
Given Every 21 Days in Patients with Advanced Solid...
27
Phase I Study of Pazopanib in Combination with Paclitaxel and Carboplatin Given Every 21 Days in Patients with Advanced Solid Tumors Howard A. Burris III 1 , Afshin Dowlati 2 , Rebecca A. Moss 3 , Jeffrey R. Infante 1 , Suzanne F. Jones 1 , David R. Spigel 1 , Kelly T. Levinson 3 , Diana Lindquist 3 , Shelby D. Gainer 4 , Mohammed M. Dar 4 , A. Benjamin Suttle 4 , Howard A. Ball 4 , Antoinette R.Tan 3 1 Sarah Cannon Research Institute, Nashville, TN; 2 Case Western Reserve University, Cleveland, OH; 3 The Cancer Institute of New Jersey, New Brunswick, NJ; 4 GlaxoSmithKline, Research Triangle Park, NC, and Upper Providence, PA Running Title: Phase I study of pazopanib, paclitaxel, and carboplatin Keywords: pazopanib, paclitaxel, carboplatin, phase I, pharmacokinetics Abbreviations: ANOVA, analysis of variance; AUC (0-23) , area under the curve from 0 to 23 hours; AUC5, dosed at area under the curve 5 (carboplatin); AUC6, dosed at area under the curve 6 (carboplatin); CI, confidence interval; C max , maximal concentration; DLT, dose-limiting toxicity; ECOG, Eastern Cooperative Oncology Group; MTR, maximum tolerated regimen; NSCLC, non-small-cell lung cancer; VEGF and VEGFR, vascular endothelial growth factor and VEGF receptor. Financial/Grant Support: This study was funded by GlaxoSmithKline Pharmaceuticals. Standard study-related costs to all investigators were supported, and no funding was provided to investigators. Corresponding Author: Howard A. Burris III, MD Sarah Cannon Research Institute 250 25th Ave North, Suite 110 Nashville, TN 37203-1632 Phone: 615-320-5090 Facsimile: 615-320-1225 E-mail: [email protected] Disclosure of Potential Conflicts of Interest: H.A. Burris, A. Dowlati, R.A. Moss, J.R. Infante, S.F. Jones, D.R. Spigel, K.T. Levinson, D. Lindquist, and A.R. Tan report no relevant financial relationships. Previous Publication: Portions of the data were presented at the 2009 AACR-NCI-EORTC International Conference on Molecular Targets and Cancer Therapeutics (abstract A6). Word Counts: Text only (limit 5,000 words) = 3,043 Abstract (limit: 250 words) = 242 Number of Figures/Tables (limit 6 total): 6 Number of References (limit 50): 26 on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997
Transcript of Given Every 21 Days in Patients with Advanced Solid...

Phase I Study of Pazopanib in Combination with Paclitaxel and Carboplatin Given Every 21 Days in Patients with Advanced Solid Tumors
Howard A. Burris III1, Afshin Dowlati2, Rebecca A. Moss3, Jeffrey R. Infante1, Suzanne F. Jones1, David R. Spigel1, Kelly T. Levinson3, Diana Lindquist3, Shelby D. Gainer4, Mohammed
M. Dar4, A. Benjamin Suttle4, Howard A. Ball4, Antoinette R.Tan3
1Sarah Cannon Research Institute, Nashville, TN; 2Case Western Reserve University, Cleveland, OH; 3The Cancer Institute of New Jersey, New Brunswick, NJ;
4GlaxoSmithKline, Research Triangle Park, NC, and Upper Providence, PA
Running Title: Phase I study of pazopanib, paclitaxel, and carboplatin
Keywords: pazopanib, paclitaxel, carboplatin, phase I, pharmacokinetics
Abbreviations: ANOVA, analysis of variance; AUC(0-23), area under the curve from 0 to 23 hours; AUC5, dosed at area under the curve 5 (carboplatin); AUC6, dosed at area under the curve 6 (carboplatin); CI, confidence interval; Cmax, maximal concentration; DLT, dose-limiting toxicity; ECOG, Eastern Cooperative Oncology Group; MTR, maximum tolerated regimen; NSCLC, non-small-cell lung cancer; VEGF and VEGFR, vascular endothelial growth factor and VEGF receptor.
Financial/Grant Support: This study was funded by GlaxoSmithKline Pharmaceuticals. Standard study-related costs to all investigators were supported, and no funding was provided to investigators.
Corresponding Author: Howard A. Burris III, MD Sarah Cannon Research Institute 250 25th Ave North, Suite 110 Nashville, TN 37203-1632 Phone: 615-320-5090 Facsimile: 615-320-1225 E-mail: [email protected]
Disclosure of Potential Conflicts of Interest: H.A. Burris, A. Dowlati, R.A. Moss, J.R. Infante, S.F. Jones, D.R. Spigel, K.T. Levinson, D. Lindquist, and A.R. Tan report no relevant financial relationships.
Previous Publication: Portions of the data were presented at the 2009 AACR-NCI-EORTC International Conference on Molecular Targets and Cancer Therapeutics (abstract A6).
Word Counts: Text only (limit 5,000 words) = 3,043 Abstract (limit: 250 words) = 242 Number of Figures/Tables (limit 6 total): 6 Number of References (limit 50): 26
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 2
ABSTRACT
Several phase III trials have demonstrated that the addition of an antiangiogenic agent to
conventional chemotherapy can improve clinical benefit in patients with advanced solid tumors.
This study examined the feasibility of combining pazopanib (Votrient), an oral antiangiogenic
agent, with paclitaxel and carboplatin. This 3 + 3 dose-escalation phase I study evaluated the
maximum tolerated regimen (MTR) of daily pazopanib in combination with paclitaxel 175 mg/m2
and carboplatin (dosed at area under the curve [AUC] 5 or 6) given every 21 days in patients
with advanced solid tumors. Plasma samples were collected to evaluate the effect of pazopanib
on the pharmacokinetics of paclitaxel and carboplatin. Thirty-four patients were enrolled. The
MTR was paclitaxel 175 mg/m2 and carboplatin AUC5 with pazopanib 200 mg. The most
common dose-limiting toxicities were neutropenia and thrombocytopenia. Two patients with
esophageal cancer had a complete response and four patients, one each with breast, small-cell
lung, pancreatic, and gastroesophageal junction cancer, had partial responses. Pazopanib at
200 mg increased paclitaxel maximal concentration (Cmax) by 43% and carboplatin (AUC5 or
AUC6) Cmax by 54%. Paclitaxel and carboplatin given every 21 days at standard doses was not
feasible in combination with the monotherapy pazopanib dose of 800 mg daily because of dose-
limiting myelosuppression. Coadministration of pazopanib increased exposure to paclitaxel and
carboplatin and likely contributed to this effect. Given the antitumor activity of this regimen,
further studies are underway to determine a clinically tolerable schedule of pazopanib with
paclitaxel and carboplatin.
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 3
INTRODUCTION
Angiogenesis is an important process for tumor growth (1,2). Therefore, the addition of
angiogenesis inhibitors to chemotherapy is a potential approach to enhance antitumor activity.
In addition to inhibiting tumor-mediated angiogenesis, antiangiogenic agents may normalize
“leaky” tumor vasculature and increase the delivery of chemotherapy agents to the tumor site
and enhance their efficacy (3). The addition of bevacizumab (Avastin), an anti-vascular
endothelial growth factor (VEGF) antibody, to chemotherapy has been shown to improve clinical
benefit in several tumor types, including metastatic colon cancer (4,5), non-small-cell lung
cancer (NSCLC) (6), and breast cancer (7,8).
Pazopanib (Votrient) is an oral agent that inhibits the tyrosine kinases of the VEGF
receptor (VEGFR), platelet-derived growth factor receptor, and c-Kit (9). Pazopanib given at 800
mg once daily has demonstrated single-agent activity in multiple tumor types (10-15), and is
approved for the treatment of advanced renal cell carcinoma in the United States and other
countries. The multikinase activity of pazopanib may potentially improve tumor control
compared with other angiogenesis inhibitors such as bevacizumab, which targets a single
component of the angiogenesis pathway. Paclitaxel combined with carboplatin is a common
chemotherapy backbone for the treatment of NSCLC and ovarian cancer (16,17). This phase I
study explored the feasibility and efficacy of adding daily pazopanib to the combination of
paclitaxel and carboplatin given every 21 days in patients with advanced solid tumors.
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 4
METHODS
Patients
Eligible patients had a confirmed histologic or cytologic diagnosis of cancer, an Eastern
Cooperative Oncology Group (ECOG) performance status of 0 or 1, adequate bone marrow,
renal, and hepatic function as well as peripheral neuropathy of grade 1 or less. Patients with
more than three lines of prior chemotherapy for metastatic disease, poorly controlled
hypertension, prolonged QTc interval (≥ 470 msec), heart failure, a history of bleeding within 6
weeks of study entry, current use of warfarin at therapeutic doses, or central nervous system
metastases were excluded. The study protocol was approved by the institutional review board at
each site and was conducted according to the Declaration of Helsinki. All patients gave written
informed consent.
Study Design
This was a phase I, multicenter, open-label, dose-finding study (VEGF105427, clinical
trial registration identifier NCT00388076) with a 3 + 3 design that was expanded at the
maximum tolerated regimen (MTR). Cohorts of patients were treated with paclitaxel in
combination with carboplatin and daily pazopanib (Figure 1A). The MTR was defined as the
maximum dose level at which no more than one of six patients experienced a dose-limiting
toxicity (DLT) during Cycle 1. A DLT was defined as grade 3 or 4 clinically significant non-
hematologic toxicity (excluding alopecia or grade 3 nausea/vomiting in the absence of
supportive therapy), hypertension (grade 3 not adequately controlled with medication),
proteinuria (grade 3 persisting > 3 weeks with no improvement to below grade 2 after
discontinuation of pazopanib), febrile neutropenia, grade 4 thrombocytopenia or
granulocytopenia lasting beyond 5 days with or without fever, and any grade 2 toxicity
considered a DLT in the judgment of the investigator and sponsor. Additionally, the inability to
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 5
begin the next course of treatment within 2 weeks of scheduled dosing because of unresolved
toxicity was considered a DLT.
Secondary endpoints included the effect of pazopanib on the pharmacokinetics of
paclitaxel and carboplatin (clearance and maximal concentration [Cmax] for paclitaxel; area under
the curve from 0 to 23 hours [AUC(0-23)] and Cmax for carboplatin) and the clinical activity of the
combination therapy. The pharmacokinetic parameters for pazopanib included Cmax.
Treatment
A phase I trial had previously shown that administration of pazopanib at 800 mg once
daily reduced paclitaxel clearance by approximately 14% (18). Therefore, paclitaxel 175 mg/m2
and carboplatin area under the curve 6 (AUC6) administered intravenously every 21 days and
pazopanib 800 mg once daily were chosen as the starting doses to achieve a predicted
systemic exposure to paclitaxel similar to that following administration of paclitaxel 200 mg/m2
and carboplatin in the absence of pazopanib. Paclitaxel 175 mg/m2 was administered as a 1-
hour infusion, and carboplatin area under the curve 5 (AUC5) or AUC6 was given as a half-hour
infusion on Day 1 of a 21-day cycle. Pazopanib was started on Day 2 of Cycle 1 to permit
assessment of paclitaxel and carboplatin pharmacokinetics individually on Day 1, after which
pazopanib was dosed continuously. Pazopanib was taken at least 1 hour before or 2 hours after
a meal.
Assessments
On Day 1 of each cycle, patients received a physical examination and hematology,
clinical chemistry, and urine protein:creatinine ratio assessments. Hematology and clinical
chemistry were also assessed on Days 8 and 15 of each cycle. An electrocardiogram, ECOG
performance status evaluation, amylase, lipase, and thyroid function tests were obtained on Day
1 of Cycle 2 and all subsequent cycles.
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 6
Blood samples for pharmacokinetic analysis of paclitaxel and carboplatin were obtained
on Day 1 of Cycle 1, and blood samples for pharmacokinetic analysis of all three agents were
obtained on Day 1 of Cycle 2. Samples for paclitaxel pharmacokinetics were collected pre-dose
(within 60 minutes before administration) and 0.5, 1 (end of infusion), 1.5, 2, 2.5, 3, 4, 5, 6, 8,
12, and 24 hours after the start of the infusion. Samples for carboplatin pharmacokinetics were
collected pre-dose and 1.5 (end of carboplatin infusion), 4, 8, and 24 hours after the start of the
paclitaxel infusion. Samples for pazopanib pharmacokinetics were collected pre-dose and 1, 2,
3, 4, 6, 8, 12, and 24 hours after administration.
Disease assessments were performed at baseline, after 6 weeks, and then every 9
weeks. Responses were recorded using Response Evaluation Criteria in Solid Tumors (19).
Statistical Assessments
Pharmacokinetic parameters were calculated by standard noncompartmental analysis
using WinNonlin Pro version 4.1 or higher (Pharsight Corporation, Mountain View, CA). An
analysis of variance (ANOVA) on logarithmic-transformed data was used to assess the
interaction effect of pazopanib on the pharmacokinetics of paclitaxel (Cmax and clearance) and
carboplatin (AUC(0-23) and Cmax). The ANOVA used a mixed-effects model with patient as a
random effect. Fixed-effect terms included dose cohort, treatment, and the dose cohort-
treatment interaction term. The test treatment was defined as pazopanib plus paclitaxel and
carboplatin (Cycle 2, Day 1) and the reference treatment was defined as paclitaxel and
carboplatin (Cycle 1, Day 1). The antilogs of the confidence limits of the 90% confidence
intervals (CI) for the difference in the treatment means of the logarithmic-transformed data were
a 90% CI for the ratio of geometric means between the test and reference treatment for Cmax
and clearance (paclitaxel). Because blood samples for analysis of ultrafilterable platinum were
collected for 23 hours after the start of the carboplatin infusion (24 hours after the start of the
paclitaxel infusion), carboplatin AUC(0-23) was included in the statistical analyses. The geometric
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 7
least squares mean ratio and associated 90% CI were provided after transformation of the
results from the logarithmic-transformed analysis back to the original scale. There was no
adjustment for the multiple comparisons of endpoints. The Statistical Analysis Software system
(SAS version 8.2 or higher; SAS Institute, Inc., Cary, NC) was used to analyze the data.
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 8
RESULTS
Between November 2006 and March 2009, 34 patients were enrolled (Table 1). All
patients were evaluable for pharmacokinetic analyses and safety, except one patient who was
not evaluable for DLT because of withdrawal from study without a DLT before completion of
Cycle 1 (Day 19). The most common tumor types were breast (29%) and esophageal (12%)
cancers. Less common tumor types (“other” in Table 1) included mesothelioma, NSCLC,
neuroendocrine, prostate cancer, small-cell lung cancer, sarcoma, pleura, and thyroid cancer
(one of each). All but two patients received prior anticancer therapy, which included
chemotherapy (88%), radiotherapy (53%), biologic therapy (29%), and endocrine therapy
(24%). Approximately 85% of patients previously received either antitubulin or platinum therapy.
Maximum Tolerated Regimen
The starting dose level in cohort 1 was paclitaxel 175 mg/m2, carboplatin AUC6, and
pazopanib 800 mg. Three of four patients experienced DLTs during the first cycle, including
grade 4 thrombocytopenia, grade 3 hypertension, and grade 4 neutropenia (Table 2). Given
these events, the dose of pazopanib was decreased to 400 mg in cohort 2. Four of five patients
experienced dose-limiting thrombocytopenia, which in some instances resulted in a delay of
Cycle 2 by more than 2 weeks. In an effort to reduce myelotoxicity in cohort 3, carboplatin was
decreased from AUC6 to AUC5 and pazopanib was decreased from 400 to 200 mg, while
paclitaxel was maintained at 175 mg/m2. The first three patients enrolled did not experience a
DLT. Accordingly, in cohort 4, pazopanib was increased to 400 mg with paclitaxel 175 mg/m2
and carboplatin AUC5, and one of the initial three patients experienced dose-limiting
neutropenia during the first cycle. This cohort was subsequently expanded and two of the next
three patients also experienced dose-limiting neutropenia.
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 9
To determine whether maximal doses of chemotherapy could still be administered with
pazopanib, a fifth cohort was treated with paclitaxel 175 mg/m2, carboplatin AUC6, and
pazopanib 200 mg; cohort 3 was also expanded in parallel. In cohort 5, one of the initial three
patients experienced dose-limiting neutropenia during the first cycle. An additional three patients
were enrolled, among whom one patient experienced dose-limiting neutropenia.
Given these findings, the MTR was determined to be paclitaxel 175 mg/m2 and
carboplatin AUC5 every 21 days, with pazopanib 200 mg once daily. Ten additional patients
were enrolled in this cohort for further study, with two patients experiencing DLTs (ie,
neutropenia, hematologic toxicity, and infection resulting in treatment delay). One patient in this
cohort withdrew consent at Day 19 and was therefore excluded for DLT analysis. Overall, two of
the 12 patients evaluable for DLT at this dose level experienced DLTs, confirming the MTR.
Adverse Events
Neutropenia, anemia, fatigue, nausea, thrombocytopenia, vomiting, diarrhea, peripheral
neuropathy, and alopecia were the most commonly reported drug-related adverse events, with
myelotoxicity being the most common grade 3 or 4 event (Table 3).
Hypertension was the most common cardiovascular event reported during the study. In
addition, nine patients experienced hemorrhagic (eg, epistaxis, hemoptysis, melena,
hematochezia, hemorrhoids, ecchymosis/petechiae, vaginal hemorrhage) adverse events
(grade 1 [n = 7] and grade 2 [n = 2]). No cases of proteinuria were reported. Elevations in
hepatobiliary parameters were considered adverse events in seven patients, most of which
were grade 2 (n = 2) or 3 (n = 3); however, one patient experienced grade 4 alanine
aminotransferase increase associated with grade 4 liver abscess and grade 3 bilirubin increase
that was not considered related to study drug.
One patient, treated at the MTR, withdrew during the study because of an adverse event
(grade 4 sepsis) that was considered serious and required hospitalization. Additionally, a patient
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 10
with metastatic esophageal cancer, also receiving treatment at the MTR, who remained on
study for more than 57 weeks, died within 4 weeks of the last dose of study drug in the setting of
rapid disease progression, esophageal stricture, and biliary obstruction.
Among all 34 patients who received at least one dose of study drug, 12 (35%)
experienced 37 serious adverse events during the study. There was no clear association
between frequency of serious adverse events and cohort treatment.
A dose interruption of at least one study drug because of adverse events was reported in
30 patients (88%). Most patients (including those at the MTR) experienced interruptions in
pazopanib dosing (79%) or delays in the scheduled administration of paclitaxel (68%) and
carboplatin (62%). The most common toxicities leading to treatment interruption, delay, or dose
reductions were neutropenia and thrombocytopenia. The frequencies of dose reductions were
as follows: pazopanib (26% overall; 0% MTR), paclitaxel (24% overall; 23% MTR), and
carboplatin (35% overall; 38% MTR).
Pharmacokinetics
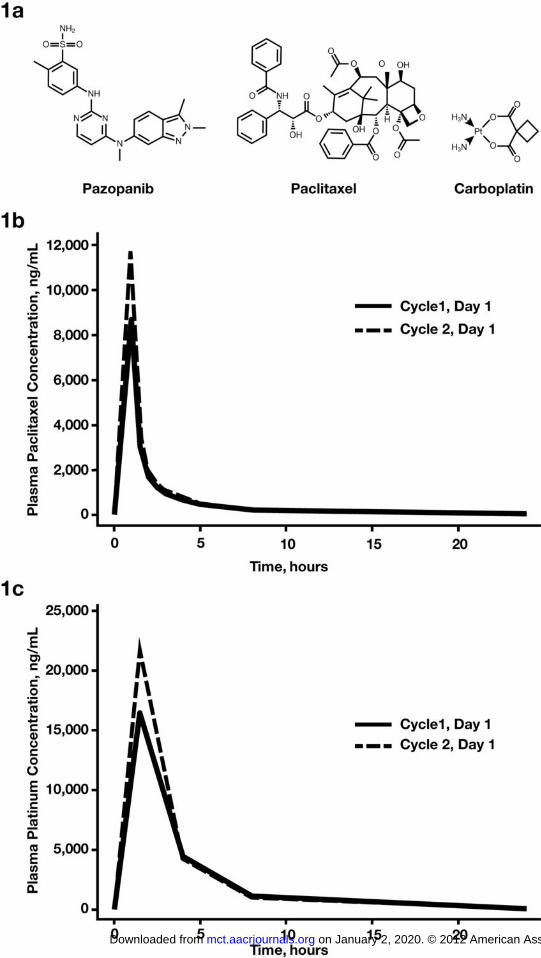
Concurrent administration of pazopanib 200 mg resulted in an approximately 43%
increase in paclitaxel Cmax (Table 4) and a 54% increase in carboplatin Cmax (AUC5 or AUC6;
Table 5) compared with paclitaxel and carboplatin without pazopanib (Figure 1B, 1C).
Pazopanib 400 mg resulted in similar increases in paclitaxel and carboplatin Cmax (40% and
68%, respectively) as that of pazopanib 200 mg. Pazopanib at 200 mg and 400 mg was found
to decrease paclitaxel clearance by 30% and 17%, respectively. However, because of the wide
variability of individual results, there was no statistically significant difference in paclitaxel
clearance between the pazopanib 200 mg and 400 mg dose.
Median plasma pazopanib Cmax on Cycle 2 Day 1 was 15.8 μg/mL in the cohort receiving
paclitaxel 175 mg/m2, carboplatin AUC5, and pazopanib 200 mg, and median pazopanib Cmax
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 11
was 27.5 μg/mL in the cohort receiving paclitaxel 175 mg/m2, carboplatin AUC5, and pazopanib
400 mg.
Efficacy
In this phase I trial, there were two complete responses and four partial responses.
Objective responses were observed at the MTR (paclitaxel 175 mg/m2, carboplatin AUC5, and
pazopanib 200 mg), and included complete responses in two patients with esophageal cancer,
one of whom had prior treatment with combination docetaxel and oxaliplatin, and one who was
chemotherapy-naive, and a partial response in a patient with small-cell lung cancer who had
received one prior line of therapy.
The other three partial responses occurred in previously treated patients with pancreatic
(paclitaxel 175 mg/m2, carboplatin AUC6, and pazopanib 400 mg), gastroesophageal junction,
and breast cancer (both at paclitaxel 175 mg/m2, carboplatin AUC5, and pazopanib 400 mg).
Overall, seven patients (21%) experienced disease stabilization, and the duration of stable
disease ranged from 24 to 77 weeks in a variety of tumor types.
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 12
DISCUSSION
Taxanes such as paclitaxel in combination with platinum-based agents are the standard
of care as first-line treatment in several solid tumor types (16,17). In the treatment of NSCLC
and ovarian cancer, the standard paclitaxel dose is 175 to 200 mg/m2 every 3 weeks and the
standard carboplatin dose is AUC5 to AUC7.5 (16,17). Previous studies have shown the
feasibility of combining antiangiogenic agents with chemotherapy in patients with colorectal,
NSCLC, and breast cancer (4-8,20). Bevacizumab is approved in combination with paclitaxel
and carboplatin in patients with stage IV, nonsquamous NSCLC, although an increase in the
incidence of treatment-related deaths has been reported with this regimen (6). In patients with
colorectal cancer, the addition of bevacizumab to chemotherapy improved progression-free and
overall survival by 2 to 5 months, but increased the incidence of hypertension and bleeding
(4,20).
Several small studies have evaluated the addition of small-molecule tyrosine kinase
inhibitors such as sorafenib (Nexavar) and cediranib (Recentin) to chemotherapy. In patients
with advanced ovarian cancer, paclitaxel 175 mg/m2 and carboplatin AUC5 with a standard
sorafenib dose of 400 mg twice daily was not feasible because of increased incidence of death
(21). Similar results were reported with paclitaxel 200 mg/m2, carboplatin AUC6, and cediranib
30 mg daily in advanced NSCLC (22). In the present study, the recommended phase II
monotherapy dose of pazopanib, 800 mg once daily, was not feasible with paclitaxel 175 mg/m2
and carboplatin AUC5 or AUC6 every 21 days in patients with advanced solid tumors, because
of myelosuppression.
The safety profile of pazopanib in combination with paclitaxel and carboplatin reflected
established adverse events for each agent. In addition to defining the MTR by reported
toxicities, tolerability was assessed by comparing the actual doses of each agent received
versus the assigned cohort dose. Among the cohorts, more cycles were administered at the
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 13
assigned dose for cohorts receiving low daily doses of pazopanib (200 mg) than for cohorts
receiving higher daily doses of pazopanib (400 or 800 mg). These results further support the
identified MTR. In addition, clinical activity was observed at the MTR; two of the four patients
with esophageal carcinomas achieved a complete response, and there were partial responses
and disease stabilization in other tumor types. Although the pazopanib dose in the MTR was
lower than the currently approved dose of 800 mg once daily in renal cell carcinoma, the median
pazopanib concentration achieved was 16 μg/mL, which is within the therapeutic concentration
range (15 - 17.4 μg/mL) (9,23).
In this trial, there was a high incidence of myelosuppression that is likely a consequence
of drug-drug interactions, resulting in increased exposure to the chemotherapy components of
this regimen. Coadministration of pazopanib 200 mg (n = 14) and 400 mg (n = 8) once daily with
paclitaxel 175 mg/m2 and carboplatin every 21 days decreased paclitaxel clearance by 30% and
17%, respectively, and increased paclitaxel Cmax by approximately 40%. Mean paclitaxel
clearance decreased by 14% and mean paclitaxel Cmax increased by 36% after administration of
pazopanib 800 mg once daily and paclitaxel 80 mg/m2 in a weekly regimen (18). These results
indicate that maximal inhibition of paclitaxel clearance is achieved at pazopanib doses at or
below 200 mg. It is known that paclitaxel is a substrate of CYP3A4 and CYP2C8 and that
pazopanib is a weak inhibitor of these cytochrome enzymes, which is likely the basis for the
altered pharmacokinetics of paclitaxel when given with pazopanib. In contrast to the primarily
metabolic elimination of paclitaxel, carboplatin is primarily excreted through the kidneys, and
inhibition of cytochrome enzymes was not expected to alter the pharmacokinetics of carboplatin.
However, coadministration of pazopanib resulted in an increase in carboplatin AUC(0-23) and
Cmax relative to administration of carboplatin and paclitaxel without pazopanib. While the
mechanism of this apparent interaction remains unknown, this is similar to what has been
observed with coadministration of other small-molecule VEGFR tyrosine kinase inhibitors such
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 14
as BIBF 1120 (24) and AZD2171 (25), namely, an increase in carboplatin AUC. Interestingly, no
change in the pharmacokinetics of carboplatin was observed when paclitaxel and carboplatin
were administered in the presence of sorafenib dosed intermittently (26). A study with a more
dense blood sampling scheme is required to characterize the pharmacokinetics of carboplatin to
determine more accurately the extent of a pharmacokinetic drug-drug interaction between
pazopanib and carboplatin or other platinum-containing regimens. Administering paclitaxel and
carboplatin at lower doses than in this study may be an alternative, because in combination with
pazopanib the increases in paclitaxel and carboplatin AUC and Cmax would still provide
adequate therapeutic exposure.
In conclusion, pharmacokinetic analysis revealed that exposures to paclitaxel and
carboplatin were higher during concurrent treatment with pazopanib relative to treatment without
pazopanib. This three-drug combination has shown clinical activity at the MTR of paclitaxel
175 mg/m2 and carboplatin AUC5 every 21 days with pazopanib 200 mg daily, and alternative
strategies of administration, such as lower doses of chemotherapy or intermittent dosing of
pazopanib, are being explored to see if a more tolerable side effect profile can be achieved.
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 15
ACKNOWLEDGMENTS
We thank the patients and their families, and acknowledge Kristi Beatty and Kathryn
Westlake for their efforts in conducting this study. We also thank Tamalette Loh, PhD, at ProEd
Communications, Inc., for her medical editorial assistance with this manuscript.
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 16
REFERENCES
1. Bergers G, Song S, Meyer-Morse N, Bergsland E, Hanahan D. Benefits of targeting both
pericytes and endothelial cells in the tumor vasculature with kinase inhibitors. J Clin
Invest 2003;111:1287-1295.
2. Folkman J. What is the evidence that tumors are angiogenesis dependent? J Natl
Cancer Inst 1990;82:4-6.
3. Jain RK. Normalization of tumor vasculature: an emerging concept in antiangiogenic
therapy. Science 2005;307:58-62.
4. Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J, Heim W, et al.
Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal
cancer. N Engl J Med 2004;350:2335-2342.
5. Saltz LB, Clarke S, Diaz-Rubio E, Scheithauer W, Figer A, Wong R, et al. Bevacizumab
in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic
colorectal cancer: a randomized phase III study. J Clin Oncol 2008;26:2013-2019.
6. Sandler A, Gray R, Perry MC, Brahmer J, Schiller JH, Dowlati A, et al. Paclitaxel-
carboplatin alone or with bevacizumab for non-small-cell lung cancer. N Engl J Med
2006;355:2542-2550.
7. Robert NJ, Dieras V, Glaspy J, Brufsky AM, Bondarenko I, Lipatov ON, et al. RIBBON-1:
randomized, double-blind, placebo-controlled, phase III trial of chemotherapy with or
without bevacizumab for first-line treatment of human epidermal growth factor receptor
2-negative, locally recurrent or metastatic breast cancer. J Clin Oncol 2011;29:1252-
1260.
8. Miller K, Wang M, Gralow J, Dickler M, Cobleigh M, Perez EA, et al. Paclitaxel plus
bevacizumab versus paclitaxel alone for metastatic breast cancer. N Engl J Med
2007;357:2666-2676.
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 17
9. Kumar R, Knick VB, Rudolph SK, Johnson JH, Crosby RM, Crouthamel MC, et al.
Pharmacokinetic-pharmacodynamic correlation from mouse to human with pazopanib, a
multikinase angiogenesis inhibitor with potent antitumor and antiangiogenic activity. Mol
Cancer Ther 2007;6:2012-2021.
10. Friedlander M, Hancock KC, Rischin D, Messing MJ, Stringer CA, Matthys GM, et al. A
Phase II, open-label study evaluating pazopanib in patients with recurrent ovarian
cancer. Gynecol Oncol 2010;119:32-37.
11. Iwamoto FM, Lamborn KR, Robins HI, Mehta MP, Chang SM, Butowski NA, et al. Phase
II trial of pazopanib (GW786034), an oral multi-targeted angiogenesis inhibitor, for adults
with recurrent glioblastoma (North American Brain Tumor Consortium Study 06-02).
Neuro Oncol 2010;12:855-861.
12. Sleijfer S, Ray-Coquard I, Papai Z, Le Cesne A, Scurr M, Schoffski P, et al. Pazopanib,
a multikinase angiogenesis inhibitor, in patients with relapsed or refractory advanced soft
tissue sarcoma: a phase II study from the European organisation for research and
treatment of cancer-soft tissue and bone sarcoma group (EORTC study 62043). J Clin
Oncol 2009;27:3126-3132.
13. Sternberg CN, Davis ID, Mardiak J, Szczylik C, Lee E, Wagstaff J, et al. Pazopanib in
locally advanced or metastatic renal cell carcinoma: results of a randomized phase III
trial. J Clin Oncol 2010;28:1061-1068.
14. Bible KC, Suman VJ, Molina JR, Smallridge RC, Maples WJ, Menefee ME, et al.
Efficacy of pazopanib in progressive, radioiodine-refractory, metastatic differentiated
thyroid cancers: results of a phase 2 consortium study. Lancet Oncol 2010;11:962-972.
15. Taylor SK, Chia S, Dent S, Clemons M, Agulnik M, Grenci P, et al. A phase II study of
pazopanib in patients with recurrent or metastatic invasive breast carcinoma: a trial of
the Princess Margaret Hospital phase II consortium. Oncologist 2010;15:810-818.
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 18
16. Azzoli CG, Baker S, Jr., Temin S, Pao W, Aliff T, Brahmer J, et al. American Society of
Clinical Oncology Clinical Practice Guideline update on chemotherapy for stage IV non-
small-cell lung cancer. J Clin Oncol 2009;27:6251-6266.
17. National Comprehensive Cancer Network. Ovarian cancer: including fallopian tube
cancer and primary peritoneal cancer. Version 2.2011. Available at:
http://www.nccn.org/professionals/physician_gls/pdf/ovarian.pdf. Accessed: February 23,
2011.
18. Tan AR, Dowlati A, Jones SF, Infante JR, Nishioka J, Fang L, et al. Phase I study of
pazopanib in combination with weekly paclitaxel in patients with advanced solid tumors.
Oncologist 2010;15:1253-1261.
19. Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al.
New guidelines to evaluate the response to treatment in solid tumors. European
Organization for Research and Treatment of Cancer, National Cancer Institute of the
United States, National Cancer Institute of Canada. J Natl Cancer Inst 2000;92:205-216.
20. Giantonio BJ, Catalano PJ, Meropol NJ, O'Dwyer PJ, Mitchell EP, Alberts SR, et al.
Bevacizumab in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for
previously treated metastatic colorectal cancer: results from the Eastern Cooperative
Oncology Group Study E3200. J Clin Oncol 2007;25:1539-1544.
21. Polcher M, Eckhardt M, Coch C, Wolfgarten M, Kubler K, Hartmann G, et al. Sorafenib in
combination with carboplatin and paclitaxel as neoadjuvant chemotherapy in patients
with advanced ovarian cancer. Cancer Chemother Pharmacol 2010;66:203-207.
22. Goss GD, Arnold A, Shepherd FA, Dediu M, Ciuleanu TE, Fenton D, et al. Randomized,
double-blind trial of carboplatin and paclitaxel with either daily oral cediranib or placebo
in advanced non-small-cell lung cancer: NCIC clinical trials group BR24 study. J Clin
Oncol 2010;28:49-55.
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 19
23. Hurwitz HI, Dowlati A, Saini S, Savage S, Suttle AB, Gibson DM, et al. Phase I trial of
pazopanib in patients with advanced cancer. Clin Cancer Res 2009;15:4220-4227.
24. du Bois A, Huober J, Stopfer P, Pfisterer J, Wimberger P, Loibl S, et al. A phase I open-
label dose-escalation study of oral BIBF 1120 combined with standard paclitaxel and
carboplatin in patients with advanced gynecological malignancies. Ann Oncol
2010;21:370-375.
25. Laurie SA, Gauthier I, Arnold A, Shepherd FA, Ellis PM, Chen E, et al. Phase I and
pharmacokinetic study of daily oral AZD2171, an inhibitor of vascular endothelial growth
factor tyrosine kinases, in combination with carboplatin and paclitaxel in patients with
advanced non-small-cell lung cancer: the National Cancer Institute of Canada clinical
trials group. J Clin Oncol 2008;26:1871-1878.
26. Okamoto I, Miyazaki M, Morinaga R, Kaneda H, Ueda S, Hasegawa Y, et al. Phase I
clinical and pharmacokinetic study of sorafenib in combination with carboplatin and
paclitaxel in patients with advanced non-small cell lung cancer. Invest New Drugs
2010;28:844-853.
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 20
TABLES
Table 1. Patient Characteristics
Demographics and Disease Characteristics Patients (N = 34)
Age, median years (range) 56 (34 - 78)
Sex, n (%) Male Female
17 (50) 17 (50)
Race, n (%) Caucasian/European African American Asian/East Asian
30 (88)
3 (9) 1 (3)
ECOG performance status, n (%) 0 1
19 (56) 15 (44)
Primary tumor type, n (%) Breast Esophagus Bile duct Bonea Colorectal Endometrial Gastroesophageal Pancreas Other
10 (29) 4 (12) 2 (6) 2 (6) 2 (6) 2 (6) 2 (6) 2 (6)
8 (24)
Prior antitubulin therapy, n (%) 16 (47)
Prior platinum therapy, n (%) 13 (38) a One patient had a primary diagnosis of osteosarcoma and the other had giant cell tumor of the bone. .
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 21
Table 2. Dose Levels and Dose-Limiting Toxicities
Cohort Dosing Regimen Patients
Enrolled, n Patients with
DLTs, n Dose-Limiting Toxicities
1 Paclitaxel 175 mg/m2 + Carboplatin AUC6 + Pazopanib 800 mg
4a 3
Grade 4 thrombocytopenia
Grade 3 hypertension
Grade 3 infection with grade 4 neutropenia Grade 4 thrombocytopenia
2 Paclitaxel 175 mg/m2 + Carboplatin AUC6 + Pazopanib 400 mg
5a 4
Grade 1 thrombocytopeniab
Grade 1 thrombocytopeniab
Grade 4 thrombocytopenia
Grade 3 thrombocytopeniac
3 Paclitaxel 175 mg/m2 + Carboplatin AUC5 + Pazopanib 200 mg
3 0 –
4 Paclitaxel 175 mg/m2 + Carboplatin AUC5 + Pazopanib 400 mg
6 3
Grade 3 neutropeniab
Grade 4 neutropeniab
Grade 3 neutropeniab
5 Paclitaxel 175 mg/m2 + Carboplatin AUC6 + Pazopanib 200 mg
6 2 Grade 4 neutropeniab
Grade 3 neutropeniab
Expansion cohortd
Paclitaxel 175 mg/m2 + Carboplatin AUC5 + Pazopanib 200 mg
10e 2
Grade 4 neutropenia
Grade 3 oral cavity infectionb Grade 3 thrombocytopeniab
Grade 2 neutropeniab
a The study protocol permitted 3 to 6 patients per cohort, and depending on the number screened and the number eligible, some cohorts contained more than 3 patients each. b Start of Cycle 2 delayed by > 2 weeks. c Grade 3 thrombocytopenia was considered to be a DLT by investigator because of grade ≥ 2 toxicity that occurred beyond Day 28. d Cohort 3 was expanded. e Although 10 patients were enrolled, only 9 were evaluable for DLTs and one patient, who did not have a DLT, withdrew before completing Cycle 1.
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 22
Table 3. Drug-Related Adverse Events (all grades) Occurring in ≥ 10% of Patients
Patients, n (%)
Pacl 175 mg/m2 + Carbo AUC6 +
Pacl 175 mg/m2 + Carbo AUC5 +
Paz 800 mg (N = 4) Paz 400 mg (N = 5) Paz 200 mg (N = 6) Paz 200 mg (N = 13)a Paz 400 mg (N = 6)
All grades Grade 3/4 All grades Grade 3/4 All grades Grade 3/4 All grades Grade 3/4 All grades Grade 3/4
Hematologic toxicities
Neutropenia 3 (75) 3 (75) 3 (60) 3 (60) 5 (83) 5 (83) 11 (85) 9 (69) 6 (100) 6 (100)
Anemia 1 (25) 1 (25) 2 (40) 0 5 (83) 0 9 (69) 4 (31) 5 (83) 1 (17)
Thrombocytopenia 2 (50) 1 (25) 4 (80) 2 (40) 2 (33) 2 (33) 6 (46) 4 (31) 6 (100) 6 (100)
Leukopenia 1 (25) 0 1 (20) 1 (20) 1 (17) 0 1 (8) 0 2 (33) 0
Non-hematologic toxicities
Fatigue 3 (75) 0 3 (60) 0 2 (33) 0 11 (85) 1 (8) 3 (50) 1 (17)
Nausea 2 (50) 0 3 (60) 0 3 (50) 0 8 (62) 0 4 (67) 0
Vomiting 3 (75) 0 3 (60) 0 2 (33) 0 7 (54) 0 3 (50) 0
Diarrhea 2 (50) 0 2 (40) 0 1 (17) 0 6 (46) 0 3 (50) 0
Peripheral neuropathy 1 (25) 0 2 (40) 0 1 (17) 0 7 (54) 0 3 (50) 0
Alopecia 2 (50) 0 2 (40) 0 1 (17) 0 5 (38) 0 2 (33) 0
Decreased appetite 1 (25) 0 0 0 2 (33) 0 5 (38) 0 1 (17) 0
Dysgeusia 1 (25) 0 1 (20) 0 0 0 2 (15) 0 3 (50) 0
Headache 1 (25) 0 0 0 0 0 3 (23) 0 2 (33) 0
Hypertension 2 (50) 2 (50) 1 (20) 0 1 (17) 1 (17) 1 (8) 1 (8) 0 0
Mucosal inflammation 0 0 1 (20) 0 0 0 2 (15) 0 2 (33) 1 (17)
Dyspepsia 1 (25) 0 1 (20) 0 0 0 0 0 2 (33) 0
Peripheral edema 0 0 0 0 0 0 3 (23) 0 1 (17) 0
Rash 3 (75) 0 0 0 0 0 1 (8) 0 0 0 Abbreviations: Carbo, carboplatin; Pacl, paclitaxel; Paz, pazopanib. a This was the determined to be the maximum tolerated regimen.
.
on January 2, 2020. © 2012 A
merican A
ssociation for Cancer R
esearch. m
ct.aacrjournals.org D
ownloaded from
Author m
anuscripts have been peer reviewed and accepted for publication but have not yet been edited.
Author M
anuscript Published O
nlineFirst on June 7, 2012; D
OI: 10.1158/1535-7163.M
CT
-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 23
Table 4. Statistical Analysis of Paclitaxel Pharmacokinetic Parameters
Geometric Least Squares Mean
Parameter N Cycle 1 Cycle 2 Ratio 90% CI
Pazopanib 200 mg once daily
Clearance, L/h/m2 14 11.6 8.16 0.70 0.61 - 0.80
Cmax, µg/mL 14 26.9 38.5 1.43 1.19 - 1.72
Pazopanib 400 mg once daily
Clearance, L/h/m2 8 11.2 9.23 0.83 0.68 - 1.01
Cmax, µg/mL 8 31.2 43.6 1.40 1.16 - 1.68
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 24
Table 5. Statistical Analysis of Ultrafilterable Platinum Pharmacokinetic Parameters Normalized to the Carboplatin AUC6 Dose
Parameter
N
Geometric Least
Squares Mean
Ratio
90% CI Cycle 1 Cycle 2
Pazopanib 200 mg once daily
AUC(0-23), µg*h/mL 11 55.5 78.3 1.41 1.25 - 1.59
Cmax, µg/mL 13 18.2 28.0 1.54 1.12 - 2.10
Pazopanib 400 mg once daily
AUC(0-23), ng*h/mL 6 54.1 70.8 1.31 0.89 - 1.93
Cmax, ng/mL 6 20.8 35.0 1.68 0.91 - 3.10
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Burris et al Phase I study of pazopanib, paclitaxel, and carboplatin Page 25
FIGURE LEGENDS
Figure 1. A: Chemical structures of pazopanib, paclitaxel, and carboplatin. B: Median plasma
paclitaxel concentration-time profile after administration of paclitaxel 175 mg/m2, carboplatin
dosed at area under the curve 5 (AUC5), and pazopanib 200 mg. C: Median ultrafilterable
platinum concentration-time profile after administration of paclitaxel 175 mg/m2, carboplatin
AUC5, and pazopanib 200 mg.
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997

Published OnlineFirst June 7, 2012.Mol Cancer Ther Howard A. Burris III, Afshin Dowlati, Rebecca A Moss, et al. Solid TumorsCarboplatin Given Every 21 Days in Patients with Advanced Phase I Study of Pazopanib in Combination with Paclitaxel and
Updated version
10.1158/1535-7163.MCT-11-0997doi:
Access the most recent version of this article at:
Manuscript
Authoredited. Author manuscripts have been peer reviewed and accepted for publication but have not yet been
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://mct.aacrjournals.org/content/early/2012/06/07/1535-7163.MCT-11-0997To request permission to re-use all or part of this article, use this link
on January 2, 2020. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on June 7, 2012; DOI: 10.1158/1535-7163.MCT-11-0997


















