
► I dan II masuk grup D (2016). Skema baru,
Pasien II, 3 x eksaserbasi , GOLD grade 4, grup
D
►Pasien I, GOLD grade 4, group B

GOLD 2017 Report: Chapters
© 2017 Global Initiative for Chronic Obstructive Lung Disease
1. Definition and Overview
2. Diagnosis and Initial Assessment
3. Evidence Supporting Prevention
& Maintenance Therapy
4. Management of Stable COPD
5. Management of Exacerbations
6. COPD and Comorbidities

Bukti Pendukung Prevensi & Terapi Pemeliharaan
© 2017 Global Initiative for Chronic Obstructive Lung Disease
► Stop rokok merupakan kunci utama
► Efektivitas dan keamanan rokok elektronik tidak tentu
► Terapi farmakologik memperbaiki simtom , mengurangi
frekuensi dan keparahan eksaserbasi dan memperbaiki status
kesehatan serta toleransi latihan
► Terapi farmakologik, individual dan didasarkan pada risiko
eksaserbasi, efek samping, komorbid, ketersediaan obat dan
beaya, dan respons pasien, kesukaan dan kemampuan memakai
obat inhaler .

Bukti Pendukung Prevensi & Terapi Pemeliharaan
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Vaksin influenza menurunkan insidens ISPB
►Vaksin Pneumococus menurunkan ISPB
►Rehabilitasi paru memperbaiki simtom, kualitas hidup
dan aktivitas fisik maupun emosi sehari-hari
►LTOT memperbaiki survival
►Desaturasi, LTOT harus rutin, respons individual perlu
Bukti Pendukung Prevensi & Terapi Pemeliharaan
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►NIV menurunkan mortalitas & re-hospitalisasi
►Emfisema refraktori berat, pembedahan dan FOB
►Paliatif efektif untuk mengontrol simtom PPOK berat

Bronkodilator pada PPOK Stabil
© 2017 Global Initiative for Chronic Obstructive Lung Disease

GOLD 2017 Report: Chapters
© 2017 Global Initiative for Chronic Obstructive Lung Disease
1. Definition and Overview
2. Diagnosis and Initial Assessment
3. Evidence Supporting Prevention
& Maintenance Therapy
4. Management of Stable COPD
5. Management of Exacerbations
6. COPD and Comorbidities

Managemen PPOK Stabil
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Managemen PPOK stabil berbasis ABCD
►Stop rokok
►Terapi: simtom dan eksaserbasi
►Strategi : farmakologik & non-farmakologik

© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Diagnosis PPOK tegak, mulai managemen berbasis
penilaian individual atas simtom dan risiko
Managemen PPOK Stabil

© 2017 Global Initiative for Chronic Obstructive Lung Disease
Identifikasi dan turunkan pajanan atas faktor risiko
►Penting untuk terapi dan prevensi
►Program berhenti merokok
►Mengurangi pajanan faktor risiko
Managemen PPOK Stabil

Pengobatan PPOK Stabil
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Farmakologik
►Perbaikan simtom, penurunan risiko eksaserbasi,
perbaikan status kesehatan dan toleransi latihan
►Teknik penggunaan inhaler yang benar sangat relevan


Pengobatan PPOK Stabil
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Pharmacologic treatment

Pengobatan PPOK Stabil
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Algoritme pengobatan farmakologik
► Inisiasi, eskalasi dan/atau de-eskalasi berdasarkan
asesmen atas simtom dan risiko eksaserbasi
►Rekomendasi berbasis data efikasi dan keamanan
►Group C dan D tak ada bukti pendukung langsung

Treatment of Stable COPD
© 2017 Global Initiative for Chronic Obstructive Lung Disease

Treatment of stable COPD
© 2017 Global Initiative for Chronic Obstructive Lung Disease © 2019 Global Initiative for Chronic Obstructive Lung Disease
Definition of abbreviations: eos: blood eosinophil count in cells per microliter; mMRC: modified Medical Research
Council dyspnea questionnaire; CAT™: COPD Assessment Test™.

Group A
© 2017 Global Initiative for Chronic Obstructive Lung Disease © 2019 Global Initiative for Chronic Obstructive Lung Disease
► All Group A patients should be offered bronchodilator treatment based on its effect on breathlessness. This can be either a short- or a long-acting bronchodilator.
► This should be continued if benefit is documented.

Group B
© 2017 Global Initiative for Chronic Obstructive Lung Disease © 2019 Global Initiative for Chronic Obstructive Lung Disease
► Initial therapy should consist of a long acting bronchodilator
(LABA or LAMA).
► Long-acting inhaled bronchodilators are superior to short-acting
bronchodilators taken as needed i.e., pro re nata (prn) and are
therefore recommended.

Group C
© 2017 Global Initiative for Chronic Obstructive Lung Disease © 2019 Global Initiative for Chronic Obstructive Lung Disease
► Initial therapy should consist of a single long acting bronchodilator.
► In two head-to-head comparisons the tested LAMA was superior to the LABA regarding exacerbation prevention therefore we recommend starting therapy with a LAMA in this group.

Group D
© 2017 Global Initiative for Chronic Obstructive Lung Disease © 2019 Global Initiative for Chronic Obstructive Lung Disease
► In general, therapy can be started with a LAMA as it has effects on both breathlessness and exacerbations.
► For patients with more severe symptoms (order of magnitude of CAT™ ≥ 20), especially driven by greater dyspnea and/or exercise limitation, LAMA/LABA may be chosen as initial treatment based on studies with patient reported outcomes as the primary endpoint where LABA/LAMA combinations showed superior results compared to the single substances.
► An advantage of LABA/LAMA over LAMA for exacerbation prevention has not been consistently demonstrated, so the decision to use LABA/LAMA as initial treatment should be guided by the level of symptoms.
Treatment of stable COPD
© 2017 Global Initiative for Chronic Obstructive Lung Disease © 2019 Global Initiative for Chronic Obstructive Lung Disease
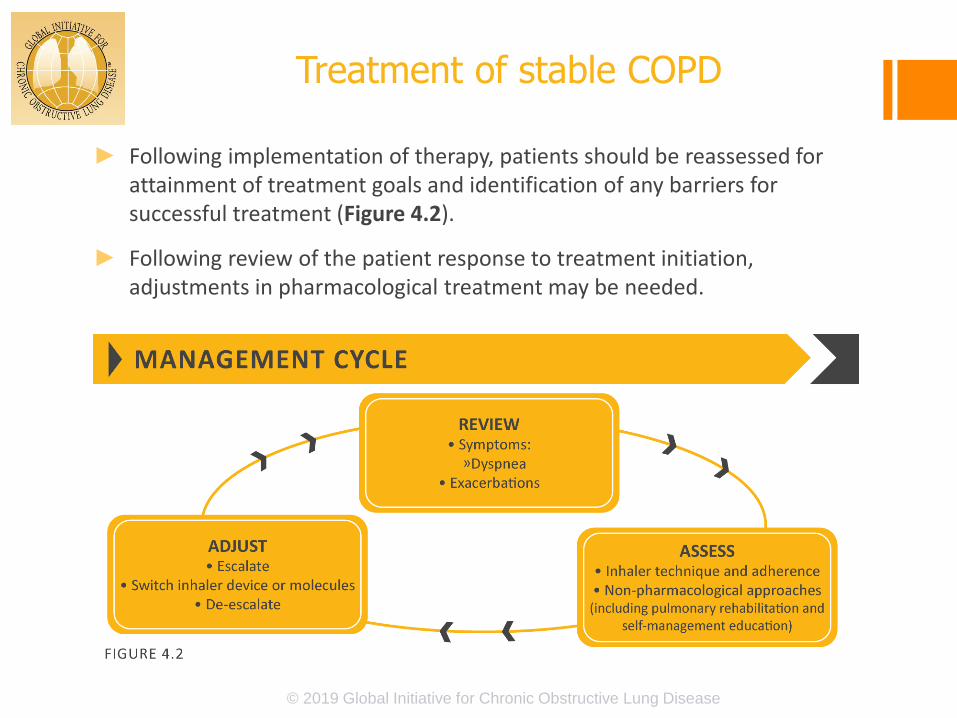
► Following implementation of therapy, patients should be reassessed for attainment of treatment goals and identification of any barriers for successful treatment (Figure 4.2).
► Following review of the patient response to treatment initiation, adjustments in pharmacological treatment may be needed.

© 2017 Global Initiative for Chronic Obstructive Lung Disease © 2019 Global Initiative for Chronic Obstructive Lung Disease

Monitoring dan Follow-up
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Pengukuran : cek FEV1/tahun
►Simptom: catat simtom, aktivitas dan pola tidur
►Eksaserbasi: frekuensi, keparahan, tipe dan kausa
► Imaging : perburukan simtom
►Status merokok

Monitoring dan Follow-up
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Monitoring harus berfokus pada :
► Dosis obat yang diberikan
► Kepatuhan/penerimaan regimen
► Teknik inhalasi
► Efektivitas regimen mutakhir
► Efek samping
Direkomendasi terapi modifikasi

GOLD 2017 Report: Chapters
© 2017 Global Initiative for Chronic Obstructive Lung Disease
1. Definition and Overview
2. Diagnosis and Initial Assessment
3. Evidence Supporting Prevention
& Maintenance Therapy
4. Management of Stable COPD
5. Management of Exacerbations
6. COPD and Comorbidities

Management of Exacerbations
Pharmacological treatment
The three classes of medications most commonly used for COPD exacerbations are:
► Bronchodilators Although there is no high-quality evidence from RCTs, it is recommended that
short-acting inhaled beta2-agonists, with or without short-acting anticholinergics, are the initial bronchodilators for acute treatment of a COPD exacerbation.
► Corticosteroids Data from studies indicate that systemic glucocorticoids in COPD exacerbations
shorten recovery time and improve lung function (FEV1). They also improve oxygenation, the risk of early relapse, treatment failure, and the length of hospitalization.
► Antibiotics

© 2017 Global Initiative for Chronic Obstructive Lung Disease © 2019Global Initiative for Chronic Obstructive Lung Disease

103
TERIMA KASIH


















