GIM Primary Care Conf. Presentation Dec. 12, 2007 University of Wisconsin School of Medicine and...
26
GIM Primary Care Conf. Presentation GIM Primary Care Conf. Presentation Dec. 12, 2007 Dec. 12, 2007 University of Wisconsin School of Medicine and University of Wisconsin School of Medicine and Public Health Center for Tobacco Research and Public Health Center for Tobacco Research and Intervention Intervention Stevens S. Smith, Ph.D. Stevens S. Smith, Ph.D. Associate Professor / Licensed Psychologist Associate Professor / Licensed Psychologist Department of Medicine Department of Medicine University of Wisconsin School of Medicine and University of Wisconsin School of Medicine and Public Health Public Health Center for Tobacco Research and Intervention Center for Tobacco Research and Intervention Psychiatric Sequelae Psychiatric Sequelae Of Fibromyalgia Of Fibromyalgia
-
Upload
muriel-nicholson -
Category
Documents
-
view
213 -
download
0
Transcript of GIM Primary Care Conf. Presentation Dec. 12, 2007 University of Wisconsin School of Medicine and...

GIM Primary Care Conf. Presentation GIM Primary Care Conf. Presentation
Dec. 12, 2007Dec. 12, 2007
University of Wisconsin School of Medicine and Public Health University of Wisconsin School of Medicine and Public Health
Center for Tobacco Research and InterventionCenter for Tobacco Research and Intervention
Stevens S. Smith, Ph.D.Stevens S. Smith, Ph.D.Associate Professor / Licensed PsychologistAssociate Professor / Licensed Psychologist
Department of MedicineDepartment of Medicine
University of Wisconsin School of Medicine and Public HealthUniversity of Wisconsin School of Medicine and Public Health
Center for Tobacco Research and InterventionCenter for Tobacco Research and Intervention
Psychiatric Sequelae Psychiatric Sequelae Of FibromyalgiaOf Fibromyalgia

Disclosure StatementDisclosure Statement
I have received no research or salary I have received no research or salary support related to today’s presentation.support related to today’s presentation.

Case: The Story of Mr. OCase: The Story of Mr. O
• Referred for treatment of depression in August 2001Referred for treatment of depression in August 2001
• 56 year-old insurance executive56 year-old insurance executive
• Supportive wife and childrenSupportive wife and children
• Multiple health problems at initial evaluation in 2001:Multiple health problems at initial evaluation in 2001:- Type II diabetes- Type II diabetes - Hypertension- Hypertension- Dyslipidemia- Dyslipidemia - Sleep apnea- Sleep apnea- Mild, intermittent asthma- Mild, intermittent asthma - Chronic pain- Chronic pain- Bilateral hearing loss- Bilateral hearing loss - Fibromyalgia- Fibromyalgia

Selected Medical HistorySelected Medical History
• Self-described “sickly child”Self-described “sickly child”
• Surgery for coarctation of aorta – age 13 yrsSurgery for coarctation of aorta – age 13 yrs
• Never used tobacco; no AODA problemsNever used tobacco; no AODA problems
• Fibromyalgia first diagnosed in 2000 at Mayo ClinicFibromyalgia first diagnosed in 2000 at Mayo Clinic
• 2002 – 2004: worsening of fibromyalgia pain resulting 2002 – 2004: worsening of fibromyalgia pain resulting in multiple ER, primary care, and specialist visitsin multiple ER, primary care, and specialist visits

Selected Psychiatric HistorySelected Psychiatric History
• First diagnosed with depression in 2000 at Mayo Clinic (when First diagnosed with depression in 2000 at Mayo Clinic (when fibromyalgia was diagnosed); no prior hx of psychiatric illnessfibromyalgia was diagnosed); no prior hx of psychiatric illness
– prescribed sertralineprescribed sertraline
• Initiation of treatment with me for depression - August 2001Initiation of treatment with me for depression - August 2001
• Fall 2001 – consult with Madison psychiatristFall 2001 – consult with Madison psychiatrist
– discontinued sertraline; discontinued sertraline;
– prescribed fluoxetine and clonazepam prnprescribed fluoxetine and clonazepam prn
• Evaluated at UW Psychiatry in late 2001Evaluated at UW Psychiatry in late 2001
– discontinued fluoxetinediscontinued fluoxetine
– prescribed bupropion; continued clonazepam prnprescribed bupropion; continued clonazepam prn

Selected Psychiatric HistorySelected Psychiatric History
• Additional psychiatric consults from 2002 – 2004 with Additional psychiatric consults from 2002 – 2004 with changes in medication and psychiatristschanges in medication and psychiatrists
– bupropion bupropion citalopram citalopram sertraline sertraline mirtazapine mirtazapine
• Because of insurance problems, our psychotherapy Because of insurance problems, our psychotherapy was interrupted from July 2002 to October 2004was interrupted from July 2002 to October 2004
• November – December 2004: significant worsening of November – December 2004: significant worsening of depression with suicidal ideation (first time ever)depression with suicidal ideation (first time ever)
– exacerbation of health problems, esp. fibromyalgiaexacerbation of health problems, esp. fibromyalgia
– high levels of work-related stresshigh levels of work-related stress

Selected Psychiatric HistorySelected Psychiatric History
• Mr. O agreed to seek further evaluation and treatment Mr. O agreed to seek further evaluation and treatment at Mayo Clinic in January 2005 resulting in a two-week at Mayo Clinic in January 2005 resulting in a two-week inpatient stayinpatient stay
• Received medical and psychiatric evaluationReceived medical and psychiatric evaluation
• Diagnosed with MDD, Recurrent, Severe, without Diagnosed with MDD, Recurrent, Severe, without psychotic featurespsychotic features
• Received cognitive-behavioral therapyReceived cognitive-behavioral therapy
• Enrolled into an ECT study and received four Enrolled into an ECT study and received four treatmentstreatments

Selected Psychiatric HistorySelected Psychiatric History
• Mayo discharge plan:Mayo discharge plan:
– recommended follow-up care at Sleep Disorder Clinic, recommended follow-up care at Sleep Disorder Clinic, Fibromyalgia Clinic, and the Pain Rehabilitation Center Fibromyalgia Clinic, and the Pain Rehabilitation Center
– recommended that Mr. O get a new psychiatristrecommended that Mr. O get a new psychiatrist
• Mayo discharge medications:Mayo discharge medications:
- glyburide, r- glyburide, rosiglitazone, metformin, valsartan, fluvastatin, osiglitazone, metformin, valsartan, fluvastatin, fluticasone, hydrocodone, aspirin, ibuprofenfluticasone, hydrocodone, aspirin, ibuprofen
- discontinuation of mirtazapine, modafinil, clonazepam, and - discontinuation of mirtazapine, modafinil, clonazepam, and gabapentingabapentin
- duloxetine started- duloxetine started

Selected Psychiatric HistorySelected Psychiatric History
• Mr. O returned to Mayo a few months later for a two-week stay at Mr. O returned to Mayo a few months later for a two-week stay at the Mayo Comprehensive Pain Rehabilitation Centerthe Mayo Comprehensive Pain Rehabilitation Center
• Addressed at Mayo:
– fibromyalgia-related pain
– memory problems
– physical deconditioning
– mood and stress management
– nutritional therapy in regard to diabetes and hyperlipidemia
– discontinuation of ibuprofen and Tylenol #3
• Retired in mid-2005; on disabilityRetired in mid-2005; on disability

Fibromyalgia- Diagnostic CriteriaFibromyalgia- Diagnostic CriteriaAmerican College of Rheumatology (1990)American College of Rheumatology (1990)
• Hx of widespread pain; present for at least 3 monthsHx of widespread pain; present for at least 3 months• Pain in 11 of 18 tender point sites

• fatigue fatigue • sleep disturbances sleep disturbances • morning stiffnessmorning stiffness• headachesheadaches• irritable bowel syndromeirritable bowel syndrome• painful menstrual periodspainful menstrual periods• numbness or tingling of the extremitiesnumbness or tingling of the extremities• restless legs syndromerestless legs syndrome• temperature sensitivitytemperature sensitivity• cognitive/memory problems (“fibro fog”)cognitive/memory problems (“fibro fog”)• difficulty concentratingdifficulty concentrating
Fibromyalgia Syndrome:Fibromyalgia Syndrome:Symptoms Other Than PAINSymptoms Other Than PAIN

• Early 1800s – called “muscular rheumatism” Early 1800s – called “muscular rheumatism” • Tender points described in 1824 Tender points described in 1824 • Psychiatrist in 1880 described widespread pain, Psychiatrist in 1880 described widespread pain,
fatigue, and emotional disturbance as “neurasthenia”fatigue, and emotional disturbance as “neurasthenia”• 1904 – syndrome called “fibrositis”1904 – syndrome called “fibrositis”• 1976 – term “fibromyalgia” coined1976 – term “fibromyalgia” coined• First recognized by the AMA in 1987First recognized by the AMA in 1987• ACR diagnostic criteria published in 1990ACR diagnostic criteria published in 1990• No consensus on causes, treatments, or nosological No consensus on causes, treatments, or nosological
statusstatus
History of FibromyalgiaHistory of Fibromyalgia

• Probably results from abnormal central pain Probably results from abnormal central pain processingprocessing
• Mechanisms may include:Mechanisms may include:- Central sensitizationCentral sensitization- suppression of descending inhibitory pathwayssuppression of descending inhibitory pathways- excessive activity of glial cellsexcessive activity of glial cells- abnormalities of neurotransmitter release or abnormalities of neurotransmitter release or regulatory proteins or bothregulatory proteins or both
Pathophysiology of FibromyalgiaPathophysiology of Fibromyalgia
(Source: Abeles et al., 2007; Annals of Internal Medicine, 146:726-734)(Source: Abeles et al., 2007; Annals of Internal Medicine, 146:726-734)

Staud R and Rodriguez ME (2006) Mechanisms of Disease: pain in fibromyalgia syndromeNat Clin Pract Rheumatol 2: 90–98 doi:10.1038/ncprheum0091
Figure 1 Pathogenesis of pain in fibromyalgia syndrome

Yunus 2007; Seminars inArthritis and Rheumatology, 36:339-356

Fibromyalgia – General EpidemiologyFibromyalgia – General Epidemiology
London Fibromyalgia Epidemiology Study London Fibromyalgia Epidemiology Study (1999; J Rheumatol., 26(7):1570-6)(1999; J Rheumatol., 26(7):1570-6)
• Random community sample of 3395 adults residing Random community sample of 3395 adults residing in London, Ontarioin London, Ontario
• Overall prevalence of 3.3% (confirmed by Overall prevalence of 3.3% (confirmed by rheumatologist exam)rheumatologist exam)
• 4.9% of women; 1.6% of men met ACR criteria4.9% of women; 1.6% of men met ACR criteria• Peak prevalence – ages 55-64: 8% of womenPeak prevalence – ages 55-64: 8% of women
2.5% of men2.5% of men

Fibromyalgia – General EpidemiologyFibromyalgia – General Epidemiology
Population-based Cohort Study using Insurance Population-based Cohort Study using Insurance Claims Claims (2006; J Clin Rheumatol., 12(3):124-8)(2006; J Clin Rheumatol., 12(3):124-8)
• 62,000 enrollees over the period 1997 through 200262,000 enrollees over the period 1997 through 2002 • Approximately 4.2% met ICD-9 fibromyalgia criteria• Females were 1.64 times more likely than males to
have fibromyalgia
• Fibromyalgia patients were 2 to 7 times more likely to have comorbid conditions (e.g., depression, anxiety, IBS, CFS, lupus, and RA).
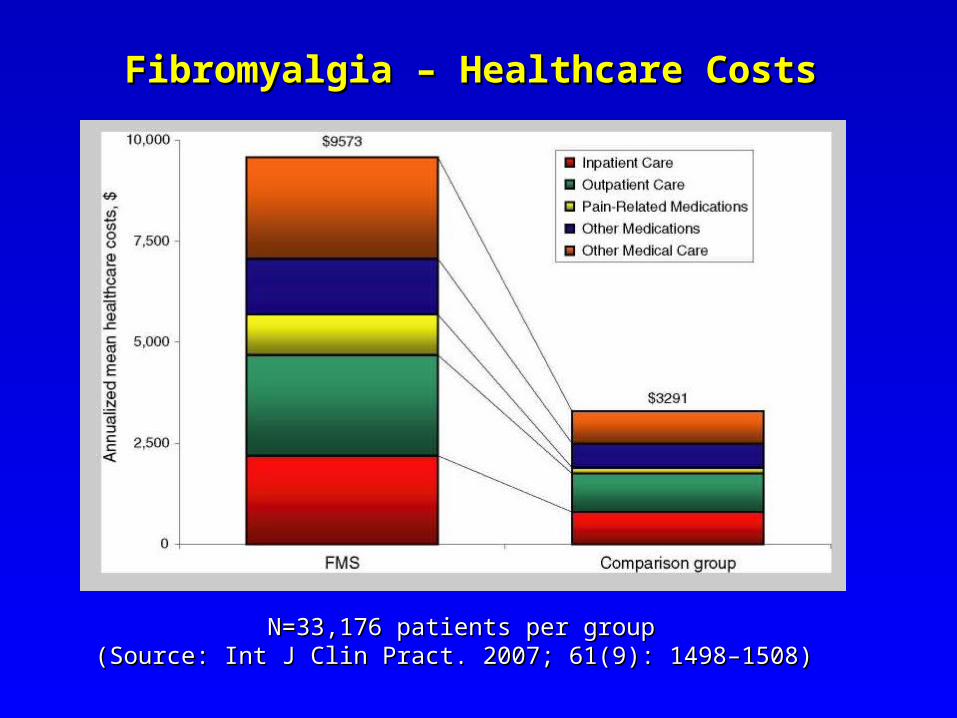
Fibromyalgia – Healthcare CostsFibromyalgia – Healthcare Costs
N=33,176 patients per groupN=33,176 patients per group(Source: Int J Clin Pract. 2007; 61(9): 1498–1508)(Source: Int J Clin Pract. 2007; 61(9): 1498–1508)

Fibromyalgia – Use of Pain-Related MedicationFibromyalgia – Use of Pain-Related Medication
(Source: Int J Clin Pract. 2007; 61(9): 1498–1508)(Source: Int J Clin Pract. 2007; 61(9): 1498–1508)
Pain-RelatedPain-Related
MedicationMedication
Fibromyalgia Fibromyalgia PatientsPatients
(N=33,176)(N=33,176)
Comparison Comparison PatientsPatients
(N=33,176)(N=33,176)
OpioidsOpioids 37.8%37.8% 12.4%12.4%
BenzodiazepinesBenzodiazepines 20.1%20.1% 5.8%5.8%
NSAIDsNSAIDs 29.3%29.3% 11.0%11.0%
Muscle relaxantsMuscle relaxants 22.4%22.4% 3.9%3.9%
AntidepressantsAntidepressants 38.7%38.7% 11.9%11.9%
Antidepressant + Antidepressant + OpioidOpioid 23.9%23.9% 3.4%3.4%

Fibromyalgia – Psychiatric Comorbidity:Fibromyalgia – Psychiatric Comorbidity:A Family StudyA Family Study
(Source: Arnold et al., 2006; J Clin Psychiatry, 67: 1219–1225)(Source: Arnold et al., 2006; J Clin Psychiatry, 67: 1219–1225)
• Patients recruited from rheumatology outpatient clinicsPatients recruited from rheumatology outpatient clinics- 78 fibromyalgia probands + 146 of their relatives78 fibromyalgia probands + 146 of their relatives- 40 RA probands + 72 of their relatives40 RA probands + 72 of their relatives
• All fibromyalgia patients met ACR criteriaAll fibromyalgia patients met ACR criteria• Utilized structured psychiatric interviews for DSM-IV Utilized structured psychiatric interviews for DSM-IV
psychiatric diagnosespsychiatric diagnoses

Fibromyalgia – Psychiatric Comorbidity:Fibromyalgia – Psychiatric Comorbidity:A Family StudyA Family Study
(Source: Arnold et al., 2006; J Clin Psychiatry, 67: 1219–1225)(Source: Arnold et al., 2006; J Clin Psychiatry, 67: 1219–1225)
Lifetime DSM-IV Lifetime DSM-IV DisorderDisorder
Fibromyalgia Fibromyalgia PatientsPatients
(N=108)(N=108)
Comparison Comparison PatientsPatients
(N=228)(N=228)
Mood DisorderMood Disorder 73.1%73.1% 34.2%34.2%
Any Anxiety DisorderAny Anxiety Disorder 55.6%55.6% 17.5%17.5%
Any Substance Use Any Substance Use DisorderDisorder
24.1%24.1% 19.3%19.3%
Eating DisorderEating Disorder 11.1%11.1% 2.6%2.6%
Somatoform DisordersSomatoform Disorders 2.8%2.8% 0%0%

(Source: Arnold et al., 2006; J Clin Psychiatry, 67: 1219–1225)(Source: Arnold et al., 2006; J Clin Psychiatry, 67: 1219–1225)

Fibromyalgia – Psychiatric Comorbidity:Fibromyalgia – Psychiatric Comorbidity:A Family Study (Arnold et al., 2006)A Family Study (Arnold et al., 2006)
(Source: Arnold et al., 2006; J Clin Psychiatry, 67: 1219–1225)(Source: Arnold et al., 2006; J Clin Psychiatry, 67: 1219–1225)
• Evidence for shared risk factors for fibromyalgia and Evidence for shared risk factors for fibromyalgia and mood and anxiety disorders mood and anxiety disorders
• This and other studies do not support the hypothesis This and other studies do not support the hypothesis that fibromyalgia results from psychiatric disordersthat fibromyalgia results from psychiatric disorders
• Fibromyalgia overlaps with both psychiatric disorders Fibromyalgia overlaps with both psychiatric disorders as well as medical conditions such as CFS, IBS, MCSas well as medical conditions such as CFS, IBS, MCS

Case: The Continuing Story of Mr. OCase: The Continuing Story of Mr. O
• Nasal surgery in 2005 helped his sleep apneaNasal surgery in 2005 helped his sleep apnea
• Continues to have significant pain and depressionContinues to have significant pain and depression
• Since 2005, Mr. O has made concerted but inconsistent effort to Since 2005, Mr. O has made concerted but inconsistent effort to use the coping strategies he learned at Mayo & UW:use the coping strategies he learned at Mayo & UW:
– Daily exerciseDaily exercise
– Deep breathingDeep breathing
– RelaxationRelaxation
– Pacing self in terms of exertionPacing self in terms of exertion
– Appropriate use of medicationsAppropriate use of medications

Case: The Continuing Story of Mr. OCase: The Continuing Story of Mr. O
• Follow-up visits to Mayo (ECT study; Pain Clinic)Follow-up visits to Mayo (ECT study; Pain Clinic)
• Added trazodone for help with sleepAdded trazodone for help with sleep
• Added tramadol and tiagabine for help with painAdded tramadol and tiagabine for help with pain
• Diabetes has worsened; now using LantusDiabetes has worsened; now using Lantus
• Arthritis now an issueArthritis now an issue
• Hearing loss has worsenedHearing loss has worsened
• Most recent follow-up at Mayo indicated a previously undetected Most recent follow-up at Mayo indicated a previously undetected heart attack; follow-up at Mayo scheduledheart attack; follow-up at Mayo scheduled
• Psychotherapy + duloxetine - ongoingPsychotherapy + duloxetine - ongoing

(Source: Sarzi-Puttini et (Source: Sarzi-Puttini et al., in press; Semin al., in press; Semin Arthritis Rheum.Arthritis Rheum. ))