Gi A&P H&P
56
12/03/09 12/03/09 1 Gastroenterology Gastroenterology Miami Dade College Miami Dade College Medical Center Campus Medical Center Campus Physician Assistant Program Physician Assistant Program Instructor: Pascale Gehy-Andrè, Instructor: Pascale Gehy-Andrè, PA-C PA-C Current Medical Dx & Tx 2007 Cecil Essentials Of Medicine 6th edition
-
Upload
miami-dade -
Category
Health & Medicine
-
view
785 -
download
4
Transcript of Gi A&P H&P

12/03/0912/03/09 11
GastroenterologyGastroenterology
Miami Dade CollegeMiami Dade CollegeMedical Center CampusMedical Center Campus
Physician Assistant ProgramPhysician Assistant ProgramInstructor: Pascale Gehy-Andrè, Instructor: Pascale Gehy-Andrè,
PA-CPA-C
Current Medical Dx & Tx 2007Cecil Essentials Of Medicine 6th edition

12/03/0912/03/09 22
Introduction to Introduction to Gastrointestinal Gastrointestinal
Medicine in Medicine in Primary CarePrimary Care ReviewReview of of
Anatomy & Anatomy & PhysiologyPhysiology

12/03/0912/03/09 33
Gastrointestinal TractGastrointestinal TractConsists of the Alimentary Tract (hollow tube), and Consists of the Alimentary Tract (hollow tube), and accessory organs (liver, gallbladder, teeth, salivary accessory organs (liver, gallbladder, teeth, salivary glands, tongue, pancreas)glands, tongue, pancreas)GI tract is 9 meters (~30 feet)GI tract is 9 meters (~30 feet)4 layers of GI tract4 layers of GI tract– 1. Mucosa-absorptive and secretory (innermost 1. Mucosa-absorptive and secretory (innermost
layer)layer)– 2. Submucosa-thick vascular connective tissue 2. Submucosa-thick vascular connective tissue
with Autonomic nervous supplywith Autonomic nervous supply– 3. Muscularis/Muscularis Externa-segmental 3. Muscularis/Muscularis Externa-segmental
contractions=peristalsis longitudinal smooth contractions=peristalsis longitudinal smooth muscle and nerve fibers.muscle and nerve fibers.
– 4. Serosa-outermost layer of connective tissue 4. Serosa-outermost layer of connective tissue for protection covered by squamous epitheliumfor protection covered by squamous epithelium

12/03/0912/03/09 44
EsophagusEsophagusCollapsible tube that connects pharynx to Collapsible tube that connects pharynx to stomach. stomach. Located Located behindbehind trachea. trachea. To introduce food from the mouth through To introduce food from the mouth through the negative pressure chest into the the negative pressure chest into the positive pressure abdomen, the esophagus positive pressure abdomen, the esophagus must transport food against a pressure must transport food against a pressure gradient and prevent reflux of gastric/ gradient and prevent reflux of gastric/ stomach contents. stomach contents. Majority of esophagus is smooth muscle= Majority of esophagus is smooth muscle= upper 1/3 skeletal, mid portion mix of upper 1/3 skeletal, mid portion mix of smooth and skeletal, lower 1/3=smooth smooth and skeletal, lower 1/3=smooth muscle. muscle. Most of esophagus is squamous Most of esophagus is squamous epithelium.epithelium.

12/03/0912/03/09 55
StomachStomach
Most distensible part of GI tractMost distensible part of GI tractConnected to esophagus above and Connected to esophagus above and duodenum below. duodenum below. Stores food, initiates digestion of Stores food, initiates digestion of protein and grinds food up that has protein and grinds food up that has not been properly masticated, also not been properly masticated, also kills bacteria and slowly moves food kills bacteria and slowly moves food into the small intestine as a pasty into the small intestine as a pasty “chyme”.“chyme”.

12/03/0912/03/09 66
Stomach (cont.)Stomach (cont.)Main parts of stomachMain parts of stomach– Fundus/CardiacFundus/Cardiac-parietal cells produces -parietal cells produces
1. HCL-makes pH<2 necessary to denature 1. HCL-makes pH<2 necessary to denature proteins+ allows pepsinogen to be converted proteins+ allows pepsinogen to be converted to active pepsin to break peptide bonds in to active pepsin to break peptide bonds in hydolysis of proteins left by HCL. hydolysis of proteins left by HCL. 2. Intrinsic factor-for absorption of B12.2. Intrinsic factor-for absorption of B12.
– BodyBody- inner surface, has long folds called - inner surface, has long folds called rugae, and openings within folds called rugae, and openings within folds called gastric pits.gastric pits.
– Antrum/Pyloric regionAntrum/Pyloric region-cell types- G -cell types- G (gastrin), Chief/zymogenic (pepsinogen), (gastrin), Chief/zymogenic (pepsinogen), goblet (mucus)goblet (mucus)

12/03/0912/03/09 77
AbsorptionAbsorption
*note that almost all absorption of *note that almost all absorption of food occurs in the small intestine. food occurs in the small intestine. The only substances absorbed by the The only substances absorbed by the stomach are alcohol and aspirin b/c stomach are alcohol and aspirin b/c of their lipid solubility.of their lipid solubility.

12/03/0912/03/09 88
Small Intestine (Small Bowel)Small Intestine (Small Bowel)
From pyloric sphincter to ileocecal From pyloric sphincter to ileocecal valve (door to large intestine)valve (door to large intestine)Largest part of GI tract (7 Largest part of GI tract (7 meters~21 ft)meters~21 ft)Parts of SIParts of SI– DuodenumDuodenum– JejunumJejunum– IleumIleum

12/03/0912/03/09 99
Small Intestine (Small Bowel)Small Intestine (Small Bowel)
Digestion absorbed across columnar Digestion absorbed across columnar epithelial lining (folded mucosa and epithelial lining (folded mucosa and submucosa=plica circulares).**submucosa=plica circulares).**Villi (fingerlike projections)Villi (fingerlike projections)MicrovilliMicrovilli

12/03/0912/03/09 1010
Large Intestine (Colon)Large Intestine (Colon)Fxn : absorption of fluid & electrolytes and for Fxn : absorption of fluid & electrolytes and for defecationdefecationFrom ileum, the chyme enters into cecum (blind From ileum, the chyme enters into cecum (blind pouch), now is fecespouch), now is fecesMore regular movements than sm. BowelMore regular movements than sm. BowelContains Haustrations and crypts (no villi)Contains Haustrations and crypts (no villi)Parts of ColonParts of Colon– Cecum/AppendixCecum/Appendix– AscendingAscending– TransverseTransverse– DescendingDescending– SigmoidSigmoid– RectumRectum– Anal CanalAnal Canal

12/03/0912/03/09 1111

12/03/0912/03/09 1212
Accessory OrgansAccessory OrgansLiver (largest internal organ) Liver (largest internal organ) – Dual blood supply (hepatic artery and portal vein)Dual blood supply (hepatic artery and portal vein)– Produces and secretes bileProduces and secretes bile
Bile salts, bile pigments (bilirubin-heme( iron containing Bile salts, bile pigments (bilirubin-heme( iron containing portion)), phospholipids (lecithin), cholesterol, inorganic portion)), phospholipids (lecithin), cholesterol, inorganic ions.ions.
– Detoxifies blood Detoxifies blood (excrete into bile, kupffer cells, chemical alteration (excrete into bile, kupffer cells, chemical alteration within hepatocytes i.e. conjugation, purines to uric acid, within hepatocytes i.e. conjugation, purines to uric acid, porphyrines to bilirubin, ammonia to urea)porphyrines to bilirubin, ammonia to urea)
– Metabolism/synthesis of Glucose, triglycerides, Metabolism/synthesis of Glucose, triglycerides, ketonesketones
– Plasma proteins made (albumin, globulins, Plasma proteins made (albumin, globulins, angiotensinogen)angiotensinogen)

12/03/0912/03/09 1313
Accessory Organs (cont.)Accessory Organs (cont.)GallbladderGallbladder– Stores bileStores bile– Secretion of CCK in response to fatty Secretion of CCK in response to fatty
acids helps contract GBacids helps contract GB
PancreasPancreas– Endocrine and Exocrine glandsEndocrine and Exocrine glands– For digestive portion, focus on exocrine For digestive portion, focus on exocrine
fxn (ducts)fxn (ducts)– Under vagus control, secretes amylase, Under vagus control, secretes amylase,
lipase (specific to pancreas), trypsinlipase (specific to pancreas), trypsin

12/03/0912/03/09 1414

12/03/0912/03/09 1515

12/03/0912/03/09 1616

12/03/0912/03/09 1717

12/03/0912/03/09 1818

12/03/0912/03/09 1919

12/03/0912/03/09 2020

12/03/0912/03/09 2121

12/03/0912/03/09 2222

12/03/0912/03/09 2323

12/03/0912/03/09 2424

12/03/0912/03/09 2525

12/03/0912/03/09 2626

12/03/0912/03/09 2727
ACID ACID SECRETIONSECRETION

12/03/0912/03/09 2828

12/03/0912/03/09 2929
Majority of nutrients absorbed in Majority of nutrients absorbed in JejunumJejunum

12/03/0912/03/09 3030
Gastrointestinal DiseasesGastrointestinal DiseasesHistory & Physical History & Physical
ExamExam

12/03/0912/03/09 3131

12/03/0912/03/09 3232

12/03/0912/03/09 3333

12/03/0912/03/09 3434

12/03/0912/03/09 3535

12/03/0912/03/09 3636

12/03/0912/03/09 3737

12/03/0912/03/09 3838

12/03/0912/03/09 3939

12/03/0912/03/09 4040

12/03/0912/03/09 4141
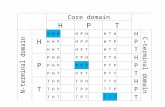
Cutaneous Hypersensitivity Pattern

12/03/0912/03/09 4242

12/03/0912/03/09 4343

12/03/0912/03/09 4444
Common Visceral Pain Patterns

12/03/0912/03/09 4545

12/03/0912/03/09 4646

12/03/0912/03/09 4747

12/03/0912/03/09 4848

12/03/0912/03/09 4949
Abdominal PainAbdominal Pain
Is the most frequent manifestation of an intra-Is the most frequent manifestation of an intra-abdominal process abdominal process Difficult to gauge pain severity & origin Difficult to gauge pain severity & origin secondary to many factors (severity is not secondary to many factors (severity is not always = seriousness)always = seriousness)Acute pain suggest sudden and more serious Acute pain suggest sudden and more serious processprocessChronic pain suggest more insidious and long Chronic pain suggest more insidious and long standing chronic disease.standing chronic disease.Requires close attention to the history & Requires close attention to the history & physical physical Usually requires diagnostic test to confirm Usually requires diagnostic test to confirm causecausePain out of proportion to exam = Pain out of proportion to exam = mesenteric ischemiamesenteric ischemia

12/03/0912/03/09 5050
Important NotesImportant Notes
ALL PATIENTS WITH ABDOMINAL ALL PATIENTS WITH ABDOMINAL PAIN SHOULD HAVE RECTAL PAIN SHOULD HAVE RECTAL EXAM EXAM
ALL FEMALE PATIENTS WITH ALL FEMALE PATIENTS WITH LOWER ABDOMINAL PAIN NEED LOWER ABDOMINAL PAIN NEED PELVIC EXAMPELVIC EXAM

12/03/0912/03/09 5151

12/03/0912/03/09 5252
The term melena refers to:The term melena refers to:– A. Blood in the vomitusA. Blood in the vomitus– B. Blood in the stool only detected by B. Blood in the stool only detected by
Hemacult/GuiaicHemacult/Guiaic– C. Black or tarry blood in the stoolC. Black or tarry blood in the stool– D. Bright red blood in the stoolD. Bright red blood in the stool

12/03/0912/03/09 5353
A patient with an upper G.I. bleed A patient with an upper G.I. bleed may present with:may present with:– A. HematemesisA. Hematemesis– B. MelenaB. Melena– C. HematocheziaC. Hematochezia– D. A, B, or CD. A, B, or C– E. A or BE. A or B

12/03/0912/03/09 5454
Absorption of digested food in the Absorption of digested food in the small intestine occurs across these small intestine occurs across these types of cellstypes of cells
– A. Squamous epitheliumA. Squamous epithelium– B. Columnar epitheliumB. Columnar epithelium– C. Pseudostratified epitheliumC. Pseudostratified epithelium– D. None of theseD. None of these

12/03/0912/03/09 5555
The most common symptom of an The most common symptom of an intra-abdominal problem isintra-abdominal problem is
– A. NauseaA. Nausea– B. VomitingB. Vomiting– C. Abdominal painC. Abdominal pain– D. Diarrhea D. Diarrhea

12/03/0912/03/09 5656
A 45 year old male presents with A 45 year old male presents with abdominal pain, diarrhea, and abdominal pain, diarrhea, and vomiting. You suspect a foodborne vomiting. You suspect a foodborne illness. Should you still offer a illness. Should you still offer a rectal exam to this patient?rectal exam to this patient?
– YesYes– NoNo











![Qå 1 1 Q+Q5QPQ#Q Q QWQ3dp.co.jp/bussiness/pdf/pdf_depalletizing.pdf · 2014. 8. 2. · +p p p p 0[`2!%46× ~ w ] î#ëh³h´h»h¯h· ±70 w ¾ · ] ¾ p åh³h¯h³h¹h¯h·h¯h¶h´hºh¢](https://static.fdocuments.us/doc/165x107/60c0ce9d864d2108c631b8ec/q-1-1-qq5qpqq-q-2014-8-2-p-p-p-p-0246-w-hhhhh-70.jpg)