Gingival curettage
52
GINGIVAL CURETTAGE DR. SWAPNIL BORKAR I-YEAR POST GRADUATE STUDENT DEPARTMENT OF PERIODONTICS & ORAL IMPLANTOLOGY S.D.K.S DENTAL COLLEGE NAGPUR 1
-
Upload
drswapnil16 -
Category
Education
-
view
2.385 -
download
9
description
Transcript of Gingival curettage

1
GINGIVAL CURETTAGE
DR. SWAPNIL BORKARI-YEAR POST GRADUATE STUDENT
DEPARTMENT OF PERIODONTICS & ORAL IMPLANTOLOGYS.D.K.S DENTAL COLLEGE
NAGPUR

2
Introduction Definitions History Terminology Procedure
Basic Technique Indication
ContraindicationExcisional New Attachment Procedure Modified ENAP Indication Contraindication Advantage Disadvantage
Caustic Drug Ultrasonic curettage
Clinical Appearance After Curettage Healing After Curettage Studies AAP Statement Regarding Gingival curettage

3
INTRODUCTION“CURETTE”: From the Latin term “curare”, to care or to cure. Then to French curer means to careBronze curette have been found in Egyptian tombs

4
Definitions :The term "gingival curettage" implies directing an operative
instrument against the gingival wall of the periodontal pocket in order to remove the ulcerated epithelium covering the sulcus.
( Nestor & Lopez ,1977)
Curettage is a technique designed to remove, by surgical debridement, the inner aspect of the diseased gingival wall, including the ulcerated and hyperplastic pocket epithelium and the contiguous zone of damaged connective tissue downward and outward to the firm and intact aspect of the gingival corium
(Simon Kon 1968 )The word curettage is used in periodontics to mean the scraping
of the gingival wall of a periodontal pocket to separate diseased soft tissue
(F.A. carranza 10th edition )

5
Rationale:
Curettage is the conversion of chronic inflammatory ulcers to the
gingival wall of the pockets into surgical wound. Curettage can be used alone
as the separate procedure after root planing has to perform or as in
combination with root planing to eliminate the pocket.
The end result of the therapy is that the remaining gingival wall will
shrink via resolution of inflammatory infiltrates and the drainage of tissue
fluid from the wound, the exposed connective tissue from the contiguous oral
epithelium will re epithelialize , the new lamina propria subjacent to the new
sulcular lining and epithelial attachment forms, and the microvascularization
of the tissue will return to the original quality and distribution.

6
History :
1902 –Zanmensky published the classic paper ”Alveolar Pyorrhea –
Its pathological anatomy and its radiacal treatment. The infiltration
with white blood corpuscles is still not deep, it embraces almost
exclusively the papillary layer of gum ; the bone of socket is yet
normal…”
He treated Pyorrhea with removal of calculus and also deep
curettage of the sockets, using cocaine anesthesia
1845-1928 -Salomon Robicsek He developed a surgical technique
consisting of a scalloped continuous gingivectomy excision, exposing
the marginal bone for subsequent curettage and remodeling

7
History :
1935-kronfeld proved that the bone in the peiodontal pockets was
neither necrotic nor infected but rather destroy by inflammatory
process, and the era of tissue curettage began as the attention was
shifted to the soft tissue surrounding the tooth as the source of
infection.
The rationale for the radical treatment was supported by the
authors such as Neuman, Widman , Robicsek ,Zemsky , Ceszynki and
Nodine who popularized the surgical procedures for the elimination of
periodontal pocket.

8
1948- Goldman discussed the rationale for curettage and
differentiated between those designed for elimination of gingival
pocket. He stated that the cure can be accomplished when the
diseased epithelium lining and attachment and the altered gingival
corium are eliminated.
He later observed the soft tissue curettage with the use of
ultrasonic instruments.
1969- Morries,Moskow & Simao Kon,goldman
Carried out a study on the healing of periodontal pocket &
microvascularization of healing of periodontal wound.

9
Terminology :-
Gingival curettage Removal of the inflammed soft
tissue lateral to the pocket wall.
Subgingival curettage Procedure that is performed
apical to the epithelial attachment, severing the
connective tissue attachment down to the osseous crest.
Inadvertent curettageSome degree of curettage is
done unintentionally when scaling and root planing is performed.

10

11
Basic technique : Curettage is a closed, definitive surgical procedure
performed under local anesthesia and aimed at pocket reduction, elimination, reattachment, or new attachment.
It is indicated primarily for edematous suprabony pockets,
where shrinkage and a reduction in inflammation will result in a shallow sulcus, or prior to surgery for pocket elimination to reduce inflammation (Hirschfeld, 1952).
It is performed with sharp curettes in an attempt to remove:
(1) The sulcular epithelium and the epithelial attachment and
(2) The inflammed connective issue of the pocket wall

12
Indications :
1. Edematous and inflammed tissues2. Shallow pockets3. Suprabony pockets4. As part of initial preparation prior to opensurgical procedures in an attempt to achievetissue quality that can be handled easily5. Progressive attachment or alveolar bone loss6. Increased levels of pathogenic
microorganisms

13
Contraindications :
1. Fibrotic tissue2. Deep pockets ≥ 5mm3. Furcation involvements4. Medically compromised patient

14
Basic Technique with a Curette
Instruments: Gracey curettesUniversal curettes
Isolation & Anesthetize : Local infiltration is given to anesthetize the
isolated selected site.
Insertion of Curettage : Sharp Gracey or Universal curette is
inserted with the cutting edge against the tissue so as to engage the inner lining of pocket wall & junctional epithelium.

15
Curette the soft tissue wall :Curette is carried along the soft tissue in a horizontal strokeThe pocket wall is supported by gentle finger pressure on the
external surfaceSeveral overlapping strokes are used to completely remove
the epithelium & underlying granulation tissue . In subgingival curettage, the tissue attached to the
bottom of the pocket & alveolar crest are removed with a scooping motion of the curette to the tooth surface.Irrigation :Irrigate the area to remove debris & press the tissue to the tooth surface gently which enables the arrest of bleeding & adaptation of soft tissue to the root surfaceSuturing :
Indicated if the clot area has been disrupted & the papilla have been separated.Healing :
It will result in shrunken, firm well adapted & well contoured tissue.

16

17
Excisional New Attachment Procedure (ENAP)
1931 Kirkland described a modified flap operation for treating periodontal disease 1939 Barkann described a conservative surgical approach to treat periodontal pockets. Barkann's procedure closely approximates the ENAP technique reported on by Yukna et al. 1976
The ENAP is essentially subgingival curettage performed with a knife.
Objectives :
•permit thorough soft tissue preparation•secure better access to the root surface•advantages over traditional subgingival curettage is the definitive, clean excision of the junctional epithelium and the subjacent tissue with a greater probability of new clinical attachment

18
Indications
1. Suprabony pockets2. Adequate keratinized tissue3. When esthetics are unimportant
Contraindictions
1. Pockets exceed mucogingival junction2. Edematous tissue3. Lack of keratinized tissue4. Osseous defects must be treated5. Hyperplastic tissue6. Close root proximity7. Furcation involvement8. Probing depths of 3 mm or less

19
Advantages
1. Improved root visualization2. Complete removal of sulcular epithelium and
epithelial attachment3. Minimal gingival trauma4. No loss of keratinized gingiva
Disadvantages
1. Difficult to determine apical extent of epithelial attachment
2. Does not result in new attachment

20
Procedure : Instruments
Surgical handle (Bard parker no. 3) surgical blades no. 11, 12, 15
CurettesTechnique Scaling and root planing are performed at least 1
week before the ENAP, which increases the healing potential
Anesthesia Adequate anesthesia is given, after which pockets are
checked to ensure that the zone of keratinized tissue is adequate and that the pockets do not exceed the mucogingival junction

21
Incision : With a no. 11 or no. 15 scalpel blade, a scalloped, partial-thickness, inverse-beveled incision is made from the crest of the gingiva to the base of the sulcus.
The incisions are carried facially, lingually, and interproximally as far as possible. The papilla is thinned interproximally to remove any inflammed connective tissue and the triangular wedge of interproximal tissue. This tissue is difficult to remove once the flap is free.
Removal of the tissue :With scalers and curettes, the inflammed
granulated and excised tissues are removed. All tissue tags are carefully removed. The root is scaled until it is hard and smooth and is free of calculus and softened cementum.

22
Irrigation The area is flushed with normal saline to remove
debris, blood clots, and tissue tags.
Suturing Interproximal sutures are used to position the tissue
as closely as possible to the presurgical height and to adapt the papillae and tissue tightly about the necks of the teeth. Primary closure is desirable.
Dressing A periodontal dressing is now placed interproximally,
without being forced.

23
Clinical improvement was reported at 1 and 3 year evaluations following the procedure but probing depths increased slightly and the amount of newly gained attachment decreased slightly at each postoperative evaluation from 1 to 5 years. However, an overall gain of 1.5 mm in clinical attachment was still evident 5 years after the treatment.
Studies by Yukna (1980) and associates suggest a trend towards a relapse somewhere around the 5-year mark.
Since no clinically significant tissue loss occurs with this technique, retreatment by the ENAP procedure every 5 years or so may well preserve the maximum amount of attachment for the longest possible time.
Both subgingival curettage and ENAP have the advantage of minimizing postsurgical recession and root sensitivity because the free gingival margin is kept virtually intact and tissue elevation is not a part of these procedures.

24

25
ENAP ModificationIn 1977, Fredi and Rosenfeld modified the
technique by advocating a partial-thickness inverse beveled incision down to the crest of bone to completely remove tissue about the periodontal ligament. The flaps were then sutured at the presurgical height . The technique is basically the same in all other aspects
A. Initial incision made to the crest of bone of the pocket
B. Inner wall removed down to the crest of bone & periodontal ligament
C. Healed tissue

26
Caustic Drugs. Since early in the development of periodontal procedures, the use of caustic drugs has been recommended to induce a chemical curettage of thelateral wall of the pocket or even the selective eliminationof the epithelium.
Drugs such as :sodium sulfidealkaline sodium hypochlorite solution (Antiformin),phenol
These drugs were discarded after studies showed their ineffectiveness. The extent of tissue destruction with these drugs cannot be controlled,and they may increase rather than reduce the amount of tissue to be removed by enzymes and phagocytes (Kenneth – 1981) (Lorraine et al-1986)

27
Ultrasonic Curettage.
The use of ultrasonic devices has been recommended for gingival curettage.When applied to the gingiva of experimental animals, ultrasonic vibrations disrupt tissue continuity, lift off epithelium, dismember collagen bundles, and alter the morphologic features of fibroblast nuclei.
Ultrasound is effective for debriding the epithelial lining of periodontalpockets. It results in a narrow band of necrotic tissue (microcauterization), which strips off the inner lining of the pocket
The Morse scaler-shaped and rod-shaped ultrasonic instrumentsare used for this purpose.
Nadler H-1962 found ultrasonic instruments to be as effective as manualinstruments for curettage but resulted in less inflammationand less removal of underlying connective tissue.

28
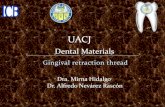
CLINICAL APPEARANCE AFTER SCALING AND CURETTAGE
Immediately after scaling and curettage, the gingiva appearshemorrhagic and bright red.
After 1 week, The gingiva appears reduced in heightowing to an apical shift in the position of the gingivalmargin. The gingiva is also slightly redder than normal,but much less so than on previous days.
After 2 weeks The normal color, consistency, surface texture, and
contour of the gingiva are attained, and the gingivalmargin is well adapted to the tooth

29
Clinical Appearance Of Gingiva

30
Visualization Of Microvascularization Of The Healing Periodontal Wound Followed By Curettage(Simao kon , H. Goldman et al 1969)
A study was carried out for the purpose of observingthe wound healing process and the behaviour of the bloodvessels when curettage was performed. Pelikan carbon black suspension (Gunther Wagner) was filtered andinjected into the common carotid arteries of youngadult mongrel dogs.The perfusion technique was performed 2, 4, 6, 7, 12, 16, 23, 31,38, 55 and 85 days after the curettage.The macroscopic aspect of the wound was evaluatedclinically by means of kodachromes. Sections (8microns in thickness) were stained by the Mallory technique(Goldman-Bloom modification) and Hematoxylin-Eosin.
HEALING FOLLOWED BY CURETTAGE

31
Zero Hour.
The connective tissue at the sulcus was exposed and in few animalswhen epithelial cells remained they were at the tip of the margin, at the middle area of the sulcus or at both locations. Beyond the epithelial attachment the connective tissue was sometimes torn from over-curettement. When the tissue was torn and the perfused material flowed into the sulcus, more vascularization was seen and there was some Hemorrhaging. The capillary loops in the rete peg area were easily observed due to the perfusion with carbon black. No inflammatory cells were present in the sulcular area.

32
Two Days.
In this animal the blood clot covers the entire sulcular area. There are no epithelial
cells from the tip of the margin to the cementum enamel junction( C E J ) .
The underlying connective tissue is still disorganized.
The connective tissue surface derived from this hand curettage is irregular but is corrected
by the blood clot which presents an even surface. A large perfused vessel seems
to give rise to the blood clot formation,
as demonstrated by the continuity between
the carbon black and the clot. No change could
be detected in the oral epithelium.

33
Four Days.
The whole area has a thick blood clot andthere was a hemorrhage deep in the connective tissue, caused by the instrument.

34
The sulcular epithelium is being formed by a proliferation of the oral epithelium which migrates underneath the clot.The subsulcular connective tissue is still disorganized.

35
Six Days. The epithelium already covers the cut surface of the connective tissue. It is very thin, being formed by an average of five layers of flat epithelial cells. The connective tissue is healed and there is noapparent inflammatory infiltrate. A large number of loaded small capillaries is present directly beneath the sulcular epithelium. At the cemento-enamel junction the bottom of the long epithelial attachment and the insertion of Group III fibers can be seen forming a well collagenated area. Group I is still disorganized..

36

37
Seven Days.
It is also completely epithelized as far as the cementum enamel junction. The epithelium is thin, but irregular and there are some epithelial projections.
Many desquamated cells and debris are present in the sulcus, in which area there is an inflammatory response.

38
12 Days.
The sulcular epithelium remains thin and is located at the
cementum enamel junction. Keratinization is present at the margin
where the sulcular and oral epithelium join. There is no
inflammatory infiltrate
in the connective tissue which underlies the newly
formed sulcular epithelium. It is well collagenated,
and Group I fibers as well as the subsulcular capillaries
show some semblance of organization.
The tip of the margin is well vascularized

39

40
16 Days.
The sulcular epithelium remains at the cementum enamel junction. It is thin and
there are no rete pegs. There is a flattening of cells against the enamel, forming the cuticle which identifies the bottom of the new sulcus. The connective tissue is well organized, with little vascularization and without inflammatory infiltrate. Group I fibers are not as distinguishable at this stage.

41
23 Days.
No significant change in the epithelium and vascularization can
be observed; however, Group I fibers seem to be better organized
and there is more delineation.
There are more dark spots of carbon black at the tip of the margin.
Flat cells, separated from the sulcular epithelium, form a cuticle
that remains free at the enamel space.

42
31 Days.
There is no significant difference between this specimen and that of the 23-day specimen. The sulcular epithelium appears to be somewhat thicker and there is a noticeable increase in vascularization, predominantly at the gingival margin. The epithelial attachment remains at the cementum enamel junction

43
38 Days.
The sulcus remains normal, with no inflammation, and the connective tissue is well collagenated. Fewer vessels can be observed here than in the control, since there is no inflammatory reaction.

44
Studies1949 Henry M. Goldman conducted a study for a treatment
of intrabony pockets with subgingival curettage procedure and he concluded that new bone formation has been achieved in all the 6 cases
1971 Herbert Oshrain, Albart Salkind conducted a study in which , a contoured mylar strips were inserted into periodontal pockets immediately after curettage, removed after ten minutes and examined for microbial population.
A viable flora was present subgingivally which probably represents remnants of a pre curettage population.
1977 Nestor Lopez , Mario conducted a comparative study to check effects upon gingival inflammation by subgingival scaling with root planing and curettage.
They concluded , the clinical appearance of gingiva after 14 days was similar in both groups where as the depth of gingival sulcus recorded prior the treatment & 4 and 6 weeks following treatment suggest that curettage accomplish a greater retraction of the gingiva than subgingival scaling and root planing.

45
Dennis et. Al. 1980 conducted his study for
testing short term clinical differences in
periodontal status after treatment with osseous
recontouring and flap curettage in humans.
Twelve systemically healthy patients with
bilaterally similar marginal periodontal
destruction received a standardized presurgical
therapy.
The posterior segments of these patients
were then treated with osseous recontouring and
flap curettage.

46
Following results are obtain in his study
(1) Osseous recontouring and open flap curettage equally
reduced plaque and gingival inflammation;
(2) Each surgical procedure equally increased attached gingiva;
(3) Pocket reduction achieved with osseous recontouring was
maintained over 6 months, pockets recurring after open
curettage;
(4) Open curettage did not induce bone regeneration;
(5) Osseous recontouring did not result in irreversible tooth
mobility;
(6) Osseous recontouring resulted in a net loss of attachment;
open curettage producing a net gain, especially in deeper
pockets;
(7) Both procedures improved periodontal health.

47
1981 Kenneth, tussing et al conducted a study
in which a histological evaluation of gingival
curettage was performed by sodium hypochlorite
solution.
According to this study chemical curettage
gives better results than routine gingival
curettage therapy
Predictable , uniform removal of pocket lining
Local anesthesia is not required
Reduce hemorrhage due to the styptic action of
sodium hypochlorite solution allowing better
vision and easier tissue management.

48
1984 Harold Meador , James et al were conducted
a study to evaluate long term effectiveness of
periodontal therapy in clinical practice.
In this study various periodontal therapies were
assessed such as non surgical treatment , close
curettage, open curettage, modified widman flap and
osseous surgery.
The major conclusions were that the modified widman
flap and open curettage were more effective that flap
and osseous surgery and much more effective than
close curettage

49
1986 Lorraine B Forgas , sherry Gound were conducted a study
to
investigate the effect of Antiformin-citric Acid chemical curettage
Combine with SRP would significantly reduce pathogenic bacteria
of the periodontal pocket when compared to SRP alone.
No significant result were found
1988 G. Biagini , L. checchi et al were conducted a study to
evaluate
Gingival repair in periodontitis were treated with scaling and root
planing
Performed with ultrasonic and hand scalers.
In this study no differences were found in the histological features of
repair
Process triggered by either type of scaler

50
AAP Statement Regarding Gingival curettage (2002)
The American Dental Association has deleted that code from the fourth editionOf current Dental Terminology(CDT-4). In addition the American Academy of Periodontology in its Guidelines for peiodontal therapy, did not includeGingival curettage as a method of treatment

51
Lindhe J, Nyman S. The effect of plaque control and surgical pocket elimination on the establishment and maintenance of periondontal health. A longitudinal study of periodontal therapy in cases of advanced disease. J Clin Periodontol 1975;2:67–79.
Stern T, Everett F, Robicsek K. S. Robicsek a pioneer in the surgical treatment of periodontal disease. J Periodontol 1965;36:265–268.
The American Academy of Periodontology; Glossary of Periodontal Terms, 3rd ed. Chicago; The American Academy of Periodontology; 1992
Nabers, CL. Repositioning the attached gingiva. J Periodontol 1954;25:38–39.
Newman M, Sanz M, Nachnani S, Saltini C, Anderson L. Effect of a 0.12% chlorhexidine on bacterial colonization following periodontal surgery. J Periodontol 1989;60:577–581.
Becker W, Becker BE, Ochsenbein C, et al. A longitudinal study comparing scaling osseous surgery and modified Widman procedures. Results after 1 year. J Periodontol 1988;59:351–365.
Trylovich D, Cobb C, Pippin D, Spencer, P, Killoy W. The effects of Nd:YAG laser on in-vitro fibroblast attachment to endotoxin treated root surfaces. J Periodontol 1992;63:626–632
Chace, R.: Subgingival curettage in periodontal therapy. J Periodontol 45:107, 1974

52
Raust, G.: What is the value of gingival curettage in periodontal therapy. Periodont Abst 17:142, 1969.
Beube, F.: A rationale approach to periodontal surgery. Dent Clin North Am 4:425, 1960
Caton, J. and Zander, H.: The attachment between tooth and gingival tissues after periodic root planning and soft tissue curettage. J Periodontol 50:462, 1979