Giardia lamblia Dr. Bimal Kumar Das Department of Microbiology All India Institute of Medical...
29
Giardia lamblia Dr. Bimal Kumar Das Department of Microbiology All India Institute of Medical Scinces New Delhi-29 Source: http://soils.cses.vt.edu
-
Upload
maude-beasley -
Category
Documents
-
view
216 -
download
1
Transcript of Giardia lamblia Dr. Bimal Kumar Das Department of Microbiology All India Institute of Medical...

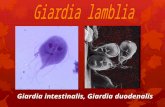
Giardia lamblia
Dr. Bimal Kumar DasDepartment of Microbiology
All India Institute of Medical ScincesNew Delhi-29
Source: http://soils.cses.vt.edu

The genus Giardia belongs to the class Zoomastigophorea, the order Diplomonadida, and the family Hexamitidae.
It is one of the most primitive eukaryotes: it has a small subunit ribosomal RNA sequence and no mitochondria and Golgi apparatus
Now Giardia can be classified according to antigen, isoenzyme, and genetic analysis in addition to their morphology and host range.
G. lamblia (also called intestinalis or duodenalis) is the species infecting humans.

Species identified
Giardia lamblia (intestinalis, duodenalis) - humans, mammals
Giardia muris - mammals Giardia ardeae - birds Giardia psittaci - birds Giardia agilis - amphibians

Cysteine-rich surface protein termed the variant specific surface protein responsible for antigenic variation within species
These proteins may help to protect the parasite against the activity of intestinal proteases, as well as play a role in immune evasion.
Of the Giardia species, only G. lamblia has been successfully cultured in vitro.
The trophozoite divides by longitudinal binary fission
Two morphological forms: Trophozoite and cyst ( infective form)

Tear drop shaped2 adhesive discs, 2 median bodies,2 nuclei 4 pairs of flagella
Source: www.sd01.k12.id.us

intracytoplasmic projections axonemes
Source: http://medlib.med.utah.edu

Haematoxilyn staining
two nuclei, each with a prominent central karyosome (characteristic facelike image )
Source: Gallery of histology Woods and Ellis2000

8 to 12 mm long and 7 to 10 mm wide
convex dorsal surface
a flat ventral surface sucking or adhesive disk
four pairs flagellae
Source: http://soils.cses.vt.edu

Epidemiology
Presumed to be zoonotic, but new evidence indicates that strains may be species specific.
Host can be humans, primates, cats, dogs, calves, beavers, rabbits, etc.
World wide distribution
Highest incidence in children, young adults in late summer.

Transmission
Person to person transmission
Water sports, surface contamination. Watershed contamination
sexually active male homosexuals and persons in custodial institutions.

Pathogenesis and Immune response (1)
•The production of diarrhea, and occasionally malabsorption, is the result of a complex interaction of Giardia with the host,
•Infection occurs after oral ingestion of as few as 10 to 25 cysts.
•After excystation, trophozoites colonize and multiply in the upper small bowel
•Adherence of G. lamblia in the human gut may be via the disk, but may also involve specific receptor-ligand interactions

Pathogenesis and Immune response (2)
Several pathogenic mechanisms have been postulated
Disruption of the brush border
Mucosal invasion
Elaboration of an enterotoxin
Stimulation of an inflammatory infiltration leading to fluid and electrolyte secretion and occasionally to villous changes

TEM micrograph showing the method of attachment to the duodenal wall.
Ventral sucking discSource: Gallery of histology Woods and Ellis2000

Giardia Lamblia clinging to the wall of a duodenal villus.
Source: Gallery of histology Woods and Ellis2000

Immune Response
Partially protective immunity may develop to Giardia
Immune response involves both cellular and humoral immunity
Ig A, serum Ig G and Ig M are detected in patients: role of Ig A is not completely understood, probably inhibits trophozoite attachment
IgA deficiency lead to chronic giardiasis
Cell mediated immune response may also play a role
Human milk may also play a role in protection of the host against Giardia : Free fatty acids and IgA antibodies

Infection with G. lamblia includesasymptomatic cyst passage (5 to 15% ) •acute self-limited diarrhea (25 to 50% ) •and a chronic syndrome of diarrhea •malabsorption, and weight loss
Symptomatic giardiasis is characterized by •acute onset of diarrhea, •abdominal cramps, bloating, and flatulence •feelings of malaise, nausea, and anorexia •may complain of sulfuric belching •Vomiting, fever, and tenesmus occur less commonly. •stools may be profuse and watery, but later they are commonly greasy, and foul-smelling and may float

The role that chronic infection with Giardia plays in the growth and development of children in the developing world has been controversial

Life Cycle
Trophozoites : Lives in duodenum, jejenum and upper ileum
They come in close contact to the mucosal, but do not invade the host. Adhesive disc fits over surface of epithelial cell
The flagella act as a pump to move nutrients away from the microvilla and hold the adhesive disc near the mucosa.
Rapid division to produce large numbers quickly


Source: Doug Allington

14 billion parasites in diarrheic stool (trophozoites only) Moderate infection: 300 million cysts.
As the organism traverses the colon it is stimulated to encyst.
Produce an oval cyst with thick walls, with 2-4 nuclei.
Dividing within cyst (4 nuclei is older cyst)
Complete division in duodenum of host after ingestion
Cyst is approximately 8-10m and ellipsoid in shape.
The cyst is the infective state and is transferred by the fecal-oral route.

Diagnosis • Giardia should be identified 50 to 70% of the time after one stool, and 90% identification after three stools
• Wet, saline mounts: falling leaf motion, fibrils present, and nucleic characteristics.
• Biopsy tissue/duodenal aspirate stained by trichrome or Giemsa stain.
• Enzyme immunoassay and fluorescent-anitbody monoclonal antigen detection systems
• Sensitivity & specificity: 90-100%( ProSpec T, GiardEIA, MeriFluor, Color Vue, and DD System)

Source: http://soils.cses.vt.edu

Source: Doug Allington

Source: Doug Allington

Source: http://www. cbc.ca

Drug Adult Pediatric
Metronidazole 250mgtidX 5-7 d 5mg/kg/tid x 7 d
Quinacrine 100mgtidX5-7d 2mg/kg tidX7d
Furazolidone 100 mg qid × 7–10 d 2 mg/kg qid × 10
Paromomycin 25–30 mg/kg/d in 3 doses × 5–10 d
Tinidazole 2 g × 1 dose

PREVENTION The prevention of giardiasis requires proper handling and treatment of water
Good personal hygiene on an individual basis
Chlorination alone is sufficient to kill G. lamblia cysts, important variables, such as water temperature, clarity, pH, and contact time, alter the efficacy of chlorine, and higher chlorine levels (4 to 6 mg/liter) may be required.
Bringing water to a boil is sufficient to kill all protozoal cysts; at high altitudes, boiling for longer periods may be necessary

Artistic impression by Russel KightleySource: http://soils.cses.vt.edu