Gina 2012 1
128
Click here to load reader
-
Upload
riskadewi-agatha -
Category
Documents
-
view
1.837 -
download
44
Transcript of Gina 2012 1

®
GLOBAL STRATEGY FORASTHMA MANAGEMENT AND PREVENTION
UPDATED 2012
© 2012 Global Initiative for Asthma
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

Global Strategy for Asthma Management and Prevention The GINA reports are available on www.ginasthma.org.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

i
GINA BOARD OF DIRECTORS*
Mark FitzGerald, MD, ChairUniversity of British ColumbiaVancouver, BC, Canada
Eric D. Bateman, MD University Cape Town Lung Institute Cape Town, South Africa
Louis-Philippe Boulet, MD Hôpital Laval Sainte-Foy, Quebec, Canada
Alvaro A. Cruz, MD Federal University of Bahia School of Medicine Salvador, Brazil
Tari Haahtela, MD Helsinki University Central Hospital Helsinki, Finland
Mark L. Levy, MD University of Edinburgh London, England, UK
Paul O’Byrne, MD McMaster University Hamilton, Ontario, Canada
Ken Ohta, MD, PhD National Hospital Organization Tokyo National Hospital Tokyo, Japan
Pierluigi Paggiaro, MD University of Pisa Pisa, Italy
Soren Erik Pedersen, M.D. Kolding Hospital Kolding, Denmark
Helen Reddel, MDWoolcock Institute of Medical ResearchCamperdown, NSW, Australia
Manuel Soto-Quiro, MD Hospital Nacional de Niños San José, Costa Rica
Gary W. Wong, MD Chinese University of Hong Kong Hong Kong ROC
GINA SCIENCE COMMITTEE*
Helen Reddel, MD, ChairWoolcock Institute of Medical ResearchCamperdown, NSW, Australia
Neil Barnes, MD London Chest Hospital London, England, UK
Peter J. Barnes, MD National Heart and Lung Institute London, England, UK
Eric D. Bateman, MD University Cape Town Lung Institute Cape Town, South Africa
Allan Becker, MD University of Manitoba Winnipeg, Manitoba, Canada
Elisabeth Bel, MDUniversity of AmsterdamAmsterdam, The Netherlands
Jeffrey M. Drazen, MD Harvard Medical School Boston, Massachusetts, USA
Mark FitzGerald, MDUniversity of British ColumbiaVancouver, BC, Canada
Johan C. de Jongste, MD, PhD Erasmas University Medical Center Rotterdam, The Netherlands
Robert F. Lemanske, Jr., MD University of Wisconsin School of Medicine Madison, Wisconsin, USA
Paul O’Byrne, MD McMaster University Hamilton, Ontario, Canada
Ken Ohta, MD, PhD National Hospital Organization Tokyo National Hospital Tokyo, Japan
Soren Erik Pedersen, MD Kolding Hospital Kolding, Denmark
Emilio Pizzichini, MD Universidade Federal de Santa Catarina Florianópolis, SC, Brazil
Sally E. Wenzel, MDUniversity of Pittsburgh Pittsburgh, Pennsylvania, USA
Global Strategy for Asthma Management and Prevention 2012 (update)
*Disclosures for members of GINA Board of Directors and Science Committees can be found at http://www.ginasthma.orgCOPY
RIGHTE
D MAT
ERIA
L - D
O NOT
ALTE
R OR R
EPRODUCE

ii
PREFACEAsthma is a serious global health problem. People of all ages in countries throughout the world are affected by this chronic airway disorder that, when uncontrolled, can place severe limits on daily life and is sometimes fatal. The prevalence of asthma is increasing in most countries, especially among children. Asthma is a significant burden, not only in terms of health care costs but also of lost productivity and reduced participation in family life.
During the past two decades, we have witnessed many scientific advances that have improved our understanding of asthma and our ability to manage and control it effectively. However, the diversity of national health care service systems and variations in the availability of asthma therapies require that recommendations for asthma care be adapted to local conditions throughout the global community. In addition, public health officials require information about the costs of asthma care, how to effectively manage this chronic disorder, and education methods to develop asthma care services and programs responsive to the particular needs and circumstances within their countries.
In 1993, the National Heart, Lung, and Blood Institute collaborated with the World Health Organization to convene a workshop that led to a Workshop Report: Global Strategy for Asthma Management and Prevention. This presented a comprehensive plan to manage asthma with the goal of reducing chronic disability and premature deaths while allowing patients with asthma to lead productive and fulfilling lives.
At the same time, the Global Initiative for Asthma (GINA) was implemented to develop a network of individuals, organizations, and public health officials to disseminate information about the care of patients with asthma while at the same time assuring a mechanism to incorporate the results of scientific investigations into asthma care. Publications based on the GINA Report were prepared and have been translated into languages to promote international collaboration and dissemination of information. To disseminate information about asthma care, a GINA Assembly was initiated, comprised of asthma care experts from many countries to conduct workshops with local doctors and national opinion leaders and to hold seminars at national and international meetings. In addition, GINA initiated an annual World Asthma Day (in 2001) which has gained increasing attention each year to raise awareness about the burden of asthma, and to initiate activities at the local/national level to educate families and health care professionals about effective methods to manage and control asthma.
In spite of these dissemination efforts, international surveys provide direct evidence for suboptimal asthma control in many countries, despite the availability of effective therapies. It is clear that if recommendations contained within this report are to improve care of people with asthma, every effort must be made to encourage health care leaders to assure availability of and access to medications, and develop means to implement effective asthma management programs including the use of appropriate tools to measure success.
In 2002, the GINA Report stated that “It is reasonable to expect that in most patients with asthma, control of the disease can, and should be achieved and maintained.” To meet this challenge, in 2005, Executive Committee recommended preparation of a new report not only to incorporate updated scientific information but to implement an approach to asthma management based on asthma control, rather than asthma severity. Recommendations to assess, treat and maintain asthma control are provided in this document. The methods used to prepare this document are described in the Introduction.
It is a privilege for me to acknowledge the work of the many people who participated in this update project, as well as to acknowledge the superlative work of all who have contributed to the success of the GINA program.
The GINA program has been conducted through unrestricted educational grants from Almirall, AstraZeneca, Boehringer-Ingelheim, Chiesi, CIPLA, GlaxoSmithKline, Merck Sharp & Dohme, Novartis, Quintiles, Takeda. The generous contributions of these companies assured that Committee members could meet together to discuss issues and reach consensus in a constructive and timely manner. The members of the GINA Committees are, however, solely responsible for the statements and conclusions presented in this publication.
GINA publications are available through the Internet (http://www.ginasthma.org).
Mark FitzGerald, MDProfessor of MedicineHead, UBC and VGH Divisions of Respiratory MedicineDirector, Centre for Lung HealthCo-Director Institute for Heart and Lung HealthThe Lung Centre, 7th FloorGordon and Leslie Diamond Health Care Centre,2775 Laurel StreetVancouver, B.C. V5Z 1M9 Canada
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

iii
GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND PREVENTIONTable of Contents
PREFACE ii
METHODOLOGY AND SUMMARY OF NEW RECOMMENDATION, 2011 UPDATE vi
INTRODUCTION x
CHAPTER 1. DEFINITION AND OVERVIEW 1
KEY POINTS 2
DEFINITION 2
THE BURDEN OF ASTHMA 3 Prevalence, Morbidity and Mortality 3 Social and Economic Burden 3
FACTORS INFLUENCING THE DEVELOPMENT AND EXPRESSION OF ASTHMA 4 Host Factors 4 Genetic 4 Obesity 5 Sex 5 Environmental Factors 5 Allergens 5 Infections 5 Occupational sensitizers 6 Tobacco smoke 6 Outdoor/Indoor air pollution 7 Diet 7
MECHANISMS OF ASTHMA 7 AirwayInflammationInAsthma 7 Inflammatory cells 8 Structural changes in airways 8 Pathophysiology 8 Airway hyperresponsiveness 8 SpecialMechanisms 9 Acute exacerbations 9 Nocturnal Asthma 9 Irreversible airflow asthma 9 Difficult-to-treat asthma 9 Smoking and asthma 9
REFERENCES 9
CHAPTER 2. DIAGNOSIS AND CLASSIFICATION 15
KEY POINTS 16
INTRODUCTION 16CLINICAL DIAGNOSIS 16
Medical History 16 Symptoms 16 Cough variant asthma 16 Exercise-Induced bronchospasm 17 PhysicalExamination 17 TestsforDiagnosisandMonitoring 17 Measurements of lung function 17 Spirometry 18 Peak expiratory flow 18 Measurement of airway responsiveness 19 Non-Invasive markers of airway inflammation 19 Measurements of allergic status 19
DIAGNOSTIC CHALLENGES AND DIFFERENTIAL DIAGNOSIS 20 Children5YearsandYounger 20 OlderChildrenandAdults 20 TheElderly 21 OccupationalAsthma 21 DistinguishingAsthmafromCOPD 21
CLASSIFICATION OF ASTHMA 21 Etiology 21 Phenotype 22 AsthmaControl 22 AsthmaSeverity 23 REFERENCES 24
CHAPTER 3. ASTHMA MEDICATIONS 29
KEY POINTS 30
INTRODUCTION 30
ASTHMA MEDICATIONS: ADULTS 30 Route of Administration 30 Controller Medications 31 Inhaled glucocorticosteroids 31 Leukotriene modifiers 32 Long-acting inhaled β2-agonists 33 Theophylline 33 Cromones: sodium cromoglycate and nedocromil sodium 34 Long-acting oral β2-agonists 34 Anti-IgE 34 Systemic glucocorticosteroids 34 Oral anti-allergic compounds 35 Other controller therapies 36 Allergen-specific immunotherapy 36
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

iv
Reliever Medications 36 Rapid-acting inhaled β2-agonists 36 Systemic glucocorticosteroids 37 Anticholinergics 37 Theophylline 37 Short-acting oral β2-agonists 37
ComplementaryandAlternativeMedicine 37
ASTHMA TREATMENT: CHILDREN 38 Route of Administration 38 Controller Medications 39 Inhaled glucocorticosteroids 39 Leukotriene modifiers 41 Long-acting inhaled β2-agonists 41 Theophylline 42 Anti-IgE 42 Cromones: sodium cromoglycate and nedocromil sodium 43 Systemic glucocorticosteroids 43 Reliever Medications 43 Rapid-acting inhaled β2-agonists and short-acting oral β2-agonists 43 Anticholinergics 43
REFERENCES 43
CHAPTER 4. ASTHMA MANAGEMENT AND PREVENTION 55
INTRODUCTION 56
COMPONENT 1: DEVELOP PATIENT/ DOCTOR PARTNERSHIP 56
KEY POINTS 56
INTRODUCTION 56
ASTHMA EDUCATION 57 AttheInitialConsultation 58 PersonalWrittenAsthmaActionPlans 58 Follow-upandReview 58 ImprovingAdherence 59 Self-ManagementinChildren 59
THE EDUCATION OF OTHERS 60
COMPONENT 2: IDENTIFY AND REDUCE EXPOSURE TO RISK FACTORS 61
KEY POINTS 61
INTRODUCTION 61
ASTHMA PREVENTION 61PREVENTION OF ASTHMA SYMPTOMS AND EXACERBATIONS 62 IndoorAllergens 62 Domestic mites 62 Furred animals 62 Cockroaches 63 Fungi 63 OutdoorAllergens 63 Indoor Air Pollutants 63 Outdoor Air Pollutants 63 OccupationalExposures 63 FoodandDrugAdditives 64 Drugs 64 InfluenzaVaccination 64 Obesity 64 Emotional Stress 64 OtherFactorsThatMayExacerbateAsthma 64
COMPONENT 3: ASSESS,TREAT AND MONITOR ASTHMA 65
KEY POINTS 65
INTRODUCTION 65
ASSESSING ASTHMA CONTROL 65
TREATMENT TO ACHIEVE CONTROL 65 TreatmentStepstoAchievingControl 66 Step 1: As-needed reliever medication 66 Step 2: Reliever medication plus a single controller 68 Step 3: Reliever medication plus one or two controllers 68 Step 4: Reliever medication plus two or more controllers 68 Step 5: Reliever medication plus additional controller options 69
MONITORING TO MAINTAIN CONTROL 69 Duration and Adjustments to Treatment 69 SteppingDownTreatmentWhenAsthmaIs Controlled 70 SteppingUpTreatmentInResponsetoLoss of Control 70 Difficult-to-Treat-Asthma 71
THERMOPLASTY 72
COMPONENT 4: MANAGE ASTHMA EXACERBATIONS 73
KEY POINTS 73
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

v
INTRODUCTION 73ASSESSMENT OF SEVERITY 74
MANAGEMENT-COMMUNITY SETTINGS 74 Treatment 75 Bronchodilators 75 Glucocorticosteroids 75
MANAGEMENT-ACUTE CARE SETTINGS 75 Assessment 75 Treatment 77 Oxygen 77 Rapid-acting inhaled β2-agonists 77 Epinephrine 77 Additionalbronchodilators 77 Systemic glucocorticosteroids 77 Inhaled glucocorticosteroids 78 Magnesium 78 Helium oxygen therapy 78 Leukotriene modifiers 78 Sedatives 78 CriteriaforDischargefromtheEmergency Departmentvs.Hospitalization 78
COMPONENT 5: SPECIAL CONSIDERATIONS 80 Pregnancy 80 Obesity 80 Surgery 80 Rhinitis,Sinusitis,andNasalPolyps 81 Rhinitis 81 Sinusitis 81 Nasal polyps 81 OccupationalAsthma 81 RespiratoryInfections 81 GastroesophagealReflux 82 Aspirin-InducedAsthma 82 AnaphylaxisandAsthma 83
REFERENCES 83
CHAPTER 5. IMPLEMENTATION OF ASTHMA GUIDELINES IN HEALTH SYSTEMS 104
KEY POINTS 105
INTRODUCTION 105
GUIDELINE IMPLEMENTATION STRATEGIES 105
ECONOMIC VALUE OF INTERVENTIONS AND GUIDELINE IMPLEMENTATION IN ASTHMA 106 UtilizationandCostofHealthCareResources 107 DeterminingtheEconomicValueofInterventionsin Asthma 107
GINA DISSEMINATION/IMPLEMENTATION RESOURCES 108
REFERENCES 108
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

vi
Background: When the Global Initiative for Asthma (GINA) program was initiated in 1993, the primary goal was to produce recommendations for the management of asthma based on the best scientific information available. Its first report, NHLBI/WHO Workshop Report: Global Strategy for Asthma Management and Prevention was issued in 1995 and revised in 2002 and 2006. In 2002 and in 2006 revised documents were prepared based on published research.
The GINA Science Committee2 was established in 2002 to review published research on asthma management and prevention, to evaluate the impact of this research on recommendations in the GINA documents related to management and prevention, and to post yearly updates on the GINA website. Its members are recognized leaders in asthma research and clinical practice with the scientific credentials to contribute to the task of the Committee, and are invited to serve for a limited period and in a voluntary capacity. The Committee is broadly representative of adult and pediatric disciplines as well from diverse geographic regions.
Updates of the 2006 report have been issued in December of each year with each update based on the impact of publications from July 1 of the previous year through June 30 of the year the update was completed. Posted on the website along with the updated documents is a list of all the publications reviewed by the Committee.
Process: To produce the updated documents a Pub Med search is done using search fields established by the Committee: 1) asthma, All Fields, All ages, only items with abstracts, Clinical Trial, Human, sorted by Authors; and 2) asthma AND systematic, All fields, ALL ages, only items with abstracts, Human, sorted by author. The first search includes publications for July 1-December 30 for review by the Committee during the ATS meeting. The second search includes publications for January 1 – June 30 for review by the Committee during the ERS meeting. (Publications that appear after June 30 are considered in the first phase of the following year.) To ensure publications in peer review journals not captured by this search methodology are not missed, the respiratory community is invited to submit papers to the Chair, GINA
Science Committee, providing an abstract and the full paper are submitted in (or translated into) English.
All members of the Committee receive a summary of citations and all abstracts. Each abstract is assigned to at least two Committee members, although all members are offered the opportunity to provide an opinion on all abstracts. Members evaluate the abstract or, up to her/his judgment, the full publication, and answer four specific written questions from a short questionnaire, and to indicate if the scientific data presented impacts on recommendations in the GINA report. If so, the member is asked to specifically identify modifications that should be made.
The entire GINA Science Committee meets twice yearly to discuss each publication that was considered by at least 1 member of the Committee to potentially have an impact on the management of asthma. The full Committee then reaches a consensus on whether to include it in the report, either as a reference supporting current recommendations, or to change the report. In the absence of consensus, disagreements are decided by an open vote of the full Committee. Recommendations by the Committee for use of any medication are based on the best evidence available from the literature and not on labeling directives from government regulators. The Committee does not make recommendations for therapies that have not been approved by at least one regulatory agency.
For the 2012 update, between July 1, 2011 and June 30, 2012, 386 articles met the search criteria. Of the 386, 19 papers were identified to have an impact on the GINA report. The changes prompted by these publications were posted on the website in December 2012. These were either: A) modifying, that is, changing the text or introducing a concept requiring a new recommendation to the report; or B) confirming, that is, adding to or replacing an existing reference.
Methodology and Summary of New Recommendations Global Strategy for Asthma Management and Prevention:
2012 Update1
1The Global Strategy for Asthma Management and Prevention (updated 2012), the updated Pocket Guides and the complete list of references examined by the Committee are available on the GINA website www.ginasthma.org.2Members (2011-2012): H. Reddel, Chair; P. Barnes, N. Barnes, E. Bateman, A. Becker, E. Bel, J. DeJongste, J. Drazen, M. FitzGerald, R. Lemanske, P. O’Byrne, K. Ohta, S. Pedersen, E. Pizzichini, S. Wenzel.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

vii
SUMMARY OF RECOMMENDATIONS IN THE 2013 UPDATE
A. Additions to the text:
Page 33, right column, insert new paragraph: Tiotropium,a long-acting inhaled anticholinergic bronchodilator, has been studied in adults with uncontrolled asthma and compared with salmeterol, doubling the dose of inhaled glucocorticosteroid and as add-on to inhaled glucocorticosteroids and salmeterol231,233. One study showed comparable bronchodilator effects with no significant changes on asthma control232. Another study showed that adding tiotropium to patients not controlled on inhaled glucocorticosteroids and long-acting ß2-agonists improved lung function but not symptoms233. The studies have been relatively short-term and no effect on exacerbations has so far been reported. There are no data about these medications in children.Reference 231: Peters SP, Kunselman SJ, Icitovic N, Moore WC, Pascual R, Ameredes BT et al. National Heart, Lung, and Blood Institute Asthma Clinical Research Network. Tiotropium bromide step-up therapy for adults with uncontrolled asthma. N Engl J Med 2010;363:1715-26.Reference 232: Kerstjens HA, Disse B, Schroder-Babo W, Bantje TA, Gahlemann M, Sigmund R, Engel M, van Noord JA. Tiotropium improves lung function in patients with severe uncontrolled asthma: a randomized controlled trial. J Allergy Clin Immunol. 2011 Aug;128(2):308-14. Reference 233: Bateman ED, Kornmann O, Schmidt P, Pivovarova A, Engel M, Fabbri LM. Tiotropium is noninferior to salmeterol in maintaining improved lung function in B16-Arg/Arg patients with asthma. J Allergy Clin Immunol. 2011 Aug;128(2):315-22.
Page 34, right column, insert line 15: …. although this was not confirmed in all studies235.Reference 235: Hanania NA, Alpan O, Hamilos DL, et al. Omalizumab in severe allergic asthma inadequately controlled with standard therapy: a randomized trial. Ann Internal Med 2011;154:573-82.
Page 38, left column, first paragraph, add sentence and reference: A systematic review of yoga interventions for asthma found no convincing evidence of benefit; the quality of studies was generally poor236.Reference 236. Posadzki P, Ernst E. Yoga for asthma? A systematic review of randomized clinical trials. J Asthma. 2011 Aug;48(6):632-9.
Page 38, right column, last paragraph, add statement and reference: although spacer devices or face masks differ in their drug delivery, and therefore may not be interchangeable237. Reference 237. Lavorini F, Fontana GA. Targeting drugs to the airways: The role of spacer devices. Expert Opin Drug Deliv 2009;6:91-102.
Page 40, left column, first paragraph replace with: The clinical benefits of intermittent systemic or inhaled glucocorticosteroids for children with intermittent, viral-induced wheeze remain controversial. A one-year study of intermittent treatment with inhaled glucocorticosteroids was equally effective as daily treatment, and reduced the total glucocorticosteroid dose threefold in preschool children with frequent wheezing and a high asthma predictive index238. Some studies in older children found small benefits while another study in young children found no effects on wheezing symptoms139. There is no evidence to support the use of maintenance low-dose inhaled glucocorticosteroids for preventing early transient wheezing136, 139, 199.Reference 238: Zeiger RS, Mauger D, Bacharier LB, Guilbert TW, Martinez FD, Lemanske RF Jr, et al; CARE Network of the National Heart, Lung, and Blood Institute. Daily or intermittent budesonide in preschool children with recurrent wheezing. N Engl J Med. 2011 Nov 24;365(21):1990-2001
Page 40, Figure 3-5, bullet 6: Modify age range to 2-10 years; add reference in figure title.Reference 239: Guilbert TW, Mauger DT, Allen DB, Zeiger RS, Lemanske RF Jr, Szefler SJ, et al; Childhood Asthma Research and Education Network of the National Heart, Lung, and Blood Institute. Growth of preschool children at high risk for asthma 2 years after discontinuation of fluticasone. J Allergy Clin Immunol. 2011 Nov;128(5):956-63.
Page 71, right column, replace second bullet and add reference: Investigate and confirm adherence with treatment. Incorrect or inadequate use of medications and inhalers405 remains the most common reason for failure to achieve good control. In patients with difficult-to-treat asthma, improved adherence and improved health outcomes can be achieved with a comprehensive concordance intervention416. Reference 416: Gamble J, Stevenson M, Heaney LG. A study of a multi-level intervention to improve non-adherence in difficult to control asthma. Respir Med. 2011 Sep;105(9):1308-15.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

viii
Page 72, left column insert in last paragraph: Extended follow-up on a small number of patients has provided some additional support for long-term safety of bronchial thermoplasty417. However, longer-term follow-up of larger number of control and active patients is needed to assess effectiveness and caution should be used in selecting patients for this procedure. Reference 417: Castro M, Rubin A, Laviolette M, Hanania NA, Armstrong B, Cox G; AIR2 Trial Study Group. Persistence of effectiveness of bronchial thermoplasty in patients with severe asthma. Ann Allergy Asthma Immunol. 2011 Jul;107(1):65-70.
Page 77, left column replace paragraph on oxygen: To achieve arterial oxygen saturation of 90% (95% in children), oxygen should be administered by nasal cannulae, by mask, or rarely by head box in some infants. For severe asthma exacerbations, controlled oxygen therapy using pulse oximetry to maintain oxygen saturation at 90 – 93% is associated with better physiological outcomes, compared to high flow 100% oxygen therapy218, 419. Oxygen therapy should be titrated against pulse oximetry to maintain a satisfactory oxygen saturation219. However, oxygen should not be withheld if oximetry is not available.Reference 419. Perrin K, Wijesinghe M, Healy B, Wadsworth K, Bowditch R, Bibby S, Baker T, Weatherall M, Beasley R. Randomised controlled trial of high concentration versus titrated oxygen therapy in severe exacerbations of asthma. Thorax. 2011Nov;66(11):937-41.
Page 78, left column, end of first paragraph, insert text and reference: Two days of oral dexamethasone can also be used to treat asthma exacerbations, but there are concerns about metabolic side-effects if dexamethasone is continued beyond two days420. Evidence suggests that there is no benefit to tapering the dose of oral glucocorticosteroids, either in the short-term245 or over several weeks, as long as the patient is on maintenance inhaled glucocorticosteroids246 (Evidence B).Reference 420: Kravitz J, Dominici P, Ufberg J, Fisher J, Giraldo P. Two days of dexamethasone versus 5 days of prednisone in the treatment of acute asthma: arandomized controlled trial. Ann Emerg Med. 2011 Aug;58(2):200-4.
Page 82, right column, paragraph 2, insert in line 4: …in adults392-394 or in children422.Reference 422. Holbrook JT, Wise RA, Gold BD, Blake K, Brown ED, Castro M, Dozor AJ, et al. Writing Committee for the American Lung Association Asthma Clinical Research Centers. Lansoprazole for children with
poorly controlled asthma: a randomized controlled trial. JAMA. 2012 Jan 25;307(4):373-81.
B. References that provided confirmation or update of previous recommendations.
Page 6, right column, first sentence in paragraph four, add reference 136. Reference 136: Burke H, Leonardi-Bee J, Hashim A, Pine-Abata H, Chen Y, Cook DG, Britton JR, McKeever TM. Prenatal and passive smoke exposure and incidence of asthma and wheeze: systematic review and meta-analysis. Pediatrics. 2012 Apr;129(4):735-44.
Page 33, right column, insert reference 234 after reference 215.Reference 234: Kemp J, Armstrong L, Wan Y, Alagappan VK, Ohlssen D, Pascoe S. Safety of formoterol in adults and children with asthma: a meta-analysis. Ann Allergy Asthma Immunol. 2011 Jul;107(1):71-8.
Page 41, right column, line 10, insert reference 234 after reference 75, and in line 17, after reference 169.Reference 234: Kemp J, Armstrong L, Wan Y, Alagappan VK, Ohlssen D, Pascoe S. Safety of formoterol in adults and children with asthma: a meta-analysis. Ann Allergy Asthma Immunol. 2011 Jul;107(1):71-8.
Page 57, right column, last paragraph, insert reference 414 after reference 22. Reference 414: Shah S, Sawyer SM, Toelle BG, Mellis CM, Peat JK, Lagleva M, Usherwood TP, Jenkins CR. Improving paediatric asthma outcomes in primary health care: a randomised controlled trial. Med J Aust. 2011 Oct 3;195(7):405-9.
Page 61, right column, paragraph 2 insert reference:Reference 415: Gehring U, de Jongste JC, Kerkhof M, Oldewening M, Postma D, van Strien RT, et al. The 8-year follow-up of the PIAMA intervention study assessing the effect of mite-impermeable mattress covers. Allergy. 2012 Feb;67(2):248-56
Page 73, right column end of first paragraph insert reference 418 after reference 349.Reference 418: Ortega H, Miller DP, Li H. Characterization of asthma exacerbations in primary care using cluster analysis. J Asthma. 2012 Mar;49(2):158-69.
Page 81, right column, last sentence under section on Occupational Asthma, insert insert (See also reference 421).
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ix
Reference 421: Fishwick D, Barber CM, Bradshaw LM, Ayres JG, Barraclough R, Burge S, et al. Standards of care for occupational asthma: an update. Thorax. 2012 Mar;67(3):278-80.
C. Inserts to add clarification or additional information
Page 20, left column, insert new paragraph: In early life, the presence of sensitization to common allergens, atopy, is a major risk factor for subsequent development of asthma. In addition, atopy also predicts that asthma may be more severe when it does develop.
Page 32, left column last paragraph: correct dose to 1000 ug/day
Page 64, under heading of obesity, insert: ...including by bariatric surgery
.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

x
Asthma is a serious public health problem throughout the world, affecting people of all ages. When uncontrolled, asthma can place severe limits on daily life, and is sometimes fatal.
In 1993, the Global Initiative for Asthma (GINA) was formed. Its goals and objectives were described in a 1995 NHLBI/WHO Workshop Report, Global Strategy for Asthma Management and Prevention. This Report (revised in 2002 and 2006), and its companion documents, have been widely distributed and translated into many languages. A network of individuals and organizations interested in asthma care has been created and several country-specific asthma management programs have been initiated. Yet much work is still required to reduce morbidity and mortality from this chronic disease.
In 2006, the Global Strategy for Asthma Management and Prevention was revised to emphasize asthma management based on clinical control, rather than classification of the patient by severity. This important paradigm shift for asthma care reflected the progress made in pharmacologic care of patients. Many asthma patients are receiving, or have received, some asthma medications. The role of the health care professional is to establish each patient’s current level of treatment and control, then adjust treatment to gain and maintain control. Asthma patients should experience no or minimal symptoms (including at night), have no limitations on their activities (including physical exercise), have no (or minimal) requirement for rescue medications, have near normal lung function, and experience only very infrequent exacerbations.
The recommendations for asthma care based on clinical control described in the 2006 report have been updated annually. This 2011 update reflects a number of modifications, described in “Methodology and Summary of New Recommendations.” As with all previous GINA reports, levels of evidence (Table A) are assigned to management recommendations where appropriate in Chapter 4, the Five Components of Asthma Management. Evidence levels are indicated in boldface type enclosed in parentheses after the relevant statement—e.g., (Evidence A).
FUTURE CHALLENGES
In spite of laudable efforts to improve asthma care over the past decade, a majority of patients have not benefited from advances in asthma treatment and many lack even the rudiments of care. A challenge for the next several years is to work with primary health care providers and public
health officials in various countries to design, implement, and evaluate asthma care programs to meet local needs. The GINA Board of Directors recognizes that this is a difficult task and, to aid in this work, has formed several groups of global experts, including: a Dissemination and Implementation Committee; the GINA Assembly, a network of individuals who care for asthma patients in many different health care settings; and two regional programs, GINA Mesoamerica and GINA Mediterranean. These efforts aim to enhance communication with asthma specialists, primary-care health professionals, other health care workers, and patient support organizations. The Board of Directors continues to examine barriers to implementation of the asthma management recommendations, especially the challenges that arise in primary-care settings and in developing countries.
While early diagnosis of asthma and implementation of appropriate therapy significantly reduce the socioeconomic burdens of asthma and enhance patients’ quality of life, medications continue to be the major component of the cost of asthma treatment. For this reason, the pricing of asthma medications continues to be a topic for urgent need and a growing area of research interest, as this has important implications for the overall costs of asthma management. Moreover, a large segment of the world’s population lives in areas with inadequate medical facilities and meager financial resources. The GINA Board of Directors recognizes that “fixed” international guidelines and “rigid” scientific protocols will not work in many locations. Thus, the recommendations found in this Report must be adapted to fit local practices and the availability of health care resources.
As the GINA Board of Directors expand their work, every effort will be made to interact with patient and physician groups at national, district, and local levels, and in multiple health care settings, to continuously examine new and innovative approaches that will ensure the delivery of the best asthma care possible. GINA is a partner organization in a program launched in March 2006 by the World Health Organization, the Global Alliance Against Chronic Respiratory Diseases (GARD). Through the work of the GINA Board of Directors, and in cooperation with GARD, progress toward better care for all patients with asthma should be substantial in the next decade.
INTRODUCTION
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

xi
Table A. Description of Levels of EvidenceEvidence Category
Sources of Evidence Definition
A Randomized controlled trials (RCTs). Rich body of data.
Evidence is from endpoints of well designed RCTs that provide a consistent pattern of findings in the population for which the recommendation is made. Category A requires substantial numbers of studies involving substantial numbers of participants.
B Randomized controlled trials (RCTs). Limited body of data.
Evidence is from endpoints of intervention studies that include only a limited number of patients, posthoc or subgroup analysis of RCTs, or meta-analysis of RCTs. In general, Category B pertains when few randomized trials exist, they are small in size, they were under-taken in a population that differs from the target population of the recommendation, or the results are somewhat inconsistent.
C Nonrandomized trials. Observational studies.
Evidence is from outcomes of uncontrolled or non-randomized trials or from observational studies.
D Panel consensus judg-ment.
This category is used only in cases where the provision of some guidance was deemed valuable but the clinical literature addressing the subject was insufficient to justify placement in one of the other categories. The Panel Consensus is based on clinical experience or knowledge that does not meet the above listed criteria.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

xii COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

CHAPTER
1
DEFINITION
AND
OVERVIEW
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

2 DEFINITION AND OVERVIEW
KEY POINTS:
• Asthmaisachronicinflammatorydisorderoftheairwaysinwhichmanycellsandcellularelementsplayarole.Thechronicinflammationisassociatedwithairwayhyperresponsivenessthatleadstorecurrentepisodesofwheezing,breathlessness,chesttightness,andcoughing,particularlyatnightorintheearlymorning.Theseepisodesareusuallyassociatedwithwidespread,butvariable,airflowobstructionwithinthelungthatisoftenreversibleeitherspontaneouslyorwithtreatment.
• Clinicalmanifestationsofasthmacanbecontrolledwithappropriatetreatment.Whenasthmaiscontrolled,thereshouldbenomorethanoccasionalflare-upsandsevereexacerbationsshouldberare.
• Asthmaisaproblemworldwide,withanestimated300millionaffectedindividuals.
• Althoughfromtheperspectiveofboththepatientandsocietythecosttocontrolasthmaseemshigh,thecostofnottreatingasthmacorrectlyisevenhigher.
• Anumberoffactorsthatinfluenceaperson’sriskofdevelopingasthmahavebeenidentified.Thesecanbedividedintohostfactors(primarilygenetic)andenvironmentalfactors.
• Theclinicalspectrumofasthmaishighlyvariable,anddifferentcellularpatternshavebeenobserved,butthepresenceofairwayinflammationremainsaconsistentfeature.
Thischaptercoversseveraltopicsrelatedtoasthma,includingdefinition,burdenofdisease,factorsthatinfluencetheriskofdevelopingasthma,andmechanisms.Itisnotintendedtobeacomprehensivetreatmentofthesetopics,butratherabriefoverviewofthebackgroundthatinformstheapproachtodiagnosisandmanagementdetailedinsubsequentchapters.Furtherdetailsarefoundinthereviewsandotherreferencescitedattheendofthechapter.
Asthmaisadisorderdefinedbyitsclinical,physiological,andpathologicalcharacteristics.Thepredominantfeatureoftheclinicalhistoryisepisodicshortnessofbreath,particularlyatnight,oftenaccompaniedbycough.
Wheezingappreciatedonauscultationofthechestisthemostcommonphysicalfinding.
Themainphysiologicalfeatureofasthmaisepisodicairwayobstructioncharacterizedbyexpiratoryairflowlimitation.Thedominantpathologicalfeatureisairwayinflammation,sometimesassociatedwithairwaystructuralchanges.
Asthmahassignificantgeneticandenvironmentalcomponents,butsinceitspathogenesisisnotclear,muchofitsdefinitionisdescriptive.Basedonthefunctionalconsequencesofairwayinflammation,anoperationaldescriptionofasthmais:
Asthma is a chronic inflammatory disorder of the airways in which many cells and cellular elements play a role. The chronic inflammation is associated with airway hyperresponsiveness that leads to recurrent episodes of wheezing, breathlessness, chest tightness, and coughing, particularly at night or in the early morning. These episodes are usually associated with widespread, but variable, airflow obstruction within the lung that is often reversible either spontaneously or with treatment.
Becausethereisnocleardefinitionoftheasthmaphenotype,researchersstudyingthedevelopmentofthiscomplexdiseaseturntocharacteristicsthatcanbemeasuredobjectively,suchasatopy(manifestedasthepresenceofpositiveskin-pricktestsortheclinicalresponsetocommonenvironmentalallergens),airwayhyperresponsiveness(thetendencyofairwaystonarrowexcessivelyinresponsetotriggersthathavelittleornoeffectinnormalindividuals),andothermeasuresofallergicsensitization.Althoughtheassociationbetweenasthmaandatopyiswellestablished,thepreciselinksbetweenthesetwoconditionshavenotbeenclearlyandcomprehensivelydefined.
Thereisnowgoodevidencethattheclinicalmanifestationsofasthma—symptoms,sleepdisturbances,limitationsofdailyactivity,impairmentoflungfunction,anduseofrescuemedications—canbecontrolledwithappropriatetreatment.Whenasthmaiscontrolled,thereshouldbenomorethanoccasionalrecurrenceofsymptomsandsevereexacerbationsshouldberare1.
DEFINITION
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

DEFINITION AND OVERVIEW 3
Prevalence, Morbidity, and Mortality
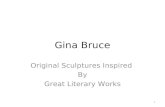
Asthmaisaproblemworldwide,withanestimated300million affected individuals2,3.Despitehundredsofreportsontheprevalenceofasthmainwidelydifferingpopulations,thelackofapreciseanduniversallyaccepteddefinitionofasthmamakesreliablecomparisonofreportedprevalencefromdifferentpartsoftheworldproblematic.Nonetheless,basedontheapplicationofstandardizedmethodstomeasuretheprevalenceofasthmaandwheezingillnessinchildren4andadults,itappearsthattheglobalprevalenceofasthmarangesfrom1%to18%ofthepopulationindifferentcountries(Figure 1-1)2,3.Thereisgoodevidencethatinternationaldifferencesinasthmasymptomprevalencehavebeenreduced,particularlyinthe13-14yearagegroup,withdecreasesinprevalenceinNorthAmericaandWesternEuropeandincreasesinprevalenceinregionswhereprevalencewaspreviouslylow.Althoughtherewaslittlechangeintheoverallprevalenceofcurrentwheeze,thepercentageofchildrenreportedtohavehadasthmaincreasedsignificantly,possiblyreflectinggreaterawarenessofthisconditionand/orchangesindiagnosticpractice.TheincreasesinasthmasymptomprevalenceinAfrica,LatinAmericaandpartsofAsiaindicatethattheglobalburdenofasthmaiscontinuingtorise,buttheglobalprevalencedifferencesarelessening118.TheWorldHealthOrganizationhasestimatedthat15milliondisability-adjustedlifeyears(DALYs)arelostannuallyduetoasthma,representing1%ofthetotalglobaldiseaseburden2.Annualworldwidedeathsfromasthmahavebeenestimatedat250,000andmortalitydoesnotappeartocorrelatewellwithprevalence(Figure 1-1)2,3.Thereareinsufficientdatatodeterminethelikelycausesofthedescribedvariationsinprevalencewithinandbetweenpopulations.
Social and Economic Burden Socialandeconomicfactorsareintegraltounderstandingasthmaanditscare,whetherviewedfromtheperspectiveoftheindividualsufferer,thehealthcareprofessional,orentitiesthatpayforhealthcare.AbsencefromschoolanddayslostfromworkarereportedassubstantialsocialandeconomicconsequencesofasthmainstudiesfromtheAsia-Pacificregion,India,LatinAmerica,theUnitedKingdom,andtheUnitedStates9-12.
Themonetarycostsofasthma,asestimatedinavarietyofhealthcaresystemsincludingthoseoftheUnitedStates13-15 andtheUnitedKingdom16aresubstantial.Inanalysesofeconomicburdenofasthma,attentionneedstobepaidtobothdirectmedicalcosts(hospitaladmissionsandcostofmedications)andindirect,non-medicalcosts(timelostfromwork,prematuredeath)17.Forexample,asthmaisamajorcauseofabsencefromworkinmanycountries4-6,includingAustralia,Sweden,theUnitedKingdom,andtheUnitedStates2,3,18,19.Comparisonsofthecostofasthmaindifferentregionsleadtoaclearsetofconclusions:
• Thecostsofasthmadependontheindividualpatient’slevelofcontrolandtheextenttowhichexacerbationsareavoided.
• Emergencytreatmentismoreexpensivethanplannedtreatment.
• Non-medicaleconomiccostsofasthmaaresubstantial.Guideline-determinedasthmacarecanbecosteffective.Familiescansufferfromthefinancialburdenoftreatingasthma.
Althoughfromtheperspectiveofboththepatientandsocietythecosttocontrolasthmaseemshigh,thecostofnottreatingasthmacorrectlyisevenhigher119.Propertreatmentofthediseaseposesachallengeforindividuals,healthcareprofessionals,healthcareorganizations,andgovernments.Thereiseveryreasontobelievethatthesubstantialglobalburdenofasthmacanbedramaticallyreducedthrougheffortsbyindividuals,theirhealthcareproviders,healthcareorganizations,andlocalandnationalgovernmentstoimproveasthmacontrol.
DetailedreferenceinformationabouttheburdenofasthmacanbefoundinthereportGlobalBurdenofAsthma*.Furtherstudiesofthesocialandeconomicburdenofasthmaandthecosteffectivenessoftreatmentareneededinbothdevelopedanddevelopingcountries.
THE BURDEN OF ASTHMA
Figure 1-1. Asthma Prevalence and Mortality2, 3
Permission for use of this figure obtained from J. Bousquet.
*(http://www.ginasthma.org/ReportItem.asp?I1=2&I2=2&intld=94COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

4 DEFINITION AND OVERVIEW
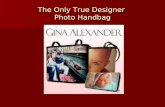
Factorsthatinfluencetheriskofasthmacanbedividedintothosethatcausethedevelopmentofasthmaandthosethattriggerasthmasymptoms;somedoboth.Theformerincludehostfactors(whichareprimarilygenetic)andthelatterareusuallyenvironmentalfactors(Figure 1-2)21.However,themechanismswherebytheyinfluencethedevelopmentandexpressionofasthmaarecomplexandinteractive.Forexample,geneslikelyinteractbothwithothergenesandwithenvironmentalfactorstodetermineasthmasusceptibility22,23.Inaddition,developmentalaspects—suchasthematurationoftheimmuneresponseandthetimingofinfectiousexposuresduringthefirstyearsoflife—areemergingasimportantfactorsmodifyingtheriskofasthmainthegeneticallysusceptibleperson.
Additionally,somecharacteristicshavebeenlinkedtoanincreasedriskforasthma,butarenotthemselvestruecausalfactors.Theapparentracialandethnicdifferencesintheprevalenceofasthmareflectunderlyinggeneticvarianceswithasignificantoverlayofsocioeconomicandenvironmentalfactors.Inturn,thelinksbetweenasthmaandsocioeconomicstatus—withahigherprevalenceofasthmaindevelopedthanindevelopingnations,inpoor
comparedtoaffluentpopulationsindevelopednations,andinaffluentcomparedtopoorpopulationsindevelopingnations—likelyreflectlifestyledifferencessuchasexposuretoallergens,accesstohealthcare,etc.
Muchofwhatisknownaboutasthmariskfactorscomesfromstudiesofyoungchildren.Riskfactorsforthedevelopmentofasthmainadults,particularlyde novo in adultswhodidnothaveasthmainchildhood,arelesswelldefined.
Thelackofacleardefinitionforasthmapresentsasignificantprobleminstudyingtheroleofdifferentriskfactorsinthedevelopmentofthiscomplexdisease,becausethecharacteristicsthatdefineasthma(e.g.,airwayhyperresponsiveness,atopy,andallergicsensitization)arethemselvesproductsofcomplexgene-environmentinteractionsandarethereforebothfeaturesofasthmaandriskfactorsforthedevelopmentofthedisease.
Host Factors
Genetic.Asthmahasaheritablecomponent,butitisnotsimple.Currentdatashowthatmultiplegenesmaybeinvolvedinthepathogenesisofasthma24,25, and different genesmaybeinvolvedindifferentethnicgroups.Thesearchforgeneslinkedtothedevelopmentofasthmahasfocusedonfourmajorareas:productionofallergen-specificIgEantibodies(atopy);expressionofairwayhyperresponsiveness;generationofinflammatorymediators,suchascytokines,chemokines,andgrowthfactors;anddeterminationoftheratiobetweenTh1andTh2immuneresponses(asrelevanttothehygienehypothesisofasthma)26.Familystudiesandcase-controlassociationanalyseshaveidentifiedanumberofchromosomalregionsassociatedwithasthmasusceptibility.Forexample,atendencytoproduceanelevatedleveloftotalserumIgEisco-inheritedwithairwayhyperresponsiveness,andagene(orgenes)governingairwayhyperresponsivenessislocatednearamajorlocusthatregulatesserumIgElevelsonchromosome5q27.However,thesearchforaspecificgene(orgenes)involvedinsusceptibilitytoatopyorasthmacontinues,asresultstodatehavebeeninconsistent24,25.
Inadditiontogenesthatpredisposetoasthmatherearegenesthatareassociatedwiththeresponsetoasthmatreatments.Forexample,variationsinthegeneencodingthebeta-adrenoreceptorhavebeenlinkedtodifferencesinsubjects’responsestoβ2-agonists
28.Othergenesofinterestmodifytheresponsivenesstoglucocorticosteroids29 andleukotrienemodifiers30.Thesegeneticmarkerswilllikelybecomeimportantnotonlyasriskfactorsinthepathogenesisofasthmabutalsoasdeterminantsofresponsivenesstotreatment28,30-33.
FACTORS INFLUENCING THE DEVELOPMENT AND EXPRESSION OF ASTHMA Factors that influence the risk of asthma can be dividedinto those that cause the development of asthma andthose that trigger asthma symptoms; some do both.The former include host factors (which are primarilygenetic) and the latter are usually environmental factors(Figure 1-2)21. However, the mechanisms whereby theyinfluence the development and expression of asthma arecomplex and interactive. For example, genes likelyinteract both with other genes and with environmentalfactors to determine asthma susceptibility22,23. In addition,developmental aspects—such as the maturation of theimmune response and the timing of infectious exposuresduring the first years of life—are emerging as importantfactors modifying the risk of asthma in the geneticallysusceptible person.
Figure 1-2. Factors Influencing the Developmentand Expression of Asthma
HOST FACTORSGenetic, e.g.,
Genes pre-disposing to atopyGenes pre-disposing to airway hyperresponsiveness
ObesitySex
ENVIRONMENTAL FACTORSAllergens
Indoor: Domestic mites, furred animals (dogs, cats,mice), cockroach allergen, fungi, molds, yeastsOutdoor: Pollens, fungi, molds, yeasts
Infections (predominantly viral)Occupational sensiti ersTobacco smoke
Passive smokingActive smoking
Outdoor/Indoor Air PollutionDiet
Additionally, some characteristics have been linked to anincreased risk for asthma, but are not themselves truecausal factors. The apparent racial and ethnic differencesin the prevalence of asthma reflect underlying geneticvariances with a significant overlay of socioeconomic andenvironmental factors. In turn, the links between asthmaand socioeconomic status—with a higher prevalence of
asthma in developed than in developing nations, in poorcompared to affluent populations in developed nations,and in affluent compared to poor populations in developingnations—likely reflect lifestyle differences such asexposure to allergens, access to health care, etc.
Much of what is known about asthma risk factors comesfrom studies of young children. Risk factors for thedevelopment of asthma in adults, particularly de novo inadults who did not have asthma in childhood, are lesswell defined.
The lack of a clear definition for asthma presents asignificant problem in studying the role of different riskfactors in the development of this complex disease,because the characteristics that define asthma (e.g.,airway hyperresponsiveness, atopy, and allergicsensiti ation) are themselves products of complexgene-environment interactions and are therefore bothfeatures of asthma and risk factors for the developmentof the disease.
Host Factors
Genetic. Asthma has a heritable component, but it is notsimple. Current data show that multiple genes may beinvolved in the pathogenesis of asthma24,25, and differentgenes may be involved in different ethnic groups. Thesearch for genes linked to the development of asthma hasfocused on four major areas: production of allergen-specific IgE antibodies (atopy); expression of airwayhyperresponsiveness; generation of inflammatorymediators, such as cytokines, chemokines, and growthfactors; and determination of the ratio between Th1 andTh2 immune responses (as relevant to the hygienehypothesis of asthma)26.
Family studies and case-control association analyses haveidentified a number of chromosomal regions associatedwith asthma susceptibility. For example, a tendency toproduce an elevated level of total serum IgE is co-inheritedwith airway hyperresponsiveness, and a gene (or genes)governing airway hyperresponsiveness is located near amajor locus that regulates serum IgE levels onchromosome 5q27. However, the search for a specificgene (or genes) involved in susceptibility to atopy orasthma continues, as results to date have beeninconsistent24,25.
In addition to genes that predispose to asthma there aregenes that are associated with the response to asthmatreatments. For example, variations in the gene encodingthe beta-adrenoreceptor have been linked to differences in
4 DEFINITION AND OVERVIEW
FACTORS INFLUENCING THEDEVELOPMENT AND EXPRESSIONOF ASTHMA
Factors that influence the risk of asthma can be dividedinto those that cause the development of asthma andthose that trigger asthma symptoms; some do both.The former include host factors (which are primarilygenetic) and the latter are usually environmental factors(Figure 1-2)21. However, the mechanisms whereby theyinfluence the development and expression of asthma arecomplex and interactive. For example, genes likelyinteract both with other genes and with environmentalfactors to determine asthma susceptibility22,23. In addition,developmental aspects—such as the maturation of theimmune response and the timing of infectious exposuresduring the first years of life—are emerging as importantfactors modifying the risk of asthma in the geneticallysusceptible person.
Figure 1-2. Factors Influencing the Developmentand Expression of Asthma
HOST FACTORSGenetic, e.g.,
Genes pre-disposing to atopyGenes pre-disposing to airway hyperresponsiveness
ObesitySex
ENVIRONMENTAL FACTORSAllergens
Indoor: Domestic mites, furred animals (dogs, cats,mice), cockroach allergen, fungi, molds, yeastsOutdoor: Pollens, fungi, molds, yeasts
Infections (predominantly viral)Occupational sensitizersTobacco smoke
Passive smokingActive smoking
Outdoor/Indoor Air PollutionDiet
Additionally, some characteristics have been linked to anincreased risk for asthma, but are not themselves truecausal factors. The apparent racial and ethnic differencesin the prevalence of asthma reflect underlying geneticvariances with a significant overlay of socioeconomic andenvironmental factors. In turn, the links between asthmaand socioeconomic status—with a higher prevalence of
asthma in developed than in developing nations, in poorcompared to affluent populations in developed nations,and in affluent compared to poor populations in developingnations—likely reflect lifestyle differences such asexposure to allergens, access to health care, etc.
Much of what is known about asthma risk factors comesfrom studies of young children. Risk factors for thedevelopment of asthma in adults, particularly de novo inadults who did not have asthma in childhood, are lesswell defined.
The lack of a clear definition for asthma presents asignificant problem in studying the role of different riskfactors in the development of this complex disease,because the characteristics that define asthma (e.g.,airway hyperresponsiveness, atopy, and allergicsensiti ation) are themselves products of complexgene-environment interactions and are therefore bothfeatures of asthma and risk factors for the developmentof the disease.
Host Factors
Genetic. Asthma has a heritable component, but it is notsimple. Current data show that multiple genes may beinvolved in the pathogenesis of asthma24,25, and differentgenes may be involved in different ethnic groups. Thesearch for genes linked to the development of asthma hasfocused on four major areas: production of allergen-specific IgE antibodies (atopy); expression of airwayhyperresponsiveness; generation of inflammatorymediators, such as cytokines, chemokines, and growthfactors; and determination of the ratio between Th1 andTh2 immune responses (as relevant to the hygienehypothesis of asthma)26.
Family studies and case-control association analyses haveidentified a number of chromosomal regions associatedwith asthma susceptibility. For example, a tendency toproduce an elevated level of total serum IgE is co-inheritedwith airway hyperresponsiveness, and a gene (or genes)governing airway hyperresponsiveness is located near amajor locus that regulates serum IgE levels onchromosome 5q27. However, the search for a specificgene (or genes) involved in susceptibility to atopy orasthma continues, as results to date have beeninconsistent24,25.
In addition to genes that predispose to asthma there aregenes that are associated with the response to asthmatreatments. For example, variations in the gene encodingthe beta-adrenoreceptor have been linked to differences in
4 DEFINITION AND OVERVIEW
FACTORS INFLUENCING THEDEVELOPMENT AND EXPRESSIONOF ASTHMA
Factors that influence the risk of asthma can be dividedinto those that cause the development of asthma andthose that trigger asthma symptoms; some do both.The former include host factors (which are primarilygenetic) and the latter are usually environmental factors(Figure 1-2)21. However, the mechanisms whereby theyinfluence the development and expression of asthma arecomplex and interactive. For example, genes likelyinteract both with other genes and with environmentalfactors to determine asthma susceptibility22,23. In addition,developmental aspects—such as the maturation of theimmune response and the timing of infectious exposuresduring the first years of life—are emerging as importantfactors modifying the risk of asthma in the geneticallysusceptible person.
Figure 1-2. Factors Influencing the Developmentand Expression of Asthma
HOST FACTORSGenetic, e.g.,
Genes pre-disposing to atopyGenes pre-disposing to airway hyperresponsiveness
ObesitySex
ENVIRONMENTAL FACTORSAllergens
Indoor: Domestic mites, furred animals (dogs, cats,mice), cockroach allergen, fungi, molds, yeastsOutdoor: Pollens, fungi, molds, yeasts
Infections (predominantly viral)Occupational sensiti ersTobacco smoke
Passive smokingActive smoking
Outdoor/Indoor Air PollutionDiet
Additionally, some characteristics have been linked to anincreased risk for asthma, but are not themselves truecausal factors. The apparent racial and ethnic differencesin the prevalence of asthma reflect underlying geneticvariances with a significant overlay of socioeconomic andenvironmental factors. In turn, the links between asthmaand socioeconomic status—with a higher prevalence of
asthma in developed than in developing nations, in poorcompared to affluent populations in developed nations,and in affluent compared to poor populations in developingnations—likely reflect lifestyle differences such asexposure to allergens, access to health care, etc.
Much of what is known about asthma risk factors comesfrom studies of young children. Risk factors for thedevelopment of asthma in adults, particularly de novo inadults who did not have asthma in childhood, are lesswell defined.
The lack of a clear definition for asthma presents asignificant problem in studying the role of different riskfactors in the development of this complex disease,because the characteristics that define asthma (e.g.,airway hyperresponsiveness, atopy, and allergicsensiti ation) are themselves products of complexgene-environment interactions and are therefore bothfeatures of asthma and risk factors for the developmentof the disease.
Host Factors
Genetic. Asthma has a heritable component, but it is notsimple. Current data show that multiple genes may beinvolved in the pathogenesis of asthma24,25, and differentgenes may be involved in different ethnic groups. Thesearch for genes linked to the development of asthma hasfocused on four major areas: production of allergen-specific IgE antibodies (atopy); expression of airwayhyperresponsiveness; generation of inflammatorymediators, such as cytokines, chemokines, and growthfactors; and determination of the ratio between Th1 andTh2 immune responses (as relevant to the hygienehypothesis of asthma)26.
Family studies and case-control association analyses haveidentified a number of chromosomal regions associatedwith asthma susceptibility. For example, a tendency toproduce an elevated level of total serum IgE is co-inheritedwith airway hyperresponsiveness, and a gene (or genes)governing airway hyperresponsiveness is located near amajor locus that regulates serum IgE levels onchromosome 5q27. However, the search for a specificgene (or genes) involved in susceptibility to atopy orasthma continues, as results to date have beeninconsistent24,25.
In addition to genes that predispose to asthma there aregenes that are associated with the response to asthmatreatments. For example, variations in the gene encodingthe beta-adrenoreceptor have been linked to differences in
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

DEFINITION AND OVERVIEW 5
Obesity.Asthmaismorefrequentlyobservedinobesesubjects(BodyMassIndex>30kg/m2)andismoredifficultto control124-127,134.Obesepeoplewithasthmahavelowerlungfunctionandmoreco-morbiditiescomparedwithnormalweightpeoplewithasthma131.Theuseofsystemicglucocorticosteroidsandasedentarylifestylemaypromoteobesityinsevereasthmapatients,butinmostinstances,obesityprecedesthedevelopmentofasthma.
Howobesitypromotesthedevelopmentofasthmaisstilluncertainbutitmayresultfromthecombinedeffectsofvariousfactors.Ithasbeenproposedthatobesitycouldinfluenceairwayfunctionduetoitseffectonlungmechanics,developmentofapro-inflammatorystate,inadditiontogenetic,developmental,hormonalorneurogenicinfluences35,129,130.Inthisregard,obesepatientshaveareducedexpiratoryreservevolume,apatternofbreathingthatmaypossiblyalterairwaysmoothmuscleplasticityandairway function34.Furthermore,thereleasebyadipocytesofvariouspro-inflammatorycytokinesandmediatorssuchasinterleukin-6,tumornecrosisfactor(TNF)-α, eotaxin, andleptin,combinedwithalowerlevelofanti-inflammatoryadipokinesinobesesubjectscanfavorasystemicinflammatorystatealthoughitisunknownhowthiscouldinfluenceairwayfunction131,132.
Sex.Malesexisariskfactorforasthmainchildren.Priortotheageof14,theprevalenceofasthmaisnearlytwiceasgreatinboysasingirls36.Aschildrengetolderthedifferencebetweenthesexesnarrows,andbyadulthoodtheprevalenceofasthmaisgreaterinwomenthaninmen.Thereasonsforthissex-relateddifferencearenotclear.However,lungsizeissmallerinmalesthaninfemalesatbirth37butlargerinadulthood.
Environmental Factors
Thereissomeoverlapbetweenenvironmentalfactorsthatinfluencetheriskofdevelopingasthma,andfactorsthatcauseasthmasymptoms—forexample,occupationalsensitizersbelonginbothcategories.However,therearesomeimportantcausesofasthmasymptoms—suchasairpollutionandsomeallergens—whichhavenotbeenclearlylinkedtothedevelopmentofasthma.RiskfactorsthatcauseasthmasymptomsarediscussedindetailinChapter 4.2.
Allergens.Althoughindoorandoutdoorallergensarewellknowntocauseasthmaexacerbations,theirspecificroleinthedevelopmentofasthmaisstillnotfullyresolved.Birth-cohortstudieshaveshownthatsensitizationtohousedustmiteallergens,catdander,dogdander38,39,andAspergillusmold40areindependentriskfactorsforasthma-likesymptomsinchildrenupto3yearsofage.However,therelationshipbetweenallergenexposureandsensitizationin
childrenisnotstraightforward.Itdependsontheallergen,thedose,thetimeofexposure,thechild’sage,andprobablygeneticsaswell.
Forsomeallergens,suchasthosederivedfromhousedustmitesandcockroaches,theprevalenceofsensitizationappearstobedirectlycorrelatedwithexposure38,41.However,althoughsomedatasuggestthatexposuretohousedustmiteallergensmaybeacausalfactorinthedevelopmentofasthma42,otherstudieshavequestionedthisinterpretation43,44.Cockroachinfestationhasbeenshowntobeanimportantcauseofallergicsensitization,particularlyininner-cityhomes45.
Inthecaseofdogsandcats,someepidemiologicstudieshavefoundthatearlyexposuretotheseanimalsmayprotectachildagainstallergicsensitizationorthedevelopmentofasthma46-48,butotherssuggestthatsuchexposuremayincreasetheriskofallergicsensitization47,49-51.Thisissueremainsunresolved.
Theprevalenceofasthmaisreducedinchildrenraisedinaruralsetting,whichmaybelinkedtothepresenceofendotoxinintheseenvironments52.
Infections.Duringinfancy,anumberofviruseshavebeenassociatedwiththeinceptionoftheasthmaticphenotype.Respiratorysyncytialvirus(RSV)andparainfluenzavirusproduceapatternofsymptomsincludingbronchiolitisthatparallelmanyfeaturesofchildhoodasthma53,54.Anumberoflong-termprospectivestudiesofchildrenadmittedtothehospitalwithdocumentedRSVhaveshownthatapproximately40%willcontinuetowheezeorhaveasthmaintolaterchildhood53.Ontheotherhand,evidencealsoindicatesthatcertainrespiratoryinfectionsearlyinlife,includingmeaslesandsometimesevenRSV,mayprotectagainstthedevelopmentofasthma55,56.Thedatadonotallowspecificconclusionstobedrawn.Parasiteinfectionsdonotingeneralprotectagainstasthma,butinfectionwithhookwormmayreducetherisk120.
The“hygienehypothesis”ofasthmasuggeststhatexposuretoinfectionsearlyinlifeinfluencesthedevelopmentofachild’simmunesystemalonga“nonallergic”pathway,leadingtoareducedriskofasthmaandotherallergicdiseases.Althoughthehygienehypothesiscontinuestobeinvestigated,thismechanismmayexplainobservedassociationsbetweenfamilysize,birthorder,day-careattendance,andtheriskofasthma.Forexample,youngchildrenwitholdersiblingsandthosewhoattenddaycareareatincreasedriskofinfections,butenjoyprotectionagainstthedevelopmentofallergicdiseases,includingasthmalaterinlife57-59.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

6 DEFINITION AND OVERVIEW
Theinteractionbetweenatopyandviralinfectionsappearstobeacomplexrelationship60,inwhichtheatopicstatecaninfluencethelowerairwayresponsetoviralinfections,viralinfectionscantheninfluencethedevelopmentofallergicsensitization,andinteractionscanoccurwhenindividualsareexposedsimultaneouslytobothallergensandviruses.
Occupational sensitizers.Over300substanceshavebeenassociatedwithoccupationalasthma61-65,whichisdefinedasasthmacausedbyexposuretoanagentencounteredintheworkenvironment.Thesesubstancesincludehighlyreactivesmallmoleculessuchasisocyanates,irritantsthatmaycauseanalterationinairwayresponsiveness,knownimmunogenssuchasplatinumsalts,andcomplexplantandanimalbiologicalproductsthatstimulatetheproductionofIgE(Figure 1-3).
Occupationalasthmaarisespredominantlyinadults66, 67, andoccupationalsensitizersareestimatedtocauseabout1in10casesofasthmaamongadultsofworkingage68.Asthmaisthemostcommonoccupationalrespiratorydisorderinindustrializedcountries69.Occupationsassociatedwithahighriskforoccupationalasthmaincludefarmingandagriculturalwork,painting(includingspraypainting),cleaningwork,andplasticmanufacturing62.
Mostoccupationalasthmaisimmunologicallymediatedandhasalatencyperiodofmonthstoyearsaftertheonsetofexposure70.IgE-mediatedallergicreactionsandcell-mediatedallergicreactionsareinvolved71, 72.
Levelsabovewhichsensitizationfrequentlyoccurshavebeenproposedformanyoccupationalsensitizers.However,thefactorsthatcausesomepeoplebutnototherstodevelopoccupationalasthmainresponsetothesameexposuresarenotwellidentified.Veryhighexposurestoinhaledirritantsmaycause“irritantinducedasthma”(formerlycalledthereactiveairwaysdysfunctionalsyndrome)eveninnon-atopicpersons.Atopyandtobaccosmokingmayincreasetheriskofoccupationalsensitization,butscreeningindividualsforatopyisoflimitedvalueinpreventingoccupationalasthma73.Themostimportantmethodofpreventingoccupationalasthmaiseliminationorreductionofexposuretooccupationalsensitizers.
Tobacco smoke.Tobaccosmokingisassociatedwithaccelerateddeclineoflungfunctioninpeoplewithasthma133,increasesasthmaseverity,mayrenderpatientslessresponsivetotreatmentwithinhaled121,122 and systemic74glucocorticosteroids,andreducesthelikelihoodofasthmabeingcontrolled75.
Exposuretotobaccosmokebothprenatally135,136 and afterbirthisassociatedwithmeasurableharmfuleffectsincludingagreaterriskofdevelopingasthma-likesymptomsinearlychildhood.However,evidenceofincreasedriskofallergicdiseasesisuncertain77, 78.Distinguishingtheindependentcontributionsofprenatalandpostnatalmaternalsmokingisproblematic79.However,studiesoflungfunctionimmediatelyafterbirthhaveshownthatmaternalsmokingduringpregnancyhasaninfluenceonlungdevelopment37.Furthermore,infantsofsmokingmothersare4timesmorelikelytodevelopwheezingillnessesinthefirstyearoflife79.Incontrast,thereislittleevidence(basedonmetaanalysis)thatmaternalsmokingduringpregnancyhasaneffectonallergicsensitization78.Exposuretoenvironmentaltobaccosmoke(passivesmoking)increasestheriskoflowerrespiratorytractillnesses in infancy80andchildhood81.
Figure 1-3. Examples of Agents Causing Asthma inSelected Occupations*
Occupation/occupational field AgentAnimal and Plant Proteins
Bakers Flour, amylaseDairy farmers Storage mitesDetergent manufacturing Bacillus subtilis enzymesElectrical soldering Colophony (pine resin)Farmers Soybean dustFish food manufacturing Midges, parasitesFood processing Coffee bean dust, meat tenderizer, tea, shellfish,
amylase, egg proteins, pancreatic enzymes,papain
Granary workers Storage mites, Aspergillus, indoor ragweed, grassHealth care workers Psyllium, latexLaxative manufacturing Ispaghula, psylliumPoultry farmers Poultry mites, droppings, feathersResearch workers, veterinarians Locusts, dander, urine proteinsSawmill workers, carpenters Wood dust (western red cedar, oak, mahogany,
ebrawood, redwood, Lebanon cedar, Africanmaple, eastern white cedar)
Shipping workers Grain dust (molds, insects, grain)Silk workers Silk worm moths and larvae
Inorganic chemicalsBeauticians PersulfatePlating Nickel saltsRefinery workers Platinum salts, vanadium
Organic chemicalsAutomobile painting Ethanolamine, dissocyanatesHospital workers Disinfectants (sulfathiazole, chloramines,
formaldehyde, glutaraldehyde), latexManufacturing Antibiotics, piperazine, methyldopa, salbutamol,
cimetidineRubber processing Formaldehyde, ethylene diamine, phthalic anhydridePlastics industry Toluene dissocyanate, hexamethyl dissocyanate,
dephenylmethyl isocyanate, phthalic anhydride,triethylene tetramines, trimellitic anhydride,hexamethyl tetramine, acrylates
*See http6//www.bohrf.org.uk for a comprehensive list of known sensitizing agents
Occupational asthma arises predominantly in adults66, 67,and occupational sensiti ers are estimated to cause about1 in 10 cases of asthma among adults of working age68.Asthma is the most common occupational respiratorydisorder in industriali ed countries69. Occupationsassociated with a high risk for occupational asthma includefarming and agricultural work, painting (including spraypainting), cleaning work, and plastic manufacturing62.
Most occupational asthma is immunologically mediatedand has a latency period of months to years after the onsetof exposure70. IgE-mediated allergic reactions and cell-mediated allergic reactions are involved71, 72.
Levels above which sensiti ation frequently occurs havebeen proposed for many occupational sensiti ers.However, the factors that cause some people but not
others to develop occupational asthma in response to thesame exposures are not well identified. Very highexposures to inhaled irritants may cause “irritant inducedasthma” (formerly called the reactive airways dysfunctionalsyndrome) even in non-atopic persons. Atopy andtobacco smoking may increase the risk of occupationalsensiti ation, but screening individuals for atopy is oflimited value in preventing occupational asthma73. Themost important method of preventing occupational asthmais elimination or reduction of exposure to occupationalsensiti ers.
tobacco smoke. Tobacco smoking is associated withaccelerated decline of lung function in people with asthma,increases asthma severity, may render patients lessresponsive to treatment with inhaled74,124 and systemic75
glucocorticosteroids, and reduces the likelihood of asthmabeing controlled76.
Exposure to tobacco smoke both prenatally and after birthis associated with measurable harmful effects including agreater risk of developing asthma-like symptoms in earlychildhood. However, evidence of increased risk of allergicdiseases is uncertain77, 78. Distinguishing the independentcontributions of prenatal and postnatal maternal smokingis problematic79. However, studies of lung functionimmediately after birth have shown that maternal smokingduring pregnancy has an influence on lung development37.Furthermore, infants of smoking mothers are 4 times morelikely to develop whee ing illnesses in the first year of life80.In contrast, there is little evidence (based on meta-analysis) that maternal smoking during pregnancy has aneffect on allergic sensiti ation78. Exposure toenvironmental tobacco smoke (passive smoking)increases the risk of lower respiratory tract illnesses ininfancy81 and childhood82.
outdoor/indoor air pollution. The role of outdoor airpollution in causing asthma remains controversial83.Children raised in a polluted environment have diminishedlung function84, but the relationship of this loss of functionto the development of asthma is not known.
Outbreaks of asthma exacerbations have been shown tooccur in relationship to increased levels of air pollution,and this may be related to a general increase in the levelof pollutants or to specific allergens to which individualsare sensiti ed85-87. However, the role of pollutants in thedevelopment of asthma is less well defined. Similarassociations have been observed in relation to indoorpollutants, e.g., smoke and fumes from gas and biomassfuels used for heating and cooling, molds, and cockroachinfestations.
6 DEFINITION AND OVERVIEW
Figure 1-3. Examples of Agents Causing Asthma inSelected Occupations*
Occupation/occupational field AgentAnimal and Plant Proteins
Bakers Flour, amylaseDairy farmers Storage mitesDetergent manufacturing Bacillus subtilis en ymesElectrical soldering Colophony (pine resin)Farmers Soybean dustFish food manufacturing Midges, parasitesFood processing Coffee bean dust, meat tenderi er, tea, shellfish,
amylase, egg proteins, pancreatic en ymes,papain
Granary workers Storage mites, Aspergillus, indoor ragweed, grassHealth care workers Psyllium, latexLaxative manufacturing Ispaghula, psylliumPoultry farmers Poultry mites, droppings, feathersResearch workers, veterinarians Locusts, dander, urine proteinsSawmill workers, carpenters Wood dust (western red cedar, oak, mahogany,
ebrawood, redwood, Lebanon cedar, Africanmaple, eastern white cedar)
Shipping workers Grain dust (molds, insects, grain)Silk workers Silk worm moths and larvae
Inorganic chemicalsBeauticians PersulfatePlating Nickel saltsRefinery workers Platinum salts, vanadium
Organic chemicalsAutomobile painting Ethanolamine, dissocyanatesHospital workers Disinfectants (sulfathia ole, chloramines,
formaldehyde, glutaraldehyde), latexManufacturing Antibiotics, pipera ine, methyldopa, salbutamol,
cimetidineRubber processing Formaldehyde, ethylene diamine, phthalic anhydridePlastics industry Toluene dissocyanate, hexamethyl dissocyanate,
dephenylmethyl isocyanate, phthalic anhydride,triethylene tetramines, trimellitic anhydride,hexamethyl tetramine, acrylates
*See http6//www.bohrf.org.uk for a comprehensive list of known sensitizing agents
Occupational asthma arises predominantly in adults66, 67,and occupational sensiti ers are estimated to cause about1 in 10 cases of asthma among adults of working age68.Asthma is the most common occupational respiratorydisorder in industriali ed countries69. Occupationsassociated with a high risk for occupational asthma includefarming and agricultural work, painting (including spraypainting), cleaning work, and plastic manufacturing62.
Most occupational asthma is immunologically mediatedand has a latency period of months to years after the onsetof exposure70. IgE-mediated allergic reactions and cell-mediated allergic reactions are involved71, 72.
Levels above which sensiti ation frequently occurs havebeen proposed for many occupational sensiti ers.However, the factors that cause some people but not
others to develop occupational asthma in response to thesame exposures are not well identified. Very highexposures to inhaled irritants may cause “irritant inducedasthma” (formerly called the reactive airways dysfunctionalsyndrome) even in non-atopic persons. Atopy andtobacco smoking may increase the risk of occupationalsensiti ation, but screening individuals for atopy is oflimited value in preventing occupational asthma73. Themost important method of preventing occupational asthmais elimination or reduction of exposure to occupationalsensiti ers.
tobacco smoke. Tobacco smoking is associated withaccelerated decline of lung function in people with asthma,increases asthma severity, may render patients lessresponsive to treatment with inhaled74,124 and systemic75
glucocorticosteroids, and reduces the likelihood of asthmabeing controlled76.
Exposure to tobacco smoke both prenatally and after birthis associated with measurable harmful effects including agreater risk of developing asthma-like symptoms in earlychildhood. However, evidence of increased risk of allergicdiseases is uncertain77, 78. Distinguishing the independentcontributions of prenatal and postnatal maternal smokingis problematic79. However, studies of lung functionimmediately after birth have shown that maternal smokingduring pregnancy has an influence on lung development37.Furthermore, infants of smoking mothers are 4 times morelikely to develop whee ing illnesses in the first year of life80.In contrast, there is little evidence (based on meta-analysis) that maternal smoking during pregnancy has aneffect on allergic sensiti ation78. Exposure toenvironmental tobacco smoke (passive smoking)increases the risk of lower respiratory tract illnesses ininfancy81 and childhood82.
outdoor/indoor air pollution. The role of outdoor airpollution in causing asthma remains controversial83.Children raised in a polluted environment have diminishedlung function84, but the relationship of this loss of functionto the development of asthma is not known.
Outbreaks of asthma exacerbations have been shown tooccur in relationship to increased levels of air pollution,and this may be related to a general increase in the levelof pollutants or to specific allergens to which individualsare sensiti ed85-87. However, the role of pollutants in thedevelopment of asthma is less well defined. Similarassociations have been observed in relation to indoorpollutants, e.g., smoke and fumes from gas and biomassfuels used for heating and cooling, molds, and cockroachinfestations.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

DEFINITION AND OVERVIEW 7
Outdoor/indoor air pollution.Theroleofoutdoorairpollutionincausingasthmaremainscontroversial82.Childrenraisedinapollutedenvironmenthavediminishedlungfunction83,buttherelationshipofthislossoffunctiontothedevelopmentofasthmaisnotknown.
Outbreaksofasthmaexacerbationshavebeenshowntooccurinrelationshiptoincreasedlevelsofairpollution,andthismayberelatedtoageneralincreaseinthelevelofpollutantsortospecificallergenstowhichindividualsaresensitized84-86.However,theroleofpollutantsinthedevelopmentofasthmaislesswelldefined.Similarassociationshavebeenobservedinrelationtoindoorpollutants,e.g.,smokeandfumesfromgasandbiomassfuelsusedforheatingandcooling,molds,andcockroachinfestations.
Diet.Theroleofdiet,particularlybreast-feeding,inrelationtothedevelopmentofasthmahasbeenextensivelystudiedand,ingeneral,thedatarevealthatinfantsfedformulasofintactcow’smilkorsoyproteinhaveahigherincidenceofwheezingillnessesinearlychildhoodcomparedwiththosefedbreastmilk87.
SomedataalsosuggestthatcertaincharacteristicsofWesterndiets,suchasincreaseduseofprocessedfoodsanddecreasedantioxidant(intheformoffruitsandvegetables),increasedn-6polyunsaturatedfattyacid(foundinmargarineandvegetableoil),anddecreasedn-3polyunsaturatedfattyacid(foundinoilyfish)intakeshavecontributedtotherecentincreasesinasthmaandatopicdisease88.
Asthmaisaninflammatorydisorderoftheairways,whichinvolvesseveralinflammatorycellsandmultiplemediatorsthatresultincharacteristicpathophysiologicalchanges89.Inwaysthatarestillnotwellunderstood,thispatternofinflammationisstronglyassociatedwithairwayhyper-responsivenessandasthmasymptoms.
Airway Inflammation In Asthma
Theclinicalspectrumofasthmaishighlyvariable,anddifferentcellularpatternshavebeenobserved,butthepresenceofairwayinflammationremainsaconsistentfeature.Theairwayinflammationinasthmaispersistenteventhoughsymptomsareepisodic,andtherelationshipbetweentheseverityofasthmaandtheintensityofinflammationisnotclearlyestablished90,91.Theinflammationaffectsallairwaysincludinginmostpatientstheupperrespiratorytractandnosebutitsphysiologicaleffectsaremostpronouncedinmedium-sizedbronchi.
MECHANISMS OF ASTHMA
Figure 1-4: Inflammatory Cells in Asthmatic Airways
Mast cells: Activated mucosal mast cells release bronchoconstrictor mediators (histamine, cysteinyl leukotrienes, prostaglandin D2)92. These cells are activated by allergens through high-affinity IgE receptors, as well as by osmotic stimuli (accounting for exercise-induced bronchoconstriction). Increased mast cell numbers in airway smooth muscle may be linked to airway hyperresponsiveness93.
Eosinophils, present in increased numbers in the airways, release basic proteins that may damage airway epithelial cells. They may also have a role in the release of growth factors and airway remodeling94.
T lymphocytes, present in increased numbers in the airways, release specific cytokines, including IL-4, IL-5, IL-9, and IL-13, that orchestrate eosinophilic inflammation and IgE production by B lymphocytes95. An increase in Th2 cell activity may be due in part to a reduction in regulatory T cells that normally inhibit Th2 cells. There may also be an increase in inKT cells, which release large amounts of T helper 1 (Th1) and Th2 cytokines96.
Dendritic cells sample allergens from the airway surface and migrate to regional lymph nodes, where they interact with regulatory T cells and ultimately stimulate production of Th2 cells from na ve T cells97.
Macrophages are increased in number in the airways and may be activated by allergens through low-affinity IgE receptors to release inflammatory mediators and cytokines that amplify the inflammatory response98.
Neutrophil numbers are increased in the airways and sputum of patients with severe asthma and in smoking asthmatics, but the pathophysiological role of these cells is uncertain and their increase may even be due to glucocorticosteroid therapy99 .
Figure 1-5: Airway Structural Cells Involved in the Pathogenesis of Asthma
Airway epithelial cells sense their mechanical environment, express multiple inflammatory proteins in asthma, and release cytokines, chemokines, and lipid mediators. Viruses and air pollutants interact with epithelial cells.
Airway smooth muscle cells express similar inflammatory proteins to epithelial cells100.
Endothelial cells of the bronchial circulation play a role in recruiting inflammatory cells from the circulation into the airway.
Fibroblasts and myofibroblasts produce connective tissue components, such as collagens and proteoglycans, that are involved in airway remodeling.
Airway nerves are also involved. Cholinergic nerves may be activated by reflex triggers in the airways and cause bronchoconstriction and mucus secretion. Sensory nerves, which may be sensiti ed by inflammatory stimuli including neurotrophins, cause reflex changes and symptoms such as cough and chest tightness, and may release inflammatory neuropeptides101.
diet. The role of diet, particularly breast-feeding, inrelation to the development of asthma has beenextensively studied and, in general, the data reveal thatinfants fed formulas of intact cow's milk or soy protein havea higher incidence of whee ing illnesses in early childhoodcompared with those fed breast milk88.
Some data also suggest that certain characteristics ofWestern diets, such as increased use of processed foodsand decreased antioxidant (in the form of fruits and vegetables),increased n-6 polyunsaturated fatty acid (found in margarineand vegetable oil), and decreased n-3 polyunsaturatedfatty acid (found in oily fish) intakes have contributed tothe recent increases in asthma and atopic disease89.
MECHANISMS OF ASTHMA
Asthma is an inflammatory disorder of the airways, whichinvolves several inflammatory cells and multiple mediatorsthat result in characteristic pathophysiological changes21,90.In ways that are still not well understood, this pattern ofinflammation is strongly associated with airway hyper-responsiveness and asthma symptoms.
Airway Inflammation In Asthma
The clinical spectrum of asthma is highly variable, anddifferent cellular patterns have been observed, but thepresence of airway inflammation remains a consistentfeature. The airway inflammation in asthma is persistenteven though symptoms are episodic, and the relationshipbetween the severity of asthma and the intensity ofinflammation is not clearly established91,92. Theinflammation affects all airways including in most patientsthe upper respiratory tract and nose but its physiologicaleffects are most pronounced in medium-si ed bronchi.The pattern of inflammation in the airways appears to besimilar in all clinical forms of asthma, whether allergic,non-allergic, or aspirin-induced, and at all ages.
inflammatory cells. The characteristic pattern ofinflammation found in allergic diseases is seen in asthma,with activated mast cells, increased numbers of activatedeosinophils, and increased numbers of T cell receptorinvariant natural killer T cells and T helper 2 lymphocytes(Th2), which release mediators that contribute tosymptoms (Figure 1-4). Structural cells of the airwaysalso produce inflammatory mediators, and contribute to thepersistence of inflammation in various ways (Figure 1-5).
inflammatory mediators. Over 100 different mediators arenow recogni ed to be involved in asthma and mediate thecomplex inflammatory response in the airways103 (Figure 1-6).
diet. The role of diet, particularly breast-feeding, inrelation to the development of asthma has beenextensively studied and, in general, the data reveal thatinfants fed formulas of intact cow's milk or soy protein havea higher incidence of whee ing illnesses in early childhoodcompared with those fed breast milk88.
Some data also suggest that certain characteristics ofWestern diets, such as increased use of processed foodsand decreased antioxidant (in the form of fruits and vegetables),increased n-6 polyunsaturated fatty acid (found in margarineand vegetable oil), and decreased n-3 polyunsaturatedfatty acid (found in oily fish) intakes have contributed tothe recent increases in asthma and atopic disease89.
Asthma is an inflammatory disorder of the airways, whichinvolves several inflammatory cells and multiple mediatorsthat result in characteristic pathophysiological changes21,90.In ways that are still not well understood, this pattern ofinflammation is strongly associated with airway hyper-responsiveness and asthma symptoms.
Airway Inflammation In Asthma
The clinical spectrum of asthma is highly variable, anddifferent cellular patterns have been observed, but thepresence of airway inflammation remains a consistentfeature. The airway inflammation in asthma is persistenteven though symptoms are episodic, and the relationshipbetween the severity of asthma and the intensity ofinflammation is not clearly established91,92. Theinflammation affects all airways including in most patientsthe upper respiratory tract and nose but its physiologicaleffects are most pronounced in medium-si ed bronchi.The pattern of inflammation in the airways appears to besimilar in all clinical forms of asthma, whether allergic,non-allergic, or aspirin-induced, and at all ages.
inflammatory cells. The characteristic pattern ofinflammation found in allergic diseases is seen in asthma,with activated mast cells, increased numbers of activatedeosinophils, and increased numbers of T cell receptorinvariant natural killer T cells and T helper 2 lymphocytes(Th2), which release mediators that contribute tosymptoms (Figure 1-4). Structural cells of the airwaysalso produce inflammatory mediators, and contribute to thepersistence of inflammation in various ways (Figure 1-5).
inflammatory mediators. Over 100 different mediators arenow recogni ed to be involved in asthma and mediate thecomplex inflammatory response in the airways103 (Figure 1-6).
Figure 1-4: Inflammatory Cells in Asthmatic Airways
Mast cells: Activated mucosal mast cells releasebronchoconstrictor mediators (histamine, cysteinyl leukotrienes,prostaglandin D2)93. These cells are activated by allergensthrough high-affinity IgE receptors, as well as by osmotic stimuli(accounting for exercise-induced bronchoconstriction). Increasedmast cell numbers in airway smooth muscle may be linked toairway hyperresponsiveness94.
Eosinophils, present in increased numbers in the airways,release basic proteins that may damage airway epithelial cells.They may also have a role in the release of growth factors andairway remodeling95.
T lymphocytes, present in increased numbers in the airways,release specific cytokines, including IL-4, IL-5, IL-9, and IL-13,that orchestrate eosinophilic inflammation and IgE production byB lymphocytes96. An increase in Th2 cell activity may be due inpart to a reduction in regulatory T cells that normally inhibit Th2cells. There may also be an increase in inKT cells, which releaselarge amounts of T helper 1 (Th1) and Th2 cytokines97.
Dendritic cells sample allergens from the airway surface andmigrate to regional lymph nodes, where they interact withregulatory T cells and ultimately stimulate production of Th2cells from na ve T cells98.
Macrophages are increased in number in the airways and maybe activated by allergens through low-affinity IgE receptors torelease inflammatory mediators and cytokines that amplify theinflammatory response99.
Neutrophil numbers are increased in the airways and sputum ofpatients with severe asthma and in smoking asthmatics, but thepathophysiological role of these cells is uncertain and theirincrease may even be due to glucocorticosteroid therapy100.
Figure 1-5: Airway Structural Cells Involved in thePathogenesis of Asthma
Airway epithelial cells sense their mechanical environment,express multiple inflammatory proteins in asthma, and releasecytokines, chemokines, and lipid mediators. Viruses and airpollutants interact with epithelial cells.
Airway smooth muscle cells express similar inflammatoryproteins to epithelial cells101.
Endothelial cells of the bronchial circulation play a role inrecruiting inflammatory cells from the circulation into the airway.
Fibroblasts and myofibroblasts produce connective tissuecomponents, such as collagens and proteoglycans, that areinvolved in airway remodeling.
Airway nerves are also involved. Cholinergic nerves may beactivated by reflex triggers in the airways and causebronchoconstriction and mucus secretion. Sensory nerves,which may be sensiti ed by inflammatory stimuli includingneurotrophins, cause reflex changes and symptoms such ascough and chest tightness, and may release inflammatoryneuropeptides102.
DEFINITION AND OVERVIEW 7
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

8 DEFINITION AND OVERVIEW
Thepatternofinflammationintheairwaysappearstobesimilarinallclinicalformsofasthma,whetherallergic,non-allergic,oraspirin-induced,andatallages.
Inflammatory cells.Thecharacteristicpatternofinflammationfoundinallergicdiseasesisseeninasthma,withactivatedmastcells,increasednumbersofactivatedeosinophils,andincreasednumbersofTcellreceptor
invariantnaturalkillerTcellsandThelper2lymphocytes(Th2),whichreleasemediatorsthatcontributetosymptoms(Figure 1-4).Structuralcellsoftheairwaysalsoproduceinflammatorymediators,andcontributetothepersistenceofinflammationinvariousways(Figure 1-5).Inflammatorymediators.Over100differentmediatorsarenowrecognizedtobeinvolvedinasthmaandmediatethecomplexinflammatoryresponseintheairways(Figure 1-6).
Structural changes in the airways.Inadditiontotheinflammatoryresponse,therearecharacteristicstructuralchanges,oftendescribedasairwayremodeling,intheairwaysofasthmapatients(Figure 1-7).Someofthesechangesarerelatedtotheseverityofthediseaseandmayresultinrelativelyirreversiblenarrowingoftheairways107,108.Thesechangesmayrepresentrepairinresponsetochronicinflammation.
Pathophysiology Airwaynarrowingisthefinalcommonpathwayleadingtosymptomsandphysiologicalchangesinasthma.Severalfactorscontributetothedevelopmentofairwaynarrowinginasthma109-111(Figure 1-8).
Airway hyperresponsiveness. Airway hyperresponsiveness,thecharacteristicfunctionalabnormalityofasthma,resultsinairwaynarrowinginapatientwithasthmainresponsetoastimulusthatwouldbeinnocuousinanormalperson.Inturn,thisairwaynarrowingleadstovariableairflowlimitationandintermittentsymptoms.Airwayhyperresponsivenessislinkedtobothinflammationandrepairoftheairwaysandispartiallyreversiblewiththerapy.Itsmechanisms(Figure 1-9)areincompletelyunderstood.
Figure 1-6: Key Mediators of Asthma
Chemokines are important in the recruitment of inflammatorycells into the airways and are mainly expressed in airwayepithelial cells102. Eotaxin is relatively selective for eosinophils,whereas thymus and activation-regulated chemokines (TARC)and macrophage-derived chemokines (MDC) recruit Th2 cells.
Cysteinyl leukotrienes are potent bronchoconstrictors andproinflammatory mediators mainly derived from mast cells and eosinophils.They are the only mediator whose inhibition has been associatedwith an improvement in lung function and asthma symptoms103.
Cytokines orchestrate the inflammatory response in asthma anddetermine its severity104. Key cytokines include IL-1 and TNF-oc,which amplify the inflammatory response, and GM-CSF, whichprolongs eosinophil survival in the airways. Th2-derived cytokinesinclude IL-5, which is required for eosinophil differentiation andsurvival; IL-4, which is important for Th2 cell differentiation; andIL-13, needed for IgE formation.
Histamine is released from mast cells and contributes tobronchoconstriction and to the inflammatory response.
Nitric oxide (NO), a potent vasodilator, is produced predominantlyfrom the action of inducible nitric oxide synthase in airway epithelialcells105. Exhaled NO is increasingly being used to monitor theeffectiveness of asthma treatment, because of its reportedassociation with the presence of inflammation in asthma106.
Prostaglandin D2 is a bronchoconstrictor derived predominantlyfrom mast cells and is involved in Th2 cell recruitment to the airways.
Structural changes in the airways. In addition to theinflammatory response, there are characteristic structuralchanges, often described as airway remodeling, in theairways of asthma patients (Figure 1-7). Some of thesechanges are related to the severity of the disease and mayresult in relatively irreversible narrowing of the airways109, 110.These changes may represent repair in response tochronic inflammation.
Figure 1-7: Structural Changes in Asthmatic Airways
Subepithelial fibrosis results from the deposition of collagen fibersand proteoglycans under the basement membrane and is seen inall asthmatic patients, including children, even before the onset ofsymptoms but may be influenced by treatment. Fibrosis occurs inother layers for the airway wall, with deposition of collagen andproteoglycans.
Airway smooth muscle increases, due both to hypertrophy(increased si e of individual cells) and hyperplasia (increased celldivision), and contributes to the increased thickness of the airwaywall111. This process may relate to disease severity and is causedby inflammatory mediators, such as growth factors.
Blood vessels in airway walls proliferate the influence of growthfactors such as vascular endothelial growth factor (VEGF) andmay contribute to increased airway wall thickness.
Mucus hypersecretion results from increased numbers of gobletcells in the airway epithelium and increased si e of submucosalglands.
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
Figure 1-8: Airway Narrowing in Asthma
Airway smooth muscle contraction in response to multiplebronchoconstrictor mediators and neurotransmitters is thepredominant mechanism of airway narrowing and is largelyreversed by bronchodilators.
Airway edema is due to increased microvascular leakage inresponse to inflammatory mediators. This may be particularlyimportant during acute exacerbations.
Airway thickening due to structural changes, often termed“remodeling,” may be important in more severe disease and isnot fully reversible by current therapy.
Mucus hypersecretion may lead to luminal occlusion (“mucusplugging”) and is a product of increased mucus secretion andinflammatory exudates.
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Figure 1-9: Mechanisms of Airway Hyperresponsiveness
Excessive contraction of airway smooth muscle may resultfrom increased volume and/or contractility of airway smoothmuscle cells112.
Uncoupling of airway contraction as a result of inflammatorychanges in the airway wall may lead to excessive narrowing of theairways and a loss of the maximum plateau of contraction found innormal ariways when bronchoconstrictor substances are inhaled113.
Thickening of the airway wall by edema and structural changesamplifies airway narrowing due to contraction of airway smoothmuscle for geometric reasons114.
Sensory nerves may be sensiti ed by inflammation, leading toexaggerated bronchoconstriction in response to sensory stimuli.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
8 DEFINITION AND OVERVIEW
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
Figure 1-8: Airway Narrowing in Asthma
Airway smooth muscle contraction in response to multiplebronchoconstrictor mediators and neurotransmitters is thepredominant mechanism of airway narrowing and is largelyreversed by bronchodilators.
Airway edema is due to increased microvascular leakage inresponse to inflammatory mediators. This may be particularlyimportant during acute exacerbations.
Airway thickening due to structural changes, often termed“remodeling,” may be important in more severe disease and isnot fully reversible by current therapy.
Mucus hypersecretion may lead to luminal occlusion (“mucusplugging”) and is a product of increased mucus secretion andinflammatory exudates.
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Figure 1-9: Mechanisms of Airway Hyperresponsiveness
Excessive contraction of airway smooth muscle may resultfrom increased volume and/or contractility of airway smoothmuscle cells112.
Uncoupling of airway contraction as a result of inflammatorychanges in the airway wall may lead to excessive narrowing of theairways and a loss of the maximum plateau of contraction found innormal ariways when bronchoconstrictor substances are inhaled113.
Thickening of the airway wall by edema and structural changesamplifies airway narrowing due to contraction of airway smoothmuscle for geometric reasons114.
Sensory nerves may be sensiti ed by inflammation, leading toexaggerated bronchoconstriction in response to sensory stimuli.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
Figure 1-6: Key Mediators of Asthma
Chemokines are important in the recruitment of inflammatorycells into the airways and are mainly expressed in airwayepithelial cells104. Eotaxin is relatively selective for eosinophils,whereas thymus and activation-regulated chemokines (TARC)and macrophage-derived chemokines (MDC) recruit Th2 cells.
Cysteinyl leukotrienes are potent bronchoconstrictors andproinflammatorymediatorsmainlyderived frommast cells andeosinophils.They are the only mediator whose inhibition has been associatedwith an improvement in lung function and asthma symptoms105.
Cytokines orchestrate the inflammatory response in asthma anddetermine its severity106. Key cytokines include IL-1[ and TNF-oc,which amplify the inflammatory response, and GM-CSF, whichprolongs eosinophil survival in the airways. Th2-derived cytokinesinclude IL-5, which is required for eosinophil differentiation andsurvival; IL-4, which is important for Th2 cell differentiation; andIL-13, needed for IgE formation.
Histamine is released from mast cells and contributes tobronchoconstriction and to the inflammatory response.
Nitric oxide (NO), a potent vasodilator, is produced predominantlyfrom the action of inducible nitric oxide synthase in airway epithelialcells107. Exhaled NO is increasingly being used to monitor theeffectiveness of asthma treatment, because of its reportedassociation with the presence of inflammation in asthma108.
Prostaglandin D2 is a bronchoconstrictor derived predominantlyfrom mast cells and is involved in Th2 cell recruitment to the airways.
Structural changes in the airways. In addition to theinflammatory response, there are characteristic structuralchanges, often described as airway remodeling, in theairways of asthma patients (Figure 1-7). Some of thesechanges are related to the severity of the disease and mayresult in relatively irreversible narrowing of the airways109, 110.These changes may represent repair in response tochronic inflammation.
Figure 1-7: Structural Changes in Asthmatic Airways
Subepithelial fibrosis results from the deposition of collagen fibersand proteoglycans under the basement membrane and is seen inall asthmatic patients, including children, even before the onset ofsymptoms but may be influenced by treatment. Fibrosis occurs inother layers for the airway wall, with deposition of collagen andproteoglycans.
Airway smooth muscle increases, due both to hypertrophy(increased si e of individual cells) and hyperplasia (increased celldivision), and contributes to the increased thickness of the airwaywall111. This process may relate to disease severity and is causedby inflammatory mediators, such as growth factors.
Blood vessels in airway walls proliferate the influence of growthfactors such as vascular endothelial growth factor (VEGF) andmay contribute to increased airway wall thickness.
Mucus hypersecretion results from increased numbers of gobletcells in the airway epithelium and increased si e of submucosalglands.
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Figure 1-9: Mechanisms of Airway Hyperresponsiveness
Excessive contraction of airway smooth muscle may resultfrom increased volume and/or contractility of airway smoothmuscle cells112.
Uncoupling of airway contraction as a result of inflammatorychanges in the airway wall may lead to excessive narrowing of theairways and a loss of the maximum plateau of contraction found innormal ariways when bronchoconstrictor substances are inhaled113.
Thickening of the airway wall by edema and structural changesamplifies airway narrowing due to contraction of airway smoothmuscle for geometric reasons114.
Sensory nerves may be sensiti ed by inflammation, leading toexaggerated bronchoconstriction in response to sensory stimuli.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
8 DEFINITION AND OVERVIEW
Figure 1-6: Key Mediators of Asthma
Chemokines are important in the recruitment of inflammatorycells into the airways and are mainly expressed in airwayepithelial cells104. Eotaxin is relatively selective for eosinophils,whereas thymus and activation-regulated chemokines (TARC)and macrophage-derived chemokines (MDC) recruit Th2 cells.
Cysteinyl leukotrienes are potent bronchoconstrictors andproinflammatorymediatorsmainlyderived frommast cells andeosinophils.They are the only mediator whose inhibition has been associatedwith an improvement in lung function and asthma symptoms105.
Cytokines orchestrate the inflammatory response in asthma anddetermine its severity106. Key cytokines include IL-1[ and TNF-oc,which amplify the inflammatory response, and GM-CSF, whichprolongs eosinophil survival in the airways. Th2-derived cytokinesinclude IL-5, which is required for eosinophil differentiation andsurvival; IL-4, which is important for Th2 cell differentiation; andIL-13, needed for IgE formation.
Histamine is released from mast cells and contributes tobronchoconstriction and to the inflammatory response.
Nitric oxide (NO), a potent vasodilator, is produced predominantlyfrom the action of inducible nitric oxide synthase in airway epithelialcells107. Exhaled NO is increasingly being used to monitor theeffectiveness of asthma treatment, because of its reportedassociation with the presence of inflammation in asthma108.
Prostaglandin D2 is a bronchoconstrictor derived predominantlyfrom mast cells and is involved in Th2 cell recruitment to the airways.
Structural changes in the airways. In addition to theinflammatory response, there are characteristic structuralchanges, often described as airway remodeling, in theairways of asthma patients (Figure 1-7). Some of thesechanges are related to the severity of the disease and mayresult in relatively irreversible narrowing of the airways109, 110.These changes may represent repair in response tochronic inflammation.
Figure 1-7: Structural Changes in Asthmatic Airways
Subepithelial fibrosis results from the deposition of collagen fibersand proteoglycans under the basement membrane and is seen inall asthmatic patients, including children, even before the onset ofsymptoms but may be influenced by treatment. Fibrosis occurs inother layers for the airway wall, with deposition of collagen andproteoglycans.
Airway smooth muscle increases, due both to hypertrophy(increased si e of individual cells) and hyperplasia (increased celldivision), and contributes to the increased thickness of the airwaywall111. This process may relate to disease severity and is causedby inflammatory mediators, such as growth factors.
Blood vessels in airway walls proliferate the influence of growthfactors such as vascular endothelial growth factor (VEGF) andmay contribute to increased airway wall thickness.
Mucus hypersecretion results from increased numbers of gobletcells in the airway epithelium and increased si e of submucosalglands.
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
Figure 1-8: Airway Narrowing in Asthma
Airway smooth muscle contraction in response to multiplebronchoconstrictor mediators and neurotransmitters is thepredominant mechanism of airway narrowing and is largelyreversed by bronchodilators.
Airway edema is due to increased microvascular leakage inresponse to inflammatory mediators. This may be particularlyimportant during acute exacerbations.
Airway thickening due to structural changes, often termed“remodeling,” may be important in more severe disease and isnot fully reversible by current therapy.
Mucus hypersecretion may lead to luminal occlusion (“mucusplugging”) and is a product of increased mucus secretion andinflammatory exudates.
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
8 DEFINITION AND OVERVIEW
Structural changes in the airways. In addition to theinflammatory response, there are characteristic structuralchanges, often described as airway remodeling, in theairways of asthma patients (Figure 1-7). Some of thesechanges are related to the severity of the disease and mayresult in relatively irreversible narrowing of the airways109, 110.These changes may represent repair in response tochronic inflammation.
Figure 1-7: Structural Changes in Asthmatic Airways
Subepithelial fibrosis results from the deposition of collagen fibersand proteoglycans under the basement membrane and is seen inall asthmatic patients, including children, even before the onset ofsymptoms but may be influenced by treatment. Fibrosis occurs inother layers for the airway wall, with deposition of collagen andproteoglycans.
Airway smooth muscle increases, due both to hypertrophy(increased si e of individual cells) and hyperplasia (increased celldivision), and contributes to the increased thickness of the airwaywall111. This process may relate to disease severity and is causedby inflammatory mediators, such as growth factors.
Blood vessels in airway walls proliferate the influence of growthfactors such as vascular endothelial growth factor (VEGF) andmay contribute to increased airway wall thickness.
Mucus hypersecretion results from increased numbers of gobletcells in the airway epithelium and increased si e of submucosalglands.
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
Figure 1-8: Airway Narrowing in Asthma
Airway smooth muscle contraction in response to multiplebronchoconstrictor mediators and neurotransmitters is thepredominant mechanism of airway narrowing and is largelyreversed by bronchodilators.
Airway edema is due to increased microvascular leakage inresponse to inflammatory mediators. This may be particularlyimportant during acute exacerbations.
Airway thickening due to structural changes, often termed“remodeling,” may be important in more severe disease and isnot fully reversible by current therapy.
Mucus hypersecretion may lead to luminal occlusion (“mucusplugging”) and is a product of increased mucus secretion andinflammatory exudates.
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Figure 1-9: Mechanisms of Airway Hyperresponsiveness
Excessive contraction of airway smooth muscle may resultfrom increased volume and/or contractility of airway smoothmuscle cells112.
Uncoupling of airway contraction as a result of inflammatorychanges in the airway wall may lead to excessive narrowing of theairways and a loss of the maximum plateau of contraction found innormal ariways when bronchoconstrictor substances are inhaled113.
Thickening of the airway wall by edema and structural changesamplifies airway narrowing due to contraction of airway smoothmuscle for geometric reasons114.
Sensory nerves may be sensiti ed by inflammation, leading toexaggerated bronchoconstriction in response to sensory stimuli.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
8 DEFINITION AND OVERVIEW
Figure 1-6: Key Mediators of Asthma
Chemokines are important in the recruitment of inflammatorycells into the airways and are mainly expressed in airwayepithelial cells104. Eotaxin is relatively selective for eosinophils,whereas thymus and activation-regulated chemokines (TARC)and macrophage-derived chemokines (MDC) recruit Th2 cells.
Cysteinyl leukotrienes are potent bronchoconstrictors andproinflammatorymediatorsmainlyderived frommast cells andeosinophils.They are the only mediator whose inhibition has been associatedwith an improvement in lung function and asthma symptoms105.
Cytokines orchestrate the inflammatory response in asthma anddetermine its severity106. Key cytokines include IL-1[ and TNF-oc,which amplify the inflammatory response, and GM-CSF, whichprolongs eosinophil survival in the airways. Th2-derived cytokinesinclude IL-5, which is required for eosinophil differentiation andsurvival; IL-4, which is important for Th2 cell differentiation; andIL-13, needed for IgE formation.
Histamine is released from mast cells and contributes tobronchoconstriction and to the inflammatory response.
Nitric oxide (NO), a potent vasodilator, is produced predominantlyfrom the action of inducible nitric oxide synthase in airway epithelialcells107. Exhaled NO is increasingly being used to monitor theeffectiveness of asthma treatment, because of its reportedassociation with the presence of inflammation in asthma108.
Prostaglandin D2 is a bronchoconstrictor derived predominantlyfrom mast cells and is involved in Th2 cell recruitment to the airways.
Structural changes in the airways. In addition to theinflammatory response, there are characteristic structuralchanges, often described as airway remodeling, in theairways of asthma patients (Figure 1-7). Some of thesechanges are related to the severity of the disease and mayresult in relatively irreversible narrowing of the airways109, 110.These changes may represent repair in response tochronic inflammation.
Figure 1-7: Structural Changes in Asthmatic Airways
Subepithelial fibrosis results from the deposition of collagen fibersand proteoglycans under the basement membrane and is seen inall asthmatic patients, including children, even before the onset ofsymptoms but may be influenced by treatment. Fibrosis occurs inother layers for the airway wall, with deposition of collagen andproteoglycans.
Airway smooth muscle increases, due both to hypertrophy(increased size of individual cells) and hyperplasia (increased celldivision), and contributes to the increased thickness of the airwaywall109. This process may relate to disease severity and is causedby inflammatory mediators, such as growth factors.
Blood vessels in airway walls proliferate the influence of growthfactors such as vascular endothelial growth factor (VEGF) andmay contribute to increased airway wall thickness.
Mucus hypersecretion results from increased numbers of gobletcells in the airway epithelium and increased size of submucosalglands.
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
Figure 1-8: Airway Narrowing in Asthma
Airway smooth muscle contraction in response to multiplebronchoconstrictor mediators and neurotransmitters is thepredominant mechanism of airway narrowing and is largelyreversed by bronchodilators.
Airway edema is due to increased microvascular leakage inresponse to inflammatory mediators. This may be particularlyimportant during acute exacerbations.
Airway thickening due to structural changes, often termed“remodeling,” may be important in more severe disease and isnot fully reversible by current therapy.
Mucus hypersecretion may lead to luminal occlusion (“mucusplugging”) and is a product of increased mucus secretion andinflammatory exudates.
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Figure 1-9: Mechanisms of Airway Hyperresponsiveness
Excessive contraction of airway smooth muscle may resultfrom increased volume and/or contractility of airway smoothmuscle cells112.
Uncoupling of airway contraction as a result of inflammatorychanges in the airway wall may lead to excessive narrowing of theairways and a loss of the maximum plateau of contraction found innormal ariways when bronchoconstrictor substances are inhaled113.
Thickening of the airway wall by edema and structural changesamplifies airway narrowing due to contraction of airway smoothmuscle for geometric reasons114.
Sensory nerves may be sensiti ed by inflammation, leading toexaggerated bronchoconstriction in response to sensory stimuli.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
Figure 1-6: Key Mediators of Asthma
Chemokines are important in the recruitment of inflammatorycells into the airways and are mainly expressed in airwayepithelial cells104. Eotaxin is relatively selective for eosinophils,whereas thymus and activation-regulated chemokines (TARC)and macrophage-derived chemokines (MDC) recruit Th2 cells.
Cysteinyl leukotrienes are potent bronchoconstrictors andproinflammatorymediatorsmainlyderived frommast cells andeosinophils.They are the only mediator whose inhibition has been associatedwith an improvement in lung function and asthma symptoms105.
Cytokines orchestrate the inflammatory response in asthma anddetermine its severity106. Key cytokines include IL-1[ and TNF-oc,which amplify the inflammatory response, and GM-CSF, whichprolongs eosinophil survival in the airways. Th2-derived cytokinesinclude IL-5, which is required for eosinophil differentiation andsurvival; IL-4, which is important for Th2 cell differentiation; andIL-13, needed for IgE formation.
Histamine is released from mast cells and contributes tobronchoconstriction and to the inflammatory response.
Nitric oxide (NO), a potent vasodilator, is produced predominantlyfrom the action of inducible nitric oxide synthase in airway epithelialcells107. Exhaled NO is increasingly being used to monitor theeffectiveness of asthma treatment, because of its reportedassociation with the presence of inflammation in asthma108.
Prostaglandin D2 is a bronchoconstrictor derived predominantlyfrom mast cells and is involved in Th2 cell recruitment to the airways.
Structural changes in the airways. In addition to theinflammatory response, there are characteristic structuralchanges, often described as airway remodeling, in theairways of asthma patients (Figure 1-7). Some of thesechanges are related to the severity of the disease and mayresult in relatively irreversible narrowing of the airways109, 110.These changes may represent repair in response tochronic inflammation.
Figure 1-7: Structural Changes in Asthmatic Airways
Subepithelial fibrosis results from the deposition of collagen fibersand proteoglycans under the basement membrane and is seen inall asthmatic patients, including children, even before the onset ofsymptoms but may be influenced by treatment. Fibrosis occurs inother layers for the airway wall, with deposition of collagen andproteoglycans.
Airway smooth muscle increases, due both to hypertrophy(increased si e of individual cells) and hyperplasia (increased celldivision), and contributes to the increased thickness of the airwaywall111. This process may relate to disease severity and is causedby inflammatory mediators, such as growth factors.
Blood vessels in airway walls proliferate the influence of growthfactors such as vascular endothelial growth factor (VEGF) andmay contribute to increased airway wall thickness.
Mucus hypersecretion results from increased numbers of gobletcells in the airway epithelium and increased si e of submucosalglands.
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Figure 1-9: Mechanisms of Airway Hyperresponsiveness
Excessive contraction of airway smooth muscle may resultfrom increased volume and/or contractility of airway smoothmuscle cells112.
Uncoupling of airway contraction as a result of inflammatorychanges in the airway wall may lead to excessive narrowing of theairways and a loss of the maximum plateau of contraction found innormal ariways when bronchoconstrictor substances are inhaled113.
Thickening of the airway wall by edema and structural changesamplifies airway narrowing due to contraction of airway smoothmuscle for geometric reasons114.
Sensory nerves may be sensiti ed by inflammation, leading toexaggerated bronchoconstriction in response to sensory stimuli.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
8 DEFINITION AND OVERVIEW
Figure 1-6: Key Mediators of Asthma
Chemokines are important in the recruitment of inflammatorycells into the airways and are mainly expressed in airwayepithelial cells104. Eotaxin is relatively selective for eosinophils,whereas thymus and activation-regulated chemokines (TARC)and macrophage-derived chemokines (MDC) recruit Th2 cells.
Cysteinyl leukotrienes are potent bronchoconstrictors andproinflammatorymediatorsmainlyderived frommast cells andeosinophils.They are the only mediator whose inhibition has been associatedwith an improvement in lung function and asthma symptoms105.
Cytokines orchestrate the inflammatory response in asthma anddetermine its severity106. Key cytokines include IL-1[ and TNF-oc,which amplify the inflammatory response, and GM-CSF, whichprolongs eosinophil survival in the airways. Th2-derived cytokinesinclude IL-5, which is required for eosinophil differentiation andsurvival; IL-4, which is important for Th2 cell differentiation; andIL-13, needed for IgE formation.
Histamine is released from mast cells and contributes tobronchoconstriction and to the inflammatory response.
Nitric oxide (NO), a potent vasodilator, is produced predominantlyfrom the action of inducible nitric oxide synthase in airway epithelialcells107. Exhaled NO is increasingly being used to monitor theeffectiveness of asthma treatment, because of its reportedassociation with the presence of inflammation in asthma108.
Prostaglandin D2 is a bronchoconstrictor derived predominantlyfrom mast cells and is involved in Th2 cell recruitment to the airways.
Structural changes in the airways. In addition to theinflammatory response, there are characteristic structuralchanges, often described as airway remodeling, in theairways of asthma patients (Figure 1-7). Some of thesechanges are related to the severity of the disease and mayresult in relatively irreversible narrowing of the airways109, 110.These changes may represent repair in response tochronic inflammation.
Figure 1-7: Structural Changes in Asthmatic Airways
Subepithelial fibrosis results from the deposition of collagen fibersand proteoglycans under the basement membrane and is seen inall asthmatic patients, including children, even before the onset ofsymptoms but may be influenced by treatment. Fibrosis occurs inother layers for the airway wall, with deposition of collagen andproteoglycans.
Airway smooth muscle increases, due both to hypertrophy(increased si e of individual cells) and hyperplasia (increased celldivision), and contributes to the increased thickness of the airwaywall111. This process may relate to disease severity and is causedby inflammatory mediators, such as growth factors.
Blood vessels in airway walls proliferate the influence of growthfactors such as vascular endothelial growth factor (VEGF) andmay contribute to increased airway wall thickness.
Mucus hypersecretion results from increased numbers of gobletcells in the airway epithelium and increased si e of submucosalglands.
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
Figure 1-8: Airway Narrowing in Asthma
Airway smooth muscle contraction in response to multiplebronchoconstrictor mediators and neurotransmitters is thepredominant mechanism of airway narrowing and is largelyreversed by bronchodilators.
Airway edema is due to increased microvascular leakage inresponse to inflammatory mediators. This may be particularlyimportant during acute exacerbations.
Airway thickening due to structural changes, often termed“remodeling,” may be important in more severe disease and isnot fully reversible by current therapy.
Mucus hypersecretion may lead to luminal occlusion (“mucusplugging”) and is a product of increased mucus secretion andinflammatory exudates.
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
8 DEFINITION AND OVERVIEW
Structural changes in the airways. In addition to theinflammatory response, there are characteristic structuralchanges, often described as airway remodeling, in theairways of asthma patients (Figure 1-7). Some of thesechanges are related to the severity of the disease and mayresult in relatively irreversible narrowing of the airways109, 110.These changes may represent repair in response tochronic inflammation.
Figure 1-7: Structural Changes in Asthmatic Airways
Subepithelial fibrosis results from the deposition of collagen fibersand proteoglycans under the basement membrane and is seen inall asthmatic patients, including children, even before the onset ofsymptoms but may be influenced by treatment. Fibrosis occurs inother layers for the airway wall, with deposition of collagen andproteoglycans.
Airway smooth muscle increases, due both to hypertrophy(increased si e of individual cells) and hyperplasia (increased celldivision), and contributes to the increased thickness of the airwaywall111. This process may relate to disease severity and is causedby inflammatory mediators, such as growth factors.
Blood vessels in airway walls proliferate the influence of growthfactors such as vascular endothelial growth factor (VEGF) andmay contribute to increased airway wall thickness.
Mucus hypersecretion results from increased numbers of gobletcells in the airway epithelium and increased si e of submucosalglands.
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
Figure 1-8: Airway Narrowing in Asthma
Airway smooth muscle contraction in response to multiplebronchoconstrictor mediators and neurotransmitters is thepredominant mechanism of airway narrowing and is largelyreversed by bronchodilators.
Airway edema is due to increased microvascular leakage inresponse to inflammatory mediators. This may be particularlyimportant during acute exacerbations.
Airway thickening due to structural changes, often termed“remodeling,” may be important in more severe disease and isnot fully reversible by current therapy.
Mucus hypersecretion may lead to luminal occlusion (“mucusplugging”) and is a product of increased mucus secretion andinflammatory exudates.
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Figure 1-9: Mechanisms of Airway Hyperresponsiveness
Excessive contraction of airway smooth muscle may resultfrom increased volume and/or contractility of airway smoothmuscle cells112.
Uncoupling of airway contraction as a result of inflammatorychanges in the airway wall may lead to excessive narrowing of theairways and a loss of the maximum plateau of contraction found innormal ariways when bronchoconstrictor substances are inhaled113.
Thickening of the airway wall by edema and structural changesamplifies airway narrowing due to contraction of airway smoothmuscle for geometric reasons114.
Sensory nerves may be sensiti ed by inflammation, leading toexaggerated bronchoconstriction in response to sensory stimuli.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
8 DEFINITION AND OVERVIEW
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
Figure 1-8: Airway Narrowing in Asthma
Airway smooth muscle contraction in response to multiplebronchoconstrictor mediators and neurotransmitters is thepredominant mechanism of airway narrowing and is largelyreversed by bronchodilators.
Airway edema is due to increased microvascular leakage inresponse to inflammatory mediators. This may be particularlyimportant during acute exacerbations.
Airway thickening due to structural changes, often termed“remodeling,” may be important in more severe disease and isnot fully reversible by current therapy.
Mucus hypersecretion may lead to luminal occlusion (“mucusplugging”) and is a product of increased mucus secretion andinflammatory exudates.
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Figure 1-9: Mechanisms of Airway Hyperresponsiveness
Excessive contraction of airway smooth muscle may resultfrom increased volume and/or contractility of airway smoothmuscle cells112.
Uncoupling of airway contraction as a result of inflammatorychanges in the airway wall may lead to excessive narrowing of theairways and a loss of the maximum plateau of contraction found innormal ariways when bronchoconstrictor substances are inhaled113.
Thickening of the airway wall by edema and structural changesamplifies airway narrowing due to contraction of airway smoothmuscle for geometric reasons114.
Sensory nerves may be sensiti ed by inflammation, leading toexaggerated bronchoconstriction in response to sensory stimuli.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
Figure 1-6: Key Mediators of Asthma
Chemokines are important in the recruitment of inflammatorycells into the airways and are mainly expressed in airwayepithelial cells104. Eotaxin is relatively selective for eosinophils,whereas thymus and activation-regulated chemokines (TARC)and macrophage-derived chemokines (MDC) recruit Th2 cells.
Cysteinyl leukotrienes are potent bronchoconstrictors andproinflammatorymediatorsmainlyderived frommast cells andeosinophils.They are the only mediator whose inhibition has been associatedwith an improvement in lung function and asthma symptoms105.
Cytokines orchestrate the inflammatory response in asthma anddetermine its severity106. Key cytokines include IL-1[ and TNF-oc,which amplify the inflammatory response, and GM-CSF, whichprolongs eosinophil survival in the airways. Th2-derived cytokinesinclude IL-5, which is required for eosinophil differentiation andsurvival; IL-4, which is important for Th2 cell differentiation; andIL-13, needed for IgE formation.
Histamine is released from mast cells and contributes tobronchoconstriction and to the inflammatory response.
Nitric oxide (NO), a potent vasodilator, is produced predominantlyfrom the action of inducible nitric oxide synthase in airway epithelialcells107. Exhaled NO is increasingly being used to monitor theeffectiveness of asthma treatment, because of its reportedassociation with the presence of inflammation in asthma108.
Prostaglandin D2 is a bronchoconstrictor derived predominantlyfrom mast cells and is involved in Th2 cell recruitment to the airways.
Structural changes in the airways. In addition to theinflammatory response, there are characteristic structuralchanges, often described as airway remodeling, in theairways of asthma patients (Figure 1-7). Some of thesechanges are related to the severity of the disease and mayresult in relatively irreversible narrowing of the airways109, 110.These changes may represent repair in response tochronic inflammation.
Figure 1-7: Structural Changes in Asthmatic Airways
Subepithelial fibrosis results from the deposition of collagen fibersand proteoglycans under the basement membrane and is seen inall asthmatic patients, including children, even before the onset ofsymptoms but may be influenced by treatment. Fibrosis occurs inother layers for the airway wall, with deposition of collagen andproteoglycans.
Airway smooth muscle increases, due both to hypertrophy(increased si e of individual cells) and hyperplasia (increased celldivision), and contributes to the increased thickness of the airwaywall111. This process may relate to disease severity and is causedby inflammatory mediators, such as growth factors.
Blood vessels in airway walls proliferate the influence of growthfactors such as vascular endothelial growth factor (VEGF) andmay contribute to increased airway wall thickness.
Mucus hypersecretion results from increased numbers of gobletcells in the airway epithelium and increased si e of submucosalglands.
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
Figure 1-8: Airway Narrowing in Asthma
Airway smooth muscle contraction in response to multiplebronchoconstrictor mediators and neurotransmitters is thepredominant mechanism of airway narrowing and is largelyreversed by bronchodilators.
Airway edema is due to increased microvascular leakage inresponse to inflammatory mediators. This may be particularlyimportant during acute exacerbations.
Airway thickening due to structural changes, often termed“remodeling,” may be important in more severe disease and isnot fully reversible by current therapy.
Mucus hypersecretion may lead to luminal occlusion (“mucusplugging”) and is a product of increased mucus secretion andinflammatory exudates.
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Figure 1-9: Mechanisms of Airway Hyperresponsiveness
Excessive contraction of airway smooth muscle may resultfrom increased volume and/or contractility of airway smoothmuscle cells112.
Uncoupling of airway contraction as a result of inflammatorychanges in the airway wall may lead to excessive narrowing of theairways and a loss of the maximum plateau of contraction found innormal ariways when bronchoconstrictor substances are inhaled113.
Thickening of the airway wall by edema and structural changesamplifies airway narrowing due to contraction of airway smoothmuscle for geometric reasons114.
Sensory nerves may be sensiti ed by inflammation, leading toexaggerated bronchoconstriction in response to sensory stimuli.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
8 DEFINITION AND OVERVIEW
Figure 1-6: Key Mediators of Asthma
Chemokines are important in the recruitment of inflammatorycells into the airways and are mainly expressed in airwayepithelial cells104. Eotaxin is relatively selective for eosinophils,whereas thymus and activation-regulated chemokines (TARC)and macrophage-derived chemokines (MDC) recruit Th2 cells.
Cysteinyl leukotrienes are potent bronchoconstrictors andproinflammatorymediatorsmainlyderived frommast cells andeosinophils.They are the only mediator whose inhibition has been associatedwith an improvement in lung function and asthma symptoms105.
Cytokines orchestrate the inflammatory response in asthma anddetermine its severity106. Key cytokines include IL-1[ and TNF-oc,which amplify the inflammatory response, and GM-CSF, whichprolongs eosinophil survival in the airways. Th2-derived cytokinesinclude IL-5, which is required for eosinophil differentiation andsurvival; IL-4, which is important for Th2 cell differentiation; andIL-13, needed for IgE formation.
Histamine is released from mast cells and contributes tobronchoconstriction and to the inflammatory response.
Nitric oxide (NO), a potent vasodilator, is produced predominantlyfrom the action of inducible nitric oxide synthase in airway epithelialcells107. Exhaled NO is increasingly being used to monitor theeffectiveness of asthma treatment, because of its reportedassociation with the presence of inflammation in asthma108.
Prostaglandin D2 is a bronchoconstrictor derived predominantlyfrom mast cells and is involved in Th2 cell recruitment to the airways.
Structural changes in the airways. In addition to theinflammatory response, there are characteristic structuralchanges, often described as airway remodeling, in theairways of asthma patients (Figure 1-7). Some of thesechanges are related to the severity of the disease and mayresult in relatively irreversible narrowing of the airways109, 110.These changes may represent repair in response tochronic inflammation.
Figure 1-7: Structural Changes in Asthmatic Airways
Subepithelial fibrosis results from the deposition of collagen fibersand proteoglycans under the basement membrane and is seen inall asthmatic patients, including children, even before the onset ofsymptoms but may be influenced by treatment. Fibrosis occurs inother layers for the airway wall, with deposition of collagen andproteoglycans.
Airway smooth muscle increases, due both to hypertrophy(increased si e of individual cells) and hyperplasia (increased celldivision), and contributes to the increased thickness of the airwaywall111. This process may relate to disease severity and is causedby inflammatory mediators, such as growth factors.
Blood vessels in airway walls proliferate the influence of growthfactors such as vascular endothelial growth factor (VEGF) andmay contribute to increased airway wall thickness.
Mucus hypersecretion results from increased numbers of gobletcells in the airway epithelium and increased si e of submucosalglands.
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
Figure 1-8: Airway Narrowing in Asthma
Airway smooth muscle contraction in response to multiplebronchoconstrictor mediators and neurotransmitters is thepredominant mechanism of airway narrowing and is largelyreversed by bronchodilators.
Airway edema is due to increased microvascular leakage inresponse to inflammatory mediators. This may be particularlyimportant during acute exacerbations.
Airway thickening due to structural changes, often termed“remodeling,” may be important in more severe disease and isnot fully reversible by current therapy.
Mucus hypersecretion may lead to luminal occlusion (“mucusplugging”) and is a product of increased mucus secretion andinflammatory exudates.
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
8 DEFINITION AND OVERVIEW
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

DEFINITION AND OVERVIEW 9
Special Mechanisms
Acute exacerbations.Transientworseningofasthmamay occurasaresultofexposuretoriskfactorsforasthmasymptoms113,or“triggers,”suchasexercise,airpollutants,andevencertainweatherconditions,e.g.,thunderstorms86.Moreprolongedworseningisusuallyduetoviralinfectionsoftheupperrespiratorytract(particularlyrhinovirusandrespiratorysyncytialvirus)114orallergenexposurewhichincreaseinflammationinthelowerairways(acuteorchronicinflammation)thatmaypersistforseveraldaysorweeks.
Nocturnal asthma.Themechanismsaccountingfortheworseningofasthmaatnightarenotcompletelyunderstoodbutmaybedrivenbycircadianrhythmsofcirculatinghormonessuchasepinephrine,cortisol,andmelatoninandneuralmechanismssuchascholinergictone.Anincreaseinairwayinflammationatnighthasbeenreported.Thismightreflectareductioninendogenousanti-inflammatorymechanisms115.
Irreversible airflow limitation.Somepatientswithsevereasthmadevelopprogressiveairflowlimitationthatisnotfullyreversiblewithcurrentlyavailabletherapy.Thismayreflectthechangesinairwaystructureinchronicasthma116.
Difficult-to-treat asthma.Thereasonswhysomepatientsdevelopasthmathatisdifficulttomanageandrelativelyinsensitivetotheeffectsofglucocorticosteroidsarenotwellunderstood.Commonassociationsarepoorcompliancewithtreatmentandpsychologicalandpsychiatricdisorders.However,geneticfactorsmaycontributeinsome.Manyofthesepatientshavedifficult-to-treatasthmafromtheonsetofthedisease,ratherthanprogressingfrommilderasthma.Inthesepatientsairwayclosureleadstoairtrappingandhyperinflation.Althoughthepathologyappearsbroadlysimilartootherformsofasthma,thereisanincreaseinneutrophils,moresmallairwayinvolvement,andmorestructuralchanges.
Smoking and asthma.Tobaccosmokingmakesasthmamoredifficulttocontrol,resultsinmorefrequentexacerbationsandhospitaladmissions,andproducesamorerapiddeclineinlungfunctionandanincreasedriskofdeath117.Asthmapatientswhosmokemayhaveaneutrophil-predominantinflammationintheirairwaysandarepoorlyresponsivetoglucocorticosteroids121,122.
REFERENCES
1. ReddelH,WareS,MarksG,et al.Differencesbetweenasthmaexacerbationsandpoorasthmacontrol.Lancet1999;353:364-9.
2. MasoliM,FabianD,HoltS,BeasleyR.Theglobalburdenofasthma:executivesummaryoftheGINADisseminationCommitteereport.Allergy2004;59(5):469-78.
3. BeasleyR.TheGlobalBurdenofAsthmaReport,GlobalInitiativeforAsthma(GINA).Availablefromhttp://www.ginasthma. org 2004.
4. YanDC,OuLS,TsaiTL,WuWF,HuangJL.Prevalenceandseverityofsymptomsofasthma,rhinitis,andeczemain13-to14-year-oldchildreninTaipei,Taiwan.Ann Allergy Asthma Immunol 2005;95(6):579-85.
5. KoFW,WangHY,WongGW,LeungTF,HuiDS,ChanDP,et al.WheezinginChineseschoolchildren:diseaseseveritydistributionandmanagementpractices,acommunity-basedstudyinHongKongandGuanghou.Clin Exp Allergy 2005;35(11):1449-56.
6. Carvajal-UruenaI,Garcia-MarcosL,Busquets-MongeR,Morales Suare -Varela M, Garcia de Andoin N, Batlles-Garrido J,et al.[GeographicvariationintheprevalenceofasthmasymptomsinSpanishchildrenandadolescents.InternationalStudyofAsthmaandAllergiesinChildhood(ISAAC)Phase3,Spain].Arch Bronconeumol 2005;41(12):659-66.
7. Reference deleted
8. Reference deleted
9. MahapatraP.Social,economicandculturalaspectsofasthma:anexploratorystudyinAndraPradesh,India.Hyderbad,India:InstituteofHealthSystems;1993.
10. LaiCK,DeGuiaTS,KimYY,KuoSH,MukhopadhyayA,SorianoJB,et al.AsthmacontrolintheAsia-Pacificregion:theAsthmaInsightsandRealityinAsia-PacificStudy.J Allergy Clin Immunol2003;111(2):263-8.
11. LenneyW.Theburdenofpediatricasthma.Pediatr Pulmonol Suppl 1997;15:13-6.
12. NeffenH,FritscherC,SchachtFC,LevyG,ChiarellaP,SorianoJB,et al.AsthmacontrolinLatinAmerica:theAsthmaInsightsandRealityinLatinAmerica(AIRLA)survey.Rev Panam Salud Publica2005;17(3):191-7.
Structural changes in the airways. In addition to theinflammatory response, there are characteristic structuralchanges, often described as airway remodeling, in theairways of asthma patients (Figure 1-7). Some of thesechanges are related to the severity of the disease and mayresult in relatively irreversible narrowing of the airways109, 110.These changes may represent repair in response tochronic inflammation.
Figure 1-7: Structural Changes in Asthmatic Airways
Subepithelial fibrosis results from the deposition of collagen fibersand proteoglycans under the basement membrane and is seen inall asthmatic patients, including children, even before the onset ofsymptoms but may be influenced by treatment. Fibrosis occurs inother layers for the airway wall, with deposition of collagen andproteoglycans.
Airway smooth muscle increases, due both to hypertrophy(increased si e of individual cells) and hyperplasia (increased celldivision), and contributes to the increased thickness of the airwaywall111. This process may relate to disease severity and is causedby inflammatory mediators, such as growth factors.
Blood vessels in airway walls proliferate the influence of growthfactors such as vascular endothelial growth factor (VEGF) andmay contribute to increased airway wall thickness.
Mucus hypersecretion results from increased numbers of gobletcells in the airway epithelium and increased si e of submucosalglands.
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
Figure 1-8: Airway Narrowing in Asthma
Airway smooth muscle contraction in response to multiplebronchoconstrictor mediators and neurotransmitters is thepredominant mechanism of airway narrowing and is largelyreversed by bronchodilators.
Airway edema is due to increased microvascular leakage inresponse to inflammatory mediators. This may be particularlyimportant during acute exacerbations.
Airway thickening due to structural changes, often termed“remodeling,” may be important in more severe disease and isnot fully reversible by current therapy.
Mucus hypersecretion may lead to luminal occlusion (“mucusplugging”) and is a product of increased mucus secretion andinflammatory exudates.
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Figure 1-9: Mechanisms of Airway Hyperresponsiveness
Excessive contraction of airway smooth muscle may resultfrom increased volume and/or contractility of airway smoothmuscle cells112.
Uncoupling of airway contraction as a result of inflammatorychanges in the airway wall may lead to excessive narrowing of theairways and a loss of the maximum plateau of contraction found innormal ariways when bronchoconstrictor substances are inhaled113.
Thickening of the airway wall by edema and structural changesamplifies airway narrowing due to contraction of airway smoothmuscle for geometric reasons114.
Sensory nerves may be sensiti ed by inflammation, leading toexaggerated bronchoconstriction in response to sensory stimuli.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
8 DEFINITION AND OVERVIEW
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
Figure 1-8: Airway Narrowing in Asthma
Airway smooth muscle contraction in response to multiplebronchoconstrictor mediators and neurotransmitters is thepredominant mechanism of airway narrowing and is largelyreversed by bronchodilators.
Airway edema is due to increased microvascular leakage inresponse to inflammatory mediators. This may be particularlyimportant during acute exacerbations.
Airway thickening due to structural changes, often termed“remodeling,” may be important in more severe disease and isnot fully reversible by current therapy.
Mucus hypersecretion may lead to luminal occlusion (“mucusplugging”) and is a product of increased mucus secretion andinflammatory exudates.
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Figure 1-9: Mechanisms of Airway Hyperresponsiveness
Excessive contraction of airway smooth muscle may resultfrom increased volume and/or contractility of airway smoothmuscle cells112.
Uncoupling of airway contraction as a result of inflammatorychanges in the airway wall may lead to excessive narrowing of theairways and a loss of the maximum plateau of contraction found innormal ariways when bronchoconstrictor substances are inhaled113.
Thickening of the airway wall by edema and structural changesamplifies airway narrowing due to contraction of airway smoothmuscle for geometric reasons114.
Sensory nerves may be sensiti ed by inflammation, leading toexaggerated bronchoconstriction in response to sensory stimuli.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
Figure 1-6: Key Mediators of Asthma
Chemokines are important in the recruitment of inflammatorycells into the airways and are mainly expressed in airwayepithelial cells104. Eotaxin is relatively selective for eosinophils,whereas thymus and activation-regulated chemokines (TARC)and macrophage-derived chemokines (MDC) recruit Th2 cells.
Cysteinyl leukotrienes are potent bronchoconstrictors andproinflammatorymediatorsmainlyderived frommast cells andeosinophils.They are the only mediator whose inhibition has been associatedwith an improvement in lung function and asthma symptoms105.
Cytokines orchestrate the inflammatory response in asthma anddetermine its severity106. Key cytokines include IL-1[ and TNF-oc,which amplify the inflammatory response, and GM-CSF, whichprolongs eosinophil survival in the airways. Th2-derived cytokinesinclude IL-5, which is required for eosinophil differentiation andsurvival; IL-4, which is important for Th2 cell differentiation; andIL-13, needed for IgE formation.
Histamine is released from mast cells and contributes tobronchoconstriction and to the inflammatory response.
Nitric oxide (NO), a potent vasodilator, is produced predominantlyfrom the action of inducible nitric oxide synthase in airway epithelialcells107. Exhaled NO is increasingly being used to monitor theeffectiveness of asthma treatment, because of its reportedassociation with the presence of inflammation in asthma108.
Prostaglandin D2 is a bronchoconstrictor derived predominantlyfrom mast cells and is involved in Th2 cell recruitment to the airways.
Structural changes in the airways. In addition to theinflammatory response, there are characteristic structuralchanges, often described as airway remodeling, in theairways of asthma patients (Figure 1-7). Some of thesechanges are related to the severity of the disease and mayresult in relatively irreversible narrowing of the airways109, 110.These changes may represent repair in response tochronic inflammation.
Figure 1-7: Structural Changes in Asthmatic Airways
Subepithelial fibrosis results from the deposition of collagen fibersand proteoglycans under the basement membrane and is seen inall asthmatic patients, including children, even before the onset ofsymptoms but may be influenced by treatment. Fibrosis occurs inother layers for the airway wall, with deposition of collagen andproteoglycans.
Airway smooth muscle increases, due both to hypertrophy(increased si e of individual cells) and hyperplasia (increased celldivision), and contributes to the increased thickness of the airwaywall111. This process may relate to disease severity and is causedby inflammatory mediators, such as growth factors.
Blood vessels in airway walls proliferate the influence of growthfactors such as vascular endothelial growth factor (VEGF) andmay contribute to increased airway wall thickness.
Mucus hypersecretion results from increased numbers of gobletcells in the airway epithelium and increased si e of submucosalglands.
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Figure 1-9: Mechanisms of Airway Hyperresponsiveness
Excessive contraction of airway smooth muscle may resultfrom increased volume and/or contractility of airway smoothmuscle cells112.
Uncoupling of airway contraction as a result of inflammatorychanges in the airway wall may lead to excessive narrowing of theairways and a loss of the maximum plateau of contraction found innormal ariways when bronchoconstrictor substances are inhaled113.
Thickening of the airway wall by edema and structural changesamplifies airway narrowing due to contraction of airway smoothmuscle for geometric reasons114.
Sensory nerves may be sensiti ed by inflammation, leading toexaggerated bronchoconstriction in response to sensory stimuli.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
8 DEFINITION AND OVERVIEW
Figure 1-6: Key Mediators of Asthma
Chemokines are important in the recruitment of inflammatorycells into the airways and are mainly expressed in airwayepithelial cells104. Eotaxin is relatively selective for eosinophils,whereas thymus and activation-regulated chemokines (TARC)and macrophage-derived chemokines (MDC) recruit Th2 cells.
Cysteinyl leukotrienes are potent bronchoconstrictors andproinflammatorymediatorsmainlyderived frommast cells andeosinophils.They are the only mediator whose inhibition has been associatedwith an improvement in lung function and asthma symptoms105.
Cytokines orchestrate the inflammatory response in asthma anddetermine its severity106. Key cytokines include IL-1[ and TNF-oc,which amplify the inflammatory response, and GM-CSF, whichprolongs eosinophil survival in the airways. Th2-derived cytokinesinclude IL-5, which is required for eosinophil differentiation andsurvival; IL-4, which is important for Th2 cell differentiation; andIL-13, needed for IgE formation.
Histamine is released from mast cells and contributes tobronchoconstriction and to the inflammatory response.
Nitric oxide (NO), a potent vasodilator, is produced predominantlyfrom the action of inducible nitric oxide synthase in airway epithelialcells107. Exhaled NO is increasingly being used to monitor theeffectiveness of asthma treatment, because of its reportedassociation with the presence of inflammation in asthma108.
Prostaglandin D2 is a bronchoconstrictor derived predominantlyfrom mast cells and is involved in Th2 cell recruitment to the airways.
Structural changes in the airways. In addition to theinflammatory response, there are characteristic structuralchanges, often described as airway remodeling, in theairways of asthma patients (Figure 1-7). Some of thesechanges are related to the severity of the disease and mayresult in relatively irreversible narrowing of the airways109, 110.These changes may represent repair in response tochronic inflammation.
Figure 1-7: Structural Changes in Asthmatic Airways
Subepithelial fibrosis results from the deposition of collagen fibersand proteoglycans under the basement membrane and is seen inall asthmatic patients, including children, even before the onset ofsymptoms but may be influenced by treatment. Fibrosis occurs inother layers for the airway wall, with deposition of collagen andproteoglycans.
Airway smooth muscle increases, due both to hypertrophy(increased si e of individual cells) and hyperplasia (increased celldivision), and contributes to the increased thickness of the airwaywall111. This process may relate to disease severity and is causedby inflammatory mediators, such as growth factors.
Blood vessels in airway walls proliferate the influence of growthfactors such as vascular endothelial growth factor (VEGF) andmay contribute to increased airway wall thickness.
Mucus hypersecretion results from increased numbers of gobletcells in the airway epithelium and increased si e of submucosalglands.
Pathophysiology
Airway narrowing is the final common pathway leading tosymptoms and physiological changes in asthma. Severalfactors contribute to the development of airway narrowingin asthma (Figure 1-8).
Figure 1-8: Airway Narrowing in Asthma
Airway smooth muscle contraction in response to multiplebronchoconstrictor mediators and neurotransmitters is thepredominant mechanism of airway narrowing and is largelyreversed by bronchodilators.
Airway edema is due to increased microvascular leakage inresponse to inflammatory mediators. This may be particularlyimportant during acute exacerbations.
Airway thickening due to structural changes, often termed“remodeling,” may be important in more severe disease and isnot fully reversible by current therapy.
Mucus hypersecretion may lead to luminal occlusion (“mucusplugging”) and is a product of increased mucus secretion andinflammatory exudates.
airway hyperresponsiveness. Airway hyperresponsive-ness, the characteristic functional abnormality of asthma,results in airway narrowing in a patient with asthma inresponse to a stimulus that would be innocuous in anormal person. In turn, this airway narrowing leads tovariable airflow limitation and intermittent symptoms. Airwayhyperresponsiveness is linked to both inflammation and re-pair of the airways and is partially reversible with therapy.Its mechanisms (Figure 1-9) are incompletely understood.
Figure 1-9: Mechanisms of Airway Hyperresponsiveness
Excessive contraction of airway smooth muscle may resultfrom increased volume and/or contractility of airway smoothmuscle cells112.
Uncoupling of airway contraction as a result of inflammatorychanges in the airway wall may lead to excessive narrowing of theairways and a loss of the maximum plateau of contraction found innormal airways when bronchoconstrictor substances are inhaled.
Thickening of the airway wall by edema and structural changesamplifies airway narrowing due to contraction of airway smoothmuscle for geometric reasons112.
Sensory nerves may be sensitized by inflammation, leading toexaggerated bronchoconstriction in response to sensory stimuli.
Special Mechanisms
acute exacerbations. Transient worsening of asthmamay occur as a result of exposure to risk factors forasthma symptoms, or “triggers,” such as exercise, air
8 DEFINITION AND OVERVIEW
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

10 DEFINITION AND OVERVIEW
13. WeissKB,GergenPJ,HodgsonTA.AneconomicevaluationofasthmaintheUnitedStates.N Engl J Med 1992;326(13):862-6.
14. WeinsteinMC,StasonWB.Foundationsofcost-effectivenessanalysisforhealthandmedicalpractices. N Engl J Med 1977;296(13):716-21.
15. WeissKB,SullivanSD.Theeconomiccostsofasthma:areviewandconceptualmodel.Pharmacoeconomics 1993;4(1):14-30.
16. Actionasthma:theoccurrenceandcostofasthma.WestSussex,UnitedKingdom:Cambridge Medical Publications;1990.
17. MarionRJ,CreerTL,ReynoldsRV.Directandindirectcostsassociatedwiththemanagementofchildhoodasthma.Ann Allergy 1985;54(1):31-4.
18. Actionagainstasthma.AstrategicplanfortheDepartmentofHealthandHumanServices.Washington,DC:Department of Health and Human Services;2000.
19. ThompsonS.Onthesocialcostofasthma.Eur J Respir Dis Suppl 1984;136:185-91.
20. KarrRM,DaviesRJ,ButcherBT,LehrerSB,WilsonMR,DharmarajanV,et al.Occupationalasthma.J Allergy Clin Immunol1978;61(1):54-65.
21. BusseWW,LemanskeRF,Jr.Asthma.N Engl J Med 2001 ;344(5):350-62.
22. OberC.Perspectivesonthepastdecadeofasthmagenetics.J Allergy Clin Immunol2005;116(2):274-8.
23. HolgateST.GeneticandenvironmentalinteractioninAllergy andasthma.J Allergy Clin Immunol1999;104(6):1139-46.
24. HollowayJW,BegheB,HolgateST.Thegeneticbasisofatopicasthma.Clin Exp Allergy1999;29(8):1023-32.
25. WieschDG,MeyersDA,BleeckerER.Geneticsofasthma.J Allergy Clin Immunol1999;104(5):895-901.
26. StrachanDP.Hayfever,hygiene,andhouseholdsize.BMJ 1989;299(6710):1259-60.
27. PostmaDS,BleeckerER,AmelungPJ,HolroydKJ,XuJ,PanhuysenCI,et al.Geneticsusceptibilitytoasthma--bronchialhyperresponsivenesscoinheritedwithamajorgeneforatopy.
N Engl J Med1995;333(14):894-900.
28. IsraelE,ChinchilliVM,FordJG,BousheyHA,CherniackR,CraigTJ,et al.Useofregularlyscheduledalbuteroltreatmentinasthma:genotype-stratified,randomised,placebo-controlledcross-overtrial.Lancet2004;364(9444):1505-12.
29. ItoK,ChungKF,AdcockIM.Updateonglucocorticoidactionandresistance.J Allergy Clin Immunol2006;117(3):522-43.
30. InKH,AsanoK,BeierD,GrobholJ,FinnPW,SilvermanEK,et al.Naturallyoccurringmutationsinthehuman5-lipoxygenasegenepromoterthatmodifytranscriptionfactorbindingandreportergenetranscription.J Clin Invest1997;99(5):1130
31. DrazenJM,WeissST.Genetics:inheritthewheeze.Nature 2002;418(6896):383-4.
32. LaneSJ,ArmJP,StaynovDZ,LeeTH.ChemicalmutationalanalysisofthehumanglucocorticoidreceptorcDNAinglucocorticoid-resistantbronchialasthma.Am J Respir Cell Mol Biol1994;11(1):42-8.
33. TattersfieldAE,HallIP.Arebeta2-adrenoceptorpolymorphismsimportantinasthma--anunravellingstory.Lancet 2004;364(9444):1464-6.
34. ShoreSA,FredbergJJ.Obesity,smoothmuscle,andairwayhyperresponsiveness.J Allergy Clin Immunol2005;115(5):925-7.
35. BeutherDA,WeissST,SutherlandER.Obesityandasthma.Am J RespirCritCareMed2006;174(2):112-9.
36. HorwoodLJ,FergussonDM,ShannonFT.Socialandfamilialfactorsinthedevelopmentofearlychildhoodasthma.Pediatrics1985;75(5):859-68.
37. MartinezFD,WrightAL,TaussigLM,HolbergCJ,HalonenM,MorganWJ.Asthmaandwheezinginthefirstsixyearsoflife.TheGroupHealthMedicalAssociates.N Engl J Med 1995;332(3):133-8.
38. WahnU,LauS,BergmannR,KuligM,ForsterJ,BergmannK,et al.Indoorallergenexposureisariskfactorforsensitizationduringthefirstthreeyearsoflife.J Allergy Clin Immunol 1997;99(6Pt1):763-9.
39. SporikR,HolgateST,Platts-MillsTA,CogswellJJ.Exposuretohouse-dustmiteallergen(DerpI)andthedevelopmentofasthmainchildhood.Aprospectivestudy.N Engl J Med 1990;323(8):502-7.
40. HogaboamCM,CarpenterKJ,SchuhJM,BucklandKF.Aspergillusandasthma--anylink?Med Mycol2005;43Suppl1:S197-202.
41. HussK,AdkinsonNF,Jr.,EgglestonPA,DawsonC,VanNattaML,HamiltonRG.HousedustmiteandcockroachexposurearestrongriskfactorsforpositiveAllergyskintestresponsesintheChildhoodAsthmaManagementProgram.J Allergy Clin Immunol2001;107(1):48-54.
42. SearsMR,GreeneJM,WillanAR,WiecekEM,TaylorDR,Flannery EM, et al.Alongitudinal,population-based,cohortstudyofchildhoodasthmafollowedtoadulthood.N Engl J Med 2003;349(15):1414-22.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

DEFINITION AND OVERVIEW 11
43. SporikR,IngramJM,PriceW,SussmanJH,HonsingerRW,Platts-MillsTA.AssociationofasthmawithserumIgEandskintestreactivitytoallergensamongchildrenlivingathighaltitude.Ticklingthedragon’sbreath.Am J Respir Crit Care Med 1995;151(5):1388-92.
44. CharpinD,BirnbaumJ,HaddiE,GenardG,LanteaumeA,Toumi M, et al.AltitudeandAllergytohouse-dustmites.Aparadigmoftheinfluenceofenvironmentalexposureonallergicsensitization.Am Rev Respir Dis1991;143(5Pt1):983-6.
45. RosenstreichDL,EgglestonP,KattanM,BakerD,SlavinRG,GergenP,et al.TheroleofcockroachAllergyandexposuretocockroachallergenincausingmorbidityamonginner-citychildrenwithasthma.N Engl J Med1997;336(19):1356-63.
46. Platts-MillsT,VaughanJ,SquillaceS,WoodfolkJ,SporikR.Sensitisation,asthma,andamodifiedTh2responseinchildrenexposedtocatallergen:apopulation-basedcross-sectionalstudy.Lancet2001;357(9258):752-6.
47. OwnbyDR,JohnsonCC,PetersonEL.Exposuretodogsandcatsinthefirstyearoflifeandriskofallergicsensitizationat6to7yearsofage.JAMA2002;288(8):963-72.
48. GernJE,ReardonCL,HoffjanS,NicolaeD,LiZ,RobergKA, et al.Effectsofdogownershipandgenotypeonimmunedevelopmentandatopyininfancy.J Allergy Clin Immunol 2004;113(2):307-14.
49. CeledonJC,LitonjuaAA,RyanL,Platts-MillsT,WeissST,GoldDR.Exposuretocatallergen,maternalhistoryofasthma,andwheezinginfirst5yearsoflife.Lancet2002;360(9335):781-2.
50. MelenE,WickmanM,NordvallSL,vanHage-HamstenM,LindforsA.Influenceofearlyandcurrentenvironmentalexposurefactorsonsensitizationandoutcomeofasthmainpre-schoolchildren.Allergy2001;56(7):646-52.
51. AlmqvistC,EgmarAC,vanHage-HamstenM,BerglindN,PershagenG,NordvallSL,et al.Heredity,petownership,andconfoundingcontrolinapopulation-basedbirthcohort.J Allergy Clin Immunol2003;111(4):800-6.
52. Braun-FahrlanderC.Environmentalexposuretoendotoxinandothermicrobialproductsandthedecreasedriskofchildhoodatopy:evaluatingdevelopmentssinceApril2002.CurrOpinAllergyClinImmunol2003;3(5):325-9.
53. SigursN,BjarnasonR,SigurbergssonF,KjellmanB.RespiratorysyncytialvirusbronchiolitisininfancyisanimportantriskfactorforasthmaandAllergyatage7.Am J Respir Crit Care Med2000;161(5):1501-7.
54. SlyPD,KuselM,HoltPG.Doearly-lifeviralinfectionscauseasthma?J Allergy Clin Immunol2010;125(6):1202-5.
55. SteinRT,SherrillD,MorganWJ,HolbergCJ,HalonenM,TaussigLM,et al.RespiratorysyncytialvirusinearlylifeandriskofwheezeandAllergybyage13years.Lancet 1999;354(9178):541-5.
56. ShaheenSO,AabyP,HallAJ,BarkerDJ,HeyesCB,ShiellAW, et al.MeaslesandatopyinGuinea-Bissau.Lancet 1996;347(9018):1792-6.
57. IlliS,vonMutiusE,LauS,BergmannR,NiggemannB,Sommerfeld C, et al.Earlychildhoodinfectiousdiseasesandthedevelopmentofasthmauptoschoolage:abirthcohortstudy.BMJ2001;322(7283):390-5.
58. BallTM,Castro-RodrigueJA,GriffithKA,HolbergCJ,MartineFD,WrightAL.Siblings,day-careattendance,andtheriskofasthmaandwheezingduringchildhood.N Engl J Med 2000;343(8):538-43.
59. deMeerG,JanssenNA,BrunekreefB.Earlychildhoodenvironmentrelatedtomicrobialexposureandtheoccurrenceofatopicdiseaseatschoolage.Allergy2005;60(5):619-25.
60. ZambranoJC,CarperHT,RakesGP,PatrieJ,MurphyDD,Platts-Mills TA, et al.Experimentalrhinoviruschallengesinadultswithmildasthma:responsetoinfectioninrelationtoIgE.J Allergy Clin Immunol2003;111(5):1008-16.
61. MaloJL,LemiereC,GautrinD,LabrecqueM.Occupationalasthma.Curr Opin Pulm Med2004;10(1):57-61.
62. VenablesKM,Chan-YeungM.Occupationalasthma.Lancet 1997;349(9063):1465-9.
63. Chan-YeungM,MaloJL.Tableofthemajorinducersofoccupationalasthma.In:BernsteinIL,Chan-YeungM,MaloJL,BernsteinDI,eds.Asthma in the workplace.NewYork:MarcelDekker;1999:p.683-720.
64. NewmanLS.Occupationalasthma.Diagnosis,management,andprevention.Clin Chest Med1995;16(4):621-36.
65. FabbriLM,CaramoriG,MaestrelliP.Etiologyofoccupationalasthma.In:RothRA,ed.Comprehensive toxicology: toxicology of the respiratory system.Cambridge:PergamonPress;1997:p.425-35.
66. BernsteinIL,Chan-YeungM,MaloJL,BernsteinDI.Definitionandclassificationofasthma.In:BernsteinIL,Chan-YeungM,MaloJL,BernsteinDI,eds.Asthma in the workplace. New York:MarcelDekker;1999:p.1-4.
67. Chan-YeungM,MaloJL.Aetiologicalagentsinoccupationalasthma.Eur Respir J1994;7(2):346-71.
68. NicholsonPJ,CullinanP,TaylorAJ,BurgePS,BoyleC.Evidencebasedguidelinesfortheprevention,identification,andmanagementofoccupationalasthma.Occup Environ Med 2005;62(5):290-9.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

12 DEFINITION AND OVERVIEW
69. BlancPD,TorenK.Howmuchadultasthmacanbeattributedtooccupationalfactors?Am J Med1999;107(6):580-7.
70. SastreJ,VandenplasO,ParkHS.Pathogenesisofoccupationalasthma.Eur Respir J2003;22(2):364-73
71. MaestrelliP,FabbriLM,MaloJL.OccupationalAllergy.In:HolgateST,ChurchMK,LichtensteinLM,eds.Allergy, 2nd edition.2ndEditioned.London:MosbyInternational.
72. FrewA,ChangJH,ChanH,QuirceS,NoertjojoK,KeownP,etal.T-lymphocyteresponsestoplicaticacid-humanserumalbuminconjugateinoccupationalasthmacausedbywesternredcedar.J Allergy Clin Immunol1998;101(6Pt1):841-7.BernsteinIL,ed.Asthma in the workplace.NewYork:MarcelDekker;1993.
73. ChalmersGW,MacleodKJ,LittleSA,ThomsonLJ,McSharryCP,ThomsonNC.Influenceofcigarettesmokingoninhaledcorticosteroidtreatmentinmildasthma.Thorax 2002;57(3):226-30.
74. ChaudhuriR,LivingstonE,McMahonAD,ThomsonL,BorlandW,ThomsonNC.Cigarettesmokingimpairsthetherapeuticresponsetooralcorticosteroidsinchronicasthma.Am J Respir Crit Care Med2003;168(11):1308-11.
75. PedersenSE,BatemanED,BousquetJ,BusseWW,YoxallS,ClarkTJ.Determinantsofresponsetofluticasonepropionateandsalmeterol/fluticasonepropionatecombinationintheGainingOptimalAsthmacontroLstudy.J Allergy Clin Immunol 2007;120:1036-42.
76. StrachanDP,CookDG.Healtheffectsofpassivesmoking.6.Parentalsmokingandchildhoodasthma:longitudinalandcase-controlstudies.Thorax1998;53(3):204-12.
77. StrachanDP,CookDG.Healtheffectsofpassivesmoking.5.Parentalsmokingandallergicsensitisationinchildren.Thorax 1998;53(2):117-23.
78. KuligM,LuckW,LauS,NiggemannB,BergmannR,KlettkeU,et al.Effectofpre-andpostnataltobaccosmokeexposureonspecificsensitizationtofoodandinhalantallergensduringthefirst3yearsoflife.MulticenterAllergyStudyGroup,Germany.Allergy1999;54(3):220-8.
79. DezateuxC,StocksJ,DundasI,FletcherME.Impairedairwayfunctionandwheezingininfancy:theinfluenceofmaternalsmokingandageneticpredispositiontoasthma.Am J Respir CritCareMed1999;159(2):403-10.
80. NafstadP,KongerudJ,BottenG,HagenJA,JaakkolaJJ.Theroleofpassivesmokinginthedevelopmentofbronchialobstructionduringthefirst2yearsoflife.Epidemiology 1997;8(3):293-7.
81. Environmentaltobaccosmoke:ahazardtochildren.AmericanAcademyofPediatricsCommitteeonEnvironmentalHealth.Pediatrics1997;99(4):639-42.
82. AmericanThoracicSociety.Whatconstitutesanadversehealtheffectofairpollution?OfficialstatementoftheAmericanThoracicSociety.Am J RespirCritCareMed2000;161(2Pt1):665-73.
83. GaudermanWJ,AvolE,GillilandF,VoraH,ThomasD,BerhaneK,et al.Theeffectofairpollutiononlungdevelopmentfrom10to18yearsofage.N Engl J Med2004;351(11):1057
84. AntoJM,SorianoJB,SunyerJ,RodrigoMJ,MorellF,RocaJ,et al.Longtermoutcomeofsoybeanepidemicasthmaafteranallergenreductionintervention.Thorax1999;54(8):670-4.
85. ChenLL,TagerIB,PedenDB,ChristianDL,FerrandoRE,WelchBS,et al.Effectofozoneexposureonairwayresponsestoinhaledallergeninasthmaticsubjects.Chest 2004;125(6):2328-35.
86. MarksGB,ColquhounJR,GirgisST,KoskiMH,TreloarAB,Hansen P, et al.Thunderstormoutflowsprecedingepidemicsofasthmaduringspringandsummer.Thorax2001;56(6):468
87. FriedmanNJ,ZeigerRS.Theroleofbreast-feedinginthedevelopmentofallergiesandasthma.J Allergy Clin Immunol 2005;115(6):1238-48.
88. DevereuxG,SeatonA.Dietasariskfactorforatopyandasthma.J Allergy Clin Immunol2005;115(6):1109-17.
89. TattersfieldAE,KnoxAJ,BrittonJR,HallIP.Asthma.Lancet 2002;360(9342):1313-22.
90. CohnL,EliasJA,ChuppGL.Asthma:mechanismsofdiseasepersistenceandprogression.Annu Rev Immunol2004;22:789
91. BousquetJ,JefferyPK,BusseWW,JohnsonM,VignolaAM.Asthma.Frombronchoconstrictiontoairwaysinflammationandremodeling.Am J RespirCritCareMed2000;161(5):1720-45.
92. GalliSJ,KalesnikoffJ,GrimbaldestonMA,PiliponskyAM,WilliamsCM,TsaiM.Mastcellsas“tunable"effectorandimmunoregulatorycells:recentadvances.Annu Rev Immunol 2005;23:749-86.
93. RobinsonDS.Theroleofthemastcellinasthma:inductionofairwayhyperresponsivenessbyinteractionwithsmoothmuscle?J Allergy Clin Immunol2004;114(1):58-65.
94. KayAB,PhippsS,RobinsonDS.Aroleforeosinophilsinairwayremodellinginasthma.Trends Immunol2004;25(9):477
95. LarcheM,RobinsonDS,KayAB.TheroleofTlymphocytesinthepathogenesisofasthma.J Allergy Clin Immunol 2003;111(3):450-63.
96. AkbariO,FaulJL,HoyteEG,BerryGJ,WahlstromJ,KronenbergM,et al.CD4+invariantT-cell-receptor+naturalkillerTcellsinbronchialasthma.N Engl J Med 2006;354(11):111729.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

DEFINITION AND OVERVIEW 13
97. KuipersH,LambrechtBN.Theinterplayofdendriticcells,Th2cellsandregulatoryTcellsinasthma.Curr Opin Immunol 2004;16(6):702-8.
98. Peters-GoldenM.Thealveolarmacrophage:theforgottencellinasthma.Am J Respir Cell Mol Biol 2004;31(1):3-7.
99. WenzelS.Mechanismsofsevereasthma.Clin Exp Allergy 2003;33(12):1622-8.
100.ChungKF.Airwaysmoothmusclecells:contributingtoandregulatingairwaymucosalinflammation?Eur Respir J 2000;15(5):961-8.
101.GronebergDA,QuarcooD,FrossardN,FischerA.Neurogenicmechanismsinbronchialinflammatorydiseases.Allergy 2004;59(11):1139-52.
102.BarnesPJ,ChungKF,PageCP.Inflammatorymediatorsofasthma:anupdate.Pharmacol Rev1998;50(4):515-96.MillerAL,LukacsNW.Chemokinereceptors:understandingtheirroleinasthmaticdisease.Immunol Allergy Clin North Am 2004;24(4):667-83,vii.
103.LeffAR.Regulationofleukotrienesinthemanagementof
asthma:biologyandclinicaltherapy.Annu Rev Med2001;52:1-14.
104.BarnesPJ.Cytokinemodulatorsasnoveltherapiesforasthma.Annu Rev Pharmacol Toxicol2002;42:81-98.
105.RicciardoloFL,SterkPJ,GastonB,FolkertsG.Nitricoxideinhealthanddiseaseoftherespiratorysystem.Physiol Rev 2004;84(3):731-65.
106.BarnesPJ,DweikRA,GelbAF,GibsonPG,GeorgeSC,Grasemann H, et al.Exhalednitricoxideinpulmonarydiseases:acomprehensivereview.Chest.2010Sep;138(3):682-92.
107.JamesA.Airwayremodelinginasthma.Curr Opin Pulm Med 2005;11(1):1-6.
108.VignolaAM,MirabellaF,CostanzoG,DiGiorgiR,GjomarkajM, Bellia V, et al.Airwayremodelinginasthma.Chest 2003;123(3Suppl):417S-22S.
109.HirstSJ,MartinJG,BonacciJV,ChanV,FixmanED,HamidQA,et al.Proliferativeaspectsofairwaysmoothmuscle.JAllergyClinImmunol2004;114(2Suppl):S2-17.
110.BlackJL.Asthma--moremusclecellsormoremuscularcells?Am J RespirCritCareMed2004;169(9):980-1.
111.McParlandBE,MacklemPT,ParePD.Airwaywallremodeling:friendorfoe?JApplPhysiol2003;95(1):426-34.
112.WangL,McParlandBE,ParePD.Thefunctionalconsequencesofstructuralchangesintheairways:implicationsforairwayhyperresponsivenessinasthma.Chest2003;123(3Suppl):356S-62S.
113.NewsonR,StrachanD,ArchibaldE,EmberlinJ,Hardaker
P,CollierC.Acuteasthmaepidemics,weatherandpolleninEngland,1987-1994.Eur Respir J1998;11(3):694-701.
114.TanWC.Virusesinasthmaexacerbations.Curr Opin Pulm Med2005;11(1):21-6.
115.CalhounWJ.Nocturnalasthma.Chest2003;123(3Suppl):399S-405S.
116.BumbaceaD,CampbellD,NguyenL,CarrD,BarnesPJ,Robinson D, et al.Parametersassociatedwithpersistentairflowobstructioninchronicsevereasthma.Eur Respir J 2004;24(1):122-8.
117.ThomsonNC,ChaudhuriR,LivingstonE.Asthmaandcigarettesmoking.Eur Respir J2004;24(5):822-33.
118.AsherMI,MontefortS,BjorkstenB,LaiCK,StrachanDP,WeilandSK,WilliamsH;ISAACPhaseThreeStudyGroup.Worldwidetimetrendsintheprevalenceofsymptomsofasthma,allergicrhinoconjunctivitis,andeczemainchildhood:ISAACPhasesOneandThreerepeatmulticountrycross-sectionalsurveys.Lancet2006Aug26;368(9537):733-43.
119.AccordiniS,BugianiM,ArossaW,GerzeliS,MarinoniA,OlivieriM,PirinaP,CarroiL,DallariR,DeTogniA,deMarcoR.Poorcontrolincreasestheeconomiccostofasthma.Amulticentrepopulation-basedstudy.Int Arch Allergy Immunol 2006;141(2):189-98.
120.Leonardi-BeeJ,PritchardD,BrittonJ.Asthmaandcurrentintestinalparasiteinfection:systematicreviewandmetaanalysis.Am J RespirCritCareMed2006Sep1;174(5):514-23
121.LazarusSC,ChinchillVM,RollingsNJ,BousheyHA,CherniackR,CraigTJ et al.;NationalHeartLungandBloodInstitute’sAsthmaClinicalResearchNetworkSmokingaffectsresponsetoinhaledcorticosteroidsorleukotrienereceptorantagonistsinasthma.Am J RespirCritCareMed2007Apr15;175(8):783
122.ChaudhuriR,LivingstonE,McMahonAD,LaffertyJ,FraserI,SpearsM,McSharryCP,ThomsonNC.Effectsofsmokingcessationonlungfunctionandairwayinflammationinsmokerswithasthma.Am J Respir Crit Care Med2006Jul15;174(2):127-33.
123.PearceN,Aït-KhaledN,BeasleyR,MallolJ,KeilU,MitchellE,RobertsonC;andtheISAACPhaseThreeStudyGroup.Worldwidetrendsintheprevalenceofasthmasymptoms:phaseIIIoftheInternationalStudyofAsthmaandAllergiesinChildhood(ISAAC).Thorax2007Sep;62(9):758-66.Epub2007May15.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

14 DEFINITION AND OVERVIEW
124.BeutherDA,SutherlandER.Overweight,obesity,andincidentasthma:ameta-analysisofprospectiveepidemiologicstudies.Am J Respir Crit Care Med2007;175(7):661-6.
125.FordES.TheEpidemiologyofobesityandasthma.J Allergy Clin Immunol2005;115(5):897-909.
126.Saint-PierreP,BourdinA,ChanezP,DauresJP,GodardP.Areoverweightasthmaticsmoredifficulttocontrol?Allergy 2006;61(1):79-84.
127.LavoieKL,BaconSL,LabrecqueM,CartierA,DittoB.HigherBMIisassociatedwithworseasthmacontrolandqualityoflifebutnotasthmaseverity.Respir Med2006;100(4):648-57.
128.PakhaleS,DoucetteS,VandemheenK,BouletLP,McIvorRA,FitzgeraldJM, et al.Acomparisonofobeseandnon-obesepeoplewithasthma:exploringanasthma-obesityinteraction.Chest.2010Jun;137(6):1316-23.
129.SchaubB,vonME.Obesityandasthma,whatarethelinks?Curr Opin Allergy Clin Immunol2005;5(6):185-93.
130.WeissST,ShoreS.Obesityandasthma:directionsforresearch.Am J RespirCritCareMed2004;169(8):963-8.
131.ShoreSA.Obesityandasthma:possiblemechanisms.J Allergy Clin Immunol2008;121(5):1087-93;
132.Juge-AubryCE,HenrichotE,MeierCA.Adiposetissue:aregulatorofinflammation.Best Pract Res Clin Endocrinol Metab2005;19(4):547-66.
133.O’ByrnePM,LammCJ,BusseWW,TanWC,PedersenS;STARTInvestigatorsGroup.Theeffectsofinhaledbudesonideonlungfunctioninsmokersandnonsmokerswithmildpersistentasthma.Chest2009;136(6):1514-20.
134.NoalRB,MenezesAM,MacedoSE,DumithSC.Childhoodbodymassindexandriskofasthmainadolescence:asystematicreview.Obes Rev.2011Feb;12(2):93-104.
135.CohenRT,RabyBA,VanSteenK,FuhlbriggeAL,CeledonJC,RosnerBA,StrunkRC,ZeigerRS,WeissST;ChildhoodAsthmaManagementProgramResearchGroup.Inuterosmokeexposureandimpairedresponsetoinhaledcorticosteroidsinchildrenwithasthma.J Allergy Clin Immunol.2010Sep;126(3):491-7.
136.BurkeH,Leonardi-BeeJ,HashimA,Pine-AbataH,ChenY,
CookDG,BrittonJR,McKeeverTM.Prenatalandpassivesmokeexposureandincidenceofasthmaandwheeze:systematicreviewandmeta-analysis.Pediatrics.2012Apr;129(4):735-44.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

CHAPTER
2
DIAGNOSIS
AND
CLASSIFICATION
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

16 DIAGNOSIS AND CLASSIFICATION
KEY POINTS: • Aclinicaldiagnosisofasthmaisoftenprompted
bysymptomssuchasepisodicbreathlessness,wheezing,cough,andchesttightness.
• Measurementsoflungfunction(spirometryorpeakexpiratoryflow)provideanassessmentoftheseverityofairflowlimitation,itsreversibility,anditsvariability,andprovideconfirmationofthediagnosisofasthma.
• Measurementsofallergicstatuscanhelptoidentifyriskfactorsthatcauseasthmasymptomsinindividualpatients.
• Extrameasuresmayberequiredtodiagnoseasthmainchildren5yearsandyoungerandintheelderly,andoccupationalasthma.
• Forpatientswithsymptomsconsistentwithasthma,butnormallungfunction,measurementofairwayresponsivenessmayhelpestablishthediagnosis.
• Asthmahasbeenclassifiedbyseverityinpreviousreports.However,asthmaseveritymaychangeovertime,anddependsnotonlyontheseverityoftheunderlyingdiseasebutalsoitsresponsivenesstotreatment.
• Toaidinclinicalmanagement,aclassificationofasthmabylevelofcontrolisrecommended.
• Clinicalcontrolofasthmaisdefinedas:
-No(twiceorless/week)daytimesymptoms-Nolimitationsofdailyactivities,includingexercise-Nonocturnalsymptomsorawakeningbecauseofasthma-No(twiceorless/week)needforrelievertreatment-Normalornear-normallungfunction-No exacerbations
Acorrectdiagnosisofasthmaisessentialifappropriatedrugtherapyistobegiven.Asthmasymptomsmaybeintermittentandtheirsignificancemaybeoverlookedbypatientsandphysicians,or,becausetheyarenon-specific,theymayresultinmisdiagnosis(forexampleofwheezybronchitis,COPD,orthebreathlessnessofoldage).Thisisparticularlytrueamongchildren,wheremisdiagnosesincludevariousformsofbronchitisorcroup,andleadtoinappropriatetreatment.
Medical History
Symptoms.Aclinicaldiagnosisofasthmaisoftenpromptedbysymptomssuchasepisodicbreathlessness,wheezing,cough,andchesttightness1.Episodicsymptomsafteranincidentalallergenexposure,seasonalvariabilityofsymptomsandapositivefamilyhistoryofasthmaandatopicdiseasearealsohelpfuldiagnosticguides.Asthmaassociatedwithrhinitismayoccurintermittently,withthepatientbeingentirelyasymptomaticbetweenseasonsoritmayinvolveseasonalworseningofasthmasymptomsorabackgroundofpersistentasthma.Thepatternsofthesesymptomsthatstronglysuggestanasthmadiagnosisarevariability;precipitationbynon-specificirritants,suchassmoke,fumes,strongsmells,orexercise;worseningatnight;andrespondingtoappropriateasthmatherapy.Insomesensitizedindividuals,asthmamaybeexacerbatedbyseasonalincreasesinspecificaeroallergens2.ExamplesincludeAlternaria,andbirch,grass,andragweedpollens.
UsefulquestionstoconsiderwhenestablishingadiagnosisofasthmaaredescribedinFigure 2-1.
Cough-variant asthma.Patientswithcough-variantasthma3havechroniccoughastheirprincipal,ifnotonly,symptom.Itisparticularlycommoninchildren,andisoftenmoreproblematicatnight;evaluationsduringthedaycanbenormal.Forthesepatients,documentationofvariabilityinlungfunctionorofairwayhyperresponsiveness,andpossiblyasearchforsputumeosinophils,areparticularlyimportant4.Cough-variantasthmamustbedistinguishedfromso-calledeosinophilicbronchitisinwhichpatientshavecoughandsputumeoinophilsbutnormalindicesoflungfunctionwhenassessedbyspirometryandairwayhyperresponsiveness5.
Otherdiagnosestobeconsideredarecough-inducedbyangiotensin-converting-enzyme(ACE)inhibitors,gastroesophagealreflux,postnasaldrip,chronicsinusitis,and vocal cord dysfunction6.
INTRODUCTION
CLINICAL DIAGNOSIS
Figure 2-1. Questions to Consider in the Diagnosis of Asthma
• Has the patient had an attack or recurrent attacks of wheezing? • Does the patient have a troublesome cough at night? • Does the patient wheeze or cough after exercise? • Does the patient experience wheezing, chest tightness, or
cough after exposure to airborne allergens or pollutants? • Do the patient's colds “go to the chest” or take more than 10
days to clear up?• Are symptoms improved by appropriate asthma treatment?
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

DIAGNOSIS AND CLASSIFICATION 17
Exercise-induced bronchoconstriction.Physicalactivityisanimportantcauseofasthmasymptomsformostasthmapatients,andforsomeitistheonlycause.Exercise-inducedbronchoconstrictiontypicallydevelopswithin5-10minutesaftercompletingexercise(itrarelyoccursduringexercise).Patientsexperiencetypicalasthmasymptoms,orsometimesatroublesomecough,whichresolvespontaneouslywithin30-45minutes.Someformsofexercise,suchasrunning,aremorepotenttriggers7.Exercise-inducedbronchoconstrictionmayoccurinanyclimaticcondition,butitismorecommonwhenthepatientisbreathingdry,coldairandlesscommoninhot,humidclimates8.
Rapidimprovementofpost-exertionsymptomsafterinhaledβ2-agonistuse,ortheirpreventionbypretreatmentwithaninhaledβ2-agonistbeforeexercise,supportsadiagnosisofasthma.Somechildrenwithasthmapresentonlywithexercise-inducedsymptoms.Inthisgroup,orwhenthereisdoubtaboutthediagnosis,exercisetestingishelpful.An8-minuterunningprotocoliseasilyperformedinclinicalpracticeandcanestablishafirmdiagnosisofasthma9.
Physical Examination
Becauseasthmasymptomsarevariable,thephysicalexaminationoftherespiratorysystemmaybenormal.Themostusualabnormalphysicalfindingiswheezingonauscultation,afindingthatconfirmsthepresenceofairflowlimitation.However,insomepeoplewithasthma,wheezingmaybeabsentoronlydetectedwhenthepersonexhalesforcibly,eveninthepresenceofsignificantairflowlimitation.Occasionally,insevereasthmaexacerbations,wheezingmaybeabsentowingtoseverelyreducedairflowandventilation.However,patientsinthisstateusuallyhaveotherphysicalsignsreflectingtheexacerbationanditsseverity,suchascyanosis,drowsiness,difficultyspeaking,tachycardia,hyperinflatedchest,useofaccessorymuscles,andintercostalrecession.
Otherclinicalsignsareonlylikelytobepresentifpatientsareexaminedduringsymptomaticperiods.Featuresofhyperinflationresultfrompatientsbreathingatahigherlungvolumeinordertoincreaseoutwardretractionoftheairwaysandmaintainthepatencyofsmallerairways(whicharenarrowedbyacombinationofairwaysmoothmusclecontraction,edema,andmucushypersecretion).Thecombinationofhyperinflationandairflowlimitationinanasthmaexacerbationmarkedlyincreasestheworkofbreathing.
Tests for Diagnosis and Monitoring
Measurements of lung function.Thediagnosisofasthmaisusuallybasedonthepresenceofcharacteristicsymptoms.However,measurementsoflungfunction,andparticularlythedemonstrationofreversibilityoflungfunctionabnormalities,greatlyenhancediagnosticconfidence.Thisisbecausepatientswithasthmafrequentlyhavepoorrecognitionoftheirsymptomsandpoorperceptionofsymptomseverity,especiallyiftheirasthmaislong-standing10.Assessmentofsymptomssuchasdyspneaandwheezingbyphysiciansmayalsobeinaccurate.Measurementoflungfunctionprovidesanassessmentoftheseverityofairflowlimitation,itsreversibilityanditsvariability,andprovidesconfirmationofthediagnosisofasthma.Althoughmeasurementsoflungfunctiondonotcorrelatestronglywithsymptomsorothermeasuresofdiseasecontrolineitheradults11orchildren12, thesemeasuresprovidecomplementaryinformationaboutdifferentaspectsofasthmacontrol.
Variousmethodsareavailabletoassessairflowlimitation,buttwomethodshavegainedwidespreadacceptanceforuseinpatientsover5yearsofage.Thesearespirometry,particularlythemeasurementofforcedexpiratoryvolumein1second(FEV1)andforcedvitalcapacity(FVC),andpeakexpiratoryflow(PEF)measurement.
Predicted values of FEV1,FVC,andPEFbasedonage,sex,andheighthavebeenobtainedfrompopulationstudies.Thesearebeingcontinuallyrevised,andwiththeexceptionofPEFforwhichtherangeofpredictedvaluesistoowide,theyareusefulforjudgingwhetheragivenvalueisabnormalornot.Ifprecisionisneeded,forexample,intheconductofaclinicaltrial,useofamorerigorousdefinition(lowerlimitofnormal-LLN)shouldbeconsidered.
Thetermsreversibility and variabilityrefertochangesinsymptomsaccompaniedbychangesinairflowlimitationthatoccurspontaneouslyorinresponsetotreatment.ThetermreversibilityisgenerallyappliedtorapidimprovementsinFEV1(orPEF),measuredwithinminutesafterinhalationofarapid-actingbronchodilator—forexampleafter200-400ugsalbutamol(albuterol)13—ormoresustainedimprovementoverdaysorweeksaftertheintroductionofeffectivecontrollertreatmentsuchasinhaledglucocorticosteroids13.Variabilityreferstoimprovementordeteriorationinsymptomsandlungfunctionoccurringovertime.Variabilitymaybeexperiencedoverthecourseofoneday(whenitiscalleddiurnalvariability),fromdaytoday,frommonthtomonth,orseasonally.Obtainingahistoryofvariabilityisanessentialcomponentofthediagnosisofasthma.Inaddition,variabilityformspartoftheassessmentofasthmacontrol.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

18 DIAGNOSIS AND CLASSIFICATION
Spirometryistherecommendedmethodofmeasuringairflowlimitationandreversibilitytoestablishadiagnosisofasthma.MeasurementsofFEV1andFVCareundertakenduringaforcedexpiratorymaneuverusingaspirometer.Recommendationsforthestandardizationofspirometryhavebeenpublished13-15.ThedegreeofreversibilityinFEV1whichindicatesadiagnosisofasthmaisgenerallyacceptedas12%and200mlfromthepre-bronchodilatorvalue13.Howevermostasthmapatientswillnotexhibitreversibilityateachassessment,particularlythoseontreatment,andthetestthereforelackssensitivity.Repeatedtestingatdifferentvisitsisadvised.
Spirometryisreproducible,buteffort-dependent.Therefore,properinstructionsonhowtoperformtheforcedexpiratorymaneuvermustbegiventopatients,andthehighestvalueofthreerecordingstaken.Asethnicdifferencesinspirometricvalueshavebeendemonstrated,appropriatepredictiveequationsforFEV1andFVCshouldbeestablishedforeachpatient.Thenormalrangeofvaluesiswiderandpredictedvaluesarelessreliableinyoungpeople(<age20)andintheelderly(>age70).BecausemanylungdiseasesmayresultinreducedFEV1, a useful assessmentofairflowlimitationistheratioofFEV1toFVC.TheFEV1/FVCratioisnormallygreaterthan0.75to0.80,andpossiblygreaterthan0.90inchildren.Anyvalueslessthanthesesuggestairflowlimitation.
Peak expiratory flowmeasurementsaremadeusingapeakflowmeterandcanbeanimportantaidinbothdiagnosisandmonitoringofasthma.ModernPEFmetersarerelativelyinexpensive,portable,plastic,andidealforpatientstouseinhomesettingsforday-to-dayobjectivemeasurementofairflowlimitation.However,measurementsofPEFarenotinterchangeablewithothermeasurementsoflungfunctionsuchasFEV1ineitheradults
16orchildren17.PEFcanunderestimatethedegreeofairflowlimitation,particularlyasairflowlimitationandgastrappingworsen.BecausevaluesforPEFobtainedwithdifferentpeakflowmetersvaryandtherangeofpredictedvaluesistoowide,PEFmeasurementsshouldpreferablybecomparedtothepatient’sownpreviousbestmeasurements18usinghis/herownpeakflowmeter.Thepreviousbestmeasurementisusuallyobtainedwhenthepatientisasymptomaticoronfulltreatmentandservesasareferencevalueformonitoringtheeffectsofchangesintreatment.
Careful instruction is required to reliably measure PEF becausePEFmeasurementsareeffort-dependent.Mostcommonly,PEFismeasuredfirstthinginthemorningbeforetreatmentistaken,whenvaluesareoftenclosetotheirlowest,andlastthingatnightwhenvaluesareusuallyhigher.OnemethodofdescribingdiurnalPEFvariabilityisastheamplitude(thedifferencebetweenthemaximum
andtheminimumvaluefortheday),expressedasapercentageofthemeandailyPEFvalue,andaveragedover1-2weeks19.AnothermethodofdescribingPEFvariabilityistheminimummorningpre-bronchodilatorPEFover1week,expressedasapercentoftherecentbest(Min%Max)(Figure 2-2)19.ThislattermethodhasbeensuggestedtobethebestPEFindexofairwaylabilityforclinicalpracticebecauseitrequiresonlyaonce-dailyreading,correlatesbetterthananyotherindexwithairwayhyperresponsiveness,andinvolvesasimplecalculation.
PEFmonitoringisvaluableinasubsetofasthmaticpatientsandcanbehelpful:
• To confirm the diagnosis of asthma.Althoughspirometryisthepreferredmethodofdocumentingairflowlimitation,a60L/min(or20%ormoreofpre-bronchodilatorPEF)improvementafterinhalationofabronchodilator20, or diurnal variation in PEF of more than20%(withtwicedailyreadings,morethan10%21)suggestsadiagnosisofasthma.
• To improve control of asthma, particularly in patients with poor perception of symptoms10.Asthmamanagementplanswhichincludeself-monitoringofsymptomsorPEFfortreatmentofexacerbationshavebeenshowntoimproveasthmaoutcomes22.ItiseasiertodiscerntheresponsetotherapyfromaPEFchartthanfromaPEFdiary,providedthesamechartformat is consistently used23.
Weeks of Inhaled Glucocorticosteroid Treatment
PEF L/min
-1 0310/700= 44% 1 2 3 4 5 6 7 8 9 10
Inhaled glucocorticosteroidscommenced
500/710= 70% 620/720= 86%0100200300400500600700800
Weeks of Inhaled Glucocorticosteroid Treatment
PE
F L
/min
-1 0
310/700= 44%
1 2 3 4 5 6 7 8 9 10
Inhaled glucocorticosteroidscommenced
500/710= 70%
620/720= 86%
0
100
200
300
400
500
600
700
800
Figure 2-2. Measuring PEF Variability*
*PEF chart of a 27-year-old man with long-standing, poorly controlled asthma, beforeand after the start of inhaled glucocorticosteroid treatment. With treatment, PEFlevels increased, and PEF variability decreased, as seen by the increase in Min%Max(lowest morning PEF/highest PEF %) over 1 week.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

DIAGNOSIS AND CLASSIFICATION 19
• To identify environmental (including occupational) causes of asthma symptoms.ThisinvolvesthepatientmonitoringPEFdailyorseveraltimeseachdayoverperiodsofsuspectedexposuretoriskfactorsinthehomeorworkplace,orduringexerciseorotheractivitiesthatmaycausesymptoms,andduringperiodsofnon-exposure.
Measurement of airway responsiveness.Forpatientswithsymptomsconsistentwithasthma,butnormallungfunction,measurementsofairwayresponsivenesstodirectairwaychallengessuchasinhaledmethacholineandhistamineorindirectairwaychallengessuchasinhaledmannitol83 orexercisechallengemayhelpestablishadiagnosisofasthma24.Measurementsofairwayresponsivenessreflectthe“sensitivity”oftheairwaystofactorsthatcancauseasthmasymptoms,sometimescalled“triggers,”andthetestresultsareusuallyexpressedastheprovocativeconcentration(ordose)oftheagonistcausingagivenfall(often20%)inFEV1(Figure 2-3).Thesetestsaresensitiveforadiagnosisofasthma,buthavelimitedspecificity25.Thismeansthatanegativetestcanbeusefultoexcludeadiagnosisofpersistentasthmainapatientwhoisnottakinginhaledglucocorticosteroidtreatment,butapositivetestdoesnotalwaysmeanthatapatienthasasthma26.Thisisbecauseairwayhyperresponsivenesshasbeendescribedinpatientswithallergicrhinitis27andinthosewithairflowlimitationcausedbyconditionsotherthanasthma,suchascysticfibrosis28,bronchiectasis,andchronicobstructivepulmonarydisease(COPD)29.
Non-invasive markers of airway inflammation.Theevaluationofairwayinflammationassociatedwithasthmamaybeundertakenbyexaminingspontaneouslyproducedorhypertonicsaline-inducedsputumforeosinophilicorneutrophilicinflammation30.Inaddition,levelsofexhalednitricoxide(FeNO)31andcarbonmonoxide(FeCO)32 havebeensuggestedasnon-invasivemarkersofairwayinflammationinasthma.LevelsofFeNOareelevatedinpeoplewithasthma(whoarenottakinginhaledglucocorticosteroids)comparedtopeoplewithoutasthma,yetthesefindingsarenotspecificforasthma.NeithersputumeosinophilianorFeNOhavebeenevaluatedprospectivelyasanaidinasthmadiagnosis,butthesemeasurementsarebeingevaluatedforpotentialuseindeterminingoptimaltreatment33,34,56,althoughithasbeenshownthattheuseofFeNOasameasureofasthmacontroldoesnotimprovecontrolorenablereductionindoseofinhaledglucocorticosteroid55.
Measurements of allergic status.Becauseofthestrongassociationbetweenasthmaandallergicrhinitis,thepresenceofallergies,allergicdiseases,andallergicrhinitisinparticular,increasestheprobabilityofadiagnosisofasthmainpatientswithrespiratorysymptoms.Moreover,thepresenceofallergiesinasthmapatients(identifiedbyskintestingormeasurementofspecificIgEinserum)canhelptoidentifyriskfactorsthatcauseasthmasymptomsinindividualpatients.Deliberateprovocationoftheairwayswithasuspectedallergenorsensitizingagentmaybehelpfulintheoccupationalsetting,butisnotroutinelyrecommended,becauseitisrarelyusefulinestablishingadiagnosis,requiresconsiderableexpertiseandcanresultinlife-threateningbronchospasm35. Skintestswithallergensrepresenttheprimarydiagnostictoolindeterminingallergicstatus.Theyaresimpleandrapidtoperform,andhavealowcostandhighsensitivity.However,whenimproperlyperformed,skintestscanleadtofalselypositiveornegativeresults.MeasurementofspecificIgEinserumdoesnotsurpassthereliabilityofresultsfromskintestsandismoreexpensive.Themainlimitationofmethodstoassessallergicstatusisthatapositivetestdoesnotnecessarilymeanthatthediseaseisallergicinnatureorthatitiscausingasthma,assomeindividualshavespecificIgEantibodieswithoutanysymptomsanditmaynotbecausallyinvolved.Therelevantexposureanditsrelationtosymptomsmustbeconfirmedbypatienthistory.MeasurementoftotalIgEinserumhasnovalueasadiagnostictestforatopy.
Figure 2-3. Measuring Airway Responsiveness*
*Airway responsiveness to inhaled methacholine or histamine in a normal subject, andin asthmatics with mild, moderate, and severe airway hyperresponsiveness.Asthmatics have an increased sensitivity and an increased maximal broncho- constric-tor response to the agonist. The response to the agonist is usually expressed as theprovocative concentration causing a 20% decline in FEV1 (PC20).
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

20 DIAGNOSIS AND CLASSIFICATION
Thedifferentialdiagnosisinpatientswithsuspectedasthmadiffersamongdifferentagegroups:infants,children,youngadults,andtheelderly.
Children 5 years and Younger
Inearlylife,thepresenceofsensitizationtocommonallergens,atopy,isamajorriskfactorforsubsequentdevelopmentofasthma.Inaddition,atopyalsopredictsthatasthmamaybemoreseverewhenitdoesdevelop.
Thediagnosisofasthmainearlychildhoodischallengingandhastobebasedlargelyonclinicaljudgmentandanassessmentofsymptomsandphysicalfindings.Sincetheuseofthelabel“asthma”forwheezinginchildrenhasimportantclinicalconsequences,itmustbedistinguishedfromothercausespersistentandrecurrentwheeze.
Episodicwheezingandcoughisverycommoneveninchildrenwhodonothaveasthmaandparticularlyinthoseunderage336.Threecategoriesofwheezinghavebeendescribedinchildren5yearsandyounger:
• Transient early wheezing,whichisoftenoutgrowninthefirst3years.Thisisoftenassociatedwithprematurityandparentalsmoking.
• Persistent early-onset wheezing(beforeage3).Thesechildrentypicallyhaverecurrentepisodesofwheezingassociatedwithacuteviralrespiratoryinfections,havenoevidenceofatopy37and,unlikechildreninthenextcategoryoflateonsetwheezing/asthma,havenofamilyhistoryofatopy.Thesymptomsnormallypersistthroughschoolageandarestillpresentatage12inalargeproportionofchildren.Thecauseoftheepisodeisusuallytherespiratorysyncytialvirusinchildrenyoungerthanage2,whileothervirusespredominateinolderpreschoolchildren.
• Late-onset wheezing/asthma.Thesechildrenhaveasthmawhichoftenpersiststhroughoutchildhoodand into adult life38, 39.Theytypicallyhaveanatopicbackground,oftenwitheczema,andairwaypathologyischaracteristicofasthma.
Thefollowingcategoriesofsymptomsarehighlysuggestiveofadiagnosisofasthma:frequentepisodesofwheeze(morethanonceamonth),activity-inducedcoughorwheeze,nocturnalcoughinperiodswithoutviralinfections,
absenceofseasonalvariationinwheeze,andsymptomsthatpersistafterage3.Asimpleclinicalindexbasedonthepresenceofawheezebeforetheageof3,andthepresenceofonemajorriskfactor(parentalhistoryofasthmaoreczema)ortwoofthreeminorriskfactors(eosinophilia,wheezingwithoutcolds,andallergicrhinitis)hasbeenshowntopredictthepresenceofasthmainlaterchildhood38.However,treatingchildrenatriskwithinhaledglucocorticosteroidshasnotbeenshowntoaffectthedevelopmentofasthma40.
Alternativecausesofrecurrentwheezingmustbeconsideredandexcluded.Theseinclude:
• Chronicrhino-sinusitis• Gastroesophagealreflux• Recurrentvirallowerrespiratorytractinfections• Cysticfibrosis• Bronchopulmonarydysplasia• Tuberculosis • Congenitalmalformationcausingnarrowingofthe intrathoracicairways• Foreignbodyaspiration• Primaryciliarydyskinesiasyndrome• Immunedeficiency• Congenitalheartdisease
Neonatalonsetofsymptoms(associatedwithfailuretothrive),vomiting-associatedsymptoms,orfocallungorcardiovascularsignssuggestanalternativediagnosisandindicatetheneedforfurtherinvestigations.
Ausefulmethodforconfirmingthediagnosisofasthmainchildren5yearsandyoungerisatrialoftreatmentwithshort-actingbronchodilatorsandinhaledglucocorticosteroids.Markedclinicalimprovementduringthetreatmentanddeteriorationwhentreatmentisstoppedsupportsadiagnosisofasthma.Useofspirometryandothermeasuresrecommendedforolderchildrenandadultssuchasairwayresponsivenessandmarkersofairwayinflammationisdifficultandseveralrequirecomplexequipment41makingthemunsuitableforroutineuse.However,children4to5yearsoldcanbetaughttouseaPEFmeter,buttoensurereliabilityparentalsupervisionisrequired42.
Older Children and Adults
Acarefulhistoryandphysicalexamination,togetherwiththedemonstrationofreversibleandvariableairflowobstruction(preferablybyspirometry),willinmostinstancesconfirmthediagnosis.Thefollowingcategoriesofalternativediagnosesneedtobeconsidered:
DIAGNOSTIC CHALLENGES ANDDIFFERENTIAL DIAGNOSIS
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

DIAGNOSIS AND CLASSIFICATION 21
• Upperairwayobstructionandinhaledforeignbodies43 • Vocal cord dysfunction44 • Otherformsofobstructivelungdisease,particularly
COPD
• Non-obstructiveformsoflungdisease(e.g.,diffuseparenchymallungdisease)
• Non-respiratorycausesofsymptoms(e.g.,leftventricularfailure)
Becauseasthmaisacommondisease,itcanbefoundinassociationwithanyoftheabovediagnoses,whichcomplicatesthediagnosisaswellastheassessmentofseverityandcontrol.Thisisparticularlytruewhenasthmaisassociatedwithhyperventilation,vocalcorddysfunction,orCOPD.Carefulassessmentandtreatmentofboththeasthmaandthecomorbidityisoftennecessarytoestablishthecontributionofeachtoapatient’ssymptoms.
The Elderly
Undiagnosedasthmaisafrequentcauseoftreatablerespiratorysymptomsintheelderly,andthefrequentpresenceofcomorbiddiseasescomplicatesthediagnosis.Wheezing,breathlessness,andcoughcausedbyleftventricularfailureissometimeslabeled“cardiacasthma,”amisleadingterm,theuseofwhichisdiscouraged.Thepresenceofincreasedsymptomswithexerciseandatnightmayaddtothediagnosticconfusionbecausethesesymptomsareconsistentwitheitherasthmaorleftventricularfailure.Useofbeta-blockers,eventopically(forglaucoma)iscommoninthisagegroup.Acarefulhistoryandphysicalexamination,combinedwithanECGandchestX-ray,usuallyclarifiesthepicture.Intheelderly,distinguishingasthmafromCOPDisparticularlydifficult,andmayrequireatrialoftreatmentwithbronchodilatorsand/ororal/inhaledglucocorticosteroids.
Asthmatreatmentandassessmentandattainmentofcontrolintheelderlyarecomplicatedbyseveralfactors:poorperceptionofsymptoms,acceptanceofdyspneaasbeing“normal”inoldage,andreducedexpectationsofmobilityandactivity.
Occupational Asthma
Asthmaacquiredintheworkplaceisadiagnosisthatisfrequentlymissed.Becauseofitsinsidiousonset,occupationalasthmaisoftenmisdiagnosedaschronicbronchitisorCOPDandisthereforeeithernottreatedatallortreatedinappropriately.Thedevelopmentofnewsymptomsofrhinitis,cough,and/orwheezeparticularlyinnon-smokersshouldraisesuspicion.Detectionofasthmaofoccupationaloriginrequiresasystematicinquiryabout
workhistoryandexposures.Thediagnosisrequiresadefinedhistoryofoccupationalexposuretoknownorsuspectedsensitizingagents;anabsenceofasthmasymptomsbeforebeginningemployment;oradefiniteworseningofasthmaafteremployment.Arelationshipbetweensymptomsandtheworkplace(improvementinsymptomsawayfromworkandworseningofsymptomsonreturningtowork)canbehelpfulinestablishingalinkbetweensuspectedsensitizingagentsandasthma45.
Sincethemanagementofoccupationalasthmafrequentlyrequiresthepatienttochangehisorherjob,thediagnosiscarriesconsiderablesocioeconomicimplicationsanditisimportanttoconfirmthediagnosisobjectively.Thismaybeachievedbyspecificbronchialprovocationtesting46, althoughtherearefewcenterswiththenecessaryfacilitiesforspecificinhalationtesting.AnothermethodistomonitorPEFatleast4timesadayforaperiodof2weekswhenthepatientisworkingandforasimilarperiodawayfromwork47-50.Theincreasingrecognitionthatoccupationalasthmacanpersist,orcontinuetodeteriorate,evenintheabsenceofcontinuedexposuretotheoffendingagent51,emphasizestheneedforanearlydiagnosissothatappropriatestrictavoidanceoffurtherexposureandpharmacologicinterventionmaybeapplied.Publicationsprovideanevidence-basedapproachtotheidentificationofoccupationalasthmaandcomparespecificinhalationchallengetestingwithalternativetestsforconfirmingtheresponsibleagents52.
Distinguishing Asthma from COPD
BothasthmaandCOPDaremajorchronicobstructiveairwaysdiseasesthatinvolveunderlyingairwayinflammation.COPDischaracterizedbyairflowlimitationthatisnotfullyreversible,isusuallyprogressive,andisassociatedwithanabnormalinflammatoryresponseofthelungstonoxiousparticlesorgases.Individualswithasthmawhoareexposedtonoxiousagents(particularlycigarettesmoking)maydevelopfixedairflowlimitationandamixtureof“asthma-like”inflammationand“COPD-like”inflammation.Thus,eventhoughasthmacanusuallybedistinguishedfromCOPD,insomeindividualswhodevelopchronicrespiratorysymptomsandfixedairflowlimitation,itmaybedifficulttodifferentiatethetwodiseases.Asymptom-basedquestionnairefordifferentiatingCOPDandasthmaforusebyprimaryhealthcareprofessionalsisavailable53,54.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

22 DIAGNOSIS AND CLASSIFICATION
Etiology
Manyattemptshavebeenmadetoclassifyasthmaaccordingtoetiology,particularlywithregardtoenvironmentalsensitizingagents.However,suchaclassificationislimitedbytheexistenceofpatientsinwhomnoenvironmentalcausecanbeidentified.Despitethis,anefforttoidentifyanenvironmentalcauseforasthma(forexample,occupationalasthma)shouldbepartoftheinitialassessmenttoenabletheuseofavoidancestrategiesinasthmamanagement.Describingpatientsashavingallergicasthmaisusuallyoflittlebenefitinguidingtreatment,unlessasinglespecifictriggeragentcanbeidentified. Phenotype
Thereisincreasingawarenessofheterogeneityinthemanifestationsofasthmaandinitsresponsetotreatment.Thisisoftendescribedintermsof‘phenotypes’57,58,thecharacteristicswhichresultfromtheinteractionbetweenapatient’sgeneticmakeupandtheirenvironment.Several
differentclinicalphenotypesarerecognizedonthebasisofclusteranalysisofclinicalandotherfeaturesofasthma,e.g.aspirin-inducedasthma,exacerbation-proneasthmaandthesearchfordistinctivepathologicalormolecularfeaturesthatcouldexplaintheseclinicalpatternscontinues.Mostworkhasbeendoneoninflammatoryphenotypes,identifiedusingsputuminduction.Patientswitheosinophilicandnon-eosinophilicphenotypeshavebeenshowntodifferintheirclinicalresponsetoinhaledglucocorticosteroids59,60, andatagrouplevel,inflammatorymarkersmaybepredictiveofriskofexacerbationafterglucocorticosteroidreduction61.Inflammatoryphenotypesappeartobemoderatelystableovertime,althoughdataarelimited62,63.Atpresent,sincefewclinicianshaveaccesstoqualifiedsputumlaboratories,identificationoftheinflammatoryphenotypeismostlikelytobeusefulforpatientswithsevereasthmaorinthecontextofresearch.
Asthma Control
Asthmacontrolmaybedefinedinavarietyofways.Inlayterms,controlmayindicatediseaseprevention,orevencure.However,inasthma,whereneitherofthesearerealisticoptionsatpresent,itreferstocontrolofthemanifestationsofdisease.Theaimoftreatmentshouldbe
Figure 2-4. LEVELS OF ASTHMA CONTROL
A. Assessment of current clinical control (preferably over 4 weeks)
Characteristic Controlled (All of the following)
Partly Controlled(Any measure present)
Uncontrolled
Daytime symptoms None (twice or less/week)
More than twice/week Three or more features of partly controlled asthma*†
Limitation of activities None Any
Nocturnal symptoms/awakening
None Any
Need for reliever/ rescue treatment
None (twice or less/week)
More than twice/week
Lung function (PEF or FEV1)‡
Normal <80% predicted or personal best (if known)
B. Assessment of Future Risk (risk of exacerbations, instability, rapid decline in lung function, side-effects)
Features that are associated with increased risk of adverse events in the future include:Poor clinical control, frequent exacerbations in past year*, ever admission to critical care for asthma, low FEV1, exposure to cigarette smoke, high dose medications
* Any exacerbation should prompt review of maintenance treatment to ensure that it is adequate† By definition, an exacerbation in any week makes that an uncontrolled asthma week‡ Without administration of bronchodilator. Lung function is not a reliable test for children 5 years and younger
CLASSIFICATION OF ASTHMA
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

DIAGNOSIS AND CLASSIFICATION 23
toachieveandmaintaincontrolforprolongedperiods64withdueregardtothesafetyoftreatment,potentialforadverseeffects,andthecostoftreatmentrequiredtoachievethisgoal.Therefore,theassessmentofasthmacontrolshouldincludenotonlycontroloftheclinicalmanifestations(symptoms,nightwaking,relieveruse,activitylimitation,lungfunction),butalsocontroloftheexpectedfuturerisktothepatientsuchasexacerbations,accelerateddeclineinlungfunction,andside-effectsoftreatment.Ingeneral,theachievementofgoodclinicalcontrolofasthmaleadstoreducedriskofexacerbations65.However,certainpatientsmaycontinuetoexperienceexacerbationsinspiteofadequateintervalcontrol.Smokersarelesslikelytoachievecontrolandremainatriskofexacerbations66.Itshouldbenotedthatinhaledglucocorticosteroidsbothimproveclinicalcontrolandreducefuturerisk,butsomepharmacologicalagentsaremoreeffectiveinimprovingfeaturesofclinicalcontrol,whileothersarerelativelymoreeffectiveatreducingexacerbations.Thus,forsomepatientphenotypes,treatmentmaybeselectedtoaddressthepredominantproblem.
Figure 2-4describestheclinicalcharacteristicsofControlled, Partly Controlled and Uncontrolledasthma.Thisisaworkingschemebasedoncurrentopinionandhasnotbeenformallyvalidated.However,thisclassificationhasbeenshowntocorrelatewellwiththeAsthmaControlTest67 andwithassessmentofasthmacontrolaccordingtotheUSNationalExpertPanelReport3guidelines68,69.Inclinicalpractice,thisclassificationshouldbeusedinconjunctionwithanassessmentofthepatient’sclinicalconditionandthepotentialrisksandbenefitsofchangingtreatment. Severalstandardizedmeasuresforassessingclinicalcontrolofasthmahavebeendeveloped,whichscorethegoalsoftreatmentascontinuousvariablesandprovidenumericalvaluestodistinguishdifferentlevelsofcontrol.ExamplesofvalidatedinstrumentsaretheAsthmaControlQuestionnaire(ACQ)(www.qoltech.co.uk/Asthma1.htm)70, theAsthmaControlTest(ACT)(www.asthmacontrol.com)71,theChildhoodAsthmaControlTest(C-ACT)72, theAsthmaTherapyAssessmentQuestionnaire(ATAQ)(www.ataqinstrument.com)73,andtheAsthmaControlScoringSystem74.Fewoftheseinstrumentsincludeameasureoflungfunction.Theyarebeingpromotedforusenotonlyinresearchbutforpatientcareaswell,evenintheprimarycaresetting.Somearesuitableforself-assessmentofasthmacontrolbypatients75, and some areavailableinmanylanguages,ontheInternet,andinpaperformandmaybecompletedbypatientspriorto,orduring,consultationswiththeirhealthcareprovider.Theyhavethepotentialtoimprovetheassessmentofasthmacontrol,providingareproducibleobjectivemeasurethatmaybechartedovertime(weekbyweekormonthby
month)andrepresentinganimprovementincommunicationbetweenpatientandhealthcareprofessional.Theirvalueinclinicaluse,asdistinctfromresearchsettings,hasyettobedemonstratedbutwilllikelybecomeevidentincomingyears.Allofthesetoolsaresubjecttocopyrightrestrictions,andsomehavefeesassociatedwiththeiruseinresearch.
Thereisconsiderableinterestincontrollingnotonlytheclinicalmanifestationsofasthma,butalsotheinflammatoryandpatho-physiologicalfeaturesofthedisease.Thereisevidencethatreducinginflammationwithcontrollertherapyachievesgoodclinicalcontrolandreducestheriskofexacerbations.Inaddition,inflammatoryandpatho-physiologicalmarkersmaybepredictorsoffutureriskofexacerbationsanddeclineinlungfunction,independentofthepatient’slevelofclinicalcontrol66,76.Biomarker-guidedtreatmentappears,primarily,tobeofvalueinasthmaphenotypesinwhichthereisdissociationbetweenmeasuresofclinicalcontrolandairwayinflammation.Forexample,treatmentbasedontheproportionofeosinophilsinsputumhasresultedinareductionofexacerbationsorminimizationofdosesofinhaledglucocorticosteroidsinpatientswithuncontrolledasthmainspiteofmoderatelevels of treatment77,78.
However,inprimarycare,becauseofthecostand/orunavailabilityoftestssuchasendobronchialbiopsyandmeasurementofsputumeosinophilsandexhalednitricoxide30-34,thecurrentrecommendationisthattreatmentshouldbeaimedatcontrollingtheclinicalfeaturesofdisease,includinglungfunctionabnormalities.
Asthma Severity
Forpatientsnotreceivinginhaledglucocorticosteroidtreatment,previousGINAdocumentssubdividedasthmabyseveritybasedonthelevelofsymptoms,airflowlimitation,andlungfunctionvariabilityintofourcategories:Intermittent, Mild Persistent, Moderate Persistent, or SeverePersistent,althoughthisclassificationwasoftenerroneouslyappliedtopatientsalreadyontreatment79.Acopyofthisclassificationsystemisarchivedatwww.ginasthma.org.Itisimportanttorecognize,however,thatasthmaseverityinvolvesboththeseverityoftheunderlyingdiseaseanditsresponsivenesstotreatment80.Thus,asthmacouldpresentwithseveresymptomsandairflowobstruction,butbecomecompletelycontrolledwithlow-dosetreatment.Inaddition,severityisnotastaticfeatureofanindividualpatient’sasthma,butmaychangeovermonthsoryears.Themainlimitationofthispreviousmethodofclassificationofasthmaseveritywasitspoorvalueinpredictingwhattreatmentwouldberequiredandwhatapatient’sresponsetothattreatmentmightbe.Forthisreason,anassessmentofasthmacontrolatinitial
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

24 DIAGNOSIS AND CLASSIFICATION
presentationandperiodicallyduringtreatmentismorerelevant and useful81.
Inviewoftheselimitations,asthmaseverityisnowbyconsensusclassifiedonthebasisoftheintensityoftreatmentrequiredtoachievegoodasthmacontrol79,80.Mildasthmaisasthmathatcanbewell-controlledwithlowintensitytreatmentsuchaslow-doseinhaledglucocorticosteroids,leukotrienemodifiersorcromones.Severeasthmaisasthmathatrequireshighintensitytreatment,e.g.GINAStep4,tomaintaingoodcontrol,orwheregoodcontrolisnotachieveddespitehighintensity treatment82.Itisrecognizedthatdifferentasthmaphenotypesmayhavedifferentlevelsofresponsivenesstoconventionaltreatment.Asphenotype-specifictreatmentbecomesavailable,asthmapreviouslyconsideredtobeseverecouldbecomemild.
Terminologyaroundasthmaseverityisconfusingbecause“severity”isalsousedtodescribethemagnitudeofairwayobstructionortheintensityofsymptoms.Patientswilloftenperceivetheirasthmaassevereiftheyhaveintenseorfrequentsymptoms,butitisimportanttoconveythatthismaymerelyrepresentinadequatetreatment.Becausetheterms“control”and“severity”areusedinothercontextsinlaylanguage,itisimportantthathealthprofessionalscommunicateclearlyhowthewordsareusedinthecontextofasthma.
REFERENCES
1. LevyML,FletcherM,PriceDB,HausenT,HalbertRJ,YawnBP.InternationalPrimaryCareRespiratoryGroup(IPCRG)Guidelines:diagnosisofrespiratorydiseasesinprimarycare.Prim Care Respir J2006;15(1):20-34.
2. YsselH,AbbalC,PeneJ,BousquetJ.TheroleofIgEinasthma.Clin Exp Allergy1998;28Suppl5:104-9.
3. CorraoWM,BramanSS,IrwinRS.Chroniccoughasthesolepresentingmanifestationofbronchialasthma.N Engl J Med 1979;300(12):633-7.
4. GibsonPG,FujimuraM,NiimiA.Eosinophilicbronchitis:clinicalmanifestationsandimplicationsfortreatment.Thorax 2002;57(2):178-82.
5. GibsonPG,DolovichJ,DenburgJ,RamsdaleEH,HargreaveFE.Chroniccough:eosinophilicbronchitiswithoutasthma.Lancet1989;1(8651):1346-8.
6. Irwin RS, Boulet LP, Cloutier MM, Fuller R, Gold PM, Hoffstein V, et al.Managingcoughasadefensemechanismandasasymptom.AconsensuspanelreportoftheAmericanCollegeofChestPhysicians.Chest1998;114(2SupplManaging):133S-81S.
7. RandolphC.Exercise-inducedasthma:updateonpathophysiology,clinicaldiagnosis,andtreatment.Curr Probl Pediatr1997;27(2):53-77.
8. TanWC,TanCH,TeohPC.Theroleofclimaticconditionsandhistaminereleaseinexercise-inducedbronchoconstriction.Ann Acad Med Singapore1985;14(3):465-9.
9. AndersonSD.Exercise-inducedasthmainchildren:amarkerofairwayinflammation.Med J Aust2002;177Suppl:S61-3.
10. KillianKJ,WatsonR,OtisJ,StAmandTA,O’ByrnePM.Symptomperceptionduringacutebronchoconstriction.Am J Respir Crit Care Med2000;162(2Pt1):490-6.
11. KerstjensHA,BrandPL,deJongPM,KoeterGH,PostmaDS.Influenceoftreatmentonpeakexpiratoryflowanditsrelationtoairwayhyperresponsivenessandsymptoms.TheDutchCNSLDStudyGroup.Thorax1994;49(11):1109-15.
12. BrandPL,DuivermanEJ,WaalkensHJ,vanEssen-ZandvlietEE,KerrebijnKF.Peakflowvariationinchildhoodasthma:correlationwithsymptoms,airwaysobstruction,andhyperresponsivenessduringlong-termtreatmentwithinhaledcorticosteroids.DutchCNSLDStudyGroup.Thorax 1999;54(2):103-7.
13. PellegrinoR,ViegiG,BrusascoV,CrapoRO,BurgosF,Casaburi R, et al.Interpretativestrategiesforlungfunctiontests.Eur Respir J2005;26(5):948-68.
14. StandardizationofSpirometry,1994Update.AmericanThoracicSociety.Am J Respir Crit Care Med1995;152(3):1107-36.
15. Standardizedlungfunctiontesting.OfficialstatementoftheEuropeanRespiratorySociety.Eur Respir J Suppl 1993;16:1-100.
16. SawyerG,MilesJ,LewisS,FitzharrisP,PearceN,BeasleyR.Classificationofasthmaseverity:shouldtheinternationalguidelinesbechanged?Clin Exp Allergy1998;28(12):1565-70.
17. EidN,YandellB,HowellL,EddyM,SheikhS.Canpeakexpiratoryflowpredictairflowobstructioninchildrenwithasthma?Pediatrics2000;105(2):354-8.
18. ReddelHK,MarksGB,JenkinsCR.Whencanpersonalbestpeakflowbedeterminedforasthmaactionplans?Thorax 2004;59(11):922-4.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

DIAGNOSIS AND CLASSIFICATION 25
19. ReddelHK,SalomeCM,PeatJK,WoolcockAJ.Whichindexofpeakexpiratoryflowismostusefulinthemanagementofstableasthma?Am J Respir Crit Care Med1995;151(5):1320-5.
20. DekkerFW,SchrierAC,SterkPJ,DijkmanJH.Validityofpeakexpiratoryflowmeasurementinassessingreversibilityofairflowobstruction.Thorax1992;47(3):162-6.
21. BoezenHM,SchoutenJP,PostmaDS,RijckenB.Distributionofpeakexpiratoryflowvariabilitybyage,genderandsmokinghabitsinarandompopulationsampleaged20-70yrs.Eur Respir J1994;7(10):1814-20.
22. GibsonPG,PowellH.Writtenactionplansforasthma:anevidence-basedreviewofthekeycomponents.Thorax 2004;59(2):94-9.
23. ReddelHK,VincentSD,CiviticoJ.Theneedforstandardisationofpeakflowcharts.Thorax2005;60(2):164-7.
24. CockcroftDW.Directchallengetests:Airwayhyperresponsivenessinasthma:itsmeasurementandclinicalsignificance.Chest. 2010Aug;138(2Suppl):18S-24S.
25. CockcroftDW,MurdockKY,BerscheidBA,GoreBP.SensitivityandspecificityofhistaminePC20determinationinarandomselectionofyoungcollegestudents.J Allergy Clin Immunol 1992;89(1Pt1):23-30.
26. BouletLP.Asymptomaticairwayhyperresponsiveness:acuriosityoranopportunitytopreventasthma?Am J Respir Crit Care Med2003;167(3):371-8.
27. RamsdaleEH,MorrisMM,RobertsRS,HargreaveFE.Asymptomaticbronchialhyperresponsivenessinrhinitis.J Allergy Clin Immunol1985;75(5):573-7.
28. vanHarenEH,LammersJW,FestenJ,HeijermanHG,GrootCA,vanHerwaardenCL.Theeffectsoftheinhaledcorticosteroidbudesonideonlungfunctionandbronchialhyperresponsivenessinadultpatientswithcysticfibrosis.Respir Med1995;89(3):209-14.
29. RamsdaleEH,MorrisMM,RobertsRS,HargreaveFE.Bronchialresponsivenesstomethacholineinchronicbronchitis:relationshiptoairflowobstructionandcoldairresponsiveness.Thorax1984;39(12):912-8.
30. PizichiniMM,PopovTA,EfthimiadisA,HussackP,EvansS,PizichiniE,et al.Spontaneousandinducedsputumtomeasureindicesofairwayinflammationinasthma.Am J Respir Crit Care Med1996;154(4Pt1):866-9.
31. KharitonovS,AlvingK,BarnesPJ.Exhaledandnasalnitricoxidemeasurements:recommendations.TheEuropeanRespiratorySocietyTaskForce.Eur Respir J1997;10(7):1683-93.
32. HorvathI,HuntJ,BarnesPJ,AlvingK,AntcakA,BaraldiE, et al.Exhaledbreathcondensate:methodologicalrecommendationsandunresolvedquestions.Eur Respir J 2005;26:523-48.
33. GreenRH,BrightlingCE,McKennaS,HargadonB,ParkerD,BraddingP,et al.Asthmaexacerbationsandsputumeosinophilcounts:arandomisedcontrolledtrial.Lancet 2002;360(9347):1715-21.
34. SmithAD,CowanJO,BrassettKP,HerbisonGP,TaylorDR.Useofexhalednitricoxidemeasurementstoguidetreatmentinchronicasthma.N Engl J Med2005;352(21):2163-73.
35. HoeppnerVH,MurdockKY,KoonerS,CockcroftDW.Severeacute“occupationalasthma!causedbyaccidentalallergenexposureinanallergenchallengelaboratory.Ann Allergy 1985;55:36-7.
36. WilsonNM.Wheezybronchitisrevisited.Arch Dis Child 1989;64(8):1194-9.
37. MartinezFD.Respiratorysyncytialvirusbronchiolitisandthepathogenesisofchildhoodasthma.Pediatr Infect Dis J2003;22(2Suppl):S76-82.
38. Castro-RodriguezJA,HolbergCJ,WrightAL,MartinezFD.Aclinicalindextodefineriskofasthmainyoungchildrenwithrecurrentwheezing.Am J Respir Crit Care Med2000;162(4Pt1):1403-6.
39. SearsMR,GreeneJM,WillanAR,WiecekEM,TaylorDR,Flannery EM, et al.Alongitudinal,population-based,cohortstudyofchildhoodasthmafollowedtoadulthood.N Engl J Med 2003;349(15):1414-22.
40. GuilbertTW,MorganWJ,ZeigerRS,MaugerDT,BoehmerSJ,SzeflerSJ,et al.Long-terminhaledcorticosteroidsinpreschoolchildrenathighriskforasthma.N Engl J Med 2006;354(19):1985-97.
41. FreyU,StocksJ,SlyP,BatesJ.Specificationforsignalprocessinganddatahandlingusedforinfantpulmonaryfunctiontesting.ERS/ATSTaskForceonStandardsforInfantRespiratoryFunctionTesting.EuropeanRespiratorySociety/AmericanThoracicSociety.Eur Respir J2000;16(5):1016-22.
42. SlyPD,CahillP,WilletK,BurtonP.Accuracyofminipeakflowmetersinindicatingchangesinlungfunctioninchildrenwithasthma.BMJ1994;308(6928):572-4.
43. MokQ,PiesowicAT.Foreignbodyaspirationmimickingasthma.Intensive Care Med1993;19(4):240-1.
44. PlaceR,MorrisonA,ArceE.Vocalcorddysfunction.J Adolesc Health2000;27(2):125-9.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

26 DIAGNOSIS AND CLASSIFICATION
45. TarloSM,LissGM.Occupationalasthma:anapproachtodiagnosisandmanagement.CMAJ2003;168(7):867-71.
46. TarloSM.Laboratorychallengetestingforoccupationalasthma.J Allergy Clin Immunol2003;111(4):692-4.
47. Chan-YeungM,DesjardinsA.Bronchialhyperresponsivenessandlevelofexposureinoccupationalasthmaduetowesternredcedar(Thujaplicata).Serialobservationsbeforeandafterdevelopmentofsymptoms.Am Rev Respir Dis 1992;146(6):1606-9.
48. CoteJ,KennedyS,Chan-YeungM.SensitivityandspecificityofPC20andpeakexpiratoryflowrateincedarasthma.J Allergy Clin Immunol1990;85(3):592-8.
49. VandenplasO,MaloJL.Inhalationchallengeswithagentscausingoccupationalasthma.Eur Respir J1997;10(11):2612-29.
50. BrightP,BurgePS.Occupationallungdisease.8.Thediagnosisofoccupationalasthmafromserialmeasurementsoflungfunctionatandawayfromwork.Thorax1996;51(8):857-63.
51. Chan-YeungM,MacLeanL,PaggiaroPL.Follow-upstudyof232patientswithoccupationalasthmacausedbywesternredcedar(Thujaplicata).J Allergy Clin Immunol1987;79(5):792-6.
52. NicholsonPJ,CullinanP,TaylorAJ,BurgePS,BoyleC.Evidencebasedguidelinesfortheprevention,identification,andmanagementofoccupationalasthma.Occup Environ Med 2005;62(5):290-9.
53. PriceDB,TinkelmanDG,HalbertRJ,NordykeRJ,IsonakaS,NonikovD,et al.Symptom-basedquestionnaireforidentifyingCOPDinsmokers.Respiration2006;73(3):285-95.
54. TinkelmanDG,PriceDB,NordykeRJ,HalbertRJ,IsonakaS,NonikovD,et al.Symptom-basedquestionnairefordifferentiatingCOPDandasthma.Respiration2006;73(3):296-305.
55. SzeflerSJ,MitchellH,SorknessCA,GergenPJ,O’ConnorGT,MorganWJ,et al.Managementofasthmabasedonexhalednitricoxideinadditiontoguideline-basedtreatmentforinner-cityadolescentsandyoungadults:arandomisedcontrolledtrial.Lancet.2008Sep20;372(9643):1065-72.
56. ShawDE,BerryMA,ThomasM,GreenRH,BrightlingCE,WardlawAJ,PavordID.Theuseofexhalednitricoxidetoguideasthmamanagement:arandomizedcontrolledtrial.Am J Respir Crit Care Med2007;176:231-7.
57. BelEH.Clinicalphenotypesofasthma. Curr Opin Pulm Med 2004;10:44-50.
58. WenzelSE.Asthma:definingofthepersistentadultphenotypes.Lancet2006;368:804-13.
59. BerryM,MorganA,ShawDE,ParkerD,GreenR,BrightlingC,BraddingP,WardlawAJ,PavordID.Pathologicalfeaturesandinhaledcorticosteroidresponseofeosinophilicandnon-eosinophilicasthma.Thorax2007;62:1043-9.
60. PavordID,BrightlingCE,WoltmannG,WardlawAJ.Non-eosinophiliccorticosteroidunresponsiveasthma.Lancet 1999;353:2213-4.
61. JatakanonA,LimS,BarnesPJ.Changesinsputumeosinophilspredictlossofasthmacontrol.Am J Respir Crit Care Med 2000;161:64-72.
62. SimpsonJL,ScottR,BoyleMJ,GibsonPG.Inflammatorysubtypesinasthma:assessmentandidentificationusinginducedsputum. Respirology2006;11:54-61.
63. vanVeenIH,TenBrinkeA,GauwSA,SterkPJ,RabeKF,BelEH.Consistencyofsputumeosinophiliaindifficult-to-treatasthma:a5-yearfollow-upstudy.J Allergy Clin Immunol 2009;124:615-7,617e1-2.
64. BatemanED,BousheyHA,BousquetJ,BusseWW,ClarkTJ,PauwelsRA,PedersenSE.Canguideline-definedasthmacontrolbeachieved?TheGainingOptimalAsthmaControLstudy.Am J Respir Crit Care Med2004;170:836-44.
65. BatemanED,BousquetJ,KeechML,BusseWW,ClarkTJ,PedersenSE.Thecorrelationbetweenasthmacontrolandhealthstatus:theGOALstudy.Eur Respir J2007;29:56-62.
66. OsborneML,PedulaKL,O’HollarenM,EttingerKM,StiboltT,BuistAS,VollmerWM.Assessingfutureneedforacutecareinadultasthmatics:theProfileofAsthmaRiskStudy:aprospectivehealthmaintenanceorganization-basedstudy.Chest2007;132:1151-61.
67. ThomasM,KayS,PikeJ,WilliamsA,RosenweigJR,HillyerEV,PriceD.TheAsthmaControlTest(ACT)asapredictorofGINAguideline-definedasthmacontrol:analysisofamultinationalcross-sectionalsurvey.Prim Care Respir J 2009;18:41-9.
68. NationalHeart,Lung,andBloodInstitute.NationalAsthmaEducationandPreventionProgram.ExpertPanelReport3:GuidelinesfortheDiagnosisandManagementofAsthma.August2007.Availablefrom: www.nhlbi.nih.gov/guidelines/asthma/asthgdln
69. KhaliliB,BoggsPB,ShiR,BahnaSL.Discrepancybetweenclinicalasthmacontrolassessmenttoolsandfractionalexhalednitricoxide.Ann Allergy Asthma Immunol2008;101:124-9.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

DIAGNOSIS AND CLASSIFICATION 27
70. JuniperEF,O’ByrnePM,GuyattGH,FerriePJ,KingDR.Developmentandvalidationofaquestionnairetomeasureasthmacontrol.Eur Respir J1999;14:902-7.
71. NathanRA,SorknessCA,KosinskiM,SchatM,LiJT,MarcusP,MurrayJJ,PendergraftTB.Developmentoftheasthmacontroltest:asurveyforassessingasthmacontrol.J Allergy Clin Immunol2004;113:59-65.
72. LiuAH,ZeigerR,SorknessC,MahrT,OstromN,BurgessS,RosenzweigJC,ManjunathR.Developmentandcross-sectionalvalidationoftheChildhoodAsthmaControlTest.J Allergy Clin Immunol2007;119:817-25.
73. VollmerWM,MarksonLE,O’ConnorE,SanockiLL,FittermanL,BergerM,BuistAS.Associationofasthmacontrolwithhealthcareutilizationandqualityoflife.Am J Respir Crit Care Med 1999;160:1647-52.
74. BouletLP,BouletV,MilotJ.Howshouldwequantifyasthmacontrol?Aproposal.Chest2002;122:2217-23.
75. SchatzM,MosenDM,KosinskiM,VollmerWM,MagidDJ,O’ConnorE,ZeigerRS.ValidityoftheAsthmaControlTestcompletedathome.Am J Manag Care2007;13:661-7.
76. vanRensenEL,SontJK,EvertseCE,WillemsLN,MauadT,HiemstraPS,SterkPJ.BronchialCD8cellinfiltrateandlungfunctiondeclineinasthma.Am J Respir Crit Care Med 2005;172:837-41.
77. HaldarP,PavordID,ShawDE,BerryMA,ThomasM,BrightlingCE,WardlawAJ,GreenRH.Clusteranalysisandclinicalasthmaphenotypes.Am J Respir Crit Care Med2008;178:218-24.
78. JayaramL,PizichiniMM,CookRJ,BouletLP,LemiereC,PizichiniE,CartierA,HussackP,GoldsmithCH,LavioletteM,ParameswaranK,HargreaveFE.Determiningasthmatreatmentbymonitoringsputumcellcounts:effectonexacerbations.Eur Respir J2006;27:483-94.
79. TaylorDR,BatemanED,BouletLP,BousheyHA,BusseWW,CasaleTB,ChaneP,EnrightPL,GibsonPG,deJongsteJC,KerstjensHA,LazarusSC,LevyML,O’ByrnePM,PartridgeMR,PavordID,SearsMR,SterkPJ,StoloffSW,SzeflerSJ,SullivanSD,ThomasMD,WenzelSE,ReddelHK.Anewperspectiveonconceptsofasthmaseverityandcontrol.Eur Respir J2008;32:545-54.
80. CockcroftDW,SwystunVA.Asthmacontrolversusasthmaseverity.J Allergy Clin Immunol1996;98:1016-8.
81. ChenH,GouldMK,BlancPD,MillerDP,KamathTV,LeeJH,SullivanSD.Asthmacontrol,severity,andqualityoflife:quantifyingtheeffectofuncontrolleddisease.J Allergy Clin Immunol2007;120:396-402.
82. ProceedingsoftheATSworkshoponrefractoryasthma:currentunderstanding,recommendations,andunansweredquestions.AmericanThoracicSociety.Am J Respir Crit Care Med 2000;162:2341-51.
83. AndersonSD.Indirectchallengetests:Airwayhyperresponsivenessinasthma:itsmeasurementandclinicalsignificance.Chest 2010;138:25S-30S.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

28 DIAGNOSIS AND CLASSIFICATIONCOPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

CHAPTER
3
ASTHMA
TREATMENTS
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

30 ASTHMA TREATMENTS
KEY POINTS:
• Medicationstotreatasthmacanbeclassifiedascontrollersorrelievers.Controllersaremedicationstakendailyonalong-termbasistokeepasthmaunderclinicalcontrolchieflythroughtheiranti-inflammatoryeffects.Relieversaremedicationsusedonanas-neededbasisthatactquicklytoreversebronchoconstrictionandrelieveitssymptoms.
• Asthmatreatmentcanbeadministeredindifferentways—inhaled,orally,orbyinjection.Themajoradvantageofinhaledtherapyisthatdrugsaredelivereddirectlyintotheairways,producinghigherlocalconcentrationswithsignificantlylessriskofsystemicsideeffects.
• Inhaledglucocorticosteroidsarethemosteffectivecontrollermedicationscurrentlyavailable.
• Rapid-actinginhaledβ2-agonistsarethemedicationsofchoiceforreliefofbronchoconstrictionandforthepretreatmentofexercise-inducedbronchoconstriction,inbothadultsandchildrenofallages.
• Increaseduse,especiallydailyuse,ofrelievermedicationisawarningofdeteriorationofasthmacontrolandindicatestheneedtoreassesstreatment.
Thegoalofasthmatreatmentistoachieveandmaintainclinicalcontrol.Medicationstotreatasthmacanbeclassifiedascontrollersorrelievers.Controllers are medicationstakendailyonalong-termbasistokeepasthmaunderclinicalcontrolchieflythroughtheiranti-inflammatoryeffects.Theyincludeinhaledandsystemicglucocorticosteroids,leukotrienemodifiers,long-actinginhaledβ2-agonistsincombinationwithinhaledglucocorticosteroids,sustained-releasetheophylline,cromones,andanti-IgE.Inhaledglucocorticosteroidsarethemosteffectivecontrollermedicationscurrentlyavailable.Relievers are medications used on an as-needed basisthatactquicklytoreversebronchoconstrictionandrelieveitssymptoms.Theyincluderapid-actinginhaledβ2-agonists,inhaledanticholinergics,short-actingtheophylline,andshort-actingoralβ2-agonists.
Route of Administration
Asthmatreatmentforadultscanbeadministeredindifferentways—inhaled,orallyorparenterally(bysubcutaneous,intramuscular,orintravenousinjection).Themajoradvantageofinhaledtherapyisthatdrugsaredelivereddirectlyintotheairways,producinghigherlocalconcentrationswithsignificantlylessriskofsystemicsideeffects.
Inhaledmedicationsforasthmaareavailableaspressurizedmetered-doseinhalers(MDIs),breath-actuatedMDIs,drypowderinhalers(DPIs),softmistinhalers,andnebulizedor“wet”aerosols*.Inhalerdevicesdifferintheirefficiencyofdrugdeliverytothelowerrespiratorytract,dependingontheformofthedevice,formulationofmedication,particlesize,velocityoftheaerosolcloudorplume(whereapplicable),andeasewithwhichthedevicecanbeusedbythemajorityofpatients.Individualpatientpreference,convenience,andeaseofusemayinfluencenotonlytheefficiencyofdrugdeliverybutalsopatientadherencetotreatmentandlong-termcontrol.
PressurizedMDIs(pMDIs)requiretrainingandskilltocoordinateactivationoftheinhalerandinhalation.Medicationsinthesedevicescanbedispensedasasuspensioninchlorofluorocarbons(CFCs)orasasolutioninhydrofluoroalkanes(HFAs).ForapMDIcontainingCFCs,theuseofaspacer(holdingchamber)improvesdrugdelivery,increaseslungdeposition,andmayreducelocal and systemic side effects1.However,CFCinhalerdevicesarebeingphasedoutduetotheimpactofCFCsupontheatmosphericozonelayer,andarebeingreplacedbyHFAdevices.ForpMDIscontainingbronchodilators,theswitchfromCFCtoHFAinhalersdoesnotresultinachangeinefficacyatthesamenominaldose2.However,forsomeglucocorticosteroids,theHFAformulationsprovideanaerosolofsmallerparticlesizethatresultsinlessoraldeposition(withassociatedreductioninoralsideeffects),andcorrespondinglygreaterlungdeposition3-5.Cliniciansareadvisedtoconsultthepackageinsertsofeachproducttoconfirmtherecommendeddoseequivalenttocurrentlyuseddrugs.SomeofthesecomparisonsareprovidedinFigure 3-1.
INTRODUCTION
ASTHMA MEDICATIONS: ADULTS
*InformationonvariousinhalerdevicesavailablecanbefoundontheGINAWebsite(http://www.ginasthma.org).
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA TREATMENTS 31
PressurizedMDIsmaybeusedbypatientswithasthmaofanyseverity,includingduringexacerbations.Breath-actuatedaerosolsmaybehelpfulforpatientswhohavedifficultyusingthe“pressandbreathe”pressurizedMDI6.Softmistinhalersappeartorequirelesscoordination.Drypowderinhalersaregenerallyeasiertouse,buttheyrequireaminimalinspiratoryflowrateandmayprovedifficultforsomepatients.DPIsdifferwithrespecttothefractionofex-actuatordosedeliveredtothelung.Forsomedrugs,thedosemayneedtobeadjustedwhenswitchingfrom an MDI6 to a DIP7.Nebulizedaerosolsarerarelyindicatedforthetreatmentofchronicasthmainadults8.
Inhaled glucocorticosteroids*
Role in therapy-Inhaledglucocorticosteroidsarecurrentlythemosteffectiveanti-inflammatorymedicationsforthetreatmentofpersistentasthma.Studieshavedemonstratedtheirefficacyinreducingasthmasymptoms9,improvingquality of life9,improvinglungfunction9,decreasingairwayhyperresponsiveness10,controllingairwayinflammation11, reducingfrequencyandseverityofexacerbations12, and reducingasthmamortality13.However,theydonotcureasthma,andwhentheyarediscontinueddeterioration
ofclinicalcontrolfollowswithinweekstomonthsinaproportionofpatients14,15.
Inhaledglucocorticosteroidsdifferinpotencyandbioavailability,butbecauseofrelativelyflatdose-responserelationshipsinasthmarelativelyfewstudieshavebeenabletoconfirmtheclinicalrelevanceofthesedifferences191.Figure 3-1listsapproximatelyequipotentdosesofdifferentinhaledglucocorticosteroidsbasedupontheavailableefficacyliterature,butthecategorizationintodosagecategoriesdoesnotimplythatcleardose-responserelationshipshavebeendemonstratedforeachdrug.Theefficacyofsomeproductsvarieswhenadministeredviadifferentinhalerdevices16.Mostofthebenefitfrominhaledglucocorticosteroidsisachievedinadultsatrelativelylowdoses,equivalentto400ugofbudesonideperday17.Increasingtohigherdosesprovideslittlefurtherbenefitintermsofasthmacontrolbutincreasestheriskof side effects17,18.However,thereismarkedindividualvariabilityofresponsivenesstoinhaledglucocorticosteroidsandbecauseofthisandtherecognizedpooradherencetotreatmentwithinhaledglucocorticosteroids,manypatientswillrequirehigherdosestoachievefulltherapeuticbenefit.Astobaccosmokingreducestheresponsivenesstoinhaledglucocorticosteroids,higherdosesmayberequiredinpatientswhosmoke240.
CONTROLLER MEDICATIONS
Figure 3-1. Estimated Equipotent Daily Doses of Inhaled Glucocorticosteriods for Adults†
Drug Low Daily Dose (µg) Medium Daily Dose (µg) High Daily Dose (µg)‡
Beclomethasone dipropionate - CFC 200-500 >500-1000 >1000-2000Beclomethasone dipropionate - HFA 100 - 250 >250 - 500 >500 - 1000
Budesonide* 200-400 >400-800 >800-1600Ciclesonide* 80-160 >160-320 >320-1280Flunisolide 500-1000 >1000-2000 >2000
Fluticasone propionate 100-250 >250-500 >500-1000Mometasone furoate* 200 ≥400 ≥800
Triamcinolone acetonide 400-1000 >1000-2000 >2000†Comparisons based on efficacy data‡Patients considered for high daily doses except for short periods should be referred to a specialist for assessment to consider alternative combinations of controllers. Maximum recommended doses are arbitrary but with prolonged use are associated with increased risk of systemic side effects.*Approved for once-daily dosing in mild patients
NOTES:• The most important determinant of approprioate dosing is the clinician’s judgement of the patient’s response therapy. The clinician must monitor the patient’s response in terms
of clinical control and adjust the dose accordingly. Once control of asthma is achieved, the dose of medication should carefully be titrated to the minimum dose required to maintain control, thus reducing the potential for adverse effects.
• Designation of low, medium, and high doses is provided from manufacturers’ recommendations where possible. Clear demonstration of dose-response relationships is seldom provided or available. The principle is therefore to establish the minimum effective controlling dose in each patient, as higher doses may not be more effective and are likely to be associated with greater potential for adverse effects
• As CFC preparations are taken from the market, medication inserts for HFA preparations should be carefully reviewed by the clinician for the equivalent correct dosage.
*In this section recommendations for doses of inhaled glococorticosteriods are given as “µ/day budesonide or equivalent,” because a majority of the clinical literature on these medications uses this standard
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

32 ASTHMA TREATMENTS
Toreachclinicalcontrol,add-ontherapywithanotherclassofcontrollerispreferredoverincreasingthedoseofinhaledglucocorticosteroids211.Thereis,however,aclearrelationshipbetweenthedoseofinhaledglucocorticosteroidsandthepreventionofsevereacuteexacerbationsofasthma12,althoughthereappeartobedifferencesinresponseaccordingtosymptom/inflammationphenotype212.Therefore,somepatientswithsevereasthmamaybenefitfromlong-termtreatmentwithhigherdosesofinhaledglucocorticosteroids. Side effects:Localadverseeffectsfrominhaledglucocorticosteroidsincludeoropharyngealcandidiasis,dysphonia,andoccasionallycoughingfromupperairwayirritation.ForpressurizedMDIstheprevalenceoftheseeffectsmaybereducedbyusingcertainspacerdevices1.Mouthwashing(rinsingwithwater,gargling,andspittingout)afterinhalationmayreduceoralcandidiasis.Theuseofprodrugsthatareactivatedinthelungsbutnotinthepharynx(e.g.,ciclesonide19andbeclometasone),andnewformulationsanddevicesthatreduceoropharyngealdeposition,mayminimizesucheffectswithouttheneedforaspacerormouthwashing.
Inhaledglucocorticosteroidsareabsorbedfromthelung,accountingforsomedegreeofsystemicbioavailability.Theriskofsystemicadverseeffectsfromaninhaledglucocorticosteroiddependsuponitsdoseandpotency,thedeliverysystem,systemicbioavailability,first-passmetabolism(conversiontoinactivemetabolites)intheliver,andhalf-lifeofthefractionofsystemicallyabsorbeddrug(fromthelungandpossiblygut)20.Therefore,thesystemiceffectsdifferamongthevariousinhaledglucocorticosteroids.Severalcomparativestudieshavedemonstratedthatciclesonide,budesonide,andfluticasonepropionateatequipotentdoseshavelesssystemic effect20-23.Currentevidencesuggeststhatinadults,systemiceffectsofinhaledglucocorticosteroidsarenotaproblematdosesof400µgorlessbudesonideorequivalentdaily.
Thesystemicsideeffectsoflong-termtreatmentwithhighdosesofinhaledglucocorticosteroidsincludeeasybruising24,adrenalsuppression1,20, and decreased bone mineral density25,26.Ameta-analysisofcase-controlstudiesofnon-vertebralfracturesinadultsusinginhaledglucocorticosteroids(BDPorequivalent)indicatedthatinolderadults,therelativeriskofnon-vertebralfracturesincreasesbyabout12%foreach1000µg/dayincreaseinthedoseBDPorequivalentbutthatthemagnitudeofthisriskwasconsiderablylessthanothercommonriskfactorsforfractureintheolderadult213.Inhaledglucocorticosteroidshavealsobeenassociatedwithcataracts27,29andglaucomain cross-sectional studies28,butthereisnoevidenceofposterior-subcapsularcataractsinprospectivestudies30-32.
Onedifficultyinestablishingtheclinicalsignificanceofsuchadverseeffectsliesindissociatingtheeffectofhigh-doseinhaledglucocorticosteroidsfromtheeffectofcoursesoforalglucocorticosteroidstakenbypatientswithsevereasthma.Thereisnoevidencethatuseofinhaledglucocorticosteroidsincreasestheriskofpulmonaryinfections,includingtuberculosis,andinhaledglucocorticosteroidsarenotcontraindicatedinpatientswithactive tuberculosis33.
Leukotriene modifiers.
Role in therapy-Leukotrienemodifiersincludecysteinyl-leukotriene1(CysLT1)receptorantagonists(montelukast,pranlukast,andzafirlukast)anda5-lipoxygenaseinhibitor(zileuton).Clinicalstudieshavedemonstratedthatleukotrienemodifiershaveasmallandvariablebronchodilatoreffect,reducesymptomsincludingcough34, improvelungfunction,andreduceairwayinflammationandasthmaexacerbations35-37.Theymaybeusedasanalternativetreatmentforadultpatientswithmildpersistentasthma38-40,andsomepatientswithaspirin-sensitiveasthmarespondwelltoleukotrienemodifiers41.However,whenusedaloneascontroller,theeffectofleukotrienemodifiersaregenerallylessthanthatoflowdosesofinhaledglucocorticosteroids,and,inpatientsalreadyoninhaledglucocorticosteroids,leukotrienemodifierscannotsubstituteforthistreatmentwithoutriskingthelossofasthmacontrol42,43.
Leukotrienemodifiersusedasadd-ontherapymayreducethedoseofinhaledglucocorticosteroidsrequiredbypatientswithmoderatetosevereasthma44, and mayimproveasthmacontrolinpatientswhoseasthmaisnotcontrolledwithloworhighdosesofinhaledglucocorticosteroids43,45-47.Withtheexceptionofonestudythatdemonstratedequivalenceinpreventingexacerbations48,severalstudieshavedemonstratedthatleukotrienemodifiersarelesseffectivethanlong-actinginhaledβ2-agonistsasadd-ontherapy
49-51,192.Acontrolledreleaseformulationofzileutonallowsthismedicationtobeusedonatwicedailybasiswitheffectsequivalenttothatofstandardzileutonusedfourtimesaday203.
Side effects-Leukotrienemodifiersarewelltolerated,andfewifanyclass-relatedeffectshavesofarbeenrecognized.Zileutonhasbeenassociatedwithlivertoxicity204,andmonitoringoflivertestsisrecommendedduringtreatmentwiththismedication.NoassociationwasfoundbetweenChurg-Strausssyndromeandleukotrienemodifiersaftercontrollingforasthmadruguse,althoughitisnotpossibletoruleoutmodestassociationsgiventhatChurg-Strausssyndromeissorareandsohighlycorrelatedwithasthmaseverity52.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA TREATMENTS 33
Long-acting inhaled bronchodilators
Role in therapy -Long-actinginhaledβ2-agonists,includingformoterolandsalmeterol,shouldnotbeusedasmonotherapyinasthmaasthesemedicationsdonotappeartoinfluenceairwayinflammationinasthma.Theyaremosteffectivewhencombinedwithinhaledglucocorticosteroids55,56,193,andthiscombinationtherapyisthepreferredtreatmentwhenamediumdoseofinhaledglucocorticosteroidalonefailstoachievecontrolofasthma.Theadditionoflong-actinginhaledβ2-agoniststoadailyregimenofinhaledglucocorticosteroidsimprovessymptomscores,decreasesnocturnalasthmasymptoms,improveslungfunction,decreasestheuseofrapid-actinginhaledβ2-agonists
57-59,reducesthenumberof exacerbations12,57-62,doesnotincreasetheriskofasthma-relatedhospitalizations214,andachievesclinicalcontrolofasthmainmorepatients,morerapidly,andatalowerdoseofinhaledglucocorticosteroidsthaninhaledglucocorticosteroidsgivenalone63.
Thisgreaterefficacyofcombinationtreatmenthasledtothedevelopmentoffixedcombinationinhalersthatdeliverbothglucocorticosteroidandlong-actingβ2-agonistsimultaneously(fluticasonepropionateplussalmeterol,budesonideplusformoterol,mometasoneplusformoterol,beclometasoneplusformoterol).Controlledstudieshaveshownthatdeliveringthistherapyinacombinationinhalerisaseffectiveasgivingeachdrugseparately64,65.Fixedcombinationinhalersaremoreconvenientforpatients,mayincreasecompliance66,andensurethatthelong-actingβ2-agonistisalwaysaccompaniedbyaglucocorticosteroid.Inaddition,combinationinhalerscontainingformoterolandbudesonidemaybeusedforbothrescueandmaintenance.Bothcomponentsofbudesonide-formoterolgivenasneededcontributetoenhancedprotectionfromsevereexacerbationsinpatientsreceivingcombinationtherapyformaintenance67,194andprovideimprovementsinasthmacontrolatrelativelylowdosesofinhaledglucocorticosteroids67-70.(SeeAppendixB,GINAPocketGuideupdated2009forinformationonAsthmaCombinationMedicationsForAdultsandChildren5YearsandOlder.)
Long-actingβ2-agonistswhenusedasacombinationmedicationwithinhaledglucocorticosteroidsmayalsobeusedtopreventexercise-inducedbronchospasm,andforthispurposemayprovidelongerprotectionthanrapid-actinginhaledβ2-agonists
71.Salmeterolandformoterolprovideasimilardurationofbronchodilationandprotectionagainstbronchoconstrictors,buttherearepharmacologicaldifferencesbetweenthem.Formoterolhasamorerapidonsetofactionthansalmeterol72, 73,whichmaymakeformoterolsuitableforsymptomreliefaswellassymptomprevention68.
Tiotropium,along-actinginhaledanticholinergicbronchodilator,hasbeenstudiedinadultswithuncontrolledasthmaandcomparedwithsalmeterol,doublingthedoseofinhaledglucocorticosteroidandasadd-ontoinhaledglucocorticosteroidsandsalmeterol231,233.Onestudyshowedcomparablebronchodilatoreffectswithnosignificantchangesonasthmacontrol232.Anotherstudyshowedthataddingtiotropiumtopatientsnotcontrolledoninhaledglucocorticosteroidsandlong-actingβ2-agonistsimprovedlungfunctionbutnotsymptoms233.Thestudieshavebeenrelativelyshort-termandnoeffectonexacerbationshassofarbeenreported.Therearenodataaboutthesemedicationsinchildren.
Side effects-Therapywithlong-actinginhaledβ2-agonistscausesfewersystemicadverseeffects—suchascardiovascularstimulation,skeletalmuscletremor,andhypokalemia—thanoraltherapy.Theregularuseofrapid-actingβ2-agonistsinbothshortandlongactingformsmaylead to relative refractoriness to β2-agonists
74.Basedondataindicatingapossibleincreasedriskofasthma-relateddeathassociatedwiththeuseofsalmeterolinasmallgroupofindividuals75long-actingβ2-agonistsshouldnotbeusedasasubstituteforinhaledororalglucocorticosteroids,andshouldonlybeusedincombinationwithanappropriatedoseofinhaledglucocorticosteroidasdeterminedbyaphysician215,234.Somemeta-analysesofstudiesoflong-actingβ2-agonistshaveshownnumericallyverysmallincreasesinthenumberofdeathsinpatientsreceivinglong-actingβ2-agonistsincombinationwithinhaledglucocorticosteroids,whencomparedtoinhaledglucocorticosteroidsalone.Wherepresent,theeffectsizesareextremelysmallandneedtobebalancedagainstthebenefitsinimprovedasthmacontrolandreductioninexacerbationsthatthesemedicationsbringwhencombinedwithinhaledglucocorticosteroids205,214.Noinfluenceofβ2-adrenergicreceptorphenotypesupontheefficacyorsafetyoflong-actingβ2-agonisttherapyhasbeenobservedwhenadministeredincombinationwithinhaledglucocorticosteroidswhetherbythesingleinhalerformaintenanceandreliefmethodorataregularfixeddoseinadults206,220.
Theophylline
Role in therapy-Theophyllineisabronchodilatorand,whengiveninalowerdose,hasmodestanti-inflammatoryproperties77-79.Itisavailableinsustained-releaseformulationsthataresuitableforonce-ortwice-dailyInaddition,combinationinhalerscontainingformoterolanddosing.Dataontherelativeefficacyoftheophyllineasalong-termcontrollerislacking.However,availableevidencesuggeststhatithaslittleeffectasafirst-linecontroller80.Itmayusedasadd-ontherapyinpatientswhodonotachievecontroloninhaledglucocorticosteroidsalone81-83.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

34 ASTHMA TREATMENTS
Additionallyinsuchpatientsthewithdrawalofsustained-releasetheophyllinehasbeenassociatedwithdeteriorationof control84.Asadd-ontherapy,theophyllineislesseffectivethanlong-actinginhaledβ2-agonists
85,86.
Side effects-Sideeffectsoftheophylline,particularlyathigherdoses(10mg/kgbodyweight/dayormore),aresignificantandreducetheirusefulness.Sideeffectscanbereducedbycarefuldoseselectionandmonitoring,andgenerallydecreaseordisappearwithcontinueduse.Adverseeffectsincludegastrointestinalsymptoms,loosestools,cardiacarrhythmias,seizures,andevendeath.Nauseaandvomitingarethemostcommonearlyevents.Monitoringisadvisedwhenahighdoseisstarted,ifthepatientdevelopsanadverseeffectontheusualdose,whenexpectedtherapeuticaimsarenotachieved,andwhenconditionsknowntoaltertheophyllinemetabolismexist.Forexample,febrileillness,pregnancy,andanti-tuberculosismedications87reducebloodlevelsoftheophylline,whileliverdisease,congestiveheartfailure,andcertaindrugsincludingcimetidine,somequinolones,andsomemacrolidesincreasetheriskoftoxicity.Lowerdosesoftheophylline,whichhavebeendemonstratedtoprovidethefullanti-inflammatorybenefitofthisdrug82, are associated withlessfrequentsideeffects,andplasmatheophyllinelevelsinpatientsonlow-dosetherapyneednotbemeasuredunlessoverdoseissuspected.
Cromones: sodium cromoglycate and nedocromil sodium.
Role in therapy–Theroleofsodiumcromoglycateandnedocromilsodiuminlong-termtreatmentofasthmainadultsislimited.Efficacyhasbeenreportedinpatientswithmildpersistentasthmaandexercise-inducedbronchospasm.Theiranti-inflammatoryeffectisweakandtheyarelesseffectivethanalowdoseofinhaledglucocorticosteroid88.
Side effects -Side effects are uncommon and include coughinguponinhalationandsorethroat.Somepatientsfindthetasteofnedocromilsodiumunpleasant.
Long-acting oral β2-agonists.
Role in therapy -Longactingoralβ2-agonistsincludeslow release formulations of salbutamol, terbutaline, and bambuterol,aprodrugthatisconvertedtoterbutalineinthebody.Theyareusedonlyonrareoccasionswhenadditionalbronchodilationisneeded.
Side effects-Thesideeffectprofileoflong-actingoralβ2-agonistsishigherthanthatofinhaledβ2-agonists,andincludescardiovascularstimulation(tachycardia),anxiety,
andskeletalmuscletremor.Adversecardiovascularreactionsmayalsooccurwiththecombinationoforalβ2-agonistsandtheophylline.Regularuseoflong-actingoralβ2-agonistsasmonotherapyislikelytobeharmfulandthesemedicationsmustalwaysbegivenincombinationwithinhaledglucocorticosteroids.
Anti-IgE*
Role in therapy-Anti-IgE(omalizumab)isatreatmentoptionlimitedtopatientswithelevatedserumlevelsofIgE.Itscurrentindicationisforpatientswithsevereallergicasthma89whoareuncontrolledoninhaledglucocorticosteroids,althoughthedoseofconcurrenttreatmenthasvariedindifferentstudies.Improvedasthmacontrolisreflectedbyfewersymptoms,lessneedfor reliever medications, and fewer exacerbations90,91, althoughthiswasnotconfirmedinallstudies235.Furtherinvestigationswilllikelyprovideadditionalclarificationoftheroleofanti-IgEinotherclinicalsettings.
Side effects:Asindicatedbyseveralstudiesinvolvingasthmapatientsages12yearsandolder207,whowerealreadyreceivingtreatmentwithglucocorticosteroids(inhaledand/ororal)andlong-actingβ2-agonists
89, anti-IgEappearstobesafeasadd-ontherapy92-94,includingpatientsgenerallyconsideredtobeathighriskforexacerbations229 .Withdrawalofglucocorticosteroidsfacilitatedbyanti-IgEtherapyhasledtounmaskingthepresenceofChurg-Strausssyndromeinasmallnumberofpatients221.Clinicianssuccessfulininitiatingglucocorticosteroidwithdrawalusinganti-IgEshouldbeawareofthissideeffect.
Systemic glucocorticosteroids.
Role in therapy-Long-termoralglucocorticosteroidtherapy(thatis,forperiodslongerthantwoweeksasaglucocorticosteroid“burst”)mayberequiredforseverelyuncontrolledasthma,butitsuseislimitedbytheriskofsignificantadverseeffects.Thetherapeuticindex(effect/sideeffect)oflong-terminhaledglucocortico-steroidsisalwaysmorefavorablethanlong-termsystemicglucocorticosteroidsinasthma95,96.Iforalglucocorticosteroidshavetobeadministeredonalong-termbasis,attentionmustbepaidtomeasuresthatminimiethesystemicsideeffects.Oralpreparationsarepreferredoverparenteral(intramuscularorintravenous)forlong-termtherapybecauseoftheirlowermineralocorticoideffect,relativelyshorthalf-life,andlessereffectsonstriatedmuscle,aswellasthegreaterflexibilityofdosingthatpermitstitrationtothelowestacceptabledosethatmaintainscontrol.
*Visit GINA website, www.ginasthma.org for GRADE review of question “In adults with asthma, does monoclonal anti-IgE, omalizumab, compared to placebo improve patient outcomes?”
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA TREATMENTS 35
Side effects-Thesystemicsideeffectsoflong-termoralorparenteralglucocorticosteroidtreatmentincludeosteoporosis,arterialhypertension,diabetes,hypothalamic-pituitary-adrenalaxissuppression,obesity,cataracts,glaucoma,skinthinningleadingtocutaneousstriaeandeasybruising,andmuscleweakness.Patientswithasthmawhoareonlong-termsystemicglucocorticosteroidsinanyformshouldreceivepreventivetreatmentforosteoporosis(Figure 3-2)97-99.Althoughitisrare,withdrawaloforalglucocorticosteroidscanelicitadrenalfailureorunmaskunderlyingdisease,suchasChurg-StraussSyndrome100.Cautionandclosemedicalsupervisionarerecommendedwhenconsideringtheuseofsystemicglucocorticosteroidsinpatientswithasthmawhoalsohavetuberculosis,parasiticinfections,osteoporosis,glaucoma,diabetes,severedepression,orpepticulcers.Fatalherpesvirus
infectionshavebeenreportedamongpatientswhoareexposedtotheseviruseswhiletakingsystemicglucocorticosteroids,evenshortbursts.
Oral anti-allergic compounds.
Role in therapy-Severaloralanti-allergiccompoundshavebeenintroducedinsomecountriesforthetreatmentofmildtomoderateallergicasthma.Theseincludetranilast,repirinast,tazanolast,pemirolast,ozagrel,seratrodast,amlexanox,andibudilast.Ingeneral,theiranti-asthmaeffectappearstobelimited101,butstudiesontherelativeefficacyofthesecompoundsareneededbeforerecommendationscanbemadeabouttheirroleinthelong-termtreatmentofasthma.
Figure 3-2. Glucocorticosteroids and Osteoporosis
Asthma patients on high-dose inhaled glucocorticosteroids or oral glucocorticosteroids at any dose are considered at risk of developingosteoporosis and fractures, but it is not certain whether this risk exists for patients on lower doses of inhaled glucocorticosteroids1. Physiciansshould consider monitoring patients who are at risk. The following summarizes monitoring and management but more detailed guidelines forthe management of steroid-induced osteoporosis are available2,3.
Screening - Chest X-rays should be reviewed for the presence of vertebral fractures. Wedging, compressions, and cod-fishing of vertebralbodies are synonymous with fractures, and indicate those who are at the highest risk for future fractures. In men, this may be a better predictorof fracture risk than bone mineral density (BMD). BMD measurements by dual energy X-ray absorptiomety (DXA scan) should be undertaken in:
• Any patient with asthma who has been taking oral glucocorticosteroids for over 6 months duration at a mean daily dose of 7.5 mgprednisone/prednisolone or above.
• Post-menopausal women taking over 5 mg prednisone/prednisolone daily for more than 3 months. • Any patient with asthma and a history of vertebral or other fractures that may be related to osteoporosis.
Bone density measurements should also be offered to:• Post-menopausal women taking > 2 mg inhaled BDP or equivalent daily• Any patient who is receiving frequent short courses of high-dose oral glucocorticosteroids
Osteoporosis is present if the bone density in lumbar spine or femoral neck shows :• T-score below -2.5 (2.5 standard deviations below the mean value of young normal subjects of the same sex in patients 19-69 years).• Z-score below -1 (1 standard deviation below the predicted value for age and sex).
follow-up scanning - Repeat scanning should be done:• In 2 years in those whose initial scan was not osteoporotic but in whom treatment (as above) with oral glucocorticosteroids continues.• In 1 year for those with osteoporosis on the first scan who are started on osteoporosis treatment.
Management• General measures include avoidance of smoking, regular exercise, use of the lowest dose of oral glucocorticosteroid possible, and a good
dietary intake of calcium.• For women with osteoporosis up to 10 years post-menopausal offer bisphosphonates or hormone therapy4,5,6 (Evidence A).• For men, pre-menopausal women, and women more than 10 years since menopause consider treatment with a bisphosphonate7 (Evidence A).
References1. Goldstein MF, Fallon JJ, Jr., Harning R. Chronic glucocorticoid therapy-induced osteoporosis in patients with obstructive lung disease. Chest 1999; 116:1733-1749.2. Eastell R, Reid DM, Compston J, Cooper C, Fogelman I, Francis RM et al. A UK Consensus Group on management of glucocorticoid-induced osteoporosis:
an update. J Intern Med 1998; 244:271-292.3. Sambrook PN, Diamond T, Ferris L, Fiatarone-Singh M, Flicker L, MacLennan A et al. Corticosteroid induced osteoporosis. Guidelines for treatment. Aust Fam
Physician 2001; 30:793-796.4. Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML et al. Risks and benefits of estrogen plus progestin in healthy
postmenopausal women: principal results From the Women's Health Initiative randomized controlled trial. JAMA. 2002;288:321-33.5. Cauley JA, Robbins J, Chen Z, Cummings SR, Jackson RD, LaCroix AZ, LeBoff M, Lewis CE, McGowan J, Neuner J, Pettinger M, Stefanick ML, Wactawski-
Wende J, Watts NB. "Effects of Estrogen Plus Progestin on Risk of Fracture and Bone Mineral Density." JAMA 2003;290(13):1729-1738. 6. Brown JP, Josse RG. 2002 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada. CMAJ. 2002;167:S1-34.7. Homik J, Cranney A, Shea B, Tugwell P, Wells G, Adachi R et al. Bisphosphonates for steroid induced osteoporosis. Cochrane Database Syst Rev 2000;CD001347.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

36 ASTHMA TREATMENTS
Side effects-Sedationisapotentialsideeffectofsomeofthesemedications.
Other controller therapies.
Role in therapy-Varioustherapeuticregimenstoreducethedoseoforalglucocorticosteroidsrequiredbypatientswithsevereasthmahavebeenproposed.Thesemedicationsshouldbeusedonlyinselectedpatientsunderthesupervisionofanasthmaspecialist,astheirpotentialsteroid-sparingeffectsmaynotoutweightheriskofserioussideeffects.Twometa-analysesofthesteroid-sparingeffectoflow-dosemethotrexateshowedasmalloverallbenefit,butarelativelyhighfrequencyofadverseeffects102,103.Thissmallpotentialtoreducetheimpactofglucocorticosteroidsideeffectsisprobablyinsufficienttooffsettheadverseeffectsofmethotrexate104.Cyclosporin105 andgold106,107havealsobeenshowntobeeffectiveinsomepatients.Themacrolide,troleandomycin,hasasmallsteroid-sparingeffectwhenusedwithsystemicmethylprednisolone,butitseffectmayresultfromthemacrolidedecreasingmetabolismoftheglucocorticosteroidandthereforenotimprovingsafety.However,othereffectsofthelong-termuseofmacrolidesinasthmaremainunderstudy108.Theuseofintravenousimmunoglobulinisnotrecommended109-111.Dataonahumanmonoclonalantibodyagainsttumornecrosisfactor(TNF)-alphasuggestthattheriskbenefitequationdoesnotfavortheuseofthisclassoftreatmentsinsevereasthma216.
Side effects-Macrolideuseisfrequentlyassociatedwithnausea,vomiting,andabdominalpainandoccasionallylivertoxicity.Methotrexatealsocausesgastrointestinalsymptoms,andonrareoccasionshepaticanddiffusepulmonaryparenchymaldisease,andhematologicalandteratogeniceffects.
Allergen-specific immunotherapy.
Role in therapy-Theroleofspecificimmunotherapyinadultasthmaislimited.Appropriateimmunotherapyrequirestheidentificationanduseofasinglewell-definedclinicallyrelevantallergen.Thelaterisadministeredinprogressivelyhigherdosesinordertoinducetolerance.ACochranereview112thatexamined75randomizedcontrolledtrialsofspecificimmunotherapycomparedtoplaceboconfirmedtheefficacyofthistherapyinasthmainreducingsymptomscoresandmedicationrequirements,andimprovingallergen-specificandnon-specificairwayhyperresponsiveness.Similarmodesteffectswereidentifiedinasystematicreviewofsublingualimmunotherapy(SLIT)196.Specificimmunotherapyhaslong-termclinicaleffectsandthepotentialofpreventingdevelopmentofasthmainchildrenwithallergicrhino
conjunctivitisupto7yearsaftertreatmenttermination208.However,inviewoftherelativelymodesteffectofallergen-specificimmunotherapycomparedtoothertreatmentoptions,thesebenefitsmustbeweighedagainsttheriskofadverseeffectsandtheinconvenienceoftheprolongedcourseofinjectiontherapy,includingtheminimumhalf-hourwaitrequiredaftereachinjection.Specificimmunotherapyshouldbeconsideredonlyafterstrictenvironmentalavoidanceandpharmacologicintervention,includinginhaledglucocorticosteroids,havefailedtocontrolapatient’sasthma113.Therearenostudiesthatcomparespecificimmunotherapywithpharmacologictherapyforasthma.Thevalueofimmunotherapyusingmultipleallergensdoesnothavesupport.Side effects -Local and systemic side effects may occur in conjunctionwithspecificimmunotherapyadministration.Reactionslocalizedtotheinjectionsitemayrangefromaminimalimmediatewhealandflaretoalarge,painful,delayedallergicresponse.Systemiceffectsmayincludeanaphylacticreactions,whichmaybelifethreatening,aswellassevereexacerbationsofasthma.Deathsfromspecificimmunotherapyhaveoccurredinpatientswithsevereasthma.
Reliever Medications
Relievermedicationsactquicklytorelievebronchoconstrictionanditsaccompanyingacutesymptoms. Rapid-acting inhaled β2-agonists.
Role in therapy -Rapid-actinginhaledβ2-agonistsarethemedicationsofchoiceforreliefofbronchospasmduringacuteexacerbationsofasthmaandforthepretreatmentofexercise-inducedbronchoconstriction.Theyincludesalbutamol, terbutaline, fenoterol, levalbuterol HFA209, reproterol,andpirbuterol.Formoterol,along-actingβ2-agonist,isapprovedforsymptomreliefbecauseofitsrapidonsetofaction,butitshouldonlybeusedforthispurposeinpatientsonregularcontrollertherapywithinhaledglucocorticosteroids230.
Rapid-actinginhaledβ2-agonistsshouldbeusedonlyonanas-neededbasisatthelowestdoseandfrequencyrequired.Increaseduse,especiallydailyuse,isawarningofdeteriorationofasthmacontrolandindicatestheneedtoreassesstreatment.Similarly,failuretoachieveaquickandsustainedresponsetoβ2-agonisttreatmentduringanexacerbationmandatesmedicalattention,andmayindicatetheneedforshort-termtreatmentwithoralglucocorticosteroids.
Side effects -Use of oral β2-agonistsgiveninstandarddosesareassociatedwithmoreadversesystemiceffects
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA TREATMENTS 37
suchastremorandtachycardiathanoccurwithinhaledpreparations.
Systemic glucocorticosteroids.
Role in therapy-Althoughsystemicglucocorticosteroidsarenotusuallythoughtofasrelievermedications,theyareimportantinthetreatmentofsevereacuteexacerbationsbecausetheypreventprogressionoftheasthmaexacerbation,reducetheneedforreferraltoemergencydepartmentsandhospitalization,preventearlyrelapseafteremergencytreatment,andreducethemorbidityoftheillness.Themaineffectsofsystemicglucocorticosteroidsinacuteasthmaareonlyevidentafter4to6hours.Oraltherapyispreferredandisaseffectiveasintravenoushydrocortisone114.Atypicalshortcourseoforalglucocorticosterodsforanexacerbationis40-50mg115 prednisolonegivendailyfor5to10daysdependingontheseverityoftheexacerbation.Whensymptomshavesubsidedandlungfunctionhasapproachedthepatient’spersonalbestvalue,theoralglucocorticosteroidscanbestoppedortapered,providedthattreatmentwithinhaledglucocorticosteroidscontinues116.Intramuscularinjectionofglucocorticosteroidshasnoadvantageoverashortcourseoforalglucocorticosteroidsinpreventingrelapse114,116.
Side effects-Adverseeffectsofshort-termhigh-dosesystemictherapyareuncommonbutincludereversibleabnormalitiesinglucosemetabolism,increasedappetite,fluidretention,weightgain,roundingoftheface,moodalteration,hypertension,pepticulcer,andasepticnecrosisofthefemur.
Anticholinergics.
Role in therapy-Anticholinergicbronchodilatorsusedinasthmaincludeipratropiumbromideandoxitropiumbromide.Inhaledipratropiumbromideisalesseffectiverelievermedicationinasthmathanrapid-actinginhaledβ2-agonists.Ameta-analysisoftrialsofinhaledipratropiumbromideusedinassociationwithaninhaledβ2-agonistsinacuteasthmashowedthattheanticholinergicproducesastatisticallysignificant,albeitmodest,improvementinpulmonaryfunction,andsignificantlyreducestheriskofhospitaladmission117.Thebenefitsofipratropiumbromideinthelong-termmanagementofasthmahavenotbeenestablished,althoughitisrecognizedasanalternativebronchodilatorforpatientswhoexperiencesuchadverseeffectsastachycardia,arrhythmia,andtremorfromrapid-actingβ2-agonists.
Side effects-Inhalationofipratropiumoroxitropiumcancauseadrynessofthemouthandabittertaste.Thereisnoevidence for any adverse effects on mucus secretion118.
Theophylline.
Roleintherapy-Short-actingtheophyllinemaybeconsideredforreliefofasthmasymptoms119.Theroleoftheophyllineintreatingexacerbationsremainscontroversial.Short-actingtheophyllinemayprovidenoadditivebronchodilatoreffectoveradequatedosesofrapid-actingβ2-agonists,butitmaybenefitrespiratorydrive.
Side effects-Theophyllinehasthepotentialforsignificantadverseeffects,althoughthesecangenerallybeavoidedbyappropriatedosingandmonitoring.Short-actingtheophyllineshouldnotbeadministeredtopatientsalreadyonlong-termtreatmentwithsustained-releasetheophyllineunlesstheserumconcentrationoftheophyllineisknowntobelowand/orcanbemonitored.
Short-acting oral β2-agonists.
Short-actingoralβ2-agonistsareappropriateforuseinthefewpatientswhoareunabletouseinhaledmedication.However,theiruseisassociatedwithahigherprevalenceofadverseeffects.
Complementary And Alternative Medicine
Therolesofcomplementaryandalternativemedicineinadultasthmatreatmentarelimitedbecausetheseapproacheshavebeeninsufficientlyresearchedandtheireffectivenessislargelyunproven.Generally,thesetherapieshavenotbeenvalidatedbyconventionalstandards.Althoughthepsychotherapeuticroleofthetherapistformspartoftheplaceboeffectofalltreatments,thisaspectisviewedasanintegralpartoftheso-calledholisticapproachusedbypractitionersofcomplementaryandalternativemethods,andmitigatesagainstperformanceofthelarge,multicenter,placebo-controlledrandomizedstudiesrequiredtoconfirmefficacy.However,withoutthesetherelativeefficacyofthesealternativemeasureswillremainunknown.
Complementaryandalternativetherapiesincludeacupuncture,homeopathy,herbalmedicine,Ayurvedicmedicine,ionizers,osteopathyandchiropracticmanipulation,andspeleotherapyamongothers.Apartfromthosementionedbelow,therehavebeenfewsatisfactorystudiesfromwhichconclusionsabouttheirefficacycanbedrawn.
Dietarysupplements,includingseleniumtherapy197 are not ofprovenbenefitandtheuseofalowsodiumdietasanadjunctivetherapytonormaltreatmenthasnoadditionaltherapeuticbenefitinadultswithasthma.Inaddition,ithasnoeffectonbronchialreactivitytomethacholine217.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

38 ASTHMA TREATMENTS
Evidencefromthemostrigorousstudiesavailabletodateindicatesthatspinalmanipulationisnotaneffectivetreatmentforasthma121.Systematicreviewsindicatethathomeopathicmedicineshavenoeffectsbeyondplacebo222.Asystematicreviewofyogainterventionsforasthmafoundnoconvincingevidenceofbenefit;thequalityofstudieswasgenerallypoor236.
Severalstudiesofbreathingand/orrelaxationtechniquesforasthmaand/ordysfunctionalbreathing,includingtheButeykomethodandthePapworthmethod210,haveshownimprovementsinsymptoms,short-actingβ2-agonistuse,qualityoflifeand/orpsychologicalmeasures,butnotinphysiologicaloutcomes.Astudyoftwophysiologically-contrastingbreathingtechniques,inwhichcontactwithhealthprofessionalsandinstructionsaboutrescueinhalerusewerematched,showedsimilarimprovementsinrelieverandinhaledglucocorticosteroiduseinbothgroups122.Thissuggeststhatperceivedimprovementwithbreathingtechniquesmaybelargelyduetofactorssuchasrelaxation, voluntary reduction in use of rescue medication, orengagementofthepatientintheircare.Breathingtechniquesmaythusprovideausefulsupplementtoconventionalasthmamanagementstrategies,particularlyinanxiouspatientsorthosehabituallyover-usingrescuemedication.Thecostofsomeprogramsmaybeapotentiallimitation.
Side effects-Acupuncture-associatedhepatitisB,bilateralpneumothorax,andburnshavebeendescribed.Sideeffectsofotheralternativeandcomplementarymedicinesarelargelyunknown.However,somepopularherbalmedicinescouldpotentiallybedangerous,asexemplifiedbytheoccurrenceofhepaticveno-occlusivediseaseassociatedwiththeconsumptionofthecommerciallyavailableherbcomfrey.Comfreyproductsaresoldasherbalteasandherbalrootpowders,andtheirtoxicityisduetothepresenceofpyrroliidinealkaloids.
Route of Administration
Inhaledtherapyisthecornerstoneofasthmatreatmentforchildrenofallages.Almostallchildrencanbetaughttoeffectivelyuseinhaledtherapy.Differentagegroupsrequiredifferentinhalersforeffectivetherapy,sothechoiceofinhalermustbeindividualized.Informationaboutthelungdoseforaparticulardrugformulationisseldomavailableforchildren,andmarkeddifferencesexistbetweenthevariousinhalers.Thisshouldbeconsideredwheneveroneinhalerdeviceissubstitutedwithanother.Inaddition,
thechoiceofinhalerdeviceshouldincludeconsiderationoftheefficacyofdrugdelivery,cost,safety,easeofuse,convenience,anddocumentationofitsuseinthepatient’sagegroup123-125.Ingeneral,ametered-doseinhaler(MDI)withspacerispreferabletonebulizedtherapyduetoitsgreaterconvenience,moreeffectivelungdeposition,lowerriskofsideeffects,andlowercost.Basedontheseconsiderations,ageneralstrategyforchoosinginhalersinchildrenisgiveninFigure 3-3.
Spacersretainlargedrugparticlesthatwouldnormallybedepositedintheoropharynx,reducingoralandgastrointestinalabsorptionandthussystemicavailabilityoftheinhaleddrug.Thisismainlyimportantwheninhaledglucocorticosteroidswithfirst-passmetabolism(beclomethasonedipropionate,flunisolide,triamcinolone,andbudesonide)aregivenviapressurizedMDI.Useofaspaceralsoreducesoropharyngealsideeffects.Duringacuteasthmaattacks,anMDIshouldalwaysbeusedwithaspacer,asinthissituationachildmaybeunabletocorrectlycoordinateinhalationwithactuationoftheMDI.
Commerciallyproducedspacerswithwell-characterizeddrugoutputcharacteristicsarepreferable,althoughspacerdevicesorfacemasksdifferintheirdrugdeliveryandthereforemaynotbeinterchangable237.Ifthesearenotavailableorfeasible,ahomemadespacer(forexample,onemadefroma500mlplasticcolddrinkbottle)maybe used126.Nebulizershaveratherimprecisedosing,areexpensive,aretimeconsumingtouseandcarefor,andrequiremaintenance.Theyaremainlyreservedforchildrenwhocannotuseotherinhalerdevices.Insevereacuteasthmaexacerbationsanebulizerisoftenused,althoughanMDIwithaspacerisequallyeffective127.
ASTHMA TREATMENT: CHILDREN**
Figure 3-3: Choosing an Inhaler Device for Children with Asthma*
Age Group Preferred Device Alternate DeviceYounger than 4 years Pressurized metered-
dose inhaler plusdedicated spacer with face mask
Nebulizer with facemask
4 – 6 years Pressurized metered-dose inhaler plusdedicated spacer with mouthpiece
Nebulizer with mouthpiece
Older than 6 years Dry powder inhaler,or breath-actuatedpressurized metered-dose inhaler, orpressurized metered-dose inhaler withspacer and mouthpiece
Nebulizer with mouthpiece
*Based on efficacy of drug delivery, cost effectiveness, safety, ease of use, andconvenience.
**See also the “Asthma Medications: Adults” section at the beginning of this chapter for more information on the therapeutic role and side effects of various therapies. In this section, only information specific to children is provided. COPY
RIGHTE
D MAT
ERIA
L - D
O NOT
ALTE
R OR R
EPRODUCE

ASTHMA TREATMENTS 39
Controller Medications
Controllermedicationsforchildrenincludeinhaledandsystemicglucocorticosteroids,leukotrienemodifiers,long-actinginhaledβ2-agonists,theophylline,cromones,andlong-actingoralβ2-agonists.
Inhaled glucocorticosteroids.
Role in Therapy-Inhaledglucocorticosteroidsarethemosteffectivecontrollertherapy,andarethereforetherecommendedtreatmentforasthmaforchildrenofallages.Figure 3-4listsapproximatelyequipotentdosesofdifferentinhaledglucocorticosteroidsadministeredviadifferentinhalationdevicesforchildrenolderthan5years.
Childrenolderthan5years.Dose-responsestudiesanddosetitrationstudiesinchildren128,129demonstratemarkedandrapidclinicalimprovementsinsymptomsandlungfunctionatlowdosesofinhaledglucocorticosteroids(e.g.,100-200µgbudesonidedaily)130-134, and mild diseaseiswellcontrolledbysuchdosesinthemajorityofpatients132.Earlyinterventionwithinhaledbudesonideisassociatedwithimprovedasthmacontrolandlessadditionalasthmamedicationuse132.Somepatientsrequirehigherdoses(400µg/day)toachieveoptimalasthmacontrolandeffectiveprotectionagainstexercise-inducedasthma.Onlyaminorityofpatientsrequiretreatment
withhighdosesofinhaledglucocorticosteroids133,134.Inchildrenolderthan5years,maintenancetreatmentwithinhaledglucocorticosteroidscontrolsasthmasymptoms,reducesthefrequencyofacuteexacerbationsandthenumberofhospitaladmissions,improvesqualityoflife,lungfunction,andbronchialhyperresponsiveness,andreducesexercise-inducedbronchoconstriction10.Symptomcontrolandimprovementsinlungfunctionoccurrapidly(after1to2weeks),althoughlongertreatment(overthecourseofmonths)andsometimeshigherdosesmayberequiredtoachievemaximumimprovementsinairwayhyperresponsiveness10.Whenglucocorticosteroidtreatmentisdiscontinued,asthmacontroldeteriorateswithinweekstomonths10.
Children5yearsandyounger.Treatmentwithinhaledglucocorticosteroidsinchildren5yearsandyoungerwithasthmagenerallyproducessimilarclinicaleffectsasinolderchildren,butdose-responserelationshipshavebeenlesswellstudied.Theclinicalresponsemaydifferdependingontheinhalerandthechild’sabilitytousetheinhalercorrectly.Withuseofaspacerdevice,alow-doseinhaledglucocorticosteroidresultsinnear-maximumbenefitsinthemajorityofpatients136,137.Useofinhaledglucocorticosteroidsdoesnotinduceremissionofasthmaanditreturnswhentreatmentisstopped138.
Figure 3-4. Estimated Equipotent Daily Doses of Inhaled Glucocorticosteroids for Children Older than 5 Years
Drug Low Daily Dose (�g) Medium Daily Dose (�g) High Daily Dose (�g)‡
Beclomethasone dipropionate 100 - 200 >200 - 400 >400 Budesonide* 100 - 200 >200 - 400 >400 Budesonide-Neb 250 - 500 >500 - 1000 >1000 Ciclesonide* 80 - 160 >160 - 320 >320 Flunisolide 500 - 750 >750 - 1250 >1250 Fluticasone propionate 100 - 200 >200 - 500 >500 Mometasone furoate* 100 - 200 >200 - 400 >400 Triamcinolone acetonide 400 - 800 >800 - 1200 >1200
† Comparisons based upon efficacy data. ‡ Patients considered for high daily doses except for short periods should be referred to a specialist for assessment to consider alternative combinations of controllers. Maximum recommended doses are arbitrary but with prolonged use are associated with increased risk of systemic side effects. * Approved for once-daily dosing in mild patients.
Notes • The most important determinant of appropriate dosing is the clinician’s judgment of the patient’s response to therapy. The clinician must monitor the
patient’s response in terms of clinical control and adjust the dose accordingly. Once control of asthma is achieved, the dose of medication should be carefully titrated to the minimum dose required to maintain control, thus reducing the potential for adverse effects.
• Designation of low, medium, and high doses is provided from manufacturers’ recommendations where possible. Clear demonstration of dose- response relationships is seldom provided or available. The principle is therefore to establish the minimum effective controlling dose in each patient, as higher doses may not be more effective and are likely to be associated with greater potential for adverse effects.
• As CFC preparations are taken from the market, medication inserts for HFA preparations should be carefully reviewed by the clinician for the correct equivalent dosage.
100 ≥200
≥400
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

40 ASTHMA TREATMENTS
Theclinicalbenefitsofintermittentsystemicorinhaledglucocorticosteroidsforchildrenwithintermittent,viral-inducedwheezeremaincontroversial.Aoneyearstudyofintermittenttreatmentwithinhaledglucocorticosteroidswas equally effective as daily treatment, and reduced thetotalglucocorticosteroiddosethreefoldinpreschoolchildrenwithfrequentwheezingandahighasthmapredictiveindex238.Somestudiesinolderchildrenfoundsmallbenefitswhileanotherstudyinyoungchildrenfoundnoeffectsonwheezingsymptoms139.Thereisnoevidencetosupporttheuseofmaintenancelow-doseinhaledglucocorticosteroidsforpreventingearlytransientwheezing136,139,199.
Side effects-Themajorityofstudiesevaluatingthesystemiceffectsofinhaledglucocorticosteroidshavebeenundertakeninchildrenolderthan5years.
Growth.Whenassessingtheeffectsofinhaledglucocorticosteroidsongrowthinchildrenwithasthma,itisimportanttoconsiderpotentialconfoundingfactors.Forexample,manychildrenwithasthmareceivinginhaledglucocorticosteroidsexperienceareductioningrowthratetowardtheendofthefirstdecadeoflife140.Thisreducedgrowthratecontinuesintothemid-teensandisassociatedwithadelayintheonsetofpuberty.Thepre-pubertaldecelerationofgrowthvelocityresemblesgrowthretardation.However,thedelayinpubertalgrowthisalsoassociatedwithadelayinskeletalmaturation,sothat
thechild’sboneagecorrespondstohisorherheight140,141 Ultimately,adultheightisnotdecreased,althoughitisreachedatalaterthannormalage.Theuseof400µginhaledbudesonideorequivalentperdaytocontrolasthmahaslessimpactongrowththandoeslowsocioeconomicstatus141.AsummaryofthefindingsofstudiesoninhaledglucocorticosteroidsandgrowthisprovidedinFigure 3-5.
Bones.Thepotentialclinicallyrelevantadverseeffectsofinhaledglucocorticosteroidsonbonesinchildrenareosteoporosisandfracture.Severalcross-sectionalandlongitudinalepidemiologicstudieshaveassessedtheeffectsoflong-terminhaledglucocorticosteroidtreatmentontheseoutcomes132,143-149.TheconclusionsaresummarizedinFigure 3-6.
Hypothalamic-pituitary-adrenal(HPA)axis.Thoughdifferencesexistbetweenthevariousinhaledglucocorticosteroidsandinhalerdevices,treatmentwithinhaledglucocorticosteroiddosesoflessthan200µgbudesonide or equivalent daily is normally not associated withanysignificantsuppressionoftheHPAaxisinchildren.Athigherdoses,smallchangesinHPAaxisfunctioncanbedetectedwithsensitivemethods148.Theclinicalrelevanceofthesefindingsisnotknown,sincetherehavenotbeenreportsofadrenalcrisisinclinicaltrialsofinhaledglucocorticosteroidsinchildren.However,adrenalcrisishasbeenreportedinchildrentreatedwithexcessivelyhighdosesofinhaledglucocorticosteroids150.
Cataracts.Inhaledglucocorticosteroidshavenotbeenassociatedwithanincreasedoccurrenceofcataractdevelopmentinchildren30.
• Uncontrolled or severe asthma adversely affects growth and final adult height.
• No long-term controlled studies have reported any statistically or clinically significant adverse effects on growth of 100 to 200 µg per day of inhaled glucocorticosteroids.
• Growth retardation may be seen with all inhaled glucocorticosteroids when a high dose is administered.
• Growth retardation in both short-and medium-term studies is dose dependent.
• Important differences seem to exist between the growth-retarding effects of various inhaled glucocorticosteroids and inhalers.
• Different age groups seem to differ in their susceptibility to the growth-retarding effects of inhaled glucocorticosteroids; children aged 2 to 10 are more susceptible than adolescents.
• Glucocorticosteroid-induced changes in growth rate during the first year of treatment appear to be temporary. Children with asthma treated with inhaled glucocorticosteroids attain normal adult height (predicted from family members) but at a later age.
Figure 3-5. Summary: Glucocorticosteroids and Growth in Children140-142,239
• No studies have reported any statistically significant increased of risk of fractures in children taking inhaled glucocorticosteroids.
• Oral or systemic glucocorticosteroid use increases the risk of fracture. The risk of fracture increases along with the number of treatments, with a 32% increase at four courses ever. Use of inhaled glucocorticosteroids reduces the need for systemic courses.
• Controlled longitudinal studies of 2 to 5 years’ duration and several cross-sectional studies found no adverse effects of inhaled glucocorticosteroid treatment on bone mineral density.
• Inhaled glucocorticosteroid use has the potential for reducing bone mineral accretion in male children progressing through puberty, but this risk is likely to be outweighed by the ability to re¬duce the amount of oral corticosteroids used in these children218 .
Figure 3-6. Summary: Bones and Glucocorticosteroids in Children10,143,144
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA TREATMENTS 41
Centralnervoussystemeffects.Althoughisolatedcasereportshavesuggestedthathyperactivebehavior,aggressiveness,insomnia,uninhibitedbehavior,andimpairedconcentrationmaybeseenwithinhaledglucocorticosteroidtreatment,noincreaseinsucheffectshasbeenfoundinalong-termcontrolledtrialofinhaledbudesonide132.
Oralcandidiasis,hoarseness,andbruising.Clinicalthrushisseldomaprobleminchildrentreatedwithinhaledorsystemicglucocorticosteroids.Thissideeffectseemstoberelatedtoconcomitantuseofantibiotics,highdailydoses,dosefrequency,andinhalerdevice.Spacersreducetheincidenceoforalcandidiasis151.Mouthrinsingisbeneficial152.Theoccurrenceofhoarsenessorothernoticeablevoicechangesduringbudesonidetreatmentissimilartoplacebo30.Treatmentwithanaveragedailydoseof500µgbudesonidefor3to6yearsisnotassociatedwithan increased tendency to bruise30.
Dentalsideeffects.Inhaledglucocorticosteroidtreatmentisnotassociatedwithincreasedincidenceofcaries.However,theincreasedlevelofdentalerosionreportedinchildrenwithasthma153maybeduetoareductioninoralpHthatmayresultfrominhalationofβ2-agonists
154.
Otherlocalsideeffects.Thelong-termuseofinhaledglucocorticosteroidsisnotassociatedwithanincreasedincidenceoflowerrespiratorytractinfections,includingtuberculosis.
Leukotriene modifiers.
Childrenolderthan5years.Leukotrienemodifiersprovideclinicalbenefitinchildrenolderthan5yearsatalllevelsof severity155-159,butgenerallylessthanthatoflow-doseinhaledglucocorticosteroids160.Leukotrienemodifiersprovidepartialprotectionagainstexercise-inducedbronchoconstrictionwithinhoursafteradministrationwithnolossofbronchoprotectiveeffect200.Asadd-ontreatmentinchildrenwhoseasthmaisinsufficientlycontrolledbylowdosesofinhaledglucocorticosteroids,leukotrienemodifiersprovidemoderateclinicalimprovements,includingasignificantreductioninexacerbations162.Combinationtherapyislesseffectiveincontrollingasthmainchildrenwithmoderatepersistentasthmathanincreasingtomoderatedosesofinhaledglucocorticosteroids201.Montelukasthasnotbeendemonstratedtobeaneffectiveinhaledglucocorticosteroidsparingalternativeinchildrenwithmoderate-to-severepersistentasthma219.
Children5yearsandyounger.Inadditiontotheefficacyasdescribed above163,164,leukotrienemodifiersreduceviral-inducedasthmaexacerbationsinchildrenages2-5withahistoryofintermittentasthma164.
Side effects-Nosafetyconcernshavebeendemonstratedfromtheuseofleukotrienemodifiersinchildren.
Long-acting inhaled β2-agonists.
Roleintherapy-Long-actinginhaledβ2-agonistsareprimarilyusedasadd-ontherapyinchildrenolderthan5yearswhoseasthmaisinsufficientlycontrolledbymediumdosesofinhaledglucocorticosteroidsorassingle-dosetherapybeforevigorousexercise.Monotherapywithlong-actinginhaledβ2-agonistsshouldbeavoided
75,234.
Childrenolderthan5years.Long-actinginhaledβ2-agonistshavemainlybeenstudiedinchildrenolderthan5yearsasadd-ontherapyforpatientswhoseasthmaisnotcontrolledonlowtohighdosesofinhaledglucocorticosteroids.Significantimprovementsinpeakflowandotherlungfunctionmeasurementshavebeenfound in most studies55,165-169, 234.However,theeffectsonotheroutcomessuchassymptomsandneedforrelievermedicationhavebeenlessconsistentandhaveonlybeenobservedinabouthalfofthetrialsconducted.Add-ontreatmentwithlong-actinginhaledβ2-agonistshasnotbeenshowntoreducethefrequencyofexacerbations170.Inhalationofasingledoseoflong-actinginhaledβ2-agonistseffectivelyblocksexercise-inducedbronchoconstrictionforseveralhours171.Withdailytherapythedurationoftheprotectionissomewhatreduced171, but is stilllongerthanthatprovidedbyshort-actingβ2-agonists.Combinationproductscontaininganinhaledglucocorticosteroidandalong-actinginhaledβ2-agonistsarepreferredtolong-actinginhaledβ2-agonistsandinhaledglucocorticosteroidsadministeredbyseparateinhalers.Fixedcombinationinhalersensurethatthelong-actingβ2-agonistsisalwaysaccompaniedbyaglucocorticosteroid.
Children5yearsandyounger.Theeffectoflong-actinginhaledβ2-agonistshasnotyetbeenadequatelystudied.Combinationtherapywithbudesonideandformoterolusedbothasmaintenanceandrescuehasbeenshowntoreduceasthmaexacerbationsinchildrenages4yearsandolderwithmoderatetosevereasthma202.
Side effects-Althoughlong-actinginhaledβ2-agonistsarewell-toleratedinchildren,evenafterlong-termuse,becauseofinconsistencyofreportsontheireffectsonexacerbationsofasthma,theyarenottherecommendedoptionwhenmorethanonecontrollerisrequired170.Ifused,long-actingβ2-agonistsshouldonlybeusedincombinationwithanappropriatedoseofinhaledglucocorticosteroidasdeterminedbyaphysician,preferablyinafixedcombinationinhaler.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

42 ASTHMA TREATMENTS
Theophylline.
Role in therapy-Theophyllinehasbeenshowntobeeffectiveasmonotherapyandasadd-ontreatmenttoinhaledororalglucocorticosteroidsinchildrenolderthan5years.Itissignificantlymoreeffectivethanplaceboatcontrollingdayandnightsymptomsandimprovinglungfunction172-174.Maintenancetreatmentoffersamarginalprotectiveeffectagainstexercise-inducedbroncho-constriction175.Add-ontreatmentwiththeophyllinehasbeenfoundtoimproveasthmacontrolandreducethemaintenanceglucocorticosteroiddosenecessaryinchildrenwithsevereasthmatreatedwithinhaledororalglucocorticosteroids176,177.Afewstudiesinchildren5yearsandyoungeralsosuggestsomeclinicalbenefit.However,theefficacyoftheophyllineislessthanthatoflow-doseinhaledglucocorticosteroids.
Mostclinicalevidenceregardingtheuseoftheophyllineinchildrenhasbeenobtainedfromstudiesinwhichplasmatheophyllinelevelsweremaintainedwithinthetherapeuticrangeof55-110µmol/L(5-10µg/ml).Furtherstudiessuggestthatitscontrollerfunctionsmayoccuratlowerplasmalevels(correspondingtodosesofaround10mg/kg/day).Sustained-releaseproductsarepreferableformaintenancetherapy,sincetheyenabletwice-dailydosing.Sustained-releaseproductswithreliableabsorptionprofilesandcompletebioavailabilitywithandwithoutconcomitantfoodintakearepreferred.Theophyllineeliminationmayvaryuptotenfoldbetweenindividuals.Measurementofplasmatheophyllinelevelsisnotnecessaryinotherwisehealthychildrenwhendoseslessthan10mg/kg/dayareused.However,whenhigherdosesareusedorwhendrugsthatmayincreasetheophyllinelevelsarealsousedchronically,plasmatheophyllinelevelsshouldbemeasuredtwohoursbeforeadministrationofthenextdoseoncesteadystatehasbeenreached(after3days).
Side effects-Themostcommonsideeffectsoftheophyllineareanorexia,nausea,vomiting,andheadache178.Mildcentralnervousstimulation,palpitations,tachycardia,arrhythmias,abdominalpain,diarrhea,and,rarely,gastricbleedingmayalsooccur.Thesesideeffectsaremainlyseenatdoseshigherthan10mg/kg/day.Theriskofadverseeffectsisreducediftreatmentisinitiatedwithdailydosesaround5mg/kg/dayandthengraduallyincreasedto10mg/kg/day.Severeoverdosingwiththeophyllinecanbefatal.
Anti-IgE.
Role in therapy -Anti-IgE(omalizumab)hasprovenefficacyinchildrenage6to12yearswithmoderate-to-severeandseverepersistentallergic(IgE-mediated)asthma.A
28week,randomized,double-blind,placebo-controlledstudy223, 224included334childrenwithmoderatetosevereallergicasthmawhowerewellcontrolledoninhaledglucocorticosteroiddosesequivalentto200-500µg/dayofbeclomethasone.Therewasnodifferenceinclinicaleffectsbetweenplaceboandanti-IgEduringa16-weekstableinhaledglucocorticosteroiddoseperiod.Duringa12-weektaperingperiodurgent,unscheduledphysicianvisitsweresignificantlyreducedfromby30.3%intheanti-IgEcomparedwithplacebo(12.9%)group223, and thereweresignificantimprovementsinqualityoflifeinthepatientsreceivinganti-IgE,bothduringstableinhaledglucocorticosteroiddosingandduringtapering224.Theremainingoutcomeswereverysimilarinthetwotreatmentgroups.
Aone-yearstudyevaluatedtheefficacyandsafetyofanti-IgEin627childrenwithIgE-mediatedasthmainadequatelycontrolledondosesofinhaledglucocorticosteroidequivalentto200µg/dayfluticasonepropionateorhigher(meandose500µg/day)225.Anti-IgEtreatmentwasassociatedwithasignificantlylowerexacerbationrateandtheoverallincidenceofseriousadverseeventswassignificantlylowerinthechildrenreceivinganti-IgEthanplacebo.
AsubstantialnumberofchildrenwithdifficultasthmawillhavehigherIgElevelsthantheupperlimitofIgErecommendedfortherapy(1,300IU)226.Itisunknownifthesepatientswillstillbenefitfromomalizumabtherapy.Therearenoteststhatcancurrentlyberecommendedinordertopredictwhowillrespond227.
Anti-IgEtherapyisexpensiveandrequiresregularinjectionsandobservationaftereachinjection.Acostbenefitanalysissuggestedthattherewouldbeafiscalsavingifthistreatmentisgiventochildrenwithfiveormorehospitaladmissionsandcumulativelytwentydaysormoreinhospital228.
Side effects:Drug-relatedadverseeventsinanti-IgEtreatedpatientsaremildtomoderateinseverityandincludeurticaria,rash,flushing,andpruritus223.Thelong-term(beyondoneyear)safetyandefficacyhasnotyetbeenstudied.
Cromones: sodium cromoglycate and nedocromil sodium.
Role in therapy-Sodiumcromoglycateandnedocromilsodiumhavealimitedroleinthelong-termtreatmentofasthmainchildren.Onemeta-analysishasconcludedthatlong-termtreatmentwithsodiumcromoglycateisnotsignificantlybetterthanplaceboformanagementofasthmainchildren179.Anotherhasconfirmedsuperiorityoflowdose
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA TREATMENTS 43
inhaledglucocorticosteroidsoversodiumcromoglycateinpersistentasthma,butastherewerenoplaceboarmsinthesestudies,theefficacyofsodiumcromoglycatecannotbeconfirmedfromthestudiesreviewed;nobetweentreatment difference in safety was observed180.
Nedocromilsodiumhasbeenshowntoreduceexacerbations,butitseffectonotherasthmaoutcomesisnotsuperiortoplacebo.Asingledoseofsodiumcromoglycateornedocromilsodiumattenuatesbroncho-spasminducedbyexerciseorcoldair181.Studiesoftheuseofthesemedicationsinchildren5yearsandyoungeraresparseandresultsareconflicting.
Side effects-Cough,throatirritation,andbroncho-constrictionoccurinasmallproportionofpatientstreatedwithsodiumcromoglycate.Abadtaste,headache,andnauseaarethemostcommonsideeffectsofnedocromil182.
Long-acting oral β2-agonists.
Treatmentwithlong-actingoralβ2-agonistsuchasslowrelease formulations of salbutamol, terbutaline, and bambuterolreducesnocturnalsymptomsofasthma183,184.Duetotheirpotentialsideeffectsofcardiovascularstimulation,anxiety,andskeletalmuscletremor,theiruseisnotencouraged.Ifused,dosingshouldbeindividualied,andthetherapeuticresponsemonitoredtolimitsideeffects185.Long-actingoralβ2-agonisttherapyofferslittleornoprotectionagainstexercise-inducedbronchoconstriction.
Systemic glucocorticosteroids.
Becauseofthesideeffectsofprolongeduse,oralglucocorticosteroidsinchildrenwithasthmashouldberestrictedtothetreatmentofacutesevereexacerbations,whetherviral-inducedorotherwise.
Reliever Medications
Rapid-acting inhaled ß2-agonists and short-acting oral ß2-agonists.
Role in therapy-Rapid-actinginhaledß2-agonistsarethemosteffectivebronchodilatorsavailableandthereforethepreferredtreatmentforacuteasthmainchildrenofallages.Theinhaledrouteresultsinmorerapidbronchodilationatalowerdoseandwithfewersideeffectsthanoralorintravenous administration186.Furthermore,inhaledtherapyofferssignificantprotectionagainstexercise-inducedbronchoconstrictionandotherchallengesfor0.5to2hours(long-actingß2-agonistsofferlongerprotection)
187.Thisisnot seen after systemic administration188.Oraltherapyisrarelyneededandreservedmainlyforyoungchildrenwhocannotuseinhaledtherapy.
Side effects-Skeletalmuscletremor,headache,palpitations,andsomeagitationarethemostcommoncomplaintsassociatedwithhighdosesofß2-agonistsinchildren.Thesecomplaintsaremorecommonaftersystemicadministrationanddisappearwithcontinuedtreatment189.
Anticholinergics.
Role in therapy-Inhaledanticholinergicsarenotrecommendedforlong-termmanagementofasthmainchildren190.
REFERENCES
1. BrownPH,GreeningAP,CromptonGK.Largevolumespacerdevicesandtheinfluenceofhighdosebeclomethasonedipropionateonhypothalamo-pituitary-adrenalaxisfunction.Thorax1993;48(3):233-8.
2. DolovichM.Newdeliverysystemsandpropellants.Can Respir J1999;6(3):290-5.
3. LeachCL,DavidsonPJ,BoudreauRJ.ImprovedairwaytargetingwiththeCFC-freeHFA-beclomethasonemetered-doseinhalercomparedwithCFC-beclomethasone.Eur Respir J1998;12(6):1346-53.
4. HarrisonLI,SoriaI,ClineAC,EkholmBP.Pharmacokineticdifferencesbetweenchlorofluorocarbonandchlorofluorocarbon-freemetereddoseinhalersofbeclomethasonedipropionateinadultasthmatics.J Pharm Pharmacol1999;51(11):1235-40.
5. JuniperEF,PriceDB,StamponePA,CreemersJP,MolSJ,FiremanP.Clinicallyimportantimprovementsinasthma-specificqualityoflife,butnodifferenceinconventionalclinicalindexesinpatientschangedfromconventionalbeclomethasonedipropionatetoapproximatelyhalfthedoseofextrafinebeclomethasonedipropionate.Chest 2002;121(6):1824-32.
6. LangleyPC.Thetechnologyofmetered-doseinhalersandtreatmentcostsinasthma:aretrospectivestudyofbreathactuationversustraditionalpress-and-breatheinhalers.Clin Ther1999;21(1):236-53.
7. NewmanSP.Acomparisonoflungdepositionpatternsbetweendifferentasthmainhalers. J Aerosol Med1995;8Suppl3:21-6S.
8. NewmanSP.InhalertreatmentoptionsinCOPD.Eur Respir Rev2005;14(96):102-8.
9. JuniperEF,KlinePA,VanzieleghemMA,RamsdaleEH,O’ByrnePM,HargreaveFE.Effectoflong-termtreatmentwithaninhaledcorticosteroid(budesonide)onairwayhyper-responsivenessandclinicalasthmainnonsteroid-dependentasthmatics.Am Rev Respir Dis1990;142(4):832-6.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

44 ASTHMA TREATMENTS
10. TheChildhoodAsthmaManagementProgramResearchGroup.Long-termeffectsofbudesonideornedocromilinchildrenwithasthma.N Engl J Med2000;343(15):1054-63.
11. JefferyPK,GodfreyRW,AdelrothE,NelsonF,RogersA,JohanssonSA.Effectsoftreatmentonairwayinflammationandthickeningofbasementmembranereticularcollageninasthma.Aquantitativelightandelectronmicroscopicstudy.Am Rev Respir Dis1992;145(4Pt1):890-9.
12. PauwelsRA,LofdahlCG,PostmaDS,TattersfieldAE,O’ByrneP,BarnesPJ,et al.Effectofinhaledformoterolandbudesonideonexacerbationsofasthma.FormoterolandCorticosteroidsEstablishingTherapy(FACET)InternationalStudyGroup.N Engl J Med1997;337(20):1405-11.
13. SuissaS,ErnstP,BenayounS,BaltanM,CaiB.Low-doseinhaledcorticosteroidsandthepreventionofdeathfromasthma.N Engl J Med2000;343(5):332-6.
14. WaalkensHJ,VanEssen-ZandvlietEE,HughesMD,GerritsenJ,DuivermanEJ,KnolK,et al.Cessationoflong-termtreatmentwithinhaledcorticosteroid(budesonide)inchildrenwithasthmaresultsindeterioration.TheDutchCNSLDStudyGroup.Am Rev Respir Dis1993;148(5):1252-7.
15. JayasiriB,PereraC.Successfulwithdrawalofinhaledcorticosteroidsinchildhoodasthma.Respirology2005;10:385-8.
16. NationalHeart,Lung,andBloodInstitute,GuidelinesforDiagnosisandManagementofAsthma.http://www.nhlbi.nih.gov/guidelines/asthma/Datelastupdated:July2007.Datelastaccessed,July15,2007.
17. PowellH,GibsonPG.Inhaledcorticosteroiddosesinasthma:anevidence-basedapproach.Med J Aust 2003;178(5):223-5.
18. SzeflerSJ,MartinRJ,KingTS,BousheyHA,CherniackRM,ChinchilliVM,et al.Significantvariabilityinresponsetoinhaledcorticosteroidsforpersistentasthma.J Allergy Clin Immunol 2002;109(3):410-8.
19. LipworthBJ,KalinerMA,LaForceCF,BakerJW,KaiserHB, Amin D, et al.Effectofciclesonideandfluticasoneonhypothalamic-pituitary-adrenalaxisfunctioninadultswithmild-to-moderatepersistentasthma.Ann Allergy Asthma Immunol 2005;94(4):465-72.
20. LipworthBJ.Systemicadverseeffectsofinhaledcorticosteroidtherapy:Asystematicreviewandmeta-analysis.Arch Intern Med1999;159(9):941-55.
21. BarnesPJ.Efficacyofinhaledcorticosteroidsinasthma.J Allergy Clin Immunol1998;102(4Pt1):531-8.
22. KamadaAK,SzeflerSJ,MartinRJ,BousheyHA,ChinchilliVM,DrazenJM,et al.Issuesintheuseofinhaledglucocorticoids.TheAsthmaClinicalResearchNetwork.Am J Respir Crit Care Med1996;153(6Pt1):1739-48.
23. Lee DK, Bates CE, Currie GP, Cowan LM, McFarlane LC, LipworthBJ.Effectsofhigh-doseinhaledfluticasonepropionateonthehypothalamic-pituitary-adrenalaxisinasthmaticpatientswithseverelyimpairedlungfunction.Ann Allergy Asthma Immunol2004;93(3):253-8.
24. MakVH,MelchorR,SpiroSG.Easybruisingasaside-effectofinhaledcorticosteroids.Eur RespirJ1992;5(9):1068-74.
25. TheLungHealthStudyResearchGroup.Effectofinhaledtriamcinoloneonthedeclineinpulmonaryfunctioninchronicobstructivepulmonarydisease.N Engl J Med 2000;343(26):1902-9.
26. PauwelsRA,YernaultJC,DemedtsMG,GeusensP.Safetyandefficacyoffluticasoneandbeclomethasoneinmoderatetosevereasthma.BelgianMulticenterStudyGroup.Am J Respir Crit Care Med1998;157(3Pt1):827-32.
27. ErnstP,BaltanM,DeschenesJ,SuissaS.Low-doseinhaledandnasalcorticosteroiduseandtheriskofcataracts.Eur RespirJ2006;27(6):1168-74.
28. GarbeE,LeLorierJ,BoivinJF,SuissaS.Inhaledandnasalglucocorticoidsandtherisksofocularhypertensionoropen-angleglaucoma.JAMA1997;277(9):722-7.
29. CummingRG,MitchellP,LeederSR.Useofinhaledcorticosteroidsandtheriskofcataracts.N Engl J Med 1997;337(1):8-14.
30. AgertoftL,LarsenFE,PedersenS.Posteriorsubcapsularcataracts,bruisesandhoarsenessinchildrenwithasthmareceivinglong-termtreatmentwithinhaledbudesonide.Eur RespirJ1998;12(1):130-5.
31. ToogoodJH,MarkovAE,BaskervilleJ,DysonC.Associationofocularcataractswithinhaledandoralsteroidtherapyduringlong-termtreatmentofasthma.J Allergy Clin Immunol 1993;91(2):571-9.
32. SimonsFE,PersaudMP,GillespieCA,CheangM,ShuckettEP.Absenceofposteriorsubcapsularcataractsinyoungpatientstreatedwithinhaledglucocorticoids.Lancet 1993;342(8874):776-8.
33. BahcecilerNN,NuhogluY,NursoyMA,KodalliN,BarlanIB,BasaranMM.Inhaledcorticosteroidtherapyissafeintuberculin-positiveasthmaticchildren.Pediatr Infect Dis J 2000;19:215-8.
34. DicpinigaitisPV,DobkinJB,ReichelJ.Antitussiveeffectoftheleukotrienereceptorantagonistafirlukastinsubjectswithcough-variantasthma.J Asthma2002;39(4):291-7.
35. LipworthBJ.Leukotriene-receptorantagonists.Lancet 1999;353(9146):57-62.
36. DrazenJM,IsraelE,O’ByrnePM.Treatmentofasthmawithdrugsmodifyingtheleukotrienepathway.N Engl J Med 1999;340(3):197-206.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA TREATMENTS 45
37. BarnesNC,MillerCJ.Effectofleukotrienereceptorantagonisttherapyontheriskofasthmaexacerbationsinpatientswithmildtomoderateasthma:anintegratedanalysisofafirlukasttrials.Thorax2000;55(6):478-83.
38. NoonanMJ,ChervinskyP,BrandonM,ZhangJ,KunduS,McBurneyJ,et al.Montelukast,apotentleukotrienereceptorantagonist,causesdose-relatedimprovementsinchronicasthma.MontelukastAsthmaStudyGroup.Eur RespirJ1998;11(6):1232-9.
39. ReissTF,ChervinskyP,DockhornRJ,ShingoS,SeidenbergB,EdwardsTB.Montelukast,aonce-dailyleukotrienereceptorantagonist,inthetreatmentofchronicasthma:amulticenter,randomized,double-blindtrial.MontelukastClinicalResearchStudyGroup.Arch Intern Med1998;158(11):1213-20.
40. LeffJA,BusseWW,PearlmanD,BronskyEA,KempJ,Hendeles L, et al.Montelukast,aleukotriene-receptorantagonist,forthetreatmentofmildasthmaandexercise-inducedbronchoconstriction.N Engl J Med1998;339(3):147-52.
41. DahlenB,NizankowskaE,SzczeklikA,ZetterstromO,BochenekG,KumlinM,et al.Benefitsfromaddingthe5-lipoxygenaseinhibitorileutontoconventionaltherapyinaspirin-intolerantasthmatics.Am J Respir Crit Care Med 1998;157(4Pt1):1187-94.
42. BleeckerER,WelchMJ,WeinsteinSF,KalbergC,JohnsonM, Edwards L, et al.Low-doseinhaledfluticasonepropionateversusoralafirlukastinthetreatmentofpersistentasthma.J Allergy Clin Immunol2000;105(6Pt1):1123-9.
43. LavioletteM,MalmstromK,LuS,ChervinskyP,PujetJC,PesekI,et al.Montelukastaddedtoinhaledbeclomethasoneintreatmentofasthma.Montelukast/BeclomethasoneAdditivityGroup.Am J Respir Crit Care Med1999;160(6):1862-8.
44. LofdahlCG,ReissTF,LeffJA,IsraelE,NoonanMJ,FinnAF, et al.Randomised,placebocontrolledtrialofeffectofaleukotrienereceptorantagonist,montelukast,ontaperinginhaledcorticosteroidsinasthmaticpatients.BMJ 1999;319(7202):87-90.
45. VirchowJC,PrasseA,NayaI,SummertonL,HarrisA.Zafirlukastimprovesasthmacontrolinpatientsreceivinghigh-doseinhaledcorticosteroids.Am J Respir Crit Care Med 2000;162(2Pt1):578-85.
46. PriceDB,HernandeD,MagyarP,FitermanJ,BeehKM,JamesIG, et al.Randomisedcontrolledtrialofmontelukastplusinhaledbudesonideversusdoubledoseinhaledbudesonideinadultpatientswithasthma.Thorax2003;58(3):211-6.
47. VaquerizoMJ,CasanP,CastilloJ,PerpinaM,SanchisJ,Sobradillo V, et al.Effectofmontelukastaddedtoinhaledbudesonideoncontrolofmildtomoderateasthma.Thorax 2003;58(3):204-10.
48. BjermerL,BisgaardH,BousquetJ,FabbriLM,GreeningAP,HaahtelaT,et al.Montelukastandfluticasonecomparedwithsalmeterolandfluticasoneinprotectingagainstasthmaexacerbation in adults: one year, double blind, randomised, comparativetrial.BMJ2003;327(7420):891.
49. NelsonHS,BusseWW,KerwinE,ChurchN,EmmettA,RickardK,et al.Fluticasonepropionate/salmeterolcombinationprovidesmoreeffectiveasthmacontrolthanlow-doseinhaledcorticosteroidplusmontelukast.J Allergy Clin Immunol 2000;106(6):1088-95.
50. FishJE,IsraelE,MurrayJJ,EmmettA,BooneR,YanceySW,et al.Salmeterolpowderprovidessignificantlybetterbenefitthanmontelukastinasthmaticpatientsreceivingconcomitantinhaledcorticosteroidtherapy.Chest2001;120(2):423-30.
51. RingdalN,EliraA,PruzinecR,WeberHH,MulderPG,AkveldM, et al.Thesalmeterol/fluticasonecombinationismoreeffectivethanfluticasoneplusoralmontelukastinasthma.Respir Med2003;97(3):234-41.
52. Harrold LR, Patterson K, Andrade SE, Dube T, Go AS, Buist AS, et al.AsthmadruguseandthedevelopmentofChurg-Strausssyndrome(CSS).Pharmcoepidemiology and Drug Safety.2007;16:620-26
53. Reference deleted
54. Reference deleted
55. LemanskeRF,Jr.,SorknessCA,MaugerEA,LazarusSC,BousheyHA,FahyJV,et al.Inhaledcorticosteroidreductionandeliminationinpatientswithpersistentasthmareceivingsalmeterol:arandomizedcontrolledtrial.JAMA 2001;285(20):2594-603.
56. LazarusSC,BousheyHA,FahyJV,ChinchilliVM,LemanskeRF,Jr.,SorknessCA,et al.Long-actingbeta2-agonistmonotherapyvscontinuedtherapywithinhaledcorticosteroidsinpatientswithpersistentasthma:arandomizedcontrolledtrial.JAMA2001;285(20):2583-93.
57. PearlmanDS,ChervinskyP,LaForceC,SeltzerJM,SouthernDL,KempJP,et al.Acomparisonofsalmeterolwithalbuterolinthetreatmentofmild-to-moderateasthma.N Engl J Med 1992;327(20):1420-5.
58. KestenS,ChapmanKR,BroderI,CartierA,HylandRH,KnightA,et al.Athree-monthcomparisonoftwicedailyinhaledformoterolversusfourtimesdailyinhaledalbuterolinthemanagementofstableasthma.Am Rev Respir Dis1991;144(3Pt1):622-5.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

46 ASTHMA TREATMENTS
59. WenzelSE,LumryW,ManningM,KalbergC,CoxF,Emmett A, et al.Efficacy,safety,andeffectsonqualityoflifeofsalmeterolversusalbuterolinpatientswithmildtomoderatepersistentasthma.Ann Allergy Asthma Immunol 1998;80(6):463-70.
60. ShrewsburyS,PykeS,BrittonM.Meta-analysisofincreaseddoseofinhaledsteroidoradditionofsalmeterolinsymptomaticasthma(MIASMA).BMJ2000;320(7246):1368-73.
61. WoolcockA,LundbackB,RingdalN,JacquesLA.Comparisonofadditionofsalmeteroltoinhaledsteroidswithdoublingofthedoseofinhaledsteroids.Am J Respir Crit Care Med 1996;153(5):1481-8.
62. GreeningAP,IndPW,NorthfieldM,ShawG.Addedsalmeterolversushigher-dosecorticosteroidinasthmapatientswithsymptomsonexistinginhaledcorticosteroid.Allen&HanburysLimitedUKStudyGroup.Lancet1994;344(8917):219-24.
63. BatemanED,BousheyHA,BousquetJ,BusseWW,ClarkTJ,Pauwels RA, et al.Canguideline-definedasthmacontrolbeachieved?TheGainingOptimalAsthmaControLstudy.Am J Respir Crit Care Med2004;170(8):836-44.
64. LallooUG,MalolepsyJ,KozmaD,KroftaK,AnkerstJ,JohansenB,et al.Budesonideandformoterolinasingleinhalerimprovesasthmacontrolcomparedwithincreasingthedoseofcorticosteroidinadultswithmild-to-moderateasthma.Chest2003;123(5):1480-7.
65. KipsJC,O’ConnorBJ,InmanMD,SvenssonK,PauwelsRA,O’ByrnePM.Along-termstudyoftheantiinflammatoryeffectoflow-dosebudesonideplusformoterolversushigh-dosebudesonideinasthma.Am J Respir Crit Care Med2000;161(3Pt1):996-1001.
66. StoloffSW,StempelDA,MeyerJ,StanfordRH,CarranaRosenweigJR.Improvedrefillpersistencewithfluticasonepropionateandsalmeterolinasingleinhalercomparedwithothercontrollertherapies.J Allergy Clin Immunol 2004;113(2):245-51.
67. RabeKF,PizichiniE,StallbergB,RomeroS,BalanatAM,Atien a T, et al.Budesonide/formoterolinasingleinhalerformaintenanceandreliefinmild-to-moderateasthma:arandomized,double-blindtrial.Chest2006;129(2):246-56.
68. O’ByrnePM,BisgaardH,GodardPP,PistolesiM,PalmqvistM,ZhuY,et al.Budesonide/formoterolcombinationtherapyasbothmaintenanceandrelievermedicationinasthma.Am J Respir Crit Care Med2005;171(2):129-36.
69. ScicchitanoR,AalbersR,UkenaD,ManjraA,FouquertL, Centanni S, et al.Efficacyandsafetyofbudesonide/formoterolsingleinhalertherapyversusahigherdoseofbudesonideinmoderatetosevereasthma.Curr Med Res Opin 2004;20(9):1403-18.
70. VogelmeierC,D’UrzoA,PauwelsR,MerinoJM,JaspalM,Boutet S, et al.Budesonide/formoterolmaintenanceandrelievertherapy:aneffectiveasthmatreatmentoption?Eur RespirJ2005;26(5):819-28.
71. NelsonJA,StraussL,SkowronskiM,CiufoR,NovakR,McFaddenER,Jr.Effectoflong-termsalmeteroltreatmentonexercise-inducedasthma.N Engl J Med1998;339(3):141-6.
72. PalmqvistM,PerssonG,LaerL,RosenborgJ,LarssonP,LotvallJ.Inhaleddry-powderformoterolandsalmeterolinasthmaticpatients:onsetofaction,durationofeffectandpotency.Eur RespirJ1997;10(11):2484-9.
73. vanNoordJA,SmeetsJJ,RaaijmakersJA,BommerAM,MaesenFP.Salmeterolversusformoterolinpatientswithmoderatelysevereasthma:onsetanddurationofaction.Eur RespirJ1996;9(8):1684-8.
74. NewnhamDM,McDevittDG,LipworthBJ.Bronchodilatorsubsensitivityafterchronicdosingwitheformoterolinpatientswithasthma.AmJ Med1994;97(1):29-37.
75. NelsonHS,WeissST,BleeckerER,YanceySW,DorinskyPM.TheSalmeterolMulticenterAsthmaResearchTrial:acomparisonofusualpharmacotherapyforasthmaorusualpharmacotherapyplussalmeterol.Chest2006;129(1):15-26.
76. Referencedeleted.
77. SullivanP,BekirS,JaffarZ,PageC,JefferyP,CostelloJ.Anti-inflammatoryeffectsoflow-doseoraltheophyllineinatopicasthma.Lancet1994;343(8904):1006-8.
78. KidneyJ,DomingueM,TaylorPM,RoseM,ChungKF,BarnesPJ.Immunomodulationbytheophyllineinasthma.Demonstrationbywithdrawaloftherapy.Am J Respir Crit Care Med1995;151(6):1907-14.
79. BarnesPJ.Theophylline:newperspectivesforanolddrug.Am J Respir Crit Care Med2003;167(6):813-8.
80. DahlR,LarsenBB,VengeP.Effectoflong-termtreatmentwithinhaledbudesonideortheophyllineonlungfunction,airwayreactivityandasthmasymptoms.Respir Med2002;96(6):432-8.
81. RivingtonRN,BouletLP,CoteJ,KreismanH,SmallDI,Alexander M, et al.EfficacyofUniphyl,salbutamol,andtheircombinationinasthmaticpatientsonhigh-doseinhaledsteroids.Am J Respir Crit Care Med1995;151(2Pt1):325-32.
82. EvansDJ,TaylorDA,ZetterstromO,ChungKF,O’ConnorBJ,BarnesPJ.Acomparisonoflow-doseinhaledbudesonideplustheophyllineandhigh-doseinhaledbudesonideformoderateasthma.N Engl J Med1997;337(20):1412-8.
83. UkenaD,HarnestU,SakalauskasR,MagyarP,VetterN,Steffen H, et al.Comparisonofadditionoftheophyllinetoinhaledsteroidwithdoublingofthedoseofinhaledsteroidinasthma.Eur RespirJ1997;10(12):2754-60.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA TREATMENTS 47
84. BabaK,SakakibaraA,YagiT,NiwaS,HattoriT,KoishikawaI, et al.Effectsoftheophyllinewithdrawalinwell-controlledasthmaticstreatedwithinhaledcorticosteroid.J Asthma 2001;38(8):615-24.
85. DaviesB,BrooksG,DevoyM.Theefficacyandsafetyofsalmeterolcomparedtotheophylline:meta-analysisofninecontrolledstudies.Respir Med1998;92(2):256-63.
86. WilsonAJ,GibsonPG,CoughlanJ.Longactingbeta-agonistsversustheophyllineformaintenancetreatmentofasthma.Cochrane Database Syst Rev2000;2.
87. AhnHC,LeeYC.Theclearanceoftheophyllineisincreasedduringtheinitialperiodoftuberculosistreatment.Int J Tuberc Lung Dis2003;7(6):587-91.
88. SzeflerSJ,NelsonHS.Alternativeagentsforanti-inflammatorytreatmentofasthma.J Allergy Clin Immunol1998;102(4Pt2):S23-35.
89. HumbertM,BeasleyR,AyresJ,SlavinR,HebertJ,BousquetJ,et al.Benefitsofomalizumabasadd-ontherapyinpatientswithseverepersistentasthmawhoareinadequatelycontrolleddespitebestavailabletherapy(GINA2002step4treatment):INNOVATE.Allergy2005;60(3):309-16.
90. MilgromH,FickRB,Jr.,SuJQ,ReimannJD,BushRK,Watrous ML, et al.Treatmentofallergicasthmawithmonoclonalanti-IgEantibody.rhuMAb-E25StudyGroup.N Engl J Med1999;341(26):1966-73.
91. BusseW,CorrenJ,LanierBQ,McAlaryM,Fowler-TaylorA,CioppaGD,et al.Omalizumab,anti-IgErecombinanthumanizedmonoclonalantibody,forthetreatmentofsevereallergicasthma.J Allergy Clin Immunol2001;108(2):184-90.
92. BousquetJ,WenzelS,HolgateS,LumryW,FreemanP,FoxH.Predictingresponsetoomalizumab,ananti-IgEantibody,inpatientswithallergicasthma.Chest2004;125(4):1378-86.
93. HolgateST,ChuchalinAG,HebertJ,LotvallJ,PerssonGB,ChungKF,et al.Efficacyandsafetyofarecombinantanti-immunoglobulinEantibody(omalizumab)insevereallergicasthma.Clin Exp Allergy2004;34(4):632-8.
94. DjukanovicR,WilsonSJ,KraftM,JarjourNN,SteelM,ChungKF,et al.Effectsoftreatmentwithanti-immunoglobulinEantibodyomalizumabonairwayinflammationinallergicasthma.Am J Respir Crit Care Med2004;170(6):583-93.
95. MashB,BheekieA,JonesPW.Inhaledvsoralsteroidsforadultswithchronicasthma.Cochrane Database Syst Rev 2000;2.
96. ToogoodJH,BaskervilleJ,JenningsB,LefcoeNM,JohanssonSA.Bioequivalentdosesofbudesonideandprednisoneinmoderateandsevereasthma.J Allergy Clin Immunol 1989;84(5Pt1):688-700.
97. Recommendationsforthepreventionandtreatmentofglucocorticoid-inducedosteoporosis.AmericanCollegeofRheumatologyTaskForceonOsteoporosisGuidelines.Arthritis Rheum1996;39(11):1791-801.
98. CampbellIA,DouglasJG,FrancisRM,PrescottRJ,ReidDM.Fiveyearstudyofetidronateand/orcalciumaspreventionandtreatmentforosteoporosisandfracturesinpatientswithasthmareceivinglongtermoraland/orinhaledglucocorticoids.Thorax2004;59(9):761-8.
99. EastellR,ReidDM,CompstonJ,CooperC,FogelmanI,Francis RM, et al.AUKConsensusGrouponmanagementofglucocorticoid-inducedosteoporosis:anupdate.J Intern Med 1998;244(4):271-92.
100.GuillevinL,PagnouxC,MouthonL.Churg-strausssyndrome.Semin Respir Crit Care Med2004;25(5):535-45.
101.KurosawaM.Anti-allergicdruguseinJapan--therationaleandtheclinicaloutcome.Clin Exp Allergy1994;24(4):299-306.
102.AaronSD,DalesRE,PhamB.Managementofsteroid-dependentasthmawithmethotrexate:ameta-analysisofrandomizedclinicaltrials.Respir Med1998;92(8):1059-65.
103.MarinMG.Low-dosemethotrexatesparessteroidusageinsteroid-dependentasthmaticpatients:ameta-analysis.Chest 1997;112(1):29-33.
104.DaviesH,OlsonL,GibsonP.Methotrexateasasteroidsparingagentforasthmainadults.Cochrane Database Syst Rev 2000;2.
105.LockSH,KayAB,BarnesNC.Double-blind,placebo-controlledstudyofcyclosporinAasacorticosteroid-sparingagentincorticosteroid-dependentasthma.Am J Respir Crit Care Med 1996;153(2):509-14.
106.BernsteinIL,BernsteinDI,DubbJW,FaifermanI,WallinB.Aplacebo-controlledmulticenterstudyofauranofininthetreatmentofpatientswithcorticosteroid-dependentasthma.AuranofinMulticenterDrugTrial.J Allergy Clin Immunol 1996;98(2):317-24.
107.NieropG,GijzelWP,BelEH,ZwindermanAH,DijkmanJH.Auranofininthetreatmentofsteroiddependentasthma:adoubleblindstudy.Thorax1992;47(5):349-54.
108.RicheldiL,FerraraG,FabbriL,LassersonT,GibsonP.Macrolidesforchronicasthma.Cochrane Database Syst Rev 2005(3):CD002997.
109.KishiyamaJL,ValacerD,Cunningham-RundlesC,SperberK,RichmondGW,AbramsonS,et al.Amulticenter,randomized,double-blind,placebo-controlledtrialofhigh-doseintravenousimmunoglobulinfororalcorticosteroid-dependentasthma.Clin Immunol1999;91(2):126-33.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

48 ASTHMA TREATMENTS
110.SalmunLM,BarlanI,WolfHM,EiblM,TwarogFJ,GehaRS, et al.Effectofintravenousimmunoglobulinonsteroidconsumptioninpatientswithsevereasthma:adouble-blind,placebo-controlled,randomizedtrial.J Allergy Clin Immunol 1999;103(5Pt1):810-5.
111.JakobssonT,CronerS,KjellmanNI,PetterssonA,VassellaC,BjorkstenB.Slightsteroid-sparingeffectofintravenousimmunoglobulininchildrenandadolescentswithmoderatelyseverebronchialasthma.Allergy1994;49(6):413-20.
112.AbramsonMJ,PuyRM,WeinerJM.Allergenimmunotherapyforasthma.Cochrane Database Syst Rev2003(4):CD001186.
113.BousquetJ,LockeyR,MallingHJ,Alvare-CuestaE,CanonicaGW,ChapmanMD,et al.Allergenimmunotherapy:therapeuticvaccinesforallergicdiseases.WorldHealthOrganiation.AmericanacademyofAllergy,AsthmaandImmunology.Ann Allergy Asthma Immunol1998;81(5Pt1):401-5.
114.HarrisonBD,StokesTC,HartGJ,VaughanDA,AliNJ,RobinsonAA.Needforintravenoushydrocortisoneinadditiontooralprednisoloneinpatientsadmittedtohospitalwithsevereasthmawithoutventilatoryfailure.Lancet1986;1(8474):181-4.
115.RoweBH,EdmondsML,SpoonerCH,DinerB,CamargoCA,Jr.Corticosteroidtherapyforacuteasthma.Respir Med 2004;98(4):275-84.
116.O’DriscollBR,KalraS,WilsonM,PickeringCA,CarrollKB,WoodcockAA.Double-blindtrialofsteroidtaperinginacuteasthma.Lancet1993;341(8841):324-7.
117.RodrigoG,RodrigoC,BurschtinO.Ameta-analysisoftheeffectsofipratropiumbromideinadultswithacuteasthma.AmJ Med1999;107(4):363-70.
118.TamaokiJ,ChiyotaniA,TagayaE,SakaiN,KonnoK.Effectoflongtermtreatmentwithoxitropiumbromideonairwaysecretioninchronicbronchitisanddiffusepanbronchiolitis.Thorax1994;49(6):545-8.
119.WeinbergerM,HendelesL.Theophyllineinasthma.N Engl J Med1996;334(21):1380-8.
120.HondrasMA,LindeK,JonesAP.Manualtherapyforasthma.Cochrane Database Syst Rev2005(2):CD001002.
121.ErnstE.Spinalmanipulationforasthma:asystematicreviewofrandomizedclinicaltrials.RespMed2009;103:1791-5.ErnstE.Spinalmanipulationforasthma:asystematicreviewofrandomizedclinicaltrials.Resp Med2009;103:1791-5.
122.SladerCA,ReddelHK,SpencerLM,BelousovaEG,ArmourCL,Bosnic-AnticevichSZ,ThienFC,JenkinsCR.Doubleblindrandomisedcontrolledtrialoftwodifferentbreathingtechniquesinthemanagementofasthma.Thorax2006Aug;61(8):651-6.
123.BisgaardH.Deliveryofinhaledmedicationtochildren.J Asthma1997;34(6):443-67.
124.PedersenS.Inhalersandnebulizers:whichtochooseandwhy.Respir Med1996;90(2):69-77.
125.DolovichMB,AhrensRC,HessDR,AndersonP,DhandR,RauJL,et al.Deviceselectionandoutcomesofaerosoltherapy:Evidence-basedguidelines:AmericanCollegeofChestPhysicians/AmericanCollegeofAsthma,Allergy,andImmunology.Chest2005;127(1):335-71.
126.ZarHJ,WeinbergEG,BinnsHJ,GallieF,MannMD.Lungdepositionofaerosol—acomparisonofdifferentspacers.Arch Dis Child2000;82(6):495-8.
127.CatesCJ,CrillyJA,RoweBH.Holdingchambers(spacers)versusnebulisersforbeta-agonisttreatmentofacuteasthma.Cochrane Database Syst Rev2006(2):CD000052.
128.ShapiroG,BronskyEA,LaForceCF,MendelsonL,PearlmanD,SchwartRH,et al.Dose-relatedefficacyofbudesonideadministeredviaadrypowderinhalerinthetreatmentofchildrenwithmoderatetoseverepersistentasthma.J Pediatr 1998;132(6):976-82.
129.AgertoftL,PedersenS.Arandomized,double-blinddosereductionstudytocomparetheminimaleffectivedoseofbudesonideTurbuhalerandfluticasonepropionateDiskhaler.J Allergy Clin Immunol1997;99(6Pt1):773-80.
130.PedersenS,O’ByrneP.Acomparisonoftheefficacyandsafetyofinhaledcorticosteroidsinasthma.Allergy1997;52(39):1-34.
131.AdamsNP,BestallJB,MaloufR,LassersonTJ,JonesPW.Inhaledbeclomethasoneversusplaceboforchronicasthma.Cochrane Database Syst Rev2005(1):CD002738.
132.PauwelsRA,PedersenS,BusseWW,TanWC,ChenYZ,OhlssonSV,et al.Earlyinterventionwithbudesonideinmildpersistentasthma:arandomised,double-blindtrial.Lancet 2003;361(9363):1071-6.
133.AdamsNP,BestallJC,JonesPW,LassersonTJ,GriffithsB,CatesC.Inhaledfluticasoneatdifferentdosesforchronicasthmainadultsandchildren.Cochrane Database Syst Rev 2005(3):CD003534.
134.PowellH,GibsonPG.Highdoseversuslowdoseinhaledcorticosteroidasinitialstartingdoseforasthmainadultsandchildren.Cochrane Database Syst Rev2004(2):CD004109.
135.Referencedeleted.
136.NielsenKG,BisgaardH.Theeffectofinhaledbudesonideonsymptoms,lungfunction,andcoldairandmethacholineresponsivenessin2-to5-year-oldasthmaticchildren.Am J Respir Crit Care Med2000;162(4Pt1):1500-6.
137.RoordaRJ,MezeiG,BisgaardH,MadenC.Responseofpreschoolchildrenwithasthmasymptomstofluticasonepropionate.J Allergy Clin Immunol2001;108(4):540-6.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA TREATMENTS 49
138.GuilbertTW,MorganWJ,ZeigerRS,MaugerDT,BoehmerSJ,SzeflerSJ,et al.Long-terminhaledcorticosteroidsinpreschoolchildrenathighriskforasthma.N Engl J Med 2006;354(19):1985-97.
139.BisgaardH,HermansenMN,LolandL,HalkjaerLB,BuchvaldF.Intermittentinhaledcorticosteroidsininfantswithepisodicwheezing.N Engl J Med2006;354(19):1998-2005.
140.PedersenS.Doinhaledcorticosteroidsinhibitgrowthinchildren?Am J Respir Crit Care Med2001;164(4):521-35.
141.AgertoftL,PedersenS.Effectoflong-termtreatmentwithinhaledbudesonideonadultheightinchildrenwithasthma.N Engl J Med2000;343(15):1064-9.
142.SharekPJ,BergmanDA.Beclomethasoneforasthmainchildren:effectsonlineargrowth.Cochrane Database Syst Rev 2000;2.
143.AgertoftL,PedersenS.Bonemineraldensityinchildrenwithasthmareceivinglong-termtreatmentwithinhaledbudesonide.Am J Respir Crit Care Med1998;157(1):178-83.
144.HoppRJ,DeganJA,BivenRE,KinbergK,GallagherGC.Longitudinalassessmentofbonemineraldensityinchildrenwithchronicasthma.Ann Allergy Asthma Immunol 1995;75(2):143-8.
145.SchliengerRG,JickSS,MeierCR.Inhaledcorticosteroidsandtheriskoffracturesinchildrenandadolescents.Pediatrics 2004;114(2):469-73.
146.vanStaaTP,BishopN,LeufkensHG,CooperC.Areinhaledcorticosteroidsassociatedwithanincreasedriskoffractureinchildren?Osteoporos Int2004;15(10):785-91.
147.vanStaaTP,CooperC,LeufkensHG,BishopN.Childrenandtheriskoffracturescausedbyoralcorticosteroids.JBoneMinerRes2003;18(5):913-8.
148.KempJP,OsurS,ShrewsburySB,HerjeNE,DukeSP,HardingSM,et al.Potentialeffectsoffluticasonepropionateonbonemineraldensityinpatientswithasthma:a2-yearrandomized,double-blind,placebo-controlledtrial.Mayo Clin Proc2004;79(4):458-66.
149.RouxC,KoltaS,DesfougeresJL,MininiP,BidatE.Long-termsafetyoffluticasonepropionateandnedocromilsodiumonboneinchildrenwithasthma.Pediatrics2003;111(6Pt1):e706-13.
150.ToddG,DunlopK,McNaboeJ,RyanMF,CarsonD,ShieldsMD.Growthandadrenalsuppressioninasthmaticchildrentreatedwithhigh-dosefluticasonepropionate.Lancet 1996;348(9019):27-9.
151.SelroosO,BackmanR,ForsenKO,LofroosAB,NiemistoM,PietinalhoA,et al.Localside-effectsduring4-yeartreatmentwithinhaledcorticosteroids--acomparisonbetweenpressurizedmetered-doseinhalersandTurbuhaler.Allergy 1994;49(10):888-90.
152.RandellTL,DonaghueKC,AmblerGR,CowellCT,FitgeraldDA,vanAsperenPP.Safetyofthenewerinhaledcorticosteroidsinchildhoodasthma.Paediatr Drugs 2003;5(7):481-504.
153.ShawL,al-DlaiganYH,SmithA.Childhoodasthmaanddentalerosion.ASDC J Dent Child2000;67(2):102-6,82.
154.KargulB,TanbogaI,ErgeneliS,KarakocF,DagliE.InhalermedicamenteffectsonsalivaandplaquepHinasthmaticchildren.J Clin Pediatr Dent 1998;22(2):137-40.
155.SzeflerSJ,PhillipsBR,MartineFD,ChinchilliVM,LemanskeRF,StrunkRC,et al.Characterizationofwithin-subjectresponsestofluticasoneandmontelukastinchildhoodasthma.J Allergy Clin Immunol2005;115(2):233-42.
156.Ostrom NK, Decotiis BA, Lincourt WR, Edwards LD, Hanson KM,CarranzaRosenzweigJR,et al.Comparativeefficacyandsafetyoflow-dosefluticasonepropionateandmontelukastinchildrenwithpersistentasthma.J Pediatr2005;147(2):213-20.
157.GarciaGarciaML,WahnU,GillesL,SwernA,ToiCA,PolosP.Montelukast,comparedwithfluticasone,forcontrolofasthmaamong6-to14-year-oldpatientswithmildasthma:theMOSAICstudy.Pediatrics2005;116(2):360-9.
158.NgD,SalvioF,HicksG.Anti-leukotrieneagentscomparedtoinhaledcorticosteroidsinthemanagementofrecurrentand/orchronicasthmainadultsandchildren.Cochrane Database Syst Rev2004(2):CD002314.
159.KempJP,DockhornRJ,ShapiroGG,NguyenHH,ReissTF,SeidenbergBC,et al.Montelukastoncedailyinhibitsexercise-inducedbronchoconstrictionin6-to14-year-oldchildrenwithasthma.J Pediatr1998;133(3):424-8.
160.VidalC,Fernande-OvideE,PineiroJ,NuneR,Gonale-QuintelaA.Comparisonofmontelukastversusbudesonideinthetreatmentofexercise-inducedbronchoconstriction.Ann Allergy Asthma Immunol2001;86(6):655-8.
161.PhipatanakulW,CroninB,WoodRA,EgglestonPA,ShihMC,SongL,et al.Effectofenvironmentalinterventiononmouseallergenlevelsinhomesofinner-cityBostonchildrenwithasthma.Ann Allergy Asthma Immunol2004;92(4):420-5.
162.Referencedeleted.
163.KnorrB,FranchiLM,BisgaardH,VermeulenJH,LeSouefP, Santanello N, et al.Montelukast,aleukotrienereceptorantagonist,forthetreatmentofpersistentasthmainchildrenaged2to5years.Pediatrics2001;108(3):E48.
164.BisgaardH,ZielenS,Garcia-GarciaML,JohnstonSL,GillesL,MentenJ,et al.Montelukastreducesasthmaexacerbationsin2-to5-year-oldchildrenwithintermittentasthma.Am J Respir Crit Care Med2005;171(4):315-22.
165.RussellG,WilliamsDA,WellerP,PriceJF.Salmeterolxinafoateinchildrenonhighdoseinhaledsteroids.Ann Allergy Asthma Immunol1995;75(5):423-8.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

50 ASTHMA TREATMENTS
166.MaloneR,LaForceC,NimmagaddaS,SchoafL,HouseK,EllsworthA,et al.Thesafetyoftwice-dailytreatmentwithfluticasonepropionateandsalmeterolinpediatricpatientswithpersistentasthma.Ann Allergy Asthma Immunol2005;95(1):66-71.
167.ZimmermanB,D’UrzoA,BerubeD.EfficacyandsafetyofformoterolTurbuhalerwhenaddedtoinhaledcorticosteroidtreatmentinchildrenwithasthma.Pediatr Pulmonol 2004;37(2):122-7.
168.MeijerGG,PostmaDS,MulderPG,vanAalderenWM.Long-termcircadianeffectsofsalmeterolinasthmaticchildrentreatedwithinhaledcorticosteroids.Am J Respir Crit Care Med 1995;152(6Pt1):1887-92.
169.BisgaardH.Long-actingbeta(2)-agonistsinmanagementofchildhoodasthma:Acriticalreviewoftheliterature.Pediatr Pulmonol2000;29(3):221-34.
170.BisgaardH.Effectoflong-actingbeta2agonistsonexacerbationratesofasthmainchildren.Pediatr Pulmonol 2003;36(5):391-8.
171.SimonsFE,GerstnerTV,CheangMS.Tolerancetothebronchoprotectiveeffectofsalmeterolinadolescentswithexercise-inducedasthmausingconcurrentinhaledglucocorticoidtreatment.Pediatrics1997;99(5):655-9.
172.KatRM,RachelefskyGS,SiegelS.Theeffectivenessoftheshort-andlong-termuseofcrystallizedtheophyllineinasthmaticchildren.J Pediatr1978;92(4):663-7.
173.BiermanCW,PiersonWE,ShapiroGG,FurukawaCT.Isauniformround-the-clocktheophyllinebloodlevelnecessaryforoptimalasthmatherapyintheadolescentpatient?Am JMed 1988;85(1B):17-20.
174.PedersenS.Treatmentofnocturnalasthmainchildrenwithasingledoseofsustained-releasetheophyllinetakenaftersupper.Clin Allergy1985;15(1):79-85.
175.MagnussenH,ReussG,JorresR.Methylxanthinesinhibitexercise-inducedbronchoconstrictionatlowserumtheophyllineconcentrationandinadose-dependentfashion.J Allergy Clin Immunol1988;81(3):531-7.
176.NassifEG,WeinbergerM,ThompsonR,HuntleyW.Thevalueofmaintenancetheophyllineinsteroid-dependentasthma.N Engl J Med1981;304(2):71-5.
177.BrennerM,BerkowitR,MarshallN,StrunkRC.Needfortheophyllineinseveresteroid-requiringasthmatics.Clin Allergy 1988;18(2):143-50.
178.EllisEF.Theophyllinetoxicity.J Allergy Clin Immunol1985;76(2Pt2):297-301.
179.TascheMJ,UijenJH,BernsenRM,deJongsteJC,vanDerWoudenJC.Inhaleddisodiumcromoglycate(DSCG)asmaintenancetherapyinchildrenwithasthma:asystematicreview.Thorax2000;55(11):913-20.
180.GuevaraJP,DucharmeFM,KerenR,NihtianovaS,ZorcJ.Inhaledcorticosteroidsversussodiumcromoglycateinchildrenandadultswithasthma.Cochrane Database Syst Rev 2006(2):CD003558.
181.SpoonerCH,SaundersLD,RoweBH.Nedocromilsodiumforpreventingexercise-inducedbronchoconstriction.Cochrane Database Syst Rev2000;2.
182.ArmenioL,BaldiniG,BardareM,BonerA,BurgioR,CavagniG, et al.Doubleblind,placebocontrolledstudyofnedocromilsodiuminasthma.Arch Dis Child1993;68(2):193-7.
183.KuuselaAL,MarenkM,SandahlG,SanderudJ,NikolajevK,PerssonB.Comparativestudyusingoralsolutionsofbambuteroloncedailyorterbutalinethreetimesdailyin2-5year-oldchildrenwithasthma.BambuterolMulticentreStudyGroup.Pediatr Pulmonol2000;29(3):194-201.
184.ZarkovicJP,MarenkM,ValovirtaE,KuuselaAL,SandahlG,Persson B, et al.One-yearsafetystudywithbambuteroloncedailyandterbutalinethreetimesdailyin2-12year-oldchildrenwithasthma.TheBambuterolMulticentreStudyGroup.Pediatr Pulmonol2000;29(6):424-9.
185.LonnerholmG,FoucardT,LindstromB.Oralterbutalineinchronicchildhoodasthma;effectsrelatedtoplasmaconcentrations.Eur J Respir Dis1984;134Suppl:205-10S.
186.WilliamsSJ,WinnerSJ,ClarkTJ.Comparisonofinhaledandintravenousterbutalineinacutesevereasthma.Thorax 1981;36(8):629-32.
187.DinhXuanAT,LebeauC,RocheR,FerriereA,ChaussainM.Inhaledterbutalineadministeredviaaspacerfullypreventsexercise-inducedasthmainyoungasthmaticsubjects:adouble-blind,randomized,placebo-controlledstudy.J Int Med Res1989;17(6):506-13.
188.FuglsangG,HertB,HolmEB.Noprotectionbyoralterbutalineagainstexercise-inducedasthmainchildren:adose-responsestudy.Eur RespirJ1993;6(4):527-30.
189.BengtssonB,FagerstromPO.Extrapulmonaryeffectsofterbutalineduringprolongedadministration.Clin Pharmacol Ther1982;31(6):726-32.
190.McDonaldNJ,BaraAI.Anticholinergictherapyforchronicasthmainchildrenovertwoyearsofage.Cochrane Database Syst Rev2003(3):CD003535.
191.AdamsNP,JonesPW.Thedose-responsecharacteristicsofinhaledcorticosteroidswhenusedtotreatasthma:anoverviewofCochranesystematicreviews.Respir Med 2006 Aug;100(8):1297-306.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA TREATMENTS 51
192.DeykinA,WechslerME,BousheyHA,ChinchilliVM,KunselmanSJ,CraigTJ,DiMangoE,FahyJV,KraftM,LeoneF,LazarusSC,LemanskeRFJr,MartinRJ,PesolaGR,PetersSP,SorknessCA,SzeflerSJ,IsraelE;NationalHeart,Lung,andBloodInstitute’sAsthmaClinicalResearchNetwork.Combinationtherapywithalong-actingbeta-agonistandaleukotrieneantagonistinmoderateasthma.Am J Respir Crit Care Med2007Feb1;175(3):228-34.
193.GibsonPG,PowellH,DucharmeFM.Differentialeffectsofmaintenancelong-actingbeta-agonistandinhaledcorticosteroidonasthmacontrolandasthmaexacerbations.J Allergy Clin Immunol2007Feb;119(2):344-50.
194.RabeKF,AtienzaT,MagyarP,LarssonP,JorupC,LallooUG.Effectofbudesonideincombinationwithformoterolforrelievertherapyinasthmaexacerbations:arandomisedcontrolled,double-blindstudy.Lancet2006Aug26;368(9537):744-53.
195.BleeckerER,YanceySW,BaitingerLA,EdwardsLD,KlotsmanM,AndersonWH,DorinskyPM.Salmeterolresponseisnotaffectedbybeta2-adrenergicreceptorgenotypeinsubjectswithpersistentasthma.J Allergy Clin Immunol2006Oct;118(4):809-16.
196.CalamitaZ,SaconatoH,PelaAB,AtallahAN.Efficacyofsublingualimmunotherapyinasthma:systematicreviewofrandomized-clinicaltrialsusingtheCochraneCollaborationmethod.Allergy2006Oct;61(10):1162-72.
197.ShaheenSO,NewsonRB,RaymanMP,WongAP,TumiltyMK,PhillipsJM,PottsJF,KellyFJ,WhitePT,BurneyPG.Randomised,doubleblind,placebo-controlledtrialofseleniumsupplementationinadultasthma.Thorax2007Jun;62(6):483-90.
198.ManochaR,MarksGB,KenchingtonP,PetersD,SalomeCM.Sahajayogainthemanagementofmoderatetosevereasthma:arandomisedcontrolledtrial.Thorax2002;57:110-5.
199.MurrayCS,WoodcockA,LangleySJ,MorrisJ,CustovicA;210.HollowayEA,WestRJ.IntegratedbreathingandrelaxationIFWINstudyteam.SecondarypreventionofasthmabytheuseofInhaledFluticasonepropionateinWheezyInfants(IFWIN):primarycare:arandomisedcontrolledtrial.Thorax 2007double-blind,randomised,controlledstudy.
200.de Benedictis FM, del Giudice MM, Foren a N, Decimo F, de BenedictisD,CapristoA.Lackoftolerancetotheprotectiveeffectofmontelukastinexercise-inducedbronchoconstrictioninchildren.Eur RespirJ2006Aug;28(2):291-5.
201.JatGC,MathewJL,SinghM.Treatmentwith400microgofinhaledbudesonidevs200microgofinhaledbudesonideandoralmontelukastinchildrenwithmoderatepersistentasthma:randomizedcontrolledtrial.Ann Allergy Asthma Immunol 2006 Sep;97(3):397-401.
202.BisgaardH,LeRouxP,BjamerD,DymekA,VermeulenJH,HultquistC.Budesonide/formoterolmaintenanceplusrelievertherapy:anewstrategyinpediatricasthma.Chest 2006 Dec;130(6):1733-43.
203.NelsonH,KempJ,BergerW,CorrenJ,CasaleT,DubeL,Walton-BowenK,LaValleeN,StepaniansM.Efficacyofzileutoncontrolled-releasetabletsadministeredtwicedailyinthetreatmentofmoderatepersistentasthma:a3-monthrandomizedcontrolledstudy.Ann Allergy Asthma Immuno 2007 Aug;99(2):178-84.
204.WatkinsPB,DubeLM,Walton-BowenK,CameronCM,KastenLE.Clinicalpatternofzileuton-associatedliverinjury:resultsofa12-monthstudyinpatientswithchronicasthma.Drug Saf 2007;30(9):805-15.
205.BatemanE,NelsonH,BousquetJ,KralK,SuttonL,OrtegaH,YanceyS.Meta-analysis:effectsofaddingsalmeteroltoinhaledcorticosteroidsonseriousasthma-relatedevents.Ann Intern Med2008Jul1;149(1):33-42.
206.BleeckerER,PostmaDS,LawranceRM,MeyersDA,AmbroseHJ,GoldmanM.EffectofADRB2polymorphismsonresponsetolong-actingbeta2-agonisttherapy:apharmacogeneticanalysisoftworandomisedstudies.Lancet 2007 Dec 22;370(9605):2118-25.
207.BousquetJ,CabreraP,BerkmanN,BuhlR,HolgateS,WenzelS,et al.Theeffectoftreatmentwithomalizumab,ananti-IgEantibody,onasthmaexacerbationsandemergencymedicalvisitsinpatientswithseverepersistentasthma.Allergy 2005;60(3):302-8.
208.JacobsenL,NiggemannB,DreborgS,FerdousiHA,HalkenS, Høst A, et al;(ThePATinvestigatorgroup).Specificimmunotherapyhaslong-termpreventiveeffectofseasonalandperennialasthma:10-yearfollow-uponthePATstudy.Allergy2007Aug;62(8):943-8.
209.PearlmanDS,ReesW,SchaeferK,HuangH,AndrewsWT.AnevaluationoflevalbuterolHFAinthepreventionofexercise-inducedbronchospasm.J Asthma2007Nov;44(9):729-33.
210.HollowayEA,WestRJ.Integratedbreathingandrelaxationtraining(thePapworthmethod)foradultswithasthmainprimarycare:arandomisedcontrolledtrial.Thorax 2007 Dec;62(12):1039-42.
211.LazarusSC,ChinchilliVM,RollingsNJ,BousheyHA,CherniackR,CraigTJ,et al.Smokingaffectsresponsetoinhaledcorticosteroidsorleukotrienereceptorantagonistsinasthma.Am J Respir Crit Care Med2007;175:783-90.
212.HaldarP,PavordID,ShawDE,BerryMA,ThomasM,BrightlingCE,WardlawAJ,GreenRH.Clusteranalysisandclinicalasthmaphenotypes.Am J Respir Crit Care Med.2008Aug1;178(3):218-24.
213.WeatherallM,JamesK,ClayJ,PerrinK,MasoliM,WijesingheM,BeasleyR.Dose-responserelationshipforriskofnon-vertebralfracturewithinhaledcorticosteroids.Clin Exp Allergy.2008Sep;38(9):1451-8.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

52 ASTHMA TREATMENTS
214.JaeschkeR,O’ByrnePM,MejzaF,NairP,LesniakW,BrozekJ,et al.Thesafetyoflong-actingbeta-agonistsamongpatientswithasthmausinginhaledcorticosteroids:systematicreviewandmetaanalysis.Am J Respir Crit Care Med.2008Nov15;178(10):1009-16.
215.CatesCJ,CatesMJ.Regulartreatmentwithsalmeterolforchronicasthma:seriousadverseevents.CochraneDatabaseofSystematicReviews2008,Issue3.Art.No.:CD006363
216.WenzelSE,BarnesPJ,BleeckerER,BousquetJ,BusseW,DahlénSE,et al;T03AsthmaInvestigators.Arandomized,double-blind,placebo-controlledstudyoftumornecrosisfactor-alphablockadeinseverepersistentasthma.Am J Respir Crit Care Med.2009Apr1;179(7):549-58.
217.PogsonZE,AntoniakMD,PaceySJ,LewisSA,BrittonJR,FogartyAW.Doesalowsodiumdietimproveasthmacontrol?Arandomizedcontrolledtrial.Am J Respir Crit Care Med.2008Jul15;178(2):132-8.
218.KellyHW,VanNattaML,CovarRA,TonasciaJ,GreenRP,StrunkRC;CAMPResearchGroup.Effectoflong-termcorticosteroiduseonbonemineraldensityinchildren:aprospectivelongitudinalassessmentinthechildhoodAsthmaManagementProgram(CAMP)study.Pediatrics.2008Jul;122(1):e53-61.
219.StrunkRC,BacharierLB,PhillipsBR,SzeflerSJ,ZeigerRS,ChinchilliVM,et al.;CARENetwork.Azithromycinormontelukastasinhaledcorticosteroid-sparingagentsinmoderate-to-severechildhoodasthmastudy.J Allergy Clin Immunol.2008Dec;122(6):1138-1144.e4.
220.WechslerME,KunselmanSJ,ChinchilliVM,BleeckerE,BousheyHA,CalhounWJ,et al.NationalHeart,LungandBloodInstitute’sAsthmaClinicalResearchNetworkEffectofbeta2-adrenergicreceptorpolymorphismonresponsetolongactingbeta2agonistinasthma(LARGEtrial):agenotype-stratified,randomised,placebo-controlled,crossovertrial.Lancet 2009;374(9703):1754-64.
221.WechslerME,WongDA,MillerMK,Lawrence-MiyasakiL.Churg-strausssyndromeinpatientstreatedwithomalizumab.Chest2009;136(2):507-18.
222.ErnstE.Homeopathy:whatdoesthe“best”evidencetellus?Med J Aust2010;192(8):458-60.
223.Milgrom,H,BergerW,NayakA,GuptaN,PollardS,McAlary M, et al.TreatmentofChildhoodAsthmawithAnti-ImmunoglobulinEAntibody(Omalizumab).Pediatrics2001;108(2):6-45
224.LemanskeR,NayakA,McAlaryM,EverhardF,Fowler-TaylorA,GuptaN.Omalizumabimprovesasthma-relatedqualityoflifeinchildrenwithallergicasthma.Pediatrics2002;110(5):e55-9
225.LanierB,BridgesT,KulusM,FowlerTaylorA,BerhaneI,VidaurreCF.Omalizumabforthetreatmentofexacerbationsinchildrenwithinadequatelycontrolledallergic(IgE-mediated)asthma.J Allergy Clinical Immunol2009;124(6):1210-1216
226.BossleyCJ,SaglaniS,KavanaghC,PayneDN,WilsonN,TsartsaliL,RosenthalM,Balfour-LynnIM,NicholsonAG,BushA.Corticosteroidresponsivenessandclinicalcharacteristicsinchildhooddifficultasthma. Eur Respir J.2009;34(5):1052-9;
227.WahnU,MartinC,FreemanP,BloggM,JimenezP.RelationshipbetweenpretreatmentspecificIgEandtheresponsetoomalizumabtherapy.Allergy2009;64(12):1780-7
228.ObaY,SalzmanGA.Cost-effectivenessanalysisofomalizumabinadultsandadolescentswithmoderate-to-severeallergicasthma.J Allergy Clin Immunol2004;114(2):265-9.
229.BusseWW,MorganWJ,GergenPJ,MitchellHE,GernJE,LiuAH, et al.Randomizedtrialofomalizumab(anti-IgE)forasthmaininner-citychildren.N Engl J Med.2011Mar17;364(11):1005-15.
230.WelshEJ,CatesCJ.Formoterolversusshort-actingbeta-agonistsasreliefmedicationforadultsandchildrenwithasthma.Cochrane Database Syst Rev.2010Sep8;(9):CD008418.
231.PetersSP,KunselmanSJ,IcitovicN,MooreWC,PascualR,AmeredesBTetal.NationalHeart,Lung,andBloodInstituteAsthmaClinicalResearchNetwork.Tiotropiumbromidestep-uptherapyforadultswithuncontrolledasthma.N Engl J Med 2010;363:1715-26.
232.KerstjensHA,DisseB,Schroder-BaboW,BantjeTA,GahlemannM,SigmundR,EngelM,vanNoordJA.Tiotropiumimproveslungfunctioninpatientswithsevereuncontrolledasthma:arandomizedcontrolledtrial.J Allergy Clin Immunol.2011Aug;128(2):308-14.
233.BatemanED,KornmannO,SchmidtP,PivovarovaA,EngelM,FabbriLM.TiotropiumisnoninferiortosalmeterolinmaintainingimprovedlungfunctioninB16-Arg/Argpatientswithasthma.J Allergy Clin Immunol.2011Aug;128(2):315-22.
234.KempJ,ArmstrongL,WanY,AlagappanVK,OhlssenD,PascoeS.Safetyof formoterolinadultsandchildrenwithasthma:ameta-analysis.Ann Allergy Asthma Immunol.2011Jul;107(1):71-8.
235.HananiaNA,AlpanO,HamilosDL,etal.OmalizumabinsevereallergicasthmaInadequatelycontrolledwithstandardtherapy:arandomizedtrial.Ann Internal Med 2011;154:573-82.
236.PosadzkiP,ErnstE.Yogaforasthma?Asystematicreviewofrandomizedclinicaltrials.J Asthma.2011Aug;48(6):632-9.
237.LavoriniF,FontanaGA.Targetingdrugstotheairways:Theroleofspacerdevices.Expert Opin Drug Deliv2009;6:91-102.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA TREATMENTS 53
238.ZeigerRS,MaugerD,BacharierLB,GuilbertTW,MartinezFD,LemanskeRFJr,etal;CARENetworkoftheNationalHeart,Lung,andBloodInstitute.Dailyorintermittentbudesonideinpreschoolchildrenwithrecurrentwheezing.N Engl J Med.2011Nov24;365(21):1990-2001
239.GuilbertTW,MaugerDT,AllenDB,ZeigerRS,LemanskeRFJr,SzeflerSJ,etal;ChildhoodAsthmaResearchandEducationNetworkoftheNationalHeart,Lung,andBloodInstitute.Growthofpreschoolchildrenathighriskforasthma2yearsafterdiscontinuationoffluticasone. J Allergy Clin Immunol.2011Nov;128(5):956-63.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

54 ASTHMA TREATMENTSCOPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

CHAPTER
4
ASTHMA MANAGEMENT
ANDPREVENTION
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

56 ASTHMA MANAGEMENT AND PREVENTION
Asthmahasasignificantimpactonindividuals,theirfamilies,andsociety.Althoughthereisnocureforasthma,appropriatemanagementthatincludesapartnershipbetweenthephysicianandthepatient/familymostoftenresultsintheachievementofcontrol.
Thegoalsforsuccessfulmanagementofasthmaareto:
• Achieveandmaintaincontrolofsymptoms• Maintainnormalactivitylevels,includingexercise• Maintainpulmonaryfunctionasclosetonormalas• possible• Preventasthmaexacerbations• Avoidadverseeffectsfromasthmamedications• Preventasthmamortality.
Thesegoalsfortherapyreflectanunderstandingofasthmaasachronicinflammatorydisorderoftheairwayscharacterizedbyrecurrentepisodesofwheezing,breathlessness,chesttightness,andcoughing.Clinicalstudieshaveshownthatasthmacanbeeffectivelycontrolledbyinterveningtosuppressandreversetheinflammationaswellastreatingthebronchoconstrictionandrelatedsymptoms.Furthermore,earlyinterventiontostopexposuretotheriskfactorsthatsensitizedtheairwaymayhelpimprovethecontrolofasthmaandreducemedicationneeds.Experienceinoccupationalasthmaindicatesthatlong-standingexposuretosensitizingagentsmayleadtoirreversibleairflowlimitation.
Themanagementofasthmacanbeapproachedindifferentways,dependingontheavailabilityofthevariousformsofasthmatreatmentandtakingintoaccountculturalpreferencesanddifferinghealthcaresystems.Therecommendationsinthischapterreflectthecurrentscientificunderstandingofasthma.Theyarebasedasfaraspossibleoncontrolledclinicalstudies,andthetextreferencesmanyofthesestudies.Forthoseaspectsoftheclinicalmanagementofasthmathathavenotbeenthesubjectofspecificclinicalstudies,recommendationsarebasedonliteraturereview,clinicalexperience,andexpertopinionofprojectmembers.
Therecommendationsforasthmamanagementarelaidoutinfiveinterrelatedcomponentsoftherapy:
1.DevelopPatient/DoctorPartnership2.IdentifyandReduceExposuretoRiskFactors3.Assess,Treat,andMonitorAsthma4.ManageAsthmaExacerbations5.SpecialConsiderations.
KEY POINTS:
• Theeffectivemanagementofasthmarequiresthedevelopmentofapartnershipbetweenthepersonwithasthmaandhisorherhealthcareprofessional(s)(andparents/caregivers,inthecaseofchildrenwithasthma).
• Theaimofthispartnershipisguidedself-management—thatis,togivepeoplewithasthmatheabilitytocontroltheirownconditionwithguidancefromhealthcareprofessionals.
• Thepartnershipisformedandstrengthenedaspatientsandtheirhealthcareprofessionalsdiscussandagreeonthegoalsoftreatment,developapersonalized,writtenasthmaactionplanincludingself-monitoring,andperiodicallyreviewthepatient’streatmentandlevelofasthmacontrol.
• Educationshouldbeanintegralpartofallinteractionsbetweenhealthcareprofessionalsandpatients,andisrelevanttoasthmapatientsofallages.
• Personalwrittenasthmaactionplanshelpindividualswithasthmamakechangestotheirtreatmentinresponsetochangesintheirlevelofasthmacontrol,asindicatedbysymptomsand/orpeakexpiratoryflow,inaccordancewithwrittenpredeterminedguidelines.
Theeffectivemanagementofasthmarequiresthedevelopmentofapartnershipbetweenthepersonwithasthmaandhisorherhealthcareprofessional(s)(andparents/caregiversinthecaseofchildrenwithasthma).Theaimofthispartnershipistoenablepatientswithasthmatogaintheknowledge,confidence,andskillstoassumeamajorroleinthemanagementoftheirasthma.Thepartnershipisformedandstrengthenedaspatientsandtheirhealthcareprofessionalsdiscussandagreeonthegoalsoftreatment,developapersonalized,writtenasthmaactionplanincludingself-monitoring,andperiodicallyreviewthepatient’streatmentandlevelofasthmacontrol(Figure 4.1-1).
COMPONENT 1: DEFINITION
INTRODUCTION COMPONENT 1: DEVELOP PATIENT/DOCTOR PARTNERSHIP
INTRODUCTION
CHAPTER 4: ASTHMA MANAGEMENT AND PREVENTIONCOPY
RIGHTE
D MAT
ERIA
L - D
O NOT
ALTE
R OR R
EPRODUCE

ASTHMA MANAGEMENT AND PREVENTION 57
Thisapproachiscalledguidedself-managementandhasbeenshowntoreduceasthmamorbidityinbothadults(Evidence A)andchildren(Evidence A).Anumberofspecificsystemsofguidedself-managementhavebeendeveloped1-10foruseinawiderangeofsettings:primarycare1,4,6,hospitals2,3,7,10,andemergencydepartments8.Internet-basedhomemonitoring340,372,andmobilephones395 havebeenshowntobesuccessfulmodestoimproveasthmacontrol.Self-managementprogramshavebeentestedindiversegroups,includingcommunityhealthworkers371,pregnantwomenwithasthma11,childrenandadolescents12,13,andinmulti-racialpopulations14.
Guidedself-managementmayinvolvevaryingdegreesofindependence,rangingbroadlyfrompatient-directedself-managementinwhichpatientsmakechangeswithoutreferencetotheircaregiver,butinaccordancewithapriorwrittenactionplan,todoctor-directedself-managementinwhichpatientsrelyfollowawrittenactionplan,butrefermostmajortreatmentchangestotheirphysicianatthe
timeofplannedorunplannedconsultations.Cochranesystematic reviews13,15-18haveexaminedtheroleofeducationandself-managementstrategiesinthecareofasthmapatients.
Educationshouldbeanintegralpartofallinteractionsbetweenhealthcareprofessionalsandpatients,andisrelevanttoasthmapatientsofallages.Althoughthefocusofeducationforsmallchildrenwillbeontheparentsandcaregivers,childrenasyoungas3yearsofagecanbetaughtsimpleasthmamanagementskills.Adolescentsmayhavesomeuniquedifficultiesregardingadherence
thatmaybehelpedthroughpeersupportgroupeducationinadditiontoeducationprovidedbythehealthcareprofessional12 butregionalissuesandthedevelopmentalstageofthechildrenmayaffecttheoutcomesofsuchprograms373.
Figure 4.1-2outlinesthekeyfeaturesandcomponentsofanasthmaeducationprogram.Theinformationandskillstrainingrequiredbyeachpersonmayvary,andtheirability
orwillingnesstotakeresponsibilitysimilarlydiffers.Thusallindividualsrequirecertaincoreinformationandskills,butmosteducationmustbepersonalizedandgiventothepersoninanumberofsteps.Socialandpsychologicalsupportmayalsoberequiredtomaintainpositivebehavioralchange.
Good communicationisessentialasthebasisforsubsequentgoodcompliance/adherence19-22,414(Evidence B).Keyfactorsthatfacilitategoodcommunicationare23:
• Acongenialdemeanor(friendliness,humor,andattentiveness)
• Engagingininteractivedialogue• Givingencouragementandpraise
ASTHMA EDUCATION
Figure 4.1-1. Essential Features of the Doctor-Patient Partnership to Achieve Guided Self-Management in Asthma
• Education• Joint setting of goals• Self-monitoring. The person with asthma is taught to combine
assessment of asthma control with educated interpretation ofkey symptoms
• Regular review of asthma control, treatment, and skills by ahealth care professional
• Written action plan. The person with asthma is taught whichmedications to use regularly and which to use as needed, andhow to adjust treatment in response to worsening asthma control
• Self-monitoring is integrated with written guidelines for both thelong-term treatment of asthma and the treatment of asthmaexacerbations.
Figure 4.1-2. Education and the Patient Doctor PartnershipGoal: To provide the person with asthma, their family, and other caregivers with suitable information and training so that they can keep well and adjust treatment according to a medication plan developed with the health care professional.
Key Components:o Focus on the development of the partnershipo Acceptance that this is a continuing processo A sharing of informationo Full discussion of expectationso Expression of fears and concerns
Key Components:o Diagnosiso Difference between “relievers” and “controllers”o Potential side effects of medicationso Use of inhaler deviceso Prevention of symptoms and attackso Signs that suggest asthma is worsening and actions to takeo Monitoring control of asthmao How and when to seek medical attention
The person then requires:o A written asthma action plano Regular supervision, revision, reward, and reinforcement
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

58 ASTHMA MANAGEMENT AND PREVENTION
• Empathy,reassurance,andprompthandlingofanyconcerns
• Givingofappropriate(personalized)information• Elicitingsharedgoals• Feedbackandreview
Teaching health care professionals to improve their communication skills can result in measurably better outcomes–includingincreasedpatientsatisfaction,betterhealth,andreduceduseofhealthcare–andthesebenefitsmaybeachievedwithoutanyincreaseinconsultationtimes24.Studieshavealsoshownthatpatientscanbetrainedtobenefitmorefromconsultations.Patientstaughthowtogiveinformationtodoctorsinaclearermanner,andhowtoseekinformationandchecktheirunderstandingofwhatthedoctorhadtoldthemgainedsignificantimprovementsincompliancewithtreatmentrecommendations25.Layeducatorscanberecruitedandtrainedtodeliveradiscreteareaofrespiratorycare(forexample,asthmaself-managementeducation)withcomparableoutcomestothoseachievedbyprimarycarebasedpracticenurses362(Evidence B).
At the Initial Consultation
Earlyintheconsultationthepersonwithasthmaneedsinformationaboutthediagnosisandsimpleinformationaboutthetypesoftreatmentavailable,therationaleforthespecifictherapeuticinterventionsbeingrecommended,andstrategiesforavoidingfactorsthatcauseasthmasymptoms374.Differentinhalerdevicescanbedemonstrated,andthepersonwithasthmaencouragedtoparticipateinthedecisionastowhichismostsuitableforthem.SomeofthesedevicesandtechniquesfortheiruseareillustratedontheGINAWebsite(http://www.ginasthma.org).Criteriaforinitialselectionofinhalerdeviceincludedeviceavailabilityandcost,patientskills,andpreferencesofthehealthprofessionalandpatient26-28.Patientsshouldbegivenadequateopportunitytoexpresstheirexpectationsofboththeirasthmaanditstreatment.Afrankappraisalshouldbemadeofhowfartheirexpectationsmayormaynotbemet,andagreementshouldbemadeaboutspecificgoalsfortherapy.
Attheinitialconsultation,verbalinformationshouldbesupplementedbytheprovisionofwrittenorpictorial29, 30 informationaboutasthmaanditstreatment.TheGINAWebsite(http://www.ginasthma.org)containspatienteducationalmaterials,aswellaslinkstoseveralasthmawebsites.Thepatientandhisorherfamilyshouldbeencouragedtomakeanoteofanyquestionsthatarisefromreadingthisinformationorasaresultoftheconsultation,andshouldbegiventimetoaddresstheseduringthenextconsultation.
Personal Written Asthma Action Plans
Personalwrittenasthmaactionplanshelpindividualswithasthmamakechangestotheirtreatmentinresponsetochangesintheirlevelofasthmacontrol,asindicatedbysymptomsand/orpeakexpiratoryflow,inaccordancewithwrittenpredeterminedguidelines23,31,32 .
Theeffectsweregreatestwheretheinterventioninvolvedeachofthefollowingelements:education,self-monitoring,regularreview,andpatient-directedmanagementusingawrittenasthmaactionplan(Evidence A).Withinthesestudies,theeffectswerealsogreaterwhentheactionplansthemselvesbothsteppedupinhaledglucocorticosteroidsandaddedoralglucocorticosteroids,andforpeakflow-basedplans,whentheywerebasedonpersonalbestratherthanpercentpredictedpeakflow32.Patientsexperienceaone-thirdtotwo-thirdsreductioninhospitalizations,emergencyroomvisits,unscheduledvisitstothedoctorforasthma,misseddaysofwork,andnocturnalwakening.Ithasbeenestimatedthattheimplementationofaself-managementprogramin20patientspreventsonehospitalization,andsuccessfulcompletionofsuchaprogrambyeightpatientspreventsoneemergencydepartmentvisit16-18,23.Lessintensiveinterventionsthatinvolveself-managementeducationbutnotawrittenplanarelesseffective15.Theefficacyissimilarregardlessofwhetherpatientsself-adjusttheirmedicationsaccordingtoanindividualwrittenplanoradjustmentsof medication are made by a doctor15(Evidence B).Thus,patientswhoareunabletoundertakeguidedself-managementcanstillachievebenefitfromastructuredprogramofregularmedicalreview.Althoughinteractivecomputerizedasthmaeducationprogramsmayimprovepatientasthmaknowledgeandsymptoms,theireffectonobjective clinical outcomes is less consistent353. ExamplesofwrittenasthmaactionplansthathavebeenrecommendedcanbefoundonseveralWebsites(UKNationalAsthmaCampaignPlan,www.asthma.org.uk;InternationalAsthmaManagementPlan“ZoneSystem,”www.nhlbisupport.com/asthma/index.html;NewZealand“CreditCard”System,www.asthmanz.co.nz.Anexampleofthecontentsforanasthmaplanforpatientstomaintaincontrolofasthma,andrespondtoworseningasthma,isshowninFigure 4.1-3.
Follow-Up and Review
Follow-upconsultationsshouldtakeplaceatregularintervals.Atthesevisits,thepatient’squestionsarediscussed,andanyproblemswithasthmaanditsinitialtreatmentarereviewed.Patientsshouldbeaskedtodemonstratetheirinhalerdevicetechniqueateveryvisit,withcorrectionandre-checkingifitisinadequate33,375.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 59
Follow-upconsultationsshouldalsoincludecheckingtheperson’sadherence/compliancetothemedicationplanandrecommendationsforreducingexposuretoriskfactors.Ifthepatienthasbeenaskedtokeepadiaryofsymptoms(andwhereappropriate,homepeakflowrecordings)this
shouldalsobereviewedregularly.Afteraperiodofinitialtraining,thefrequencyofhomepeakflowandsymptommonitoringdependsinpartonthelevelofcontroloftheperson’sasthma.Routinefollow-upvisitsmaybeaneffectivetimetoreviewthewrittenasthmaactionplananditsunderstanding354.Educationalmessagesshouldbereviewedandrepeatedoraddedtoifnecessary.Asinglepageprompttoclinicianshasbeenshowntoimprovetheprovisionofpreventivecaretochildrenwithasthmaduringofficevisits341.Telehealthcarefollow-upisunlikelytobenefitinmildasthmabutmaybeofbenefitinthosewithseverediseaseatriskofhospitaladmission397. Improving Adherence
Althoughinterventionsforenhancingmedicationadherencehavebeendeveloped363,studiesofadultsandchildrenwithasthma34haveshownthataround50%ofthoseonLong-termtherapyfailtotakemedicationsasdirectedatleastpartofthetime.Patientconcernaboutside-effectsofinhaledglucocorticosteroidswhetherrealorperceivedmayinfluenceadherence342.Non-adherencemaybedefinedinanonjudgmentalwayasthefailureoftreatmenttobetakenasagreeduponbythepatientandthehealthcareprofessional. Non-adherencemaybeidentifiedbyprescriptionmonitoring,pillcounting,ordrugassay,butataclinicallevelitisbestdetectedbyaskingabouttherapyinawaythatacknowledgesthelikelihoodofincompleteadherence(e.g.,“Sothatwemayplantherapy,doyoumindtellingmehowoftenyouactuallytakethemedicine?”).Shortquestionnairescanassistwithidentificationofpooradherence376.Providingadherenceinformationtocliniciansdoesnotimproveuseofinhaledglucocorticosteroidamongpatientswithasthmaunlesscliniciansaresufficientlyinterestedinadherencetoviewthedetailsofthismedicationuse398.Specificdrugandnon-drugfactorsinvolvedinnon-adherencearelistedinFigure 4.1-4.
Self-Management in Children
Childrenwithasthma(withthehelpoftheirparents/caregivers)alsoneedtoknowhowtomanagetheirowncondition.Simpleeducationalinterventions(designedtoteachself-managementskills)amongchildrenadmittedtothehospitalwithasthmahavebeenshowntosignificantlyreducethereadmissionrateandreducemorbidity13.Asystematicreviewfoundthateducationalprogramsfortheself-managementofasthmainchildrenandadolescentsledtoimprovementsinlungfunctionandfeelingsofself-control,andreducedabsencesfromschool,thenumberofdayswithrestrictedactivity,andthenumberofemergencydepartmentvisits13,343.Forchildren,symptom-basedactionplansaremoreeffectivethanthosebasedonpeakflows355.School-basedasthmaeducationimprovesknowledgeof
Figure 4.1-3 Example of Contents of Written AsthmaAction Plan to Maintain Asthma Control
Your Regular Treatment:1. Each day take ___________________________2. Before exercise, take _____________________
WHEN TO INCREASE TREATMENTAssess your level of Asthma ControlIn the past week have you had:
Daytime asthma symptoms more than 2 times ? No YesActivity or exercise limited by asthma? No YesWaking at night because of asthma? No YesThe need to use your [rescue medication] more than 2 times? No YesIf you are monitoring peak flow, peak flow less than______? No Yes
if you answered YeS to three or more of these questions, your asthma isuncontrolled and you may need to step up your treatment.
HOW TO INCREASE TREATMENTSTEP-UP your treatment as follows and assess improvement every day:_________________________________ [Write in next treatment step here] Maintain this treatment for _____________ days [specify number]
WHEN TO CALL THE DOCTOR/CLINIC.Call your doctor/clinic: _______________ [provide phone numbers]If you don’t respond in _________ days [specify number]____________________________ [optional lines for additional instruction]
EMERGENCY/SEVERE LOSS OF CONTROL3If you have severe shortness of breath, and can only speak in short sentences,3 If you are having a severe attack of asthma and are frightened,3 If you need your reliever medication more than every 4 hours and are not
improving.1. Take 2 to 4 puffs ___________ [reliever medication] 2. Take ____mg of ____________ [oral glucocorticosteroid]3. Seek medical help: Go to ________________; Address______________
Phone: _______________________4. Continue to use your _________[reliever medication] until you are able
to get medical help.
Figure 4.1-4. Factors Involved in Poor Adherence
Drug factors
Difficulties with inhaler devices
Awkward regimes (e.g., four times daily ormultiple drugs)
Side effectsCost of medicationDislike of medicationDistant pharmacies
Non-drug factors
Misunderstanding or lack of instructionFears about side effectsDissatisfaction with health care professionalsUnexpressed/undiscussed fears or concernsInappropriate expectationsPoor supervision, training, or follow-upAnger about condition or its treatmentUnderestimation of severityCultural issuesStigmatizationForgetfulness or complacencyAttitudes toward ill healthReligious issues
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

60 ASTHMA MANAGEMENT AND PREVENTION
asthma,self-efficacy,andself-managementbehaviors377.Acomprehensiveschool-basedprogramforadolescentsandacademicdetailingfortheirphysicianswasassociatedwithsignificantlyimprovedasthmaoutcomesincludingreducedhospitalizations399.
THE EDUCATION OF OTHERS
Theeducationofthegeneralpublicaboutasthmaishelpfulinthatitenablesmembersofthepublictorecognizeasthmasymptomsandtheirconsequencesandencouragesthosewithasthmatoseekmedicalattentionandfollowtheirasthmamanagementprogram.Greaterawarenessofasthmaisalsolikelytohelpdispelmisconceptionsthatmayexistabouttheconditionandreducefeelingsofstigmatizationonthepartofpatients.
Specificadviceaboutasthmaanditsmanagementshouldbeofferedtoschoolteachersandphysicaleducationinstructors,andseveralorganizationsproducematerialsforthispurpose.Schoolsmayneedadviceonimprovingtheenvironmentandairqualityforchildrenwithasthma35.Itisalsohelpfulforemployerstohaveaccesstoclearadviceaboutasthma.Mostoccupationsareassuitableforthosewithasthmaasforthosewithout,buttheremaybesomecircumstanceswherecautionisneeded.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 61
KEY POINTS: • Pharmacologicinterventiontotreatestablished
asthmaishighlyeffectiveincontrollingsymptomsandimprovingqualityoflife.However,measurestopreventthedevelopmentofasthma,asthmasymptoms,andasthmaexacerbationsbyavoidingorreducingexposuretoriskfactorsshouldbeimplementedwhereverpossible.
• Atthistime,fewmeasurescanberecommendedforpreventionofasthmabecausethedevelopmentofthediseaseiscomplexandincompletelyunderstood.
• Asthmaexacerbationsmaybecausedbyavarietyofriskfactors,sometimesreferredtoas"triggers",includingallergens,viralinfections,pollutants,anddrugs.
• Reducingapatient’sexposuretosomecategoriesofriskfactorsimprovesthecontrolofasthmaandreducesmedicationneeds.
• Theearlyidentificationofoccupationalsensitizersandtheremovalofsensitizedpatientsfromanyfurtherexposureareimportantaspectsofthemanagementofoccupationalasthma.
Althoughpharmacologicinterventiontotreatestablishedasthmaishighlyeffectiveincontrollingsymptomsandimprovingqualityoflife,measurestopreventthedevelopmentofasthma,asthmasymptoms,andasthmabyavoidingorreducingexposuretoriskfactorsshouldbeimplementedwhereverpossible36.Atthistime,fewmeasurescanberecommendedforpreventionofasthmabecausethedevelopmentofthediseaseiscomplexandincompletelyunderstood.Thisareaisafocusofintensiveresearch,butuntilsuchmeasuresaredevelopedpreventioneffortsmustprimarilyfocusonpreventionofasthmasymptomsandattacks.
Measurestopreventasthmamaybeaimedatthepreventionofallergicsensitization(i.e.,thedevelopmentof
atopy,likelytobemostrelevantprenatallyandperinatally),orthepreventionofasthmadevelopmentinsensitizedpeople.Otherthanpreventingtobaccoexposurebothin uteroandafterbirth,therearenoprovenandwidelyacceptedinterventionsthatcanpreventthedevelopmentofasthma.
Allergicsensitzationcanoccurprenatally37,38.Thereiscurrentlyinsufficientinformationonthecriticaldosesandtimingofallergenexposuretopermitinterventioninthisprocess,andnostrategiescanberecommendedtopreventallergicsensitizationprenatally415.Prescriptionofanantigen-avoidancediettoahigh-riskwomanduringpregnancyisunlikelytoreducesubstantiallyherriskofgivingbirthtoanatopicchild39.Moreover,suchadietmayhaveanadverseeffectonmaternaland/orfetalnutrition.
Theroleofdiet,particularlybreast-feeding,inrelationtothedevelopmentofasthmahasbeenextensivelystudiedand,ingeneral,infantsfedformulasofintactcow’smilkorsoyproteincomparedwithbreastmilkhaveahigherincidenceofwheezingillnessesinearlychildhood40.Exclusivebreast-feedingduringthefirstmonthsafterbirthisassociatedwithlowerasthmaratesduringchildhood41. The“hygienehypothesis”ofasthma,thoughcontroversial,hasledtothesuggestionthatstrategiestopreventallergicsensitizationshouldfocusonredirectingtheimmuneresponseofinfantstowardaTh1,nonallergicresponseoronmodulatingTregulatorcells42,butsuchstrategiescurrentlyremainintherealmofhypothesisandrequirefurtherinvestigation.Theroleofprobioticsinthepreventionofallergyandasthmaisalsounclear43.Exposuretocatshasbeenshowntoreduceriskofatopyinsomestudies44. Exposuretotobaccosmokebothprenatallyandpostnatallyisassociatedwithmeasurableharmfuleffects,includingeffectsonlungdevelopment45andagreaterriskofdevelopingwheezingillnessesinchildhood46.Althoughthereislittleevidencethatmaternalsmokingduringpregnancyhasaneffectonallergicsensitization47,passivesmokingincreasestheriskofallergicsensitizationinchildren47,48.Bothprenatalandpostnatalmaternalsmokingisproblematic49.Pregnantwomenandparentsofyoungchildrenshouldbeadvisednottosmoke(Evidence B).
Onceallergicsensitizationhasoccurred,therearetheoreticallystillopportunitiestopreventtheactual
COMPONENT 2: IDENTIFY AND REDUCEEXPOSURE TO RISK FACTORS
INTRODUCTION
ASTHMA PREVENTION
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

62 ASTHMA MANAGEMENT AND PREVENTION
developmentofasthma.WhetherH1-antagonists(antihistamines)50,51orallergen-specificimmunotherapy52,53 canpreventthedevelopmentofasthmainchildrenwhohaveotheratopicdiseasesremainsanareaofinvestigation,andtheseinterventionscannotberecommendedforwideadoptioninclinicalpracticeatthistime.
Asthmaexacerbationsmaybecausedbyavarietyoffactors,sometimesreferredtoas“triggers,”includingallergens,viralinfections400,pollutants,anddrugs.Reducingapatient’sexposuretosomeofthesecategoriesofriskfactors(e.g.,smokingcessation,reducingexposuretosecondhandsmoke,reducingoreliminatingexposuretooccupationalagentsknowntocausesymptoms,andavoidingfoods/additives/drugsknowntocausesymptoms)improvesthecontrolofasthmaandreducesmedicationneeds.Inthecaseofotherfactors(e.g.,allergens,viralinfectionsandpollutants),measureswherepossibleshouldbetakentoavoidthese.Becausemanyasthmapatientsreacttomultiplefactorsthatareubiquitousintheenvironment,avoidingthesefactorscompletelyisusuallyimpracticalandverylimitingtothepatient.Thus,medicationstomaintainasthmacontrolhaveanimportantrolebecausepatientsareoftenlesssensitivetotheseriskfactorswhentheirasthmaisundergoodcontrol.Patientswithwell-controlledasthmaarelesslikelytoexperienceexacerbationsthanthosewhoseasthmaisnotwell-controlled364.
Indoor Allergens
Amongthewidevarietyofallergensourcesinhumandwellingsaredomesticmites,furredanimals,cockroaches,andfungi.However,thereisconflictingevidenceaboutwhethermeasurestocreatealow-allergenenvironmentinpatients'homesandreduceexposuretoindoorallergensareeffectiveatreducingasthmasymptoms54,55.Themajorityofsingleinterventionshavefailedtoachieveasufficientreductioninallergenloadtoleadtoclinicalimprovement55-57.Itislikelythatnosingleinterventionwillachievesufficientbenefitstobecosteffective.However,amonginner-citychildrenwithatopicasthma,anindividualized,home-based,comprehensiveenvironmentalinterventiondecreasedexposuretoindoorallergensandresultedinreducedasthma-associatedmorbidity58.Moreproperlypoweredandwell-designedstudiesofcombinedallergen-reductionstrategiesinlargegroupsofpatientsareneeded.
Figure 4.2-1: Effectiveness of Avoidance Measuresfor Some Indoor Allergens*
Measure Evidenceof effect
on allergenlevels
Evidence of clinical
benefit
House dust mitesEncase bedding in impermeable covers Some None
(adults)Some
(children)
Wash bedding in the hot cycle (55-60oC) Some NoneReplace carpets with hard flooring Some NoneAcaricides and/or tannic acid Weak NoneMinimize objects that accumulate dust None NoneVacuum cleaners with integral HEPA filterand double-thickness bags
Weak None
Remove, hot wash, or freeze soft toys None None
PetsRemove cat/dog from the home Weak NoneKeep pet from main living areas/bedrooms Weak NoneHEPA-filter air cleaners Some NoneWash pet Weak NoneReplace carpets with hard flooring None NoneVacuum cleaners with integral HEPA filterand double-thickness bags
None None
*Adapted from Custovic A, Wijk RG. The effectiveness of measures to change theindoor environment in the treatment of allergic rhinitis and asthma: ARIA update(in collaboration with GA(2)LEN). Allergy 2005;60(9):1112-1115.
Domestic mites.Domesticmiteallergyisauniversalhealthproblem59.Sincemitesliveandthriveinmanysitesthroughoutthehouse,theyaredifficulttoreduceandimpossibletoeradicate(Figure 4.2-1).Nosinglemeasureislikelytoreduceexposuretomiteallergens,andsinglechemicalandphysicalmethodsaimedatreducingmiteallergensarenoteffectiveinreducingasthmasymptomsinadults55,60-62(Evidence A).Onestudyshowedsomeefficacyofmattressencasingatreducingairwayhyperresponsivenessinchildren63(Evidence B).Anintegratedapproachincludingbarriermethods,dustremoval,andreductionofmicrohabitatsfavorabletomiteshasbeensuggested,althoughitsefficacyatreducingsymptomshasonlybeenconfirmedindeprivedpopulationswithaspecificenvironmentalexposure58(Evidence B)andarecommendationforitswidespreadusecannotbemade.
Furred animals.Completeavoidanceofpetallergensisimpossible,astheallergensareubiquitousandcanbefoundinmanyenvironmentsoutsidethehome64,includingschools65,publictransportation,andcat-freebuildings66.Althoughremovalofsuchanimalsfromthehomeisencouraged,evenafterpermanentremovaloftheanimal
PREVENTION OF ASTHMA SYMPTOMS AND EXACERBATIONS
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 63
itcanbemanymonthsbeforeallergenlevelsdecrease67 andtheclinicaleffectivenessofthisandotherinterventionsremainsunproven(Figure 4.2-1).
Cockroaches.Avoidancemeasuresforcockroachesincludeeliminatingsuitableenvironments(restrictinghavensbycaulkingandsealingcracksintheplasterworkandflooring,controllingdampness,andreducingtheavailabilityoffood),restrictingaccess(sealingentrysourcessuchasaroundpaperworkanddoors),chemicalcontrol,andtraps.However,thesemeasuresareonlypartiallyeffectiveinremovingresidualallergens68 (Evidence C).
Fungi.Fungalexposurehasbeenassociatedwithexacerbationsfromasthmaandthenumberoffungalsporescanbestbereducedbyremovingorcleaningmold-laden objects69.Intropicalandsubtropicalclimates,fungimaygrowonthewallsofthehouseduetowaterseepageandhumidity.Toavoidthis,thewallscouldbetiledorcleanedasnecessary.Airconditionersanddehumidifiersmaybeusedtoreducehumiditytolevelslessthan50%andtofilterlargefungalspores.However,airconditioningandsealingofwindowshavealsobeenassociatedwithincreasesinfungalandhousedustmiteallergens70.
Outdoor Allergens
Outdoorallergenssuchaspollensandmoldsareimpossibletoavoidcompletely.Exposuremaybereducedbyclosingwindowsanddoors,remainingindoorswhenpollenandmoldcountsarehighest,andusingairconditioningifpossible.Somecountriesuseradio,television,andtheInternettoprovideinformationonoutdoorallergenlevels.Theimpactofthesemeasuresisdifficulttoassess.
Indoor Air Pollutants
Themostimportantmeasureincontrollingindoorairpollutantsistoavoidpassiveandactivesmoking.Secondhandsmokeincreasesthefrequencyandseverityofsymptomsinchildrenwithasthma.Parents/caregiversofchildrenwithasthmashouldbeadvisednottosmokeandnottoallowsmokinginroomstheirchildrenuse.Inadditiontoincreasingasthmasymptomsandcausinglong-termimpairmentsinlungfunction,activecigarettesmokingreducestheefficacyofinhaledandsystemicglucocorticosteroids71,72(Evidence B).Asthmapatientswhosmoke,andarenottreatedwithinhaledglucocorticosteroids,haveagreaterdeclineinlungfunctionthanasthmaticpatientswhodonotsmoke378.Smokingcessationneedstobevigorouslyencouragedforallpatientswithasthmawhosmoke.
Othermajorindoorairpollutantsincludenitricoxide,nitrogenoxides,carbonmonoxide,carbondioxide,sulfurdioxide,formaldehyde,andbiologicals(endotoxin)73.Installationofnon-polluting,moreeffectiveheating(heatpump,woodpelletburner,fluedgas)inthehomesofchildrenwithasthmadoesnotsignificantlyimprovelungfunctionbutdoessignificantlyreducesymptomsofasthma,daysoffschool,healthcareutilization,andvisitstoapharmacist365.
Outdoor Air Pollutants
Severalstudieshavesuggestedthatoutdoorpollutantsaggravateasthmasymptoms74, 356,possiblyhavinganadditiveeffectwithallergenexposure75.Outbreaksofasthmaexacerbationshavebeenshowntooccurinrelationshiptoincreasedlevelsofairpollution,andthismayberelatedtoageneralincreaseinpollutantlevelsortoanincreaseinspecificallergenstowhichindividualsaresensitized76-78.Mostepidemiologicalstudiesshowasignificantassociationbetweenairpollutants–suchasozone,nitrogenoxides,acidicaerosols,andparticulatematter–andsymptomsorexacerbationsofasthma.Onoccasion,certainweatherandatmosphericconditions,e.g.,thunderstorms78favorthedevelopmentofasthmaexacerbationsbyavarietyofmechanisms,includingdustandpollution,increasesinrespirableallergens,andchangesintemperature/humidity.
Avoidance of unfavorable environmental conditions isusuallyunnecessaryforpatientswhoseasthmaiscontrolled.Forpatientswithasthmathatisdifficulttocontrol,practicalstepstotakeduringunfavorableenvironmentalconditionsincludeavoidingstrenuousphysicalactivityincoldweather,lowhumidity,orhighairpollution;avoidingsmokingandsmoke-filledrooms;andstayingindoorsinaclimate-controlledenvironment.
Occupational Exposures
Occupationalexposuresaccountforasubstantialproportionofadultasthmaincidence357.Theearlyidentificationofoccupationalsensitizersandtheremovalofsensitizedpatientsfromanyfurtherexposureareimportantaspectsofthemanagementofoccupationalasthma(Evidence B).Onceapatienthasbecomesensitizedtoanoccupationalallergen,thelevelofexposurenecessarytoinducesymptomsmaybeextremelylow,andresultingexacerbationsbecomeincreasinglysevere.Attemptstoreduceoccupationalexposurehavebeensuccessfulespeciallyinindustrialsettings,andsomepotentsensitizers,suchassoycastorbean,havebeenreplacedbylessallergenicsubstances80(Evidence B).Preventionoflatexsensitizationhasbeenmadepossiblebythe
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

64 ASTHMA MANAGEMENT AND PREVENTION
productionofhypoallergenicgloves,whicharepowderfreeandhavealowerallergencontent81,82(Evidence C).Althoughmoreexpensivethanuntreatedgloves,theyarecosteffective.
Food and Food Additives
Foodallergyasanexacerbatingfactorforasthmaisuncommonandoccursprimarilyinyoungchildren.Foodavoidanceshouldnotberecommendeduntilanallergyhasbeenclearlydemonstrated(usuallybyoralchallenges)83.Whenfoodallergyisdemonstrated,foodallergenavoidancecanreduceasthmaexacerbations84(Evidence D).Sulfites(commonfoodanddrugpreservativesfoundinsuchfoodsasprocessedpotatoes,shrimp,driedfruits,beer,andwine)haveoftenbeenimplicatedincausingsevereasthmaexacerbationsbutthelikelihoodofareactionisdependentonthenatureofthefood,thelevelofresidualsulfite,thesensitivityofthepatient,theformofresidualsulfiteandthemechanismofthesulfite-inducedreaction85.Theroleofotherdietarysubstances—includingtheyellowdyetartrazine,benzoate,andmonosodiumglutamate—inexacerbatingasthmaisprobablyminimal;confirmationoftheirrelevancerequiresdouble-blindchallengebeforemakingspecificdietaryrestrictions.
Drugs
Somemedicationscanexacerbateasthma.Aspirinandothernonsteroidalanti-inflammatorydrugscancausesevereexacerbationsandshouldbeavoidedinpatientswithahistoryofreactingtotheseagents86.Thereissomeevidencethatexposuretoacetaminophenincreasestheriskofasthmaandwheezinginchildren401 and adults but furtherstudiesareneeded379.
Beta-blockerdrugsadministeredorallyorintraocularlymayexacerbatebronchospasm(Evidence A)andclosemedicalsupervisionisessentialwhentheseareusedbypatientswithasthma87.Betablockershaveaprovenbenefitinthemanagementofpatientswithacutecoronarysyndromesandforsecondarypreventionofcoronaryevents.Datasuggestthatpatientswithasthmawhoreceivenewermorecardio-selectivebetablockerswithin24hoursofhospitaladmissionforanacutecoronaryeventhavelowerin-hospitalmortalityrates366, 367.
Influenza Vaccination
Patientswithmoderatetosevereasthmashouldbeadvisedtoreceiveaninfluenzavaccinationeveryyear88 oratleastwhenvaccinationofthegeneralpopulationisadvised.However,routineinfluenzavaccinationofchildren89 and adults90withasthmadoesnotappearto
protectthemfromasthmaexacerbationsorimproveasthmacontrol.Inactivatedinfluenzavaccinesareassociatedwithfewsideeffectsandaresafetoadministertoasthmaticadultsandchildrenovertheageof3years,includingthosewithdifficult-to-treatasthma91.Therearedatatosuggestthatintranasalvaccinationinchildrenunderage3maybeassociatedwithanincreasedincidenceofasthmaexacerbations92.
Obesity
Increasesinbodymassindex(BMI)havebeenassociatedwithincreasedprevalenceofasthma93.Weightreductioninobesepatientswithasthma,includingbybariatricsurgery,hasbeenhasbeendemonstratedtoimprovelungfunction,symptoms,morbidity,andhealthstatus94(Evidence B).
Emotional Stress
Emotionalstressmayleadtoasthmaexacerbationsinchildren402andadults.Extremeemotionalexpressions(laughing,crying,anger,orfear)canleadtohyperventilationandhypocapniathatcancauseairwaynarrowing95,96.Panicattacks,thatarerarebutnotexceptionalinsomepatientswithasthma,haveasimilareffect97,98.However,itisimportanttonotethatasthmaisnotprimarilyapsychosomaticdisorder.
Other Factors That May Exacerbate Asthma
Rhinitis,sinusitis,andpolyposisarefrequentlyassociatedwithasthmaandneedtobetreated.Inchildren,antibiotictreatmentofbacterialsinusitishasbeenshowntoreducetheseverityofasthma99.However,sinusitisandasthmamaysimplycoexist.Apartfromsinusitis,thereislittleevidencethatbacterialinfectionsexacerbateasthma.Gastroesophagealrefluxcanexacerbateasthma,especiallyinchildren,andasthmasometimesimproveswhentherefluxiscorrected100,101.Manywomencomplainthattheirasthmaisworseatthetimeofmenstruation,andpremenstrualexacerbationshavebeendocumented102.Similarly,asthmamayimprove,worsen,orremainunchangedduringpregnancy103.Arandomizedclinicaltrialofaself-regulation,telephonecounselinginterventionemphasizingsexandgenderrolefactorsinthemanagementofasthmaindicatedthataprogramwithafocusonasthmamanagementproblemsparticulartowomencansignificantlyassistfemaleasthmapatients358.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 65
KEY POINTS:
• Thegoalofasthmatreatment,toachieveandmaintainclinicalcontrol,canbereachedinamajorityofpatientswithapharmacologicinterventionstrategydevelopedinpartnershipbetweenthepatient/familyandthedoctor.
• Treatmentshouldbeadjustedinacontinuouscycledrivenbythepatients’asthmacontrolstatus.Ifasthmaisnotcontrolledonthecurrenttreatmentregimen,treatmentshouldbesteppedupuntilcontrolisachieved.Whencontrolismaintainedforatleastthreemonths,treatmentcanbesteppeddown.
• Intreatment-naïvepatientswithpersistentasthma,treatmentshouldbestartedatStep 2, or, if very symptomatic(uncontrolled),atStep 3.ForSteps 2 through5, a variety of controller medications are available.
• Ateachtreatmentstep,relievermedicationshouldbeprovidedforquickreliefofsymptomsasneeded.
• Ongoingmonitoringisessentialtomaintaincontrolandtoestablishtheloweststepanddoseoftreatmenttominimizecostandmaximizesafety.
Thegoalofasthmatreatment,toachieveandmaintainclinicalcontrol,canbereachedinamajorityofpatients104,344 withapharmacologicinterventionstrategydevelopedinpartnershipbetweenthepatient/familyandthedoctor.Eachpatientisassignedtooneoffive“treatmentsteps”dependingontheircurrentlevelofcontrolandtreatmentisadjustedinacontinuouscycledrivenbychangesintheirasthmacontrolstatus.Thiscycleinvolves:
• AssessingAsthmaControl• TreatingtoAchieveControl• MonitoringtoMaintainControl
InthisComponent,thiscycleisdescribedforlong-termtreatmentofasthma.TreatmentforexacerbationsisdetailedinComponent4.
Eachpatientshouldbeassessedtoestablishhisorhercurrenttreatmentregimen,adherencetothecurrentregimen,andlevelofasthmacontrol.Asimplifiedschemeforrecognizingcontrolled,partlycontrolled,anduncontrolledasthmainagivenweekisprovidedinFigure 4.3-1.Thisisaworkingschemebasedoncurrentopinionandhasnotbeenvalidated.Severalcompositecontrolmeasures(e.g.,AsthmaControlTest105,AsthmaControlQuestionnaire106-108,AsthmaTherapyAssessmentQuestionnaire109,AsthmaControlScoringSystem110)havebeendevelopedandarebeingvalidatedforvariousapplications,includingusebyhealthcareproviderstoassessthestateofcontroloftheirpatients'asthmaandbypatientsforself-assessmentsaspartofawrittenpersonalasthmaactionplan.Uncontrolledasthmamayprogresstothepointofanexacerbation,andimmediatesteps,describedinComponent4,shouldbetakentoregaincontrol.
Thepatient’scurrentlevelofasthmacontrolandcurrenttreatmentdeterminetheselectionofpharmacologictreatment.Forexample,ifasthmaisnotcontrolledonthecurrenttreatmentregimen,treatmentshouldbesteppedupuntilcontrolisachieved.Ifcontrolhasbeenmaintainedforatleastthreemonths,treatmentcanbesteppeddownwiththeaimofestablishingtheloweststepanddoseoftreatmentthatmaintainscontrol(seeMonitoringtoMaintainControlbelow).Ifasthmaispartlycontrolled,anincreaseintreatmentshouldbeconsidered,subjecttowhethermoreeffectiveoptionsareavailable(e.g.,increaseddoseoranadditionaltreatment),safetyandcostofpossibletreatmentoptions,andthepatient’ssatisfactionwiththelevelofcontrolachieved.TheschemepresentedinFigure 4.3-2 is basedupontheseprinciples,buttherangeandsequenceofmedicationsusedineachclinicalsettingwillvarydependingonlocalavailability(forcostorotherreasons),acceptability,andpreference.
COMPONENT 3: ASSESS, TREAT, AND MONITOR ASTHMA
INTRODUCTION
ASSESSING ASTHMA CONTROL
TREATING TO ACHIEVE CONTROL
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

66 ASTHMA MANAGEMENT AND PREVENTION
Treatment Steps for Achieving Control
Mostofthemedicationsavailableforasthmapatients,whencomparedwithmedicationsusedforotherchronicdiseases,haveextremelyfavorabletherapeuticratios.Eachsteprepresentstreatmentoptionsthat,althoughnotofidenticalefficacy,arealternativesforcontrollingasthma.Steps 1 to 5provideoptionsofincreasingefficacy,exceptfor Step 5whereissuesofavailabilityandsafetyinfluencetheselectionoftreatment.Step 2istheinitialtreatmentformosttreatment-naïvepatientswithpersistentasthmasymptoms.Ifsymptomsattheinitialconsultationsuggestthatasthmaisseverelyuncontrolled(Figure 4.3-1),treatmentshouldbecommencedatStep 3.
Ateachtreatmentstep,arelievermedication(rapid-onset bronchodilator,eithershort-actingorlong-acting)shouldbeprovidedforquickreliefofsymptoms.However,regularuseofrelievermedicationisoneoftheelementsdefininguncontrolledasthma,andindicatesthatcontrollertreatmentshouldbeincreased.Thus,reducingoreliminatingtheneedforrelievertreatmentisbothanimportantgoalandmeasureofsuccessoftreatment.ForSteps 2through5, a variety of controller medications are
available.
Step 1: as-needed reliever medication. Step 1 treatment withanas-neededrelievermedicationisreservedforuntreatedpatientswithoccasionaldaytimesymptoms(cough,wheeze,dyspneaoccurringtwiceorlessperweek,orlessfrequentlyifnocturnal)ofshortduration(lastingonlyafewhours)comparablewithcontrolledasthma(Figure 4.3-1).Betweenepisodes,thepatientisasymptomaticwithnormallungfunctionandthereisnonocturnalawakening.Whensymptomsaremorefrequent,and/orworsenperiodically,patientsrequireregularcontrollertreatment(seeSteps 2orhigher)inadditiontoas-needed reliever medication111-113(Evidence B).
ForthemajorityofpatientsinStep 1, a rapid-acting inhaled β2-agonististherecommendedrelievertreatment114(Evidence A).Aninhaledanticholinergic,short-actingoralβ2-agonist,orshort-actingtheophyllinemaybeconsideredasalternatives,althoughtheyhaveasloweronsetofactionandhigherriskofsideeffects(Evidence A).
Figure 4.3-1. LEVELS OF ASTHMA CONTROL
A. Assessment of current clinical control (preferably over 4 weeks)
Characteristic Controlled (All of the following)
Partly Controlled(Any measure present)
Uncontrolled
Daytime symptoms None (twice or less/week)
More than twice/week Three or more features of partly controlled asthma*†
Limitation of activities None Any
Nocturnal symptoms/awakening
None Any
Need for reliever/ rescue treatment
None (twice or less/week)
More than twice/week
Lung function (PEF or FEV1)‡
Normal <80% predicted or personal best (if known)
B. Assessment of Future Risk (risk of exacerbations, instability, rapid decline in lung function, side-effects)
Features that are associated with increased risk of adverse events in the future include:Poor clinical control, frequent exacerbations in past year*, ever admission to critical care for asthma, low FEV1, exposure to cigarette smoke, high dose medications
* Any exacerbation should prompt review of maintenance treatment to ensure that it is adequate† By definition, an exacerbation in any week makes that an uncontrolled asthma week‡ Without administration of bronchodilator. Lung function is not a reliable test for children 5 years and younger.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 67
Management Approach Based On ControlFor Children Older Than 5 Years, Adolescents and Adults
Controlleroptions***
* ICS = inhaled glucocorticosteroids**= Receptor antagonist or synthesis inhibitors *** = Preferred controller options are shown in shaded boxes
Treatment StepsAs needed rapid-acting β2-agonistAs needed rapid-acting β2-agonistLow-dose ICS pluslong-acting β2-agonistSelect one
Leukotrienemodifier**Select oneMedium-orhigh-dose ICSMedium-or high-doseICS plus long-actingβ2-agonistLow-dose ICS plusleukotriene modifierLow-dose ICS plussustained releasetheophylline
To Step 3 treatment,select one or more To Step 4 treatment,add eitherAsthma educationEnvironmental control
Low-dose inhaledICS* Oral glucocorticosteroid(lowest dose)Anti-IgEtreatmentLeukotrienemodifierSustained releasetheophylline
ControlledMaintain and find lowest controlling stepPartly controlledConsider stepping up to gain controlUncontrolledStep up until controlledExacerbationTreat as exacerbation
Treatment ActionLevel of ControlReduce
Reduce IncreaseI nc re ase
2Step1Step 3Step 4Step 5Step
Management Approach Based On ControlFor Children Older Than 5 Years, Adolescents and Adults
Controlleroptions***
* ICS = inhaled glucocorticosteroids**= Receptor antagonist or synthesis inhibitors
Treatment Steps
As needed rapid-acting β2-agonist As needed rapid-acting β2-agonist
Low-dose ICS pluslong-acting β2-agonist
Select one
Leukotrienemodifier**
Select one
Medium-orhigh-dose ICS
Medium-or high-doseICS plus long-acting
β2-agonist
Low-dose ICS plusleukotriene modifier
Low-dose ICS plussustained release
theophylline
To Step 3 treatment,select one or more
To Step 4 treatment,add either
Asthma education. Environmental control.(If step-up treatment is being considered for poor symptom control, first check inhaler technique, check adherence, and confirm symptoms are due to asthma.)
Low-dose inhaledICS*
Oral glucocorticosteroid(lowest dose)
Anti-IgEtreatment
Leukotrienemodifier
Sustained releasetheophylline
Controlled Maintain and find lowest controlling step
Partly controlled Consider stepping up to gain control
Uncontrolled Step up until controlled
Exacerbation Treat as exacerbation
Treatment ActionLevel of Control
Red
uce
Reduce Increase
Incr
ease
2Step1Step 3Step 4Step 5Step
*** = Recommended treatment (shaded boxes) based on group mean data. Individual patient needs, preferences, and circumstances (including costs) should be considered.
Figure 4.3-2.
For management of asthma in children 5 years and younger, refer to the Global Strategy for the Diagnosis and Management of Asthma in Children 5 Years and Younger, available at http://www.ginasthma.org.
Alternative reliever treatments include inhaled anticholinergics, short-acting oral β2-agonists, some long-acting β2-agonists, and short-acting theophylline.Regular dosing with short and long-acting β2-agonists is not advised unless accompanied by regular use of an inhaled glucocorticorsteriod.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

68 ASTHMA MANAGEMENT AND PREVENTION
Exercise-induced bronchoconstriction.Physicalactivityisanimportantcauseofasthmasymptomsformostasthmapatients,andforsomeitistheonlycause.However,exercise-inducedbronchoconstrictionoftenindicatesthatthepatient’sasthmaisnotwellcontrolled,andsteppingupcontrollertherapygenerallyresultsinthereductionofexercise-relatedsymptoms.Forthosepatientswhostillexperienceexercise-inducedbronchoconstrictiondespiteotherwisewell-controlledasthma,andforthoseinwhomexercise-inducedbronchoconstrictionistheonlymanifestationofasthma,arapid-actinginhaledβ2-agonist(short-orlong-acting),takenpriortoexerciseortorelievesymptomsthatdevelopafterexercise,isrecommended115.Aleukotrienemodifier116,345 or cromone117 are alternatives (Evidence A).Trainingandsufficientwarm-upalsoreducetheincidenceandseverityofexercise-inducedbronchoconstriction118,119(Evidence B).Informationontreatmentofexercise-inducedasthmainathletescanbefoundinaJointTaskForceReportpreparedbytheEuropeanRespiratorySociety,theEuropeanAcademyofAllergyandClinicalImmunology,andGA(2)LEN359andtheWorldAnti-DopingAgencywebsite(www.wada-ama.org).
Step 2: Reliever medication plus a single controller. Treatment Steps 2through5, combine an as-needed relievertreatmentwithregularcontrollertreatment.At Step 2,a low-dose inhaled glucocorticosteroid is recommendedastheinitialcontrollertreatmentforasthmapatientsofallages111,120(Evidence A).Equivalentdosesofinhaledglucocorticosteroids,someofwhichmaybegivenasasingledailydose,areprovidedinFigure 3-1 for adults and in Figure 3-4forchildrenolderthan5years.
Alternative controller medications include leukotriene modifiers121-123(Evidence A),appropriateparticularlyforpatientswhoareunableorunwillingtouseinhaledglucocorticosteroids,orwhoexperienceintolerablesideeffectssuchaspersistenthoarsenessfrominhaledglucocorticosteroidtreatmentandthosewithconcomitantallergicrhinitis124,125(Evidence C).
Otheroptionsareavailablebutnotrecommendedforroutineuseasinitialorfirst-linecontrollersinStep 2.Sustained-release theophyllinehasonlyweakanti-inflammatoryandcontrollerefficacy126-130(Evidence B)andiscommonlyassociatedwithsideeffectsthatrangefromtrivialtointolerable131,132.Cromones (nedocromil sodium and sodium cromoglycate)havecomparativelylowefficacy,thoughafavorablesafetyprofile133-136(Evidence A).
Step 3: Reliever medication plus one or two controllers. At Step 3,therecommendedoptionforchildren403 and adolescents and adults is to combine a low-dose of inhaled glucocorticosteroid with an inhaled long-
acting ß2-agonist,eitherinacombinationinhalerdeviceorasseparatecomponents137-144(Evidence A).Becauseoftheadditiveeffectofthiscombination,thelow-doseofglucocorticosteroidisusuallysufficient,andneedonlybeincreasedifcontrolisnotachievedwithin3or4monthswiththisregimen(Evidence A).Thelong-actingβ2-agonistformoterol,whichhasarapidonsetofactionwhethergivenalone145,146,148orincombinationinhalerwithbudesonide149,hasbeenshowntobeaseffectiveasshort-actingβ2-agonistinacuteasthmaexacerbation.Howeveritsuseasmonotherapyasarelievermedicationisstronglydiscouragedsinceitmustalwaysbeusedinassociationwithaninhaledglucocorticosteroid.
Forallchildrenbutparticularlythose5yearsandyounger,combinationtherapyhasbeenlesswellstudiedandtheadditionofalong-actingβ2-agonistmaynotbeaseffectiveasincreasingthedoseofinhaledglucocorticosteroidsinreducingexacerbations151-153.However,theinterpretationofsomestudiesisproblematicasnotallchildrenreceivedconcurrentinhaledglucocorticosteroids152,153.
Ifacombinationinhalercontainingformoterolandbudesonideisselected,itmaybeusedforbothrescueandmaintenance.Thisapproachhasbeenshowntoresultinreductionsinexacerbationsandimprovementsinasthmacontrolinadultsandadolescentsatrelativelylow doses of treatment154-157(Evidence A).Whetherthisapproachcanbeemployedwithothercombinationsofcontrollerandrelieverrequiresfurtherstudy.
Anotheroptionforbothadultsandchildren,buttheonerecommendedforchildren158, is to increase to a medium-dose of inhaled glucocorticosteroids104,159-161 (Evidence A).Forpatientsofallagesonmedium-orhigh-doseofinhaledglucocorticosteroiddeliveredbyapressurizedmetered-doseinhaler,useofaspacerdeviceisrecommendedtoimprovedeliverytotheairways,reduceoropharyngealsideeffects,andreducesystemicabsorption162-164(Evidence A).
AnotheroptionatStep 3istocombinealow-doseinhaledglucocorticosteroidwithleukotrienemodifiers165-173 (Evidence A).Alternatively,theuseofsustained-releasetheophyllinegivenatlow-dosemaybeconsidered129 (Evidence B).Theseoptionshavenotbeenfullystudiedinchildren5yearsandyounger.
Step 4: Reliever medication plus two or more controllers. TheselectionoftreatmentatStep 4dependsonpriorselectionsatSteps 2 and 3.However,theorderinwhichadditionalmedicationsshouldbeaddedisbased,asfaraspossible,uponevidenceoftheirrelativeefficacyinclinicaltrials.Wherepossible,patientswhoarenot
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 69
controlled on Step 3treatmentsshouldbereferred to a health professional with expertise in the management of asthmaforinvestigationofalternativediagnosesand/orcausesofdifficult-to-treatasthma.
ThepreferredtreatmentatStep 4 is to combine a medium-or high-dose of inhaled glucocorticosteroid with a long-acting inhaled β2-agonist.However,inmostpatients,theincreasefromamedium-toahigh-doseofinhaledglucocorticosteroidprovidesrelativelylittleadditionalbenefit104,159-161,174(Evidence A),andthehigh-doseisrecommendedonlyonatrialbasisfor3to6monthswhencontrolcannotbeachievedwithmedium-doseinhaledglucocorticosteroidcombinedwithalong-actingβ2-agonistand/orathirdcontroller(e.g.leukotrienemodifiersorsustained-releasetheophylline)130,175,346 (Evidence B).Prolongeduseofhigh-doseinhaledglucocorticosteroidsisalsoassociatedwithincreasedpotentialforadverseeffects.Atmedium-andhigh-doses,twice-dailydosingisnecessaryformostbutnotallinhaledglucocorticosteroids176(Evidence A).Withbudesonide,efficacymaybeimprovedwithmorefrequentdosing(fourtimesdaily)177(Evidence B).(RefertoFigure 3-1 for adults and Figure 3-4forchildrenolderthan5yearsforrecommendationsondosingandfrequencyfordifferentinhaledglucocorticosteroids.)
Leukotriene modifiers as add-on treatment to medium-tohigh-doseinhaledglucocorticosteroidshavebeenshowntoprovidebenefit(Evidence A),butusuallylessthanthatachievedwiththeadditionofalong-actingβ2-agonist165-168,175,178(Evidence A).Theadditionofalow-dose of sustained-release theophylline130 to medium-or high-doseinhaledglucocorticosteroidandlong-actingβ2-agonistmayalsoprovidebenefit(Evidence B)129.
Step 5: Reliever medication plus additional controller options. Addition of oral glucocorticosteroidstoothercontroller medications may be effective179(Evidence D)butisassociatedwithseveresideeffects180(Evidence A)andshouldonlybeconsideredifthepatient’sasthmaremains severely uncontrolled on Step 4medicationswithdailylimitationofactivitiesandfrequentexacerbations.Patientsshouldbecounseledaboutpotentialsideeffectsandallotheralternativetreatmentsmustbeconsidered.
Addition of anti-IgE treatment toothercontrollermedicationshasbeenshowntoimprovecontrolofallergicasthmawhencontrolhasnotbeenachievedoncombinationsofothercontrollersincludinghigh-dosesofinhaledororalglucocorticosteroids181-186(Evidence B).
Whenasthmacontrolhasbeenachieved,ongoingmonitoringisessentialtomaintaincontrolandtoestablishtheloweststepanddoseoftreatmentnecessary,whichminimizesthecostandmaximizesthesafetyoftreatment.Ontheotherhand,asthmaisavariabledisease,andtreatmenthastobeadjustedperiodicallyinresponsetolossofcontrolasindicatedbyworseningsymptomsorthedevelopmentofanexacerbation.
Asthmacontrolshouldbemonitoredbythehealthcareprofessionalandpreferablyalsobythepatientatregularintervals,usingeitherasimplifiedschemeaspresentedinFigure 4.3-1 oravalidatedcompositemeasureofcontrol.Thefrequencyofhealthcarevisitsandassessmentsdependsuponthepatient’sinitialclinicalseverity,andthepatient’strainingandconfidenceinplayingaroleintheon-goingcontrolofhisorherasthma.Typically,patientsareseenonetothreemonthsaftertheinitialvisit,andeverythreemonthsthereafter.Afteranexacerbation,follow-upshouldbeofferedwithintwoweekstoonemonth(Evidence D).Generalpractitionersshouldbeencouragedtoassessasthmacontrolateveryvisit,notjustwhenthepatientpresentsbecauseoftheirasthma380.
Duration and Adjustments to Treatment
Formostclassesofcontrollermedications,improvementbeginswithindaysofinitiatingtreatment,butthefullbenefitmayonlybeevidentafter3or4months 360.Insevereandchronicallyundertreateddisease,thiscantakeevenlonger188.
Thereducedneedformedicationoncecontrolisachievedisnotfullyunderstood,butmayreflectthereversalofsomeoftheconsequencesoflong-terminflammationoftheairways.Higherdosesofanti-inflammatorymedicationmayberequiredtoachievethisbenefitthantomaintainit.Alternatively,thereducedneedformedicationmightsimplyrepresentspontaneousimprovementaspartofthecyclicalnaturalhistoryofasthma.Rarely,asthmamaygointoremissionparticularlyinchildrenaged5yearsandyoungerandduringpuberty.Whatevertheexplanation,inallpatientstheminimumcontrollingdoseoftreatmentmustbesoughtthroughaprocessofregularfollow-upandstageddosereductions.
Atothertimestreatmentmayneedtobeincreasedeitherinresponsetolossofcontrolorthreatoflossofcontrol(returnofsymptoms)oranacuteexacerbation,whichisdefinedasamoreacuteandseverelossofcontrolthat
MONITORING TO MAINTAINCONTROL
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

70 ASTHMA MANAGEMENT AND PREVENTION
requiresurgenttreatment.(AnapproachtoexacerbationsisprovidedinComponent4.4.)
Stepping Down Treatment When Asthma Is Controlled
Thereislittleexperimentaldataontheoptimaltiming,sequence,andmagnitudeoftreatmentreductionsinasthma,andtheapproachwilldifferfrompatienttopatientdependingonthecombinationofmedicationsandthedosesthatwereneededtoachievecontrol.Thesechangesshouldideallybemadebyagreementbetweenpatientandhealthcareprofessional,withfulldiscussionofpotentialconsequencesincludingreappearanceofsymptomsandincreasedriskofexacerbations.Althoughfurtherresearchonsteppingdownasthmatreatment is needed, some recommendations can be madebasedonthecurrentevidence:
• Wheninhaled glucocorticosteroids alone in medium-tohigh-dosesarebeingused,a50%reductionindoseshouldbeattemptedat3monthintervals189-191(Evidence B).
• Wherecontrolisachievedatalow-doseofinhaledglucocorticosteroidsalone,inmostpatientstreatmentmaybeswitchedtoonce-dailydosing192,193(Evidence A).
• Whenasthmaiscontrolledwithacombination of inhaled glucocorticosteroid and long-acting ß2-agonist,thepreferredapproachtoistobeginbyreducingthedoseofinhaledglucocorticosteroidbyapproximately50%whilecontinuingthelong-actingβ2-agonist
(Evidence B).Ifcontrolismaintained,furtherreductionsintheglucocorticosteroidshouldbeattempteduntilalow-doseisreached,whenthelong-actingβ2-agonistmaybestopped(Evidence D).Analternativeistoswitchthecombinationtreatmenttoonce-dailydosing187,194.Asecondalternativeistodiscontinuethelong-actingβ2-agonistatanearlierstageandsubstitutethecombinationtreatmentwithinhaledglucocorticosteroidmonotherapyatthesamedosecontainedinthecombinationinhaler.However,thisismorelikelytoleadtolossofasthmacontrol368 (Evidence B).
• Whenasthmaiscontrolledwithinhaled glucocorticosteroids in combination with controllers other than long-acting β2-agonists, thedoseofinhaledglucocorticosteroidshouldbereducedby50%untilalow-doseofinhaledglucocorticosteroidisreached,thenthecombinationtreatmentstoppedasdescribedabove(Evidence D).
• Controller treatment may be stoppedifthepatient’s
asthmaremainscontrolledonthelowestdoseofcontrollerandnorecurrenceofsymptomsoccursforoneyear(Evidence D).
Stepping Up Treatment In Response To Loss Of Control
Treatmenthastobeadjustedperiodicallyinresponsetoworseningcontrol,whichmayberecognizedbytheminorrecurrenceorworseningofsymptoms195.Treatmentoptionsareasfollows:
• Rapid-onset, short-acting or long-acting ß2-agonist bronchodilators.Repeateddosingwithbronchodilatorsinthisclassprovidestemporaryreliefuntilthecauseoftheworseningsymptomspasses.Theneedforrepeateddosesovermorethanoneortwodayssignalstheneedforreviewandpossibleincreaseofcontrollertherapy.
• Inthecontextofasthmaself-managementstudies,actionplansinwhichthedoseofinhaledglucocorticosteroidswasatleastdoubledwereassociatedwithimprovedasthmaoutcomesandreducedhealthcareutilisation32.Inplacebo-controlledtrials,temporarilydoublingthedoseofinhaledglucocorticosteroidswasnoteffective404 (Evidence A),butanaverageintervalof5-7daysbetweentheonsetofworseningsymptomsandincreaseoftheinhaledglucocorticosteroiddose194, 196 mayhavebeenafactor.Thereisemergingevidencethathigherdosesofinhaledglucocorticosteroidmightbeeffectiveforpreventingprogressionto severe exacerbation195,404.Patientswhoquadrupledtheirdoseofinhaledglucocorticosteroidaftertheirpeakflowfellweresignificantlylesslikelytorequireoralglucocorticosteroids381.Inadultpatientswithanacutedeterioration,high-doseinhaledglucocorticosteroidshavebeendemonstratedtobeequivalenttoashortcourseoforalglucocorticosteroids195(Evidence A).Inthesestudies,thehigherdosewasmaintainedforseventofourteendays.Moreresearchisneededinbothadultsandchildrentostandardizetheapproach.
• Combination of inhaled glucocorticosteroids and rapid and long-acting ß2-agonist bronchodilator (e.g. formoterol) for combined relief and control. Theuseofthecombinationofarapidandlong-actingβ2-agonist(formoterol)andaninhaledglucocorticosteroid(budesonide)inasingleinhalerbothasacontrollerandrelieveriseffectiveinmaintainingahighlevelofasthmacontrolandreducesexacerbationsrequiringsystemicglucocorticosteroidsandhospitalization111,156,157,197
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 71
(Evidence A).Thebenefitinpreventingexacerbationsappearstobetheconsequenceofearlyinterventionataveryearlystageofathreatenedexacerbationsincestudiesinvolvingdoublingorquadruplingdosesofcombinationtreatmentoncedeteriorationisestablished(for2ormoredays)showsomebenefitbutresultsareinconsistent195.Becausetherearenostudiesusingthisapproachwithothercombinationsofcontrollerandrelievers,otherthanbudesonide/formoterol,thealternativeapproachesdescribedinthissectionshouldbeusedforpatientsonothercontrollertherapies.
Forchildren(6to17years)whohaveuncontrolledasthmadespitetheuseoflow-doseinhaledglucocorticosteroids,step-uptherapywithlong-actingβ2-agonistbronchodilatorwassignificantlymorelikelytoprovidethebestresponsethaneitherstep-uptherapywithinhaledglucocorticosteroidsorleukotrienereceptorantagonist.However,manychildrenhadabestresponsetoinhaledglucocorticosteroidsorleukotrienereceptorantagoniststep-uptherapy,highlightingtheneedtoregularlymonitorandappropriatelyadjusteachchild’sasthmatherapy382.
Combinationtherapywithbudesonideandformoterolusedbothasmaintenanceandrescuehasbeenshowntoreduceasthmaexacerbationsinchildrenages4yearsandolderwithmoderatetosevereasthma347.
Theusualtreatmentforanacuteexacerbationisahigh-doseofβ2-agonistandaburstofsystemicglucocorticosteroidsadministeredorallyorintravenously.(RefertoComponent4formoreinformation.)
Followingtreatmentforanexacerbationofasthma,maintenancetreatmentcangenerallyberesumedatpreviouslevelsunlesstheexacerbationwasassociatedwithagraduallossofcontrolsuggestingchronicundertreatment.Inthiscase,providedinhalertechniquehasbeenchecked,astep-wiseincreaseintreatment(eitherindoseornumberofcontrollers)isindicated.
Difficult-to-Treat Asthma
Althoughthemajorityofasthmapatientscanobtainthetargetedlevelofcontrol(Figure 4.3-1),somepatientswillnotdosoevenwiththebesttherapy104.PatientswhodonotreachanacceptablelevelofcontrolatStep 4 (reliever medication plus two or more controllers)canbeconsideredtohavedifficult-to-treatasthma198.Thesepatientsmayhaveanelementofpoorglucocorticosteroidresponsiveness,andrequirehigherdosesofinhaled
glucocorticosteroidsthanareroutinelyusedinpatientswhoseasthmaiseasytocontrol.However,thereiscurrentlynoevidencetosupportcontinuingthesehigh-dosesofinhaledglucocorticosteroidsbeyond6monthsinthehopeofachievingbettercontrol.Instead,doseoptimizationshouldbepursuedbysteppingdowntoadosethatmaintainsthemaximallevelofcontrolachievedonthehigherdose.
Becauseveryfewpatientsarecompletelyresistanttoglucocorticosteroids,thesemedicationsremainamainstayoftherapyfordifficult-to-treatasthma,whileadditionaldiagnosticandgeneralizedtherapeuticoptionscanandshouldalsobeconsidered:
• Confirmthediagnosisofasthma.Inparticular,thepresenceofCOPDmustbeexcluded.Vocalcorddysfunctionmustbeconsidered.
• Investigateandconfirmadherencewithtreatment.Incorrect or inadequate use of medications and inhalers405remainsthemostcommonreasonforfailuretoachievegoodcontrol.Inpatientswithdifficult-to-treatasthma,improvedadherenceandimprovedhealthoutcomescanbeachievedwithacomprehensiveconcordanceintervention416.
• Consider smoking, current or past, and encouragecompletecessation.Ahistoryofpasttobaccosmokingisassociatedwithareducedlikelihoodofcompleteasthmacontrol,andthisisonlypartlyattributabletothepresenceoffixedairflowobstruction.Inaddition,currentsmokingreducestheeffectivenessofinhaledandoralglucocorticosteroids71,72,378.Counselingandsmokingcessationprogramsshouldbeofferedtoallasthmapatientswhosmoke.
• Investigatethepresenceofcomorbidities thatmayaggravateasthma.Chronicsinusitis,gastroesophagealreflux,andobesity/obstructivesleepapneahavebeenreportedinhigherpercentagesinpatientswithdifficult-to-treatasthma.Psychologicalandpsychiatricdisordersshouldalsobeconsidered.Iffound,thesecomorbiditiesshouldbeaddressedandtreatedasappropriate,althoughtheabilitytoimproveasthmacontrolbydoingsoremainsunconfirmed200,348.
Whenthesereasonsforlackoftreatmentresponsehavebeenconsideredandaddressed,acompromiselevelofcontrolmayneedtobeacceptedanddiscussedwiththepatienttoavoidfutileover-treatment(withitsattendantcostandpotentialforadverseeffects).Theobjectiveisthentominimizeexacerbationsandneedforemergencymedicalinterventionswhileachievingashighalevelof
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

72 ASTHMA MANAGEMENT AND PREVENTION
clinicalcontrolwithaslittledisruptionofactivitiesandasfewdailysymptomsaspossible.Forthesedifficult-to-treatpatients,frequentuseofrescuemedicationisaccepted,asisadegreeofchroniclungfunctionimpairment.Althoughlowerlevelsofcontrolaregenerallyassociatedwithanincreasedriskofexacerbations,notallpatientswithchronicallyimpairedlungfunction,reducedactivitylevels,anddailysymptomshavefrequentexacerbations.Insuchpatients,thelowestleveloftreatmentthatretainsthebenefitsachievedatthehigherdosesoftreatmentshouldbeemployed.Reductionsshouldbemadecautiouslyandslowlyatintervalsnotmorefrequentthan3to6months,ascarryoveroftheeffectsofthehigherdosemaylastforseveralmonthsandmakeitdifficulttoassesstheimpactofthedosereduction(Evidence D).Referraltoaphysicianwithaninterestinand/orspecialfocusonasthmamaybehelpfulandpatientsmaybenefitfromphenotypingintocategoriessuchasallergic,aspirin-sensitive,and/oreosinophilicasthma201.Patientscategorizedasallergicmightbenefitfromanti-IgEtherapy183,andleukotrienemodifierscanbehelpfulforpatientsdeterminedtobeaspirinsensitive(whoareofteneosinophilicaswell)172.
Thermoplasty
GRADEevidencetechnologywasusedtoevaluateresearchonthermoplasty:
Question: “In adult patient whose asthma is uncontrolled despite recommended therapeutic regimens, does thermoplasty, compared to placebo improve patient outcomes?” The consensus recommendation:
• Foradultpatientswhoseasthmaremainsuncontrolleddespiteapplicationofthistherapeuticparadigm,andreferraltoanasthmaspecialtycenter,bronchialthermoplastyisnowapossibleoptioninsomecountries406-408.Inthisbronchoscopictreatment,airwaysaretreatedonthreeoccasionswithalocalizedradiofrequencypulse.Thetreatment,whichitselfisassociatedwithasthmaexacerbationsinthemonthspostbronchoscopy,resultsinasubsequentdecreaseinexacerbations.Therearenosignificanteffectsonlungfunctionorasthmasymptoms.Extendedfollow-uponasmallnumberofpatientshasprovidedsomeadditionalsupportforlong-termsafetyofbronchialthermoplasty417.However,longer-termfollow-upoflargernumberofcontrolandactivepatientsisneededtoassesseffectivenessandcautionshouldbeusedinselectingpatientsforthisprocedure.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 73
KEY POINTS:
• Exacerbationsofasthma(asthmaattacksoracuteasthma)areepisodesofprogressiveincreaseinshortnessofbreath,cough,wheezing,orchesttightness,orsomecombinationofthesesymptoms.
• Exacerbationsarecharacterizedbydecreasesinexpiratoryairflowthatcanbequantifiedandmonitoredbymeasurementoflungfunction(PEForFEV1).
• Theprimarytherapiesforexacerbationsincludetherepetitiveadministrationofrapid-actinginhaledbronchodilators,theearlyintroductionofsystemicglucocorticosteroids,andoxygensupplementation.
• Theaimsoftreatmentaretorelieveairflowobstructionandhypoxemiaasquicklyaspossible,andtoplanthepreventionoffuturerelapses.
• Severeexacerbationsarepotentiallylifethreatening,andtheirtreatmentrequiresclosesupervision.Mostpatientswithsevereasthmaexacerbationsshouldbetreatedinanacutecarefacility.Patientsathighriskofasthma-relateddeathalsorequirecloserattention.
• Milderexacerbations,definedbyareductioninpeakflowoflessthan20%,nocturnalawakening,andincreaseduseofshortactingβ2-agonistscanusuallybetreatedinacommunitysetting.
Exacerbationsofasthma(asthmaattacksoracuteasthma)areepisodesofprogressiveincreaseinshortnessofbreath,cough,wheezing,orchesttightness,orsomecombinationofthesesymptoms.Exacerbationsusuallyhaveaprogressiveonsetbutasubsetofpatients(mostlyadults)presentmoreacutely361.Respiratorydistressiscommon.Exacerbationsarecharacterizedbydecreasesinexpiratoryairflowthatcanbequantifiedbymeasurementoflungfunction(PEForFEV1)
202.Thesemeasurementsaremorereliableindicatorsoftheseverityofairflowlimitationthanisthedegreeofsymptoms.Thedegreeofsymptomsmay,however,beamoresensitivemeasureoftheonsetofanexacerbationbecausetheincreaseinsymptomsusuallyprecedesthedeteriorationinpeakflowrate203.Still,aminorityofpatientsperceivesymptomspoorly,andmayhaveasignificantdeclineinlungfunctionwithoutasignificantchangeinsymptoms.Thissituationespeciallyaffectspatientswithahistoryofnear-fatalasthmaandalso
appearstobemorelikelyinmales.Aclinicallyusefultooltoassessthelikelihoodofasthma-relatedhospitalizationsoremergencydepartmentvisitsinadultswithsevereordifficulttotreatasthmahavebeendescribed349,418.
Strategiesfortreatingexacerbations,thoughgeneralizable,arebestadaptedandimplementedatalocallevel204,205.Severeexacerbationsarepotentiallylifethreatening,andtheirtreatmentrequiresclosesupervision.Patientswithsevereexacerbationsshouldbeencouragedtoseetheirphysicianpromptlyor,dependingontheorganizationoflocalhealthservices,toproceedtothenearestclinicorhospitalthatprovidesemergencyaccessforpatientswithacuteasthma.Closeobjectivemonitoring(PEF)oftheresponsetotherapyisessential.
Theprimarytherapiesforexacerbationsinclude—intheorderinwhichtheyareintroduced,dependingonseverity—repetitiveadministrationofrapid-actinginhaledbronchodilators,earlyintroductionofsystemicglucocorticosteroids,andoxygensupplementation202.Theaimsoftreatmentaretorelieveairflowobstructionandhypoxemiaasquicklyaspossible,andtoplanthepreventionoffuturerelapses.
Patientsathighriskofasthma-relateddeathrequirecloserattentionandshouldbeencouragedtoseekurgentcareearlyinthecourseoftheirexacerbations.Thesepatientsincludethose:
• Withahistoryofnear-fatalasthmarequiringintubationandmechanicalventilation206
• Whohavehadahospitalizationoremergencycarevisitforasthmainthepastyear
• Whoarecurrentlyusingorhaverecentlystoppedusingoralglucocorticosteroids
• Whoarenotcurrentlyusinginhaledglucocorticosteroids207
• Whoareoverdependentonrapid-actinginhaledβ2-agonists,especiallythosewhousemorethanonecanisterofsalbutamol(orequivalent)monthly208
• Withahistoryofpsychiatricdiseaseorpsychosocial350 problems,includingtheuseofsedatives209
• Withahistoryofpooradherencewithasthmamedicationsand/orawrittenasthmaactionplan.
Responsetotreatmentmaytaketimeandpatientsshouldbecloselymonitoredusingclinicalaswellasobjectivemeasurements.Theincreasedtreatmentshouldcontinue
COMPONENT 4: MANAGE ASTHMA EXACERBATIONS
INTRODUCTION
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

74 ASTHMA MANAGEMENT AND PREVENTION
untilmeasurementsoflungfunction(PEForFEV1)returntotheirpreviousbest(ideally)orplateau,atwhichtimeadecisiontoadmitordischargecanbemadebaseduponthesevalues.Patientswhocanbesafelydischargedwillhaverespondedwithinthefirsttwohours,atwhichtimedecisionsregardingpatientdispositioncanbemade.
Theseverityoftheexacerbation(Figure 4.4-1)determinesthetreatmentadministered.Indicesofseverity,particularly
PEF(inpatientsolderthan5years),pulserate,respiratoryrate,andpulseoximetry210,shouldbemonitoredduringtreatment.
Mostpatientswithsevereasthmaexacerbationsshouldbetreatedinanacutecarefacility(suchasahospitalemergencydepartment)wheremonitoring,including
ASSESSMENT OF SEVERITY
MANAGEMENT—COMMUNITY SETTINGS
Figure 4.4-1. Severity of Asthma Exacerbations*
Mild Moderate Severe Respiratory arrestimminent
Breathless Walking Talking At restInfant—softer Infant stops feedingshorter cry;difficulty feeding
Can lie down Prefers sitting Hunched forwardTalks in Sentences Phrases WordsAlertness May be agitated Usually agitated Usually agitated Drowsy or confusedRespiratory rate Increased Increased Often > 30/min
Normal rates of breathing in awake children:Age Normal rate< 2 months < 60/min2-12 months < 50/min1-5 years < 40/min6-8 years < 30/min
Accessory muscles Usually not Usually Usually Paradoxical thoraco-and suprasternal abdominal movementretractionsWheeze Moderate, often only Loud Usually loud Absence of wheeze
end expiratoryPulse/min. < 100 100-120 >120 Bradycardia
Guide to limits of normal pulse rate in children:Infants 2-12 months–Normal Rate < 160/minPreschool 1-2 years < 120/minSchool age 2-8 years < 110/min
Pulsus paradoxus Absent May be present Often present Absence suggests< 10 mm Hg 10-25 mm Hg > 25 mm Hg (adult) respiratory muscle
20-40 mm Hg (child) fatiguePEF Over 80% Approx. 60-80% < 60% predicted orafter initial personal bestbronchodilator (< 100 L/min adults)% predicted or or% personal best response lasts < 2 hrsPaO2 (on air)† Normal > 60 mm Hg < 60 mm Hg
Test not usuallynecessary Possible cyanosis
and/orPaCO2† < 45 mm Hg < 45 mm Hg > 45 mm Hg;
Possible respiratoryfailure (see text)
SaO2% (on air)† > 95% 91-95% < 90%Hypercapnea (hypoventilation) develops more readily in young children than inadults and adolescents.
*Note: The presence of several parameters, but not necessarily all, indicates the general classification of the exacerbation.†Note: Kilopascals are also used internationally; conversion would be appropriate in this regard.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 75
objectivemeasurementofairflowobstruction,oxygensaturation,andcardiacfunction,ispossible.Milderexacerbations,definedbyareductioninpeakflowoflessthan20%,nocturnalawakening,andincreaseduseofshortactingβ2-agonistscanusuallybetreatedinacommunitysetting.Ifthepatientrespondstotheincreaseininhaledbronchodilatortreatmentafterthefirstfewdoses,referraltoanacutecarefacilityisnotrequired,butfurthermanagementunderthedirectionofaprimarycarephysicianmayincludetheuseofsystemicglucocorticosteroids.Patienteducationandreviewofmaintenancetherapyshouldalsobeundertaken.
Treatment
Bronchodilators. For mild to moderate exacerbations, repeatedadministrationofrapid-actinginhaledβ-agonists(2to4puffsevery20minutesforthefirsthour)isusuallythebestandmostcost-effectivemethodofachievingrapidreversalofairflowlimitation.Afterthefirsthour,thedoseof β-agonistrequiredwilldependontheseverityoftheexacerbation.Mildexacerbationsrespondto2to4puffsevery3to4hours;moderateexacerbationswillrequire6to10puffsevery1or2hours.Treatmentshouldalsobetitrateddependingupontheindividualpatient’sresponse,andifthereisalackofresponseorotherconcernabouthowthepatientisresponding,thepatientshouldbereferredtoanacutecarefacility.
ManypatientswillbeabletomonitortheirPEFaftertheinitiationofincreasedbronchodilatortherapy.Bronchodilatortherapydeliveredviaametered-doseinhaler(MDI),ideallywithaspacer,producesatleastanequivalentimprovementinlungfunctionasthesamedose164,211deliveredvianebulizer.Atthecliniclevel,thisrouteofdeliveryisthemostcosteffective212,providedpatientsareabletouseanMDI.Noadditionalmedicationisnecessaryiftherapid-actinginhaledβ-agonistproducesacompleteresponse(PEFreturnstogreaterthan80%ofpredictedorpersonalbest)andtheresponselastsfor3to4hours.
Glucocorticosteroids.Oralglucocorticosteroids(0.5to1mgofprednisolone/kgorequivalentduringa24-hourperiod)shouldbeusedtotreatexacerbations,especiallyiftheydevelopafterinstitutingtheothershort-termtreatmentoptionsrecommendedforlossofcontrol(see“Steppinguptreatmentinresponsetolossofcontrol”inComponent3).Ifpatientsfailtorespondtobronchodilatortherapy,asindicatedbypersistentairflowobstruction,prompttransfertoanacutecaresettingisrecommended,especiallyiftheyareinahighriskgroup.
Severeexacerbationsofasthmaarelife-threateningmedicalemergencies,treatmentofwhichisoftenmostsafelyundertakeninanemergencydepartment.Figure 4.4-2illustratestheapproachtoacutecare-basedmanagementofexacerbations.
Assessment
Abriefhistoryandphysicalexaminationpertinenttotheexacerbationshouldbeconductedconcurrentlywiththepromptinitiationoftherapy.Thehistoryshouldinclude:severityanddurationofsymptoms,includingexerciselimitationandsleepdisturbance;allcurrentmedications,includingdose(anddevice)prescribed,doseusuallytaken,dosetakeninresponsetothedeterioration,andthepatient’sresponse(orlackthereof)tothistherapy;timeofonsetandcauseofthepresentexacerbation;andriskfactorsforasthma-relateddeath.
Thephysicalexaminationshouldassessexacerbationseveritybyevaluatingthepatient’sabilitytocompleteasentence,pulserate,respiratoryrate,useofaccessorymuscles,andothersignsdetailedinFigure 4.4-2.Anycomplicatingfactorsshouldbeidentified(e.g.,pneumonia,atelectasis,pneumothorax,orpneumomediastinum).FunctionalassessmentssuchasPEForFEV1 and arterialoxygensaturationmeasurementsarestronglyrecommendedasphysicalexaminationalonemaynotfullyindicatetheseverityoftheexacerbation,particularlythedegreeofhypoxemia213,214.Withoutundulydelayingtreatment, a baseline PEF or FEV1measurementshouldbemadebeforetreatmentisinitiated,althoughspirometrymaynotbepossibleinchildrenwithacuteasthma.Subsequentmeasurementsshouldbemadeatintervalsuntilaclearresponsetotreatmenthasoccurred.
Oxygensaturationshouldbecloselymonitored,preferablybypulseoximetry.Thisisespeciallyusefulinchildrenbecauseobjectivemeasurementsoflungfunctionmaybedifficult.Oxygensaturationinchildrenshouldnormallybegreaterthan95%,andoxygensaturationlessthan92%isagoodpredictoroftheneedforhospitalization210 (Evidence C).
InadultsachestX-rayisnotroutinelyrequired,butshouldbecarriedoutifacomplicatingcardiopulmonaryprocessissuspected,inpatientsrequiringhospitalization,andinthosenotrespondingtotreatmentwhereapneumothoraxmaybedifficulttodiagnoseclinically215.Similarly,inchildrenroutinechestX-raysarenotrecommendedunlesstherearephysicalsignssuggestiveofparenchymaldisease216.
MANAGEMENT—ACUTE CARE SETTINGS
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

76 ASTHMA MANAGEMENT AND PREVENTION
Figure 4.4-2: Management of Asthma Exacerbations in Acute Care Setting
Reassess after 1-2 Hours
Reassess at intervals
Improved (see opposite)
Initial Assessment (see Figure 4.4-1)• History, physical examination (auscultation, use of accessory muscles, heart rate, respiratory rate, PEF or FEV1, oxygen
saturation, arterial blood gas if patient in extremis)
Reassess after 1 HourPhysical Examination, PEF, O2 saturation and other tests as needed
Initial Treatment• Oxygen to achieve O2 saturation ≥ 90% (95% in children)• Inhaled rapid-acting �2-agonist continuously for one hour.• Systemic glucocorticosteroids if no immediate response, or if patient recently took oral glucocorticosteroid, or if episode is severe.• Sedation is contraindicated in the treatment of an exacerbation.
Criteria for Moderate Episode:• PEF 60-80% predicted/personal best• Physical exam: moderate symptoms, accessory muscle useTreatment:• Oxygen• Inhaled �2-agonist and inhaled anticholinergic every 60 min• Oral glucocorticosteroids• Continue treatment for 1-3 hours, provided there is improvement
Good Response within 1-2 Hours:• Response sustained 60 min after last
treatment• Physical exam normal: No distress• PEF > 70% • O2 saturation > 90% (95% children)
Incomplete Response within 1-2Hours:• Risk factors for near fatal asthma• Physical exam: mild to moderate signs• PEF < 60%• O2 saturation not improving
Poor Response within 1-2 Hours:• Risk factors for near fatal asthma• Physical exam: symptoms severe,
drowsiness, confusion• PEF < 30%• PCO2 > 45 mm Hg• P O2 < 60mm HgAdmit to Intensive Care• Oxygen • Inhaled �2-agonist + anticholinergic • Intravenous glucocorticosteroids • Consider intravenous �2-agonist • Consider intravenous theophylline• Possible intubation and mechanical
ventilation
Poor Response (see above):• Admit to Intensive CareIncomplete response in 6-12 hours(see above)• Consider admission to Intensive Care
if no improvement within 6-12 hours
Admit to Acute Care Setting• Oxygen• Inhaled �2-agonist ± anticholinergic• Systemic glucocorticosteroid• Intravenous magnesium• Monitor PEF, O2 saturation, pulse
Improved: Criteria for Discharge Home• PEF > 60% predicted/personal best• Sustained on oral/inhaled medicationHome Treatment:• Continue inhaled �2-agonist• Consider, in most cases, oral glucocorticosteroids• Consider adding a combination inhaler• Patient education: Take medicine correctly
Review action planClose medical follow-up
Criteria for Severe Episode:• History of risk factors for near fatal asthma• PEF < 60% predicted/personal best• Physical exam: severe symptoms at rest, chest retraction• No improvement after initial treatmentTreatment:• Oxygen• Inhaled �2-agonist and inhaled anticholinergic• Systemic glucocorticosteroids• Intravenous magnesium
tt
ttt
t
t
tt
t
t
t t
t
t
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 77
Althougharterialbloodgasmeasurementsarenotroutinelyrequired216,theyshouldbecompletedinpatientswithaPEFof30to50%predicted,thosewhodonotrespondtoinitialtreatment,orwhenthereisconcernregardingdeterioration.Thepatientshouldcontinueonsupplementaloxygenwhilethemeasurementismade.APaO2<60mmHg(8kPa)andanormalorincreasedPaCO2(especially>45mmHg,6kPa)indicatesthepresenceofrespiratoryfailure.
Treatment
Thefollowingtreatmentsareusuallyadministeredconcurrentlytoachievethemostrapidresolutionoftheexacerbation217:
Oxygen.Toachievearterialoxygensaturationof90%(95%inchildren),oxygenshouldbeadministeredbynasalcannulae,bymask,orrarelybyheadboxinsomeinfants.Forsevereasthmaexacerbations,controlledoxygentherapyusingpulseoximetrytomaintainoxygensaturationat90–93%isassociatedwithbetterphysiologicaloutcomes,comparedtohighflow100%oxygentherapy218,
419.Oxygentherapyshouldbetitratedagainstpulseoximetrytomaintainasatisfactoryoxygensaturation219.However,oxygenshouldnotbewithheldifoximetryisnotavailable.
Rapid-acting inhaled ß2–agonists.Rapid-actinginhaledβ2-agonistsshouldbeadministeredatregularintervals
220-222 (Evidence A).Themostcosteffectiveandefficientdeliveryisbymetereddoseinhalerandaspacerdevice164, 211.Althoughmostrapid-actingβ2-agonistshaveashortdurationofeffect,thelong-actingbronchodilatorformoterol,whichhasbotharapidonsetofactionandalongdurationofeffect,hasbeenshowntobeequallyeffectivewithoutincreasingsideeffects,thoughitisconsiderablymoreexpensive148.Theimportanceofthisfeatureofformoterolisthatitprovidessupportandreassuranceregardingtheuse of a combination of formoterol and budesonide early in asthmaexacerbations. Amodestlygreaterbronchodilatoreffecthasbeenshownwithlevabuterolcomparedtoracemicalbuterolinbothadultsandchildrenwithanasthmaexacerbation223-226.Inalargestudyofacuteasthmainchildren227, and in adults not previouslytreatedwithglucocorticosteroids226, levabuterol treatmentresultedinlowerhospitalizationratescomparedtoracemicalbuteroltreatment,butinchildrenthelengthofhospitalstaywasnodifferent227.
Studiesofintermittentversuscontinuousnebulizedshort-actingβ2-agonistsinacuteasthmaprovideconflictingresults.Inasystematicreviewofsixstudies228,therewere
nosignificantdifferencesinbronchodilatoreffectorhospitaladmissionsbetweenthetwotreatments.Inpatientswhorequirehospitalization,onestudy229foundthatintermittenton-demandtherapyledtoasignificantlyshorterhospitalstay,fewernebulizations,andfewerpalpitationswhencomparedwithintermittenttherapygivenevery4hours.Areasonableapproachtoinhaledtherapyinexacerbations,therefore,wouldbetheinitialuseofcontinuoustherapy,followedbyintermittenton-demandtherapyforhospitalizedpatients.Thereisnoevidencetosupporttheroutineuseof intravenous β2-agonistsinpatientswithsevereasthmaexacerbations230.
Epinephrine. A subcutaneous or intramuscular injection ofepinephrine(adrenaline)maybeindicatedforacutetreatmentofanaphylaxisandangioedema,butisnotroutinelyindicatedduringasthmaexacerbations.
Additional bronchodilators.
Ipratropiumbromide.Acombinationofnebulizedβ2-agonistwithananticholinergic(ipratropiumbromide)mayproducebetterbronchodilationthaneitherdrugalone231(Evidence B)andshouldbeadministeredbeforemethylxanthinesareconsidered.Combinationβ2-agonist/anticholinergictherapyisassociatedwithlowerhospitalizationrates212,232,233 (Evidence A)andgreaterimprovementinPEFandFEV1
233(Evidence B).Similardatahavebeenreportedinthepediatricliterature212(Evidence A).However,oncechildrenwithasthmaarehospitalizedfollowingintensiveemergencydepartmenttreatment,theadditionofnebulizedipratropiumbromidetonebulizedβ2-agonistandsystemicglucocorticosteroidsappearstoconfernoextrabenefit234. Theophylline.Inviewoftheeffectivenessandrelativesafetyofrapid-actingβ2-agonists,theophyllinehasaminimalroleinthemanagementofacuteasthma235.Itsuseisassociatedwithsevereandpotentiallyfatalsideeffects,particularlyinthoseonlong-termtherapywithsustained-releasetheophylline,andtheirbronchodilatoreffectislessthanthatofβ2-agonists.Thebenefitasadd-ontreatmentinadultswithsevereasthmaexacerbationshasnotbeendemonstrated.However,inonestudyofchildrenwithnear-fatalasthma,intravenoustheophyllineprovidedadditionalbenefittopatientsalsoreceivinganaggressiveregimenofinhaledandintravenousβ2-agonists,inhaledipatropiumbromide,andintravenoussystemicglucocorticosteroids236.
Systemic glucocorticosteroids. Systemic glucocorticosteroidsspeedresolutionofexacerbationsandshouldbeutilizedintheallbutthemildestexacerbations237,238(Evidence A),especiallyif:
• Theinitialrapid-actinginhaledβ2-agonisttherapyfailstoachievelastingimprovement
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

78 ASTHMA MANAGEMENT AND PREVENTION
• Theexacerbationdevelopseventhoughthepatientwasalreadytakingoralglucocorticosteroids
• Previous exacerbations required oral glucocorticosteroids.
Oralglucocorticosteroidsareusuallyaseffectiveasthoseadministeredintravenouslyandarepreferredbecausethisrouteofdeliveryislessinvasiveandlessexpensive239,240 .Ifvomitinghasoccurredshortlyafteradministrationoforalglucocorticosteroids,thenanequivalentdoseshouldbere-administeredintravenously.Inpatientsdischargedfromtheemergencydepartment,intramuscularadministrationmaybehelpful241,especiallyifthereareconcernsaboutcompliancewithoraltherapy.Oralglucocorticosteroidsrequireatleast4hourstoproduceclinicalimprovement.Dailydosesofsystemicglucocorticosteroidsequivalentto60-80mgmethylprednisoloneasasingledose,or300-400mghydrocortisoneindivideddoses,areadequateforhospitalizedpatients,and40mgmethylprednisoloneor200mghydrocortisoneisprobablyadequateinmostcases238,242(Evidence B).Anoralglucocorticosteroiddoseof1mg/kgdailyisadequatefortreatmentofexacerbationsinchildrenwithmildpersistentasthma243.A7-daycourseinadultshasbeenfoundtobeaseffectiveasa14-daycourse244,anda3-to5-daycourseinchildrenisusuallyconsideredappropriate(Evidence B).Twodaysoforaldexamethasonecanalsobeusedtotreatasthmaexacerbations,butthereareconcernsaboutmetabolicside-effectsifdexamethasoneiscontinuedbeyondtwodays420.Evidencesuggeststhatthereisnobenefittotaperingthedoseoforalglucocorticosteroids,eitherintheshort-term245oroverseveralweeks,aslongasthepatientisonmaintenanceinhaledglucocorticosteroids246 (Evidence B).
Inhaled glucocorticosteroids.Inhaledglucocorticosteroidsareeffectiveaspartoftherapyforasthmaexacerbations.Inonestudy,thecombinationofhigh-doseinhaledglucocorticosteroidsandsalbutamolinacuteasthmaprovidedgreaterbronchodilationthansalbutamol alone247(Evidence B),andconferredgreaterbenefitthantheadditionofsystemicglucocorticosteroidsacrossallparameters,includinghospitalizations,especiallyforpatientswithmoresevereattacks248.
Inhaledglucocorticosteroidscanbeaseffectiveasoralglucocorticosteroidsatpreventingrelapses249,250.Patientsdischargedfromtheemergencydepartmentonprednisoneandinhaledbudesonidehavealowerrateofrelapsethanthoseonprednisonealone237(Evidence B).Ahigh-doseofinhaledglucocorticosteroid(2.4mgbudesonidedailyinfourdivideddoses)achievesarelapseratesimilarto40mgoralprednisonedaily251(Evidence A).Costisasignificantfactorintheuseofsuchhigh-dosesofinhaled
glucocorticosteroids,andfurtherstudiesarerequiredtodocumenttheirpotentialbenefits,especiallycosteffectiveness,inacuteasthma252.
Magnesium*.Intravenousmagnesiumsulphate(usuallygivenasasingle2ginfusionover20minutes)isnotrecommendedforroutineuseinasthmaexacerbations,butcanhelpreducehospitaladmissionratesincertainpatients,includingadultswithFEV125-30%predictedatpresentation,adultsandchildrenwhofailtorespondtoinitialtreatment,andchildrenwhoseFEV1failstoimproveabove60%predictedafter1hourofcare253,254,409(Evidence A).Nebulizedsalbutamoladministeredinisotonicmagnesiumsulfateprovidesgreaterbenefitthanifitisdelivered in normal saline255,256(Evidence A).Intravenousmagnesiumsulphatehasnotbeenstudiedinyoungchildren.
Helium oxygen therapy. A systematic survey of studies thathaveevaluatedtheeffectofacombinationofheliumandoxygen,comparedtoheliumalone,suggeststhereisnoroutineroleforthisintervention.Itmightbeconsideredforpatientswhodonotrespondtostandardtherapy257.
Leukotriene modifiers.Therearelittledatatosuggestaroleforleukotrienemodifiersinacuteasthma258.SmallinvestigationshavedemonstratedimprovementinPEF410, butclinicalrelevancerequiresmorestudy.
Sedatives.Sedationshouldbestrictlyavoidedduringexacerbationsofasthmabecauseoftherespiratorydepressanteffectofanxiolyticandhypnoticdrugs.Anassociationbetweentheuseofthesedrugsandavoidableasthmadeaths209,259hasbeendemonstrated.
Criteria for Discharge from the Emergency Department vs. Hospitalization
Criteriafordeterminingwhetherapatientshouldbedischargedfromtheemergencydepartmentoradmittedtothehospitalhavebeensuccinctlyreviewedandstratifiedbased on consensus260.Patientswithapre-treatmentFEV1 orPEF<25%percentpredictedorpersonalbest,orthosewithapost-treatmentFEV1orPEF<40%percentpredictedorpersonalbest,usuallyrequirehospitalization.Patientswithpost-treatmentlungfunctionof40-60%predictedmaybedischarged,providedthatadequatefollow-upisavailableinthecommunityandcomplianceisassured.Patientswithpost-treatmentlungfunction60%predictedcanbedischarged.
Managementofacuteasthmaintheintensivecareunitisbeyondthescopeofthisdocumentandreadersarereferredtorecentcomprehensivereviews261.*Visit GINA website, www.ginasthma.org for GRADE review of question “In adults with acute exacerbations of asthma, does intravenous magnesium sulphate compared to placebo improve patient important outcomes?”COPY
RIGHTE
D MAT
ERIA
L - D
O NOT
ALTE
R OR R
EPRODUCE

ASTHMA MANAGEMENT AND PREVENTION 79
Forpatientsdischargedfromtheemergencydepartment:
• At a minimum, a 7-day course of oral glucocorticosteroidsforadultsandashortercourse(3-5days)forchildrenshouldbeprescribed,alongwithcontinuationofbronchodilatortherapy.
• Thebronchodilatorcanbeusedonanas-neededbasis,basedonbothsymptomaticandobjectiveimprovement,untilthepatientreturnstohisorherpre-exacerbationuseofrapid-actinginhaledβ2-agonists.
• Ipratropiumbromideisunlikelytoprovideadditionalbenefitbeyondtheacutephaseandmaybequicklydiscontinued.
• Patientsshouldinitiateorcontinueinhaledglucocorticosteroids.
• Thepatient’sinhalertechniqueanduseofpeakflowmetertomonitortherapyathomeshouldbereviewed.Patientsdischargedfromtheemergencydepartmentwithapeakflowmeterandactionplanhaveabetterresponsethanpatientsdischargedwithouttheseresources8.
• Thefactorsthatprecipitatedtheexacerbationshouldbeidentifiedandstrategiesfortheirfutureavoidanceimplemented.
• Thepatient’sresponsetotheexacerbationshouldbeevaluated.Theactionplanshouldbereviewedandwrittenguidanceprovided411.
• Useofcontrollertherapyduringtheexacerbationshouldbereviewed:whetherthistherapywasincreasedpromptly,byhowmuch,and,ifappropriate,whyoralglucocorticosteroidswerenotadded.Considerprovidingashortcourseoforalglucocorticosteroidstobeonhandforsubsequentexacerbations.
• Thepatientorfamilyshouldbeinstructedtocontacttheprimaryhealthcareprofessionalorasthmaspecialistwithin24hoursofdischarge.Afollow-upappointmentwiththepatient’susualprimarycareprofessionalorasthmaspecialistshouldbemadewithinafewdaysofdischargetoassurethattreatmentiscontinueduntilbaselinecontrolparameters,includingpersonalbestlungfunction,arereached.Prospectivedataindicatethatpatientsdischargedfromtheemergencydepartmentforfollow-upwithspecialistcaredobetterthanpatientsreturnedtoroutine care262.
Anexacerbationsevereenoughtorequirehospitalizationmayreflectafailureofthepatient’sasthmamanagementorlackofawrittenasthmaactionplan.Hospitalizedpatientsmaybeparticularlyreceptivetoinformationandadviceabouttheirillness.Healthcareprovidersshouldtakethe
opportunitytoreviewpatientunderstandingofthecausesofasthmaexacerbations,avoidanceoffactorsthatmaycauseexacerbations(including,whererelevantsmokingcessation),thepurposesandcorrectusesoftreatment,andtheactionstobetakentorespondtoworseningsymptomsorpeakflowvalues263(Evidence A).Referraltoanasthmaspecialistshouldbeconsideredforhospitalizedpatients.Followingdischargefromcontinuoussupervision,thepatientshouldbereviewedbythefamilyhealthcareprofessionalorasthmaspecialistregularlyoverthesubsequentweeksuntilpersonalbestlungfunctionisreached.Useofincentivesimprovesprimarycarefollowupbuthasshownnoeffectonlongtermoutcomes264.Patientswhocometotheemergencydepartmentwithanacuteexacerbationshouldbeespeciallytargetedforanasthmaeducationprogram,ifoneisavailable.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

80 ASTHMA MANAGEMENT AND PREVENTION
Specialconsiderationsarerequiredinmanagingasthmainrelationtopregnancy;obesity;surgery;rhinitis,sinusitis,andnasalpolyps;occupationalasthma;respiratoryinfections;gastroesophagealreflux;aspirin-inducedasthma;andanaphylaxis.
Pregnancy
Duringpregnancytheseverityofasthmaoftenchanges,andpatientsmayrequireclosefollow-upandadjustmentofmedications.Inapproximatelyone-thirdofwomenasthmabecomesworse;inone-thirdasthmabecomeslesssevere;andintheremainingone-thirditremainsunchangedduringpregnancy265-267.
Althoughthereisageneralconcernabouttheuseofanymedicationinpregnancy,poorlycontrolledasthmacanhaveanadverseeffectonthefetus,resultinginincreasedperinatalmortality,increasedprematurity,andlowbirthweight266,267.Theoverallperinatalprognosisforchildrenborntowomenwithasthmathatiswell-managedduringpregnancyiscomparabletothatforchildrenborntowomenwithoutasthma268.Forthisreason,usingmedicationstoobtainoptimalcontrolofasthmaisjustifiedevenwhentheirsafetyinpregnancyhasnotbeenunequivocallyproven.Formostmedicationsusedtotreatasthmathereislittleevidencetosuggestanincreasedrisktothefetus.Appropriatelymonitoreduseoftheophylline,inhaledglucocorticosteroids351, β2-agonists,andleukotrienemodifiers(specificallymontelukast)isnotassociatedwithanincreasedincidenceoffetalabnormalities369.Inhaledglucocorticosteroidshavebeenshowntopreventexacerbationsofasthmaduringpregnancy269,270(Evidence B).Asinothersituations,thefocusofasthmatreatmentmustremainoncontrolofsymptomsandmaintenanceofnormallungfunction271.Acuteexacerbationsshouldbetreatedaggressivelyinordertoavoidfetalhypoxia.Treatmentshouldincludenebulizedrapid-actingβ2-agonistsandoxygenandsystemicglucocorticosteroidsshouldbeinstitutedwhennecessary.
Whileallpatientsshouldhaveadequateopportunitytodiscussthesafetyoftheirmedications,pregnantpatientswithasthmashouldbeadvisedthatthegreaterrisktotheirbabylieswithpoorlycontrolledasthma,andthesafetyofmostmodernasthmatreatmentsshouldbestressed.Evenwithagoodpatient/healthcareprofessionalrelationship,independentprintedmaterial,suchasastatementfromtheUSNationalAsthmaEducationandPreventionProgramonthetreatmentofasthmaduringpregnancy272,willprovideimportantadditionalreassurance265,273.
Obesity
Asthmaismoredifficulttocontrolintheobesepatient383-386.Thismaybeduetoadifferenttypeofairwayinflammation(lesseosinophilic),obesity-relatedco-morbiditiessuchasobstructivesleepapneaandgastroesophagealreflux,mechanicalfactorsorotherasyetundefinedfactors.Thereisnotsufficientevidencetosuggestthatthemanagementofasthmaintheobeseshouldbedifferentthaninpatientswithnormalweight.However,thereseemstobeareducedresponsetoinhaledglucocorticosteroidsintheobesepatient,andalthoughthisseemstobelessevidentwithleukotrieneantagonists,inhaledglucocorticosteroidsareconsideredthemainstayofasthmatreatmentinthispopulation385, 386.
Althoughasthmaisnotmoreoftenover-diagnosedinobesecomparedtonon-obesepatients,itisparticularlyimportanttoconfirmthediagnosisbyobjectivemeasuresofvariableairwayobstructionorbronchialhyper-responsiveness,asrespiratorysymptomsassociatedtoobesitymaymimicasthma388.Weightlossintheobesepatientimprovesasthmacontrol,lungfunctionandreducesmedicationneedsandshouldbeincludedinthetreatmentplan94,389,390
Surgery
Airwayhyperresponsiveness,airflowlimitation,andmucushypersecretionpredisposepatientswithasthmatointraoperativeandpostoperativerespiratorycomplications.Thelikelihoodofthesecomplicationsdependsontheseverityofasthmaatthetimeofsurgery,thetypeofsurgery(thoracicandupperabdominalsurgeriesposethegreatestrisks),andtypeofanesthesia(generalanesthesiawithendotrachealintubationcarriesthegreatestrisk).Thesevariablesneedtobeassessedpriortosurgeryandpulmonaryfunctionshouldbemeasured.Ifpossible,thisevaluationshouldbeundertakenseveraldaysbeforesurgerytoallowtimeforadditionaltreatment.Inparticular,ifthepatient’sFEV1islessthan80%ofpersonalbest,abriefcourseoforalglucocorticosteroidsshouldbeconsideredtoreduceairflowlimitation274,275(Evidence C).Furthermore,patientswhohavereceivedsystemicglucocorticosteroidswithinthepast6monthsshouldhavesystemiccoverageduringthesurgicalperiod(100mghydrocortisoneevery8hoursintravenously).Thisshouldberapidlyreduced24hoursfollowingsurgery,asprolongedsystemicglucocorticosteroidtherapymayinhibitwoundhealing276(Evidence C).
COMPONENT 5: SPECIAL CONSIDERATIONS
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 81
Rhinitis, Sinusitis, and Nasal Polyps
Upperairwaydiseasescaninfluencelowerairwayfunctioninsomepatientswithasthma.Althoughthemechanismsbehindthisrelationshiphavenotbeenestablished,inflammationlikelyplaysasimilarlycriticalroleinthepathogenesisofrhinitis,sinusitis,andnasalpolypsasinasthma.
Rhinitis.Themajorityofpatientswithasthmahaveahistoryorevidenceofrhinitisandupto30%ofpatientswithpersistentrhinitishaveordevelopasthma277,278.Rhinitisfrequentlyprecedesasthma,andisbothariskfactorforthedevelopmentofasthma279andisassociatedwithincreasedseverityandhealthresourceuseinasthma280.Rhinitisandasthmashareseveralriskfactors:commonindoorandoutdoorallergenssuchashousedustmites,animaldander,and,lesscommonly,pollenaffectingboththenoseandbronchi281,282,occupationalsensitizers283,andnon-specificfactorslikeaspirin.Forthesereasons,theAllergicRhinitisanditsImpactonAsthma(ARIA)initiativerecommendsthatthepresenceofasthmamustbeconsideredinallpatientswithrhinitis,andthatinplanningtreatment,bothshouldbeconsideredtogether284.
Bothasthmaandrhinitisareconsideredtobeinflammatorydisordersoftheairway,buttherearesomedifferencesbetweenthetwoconditionsinmechanisms,clinicalfeatures,andtreatmentapproach.Althoughtheinflammationofthenasalandbronchialmucosamaybesimilar,nasalobstructionislargelyduetohyperemiainrhinitis,whileairwaysmoothmusclecontractionplaysadominantroleinasthma285.
Treatmentofrhinitismayimproveasthmasymptoms286,287 (Evidence A).Anti-inflammatoryagentsincludingglucocorticosteroidsandcromonesaswellasleukotrienemodifiersandanticholinergicscanbeeffectiveinbothconditions.However,somemedicationsareselectivelyeffectiveagainstrhinitis(e.g.,H1-antagonists)andothersagainstasthma(e.g.,β2-agonists)
288(Evidence A).Useofintra-nasalglucocorticosteroidsforconcurrentrhinitishasbeenfoundtohavealimitedbenefitinimprovingasthmaandreducingasthmamorbidityinsomebutnotallstudies289-291.Leukotrienemodifiers125,292,allergen-specificimmunotherapy284,293,andanti-IgEtherapy294,295 are effective inbothconditions(Evidence A).
AdditionalinformationonthistopicfromtheAllergicRhinitisanditsImpactonAsthma(ARIA)initiativecanbefoundathttp://www.whiar.org284.
Sinusitis.Sinusitisisacomplicationofupperrespiratoryinfections,allergicrhinitis,nasalpolyps,andotherforms
ofnasalobstruction.Bothacuteandchronicsinusitiscanworsenasthma.Clinicalfeaturesofsinusitislackdiagnosticprecision296,andCTScanconfirmationisrecommendedwhenavailable.Inchildrenwithsuspectedrhinosinusitis,antibiotictherapyfor10daysisrecommended(Evidence B).Treatmentshouldalsoincludemedicationstoreducenasalcongestion,suchastopicalnasaldecongestantsortopicalnasalorevensystemicglucocorticosteroids.Theseagentsremainsecondarytoprimaryasthmatherapies279,288.
Nasal polyps.Nasalpolypsassociatedwithasthmaandrhinitis,andsometimeswithaspirinhypersensitivity298, are seenprimarilyinpatientsover40yearsold.Between36%and96%ofaspirin-intolerantpatientshavepolyps,and29%to70%ofpatientswithnasalpolypsmayhaveasthma298,299.Childrenwithnasalpolypsshouldbeassessedforcysticfibrosisandimmotileciliasyndrome.Nasalpolypsarequiteresponsivetotopicalglucocorticosteroids288.Alimitednumberofpatientswithglucocorticosteroid-refractorypolypsmaybenefitfromsurgery.
Occupational Asthma
Onceadiagnosisofoccupationalasthmaisestablished,completeavoidanceoftherelevantexposureisideallyanimportantcomponentofmanagement300-302,412.Occupationalasthmamaypersistevenseveralyearsafterremovalfromexposuretothecausativeagent,especiallywhenthepatienthashadsymptomsforalongtimebeforecessationofexposure303,304.Continuedexposuremayleadtoincreasinglysevereandpotentiallyfatalasthmaexacerbations305,aGastroesophagealRefluxlowerprobabilityofsubsequentremission,and,ultimately,permanentlyimpairedlungfunction306.Pharmacologictherapyforoccupationalasthmaisidenticaltotherapyforotherformsofasthma,butitisnotasubstituteforadequateavoidance.Consultationwithaspecialistinasthmamanagementoroccupationalmedicineisadvisable.
TheBritishOccupationalHealthResearchFoundationGuidelinesfortheprevention,identification,andmanagementofoccupationalasthmaareavailableathttp://www.bohrf.org.uk/downloads/asthevre.pdf.(Seealsoreference421.)
Respiratory Infections
Respiratoryinfectionshaveanimportantrelationshiptoasthmaastheyprovokewheezingandincreasedsymptomsinmanypatients307 and are commonly found inchildrenwithasthmaexacerbation391.Epidemiologicalstudieshavefoundthatinfectiousmicroorganismsassociatedwithincreasedasthmasymptomsareoften
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

82 ASTHMA MANAGEMENT AND PREVENTION
respiratoryviruses308, but seldom bacteria309.Respiratorysyncytialvirusisthemostcommoncauseofwheezingininfancy45,whilerhinoviruses(whichcausethecommoncold),aretheprincipaltriggersofwheezingandworseningofasthmainolderchildrenandadults310.Otherrespiratoryviruses,suchasparainfluenza,influenza,adenovirus,andcoronavirus,arealsoassociatedwithincreasedwheezingandasthmasymptoms311.Adultswithasthmamaybeatincreasedriskofseriouspneumococcaldisease370.
Anumberofmechanismshavebeenidentifiedthatexplainwhyrespiratoryinfectionstriggerwheezingandincreasedairwayresponsiveness,includingdamagetoairwayepithelium,stimulationofvirus-specificIgEantibody,enhancedmediatorrelease,andtheappearanceofalateasthmaticresponsetoinhaledantigen312.Thus,thereisevidencethatviralinfectionsarean“adjuvant”totheinflammatoryresponseandpromotethedevelopmentofairwayinjurybyenhancingairwayinflammation313.
Treatmentofaninfectiousexacerbationfollowsthesameprinciplesastreatmentofotherasthmaexacerbations—thatis,rapid-actinginhaledβ2-agonistsandearlyintroductionoforalglucocorticosteroidsorincreasesininhaledglucocorticosteroidsbyatleastfour-foldarerecommended.Becauseincreasedasthmasymptomscanoftenpersistforweeksaftertheinfectioniscleared,anti-inflammatorytreatmentshouldbecontinuedforthisfullperiodtoensureadequatecontrol.
TheroleofchronicinfectionwithChlamydiapneumoniaeandMycoplasmapneumoniaeinthepathogenesisorworseningofasthmaiscurrentlyuncertain314.Thebenefitfrom macrolide antibiotics remains unclear315-317.Arelativelysmallbutwellconductedstudyshowednoevidenceofbenefitfromtheadditionofclarithromycintoadultswithmildtomoderatelysevereasthmaonlowdoseinhaledglucocorticosteroids413.However,furtherresearchinthisareaisrequired.
Gastroesophageal Reflux.
Thereisconsiderableevidencethatgastroesophagealrefluxismorecommoninpatientswithasthmathaninthegeneralpopulation392.Thishasledtoresearchtodeterminewhethertreatmentofgastroesophagealrefluxcanimproveasthmasymptomsorcontrol.Gastroesophagealrefluxisundoubtedlyacauseofdrycoughandsomeoftheconfusionintheliteratureisprobablyduetopatientswithdrycoughsymptomsbeingattributedtoasthma.Thisrelationshipmayinpartrelatetotheuseofmedicationstomanageasthma,suchasβ2-agonistsandtheophyllinethatcauserelaxationoftheloweresophagealsphincter.
A review320oftheeffectivetreatmentsofgastroesophagealrefluxwithavarietyofmeasuresincludingprotonpumpinhibitors,H2antagonists,andsurgeryfailedtoshowbenefit.Astudyonadultpatientswithsymptomaticasthmawithoutsymptomsofgastroesophagealrefluxfoundthattreatmentwithhighdoseprotonpumpinhibitorsdidnotimprovesymptomsorexacerbationsofasthma393.Inpatientswithmoderatetosevereasthmatreatedwithanti-inflammatoryasthmamedicationsandsymptomaticgastroesophagealreflux,treatmentwithprotonpumpinhibitorsdemonstratedasmallandprobablyclinicallynon-significantimprovementinlungfunctionandqualityof life392.Fewdataareavailableonstudiesoftreatmentforchildrenwithasthmasymptomsandsymptomsofgastroesophagealreflux394.
Insummary,despiteahighprevalenceofasymptomaticgastroesophagealrefluxamongpatientswithpoorlycontrolledasthma,treatmentwithproton-pumpinhibitorsdoesnotimproveasthmacontrolinadults392-394 or children422.Asymptomaticgastroesophagealrefluxisnotalikelycauseofpoorlycontrolledasthma.Surgeryforgastroesophagealrefluxisreservedfortheseverelysymptomaticpatientwithwell-documentedesophagitisandfailureofmedicalmanagement.Inpatientswithasthma,itshouldbedemonstratedthattherefluxcausesasthmasymptomsbeforesurgeryisadvised321,322.
Aspirin-Induced Asthma (AIA)
Upto28%ofadultswithasthma,butrarelychildrenwithasthma,sufferfromasthmaexacerbationsinresponsetoaspirinandothernonsteroidalanti-inflammatorydrugs(NSAIDs).Thissyndromeismorecommoninsevereasthma323.
Theclinicalpictureandcourseofaspirin-inducedasthma(AIA)arecharacteristic324.Themajorityofpatientsfirstexperiencesymptoms,whichmayincludevasomotorrhinitisandprofuserhinorrhea,duringthethirdtofourthdecadeoflife.Chronicnasalcongestionevolves,andphysicalexaminationoftenrevealsnasalpolyps.Asthmaandhypersensitivitytoaspirinoftendevelopsubsequently.Thehypersensitivitytoaspirinpresentsauniquepicture:withinminutestooneortwohoursfollowingingestionofaspirin,anacute,oftensevere,asthmaattackdevelops,andisusuallyaccompaniedbyrhinorrhea,nasalobstruction,conjunctivalirritation,andscarletflushoftheheadandneck.Thismaybeprovokedbyasingleaspirinorothercyclooxygnease-1(COX-1)inhibitorandincludeviolentbronchospasm,shock,lossofconsciousness,andevenrespiratoryarrest325,326.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 83
Persistentmarkedeosinophilicinflammation,epithelialdisruption,cytokineproduction,andupregulationofadhesionmoleculesarefoundintheairwaysofpatientswithAIA327,328.Airwayexpressionofinterleukin-5(IL-5),whichisinvolvedinrecruitmentandsurvivalofeosinophils,is also increased328.AIAisfurthercharacterizedbyincreasedactivationofcysteinylleukotrienepathways,whichmaybepartlyexplainedbyageneticpolymorphismoftheLTC4synthasegenefoundinabout70%percentofpatients329.However,theexactmechanismbywhichaspirintriggersbronchoconstrictionremainsunknown330. Theabilityofacyclooxygenaseinhibitortotriggerreactionsdependsonthedrug’scyclooxygenaseinhibitorypotency,aswellasontheindividualsensitivityofthepatient329.
Acharacteristichistoryofreactionisconsideredadequateforinitiatingavoidancestrategies.However,thediagnosiscanonlybeconfirmedbyaspirinchallenge,astherearenosuitableinvitrotestsfordiagnosis.Theaspirinchallengetestisnotrecommendedforroutinepracticeasitisassociatedwithahighriskofpotentiallyfatalconsequences and must only be conducted in a facility withcardiopulmonaryresuscitationcapabilities331.FurthersafeguardsarethatpatientsshouldonlybechallengedwhentheirasthmaisinremissionandtheirFEV1 is greaterthan70%ofpredictedorpersonalbest.Bronchial(inhalational)andnasalchallengeswithlysineaspirinaresaferthanoralchallengesandmaybeperformedinspecializedcenters332,333.OnceaspirinorNSAIDhypersensitivitydevelops,itispresentforlife.PatientswithAIAshouldavoidaspirin,productscontainingit,otheranalgesicsthatinhibitCOX-1,andoftenalsohydrocortisonehemisuccinate334.Avoidancedoesnotpreventprogressionoftheinflammatorydiseaseoftherespiratorytract.WhereanNSAIDisindicated,acyclooxygenase-2(COX-2)inhibitormaybeconsidered352 withappropriatephysiciansupervisionandobservationforatleastonehourafteradministration335(Evidence B).Glucocorticosteroidscontinuetobethemainstayofasthmatherapy,butleukotrienemodifiersmayalsobeusefulforadditionalcontroloftheunderlyingdisease332,336(Evidence B).ForNSAID-sensitivepatientswithasthmawhorequireNSAIDsforothermedicalconditions,desensitizationmaybeconductedinthehospitalunderthecareofaspecialist337.AspirindesensitizationhasalsobeenusedasatreatmentforAIA,butlong-termimprovementsappeartobemorecommonwithsinussymptomsthanwithlowerairwaydisease.Afteraspirindesensitization,dailyingestionof600-1200mgofaspirinmayreduceinflammatorymucosaldiseasesymptoms,especiallyinthenose,inmostpatientswithAIA332.Generally,asthmapatients,especiallythosewithadultonsetasthmaandassociatedupperairwaydisease(nasalpolyposis),shouldbecounseledtoavoidNSAIDs,takingacetominophen/paracetemolinstead.
Anaphylaxis and Asthma
Anaphylaxisisapotentiallylife-threateningconditionthatcanbothmimicandcomplicatesevereasthma.Effectivetreatmentofanaphylaxisdemandsearlyrecognitionoftheevent.Thepossibilityofanaphylaxisshouldbeconsideredinanysettingwheremedicationorbiologicalsubstancesaregiven,especiallybyinjection.Examplesofdocumentedcausesofanaphylaxisincludetheadministrationofallergenicextractsinimmunotherapy,foodintolerance(nuts,fish,shellfish,eggs,milk),avian-basedvaccines,insectstingsandbites,latexhypersensitivity,drugs(β-lactamantibiotics,aspirinandNSAIDs,andangiotensinconvertingenzyme(ACE)inhibitors),andexercise.
Symptomsofanaphylaxisincludeflushing,pruritis,urticaria,andangioedema;upperandlowerairwayinvolvementsuchasstridor,dyspnea,wheezing,orapnea;dizzinessorsyncopewithorwithouthypotension;andgastrointestinalsymptomssuchasnausea,vomiting,cramping,anddiarrhea.Exercise-inducedanaphylaxis,oftenassociatedwithmedicationorfoodallergy,isauniquephysicalallergyandshouldbedifferentiatedfromexercise-inducedbronchoconstriction338.
Airwayanaphylaxiscouldaccountforthesuddenonsetofasthmaattacksinsevereasthmaandtherelativeresistanceoftheseattackstoincreaseddosesofβ2-agonists180.Ifthereisapossibilitythatanaphylaxisisinvolvedinanasthmaattack,epinephrineshouldbethebronchodilatorofchoice.Prompttreatmentforanaphylaxisiscrucialandincludesoxygen,intramuscularepinephrine,injectableantihistamine,intravenoushydrocortisone,oropharyngealairway,andintravenousfluid.Preventingarecurrenceofanaphylaxisdependsonidentifyingthecauseandinstructingthepatientonavoidancemeasuresandself-administeredemergencytreatmentwithpre-loadedepinephrinesyringes339.
REFERENCES
1. CharltonI,CharltonG,BroomfieldJ,MulleeMA.Evaluationofpeakflowandsymptomsonlyselfmanagementplansforcontrolofasthmaingeneralpractice.BMJ1990;301(6765):1355-9.
2. CoteJ,CartierA,RobichaudP,BoutinH,MaloJL,Rouleau M, et al.Influenceonasthmamorbidityofasthmaeducationprogramsbasedonself-managementplansfollowingtreatmentoptimization.Am J Respir Crit Care Med1997;155(5):1509-14.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

84 ASTHMA MANAGEMENT AND PREVENTION
3. Ignacio-GarciaJM,Gonale-SantosP.Asthmaself-managementeducationprogrambyhomemonitoringofpeakexpiratoryflow.Am J Respir Crit Care Med 1995;151(2Pt1):353-9.
4. JonesKP,MulleeMA,MiddletonM,ChapmanE,HolgateST.Peakflowbasedasthmaself-management:arandomisedcontrolledstudyingeneralpractice.BritishThoracicSocietyResearchCommittee.Thorax 1995;50(8):851-7.
5. LahdensuoA,HaahtelaT,HerralaJ,KavaT,KivirantaK, Kuusisto P, et al.Randomisedcomparisonofguidedselfmanagementandtraditionaltreatmentofasthmaoveroneyear.BMJ1996;312(7033):748-52.
6. TurnerMO,TaylorD,BennettR,FitzGeraldJM.Arandomizedtrialcomparingpeakexpiratoryflowandsymptomself-managementplansforpatientswithasthmaattendingaprimarycareclinic.Am J Respir Crit Care Med1998;157(2):540-6.
7. SommarugaM,SpanevelloA,MiglioriGB,NeriM,CallegariS,MajaniG.Theeffectsofacognitivebehaviouralinterventioninasthmaticpatients.Monaldi Arch Chest Dis1995;50(5):398-402.
8. CowieRL,RevittSG,UnderwoodMF,FieldSK.Theeffectofapeakflow-basedactionplaninthepreventionofexacerbationsofasthma.Chest 1997;112(6):1534-8.
9. KohlerCL,DaviesSL,BaileyWC.Howtoimplementanasthmaeducationprogram.Clin Chest Med 1995;16(4):557-65.
10. BaileyWC,RichardsJM,Jr.,BrooksCM,SoongSJ,WindsorRA,ManellaBA.Arandomizedtrialtoimproveself-managementpracticesofadultswithasthma.Arch Intern Med1990;150(8):1664-8.
11. MurphyVE,GibsonPG,TalbotPI,KessellCG,CliftonVL.Asthmaself-managementskillsandtheuseofasthmaeducationduringpregnancy.Eur Respir J 2005;26(3):435-41.
12. ShahS,PeatJK,MaurskiEJ,WangH,SindhusakeD,Bruce C, et al.Effectofpeerledprogrammeforasthmaeducation in adolescents: cluster randomised controlled trial.BMJ2001;322(7286):583-5.
13. GuevaraJP,WolfFM,GrumCM,ClarkNM.Effectsofeducationalinterventionsforselfmanagementofasthmainchildrenandadolescents:systematicreviewandmeta-analysis.BMJ2003;326(7402):1308-9.
14. GriffithsC,FosterG,BarnesN,EldridgeS,TateH,BegumS,et al.Specialistnurseinterventiontoreduceunscheduledasthmacareinadeprivedmultiethnicarea:theeastLondonrandomisedcontrolledtrialforhighriskasthma(ELECTRA).BMJ2004;328(7432):144.
15. PowellH,GibsonPG.Optionsforself-managementeducationforadultswithasthma.Cochrane Database Syst Rev2003(1):CD004107.
16. GibsonPG,PowellH,CoughlanJ,WilsonAJ,Abramson M, Haywood P, et al.Self-managementeducationandregularpractitionerreviewforadultswithasthma.Cochrane Database Syst Rev 2003(1):CD001117.
17. Haby MM, Waters E, Robertson CF, Gibson PG, DucharmeFM.Interventionsforeducatingchildrenwhohaveattendedtheemergencyroomforasthma.Cochrane Database Syst Rev 2001;1.
18. GibsonPG,PowellH,CoughlanJ,WilsonAJ,HensleyMJ,AbramsonM, et al.Limited(informationonly)patienteducationprogramsforadultswithasthma.Cochrane Database Syst Rev2002(2):CD001005.
19. CabanaMD,SlishKK,EvansD,MellinsRB,Brown RW, Lin X, et al.ImpactofphysicianasthmacareeducationonpatientoutcomesPediatrics 2006;117:2149-57.
20. LevyM,BellL.Generalpracticeauditofasthmainchildhood.BMJ(ClinResEd)1984;289(6452):1115-6.
21. OngLM,deHaesJC,HoosAM,LammesFB.Doctor-patientcommunication:areviewoftheliterature.Soc Sci Med1995;40(7):903-18.
22. StewartMA.Effectivephysician-patientcommunicationandhealthoutcomes:areview.CMAJ 1995;152(9):1423-33.
23. PartridgeMR,HillSR.Enhancingcareforpeoplewithasthma:theroleofcommunication,education,trainingandself-management.1998WorldAsthmaMeetingEducationandDeliveryofCareWorkingGroup.Eur Respir J2000;16(2):333-48.
24. ClarkNM,CabanaMD,NanB,GongZM,SlishKK,BirkNA,KacirotiN.Theclinician-patientpartnershipparadigm:outcomesassociatedwithphysiciancommunicationbehavior.Clin Pediatr (Phila) 2008 Jan;47(1):49-57.
25. CegalaDJ,MarinelliT,PostD.Theeffectsofpatientcommunicationskillstrainingoncompliance.Arch Fam Med2000;9(1):57-64.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 85
26. ChapmanKR,VoshaarTH,VirchowJC.Inhalerchoiceinprimarycare.Eur Respir Rev2005;14(96):117-22.
27. DolovichMB,AhrensRC,HessDR,AndersonP,DhandR,RauJL,et al.Deviceselectionandoutcomesofaerosoltherapy:Evidence-basedguidelines:AmericanCollegeofChestPhysicians/AmericanCollegeofAsthma,Allergy,andImmunology.Chest 2005;127(1):335-71.
28. VoshaarT,AppEM,BerdelD,BuhlR,FischerJ,Gessler T, et al.[Recommendationsforthechoiceofinhalatorysystemsfordrugprescription].Pneumologie 2001;55(12):579-86.
29. MeadeCD,McKinneyWP,BarnasGP.Educatingpatientswithlimitedliteracyskills:theeffectivenessofprintedandvideotapedmaterialsaboutcoloncancer.Am J Public Health1994;84(1):119-21.
30. HoutsPS,BachrachR,WitmerJT,TringaliCA,BucherJA,LocalioRA.Usingpictographstoenhancerecallofspokenmedicalinstructions.Patient Educ Couns 1998;35(2):83-8.
31. FishwickD,D’SouzaW,BeasleyR.Theasthmaself-managementplansystemofcare:whatdoesitmean,howisitdone,doesitwork,whatmodelsareavailable,whatdopatientswantandwhoneedsit?Patient Educ Couns1997;32(1Suppl):S21-33.
32. GibsonPG,PowellH.Writtenactionplansforasthma:anevidence-basedreviewofthekeycomponents.Thorax2004;59(2):94-9.
33. NewmanSP.InhalertreatmentoptionsinCOPD.Eur Respir Rev2005;14(96):102-8.
34. CouttsJA,GibsonNA,PatonJY.Measuringcompliancewithinhaledmedicationinasthma.Arch Dis Child1992;67(3):332-3.
35. FranchiM,CarrerP.Indoorairqualityinschools:theEFAproject.Monaldi Arch Chest Dis2002;57(2):120-2.
36. ArshadSH.Primarypreventionofasthmaandallergy.J Allergy Clin Immunol2005;116(1):3-14.
37. BousquetJ,YsselH,VignolaAM.Isallergicasthmaassociatedwithdelayedfetalmaturationorthepersistenceofconservedfetalgenes?Allergy 2000;55(12):1194-7.
38. JonesCA,HollowayJA,WarnerJO.Doesatopicdiseasestartinfoetallife?Allergy 2000;55(1):2-10.
39. KramerMS.Maternalantigenavoidanceduringpregnancyforpreventingatopicdiseaseininfantsofwomenathighrisk.Cochrane Database Syst Rev 2000;2.
40. FriedmanNJ,ZeigerRS.Theroleofbreast-feedinginthedevelopmentofallergiesandasthma.J Allergy Clin Immunol2005;115(6):1238-48.
41. GdalevichM,MimouniD,MimouniM.Breast-feedingandtheriskofbronchialasthmainchildhood:asystematicreviewwithmeta-analysisofprospectivestudies.J Pediatr2001;139(2):261-6.
42. RobinsonDS,LarcheM,DurhamSR.Tregsandallergicdisease.J Clin Invest2004;114(10):1389-97.
43. IsolauriE,SutasY,KankaanpaaP,ArvilommiH,SalminenS.Probiotics:effectsonimmunity.Am J Clin Nutr2001;73(2Suppl):444S-50S.
44. OwnbyDR,JohnsonCC,PetersonEL.Exposuretodogsandcatsinthefirstyearoflifeandriskofallergicsensitizationat6to7yearsofage.JAMA 2002;288(8):963-72.
45. MartinezFD,WrightAL,TaussigLM,HolbergCJ,HalonenM,MorganWJ.Asthmaandwheezinginthefirstsixyearsoflife.TheGroupHealthMedicalAssociates.N Engl J Med 1995;332(3):133-8.
46. DezateuxC,StocksJ,DundasI,FletcherME.Impairedairwayfunctionandwheezingininfancy:theinfluenceofmaternalsmokingandageneticpredispositiontoasthma.Am J Respir Crit Care Med1999;159(2):403-10.
47. StrachanDP,CookDG.Healtheffectsofpassivesmoking.5.Parentalsmokingandallergicsensitisationinchildren.Thorax1998;53(2):117-23.
48. StrachanDP,CookDG.Healtheffectsofpassivesmoking.1.Parentalsmokingandlowerrespiratoryillnessininfancyandearlychildhood.Thorax 1997;52(10):905-14.
49. KuligM,LuckW,LauS,NiggemannB,BergmannR,KlettkeU,et al. Effectofpre-andpostnataltobaccosmokeexposureonspecificsensitizationtofoodandinhalantallergensduringthefirst3yearsoflife.MulticenterAllergyStudyGroup,Germany.Allergy 1999;54(3):220-8.
50. IikuraY,NaspitCK,MikawaH,TalaricofichoS,Baba M, Sole D, et al. Preventionofasthmabyketotifenininfantswithatopicdermatitis.Ann Allergy 1992;68(3):233-6.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

86 ASTHMA MANAGEMENT AND PREVENTION
51. Allergicfactorsassociatedwiththedevelopmentofasthmaandtheinfluenceofcetirizineinadouble-blind,randomised,placebo-controlledtrial:firstresultsofETAC.EarlyTreatmentoftheAtopicChild.Pediatr Allergy Immunol 1998;9(3):116-24.
52. JohnstoneDE,DuttonA.Thevalueofhyposensitizationtherapyforbronchialasthmainchildren--a14-yearstudy.Pediatrics1968;42(5):793-802.
53. MollerC,DreborgS,FerdousiHA,HalkenS,HostA,JacobsenL,et al.Pollenimmunotherapyreducesthedevelopmentofasthmainchildrenwithseasonalrhinoconjunctivitis(thePAT-study).J Allergy Clin Immunol2002;109(2):251-6.
54. GotzschePC,HammarquistC,BurrM.Housedustmitecontrolmeasuresinthemanagementofasthma:meta-analysis.BMJ 1998;317(7166):1105-10.
55. GotzschePC,JohansenHK,SchmidtLM,BurrML.Housedustmitecontrolmeasuresforasthma.Cochrane Database Syst Rev 2004(4):CD001187.
56. ShefferAL.Allergenavoidancetoreduceasthma-relatedmorbidity.N Engl J Med2004;351(11):1134-6.
57. Platts-MillsTA.Allergenavoidanceinthetreatmentofasthmaandrhinitis.N Engl J Med2003;349(3):207-8.
58. MorganWJ,CrainEF,GruchallaRS,O’ConnorGT,Kattan M, Evans R, 3rd, et al.Resultsofahome-basedenvironmentalinterventionamongurbanchildrenwithasthma.N Engl J Med2004;351(11):1068-80.
59. Platts-MillsTA,ThomasWR,AalberseRC,VervloetD,ChampmanMD.Dustmiteallergensandasthma:reportofasecondinternationalworkshop.J Allergy Clin Immunol 1992;89(5):1046-60.
60. CustovicA,WijkRG.Theeffectivenessofmeasurestochangetheindoorenvironmentinthetreatmentofallergicrhinitisandasthma:ARIAupdate(incollaborationwithGA(2)LEN).Allergy2005;60(9):1112-5.
61. LuczynskaC,TredwellE,SmeetonN,BurneyP.Arandomizedcontrolledtrialofmiteallergen-impermeablebedcoversinadultmite-sensitizedasthmatics.Clin Exp Allergy2003;33(12):1648-53.
62. WoodcockA,ForsterL,MatthewsE,MartinJ,LetleyL,VickersM, et al.Controlofexposuretomiteallergenandallergen-impermeablebedcoversforadultswithasthma.N Engl J Med2003;349(3):225-36.
63. HalkenS,HostA,NiklassenU,HansenLG,NielsenF, Pedersen S, et al.Effectofmattressandpillowencasingsonchildrenwithasthmaandhousedustmiteallergy.J Allergy Clin Immunol2003;111(1):169-76.
64. CustovicA,GreenR,TaggartSC,SmithA,PickeringCA,ChapmanMD,et al.Domesticallergensinpublicplaces.II:Dog(Canf1)andcockroach(Blag2)allergensindustandmite,cat,dogandcockroachallergensintheairinpublicbuildings.Clin Exp Allergy 1996;26(11):1246-52.
65. AlmqvistC,LarssonPH,EgmarAC,HedrenM,MalmbergP,WickmanM.Schoolasariskenvironmentforchildrenallergictocatsandasitefortransferofcatallergentohomes.J Allergy Clin Immunol 1999;103(6):1012-7.
66. EnbergRN,ShamieSM,McCulloughJ,OwnbyDR.Ubiquitouspresenceofcatallergenincat-freebuildings:probabledispersalfromhumanclothing.Ann Allergy1993;70(6):471-4.
67. WoodRA,ChapmanMD,AdkinsonNF,Jr.,EgglestonPA.Theeffectofcatremovalonallergencontentinhousehold-dustsamples.J Allergy Clin Immunol 1989;83(4):730-4.
68. EgglestonPA,WoodRA,RandC,NixonWJ,ChenPH,LukkP.Removalofcockroachallergenfrominner-cityhomes.J Allergy Clin Immunol 1999;104(4Pt1):842-6.
69. DenningDW,O’DriscollBR,HogaboamCM,BowyerP,NivenRM.Thelinkbetweenfungiandsevereasthma:asummaryoftheevidence.Eur Respir J 2006;27(3):615-26.
70. HirschT,HeringM,BurknerK,HirschD,LeupoldW,KerkmannML,et al.House-dust-miteallergenconcentrations(Derf1)andmoldsporesinapartmentbedrooms before and after installation of insulated windowsandcentralheatingsystems.Allergy2000;55(1):79-83.
71. ChaudhuriR,LivingstonE,McMahonAD,ThomsonL,BorlandW,ThomsonNC.Cigarettesmokingimpairsthetherapeuticresponsetooralcorticosteroidsinchronicasthma.Am J Respir Crit Care Med 2003;168(11):1308-11.
72. ChalmersGW,MacleodKJ,LittleSA,ThomsonLJ,McSharryCP,ThomsonNC.Influenceofcigarettesmokingoninhaledcorticosteroidtreatmentinmildasthma. Thorax2002;57(3):226-30.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 87
73. UphamJW,HoltPG.Environmentanddevelopmentofatopy.Curr Opin Allergy Clin Immunol2005;5(2):167-72.
74. BarnettAG,WilliamsGM,SchwartJ,NellerAH,BestTL,PetroeschevskyAL,et al.Airpollutionandchildrespiratoryhealth:acase-crossoverstudyinAustraliaandNewZealand.Am J Respir Crit Care Med 2005;171(11):1272-8.
75. DalesRE,CakmakS,JudekS,DannT,CoatesF,BrookJR,et al.InfluenceofoutdooraeroallergensonhospitalizationforasthmainCanada.J Allergy Clin Immunol2004;113(2):303-6.
76. AntoJM,SorianoJB,SunyerJ,RodrigoMJ,MorellF,RocaJ, et al.Longtermoutcomeofsoybeanepidemicasthmaafteranallergenreductionintervention.Thorax 1999;54(8):670-4.
77. ChenLL,TagerIB,PedenDB,ChristianDL,FerrandoRE,WelchBS,et al.Effectofozoneexposureonairwayresponsestoinhaledallergeninasthmaticsubjects.Chest2004;125(6):2328-35.
78. MarksGB,ColquhounJR,GirgisST,KoskiMH,TreloarAB, Hansen P, et al.Thunderstormoutflowsprecedingepidemicsofasthmaduringspringandsummer.Thorax 2001;56(6):468-71.
79. NewsonR,StrachanD,ArchibaldE,EmberlinJ,HardakerP,CollierC.Acuteasthmaepidemics,weatherandpolleninEngland,1987-1994.Eur Respir J1998;11(3):694-701.
80. NicholsonPJ,CullinanP,TaylorAJ,BurgePS,BoyleC.Evidencebasedguidelinesfortheprevention,identification,andmanagementofoccupationalasthma.Occup Environ Med2005;62(5):290-9.
81. VandenplasO,DelwicheJP,DepelchinS,SibilleY,VandeWeyerR,DelaunoisL.Latexgloveswithalowerproteincontentreducebronchialreactionsinsubjectswithoccupationalasthmacausedbylatex.Am J Respir Crit Care Med1995;151(3Pt1):887-91.
82. HuntLW,Boone-OrkeJL,FranswayAF,FremstadCE,JonesRT,SwansonMC,et al.Amedical-center-wide,multidisciplinaryapproachtotheproblemofnaturalrubberlatexallergy.J Occup Environ Med 1996;38(8):765-70.
83. SichererSH,SampsonHA.9.Foodallergy.J Allergy Clin Immunol2006;117(2SupplMini-Primer):S470-5.
84. RobertsG,PatelN,Levi-SchafferF,HabibiP,LackG.Foodallergyasariskfactorforlife-threateningasthmainchildhood:acase-controlledstudy.J Allergy Clin Immunol2003;112(1):168-74.
85. TaylorSL,BushRK,SelnerJC,NordleeJA,WienerMB, Holden K, et al.Sensitivitytosulfitedfoodsamongsulfite-sensitivesubjectswithasthma.J Allergy Clin Immunol1988;81(6):1159-67.
86. SzczeklikA,NizankowskaE,BochenekG,NagrabaK,MejzaF,SwierczynskaM.SafetyofaspecificCOX-2inhibitorinaspirin-inducedasthma.Clin Exp Allergy 2001;31(2):219-25.
87. CovarRA,MacomberBA,SeflerSJ.Medicationsasasthmatriggers.Immunol Allergy Clin North Am 2005;25(1):169-90.
88. NicholsonKG,Nguyen-Van-TamJS,AhmedAH,WiselkaMJ,LeeseJ,AyresJ,et al. Randomised placebo-controlledcrossovertrialoneffectofinactivatedinfluenzavaccineonpulmonaryfunctioninasthma.Lancet 1998;351(9099):326-31.
89. BuevingHJ,BernsenRM,deJongsteJC,vanSuijlekom-SmitLW,RimmelwaanGF,OsterhausAD,et al.Influenzavaccinationinchildrenwithasthma:randomizeddouble-blindplacebo-controlledtrial.Am J Respir Crit Care Med2004;169(4):488-93.
90. CatesCJ,JeffersonTO,RoweBH.Vaccinesforpreventinginfluenzainpeoplewithasthma.Cochrane Database Syst Rev2008Apr16;(2):CD000364.
91. Thesafetyofinactivatedinfluenzavaccineinadultsandchildrenwithasthma.N Engl J Med 2001;345(21):1529-36.
92. BergenR,BlackS,ShinefieldH,LewisE,RayP,HansenJ, et al.Safetyofcold-adaptedliveattenuatedinfluenzavaccineinalargecohortofchildrenandadolescents.Pediatr Infect Dis J2004;23(2):138-44.
93. TantisiraKG,LitonjuaAA,WeissST,FuhlbriggeAL.AssociationofbodymasswithpulmonaryfunctionintheChildhoodAsthmaManagementProgram(CAMP).Thorax 2003;58(12):1036-41.
94. Stenius-AarnialaB,PoussaT,KvarnstromJ,GronlundEL,YlikahriM,MustajokiP.Immediateandlongtermeffectsofweightreductioninobesepeoplewithasthma:randomisedcontrolledstudy.BMJ 2000;320(7238):827-32.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

88 ASTHMA MANAGEMENT AND PREVENTION
95. RietveldS,vanBeestI,EveraerdW.Stress-inducedbreathlessnessinasthma.Psychol Med 1999;29(6):1359-66.
96. SandbergS,PatonJY,AholaS,McCannDC,McGuinness D, Hillary CR, et al.Theroleofacuteandchronicstressinasthmaattacksinchildren.Lancet 2000;356(9234):982-7.
97. LehrerPM,IsenbergS,HochronSM.Asthmaandemotion:areview.J Asthma1993;30(1):5-21.
98. NouwenA,FreestonMH,LabbeR,BouletLP.Psychologicalfactorsassociatedwithemergencyroomvisitsamongasthmaticpatients.Behav Modif 1999;23(2):217-33.
99. RachelefskyGS,KatRM,SiegelSC.Chronicsinusdiseasewithassociatedreactiveairwaydiseaseinchildren.Pediatrics1984;73(4):526-9.
100.HardingSM,GuzoMR,RichterJE.Theprevalenceofgastroesophagealrefluxinasthmapatientswithoutrefluxsymptoms.Am J Respir Crit Care Med 2000;162(1):34-9.
101.PattersonPE,HardingSM.Gastroesophagealrefluxdisordersandasthma.Curr Opin Pulm Med 1999;5(1):63-7.
102.ChienS,MintzS.Pregnancyandmenses.In:WeissEB,SteinM,eds.Bronchial asthma Mechanisms and therapeutics. Boston:LittleBrown;1993:p.1085-98.
103.BarronWM,LeffAR.Asthmainpregnancy.Am Rev Respir Dis1993;147(3):510-1.
104.BatemanED,BousheyHA,BousquetJ,BusseWW,ClarkTJ,PauwelsRA,et al.Canguideline-definedasthmacontrolbeachieved?TheGainingOptimalAsthmaControlstudy.Am J Respir Crit Care Med 2004;170(8):836-44.
105.NathanRA,SorknessCA,KosinskiM,SchatM,LiJT,Marcus P, et al.Developmentoftheasthmacontroltest:asurveyforassessingasthmacontrol.J Allergy Clin Immunol2004;113(1):59-65.
106.JuniperEF,O’ByrnePM,GuyattGH,FerriePJ,KingDR.Developmentandvalidationofaquestionnairetomeasureasthmacontrol.Eur Respir J1999;14:902-7.
107.JuniperEF,BousquetJ,AbetL,BatemanED.Identifying‘well-controlled’and‘notwell-controlled’asthmausingtheAsthmaControlQuestionnaire.Respir Med2005.
108.JuniperEF,SvenssonK,MorkAC,StahlE.Measurementpropertiesandinterpretationofthreeshortenedversionsoftheasthmacontrolquestionnaire.Respir Med2005;99(5):553-8.
109.VollmerWM,MarksonLE,O’ConnorE,SanockiLL,FittermanL,BergerM,et al.Associationofasthmacontrolwithhealthcareutilizationandqualityoflife.Am J Respir Crit Care Med1999;160(5Pt1):1647-52.
110.BouletLP,BouletV,MilotJ.Howshouldwequantifyasthmacontrol?Aproposal.Chest2002;122(6):2217-23.
111.O’ByrnePM,BarnesPJ,Rodrigue-RoisinR,Runnerstrom E, Sandstrom T, Svensson K, et al. Lowdoseinhaledbudesonideandformoterolinmildpersistentasthma:theOPTIMArandomizedtrial.Am J Respir Crit Care Med2001;164(8Pt1):1392-7.
112.Pauwels RA, Pedersen S, Busse WW, Tan WC, ChenYZ,OhlssonSV, et al.Earlyinterventionwithbudesonideinmildpersistentasthma:arandomised,double-blindtrial. Lancet2003;361(9363):1071-6.
113.ZeigerRS,BakerJW,KaplanMS,PearlmanDS,SchatM,BirdS,et al. Variabilityofsymptomsinmildpersistentasthma:baselinedatafromtheMIAMIstudy.Respir Med2004;98(9):898-905.
114.Usingbeta2-stimulantsinasthma.Drug Ther Bull 1997;35(1):1-4.
115.GodfreyS,Bar-YishayE.Exercise-inducedasthmarevisited.Respir Med 1993;87(5):331-44.
116.FogelRB,RosarioN,AristizabalG,LoeysT,NoonanG,GaileS,SmugarSS,PolosPG.Effectofmontelukastorsalmeteroladdedtoinhaledfluticasoneonexercise-inducedbronchoconstrictioninchildren.Ann Allergy Asthma Immunol2010;104:511-7.
117.SpoonerCH,SaundersLD,RoweBH.Nedocromilsodiumforpreventingexercise-inducedbronchoconstriction.Cochrane Database Syst Rev 2000;2.
118.ReiffDB,ChoudryNB,PrideNB,IndPW.Theeffectofprolongedsubmaximalwarm-upexerciseonexercise-inducedasthma.Am Rev Respir Dis1989;139(2):479-84.
119.RamFS,RobinsonSM,BlackPN.Physicaltrainingforasthma.Cochrane Database Syst Rev2000;2.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 89
120.AdamsNP,BestallJB,MaloufR,LassersonTJ,JonesPW.Inhaledbeclomethasoneversusplaceboforchronicasthma.Cochrane Database Syst Rev 2005(1):CD002738.
121.DrazenJM,IsraelE,O’ByrnePM.Treatmentofasthmawithdrugsmodifyingtheleukotrienepathway.N Engl J Med1999;340(3):197-206.
122.BarnesNC,MillerCJ.Effectofleukotrienereceptorantagonisttherapyontheriskofasthmaexacerbationsinpatientswithmildtomoderateasthma:anintegratedanalysisofzafirlukasttrials.Thorax2000;55(6):478-83.
123.BleeckerER,WelchMJ,WeinsteinSF,KalbergC,JohnsonM,EdwardsL,et al.Low-doseinhaledfluticasonepropionateversusoralzafirlukastinthetreatmentofpersistentasthma.J Allergy Clin Immunol 2000;105(6Pt1):1123-9.
124.WilsonAM,DempseyOJ,SimsEJ,LipworthBJ.Acomparisonoftopicalbudesonideandoralmontelukastinseasonalallergicrhinitisandasthma.Clin Exp Allergy 2001;31(4):616-24.
125.PhilipG,NayakAS,BergerWE,LeynadierF,VrijensF, Dass SB, et al.Theeffectofmontelukastonrhinitissymptomsinpatientswithasthmaandseasonalallergicrhinitis.Curr Med Res Opin2004;20(10):1549-58.
126.DahlR,LarsenBB,VengeP.Effectoflong-termtreatmentwithinhaledbudesonideortheophyllineonlungfunction,airwayreactivityandasthmasymptoms.Respir Med2002;96(6):432-8.
127.KidneyJ,DomingueM,TaylorPM,RoseM,ChungKF,BarnesPJ.Immunomodulationbytheophyllineinasthma.Demonstrationbywithdrawaloftherapy.Am J Respir Crit Care Med1995;151(6):1907-14.
128.SullivanP,BekirS,JaffarZ,PageC,JefferyP,CostelloJ.Anti-inflammatoryeffectsoflow-doseoraltheophyllineinatopicasthma.Lancet 1994;343(8904):1006-8.
129.EvansDJ,TaylorDA,ZetterstromO,ChungKF,O’ConnorBJ,BarnesPJ.Acomparisonoflow-doseinhaledbudesonideplustheophyllineandhigh-doseinhaledbudesonideformoderateasthma.N Engl J Med 1997;337(20):1412-8.
130.RivingtonRN,BouletLP,CoteJ,KreismanH,SmallDI,Alexander M, et al.EfficacyofUniphyl,salbutamol,andtheircombinationinasthmaticpatientsonhigh-doseinhaledsteroids.Am J Respir Crit Care Med1995;151(2Pt1):325-32.
131.TsiuSJ,SelfTH,BurnsR.Theophyllinetoxicity:update.Ann Allergy1990;64(2Pt2):241-57.
132.EllisEF.Theophyllinetoxicity.J Allergy Clin Immunol 1985;76(2Pt2):297-301.
133.OstergaardP,PedersenS.Theeffectofinhaleddisodiumcromoglycateandbudesonideonbronchialresponsivenesstohistamineandexerciseinasthmaticchildren:aclinicalcomparison.In:GodfreyS,ed.Glucocortiocosteroids in childhood asthma.1987:55-65.
134.FrancisRS,McEneryG.Disodiumcromoglycatecomparedwithbeclomethasonedipropionateinjuvenileasthma.Clin Allergy1984;14(6):537-40.
135.TascheMJ,UijenJH,BernsenRM,deJongsteJC,vanderWoudenJC.Inhaleddisodiumcromoglycate(DSCG)asmaintenancetherapyinchildrenwithasthma:asystematicreview.Thorax2000;55(11):913-20.
136.TascheMJ,vanderWoudenJC,UijenJH,PonsioenBP,BernsenRM,vanSuijlekom-SmitLW,et al.Randomisedplacebo-controlledtrialofinhaledsodiumcromoglycatein1-4-year-oldchildrenwithmoderateasthma.Lancet 1997;350(9084):1060-4.
137.LemanskeRF,Jr.,SorknessCA,MaugerEA,LazarusSC,BousheyHA,FahyJV,et al.Inhaledcorticosteroidreductionandeliminationinpatientswithpersistentasthmareceivingsalmeterol:arandomizedcontrolledtrial.JAMA2001;285(20):2594-603.
138.LazarusSC,BousheyHA,FahyJV,ChinchilliVM,LemanskeRF,Jr.,SorknessCA,et al.Long-actingbeta2-agonistmonotherapyvscontinuedtherapywithinhaledcorticosteroidsinpatientswithpersistentasthma:arandomizedcontrolledtrial.JAMA 2001;285(20):2583-93.
139.PearlmanDS,ChervinskyP,LaForceC,SelterJM,SouthernDL,KempJP,et al.Acomparisonofsalmeterolwithalbuterolinthetreatmentofmild-to-moderateasthma.N Engl J Med1992;327(20):1420-5.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

90 ASTHMA MANAGEMENT AND PREVENTION
140.KestenS,ChapmanKR,BroderI,CartierA,HylandRH,KnightA,et al. Athree-monthcomparisonoftwicedailyinhaledformoterolversusfourtimesdailyinhaledalbuterolinthemanagementofstableasthma.Am Rev Respir Dis1991;144(3Pt1):622-5.
141.WenzelSE,LumryW,ManningM,KalbergC,CoxF, Emmett A, et al.Efficacy,safety,andeffectsonqualityoflifeofsalmeterolversusalbuterolinpatientswithmildtomoderatepersistentasthma.Ann Allergy Asthma Immunol 1998;80(6):463-70.
142.ShrewsburyS,PykeS,BrittonM.Meta-analysisofincreaseddoseofinhaledsteroidoradditionofsalmeterolinsymptomaticasthma(MIASMA).BMJ 2000;320(7246):1368-73.
143.GreeningAP,IndPW,NorthfieldM,ShawG.Addedsalmeterolversushigher-dosecorticosteroidinasthmapatientswithsymptomsonexistinginhaledcorticosteroid.Allen&HanburysLimitedUKStudyGroup. Lancet 1994;344(8917):219-24.
144.WoolcockA,LundbackB,RingdalN,JacquesLA.Comparisonofadditionofsalmeteroltoinhaledsteroidswithdoublingofthedoseofinhaledsteroids.Am J Respir Crit Care Med1996;153(5):1481-8.
145.PauwelsRA,SearsMR,CampbellM,VillasanteC,HuangS,LindhA,et al.Formoterolasreliefmedicationinasthma:aworldwidesafetyandeffectivenesstrial.Eur Respir J2003;22(5):787-94.
146.IndPW,VillasanteC,ShinerRJ,PietinalhoA,BoszormenyiNG,SolimanS,et al. Safety of formoterol byTurbuhalerasrelievermedicationcomparedwithterbutalineinmoderateasthma.Eur Respir J 2002;20(4):859-66.
147.Referencedeleted.
148.RodrigoGJ,NeffenH,ColodencoFD,Castro-RodriguezJA.Formoterolforacuteasthmaintheemergencydepartment:asystematicreviewwithmeta-analysis.Ann Allergy Asthma Immunol2010;104(3):247-52.
149.BalanagVM,YunusF,YangPC,JorupC.Efficacyandsafetyofbudesonide/formoterolcomparedwithsalbutamolinthetreatmentofacuteasthma.Pulm Pharmacol Ther2006;19(2):139-47.
150.Reference deleted
151.VerberneAA,FrostC,DuivermanEJ,GrolMH,KerrebijnKF.Additionofsalmeterolversusdoublingthedoseofbeclomethasoneinchildrenwithasthma.TheDutchAsthmaStudyGroup.Am J Respir Crit Care Med 1998;158(1):213-9.
152.BisgaardH.Long-actingbeta(2)-agonistsinmanagementofchildhoodasthma:Acriticalreviewoftheliterature.Pediatr Pulmonol2000;29(3):221-34.
153.BisgaardH.Effectoflong-actingbeta2agonistsonexacerbationratesofasthmainchildren.Pediatr Pulmonol2003;36(5):391-8.
154.O’ByrnePM,BisgaardH,GodardPP,PistolesiM,PalmqvistM,ZhuY,et al.Budesonide/formoterolcombinationtherapyasbothmaintenanceandrelievermedicationinasthma.Am J Respir Crit Care Med 2005;171(2):129-36.
155.ScicchitanoR,AalbersR,UkenaD,ManjraA,FouquertL, Centanni S, et al.Efficacyandsafetyofbudesonide/formoterolsingleinhalertherapyversusahigherdoseofbudesonideinmoderatetosevereasthma.Curr Med Res Opin2004;20(9):1403-18.
156.RabeKF,PizichiniE,StallbergB,RomeroS,BalanatAM, Atien a T, et al. Budesonide/formoterolinasingleinhalerformaintenanceandreliefinmild-to-moderateasthma:arandomized,double-blindtrial.Chest 2006;129(2):246-56.
157.VogelmeierC,D’UrzoA,PauwelsR,MerinoJM,JaspalM, Boutet S, et al. Budesonide/formoterol maintenance andrelievertherapy:aneffectiveasthmatreatmentoption?Eur Respir J 2005;26(5):819-28.
158.DucharmeFM,NiChroininM,GreenstoneI,LassersonTJ.Additionoflong-actingbeta2-agoniststoinhaledsteroidsversushigherdoseinhaledsteroidsinadultsandchildrenwithpersistentasthma.Cochrane Database Syst Rev2010:CD005533.
159.PauwelsRA,LofdahlCG,PostmaDS,TattersfieldAE,O’ByrneP,BarnesPJ,et al.Effectofinhaledformoterolandbudesonideonexacerbationsofasthma.FormoterolandCorticosteroidsEstablishingTherapy(FACET)InternationalStudyGroup.N Engl J Med 1997;337(20):1405-11.
160.SzeflerSJ,MartinRJ,KingTS,BousheyHA,CherniackRM,ChinchilliVM, et al.Significantvariabilityinresponsetoinhaledcorticosteroidsforpersistentasthma.J Allergy Clin Immunol 2002;109(3):410-8.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 91
161.PowellH,GibsonPG.Inhaledcorticosteroiddosesinasthma:anevidence-basedapproach.Med J Aust 2003;178(5):223-5.
162.BrownPH,GreeningAP,CromptonGK.Largevolumespacerdevicesandtheinfluenceofhighdosebeclomethasonedipropionateonhypothalamo-pituitary-adrenalaxisfunction.Thorax 1993;48(3):233-8.
163.CatesCC,BaraA,CrillyJA,RoweBH.Holdingchambersversusnebulisersforbeta-agonisttreatmentofacuteasthma.Cochrane Database Syst Rev 2003(3):CD000052.
164.TurnerMO,PatelA,GinsburgS,FitzGeraldJM.Bronchodilatordeliveryinacuteairflowobstruction.Ameta-analysis.Arch Intern Med 1997;157(15):1736-44.
165.LavioletteM,MalmstromK,LuS,ChervinskyP,PujetJC,PesekI, et al.Montelukastaddedtoinhaledbeclomethasoneintreatmentofasthma.Montelukast/BeclomethasoneAdditivityGroup.Am J Respir Crit Care Med1999;160(6):1862-8.
166.LofdahlCG,ReissTF,LeffJA,IsraelE,NoonanMJ,Finn AF, et al.Randomised,placebocontrolledtrialofeffectofaleukotrienereceptorantagonist,montelukast,ontaperinginhaledcorticosteroidsinasthmaticpatients.BMJ1999;319(7202):87-90.
167.PriceDB,HernandeD,MagyarP,FitermanJ,BeehKM,JamesIG,et al.Randomisedcontrolledtrialofmontelukastplusinhaledbudesonideversusdoubledoseinhaledbudesonideinadultpatientswithasthma.Thorax2003;58(3):211-6.
168.VaquerizoMJ,CasanP,CastilloJ,PerpinaM,SanchisJ,SobradilloV,et al.Effectofmontelukastaddedtoinhaledbudesonideoncontrolofmildtomoderateasthma.Thorax2003;58(3):204-10.
169.NelsonHS,BusseWW,KerwinE,ChurchN,EmmettA,RickardK,et al.Fluticasonepropionate/salmeterolcombinationprovidesmoreeffectiveasthmacontrolthanlow-doseinhaledcorticosteroidplusmontelukast.J Allergy Clin Immunol2000;106(6):1088-95.
170.FishJE,IsraelE,MurrayJJ,EmmettA,BooneR, Yancey SW, et al.Salmeterolpowderprovidessignificantlybetterbenefitthanmontelukastinasthmaticpatientsreceivingconcomitantinhaledcorticosteroidtherapy.Chest 2001;120(2):423-30.
171.RingdalN,EliraA,PruinecR,WeberHH,MulderPG,AkveldM,et al.Thesalmeterol/fluticasonecombinationismoreeffectivethanfluticasoneplusoralmontelukastinasthma.Respir Med2003;97(3):234-41.
172.DahlenB,NizankowskaE,SzczeklikA,ZetterstromO,BochenekG,KumlinM,et al.Benefitsfromaddingthe5-lipoxygenaseinhibitorzileutontoconventionaltherapyinaspirin-intolerantasthmatics.Am J Respir Crit Care Med1998;157(4Pt1):1187-94.
173.DucharmeFM,LassersonTJ,CatesCJ.Additiontoinhaledcorticosteroidsoflong-actingbeta2-agonistsversusanti-leukotrienesforchronicasthma.Cochrane Database Syst Rev.2011May11;5:CD003137.
174.PedersenS,HansenOR.Budesonidetreatmentofmoderateandsevereasthmainchildren:adose-responsestudy.J Allergy Clin Immunol1995;95(1Pt1):29-33.
175.VirchowJC,PrasseA,NayaI,SummertonL,HarrisA.Zafirlukastimprovesasthmacontrolinpatientsreceivinghigh-doseinhaledcorticosteroids.Am J Respir Crit Care Med2000;162(2Pt1):578-85.
176.MaloneR,LaForceC,NimmagaddaS,SchoafL,HouseK,EllsworthA,et al.Thesafetyoftwice-dailytreatmentwithfluticasonepropionateandsalmeterolinpediatricpatientswithpersistentasthma.Ann Allergy Asthma Immunol2005;95(1):66-71.
177.ToogoodJH,BaskervilleJC,JenningsB,LefcoeNM,JohanssonSA.Influenceofdosingfrequencyandscheduleontheresponseofchronicasthmaticstotheaerosolsteroid,budesonide.J Allergy Clin Immunol 1982;70(4):288-98.
178.TamaokiJ,KondoM,SakaiN,NakataJ,TakemuraH,NagaiA,et al.Leukotrieneantagonistpreventsexacerbationofasthmaduringreductionofhigh-doseinhaledcorticosteroid.TheTokyoJoshi-IdaiAsthmaResearchGroup.Am J Respir Crit Care Med 1997;155(4):1235-40.
179.MashB,BheekieA,JonesPW.Inhaledvsoralsteroidsforadultswithchronicasthma.Cochrane Database Syst Rev2000;2.
180.AyresJG,JyothishD,NinanT.Brittleasthma.Paediatr Respir Rev2004;5(1):40-4.
181.MilgromH,FickRB,Jr.,SuJQ,ReimannJD,BushRK, Watrous ML, et al.Treatmentofallergicasthmawithmonoclonalanti-IgEantibody.rhuMAb-E25StudyGroup.N Engl J Med1999;341(26):1966-73.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

92 ASTHMA MANAGEMENT AND PREVENTION
182.BusseW,CorrenJ,LanierBQ,McAlaryM,Fowler-TaylorA,CioppaGD,et al.Omalizumab,anti-IgErecombinanthumanizedmonoclonalantibody,forthetreatmentofsevereallergicasthma.J Allergy Clin Immunol 2001;108(2):184-90.
183.HumbertM,BeasleyR,AyresJ,SlavinR,HebertJ,BousquetJ,et al.Benefitsofomalizumabasadd-ontherapyinpatientswithseverepersistentasthmawhoareinadequatelycontrolleddespitebestavailabletherapy(GINA2002step4treatment):INNOVATE.Allergy2005;60(3):309-16.
184.BousquetJ,WenzelS,HolgateS,LumryW,FreemanP,FoxH.Predictingresponsetoomalizumab,ananti-IgEantibody,inpatientswithallergicasthma.Chest2004;125(4):1378-86.
185.HolgateST,ChuchalinAG,HebertJ,LotvallJ,PerssonGB,ChungKF,et al.Efficacyandsafetyofarecombinantanti-immunoglobulinEantibody(omalizumab)insevereallergicasthma.Clin Exp Allergy 2004;34(4):632-8.
186.DjukanovicR,WilsonSJ,KraftM,JarjourNN,SteelM,ChungKF,et al.Effectsoftreatmentwithanti-immunoglobulinEantibodyomalizumabonairwayinflammationinallergicasthma.Am J Respir Crit Care Med2004;170(6):583-93.
187.KerwinEM,OppenheimerJJ,LaForceC,ParasuramanB,MillerCJ,O’DowdL,GoldmanM.Efficacyandtolerability of once-daily budesonide/formoterol pressurizedmetered-doseinhalerinadultsandadolescentswithasthmapreviouslystablewithtwice-dailybudesonide/formoteroldosing.Annals of Allergy, Asthma & Immunology2009;103:62-72.
188.SontJK,WillemsLN,BelEH,vanKriekenJH,VandenbrouckeJP,SterkPJ.Clinicalcontrolandhistopathologicoutcomeofasthmawhenusingairwayhyperresponsivenessasanadditionalguidetolong-termtreatment.TheAMPULStudyGroup.Am J Respir Crit Care Med1999;159(4Pt1):1043-51.
189.HawkinsG,McMahonAD,TwaddleS,WoodSF,FordI,ThomsonNC.Steppingdowninhaledcorticosteroidsinasthma:randomisedcontrolledtrial.BMJ 2003;326(7399):1115.
190.PowellH,GibsonPG.Initialstartingdoseofinhaledcorticosteroidsinadultswithasthma:asystematicreview.Thorax2004;59(12):1041-5.
191.PowellH,GibsonPG.Highdoseversuslowdoseinhaledcorticosteroidasinitialstartingdoseforasthmainadultsandchildren.Cochrane Database Syst Rev 2004(2):CD004109.
192.BouletLP,DrollmannA,MagyarP,TimarM,KnightA,EngelstatterR,et al.Comparativeefficacyofonce-dailyciclesonideandbudesonideinthetreatmentofpersistentasthma.Respir Med2006;100(5):785-94.
193.MasoliM,WeatherallM,HoltS,BeasleyR.Budesonide once versus twice-daily administration: meta-analysis.Respirology2004;9(4):528-34.
194.FitzGeraldJM,BeckerA,SearsMR,MinkS,ChungK,LeeJ,et al.Doublingthedoseofbudesonideversusmaintenancetreatmentinasthmaexacerbations.Thorax2004;59:550-56.
195.ReddelHK,BarnesDJ.Pharmacologicalstrategiesforself-managementofasthmaexacerbations.Eur Respir J2006;28(1):182-99.
196.HarrisonTW,OborneJ,NewtonS,TattersfieldAE.Doublingthedoseofinhaledcorticosteroidtopreventasthmaexacerbations:randomisedcontrolledtrial.Lancet2004;363(9405):271-5.
197.RabeKF,AtienzaT,MagyarP,LarssonP,JorupC,LallooUG.Effectofbudesonideincombinationwithformoterolforrelievertherapyinasthmaexacerbations:arandomisedcontrolled,double-blindstudy.Lancet 2006;368(9537):744-53.
198.WenzelS.Severeasthmainadults.Am J Respir Crit Care Med2005;172(2):149-60.
199.Referencedeleted.
200.LeggettJJ,JohnstonBT,MillsM,GambleJ,HeaneyLG.Prevalenceofgastroesophagealrefluxindifficultasthma:relationshiptoasthmaoutcome.Chest 2005;127(4):1227-31.
201.HeaneyLG,RobinsonDS.Severeasthmatreatment:needforcharacterisingpatients.Lancet 2005;365(9463):974-6.
202.FitzGeraldJM,GrunfeldA.Statusasthmaticus.In:LichtensteinLM,FauciAS,eds.Current therapy in allergy, immunology, and rheumatology.5thedition.St.Louis,MO:Mosby;1996:p.63-7.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 93
203.Chan-YeungM,ChangJH,ManfredaJ,FergusonA,BeckerA.Changesinpeakflow,symptomscore,andtheuseofmedicationsduringacuteexacerbationsofasthma.Am J Respir Crit Care Med1996;154(4Pt1):889-93.
204.BeasleyR,MilesJ,FishwickD,LeslieH.Managementofasthmainthehospitalemergencydepartment.Br J Hosp Med1996;55(5):253-7.
205.FitzGeraldJM.Developmentandimplementationofasthmaguidelines.Can Respir J1998;5SupplA:85-8S.
206.TurnerMO,NoertjojoK,VedalS,BaiT,CrumpS,FitzGeraldJM.Riskfactorsfornear-fatalasthma.Acase-controlstudyinhospitalizedpatientswithasthma.Am J Respir Crit Care Med1998;157(6Pt1):1804-9.
207.ErnstP,SpitzerWO,SuissaS,CockcroftD,HabbickB, Horwit RI, et al.Riskoffatalandnear-fatalasthmainrelationtoinhaledcorticosteroiduse.JAMA 1992;268(24):3462-4.
208.SuissaS,BlaisL,ErnstP.Patternsofincreasingbeta-agonistuseandtheriskoffatalornear-fatalasthma.Eur Respir J1994;7(9):1602-9.
209.JosephKS,BlaisL,ErnstP,SuissaS.Increasedmorbidityandmortalityrelatedtoasthmaamongasthmaticpatientswhousemajortranquillisers.BMJ 1996;312(7023):79-82.
210.GeelhoedGC,LandauLI,LeSouefPN.EvaluationofSaO2asapredictorofoutcomein280childrenpresentingwithacuteasthma.Ann Emerg Med 1994;23(6):1236-41.
211.CatesCJ,RoweBH.Holdingchambersversusnebulisersforbeta-agonisttreatmentofacuteasthma.Cochrane Database Syst Rev2000;2.
212.PlotnickLH,DucharmeFM.Shouldinhaledanticholinergicsbeaddedtobeta2agonistsfortreatingacutechildhoodandadolescentasthma?Asystematicreview.BMJ1998;317(7164):971-7.
213.ShimCS,WilliamsMH,Jr.Evaluationoftheseverityofasthma:patientsversusphysicians.Am J Med 1980;68(1):11-3.
214.AttaJA,NunesMP,Fonseca-GuedesCH,AvenaLA,BorgianiMT,FiorenzaRF,et al.Patientandphysicianevaluationoftheseverityofacuteasthmaexacerbations.Braz J Med Biol Res2004;37(9):1321-30.
215.FindleyLJ,SahnSA.Thevalueofchestroentgenogramsinacuteasthmainadults.Chest1981;80(5):535-6.
216.NowakRM,TomlanovichMC,SarkarDD,KvalePA,AndersonJA.Arterialbloodgasesandpulmonaryfunctiontestinginacutebronchialasthma.Predictingpatientoutcomes.JAMA1983;249(15):2043-6.
217.CatesC,FitzGeraldJM,O’ByrnePM.Asthma.Clin Evidence2000;3:686-700.
218.ChienJW,CiufoR,NovakR,SkowronskiM,NelsonJ,CorenoA,et al.Uncontrolledoxygenadministrationandrespiratoryfailureinacuteasthma.Chest 2000;117(3):728-33.
219.RodrigoGJ,RodriqueVerdeM,PeregalliV,RodrigoC.Effectsofshort-term28%and100%oxygenonPaCO2andpeakexpiratoryflowrateinacuteasthma:arandomizedtrial.Chest2003;124(4):1312-7.
220.RudnitskyGS,EberleinRS,SchoffstallJM,MazurJE,SpiveyWH.Comparisonofintermittentandcontinuouslynebulizedalbuterolfortreatmentofasthmainanurbanemergencydepartment.Ann Emerg Med1993;22(12):1842-6.
221.LinRY,SauterD,NewmanT,SirleafJ,WaltersJ,TavakolM.Continuousversusintermittentalbuterolnebulizationinthetreatmentofacuteasthma.Ann Emerg Med1993;22(12):1847-53.
222.ReisnerC,KotchA,DworkinG.Continuousversusfrequentintermittentnebulizationofalbuterolinacuteasthma:arandomized,prospectivestudy.Ann Allergy Asthma Immunol1995;75(1):41-7.
223.GawchikSM,SaccarCL,NoonanM,ReasnerDS,DeGrawSS.Thesafetyandefficacyofnebulizedlevalbuterolcomparedwithracemicalbuterolandplacebointhetreatmentofasthmainpediatricpatients.J Allergy Clin Immunol1999;103(4):615-21.
224.LotvallJ,PalmqvistM,ArvidssonP,MaloneyA,VentrescaGP,WardJ.ThetherapeuticratioofR-albuteroliscomparablewiththatofRS-albuterolinasthmaticpatients.J Allergy Clin Immunol 2001;108(5):726-31.
225.MilgromH,SkonerDP,BenschG,KimKT,ClausR,BaumgartnerRA.Low-doselevalbuterolinchildrenwithasthma:safetyandefficacyincomparisonwithplaceboandracemicalbuterol.J Allergy Clin Immunol 2001;108(6):938-45.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

94 ASTHMA MANAGEMENT AND PREVENTION
226.NowakR,EmermanC,HanrahanJP,ParseyMV, Hanania NA, Claus R, et al.Acomparisonoflevalbuterolwithracemicalbuterolinthetreatmentofacutesevereasthmaexacerbationsinadults.Am J Emerg Med2006;24(3):259-67.
227.CarlJC,MyersTR,KirchnerHL,KercsmarCM.Comparisonofracemicalbuterolandlevalbuterolfortreatmentofacuteasthma.J Pediatr2003;143(6):731-6.
228.RodrigoGJ,RodrigoC.Continuousvsintermittentbeta-agonistsinthetreatmentofacuteadultasthma:asystematicreviewwithmeta-analysis.Chest 2002;122(1):160-5.
229.BraddingP,RushbyI,ScullionJ,MorganMD.As-requiredversusregularnebulizedsalbutamolforthetreatmentofacutesevereasthma.Eur Respir J 1999;13(2):290-4.
230.TraversA,JonesAP,KellyK,BarkerSJ,CamargoCA,RoweBH.Intravenousbeta2-agonistsforacuteasthmaintheemergencydepartment.Cochrane Database Syst Rev2001;2.
231.RodrigoG,RodrigoC,BurschtinO.Ameta-analysisoftheeffectsofipratropiumbromideinadultswithacuteasthma.Am J Med1999;107(4):363-70.
232.LanesSF,GarrettJE,WentworthCE,3rd,FitzGeraldJM,KarpelJP.Theeffectofaddingipratropiumbromidetosalbutamolinthetreatmentofacuteasthma:apooledanalysisofthreetrials.Chest1998;114(2):365-72.
233.RodrigoGJ,RodrigoC.First-linetherapyforadultpatientswithacuteasthmareceivingamultiple-doseprotocolofipratropiumbromideplusalbuterolintheemergencydepartment.Am J Respir Crit Care Med 2000;161(6):1862-8.
234.GogginN,MacarthurC,ParkinPC.Randomizedtrialoftheadditionofipratropiumbromidetoalbuterolandcorticosteroidtherapyinchildrenhospitalizedbecauseofanacuteasthmaexacerbation.Arch Pediatr Adolesc Med2001;155(12):1329-34.
235.ParameswaranK,BeldaJ,RoweBH.Additionofintravenousaminophyllinetobeta2-agonistsinadultswithacuteasthma.Cochrane Database Syst Rev 2000;4.
236.ReamRS,LoftisLL,AlbersGM,BeckerBA,LynchRE,MinkRB.EfficacyofIVtheophyllineinchildrenwithseverestatusasthmaticus.Chest2001;119(5):1480-8.
237.RoweBH,BotaGW,FabrisL,TherrienSA,MilnerRA,JaconoJ.Inhaledbudesonideinadditiontooralcorticosteroidstopreventasthmarelapsefollowingdischargefromtheemergencydepartment:arandomizedcontrolledtrial.JAMA1999;281(22):2119-26.
238.ManserR,ReidD,AbramsonM.Corticosteroidsforacutesevereasthmainhospitalisedpatients.Cochrane Database Syst Rev2000;2.
239.RattoD,AlfaroC,SipseyJ,GlovskyMM,SharmaOP.Areintravenouscorticosteroidsrequiredinstatusasthmaticus?JAMA1988;260(4):527-9.
240.HarrisonBD,StokesTC,HartGJ,VaughanDA,AliNJ,RobinsonAA.Needforintravenoushydrocortisoneinadditiontooralprednisoloneinpatientsadmittedtohospitalwithsevereasthmawithoutventilatoryfailure.Lancet1986;1(8474):181-4.
241.GriesDM,MoffittDR,PulosE,CarterER.Asingledoseofintramuscularlyadministereddexamethasoneacetateisaseffectiveasoralprednisonetotreatasthmaexacerbationsinyoungchildren.J Pediatr 2000;136(3):298-303.
242.RoweBH,SpoonerC,DucharmeFM,BretzlaffJA,BotaGW.Earlyemergencydepartmenttreatmentofacuteasthmawithsystemiccorticosteroids.Cochrane Database Syst Rev2000;2.
243.KayaniS,ShannonDC.Adversebehavioraleffectsoftreatmentforacuteexacerbationofasthmainchildren:acomparisonoftwodosesoforalsteroids.Chest 2002;122(2):624-8.
244.HasegawaT,IshiharaK,TakakuraS,FujiiH,NishimuraT,OkazakiM,et al.Durationofsystemiccorticosteroidsinthetreatmentofasthmaexacerbation;arandomizedstudy.Intern Med2000;39(10):794-7.
245.O’DriscollBR,KalraS,WilsonM,PickeringCA,CarrollKB,WoodcockAA.Double-blindtrialofsteroidtaperinginacuteasthma.Lancet1993;341(8841):324-7.
246.LederleFA,PluharRE,JosephAM,NiewoehnerDE.Taperingofcorticosteroidtherapyfollowingexacerbationofasthma.Arandomized,double-blind,placebo-controlledtrial.Arch Intern Med 1987;147(12):2201-3.
247.RodrigoG,RodrigoC.Inhaledflunisolideforacutesevereasthma.Am J Respir Crit Care Med1998;157(3Pt1):698-703.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 95
248.RodrigoGJ.Comparisonofinhaledfluticasonewithintravenoushydrocortisoneinthetreatmentofadultacuteasthma.Am J Respir Crit Care Med 2005;171(11):1231-6.
249.Lee-WongM,DayritFM,KohliAR,AcquahS,MayoPH.Comparisonofhigh-doseinhaledflunisolidetosystemiccorticosteroidsinsevereadultasthma.Chest 2002;122(4):1208-13.
250.NanaA,YoungchaiyudP,CharoenratanakulS,BoeJ,LofdahlCG,SelroosO,et al.High-doseinhaledbudesonidemaysubstitutefororaltherapyafteranacuteasthmaattack.J Asthma1998;35(8):647-55.
251.FitzGeraldJM,ShraggeD,HaddonJ,JenningsB,LeeJ,BaiT,et al.Arandomizedcontrolledtrialofhighdose,inhaledbudesonideversusoralprednisoneinpatientsdischargedfromtheemergencydepartmentfollowinganacuteasthmaexacerbation.Can Respir J 2000;7(1):61-7.
252.EdmondsML,CamargoCA,SaundersLD,BrennerBE,RoweBH.Inhaledsteroidsinacuteasthmafollowingemergencydepartmentdischarge(Cochranereview).Cochrane Database Syst Rev2000;3.
253.RoweBH,BretzlaffJA,BourdonC,BotaGW,CamargoCA,Jr.Magnesiumsulfatefortreatingexacerbationsofacuteasthmaintheemergencydepartment.Cochrane Database Syst Rev2000;2.
254.FitzGeraldJM.Magnesiumsulfateiseffectiveforsevereacuteasthmatreatedintheemergencydepartment.West J Med2000;172(2):96.
255.BlitzM,BlitzS,BeaselyR,DinerB,HughesR,KnoppJ,et al.Inhaledmagnesiumsulfateinthetreatmentofacuteasthma.Cochrane Database Syst Rev 2005(4):CD003898.
256.BlitzM,BlitzS,HughesR,DinerB,BeasleyR,KnoppJ,et al.Aerosolizedmagnesiumsulfateforacuteasthma:asystematicreview.Chest 2005;128(1):337-44.
257.ColebournCL,BarberV,YoungJD.Useofhelium-oxygenmixtureinadultpatientspresentingwithexacerbationsofasthmaandchronicobstructivepulmonarydisease:asystematicreview.Anaesthesia 2007Jan;62(1):34-42.
258.SilvermanRA,NowakRM,KorenblatPE,SkobeloffE,ChenY,BonuccelliCM,et al.Zafirlukasttreatmentforacuteasthma:evaluationinarandomized,double-blind,multicentertrial.Chest2004;126(5):1480-9.
259.FitzGeraldJM,MacklemP.Fatalasthma.Annu Rev Med1996;47:161-8.
260.GrunfeldA,FitzgeraldJM.Dischargeconsiderationsinacuteasthma.Can Respir J1996;3:322-24.
261.RodrigoGJ,RodrigoC,HallJB.Acuteasthmainadults:areview.Chest2004;125(3):1081-102.
262.ZeigerRS,HellerS,MellonMH,WaldJ,FalkoffR,SchatM.Facilitatedreferraltoasthmaspecialistreducesrelapsesinasthmaemergencyroomvisits.J Allergy Clin Immunol1991;87(6):1160-8.
263.GibsonPG,CoughlanJ,WilsonAJ,AbramsonM,BaumanA,HensleyMJ,et al.Self-managementeducationandregularpractitionerreviewforadultswithasthma.Cochrane Database Syst Rev 2000;(2):CD001117.
264.BarenJM,BoudreauxED,BrennerBE,CydulkaRK,RoweBH,ClarkS,et al.Randomizedcontrolledtrialofemergencydepartmentinterventionstoimproveprimarycarefollow-upforpatientswithacuteasthma.Chest2006;129:257-65.
265.SchatzM,HardenK,ForsytheA,ChilingarL,HoffmanC,SperlingW,et al.Thecourseofasthmaduringpregnancy,postpartum,andwithsuccessivepregnancies:aprospectiveanalysis.J Allergy Clin Immunol1988;81(3):509-17.
266.SchatzM.Interrelationshipsbetweenasthmaandpregnancy:aliteraturereview.J Allergy Clin Immunol 1999;103(2Pt2):S330-6.
267.DemissieK,BreckenridgeMB,RhoadsGG.Infantandmaternaloutcomesinthepregnanciesofasthmaticwomen.Am J Respir Crit Care Med1998;158(4):1091-5.
268.BakhirevaLN,SchatzM,JonesKL,ChambersCD;OrganizationofTeratologyInformationSpecialistsCollaborativeResearchGroup.Asthmacontrolduringpregnancyandtheriskofpretermdeliveryorimpairedfetalgrowth.Ann Allergy Asthma Immunol.2008Aug;101(2):137-43.
269.NationalAsthmaEducationProgram.Reportoftheworkinggrouponasthmaandpregnancy:managementofasthmaduringpreganacy.Bethesda,MD:NationalHeart,Lung,andBloodInstitute.NationalInstitutesofHealth;1993.ReportNo.:NIHPublicationNumber93-3279A.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

96 ASTHMA MANAGEMENT AND PREVENTION
270.WendelPJ,RaminSM,Barnett-HammC,RoweTF,CunninghamFG.Asthmatreatmentinpregnancy:arandomizedcontrolledstudy.Am J Obstet Gynecol 1996;175(1):150-4.
271.MurphyVE,GibsonPG,SmithR,CliftonVL.Asthmaduringpregnancy:mechanismsandtreatmentimplications.Eur Respir J2005;25(4):731-50.
272.NAEPPexpertpanelreport.Managingasthmaduringpregnancy:recommendationsforpharmacologictreatment•2004update.J Allergy Clin Immunol 2005;115(1):34-46.
273.SchatzM,ZeigerRS,HardenKM,HoffmanCP,ForsytheAB,ChilingarLM,et al.Thesafetyofinhaledbeta-agonistbronchodilatorsduringpregnancy.J Allergy Clin Immunol1988;82(4):686-95.
274.FungDL.Emergencyanesthesiaforasthmapatients.Clin Rev Allergy1985;3(1):127-41.
275.KingstonHG,HirshmanCA.Perioperativemanagementofthepatientwithasthma.Anesth Analg 1984;63(9):844-55.
276.OhSH,PattersonR.Surgeryincorticosteroid-dependentasthmatics.J Allergy Clin Immunol 1974;53(6):345-51.
277.LeynaertB,BousquetJ,NeukirchC,LiardR,NeukirchF.Perennialrhinitis:anindependentriskfactorforasthmainnonatopicsubjects:resultsfromtheEuropeanCommunityRespiratoryHealthSurvey.J Allergy Clin Immunol1999;104(2Pt1):301-4.
278.SibbaldB,RinkE.Epidemiologyofseasonalandperennialrhinitis:clinicalpresentationandmedicalhistory.Thorax1991;46(12):895-901.
279.ShaabanR,ZureikM,SoussanD,NeukirchC,HeinrichJ,SunyerJ,et al.Rhinitisandonsetofasthma:alongitudinalpopulation-basedstudy.Lancet.2008Sep20;372(9643):1049•57.
280.PriceD,ZhangQ,KocevarVS,YinDD,ThomasM.Effectofaconcomitantdiagnosisofallergicrhinitisonasthma-relatedhealthcareusebyadults.Clin Exp Allergy2005;35(3):282-7.
281.SearsMR,HerbisonGP,HoldawayMD,HewittCJ,FlanneryEM,SilvaPA.Therelativerisksofsensitivitytograsspollen,housedustmiteandcatdanderinthedevelopmentofchildhoodasthma.Clin Exp Allergy 1989;19(4):419-24.
282.ShibasakiM,HoriT,ShimizuT,IsoyamaS,TakedaK,TakitaH.Relationshipbetweenasthmaandseasonalallergicrhinitisinschoolchildren.Ann Allergy 1990;65(6):489-95.
283.MaloJL,LemiereC,DesjardinsA,CartierA.Prevalenceandintensityofrhinoconjunctivitisinsubjectswithoccupationalasthma.Eur Respir J 1997;10(7):1513-5.
284.BousquetJ,VanCauwenbergeP,KhaltaevN.Allergicrhinitisanditsimpactonasthma.J Allergy Clin Immunol 2001;108(5Suppl):S147-334.
285.BentleyAM,JacobsonMR,CumberworthV,BarkansJR,MoqbelR,SchwartLB,et al.Immunohistologyofthenasalmucosainseasonalallergicrhinitis:increasesinactivatedeosinophilsandepithelialmastcells.J Allergy Clin Immunol1992;89(4):877-83.
286.PauwelsR.Influenceoftreatmentonthenoseand/orthelungs.Clin Exp Allergy1998;28Suppl2:37-40S.
287.AdamsRJ,FuhlbriggeAL,FinkelsteinJA,WeissST.Intranasalsteroidsandtheriskofemergencydepartmentvisitsforasthma.J Allergy Clin Immunol 2002;109(4):636-42.
288.DykewicMS,FinemanS.ExecutiveSummaryofJointTaskForcePracticeParametersonDiagnosisandManagementofRhinitis.Ann Allergy Asthma Immunol 1998;81(5Pt2):463-8.
289.TaramarcaP,GibsonPG.Intranasalcorticosteroidsforasthmacontrolinpeoplewithcoexistingasthmaandrhinitis.Cochrane Database Syst Rev 2003(4):CD003570.
290.DahlR,NielsenLP,KipsJ,ForesiA,CauwenbergeP, Tudoric N, et al.Intranasalandinhaledfluticasonepropionateforpollen-inducedrhinitisandasthma.Allergy2005;60(7):875-81.
291.CorrenJ,ManningBE,ThompsonSF,HennessyS,StromBL.Rhinitistherapyandthepreventionofhospitalcareforasthma:acase-controlstudy.J Allergy Clin Immunol2004;113(3):415-9.
292.WilsonAM,O’ByrnePM,ParameswaranK.Leukotrienereceptorantagonistsforallergicrhinitis:asystematicreviewandmeta-analysis.Am J Med 2004;116(5):338-44.
293.AbramsonMJ,PuyRM,WeinerJM.Allergenimmunotherapyforasthma.Cochrane Database Syst Rev2003(4):CD001186.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 97
294.VignolaAM,HumbertM,BousquetJ,BouletLP,HedgecockS,BloggM,et al.Efficacyandtolerabilityofanti-immunoglobulinEtherapywithomalizumabinpatientswithconcomitantallergicasthmaandpersistentallergicrhinitis:SOLAR. Allergy 2004;59(7):709-17.
295.KoppMV,BrauburgerJ,RiedingerF,BeischerD,IhorstG, Kamin W, et al.Theeffectofanti-IgEtreatmentoninvitroleukotrienereleaseinchildrenwithseasonalallergicrhinitis.J Allergy Clin Immunol2002;110(5):728-35.
296.RossiOV,PirilaT,LaitinenJ,HuhtiE.Sinusaspiratesandradiographicabnormalitiesinsevereattacksofasthma.Int Arch Allergy Immunol 1994;103(2):209-13.
297.Referencedeleted.
298.LarsenK.Theclinicalrelationshipofnasalpolypstoasthma.Allergy Asthma Proc1996;17(5):243-9.
299.LamblinC,Tillie-LeblondI,DarrasJ,DubrulleF,ChevalierD,CardotE,et al.Sequentialevaluationofpulmonaryfunctionandbronchialhyperresponsivenessinpatientswithnasalpolyposis:aprospectivestudy.Am J Respir Crit Care Med1997;155(1):99-103.
300.BernsteinIL,Chan-YeungM,MaloJL,BernsteinDI.Definitionandclassificationofasthma.In:BernsteinIL,Chan-YeungM,MaloJL,BernsteinDI,eds.Asthma in the workplace.NewYork:MarcelDekker;1999:p.1-4.
301.Chan-YeungM,DesjardinsA.Bronchialhyperresponsivenessandlevelofexposureinoccupationalasthmaduetowesternredcedar(Thujaplicata).Serialobservationsbeforeandafterdevelopmentofsymptoms.Am Rev Respir Dis 1992;146(6):1606-9.
302.BernsteinDI,CohnJR.Guidelinesforthediagnosisandevaluationofoccupationalimmunologiclungdisease:preface.J Allergy Clin Immunol1989;84(5Pt2):791-3.
303.MappCE,CoronaPC,DeMarzoN,FabbriL.Persistentasthmaduetoisocyanates.Afollow-upstudyofsubjectswithoccupationalasthmaduetotoluenediisocyanate(TDI).Am Rev Respir Dis 1988;137(6):1326-9.
304.LinFJ,Dimich-WardH,Chan-YeungM.Longitudinaldeclineinlungfunctioninpatientswithoccupationalasthmaduetowesternredcedar.Occup Environ Med 1996;53(11):753-6.
305.Fabbri LM, Danieli D, Crescioli S, Bevilacqua P, Meli S, Saetta M, et al.Fatalasthmainasubjectsensitizedtotoluenediisocyanate.Am Rev Respir Dis 1988;137(6):1494-8.
306.MaloJL.CompensationforoccupationalasthmainQuebec.Chest1990;98(5Suppl):236S-9S.
307.GernJE,LemanskeRF,Jr.Infectioustriggersofpediatricasthma.Pediatr Clin North Am2003;50(3):555-75,vi.
308.BusseWW.Theroleofrespiratoryvirusesinasthma.In:HolgateS,ed.Asthma: physiology, immunopharmcology and treatment.London:AcademicPress;1993:p.345-52.
309.KraftM.Theroleofbacterialinfectionsinasthma.Clin Chest Med2000;21(2):301-13.
310.GrunbergK,SterkPJ.Rhinovirusinfections:inductionandmodulationofairwaysinflammationinasthma.Clin Exp Allergy1999;29Suppl2:65-73S.
311.JohnstonSL.Virusesandasthma.Allergy 1998;53(10):922-32.
312.WeissST,TagerIB,MunoA,SpeizerFE.Therelationshipofrespiratoryinfectionsinearlychildhoodtotheoccurrenceofincreasedlevelsofbronchialresponsivenessandatopy.Am Rev Respir Dis 1985;131(4):573-8.
313.BusseWW.Respiratoryinfections:theirroleinairwayresponsivenessandthepathogenesisofasthma.J Allergy Clin Immunol1990;85(4):671-83.
314.HansbroPM,BeagleyKW,HorvatJC,GibsonPG.Roleofatypicalbacterialinfectionofthelunginpredisposition/protectionofasthma.Pharmacol Ther 2004;101(3):193-210.
315.RicheldiL,FerraraG,FabbriLM,GibsonPG.Macrolidesforchronicasthma.Cochrane Database Syst Rev2002(1):CD002997.
316.RicheldiL,FerraraG,FabbriL,LassersonT,GibsonP.Macrolidesforchronicasthma.Cochrane Database Syst Rev2005(3):CD002997.
317.JohnstonSL,BlasiF,BlackPN,MartinRJ,FarrellDJ,NiemanRB.Theeffectoftelithromycininacuteexacerbationsofasthma.N Engl J Med 2006;354(15):1589-600.
318.HardingSM.Acidrefluxandasthma.Curr Opin Pulm Med2003;9(1):42-5.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

98 ASTHMA MANAGEMENT AND PREVENTION
319.SontagSJ.Whydothepublisheddatafailtoclarifytherelationshipbetweengastroesophagealrefluxandasthma?Am J Med2000;108Suppl4A:159-69S.
320.ChanWW,ChiouE,ObsteinKL,TignorAS,WhitlockTL.Theefficacyofpumpinhibitorsforthetreatmentofasthmainadults:ameta-analysis.Arch Intern Med.2011Apr11;171(7):620-9.
321.BarishCF,WuWC,CastellDO.Respiratorycomplicationsofgastroesophagealreflux.Arch Intern Med1985;145(10):1882-8.
322.NelsonHS.Isgastroesophagealrefluxworseningyourpatientswithasthma.J Resp Dis1990;11:827-44.
323.SzczeklikA,StevensonDD.Aspirin-inducedasthma:advancesinpathogenesis,diagnosis,andmanagement.J Allergy Clin Immunol2003;111(5):913-21.
324.SzczeklikA,NizankowskaE,DuplagaM.Naturalhistoryofaspirin-inducedasthma.AIANEInvestigators.EuropeanNetworkonAspirin-InducedAsthma.Eur Respir J2000;16(3):432-6.
325.SzczeklikA,SanakM,Nizankowska-MogilnickaE,KielbasaB.Aspirinintoleranceandthecyclooxygenase-leukotrienepathways.Curr Opin Pulm Med2004;10(1):51-6.
326.StevensonDD.Diagnosis,prevention,andtreatmentofadversereactionstoaspirinandnonsteroidalanti-inflammatorydrugs.J Allergy Clin Immunol1984;74(4Pt2):617-22.
327.NasserSM,PfisterR,ChristiePE,SousaAR,BarkerJ,Schmit-SchumannM,et al.Inflammatorycellpopulationsinbronchialbiopsiesfromaspirin-sensitiveasthmaticsubjects.Am J Respir Crit Care Med 1996;153(1):90-6.
328.SampsonAP,CowburnAS,SladekK,AdamekL,NizankowskaE,SzczeklikA,et al.ProfoundoverexpressionofleukotrieneC4synthaseinbronchialbiopsiesfromaspirin-intolerantasthmaticpatients.Int Arch Allergy Immunol 1997;113(1-3):355-7.
329.SzczeklikA,SanakM.Geneticmechanismsinaspirin-inducedasthma.Am J Respir Crit Care Med2000;161(2Pt2):S142-6.
330.SlepianIK,MathewsKP,McLeanJA.Aspirin-sensitiveasthma.Chest1985;87(3):386-91.
331.NizankowskaE,Bestynska-KrypelA,CmielA,SzczeklikA.Oralandbronchialprovocationtestswithaspirinfordiagnosisofaspirin-inducedasthma.Eur Respir J2000;15(5):863-9.
332.SzczeklikA,StevensonDD.Aspirin-inducedasthma:advancesinpathogenesisandmanagement.J Allergy Clin Immunol1999;104(1):5-13.
333.MilewskiM,MastalerL,NizankowskaE,SzczeklikA.Nasalprovocationtestwithlysine-aspirinfordiagnosisofaspirin-sensitiveasthma.J Allergy Clin Immunol 1998;101(5):581-6.
334.SzczeklikA,NizankowskaE,Czerniawska-MysikG,SekS.Hydrocortisoneandairflowimpairmentinaspirin-inducedasthma.J Allergy Clin Immunol 1985;76(4):530-6.
335.DahlenSE,MalmstromK,NizankowskaE,DahlenB,KunaP,KowalskiM,et al.Improvementofaspirin-intolerantasthmabymontelukast,aleukotrieneantagonist:arandomized,double-blind,placebo-controlledtrial.Am J Respir Crit Care Med2002;165(1):9-14.
336.DrazenJM.Asthmatherapywithagentspreventingleukotrienesynthesisoraction.ProcAssocAmPhysicians1999;111(6):547-59.
337.PleskowWW,StevensonDD,MathisonDA,SimonRA,SchatM,ZeigerRS.Aspirindesensitizationinaspirin-sensitiveasthmaticpatients:clinicalmanifestationsandcharacterizationoftherefractoryperiod.J Allergy Clin Immunol1982;69(1Pt1):11-9.
338.ShefferAL,AustenKF.Exercise-inducedanaphylaxis.J Allergy Clin Immunol1980;66(2):106-11.
339.Thediagnosisandmanagementofanaphylaxis.JointTaskForceonPracticeParameters,AmericanAcademyofAllergy,AsthmaandImmunology,AmericanCollegeofAllergy,AsthmaandImmunology,andtheJointCouncilofAllergy,AsthmaandImmunology.J Allergy Clin Immunol1998;101(6Pt2):S465-528.
340.ChanDS,CallahanCW,Hatch-PigottVB,LawlessA,ProffittHL,ManningNE,SchweikertM,MaloneFJ.Internet-basedhomemonitoringandeducationofchildrenwithasthmaiscomparabletoidealoffice-basedcare:resultsofa1-yearasthmain-homemonitoringtrial.Pediatrics2007Mar;119(3):569-78.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 99
341.HaltermanJS,FisherS,ConnKM,FagnanoM,LynchK,MarkyA,SzilagyiPG.Improvedpreventivecareforasthma:arandomizedtrialofclinicianpromptinginpediatricoffices.Arch Pediatr Adolesc Med 2006 Oct;160(10):1018-25.
342.BouletLP.Perceptionoftheroleandpotentialsideeffectsofinhaledcorticosteroidsamongasthmaticpatients.Chest1998;113:587-92.
343.BhogalS,ZemekR,DucharmeFM.Writtenactionplansforasthmainchildren.Cochrane Database Syst Rev2006Jul19;3:CD005306
344.BatemanED,BousquetJ,KeechML,BusseWW,ClarkTJ,PedersenSE.Thecorrelationbetweenasthmacontrolandhealthstatus:theGOALstudy.Eur Respir J 2007Jan;29(1):56-62
345.PearlmanDS,vanAdelsbergJ,PhilipG,TillesSA,BusseW,HendelesL,LoeysT,DassSB,ReissTF.Onsetanddurationofprotectionagainstexercise-inducedbronchoconstrictionbyasingleoraldoseofmontelukast.Ann Allergy Asthma Immunol 2006 Jul;97(1):98-104.
346.AmericanLungAssociationAsthmaClinicalResearchCenters.Clinicaltrialoflow-dosetheophyllineandmontelukastinpatientswithpoorlycontrolledasthma.Am J Respir Crit Care Med2007Feb1;175(3):235-42.
347.BisgaardH,LeRouxP,BjamerD,DymekA,VermeulenJH,HultquistC.Budesonide/formoterolmaintenanceplusrelievertherapy:anewstrategyinpediatricasthma.Chest2006Dec;130(6):1733-43.
348.SmithJR,MugfordM,HollandR,NobleMJ,HarrisonBD.Psycho-educationalinterventionsforadultswithsevereordifficultasthma:asystematicreview.J Asthma2007Apr;44(3):219-41.
349.MillerMK,LeeJH,BlancPD,PastaDJ,GujrathiS,BarronH,WenzelSE,WeissST;TENORStudyGroup.TENORriskscorepredictshealthcareinadultswithsevereordifficult-to-treatasthma.Eur Respir J 2006 Dec;28(6):1145-55.
350.SerranoJ,PlazaV,SuredaB,dePabloJ,PicadoC,BardagiS,LamelaJ,SanchisJ;SpanishHighRiskAsthmaResearchGroup.Alexithymia:arelevantpsychologicalvariableinnear-fatalasthma.Eur Respir J2006Aug;28(2):296-302.
351.RahimiR,NikfarS,AbdollahiM.Meta-analysisfindsuseofinhaledcorticosteroidsduringpregnancysafe:asystematicmeta-analysisreview.Hum Exp Toxicol 2006 Aug;25(8):447-52.
352.ElMiedanyY,YoussefS,AhmedI,ElGaafaryM.Safetyofetoricoxib,aspecificcyclooxygenase-2inhibitor,inasthmaticpatientswithaspirin-exacerbatedrespiratorydisease.Ann Allergy Asthma Immunol 2006 Jul;97(1):105-9.
353.Bussey-SmithKL,RossenRD.Asystematicreviewofrandomizedcontroltrialsevaluatingtheeffectivenessofinteractivecomputerizedasthmapatienteducationprograms.Ann Allergy Asthma Immunol 2007 Jun;98(6):507-16.
354.RingN,MalcolmC,WykeS,MacgillivrayS,DixonD,HoskinsG,PinnockH,SheikhA.PromotingtheuseofPersonalAsthmaActionPlans:asystematicreview.Prim Care Respir J2007Oct;16(5):271-83.
355.ZemekRL,BhogalSK,DucharmeFM.Systematicreviewofrandomizedcontrolledtrialsexaminingwrittenactionplansinchildren:whatistheplan?Arch Pediatr Adolesc Med2008Feb;162(2):157-63.
356.McCreanorJ,CullinanP,NieuwenhuijsenMJ,Stewart-EvansJ,MalliarouE,JarupL,HarringtonR,SvartengrenM,HanIK,Ohman-StricklandP,ChungKF,ZhangJ.Respiratoryeffectsofexposuretodieseltrafficinpersonswithasthma.N Engl J Med 2007 Dec 6;357(23):2348-58.
357.KogevinasM,ZockJP,JarvisD,KromhoutH,LillienbergL,PlanaE,et al.Exposuretosubstancesintheworkplaceandnew-onsetasthma:aninternationalprospectivepopulation-basedstudy(ECRHS-II).Lancet 2007Jul28;370(9584):336-41.
358.ClarkNM,GongZM,WangSJ,LinX,BriaWF,JohnsonTR.Arandomizedtrialofaself-regulationinterventionforwomenwithasthma.Chest 2007 Jul;132(1):88-97.
359.Carlsen KH, Anderson SD, Bjermer L, Bonini S, Brusasco V, Canonica W, et al.;EuropeanRespiratorySociety;EuropeanAcademyofAllergyandClinicalImmunology;GA(2)LEN.Treatmentofexercise-inducedasthma,respiratoryandallergicdisordersinsportsandtherelationshiptodoping:PartIIofthereportfromtheJointTaskForceofEuropeanRespiratorySociety(ERS)andEuropeanAcademyofAllergyandClinicalImmunology(EAACI)incooperationwithGA(2)LEN.Allergy2008May;63(5):492-505.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

100 ASTHMA MANAGEMENT AND PREVENTION
360.BatemanED,ClarkTJ,FrithL,BousquetJ,BusseWW,PedersenSE;GoalInvestigatorsGroup.Rateofresponseofindividualasthmacontrolmeasuresvariesandmayoverestimateasthmacontrol:ananalysisofthegoalstudy.J Asthma2007Oct;44(8):667-73.
361.RamnathVR,ClarkS,CamargoCAJr.Multicenterstudy of clinical features of sudden-onset versus slower-onsetasthmaexacerbationsrequiringhospitaliation.Respir Care2007Aug;52(8):1013-20.
362.PartridgeMR,CaressAL,BrownC,HenningsJ,LukerK,WoodcockA,CampbellM.Canlaypeopledeliverasthmaself-managementeducationaseffectivelyasprimarycarebasedpracticenurses?Thorax.2008Sep;63(9):778-83.
363.HaynesRB,AcklooE,SahotaN,McDonaldHP,YaoX.Interventionsforenhancingmedicationadherence.Cochrane Database Syst Rev.2009Apr16;(2):CD000011
364.BatemanED,BousquetJ,BusseWW,ClarkTJ,GulN,GibbsM,PedersenS;GOALSteeringCommitteeandInvestigators.Stabilityofasthmacontrolwithregulartreatment:ananalysisoftheGainingOptimalAsthmacontroL(GOAL)study.Allergy.2008Jul;63(7):932-8.
365.Howden-ChapmanP,PierseN,NichollsS,Gillespie-BennettJ,ViggersH,CunninghamM,etal.Effectsofimprovedhomeheatingonasthmaincommunitydwellingchildren:randomisedcontrolledtrial.BMJ.2008Sep23;337:a1411.doi:10.1136/bmj.a1411.
366.BabuKS,GadzikF,HolgateST.Absenceofrespiratoryeffectswithivabradineinpatientswithasthma.Br J Clin Pharmacol.2008Jul;66(1):96-101.
367.OlenchockBA,FonarowGG,PanW,HernandeA,CannonCP;GetWithTheGuidelinesSteeringCommittee.Currentuseofbetablockersinpatientswithreactiveairwaydiseasewhoarehospitalizedwithacutecoronarysyndromes.Am J Cardiol.2009Feb1;103(3):295-300.
368.GodardP,GreillierP,PigeariasB,NachbaurG,DesfougeresJL,AttaliV.Maintainingasthmacontrolinpersistentasthma:comparisonofthreestrategiesina6-monthdouble-blindrandomisedstudy.Respir Med.2008Aug;102(8):1124-31.
369.TataLJ,LewisSA,McKeeverTM,SmithCJ,DoyleP,SmeethL,GibsonJE,HubbardRB.Effectofmaternalasthma,exacerbationsandasthmamedicationuseoncongenitalmalformationsinoffspring:aUKpopulation-basedstudy.Thorax.2008Nov;63(11):981-7.
370.JuhnYJ,KitaH,YawnBP,BoyceTG,YooKH,McGreeME,WeaverAL,WollanP,JacobsonRM.Increasedriskofseriouspneumococcaldiseaseinpatientswithasthma.J Allergy Clin Immunol.2008Oct;122(4):719-23.
371.PostmaJ,KarrC,KieckheferG.Communityhealthworkersandenvironmentalinterventionsforchildrenwithasthma:asystematicreview.J Asthma 2009;46(6):564-76.
372.vanderMeerV,BakkerMJ,vandenHoutWB,RabeKF,SterkPJ,KievitJ,AssendelftWJ,SontJK;SMASHING(Self-ManagementinAsthmaSupportedbyHospitals,ICT,NursesandGeneralPractitioners)StudyGroup.Internet-basedself-managementpluseducationcomparedwithusualcareinasthma:arandomizedtrial.Ann Intern Med2009;151(2):110-20.
373.ClarkNM,ShahS,DodgeJA,ThomasLJ,AndridgeRR,LittleRJ.Anevaluationofasthmainterventionsforpreteenstudents.J Sch Health2010;80(2):80-7.
374.Wilson SR, Strub P, Buist AS, Knowles SB, Lavori PW, LapidusJ,VollmerWM;BetterOutcomesofAsthmaTreatment(BOAT)StudyGroup.Sharedtreatmentdecisionmakingimprovesadherenceandoutcomesinpoorlycontrolledasthma.Am J Respir Crit Care Med 2010;181(6):566-77.
375.Bosnic-AnticevichSZ,SinhaH,SoS,ReddelHK.Metered-doseinhalertechnique:theeffectoftwoeducational interventions delivered in community pharmacyovertime.J Asthma2010;47(3):251-6.
376.CohenJL,MannDM,WisniveskyJP,HomeR,LeventhalH,Musumeci-SzabóTJ,HalmEA.Assessingthevalidityofself-reportedmedicationadherenceamonginner-cityasthmaticadults:theMedicationAdherenceReportScaleforAsthma.Ann Allergy Asthma Immunol2009;103(4):325-31.
377.CoffmanJM,CabanaMD,YelinEH.Doschool-basedasthmaeducationprogramsimproveself-managementandhealthoutcomes?Pediatrics2009;124(2):729-42.
378.O’ByrnePM,LammCJ,BusseWW,TanWC,PedersenS;STARTInvestigatorsGroup.Theeffectsofinhaledbudesonideonlungfunctioninsmokersandnonsmokerswithmildpersistentasthma.Chest 2009;136(6):1514-20.
379.EtminanM,SadatsafaviM,JafariS,Doyle-WatersM,AminzadehK,FitzgeraldJM.Acetaminophenuseandtheriskofasthmainchildrenandadults:asystematicreviewandmetaanalysis.Chest 2009;136(5):1316-23.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 101
380.MintzM,GilsenanAW,BuiCL,ZiemieckiR,StanfordRH,LincourtW,OrtegaH.Assessmentofasthmacontrolinprimarycare.Curr Med Res Opin 2009;25(10):2523-31.
381.OborneJ,MortimerK,HubbardRB,TattersfieldAE,HarrisonTW.Quadruplingthedoseofinhaledcorticosteroidtopreventasthmaexacerbations:arandomized,double-blind,placebo-controlled,parallel-groupclinicaltrial.Am J Respir Crit Care Med 2009;180(7):598-602.
382.LemanskeRFJr,MaugerDT,SorknessCA,JacksonDJ,BoehmerSJ,MartinezFD,etal.;ChildhoodAsthmaResearchandEducation(CARE)NetworkoftheNationalHeart,Lung,andBloodInstitute.Step-uptherapyforchildrenwithuncontrolledasthmareceivinginhaledcorticosteroids.N Engl J Med2010;362(11):975-85.
383.Saint-PierreP,BourdinA,ChanezP,DauresJP,GodardP.Areoverweightasthmaticsmoredifficulttocontrol?Allergy2006;61(1):79-84.
384.LavoieKL,BaconSL,LabrecqueM,CartierA,DittoB.HigherBMIisassociatedwithworseasthmacontrolandqualityoflifebutnotasthmaseverity.Respir Med 2006;100(4):648-57.
385.DixonAE,ShadeDM,CohenRIetal.Effectofobesityonclinicalpresentationandresponsetotreatmentinasthma.J Asthma 2006;43(7):553-8.
386.BouletLP,FranssenE.Influenceofobesityonresponsetofluticasonewithorwithoutsalmeterolinmoderateasthma.Respir Med 2007;101(11):2240-7
387.Peters-Golden M, Swern A, Bird SS, Hustad CM, Grant E,EdelmanJM.Influenceofbodymassindexontheresponsetoasthmacontrolleragents.Eur Respir J 2006;27(3):495-503.
388.AaronSD,VandemheenKL,BouletLP,McIvorRA,FitzgeraldJM,HernandezP,LemiereC,SharmaS,FieldSK,AlvarezGG,DalesRE,DoucetteS,FergussonD;CanadianRespiratoryClinicalResearchConsortium.Overdiagnosisofasthmainobeseandnonobeseadults. CMAJ2008;179(11):1121-31.
389.EneliIU,SkyboT,CamargoCAJr.Weightlossandasthma:asystematicreview.Thorax2008;63(8):671-6.
390.AaronSD,FergussonD,DentR,ChenY,VandemheenKL,DalesRE.Effectofweightreductiononrespiratoryfunctionandairwayreactivityinobesewomen. Chest 2004;125(6):2046-52.
391.LeungTF,ToMY,YeungAC,WongYS,WongGW,ChanPK.Multiplexmoleculardetectionofrespiratorypathogensinchildrenwithasthmaexacerbation.Chest 2010;137(2):348-54.
392.KiljanderTO,HardingSM,FieldSK,SteinMR,NelsonHS,EkelundJ,IlluecaM,BeckmanO,SostekMB.Effectsofesomeprazole40mgtwicedailyonasthma:arandomizedplacebo-controlledtrial.Am J Respir Crit Care Med 2006;173(10):1091-7.
393.MastronardeJG,AnthonisenNR,CastroM,HolbrookJT,LeoneFT,TeagueWG,WiseRA.Efficacyofesomeprazolefortreatmentofpoorlycontrolledasthma.N Engl J Med 2009;360(15):1487-99.
394.SopoSM,RadzikD,CalvaniM.Doestreatmentwithprotonpumpinhibitorsforgastroesophagealrefluxdisease(GERD)improveasthmasymptomsinchildrenwithasthmaandGERD?Asystematicreview.J Investig Allergol Clin Immunol2009;19(1):1-5.Review.
395.LiuWT,HuangCD,WangCH,LeeKY,LinSM,KuoHP.Amobiletelephone-basedinteractiveself-caresystemimprovesasthmacontrol.Eur Respir J. 2011 Feb;37(2):310-7.
396.Referencedeleted.
397.McLeanS,ChandlerD,NurmatovU,LiuJ,PagliariC,CarJ,SheikhA.Telehealthcareforasthma.Cochrane Database Syst Rev.2010Oct6;(10):CD007717.
398.WilliamsLK,PetersonEL,WellsK,CampbellJ,WangM,ChowdhryVK,etal.Acluster-randomizedtrialtoprovidecliniciansinhaledcorticosteroidadherenceinformationfortheirpatientswithasthma.J Allergy Clin Immunol. 2010Aug;126(2):225-31,231.e1-4.
399.BruzzeseJM,ShearesBJ,VincentEJ,DuY,SadeghiH,LevisonMJ,MellinsRB,EvansD.Effectsofaschool-basedinterventionforurbanadolescentswithasthma.Acontrolledtrial.Am J Respir Crit Care Med.2011Apr15;183(8):998-1006.
400.BusseWW,LemanskeRFJr,GernJE.Roleofviralrespiratoryinfectionsinasthmaandasthmaexacerbations.Lancet.2010Sep4;376(9743):826-34.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

102 ASTHMA MANAGEMENT AND PREVENTION
401.BeasleyRW,ClaytonTO,CraneJ,LaiCK,MontefortSR,MutiusE,StewartAW;ISAACPhaseThreeStudyGroup.Acetaminophenuseandriskofasthma,rhinoconjunctivitis,andeczemainadolescents:InternationalStudyofAsthmaandAllergiesinChildhoodPhaseThree.Am J Respir Crit Care Med. 2011Jan15;183(2):171-8.
402.TiboschMM,VerhaakCM,MerkusPJ.Psychologicalcharacteristicsassociatedwiththeonsetandcourseofasthmainchildrenandadolescents:asystematicreviewoflongitudinaleffects.Patient Educ Couns.2011Jan;82(1):11-9.
403.Vaessen-VerberneAA,vandenBergNJ,vanNieropJC,BrackelHJ,GerritsGP,HopWC,DuivermanEJ;COMBOStudyGroup.Combinationtherapysalmeterol/fluticasoneversusdoublingdoseoffluticasoneinchildrenwithasthma.Am J Respir Crit Care Med. 2010 Nov15;182(10):1221-7.
404.QuonBS,FitzGeraldJM,LemiereC,ShahidiN,DucharmeFM.Increasedversusstabledosesofinhaledcorticosteroidsforexacerbationsofchronicasthmainadultsandchildren.Cochrane Database Syst Rev.2010Oct6;(10):CD007524.
405.Melani AS, Bonavia M, Cilenti V, Cinti C, Lodi M, MartucciP,SerraM,ScichiloneN,SestiniP,AlianiM,NeriM;GruppoEducazionaleAssociazioneItalianaPneumologiOspedalieri.Inhalermishandlingremainscommoninreallifeandisassociatedwithreduceddiseasecontrol.Respir Med.2011Jun;105(6):930-8.
406.CastroM,RubinAS,LavioletteM,FitermanJ,DeAndradeLimaM,ShahPL,etal;AIR2TrialStudyGroup.Effectivenessandsafetyofbronchialthermoplastyinthetreatmentofsevereasthma:amulticenter,randomized,double-blind,sham-controlledclinicaltrial.Am J Respir Crit Care Med.2010Jan15;181(2):116-24.
407.ThomsonNC,RubinAS,NivenRM,CorrisPA,SierstedHC,OlivensteinR,etal;AIRTrialStudyGroup.Long-term(5year)safetyofbronchialthermoplasty:Asthma Intervention Research (AIR) trial.BMC Pulm Med.2011Feb11;11:8.
408.CoxG,ThomsonNC,RubinAS,etal.Asthmacontrolduringtheyearafterbronchialthermoplasty.N Engl J Med. 2007;356:1327-37.
409.Gallegos-SolorzanoMC,Perez-PadillaR,Hernandez-ZentenoRJ.Usefulnessofinhaledmagnesiumsulfateinthecoadjuvantmanagementofsevereasthmacrisisinanemergencydepartment.Pulm Pharmacol Ther. 2010 Oct;23(5):432-7.
410.RamsayCF,PearsonD,MildenhallS,WilsonAM.Oralmontelukastinacuteasthmaexacerbations:arandomised,double-blind,placebo-controlledtrial.Thorax. 2011 Jan;66(1):7-11.
411.DucharmeFM,ZemekRL,ChalutD,McGillivrayD,NoyaFJ,ResendesS,KhomenkoL,RouleauR,ZhangX.Writtenactionplaninpediatricemergencyroomimprovesasthmaprescribing,adherence,andcontrol.Am J Respir Crit Care Med.2011Jan15;183(2):195-203.
412.deGroeneGJ,PalTM,BeachJ,TarloSM,SpreeuwersD,Frings-DresenMH,MattioliS,VerbeekJH.Workplaceinterventionsfortreatmentofoccupationalasthma.Cochrane Database Syst Rev. 2011 May 11;5:CD006308.
413.SutherlandER,KingTS,IcitovicN,AmeredesBT,BleeckerE,BousheyHA,etal;NationalHeart,LungandBloodInstitute’sAsthmaClinicalResearchNetwork.Atrialofclarithromycinforthetreatmentofsuboptimallycontrolledasthma.J Allergy Clin Immunol. 2010 Oct;126(4):747-53.
414.ShahS,SawyerSM,ToelleBG,MellisCM,PeatJK.LaglevaM,et al.Improvingpaediatricasthmaoutcomesinprimaryhealthcare:arandomisedcontrolledtrial.Med J Aust.2011Oct3;195(7):405-9.
415.GehringU,deJongsteJC,KerkhofM,OldeweningM,Postma D, van Strien RT, et al.The8-yearfollow-upofthePIAMAinterventionstudyassessingtheeffectofmite-impermeablemattresscovers.Allergy. 2012 Feb;67(2):248-56
416.GambleJ,StevensonM,HeaneyLG.Astudyofamulti-levelinterventiontoimprovenon-adherenceindifficulttocontrolasthma.Respir Med.2011Sep;105(9):1308-15.
417.CastroM,RubinA,LavioletteM,HananiaNA,ArmstrongB,CoxG;AIR2TrialStudyGroup.Persistenceofeffectivenessofbronchialthermoplastyinpatientswithsevereasthma.Ann Allergy Asthma Immunol. 2011 Jul;107(1):65-70.
418.OrtegaH,MillerDP,LiH.Characterizationofasthmaexacerbationsinprimarycareusingclusteranalysis.J Asthma.2012Mar;49(2):158-69.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

ASTHMA MANAGEMENT AND PREVENTION 103
419.PerrinK,WijesingheM,HealyB,WadsworthK,BowditchR,BibbyS,BakerT,WeatherallM,BeasleyR.Randomisedcontrolledtrialofhighconcentrationversustitratedoxygentherapyinsevereexacerbationsofasthma. Thorax.2011Nov;66(11):937-41.
420.KravitzJ,DominiciP,UfbergJ,FisherJ,GiraldoP.Twodaysofdexamethasoneversus5daysofprednisoneinthetreatmentofacuteasthma:arandomizedcontrolledtrial.Ann Emerg Med.2011Aug;58(2):200-4.
421.FishwickD,BarberCM,BradshawLM,AyresJG,BarracloughR,BurgeS,etal.Standardsofcareforoccupationalasthma:anupdate.Thorax.2012Mar;67(3):278-80.
422.HolbrookJT,WiseRA,GoldBD,BlakeK,BrownED,Castro M, et al.WritingCommitteefortheAmericanLungAssociationAsthmaClinicalResearchCenters.Lansoprazoleforchildrenwithpoorlycontrolledasthma:arandomizedcontrolledtrial.JAMA.2012Jan25;307(4):373-81.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

104 ASTHMA MANAGEMENT AND PREVENTIONCOPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

CHAPTER
5
IMPLEMENTATION OF ASTHMA
GUIDELINES INHEALTH SYSTEMS
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

106 IMPLEMENTATION OF ASTHMA GUIDELINES IN HEALTH SYSTEMS
KEY POINTS:
• Inordertoeffectchangesinmedicalpracticeandconsequentimprovementsinpatientoutcomes,evidence-basedguidelinesmustbeimplementedanddisseminatedatthenationalandlocallevels.
• Implementationofasthmaguidelinesshouldinvolveawidevarietyofprofessionalgroupsandotherstakeholders,andtakeintoaccountlocalculturalandeconomicconditions.
• Animportantpartoftheimplementationprocessistoestablishasystemtoevaluatetheeffectivenessandqualityofcare.
• Thoseinvolvedintheadaptationandimplementationofasthmaguidelinesrequireanunderstandingofthecostandcosteffectivenessofvariousmanagementrecommendationsinasthmacare.
• GINAhasdevelopedanumberofresourcesandprogramstoaidinguidelineimplementationanddissemination.
Ithasbeendemonstratedinavarietyofsettingsthatpatientcareconsistentwithrecommendationsinevidence-basedasthmaguidelinesleadstoimprovedoutcomes.Guidelinesaredesignedtoensurethatallmembersofapatient’shealthcareteamareawareofthegoalsoftreatmentandofthedifferentwaysofachievingthesegoals.Theyhelpsetstandardsofclinicalcare,mayserveasabasisforauditandpayment,andactasastartingpointfortheeducationofhealthprofessionalsandpatients. However,inordertoeffectchangesinmedicalpracticeandconsequentimprovementsinpatientoutcomes,evidence-basedguidelinesmustbeimplementedanddisseminatedatnationalandlocallevels.Disseminationinvolveseducatingclinicianstoimprovetheirawareness,knowledge,andunderstandingofguidelinerecommendations.Itisonepartofimplementation,whichinvolvesthetranslationofevidence-basedasthmaguidelinesintoreal-lifepracticewithimprovementofhealthoutcomesforthepatient.Implementationremainsadifficult
problemworldwide.Barrierstoimplementationrangefrompoorinfrastructurethathampersdeliveryofmedicinestoremotepartsofacountry,toculturalfactorsthatmakepatientsreluctanttouserecommendedmedications(e.g.,inhaledpreparations),suboptimaluseofmedications21, and lackofphysicianuseofguidelines.
Animportantbarriertothesuccessfultranslationofasthmaguidelinesintoclinicalpracticeisaccesstoavailableandaffordablemedicationespeciallyforpatientsinlessdevelopedeconomieswherethecostoftreatmentishighincomparisontoincomeandassets.
Implementationofasthmaguidelinesshouldbeginwiththesettingofgoalsanddevelopmentofstrategiesforasthmacarethroughcollaborationamongdiverseprofessionalgroupsincludingbothprimaryandsecondaryhealthcareprofessionals,publichealthofficials,patients,asthmaadvocacygroups,andthegeneralpublic.Goalsandimplementationstrategieswillvaryfromcountrytocountry-andwithincountries-forreasonsofeconomics,culture,andenvironment.However,commonissuesareshowninFigure 5-1.
Thenextstepisadaptationofguidelinesonasthmamanagementforlocalusebyteamsoflocalprimaryandsecondarycarehealthprofessionals.Manylow-andmiddleincomecountriesdonotconsiderasthmaahigh-priorityhealthconcernbecauseother,morecommonrespiratorydiseasessuchastuberculosisandpneumoniaareofgreaterpublichealthimportance1.Therefore,practicalasthmaguidelinesforimplementationinlow-incomecountriesshouldhaveasimplealgorithmforseparatingnon-infectiousfrominfectiousrespiratoryillnesses;simpleobjectivemeasurementsfordiagnosisandmanagementsuchaspeakflowvariability2;available,affordable,andlow-riskmedicationsrecommendedforasthmacontrol;asimpleregimeforrecognizingsevereasthma;andsimplediagnosisandmanagementapproachesrelevanttothefacilitiesandlimitedresourcesavailable. Next,adaptedguidelinesmustbewidelydisseminatedinmultiplevenuesandusingmultipleformats.Thiscanbeaccomplished,forexample,bypublicationinprofessional
CHAPTER 5: IMPLEMENTATION OF ASTHMA GUIDELINES IN HEALTH SYSTEMS
INTRODUCTION
GUIDELINE IMPLEMENTATION STRATEGIES
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

IMPLEMENTATION OF ASTHMA GUIDELINES IN HEALTH SYSTEMS 107
Figure 5-1. Checklist of Issues for National or LocalAsthma Implementation
• What is the size of the problem and burden of asthma in thiscountry or district?
• What arrangements will be made for shared care amongdifferent health care providers (doctors and nurses, hospital and primary care)?
• How will medical care be linked with community health facilitiesand educational initiatives?
• What are the major preventable factors in this country or districtthat could help prevent asthma from developing or couldprevent asthma exacerbations from occurring in those whoalready have asthma?
• What preconceived assumptions about asthma and its treatmentand what cultural factors will need special attention?
• What treatments are currently used?• How affordable and accessible are medications and services to
the patient? • What other treatments are available, cheap enough for
purchase, and stable in local climatic conditions? • Can inhaler devices and medicines be standardized to reduce
cost/storage/availability problems? • Who will provide emergency care? • Which groups of the population are at special risk (e.g., inner-
city, poor, teenage, minority)? • Whom can we enlist to help in education (community health
workers/health-promotion facilitators/trained educators currentlyworking on other programs/self-help support groups)?
• Who will take responsibility for the education of health careprofessionals?
• Who will take responsibility for the education of people withasthma and their family members/caregivers?
• How can asthma education and treatment be integrated intoother programs (e.g., child health)?
journals,accompaniedbymultidisciplinarysymposia,workshops,andconferencesinvolvingnationalandlocalexpertswithinvolvementoftheprofessionalandmassmediatoraiseawarenessofthekeymessages3.Themosteffectiveinterventionstoimproveprofessionalpracticearemultifaceted and interactive4,5.However,littleisknownofthecosteffectivenessoftheseinterventions6.Integratedcarepathwaysarebeingexploredasameantoimproveasthmacareinspecificsettings,suchaspatientscomingtoemergencydepartments22.
Insomecountries,implementationofasthmaguidelineshasbeendoneatanationallevelwithgovernmenthealthdepartmentcollaboration.AmodelforanimplementationprogramthathasimprovedpatientoutcomesisprovidedbythenationalasthmaprograminFinland,along-term,comprehensive,multifacetedpublichealthinitiativewithwell-definedtargetsforasthmaguidelineimplementation7,8.
Publichealthstrategiesinvolvingabroadcoalitionofstakeholdersinasthmacare,includingmedicalsocieties,healthcareprofessionals,patientsupportgroups,government,andtheprivatesector,havebeenimplementedinAustralia(AustralianNationalAsthmaCouncil,http://www.nationalasthma.org.au),andtheUnitedStates(NationalAsthmaEducationandPreventionProgram,http://www.nhlbi.nih.gov).
Animportantpartoftheimplementationprocessistoestablishasystemtoevaluatetheeffectivenessandqualityofcare.Evaluationinvolvessurveillanceoftraditionalepidemiologicalparameters,suchasmorbidityandmortality,aswellasthespecificauditofbothprocessandoutcomewithindifferentsectorsofthehealthcaresystem.Eachcountryshoulddetermineitsownminimumsetsofdatatoaudithealthoutcomes.Thereareavarietyofassessmenttoolswhichprovideaconsistentandobjectiveassessmentofasthmamorbidityorcontrol(e.g.,AsthmaControlTest9,AsthmaControlQuestionnaire10-12 , AsthmaTherapyAssessmentQuestionnaire13).Resultsoftheseassessmentsshouldberecordedateachvisit,providingarecordofthelong-termclinicalresponseofthepatienttotreatment.Directfeedbackprovidesseveralbenefits-ameansforthepatient/caregivertobecomefamiliarwith,andsensitizedto,satisfactoryversuspoorcontrolofasthma;areferencepointfromwhichtoevaluatedeterioratingasthma;andanindicatorofchangesinasthmacontrolinresponsetochangesintreatment.Useofadministrativedatasets(e.g.,dispensingrecords)orurgenthealthcareutilizationcanhelptoidentifyat-riskpatientsortoauditthequalityofhealthcare23.Thestrategyofculturallyappropriatedirectfeedbackofclinicaloutcomestophysiciansaboutspecifichealthcareresultsoftheirpatientsmaybeimportantforgeneralpractitionerswhotreatmanydiseasesinadditiontoasthmaandthuscouldnotbeexpectedtoknowguidelinesindetailandhandlepatientsaccordingly.
Costisrecognizedasanimportantbarriertothedeliveryofoptimalevidence-basedhealthcareinalmosteverycountry,althoughitsimpactonpatients’accesstotreatmentsvarieswidelybothbetweenandwithincountries.Atthecountryorlocallevel,healthauthoritiesmakeresourceavailabilityandallocationdecisionsaffectingpopulationsofasthmapatientsbyconsideringthebalanceand tradeoffs between costs and clinical outcomes (benefitsandharms),ofteninrelationtocompetingpublichealthandmedicalneeds.Treatmentcostsmustalsobe
ECONOMIC VALUE OF INTERVENTIONS AND GUIDELINE IMPLEMENTATION IN ASTHMA
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

108 IMPLEMENTATION OF ASTHMA GUIDELINES IN HEALTH SYSTEMS
explicitlyconsideredateachconsultationbetweenhealthcareproviderandpatienttoassurethatcostdoesnotpresentabarriertoachievingasthmacontrol.Thus,thoseinvolvedintheadaptationandimplementationofasthmaguidelinesrequireanunderstandingofthecostandcosteffectivenessofvariousmanagementrecommendationsinasthmacare.Tothisend,ashortdiscussionofcost-effectivenessevaluationforasthmacarefollows.
Utilization and Cost of Health Care Resources
Between35and50%ofmedicalexpendituresforasthmaareconsequencesofexacerbations14,anasthmaoutcomemostviewasrepresentingtreatmentfailure.Hospitalization,emergencydepartmentandunscheduledclinicvisits,anduseofrescuemedicationcomprisethemajorityofexacerbation-relatedtreatmentcosts.Inclinicaltrialsofasthmatreatments,exacerbationsarecustomarilycharacterizedbyuseofhealthcareresources,aloneorincombinationwithsymptomandlungfunctiondata,especiallywhentheprimarystudyoutcomeisreductionintheexacerbationfrequencyortimetoanexacerbationevent.Routinecollectionofhealthcareresourceconsumptiondatacanbeundertakeninthefieldthroughpatientorcaregiverself-report.Insomecircumstances,automateddatafromclinicalorbillingrecordscansubstituteforself-reportandaremorereliableandvalid13,15.
Compositedefinitionsofasthmacontrol16,17 may include oneormorehealthcareutilizationitems.Theseitemstypicallydescribethepresenceofanexacerbationoranexacerbation-relatedtreatmentinpreciseandvalidterms.Manyofthepublishedcompositemeasuresofasthmacontrolhaveincludedhospitalizationandemergencytreatmentdata,suchasunscheduledorurgentcarevisitsoruseofnebulizedβ2-agonistsand/ororalglucocorticosteroids17.Althoughhealthcareutilizationelementsareessentialtoanypragmaticdefinitionofasthmacontrol,asyetunansweredintheliteratureiswhichofthenumberofpossiblehealthcareoptions(singleitemsorcombinationsofitems)cancontributetoanacceptabledefinitionofcontrol,andthevaluesofeachthatmightbeviewedasacceptablecontrol.
Forstudiestoevaluatethecostimpactofguidelineimplementationorofspecificasthmainterventions,dataoncostsofimplementation(e.g.,costsrelatedtodisseminationandpublicationofguidelines,costsofhealthprofessionaleducation),preventivepharmacotherapy,diagnosticandfollow-upspirometry,useofdevices(spacers,peakflowmeters),androutineofficevisitsarerequiredtosupplementdataonexacerbation-relatedtreatments.Together,thesedataprovideacomprehensiveprofileofhealthcareresourceconsumption.Thesedata
canbeacquiredinasimilarfashionusingself-reportorfromautomateddatabases.
Oncedataonuseofhealthcareresourcesarecollected,costscanbedeterminedbyassigninglocalcurrencypriceweightstohealthcareresourcesconsumed.Unitpriceweightsarenormallycollectedfromgovernmentreports,priceauditsoflocalpayers,billingrecords,claimsdatabases,andpatientsurveys.
Assessmentofpatientandcaregivertravelandwaitingtime for medical visits, as well as absences from and productivitywhileatschoolorwork,compriseadditionalandimportantoutcomemeasuresinasthma.Theseindirectcostsofasthmaaresubstantial,estimatedtoberoughly50%oftheoveralldiseaseburden14.However,therearenostandardized,validated,andculturallyadaptedinstrumentsforassessingthesemeasuresinavarietyofpopulations.
Determining the Economic Value of Interventions in Asthma
Economicevaluationsrequiretheselectionofthreemainoutcomeparameters-estimatesoftreatment-relatedhealthbenefits,treatment-relatedrisks,andtreatment-relatedcosts.Theseparameterscanbedetermineddirectlyfromclinicalstudiesorthroughtheapplicationofmodelingstudies.Localevidencerequirementsforeconomicevaluationsdeterminethechoicesofhealthbenefitmeasures.Whenthedecisiontobeconsideredisatthemacro-level,forexampletheinclusionofanewtreatmentinagovernment-sponsoredhealthcareprogramorthebenefitspackageofahealthinsurer,economicevaluationsrequiretheuseofacommonmetricsuchaslifeyearsgained,improvementingenericqualityoflife,orquality-adjustedlifeyears(QALY)gained18.Theseoutcomessupportcomparisonofcost-effectivenessratiosacrossdifferentdiseasestatesandpatientpopulations.However,inasthma,QALYsaredifficulttomeasure,particularlyinchildrenwherevalidatedpreferencemeasuresarenotavailable.Somehaveadvocatedtheuseofclinicalmeasuressuchassymptom-freedaysorasthmacontrolasthedenominatorineconomicevaluations19.Aunifieddefinitionofasthmacontrolwouldsubstantiallyimprovetheacceptanceofnon-QALYeconomicevaluationsamongthoseinterestedintheirdesignandapplication.
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

IMPLEMENTATION OF ASTHMA GUIDELINES IN HEALTH SYSTEMS 109
EducationalmaterialsbasedonthisGlobal Strategy for Asthma Management and Prevention are available in severalforms,includingapocketguideforhealthcareprofessionalsandoneforpatientsandfamilies.TheseareavailableontheGINAWebsite(http://www.ginasthma.org).Eachyear,theGINAScienceCommitteeexaminespeer-reviewedliteratureonasthmamanagementandupdatesvariousGINAdocuments.AreportofaGINAWorkingGroup20providesablueprintforimplementationstrategies. OtheractivitiestoassistwithimplementationofasthmamanagementrecommendationsthroughtheGINAprograminclude:
Gina Website -www.ginasthma.org.TheInternetiscreatingaconduitfortheaccess,sharing,andexchangeofinformationandpermitstheglobaldistributionofmedicalinformation.Althoughitisstillnotwidelyavailable,especiallyinlow-incomecountries,theglobaltrendisforincreasinguseoftheInternetformedicaleducationbyasthmapatientsandtheirhealthcareproviders.Thus,tofacilitatecommunicationwithhealthprofessionals,healthpolicyexperts,patients,andtheirfamiliesinternationally,GINAhasmaintainedaWebsitesince1995toprovideaccesstotheGINAdocumentsandeducationalmaterialsforpatientsandthepublicaswellasupdatesofactivitiesandinformationaboutcollaboratinggroupsandcontactsthroughouttheworld.
World Asthma Day.Initiatedin1998,andheldonthefirstTuesdayinMay,WorldAsthmaDayisorganizedbyGINAincollaborationwithhealthcaregroupsandasthmaeducatorsthroughouttheworld.WorldAsthmaDay activities focus on dissemination of information aboutasthmaamongthegeneralpopulation,healthcareprofessionals,andgovernmentofficials.Forpatientswithasthmaandtheirrelatives,theseactivitiesfosteranappreciationoftheimportanceofasthmaonalocal,regional,national,andinternationallevel.Activitiesincludesportingevents;meetingsofpeoplewithasthmaandtheirfamilieswithhealthprofessionals;meetingswithlocalhealthofficialstodiscussprogressinasthmacare;andreportsinprintmedia,radio,andtelevision.InformationaboutWorldAsthmaDaycanbefoundontheGINAWebsite.
Regional Initiatives.Toexaminetheformationofnetworkstofacilitatetheprocessofguidelineimplementation,twopilotinitiativeshavebeenimplementedintheMesoamericaandMediterraneanregions.GINAleadershavebeen
identifiedineachcountryineachregionwhowillsupervisecollaborationbetweenGINAandlocalgroupsandbringtheGINAguidelinesintoformsthatcanbereadilyusedbyhealthcareprofessionalsandpatientsineachregion.
GINA Assembly.Tomaximizeinteractionwithglobalasthma-carepractitioners,aGINAAssemblywasinitiatedinJanuary2005.TheAssemblyprovidesaforumfordialogueamongthesehealthcareprofessionalsandfacilitatessharingofinformationaboutscientificadvancesandimplementationofhealtheducation,management,andpreventionprogramsforasthma.
Global Alliance Against Chronic Respiratory Diseases (GARD). GINAisapartnerorganizationoftheGlobalAllianceAgainstChronicRespiratoryDiseases(GARD),aWorldHealthOrganizationinitiative(http://www.who.int/respiratory/gard/en/).ThegoalofGARDistofacilitatecollaborationamongexistinggovernmentalandnongovernmentalprogramsinterestedinchronicrespiratorydiseasestoassuremoreefficientutilizationofresourcesandavoidduplicationofefforts.Theparticipatingorganizationswilldevelopacomprehensiveglobalapproachtothepreventionandcontrolofchronicrespiratorydiseases,withaspecialemphasisondevelopingcountries.StrategiesforaffordabledrugprocurementthroughanAsthmaDrugFacility(www.GlobalADF.org)areamongthegoalsofGARDandarebeingpursuedactivelybyoneofthepartnergroups,theInternationalUnionAgainstTuberculosisandLungDiseases(IUATLD).
REFERENCES
1. StewartAW,MitchellEA,PearceN,StrachanDP,WeilandonSK.Therelationshipofpercapitagrossnationalproducttotheprevalenceofsymptomsofasthmaandotheratopicdiseasesinchildren(ISAAC).Int J Epidemiol2001;30(1):173-9.
2. HigginsBG,BrittonJR,ChinnS,CooperS,BurneyPG,TattersfieldAE.Comparisonofbronchialreactivityandpeakexpiratoryflowvariabilitymeasurementsforepidemiologicstudies.Am Rev Respir Dis1992;145(3):588-93.
3. PartridgeMR,HarrisonBD,RudolphM,BellamyD,SilvermanM.TheBritishAsthmaGuidelines--theirproduction,disseminationandimplementation.BritishAsthmaGuidelinesCo-ordinatingCommittee.Respir Med1998;92(8):1046-52.
4. DavisDA,ThomsonMA,OxmanAD,HaynesRB.Changingphysicianperformance.Asystematicreviewoftheeffectofcontinuingmedicaleducationstrategies.JAMA 1995;274(9):700-5.
5. BeroLA,GrilliR,GrimshawJM,HarveyE,OxmanAD,ThomsonMA.Closingthegapbetweenresearchandpractice:anoverviewofsystematicreviewsofinterventionstopromotetheimplementationofresearchfindings.TheCochraneEffectivePracticeandOrganizationofCareReviewGroup.BMJ1998;317(7156):465-8.
GINA DISSEMINATION AND IMPLEMENTATION RESOURCES
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

110 IMPLEMENTATION OF ASTHMA GUIDELINES IN HEALTH SYSTEMS
6. SullivanSD,LeeTA,BloughDK,FinkelsteinJA,LozanoP,InuiTS, et al.AmultisiterandomizedtrialoftheeffectsofphysicianeducationandOrganizationalchangeinchronicasthmacare:cost-effectivenessanalysisofthePediatricAsthmaCarePatientOutcomesResearchTeamII(PAC-PORTII).Arch Pediatr Adolesc Med2005;159(5):428-34.
7. HaahtelaT,KlaukkaT,KoskelaK,ErholaM,LaitinenLA.AsthmaprogrammeinFinland:acommunityproblemneedscommunitysolutions.Thorax 2001;56(10):806-14.
8. HaahtelaT,TuomistoLE,PietinalhoA,KlaukkaT,ErholaM,Kaila M, et al.A10yearasthmaprogrammeinFinland:majorchangeforthebetter.Thorax2006;61(8):663-70.
9. NathanRA,SorknessCA,KosinskiM,SchatzM,LiJT,Marcus P, et al.Developmentoftheasthmacontroltest:asurveyforassessingasthmacontrol.J Allergy Clin Immunol 2004;113(1):59-65.
10. JuniperEF,O’ByrnePM,GuyattGH,FerriePJ,KingDR.Developmentandvalidationofaquestionnairetomeasureasthmacontrol.Eur Respir J1999;14:902-7.
11. JuniperEF,BousquetJ,AbetL,BatemanED.Identifying‘wellcontrolled’and‘notwell-controlled’asthmausingtheAsthmaControlQuestionnaire.Respir Med2005.
12. JuniperEF,SvenssonK,MorkAC,StahlE.Measurementpropertiesandinterpretationofthreeshortenedversionsoftheasthmacontrolquestionnaire.Respir Med2005;99(5):553-8.
13. VollmerWM,MarksonLE,O’ConnorE,SanockiLL,FittermanL,BergerM,et al.Associationofasthmacontrolwithhealthcareutilizationandqualityoflife.Am J Respir Crit Care Med 1999;160(5Pt1):1647-52.
14. WeissKB,SullivanSD.Thehealtheconomicsofasthmaandrhinitis.I.Assessingtheeconomicimpact.J Allergy Clin Immunol2001;107(1):3-8.
15. VollmerWM,MarksonLE,O’ConnorE,FrazierEA,BergerM,BuistAS.Associationofasthmacontrolwithhealthcareutilization:aprospectiveevaluation.Am J Respir Crit Care Med 2002;165(2):195-9.
16. GlobalStrategyforAsthmaManagementandPrevention,2006;GlobalInitiativeforAsthma(GINA),http://www.ginasthma.org.
17. BatemanED,BousheyHA,BousquetJ,BusseWW,ClarkTJ,Pauwels RA, et al.Canguideline-definedasthmacontrolbeachieved?TheGainingOptimalAsthmaControLstudy.Am J Respir Crit Care Med2004;170(8):836-44.
18. PriceMJ,BriggsAH.Developmentofaneconomicmodeltoassessthecosteffectivenessofasthmamanagementstrategies.Pharmacoeconomics2002;20(3):183-94.
19. SullivanS,ElixhauserA,BuistAS,LuceBR,EisenbergJ,WeissKB.NationalAsthmaEducationandPreventionProgramworkinggroupreportonthecosteffectivenessofasthmacare.Am J Respir Crit Care Med1996;154(3Pt2):S84-95.
20. BouletLP,FitzGeraldJM,LevyML,CruzAA,PedersenS,Haahtela,T,BatemanED.AguidetothetranslationoftheGlobalInitiativeforAsthma(GINA)strategyintoimprovedcare.Eur Respir J2012;39:1220-9..
21. CazzolettiL,MarconA,JansonC,CorsicoA,JarvisD,PinI,et al;TherapyandHealthEconomicsGroupoftheEuropeanCommunityRespiratoryHealthSurvey.AsthmacontrolinEurope:areal-worldevaluationbasedonaninternationalpopulation-basedstudy.J Allergy Clin Immunol 2007 Dec;120(6):1360-7.
22. CunninghamS,LoganC,LockerbieL,DunnMJ,McMurrayA,PrescottRJ.Effectofanintegratedcarepathwayonacuteasthma/wheezeinchildrenattendinghospital:clusterrandomizedtrial.J Pediatr2008Mar;152(3):315-20.Epub2007Nov26.
23. BereznickiBJ,PetersonGM,JacksonSL,WaltersEH,FitzmauriceKD,GeePR.Data-miningofmedicationrecordstoimproveasthmamanagement.Med J Aust. 2008Jul7;189(1):21-5
COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

NOTESCOPY
RIGHTE
D MAT
ERIA
L - D
O NOT
ALTE
R OR R
EPRODUCE

NOTESCOPY
RIGHTE
D MAT
ERIA
L - D
O NOT
ALTE
R OR R
EPRODUCE

COPYRIG
HTED M
ATER
IAL
- DO N
OT AL
TER O
R REP
RODUCE

Almirall
AstraZeneca
Boehringer Ingelheim
CIPLA
Chiesi
GlaxoSmithKline
Merck Sharp & Dohme Novartis
Quintiles
Takeda
The Global Initiative for Asthma is supported by unrestricted educational grants from:
Visit the GINA website at www.ginaasthma.org© 2012 Global Initiative for Asthma COPY
RIGHTE
D MAT
ERIA
L - D
O NOT
ALTE
R OR R
EPRODUCE