Gingival Bleeding
25
DEPARTMENT OF PERIODONTICS A SEMINAR ON GINGIVAL BLEEDING Presented by SYED NABI AHMED C.R.I.
-
Upload
callmeantz -
Category
Documents
-
view
4.667 -
download
49
Transcript of Gingival Bleeding

DEPARTMENT OF PERIODONTICS
A SEMINAR ON
GINGIVAL BLEEDING
Presented bySYED NABI AHMEDC.R.I.

INTRODUCTION
The two earliest symptoms of gingival
inflammation proceeding established gingivitis are
(1) increased gingival crevicular fluid production rate
(2) bleeding from gingival sulcus on gentle probing.

Gingival bleeding varies in severity, duration and
the ease with which it is provoked.
Bleeding on probing is easily detectable clinically
& therefore is of value for the early diagnosis and
prevention of were advanced gingivitis.
Pregnancy gingivitis.

It has been known that bleeding on probing
appears earlier than a change in color or other visual
signs of inflammation, in addition the use of
bleeding rather than color changes to diagnose early
gingival inflammation is advantages in that bleeding is a
were objective sign that requires less subjective
estimation.

CLASSIFICATION
Gingival bleeding can be due to a series of
factors, which can be grouped broadly into two
categories such as
Local
Systemic

Local factors
a. Infectious
Acute : 1. ANUG (Acute Necrotizing
Ulcerative Gingivitis)
2. AHGS (Acute Herpetic
Gingive Stomatitis)
Chronic : 1. Gingivitis
2. Periodontitis

b. Traumatic
1. Brushing
2. Food impaction
3. Irritation (due to prosthesis)
4. Tooth pick injury
5. Gingival burns
c. Post Surgical
d. Congenital (eg) Hemangioma

Systemic factors
a. Deficiencies
i) Hereditary : Haemophilia A & B, Von.wille
brand’s disease
ii) Liver disease: vit K deficiency
iii) Deficiency of factor II,VII,IX,X
iv) Idiopathic: eg.Thrombocytopenic purpura
v) Leubemic
vi) Nutritional :vit A, vit C and protein deficiency

b. Dysfunctioni) Multiple myelomaii) Systemic Lupus Erythematous
c. Drugs & chemical allergiesSalicylates, anticoagulant
d. Excess: Thrombocytosis
e. Defective aggregation
f. Infections: Infections mononucleuses
g. Hereditary: Haemorhagic telengetiasis
h. Hormones: Pregnancy, Menstruation
I. Malignancies

HISTOPATHOLOGICAL ALTERATION IN GINGIVAL
BLEEDING
In gingival inflammation the following
histopathological alterations result in abnormal
bleeding:
Dilatation & eugargeuant of capillaries is thinning
or ulceration of sulcular epithelium.
Gingival Inflammation

Because the capillaries are engorged and closes to
the surface & the thinned, degenerated epithelium
is less protective, stimuli that are ordinarily
innocuous cause rupture of capillaries and gingival
bleeding.

GINGIVAL BLEEDING CAUSED BY LOCAL FACTORS
This can be divided into:
Chronic & recurrent bleeding
Acute

CHRONIC AND RECURRENT BLEEDING
The most common cause of abnormal gingival
bleeding on probing is chronic inflammation.
The bleeding is chronic or recurrent & is provoked
by mechanical trauma (e.g. from tooth brushing,
tooth picks or food impaction) or by biting into solid
foods such as apples.
Chronic Generalized diffused Gingivitis

ACUTE BLEEDING
Acute episodes of gingival bleeding are caused by
injury or occur spontaneously in acute gingival
disease.
Laceration of gingival by tooth brush bristles
during aggressive tooth brushing or by sharp pieces
of hard food can cause gingival bleeding even in the
absence of gingival disease.
Gingival burrs from foods or chemicals increase
the ease of gingival bleeding.
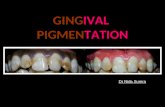
Gingival enlargement seen in a patient taking a calcium channel blocker.

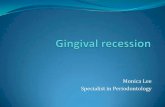
Gingival bleeding associated with systemic changes.
In some systemic disorders, gingival
haemorrhage occurs spontaneously or after
irritation and is excessive and different to
control. Such conditions have the common
feature of hemostatic mechanism failure and result
in abnormal bleeding in the skin, internal organs and
other tissues including the oral mucosa.
The various systemic conditions that can result
in gingival bleeding have been listed in the
classification.

CLINICAL EVALUATION OF GINGIVAL BLEEDING
Sites that bleed on probing have a greater area
of inflamed connective tissue (i.e., cell-ribs, collagens
per tissue) than do sites that do not bleed. In most
cases the cellular infiltrate of sites that bleed on
probing is predominantly lymphocytic. The severity of
bleeding and the ease with which it is provoked
depend on the intensity of inflammation. Hence they
can be grouped into two categories:
1. Spontaneous
2. Bleeding on provocation

SPONTANEOUS BLEEDING or bleeding on slight
provocation can occur in acute necrotizing ulcerative
gingivitis. In this condition, engorged blood vessels in
the inflamed connective tissue are exposed by
ulceration of necrotic surface epithelium.
spontaneous bleeding of the gingiva

BLEEDING ON PROVOCATION can be seen in varying
stages of the disease. In case of moderate or
advanced periodontitis, the presence of bleeding on
probing is considered a sign of active tissue
destruction.
bleeding of the gums upon probing.

Thus bleeding can be considered of diagnostic
value in many of the gingival diseases. However its
relationship to disease progression is unclean.
A periodontal probe or a wooden interdental
cleaves can be used in the evaluation of gingival
bleeding. It has to known that any force greater than
0.25N can produce gingival bleeding in healthy
tissues.

GINGIVAL BLEEDING INDICES
The clinical assessment of gingival color, form and
texture is subjective in nature, gingival bleeding is
an objective diagnostic sign of inflammation.
Periodontal probes are used with most indices
however toothpicks and dental floss are used to elicit
bleeding with some indices.
Gingival bleeding indices are used in clinical
practice, surveys of population groups and clinical
trials of antiplaque and antigingivitis agents.
Although there are many indices are available for
assessment of gingival bleeding.

Some which are used were commonly are as follows:
1. Gingival sulcus bleeding index
2. Gingival index-loe & sillness
3. Gingival bleeding index
4. Eastman interdental bleeding index
5. NIDCR protoacd for recording gingival bleeding

MANAGEMENT OF GINGIVAL BLEEDING
Increased gingival bleeding and tenderness
requires routine periodontal monitoring.
Periodontal maintenance should be titrated to
the individual patients need.
Preventive care including a vigorous program of
oral hygiene is also vial.

Hilder gingivitis eases respond well to scaling
and root planning with frequent oral hygiene
reinforcement.
Some cases of gingivitis & bleeding may require
microbial culturing, antimicrobial mouthwashes
and local site delivery, or antibiotic therapy.
Periodontal maintenance appointments may
used to be frequent when periodontal instability
is noted.

CONCLUSION
Gingival bleeding therefore is critical in early
diagnosis and prompt treatment of diseases involving
the periodontium. Proper awareness should be
inoculated in patients to consider bleeding as a early
sign of gingival disease. The woven diagnostic
techniques should also be used for their purpose.