Getting the Lead Out: Screening, Intervening, and Following-up Ginger Wagoner, R.N. Childhood Lead...
40
Getting the Lead Out: Screening, Intervening, and Following-up Ginger Wagoner, R.N. Childhood Lead Poisoning Prevention Program (CLPPP)
-
Upload
frank-airey -
Category
Documents
-
view
215 -
download
1
Transcript of Getting the Lead Out: Screening, Intervening, and Following-up Ginger Wagoner, R.N. Childhood Lead...

Getting the Lead Out: Screening, Intervening, and Following-up
Ginger Wagoner, R.N.
Childhood Lead Poisoning Prevention Program (CLPPP)

Adult & Child Health Improvement Lead Program Team
Justin Carey – Program Coordinator Ginger Wagoner – Case Manager/Health
Educator Susanna Ferguson – Environmentalist Krista Bailey – Secretary, III Vacant – Epidemiologist

History Lead was probably one of
the first metals to be produced by man dating back to 3500 B.C.
A small statue, found in Turkey, is the oldest known lead containing object made by human hands. It dates back to 6500 A.D.
History Continued…………. In 100 B.C. Greek doctors described
medical symptoms of lead poisoning among laborers and the lower classes.
27 B.C. – 476 A.D. – The time of the Roman Empire.
Lead was used to make pipes, dishes, cosmetics, coins and paint.

History Continued…… (Roman Empire)
Grapes to make wine were boiled in lead pots or lead lined copper kettles.
1/5 of the 450 recipes in the Roman Apician Cookbook, were enhanced with
lead.Lead acetate or “sugar of lead” was put
into wine and other foods to make them sweeter.
History Continued…… (Roman Empire)
Julius Caesar fathered only one child (even though he enjoyed many women.)
Caesar Augustus was sterile.
Some scholars believe lead poisoning may have contributed to the fall of the Roman empire. (1)
History Continued……. (Beethoven)
Ludwig van Beethoven died in 1827. The German composer suffered with digestive problems, abdominal pain, irritability and depression. Recent chemical analysis suggest that lead poisoning may have contributed to his death. (2)

History Continued…….. (Lead in Paint)
Paint has contained lead since the time of the Roman Empire.
In 1904 Dr. J.L. Gibson in Queensland, Australia, published an article showing that lead paint is harmful to painters & children.
In 1906 the National Lead Company copyrighted the Dutch Boy Painter Image. (3)

History Continued…….. (Lead in Paint)
By 1910 the majority of paints in the United States contained lead. (3)
In 1914 the first article appeared in the U.S. describing a case of lead paint poisoning in an infant. Over the next 25 years, scores of these articles appeared. (4)
Lead in paint was greatly reduced in 1955 & banned completely in 1978.

History Continued……..Lead is a toxic metal that has been known to
be harmful to man as far back as 100 B.C.Today lead poisoning is the number one
environmental health risk for children.Lead affects virtually every system of the
body, especially the developing brain and nervous system of fetuses & children less than 6 years of age.

Sources of Lead PoisoningThe 3 media to which
children are most likely to be either directly or indirectly exposed to lead are:
1. Deteriorated paint.(pre 1978)
2. Interior dust.3. Exterior soil or dust.

Other Sources of Lead Poisoning Vinyl Mini-blinds
(pre-1996) Fishing Sinkers &
Bullets Home Remedies such
as Azarcon & Greta (used for stomach aches)

Other Sources Continued…….. Hobbies (ceramics &
electronics) Candle Wicks Lead Crystal Lead Pipes Stained Glass Some Crayons & Side
Walk Chalk

Routes of ExposurePrimary route – Oral
Secondary routes – Inhalation Dermal
Storage of Lead in the BodyShortly after lead gets
into the body, it travels in the blood to the soft tissues – liver, kidneys, lungs, brain, spleen, muscles, & heart.
After several weeks, most lead is stored in the bones & teeth.

Elimination of Lead from the BodyLead that is not stored is eliminated in the urine and
feces.
60% loss in urine
30% loss in feces
10% loss in hair, nail growth, & sweat
About 99% of lead taken into the body of an adult will leave in the waste within a few weeks, but only about 32% will be eliminated from a child.

Treatment for Lead Poisoning Diet & Nutrition
Foods with Calcium, Iron, and Vitamin C help protect the body from lead.
Foods Low in Fat – Fat increases the amount of lead absorbed by the body.
Chelation Therapy

Signs & Symptoms of Lead Poisoning
Anemia Abdominal Pain Headache Constipation Seizures Coma Death

Neurological & Cognitive Effects of Lead Poisoning
Learning Disabilities Decreased IQ Decreased Attention
Span Hyperactivity Impaired Hearing Decreased Growth

Effects of Lead Poisoning 10µg/dL – Child will have learning
disabilities; impaired growth; IQ decline and some hearing loss.
20µg/dL – Interference with ability to make red blood cells.
30µg/dL – Less ability to use vitamin D; higher blood pressure & hearing loss.

Effects of Lead Poisoning Continued……..
40µg/dL – Less ability to make red blood cells. Nerve problems develop (decreased sensation, less ability to move quickly, infertility in men, kidney damage).
60µg/dL – Stomach aches/cramps. 70µg/dL – Mental retardation. 90µg/dL – Seizures, coma, kidney damage &
anemia. 130µg/dL & up – Seizures, coma & death.
Screening GuidelinesAll children between 6
months and 6 years of age should be given a verbal risk assessment for lead poisoning each time they visit their private physician or a health clinic.

Verbal Risk Assessment for Lead Poisoning
1. Does child live in or visit a building built before 1978 with peeling/chipping paint or with recent or ongoing remodeling?
2. Does child have a brother/sister/playmate who has or did have lead poisoning?
3. Do you (or a family member) work on a farm; in a bridge, tunnel, or high construction area; with batteries; ammunition, or visit a firing range?
4. Do you use any folk remedies that may contain lead or use pottery or ceramic ware for cooking, eating, or drinking?

Screening Guidelines Continued……..
If the verbal risk assessment is negative at each visit: A blood lead test should be performed on all
children at the ages of 12 months of age and again at 24 months of age.
A blood lead test should be performed on any child between 25 months of age and 72 months of age who has not previously been tested.

Screening Guidelines Continued……..
If a positive or “don’t know” answer is given to any question on the Verbal Risk Assessment the child should be given a blood test for lead poisoning beyond the routine periodicity schedule.

Federal Screening Guidelines Medicaid
It is a FEDERAL MANDATE that children who are Medicaid recipients receive a blood lead test at 9-12 months and again at 24 months of age.
Any child age 2 to 6 for whom no record of a lead test exists should also be screened.
Medicaid pays for screenings and any diagnostic or treatment services for EBL cases (e.g. x-rays, medicines) including case management.
Medicaid also reimburses for one environmental investigation per EBL household.

Case Management of Children with EBLLs
What is case management?Case management of children with EBLLs
involves coordinating, providing, and overseeing the services required to reduce their BLLs below the level of concern. (10µg/dL) (5)

Case Management The case manager
should develop a plan of care for each child with a EBLL.
This care plan will ensure appropriate care for all children with EBLLs.
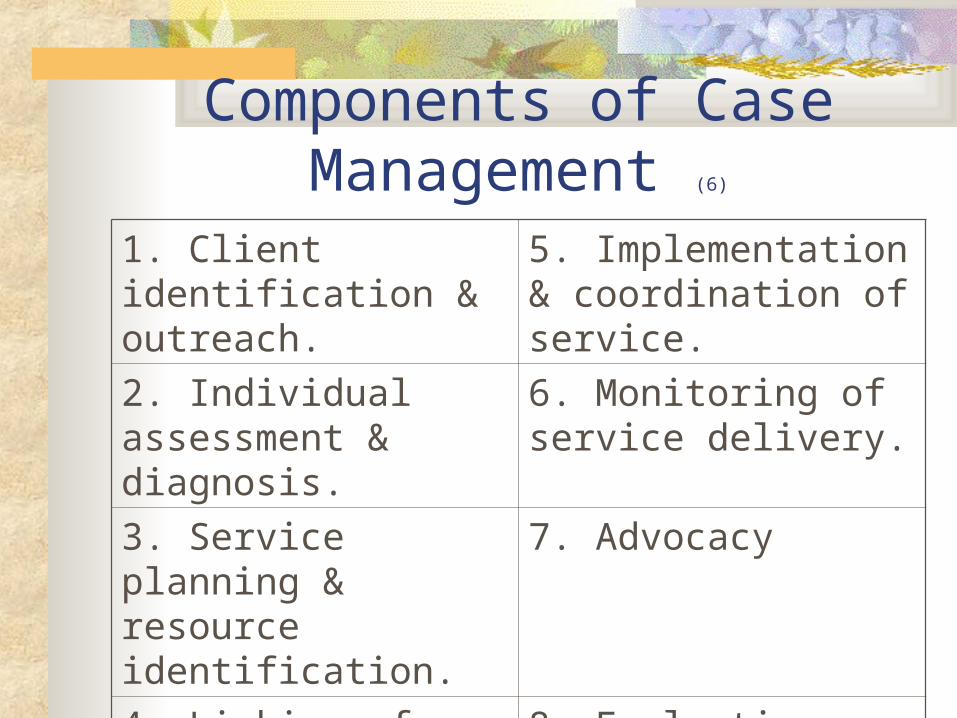
Components of Case Management (6)
1. Client identification & outreach.
5. Implementation & coordination of service.
2. Individual assessment & diagnosis.
6. Monitoring of service delivery.
3. Service planning & resource identification.
7. Advocacy
4. Linking of clients to needed services.
8. Evaluation

Lead Classification Chart The Lead Classification Chart is guidelines
for local health departments or private providers. The chart includes guidelines on assessment, interventions and follow-up, based on the child’s blood lead level.

Lead Classification ChartFinding/ Condition/Need
Assess. Interventions Follow-Up
<10 µg/dL Not considered lead poisoning
Continue to review risk assessment questions at each preventive health visit up to age 6 with routine blood lead testing at 9-12 & 24 months.Parent ed. Pamphlet.
Annual BLL’s once a positive risk factor is identified.Retest at next periodicity visit if risk factor changes.Routine BLL obtained at 1 & 2 & all children 3-6 who have never been screened unless other risk factors are identified.

Lead Classification ChartFinding/
Condition/Need
Assess. Interventions Follow-Up
Class II A
10-14 µg/dL
Level of concern
Parent ed. PamphletContact state CLPPP nurse consultant
Repeat BLL’s every 12-20 weeks until BLL is <10 µg/dLCase Management

Lead Classification ChartFinding/
Condition/Need
Assess. Interventions Follow-Up
Class II B
15-19 µg/dL
1st specimen at this level.
2nd specimen remaining 15-19 µg/dL range
Parent ed. PamphletContact state CLPPP nurse consultantNurse & or local environmentalist may make home visit for visual investigation
Repeat BLL’s every 12 weeks or until level is <10 µg/dLRepeat testing as for first 15-19 µg/dL specimen.Establish a tracking system that assures retesting.Case Management

Lead Classification ChartFinding/
Condition/
Need
Assess Interventions Follow/Up
Class III
20-44 µg/dL
Two capillary specimens or one venous specimen in this range or higher confirms diagnosis of lead poisoning.
First capillary specimen at this level .
First venous specimen or 2nd capillary specimen at this level.
Parent ed. PamphletContact state CLPPP nurse MNTRefer to PCP for MERefer to someone certified to do a risk assess.HV by nurse if confirmed BLL >20
Submit second specimen within one week (if capillary).Repeat blood lead levels at 1-2 month intervals until:
a)BLL is <10µg/dL for 6 months
b)Hazards have been removed and
c)There are no new hazardsCase Management

Lead Classification ChartFinding/
Condition/
Need
Assess Interventions Follow/Up
Class IV
45-69 µg/dL
Two capillary specimens or one venous specimen in this range or higher confirms diagnosis of lead poisoning
Same as Class III except refer for medical evaluation and possible chelation therapy within 48 hours.
Submit the 2nd specimen as soon as possible but no later than 48 hours.
During and post chelation, retest monthly until:
a) BLL is <10 µg/dL for 6 months
b) Hazards have been removed and
c) There are no new hazards
or as ordered by the MD.

Lead Classification ChartFinding/
Condition/
Need
Assess Interventions Follow-Up
Class V
70 µg/dL & above
Two capillary specimens or one venous specimen in this range or higher confirms diag. of lead poisoning.
Same as Class III, except refer for medical evaluation immediately while results of confirmatory test are awaited.
Submit the second specimen as soon as possible but no later than 48 hours.
During and post chelation, retest monthly until:
a) BLL is <10µg/dL for 6 months
b) Hazards have been removed and
c) There are no new hazards
or as ordered by the physician.

Family Teaching Have child tested at appropriate ages Keep home clean, especially floors, window
frames, window sills Keep play areas clean (toys, pacifiers,
bottles) Keep children from chewing on painted
surfaces such as cribs and window sills.

Family Teaching—Cont…. Have children play in grassy areas instead
of soil Have children wash their hands and face
before eating and going to bed Ensure a well-balanced diet high in calcium
and iron and low in fat Clean or remove shoes before entering your
home to avoid tracking in lead from the soil

References1. http://www.dartmouth.edu/toxmetal/TXSHpb.shtml
2. http://www2.sjsu.edu/depts/beethoven/hair/hairtestpc.html
3. http://vocalnow.org/time_line.htm
4. http://www.sueleadindustry.homestead.com/2~ns4.html
5. “Managing Elevated Blood Levels Among Young Children: Recommendations from the Advisory Committee on Childhood Lead Poisoning Prevention” – CDC, 2002

Lead Poisoning Prevention ResourcesState CLPPP nurse: (502) 564-2154
Web Sites: www.epa.gov www.hud.gov www.aeclp.org www.atsdr.cdc.gov