Git ibd 2012 pretest.
84
Inflammatory Inflammatory Bowel Disease Bowel Disease Dr. Mohammad Shaikhani Dr. Mohammad Shaikhani CABM,FRCP CABM,FRCP . . Updated:2/2011 Updated:2/2011
description
Git ibd 2012 pretest.
Transcript of Git ibd 2012 pretest.

Inflammatory Inflammatory Bowel DiseaseBowel DiseaseDr. Mohammad ShaikhaniDr. Mohammad Shaikhani
CABM,FRCPCABM,FRCP..
Updated:2/2011Updated:2/2011

Pretest 1Pretest 1:: What % of IBD is regarded to be What % of IBD is regarded to be
intederminate:intederminate: A.90%A.90% B. 70%B. 70% C.10%.C.10%. D.25%.D.25%. E.0%.E.0%.

Pretest 2Pretest 2:: Appendisectomy in crease the risk of:Appendisectomy in crease the risk of: A.UCA.UC B. CDB. CD C. Both.C. Both. D. Neither.D. Neither.

Pretest 3Pretest 3:: Smoking:Smoking: A. Increase the risk of UC.A. Increase the risk of UC. B. Protect against UC.B. Protect against UC. C. Protect against CD.C. Protect against CD. D. ALL.D. ALL. E. None..E. None..

Pretest 4Pretest 4:: Proctitis in UC leads to:Proctitis in UC leads to: A. Constipation > diarrhea.A. Constipation > diarrhea. B. Diarrhea> constipation.B. Diarrhea> constipation. C. Both.C. Both. D. Neither.D. Neither.

Pretest 5Pretest 5:: CD can cause the following except:CD can cause the following except: A. GOO.A. GOO. B. Mouth ulcer.B. Mouth ulcer. C. Perianal fistulas.C. Perianal fistulas. D. diverticuli.D. diverticuli. E. RIF massE. RIF mass

Pretest 6Pretest 6:: CD can cause the following except:CD can cause the following except: A. GOO.A. GOO. B. Mouth ulcer.B. Mouth ulcer. C. Perianal fistulas.C. Perianal fistulas. D. diverticuli.D. diverticuli. E. RIF massE. RIF mass

Pretest 7Pretest 7:: Granulomas, characteristic of CD, occur Granulomas, characteristic of CD, occur
in:in: A. Nearly all.A. Nearly all. B. Nearly none.B. Nearly none. C. Around 1/3.C. Around 1/3. D. Most of them.D. Most of them. E. None of the above.E. None of the above.

Pretest 8Pretest 8:: Primary sclerosing cholangitis:Primary sclerosing cholangitis: A. Occurs in CD > UC.A. Occurs in CD > UC. B. Occurs in most patients with UC.B. Occurs in most patients with UC. C. Most patients with PSC have UC.C. Most patients with PSC have UC. D. All of the above.D. All of the above. E. None of the above.E. None of the above.

Pretest 9Pretest 9:: IBD with Primary sclerosing cholangitis IBD with Primary sclerosing cholangitis
have increases risk of:have increases risk of: A. CRC.A. CRC. B. Cholangiocarcinoma.B. Cholangiocarcinoma. C. Both.C. Both. D. Neither.D. Neither.

Pretest 10Pretest 10:: The most serious acute complications of The most serious acute complications of
IBD is:IBD is: A. Pyoderma gangrenosa.A. Pyoderma gangrenosa. B. Toxic megacolon.B. Toxic megacolon. C. PSC.C. PSC. D. EN.D. EN. E. Peripheral arthritis.E. Peripheral arthritis.

Introduction Introduction IBD: an idiopathic chronic inflammatory disease of the GIT IBD: an idiopathic chronic inflammatory disease of the GIT
consistsing of 2 distinct clinical entities: ulcerative colitis & Crohn consistsing of 2 distinct clinical entities: ulcerative colitis & Crohn disease (regional enteritis),both cause macroscopic inflammation.disease (regional enteritis),both cause macroscopic inflammation.
Microscopic colitis is less common& does not cause significant Microscopic colitis is less common& does not cause significant macroscopic abnormalities.macroscopic abnormalities.
The pathogenesis not fully understood but likely involves a The pathogenesis not fully understood but likely involves a genetic predisposition& a dysregulated immunologic response to genetic predisposition& a dysregulated immunologic response to the local microenvironment of luminal bacteria. the local microenvironment of luminal bacteria.
Both are usually differentiated on the basis of differences in the Both are usually differentiated on the basis of differences in the distribution of pathology in the bowel & histopathologic distribution of pathology in the bowel & histopathologic appearance of the lesion. appearance of the lesion.
10% of patients cannot be shown to have either Crohn disease or 10% of patients cannot be shown to have either Crohn disease or ulcerative colitis ( indeterminate colitis).ulcerative colitis ( indeterminate colitis).

Risk factors: Risk factors: The peak incidence :second, third& fourth decades of lifeThe peak incidence :second, third& fourth decades of life A second peak in the seventh&eighth decades.A second peak in the seventh&eighth decades. There are no sex differences.There are no sex differences. Ashkenazi Jewish descent have a higher risk. Ashkenazi Jewish descent have a higher risk. A 5-10% risk for first-degree relatives of affected patients. A 5-10% risk for first-degree relatives of affected patients. Many candidate genes:Many candidate genes: 1.Established link between Crohn disease &variants of the 1.Established link between Crohn disease &variants of the
CARD15CARD15 (also known as (also known as NOD2NOD2) gene, in only some patients & ) gene, in only some patients & does not affect the risk for colitis. does not affect the risk for colitis.
2. IL-23 receptor affects the risk for both Crohn disease & colitis., 2. IL-23 receptor affects the risk for both Crohn disease & colitis., as monoclonal antibody against the p40 subunit have as monoclonal antibody against the p40 subunit have demonstrated benefit in the treatment of Crohn disease.demonstrated benefit in the treatment of Crohn disease.


Less common colitis forms Less common colitis forms are:are:
Microscopic colitis (collagenous& Microscopic colitis (collagenous& lynphocytic)lynphocytic)
OthersOthers Diversion colitis after clostomies.Diversion colitis after clostomies. Radiation colitisRadiation colitis Drug induced colitisDrug induced colitis Infectious colitisInfectious colitis Ischemic colitis Ischemic colitis

Clinical features: UCClinical features: UC Generally present with bloody diarrhea with rectal urgency, Generally present with bloody diarrhea with rectal urgency,
discomfort& cramps.discomfort& cramps. They have profound tenesmus (feelings of urgency& incomplete They have profound tenesmus (feelings of urgency& incomplete
evacuation), secondary to proctitis, this can cause constipation to evacuation), secondary to proctitis, this can cause constipation to be a more common manifestation than diarrhea; in such patients, be a more common manifestation than diarrhea; in such patients, determining the activity of the disease& treating it can be determining the activity of the disease& treating it can be challenging. challenging.
UC extends proximally from the anal verge&can progress to UC extends proximally from the anal verge&can progress to pancolitis involving the cecum. pancolitis involving the cecum.
Fever is infrequent, but weight loss secondary to the inflammatory Fever is infrequent, but weight loss secondary to the inflammatory disease itself or to the chronic diarrhea is common. disease itself or to the chronic diarrhea is common.
Physical examination findings can range from mild lower Physical examination findings can range from mild lower abdominal tenderness to abdominal distention with rebound abdominal tenderness to abdominal distention with rebound tenderness& hypoactive bowel sounds, suggestive of toxic tenderness& hypoactive bowel sounds, suggestive of toxic megacolon. megacolon.

Clinical features: Crohn diseaseClinical features: Crohn disease More protean in its manifestations than ulcerative colitis, as the More protean in its manifestations than ulcerative colitis, as the
disease can affect any portion of the GIT& frequently has so-disease can affect any portion of the GIT& frequently has so-called “skip lesions” with areas of normal mucosa juxtaposed called “skip lesions” with areas of normal mucosa juxtaposed with severe inflammation. with severe inflammation.
The transmural nature of the disease results in three distinct The transmural nature of the disease results in three distinct manifestations: inflammatory, fistulizing& fibrostenotic. manifestations: inflammatory, fistulizing& fibrostenotic.
Large-volume diarrhea can occur; diarrhea is associated with Large-volume diarrhea can occur; diarrhea is associated with both small& large-bowel Crohn disease, whereas hematochezia is both small& large-bowel Crohn disease, whereas hematochezia is almost always a sign of colonic disease. almost always a sign of colonic disease.
The inflamed tissue causes a secretory diarrhea& a protein-losing The inflamed tissue causes a secretory diarrhea& a protein-losing enteropathy, steatorrhea from fat malabsorption (with patients enteropathy, steatorrhea from fat malabsorption (with patients who have ileal or ilealocolic disease frequently being vitamin B12- who have ileal or ilealocolic disease frequently being vitamin B12- & vitamin D-deficient)& other types of malabsorption. & vitamin D-deficient)& other types of malabsorption.
Patients who have had their terminal ileum resected are also at Patients who have had their terminal ileum resected are also at risk for a choleretic diarrhea secondary to bile salt wasting. risk for a choleretic diarrhea secondary to bile salt wasting.

Clinical features: Crohn diseaseClinical features: Crohn disease FistulaeFistulae are abnormal connections between the bowel& are abnormal connections between the bowel&
adjacent organs. adjacent organs. Abscesses may form& the fistula acts as a natural drainage Abscesses may form& the fistula acts as a natural drainage
mechanism, causing pus to emerge from the fistulae.mechanism, causing pus to emerge from the fistulae. The fistulae become symptomatic with drainage of fecal The fistulae become symptomatic with drainage of fecal
material around the anus (perianal fistulae), seepage of material around the anus (perianal fistulae), seepage of bowel contents through the skin (enterocutaneous fistulae), bowel contents through the skin (enterocutaneous fistulae), passage of feces through the vagina (rectovaginal passage of feces through the vagina (rectovaginal fistulae)& pneumaturia or recurrent urinary tract fistulae)& pneumaturia or recurrent urinary tract infections (enterovesical fistulae).infections (enterovesical fistulae).
The intestinal inflammation may extend to adjacent The intestinal inflammation may extend to adjacent musculature &result in neuromuscular sequelae; for musculature &result in neuromuscular sequelae; for example, a patient with Crohn disease&a new limp likely example, a patient with Crohn disease&a new limp likely has a psoas muscle abscess. has a psoas muscle abscess.

Clinical features: Crohn diseaseClinical features: Crohn disease Patients with intestinal Patients with intestinal stricturesstrictures present with signs of present with signs of
obstruction: fever, abdominal distention, pain, nausea, vomiting. obstruction: fever, abdominal distention, pain, nausea, vomiting. Strictures may be secondary to severe inflammation or to fibrosis Strictures may be secondary to severe inflammation or to fibrosis
of the bowel& can be relieved only by surgical resection. of the bowel& can be relieved only by surgical resection. The most common site of strictures is in the terminal ileum where The most common site of strictures is in the terminal ileum where
they result in partial or complete small-bowel obstruction. they result in partial or complete small-bowel obstruction. Patients with duodenal Crohn disease may develop gastric outlet Patients with duodenal Crohn disease may develop gastric outlet
obstruction. obstruction. In patients with ileal disease, the abdominal examination In patients with ileal disease, the abdominal examination
commonly shows right lower quadrant tenderness; a commonly shows right lower quadrant tenderness; a phlegmonous mass may be present. phlegmonous mass may be present.
A detailed anorectal examination is important in patients with A detailed anorectal examination is important in patients with suspected Crohn disease: the presence of skin tags suggests the suspected Crohn disease: the presence of skin tags suggests the diagnosis& the examination may also show fistulae.diagnosis& the examination may also show fistulae.



Environmental Environmental PrecipitantsPrecipitants
Factors: Early appendectomy (increase UC
incidence) Smoking (protects against UC but
increases the risk of CD).


UCUC

Distinguishing characteristics of Distinguishing characteristics of CD and UCCD and UC
Feature CDUC
Location SB or colonOnly colon (rarely
“backwash ileitis”
Anatomic distribution
Skip lesionsContinuous, begins distally
Rectal involvement
Rectal spareInvolved in >90%
Gross bleeding
Only 25%Universal
Peri-anal disease
75%Rare
Fistulization Yes No
Granulomas 10-30%No

Endoscopic features of CD Endoscopic features of CD and UCand UC
Feature CDUC
Mucosal involvement
Discontinuous
Continuous
Aphthous ulcers
Common Rare
Surrounding mucosa
Relatively normal
Abnormal
Longitudinal ulcer
Common Rare
Cobble stoningIn severe cases
No
Mucosal friability
Uncommon Common
Vascular pattern
Normal distorted

Pathologic features of CD Pathologic features of CD and UCand UC
Feature CDUC
Transmural inflammation
Yes Uncommon
Granulomas 50-75%No
Fissures Common Rare
Fibrosis Common No
Submucosal inflammation
Common Uncommon

Radiologic features of CD Radiologic features of CD and UCand UC
Feature CDUC
Nodularitygranularity
cobble stoningstring sign of SB
Collar button ulcers

Comparison of Features in Ulcerative Colitis and Crohn's Disease
FeatureUlcerative ColitisCrohn's Disease
Depth of inflammation
MucosalTransmural
Pattern of diseaseContiguousSkip areas
LocationColorectumMouth to anus
Rectal involvementUsualLess common
Ileal diseaseBackwash ileitis (15%–20% of patients)
Common
FistulasRareCommon
Perianal diseaseRareCommon
GranulomasUnlikely10%–30% of patients
Overt bleedingUsualLess common
MalnutritionUnlikelyMore common
Cancer riskColorectal cancer, cholangiocarcinoma (if primary sclerosing cholangitis is present)
Colorectal cancer, small bowel cancer (depending on disease location)
Tobacco useProtectiveHarmful

UCUC

CDCD


DDX of UCDDX of UC
InfectiousInfectious Drug inducedDrug induced Microscopic colitisMicroscopic colitis

CDCD
Anatomic Anatomic distributiondistribution
CD activity CD activity indexindex
DDx DDx (lymphoma, (lymphoma, Yersinea Yersinea Enterocolitis, Enterocolitis, TB)TB)

CD ilitis: DDxCD ilitis: DDx
LymphomaLymphoma
Yersinea Enterocolitis Yersinea Enterocolitis TBTB

Extra-intestinal manifestations Extra-intestinal manifestations of IBDof IBD
Arthritis:Arthritis: Peripheral arthritis, usu paralels the disease Peripheral arthritis, usu paralels the disease
activityactivity Ankylosing Spondylitis, 1-6%, sacroiliitisAnkylosing Spondylitis, 1-6%, sacroiliitis
Ocular lesions:Ocular lesions: Iritis (uvietis) (0.5-3%), episcleritis, keratitis,Iritis (uvietis) (0.5-3%), episcleritis, keratitis,
Skin and oral cavity:Skin and oral cavity: Erythema nodosum 1-3%Erythema nodosum 1-3% Pyoderma Gangrenosum 0.6%Pyoderma Gangrenosum 0.6% Aphthus stomatitis, metastatic CD.Aphthus stomatitis, metastatic CD.

Extra-intestinal manifestations Extra-intestinal manifestations of IBDof IBD
Occur in 10-20% at some time in the course of their disease. Occur in 10-20% at some time in the course of their disease. Arthritis, the most common, can either be related to the intestinal Arthritis, the most common, can either be related to the intestinal
inflammation itself or be part of an overlap syndrome with inflammation itself or be part of an overlap syndrome with rheumatoid arthritis. rheumatoid arthritis.
Sacroiliitis &ankylosing spondylitis, in association with HLA Sacroiliitis &ankylosing spondylitis, in association with HLA B27, occur in 5-10%. B27, occur in 5-10%.
Uveitis & episcleritis may also occur. Uveitis & episcleritis may also occur. Erythema nodosum, which manifests as small exquisitely tender Erythema nodosum, which manifests as small exquisitely tender
nodules on the anterior tibial surface, occurs more commonly in nodules on the anterior tibial surface, occurs more commonly in Crohn disease, whereas pyoderma gangrenosum is more common Crohn disease, whereas pyoderma gangrenosum is more common in ulcerative colitis& can range from small lesions to large ulcers. in ulcerative colitis& can range from small lesions to large ulcers. Even small amounts of trauma to the skin can activate this Even small amounts of trauma to the skin can activate this inflammatory process. inflammatory process.

Extra-intestinal manifestations Extra-intestinal manifestations of IBDof IBD
Primary sclerosing cholangitis:Primary sclerosing cholangitis: occurs in 5% of patients with UC occurs in 5% of patients with UC & may occur in Crohn disease as well. & may occur in Crohn disease as well.
Up to 80% of patients with PSC have underlying IBD. Up to 80% of patients with PSC have underlying IBD. May present with only an isolated elevation in SAP or with May present with only an isolated elevation in SAP or with
jaundice, biliary obstruction, & evidence of portal hypertension. jaundice, biliary obstruction, & evidence of portal hypertension. These patients may have recurrent episodes of cholangitis as well These patients may have recurrent episodes of cholangitis as well
as a malignant transformation to cholangiocarcinoma& a much as a malignant transformation to cholangiocarcinoma& a much higher than normal incidence of colorectal cancer. higher than normal incidence of colorectal cancer.
Therapy with ursodeoxycholic acid has been shown to be Therapy with ursodeoxycholic acid has been shown to be chemoprotective against colon cancer. chemoprotective against colon cancer.

Extra-intestinal manifestations Extra-intestinal manifestations of IBDof IBD
Increased risk for Increased risk for CRC;CRC; the risk is associated with the age of the risk is associated with the age of onset; duration, extent, severity of disease& whether the patient onset; duration, extent, severity of disease& whether the patient has a family history of CRC. has a family history of CRC.
Annual CRC rate in extensive colitis is at least 0.5% /year after Annual CRC rate in extensive colitis is at least 0.5% /year after the first decade of colitis. the first decade of colitis.
Screening recommendations include colonoscopy every 1 to 2 Screening recommendations include colonoscopy every 1 to 2 years beginning 8 years after diagnosis. years beginning 8 years after diagnosis.
Unlike sporadic colorectal cancer that develops primarily from Unlike sporadic colorectal cancer that develops primarily from colon polyps, inflammatory bowel disease-associated colon cancer colon polyps, inflammatory bowel disease-associated colon cancer can arise from flat dysplastic mucosa which is not readily can arise from flat dysplastic mucosa which is not readily detectable from underlying inflammatory tissue. detectable from underlying inflammatory tissue.

Extra-intestinal manifestations Extra-intestinal manifestations of IBDof IBD
50% with IBD have 50% with IBD have osteopenia,osteopenia, with a substantially increased risk with a substantially increased risk of osteoporosis & fracture. of osteoporosis & fracture.
The risk is present in patients with ulcerative colitis / Crohn The risk is present in patients with ulcerative colitis / Crohn disease, in both sexes&in patients who are taking corticosteroids disease, in both sexes&in patients who are taking corticosteroids & those who have never taken them.& those who have never taken them.
Patients with prolonged IBD, malabsorption, a history of using Patients with prolonged IBD, malabsorption, a history of using corticosteroids for >3 months, cigarette smoking, older age, corticosteroids for >3 months, cigarette smoking, older age, history of fractures, or a family history of osteoporosis should be history of fractures, or a family history of osteoporosis should be evaluated for the presence of metabolic bone disease. evaluated for the presence of metabolic bone disease.
Kidney stones / gallstones are other extraintestinal manifestations Kidney stones / gallstones are other extraintestinal manifestations of inflammatory bowel disease.of inflammatory bowel disease.






Complications of IBDComplications of IBD
BleedingBleeding StrictureStricture FistulaFistula Toxic megacolonToxic megacolon Cancer: Cancer: Patients with either UC or CD have an increased risk Patients with either UC or CD have an increased risk
of intestinal dysplasia & CRC that is related to the duration, of intestinal dysplasia & CRC that is related to the duration, extent& severity of the inflammation,so those with extent& severity of the inflammation,so those with extensive/longstanding disease should undergo regular extensive/longstanding disease should undergo regular colonoscopic examinations with mucosal biopsies to detect these colonoscopic examinations with mucosal biopsies to detect these complications. complications.

Complications of Complications of IBDIBD

Dignosis/assessing severity & Dignosis/assessing severity & extent:extent:
Should be considered in any young patient with chronic Should be considered in any young patient with chronic diarrhea or hematochezia.diarrhea or hematochezia.
Infection should be excluded by stool culture for ova/ Infection should be excluded by stool culture for ova/ parasites, parasites, Giardia&Giardia& Clostridium difficileClostridium difficile..
Laboratory findings suggestive of IBD include anemia, Laboratory findings suggestive of IBD include anemia, hypoalbuminemia, leukocytosis, vitamin deficiencies (more hypoalbuminemia, leukocytosis, vitamin deficiencies (more likely in small-intestinal Crohn disease than ulcerative likely in small-intestinal Crohn disease than ulcerative colitis). colitis).

Dignosis/assessing severity & Dignosis/assessing severity & extent:extent:
2/3 with ulcerative colitis, but only 15- 20% with Crohn disease 2/3 with ulcerative colitis, but only 15- 20% with Crohn disease &< 5% of persons without IBD have p-ANCA&< 5% of persons without IBD have p-ANCA,, a serum antibody a serum antibody directed against a particular histone H1 antigen& detectable by directed against a particular histone H1 antigen& detectable by immunofluorescence or specific enzyme immunoassay. immunofluorescence or specific enzyme immunoassay.
Approximately 50% with Crohn disease have anti-Approximately 50% with Crohn disease have anti-Saccharomyces Saccharomyces cerevisiaecerevisiae antibodies (ASCA), as opposed to < 5% of patients with antibodies (ASCA), as opposed to < 5% of patients with ulcerative colitis &control subjects. ulcerative colitis &control subjects.
So measuring both serum p-ANCA & ASCA is reasonably So measuring both serum p-ANCA & ASCA is reasonably reliable for the diagnosis of Crohn disease or ulcerative colitis. reliable for the diagnosis of Crohn disease or ulcerative colitis.
Newer antibody tests, directed against the outer membrane porin Newer antibody tests, directed against the outer membrane porin of of Escherichia coliEscherichia coli (Omp-C)& against the flagellum of pathogenic (Omp-C)& against the flagellum of pathogenic polyflagellated organisms (Cbir1), are also predictive of classic polyflagellated organisms (Cbir1), are also predictive of classic Crohn disease,but not differentiating atypical presentations or Crohn disease,but not differentiating atypical presentations or diagnosing indeterminate colitis. diagnosing indeterminate colitis.

Dignosis/assessing severity & Dignosis/assessing severity & extent:extent:
50% with ulcerative colitis have proctosigmoiditis only50% with ulcerative colitis have proctosigmoiditis only 15-20% have left-sided disease. 15-20% have left-sided disease. 1/3 present with pancolitis. 1/3 present with pancolitis. Patients with proctitis generally have a benign course, but Patients with proctitis generally have a benign course, but
11% develop more extensive disease by 5 years&19% by 11% develop more extensive disease by 5 years&19% by 10 years. 10 years.
Endoscopic findings range from a decreased vascular Endoscopic findings range from a decreased vascular pattern& minimal friability in patients with mild disease to pattern& minimal friability in patients with mild disease to spontaneous bleeding&deep ulcerations in severe disease. spontaneous bleeding&deep ulcerations in severe disease.
Histopathology typically consists of crypt abscesses with Histopathology typically consists of crypt abscesses with branching&architecture distortion& acute/ chronic branching&architecture distortion& acute/ chronic inflammation. inflammation.

Dignosis/assessing severity & Dignosis/assessing severity & extent:extent:
Crohn disease has a different pattern of distribution than Crohn disease has a different pattern of distribution than ulcerative colitisulcerative colitis
30% having isolated small-bowel disease30% having isolated small-bowel disease 25% colonic disease25% colonic disease 40% ileocolonic disease.40% ileocolonic disease. A few patients have upper GIT or isolated perianal disease in A few patients have upper GIT or isolated perianal disease in
the absence of colonic inflammation. the absence of colonic inflammation. The mildest endoscopic lesions are aphthous ulcers, which can, The mildest endoscopic lesions are aphthous ulcers, which can,
however, coalesce to form deep ulcerations&cobblestone however, coalesce to form deep ulcerations&cobblestone appearance. appearance.
Affected areas are commonly separated by normal mucosa, the Affected areas are commonly separated by normal mucosa, the so-called “skip lesions” that are the hallmark of Crohn disease. so-called “skip lesions” that are the hallmark of Crohn disease.
Granulomas are almost pathognomonic of Crohn disease but Granulomas are almost pathognomonic of Crohn disease but are rarely seen on endoscopic mucosal biopsies. are rarely seen on endoscopic mucosal biopsies.

Dignosis/assessing severity & Dignosis/assessing severity & extent:extent:
Radiographic studies establish the location, extent& Radiographic studies establish the location, extent& severity of inflammatory bowel disease. severity of inflammatory bowel disease.
The plain abd radiograph can show a dilated colon& The plain abd radiograph can show a dilated colon& small-bowel obstruction. small-bowel obstruction.
A barium-contrast small-bowel series or enteroclysis A barium-contrast small-bowel series or enteroclysis provides information about location& amount of provides information about location& amount of inflammatory or stricturing small-bowel disease. inflammatory or stricturing small-bowel disease.
Separation of loops of bowel, thumbprinting,spiculation Separation of loops of bowel, thumbprinting,spiculation (formation of needle-like projections) are all indicators of (formation of needle-like projections) are all indicators of jejunoileitis. jejunoileitis.
CT enterography is the most comprehensive study, CT enterography is the most comprehensive study, highlights the areas of bowel inflammation,stricture, highlights the areas of bowel inflammation,stricture, abscesses, fistulae& mesenteritis. abscesses, fistulae& mesenteritis.

Dignosis/assessing severity & Dignosis/assessing severity & extent:extent:
Video capsule endoscopy provides the most direct evidence Video capsule endoscopy provides the most direct evidence of small bowel ulcerations & approved in the diagnosis of of small bowel ulcerations & approved in the diagnosis of Crohn disease. Crohn disease.
It is highly sensitive& can lead to a false-positive diagnosis It is highly sensitive& can lead to a false-positive diagnosis because 15% of normal volunteers may have ulcerations in because 15% of normal volunteers may have ulcerations in the small bowel. the small bowel.
In a patient with possible obstruction, a patency capsule, In a patient with possible obstruction, a patency capsule, which is a capsule system designed to determine small-which is a capsule system designed to determine small-bowel patency before video capsule endoscopy, should be bowel patency before video capsule endoscopy, should be ingested by the patient.ingested by the patient.











TreatmentTreatment :outline :outline
Treatment of inflammatory bowel Treatment of inflammatory bowel disease involves drug therapy disease involves drug therapy and in certain cases surgeryand in certain cases surgery

TreatmentTreatment : :Medication Indication Side Effects
5-ASA (sulfasalazine, olsalazine,
balsalazide, mesalamine:
oral, rectal UC: induction/maintenance
CD (weak): induction/maintenance
Inters nephritis (rare
Diarrhea (olsalazine)

TreatmentTreatment : :Medication Indication Side Effects
Antibiotics: Metronidazole, Ciprofloxacin CD: perianal/ colonic disease
Metronidazole:PN , metallic taste, antabuse effect
Ciprofloxacin: arthropathy, seizure(

TreatmentTreatment : :Medication Indication Side Effects
CS (oral, IV, rectal) UC/CD: induction, not maintenance
Acne, moon facies, truncal obesity, osteoporosis, osteonecrosis, DM, hypertension, cataracts, inf
Budesonide CD (ileal/R colon): induction Minimal CS effects

TreatmentTreatment : :Medication Indication Side Effects
Methotrexate CD: induction/maintenance
Bone marrow suppression, hepatotoxicity, pulmonitis
6-MP, Azathioprine UC/CD: steroid withdrawal, maintenance
Pancreatitis, fever, infection, leukopenia, hepatotoxicity, lymphoma
Anti–TNF-α: Infliximab UC/CD: induction/maintenance
Infusion reaction, tuberculosis reactivation, demyelination, infection,HF,Lymphoma.Adalimumab UC/CD: induction/maintenance
Cyclosporine UC: steroid refractory
Hypertension, nephro &neurotoxicity

TreatmentTreatment : :Crohn DiseaseCrohn Disease 5-Aminosalicylates MOA: anti-inflammatory effects secondary to inhibition of
arachidonic acid in the bowel mucosa by cyclooxygenase. 5 oral formulations developed from sulphaslazine. 2 mesalamines are released in the small bowel in a pH- time-
dependent manner used to treat both CD &ulcerative colitis. Mesalamine is available in suppository & enema formulations,
which are effective alone in patients who have inflammation limited to the rectosigmoid & may also be used in combination with an oral 5-ASA.

TreatmentTreatment : :Crohn DiseaseCrohn Disease Because Crohn disease is a transmural disease, the 5-ASA agents
have not proved to be as efficacious as they are in ulcerative colitis but are often used in the treatment of mild disease.
Delayed-release mesalamine is commonly used for SB disease. Other preparations of mesalamine are released in the distal
ileum& therefore may have a role in treating ileal disease. The azo-bonded 5-ASAs, such as balsalazide, olsalazine, and
sulfasalazine have a potential effect only in Crohn colitis.

TreatmentTreatment : :Crohn DiseaseCrohn Disease CSs: Ileal-release preparations of budesonide are indicated for the
treatment of patients with mild ileal & right-sided colonic Crohn disease.
Budesonide is a topically active corticosteroid with a very high affinity for the glucocorticoid receptor (*15 that of prednisolone *195 that of hydrocortisone).
Only 10-15% of the drug reaches the systemic circulation; the rest is converted in the liver to inactive metabolites.
Conventional corticosteroids are effective in the short-term induction of remission in patients with Crohn disease but are generally used in patients with moderate disease at any location or in patients with ileal disease who have failed to respond to the 5-ASAs or budesonide.
Because of the toxic effects of long-term corticosteroid therapy (for example, osteoporosis, avascular necrosis, psychosis), it is important to devise a strategy for tapering the dosage& discontinuing corticosteroid therapy before the therapy is started.

TreatmentTreatment : :Crohn DiseaseCrohn Disease Immunomodulator:Azathioprine/ 6-mercaptopurine Their onset of full activity is slow, may take up to 3 months. These drugs are effective for the maintenance of remission in
patients with Crohn disease regardless of disease distribution. Adverse side effects include leukopenia, hepatotoxicity. Before being treated with these agents, patients should be tested
for thiopurine methyltransferase, the enzyme involved in the conversion of 6-mercaptopurine to inactive metabolites; patients who have low enzyme activity (or who are homozygous deficient in thiopurine methyltransferase) should not be treated with these agents.
Methotrexate is an immunomodulator induce / maintain remission in Crohn disease but not in ulcerative colitis.
There is a risk for hepatotoxicity& patients with persistently elevated liver tests may need to undergo liver biopsy.
Methotrexate is both a teratogen&abortifacient contraindicated in pregnant patients & breastfeeding.

TreatmentTreatment : :Crohn DiseaseCrohn Disease Biologicals: (TNF-α) is a potent proinflammatory cytokine involved in the
pathogenesis of both IBDs. Infliximab / adalimumab are monoclonal antibodies against TNF-α:
infliximab a chimeric antibody givenIV; adalimumab / certolizumab are humanized antibodies given subcutaneously.
These medications can reduce & close fistulae&induce remission in inflammatory Crohn disease within 4 to 8 weeks.
? earlier use of potent biologic therapies to induce remission quickly while sparing the effects of systemic corticosteroid therapy.
All three anti-TNF-α agents are contraindicated in patients with active tuberculosis, tuberculin skin test / chest radiograph are required before the initiation of therapy.
Patients with latent tuberculosis require isoniazid prophylaxis because the disease can reactivate.
Treatment can lead to the reactivation of viral hepatitis , results in other infections& possibly lymphomam,specially concomitant use of infliximab /6-mercaptopurine.

TreatmentTreatment : :Crohn DiseaseCrohn Disease Biologicals: In fibrostenotic stricturing disease leading to bowel obstruction,
there is generally no viable medical therapy. Limited small-bowel or ileocolic resection or bowel-sparing small-
bowel stricturoplasties are the only therapy in this setting. Recurrence of disease at the sites of previous surgery is common,
and therefore surgery is not a preferred strategy for inflammatory disease.
3 months of metronidazole reduce severe recurrences 12 months after surgery.
6-mercaptopurine& likely azathioprine is modestly effective for decreasing both endoscopic&clinical postoperative recurrences in patients with Crohn disease.

TreatmentTreatment : :UCUC The choice depends on both severity& extent of disease. The 5-ASAs, which are not widely effective in Crohn disease, have
well-documented efficacy& remain the mainstay of both induction & maintenance therapy in mild to moderate ulcerative colitis.
The 5-ASAs are the only medications shown to be effective as chemoprophylaxis for colorectal cancer in patients with ulcerative colitis.

TreatmentTreatment : :UCUC CSs: In patients not responsive to the 5-ASAs or in those with more
severe disease, corticosteroids may induce remission. In hospitalized patients IV therapy is usually administered,
whereas in the outpatient setting oral & rectal corticosteroids are used.
No dose effect above the equivalent of prednisone 60 mg/d has been found.
Corticosteroid therapy does not maintain remission & is appropriate only as short-term therapy.
Although some patients may be put back successfully to 5-ASA as maintenance therapy after corticosteroid induction therapy, often an immunomodulator such as 6-mercaptopurine or its prodrug azathioprine is warranted; these agents are corticosteroid-sparing & maintain remission.

TreatmentTreatment : :UCUC Inflixi/cyclospoine: If corticosteroid therapy does not induce remission, patients may
be treated with either infliximab or cyclosporine; in hospitalized patients, these medications are considered after a 7- to 10-day trial of corticosteroids.
Cyclosporine requires close monitoring for hypertension, neurologic& renal toxicity, infliximab may be favored despite its increased risk for opportunistic infection & possibly malignancy.

TreatmentTreatment : :UCUC Surgery: Medically refractory UC is treated surgically with curative total
proctocolectomy with either end-ileostomy or ileal pouch-anal anastomosis, in which a neorectum is constructed from a segment of ileum and connected to the anus to retain continence.
Total proctocolectomy may also be warranted in patients with neoplasia, toxic megacolon, perforation, and refractory bleeding.

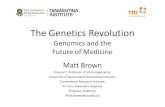
Infliximab - mucosal healing
Baseline Week 10 Week 54
Rutgeerts et al. DDW 2002: [abstract] W1367.


Microscopic colitis Microscopic colitis is another type of IBD and may be classified as
lymphocytic colitis or collagenous colitis. The incidence of microscopic colitis parallels that of ulcerative
colitis, more common in northern industrialized countries. The disorder occurs disproportionately in middle-aged women,
with a peak incidence at age 65 years. Symptoms include a chronic relapsing-remitting pattern of watery
diarrhea that varies in severity and may be accompanied by weight loss, abdominal pain, fatigue, and nausea.
Comorbid autoimmune diseases are common, including thyroid disorders, celiac disease, diabetes mellitus, RA.
The cause is probably multifactorial& likely represents an abnormal mucosal response to various luminal exposures including infection and drugs such as NSAIDs.
The mucosa usually appears normal macroscopically Diagnosis is made solely on characteristic histologic findings.

Microscopic colitis Collagenous colitis is characterized by a thickened subepithelial
collagen layer Lymphocytic colitis by increased number of intraepithelial
lymphocytes is found in. Supportive treatment with antidiarrheal agents, as loperamide,
bismuth subsalicylate, diphenoxylate, may be effective for mild cases.
Otherwise, budesonide has the best-documented efficacy; prednisolone, 5-ASA, antibiotics& probiotics have been studied but the data is less robust.