
Geriatric Services - nzhta.chmeds.ac.nz
169
NZHTA REPORT February 2004 Volume 7 Number 3 What is the evidence for the effectiveness of specialist geriatric services in acute, post-acute and sub-acute settings? A critical appraisal of the literature Peter Day Patricia Rasmussen New Zealand Health Technology Assessment Department of Public Health and General Practice Christchurch School of Medicine Christchurch, NZ. Division of Health Sciences, University of Otago
Transcript of Geriatric Services - nzhta.chmeds.ac.nz

NZHTA REPORTFebruary 2004Volume 7 Number 3
What is the evidence for the effectiveness ofspecialist geriatric services in acute, post-acute
and sub-acute settings?
A critical appraisal of the literature
Peter DayPatricia Rasmussen
New ZealandHealth Technology Assessment
Department of Public Health and General PracticeChristchurch School of Medicine
Christchurch, NZ.
Division of Health Sciences, University of Otago

NEW ZEALAND HEALTH TECHNOLOGY ASSESSMENT (NZHTA)
Department of Public Health and General PracticeChristchurch School of Medicine, Christchurch, New Zealand
What is the evidence for theeffectiveness of specialist geriatricservices in acute, post-acute and sub-acute settings?
A critical of the literature
Peter DayPatricia Rasmussen
NZHTA REPORTFebruary 2004 Volume 7 Number 3

This report should be referenced as follows:
Day, P. and Rasmussen, P. What is the evidence for the effectiveness of specialist geriatricservices in acute, post-acute and sub-acute settings? NZHTA Report 2004; 7(3).
2004 New Zealand Health Technology Assessment (NZHTA)
ISBN 1-877235-56-3ISSN 1174-5142


WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
i
ACKNOWLEDGEMENTS
This critical appraisal review was conducted by staff of NZHTA. It was prepared by Mr Peter Day(Research Fellow), who conducted the critical appraisals and along with Dr Ray Kirk (Director)co-ordinated the project. Mrs Patricia Rasmussen (Assistant Research Fellow) provided the descriptivereview section on the key components of published specialist geriatric service protocols and guidelines.Dr Kirk and Mrs Susan Bidwell (Information Specialist Manager) provided comment on the final draft.Mrs Bidwell developed and undertook the search strategy and coordinated retrieval of documents.Miss Becky Mogridge (Library Assistant) and Mrs Philippa Monkman (Library Assistant) assisted withthe retrieval of documents. Mrs Ally Reid (Administrative Secretary) provided document formatting.
The Canterbury Medical Library assisted with the retrieval of articles.
NZHTA is a Research Unit of the University of Otago funded under contract to the Ministry of Health.
This report was commissioned by Ms Pam Fletcher, Senior Analyst, Health of Older People, SectorPolicy Directorate of New Zealand’s Ministry of Health. We also thank Pam for assisting us indeveloping the scope of the review and providing background material for the review.
We also thank Ms Linda Norman and Prof. Gillian Parker of the Nuffield Community Care StudiesUnit, University of Leicester, UK for providing us with a comprehensive working paper version of apublished systematic review on the best place of care (Parker et al. 2000).
This document was externally peer reviewed by Dr Carl Hanger, Consultant Physician, Older PersonsHealth Princess Margaret Hospital, Christchurch and Dr John Scott, Geriatrician, Home and OlderAdults Service, North Shore Hospital, Auckland.
DISCLAIMER
New Zealand Health Technology Assessment (NZHTA) takes great care to ensure the informationsupplied within the project timeframe is accurate, but neither NZHTA, the University of Otago, nor thecontributors involved can accept responsibility for any errors or omissions. The reader should alwaysconsult the original database from which each abstract is derived along with the original articles beforemaking decisions based on a document or abstract. All responsibility for action based on anyinformation in this report rests with the reader. NZHTA and the University of Otago accept no liabilityfor any loss of whatever kind, or damage, arising from reliance in whole or part, by any person,corporate or natural, on the contents of this report. This document is not intended as personal healthadvice. People seeking individual medical advice are referred to their physician. The views expressedin this report are those of NZHTA and do not necessarily represent those of the University of Otago orthe New Zealand Ministry of Health.
COPYRIGHT
This work is copyright. Apart from any use as permitted under the Copyright Act 1994 no part may bereproduced by any process without written permission from New Zealand Health TechnologyAssessment. Requests and inquiries concerning reproduction and rights should be directed to theDirector, New Zealand Health Technology Assessment, Christchurch School of Medicine and HealthSciences, P O Box 4345, Christchurch, New Zealand.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
ii
CONTACT DETAILS
New Zealand Health Technology Assessment (NZHTA)Department of Public Health and General PracticeChristchurch School of Medicine and Health SciencesPO Box 4345ChristchurchNew ZealandTel: +64 3 364 3696 Fax: +64 3 364 3697
Email: [email protected]
Web Site: http://nzhta.chmeds.ac.nz/

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
iii
EXECUTIVE SUMMARY
Objective
To provide the evidence base through the identification and appraisal of the literature on theeffectiveness of specialist geriatric services for developing a sound practice framework. The reviewhad three components, with background and methodology, critical appraisal and write-up of primaryand secondary research work and thirdly, a descriptive outline of key recommendations from publishedspecialist geriatric services protocols, guidelines and specified expert opinion.
Data sources
The literature was searched using the following bibliographic databases: Medline, Embase, CurrentContents, Web of Science and Cinahl. Other electronic and library catalogue sources searchedincluded: Cochrane Library, Database of Abstracts of Reviews of Effectiveness, Health TechnologyAssessment database, UK National Coordinating Centre for Health Technology Assessment, ACPJournal Club database and the TRIP database. A number of Internet websites were also searched toaccess the Scottish Intercollegiate Guidelines Network, US National Guidelines Clearinghouse,Australian Department of Health & Ageing (including subsites & related links), Health Canada(including subsites & related links), UK Department of Health Publications (including subsites &related links), World Health Organisation, various international professional geriatric/gerontologysocieties and organisations. In New Zealand, databases were accessed from the National BibliographicDatabase, Index New Zealand, Ministry of Health website and library, university and medical librarycatalogues and the NZHTA in-house collection, New Zealand Geriatrics Society, Elder CareCanterbury. Relevant publications referenced in material obtained in the course of research on the topicwere also identified. Relevant papers that had cited included papers published from 1980 onwardswere also identified using Science Citation Index.
Searches were limited to English language from 1980 to March 2003.
Selection criteria
Studies were included if they identified key components of specialist geriatric services for older people.The included study population was people aged 65 years and over who have multiple, changing andcomplex morbidities, and who are at risk of functional decline. The outcome of interestincluded functional status, health status, mortality, hospital length of stay, readmissionor first time admission rates, admission to residential care, likelihood of remaining/returning home.The study designs included were systematic reviews, meta-analyses, randomised controlled trials,controlled clinical trials, cohort studies, case-control studies, comparative studies, quasi-experimentalstudies, and descriptive studies.
Excluded studies were studies focusing on long-term residential care without reference to assessmentand rehabilitation, peripatetic condition-specific team services on general wards, studies with fewerthan 50 persons included in reported outcomes, follow-up period of three months or less, and studieswith significant methodological problems. Literature that was narrative reviews, expert opinion, booksand book chapters were excluded from appraisal but were included in the descriptive overview sectionon services guideline and protocols.
Of more than 549 articles identified by the search strategy, 165 articles were retrieved as full text.From these, a final group of 58 primary research papers and nine systematic reviews and meta-analyseswere identified as eligible for appraisal and inclusion in the review. A further 33 articles wereretrieved for the descriptive overview of specialist geriatric service guidelines and protocols of which27 articles were included.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
iv
Data extraction and synthesis
A systematic method of literature searching, selection and appraisal was employed in the preparation ofthis report. Articles were appraised using an adapted schedule of the Cochrane Effective Practice andOrganisation of Care Review Group (EPOC) and in-house checklists developed by NZHTA. Resultswere summarised in evidence tables and studies were classified according to the dimensions ofevidence set out by the National Health and Medical Research Council (NH&MRC). Descriptivesummaries of specialist geriatric service guidelines and protocols were also compiled.
Key results and conclusions
A number of key points arise from the critical appraisal of the eligible literature:
Community care:
� The evidence from this review generally supports the efficacy of specialist geriatric team servicestrained in geriatrics with a multidisciplinary collaborative focus undertaking assessment,rehabilitation and coordinated case management in community settings. Both preventive care andsupportive discharge in these settings appear to provide greater benefit over usual care. However,these benefits were not consistent across all outcomes and although improvement in outcomes wasoften apparent, these were not always significant when compared with the comparison group.
Inpatient care:
� The evidence for the efficacy of specialist geriatric services for inpatient settings was morediverse. This was due to the diversity of studies across the continuum of sub-acute, acute, post-acute care in unit or acute ward settings with resulting heterogeneous outcomes (both in effect andthe particular outcome measured) and only some of these outcomes showing significance overusual care. Specific findings were:
- Integrated comprehensive programmes involving multi-disciplinary care in an acute setting(with follow through from rehabilitation in hospital to rehabilitation in the community) andearly supported discharge programmes should be a part of geriatric hip fracture programmesas these achieved significant benefits over usual care for orthopaedic patients in terms ofreduced length of hospital stay, return to previous residential status and cost-effectiveness.Such outcomes were not apparent for physically distinct orthopaedic rehabilitation units.
- Stroke units with comprehensive acute and rehabilitation care with multidisciplinary teams,patient/carer involvement, comprehensive assessment and management (and dischargeprotocols) and early mobilisation showed significant benefits in terms of mortality reductionand discharge home compared to usual care for acute and sub-acute patients.
- Inpatient comprehensive geriatric assessment (CGA) and rehabilitation programmes showedoverall benefit across a range of settings compared to usual care, especially those programmeswith “medical control” over CGA recommendations with long-term follow-up management.The CGA reported in the literature is similar to the model of assessment, treatment andrehabilitation (AT&R) practiced in New Zealand.
- The overall efficacy of multi-disciplinary specialist geriatric team services in general inpatientgeriatric acute care unit settings (GEU/GEMU) compared to usual care was more inconclusivealthough positive outcomes such as improved functionality, discharge home and reducedhospital length of stay were reported up to the first 12 months post-discharge.
- Multi-component interventions for the prevention of delirium compared with usual preventivecare showed positive overall results with the incidence of delirium and number ofdays/episodes with delirium being significantly lower for the intervention group.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
v
Day hospital and outpatient care:
� Evidence for the efficacy of specialist geriatric services in geriatric day hospitals and outpatientsettings was lacking, with no conclusive evidence that the services in these settings are of greaterbenefit than usual care. Many outpatient studies were in US Veteran Association settings and soof limited applicability to the New Zealand context.
Specialist team service models:
� For patients as well as caregivers, targeted comprehensive services (including training andeducation in addition to assessment and treatment) provided by a multidisciplinary team, tailoredto individual need, appear to be the most effective specialist team service models.
Limitations of research base:
� There were limitations in the current evidence base, particularly problems identifying the mosteffective components of services, identifying important clinical differences in health outcomesbetween intervention and control arms in primary studies, methodological problems affecting theinternal validity of both primary and secondary studies, and a lack of literature set in theNew Zealand context limiting the generalisability of study outcomes to the New Zealandpopulation and health care setting.
� Further research is required to address these limitations, and evaluations of the components ofservice delivery models is required to identify those service features which are most effective interms of outcomes.
Findings from the descriptive analysis of service guidelines, policy and protocols and expert opinion:
� The descriptive analysis of service guidelines, policy and protocols and expert opinion shows aconsensus towards needs-based age-related services with a multi-disciplinary or inter-disciplinaryinterface. The literature described service framework development, systems and processes in asomewhat abstract theoretical manner, rather than descriptions of actual services. It focused onplanning at governance level for such services rather than specific organisational criteria andstrategies for implementation.
A general consensus on the principles of care, service implementation and themes from the literature,identified the following main points:
� a strong focus on functional, social and needs assessment
� need for comprehensive geriatric services across the phases of care whether integrated or separate.A continuum of care model is supported and an identified need for more prevention and screening
� geriatric care requires a high degree of collaborative, multi disciplinary and interdisciplinary carebecause of multi-comorbidities, functional and social impact of illness and polypharmacy
� individualised care where patient, family and carer participation in planning and care managementis maximised and support for carers
� focus on deinstitutionalisation and community and informal care with preference for home andcommunity-based care and avoidance or deferral of admission to acute or long stay hospital care orresidential care
� specialist and comprehensive education in health care of older people is vital but lacking acrossand between all disciplines and services – e.g., old age psychiatry and geriatric services
� need for comprehensive patient management information and monitoring systems and improvedfunding.
WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
vi
There were several key findings common to both the appraisal research and the protocols/guidelinesreviews. These relate directly to the characteristics and design features of most effective services:
� More effective specialist geriatric services are those that:- are comprehensive in their scope, with a multi-faceted approach to assessment, treatment and
management across a continuum of care
- focus on deinstitutionalisation and community and informal care and avoidance or deferral ofadmission to acute or long stay hospital care or residential care.
- are staffed by competent and knowledgeable health professionals trained in geriatric care
- are supported by informed families and communities
- are tailored, flexible and responsive to individual need (culturally appropriate, at home)
- are provided by a multidisciplinary team.
� Another similar finding that relates to the available research base:
- there is material on evidence-based practice research and service evaluation, however this hassignificant limitations. Much of the available evidence does not allow for adequate evaluationof the effectiveness of the different components of service models described in the literature.
Where the evidence reviewed and the descriptive analysis of guideline and protocols differ is that theevidence for the effectiveness of specialist geriatric services in outpatient and geriatric day hospitalsettings compared to usual care was not supported by the published research. This was different fromthe service provisions advocated for all settings in guidelines and protocols, as including those forminority and ethnic groups where in reality there is little research. Research for inpatient settings wasinconclusive at times with outcomes in only some settings showing an overall positive benefit fromthese services. However, more research is required as the current research base in these areas is limitedby study heterogeneity and the inability of studies to detect true differences in outcomes.
In summary, both the evidence base and the body of literature with guideline, protocols and expertopinion generally concur with each other in deriving a “best-practice” framework for geriatricspecialist services. However, gaps and differences remain and further research is required.
WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
vii
TABLE OF CONTENTS
ACKNOWLEDGEMENTS............................................................................................................................... iDISCLAIMER............................................................................................................................................... iCOPYRIGHT................................................................................................................................................ iCONTACT DETAILS ....................................................................................................................................iiEXECUTIVE SUMMARY .............................................................................................................................iiiObjective .................................................................................................................................................iiiData sources............................................................................................................................................iiiSelection criteria .....................................................................................................................................iiiData extraction and synthesis ................................................................................................................. ivKey results and conclusions .................................................................................................................... ivTABLE OF CONTENTS...............................................................................................................................viiLIST OF TABLES........................................................................................................................................ ixLIST OF ABBREVIATIONS AND ACRONYMS................................................................................................. xGLOSSARY ..............................................................................................................................................xiiService type ...........................................................................................................................................xiiiService location ..................................................................................................................................... xivTeam defined ......................................................................................................................................... xiv
SECTION 1 1
BACKGROUND ......................................................................................................................1OBJECTIVE ................................................................................................................................................2REVIEW SCOPE ..........................................................................................................................................2STRUCTURE OF REPORT.............................................................................................................................2
SECTION 2 3
METHODOLOGY ..................................................................................................................3SELECTION CRITERIA.................................................................................................................................3Study inclusion criteria ............................................................................................................................3Study exclusion criteria ............................................................................................................................5SEARCH STRATEGY ...................................................................................................................................5Previous scoping search...........................................................................................................................5Detailed search ........................................................................................................................................6Principal sources of information..............................................................................................................6Search sources..........................................................................................................................................6STUDY SELECTION.....................................................................................................................................7APPRAISAL OF STUDIES .............................................................................................................................7Evidence tables.........................................................................................................................................7APPRAISAL AND LEVELS OF EVIDENCE ......................................................................................................8LEVELS OF EVIDENCE................................................................................................................................8LIMITATIONS OF THE REVIEW....................................................................................................................9
RESULTS ...............................................................................................................................11SUMMARY OF FINDINGS FROM LITERATURE APPRAISAL ..........................................................................11Discussion on Tables 2a-2f: Specialist geriatric services in unit and acute, sub-acute andpost-acute care settings ..........................................................................................................................11Discussion on Table 3: Specialist geriatric services in outpatient settings...........................................15Discussion on Table 4: Specialist geriatric services in day hospital settings .......................................17Discussion on Tables 5a-5b: Specialist geriatric services in community or patient’s home settings ...19PRIMARY AND SECONDARY RESEARCH: STUDY DESIGNS AND QUALITY ..................................................23Study design ...........................................................................................................................................23Study setting ...........................................................................................................................................23Samples ..................................................................................................................................................23

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
viii
Interventions ...........................................................................................................................................24Outcomes ................................................................................................................................................24CRITICAL APPRAISAL DISCUSSION ...........................................................................................................24LIMITATIONS OF THE CURRENT RESEARCH BASE .....................................................................................24DIRECTIONS FOR FUTURE RESEARCH .......................................................................................................25CONCLUSION ...........................................................................................................................................26
SECTION 3 95SPECIALIST GERIATRIC SERVICE GUIDELINE AND PROTOCOL ANALYSIS...................................................95SYNOPSIS.................................................................................................................................................95SEARCH STRATEGY FOR SECTION 3........................................................................................................122Bibliographic databases .......................................................................................................................122Review databases..................................................................................................................................122
REFERENCES.....................................................................................................................125
APPENDIX 1A: SEARCH STRATEGY FOR SECTION 2............................................127SEARCH STRATEGIES .............................................................................................................................127Medline .................................................................................................................................................127Embase .................................................................................................................................................128Cinahl search........................................................................................................................................129Cross database free text search of Cinahl, Embase, Medline, Pre-Medline ........................................130SEARCHES FROM OTHER SOURCES .........................................................................................................130
APPENDIX 1B: SEARCH STRATEGY FOR SECTION 3...........................................131SEARCH STRATEGIES .............................................................................................................................131Medline .................................................................................................................................................131Embase .................................................................................................................................................131Psychinfo ..............................................................................................................................................132Cinahl ...................................................................................................................................................132SEARCHES FROM OTHER SOURCES .........................................................................................................132
APPENDIX 2: INCLUDED STUDIES FOR SECTION 2...............................................133RETRIEVED STUDIES INCLUDED IN REVIEW APPRAISAL..........................................................................133
APPENDIX 3: EXCLUDED STUDIES FROM SECTION 2..........................................139RETRIEVED STUDIES EXCLUDED FOR REVIEW........................................................................................139
APPENDIX 4: INCLUDED STUDIES FOR SECTION 3...............................................147RETRIEVED STUDIES INCLUDED IN REVIEW APPRAISAL..........................................................................147
APPENDIX 5: EXCLUDED STUDIES FROM SECTION 3..........................................149RETRIEVED STUDIES EXCLUDED FOR REVIEW AND REASON FOR EXCLUSION .........................................149

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
ix
LIST OF TABLES
Table 1. Designations of levels of evidence .........................................................................................8Table 2a. Evidence table of specialist geriatric services for inpatient settings – orthopaedic patient
interventions .........................................................................................................................28Table 2b. Evidence table of specialist geriatric services for inpatient settings – stroke patient
intervention...........................................................................................................................32Table 2c. Evidence table of specialist geriatric services for inpatient settings – general geriatric
patients, preventive interventions .........................................................................................34Table 2d. Evidence table of specialist geriatric services for inpatient settings – comprehensive
geriatric assessment ..............................................................................................................39Table 2e. Evidence table of specialist geriatric services for inpatient settings – comprehensive
rehabilitation programme interventions................................................................................42Table 2f. Evidence table of specialist geriatric services for inpatient settings – general geriatric
patients, specialist geriatric unit interventions......................................................................43Table 3. Evidence table of specialist geriatric services in outpatient settings ....................................52Table 4. Evidence table of specialist geriatric services in day hospital settings.................................64Table 5a. Evidence table of specialist geriatric services in community/clients own homes
– preventive services ...........................................................................................................71Table 5b. Evidence table of specialist geriatric services in community/clients own homes
– supported discharge services ............................................................................................83Table 6. Descriptive overview of published specialist geriatric service models and expert
opinion..................................................................................................................................97

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
x
LIST OF ABBREVIATIONS AND ACRONYMS
ACE – accident and emergency department
A&E – accident and emergency department
AGS – American Geriatrics Society
ADL – activities of daily living
AT&R – assessment, treatment and rehabilitation
BAAEM – British Association of Accident and Emergency Medicine
BGS – British Geriatrics Society
CARE – coordination and advocacy for rural elders
GAS – goal attainment scaling
CGA – comprehensive geriatric assessment
CGAT – comprehensive geriatric assessment team
DGH – district general hospitals
ED – emergency department
ESD – early supported discharge
GACS – geriatric ambulatory consultative service
GAT – geriatric assessment team
GAU – geriatric assessment unit
GEM – geriatric evaluation and management
GEU – geriatric evaluation unit
GEMU – geriatric evaluation and management unit
GHFP – geriatric hip fracture programme
GNA – geriatric nurse assessors,
GNP – gerontologic nurse practitioner
GMC – general medical clinic care
GORU – geriatric orthopaedic rehabilitation unit
GP – general practitioner
GQLQ – geriatric quality of life questionnaire
HAPSA – the home assessment program for successful aging
HAS – home assessment service
HHAS – hospital home assessment service
HMO – health management organisation
IADL – instrumental activities of daily living
IDT – interdisciplinary team
IGCS – inpatient geriatrics consultation service
MARU – mixed assessment and rehabilitation unit
MDSHC – minimum data set for home care tool
MDT – multidisciplinary team

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
xi
MGAT – mobile geriatric assessment team
MPS – multipurpose service
MRT – mobile rehabilitation team
NSF – national service framework
OAS – outpatient assessment service
OT – occupational therapist
PAC – post-acute care programme
PACE – Program for All-inclusive Care of the Elderly
PPS – prospective payment system
QoL – quality of life
RCT – randomised controlled trial
RCN – Royal College of Nursing
TAG – technical advisory group
VA – veterans association
VAMC – veterans association medical center
WHO – World Health Organisation

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
xii
GLOSSARY
Acute phase - period during which an illness or injury is being intensively treated and stabilised. Thefocus is on diagnosis and cure or minimising impairment.
Case management - case management, as a process of needs identification and health care servicecoordination and delivery. Includes assessment, implementation and monitoring of health outcomes.
Common geriatric symptom complexes - atypical presentation of disease in older people whereclassical symptoms are masked and patients present with common symptom complexes including:unexplained collapse, dizzy spells, falls, instability, incontinence, delirium and febrile illness causeunknown.
Disability - the resultant limitation in functional capacity from an impairment.
Handicap - the resultant social disadvantage and distress from disability to the individual or society.
New revisions to the terminology of the International Classification of Impairments, Disability andHandicaps (ICIDH-2) introduced by WHO replaces “disability” with “activity limitation” and“handicap” with “participation restriction”.
Impairment - a specific health deficit.
Patient centred care - planning, treatment and management involves patient, family carers andadvocates at all levels and goals are related to patient outcomes.
Post acute and subacute phase - following stabilisation of a disease or injury or intervention tominimise further deterioration in a chronic or progressive condition, the focus is on assessingfunctional ability and establishing a goal-oriented programme (of treatment and rehabilitation) tomaximise functional independence or prevent further limitation. The prime aim is to re-establish theperson successfully in the community where possible. The presence of comorbidities can mean thatolder people can have an acute episode while receiving post acute or subacute care.
Protocols - documented standard practice procedures.
Complex morbidity - means a mix of acute and/or chronic conditions and/or functional impairmentsthat affects more than one domain rather than a single organ system disease or isolated impairment.Examples include:
� two or more conditions which may be acute or chronic – e.g., fractured femur with osteoporosis, ora stroke with urinary incontinence, delirium and osteoarthritis
� chronic or degenerative condition with multiple medication – e.g., neurodegenerative conditionssuch as Parkinsons, Multiple Sclerosis
� dementia
� non-specific presentation/conditions with different symptomatology in older age.
Community geriatric services - assessment and/or rehabilitation provided in a community setting(either the person’s own home, workplace or residential care facility or as part of a community facilitysuch as a day centre or a general practice). When the service is provided in the person’s home, it isgenerally called domiciliary geriatric services.
Rehabilitation clients fall into three broad groups:
� people with an acute catastrophic event, who will need an initial period of rehabilitation and mayor may not need long-term follow-up

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
xiii
� people with a progressive or chronic recurring condition who will need bursts of rehabilitationover a long period (Rehabilitation into the 21st Century. 1997, p 15)
� frail people who have a seemingly “minor” event, who need rehabilitation to maximise theirfunctional abilities and chance of returning home.
About 70 percent of those requiring rehabilitation fall into the older age group, with the majority ofclients having stroke and orthopaedic conditions.
Clients span a continuum in terms of potential for change or improvement between:
� those who will need a brief, intensive burst of services to return to a normal and active life
� those who will remain highly dependent, who may require nursing home care or may be managedat home, but for whom rehabilitation can:
- maintain an optimal level of function and slow the rate of deterioration, or increase theperson’s functional independence, mobility, self-respect and quality of life. (AustralasianFaculty of Rehabilitation Medicine. Rehabilitation into the 21st Century. 1997, p 15)
Service type
Specialist geriatric service - a time-limited service (although not always so – e.g., a “shared-care”model) providing assessment, treatment, management and rehabilitation for older people with multipleor complex medical conditions or disabilities. It may also include mental health conditions for olderpeople if there is no separate psychogeriatric service.
The service links with acute care wards caring for older people, primary health care, community healthservices and disability support services, particularly the needs assessment and service coordinationagencies.
Age related model of service provision - specialist geriatric services for patients above a specifiedage; varies from 65 to 85 years.
Continuing care - long-term placement appropriate to needs – e.g., sheltered accommodation,residential home, nursing home and long-stay care wards.
Culturally appropriate services - services that are delivered in a holistic way that acknowledges andtakes account of the client’s cultural, social and spiritual needs as well as their health and disabilityneeds.
Integrated model of service provision - geriatricians and geriatric care health professionals providespecialist geriatric services in adult care services.
Managed care - MCO managed care organisation, HMO health management organisations: a systemof private budget holding entities where individuals subscribe to managed care organisations whomanage the risk for their health care. The organisation has a global government budget and all of thesubscribers’ health care is funded through them (like Pegasus Health in Christchurch but is muchlarger). MCOs usually fund and provide direct services or contract for provision of services.
Needs related model of service provision - is referral to service based on individual patient needs –e.g., elderly with single pathology illness to general medicine, elderly patients with common symptomcomplexes (see above) or specified conditions to geriatric care.
Rehabilitation services -
� individual rehabilitation assessment, care planning, discharge planning, review and long-termfollow-up
� psychosocial support and counselling for patients and families

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
xiv
� information and education, including preventive education, for patients and families
� community, social and vocational reintegration, including development of alternatives foraccommodation, transport, vocation, recreation and leisure, lifestyles
� advocacy (Australasian Faculty of Rehabilitation Medicine Rehabilitation into the 21st Century.1997, p 22). Note: geriatric services also include treatment.
Service location
The service may be provided in one or more of the following:
� in a dedicated unit for:- assessment, treatment management and rehabilitation- rehabilitation and management
� acute care, assessment, treatment management and rehabilitation
� as part of a generic assessment, treatment and rehabilitation unit
� in beds in a general medical or surgical ward
� geriatric outpatient clinics, including outreach to rural and remote areas
� geriatric day hospital
� community/domiciliary assessment and rehabilitation teams, including outreach to rural andremote areas
� slow stream rehabilitation or step-down services in dedicated facilities (ward or unit attached to thegeneral hospital or stand alone)
� slow stream rehabilitation in a designated unit or beds in residential care facilities.
Team defined
Specialist geriatric team - specialist meaning dedicated team approaches to geriatric care or team careinformed by specialist expertise in physically distinct locations – e.g., AT&R/GAU/GEM units, ACE,ortho-geriatric units, community setting, person’s home.
A specialist geriatric team is an interdisciplinary team of professionals with specific qualificationsand/or expertise in disease processes and injury in older people, and in assessment, treatment,management and rehabilitation for older people. As a minimum, the team consists of a physicianusually with recognised training in geriatric medicine and nurse, but can also include therapists (e.g.,physiotherapist, occupational therapist, speech-language therapist etc), social worker, dietitian,pharmacist and/or psychologist.
Interdisciplinary team -
� works across discipline boundaries towards common clinical goals
� involves the patient, and where appropriate, the family in setting goals and making decisions abouttreatment
� recognises the specialist contribution of each discipline. (Australasian Faculty of RehabilitationMedicine Rehabilitation into the 21st Century. 1997, p 20)
Intermediate care - service interface between provision of primary and secondary care that aims toprovide alternatives to admission or prolonged hospital stay.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
xv
Multidisciplinary team -
� includes a range of disciplines working collaboratively
� team members do not work across discipline boundaries
� tends to have a team hierarchy based on discipline.


WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
1
SECTION 1This section provides background and context for the review on the effectiveness of specialist geriatricservices for older people.
BackgroundMost older people are fit and healthy. A minority are frail and vulnerable and require high levels ofcare and disability support. This is usually as a result of chronic illness or disability that may havebeen present for many years.
Geriatric services include assessment, treatment, rehabilitation and clinical advice/liaison for peopleaged 65 years and over with physical, mental health and/or disability support needs. They are providedby interdisciplinary teams of professionals with specific qualifications and/or expertise in diseaseprocesses and injury in older people and in assessment, treatment and rehabilitation for older people.Members of the interdisciplinary team may include physicians, medical officers of special scale,nurses, physiotherapists, occupational therapists, speech-language therapists, social workers, dietitians,pharmacists and/or psychologists. The main client groups are older people with one or more of thefollowing:
� requiring rehabilitation following admission for an acute episode (e.g., stroke or fractured hip)
� with chronic, complex medical or disability support needs, a number of whom require multiplemedications
� who are frail (at risk of functional decline from even small physiological, psychological orenvironmental changes)
� who have unclear diagnoses, atypical presentation of illness or sudden unexplained decline infunctional abilities.
During the history of the development of geriatric and psychogeriatric services the main client grouphas been Päkeha aged 75 years and over. Smaller population size and higher mortality rates at earlierages has meant that few Mäori or Pacific peoples have accessed either service. A combination ofincreasing longevity and earlier onset of conditions generally associated with ageing is resulting inmore Mäori and Pacific people needing specialist geriatric and psychogeriatric services. Over time, thepopulation aged 65 years and over is expected to become more ethnically diverse as increasingnumbers of people from a variety of European and Asian backgrounds reach older age. There is also asmall, but growing group of people with intellectual disability requiring these services.
Components of specialist geriatric and psychogeriatric services are currently provided in a variety ofsettings including:
� generic or dedicated assessment, treatment and rehabilitation (AT&R) services which may operatein hospital-based units, outpatient clinics, day hospitals and carry out assessments andrehabilitation in people’s own homes
� some acute wards
� private and community-based non-acute rehabilitation services (e.g., Oakland Health in Taurangaprovides intensive intermediate rehabilitative residential and day care for older people and braininjured younger people).
The aim of the review of specialist geriatric services for older people is to provide part of the evidencebase (together with the reviews of psychogeriatric services and management of hospital/community
WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
2
interface) for developing a sound practice service framework for specialist geriatric and psychogeriatricservices that are integrated:
� across mental and physical health and disability support care
� with primary and community health care and other specialist health services.
Overall, the project is divided into three interrelated reviews:
� specialist geriatric services
� psychogeriatric services
� intermediate care (interface between hospital and community-based care).
OBJECTIVE
To identify and appraise international evidence for the effectiveness of specialist geriatric services(acute, post-acute, sub-acute care).
REVIEW SCOPE
Studies were included for review if they reported on specialist geriatric services with a focus onevidence for the effectiveness of service design and delivery outcomes rather than clinical treatmentprotocols, although it is recognised that both have an impact on outcomes for older people. The keycomponents of the service reviewed were assessment, treatment, rehabilitation and clinicaladvice/liaison. This includes links with other related services including primary and community healthcare, disability support services (both home-based and residential care) and hospital-based services.
STRUCTURE OF REPORT
The review on specialist geriatric services is divided into three sections:
� the first section contains a summary overview and general conclusions
� the second section is a critical appraisal and write-up of original primary and secondary researchaddressing the efficacy of specialist geriatric team services on the health and service utilisation forolder people compared to “usual care” services provided by staff or teams:
- who do not have specialist expertise in caring for and treating older people – e.g., a team withno specialised geriatric training, geriatric nurse, geriatrician or
- a condition-specific specialist team which could include a geriatrician but is condition-specific rather than age-specific generic condition focused – e.g., stroke team. It is recognisedthough that this literature may overlap with specialist geriatric services. Some areas have beenwell covered in a number of relevant guidelines including the management of stroke (not justthe 65 years and over group), and the acute management and intermediate rehabilitation afterhip fracture of adults aged over 65 years and are available at the New Zealand GuidelinesGroup web site: www.nzgg.org,nz.
� the third section provides a descriptive outline of the key recommendations from publishedspecialist geriatric service protocols and guidelines and specified expert opinion.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
3
SECTION 2This section provides a critical appraisal of key primary and secondary literature for the review.
MethodologySELECTION CRITERIA
Study inclusion criteria
Publication type
Studies published between 1980 and March, 2003 inclusive in the English language, including primary(original) research (published as full original reports) and secondary research (systematic reviews andmeta-analyses) appearing in the published literature. The restriction to 1980 was used as an initialscoping search found the majority of relevant literature to be published post-1980 and it was also tokeep the project to a manageable size. In the last 20 years, the published literature shows considerablechange and innovation in the patterns of care for older people.
Context
Studies which identify the key components of specialist health services for older people that have themost impact on the outcomes of interest. These include:
� service design features (range of services, location, access and exit criteria, relationship to otherhealth and social support services, degree of integration/coordination with other health anddisability support services for older people)
� staff competencies
Studies that evaluate or describe specialist geriatric services that provide at least one of the following:
� assessment
� treatment and/or management
� rehabilitation.
These may also provide:
� advice to and/or liaison with other health and social support service providers
� information to older people to enable them to make informed choices about treatment and careoptions
� advocacy for older people’s health and social support needs
� discharge/transfer planning.
Study comparators: any of “conventional care”, “usual care” defined as non-specialist geriatricservices, other dedicated team care approaches.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
4
Study population
Study population is people aged 65 years and over with complex morbidities or at risk of deterioratingfunction who:
� require rehabilitation following hospitalisation for an acute episode
� have multiple chronic health conditions or changing disabilities
� are frail (at risk of functional decline from even small physiological, psychological orenvironmental changes)
� have unclear diagnosis, atypical presentation of illness or sudden unexplained decline in functionalabilities.
The most common complex morbidities treated by geriatric services are specified as the followingconditions:
� cardiovascular conditions, particularly stroke
� congestive cardiac failure
� COAD
� falls and syncope
� reduced mobility (generic)
� degenerative arthritis, osteoporosis and associated fragility fractures and orthopaedic conditions
� delirium/confusion.
Outcomes
Studies where outcomes considered include one or more of the following:
� functional status
� health status
� psychosocial wellbeing
� client satisfaction
� cultural appropriateness
� impact on family/whänau carer(s)
� costs (relevant to studies conducted in Commonwealth countries with similarities in healthsystems)
� likelihood of remaining/returning home post intervention
� admission to residential care
� reducing ambulatory sensitive hospitalisation rates
� death
� for hospitalised clients: hospital length of stay.
WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
5
Study design
Peer reviewed studies will be considered for this section of the review if they used one of the followingstudy designs:
� systematic review or meta-analysis design
� clinical controlled trials randomised, quasi-randomised, non-randomised
� analytic studies (cohort and case-control designs)
� quasi-experimental studies (before/after design)
� descriptive studies and descriptive analytic studies (case series, cross-sectional, longitudinaldesigns).
Levels of evidence are based on the notion that experimental study designs minimise or eliminate biasmore effectively than non-experimental designs. However, it is recognised that lower level evidencemay be more useful in their descriptions of specialist geriatric service design and delivery and representthe best available evidence in this area of older persons health.
Note: Any identified unpublished or ‘grey’ literature will be included for New Zealand specific studieswhere this meets selection criteria and other higher-level evidence is unavailable.
Study exclusion criteria
Research papers were excluded if they were:
� studies focusing on long-term residential care without reference to assessment or rehabilitation
� studies in which patients were treated in general wards but visited by peripatetic condition-specificteams
� studies in stroke unit settings
� studies with fewer than 50 persons included in reported outcomes
� studies with a prospective follow-up/evaluation period of less than three months
� studies with inadequate description of methodology and/or results or significant error ormethodological problems
� systematic reviews and meta-analysis with inadequate search methodologies – i.e., use of a singlesearch database
� narrative reviews, expert opinion, letters to the editor, comments, editorials, conferenceproceedings, abstract only, books and book chapters. Such material will not be included in thecritical appraisal section but key material will be included in Section 3 of the review looking atguideline, protocols and specified expert opinion.
SEARCH STRATEGY
A systematic method of literature searching and selection was employed in the preparation of thisreview.
Previous scoping search
A broad scoping search on specialist geriatric services was carried out in December 2002/January 2003using the Medline database only and restricted to a number of study designs. References from thissearch had been seen prior to carrying out the specific search for specialist services in acute, post-acute,and sub-acute settings.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
6
Detailed search
The search was carried out in February/March 2003 for information in English. The search at this stagewas not limited by date but for the reason given earlier was limited from 1980 onwards. The initialscoping search was updated, refined, and expanded to reflect the more detailed nature of the topic.
A search using mostly database index terms was carried out on Medline, Embase, and Cinahlindividually. As a crosscheck, a free text search across all three databases simultaneously was doneincorporating any additional words suggested by the Technical Advisory Group to the project.
Principal sources of information
The following databases were searched (using the search strategy outlined in Appendix 1):
Medline Index terms
Geriatric assessment, geriatrics, health services for the aged, rehabilitation, patient care team, geriatrics,acute disease, hip fractures, femoral neck fractures, rural health services, telemedicine, medicallyunderserved area, rural health, randomized controlled trials, controlled clinical trials, comparativestudy, program evaluation, follow-up studies, meta-analysis, evaluation studies.
Cinahl Index terms
Geriatric assessment, gerontological nurse practitioners, gerontological nursing, geriatric rehabilitation,multidisciplinary care team, femoral fractures, hip fractures, rural health services, rural health,medically underserved area, telemedicine, acute disease, rehabilitation, health services for the aged,gerontologic care, clinical trials, comparative studies, evaluation research, meta-analysis, programevaluation.
Embase Index terms
Geriatrics, hip fracture, telecommunication, rural health care, rural area, elderly care, geriatric care,randomized controlled trial, clinical trial, randomization, meta-analysis, evaluation, evaluation andfollow-up.
The above indexed terms will be adapted for use in sources of information that are not indexed.
Additional free-text keywords (used in all sources)
Orthogeriatric, geriatric$, elder$, older, aged care, aged person$, rural, remote, subacute care, sub-acute care, post-acute care, postacute care, stepdown bed$, geriatric rehabilitation, acute geriatric, dayhospital, hospital adj2 home, home hospital, acute adj2 home, (geriatric or elder or older or aged) adj3(clinic or unit or specialist), (acute care or gp led or general practi$ led or nurse led) adj2 (elder$ orolder or geriatric$), geriatric evaluation, geriatric management.
Search sources
Bibliographic databases
� Medline
� Cinahl
� Embase
� Current Contents
� Web of Science

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
7
� Cochrane Controlled Trials Register
� Index New Zealand
Review databases
� Cochrane Database of Systematic Reviews
� HTA database
� Database of Abstracts of Reviews of Effects (DARE)
� ACP Journal Club
� TRIP database
Other sources
� Scottish Intercollegiate Guidelines Network
� US National Guidelines Clearinghouse
� UK National Coordinating Centre for Health Technology Assessment
� Australian Department of Health & Aging (including subsites & related links)
� Health Canada (including subsites & related links)
� UK Department of Health Publications (including subsites & related links)
� World Health Organisation
STUDY SELECTION
Studies were selected for appraisal using a two-stage process. Initially, the titles and abstracts (whereavailable) identified from the search strategy, were scanned and excluded as appropriate. The full textarticles were retrieved for the remaining studies and these were appraised if they fulfilled the studyselection criteria outlined above.
There were approximately 549 studies identified by the search strategy. Of these 165, full text articleswere obtained after excluding studies from the search titles and abstracts. A further 98 of these full textarticles did not fulfil the inclusion criteria and are presented in Appendix 3. Therefore, 67 articleswere included in the critical appraisal section of this report, and presented in Appendix 2. Other citedpublications (e.g., those providing background material) are presented in the References.
APPRAISAL OF STUDIES
Evidence tables
The Evidence tables for research studies appraised in Section 2 of the review present key informationsummaries as described below:
� Study citation, source and design - including authors, year published, country of origin, studydesign, sample size and characteristics and level of evidence.
� Study location - acute ward, unit (AT&R, GEM, rehab; age, specific or generic), outpatients, dayhospital, out reach clinics (e.g., in drop-in centres, general practice centres, super clinics), clientsown home.
� Within each location - type of staffing, size of operation (number of beds or clients seen), clientgroup (who they include and exclude and why) aims of the service (e.g., increase independence,facilitate discharge), inclusion and exclusion criteria for the study.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
8
� Study interventions - assessment, rehabilitation, training, education, treatment (pharmaceutical),counselling, length of stay (is there a maximum length of stay) and comparator.
� Outcomes - including statistically tested comparisons (statistical precision) of outcomes andreporting of relevant statistical data and authors conclusions.
� Comments and conclusions - including the key study limitations such as internal validity issuesarising from the study appraisal.
Systematic reviews and meta-analyses were described and critiqued in terms of their search strategy,inclusion/exclusion criteria, data synthesis and interpretation.
APPRAISAL AND LEVELS OF EVIDENCE
Articles were formally appraised using an adapted schedule of the Cochrane Effective Practice andOrganisation of Care Review Group (EPOC) of the Cochrane Collaboration and in-house checklistsdeveloped by NZHTA for the appraisal of descriptive studies. Summaries of appraisal results arepresented in both text and tabular form and conclusions drawn from the study design and anylimitations noted.
The evidence presented in the selected research studies is classified using the dimensions of evidencedefined by the National Health and Medical Research Council (NHMRC, 2000). The designations ofthe levels of evidence are shown in Table 1 below.
LEVELS OF EVIDENCE
Levels of evidence were ascribed to each study in relation to their study design, so as to rank them interms of quality according to a pre-determined “evidence hierarchy”. These evidence levels are only abroad indicator of the quality of the research. The levels describe groups of research which are broadlyassociated with particular methodological limitations. These levels are only a general guide to quality,because each study may be designed and/or conducted with particular strengths and weaknesses.
Table 1. Designations of levels of evidence*
Level of evidence Study design
I Evidence obtained from a systematic review of all relevant randomised controlled trials
II Evidence obtained from at least one properly-designed randomised controlled trial
III-1 Evidence obtained from well-designed pseudorandomised controlled trials (alternateallocation or some other method)
III-2 Evidence obtained from comparative studies (including systematic reviews of such studies)with concurrent controls and allocation not randomised, cohort studies, case-controlstudies, or interrupted time series with a control group
III-3 Evidence obtained from comparative studies with historical control, two or more single armstudies, or interrupted time series without a parallel control group
IV Evidence obtained from descriptive studies – e.g., case series, either post-test or pre-test/post-test designs
*Modified from NHMRC (2000)

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
9
LIMITATIONS OF THE REVIEW
This study has used a structured approach to review the literature. However, there were some inherentlimitations with this approach. Namely, critical appraisal reviews are limited by the quality of thestudies included in the review and the review’s methodology.
This review has been limited by the restriction to English language studies. Restriction by languagemay result in study bias, but the direction of this bias cannot be determined. In addition, the review hasbeen limited to the published academic literature, and has not appraised unpublished work. Restrictionto the published literature is likely to lead to bias since the unpublished literature tends to consist ofstudies not identifying a significant result.
The studies were initially selected by examining the abstracts of these articles. Therefore, it is possiblethat some studies were inappropriately excluded prior to examination of the full text article.
All but one of the studies included in this section of the review were conducted outside New Zealand,and therefore, their generalisability to the New Zealand population and context may be limited andneeds to be considered.
This review was confined to an examination of the effectiveness of specialist geriatric services and didnot consider the acceptability, or any ethical, economic (other than healthcare costs in certain settings)or legal considerations associated with these interventions.
The review is based on a qualitative analysis of the appraised literature and is not a comprehensivesystematic review. Rather it is an appraisal and description of key literature. The overall descriptionsare general inferences of the effectiveness of the service delivery models. Only what was availablefrom the appraised papers is reported. The degree of information provided on the service deliverymodels varied considerably and more information may have been available but authors were notcontacted to provide it. There were many similarities across the literature and these are sometimesrepeated points in each of the sections below. More detailed information is available from the evidencetables.
The review is broad and examines literature from across a range of hospital and community settings,with significant heterogeneity in study assessment tools/measures and outcomes and also a wide rangeof interventions and patient populations. Meta-analytic work in this area is limited to only a fewoutcomes such as mortality or survival due to problems with study measurement/outcomeheterogeneity.
A number of conceptual difficulties with undertaking a review in service delivery and organisationwere identified as in other reviews (Parker et al. 2000). These included differing terminology anddescriptions of the stages and models of care in the literature, difficulties with constructing acomprehensive search strategy with non-condition specific searches, and differences in recovery. Mostliterature (through research study design) did not specifically identify what aspect(s) of a servicedelivery model was linked to efficacy and improved outcomes.
Although two researchers appraised/reviewed the articles included in separate sections of this reviewthey did not cross validate the data extraction and appraisal/review process.
The review scope was developed with the assistance of Ministry of Health staff. This review hasgreatly benefited from the advice provided by the Technical Advisory Group (TAG) and the review hasbeen exposed to wider peer review.
This review was conducted over a limited timeframe (February 2003 – July 2003) and (February 2004).Earlier drafts of this review have been used by the Ministry of Health to provide material for the bestpractice framework for integrated specialist geriatric services.
For a detailed description of interventions and evaluation methods, and results of the studies appraised,the reader is referred to the original papers cited.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
10

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
11
Results
SUMMARY OF FINDINGS FROM LITERATURE APPRAISAL
What is the evidence for the efficacy of specialist geriatric services in acute, post-acute and sub-acutesettings? The evidence tables contain comprehensive details of the reviewed studies and readers arereferred there.
Discussion on Tables 2a-2f: Specialist geriatric services in unit and acute, sub-acute and post-acute care settings
� Overall, 25 primary and secondary studies were included in this section. These included foursystematic reviews (three grade 1 and one grade III-2), two meta-analyses (grade 1), one narrativereview (grade IV), 10 RCTs (two grade II and eight grade III-1), four controlled trials (grade III-2),and four descriptive studies (grade IV). Fourteen studies were either set or conducted in the USA,four in the UK, two studies each in Australia and Finland, and one study each in Switzerland,Germany, Norway and Sweden. Follow-up periods for the primary studies ranged from threemonths to three years, with 75 percent of studies having a follow-up period of 12 months or less.
� The outcomes associated with specialist geriatric team interventions for inpatient (acute/unit)settings contain a mixture of outcomes/results because of the heterogeneity of studies compared.Within studies, only some patient outcome measures showed statistically significant differencesbetween the intervention and control groups. Patient outcomes most commonly measured weresurvival, mortality, morbidity, the number of readmissions, hospital bed utilisation, length ofhospital stay, measures of mobility/functionality including ADL, institutionalisation/nursing homeadmissions/stays, destination at discharge, severity/incidence of delirium and direct costs/savings.Hospital admission reductions, improved functional outcomes and reduced nursing homeplacement outcomes were generally more important than reduced mortality.
� The patient samples of the included studies were inpatients with acute/sub-acute illness (includingstroke) or multiple chronic conditions, or in recovery or requiring post-operative rehabilitation, orfunctionally impaired or at risk of functional decline or nursing home placement. Several sub-populations were included; patients with fractures (proximal femoral fracture/hip/lowerlimb/spine/pelvis) requiring rehabilitation, post-discharge patients requiring supported discharge,and patients at high risk of developing delirium.
� For study limitations refer to Tables 2a-2f (pages 28-51) and also the section on limitations withthe current evidence base.
The different interventions and populations covered by the studies in the section are set out as follows:
Orthopaedic patient interventions (Table 2a, pages 28-31)
� Two systematic reviews (Cameron et al. (2000) and Cameron et al. (2003), evidence grade 1)looked at multidisciplinary programmes and geriatric orthopaedic unit/hospital geriatric hipfracture programmes/supported discharge/clinical pathways for older inpatients withproximal femoral fractures/fractures of lower limbs/spine/pelvis. In all 50 studieswere included in these reviews, including 25 RCTs and 10 cohort studies.
The study by Cameron et al. (2003) (with nine RCTs) on multidisciplinary interventions reportedno significant differences in survival, morbidity, mortality and deterioration leading toinstitutionalisation at 12 months follow-up compared with the usual care group. Wide variation inmeasures of length of stay and resulting heterogeneity in outcomes meant results could often notbe compared.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
12
For the study by Cameron et al. (2000), outcomes for various hospital programmes with the aim ofreducing hospital stay and improving the functionality of patients with fractures were compared.The overall conclusions of the authors were that early supported discharge programmes should bea component of geriatric hip fracture programmes to enable suitable patients to return homesooner. GHFP (Geriatric Hip Fracture Programmes involving multi-disciplinary care in an acutesetting with follow through from rehabilitation in hospital to rehabilitation in the community) andESD programmes (early supported discharge) achieved a significant reductions in hospital lengthof stay, higher rates of return to previous residential status, and were more likely to be cost-effective/produce cost saving compared to conventional orthopaedic units. This was not evident orclear for stays in a physically distinct orthopaedic rehabilitation unit (GORU) which is mainlyconcerned with the inpatient rehabilitation phase, separate from acute units. Another conclusionmade was that new physically distinct orthogeriatric rehabilitation units (GORU) should not beestablished until their superiority over mixed assessment and rehabilitation units is clearlydemonstrated. The authors also concluded that acute units managing hip fractures should maintainaccess to unit services for the more disabled. There was weak evidence that clinical pathways maybe advantageous in association with these practice parameters.
Stroke patient interventions (Table 2b, pages 32-33)
� The review by Langhorne et al. (2002) (grade IV) included 11 trials. This looked at stroke unitswith comprehensive acute and rehabilitation care. Although this was not specifically relevant tothe topic, detailed information on the service design and delivery features was provided. Theseunits were shown to produce reductions in mortality, institutional placement and dependency.Units characteristically had multidisciplinary teams of staff with stroke expertise, team goalsetting, some formal patient involvement, and information for patients and carers. Those unitswith acute admissions had comprehensive assessment protocols, management with earlymobilisation – e.g., early physiotherapy, OT, and discharge assessments. The limitation with thisreview was that it was based only on a subset of trials with “positive results” from an earlierCochrane review on stroke units. Trials with “positive results” were those trials demonstrating thesame direction of effect as the Cochrane systematic review on organised (inpatient) stroke unitcare (i.e., reductions in mortality, institutionalisation or dependency). The specific characteristicsof units that did not produce a “positive effect” were not compared.
General inpatient populations (Table 2c, pages 34-38)
Preventive interventions in acute, sub-acute and post-acute settings
� The review by Parker et al. (2000) (grade 1) looked at a wide range of preventiveintervention/models of care compared to usual care in acute wards, hospital, post-acute or sub-acute episodes or rehabilitation. Patients with acute or sub-acute illness were considered. Overall,84 studies from 45 RCTs were included. The main outcomes were that physically distinct strokeunits improve mortality, but this was not evident for hip, or GAU/ACE units. Significantly greaternumbers of patients were returned home from stroke units than other units, which showed littlebenefit over controls. Inpatient rehabilitation (often specialist condition-specific rehabilitation)showed significant reductions in mortality and discharge to home destinations compared to othersettings. Cost data quality was variable with no consensus of results.
� Four other studies (three CTs grade III-2 and one descriptive study all from same original trial,Inouye et al. (1999); Inouye (2000); Rizzo et al. (2001); Bogardus at al. (2003) looked at multi-component interventions for the prevention of delirium compared with usual preventive care.These interventions showed positive overall results with the incidence of delirium and number ofdays/episodes with delirium being significantly lower for the intervention group. There were nosignificant differences in combined costs in the intermediate risk group but higher costs in thehigh-risk group. There were also no differences in other outcomes at six-months follow-up,although incontinence was less common in the intervention group and base-line high-risk patients(poor prognosis) had higher self-rated health and better functional status.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
13
� Two descriptive studies (Weiland et al. (2000) and Eng et al. (1997); all grade IV) reported on theinnovative Program of All Inclusive Care for the Elderly (PACE). Although this particularintervention was not tested in these studies, the approach involved interdisciplinary teamsproviding comprehensive, integrated care as a continuum of care from assessment to supportiveend-of-life care. The programme was designed to limit hospital and nursing home use.
Comprehensive geriatric assessment interventions (Table 2d, pages 39-41)
� The meta-analysis by Stuck et al. (1993) (grade 1) looked at the efficacy of CGA programmesacross a broad range of settings. These included specialist unit (GEMU – a designated inpatientunit for post-acute CGA and rehabilitation), acute ward (inpatient geriatrics consultation service(IGCS) - CGA provided on a consultative basis in non-designated units), home (CGA for home-dwelling older persons), hospital at home (in-home CGA for patients recently discharged fromhospital) and CGA in outpatient settings. Twenty-eight studies were included in the analysis.
Pooled data showed greater proportions of patients living at home at follow-up for all settingscombined. GEMUs, hospital at home and home services at 12-months follow-up had a positiveeffect on living location. GEMU programmes showed reductions in mortality risk at six months.Other settings showed reductions, but positive heterogeneity tests limited the significance of theseresults. CGA in each setting had no significant effect on mortality risk at 12 months. All CGAprogrammes combined (but not individually) reduced hospital readmissions during follow-up.Specialist unit (GEMU) studies showed a significant effect on functionality (measured in half ofthe included studies) at six and 12 months. Characteristics of CGA showing most benefit were“medical control” over CGA recommendations and geriatric evaluation linked with long-termambulatory follow-up. There were limitations with this review, including study heterogeneity,inadequate methodology and study description and limited search. Inpatient unit CGA orpost-acute GEMUs reported in the literature are similar to the model of AT&R practiced inNew Zealand.
� Two RCTs (1 grade II and 1 grade III-1) examined CGA within inpatient settings. One study byReuben et al. (1995) showed no significant differences (even after adjusting for baselinedifferences) at 12 months in survival rates but significant improvements with high implementationrates of recommendations related to rehabilitation. The other RCT by Nikolaus et al. (1999)included inpatient CGA plus post-discharge home interventions. Although this showed asignificant reduction in hospital length of stay and the nursing home placement rate there was nosignificant difference in survival, acute care readmission or new admission to nursing homes.Direct costs were lower for the intervention group.
Comprehensive rehabilitation programme interventions (Table 2e, page 42)
� A second meta-analysis by Evans et al. (1995) (grade 1) with 11 clinical trials, examined multi-disciplinary comprehensive rehabilitation programmes within inpatient settings compared withusual non-intervention medical care. Patients receiving the interventions had significantly highersurvival rates and improved functionality at discharge but this was not evident at follow-up. Theywere also significantly more likely to be returned home. This meta-analysis was limited in view ofprobable study publication bias through a limited search.
Specialist geriatric unit interventions (Table 2f, pages 43-51)
� A systematic review by Scott (1999) (grade III-2) looked at the efficacy of different models ofgeriatric care. This had a limited search strategy and the number and type of studies included wasnot indicated. Acute geriatric care units showed no significant differences in mortality orinstitutionalisation compared to usual care. Post-acute GEM with a rehabilitation focus and long-term follow-up which target patients neither too well or too sick seem to show greatest benefit inoutcomes. Condition-specific interventions targeting geriatric conditions associated withsignificant morbidity and mortality had the greatest promise. Inpatient specialist team servicesshowed a mixture of results. Community-based assessment reported more consistentimprovements in mortality, readmissions and functionality.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
14
� Eight RCTs (one grade II and seven grade III-1) looked at inpatient GEU/GEMU/ACEinterventions compared to usual care. The GEU/GEMU interventions, most with multi-disciplinary teams tended to have reduced mortality, shorter median hospital stays, greaterlikelihood of discharge home, and some improvement in functionality in the first 12 months. Atlonger follow-up periods, these differences were usually not apparent. The study by Applegateet al. (1990) found greater functional improvement and return to community up to six months butnot at 12-months compared to the usual care group. High risk patients showed no differences.Three studies all based on the same trial, evaluated a Geriatric Evaluation Unit (GEU) in a USVeterans Administration medical center (Rubenstein et al. 1984, 1988 and 1995). There wereimprovements up to 12 months in functionality, discharge home and reduced mortality comparedto the control group, however given the setting the study results are of limited applicability to theNew Zealand setting. Another study looking at Geriatric Evaluation and Management Unit(GEMU) providing multi-disciplinary comprehensive assessment compared to usual medical wardcare fond reduced mortality, greater numbers of diagnoses but longer stays for the GEMU service(Saltvedt et al. 2002). Another two studies analysed data from the same trial of a hospital geriatricunit involved in geriatric assessment and rehabilitation. This found that patients in the GEU hadfewer days in health center hospitals but after 12 months there were no differences in cumulativeinstitutionalisation or mortality.
The RCT, by Counsell et al. (2000) (grade III-1) reported on an Acute Care for Elders (ACE) unit.The authors reported no significant differences between the intervention and control groups interms of self-reported measures of functionality, hospital length of stay, costs and hospitalreadmissions. However, there were significantly better implementation rates, patient satisfaction,and less composite ADL decline between discharge and institutionalisation.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
15
Discussion on Table 3: Specialist geriatric services in outpatient settings
� Overall, 11 studies were included in this section, including two studies that reported on data fromthe same trial but for longer follow-up periods. These include 11 RCTs (seven grade II and fourgrade III-1). All of the studies were set in the USA. Trial follow-up periods were eight months(one study), 12 months (six studies) 16 to 18 months (three studies), and two years (one study).Patient populations were mainly non-institutionalised older persons with “chronic” conditions or“unstable” health or at high risk of decline or admission to institutional care. Six of the studieswere in US Veterans Association (often single site) settings with 98 percent plus male patientsamples. Therefore, the generalisability of the outcomes of these Veteran Association studies topopulations in the New Zealand context may be limited. Patients very ill or terminally ill,cognitively impaired and/or institutionalised were mostly excluded from studies.
� Patient outcomes most commonly measured were functionality, hospital readmission, nursinghome admission, survival, mortality, quality of life, cognitive status and mental/social healthissues. The outcomes associated with specialist geriatric team interventions in outpatient settingsshowed a mixture of outcomes/results because of the heterogeneity of studies compared. Withinstudies, only some patient outcome measures showed statistically significant differences betweenthe intervention and control groups. Functional outcomes and patient’s ability to remain in theirown homes weighted together could be considered more important outcomes than just reducedmortality.
� For study limitations refer to Table 3 (pages 52-63) and also the section on limitations with thecurrent evidence base.
Some specific outcomes reported were:
� The systematic review by Stuck et al. (1993) (see Table 2d, pages 39-41 for results) showed thatoutpatient assessment services had no significant effect on institutional placement or mortality andcognitive outcomes compared with usual outpatient care. The systematic review by Scott (1999),(see Table 2f, pages 43-51) reported a mixture of positive and negative outcomes in mortality,unplanned readmissions and functionality for outpatient settings.
� Improvement in many outcome measures (quality of life, mental health, functionality) was evidentfor the study intervention groups but many of these did not show any significant difference whencompared with control groups.
� The length of follow-up of these studies was at least 12 months in all but one study, therefore theresults reflect outcomes with longer follow-up periods than is characteristic in other settings.
� Mortality and/or survival rates generally showed no significant difference between the interventionand control groups.
� It is difficult to correlate the outcomes (efficacy) based on the strength of the evidence grading,follow-up period, and specifics of the service design because of the heterogeneity of study patientgroups and outcomes/results.
� The most common service delivery model consisted of variations of outpatient geriatric evaluationand management (GEM) by multi-disciplinary teams trained in geriatric care. GEM generallyencompassed team history taking, assessment (CGA), physical examination, formulation ofindividual care plans and case management through regular team meeting(s), recommendationsand follow-up for ongoing care by individual team members.
A number of consistent specific service features stand out.
� Specialist teams usually consisted of a minimum of a specialist geriatric nurse, geriatrician, andsocial worker.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
16
� Team-based comprehensive geriatric assessment and evaluation, care planning.
� Coordination with regular care providers was a common feature, also telephone follow-up, patientfamily and caregiver consultation was also done in some studies.
� The control arms of the RCTs received usual outpatient care, or were referred back to primary careproviders, or no description was provided. These controls were “active” in that patients receivednon-intervention outpatient care which provided questionable differences between the careprovided by the intervention. This may be a primary reason why there were fewer significantdifferences in outcomes between the intervention and control groups.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
17
Discussion on Table 4: Specialist geriatric services in day hospital settings
� Overall, seven studies were included in this section of the appraisal. These include one systematicreview (grade 1), four RCTs (one grade II and three grade III-1), one prospective observationalstudy (grade III-2) and one before/after study (grade IV). Two studies each were set in the UK andCanada and one each in Finland, New Zealand and the USA. Trial follow-up periods were threemonths (two studies), 12 months (three studies) and 18 months (one study). Patient populationstended to be older patients 70+ years old referred to day hospital for short-term rehabilitation butalso in several studies for ongoing care of chronic conditions.
� Patient outcomes most commonly measured were functionality, mortality, quality of life andphysical and mental health status. The outcomes associated with specialist geriatric teaminterventions in day hospital settings do not show a clear benefit of these services compared withcontrol group care. There was a mixture of outcomes/results because of the heterogeneity ofstudies compared. Within studies, only some patient outcome measures showed statisticallysignificant difference between the intervention and control groups or in before/after and cohortanalysis. Functional outcomes and physical and mental status weighted together could beconsidered more important outcomes than simply reduced mortality.
� For study limitations refer to Table 4 (pages 64-70) and also the section on limitations with thecurrent evidence base.
Some specific outcomes reported were:
� The Cochrane systematic review (Forster et al. 2002) which included 12 RCTs, reported strongevidence suggesting that day hospitals have no great benefit in terms of outcomes than othersimilar comprehensive or domiciliary care. However, some benefit was apparent when comparedto groups receiving no comprehensive care. Day hospital attendance was more expensive butshowed reductions in bed use and institutional placement compared with other care. Althoughdescriptions of “usual care” were not provided this did not mean no care.
� The Cochrane review was limited in that specific specialist service delivery descriptions were notprovided other than stating that day hospitals were general medical hospitals providingrehabilitation services for part or full days. There may be some limitations in the applicability ofthis review. Three studies included in this review were included in the appraised literature asexamples of specialist geriatric services in these settings.
� The systematic review by Parker et al. (2000) (see Table 2c, pages 34-38 for results) examiningfour studies showed no benefit of geriatric day hospitals in terms of mortality reduction. Thesystematic review by Scott (1999) (see Table 2f, pages 43-51) examined four studies which alsoshowed geriatric day hospitals to have minimal impact on mortality and other outcomes.
� It is difficult to correlate the outcomes (efficacy) based on the strength of the evidence grading,follow-up period, and specifics of the service design because of the heterogeneity of study patientgroups and outcomes/results.
� The most common service delivery model consisted of slight variants of day hospital care bymulti-disciplinary specialist teams trained in geriatric care. The type of care was primarilyinterdisciplinary team assessment and short-term rehabilitation. Three studies also indicatedongoing medical care and management of complex chronic conditions including the formulation ofindividual care plans through team meeting(s) and recommendations for ongoing care.
A number of consistent specific service features stand out.
� Specialist teams usually consisted of a minimum of a specialist nurse, geriatrician, and were wellrepresented with rehabilitative personnel including OTs, physiotherapists, and speech therapists.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
18
� The focus of care was on interdisciplinary team assessment and short-term rehabilitation.
� Reported day hospital bed size was 10 beds (3 studies) and 25 beds (one study).
� The control arms of the RCTs and comparative studies received usual or normal discharge care.Detailed descriptions of this care were not usually provided which did not mean no care. Thesecontrols were “active” in that patients received non-intervention care which at times providedquestionable differences between the care provided by the intervention. This may be an importantreason why there were fewer significant differences in outcomes between the intervention andcontrol groups.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
19
Discussion on Tables 5a-5b: Specialist geriatric services in community or patient’shome settings
� Overall, 22 studies were included in this section. These included two systematic reviews (grade1), 12 RCTs (five grade II and seven grade III-1), two controlled trials (grade III-2) and six othertypes of studies (all grade IV) which were one before/after study, one prospective observationalstudy, one retrospective study with comparison group and three descriptive studies. Nine studieswere set in the USA, two each in Switzerland, Italy, Denmark, Canada and Australia and one eachin Sweden and Hong Kong. Trial follow-up periods were six months or less (seven studies), 12months (ten studies), 20 months (1 study) and three years (three studies). Patient populations werepeople with a wide range of geriatric conditions that were living at home and possibly receivinghome-care, or had been recently discharged from hospital care and were at risk of functionaldecline and/or readmission to hospital. The seriously ill and cognitively impaired were mostlyexcluded. The type of care provided by these services was either preventive care (12 studies) orsupported discharge care (10 studies).
� Patient outcomes most commonly measured were functionality, hospital readmission, nursinghome admission, mortality, quality of life and identification of medical/social/psychologicalproblems. The outcomes associated with specialist geriatric team interventions (includingmobile/outreach services) in community/home settings show a mixture of outcomes/resultsbecause of the heterogeneity of studies compared. Within studies, only some patient outcomemeasures showed statistically significant differences between the intervention and control groups.Functional outcomes and patient’s ability to remain in their own homes were considered moreimportant outcomes than reduced mortality.
� For study limitations refer to Tables 5a-5b (pages 71-93) and also the section on limitations withthe current evidence base.
Preventive community/in-home care
� Preventive in-home services included 12 studies comprising one systematic review (grade I), sixRCTs (three grade II and three grade III-1), one controlled trial (grade III-2), three descriptivestudies and one before and after study (all grade IV). The populations included in these studieswere community-dwelling older persons and in several studies subjects were receiving in-homecare. Refer to Table 5a (pages 71-82).
Some specific outcomes reported were:
� One systematic review (Stuck et al. 2002) included 18 RCTs, although only about one-quarter ofthe studies indicated that the preventive intervention was delivered by a “specialist geriatric team”.Three of these studies were separately included in the appraised literature. Other studies reportednurse-led interventions. Only one-third of studies had “multidimensional” geriatric assessment andfollow-up. Therefore, this should be kept in mind in terms of the applicability of results. Theinterventions were preventive in-home multidimensional CGA and follow-up. There were onlysmall reductions in nursing home admissions and mortality, and improvement in functional status.However, the frequency of follow-up visits (>5 visits) and CGA related to improved outcomes.Study heterogeneity was a reported problem.
� The meta-analysis by Stuck et al. (1993) included CGA programmes for home-assessment services(including hospital at home). These interventions had a significant effect with people living athome in reducing institutionalisation and mortality at 12 and 36 months. Two studies showedsignificant reductions in admissions but no effect on other outcomes. Community and home-basedGEM services in the systematic review by Scott (1999) showed positive results for carefullyselected patients with specific conditions compared to patients with non-specific conditions.Combined nursing and rehabilitation may not be effective from the studies reviewed.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
20
� Overall, the included primary studies generally showed an improvement in functionality, reductionin nursing home admission, greater likelihood of remaining at home, reduction in the number offalls and reduction in health care usage such as hospitalisation but often did not show anysignificant difference between the intervention and control groups.
� One consistent finding was that patient groups receiving CGA had a significantly greater numberof new (medical etc) problems identified compared to control groups.
� Improvement in functionality measures (ADL and IADL) was evident for the study interventiongroups sometimes showing a significant difference between the intervention and control groups.
� One study (Hui & Woo 2002) looked at tele-medicine with video conferencing between thespecialist team and patients in a nursing home. The focus was on new problem identification andface to face consults were performed when necessary. Overall, the feasibility of these electronicconsults ranged from 60 to 99 percent dependent upon the discipline of the consultant.
� It was difficult to correlate the outcomes (efficacy) based on the strength of the evidence grading,follow-up periods, and specifics of the service design because of the heterogeneity of study patientgroups and outcomes/results.
� The most common service delivery model in preventive in-home schemes consisted of slightvariants of in-home comprehensive (multi-dimensional) geriatric assessment (CGA) by multi-disciplinary teams trained in geriatric care (including mobile/outreach teams). CGA with casemanagement often by a specialist geriatric nurse, the formulation of individual care plans at teammeeting(s), recommendations for ongoing preventive care, frequent follow-up in-home visits byvarious team members (dependent on patient need) for implementation of plan recommendationsto patients and consultation with patient primary-care provider for approval of care plans.
A number of consistent specific service features stand out.
� Written communication between the specialist team and patient’s primary medical practitioner ofteam recommendations initially and during on-going care.
� Specialist teams usually consisted of a minimum of a specialist nurse, geriatrician, OT,physiotherapist and, less commonly, a social worker.
� The focus of the CGA was on new problem identification.
� Interventions were preventive care schemes for community-dwelling older persons some of whomwere already receiving home-care and had a range of geriatric conditions.
� Follow-up patient visits were a blend of health education/promotion/reinforcement of teamrecommendations.
� Specialist geriatric nurses often performed CGAs. Follow-up visits by team members were multi-disciplinary.
� The control arms of the RCTs and comparative studies received usual or normal preventive in-home care which ranged from a telephone call to routine medical care to ad-hoc coordination ofhome-care services. Detailed descriptions of this care were not usually provided. It was oftendifficult to ascertain what care was received and whether or not contamination between the twogroups occurred which could mean questionable differences between the care provided by theintervention. This may be a primary reason why there were fewer significant differences inoutcomes between the intervention and control groups.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
21
Supported discharge for community/in-home care
� Supported discharge in-home services included 10 studies comprising one systematic review(grade 1), six RCTs (two grade II and four grade III-1), two comparative studies and oneprospective observational study (all grade IV). The populations included in these studies wereolder patients recently discharged home (including nursing homes for respite care) from hospitalcare (acute, sub-acute care) who were deemed “unstable”, at risk of further decline and havingchronic but potentially reversible geriatric conditions. Refer to Table 5b (pages 83-93).
Some specific outcomes reported were:
� The systematic review by Hyde et al. (2000) included nine RCTs and looked at supporteddischarge services following acute admission to hospital compared to non-supported discharge.Supported discharge schemes showed no significant difference in mortality rates (9 trials) but moreimportantly a beneficial effect in terms of numbers not requiring institutionalisation at six to 12months (7 trials) and a greater number of patients staying at home at six months (4 trials). Severaloutcomes showed considerable variation – e.g., hospitalisation and functional status measuresreported mixed results and could not be combined for an overall assessment.
� The systematic review by Parker et al. (2000) (see Table 2c, pages 34-38 for results) also lookedat five studies on community-based rehabilitation which showed no difference in terms ofmortality compared with usual care. The systematic review by Scott (1999) (see Table 2f,pages 43-51 for results) reported that specific-condition targeted home/community GEMinterventions appeared to show the greatest benefits and that community-based assessmentreported more consistent improvements in readmissions, functionality and mortality.
� Overall, included primary studies generally showed an improvement in terms of fewer hospitalreadmissions, quality of life in the short-term, and an increase in the use of medical services.However, these results show both significant and non-significant differences between theintervention and control groups, making it difficult to gauge the overall efficacy of such schemes.
� Measures of functionally were similar and showed no significant difference between theintervention and control groups.
� One consistent finding was that patient groups receiving CGA as a part of supported discharge hada significantly greater number of problems identified compared to control groups.
� As with preventive in-home services it was difficult to correlate the outcomes (efficacy) based onthe strength of the evidence grading, follow-up periods, and specifics of the service design becauseof the heterogeneity of study patient groups and outcomes/results.
� The most common service delivery model of in-home supported discharge schemes consisted ofvariants of in-home comprehensive geriatric assessment (CGA) either shortly before or afterdischarge with a needs-based focus looking at functionality and medical and social servicerequirements. This was performed by a multi-disciplinary team trained in geriatric care. Theregimen of care consisted of CGA and coordinated case management, often by a specialist geriatricnurse coordinator, the formulation of individual care plans at team meeting(s), recommendationsfor ongoing care, and varying intensity of follow-up in-home visits by various team members(dependent on patient problems). Team recommendations were communicated to primary careproviders for approval.
A number of consistent specific service features stand out.
� Communication by supported discharge team (including approval requests) of teamrecommendations with patient primary medical practitioner and continued communication duringongoing care.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
22
� Specialist teams usually consisted of a minimum of a specialist nurse, geriatrician, OT,physiotherapist and less commonly a social worker.
� The focus of the CGA often performed by specialist geriatric nurses, was on problem/needsidentification.
� Interventions were targeted in-home supported discharge schemes for community-dwelling olderpersons recently discharged from hospital. Follow-up visits by team members were multi-disciplinary and were generally governed by patient needs.
� Patient follow-up varied in frequency and visits were a blend of health consultations, education,promotion, and reinforcement of team recommendations.
� The control arms of the RCTs and comparative studies received usual or normal discharge care.Detailed descriptions of this care were not usually provided. These controls were “active” in thatpatient’s received non-intervention care. It was difficult to ascertain often what care was receivedand whether or not contamination between the two groups occurred which could meanquestionable differences between the care provided by the intervention. This may be a primaryreason why there were fewer significant differences in outcomes between the intervention andcontrol groups.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
23
PRIMARY AND SECONDARY RESEARCH: STUDY DESIGNS ANDQUALITY
The search identified 67 primary and secondary studies for inclusion in the evidence tables. Below is asummary of the study design, setting, sample, intervention and outcome characteristics of this material.
Study design
Overall the majority (73%) of included studies were of higher evidence quality and were systematicreviews, meta-analyses, or RCTs. All but one systematic review/meta-analysis was graded as level 1evidence according to the NH&MRC evidence hierarchy. Approximately half of the 40 included RCTswere graded as level II evidence and the other half level III-1. Eleven of the included studies weredescriptive/quasi-experimental or narrative reviews and were graded as level IV. Other studiesincluded five controlled trials and two cohort/comparison studies (all level III-2). Most of thesystematic review and meta-analysis literature was of geriatric specialist services in unit and acute wardsettings (Tables 2a-2f, pages 28-51). RCTs were the most predominant study design across all servicedelivery settings.
Study setting
Various service delivery settings were included in the appraised literature. These included hospitalinpatient settings either as acute wards, distinct specialist units or general wards. There were alsogeriatric day hospitals and outpatient settings including hospital, medical clinic, ambulatory andemergency department settings. US Veteran Administration health care settings were common in theoutpatient literature. Community-based settings included patients’ own homes, nursing homes andoutreach services to these settings. The most common countries in which a study was set or secondaryresearch conducted were USA (37/67 studies), United Kingdom (6/67 studies), Australia and Canada (4studies each) and Finland and Switzerland (3 studies each).
Samples
Study samples ranged from 55 years upwards, most commonly being 65 years plus. The most commonmean age of study samples was over 75 years of age. The proportion of male patients in study samplesranged from 22 percent to 98 percent. The latter high proportion of males was attributable to USVeteran Association health care settings. Many of the US studies also had patient samples that weremembers of Health maintenance Organisations (HMOs). Over 70 percent of the included samples hadfewer than 500 patients enrolled at the beginning of the study. Often the recruitment populationscreened before inclusion in a particular study was considerably larger but due to exclusions andunwillingness to participate only a small proportion of potentially eligible patients were finally enrolledin the study.
Patients included in the studies were mostly of a diverse case-mix. They often had multiple chronicconditions or were in post-acute recovery requiring comprehensive assessment, rehabilitation, andtherapy through hospitalisation, outpatient care and/or preventive community care or supporteddischarge. Patients were commonly described as being “at risk”, having “probable” deterioration, atrisk of readmission to hospital, having instability in their health status, or having potentially reversibleconditions. Specific conditions such as hip or lower limb fracture were addressed in a number ofsystematic reviews. Common reasons for patient exclusion from study samples were terminal illness,palliative care, short hospital stay (< 2 days), severe dementia or other cognitive difficulties,psychological diagnoses, pending nursing home placement and having less than six months to live.The notion of recruiting patients neither too healthy nor too sick for study patient samples and howwell this was achieved had a significant influence on the efficacy of geriatric service interventionsmeasured through the outcomes of interest.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
24
Interventions
The interventions of interest were those implemented by specialist geriatric team services. These werevaried and included comprehensive geriatric team assessment, evaluation, treatment, case management,rehabilitation, carer and patient education, discharge planning, in-home care with post-discharge andpreventive care. The framework of services was often a continuum of care across various stages.Interventions were often structured with programmes involving multi-disciplinary teams, carecoordination, and patient-centred care. These interventions were compared (where experimental studydesigns were used) with patient groups receiving “usual” or “standard” care as controls. The literaturedid not often describe the type of care planned for the control group, making it difficult to determinewhat actual care they received. It was also difficult to determine what particular part of an interventionwithin a broader service framework had been instrumental in achieving successful outcomes.
Outcomes
A wide range of outcome measures was used to assess the efficacy of specialist geriatric services in theappraised studies. The sources of this data included hospital inpatient records, primary practitionerrecords, and assessment tools and questionnaires including psychological, functionality, quality of life,service usage and health status scales, both self and investigator administered. Many of the assessmenttools used were referenced from the literature and the validity and reliability of some was also specifiedin the study methods section. Different variations of similar assessment scales were commonly used –e.g., the activities of daily living index (ADL) or instrumental activities of daily living index (IADL).The diversity of outcome measures used was a problem in meta-analytic research in this area as it wasnot often possible to combine studies in a quantitative way, other than for the most common ofoutcome measures such as mortality, survival and the number of readmissions etc. Qualitative researchand evaluation was equally problematic because of the variation in outcome measures.
Outcome data included mortality, survival, time to institutionalisation, health servicescosts/expenditure, length of hospital stay, number of readmissions, destination at discharge, dischargehome, and nursing home admission/placement/transfer. Measures of functionality, quality of life,patient/carer satisfaction, health status, cognitive functioning, numbers of and duration between fallsand assessments of the number of new diagnoses, changes in medications, and further diagnostictesting were also used. Outcomes such as re-admissions, functionality, discharge, returning home,institutionalisation etc were considered to be of greater importance for older people than reductions inmortality.
CRITICAL APPRAISAL DISCUSSION
Limitations to the current research database, directions for future research and conclusions.
LIMITATIONS OF THE CURRENT RESEARCH BASE
The evidence considered in this critical appraisal exhibited methodological limitations, there was asimilarity of these limitations across all settings and are also identified in other literature reviews on thesubject (Alexander (1990); Rubenstein et al. (1991); Borok et al. (1994); Boult et al. (1998); Wieland etal. (1995); Wieland et al. (1996)). These limitations are summarised below:
� There were problems identifying true and important clinical differences in health outcomesbetween specialist geriatric service interventions and control arms in primary studies. This was inlarge part due to small sample sizes and contamination between groups as at times patients fromboth groups received similar assessments and treatments from the same physicians. Differentlevels of care were reported for control/comparison groups ranging from “usual” care to“enhanced” usual care making differences between the two patient groups subtle in some cases.
� Methodological limitations of primary studies included patient selection bias from age-relatedpatient selection (rather than targeted), single or homogenous site study settings, variable sampleswith multiple conditions, and unbalanced patient sample gender – e.g., US Veteran Affairs setting

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
25
studies. Commonly, huge numbers of patients had to be screened before enough study participantscould be recruited. There were differences in the timing of interventions across studies – e.g., atadmission versus post-acute care etc. There were varied assessment approaches and processes andspecialist teams ranging from a basic core to expanded multi-disciplinary team. There werevariable patient lengths of hospital stay and follow-up intervals and a large range of assessmenttools/outcome measures. Different assessment tools measured the same outcome and a wide rangeof outcomes made study comparability difficult. Although these were often referenced, anindication of the validity and reliability of few assessment tools was specified. There were fewreplications of intervention packages only longer follow-ups or secondary or economic outcomesfrom existing trials. Often it was not clear whether or not results were based on an intention totreat analysis and losses to follow-up were considerable in a number of studies.
� Other limitations included a lack of literature in New Zealand settings. Only one included studywas set in New Zealand and four in Australia. A limitation in the generalisability of the results ofthe review to the New Zealand context and population is therefore a real issue. Also, there waslittle relevant data in studies on cost effectiveness and the cost of care. There was a lack ofliterature specifically inclusive of staff education within multi-disciplinary specialist team servicesettings. There was a severe lack of studies on interventions for and the needs of older personsbased on ethnicity, race, SES and education level. No studies were identified which addressedthese issues for Maori and other groups in the New Zealand context.
� For secondary research (e.g., systematic reviews and meta-analyses), common limitations includedsignificant heterogeneity among the included studies at different analysis levels, with differentstudy populations (some compared samples of frail older people with those from the generalpopulation, while others included only frail or only those at risk for functional decline), differentstudy designs, variations in the follow-up period, different intervention and outcome measures.There was considerable heterogeneity in the outcomes reported between studies as well as indifferences in the way same outcomes were reported by these studies. The included studies variedin the intensity and nature of the interventions tested as well as the outcomes assessed. Meta-analysis (pooled analysis) was sometimes not able to be carried out because consistent quantitativeinformation was not available. Very few outcomes were analysed in this way – e.g., mortality,survival. Other limitations included services provided by a range of different staffratios/modalities, including multidisciplinary teams, single-person services and services deliveredover the telephone. Studies also described a range of service models, which were not easilyclassified into specific intervention types. There was overlap in terms of included secondaryresearch containing the same studies in their analysis.
DIRECTIONS FOR FUTURE RESEARCH
Further research should address the limitations of the current research base demonstrated in this review.Further studies across all settings with improved designs – e.g., multi-center RCTs and methodologieswill be important in detecting important clinical differences in health outcomes from serviceframework interventions and improve evidence-based practice. Evaluations of the components ofCGA, GEM, home-based interventions etc are needed to identify what features of these services aremost effective on positive patient outcomes. Research using targeted interventions with improvedquality and validity of assessment processes is required. Research into transitional care models whichprovide an underlying framework in the continuum of care as patients transfer between one level/typeof care and another is required to ensure patient needs are met (Naylor, 2002). More research isneeded, particularly in New Zealand because models that provide interventions across specialistgeriatric services have not been adequately evaluated. Further research to explore the issue of cross-national comparability of studies between different healthcare systems is required. Health systems andmodels of care have undergone significant changes in the past 30 years and the quality of the evidencebase has been constantly evolving as new empirical research attempts to keep pace with these changes.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
26
CONCLUSION
A number of important findings arise from the from the critical appraisal of the literature:
Community care:
� The literature evidence from this review generally supports the efficacy of specialist geriatric teamservices, trained in geriatrics with a multidisciplinary collaborative focus undertaking assessment,rehabilitation, and coordinated case management in community settings. Both preventive care andsupportive discharge in these settings appear to provide greater benefit over usual care. However,these benefits were not consistent across all outcomes measured and although improvement inoutcomes was often apparent, these were not always significant when compared with thecomparison group.
Inpatient care:
� The evidence from the literature appraisal for the efficacy of specialist geriatric services withininpatient settings was more diverse. This was because of the diversity of studies across thecontinuum of sub-acute, acute, post-acute care in unit or acute ward settings. This resulted inheterogeneous outcomes (both in effect and the particular outcome measured) with only someoutcomes showing significance compared with usual care. Specific findings were:
- Integrated comprehensive programmes involving multi-disciplinary care in an acute setting(with follow through from rehabilitation in hospital to rehabilitation in the community) andearly supported discharge programmes should be a part of geriatric hip fracture programmesas these achieved significant benefits over usual care for orthopaedic patients in terms ofreduced length of hospital stay, return to previous residential status and cost-effectiveness.Such outcomes were not apparent for physically distinct orthopaedic rehabilitation units.
- Stroke units with comprehensive acute and rehabilitation care with multidisciplinary teams,patient/carer involvement, comprehensive assessment and management (and dischargeprotocols) and early mobilisation showed significant benefits in terms of mortality reductionand discharge home compared to usual care for acute and sub-acute patients.
- Inpatient comprehensive geriatric assessment (CGA) and rehabilitation programmes showedoverall benefit across a range of settings compared to usual care, especially those programmeswith “medical control” over CGA recommendations with long-term follow-up management.The CGA reported in the literature is similar to the model of assessment, treatment andrehabilitation (AT&R) practiced in New Zealand.
- The overall efficacy of multi-disciplinary specialist geriatric team services in general inpatientgeriatric acute care unit settings (GEU/GEMU) compared to usual care was more inconclusivealthough positive outcomes such as improved functionality, discharge home and reducedhospital length of stay were reported up to the first 12 months post-discharge.
- Multi-component interventions for the prevention of delirium compared with usual preventivecare showed positive overall results with the incidence of delirium and number ofdays/episodes with delirium being significantly lower for the intervention group.
Day hospital and outpatient care:
� The evidence for the efficacy of specialist geriatric services in geriatric day hospitals andoutpatient settings was insufficient, with no conclusive evidence that the services in these settingsare of greater benefit than usual care. Many outpatient settings were US Veteran Associationhospitals and clinics and so of limited applicability to the New Zealand context.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
27
Specialist team service models:
� The most effective specialist team service models for patients (and caregivers) appear to betargeted comprehensive services tailored to individual need (including training and education inaddition to assessment and treatment) provided by a multidisciplinary team.
Limitations of research base:
� There were limitations in the current evidence base, particularly problems identifying the mosteffective components of services, identifying important clinical differences in health outcomesbetween the intervention and control arms in primary studies, methodological problems affectingthe internal validity of both primary and secondary studies, and a lack of literature in theNew Zealand context, thereby limiting the generalisability of the studies to the New Zealandpopulation and health care setting.
� There is a need for further research designed to address these limitations, providing evaluations ofthe components of service delivery models to better identify those service features which are mosteffective in terms of outcomes.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
28
Table 2a. Evidence table of specialist geriatric services for inpatient settings – orthopaedic patient interventions
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Cameron et al. (2003)
Cochrane,Systematic Review
Australia
Grade: Level I
Nine RCTs with 1,869 patients were included,mean age range 78 to 82 years for interventiongroup and 78 to 85 years for control group.
Searched from the Cochrane MusculoskeletalInjuries group register as at December 2001,MEDLINE 1966 to December 2001, referencesfrom books and articles, experts in the field.
Inclusion criteriaRCTs and quasi-RCTs of post-surgical care withspecialised rehabilitation of hip fracture (of theproximal femur) patients aged 65 plus years.
Exclusion criteriaNone specified.
Service and study descriptionThe intervention of interest was treatment in ageriatric-orthopaedic rehabilitation unit (GORU) orother types of specialised multi-disciplinary inpatientunits compared with usual orthopaedic care inorthopaedic wards or rehabilitation in a communityhospital (control group).
The description of the intervention varied in the nineincluded trials.Five trials were based on rehab services in a GORU ina hospital or hospital away from where theorthopaedic department. Combined ward roundswith geriatricians and orthopaedic surgeons andmultidisciplinary case conferences. Control groupshere received usual care provided by orthopaedicteams and had access to allied health staff andconsultant geriatricians if required.
In two trials the intervention was intensive rehabprogrammes and the control groups here receivedusual hospital rehab. These trials had earlyassessment by a rehab physician or geriatrician,focusing on developing physical independence anddischarge planning. One of these trials also involvedearly surgery and anaesthesia. The interventions herewere for hip fracture patients care was provided inMARU (mixed assessment and rehab unit) in one trialhere and several other trials.
One other trial evaluated the effects of assessmentby a nurse form a “Geriatric Functional Unit”, with adiscussion by the geriatric team to develop amanagement plan and implementation monitoredby the unit with an emphasis on co-morbiditytreatment with optional physiotherapy in themanagement plan. Both groups shared the samewards and were managed by orthopaedic teams.
One trial compared multidisciplinary intensive rehabin a geriatric ward, detailed discharge planning andhome follow-up by multidsiciplinary team in the samehospital where surgery had occurred with communityhospitals with GP supervision.
Multidisciplinary approaches forinpatient rehab for older peoplewith proximal femoral fracturescompared with usual care.� there was no significant
difference in survival to end offollow-up compared with usualcare group (9 studies)
� aside from one study all othersreported no significantdifferences between groups interms of morbidity
� there was considerablevariation in the length of stay,which included the initialtreatment and rehab stay. Thelengths of stay wereconsiderably longer in controlsof 4 studies, shorter in 3 andsimilar in 1. As a result ofsignificant heterogeneity nodefinite conclusions could bemade. Readmissions werereported in 4 trials, with 3 trialsreported greater admissions ofintervention group patients
� there was a wide variation ofmeasures of mobility; thereforethese indices were unable to becompared. Only 1 studyreported improvement atdischarge and follow-up, andanother at discharge only
� there was no significantdifference between groups indeath at 12 months ordeterioration leading toinstitutionalisation (9 studies).Testing for different definitions ofoutcomes did not alter theresults, nor by type ofintervention.
� Cochrane Systematicreview
� the method ofrandomisation wasdescribed in all but onetrial. Also only one trialhad blinding ofoutcome assessors.There was somevariation in the time ofrandomisation in studies
� the Comparison(control) groups wereall ‘active’ receivingalternative inpatientcare in all studies.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
29
Table 2a. Evidence table of specialist geriatric services for inpatient settings – orthopaedic patient interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Cameron et al. (2000)
Systematic Review
UK
Grade: Level I
Forty-one studies included, with 14 RCTs, 2pseudo RCTs, 10 cohort studies with concurrentcontrols and 15 cohort studies with historicalcontrols.
Studies were identified using MEDLINE (1976-Aug1998), EMBASE (1980-July 1998) and CINAHL(1982-April 1998). Bibliography searching fromconsidered studies, experts in the field,Cochrane database, Current Contents.
Inclusion criteriaAny systematic review, RCT, pseudo RCT, cohortstudy which reported outcomes associated witha programme to improve function and reducehospital stay of patients aged 65+ years with afracture of the lower limbs, pelvis, upper limbs orspine requiring inpatient or ambulatory hospitalcare.
Exclusion criteriaStudies whose subjects whose fractures were aresult of high-energy transfer – e.g., roadaccidents, studies with rehab following rib andfacial fractures.
Service and study descriptionIncluded studies were categorised into the followingcomparisons:
1.) Hospital physically distinct geriatric orthopaedicrehab unit (GORU) compared to rehab in a generalorthopaedic unit (7 studies). These were unitsspecifically for orthopaedic patients. A geriatricteam was responsible for rehab selection andsupervision following admission, fracture responsibilityof orthopaedic team. Acute and post-acute seen asrequiring separate expertise, post-acutemultidisciplinary, multi disciplinary consensus onpatient decisions. Care model drives costs.
2.) Geriatric hip fracture programme (GHFP) withinan existing acute orthopaedic unit (transfer ofselected patients) compared with orthopaedic teamcare in general orthopaedic unit (5 studies).Geriatrician has expert input on care in unit fromadmission. Multi-disciplinary acute care and rehab.Care model drives costs.
3.) Early supported discharge (ESD) programme(transfer home after early identification in unit)compared to in-hospital care programme (6 studies).Usually non-significant amounts of geriatrician input,but multidisciplinary assessment, discharge planning,community resources and coordination. Stimulatedby costs in acute care sector, transfer of costs tocommunity sector.
Various programmes 1.) to 7.)compared to usual care.� thirty-seven studies had
participants with proximalfemoral fractures, one studyhad mixed patients, and fourstudies had patients with upperlimb fractures. The majority ofparticipants were women butmany patients with poorprognosis were excluded
� both the GHFP (2.) and ESD (3.)programmes reduce the lengthof stay in hospital, but this is notevident for stay in a GORU (1.)compared to a conventionalorthopaedic unit. Length of staymay be reduced by theintroduction of PPS (5.)
� there was a non-significantincrease in readmission ratesafter ESD (3.)
� GHFP (2.) and ESD (3.) achievedsignificantly higher rates ofreturn to previous residentialstatus
� PPSs (5.) have led to a trend ofincreased nursing home use inthe USA
� no evidence was found in theprogrammes evaluated orthrough the introduction of PPSthat there was any associationwith mortality.
� details of individualstudies presented
� overall poormethodologicalquality of includedstudies, out of possible14 mean score 6.2, forRCTs the score was 9.9and 5.7 for otherstudies. The quality ofscore ranged from 8.0for the GORU studiesto 4.3 formiscellaneous andclinical pathwaysstudies
� common deficienciesincluded a lack ofrandomisation,inadequately definedoutcome measures,lack of blinding tooutcome assessment,limited follow-upduration, reporting ofcontrol interventions
� a wide variety ofoutcomes andcomparisons werereported amongincluded studies somewith incompatible andincomplete data,limiting the pooling ofresults. Mortality mostcommonly (26studies), proxymeasures of resourceconsumption likelength of stay (27studies) or place ofresidence atdischarge (24 studies).

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
30
Table 2a. Evidence table of specialist geriatric services for inpatient settings – orthopaedic patient interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Cameron et al. (2000)
Systematic Review
UK
Grade: Level I
(Continued)
4.) Hospital care plan application/clinical pathwaysfor hip fracture treatment compared to standardcare programmes (3 studies). These were generallyprotocol driven in acute orthopaedic units withstandard approaches that may not be sensitive toindividual patient variation. Geriatric teamresponsibility was variable and pathway determined.Time dependent and specific framework involvingexpertise from multiple disciplines determinesdecision-making. Stimulated by costs in acute caresector, designed to improve clinical outcomes.
5.) Effects of Changes in health system strategy andfunding (6 studies). Prospective payment system(PPS). Overall payment regardless of location, theencouragement towards less costly settings. Variablegeriatric team responsibility, care determined by costissues.
6.) Miscellaneous hospital programme comparisonswith other hospital programmes (4 studies). Variablelocations and geriatric team responsibility, staffingand multidisciplinary team makeup and costs.
7.) Therapy, nursing or medical care post-fracture (10studies). Variable locations, multidisciplinary staffingand costs but individual team member responsibility.
The control groups in these studies varied. Generallythe control group received care in an orthopaedicward, other health professionals includinggeriatricians provided care on a consultative basis.
� there was inadequate dataavailable to evaluate theeffectiveness of anyprogramme on the level offunction, morbidity, quality oflife or impact on carers
� GHFP (2.) and ESD (3.)programmes are more likely tobe cost-effective/cost saving. Itwas not clear what the cost-saving implications of GORU (1.)were. The evidence show thatcost saving is stronglyassociated with increased ratesof return of patients to previousresidential status.
� in view of datalimitations only weakgeneralisations can bemade about someoutcomes. Theseinclude length ofhospital stay,readmission tohospital, residence atdischarge, mortality,and level of function
� authors acknowledgethat some outcomesshow significantheterogeneity whenresults are pooled –e.g., length of stay forGORUs. This isunavoidable given thediverse populationcase mix and variableevaluations in evolvingand different systemsof care/healthcareenvironments.
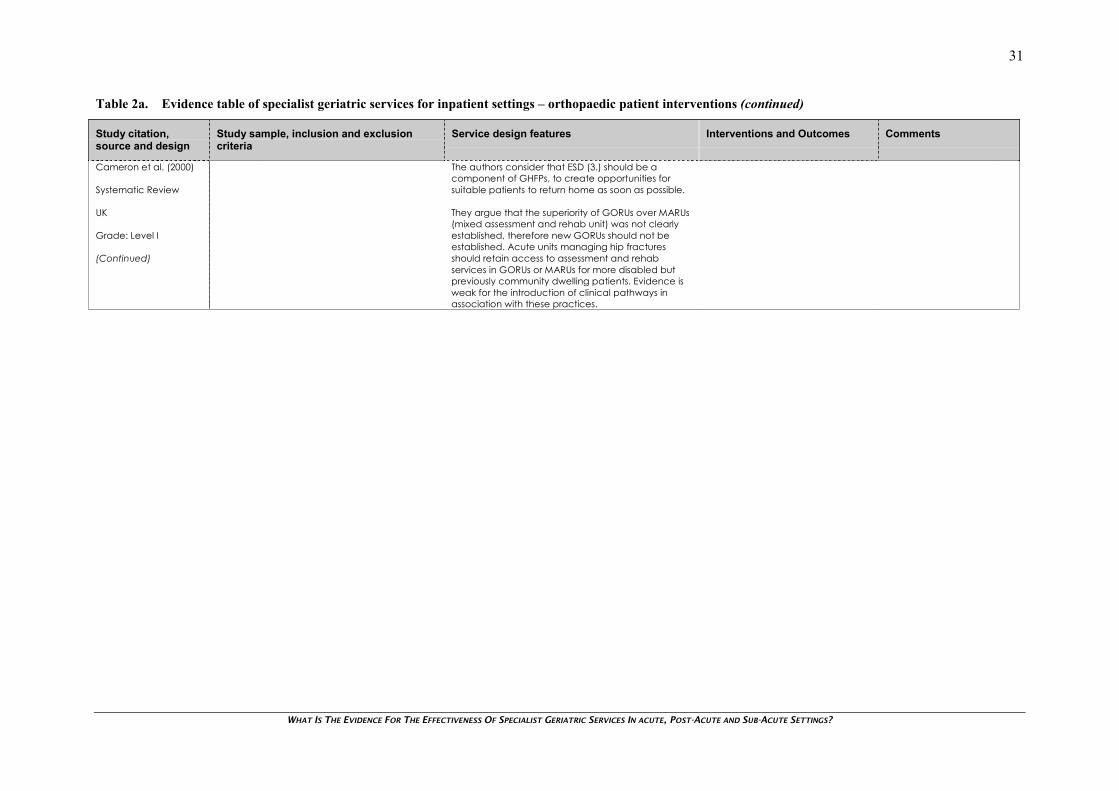
WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
31
Table 2a. Evidence table of specialist geriatric services for inpatient settings – orthopaedic patient interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Cameron et al. (2000)
Systematic Review
UK
Grade: Level I
(Continued)
The authors consider that ESD (3.) should be acomponent of GHFPs, to create opportunities forsuitable patients to return home as soon as possible.
They argue that the superiority of GORUs over MARUs(mixed assessment and rehab unit) was not clearlyestablished, therefore new GORUs should not beestablished. Acute units managing hip fracturesshould retain access to assessment and rehabservices in GORUs or MARUs for more disabled butpreviously community dwelling patients. Evidence isweak for the introduction of clinical pathways inassociation with these practices.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
32
Table 2b. Evidence table of specialist geriatric services for inpatient settings – stroke patient interventions
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Langhorne et al.(2002)
Narrative Review
Glasgow, ScotlandUK
Grade: Level IV
24 clinical trials were identified using the mostrecent Cochrane systematic review of inpatientstroke unit care. Of these 11 trials wereconsidered to meet the inclusion criteria.
Inclusion criteriaPublished controlled clinical trials 1985-2000,study evaluation based on a unit in a discreteward, trials that show positive results – i.e.,reductions in mortality, institutionalisation ordependency.
Trial information obtained using a datacollection schedule accessing all published andunpublished information available to the StrokeUnit Trialists’ Collaboration.
Exclusion criteriaNone specified.
Service and study descriptionComprehensive units with acute and rehab care:Units had 6-12 beds, most-all stroke patients eligiblefor admission, median length of stay 24 days. Staffinglevels for a 10-bed unit were medical 1-2, nursing 3-5physiotherapy 1.2-1.7, OT 0.6-1.7, speech therapy0.25-0.75, social work 0.6.
Rehab onlyUnits had 13-15 beds, half stroke patients eligible foradmission, median length of stay 52 days. Staffinglevels for a 10-bed unit were medical 0.6, nursing 3-4physiotherapy 1-2, OT 1-1.3, speech therapy 0.2-0.6,social work 0.4-0.6.
Most units had medical and nursing expertise instroke management. Goal setting was done by teamstaff, but in some studies there was formal patientinvolvement. Information was provided to patientsand carers in all cases as well as educationprogrammes for staff.
All units had a multidisciplinary team of medical,nursing, physiotherapy, OT, speech and languagetherapy staff and 7/11 studies reported social workerinput. Most often formal multidisciplinary teammeetings were held once per week and informallyup to twice per week.
Most units with acute admissions reported assessmentprotocols inclusive of clinical history, examination,routine biochemistry, haematology investigations,ECG and CT scanning, cartoid Doppler ultrasoundand echocardiography in selected patients. Mosthad general nursing assessments and therapy, anduse of a neurological impairment scales in the firstfew days to monitor progress.
11 studies were included, of which 8described a comprehensive unitcombining acute care and rehab,two described rehab stroke unitsand one described a unit with a‘continuum of care’ with bothcomprehensive care and ‘stepdown’ rehab.
The trials selected show effectiveresults consistent with the directionof the Cochrane systematic reviewwith reductions in mortality,institutional placement ordependency.
� this review deals withstroke units which arebeyond the parametersof the topic but thedescriptions of the keycomponents of strokeunit care aregeneralisable to thespecialist geriatricservices topic. TAGgroup members arealso referred to thestudy for greater detailof the processes ofstroke unit care
� this study was asystematic descriptivesurvey of limitedpublished literature. Theefficacy of the specificcomponents of strokeunit care were nottested other thanincluding studies withpositive results on theoutcomes of interest.No control group ofunits is compared ordescribed
� retrospective analysisand reporter bias as thetrialists’ themselvesprovided the requesteddata
� a subset of effectivestroke unit trials from asingle Cochranereview, non-effectiveunits not compared.No search undertaken
� data collectionschedule used tocollect trial informationbased on previouslypublished pilot work.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
33
Table 2b. Evidence table of specialist geriatric services for inpatient settings – stroke patient interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Langhorne et al.(2002)
Narrative Review
Glasgow, ScotlandUK
Grade: Level IV
(Continued)
Management in the first 0-3 days in almost all studiesincluded early mobilisation, generally beginning onthe day of admission. Other common measures werecareful management of food and fluid intake (use ofsaline IV in first 12-24 hours), insulin forhypoglycaemia, selective use of oxygen, cautiousreduction of high blood pressure. Prevention andmanagement of complications using compressionstockings and antibiotics for infections, avoidance ofurinary catheters, constipation treatment.
General patient management polices during theinpatient care period included:� early physiotherapy using a variety of treatment
approaches, median 45 minute per patientweekday
� early OT using a variety of approaches, median40 minutes per patient weekday
� speech and language therapy mainly fortreatment of dysphagia and communicationproblems, social work and clinical psychologyinput in some trials.
Most units (9/11) made early contact withdischarged patients and carers to makecomprehensive assessments for hospital discharge. Asmall number of trials reported a pre-discharge homevisit or follow-up from a stroke liaison nurse.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
34
Table 2c. Evidence table of specialist geriatric services for inpatient settings – general geriatric patients, preventive interventions
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Parker et al. (2000)
Systematic Review
Leicester, UK
Grade: Level I
84 studies from 45 trials, from searches of 25databases including MEDLINE, EMBASE, CINAHL,Cochrane, SCI, NHS databases, Healthstar,AgeINFO etc. Most from 1988 onwards.
Inclusion criteriaPersons 65+ years, with acute or sub-acute illness(inclusive of psycho-geriatric conditions); in post-operative or rehab stage.
Studies were restricted to RCTs or pseudo-randomised trials, other SRs given volume ofmaterial identified.
Exclusion criteriaDental patients, long-term care, respite care,palliative/terminal care, intensive care, impactof insurance or funding regime, long-termprevention, surgical intervention, drug therapy,screening, housing, clinical treatment.
Any intervention/model of care as an alternative totraditional or usual care in acute wards, hospital orpost-acute care or during sub-acute episodes orrehab and also including post-operative models ofcare and care for medical conditions.
Any model of care with the aim of preventing acutehospital admission, reduce length of stay, hastendischarge, care level adjustment. This could include:� preadmission interventions to prevent
hospitalisation or reduce length of stay� interventions at the point of admission to direct
towards appropriate care� innovative care models within acute hospital
settings that improve outcomes and reducelength of stay
� community-based care to prevent immediatehospital admission
� community-based care immediately post-discharge
� rehabilitation services in any setting.
Outcomes considered in this study were mortality,readmission, destination outcome and health servicecosts. Additional outcomes such as QoL, physicalfunction, patient satisfaction were analysed in the fullreview document. However, studies used manydifferent outcome measures and results werereported in different ways, so only a qualitativeanalysis was possible which was not suitable forinclusion.
Effectiveness of different locationsof acute, post-acute and rehabcare for older patients.� physically distinct Stroke units (8
studies) significantly improvepatient survival over controls,however this was not evident forhip (3 studies) or GAU/ACE units(9 studies). These studies werephysically distinct locations thatdelivered acute care informedby specialist expertise
� a weakening of survival rateswas apparent in stroke units thefurther into follow-up at 6 weeks,6 months and 12 months
� also a significantly greaternumber of patients were at ordestined home at follow-uptime or discharge from strokeunits than the other settingswhich only show small benefitcompared to controls. Costswere either not reported or notsignificant in all but 1 study
� inpatient rehab (often specialistcondition-specific) (10 studies)showed significantly greaterreduction in mortalitycompared to usual care. Thisreduced over time to follow-up
� this was not evident incommunity-based rehab (5studies) or day hospitals (4studies) which showed nodifference in death rates (note:small numbers).
� quality assessment ofincluded studies wasdone using CochraneEffective Practice andOrganisation of Care(EPOC) Group andother previouslypublished assessmenttools
� the analysis wasprimarily qualitative, nodetailed description ofservice delivery modelsof included studiesmaking it impossible todetermine specificservice featurescontributing tooutcomes
� scatter-plots to assessany publication biaswere not available.Where significantheterogeneity waspresent, a randomeffects model was usedto combine results
� inherent difficulties indefining stages of care,variation of terms usedto describe differentmodels of care (i.e.,same terms meandifferent models) anddistinguishinginterventions fromsettings in the literaturewas problematic fordeveloping searchstrategies and datainterpretation.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
35
Table 2c. Evidence table of specialist geriatric services for inpatient settings – general geriatric patients, preventive interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Parker et al. (2000)
Systematic Review
Leicester, UK
Grade: Level I
(Continued)
� inpatient rehab showed asignificant advantage overother settings for homedestinations after discharge/atfollow-up. The two communityrehab and one day hospital trialreported effects in oppositedirections
� cost data quality differedsignificantly. Three papers oninpatient and day hospitalrehab suggest significantbenefit c.f. usual care, two theopposite and the rest nodifference.
� some trials reported tohave generalisabilityissues as very specificpatient groups andtreatments orcomprehensiveexclusion criteria, andmissing information oneligible population
� a number of studiesincluded in this reviewwere also included inthese evidence tables.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
36
Table 2c. Evidence table of specialist geriatric services for inpatient settings – general geriatric patients, preventive interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Inouye et al. (1999),Rizzo et al. (2001) &Bogardus et al. (2003)
Controlled trial
Connecticut,USA
Grade: Level III-2
Also:Inouye (2000)
Descriptive studyConnecticut,USA
Grade: Level IV
426 patients in intervention group, mean age 80years, 39% male.
426 patients in control group, mean age 80years, 39% male.
Inclusion criteriaAll patients 70+ years, sequentially admitted togeneral medicine services in 3 units. No deliriumat admission, intermediate/high risk for deliriumat admission. Admissions from March 1995-March 1995.
Exclusion criteriaCommunication barriers, terminal condition,severe dementia, 48-hour discharge, onventilation, respiratory isolation.
Service and study descriptionYale-New Haven hospital, 800-bed urban teachinghospital, with 200 medical beds. Hospital Elder LifeProgram model with goal of retaining patientindependence throughout hospitalisation withtargeted interventions for risk factors (functionaldecline during stay) by interdisciplinary team,including a geriatric nurse specialist, two Elder Lifespecialists, trained volunteers, a geriatrician, primarycare nurses, other consultative experts (input duringtwice weekly interdisciplinary rounds.
Intervention protocolsHospital unit where six risk factors were targeted(evidence of association with delirium). Cognitiveimpairment, sleep deprivation, immobility, visual andhearing impairment and dehydration. Managementthrough implementation of an orientation protocol,therapeutic activities protocol, non-pharmacologicalsleep protocol, sleep enhancement protocol, early-mobilisation protocol, vision protocol, hearingprotocol, and dehydration protocol.
Quarterly staff audit to ensure protocol adherence.
Usual care was provided by physicians, nurses andtherapists in the other two units (non-interventionstaff).
Effectiveness of a multifacetedintervention for the prevention ofdelirium in hospitalised patientscompared to usual prevention care.� the incidence of delirium,
number of days with delirium,number of episodes wassignificantly lower in theintervention group than thecontrol group
� severity of delirium was notsignificant between the twogroups. Rate of adherence 87%.Risk factor numbers werereduced.
Economic evaluation by Rizzo et al.(2001).� the multi-component targeted
intervention reduced non-intervention costs amongpatients with intermediate risk ofdeveloping delirium but not withthose at high risk
� combined costs (includingintervention costs) showed nosignificant difference on healthcare costs in the intermediaterisk group and higher costs inthe in the high risk groupcompared to the usual caregroup.
Outcomes at 6 months post-discharge by Bogardus et al. (2003)� no differences in any of the 10
outcomes between groupsassessed at 6-months, exceptincontinence less common inthe intervention group. High-riskpatients (poor base-lineprognosis) did have better self-rated health and betterfunctional status. No effects insix other high-risk sub-groups.
� another study alsoreported a similaroverview of the DeliriumPrevention Trial(Inouye, 2000). Alsorefer to descriptivestudy, by Inouye et al.(2000) below on theeffectiveness of theHospital Elder lifeProgram in hospitalisedpatients
� another study byRizzo et al. (2001) useddata from this same trialto assess costevaluations of the multi-component targetedinterventions. Refer tointerventions/outcomescolumn
� another study byBogardus et al. (2003)used data from this trialto assess outcomes at6-months post-discharge. Refer tointerventions/outcomescolumn. The majorlimitations of this studywere an unmatchedanalysis and a greaternumber of patients whodied in the interventiongroup may haveintroduced bias inresults.
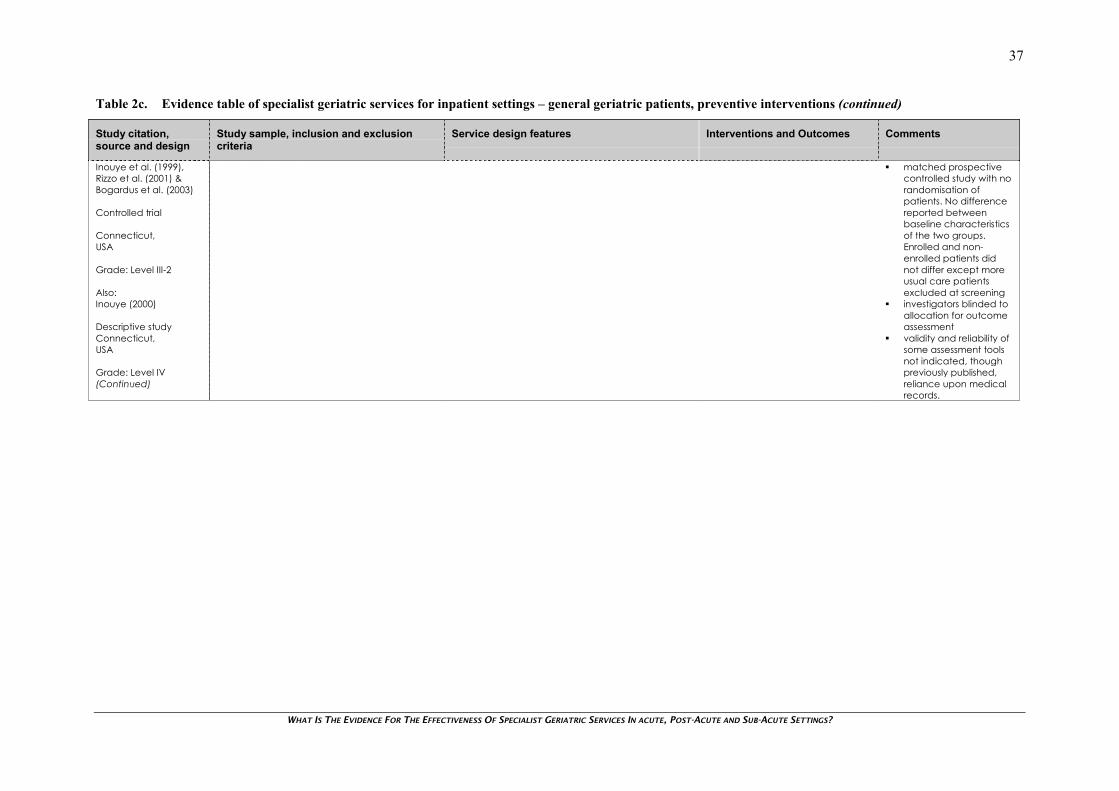
WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
37
Table 2c. Evidence table of specialist geriatric services for inpatient settings – general geriatric patients, preventive interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Inouye et al. (1999),Rizzo et al. (2001) &Bogardus et al. (2003)
Controlled trial
Connecticut,USA
Grade: Level III-2
Also:Inouye (2000)
Descriptive studyConnecticut,USA
Grade: Level IV(Continued)
� matched prospectivecontrolled study with norandomisation ofpatients. No differencereported betweenbaseline characteristicsof the two groups.Enrolled and non-enrolled patients didnot differ except moreusual care patientsexcluded at screening
� investigators blinded toallocation for outcomeassessment
� validity and reliability ofsome assessment toolsnot indicated, thoughpreviously published,reliance upon medicalrecords.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
38
Table 2c. Evidence table of specialist geriatric services for inpatient settings – general geriatric patients, preventive interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Wieland et al. (2000)
Descriptivecross-sectional study
South CarolinaUSA
Grade: Level IV
5,478 patients enrolled, mostly living at homemean age 79 years and 30% male.
Patient admissions between January 1990 andMarch 1997.
Inclusion criteriaPatients 55+ years, eligible for Medicare,meeting nursing home admission eligibilitycriteria, high prevalence of cognitiveimpairment, physical disablement and chronicdisease.
Service and study descriptionProgram of All Inclusive Care for the Elderly (PACE). Acomprehensive community-based geriatric careprogramme pioneered by On Lok. The object of theprogramme was to limit hospital and nursing homeuse and meet patient preferences throughintegrated primary and specialist care.
PACE interdisciplinary teams provided collaborativeassessment, team meetings, individualised treatmentplans and effectiveness monitoring of preventive,rehab, supportive and end-of-life care. Quarterlyevaluation of patients enrolled in programme.Team consisted of primary care physicians, nursepractitioners, clinic nurses, home health nurses, socialworkers, OTs and physiotherapists, health workers,recreation therapists.
Care carried out mostly in PACE day centers, butalso private homes and programme related housing.PACE delivery of short-term hospitalisation andnursing care.
Services were no different from those of usualservices but were consolidated in one center.
Short-term hospital utilisation amongPACE participants.� hospital utilisation (bed-days)
was similar between PACEenrollees and those receivingusual care
� the median time tohospitalisation from enrollmentwas a median 773 days
� hospital mortality occurred in 8%of deaths and one-third ofpatients spent no time inhospital in the 6-months beforedeath. One-third of patientsenrolled died by the end of thestudy.
� descriptive cross-sectional study with nocomparison or controlgroup. Actual efficacyof intervention notevaluated
� a previous study byEng et al. (1997) alsoprovided detailedinformation of the PACEmodel of integratedgeriatric care
� validity and reliability ofassessment tools notindicated, thoughpreviously published,and reliance uponhospital medicalrecords
� possible generalisabilitylimitations of results ofstudy to the NZ contextas HMO health centersin USA health caresetting.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
39
Table 2d. Evidence table of specialist geriatric services for inpatient settings – comprehensive geriatric assessment
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Stuck et al. (1993)
Meta-analysis
Bern, Switzerland
Grade: Level I
28 studies included with 4,959 subjects in CGAinterventions and 4,912 control subjects. FromMEDLINE search and bibliographies in identifiedarticles, abstracts of scientific meetings andexpert sources.
The patient targeting approach in studiesdiffered with 25% excluding either the toohealthy or too ill patients.
Inclusion criteriaNot explicitly stated.
Exclusion criteriaNot explicitly stated.
Service and study description
CGA programmes were categorised into:� GEMU: hospital geriatric evaluation and
management unit, a designated inpatient unit forCGA and rehab.
� IGCS: inpatient geriatrics consultation service,non-designated units where CGA provided tohospital patients on a consultative basis.
� HAS: home assessment service, in-home CGA forcommunity dwelling persons.
� HHAS: hospital home assessment service, in-homeassessment for recently discharged patients.
� OAS: outpatient assessment service, CGA inoutpatient settings.
The intervention team had medical control overimplementation of recommendations in 61% ofstudies, ambulatory intervention follow-up wasincluded in 21% of studies with institutionalprogrammes, non-institutional programmes were50%.
� GEMU programmes showed asignificant reduction onmortality risk at 6 months and 12months. HAS programmesshowed this at 12 and 36months. Statisticalheterogeneity in some resultsmean these should be viewedwith caution
� the combined effects of HHASand OAS studies did not showany effect in mortality
� in 23 studies for people living athome versus death orinstitutional placement, GEMU(6 & 12 months), HAS (at 36months), and HHAS (12 months)programmes had a significanteffect on home living location.The IGCS and OAS programmeshad no significant effect
� all CGA programmes combinedsignificantly reduced hospitalreadmissions during follow-up. Ifseparately analysed, HAS trialswere statistically heterogeneouswith two studies showing asignificant reduction inadmissions but no effect for theother individual CGAprogrammes
� in 14 trials reporting physicalfunctioning the combined resultof GEU studies showed asignificant effect at 6 and 12months, other studies did notreveal an effect in other CGAtypes.
� there was noassessment of thequality of includedstudies and individualstudy characteristicswere not provided.Explicit inclusion andexclusion criteria werenot outlined
� the presence ofheterogeneity(identified throughstatistical tests) in thestudy outcomes meansthat results shouldregarded with somecaution
� authors werecontacted to provideadditional intention totreat data onoutcomes and this wasprovided in 88% ofcases
� potential publicationbias acknowledged byauthors despiteprecautions but funnelplots etc not provided
� limited scope of searchas only one electronicdatabase wassearched in addition tocitation searching andconsulting experts
� a number of studiesincluded in this reviewwere also included inthese evidence tables.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
40
Table 2d. Evidence table of specialist geriatric services for inpatient settings – comprehensive geriatric assessment (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Stuck et al. (1993)
Meta-analysis
Bern, Switzerland
Grade: Level I
(Continued)
� cognitive outcomes wereavailable from 7 studies andthese showed a beneficialeffect for GEMU studies but noeffect for HHAS and OAS studies
� a logistic regression analysis ofthe characteristics CGAprogrammes showed that‘medical control over CGArecommendations’ (HAS at 24months, non-institutional at 24months) and living location(institutional 6 & 12 months,IGCS at 12 months, HAS at 12months) was associated withimproved mortality. Thecovariate ‘ambulatory follow-up’ (GEMU at 12 months) wasassociated with improvedmortality and functionality(institutional studies).
Nikolaus et al. (1999)
RCT, single blind,12 month follow-up
Heidelberg, Germany
Grade: Level II
181 patients in home intervention group,unknown demographics.
179 patients in CGA only group, unknowndemographics.
185 patients in control group, unknowndemographics.
Inclusion criteriaPatients 65+ years with acute disease, multiplechronic conditions and functional deterioration,at risk of nursing home placement.
Exclusion criteriaTerminal illness, severe dementia, remotelocation from services.
Service and study descriptionUniversity hospital at Heidelberg. Patients receivedeither CGA and additional in-hospital and post-hospital follow-up treatment by an interdisciplinaryhome intervention team.OrCGA with recommendations followed by usual careat home.OrAssessment of activities of daily living and cognition(usual care).
Intervention team consisted of three nurses, an OT,social worker and a secretary. They worked closelywith hospital staff and the primary care physician.Team provided additional training in daily livingactivities to patients during hospital stay. Home visitto evaluate patient home during stay. Afterdischarge the team provided treatment (OT etc)which home services could not provide.At least one home visit made after discharge, follow-up visit at 3 months to check implementation. One-year follow-up via telephone interview.
CGA and post-discharge homeintervention compared with CGAalone or usual care (control).� the intervention group showed
a significant reduction in thelength of hospital stay and rateof nursing home placementcompared to the other groups
� there was no significantdifference in the survival, acutecare hospital readmissions ornew admissions to nursinghomes compared to the othergroups. The intervention grouphad shorter hospitalreadmissions and nursing homeplacements
� direct costs were lower for theintervention group.
� baseline characteristicswere described asbeing similar butdemographics ofsample not describedin this paper but were inearlier publishedprotocol
� adequaterandomisation methoddescribed, blinding ofassessors andinterviewers to groupallocation
� validity and reliability ofassessment tools wasnot indicated, thoughpreviously published,reliance upon medicalrecords
� inadequate descriptionof control group care.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
41
Table 2d. Evidence table of specialist geriatric services for inpatient settings – comprehensive geriatric assessment (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Reuben et al. (1995)
RCT, with 3 and 12months follow-up.
California,USA
Grade: Level III-1
1,337 patients in CGA group, mean age 78years, 34% male. 1,016 patients in control group,mean age 77 years, 52% male.
Inclusion criteriaHospital patients in whom at least 1 of 13conditions present – e.g., stroke, dementia,confusion, recent falls, depression, immobility,ADL impairment, unplanned readmission withinpast 3 months. March 1991 to March 1994.
Exclusion criteriaAdmission to hospice, terminal care, admissionto nursing home, non-HMO member.
Service descriptionFour medical centres of a Southern Californiainpatient consultation service performing CGA in theKaiser Permanente Health MaintenanceOrganisation (HMO).
Study descriptionInterdisciplinary team performing CGA, consisting ofa geriatrician, social worker and geriatric nursepractitioner. The team did interview, exam and multi-dimensional assessment. The nurse carried outinterview and assessment and social worker thecognitive function and emotional health tests. Ateam meeting was held and the geriatriciancompiled summary and consultation note toattending physician and primary care practitioner.Significant changes in therapy were discussed withattending physicians by geriatrician.
Follow-up questionnaires on functionality and healthwere completed at 3 and 12 months.
Recommendation compliance was assessed bychart review.
Control group received usual inpatient care from arange of specialties.
CGA by specialist team withininpatient consultation servicecompared with usual care withininpatient settings.� no significant difference in
survival rates at 12-months norafter adjustment for baselinedifferences and analysis by sub-group characteristic comparedto control group
� there were similar functionalityand health status scores,however at 3 months there wasa significant difference(favourable) in mental healthscore and at 12 months inhealth perception c.f. controlgroup
� implementation rates were highfor recommendations related torehab facility placement,moderate for home-health,medical adjustment, diagnostictests, interventions for specificconditions and low for referralsfor other physicians/specialists.
� at baseline there weresmall differencesbetween the twogroups of patients inage and sex. Thesewere adjusted for in theanalysis
� randomisation methoddescribed butinadequate method.Unclear if adequateblinding, physicianstreating both groups ofpatients
� broad selection criteriainclusive of manyphysical and mentalhealth conditions.Investigators usedproxies (familymembers) for obtainingmissing information
� validity and reliability ofassessment tools notindicated, thoughpreviously published,reliance upon medicalrecords
� limited generalisabilityof results of study to theNZ context as HMOhealth centers in USAhealth care setting
� inadequate descriptionof control group care.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
42
Table 2e. Evidence table of specialist geriatric services for inpatient settings – comprehensive rehabilitation programme interventions
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Evans et al. (1995)
Meta-analysis
Washington,USA
Grade: Level I
Eleven clinical trials included, 9 were RCTs.Mean age of patients 75 years, 50% male andmean sample size 199 subjects.
Inclusion criteriaLiterature search for English language studiespublished between 1974-1994 from Medline,CINAHL, citation searching from other meta-analyses and retrieved papers.
Studies dealing with multidisciplinaryrehabilitation from any disabling diagnosis,prospective or crossover designed trials, resultsquantifiable in a meta-analysis.
Exclusion criteriaStudies with sample size not specified, nountreated control group or comprehensiverehab program.
Service and study descriptionMulti-disciplinary comprehensive rehab programmeswithin inpatient settings. Comparison groupsreceived usual non-intervention medical care.
Multi-disciplinary comprehensiverehab programmes compared withusual medical care in inpatientsettings.� patients receiving rehab
interventions had significantlyhigher survival rates atdischarge compared to thosewho received usual care. Thiswas not evident at follow-up
� patients receiving rehabinterventions had significantlyimproved functionality atdischarge compared to thosewho received usual care. Thiswas not evident at follow-up
� patients receiving rehabinterventions were significantlylikely to be returned home atdischarge and remain at homeduring follow-up compared tothose who received usual care.
� limited descriptions ofservice models anddetails of includedstudies reported. Onlythree were non-strokestudies. This may limitgeneralisability of thismeta-analysis to thecurrent topic
� aspects of study qualityevaluated, mostnotably found studiesto be free of patientselection bias
� homogeneity of studyresults was tested andconstant treatmenteffect across studies forsurvival, return homeand functional abilitywas found for bothdischarge and follow-up times
� possible study selectionbias through limiteddatabase search.Uncertain if publicationbias but a sensitivity testperformed to estimatethe number of studiesrequired to offset meta-analytic treatmenteffects.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
43
Table 2f. Evidence table of specialist geriatric services for inpatient settings – general geriatric patients, specialist geriatric unit interventions
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Scott (1999)
Systematic Review
Australia
Grade: Level III-2
Unknown number of studies included in review.
MEDLINE search 1984-1998, Cochrane library,Best Evidence, bibliographies of retrievedarticles. Also non-RCTs providing economicevaluations, descriptions of organisationalaspects of care. Relevant Australian literature.
Inclusion criteriaRCTs or systematic reviews of RCTs , published inEnglish, studies with well defined interventions,outcome measures and patient populations(65+ years), studies with 75+% follow-up andintention-to-treat analysis.
Exclusion criteriaNone specified.
Service and study descriptionAcute geriatric units/service: Older patients admitteddirectly (age- related needs-based criteria) to thegeriatric service after presenting at the emergencydepartment.
Post-acute Geriatric Evaluation and management(GEM): After acute medical illness has beenstabilised, older patients referred to specialisedinpatient or outpatient programmes which provideCGA and rehab.
Geriatric consultation services providing CGA: Thisincludes inpatient consultation by a hospital-based/community-based consultative team tohospitalised patients in general acute care units. Italso includes consultation provided in hospital clinicson a referral basis, home assessments for community-dwelling older which patients recently dischargedfrom hospital.
Geriatric day hospital: hospital or facility based CGAand rehab provided to impaired but at least semi-ambulant community-dwelling older persons on anoutpatient basis, which includes patients recentlydischarged from inpatient GEM units.
Condition-specific interventions: Care programmesaddressing specific patient needs and desiredoutcomes for patients with specific clinicalconditions.
The efficacy for models of geriatriccare
Acute geriatric unitsNo significant differences inmortality or institutionalisation rates.One study promoting rehab andprotocol-based care in a speciallydesigned unit showed functionalimprovement and fewer nursinghome transfers, but not beyond 3-months.
Post-acute GEMHospital based GEM with a rehaband restoration of independentfunction focus improve mortality,functional outcomes, dischargehome. Medically stable eligiblepatients awaiting GEM placementappear to have reduced length ofhospital stay if care is transferred togeriatric teams.
The effectiveness of the unitdepends upon its ability tot targetfrail patients who are neither toosick nor too well to benefit.Predictors of success appear to belong-term follow-up, carercompliance with geriatric teamrecommendations and sufficientcommunity support.
� this systematic reviewwas graded III-2 as thenumber of studiesincluded in the analysiswas not clear. Thequalitative analysisincluded reportedfindings from RCTs andnon-RCTs. Nodescription of individualincluded studies wasprovided
� limited search sourceswith likely studyselection bias. Thedegree of publicationbias in results was notassessed
� the methodologicalquality of includedstudies was notassessed. Results werenot pooled andheterogeneity of resultsbetween studies wasnot evaluated.
Outcomes continuedWith outpatient services,studies reported a mixtureof results, some improvingfunctional mental statusand self-help measures.Studies (3 trials) looking atcommunity and home-based assessment moreconsistently reportedimprovements in mortality,unplanned readmissionsand functionality.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
44
Table 2f. Evidence table of specialist geriatric services for inpatient settings – general geriatric patients, specialist geriatric unit interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Scott (1999)
Systematic Review
Australia
Grade: Level III-2
(Continued)
Community and home-based GEMon selected patients with specificconditions showed success,however studies focussing on non-specific patients did not unlessintervention was intensive andtargeted very frail older.
Combining rehab with nursing andhome care to decrease hospitalreadmission may not be effectivefrom the studies reviewed.
Geriatric consultation services theprovision of CGA to inpatients oroutpatients.
Community and hospital basedspecialist teams (from 3 inpatienttrials) either improved functionalmeasures, lowered mortality, orreduced nursing home transfers.
Some studies (3 inpatient trials)however reported no significantdifference, including a large trialtargeting at-risk patients.
Although other studies showno such differencescompared to non-geriatriccommunity care. Multi-component services withgeriatric assessment preand post dischargetargeting patients at highrisk of readmission appearto have the greatestsuccess.
Day hospitals appear tohave minimal impact fromthe 4 studies reviewed.Trials with condition-specificinterventions show thattargeting at specificgeriatric conditionsassociated with significantmortality and morbidity –e.g., stroke units andorthogeriatric teamsshowed the greatestpromise.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
45
Table 2f. Evidence table of specialist geriatric services for inpatient settings – general geriatric patients, specialist geriatric unit interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Applegate et al. (1990)
RCT, single blinded, 6week, 6 month and 12month follow-up
Memphis, USA
Grade: Level II
78 patients included in geriatric assessment unitintervention, mean age 79 years, 20% male77 patients included in geriatric assessmentcontrol group, mean age 78 years, 26% male.
Inclusion criteriaPatients who were referred by dischargeplanners, primary care personnel and hospitalspecialties to the GAU, who were functionallyimpaired, in recovery from acute medical orsurgical illness and at risk of nursing homeplacement but had reversible functionalimpairment. Enrolment period from July 1985-June 1987.
Exclusion criteriaPatients with unstable medical problems andmonitoring, less than 6 months life expectancy,inevitable nursing home placement.
Service and study descriptionA 1,500 bed university affiliated community hospitalin Memphis Tennessee. The Geriatric Assessment Unit(GAU) was a 10-bed unit in a separate rehabilitationhospital in the larger hospital complex.
The GAU performed interdisciplinary assessments ofmedical, social and psychological function within 72hours of admission by a multidisciplinary team. Theteam was made up of physicians (university facultyand fellows), rehab nurses, physiotherapists, OTs,social workers, psychologists, nutritionists andspeech/audiology specialists.
The service emphasis was equally on assessment andrehabilitation with the primary aim beings to minimisethe risk of patient institutionalisation through assistingwith functional improvement.
Patients were assessed for study inclusion by the GAUand if suitable patients stratified according to low orhigh risk of nursing home institutionalisation pre-randomisation. Once randomised, after assessmentscompleted, a weekly team meeting discussedpatient suitability for specific rehabilitation ortreatment or both. For treatment the patient wastreated in the unit or referred back to referringphysician. For rehab, a goal specific rehabilitativeplan was developed and the patient was required toneed treatment on 3 days per week (for Medicarepurposes).
When patient reached rehab goals or stable level offunction they were discharged with no furthersubsequent services from the GAU team.
The control group received usual care provided bytheir primary physicians, GAU staff were not involvedin their care. There were no differences between thetwo groups in the specialties providing care, andtwo-thirds of patients in both groups receivedprimary care from internists in the community. Thecontrol group received home health care followingdischarge (47% of patients) and care in other rehabunits (22%).
A GAU intervention in a communityhospital versus usual hospital care(control group)� over 6 months the GAU treated
patients had significantlygreater functional improvementthan the control group in 3/8basic self-care activities and 7/8self-care activities for the lowerinstitutional risk stratum. Nodifferences in higher risk stratum.No differences in any after 12months
� over 6 months (but not 1 year)significantly more GAU treatedpatients than control grouppatients were residing in thecommunity
� during 12 months of follow-upthe control group hadsignificantly more nursing homestays than the GAU treatedpatients. Significantly fewer GAUpatients stayed in a nursinghome longer than 6 months
� during the 12 months there wereno differences between groupsin the mean number of daysspent in health care facilities
� based on survival analysis therewere fewer deaths of patientstreated by the GAU c.f. thecontrol group.
� both patient groupssimilar at baseline, butlow/high risk of nursinghome placementcomparison showshigher risk group hadgreater proportionmarried, longer initialhospital stay andgreater severity ofillness
� adequaterandomisation methoddescribed. Singleblinded trial as patientdata collected bytrained interviewers notinvolved in clinical careof patients
� validity and reliability ofassessment tools notindicated althoughthese were previouslypublished
� some 65% of patientswere regarded as low-risk patients
� high probability of typeII error as inadequatesample enrolled forstudy
� despite attempts tocomparable carebetween the twopatient groups, aquarter of the controlgroup had care inother rehab units.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
46
Table 2f. Evidence table of specialist geriatric services for inpatient settings – general geriatric patients, specialist geriatric unit interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Counsell et al. (2000)
RCT, 12 month follow-up
Akron City, Ohio,USA
Grade: Level III-1
767 patients in intervention group, mean age 80years, 40% male.
764 patients in usual care group, mean age 79years, 39% male.
Inclusion criteriaCommunity dwelling persons 70+ years admittedto medical or family practice services in hospitalbetween November 1994 and May 1997.
Exclusion criteriaTransfers from nursing or another hospital facility,specialty unit admission elective admission,length of stay less than 2 days.
Service and study descriptionAkron city hospital, 550-bed private non-profitcommunity teaching hospital HMO affiliated.
Acute Care for Elder (ACE) intervention implementedin a 34-bed unit which was renovated to provide aprepared environment for ACE. Admitting nurseassessed physical/psychosocial function and dailyinterdisciplinary rounds were performed by thegeriatrician medical director and geriatric clinicalnurse. Patient centered care.
Team recommendations recorded andcommunicated to attending physician and nursingcare plans for prevention of disability, and rehabimplemented where appropriate (modified fromthose used by the interventions), discharge planning,medical care review to prevent iatrogenic illness.
Control group patients received usual inpatient care.
ACE unit multi-componentintervention compared with usualinpatient care.� no difference in self-reported
measures of function atdischarge by intention to treatanalysis between groups
� composite outcome of ADLdecline between discharge andyear following hospitalisationnursing home placement wassignificantly less frequent inintervention group
� no significant differences inhospital length of stay, costs,home health care visits, orreadmissions
� nursing care plans significantlymore often implemented andmore frequent physical therapyin the intervention group
� satisfaction with care forpatients, carers, physicians andnurses was higher for theintervention group.
� at baseline there wereno statistical differencesbetween the twogroups reported apartfrom usual carepatients who wereslightly older
� randomisation methodno described in detail.No blinding ofresearchers or patientsto group allocationmay have introducedbias into self-reportedoutcomes – e.g.,mobility
� validity and reliability ofassessment toolsindicated, previouslypublished. Use ofhospital system data
� inadequate descriptionof control group usualcare
� some data on healthstatus was obtained byproxies in some cases.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
47
Table 2f. Evidence table of specialist geriatric services for inpatient settings – general geriatric patients, specialist geriatric unit interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Rubenstein et al.(1984),Rubenstein et al. (1988)& Rubenstein et al.(1995)
RCT, with 12, 24 and36 months follow-up.
Los Angeles,USA
Grade: Level III-1
63 patients included in intervention group, meanage 79 years, 95% male.
60 patients included in control group, mean age77 years, 96% male.
Inclusion criteriaAll persons admitted to acute-care services of aVA medical center that were still in hospital afterone-week. Patients 65+ years, with continuedmedical, functional or psychosocial problemspreventing discharge home.
Exclusion criteriaPatients with severe dementia, terminal illness,other severe conditions resistant to treatment,inevitable nursing home placement. Those wellenough to return home without further supportservices.
Service and study descriptionThe Geriatric Unit of the Sepulveda VeteransAdministration Medical Center. This contains 15-bedson a 29-bed ward in an intermediate care (non-acute) area of the hospital. It was staffed by aninterdisciplinary team including a faculty physician,geriatrics Fellow, assistant physician, social worker,nurses and nursing assistants. Part-time staff wereattached including a clinical psychologist, dietitian,OT, physiotherapist, audiologist, public health nurse.
After random assignment patients were admitted tothe Geriatric Unit intervention usually within 48 hours.Patients’ medical, psychosocial, and functionalstatus was assessed by appropriate team member.
Weekly team meetings were held to finalisetreatment plans. The goal was short-term treatmentand rehab services in the unit. Patient progress andtreatment plans were followed closely during dailyward rounds and reviews took place at weekly teammeetings. Reassessments done at 3, 6, 9, and 12months. Additional data collected at 6 and 12months.
Those patients assigned to the control group wentthrough usual hospital acute care services and weredischarged home or put into long-term care facilities.Consultative and other services were also availableto control patients.
Geriatric evaluation unit (GEU)compared with usual care.� patients in the GEU had
significantly less mortality thanthe control group patients
� at 12 months, half the controlgroup had died and one-quarter of the unit group. Overthe 3 years (43% versus 38%) thesurvival curves were significantlydifferent, the greatestdivergence between groups at1 year, then gradualconvergence, the last 5 quartersindividually were not statisticallysignificant
� at 12 months, GEU patients weresignificantly more likely to bedischarged home and not tohave spent time in a nursinghome, have improved moraleand personal self-maintenanceduring follow-up compared tothe control group
� there was significantimprovement in functionality inboth groups at 6 and 12 monthsbut significantly more in GEUpatients compared to controls.Data examining the degree offunctionality showed that in thefirst year there were nodifferences in time spent in low,moderate and high functioningduring the first year. During thesecond year, GEU patientsspent significantly more time inmoderate functioning, butaverage times in low or highfunctioning were not different.GEU patients with greatersurvival did not have reducedlevels of function.
� the three studies reportdata from the sametrial, the study byRubenstein et al. (1984)reported outcomesover the first 12 months,Rubenstein et al. (1988)reported outcomes at24 months and the trialby Rubenstein et al.(1995) reportedoutcomes for the 24and 36 month period
� both patient groupshad similar baselinecharacteristics, exceptin 4 minor variables
� only 8.5% of patientsscreened wereincluded in the finalsample
� randomisation methodnot described,uncertain of blinding ofinvestigators to patientgroup allocation andoutcome assessment
� limited generalisabilityof results of study to theNZ context as mostlymale patients from VAhealth centers in USAhealth care setting
� validity and reliability ofassessment tools notindicated althoughthese were previouslypublished
� similar functionalityresults up to one yearreflect the ‘selective’attrition effect of highmortality losses to thecontrol group.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
48
Table 2f. Evidence table of specialist geriatric services for inpatient settings – general geriatric patients, specialist geriatric unit interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Rubenstein et al.(1984),Rubenstein et al. (1988)& Rubenstein et al.(1995)
RCT, with 12, 24 and36 months follow-up.
Los Angeles,USA
Grade: Level III-1
(Continued)
� GEU patients had higherindependence (>2 ADLcategories) than controls at twoyears
� over the 3 year period percapita cost was not significantlydifferent either before or aftersurvival adjustment. However forpatients who died during thefollow-up period, per capitahealth care costs for GEU weresignificantly lower in the GEUthan control group.
Karppi & Tilvis (1995)and Karppi (1995)
RCT, 24 month follow-up
Central health caredistrictFinland
Grade: Level III-1
104 patients in intervention group, mean age 79years and 22% male.
208 patients in control group, mean age 78 and22% male.
Inclusion criteriaSupervised home care patients 65+ years,multiple problems, polypharmacy and problemscoping at home.
Exclusion criteriaTerminal care, acute disease or injury bettertreatable elsewhere than in the unit.
Service and study descriptionGeriatric unit with 8 beds in a Finish central hospital.Team consisted of a doctor, five nurses, sevenauxiliary nurses, three assistants, one secretary, onepsychologist, OT, part-time social worker and twophysios. Specialists consulted as needed. Targetedpatients admitted to unit were individually assessedand rehabilitated.
The control group received usual home care with nogeriatric consult.
Outcomes assessed at hospital discharge and follow-up at 12 months.
Assessment and rehab in geriatricinpatient ward compared with usualhome care� the intervention group had
significantly fewer days in healthcentre hospitals than controls
� no significant differences incumulative institutionalisation ormortality over 24 months
� at 3 months (but not 12 months)the intervention groupexperienced significantly morepositive changes than controlsin continence, housekeepingand satisfaction.
� study by Karppi (1995)also used data andpresented results fromsame trial
� at baseline there wereno statistical differencesbetween the twogroups reported
� randomisation methodadequate anddescribed in detail. Noblinding of researcherto group allocation
� validity and reliability ofassessment tools notindicated, thoughpreviously published
� inadequate descriptionof control group care.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
49
Table 2f. Evidence table of specialist geriatric services for inpatient settings – general geriatric patients, specialist geriatric unit interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Saltvedt et al. (2002)
RCT, with 6 and 12months follow-up.
Trondheim, Norway
Grade: Level III-1
127 patients allocated to geriatric evaluationand management unit (GEMU), mean age 82years, 36% male. 127 patients allocated togeneral medical ward, mean age 82 years, 34%male.
Inclusion criteriaEmergency acute admissions to Department ofInternal Medicine, patients suitable for GEMUtransfer, not in need of specific treatment,patients 75+ years, patients with acute strokeonly if unit full. Patients included betweenNovember 1994 and November 1995.
Exclusion criteriaNursing home patients, discharge within 3 days,quick recovery from acute illness, dementia,terminal illness, <6 month life expectancy.
Service and study descriptionA regional university hospital of Trondheim servingpopulation of 200,000. With 190 beds in ninedifferent sections.
In the GEMU a comprehensive assessment wasemphasised and prevention of complications andiatrogenic conditions. An interdisciplinary approachwas taken, with close collaboration between staff.Twice weekly staff meetings were held for assessmentreports, goal setting, problem discussions anddischarge planning.
Staff: one geriatrician and one (occasionally two)residents, nurses with training in geriatrics, 2 OTs, andone physiotherapist (OTs and PTs performedassessments in both groups during study). A socialworker, dentist and other specialties were consultedwhen necessary. Average of 1 physician per 5 beds.
Early mobilisation was instituted for patients andrelevant rehabilitation. Follow-up was initiatedfollowing a joint meeting between GEMU staff, GPs,home care nurses and patients and their families. Thiswas GP led with assistance from home-care nurses,OTs and physiotherapists.
The medical ward (control) patient group was caredfor according to the Department of InternalMedicine protocols. Assessment mostly carried out bydoctors and nurses. Staff from different specialtieswere responsible for ongoing care. One physicianper 5-10 beds.
GEMU compared with a generalmedical ward.� the median length of hospital
stay was significantly longer inthe GEMU than control settings
� an average of 3 diagnoseswere made in the GEMU groupcompared to the control groupwhere there were 2 diagnoses
� mortality was lower in the GEMUgroup during the first yearcompared to the control group,significantly so for the 3, 6, 9month period.
� at baseline bothpatient groups werereported to have similarcharacteristics
� adequaterandomisation methoddescribed, uncertain ofblinding/concealmentof investigators topatient groupallocation andoutcome assessment.Some staff (OTs & PT)treated patients in bothgroups
� only 18% of patientsscreened enrolled instudy
� validity and reliability ofassessment tools notindicated, relianceupon medical records.
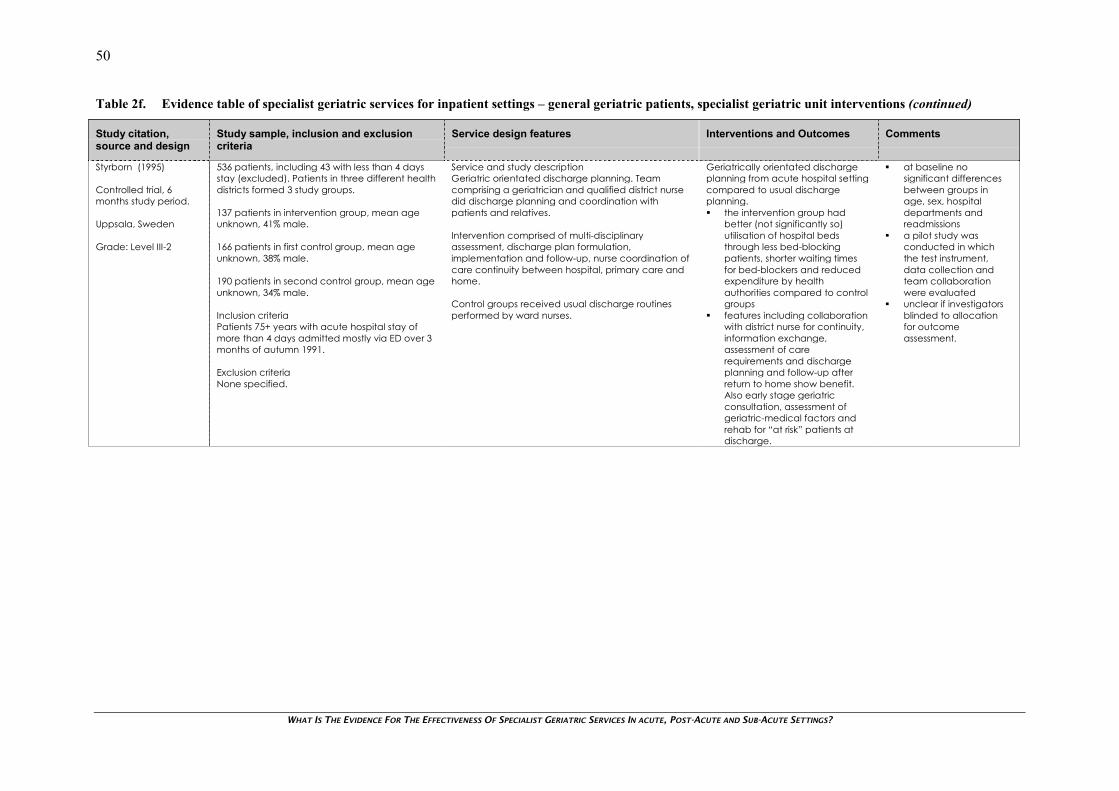
WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
50
Table 2f. Evidence table of specialist geriatric services for inpatient settings – general geriatric patients, specialist geriatric unit interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Styrborn (1995)
Controlled trial, 6months study period.
Uppsala, Sweden
Grade: Level III-2
536 patients, including 43 with less than 4 daysstay (excluded). Patients in three different healthdistricts formed 3 study groups.
137 patients in intervention group, mean ageunknown, 41% male.
166 patients in first control group, mean ageunknown, 38% male.
190 patients in second control group, mean ageunknown, 34% male.
Inclusion criteriaPatients 75+ years with acute hospital stay ofmore than 4 days admitted mostly via ED over 3months of autumn 1991.
Exclusion criteriaNone specified.
Service and study descriptionGeriatric orientated discharge planning. Teamcomprising a geriatrician and qualified district nursedid discharge planning and coordination withpatients and relatives.
Intervention comprised of multi-disciplinaryassessment, discharge plan formulation,implementation and follow-up, nurse coordination ofcare continuity between hospital, primary care andhome.
Control groups received usual discharge routinesperformed by ward nurses.
Geriatrically orientated dischargeplanning from acute hospital settingcompared to usual dischargeplanning.� the intervention group had
better (not significantly so)utilisation of hospital bedsthrough less bed-blockingpatients, shorter waiting timesfor bed-blockers and reducedexpenditure by healthauthorities compared to controlgroups
� features including collaborationwith district nurse for continuity,information exchange,assessment of carerequirements and dischargeplanning and follow-up afterreturn to home show benefit.Also early stage geriatricconsultation, assessment ofgeriatric-medical factors andrehab for “at risk” patients atdischarge.
� at baseline nosignificant differencesbetween groups inage, sex, hospitaldepartments andreadmissions
� a pilot study wasconducted in whichthe test instrument,data collection andteam collaborationwere evaluated
� unclear if investigatorsblinded to allocationfor outcomeassessment.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
51
Table 2f. Evidence table of specialist geriatric services for inpatient settings – general geriatric patients, specialist geriatric unit interventions (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Inouye et al. (2000)
Descriptive study
Connecticut,USA
Grade: Level IV
1,716 admissions of 1,507 patients, mean age 81years, 36% male.
Inclusion criteriaAll patients in the program, 70+ years, screenedon 6 risk factors (cognitive impairment, sleepdeprivation, immobility, dehydration, vision andhearing impairment), at risk of further decline inone or more risk factors while in hospital.March 1995 to August 1999.
Exclusion criteriaTerminal condition, severe dementia, 48-hourdischarge, on ventilation, respiratory isolation.
Service descriptionYale-New Haven hospital, 800-bed urban teachinghospital, with 200 medical beds. Hospital Elder LifeProgram model with goal of retaining patientindependence throughout hospitalisation withtargeted interventions for risk factors (functionaldecline during stay) by interdisciplinary team,including geriatric nurse specialist, Elder Lifespecialist, trained volunteers, geriatricians, primarycare nurses, other consultative experts (input duringtwice weekly interdisciplinary rounds.
Intervention protocolsDaily visitor/orientation*, sleep enhancement*, oralvolume repletion*, feeding assistance*, therapeuticactivities protocol*, early mobilisation*, vision-hearingadaptions* (*volunteer assisted).
Geriatric nursing interventions, interdisciplinaryrounds, provider education. Daily tracking ofimplementation adherence.
Staff rolesElder Life Specialist - daily assessment, rounds withintervention focus on prevention of cognitive andfunctional decline. Educational activities for nursingstaff. Interdisciplinary rounds twice weekly, reviews ofall patients in program and follow-up ofimplementation of recommendations. Staff liaison,discharge planning and communication withcommunity caregivers on as-needed basis.Geriatrician - geriatric medical expertise and back-up to staff. Participation in twice weekly HospitalElder Life Program interdisciplinary rounds andpatient consultations when requested by attendingphysicians. Targeted consultations to staff ongeriatric issues, liaison with the medical staff on anas-needed basis. Formal education for physician staffon geriatric issues.Elder life Specialist/Volunteer coordinator - programoperations, conduct of interventions and completionof these, and volunteer training/coordination. Patientscreening and enrolment. Development of individualpatient plans for programme.
Hospital Elder Life Program� there was partial or complete
program adherence for 89% ofpatients over 37,131 patient-days
� median length of stay was 7days (range 1-163 days).Discharge home 56% ofpatients, short-term rehab in anursing home 15%
� over 8% of patients tested withthe Mini-Mental StateExamination (MMSE) scale and14% of patients with the ADLfunctioning scale showed adecline of at least 2 pointsbetween admission anddischarge.
� descriptive study, nocomparator or controlgroup. Refer to earliercontrolled trial byInouye et al. (1999) onthe effectiveness of theHospital Elder lifeProgram on theprevention of deliriumin hospitalised patients
� validity and reliability ofassessment tools notindicated, thoughpreviously published,reliance upon medicalrecords
� complete adherenceto the programme wasdefined as a patientreceiving all parts ofthe protocol whilepartial adherence wasdefined as a patientreceiving parts of theassigned protocol.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
52
Table 3. Evidence table of specialist geriatric services in outpatient settings
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Boult et al. (2001) &Boult et al. (1994)
RCT, single blinded with18 month follow-up
Minnesota, USA
Grade: Level II
294 patients in the GEM outpatient group, meanage 79 years, 54% male.
274 patients in the control group, mean age 79years, 58% male.
Inclusion criteriaCommunity dwelling Medicare beneficiaries athigh risk of future hospitalisation and functionaldecline based on results of mailedquestionnaire.
Exclusion criteriaNursing home residence, serious illness, andprimary care provider refusal for person’sparticipation.
Service descriptionAmbulatory clinic in a community hospital.
Study descriptionPatients in the GEM outpatient group received ahome visit by a social worker and two visits to theGEM clinic. The first was for a history and physicalexamination by a GNP, the second for evaluation bya geriatrician and a nurse. This team assessed thingssuch as medical conditions, functional ability,cognitive status, and psychosocial status. After thepatient’s second visit a brief team meeting was heldto set intervention priorities, create a care plan andassign responsibility from the GEM team for follow-upaction. A 24-hour on-call service was available for anumber of months. The team was involved in thediagnosis and treatment of problems, counseling,health education, maintaining medication, andreferrals.
The team individually saw patients monthly in theclinic and further team meetings were held. Betweenvisits, regular telephone monitoring of patients’ careplans was provided. Hospital care was provided(patient choice) by either the GEM geriatrician orprimary care physician.
The GEM outpatient care continued until significantresolution of problems or stable treatment statusreached (average 6 months). Patients’ dischargedto primary care physician, detailed dischargesummary.
Outpatient GEM care comparedwith usual care.� the outpatient GEM group had
significantly greater functionalability at 6, 12, and 18-monthassessments in sickness impactprofiles
� differences were only significantat 12 and 18 monthsrespectively for bed disabilitydays and restricted activity days
� the GEM outpatient group hadsignificantly less evidence ofdepression than the controlgroup at 12 and 18 months.After controlling for baselineconfounding variablessignificance was reached at 18months follow-up
� there was no significantdifference between the groupsin terms of rates of survival.
� baseline characteristicsreported as similarbetween groups
� this trial was based onearlier pilot study byBoult et al. (1994). Thisfound outpatient GEMled to reducedmortality, use of EDfacilities and nursinghomes. Also study byBoult et al. (1998), avery similar RCT but wasexcluded as outcomesfocused on servicefrequency use ratherthan measures ofefficacy
� possible subjectselection bias throughmailed questionnaireresponse bias. Analysisshowed significantdifferences incharacteristics ofresponders (healthier,younger, male) versusnon-responders
� adequaterandomisation methoddescribed, singleblinding of investigatorsto patient groupallocation
� validity and reliability ofassessment tools notindicated althoughthese were previouslypublished
� usual care model ofcare not adequatelydescribed.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
53
Table 3. Evidence table of specialist geriatric services in outpatient settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Burns et al. (2000) &Burns et al. (1995)
RCT, with 1 and 2 yearfollow-up
Tennessee, USA
Grade: Level II
60 patients were in the GEM intervention, meanage 72 years, 95% male.
68 patients were in the usual care group, meanage 71 years, 99% male.
Inclusion criteriaSubjects aged 65+ years admitted to eithersurgical, medical or neurology services at theVeterans Affairs Medical Center, Memphis.Required to have one or more ADL deficiencies,two or more chronic health conditions, two ormore acute-care hospitalisations in past year, 6+prescription drugs.
Exclusion criteriaAdmitted from or planned placement in nursinghome, required inpatient GEM during hospitalstay, terminal illness, <6 months to live,moderate-severe dementia.
Service description and study descriptionThe outpatient GEM unit had an interdisciplinaryteam with physicians, a nurse practitioner, a socialworker, psychologists, and clinical pharmacists. Theteam clinical focus was evaluation and long-termmanagement. The initial assessment took up to 2-hours involving all the team. Once these werecomplete the team developed goals, interventions,treatment and individualised patient follow-up.Follow-up care consisted of a range of services fromshort-term hospital admission to routine clinic careand telephone follow-up. For follow-up care thepatient saw the most appropriate healthcareprofessional and received consultations from otherteam members.
Return visits were not scheduled other than thecollection of study data, but patient’s were followedup indefinitely.
The control group was made up of patients who atthe time of hospital discharge were referred back totheir original or new providers by the inpatienttreatment team. Outpatient care was provided inthe ambulatory care clinics of the medical center orby community physicians. Patients requiring inpatientevaluation or rehab were referred to the rehabservice or extended care unit but not the inpatientGEM, nor were patients referred to the outpatientGEM or outpatient geriatrics clinic.
Outpatient interdisciplinary GEMcare compared with usual care.� at 2-years there was no
significant relationship betweengroup assignment and mortalitystatus
� during the 2-years there was asignificant treatment effect onhealth perception for the GEMgroup compared to the usualcare group
� by the second year the controlgroup had significantly moreclinic visits than the GEM group.No significant differences werefound between grouphospitalisation rates during thetwo years
� functional status as reflected inADL and IADL scores showed nosignificant difference in the 2-year group-time interaction forADL, but was significant for IADLwith less impairments
� the 3 measures of QoL (generalwell being, life satisfaction,depression scales) showedsignificant improvement for bothgroups over the 2-years, but thisgreater in the GEM group.
� study methodologypublished in earlierpaper by Burns et al.(1995) which containsdetailed methodologyinformation andoutcome assessment atone year and is referredto here in the outcomes
� baseline characteristicsreported as similarbetween groups
� limited generalisabilityof results of study to theNZ context as mostlymale patients from aVA health center in USAhealth care setting
� two-year follow-updata were available for98/128 (77%) patients.Intention to treatanalysis
� adequaterandomisation methoddescribed, butinvestigators were notblinded to groupallocation for outcomeassessment
� validity and reliability ofassessment tools notindicated althoughthese were previouslypublished.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
54
Table 3. Evidence table of specialist geriatric services in outpatient settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Cohen et al. (2002)
RCT, single blinded with6 and 12 month follow-up
Various states, USA
Grade: Level II
1,388 patients were enrolled in the study, meanage 74 years, 98% male.
Inclusion criteriaAged 65+ years, on a medical or surgical wardwith expected length of stay 2+ days, frailcondition recruited from August 1995 to June1996.
Exclusion criteriaHospital admission from a nursing home, alreadyreceiving care at an GEM outpatient clinic,previously hospitalised in an inpatient unit forGEM, severe or terminal illness.
Service descriptionEleven Veteran Affairs medical centers withestablished inpatient and outpatient care programsof GEM.
Study descriptionInpatient and outpatient GEM intervention teamseach consisted of a geriatrician, social worker, anurse followed a standard GEM protocol. Thisinvolved history taking, examination, screening forgeriatric syndromes within 3 days of admission toGEM unit. A problem list was compiled, assessmentwas performed, and a care plan developed and theteam met twice weekly to discuss the plan.Preventive and management services were alsocoordinated to particularly maintain functionality.
Patients assigned to receive either usual inpatient oroutpatient care received appropriate care, exceptno care directly from the GEM unit team.
Randomisation to either inpatientcare in a GEM unit or usual inpatientcare followed by randomisationfollowing care to either outpatientcare in a GEM unit or usualoutpatient care.� no significant differences
between any of the four-inpatient and outpatient groupsin survival or in the analysis ofinteraction effects (combininginpatient and outpatient GEMversus usual care) at 6 and 12months
� QoL scores were positive atdischarge for inpatient GEMpatients for physicalperformance and basicactivities of daily living
� compared with QoL scores atdischarge only the effect onbodily pain remained significantat 12 months in the GEMinpatient group
� QoL scores were significantlypositive at discharge comparedto 12 months later for outpatientGEM patients for energy, mentalhealth, and general health
� compared with QoL scores atdischarge only mental healthimprovement remainedsignificant at 12 months in theGEM outpatient group.
� all four patienttreatment groups weredescribed as similar atbaseline but data notprovided
� limited generalisabilityof results of study to theNZ context as mostlymale patients from VAhealth centers in USAhealth care setting
� adequaterandomisation methoddescribed, singleblinding of investigatorsto patient groupallocation for alloutcome data excepta Physical Performancetest. However, clinicianswere not blinded topatient allocation
� outpatient GEM carenot adequatelydescribed and usualinpatient andoutpatient care notdescribed
� validity and reliability ofassessment tools notindicated althoughthese were previouslypublished.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
55
Table 3. Evidence table of specialist geriatric services in outpatient settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Epstein et al. (1990)
RCT, single blindedwith 12 month follow-up
Rhode Island,USA
Grade: Level II
185 patients in geriatric assessment group, meanage 77 years, 49% male.
210 patients in second opinion internist group,mean age 77 years, 52% male.
205 patients in geriatric assessment group, meanage 77 years, 50% male.
Inclusion criteriaPatients enrolled in an HMO and older than 70years rated by their primary physician as havingfair or worse health and experiencing probabledeterioration. Patients recruited betweenMarch 1985 and February 1996.
Exclusion criteriaNone specified.
Service descriptionA large Health Management Organisation (HMO)called the Rhode Island Group Health Association(RIGHA) made up of an 80,000-pateint staff model.
Study descriptionStudy to determine if the benefits obtained fromconsultative geriatric assessment were related to theunique features of the assessment and not theprovision of extra medical attention. Aim was tomaximise the number of individuals representingdifferent disciplines to generalise positive outcomesfrom a team approach to care and to minimise theuse of multiple different staff and ensure coordinatedcare among the geriatric teams.
Ambulatory patients were stratified according to 70-74 and 75+ year age groups and randomised intothree groups. Consultation by a geriatric team (10geriatricians, 3 nurse-social worker teams) andtelephone follow-up, consultation by a “secondopinion” internist (11 internists at RIGHA with nospecialist geriatric training/experience), and usualHMO services (control group).
The geriatric assessment and second opinion internistexaminations were given about 1-month post-randomisation. The geriatric assessment(2 hours) was carried out by a geriatrician, geriatricnurse practitioner, and geriatric social worker. Abroad range of clinical and functional status datawas obtained. The geriatricians (all with 1+ years ofclinical training in a geriatric fellowship program)reviewed patient medical records, performedphysical examination (drugs, nutrition, newdiagnoses), and functionality.
The nurse administered a standard protocol forclinical assessment and the social worker reviewedsocial support, activities, coping and psychologicalfunction. The team met for 15 minutes after meetingpatient to formulate care plans and also consultedas a group with patient and family. Carecoordination and on-going care by written ortelephone communication with regular providers.
Patients were randomised into 3groups, either consultation by ageriatric assessment team,consultation by a “second opinion”internist or usual HMO services(control group).
Comparison of geriatric assessmentteam and second opinion patientgroups:Both groups identified newdiagnoses in about 30% of patientsand advised further diagnostictesting, and changes in medicationin a similar proportion of patients.� geriatric assessment teams
made significantly more newdiagnoses, provided morepsychosocial evaluations,suggested more medicationregimen changes, andhome/community servicechanges
� no difference between the 3patient groups in terms ofmortality, hospitalisation, ornursing home placement
� significant advantage forgeriatric assessment group incognitive function at 3 monthsbut not 1 year compared tocontrol group. No otherdifferences in geriatricassessment versus control group
� an interaction analysis did notshow any consistent benefitfrom assessment for those whowere older, more debilitated orliving alone.
� baseline characteristicswere similar betweenthe 3 groups of patients
� adequaterandomisation methoddescribed, an internistblinded to interventiongroup allocationabstracted consultationletters using a strictprotocol, with reliabilitytested by reabstractionof a sample by anotherinvestigator (inter-rateragreement 90%)
� assessment andinterview instrumentswere validated in mostcases and small pilottest performed on 50non-study participantsto enhance reliability
� possible limitedgeneralisability of resultsin a New Zealandsetting as HMO settingin the USA
� study powercompromised at sub-group interactionanalysis
� similar losses to follow-up between the 3groups, about 12% ineach group. Intentionto treat analysis.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
56
Table 3. Evidence table of specialist geriatric services in outpatient settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Epstein et al. (1990)
RCT, single blindedwith 12 month follow-up
Rhode Island,USA
Grade: Level II
(Continued)
Depending on findings follow-up tests etc orderedfollowing confirmation with regular physician. Threetelephone follow-ups in the first 2 months post-examination by team and also 3 and 12-monthfollow-up examinations for outcome assessment.
The second opinion consultations by internists whoperformed unstructured examinations (1 hour) withhistory and physical exam. Integration ofconsultation was accomplished by writtencommunication.
The control group received regular RIGHA serviceswith no extra evaluations.
� null results may reflectintervention focus onassessment with onlylimited continuing carefollow-up viatelephone. Also relativehealthiness of patientsincluded in study andsimilarity of geriatricteam patient care andcontrol patient carebeing based in thesame HMO setting.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
57
Table 3. Evidence table of specialist geriatric services in outpatient settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Rubin et al. (1993)
RCT, with 1 year follow-up
Texas, USA
Grade: Level II
100 patients included in the outpatient GATgroup, mean age 77 years, 41% male.
100 patients included in usual care group, meanage 77 years, 36% male.
Inclusion criteriaIndigent acutely ill patients recruited from themedicine inpatient service, admitted fromemergency room. Initiation of intervention afterdischarge. Patients were at high risk of hospitalreadmission and suitable candidates foroutpatient management of existing chronicconditions as alternative to inpatient treatment.
Exclusion criteriaTerminal illness, dementia.
Service description and study descriptionThis was a long-term outpatient comprehensivegeriatric care model. This service was provided by ageriatric assessment team (GAT) set in a largemedical school affiliated public hospital. The teamconsisted of an internist, psychiatrist, nurse specialist,and social worker all specialising in geriatrics.The team provided a CGA and developed a long-term care plan during interdisciplinary staff meetings.The inpatient team providing care was informed thatsubsequent primary care would be provided by theGAT team, which provided discharge planningdirection. This was the only GAT team provided careduring hospitalisation.
GAT team discharge planning consisted ofcontacting family members, making them familiarwith the team an its purpose. Home health referralswere also made where appropriate.
At discharge the patients were given a GAT clinicappointment. Other appointments were cancelledunless approved by the GAT team, and were seenby a GAT team member if possible.
Patients were encouraged to call the GAT office forany medical problems instead of going to theemergency room. Ongoing interdisciplinary care wasprovided in the GAT clinic and patient care wasprovided by the same team members throughoutthe study.
Readmissions to hospital were seen by the standardmedical team but were monitored and dischargeplanning was resumed by the GAT team.
Outpatient GEM team compared tousual inpatient discharge andfollow-up care.� no significant difference
between groups in cognitivestatus. Both groups hadreasonably high level offunctioning at follow-up
� no significant differencebetween groups in functionalstatus: activities of daily living.Both groups showed nosignificant decline at follow-up
� a significant difference betweengroups was found ininstrumental activities of dailyliving (IADL). Control group hada greater degree of impairmentat follow-up
� no significant difference in lifesatisfaction scores at follow-up.GEM patients were likely to havesignificantly greater subjectiveassessments of health andphysical wellbeing than controls.
� data analysed here isfrom an earlier study byRubin et al. (1992). Thiswas excluded as itlooked at non-relevantoutcomes, Medicarebilling and serviceutilisation data etc
� baseline characteristicswere similar betweenthe 2 groups ofpatients. Both groupswere predominantlyblack or Hispanicminorities. Limitation ingeneralisability of resultsto NZ context
� adequaterandomisation methoddescribed, unclear ifinvestigators wereblinded to groupallocation for outcomeassessment
� high participant lossesat follow-up interview,36% in each group, butanalysis reported noeffect on groupcomparability. Intentionto treat analysis
� validity and reliability ofassessment tools notindicated althoughthese were previouslypublished.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
58
Table 3. Evidence table of specialist geriatric services in outpatient settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Rubin et al. (1993)
RCT, with 1 year follow-up
Texas, USA
Grade: Level II
(Continued)
Usual care for patients admitted was provided by amedical team consisting of a physician, intern, andmedical students. No recommendations wereoffered to the team. At discharge these patientsreceived usual care as provided by the medicalteam at a hospital general medicine clinic staffed bya physician and medicine residents. A social workerwas available and emergency room referral wherenecessary, outpatient care was provided by theclinic and alternatives such as sub-specialty clinics,neighbourhood clinics and non-medicine clinics asrequired.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
59
Table 3. Evidence table of specialist geriatric services in outpatient settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Williams et al. (1987)
RCT, with singleblinding and 4, 8, and12 month follow-up
New York, USA
Grade: Level II
58 persons in Geriatric Ambulatory ConsultativeService (GACS) group, median age 76 years,36% male.
59 persons in control group, median age 77years, 44% male.
Inclusion criteriaNon-institutionalised persons living in MonroeCounty, New York, 65+ years, meeting one ofthe following criteria. Had a significantfunctional decline and not received medicalevaluation in previous 12 months, identifiedunstable medical problem, identified unmetneeds in daily living performance, taking 3+medications, dissatisfied patient seeking secondmedical opinion.
Exclusion criteriaNot specified.
Service description and study descriptionAn outpatient consultation service in operation since1980. The type of patient population dealt with wereolder persons, chronically ill persons with changingmedical, psychological, social support andfunctional conditions.
These conditions in many cases have reached crisisor urgent status and require ongoing long-term care.Patients with a wide diagnostic or behavioural rangeof factors were eligible.
The service was run by a team consisting of internists,family physicians, psychiatrists, nurses, social workers,and nutritionists trained in geriatrics. A wide range ofspecialty consultants were available.
Patients requiring evaluation were seen within 2weeks of their notification to the GACS. This wasinitiated by telephone where a nurse interviewed thereferring party and scheduled an appointment.At the first initial visit the physician saw the patient for1-hour, a nurse and social worker for 30 minutes, anddietitian for 15 minutes. Extra specialty consultationsand tests were scheduled as necessary.
The control group received a geriatric evaluation bya qualified internist, none of whom worked as part ofan interdisciplinary team. These were permitted touse any necessary professional or communityservices to carry out their assessments.
Geriatric Ambulatory ConsultativeService (GACS) compared withusual care� at 8-months there was a trend
for control subjects to havegreater functional and mentalimpairment than the GACSgroup but not significantly so. At12 months meaningfulcomparisons could not bemade because of missing data
� no significant trends forinstitutional placement wereevident between groups.Control subjects were morelikely to be hospitalised thanGACS subjects at 8 and 12months
� over the 12 months the numberof admissions were not differentbetween the two subjectgroups. Average length of staywas 26 days in the GACS groupand 48 days in control group.
� baseline characteristicswere reported to besimilar between the 2groups of patients(except persons livingalone). However thesewere reported post-randomisation after 33%of subjects were lostbefore baselineinformation could beobtained
� adequaterandomisation methoddescribed, investigatorswere blinded to groupallocation for outcomeassessment
� initial high participantlosses may introduceselection bias throughreduction in studypower to detect trueeffects
� validity and reliability ofassessment tools notindicated althoughthese were previouslypublished.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
60
Table 3. Evidence table of specialist geriatric services in outpatient settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Silverman et al. (1995)
RCT, with 12 monthfollow-up.
Pennsylvania, USA
Grade: Level III-1
239 patients in the GAU intervention, mean age75 years, 22% male.
203 patients in the control group, mean age 75years, 17% male.
Inclusion criteriaNon-institutionalised older Medicare/Medicaidpatients aged 65+ years, experiencing instabilityor health status change (deterioration, risk ofinstitutionalisation) in previous 6 months.
Patients were recruited between 1988 and 1991from referrals from participating GAUs,presentations made to senior centers and insenior housing, referrals from friends and relativesof participants, affiliated clinics or hospitals.
Exclusion criteria“Too healthy”, terminal illness, living in nursinghome.
Service and study descriptionOutpatient geriatric assessment units (GAU), aconsultative model based in four geriatricassessment units. These were attached to oneuniversity-based and three community-basedhospitals.
Each site had a core assessment team made up ofan internist trained in geriatrics, a geriatric nurse anda geriatric social worker. The team produced acomprehensive outpatient evaluation of medical,psychological and social health problems andproduced a treatment plan for the patient.
The findings and treatment plan were discussed withpatient and family. The assessment period varieddependent on if extra tests/referrals were required.No rehabilitative services were provided directly bythe assessment units.
Recommendations were communicated to referringphysicians; the unit itself implemented some.
The control group received usual care fromcommunity-based physicians, their own or a choiceof physician from a pool of physicians chosen by thestudy geriatricians.
Outpatient consultative geriatricassessment compared with usualcommunity care.� the outpatient geriatric
assessment resulted in resulted inthe identification of asignificantly greater number ofpatients with cognitiveimpairment, incontinence anddepression
� caregivers had less stress in thegeriatric assessment patientgroup
� there were no differencesbetween groups in terms ofmortality, nursing homeadmissions, cognitive health,functional health, or healthservice utilisation.
� baseline characteristicsreported as similarbetween groups
� possible patientselection bias throughrecruitment methods,payment for patientinvolvement and extrarecruitment to ensureadequate study power
� limited generalisabilityof results of study to theNZ context as entirely inUSA health care setting
� randomisation methodnot adequatelydescribed, unknown ifinvestigators wereblinded to groupallocation for outcomeassessment
� validity and reliability ofassessment tools notreported but most toolswere previouslypublished
� intention to treatanalysis, variablenumbers of the sampleincluded in the variousaspects of the analysis.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
61
Table 3. Evidence table of specialist geriatric services in outpatient settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Toseland et al. (1996) &Engelhardt et al. (1996)
RCT, with 8 monthfollow-up.
New York, USA
Grade: Level III-1
80 patients included in GEM outpatient group,mean age 72 years, 100% male.
80 patients included in usual care group, meanage 72 years, 100% male.
Inclusion criteriaPatient recruited from a Veterans AssociationMedical Center (VAMC) during 1992 usingdatabases to identify patients. Aged 55+ yearsAbove average user of VAMC outpatientservices in previous 12 months, having at least 2ADL or IADL functional impairments.
Exclusion criteriaPatients hospitalised with psychiatric diagnosis inprevious year, cognitive impairment, receivedalternative interdisciplinary or geriatrics care orsubstantial non-VA provider care in past year.
Service description and study descriptionThe GEM team consisted of a geriatrician, a nursepractitioner and a social worker. The geriatriciansupervised the patients’ care plan and ongoingoutpatient treatment. The nurse provided most of themedical care. The social worker assisted patientsand caregivers with psychosocial problems andcoordinated team care.
The team performed an initial CGA (2 hours),developed a care plan, implemented the plan,performed periodic reassessment, monitored andupdated the care plan as required and providedreferral to and coordination with other health andservice providers. Weekly team meetings were heldto discuss assessments and develop plans. Patientswere seen in the GEM clinic for routine follow-up andteam members followed up patient hospitalisations.
Team members also provided emergency care,provided care for patient’s hospitalised forintermediate care, provided treatmentrecommendations for patients hospitalised for acutecare and were also involved in discharged planning.Outpatient care was centralised in the GEM clinic.
Usual care was performed in designated primarycare clinics staffed by internists who did most of theoutpatient care and referrals to specialists and alsonurse support was available.
Outpatient GEM care comparedwith usual care.
Study by Toseland et al. (1996)The outpatient GEM was significantlymore effective than usual care at 8-months:� in reducing mortality� increasing patient satisfaction� improving social quality of social
care� improving the quality of health.
Outpatient GEM was not significantin lowering health care use or thecost of care, which weresignificantly greater than the usualcare group.
Study by Engelhardt et al. (1996)The outpatient GEM was significantlymore effective than usual care at16-months:� improving social quality of social
care� improving the quality of health
but not psychosocial wellbeing.
There was no significant differencein mortality between groups at 16months.
Outpatient GEM was not significantin lowering health care use or thecost of care which were significantlygreater than the usual care groupat 16-months.
� q later study byToseland et al. (1996)used data from thesame trial but wasexcluded as thismostly focused oncost of care andutilisation outcomes.Health and functionalstatus was examinedbut there were nosignificant differencesbetween patientgroups at 2-yearfollow-up
� another study byEngelhardt et al.(1996) used data fromthe same study andevaluated outcomesat 8 and 16 months,These are included inthe outcomes section
� baselinecharacteristicsreported as similarbetween groups
� limited generalisabilityof results of study tothe NZ context asentirely male patientsfrom a VA healthcenter in USA healthcare setting
� randomisationmethod notadequatelydescribed, butinvestigators wereblinded to groupallocation foroutcome assessment.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
62
Table 3. Evidence table of specialist geriatric services in outpatient settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Toseland et al. (1996) &Engelhardt et al. (1996)
RCT, with 8 monthfollow-up.
New York, USA
Grade: Level III-1
(Continued)
� validity and reliabilityof assessment toolsreported and toolswere previouslypublished
� intention to treatanalysis, 88% ofsample included inthe analysis at 8-month follow-up and77% at 16 months.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
63
Table 3. Evidence table of specialist geriatric services in outpatient settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Yeo et al. (1987)
RCT, with 18 monthfollow-up
California,USA
Grade: Level III-1
120 patients in the Geriatric Clinic group (GER),mean age 73 years and 99% male based onthose completing study.
120 patients in the General Medical Clinic(GMC) (control) group, mean age 73 years and99% male based on those who completedstudy.
Inclusion criteriaPatients recruited from a VA center, a primarycare ambulatory clinic in 1979 and 1980. Allpatients aged 65+ consecutively attending.
Exclusion criteriaCognitive impairment based on cutoffs onmental status questionnaire.
Service descriptionThe geriatric clinic (GER) was staffed by two interniststrained in geriatrics, two medical geriatrics fellows (9-month placement), a GNP/geriatric nurse specialist,and a geriatric-trained social worker. The generalmedical clinic GMC was staffed by internists,residents in internal medicine and nurse practitionerson a rotational basis.
Study descriptionIn both the GER and GMC groups patients wereassigned to one primary care provider and givenregular primary care, access to specialty clinics andhospital services. The GER team held weekly casemeetings. The GER group received social workassessments services, this was part of their primarycare and not available to the GMC group in thisform but was available through the VA system.
The GER group also received nursing assessmentsand services, health education and home visits bygeriatric nurse specialists on referral from physicians.These were available to GMC patients.
Geriatric clinic care (GER)compared to general medical cliniccare (GMC).� patients receiving geriatric clinic
care had significantly lessfunctional health decline interms of the total SicknessImpact Profile and its physicaldimension compared topatients at the general medicalclinic
� this was not evident for thepsychosocial dimension, lifesatisfaction, depression, self-rated health, or affect balancewhere there was no significantdifference between groups
� nearly twice as many geriatricpatients died from the GERgroup compared to the GMCgroup.
� baseline characteristicswere described asbeing similar betweenthe 2 groups of patients
� randomisation methodnot adequatelydescribed, unknown ifinvestigators wereblinded to groupallocation for outcomeassessment
� assessment andinterview instrumentswere validated andreliability rated, thesehad been previouslypublished
� high losses to follow-upmay introduce bias inresults as only 68% ofparticipants completedthe study, 64% in theGER group and 72% ofthe GMC group
� limited generalisabilityof results of study to theNZ context as almostentirely maleparticipants in USAVeterans health caresetting.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
64
Table 4. Evidence table of specialist geriatric services in day hospital settings
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Forster et al. (2002)
CochraneSystematic Review
United Kingdom
Grade: level 1
12 RCTs included, with 22 hospitals and 2,867patients.
Search strategyThe Cochrane library, MEDLINE, Sigle, Bids,CINAHL, Index Medicus, InternationalDissertation Abstracts up to January 1997.
Inclusion criteriaOlder medical patients >60 years, prospectivecontrolled trials, day hospital care intervention,and primary outcomes: death, place ofresidence, dependency, global ‘poor’outcomes (death, institutionalisation,dependency), activities of daily (ADL) score,resource use.
Exclusion criteriaTrials evaluating social day centres, psychiatricand single condition day hospitals.
Service and study descriptionGeriatric medical day hospitals. Outpatient facilitywhere older patients receive multi-disciplinaryrehabilitation for a part or full day.
Day hospital c.f. comprehensivecare (5 studies). Day hospital c.f.domiciliary care (4 studies).Day hospital c.f. no comprehensivecare (3 studies).� results show similarity between
geriatric medical day hospitalsand comparable alternativeservices
� medical day hospital moreeffective than no intervention interms of favourable outcomes
� day hospital attendance moreexpensive option but showedreductions in hospital bed useand institutional placement
� medical day hospital has noclear advantage over otherforms of comprehensive olderpersons medical services.
� service design featuresof specialist geriatricservices not describedmaking it difficult todetermine specificservice featurescontributing tooutcomes
� review period spanned30 years of publishedstudies with policychanges and studiesset in multinationallocations
� trials reported to havesmall samples,heterogeneous patientgroups and treatments,missing outcome data
� comparison (control)groups were ‘active’receiving alternativecomprehensive care in9 out of the 12 studies
� studies included in thisreview by Burch et al.(1999), Tucker et al.(1994), and Eagle et al.(1991) were alsoincluded in appraisalsto provide servicedescription information.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
65
Table 4. Evidence table of specialist geriatric services in day hospital settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Burch et al. (1999)
RCT single blinded, with3 month follow-up
Huntington, UK
Grade: Level II
50 patients (day hospital), 40% male, mean age81 years. 55 patients (day centres), 33% male,mean age 80 years.
Inclusion criteriaPatients referred for day hospital bymultidisciplinary team at inpatient dischargeplanning or outpatient assessment.
Exclusion criteriaPatients suffering from dysphasia, requiringnursing, medical procedure, drug monitoring,treatment twice a week or more, specific andfocused occupational therapy.
Service descriptionDay hospital: part of a larger hospital. A 25-placefacility serving mainly rural catchment. To provideshort-term local rehab services for disabled olderpersons.
Social day centre: part of residential homecomplexes. Provide companionship, recreation andcater for long-term attendance.
Study descriptionDay hospital: two-person ambulance collectedpatients who were assessed at arrival by a nurse.One-third received occupational therapy, the restjoined in social, gardening, craft etc. Physiotherapistsassessed patients in afternoon and devisedpragmatic individualised plans. Short-term care.
Day centres (2): 5 places on 2 days a weekavailable. Volunteer driver picked patients up inmini-bus. These were assessed and treated by asenior physiotherapist and two health supportworkers. Individual plans formulated. Long-termattendance care envisaged.
Patient’s randomised to day hospitalrehabilitation versus day centrerehabilitation.� both groups improved but no
statistically significant differencewas found in functional ability,morale or caregiver strainbetween the two settings
� day centre rehab was lesspopular and had practicaldifficulties – e.g., lack of spaceand equipment, transportdifficulties, differing healthservice philosophies to dayhospital care. Also, patientperception of day centre aslower standard of care than dayhospital.
� both patient treatmentgroups were similar atbaseline
� compliance, retentionand recruitmentproblems of very old inRCTs of rehabilitation
� adequaterandomisation method,single blinding
� high number of patientexclusions and losses tofollow-up reducedstudy power to detecttrue differencebetween interventions.Short follow-up period
� interventions notconsistent as the dayhospital group alsoreceived occupationaltherapy.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
66
Table 4. Evidence table of specialist geriatric services in day hospital settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Eagle et al. (1991)
RCT, with 3, 6 and 12month follow-up
Ontario, Canada
Grade: Level III-1
55 patients in treatment (day hospital) group,mean age 80 years, 36% male. 58 patients incontrol (inpatient unit or outpatient clinic) group,mean age 78 years, 43% male.
Inclusion criteriaCommunity dwelling subjects referred to twoDay hospital consultant geriatricians betweenApril 1986 and October 1987 or were about tobe discharged from an acute-care inpatientsetting. Day hospital eligibility included impairedfunction and no acute illness and positiveprognosis for long-term improvement.
Exclusion criteriaPatients with life expectancy of less than 6months.
Service descriptionA Day hospital established in 1984 as part of largeUniversity teaching hospital. The facilities includedareas for physical and occupational therapy, livingroom, indoor garden, workshop, crafts room kitchenand communal dining area.
Study descriptionPatients attended Day hospital 2 days per week,each visit for 4-5 hours. An interdisciplinary teamassessed physical, mental, and emotional functionand medical diagnoses and needs, social and familyrelationships.
The team consisted of a Day hospital physician (aphysician with additional training in geriatricsresponsible for on-going care and managementplan implementation), 3 RNs (one of whom was thenurse coordinator, two were part-time), an RNassistant, occupational, physical and speechtherapists (there on most days), a nutritionist, socialworker and a pharmacist (available when needed).
After the assessment phase involving 1-3 visits, theteam met to plan the required therapeutic andrehabilitative services. Discharge planning withrelatives and caregivers and follow-up home care asrequired.
The control group received conventional care ineither an inpatient geriatric assessment unit (CGA) orin an outpatient geriatric clinic with limiteddiagnostic and rehabilitative opportunities or earlydischarge from an inpatient unit and communityfollow-up service.
Day hospital care with multi-disciplinary care team (Intervention)versus conventional care frominpatient unit or outpatient clinic orearly discharge with requiredcommunity services follow-up(Control).� no significant difference in the
number of deaths betweengroups
� no significant difference infunctional status between thewtwo groups. Functional statusdid deteriorate in both groups(less in the control group) overthe 12 months
� no significant differencesbetween groups in the ability toperform daily living activitiesand in reduction of symptomsover time (using a local GeriatricQuality of Life Questionnaire –GQLQ)
� a significant treatment effectwas evident in favour of thecontrol group on the emotionsdimension of the GQLQ.
� both groups had similarbaseline characteristics
� randomisation methodnot clearly described.No blinding ofinvestigatorsadministeringquestionnaires andinstruments to groupallocation
� generally the samehealth professionalsprovided care to thesubjects of both groups
� those patients who diedduring the study werenot included in theanalysis, the differencein deaths favoured thecontrol group but wasnot consideredsignificant in terms ofbias in results
� the control group’saccess to care was nothindered by financialrestraints, waiting timesand all subjects wereassessed by anexperiencedgeriatrician.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
67
Table 4. Evidence table of specialist geriatric services in day hospital settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Pitkala (1998)
RCT, with 2, 5 and 12month follow-up
Kirkkonummi-Siunto,Finland
Grade: Level III-1
88 patients in the intervention group, mean age77 years, 30% male. 86 patients in control group,mean age 77 years, 40% male.
Inclusion criteriaChronically ill patients receiving home healthcare in 2 rural communities in Finland.
Exclusion criteriaNone specified.
Service descriptionA new geriatric 10-bed day hospital was establishedat a primary health center in a rural area.
Study descriptionThe intervention group received a 2-month period ofrehabilitation and medical care in the new dayhospital and assessment at 2, 5 and 12 months. Theday hospital provided medical care, nursingassessment and care, with attendant doctorsexamining patients daily and a visiting consultantonce per week. Also intensive physiotherapy, OT,Speech therapy and consultation with social workersprovided, according to specific individual needsprograms.
The control group of patients were treated as theyhad been before the opening of the Day hospitalwith home health care and referrals to hospital oroutpatient care.
The intervention group receivedrehabilitation and medical care inthe day hospital versus a controlgroup who received home healthcare and when required, referral toa hospital or outpatient care.� the intervention group had a
significantly greater number ofspecialist consultations (outsideof day hospital) than the controlgroup. No significantdifferences between groups inthe physical functioning ADLindex but more changes frombaseline in intervention group
� the intervention group had asignificantly reduced number ofsymptoms than the controlgroup
� both groups had a similarnumber of hospital bed-daysand number of GP visits (outsideof day hospital).
� both groups had similarcharacteristics atbaseline, except thatthe intervention grouphad a significantlygreater level of needaccording to the ADLindex
� positive changes in theactivities of daily livingindex for theintervention group likelyreflect the high initialbaseline level of need
� inadequaterandomisation methodand description,patients randomisedaccording to date ofbirth
� not clear whetherinvestigators wereblinded to patientallocation
� high losses to follow-uppost-randomisation,intention to treatanalysis included thosepersons refusing theintervention, which maynullify the true effect.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
68
Table 4. Evidence table of specialist geriatric services in day hospital settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Tucker et al. (1984)
RCT, with 6 week and 5month and 78 weekfollow-up
Auckland,New Zealand
Grade: Level III-1
62 patients were included in the interventiongroup, mean age 73 years, 46% male.
58 patients were included in the control group,mean age 72 years, 50% male.
Inclusion criteriaPatient referrals (from hospital 40% andcommunity 60%) aged over 55 years living in thecatchment area of the geriatric unit requiringassessment and rehabilitation (but not 24-hourinstitutional care). Patients admitted to dayhospital between July 1981 and July 1982.
Exclusion criteriaDementia patients and patients with high socialday care and family relief needs.
Service descriptionA 10-bed day hospital attached to the geriatric unitof Auckland hospital was opened in 1981.
Study descriptionPatients were randomised at first assessment into dayhospital or control groups. The day hospital patientsattended 2-3 days per week between 0830 to 1400hours. The hospital provided intensive physiotherapy,OT, speech therapy, medical and nursing assessmentand supervision over a period of 6-8 weeks.
During the trial a total of 93 new patients attendedthe day hospital (59 in the trial and 34 not). The totalnumber of attendance’s during the period was 2176(mean per patient 23).
Control group patients were cared for as they werebefore the Day hospital was opened. This includedadmission to hospital, continued inpatientmanagement, outpatient follow-up with/withoutphysiotherapy, referral to the sole care of their GP orreferral to day care. Placement was decided beforerandomisation.
The intervention group received Dayhospital care versus a control group,which received standardinpatient/outpatient care.� day hospital patients showed a
significant improvement in theactivities of daily living (ADL) at6 weeks but this was not evidentat 5 months
� day hospital patients had asustained improvement in moodcompared to the control group
� day hospital rehabilitation costswere one-third greater thanrehabilitation alternatives in thecontrol group (over 35-weekperiod of trial patient usageonly)
� these were $3,052 per patientversus $2,083 for the controlgroup.
� both groups had similarbaseline characteristics
� randomisation methodis described. It is notclear whetherinvestigators wereblinded to groupallocation
� assessment tools validityand reliabilityreferenced, howevershortened version of theADL index used was not
� only a limiteddescription of theservices provided to theDay hospital group andcontrol group isprovided
� patients lost to follow-up were not included inthe analysis, but thesmall numbers areunlikely to haveaffected study results.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
69
Table 4. Evidence table of specialist geriatric services in day hospital settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Siu et al. (1994)
Retrospectivecomparative cohortstudy, 1 yearretrospective follow-up
Los Angeles,USA
Grade: Level III-2
199 patients in day hospital patient group, meanage 81 years, 24% male.
269 patients in a clinic patient group, mean age80 years, 24% male.
Inclusion criteria(General cohort) all new patients seen for CGAin a 12-month period by geriatricians in ageriatric day hospital and in two other clinic siteswithout a day hospital.
(Restricted cohort) all of above plus 65+ yearsage, limitation in at least 1 area of basic ADL or2+ areas of instrumental ADL, residence inenvironment providing personal assistance.
Exclusion criteria(General cohort) patients for whom it wasdifficult to obtain data, patients seen for reasonsother than assessment.
Service descriptionThe geriatric day hospital had a day room, 10-beds,a nursing station, rehab area and offices for staff.On average 18 patients were seen per day. The unitwas staffed by an interdisciplinary team, includingnurse practitioners, geriatricians, nurses, socialworkers, physical therapists, OTs, and speechtherapists. Consultant psychiatrists and othermedical specialists were available. Close medicalobservation could be performed and acute nursingcare could take place all day at the day hospital.Patients needing multiple diagnostic tests, acutely illpatients not requiring overnight admission, andpatients requiring frequent intensive physical, speechand OT therapy could all receive coordinated careat the day hospital.
Patients attended day hospital during the day,returned home at night and returned for continuingcare as needed. Most patients only made one ortwo visits while 24% visited 4+ times per year. Patientswere also referred to social services in thecommunity.
Study descriptionSubjects were contacted after first visit, and baselinedata of included patients reviewed from medicalrecords by nurse practitioner blinded to researchquestion. After 6 months patients were interviewedby telephone. Analysis of outcomes performed at 3levels. A full cohort of all referrals, restricted cohortwith defined inclusion criteria and restricted cohortwith severity adjustment using multivariate methods.
Two other geriatric medicine clinic sites were used ascomparators, these were staffed by medicalresidents, fellows, a nurse practitioner andgeriatricians. Consultations from other specialtieswere available by referral.
CGA in a geriatric day hospitalcompared with assessmentreceived in a University based clinicand a community-based cliniccombined.� patients in the day hospital
group were significantly morelikely to receive psychiatry,specialised nursing, and socialwork services than the two clinicpatient groups. There was nosignificant difference in thereceipt of rehabilitative services.This was observed for all cohortlevels of analysis
� day hospital patients were morelikely to be in a nursing homeand more likely to have movedinto higher levels of care at 6months than clinic patients.Adjusted results showed therewas no significant difference
� no significant difference wasapparent between patients at 6months in responses to questionson health compared to oneyear ago
� adjusting for baselinecharacteristics Day hospital hadno significant effect onmortality, use of emergency orhospital services at 6 months.
� patient groups at theday hospital and 2clinics combined hadmostly similar baselinecharacteristics whenthe full cohort andrestricted cohort wereanalysed separately
� day hospital patientshad significantlygreater homeassistance, dementia,depression and ADLdependence than theclinic patients in bothcohorts
� possible patientselection bias in cohort,though sensitivity testsnot significant in choiceof inclusion criteria
� retrospective analysis ofmedical records andtelephone survey data.Outcomes derived andextraction of data frommedical records andsurvey not validated.Missing data was notsignificant
� validity and reliability ofco-morbidity andhealth statusassessment tools notindicated althoughthese were previouslypublished.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
70
Table 4. Evidence table of specialist geriatric services in day hospital settings (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Malone et al. (2002)
Quasi-experimental,prospective beforeand after study with 3month follow-up
Vancouver,Canada
Grade: Level IV
41 patients included, mean age 81 years, %male unknown.
Inclusion criteriaConsecutive patients discharged from dayhospital between August 1999 and March 2000who attended at least 5 visits.
Exclusion criteriaNone specified.
Service and study descriptionA University affiliated geriatric day hospital thatadmits 165 patients annually. Staff of the unit madeup of geriatricians, nurses, rehab assistants, a socialworker, an OT, a physiotherapist andneuropsychologist. Referrals to the day unit are forinterdisciplinary assessment and management of“complex medical, social, psychiatric and functionaldifficulties”. Historically the unit has focused uponmedical diagnosis and the management of chronicdiseases.
Patients discharged from dayhospital and followed-up at 3months. Measurements were madeat admission, discharge and 3month follow-up.� between admission and
discharge there were significantimprovements in measures ofmobility, balance, cognitionand depression scales. Fromadmission to 3-month follow-upcognition measures declined,depression measures improvedand were constant for all otheroutcomes
� improvements were notmaintained from discharge tofollow-up and declined formeasures of mobility, balance,and cognition with no significantchange for depression andfunctional status.
� descriptive study withno control orcomparison group. Anintervention not tested
� validity and reliability ofassessment tools notindicated althoughthese were previouslypublished
� no blinding to outcomeassessment
� lack of servicedescription makes itdifficult to assignoutcomes to specificfeatures of the dayhospital service.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
71
Table 5a. Evidence table of specialist geriatric services in community/clients own homes – preventive services
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Stuck et al. (2002)
Systematic Review
BernSwitzerland
Grade: Level I
Inclusion criteriaRCTs testing in-home interventions for olderpersons published in English. French, Spanish,German, Italian through searches in MEDLINE,EMBASE, and PSYCHINFO. January 1985-November 2001. Cochrane trials register,reference lists, conference proceedings.
Exclusion criteriaNone stated.
Trial data were extracted and themethodological quality of the trial assessed.Meta-regression analysis was also performed.
Preventive in-home service and study descriptionPreventive in-home visits using multidimensionalgeriatric assessment and frequent follow-up for olderpeople on functional status, nursing home admissionand mortality.
Some 1,349 abstracts screened and a total of 18trials were included, with 13,447 persons aged 65years and over. These patients were selected fromgeneral practice lists or insurance registers.
Effect of preventive in-home visits onfunctional status, nursing homeadmission and mortality.� on nursing home admissions: 13
trials, reduction modest, butassociation of treatment effectwith number of follow-up homevisits. Stratified analysis of thenumber of visits showsreductions in admissions only forprograms of >5 visits
� on functional status: 16 trials,little effect on functional status,but study results heterogeneous.In meta-regression analysis somebeneficial effects associatedwith multidimensional geriatricassessment with follow-up andinversely correlated with control-group mortality
� on mortality: 18 trials, somereduction in mortality butheterogeneous study results.Mean age <80 years negativelyassociated with effects onmortality.
� limited descriptions ofin-home visitingservices, patientpopulations and controlgroups
� according to authorsmeta-regressionanalysis showed littleevidence ofmethodological qualityaffecting results norfunnel plot asymmetry
� study resultsheterogeneous butmeta-regressionanalysis used to controlfor this
� limited generalisabilityas this analysis limited topreventive homevisitation programmesand excludes home-based carecoordinationprogrammes forpatients dischargedfrom hospital.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
72
Table 5a. Evidence table of specialist geriatric services in community/clients own homes – preventive services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Fabacher et al. (1994)
RCT, with 1 yearfollow-up
Los Angeles,USA
Grade: Level II
131 subjects were included in the intervention(HAPSA) group, mean age 74 years, 98% male.123 subjects were included in the control group,mean age 72 years, 98% male.
Inclusion criteriaCommunity dwelling veterans aged 70+ yearsand not currently receiving outpatient healthcare.
Exclusion criteriaSubjects suffering from terminal disease,dementia, planning to move away.
Preventive in-home service descriptionThe Home Assessment Program for Successful Aging(HAPSA) was developed in 1988. It was adaptedfrom the Department of Veteran Affairs health caresystem. It was set up to evaluate effectiveness ofpreventive home visits in health and functionimprovement.
Study descriptionEligible subjects in the HAPSA group received an in-home multi-dimensional assessment that wasperformed by a physician’s assistant or researchnurse trained in geriatrics. Following assessment theresearch staff in consultation with a geriatricianprepared a written communication describingfindings for the subject who was encouraged todiscuss it with their personal physician.
Following this 4-monthly follow-up was performed byvolunteers (retired social workers and nurses) andstaff members in order to assist with compliance,identify new problems and provide healtheducation. Information was collected via astructured interview, an abbreviated version of initialinterview.
The control group received only telephone interviewsat 4-month intervals.
The intervention group received in-home assessment and follow-upversus the control group whoreceived only telephone interviews.� at 12 months intervention group
subjects had significantlygreater immunization rates, agreater likelihood of having aprimary care physician, higherfunctional status (IADL) scoresand maintenance offunctionality than the controlgroup
� in the intervention group anaverage of 4 new or partiallytreated problems wereidentified and subjectcompliance withrecommendations to see aphysician or initiate a healthpractice was 76%
� hospitalisation rates were similarbetween the two groups, nosubjects were admitted to anursing home.
� both subject groupssimilar at baseline
� adequaterandomisation methoddescribed, unclear ifinvestigator(s) wereblinded to groupallocation
� study generalisabilitymay be limited due tosubject selection ofrelatively healthy whitemale veterans
� losses to follow-upreported, 24% and 23%in respective groups,these were notincluded in the analysisof outcomes at 12months, no intention totreat analysis
� validity and reliability ofassessment tools notindicated althoughthese were previouslypublished.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
73
Table 5a. Evidence table of specialist geriatric services in community/clients own homes – preventive services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Hogan et al. (2001)
RCT, single blinded,3, 6 & 12 month follow-up
Calgary,Canada
Grade: Level II
79 subjects in intervention group, mean age 77years, 45% male.
84 subjects in control group, mean age 78 years,38% male.
Inclusion criteriaCalgary community dwelling, ambulatorypatients 65+ years old who had fallen in theprevious 3 months, recruited between June 1997and June 1999.
Exclusion criteriaSubjects having falls during vigorous or high-riskactivities.
Preventive in-home service and study descriptionSubject were visited and followed up by a researchassistant blinded to allocation. An assessor visitedsubjects assigned to the intervention group at home.The assessors were specialists in geriatric medicine, 2nurses, 2 OTs and physiotherapist. The initial visit took1-2 hours, and all assessors met to discuss and agreeon individualised plans to decrease subjects risk offalling. Recommendations were communicated inwriting to the patient, attending physician. Assessorsdid not implement recommendations other thanreferring some subjects to exercise classes.
The Control group received a home visit from arecreational therapist who performed a leisureassessment. A letter was sent to control the subject’sattending physician.
An in-home intervention ofassessment and individualisedtreatment plans versus usual care� no significant differences
between intervention andcontrol groups in the number ofcumulative falls, one or morefalls or mean number of falls
� there was a significantly longertime in the intervention groupbetween falls than in the controlgroup
� subjects with 2 or more falls inthe 3 months preceding thestudy assigned to theintervention group weresignificantly less likely to fall anda had longer time between falls
� no significant differencesbetween groups in health careusage.
� both patient groupssimilar at baseline.Adequaterandomisation methoddescribed, singleblinding with outcomesdata collected byinterviewer blinded togroup allocation
� possible patientselection bias as limiteddescription of studypopulation source andpre-studycare/dischargeregimen
� study withdrawals were16% from theintervention group and13% from the controlgroup. Intention to treatanalysis.
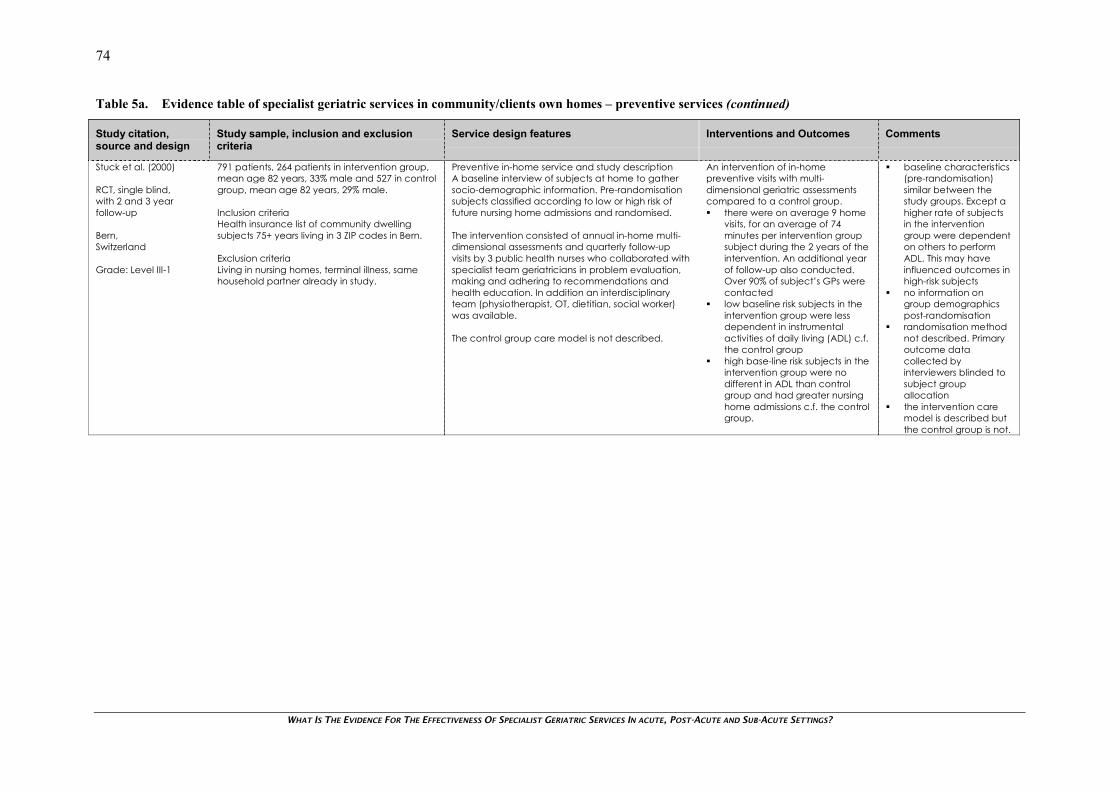
WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
74
Table 5a. Evidence table of specialist geriatric services in community/clients own homes – preventive services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Stuck et al. (2000)
RCT, single blind,with 2 and 3 yearfollow-up
Bern,Switzerland
Grade: Level III-1
791 patients, 264 patients in intervention group,mean age 82 years, 33% male and 527 in controlgroup, mean age 82 years, 29% male.
Inclusion criteriaHealth insurance list of community dwellingsubjects 75+ years living in 3 ZIP codes in Bern.
Exclusion criteriaLiving in nursing homes, terminal illness, samehousehold partner already in study.
Preventive in-home service and study descriptionA baseline interview of subjects at home to gathersocio-demographic information. Pre-randomisationsubjects classified according to low or high risk offuture nursing home admissions and randomised.
The intervention consisted of annual in-home multi-dimensional assessments and quarterly follow-upvisits by 3 public health nurses who collaborated withspecialist team geriatricians in problem evaluation,making and adhering to recommendations andhealth education. In addition an interdisciplinaryteam (physiotherapist, OT, dietitian, social worker)was available.
The control group care model is not described.
An intervention of in-homepreventive visits with multi-dimensional geriatric assessmentscompared to a control group.� there were on average 9 home
visits, for an average of 74minutes per intervention groupsubject during the 2 years of theintervention. An additional yearof follow-up also conducted.Over 90% of subject’s GPs werecontacted
� low baseline risk subjects in theintervention group were lessdependent in instrumentalactivities of daily living (ADL) c.f.the control group
� high base-line risk subjects in theintervention group were nodifferent in ADL than controlgroup and had greater nursinghome admissions c.f. the controlgroup.
� baseline characteristics(pre-randomisation)similar between thestudy groups. Except ahigher rate of subjectsin the interventiongroup were dependenton others to performADL. This may haveinfluenced outcomes inhigh-risk subjects
� no information ongroup demographicspost-randomisation
� randomisation methodnot described. Primaryoutcome datacollected byinterviewers blinded tosubject groupallocation
� the intervention caremodel is described butthe control group is not.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
75
Table 5a. Evidence table of specialist geriatric services in community/clients own homes – preventive services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Stuck et al. (1995)
RCT, single blinded,3 year follow-up
California,USA
Grade: Level II
215 subjects in intervention group, mean age 81years, 31% male.
199 subjects in control group, mean age 81years, 29% male.
Inclusion criteriaSanta Monica voter registration list, personsaged 75+ years living at home.
Exclusion criteriaSevere cognitive difficulties, plans to move awayor into a nursing home, terminal illness.
Preventive in-home service descriptionCGA model identifying problems and risk for futuredisability, development of recommendations andsubject adherence. Model attempted to test thatimportant problems were identified from all domains(medical, social, mental health, functional) of theCGA, a consistent incidence of new problems wereidentified and recommendations made, repeatedreinforcement via follow-up visits.
Study descriptionGerontologic nurse practitioners (GNPs) inconsultation with geriatricians administered CGAs tointervention subjects in their homes annually for 3years. Subjects continued with their usual healthcarefrom community physicians. Annual visits included aCGA and based on identified problems,recommendations were made. Also healtheducation was provided GNPs performed thee-monthly follow-up visits to reinforce previousrecommendations and determine adherence.Subjects were encouraged to take active andprimary role in their healthcare, GNPs andgeriatricians only contacted subjects’ physicians incomplex situations.
Control group subjects received regular medicalcare.
Intervention group received annualin-home CGA by GNPs incollaboration with geriatriciansevaluating problems, providingrecommendations and healtheducation versus a control groupthat received usual medical care.� no significant difference
between groups in the numberof subjects dependent onassistance in performinginstrumental activities of dailyliving (ADL)
� intervention group hadsignificantly less subjectsdependent on basic ADL,permanently admitted tonursing homes and more visits toGPs (in 2nd and 3rd years) thancontrol group
� no significant differencebetween groups in acute carehospital admissions, short-termnursing home admissions insecond and third year of studyand in-home communityservices usage (over 3 years).
� both patient groupssimilar at baseline.Adequaterandomisation methoddescribed, singleblinding with outcomesdata collected byinterviewersindependent from study
� intention to treatanalysis performed,however at 3-yearfollow-up significantlosses (21%) inintervention group and(26%) in control group
� degree of specialistgeriatric serviceinvolvement not clearlydetermined in thisstudy. May be of limitedrelevance to topic
� validity and reliability ofassessment tools notindicated althoughthese were previouslypublished
� GNPs collected mostdata and these alsoprovided theintervention, whichcould promote bias intheir reporting of results
� also refer toprospective study byAlessi et al. (1997) whichprovides detailedanalysis of theintervention arm of thisstudy.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
76
Table 5a. Evidence table of specialist geriatric services in community/clients own homes – preventive services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Bernabei et al. (1998)
RCT, with 12 monthfollow-up
A town (Rovereto) inNorthern Italy
Grade: Level III-1
99 patients, mean age 81 years, 30% male inintervention group.
100 patients, mean age 81 years, 29% male incontrol group.
Inclusion criteriaAll people over 65 years who were in homeassistance programmes or received homehealth services whose evaluation precedingcare planning was not CGA.
Exclusion criteriaNone specified.
Preventive in-home service descriptionHealth agency of Rovereto (popn 35,000) created inearly 1990’s array of health services for older people.Including a GEU, skilled nursing facility and homehealth agency. No coordination of these, norintegration with social services.
Study descriptionThe intervention group received case managementand care planning by the community geriatricevaluation unit and GPs. All necessary servicesprovided in integrated fashion after agreementbetween local health agency and municipality. In all21 GPs took part and GEU staff of a geriatrician,social worker, several nurses. Also 2 case managersappointed and trained who did initial assessmentand every 2 months thereafter.
Control group received primary and communitycare with conventional and fragmentedorganisation of services including GPs regularambulatory and home visits, nursing, social services,home aids and meals on wheels.
Randomisation to intervention groupreceiving integrated social andmedical care and casemanagement versus a controlgroup receiving conventional care.� survival analysis showed later or
less common admission tohospital or nursing home inintervention group comparedwith control group
� health services were used to thesame extent between the twogroups, controls received morehome visits from GPs
� intervention group hadimproved physical function andfewer declines in cognitivestatus than control group
� per capita costs over periodwere 23% less than controlgroup, or 1,125 pounds perindividual per year of follow-up.
� both patient groupssimilar at baseline
� validity and reliability ofassessment tools notindicated althoughthese were previouslypublished
� randomisation methoddescribed, but allprofessionals aware ofpatent allocation butblinding to outcomeassessment as baselineand final assessmentsperformed by staff notinvolved in assessmentand treatment of theintervention group
� possible contaminationbias as GPs followedpatient from bothgroups.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
77
Table 5a. Evidence table of specialist geriatric services in community/clients own homes – preventive services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Rockwood et al. (2000)
RCT single blinded, with3, 6 and 12 monthfollow-up
Nova ScotiaCanada
Grade: Level III-1
95 patients (MGAT care), 57% male, mean age81 years, 87 patients (usual care), 58% male,mean age 82 years.
Inclusion criteriaCommunity dwelling older patients of ruralfamily practitioners in 3 counties. Patients invulnerable state of health, social problems or riskof decline in functionality.
Exclusion criteriaNone specified.
Preventive in-home service and study descriptionMobile Geriatric Assessment Team (MGAT) consistingof 2 geriatric nurse assessors (GNA), 4 geriatricians, aphysiotherapist, occupational therapist, socialworker, dietitian, audiologist, speech-languagepathologist.
Post-randomisation a GNA visited patients at hometo determine if interdisciplinary care required. TheGNA completed a standard CGA. Within 1 weeknurse met with the geriatrician (blind to groupallocation) to review CGA and baseline needs andset patient-centred goals using the primary outcomeGoal Attainment Scaling (GAS). These includedoutcomes of care, process issues and preventivepractises. Goals finalised at team conference afterwhich group allocation revealed.
Intervention group received MGAT care over first 3months with an average of 3 interdisciplinary consultsand average of 2 follow-up visits. MGAT performedmore detailed, discipline specific assessments andinterventions for up to 3 months than control group.
Control group received usual care and primary carephysician was routinely informed of allocation.Follow-up assessments performed by GNA at 3, 6,and 12 months blind to group allocation.
Patients randomised to MGAT caregroup versus usual care group totest CGA as an adjunct to usualcare.� over 12 months intervention
MGAT care group was morelikely to attain their outcomegoals than the control group
� standard assessments offunction, cognition and qualityof life showed no differencebetween groups over 12 months
� no difference between groupsin survival or time toinstitutionalisation.
� both patient groupssimilar at baseline
� randomisation methodnot described, singleblinding
� usual care not welldescribed
� CGA tools and goalachievement toolspreviously validated.Reliability ofassessments tested.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
78
Table 5a. Evidence table of specialist geriatric services in community/clients own homes – preventive services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Tinetti et al. (2002)
Matched prospectivecontrolled trial
Connecticut,USA
Grade: Level III-2
691 matched pairs (age, sex, race, baseline self-care function, cognitive status etc) of patientsfor the restorative (1 office) and usual care (5offices) from six home care agency offices.Mean age 79 years, 41% male.
Inclusion criteriaPatients 65+ years receiving home care (at least7+ days) from the restorative care office,November 1998 to 30th April 2000.
Exclusion criteriaSevere cognitive impairment, terminal illness,requiring total care.
Preventive in-home service and study descriptionA Connecticut home-care agency providingrestorative care. Nursing, OT and physiotherapy andhome health aides under the approval of patients’physicians and also Medicare regulations.
Restorative care strategy: diagnosis and treatmentof individual diseases/impairments, multi-facetedcare plan addressing these diseases, impairmentsetc and patient centered goal setting and processdetermination.
Restorative care model:� training of home care nurses, therapists and
aides in rehab, geriatric medicine and goalattainment
� integrated, coordinated interdisciplinary teamwith shared goals
� reorientation of home care team focus towardsmaximising function and comfort
� patient/family centered goals and agreementbetween these and home-care staff
� self-care progress report helped identify goals,baseline/standardise assessment and clarifycare responsibility. Treatment programmecomprised of combinations ofexercise/training/counseling/support/training/education of patient/family/medicationadjustments.
Usual care practices in home care offices weredirected by medical order developed to managespecific diseases. Nurses and therapists made effortsto communicate regularly.
Restorative home-care modelcompared with usual home-care.� after adjusting for baseline
characteristics, restorative carewas associated with a greaterlikelihood of being at home,reduced likelihood of visiting anED, and shorter home careepisodes than usual home care
� restorative care patients afterbaseline adjustment had bettermean scores in self care, homemanagement, and mobility.
� baseline characteristicswere matched onseven characteristics
� assessment ofoutcomes wasperformed by differentstaff members providingcare and may besubject to potentialrecording bias
� limited information onreliability and validity ofassessment instrument.This was previouslytested in pilot study,one other reference tocited
� single home-careagency may limit thegeneralisability of thisstudy to all home-carepatients.
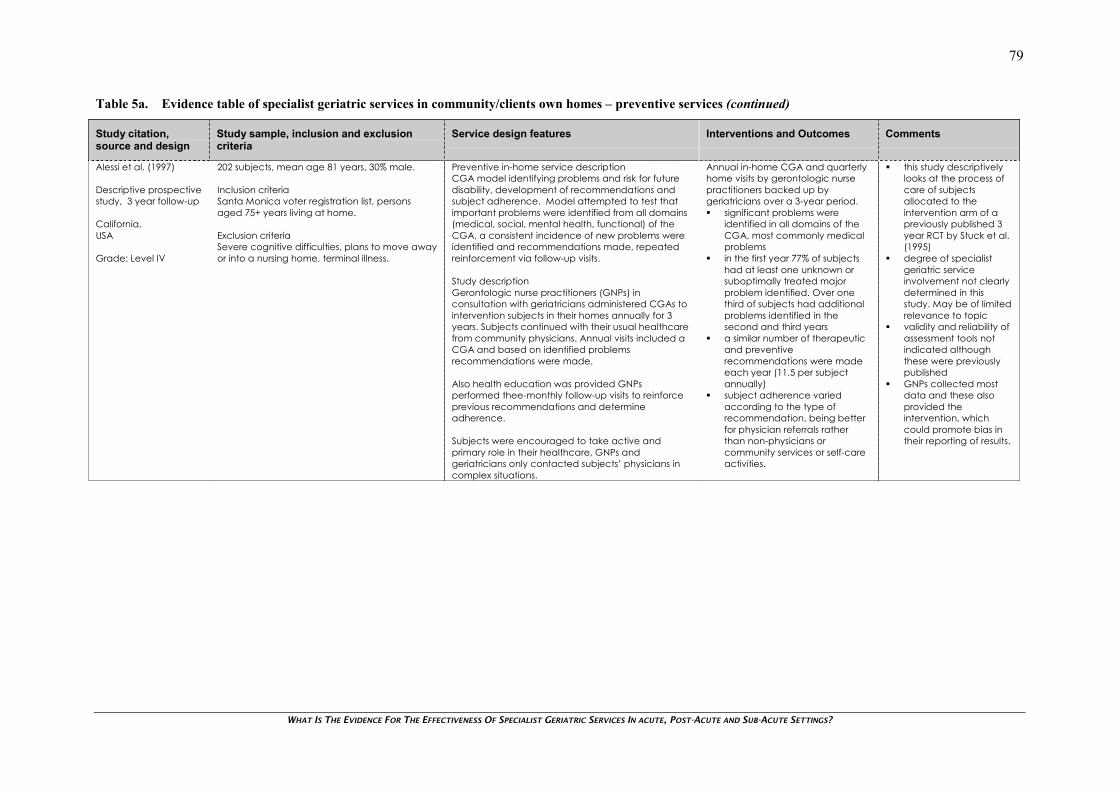
WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
79
Table 5a. Evidence table of specialist geriatric services in community/clients own homes – preventive services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Alessi et al. (1997)
Descriptive prospectivestudy, 3 year follow-up
California,USA
Grade: Level IV
202 subjects, mean age 81 years, 30% male.
Inclusion criteriaSanta Monica voter registration list, personsaged 75+ years living at home.
Exclusion criteriaSevere cognitive difficulties, plans to move awayor into a nursing home, terminal illness.
Preventive in-home service descriptionCGA model identifying problems and risk for futuredisability, development of recommendations andsubject adherence. Model attempted to test thatimportant problems were identified from all domains(medical, social, mental health, functional) of theCGA, a consistent incidence of new problems wereidentified and recommendations made, repeatedreinforcement via follow-up visits.
Study descriptionGerontologic nurse practitioners (GNPs) inconsultation with geriatricians administered CGAs tointervention subjects in their homes annually for 3years. Subjects continued with their usual healthcarefrom community physicians. Annual visits included aCGA and based on identified problemsrecommendations were made.
Also health education was provided GNPsperformed thee-monthly follow-up visits to reinforceprevious recommendations and determineadherence.
Subjects were encouraged to take active andprimary role in their healthcare, GNPs andgeriatricians only contacted subjects’ physicians incomplex situations.
Annual in-home CGA and quarterlyhome visits by gerontologic nursepractitioners backed up bygeriatricians over a 3-year period.� significant problems were
identified in all domains of theCGA, most commonly medicalproblems
� in the first year 77% of subjectshad at least one unknown orsuboptimally treated majorproblem identified. Over onethird of subjects had additionalproblems identified in thesecond and third years
� a similar number of therapeuticand preventiverecommendations were madeeach year (11.5 per subjectannually)
� subject adherence variedaccording to the type ofrecommendation, being betterfor physician referrals ratherthan non-physicians orcommunity services or self-careactivities.
� this study descriptivelylooks at the process ofcare of subjectsallocated to theintervention arm of apreviously published 3year RCT by Stuck et al.(1995)
� degree of specialistgeriatric serviceinvolvement not clearlydetermined in thisstudy. May be of limitedrelevance to topic
� validity and reliability ofassessment tools notindicated althoughthese were previouslypublished
� GNPs collected mostdata and these alsoprovided theintervention, whichcould promote bias intheir reporting of results.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
80
Table 5a. Evidence table of specialist geriatric services in community/clients own homes – preventive services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Hui & Woo (2002)
Descriptive study, 12months follow-up
Hong Kong
Grade: Level IV
200 patients resident at a nursing home, meanage 82 years, ration of male to female 1:2.Project lasted from July 1998 to June 1999.
Inclusion criteriaAdequate score in an abbreviated mental test,tele-consultation use recall and communicationability.
Exclusion criteriaNone specified.
Preventive in-home service descriptionShatin hospital, Hong Kong with an outreach CGATsupporting 21 nursing homes with 3000 residents. Theteam consisted of a part-time geriatrician andpyschogeriatrician, a nurse with geriatrics training, aphysiotherapist and OT, and a podiatrist.
Study descriptionThe use of video-conferencing for service delivery toa 200-bed nursing home serviced by the CGAT.Videoconferencing equipment was installed at thehospital and nursing home. High-resolution cameraequipment was used and a computer wasconnected to the view station at the hospital fordownloading photographs.
A research nurse was assigned to the nursing homefor project coordination. The CGAT participated inthe project with the addition of a dermatologist usingrealtime tele-consultation instead of face-to-faceconsultations. The service was for patients with newproblems and follow-up and operated in office hoursduring weekdays.
After every tele-consultation the team evaluatedwhether this was sufficient to replace normaloutreach or clinic consults. Follow-up face-to-faceconsults were conducted the next day if necessary.The dermatologist and podiatrist assessed each caseby both consult methods.
Overall, 1,001 tele-consultationswere made over the study period.� the feasibility of consults by
discipline ranged from 60% (OT),74% (dermatologist), 85%(podiatrist), 87%(physiotherapist), 89% (nurse),97% (geriatrician), 99% for thepsychogeriatrician
� compared to conventionalservices operating costs werelower for telemedicine, as wereemergency departmentattendances, and bed-days inacute hospital
� 96% of resident respondents feltcomfortable with the service
� limitations by discipline wereevident, with chest auscultationand physical examination ofnew patients, wounds, chestphysiotherapy, massagetherapy, and some OT etcrequiring hands-on treatment.
� descriptive study withno comparison orcontrol group. Nomeasures of statisticalprecision provided,intervention not tested
� probable patientselection bias asintervention at onenursing home
� the “feasibility” ofconsults was notadequately defined asan outcome measure
� longer term QoL,mobility outcomes etcnot evaluated
� patient satisfactionsurvey not validatedand reliability nottested.
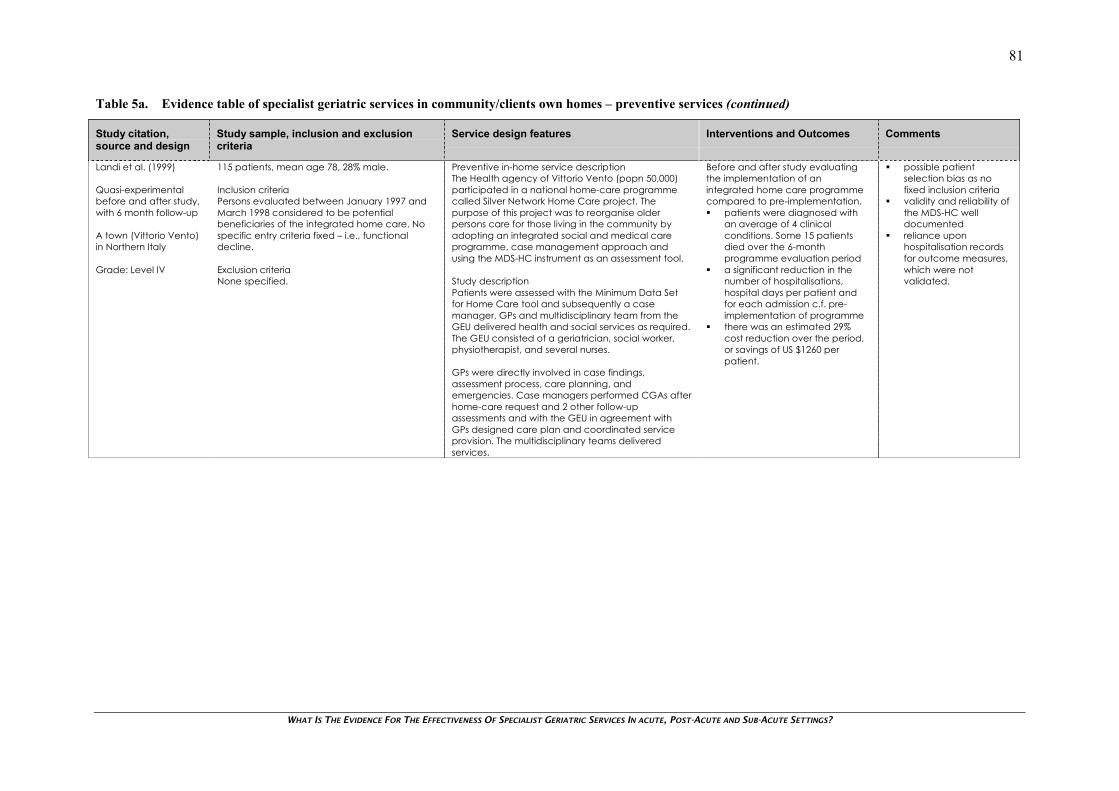
WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
81
Table 5a. Evidence table of specialist geriatric services in community/clients own homes – preventive services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Landi et al. (1999)
Quasi-experimentalbefore and after study,with 6 month follow-up
A town (Vittorio Vento)in Northern Italy
Grade: Level IV
115 patients, mean age 78, 28% male.
Inclusion criteriaPersons evaluated between January 1997 andMarch 1998 considered to be potentialbeneficiaries of the integrated home care. Nospecific entry criteria fixed – i.e., functionaldecline.
Exclusion criteriaNone specified.
Preventive in-home service descriptionThe Health agency of Vittorio Vento (popn 50,000)participated in a national home-care programmecalled Silver Network Home Care project. Thepurpose of this project was to reorganise olderpersons care for those living in the community byadopting an integrated social and medical careprogramme, case management approach andusing the MDS-HC instrument as an assessment tool.
Study descriptionPatients were assessed with the Minimum Data Setfor Home Care tool and subsequently a casemanager, GPs and multidisciplinary team from theGEU delivered health and social services as required.The GEU consisted of a geriatrician, social worker,physiotherapist, and several nurses.
GPs were directly involved in case findings,assessment process, care planning, andemergencies. Case managers performed CGAs afterhome-care request and 2 other follow-upassessments and with the GEU in agreement withGPs designed care plan and coordinated serviceprovision. The multidisciplinary teams deliveredservices.
Before and after study evaluatingthe implementation of anintegrated home care programmecompared to pre-implementation.� patients were diagnosed with
an average of 4 clinicalconditions. Some 15 patientsdied over the 6-monthprogramme evaluation period
� a significant reduction in thenumber of hospitalisations,hospital days per patient andfor each admission c.f. pre-implementation of programme
� there was an estimated 29%cost reduction over the period,or savings of US $1260 perpatient.
� possible patientselection bias as nofixed inclusion criteria
� validity and reliability ofthe MDS-HC welldocumented
� reliance uponhospitalisation recordsfor outcome measures,which were notvalidated.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
82
Table 5a. Evidence table of specialist geriatric services in community/clients own homes – preventive services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Ritchie et al. (2002)
Descriptive study
Georgia and SouthCarolinaUSA
Grade: Level IV
Inclusion criteriaAt risk and frail Veterans aged 75+ years living50-100 miles from host VA medical centres andat risk of repeated hospital admission on thePRA-Plus telephone questionnaire.
Exclusion criteriaHigh-risk (PRA-Plus scale) patients, inadequatecontact information.
Approximately 2,600 Veterans identified, from 5years of VA utilisation files. Of these 238 enrolled,99.6% male mean age 79 years.
Preventive in-home service descriptionThe Coordination and Advocacy for Rural Elders(CARE) program began in 1997. A rural caremanagement model with goal to improve healthand functioning and improve access to services inown homes, community and VA facilities. CAREteam performed assessment, identified problems,developed plans and tracked progress, providedadvocacy and linkage services.
Service and study descriptionPatients were identified and screened via telephonequestionnaire and visited by evaluators whoadministered a comprehensive health questionnairebefore patients were assessed and followed-up (4-6months) at home by CARE programme clinicalteams.
Teams were made up of a nurse and social workerusing in-home standardised assessments (MDS-HC),the development of patient-specific care plans andactivating family, community and VHA resources toimplement care plans.
� an average of 8 problems wasidentified for each assessedpatient. The most commonbeing falls/falls risk, social needs,pain and disability needs,cardiorespiratory problems andhealth promotion, registering inmore than 50% of patients
� following assessment, 79% ofpatients received at least oneintervention, 7.7 interventionsper patient
� one third of patients receivedformal service coordination andtwo-thirds linked/referred toservice for identified need.
� descriptive study withno control orcomparison group.Intervention not tested
� teams received formaltraining in usingstandardisedassessment protocols
� study identified highdegree of unmet needsand benefits of routinestandardised CGA inthis population
� the degree theseunmet needs arereflective ofinaccessibility,underdevelopmentand unavailabilityunknown.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
83
Table 5b. Evidence table of specialist geriatric services in community/clients own homes – supported discharge services
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Hyde et al. (2000)
Systematic Review
Birmingham,UK
Grade: Level I
Nine randomised or quasi-randomised studiesincluded. There were 1,351patients allocated tosupported discharge and 1,286 to controlgroups.
Inclusion criteriaLiterature search of studies from Medline,CINAHL, Psychlit, Cochrane library, SSI, up to endof 1997. Hand searching, biographies of otherSRs, author enquiries,
RCTs, older persons 65+ years, withundifferentiated medical problems, supporteddischarge services after acute admission (within1 week of discharge) comparing eithersupported discharge with non-supporteddischarge or highly supported discharge withnormally supported discharge.
Exclusion criteriaNone specified.
Service and study descriptionProvision of support services following discharge fromhospital after acute admission.
Variable interventions with geriatric treatment teams,or home health visitors checking on provision ofservices, aids, appliances, drug compliance andcorrection of shortfall. Home visits by nursing staffcoordinating service provision or home aidesproviding practical assistance.
Supported discharge interventionscompared to non-supported ornormally supported discharge.
In most studies support withdrawnby 16-weeks post-discharge.� functional status was assessed in
6 trials but because of variety ofmeasurement tools employedand high losses to follow-up anoverall combined assessmentwas not made
� there was no overall (9 trials)significant difference in mortalityrates between supported andnon/normally-supporteddischarge groups
� institutionalisation over 6-12months was quantified invarying ways thus precluding itfrom meta-analysis. Results fromthe 7 included trials where thiswas reported by any measureshow a consistent ‘beneficialeffect of supported discharge’in 6/7 studies
� supported discharge showed asignificantly greater number ofparticipants at home after6 months (4 studies), after 12months (one study)
� measures of hopsitalisationvaried across studies and noclear treatment effect wasapparent with two studiesshowing no difference, fourshowing effects favouringsupported discharge and twostudies showing negative effectsof supported discharge.
� details of characteristicsof included studiesprovided, includingquality assessment ofselection, attrition anddetection bias. Authorsconcluded that allstudies open to somedegree of selectionbias given small samplesize, high losses tofollow-up, allocationconcealmentinadequate or not clear
� methods used werefrom the CochraneCollaboration and theNational HealthServices Centre
� the definition of‘supported discharge’,‘non-supporteddischarge’, ‘highlysupported discharge’and ‘normallysupported discharge’not defined other thandescriptions ofinterventions
� a range of supporteddischarge interventionswere included only fourtrial interventionsperformed by geriatricteam services, others bynurse or health visitorassistants
� lack of data onpatient/carersatisfaction andfunctionality
� the extent ofpublication bias inanalysis not known.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
84
Table 5b. Evidence table of specialist geriatric services in community/clients own homes – supported discharge services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Lim et al. (2003)
RCT, single blind,multicentre trialwith 6 month follow-up
Victoria,Australia
Grade: Level II
654 patients, 340 patients in intervention group,mean age 77 years, 40% male and 314 in controlgroup, mean age 77 years, 43% male.
Inclusion criteriaPatients 65+ years that were in acute ward forover 48 hours and discharged home. Patientsexpected to live at least 1 month post-discharge.
Patient eligibility risk criteria including self-caremanagement problems, lived alone, communityservices user pre-hospitalisation and requiredservices on discharge.
Exclusion criteriaPatients admitted from/discharged to a nursinghome, ED and required community care ondischarge.
In-home post-discharge service descriptionPost-Acute Care (PAC) programme where PACcoordinators have a separate budget to purchasetherapeutic and support services for patients in thepost-discharge period.
Study descriptionStudy setting in four university-affiliated metropolitangeneral hospitals.
PAC intervention group patients were referred toPAC coordinators who were hospital based staff withnursing and allied health backgrounds. The PACcoordinators assessed patients and developeddischarge plans. Usual care was similar except PACcoordinators provided more time and expertise andalso provided short-term case management. Thisincluded telephone follow-up, crisis intervention,liaison with service providers, coordination of serviceprovision and ensuring adequate referral beforedischarge.
A budget was available for PAC coordinator topurchase community services directly in post-discharge period. This service plan was not availableto control patients.
Control group patients received usual hospitaldischarge planning provided by ward nursing staffand the social work department.
Patients were randomised toreceive either (intervention) servicesfrom a Post-Acute Care Coordinator(PAC) or (control) usual dischargeplanning care.� no difference between groups
in unplanned hospitalreadmissions over 6 monthspost-discharge, but PACpatients used significantly fewerbed days over the period
� significant difference betweengroups in greater quality of life(at 1 month) for PAC patients
� no difference in mortalitybetween the two groups
� total costs (hospitalisation,community services andintervention) were lower in PACgroup (mean difference $1,545.
� both patient groupssimilar at baseline
� adequaterandomisation methoddescribed. Researchstaff blinded toallocation for outcomeassessment
� losses to follow-upthough hospital transfer,death or nursing homesadmission wereapproximately 9% inboth groups
� the economic analysisused averages tocompute costs ofcommunity servicesand hospital bed-dayutilisation. Morecomprehensive analysisbeyond scope of study
� actual degree oflinkage to specialistgeriatric services notdescribed.
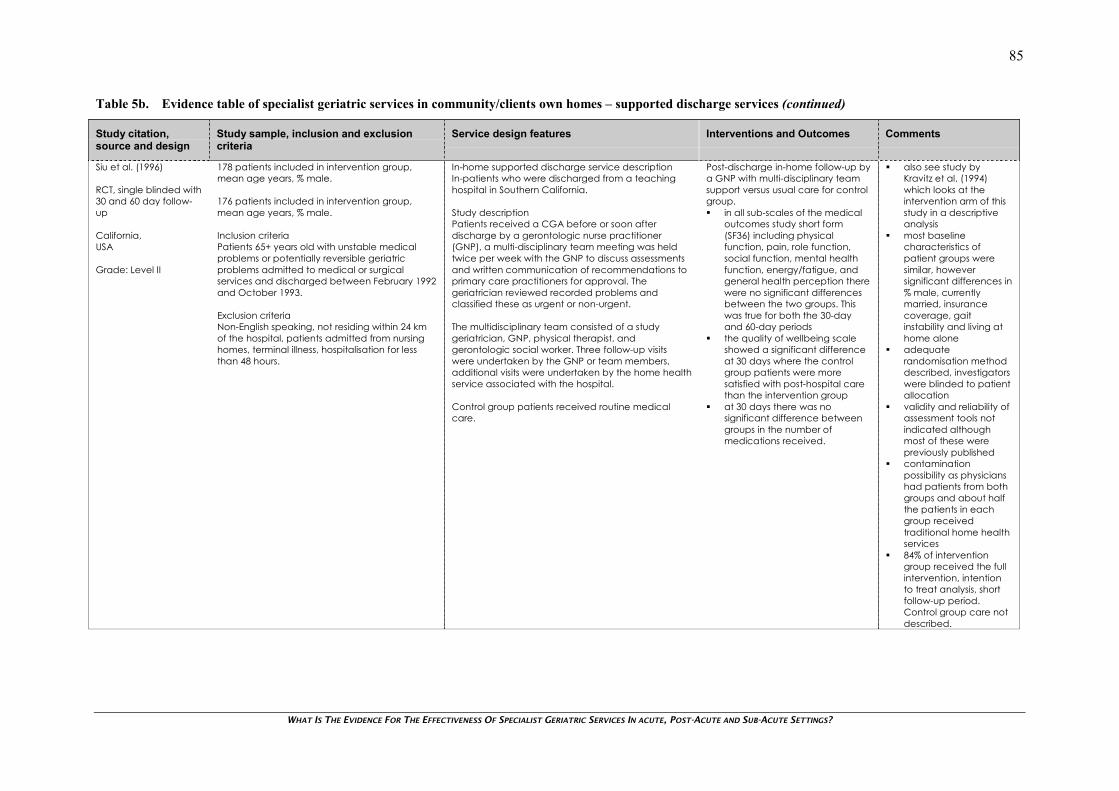
WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
85
Table 5b. Evidence table of specialist geriatric services in community/clients own homes – supported discharge services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Siu et al. (1996)
RCT, single blinded with30 and 60 day follow-up
California,USA
Grade: Level II
178 patients included in intervention group,mean age years, % male.
176 patients included in intervention group,mean age years, % male.
Inclusion criteriaPatients 65+ years old with unstable medicalproblems or potentially reversible geriatricproblems admitted to medical or surgicalservices and discharged between February 1992and October 1993.
Exclusion criteriaNon-English speaking, not residing within 24 kmof the hospital, patients admitted from nursinghomes, terminal illness, hospitalisation for lessthan 48 hours.
In-home supported discharge service descriptionIn-patients who were discharged from a teachinghospital in Southern California.
Study descriptionPatients received a CGA before or soon afterdischarge by a gerontologic nurse practitioner(GNP), a multi-disciplinary team meeting was heldtwice per week with the GNP to discuss assessmentsand written communication of recommendations toprimary care practitioners for approval. Thegeriatrician reviewed recorded problems andclassified these as urgent or non-urgent.
The multidisciplinary team consisted of a studygeriatrician, GNP, physical therapist, andgerontologic social worker. Three follow-up visitswere undertaken by the GNP or team members,additional visits were undertaken by the home healthservice associated with the hospital.
Control group patients received routine medicalcare.
Post-discharge in-home follow-up bya GNP with multi-disciplinary teamsupport versus usual care for controlgroup.� in all sub-scales of the medical
outcomes study short form(SF36) including physicalfunction, pain, role function,social function, mental healthfunction, energy/fatigue, andgeneral health perception therewere no significant differencesbetween the two groups. Thiswas true for both the 30-dayand 60-day periods
� the quality of wellbeing scaleshowed a significant differenceat 30 days where the controlgroup patients were moresatisfied with post-hospital carethan the intervention group
� at 30 days there was nosignificant difference betweengroups in the number ofmedications received.
� also see study byKravitz et al. (1994)which looks at theintervention arm of thisstudy in a descriptiveanalysis
� most baselinecharacteristics ofpatient groups weresimilar, howeversignificant differences in% male, currentlymarried, insurancecoverage, gaitinstability and living athome alone
� adequaterandomisation methoddescribed, investigatorswere blinded to patientallocation
� validity and reliability ofassessment tools notindicated althoughmost of these werepreviously published
� contaminationpossibility as physicianshad patients from bothgroups and about halfthe patients in eachgroup receivedtraditional home healthservices
� 84% of interventiongroup received the fullintervention, intentionto treat analysis, shortfollow-up period.Control group care notdescribed.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
86
Table 5b. Evidence table of specialist geriatric services in community/clients own homes – supported discharge services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Avlund et al. (2002)
RCT, single blinded with3 month follow-up
Storstroem,Denmark
Grade: Level III-1
59 patients in CGA patient group, mean ageand % male not specified.90 patients in control group, mean age and %male not specified.
Inclusion criteriaPatients discharged home from geriatric andmedical wards at 3 county hospitals. Patientsrecruited between February 1996 and October1997. Patients 70+ years (medical wards) and60+ (geriatric wards), having geriatric problem(e.g., instability, incontinence, immobility),needing ongoing treatment/rehab, needingcomprehensive interdisciplinary home services.
Exclusion criteriaImpressive aphasia, severe dementia, terminalillness, hospitalisation for less than 4 days.
In-home supported discharge service descriptionA large county hospital with three wards with mostlycardiological, respiratory and endocrinologicalpatients with mean lengths of stay of 5.3, 8.9 and 7.8days respectively. Patients generally referred fromprimary care. Geriatric wards received patients frommedical and surgical wards in need of longertreatment.
Study descriptionEach patient discharged was visited by a member ofthe geriatric team on the day of and second dayafter discharge and in second, fourth and sixth weekafter discharge. The patient received a CGA by amember of the interdisciplinary geriatric team, theteam member being dependent on the patient’sproblems. Follow-up occurred at next home visit.Medical problems were reported and discussed withGP. A home nurse and a home helper were presentat first two visits and based on individual needs it wasdecided whether primary healthcare staff (nurse,physio, OT) would be present with geriatric team atvisits.
A research nurse and research OT interviewed thestudy population about functional ability just beforedischarge and at 3-months.
The control group received existing dischargeplanning norms, including coordination betweenprimary and secondary health services by thegeriatric team. These services were available topatients discharged from the geriatric ward andpatients with complicated discharges from otherwards of the hospital.
CGA at home by interdisciplinaryteam versus existing dischargeprocedures.� over two-thirds of patients were
hospitalised in a geriatric wardand one-third at a medicalward
� there was no significantdifference in functional abilitymeasurements at 3 monthsbetween groups, though bothgroups showed improvement
� improvement at 3 months infunctionality measurements wasevident for the interventiongroup for patients from medicalwards and from the sub-acutegeriatric wards but there was nosignificant difference betweenpatient groups
� improvement was evident in thecontrol group but notintervention group for geriatricward patients but no significantdifferences between groups
� no significant differencebetween groups in terms ofreadmissions.
� characteristics ofpatient groups notreported thoughbaseline characteristicswere reported to besimilar with respect ofage and gender
� possible subjectselection bias and studypower issues given thatanalysis of patientgroups was not doneon the basis of therandomisation
� randomisation methodnot described, althoughinvestigators wereblinded to allocation
� functionality assessmenttool validated andreliability tested fromprevious references
� intention to treatanalysis, although lossesto follow-up notspecified
� interdisciplinary teammix not described.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
87
Table 5b. Evidence table of specialist geriatric services in community/clients own homes – supported discharge services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Hansen et al. (1995)
RCT, with 6-monthfollow-up
Copenhagen,Denmark
Grade: Level III-1
96 patients in team care group, mean age 79years, 30% male.
97 patients in control group, mean age 81 years,35% male.
Inclusion criteriaPatients selected by geriatric team for admissionto and discharged home from the sub-acutegeriatric ward over the period February 1991 toMarch 1992.
Exclusion criteriaNone specified.
In-home supported discharge service descriptionA University based hospital with 780 beds and 21specialties in a catchment of 7 municipalities ofCopenhagen with population of 210,000, of whom6% were 70+ years old. The hospital had a geriatricsdepartment with 20 beds for long-term care, a 10-bed sub-acute geriatrics ward, a day hospital with 30beds and an interdisciplinary geriatric team with ageriatrician, a nurse, and a physical therapist whoprovided services to older hospital patients andthose living at home after referral from their GPs.
The sub-acute ward provided patients with 1-2weeks of intensive geriatric management inclusive ofdiagnostic work-up, medical treatment, rehab, earlysocial assessment and discharge planning.
Study descriptionPatients discharged home from sub-acute wardwere visited at home by one of the team membersat 1, 3, 8 and 16 weeks after discharge, plusadditional as needed. At each visit a geriatricevaluation was performed. Adjustments tomedication were made as required and GP notified.Limited rehab was performed by a physiotherapist. Iftreatment was needed patient admitted to dayhospital or sub-acute ward. Planned social servicescould be altered in cooperation with patient’s homenurse.
Control group patients had a discharge summarysent to the GP and social support was arranged onday of discharge. No patients were offered geriatricfollow-up visits.
Regular follow-up of dischargedpatients by interdisciplinary geriatricconsult team versus usual dischargewith no geriatric follow-up visits.� over the 6 months post-
discharge significantly morepatients from the interventiongroup received home help thanthe control group
� significantly more control grouppatients were readmitted tohospital than in the interventiongroup
� there were no significantdifferences between the groupsin nursing home admissions andmortality.
� baseline characteristicsof patient groups weresimilar
� randomisation methodnot described, unclearif investigators wereblinded to patientallocation
� generalisabilty limitationas study focus was oncare of chronically illand probable long-term care
� outcome measures andmethods of patientdata collection notvalidated and reliabilitynot tested
� patients re-admittedretained their initialgroup assignment.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
88
Table 5b. Evidence table of specialist geriatric services in community/clients own homes – supported discharge services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Cavalieri et al. (1993)
RCT, 1 year follow-up
Washington DC,USA
Grade: Level III-1
33 patients in the CGAT group, mean age 82years.
36 patients in the non-CGAT group, mean age82 years.
Inclusion criteriaNewly admitted patients (75% from acute care,the rest from community) between June andNovember 1986.
Exclusion criteriaPatients with terminal illness.
In-home supported discharge service and studydescription
A Health Care Center with a 120-bed skilled nursinghome facility. Two distinct modes of service toresidents. A Comprehensive Geriatric AssessmentTeam (CGAT) made up of a group of geriatriciansand geriatric nurse practitioners that all havespecialised training in care for older persons. Theother service available to nursing home patients is aroutine model of care where patients are managedentirely by individual physicians who have not hadspecialised training in geriatric care.
A Comprehensive GeriatricAssessment Team (CGAT) versus atraditional medical model of non-specialist trained single–physiciancare (non-CGAT) in nursing homepatients.� a significantly greater number of
diagnoses were made in theCGAT group compared to non-CGAT group throughout the 12-month period
� the CGAT group usedsignificantly more medical andother consultations than thenon-CGAT group
� the CGAT group had greater(but not significantly) longevitythan non-CGAT group
� no difference in hospitaladmissions, but there were more(but not significantly) ED visits bythe non-CGAT group.
� no significantdifference betweenpatient groups infunctional status andcognitive dysfunction.Other socio-demographic featuresnot described
� randomisation methodnot described, unclearif investigator(s) wereblinded to groupallocation
� no losses to follow-up(i.e., deaths) reported,unclear if intention totreat analysis
� validity and reliability ofassessment tools notindicated althoughthese were previouslypublished.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
89
Table 5b. Evidence table of specialist geriatric services in community/clients own homes – supported discharge services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Melin et al. (1993)
RCT with 6 monthfollow-up
Stockholm,Sweden
Grade: Level III-1
150 subjects were included in the intervention(Team) group, mean age 81 years, 29% male.99 subjects were included in the control group,mean age 80 years, 27% male.
Inclusion criteriaPatients living in a specified inner city catchmentarea, inpatient at a general county hospital incentral Stockholm, chronically ill and predictedto be dependent in 1-5 activities of daily living(ADL) at discharge.
Exclusion criteriaPatients with dementia, living in communityservice hotels, dependent in 6 ADL functions.
In-home supported discharge service descriptionIn 1997, a primary care team unit started in a primarycare center in Inner city Stockholm. The unitconsisted of a project physician, a primary careteam physician a district nurse, a physiotherapist, anOT, an assistant nurse and a secretary. Many wereemployed part-time, and the team had anadministrative function except for the teamphysician who had an in-home care function.
The team physician guided the team whocoordinated 24-hour post-hospital care andrehabilitation. The team nurse assisted the teamphysician and administered all medical and socialservices on a 24-hour basis, the assistant nurseinterviewed and assessed patients at study entry andassisted team physician. The team OT reassessedpatients at follow-up. Weekly team meetings wereheld (also attended by a consultant geriatrician andpsychiatrist) the OT and physiotherapist coordinatedhome visits to team patients and initiated supply ofmechanical aids and devices.
Study descriptionThe team physician determined patients’ readinessfor discharge from acute care and if they fittedinclusion criteria were randomised them to eitherpatient group. On the day of discharge, a districtnurse and home service assistant visited andassessed patient’s need for medical and homeservices. Within a few days the project and teamphysicians did an in-home assessment of functionaland medical status and initiated treatment plan.
A primary home care interventionprogram versus ordinary home carein a control group.� no significant differences
between groups recorded forpersonal activities of daily living,indoor walking, cognition, andsocial function
� the team home care group hadsignificantly higher instrumentalactivities of daily living scores(ADL) than the control group
� there were an increasednumber of diagnoses in thecontrol group and decreasednumber in the team group
� there were higher rates (notsignificant) of accidents, drugside effects and mistreatment inthe control group
� team patients on average spentfewer days in hospital. Theaverage number of days inshort-term care andrehabilitation was similarbetween groups but significantlydifferent in long-term carewhere the team patient groupspent fewer days than thecontrol group
� team patients receivedsignificantly more staff visits andhome aides than control group
� a significant greater proportionof control group patients were inhospital at follow-up but bothgroups were similar on thenumber of readmissions, andlength of admission.
� baseline characteristicswere similar except thatthe team patientsgroup had a highernumber and greaterseverity of diagnoses
� randomisation methodnot described. Blindingto group allocation atbaseline assessment.Not clear if investigatorsblinded to allocation foroutcome assessment
� in-home care for thecontrol group not welldescribed making itdifficult to attributeinter-patient groupoutcome differences toservice delivery
� the social functionassessment and ADLtool was not validated.Other tools’ validity andreliability referenced
� losses to follow-up(survival)at 6-months wereapproximately 25% ineach patient group.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
90
Table 5b. Evidence table of specialist geriatric services in community/clients own homes – supported discharge services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Melin et al. (1993)
RCT with 6 monthfollow-up
Stockholm,Sweden
Grade: Level III-1
(Continued)
On-going care determined at weekly teammeetings, emergency and ordinary home-visits wereavailable around the clock. The team physicianmade house calls every weekday and could becontacted by staff after hours. District nurses,assistant nurses and home aides made visits whenneeded and patients also had 24-hour telephoneservice access managed by the team unit duringdaytime and community-based pensioners’telephone service during the night.
The control group received “ordinary care” –ordinary home care and home help service and noaccess to the intervention program.
� a later study byMelin et al. (1995) useddata from the same trialto examine secondaryoutcomes. Whilecontrolling for otherfactors team care wasshown to improve thelikelihood of ambulationindependent ofpersonal assistance atfollow-up and hadstabilised functional riskand mortalitycompared to usualcare
� an earlier study byMelin et al. (1992) wasexcluded as this useddata from the same trialand evaluated similaroutcomes to the oneshere.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
91
Table 5b. Evidence table of specialist geriatric services in community/clients own homes – supported discharge services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Salgado et al. (1995)
Comparative studywith parallel controls,20 months follow-up
Sydney,Australia
Grade: Level III-2
40 patients (supported group), mean age 82years.
24 patients (control group), mean age 82 years.
Inclusion criteriaPatients who had geriatric assessment but wentto nursing homes as not well enough to go homebut were considered likely to improve and bedischarged home. Controls were patientsdischarged by other hospital departments.
Exclusion criteriaNone specified.
In-home supported discharge service descriptionAn acute hospital in metropolitan area with ageriatric team but no geriatric ward or slow streamrehabilitation unit but relative abundance of nursinghome beds. Older persons were dischargeddependent on their physical condition to home,hostel, nursing home or hospice placement withdiffering degrees of support.
Study descriptionA hospital-based Mobile Rehabilitation Team (MRT)discharge program was evaluated on patientsdischarged after assessment to five nursing homesfor slow stream rehabilitation supported by the MRTfor eventual return home. The MRT consisted of aconsultant geriatrician or professor of rehabilitationand aged care, OT, clinical nurse consultant andsocial worker. Also patient under care of familydoctor. Team members visited patients in the nursinghomes once per week. Nursing homessupplemented this by attendant physiotherapists.Aim of the service was to benefit patients throughincreased independence and avoidance ofextended institutionalisation.
A control group of patients matched for age, sex,activities of daily living status (ADL), comparability ofdiagnosis who were discharged by other hospitaldepartments over the same period and placed innursing homes.
The intervention group of MRTsupported patients discharged tonursing homes versus a controlgroup discharged to nursing homeswithout MRT support.� the MRT supported group had
significantly greater numbers ofpatients discharged home fromnursing home care than thecontrol group
� no statistically significantdifference in the numbers ofpatients who died in the twogroups
� qualitative assessment alsoidentified fears and concerns ofolder persons regardingpermanent placement innursing homes, carerambivalence and relief atnursing home placement andresistance to return home,conflicts of managementbetween GPs and specialistteam.
� comparative studyusing matched controlsto ensure comparablerecovery processbetween the twogroups
� lack of demographicinformation providedfor supported andcontrol groups
� possible patientselection bias as patientselection criteria non-specific
� the numbers of patientsentered into the studyand included in theanalysis do notreconcile, as losses arenot accounted for.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
92
Table 5b. Evidence table of specialist geriatric services in community/clients own homes – supported discharge services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
Kravitz et al. (1994)
Prospectiveobservational studywithin an RCT, with 13month follow-up period
California,USA
Grade: Level IV
152 patients in the intervention arm of an RCT,mean age 80 years, 28% male.
Inclusion criteriaPatients living within 15 miles radius of thehospital with specific risk factors for functionaldecline or increased mortality discharged fromhospital and assigned to the intervention arm ofan RCT.
Exclusion criteriaPatients with terminal illness, hospitalisation ofless than 48 hours, discharge to a nursing home.
In-home supported discharge service descriptionIn-patients who were discharged from a teachinghospital in Southern California.
Study descriptionPatients received a CGA before or soon afterdischarge by a gerontologic nurse practitioner(GNP), a multi-disciplinary team meeting was heldtwice per week with the GNP to discuss assessmentsand written communication of recommendations toprimary care practitioners for approval. Thegeriatrician reviewed recorded problems andclassified these as urgent or non-urgent. Themultidisciplinary team consisted of a studygeriatrician, GNP, physical therapist, andgerontologic social worker.
The intervention group of an RCTreceiving post-discharge geriatric in-home assessment and follow-up.� the GNP identified new or
worsening problems in 99% ofpatients, 11% of problems werejudged to be urgent byreviewing physician
� the specialist team made 3.4recommendations per patient.The most common werediagnostic evaluation andmonitoring, further discussion ofadvanced directives, physicaland occupational therapy, andaltering medication regimens
� primary care physiciansrejected only 2% ofrecommendations.
Prospective observationalstudy as part of an RCT bySiu et al. (1996), appraisedabove.� limited descriptive
analysis with nocomparator
� not clear if theassessment tools werevalidated or reliabilitytested.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
93
Table 5b. Evidence table of specialist geriatric services in community/clients own homes – supported discharge services (continued)
Study citation,source and design
Study sample, inclusion and exclusioncriteria
Service design features Interventions and Outcomes Comments
von Sternberg et al.(1997)
Retrospective studywith a comparisongroup, 12 month follow-up
Minnesota,USA
Grade: Level IV
1,144 patients participated who required rehabtherapy for post-cardiovascular accident, post-fracture/replacement, those who were de-conditioned or had uncomplicated infection.
Inclusion criteriaNone specified.
Exclusion criteriaNone specified.
In-home supported discharge service descriptionand study description
A non-profit HMO, HealthPartners with 21,000geriatrics patients enrolled providing preventive,acute, rehab, and ancillary services. New sub-acutegeriatric rehab and assessment units known asTransitional Care Centers (TCC) were setup as part ofan HMO. These were contractually established inpartnership with 5 area nursing homes. These centerskept aside a minimum of 15 beds available foraround the clock admissions. These were serviced bya team of designated staff, including nursing, socialworker and rehab therapy staff from the nursinghomes and GNPs and geriatricians from the parentHMO.
Patients were either hospital acute-care transfers(80%) or placed directly into the TCC from primarycare (20%). The TCCs were staffed at a nurse-patientratio of 1:9.
Teams undertook to provide targeted care to rehabpatients, with admission, assessment, care planningand discharge planning services.
On admission to TCC from acute care an initial CGAwas done and weekly thereafter components of thiswere repeated. Weekly team meetings were held toreview each patient. After this meeting the patientswere seen by the geriatrician and GNP.
Transitional Care Centers (TCC)providing rehab care compared tosimilar care in other facilities.� the average length of stay for
TCC facilities was 14.3 daysversus 20.5 days at otherfacilities
� post-discharge follow-up at 3and 6 months showed by TCC76% to 80% of patients were stillliving at home and ADLfunctional status remained thesame or greater than atdischarge
� a satisfaction survey of all 253patients surviving at dischargeand 6 months post-dischargewas rated as high
� re-hospitalisation rates at theunits were comparable or betterthan those of other sub-acuteunits.
� potential subjectselection bias as noselection criteriaprovided other thantargeted specificconditions
� patient demographicinformation notprovided
� comparison group andcare received notdescribed
� patient satisfactionsurvey not validated orreliability tested
� limited generalisabilityof this study to NZcontext as serviceprovider setting in a USHealth ManagementOrganisation.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
94

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
95
SECTION 3
SPECIALIST GERIATRIC SERVICE GUIDELINE AND PROTOCOLANALYSIS
The following is a descriptive overview of the key components of published evidence-based specialistservice guidelines and protocols and limited specified expert opinion literature. No attempt has beenmade to appraise the quality of the publications or the evidence base.
SYNOPSIS
This section is a descriptive summary of actual and proposed health services and service frameworksfor older people. The literature relating to service provision examples tends to be supported byunderlying principles of gerontology and geriatric medicine, common sense practice, rhetoric andanecdotal evidence, rather than on robust evidence or description of successful implementation ofservice models. Quality indicators are often suggested but have not been evaluated.
There are three main models of geriatric services; age-related services, integrated care models andneeds- based services. The predominant trend appears to be towards needs-based, age-related serviceswith a multidisciplinary or interdisciplinary interface rather than services integrated with the generaladult population. The proponents of an integrated adult service claim that health service access shouldbe based on need not on chronological age and that only identified beneficial age-specific managementservices should continue.
There is little hard evidence in this literature that proves anything one way or the other with theexception of claims for specialist clinics, for example for Parkinson’s Disease, continence, and fallsand clinical care pathways such as for stroke, fractured hip. These services tend to be age related byvirtue of the age of patients presenting with the health problem rather than any other rationale ofservice design.
Most of the literature describes frameworks of services at a higher level of abstraction concerningservice development programmes and service systems and processes appropriate to the principles ofgeriatric care rather than descriptions of actual services. This level of literature tends to focus onplanning at governance level rather than on specific organisational criteria and implementationstrategies.
Analysis of service descriptions shows a consensus on general principles of care, serviceimplementation and themes:
� there is a strong focus on functional, social and needs assessment, which although beyond thescope of this report tends to underpin much of the rationale for service structure
� need for comprehensive geriatric services across acute care, post acute care, rehabilitation andlong-term care whether integrated or separate
� geriatric care requires a high degree of collaborative, multi disciplinary and interdisciplinary carebecause of multi comorbidities, functional and social impact of illness and polypharmacy
� a continuum of care model is supported
� focus on deinstitutionalisation and community and informal care
� antiageist stance
� specialist and comprehensive education in health care of older people is vital but lacking acrossand between all disciplines and services – e.g., old age psychiatry and geriatric services.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
96
� need for comprehensive information systems that can manage vast complex clinical data withaccess by and between all health professions and care sites including primary, secondary andtertiary care
� increased, coordinated, global and flexible funding is required
� individualised care where patient, family and carer participation in planning and care managementis maximised
� preference for home and community-based care and avoidance or deferral of admission to acute orlong stay hospital care or residential care
� more support is required for voluntary and informal carers
� a flexible service integration of health and social services and public, private and voluntary sectorsis required
� there are many recommendations for research into service development and care models
� there are many recommendations for service development
� an identified need for more prevention and screening
� need for funding for community services and equipment
� need for monitoring and quality improvement systems.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
97
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion
Publication title, author and originAmerican Geriatrics Society (2000)Care management position statement 2001USAService concept, setting, staffing and other componentsCare management� a process of needs identification and health care service coordination and delivery that includes assessment,
implementation and monitoring of health outcomes� includes medical, functional, psychological and social domains of health care in the home, community, clinic, hospital,
sub-acute and long-term care institutions� individual case manager or team case management� care manager may be a member of service provider organisation� client and family are informed and participate in decision making� communication with all services and individuals involved� linked to the primary medical care provider or health professional – e.g., GP, nurse practitioner.
.
Evidence or rationale� increasing demand for complex, multidisciplinary medical and personal care with ageing population� older people often require on going long-term care� complex service provision requires central management and coordination� scarce resources and competition for funding� international focus on community care, informal care and deinstitutionalisation� assures appropriate use and allocation of health and social services coordinated with family-provided care� encourages multidisciplinary participation communication, continuity and coordination of long-term care� encourages multidisciplinary insight into client care across all domains of health care� increases services, reduces unmet needs, increases confidence in receipt of care and increased life satisfaction for client� empowers clients and promotes cultural sensitivity� need more research in to case management model� risk for under or over utilisation of services or conflict of interest between care managers and service providers if care
manager is a member of the service provider organisation. Need third party quality assurance and utilisation review� federal, state and private sources must recognise and support the role of care management teams to ensure quality and
cost effectiveness� critical that the care manager and team members have extensive specialist geriatric focussed knowledge and clinical
experience and cultural awareness education.Recommendations� none.
Publication title, author and originAmerican Geriatrics Society (1999)Role of the geriatrician in managed careUSAService concept, setting, staffing and other componentsRole of the geriatrician in managed care� managed care is a process of needs identification and health care service coordination and delivery, including
assessment, implementation and monitoring of health outcomes� managed care should be lead by consultant geriatrician.
.
Evidence or rationale� assures appropriate use and allocation of health and social services coordinated with family-provided care� older people have high frequency of health care use across all services, more complex presentations, slower recovery
from acute illness and require social and functional supports� care and management systems meet clinical needs of the patient and the operational needs of the health plan� need to develop new models of managed care with a risk contract to cater for high cost users and distribute costs more
equitably� rapid growth of Medicare capitated risk programmes requires rapid service growth of to cater for increased demand on
services and development of new approaches to care such as managed care programmes� geriatricians have a unique capacity and training to develop patient care and operational management systems in a
variety of capacities – e.g., governance, staff and resource management, service design and implementation,collaboration, clinical consultancy, liaison and education.
Recommendations� none.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
98
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originAmerican Geriatrics Society (2002)Improving the quality of transitional care for persons with complex care needsUSAService concept, setting, staffing and other componentsTransitional care� coordinated and continuous planning for health care during transfer of patients between locations or levels of care –
e.g., hospitals, acute, post acute and long-term nursing facilities, home, and specialist referral� includes logistical arrangements, patient and family education and coordination among health care professionals in the
sending or receiving patients with complex health care needs� experienced health professional acts as transfer coordinator to oversee sending and receiving of patient and liaisons with
multidisciplinary care team and informal care providers� patients and informal carers involved in planning and know what to expect at next care site� care and management systems meet clinical needs of the patient and the operational needs of the health plan� referral and transfer arrangements completed before transfer� early evaluation of patient at receiving site� personal health information must go with the patient or be accessible to new site – e.g., Problem list, medications,
medical alerts, advance directives, base line health status and cognitive function, contact information for family andformal and informal care providers.
.
Evidence or rationale� people with complex continuous health care needs require care from multiple services in multiple settings� assures appropriate use and allocation of health and social services coordinated with family-provided care� national trends for specialisation of health professionals increases risk for fragmentation of care in patients with multiple
co-morbid conditions and complex care needs� during transitions patients at risk for medical errors, service duplication and inappropriate or inadequate care.� health professionals often work independently but care for the chronically ill needs to be a collaborative, multi
disciplinary process� communication between caregivers and between care givers and patients is critical to quality care� need performance indicators of effectiveness of transitional care� need monitoring by quality improvement entity� need development of heterogeneous electronic data transfer systems between health care sites� need financial incentives for provision of transitional care – e.g., Medicare benefits for inter-institutional or inter-
professional communication for patient care plan coordination� link payment to quality of care including transitional care� need to educate health professionals in care planning, communication (telephonic, electronic and print), coordination,
transfer and patient follow-up procedures.
RecommendationsRecommended research� development of patient transfer systems and payment mechanisms� patient and family participation in care preference and self management including ethnic and racial considerations� development of performance indicators and quality improvement technologies for transitional care� incentive strategies for improvement of transitional care� improve effectiveness of training of health care professionals in transitional care� development of information technology systems that facilitate confidential information transfer.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
99
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originBritish Geriatrics Society (2001b)Summary of the National Service Framework for Older People in EnglandEnglandService concept, setting, staffing and other componentsEight national service framework standards� anti ageism - eligibility based on clinical need not age� individualised service provision, consumer choice and participation� new range of home and community-based intermediate care – e.g., free home services by registered nurse, promoting
independence, early discharge and rehabilitation including equipment resources and avoiding unnecessaryhospitalisation, and residential care
� specialist care and skilled hospital staff� stroke prevention plan, early diagnosis and specialist multidisciplinary stroke services� falls and injury prevention plan and rehabilitation from specialist falls service� integrated accessible mental health services including carer support� coordinated health and active ageing programmes.
.
Evidence or rationale� ageing population� increasing demand for services� cooperation between NHS and Councils for development and provision of services� single assessment process� integrated service provision� coordinated commissioning arrangements� specialised multidisciplinary staffing� increased funding available in NHS� high quality care regardless of age� individualised care, respect and dignity� fair rationing of resources� reducing burden of long-term residential care� better and quicker care� privacy and dignity promoted – e.g., single sex units� needs better coordination between NHS and social services� need one stop assessment� rehabilitation holds precedence over long-term care� need specialist staff� early discharge a priority� health promotion and prevention as important as care� emphasis on based patient participation and informed options.
Recommendations� none.
Publication title, author and originBritish Geriatrics Society (2001a)Response to the National Service Framework for Older People in England: Delivery is the key – but we see some pitfalls to beaddressed!EnglandService concept, setting, staffing and other componentsNational service framework England� (See summary above)
.
Evidence or rationale� need clear funding streams of budgets tied to local costed programmes, and accountable general management to
avoid displacement of funds to competing interests – e.g., deficit retrieval� need a stronger impetus in geriatric focussed training, expertise and leadership development across all disciplines� need massive investment in information technology for an effective and efficient system to avoid substituting
bureaucracy for professional ineptitude� admission of older people to intermediate care must involve consultation with specialist physicians “preoccupation” with
preventing inappropriate admission of older people to acute hospitals is ageist and Intermediate care could become alower grade substitute
� need immediate increase in numbers training to become medical specialists to support proposed increasemultidisciplinary staffing
� require clear procedures for free delivery of long-term care based on needs assessment� need a national quality assurance framework rather than local responsibility for managerial, financial and clinical
performance to assure achievement of NSF agenda for services, standards and milestones.
Recommendations� none.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
100
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originBritish Geriatrics Society (1997a)NHS medical services for older people.EnglandService concept, setting, staffing and other componentsSpecialist hospital based department for medical care of older people� one NHS provider should supply all services� all services provided in the one specialist department for medical care of older people� access to all medical services under the care of one consultant� some rehabilitation, respite, continuing care and community health services could be managed by other providers.Core policies� referral from GP includes assessment at patient’s home� dissemination of geriatric ward admission criteria to GPs administrators, health centres and junior staff� policy on age and disability access to service criteria� policy on management of mixed medical and psychiatric illness� policy on respite care� liaison procedures with other departments and specialties.Acute Medical Care� access for all ages to diagnostic and therapeutic services� admission criteria policy� older patients should have access to geriatric medical consultant/service rather than general medical consultant/service
if appropriate� all wards admitting older patients as medical emergencies should include consultant physicians, doctors, nurses and
therapists trained in geriatric care and special needs of the elderly.Post acute care� post acute care requires multidisciplinary discharge planning and access to physiotherapy, occupational therapy and
social work assessment� immediate referral to consultant geriatrician as necessary.Rehabilitation� optimal recovery and appropriate reintegration� Inpatient, outpatient or at home� rehabilitation services for frail elderly, stroke and fractures should be incorporated into a generic geriatric rehabilitation
ward� respite care a responsibility of NHS� respite care can occur in long-term care facility or in a rehabilitation facility if therapy would be beneficial.General outpatient clinics� hospital based outpatient clinics source of non emergency advice for GP for illness relating to multiple pathology and
disability� all geriatricians should have outpatient sessions for GP referrals and follow-up.Special clinics in hospital or day hospital� e.g., for Parkinson’s disease, continence assessment, falls and syncope, and memory loss� multidisciplinary and specialist medical, nursing and paramedical staff.Day Hospital� functional and medical assessment� multidisciplinary assessment� short-term care – e.g., transfusions that would otherwise require admission� rehabilitation of chronic physical conditions� unique position at interface of hospital and community services assisting older people to stay at home.Provision of services in support hospitals� provide rehabilitation, respite and continuing care� MDT and facilities for assessment, treatment and rehabilitation� immediate access to day hospital� provision of maintenance therapy� admission after multidisciplinary assessment� patient and carers involved in care planning� respite care service� palliative, terminal care and bereavement counseling with access to community services� psychiatric liaison service� access to community facilities, equipment and services on discharge.Ageism� health and social service access based on need not chronological age however, identified beneficial age specific
management and services should continue� older people represented , consulted and involved at all levels� clinical and managerial proponents for older people identified� review all policies for ageist values� national guidelines for resuscitation policies� representation and planning for minority groups� empower staff to promote anti ageism.� .

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
101
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originBritish Geriatrics Society (1997a) (continued)NHS medical services for older people.EnglandEvidence or rationaleMultidimensional nature of illness in older people demands a multidisciplinary team (MDT) approach� MDT collaboration, communication and discharge planning� primary nurse is at the centre coordinating care and discharge� patient centred and lead and realistic patient centred goals� multidisciplinary case notes� coordinated care� no overlap� functionally orientated medical care complimentary to multidisciplinary care.Skills and attitudesNurses� appropriately trained and experienced nurses with rehabilitation focus� knowledge and skills in common conditions – e.g., continence, confusional states, falls, mobility and sensory impairment,
social aspects and support networks� skilled discharge planning� MDT planning and management central to care� confidence.Doctors� skilled in occult presentation and multiple pathology� MDT leadership� consultants ward based� weekly MDT meeting with consultant leadership� post acute care requires multidisciplinary discharge planning and access to physiotherapy, occupational therapy and
social work assessment� immediate referral to consultant geriatrician as necessary� requires effective medical leadership� requires skilled staff� staff trained in interdisciplinary working� accessible modified facilities for frail and disabled patients� primary care responsibility returned to GP ASAP� short waiting lists� immediate written communication by letter or phone if necessary.Auditing of efficiency, quality and patient satisfaction� routine� regular review by medical staff to ensure discharge when objects met.Commissioning of services� underpinned by cooperation and collaboration between primary health and social services including housing and
voluntary sector and users� strategy� effective contracts� knowledge base� responsiveness to local people� mature relationships with providers� local alliances� organisational capacity.Recommendations for District General hospitals (DGH)� specialist department for care of elderly� effective liaison between care of elderly and all other departments� operational policies ensuring appropriate admission and efficiency� staffing that meets agreed national criteria of structure� efficient comprehensive discharge procedures� liaison and communication with GPs regarding discharge and transfer to primary care� information and education available to older people and the public� multidisciplinary individualised rehabilitation with patient input� care of the elderly staff at senior management and board level.Person centred care� patient/carer involvement in individualised planning and choice of treatment and care� involvement of older people in service planning� patient involved in decision making� adequate numbers of trained staff� clear explanation of condition and treatment options� consent to sharing of information with others or advocates� verbal and written information and advice on health and disability services and benefits� support from family and friends� access to confidential personal records� accessibility of and transport to health facilities if required.Quality indicators� number of new policies/services introduced without consultation with users and carers� percent of patients over 80 appropriately admitted to coronary unit or stroke units.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
102
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originBritish Geriatrics Society (1997a) (continued)NHS medical services for older people.EnglandEvidence or rationalePolicies in place for� discharge� communication with community services and GP� medication provision� written information for patient on choices, plan and continuing care arrangements� discharge communications received in less than 48 hours� patient discharge satisfaction monitored� number of failed discharges or delays due to equipment provision.
Recommendations� none.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
103
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originBritish Geriatrics Society (2003)Standards of medical care for older peopleEnglandService concept, setting, staffing and other componentsKey elements� acute teams with MDT support specialising in care of elderly at main hospital site. disseminate policy on referral and
admission� specialist rehabilitation wards with IDT support� comprehensive non inpatient assessment and rehabilitation services including rapid access to intermediate care� specialist outpatient clinics for common problems� IDT community rehabilitation with specialist medical involvement� training and support for non-specialised wards and staff� care pathways for common acute problems� partnership with all stakeholders including users including education� health promotion and prevention programmes� quality assurance systems.Three major models of geriatric medicine� age related services� integrated care models� needs-based services.Acute Assessment and General hospital Care� all care of older people should be delivered by specialist teams� any change in health or function should be investigated immediately� easy access by GP for documented specialist advice as outpatient, day patient, community rehabilitation team, or
domiciliary assessment.Medicines� maximise effect and minimise side effects by appropriate prescribing of amount and type of medications� regular review of medications in ward or by GP (6 monthly)� one stop hospital dispensing schemes� self administration schemes� specialist advice from pharmacies� clearly labelled easy open containers.
.
Evidence or rationaleAcute care services� older people have equal rights to services� patient involvement in decision making� health promotion� Illness prevention� disability reduction� ageing in place� preservation of dignity, autonomy and respect� old age is not a cause of physical or mental illness.Statutory service framework provided by NHS and local partner agencies promote� prediction and prevention programmes� acute assessment and diagnosis� MDT assessment , treatment, rehabilitation in intermediate or community-based care� prompt access to recovery and independence aids� multi agency supportive continuing care� palliative care.Standards of care� understanding needs� involving patient and family in planning� partnership between all stakeholders� patient centred IDT focus� integration of specialist services with hospital based services for common problems including mental health and
intermediate support.Specialist services for person centred care� continence services, access, assessment, information, advice, treatment and aids.Inpatient care� IDT trained in geriatrics� functional problems assessed by IDT within 72 hours� discharge and rehabilitation planning commenced early in the admission� waiting times in A&E less than four hours� seen by geriatrician within 24 hours� private single sex accommodation with access to rehabilitation space� care continues as long as required� protocols in place for management of pain, nutrition, pressure sores, fluid balance, delirium, falls, continence depression,
infection control and palliative care.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
104
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originBritish Geriatrics Society (2003) (continued)Standards of medical care for older peopleEnglandEvidence or rationaleSpecialist services – e.g., stroke and falls, policies and guidelines for� delirium and dementia� routine memory and cognitive function testing� restraint (chemical or physical)� use of anticholinesterase� advocacy services� support for carers� specialist services need to develop a health promotion culture.Services for older people require� policy for admission to acute care and interface with general medicine and GP services (set up of immediate care)� policies and guidelines for administrators and telephonists for managing referrals and telephone advice by consultants� policies regarding: manual handling, nutrition assessment, pain management, restraint, pressure sore risk assessment,
wound care, infection control and resuscitation orders� dissemination of protocols for management of common symptom complexes (G)� IDT that review older patients in non specialist wards – e.g., with development of role of gerontological specialist nurse� Initiatives that help A&E deal with referrals of older people for admission.Quality indicators� number of patients discharged on more than four medications� disparity between prescription and self administration after two months� local formulary taking into account of older persons needs� adherence to guidelines for use of aperients, antibiotics, antidepressants and antiplatelet drugs� incidence of clostridium difficile on wards as indicator of over use of broad spectrum antibiotics.
Recommendations� none.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
105
Table 6. Descriptive overview of published specialist geriatric service models and expert opinion (continued)
Publication title, author and originBritish Geriatrics Society (2000)The older patient in the accident and emergency departmentEnglandService concept, setting, staffing and other componentsKeys to high quality care� clinical skills of staff in A&E and effective liaison and MDT communication� A&E the interface between primary and community care and specialist hospital based departments� care for older people based on needs not age defined criteria� equity of access to all services.Interdepartmental and MDT guidelines for� pressure sore prevention� mental health referral� suspicion of elder abuse� falls� hip fracture� hypothermia� social care needs� discharge planning and procedures.Training� senior staff education on care of elderly� assigned responsibility for nurse education and clinical liaison with other departments and lead auditing� senior doctor assigned responsibility for training needs of junior doctors� training to include mental state and functional assessment, practice guidelines and operational policies and procedures.Performance standards� all A&E attendees assessed immediately for urgency of clinical need – e.g., by triage nurse 94% of A&E attendees seen
within five minutes delay from decision to admit to arrival on ward not exceeding two hours..
Evidence or rationale� older people are relatively frequent users of A&E particularly over 85 years of which 50% for falls and accidents and most
others for illness� social isolation is associated with attendance at A&E� primary health care type presentations lower among older patients.Challenges� history taking impeded by cognitive and sensory deficits� atypical or altered presentation of symptoms� predominance of typical problems such as immobility, confusion, incontinence and non-specific functional difficulties
may obscure new problems� significant disability may follow trivial illness or injury� disability may be reversible� anticipating and meeting care needs as important as diagnosis, treatment and rehabilitation.Special issues� falls, elder abuse, deliberate self-harm and delirium.
Recommendations� appropriate staffing, equipment and training� coherent clinical services foe older patients across all services� continuing review of policies regarding staff, equipment, facilities and interdepartmental and interoperational boundaries� identification of obstacles to quality care� minimising delays� appropriate facilities for older people – e.g., toilets, chairs and beds and availability of food and drinks� timely admission to appropriate services – e.g., acute medical beds, geriatric care beds, mental health services,
observation ward or referral to urgent clinic, day hospital, community rehabilitation, urgent social care, urgent residentialcare and home support services
� protocol for assignment of MDT responsibility� senior clinician available to make admission or discharge decisions� policies and procedures and governance resources and documents available in A&E.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
106
Table 6. Descriptive overview of published specialist geriatric service models and expert opinion (continued)
Publication title, author and originBritish Geriatrics Society (1995)Acute medical care of elderly peopleEnglandService concept, setting, staffing and other componentsThree main models of service provision – a combination of all three may be appropriate� the needs related model� the age related model� the integrated model� traditional model of health care is needs related� development of facilities for acute care of the elderly have led to the development of age related and integrated
models� central tenet of access to MDT services and immediate assessment and treatment by trained staff� GP in best position to decide on acute care or less acute assessment and rehabilitation� patients with single pathology should be referred to appropriate sub-specialty� patients with complex needs referred to geriatrician� no age-defined restriction on access to resources� geriatricians to work alongside general physicians in management and discharge of elderly patients in sub-specialty
services� geriatric experience recommended for all junior doctors.
.
Evidence or rationale� none.RecommendationsRecommendationsAcute service� admission not age related� written operational policy on acute emergency care of elderly� liaison between geriatricians and A&E department� receiving unit staff trained in assessment and care of elderly people� documented management protocols – e.g., for myocardial infarction� transfer of patients between medical and geriatric services to occur at senior staff level� discharge planning to start on admission.Training� medical training to include geriatric medicine experience at all levels all involved in management of acute elderly
patients should have postgraduate training in geriatric medicine.
Publication title, author and originBritish Geriatrics Society (1997c)Seamless care- obstacles and solutionsEnglandService concept, setting, staffing and other componentsReorganisation of services� introduction of an internal market in the health services� split between purchasers and providers of health Care. Emphasis on purchasing secondary care from GPs not Health
Authorities� Health Authorities have been encouraged to split care into acute care services in hospital arm of their business and
rehabilitation and continuing care in the community arm of their business. Potential to fragment services for elderly� some HA (G) may provide both services through one business� more emphasis required on rehabilitation and focus on frail elderly and continuing care rather than continued emphasis
on acute care – e.g., shortening hospital waiting lists by:- improving discharge arrangements for frail elderly- defining responsibilities for continuing care- balancing service provision including rehabilitation facilities
� policies to avoid premature discharge� to provide for continuing care within the NHS (G)� provision of specialist medical and nursing support within community residential care and nursing homes� LA (G) at the centre of purchasing for social and health care of the elderly (NHS and Community Care Act 1990)� government supporting development of private residential and nursing sector has reduced long-term care in secondary
care sector. Evidence of poor transfer of information..
Evidence or rationale� require a patient centre focus not a services focus to reduce the difficulty for elderly people moving between the
compartments of the health care system� need: easy transfer, effective communication, and integration� splitting of acute and continuing care isolates the service� health and social care budgets are separated� barriers at the interface of hospital and community care and within hospitals� older people have complex acute, rehabilitation and social needs that cannot be separated.
Recommendations� none.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
107
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originBritish Geriatrics Society (1999)Guidelines for the implementation of clinical governance in geriatric medicineEnglandService concept, setting, staffing and other componentsLeadership� each department of Geriatric medicine or group of consultant geriatricians should have a nominated lead consultant in
organisational service quality� demonstrable participation of consultants in governance processes.Resources� lead consultant in organisational quality (e.g., clinical director) is trained in governance and supported by guidelines� minimum of one funded session per week� all consultants participate in protected time set aside for this and role stipulated in job plan� specialist registrars involved� managerial and administrative staff involvement� avoid duplication with other subspecialties – e.g., general medicine.Content� annual investigation of a minimum of one selected area of specialist practice and service delivery per department – e.g.,
management of: falls and syncope, stroke, delirium, dementia, depression, continence, Parkinson's Disease, pressuresores, resuscitation orders, fractured femur, evidence-based prescribing.
Implementation� aim to prevent rather than redress shortcomings� use of clinical governance tools – i.e., clinical service audit, complaints, risk assessment, critical incident review, national
patient surveys, service agreement performance monitoring, national indicators, peers review of accepted standards ofcare
� case discussion� independent “blind” review by two people of difficult cases� anonymous patient reviews.Implementation outcomes� clear action plan including action, person responsible and date� professional development and performance of team managed by the nominated leader at governance level or a
delegated person� service development needs and responsibilities clearly stated with clear audit trail of accountability.� procedures outlined for problems with clinical governance processes, concerns about competence or patient safety or
service issues and management.Records and reporting� kept for seven years� annual or biannual summary report� kept in secure area by clinical governance lead� use of technologies if feasible, practicable and cost effective� i.e., audit, indicators, NSF and SIGN guidelines, consensus documents, performance management framework, complaints
in health ombudsman reports, critical incident review, patient surveys etc� audit trail of decision making to achieve service development plan� evidence of improvement in terms of set targets.Minimum Standard Indicators� individual� fifty hours clinical professional develop per annum� participation in annual performance appraisal� include curriculum components of the JCHMT specialist training� include CME topics� 50% of personal development objectives reached by next annual appraisal� evidence of participation in governance process.Service� written evidence that all career grade medical staff have achieved minimum requirements for governance activities or
action taken� written two to five year development plan including outputs of governance process.
.
Evidence or rationale� auditable� enable early initiation of preventative and remedial measures.
Recommendations� none.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
108
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originBritish Geriatrics Society (1997b)Rehabilitation of older peopleEvidence of effectiveness to assist purchasing of general rehabilitation, and specific packages for rehabilitation of stroke andfractured neck of femur.EnglandService concept, setting, staffing and other componentsRehabilitation of Older People� “ the reduction of functional deficits without necessarily reversing the underlying biology of the disease”� includes acute and chronic perspectives� an intervention between impairment (G) and disability (G) or between disability and handicap (G)� overall aim of reducing handicap� requires MDT approach� generic approach or disease specific approach� part of continuing care in the community including residential and nursing care.
.
Evidence or rationaleComprehensive geriatric assessment (CGA) crucial� most effective ‘packages’ are the geriatric assessment unit and the combined geriatric assessment and rehabilitation unit� outcomes include prolonged survival, rational use of drug therapy, reduced annual medication costs and reduced use of
acute hospitals and nursing homes� appropriate targeting and selection for CGA essential – i.e., independent or terminally ill excluded, over 75 years and with
reversible conditions included.Needs� systematic evaluation at key stages� well validated standardised measures� measures of customer satisfaction including view of carers� ongoing research� more resources� measurement of cost effectiveness� interface and collaboration with other rehabilitation services.
Recommendations� none.
Publication title, author and originCampion (2002)The New England Journal of MedicineSpecialized Care for Elderly PatientsUSAService concept, setting, staffing and other componentsSpecialised care for elderly patients� interdisciplinary team model� including social workers, nurse specialists, physical therapists, occupational therapists, and geriatricians working together.
.
Evidence or rationale� ageing is poorly understood� altered manifestation and progress of disease and recovery� multiple medical conditions are usual� drug interactions and adverse reactions are common, depression and delirium are common with hospitalisation� studies have shown that better physical functioning and control of pain can gained from specialist geriatirc care� benefits of geriatric care have not been as dramatic as expected.
Recommendations� none.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
109
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originSainsbury (1994)The effects of the health reforms on the elderlyNew ZealandService concept, setting, staffing and other componentsPrinciples of good service for the elderly� prompt GP referral� a wide choice of help available� high turnover and no waiting lists� early consultation with medicine, orthopaedics and ED� cooperation between psychiatry and medicine� a strong emphasis on prevention and surveillance� full assessment before placement in long stay care.International trends� a reduction in institutional care� integration with general medicine� coordination of medical and psychiatric services� move towards community care.
.
Evidence or rationale� geriatric medicine is a branch of general medicine concerned with the preventative, remedial, clinical and social
aspects of older people� older people have multiple pathology, altered presentation of disease and prolonged recovery time� flexible home-based care� rapid access to care critical to remaining at home� need well integrated and coordinated community services� integration of primary and secondary care� need more emphasis on health promotion and preventative medicine� need coordination and cooperation between services� separation of services for the elderly runs the risk of separating the services from acute care and considering them as
disability services� clinical assessment needs to be separated from any gate keeping role on funding� separation of geriatric services may fragment services and move elder care away from mainstream medical care.
Recommendations� none.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
110
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originSainsbury and Wilkinson (1999)The achievements of geriatric medicineNew ZealandService concept, setting, staffing and other components� based on efficient and meticulous diagnosis and treatment and coordinated rehabilitation by skilled multidisciplinary
team� good geriatric service delivery depends on how not just what is done� collaboration, teamwork and attention to multiple aspects of the persons problems� holistic asses� innovative methods of service delivery – e.g., orthogeriatric rehabilitation, psychogeriatric care, comprehensive
assessment and rehabilitation and stroke units, teamwork and attention to detail – e.g., footwear and hearing as well asprimary presenting problem
� close liaison between geriatric and psychogeriatric services needed for complex needs of unwell older people� orthopaedic geriatric liaison and joint rehabilitation reduces lengths of hospital stay with improved costs and outcomes� stroke units show improved� multidisciplinary teaching introduced into core undergraduate medical programmes has improved skills and attitudes� postgraduate multidisciplinary courses in gerontology available in Christchurch and Auckland� two academic departments of gerontology in Christchurch and Auckland prompting multidisciplinary research in
gerontology..
Evidence or rationale� ageing population with fastest growing segment in over 80 years� some still question need for separate geriatric specialty� historically solutions for geriatric care lay in long-term care in chronic and custodial care in bed� advocacy and anti-ageism part of the purpose of separate specialty� recognition of remediability of older persons problems and emphasis on function and independence� attitude that aged care is less rewarding and less interesting than other high tech and health care of younger population� geriatric specialty at forefront of innovations in teaching, service delivery and interdisciplinary teamwork� geriatric specialty assessment and treatment and rehabilitation shown to reduce acute care hospital days, delayed long-
term care placement and readmission rates and result in improved functional status, survival and morale outcomes withsocial and financial benefits to the community
� in Canterbury in 1980, there were 400 older people on long-term care waiting lists since 1992 there has been no waiting listfor continuing hospital care despite a reduction in beds
� patient outcomes and reduced mortality with coordination of care across disciplines and inpatient and communityservices.
Recommendations� service innovation and evaluation� ongoing research for policies in purchasing of services for older people� integration between geriatric and general medicine� retention of principles of geriatric medicine and cooperative, collaborative models of service provision� collaboration between inpatient services and primary and secondary care services� longitudinal research� emphasis on health promotion.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
111
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originBachman et al. (1987)An innovative approach to geriatric acute care delivery: The Choate-Symmes experienceUSAService concept, setting, staffing and other components� Ten bed geriatric special care units (SCU) opened in two community medical surgical hospitals� nurse lead primary care model compared to control groups task oriented model introduced� participating staff trained and nurses trained in primary care nursing� each unit had a medical director and a shared full-time social worker, physiotherapists, social workers and physicians
shared with other units� comprehensive assessment, self reliance, individualised nursing care plans and interventions, discharge planning began
on admission, interdisciplinary team with regular team conferences and family and patient input� patients randomly assigned to control group who received traditional care or study group in GSCU� patients dressed in own clothes, to perform own activities of daily living and participate in exercise programme and
communal dining� post discharge weekly phone calls by primary nurse and three week home visit follow-up and assessment� during hospital stay and after discharge patient or representative completed questionnaire, other outcome measures
ascertained at discharge or from patient files� care focus on patient not convenience� care humanised and individualised.Limitations� nursing assessment and discharge planning not always completed/started on admission� multidisciplinary meeting unable to accommodate everyone’s schedules� patients preferred to wear hospital gown and robe� shared support services gave priority to other units� fluctuating and inadequate staffing levels RNs often transferred to cover other shortages and replaced with second level
nurses� inadequate administrative support requiring nurses to undertake clerical duties� delays in structural requirements – e.g., phones� anticipated negative response to role changes with introduction of primary nursing and nurse lead team approach did
not occur� other hospital staff negative about higher staff ratios in study units� 10 bed units inefficient 12 to 15 beds more cost effective� phone and home visits not always completed because of staffing issues� multiple level of decision making a hindrance.Evidence or rationale� ageing population� over 654 are 11% of population using 30% of hospital expenditure� 60% of inpatients in medical surgical units are over 65� need high quality cost effective health care� hospitals must find new ways to provide care within fiscal constraints.Outcomes� quality of care improved, fewer "expirations" in study group� no impact on functional ability� day charges increased but total charges and length of stay reduced.Recommendations� training in primary nursing care model� adequate staffing and support from rest of hospital� priority given fairly to GSCU� training and education for all staff� monitoring of processes� structural processes in place before unit opened� key decision makers identified� 12- to 5 beds� involvement/awareness of other staff.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
112
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originBoult et al. (1998)Systems of care for older populations of the futureUSAService concept, setting, staffing and other componentsACE units� ACE acute care units attached to main hospitals for elders� elder friendly environment� intensive review by geriatrics experts� patient centred rehabilitation and disability prevention focus� discharge geared around discharge home.Home hospitalisation� low technology elements of hospital care carried out in patients home – e.g., medications, IV infusions, laboratory testing,
and treatment of chronic conditions such ad congestive heart failure and respiratory disease.Sub-acute care units� variety of transitional care units, providing low tech goal oriented multidisciplinary care rehabilitation facilities and nursing
home wards aimed at shortening expensive and potentially hazardous hospitalisations� for example, rehabilitation, chemotherapy, post operative care, ventilator care, wound care, hospice care, total
perenteral nutrition, peritoneal dialysis, transfusions and IV therapy.Care of high risk older adults� recognition by clinicians using risk screening instruments� periodic screening by mail or phone� analysis of administrative data� requires systematic collection, entry, management and analysis and reporting of data� referral to proactive clinical programmes as necessary.Geriatric Evaluation and Management (GEM)� a step up from comprehensive Geriatric Assessment by multidisciplinary teams� GEM is an expanded process that links assessment to control of patient care combining assessment with sustained
treatment.Case management� proactive intervention to allocate health related services appropriately and to coordinate them efficiently across health
care settings� involves screening, care planning, implementation, usually by a nurse or social worker and monitoring and overseeing of
care provided.Interdisciplinary home care� physician led interdisciplinary home care with integration of medical and supportive services� nurses monitor and evaluate patient needs and provides education and refers to supportive and therapeutic services
including personal care and home care, occupational and physical therapy, medical and rehabilitation services.Proactive primary care� prevention and management of chronic conditions through group sessions and individual consultation in "cooperative
health care clinics"� nursing home example is where physician, physicians assistant or nurse practitioner visits nursing home residents monthly or
as needed for acute changes with physician consult available and occasional joint rounds.Adult day health care� combines social care with health care� clients participate in recreational activities while their chronic conditions are monitored and treated� older adults at highest risk are targeted.Care of low risk older adults� screening of low risk older adults, and preventative care, monitoring and treatment of chronic problems.
.
Evidence or rationale� 5% to 10% of older population incur 60% to 70% of older persons health care expenses� need to focus resources for cost effectiveness in special programmes in the care of common acute conditions such as
strokes, hip fractures, infections and congestive heart failure� fragmented care is the Achilles heel of older persons health care services.Recommendations� research and data collection on service models� harder evidence compared to or anecdotal needed� proactive and preventative programmes for high and low risk older adults� prevention oriented programmes� integrated information systems� geriatric focussed education for all health professionals schools� support and development of interdisciplinary teams� coordination of care.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
113
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originAnonymous (2000)A statement of principles; towards improved care of older patients in surgical and medical specialtiesUSAService concept, setting, staffing and other components� see recommendations
.
Evidence or rationale� ageing population� disproportionate increase in people aged over 65 and over 85 years� shortage of geriatricians� shortage of academic geriatricians� frequent and partially preventable hazards of hospitalisation and surgery for older people� surgical and medical specialists need to take responsibility for geriatric care� need to create learning opportunities.Recommendations� enhanced education and faculty development in geriatric care� eliminate historical disinterest in geriatrics and increase awareness through specialty-oriented publication of evidence for
excellent geriatric care� demystify ageist myths through courses, symposia and publications for public and professionals� expand geriatric research in medical/surgical specialties through multidisciplinary and biogerontological research
initiatives and funding for controlled clinical trials� disseminate research findings� specific learning objectives and curricula in geriatric care in medical residency programmes� incorporate research evidence and geriatrics content into inservice and professional board examinations� improve communication and collaboration between geriatric and medical/surgical specialties by strengthening geriatric
services with affiliates or members of other programmes and centres/institutes on aging� define the place of in-hospital care on specialty services in the overall care of older persons through collaboration and
integration of services with seamless financing mechanisms� enhance remuneration for care of older persons including increased physician time� enhance educational emphasis on the care of the older patient� encourage physicians and surgeons' interest in geriatric aspects of their discipline as a career focus.
Publication title, author and originGrachek (2000)Joint Commission Accreditation: A Framework for coordinating Care for Older AdultsUSAService concept, setting, staffing and other components� accreditation of health care organisations by the Joint Commission on Accreditation of Healthcare Organisations will
enhance coordinated care and outcomes and satisfaction by establishing systems and processes needed to supportsafety and quality and continuously improve performance in the delivery of care and services
� approximately 20,000 health care organisations have been accredited.Key functions of accreditation framework� respect of patients rights� ethical business relationships� care coordination across all settings� assessment to meet initial and changing needs� individualised care� education of patients and family/carers� health promotion and prevention education� family involvement in care decisions� improving organisational performance� leadership� safe, effective and functional environment� competent and adequate numbers of staff� information management� surveillance, prevention and control of infection.
.
Evidence or rationale� the Joint Commission's functional framework provides direction for comprehensive and accurate assessment and
emphasises interdisciplinary collaboration consensus and communication of the care plan across health care settingsmaking outcomes more meaningful to patients and enhancing satisfaction.
Recommendations� none.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
114
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originFlaherty (1987)Health care of the elderly: the need for inter professional cooperationCanadaService concept, setting, staffing and other components� promote quality of life as well as length of life� autonomy of older person and choices� address income deficits� address housing needs� religious and spiritual needs� significance of informal care� transportation assistance� elder friendly environments� importance of nutrition� importance of exercise� educational programmes for older people family and public� role of advocacy and volunteers� physicians have central role in assessment and coordination of care� comprehensive coordination of continuing care� simplified single funding across inpatient and community care services� rehabilitation and specialised day hospitals, assessment units, and respite care� development of mental health services� drug therapy management programmes� needs of rural elderly� terminally ill� education for health professionals.
.
Evidence or rationale� inappropriate attitudes – e.g., benevolent paternalism has encouraged premature institutionalisation and lack of respect
in the treatment of older people� inadequate education in gerontology and geriatric medicine� emphasis on body systems rather than general health� narrow range of professionals� fragmentation of health services at government and carer levels� lack of coordination of community services to provide rapid response and continuity of care� lack of financial resources at all levels form individual to providers� confusion of terminology for types of institutional and home care.
Recommendations� none

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
115
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originSolomon et al. (2000)The new frontier: increasing geriatrics expertise in surgical and medical specialtiesUSAService concept, setting, staffing and other components� need to infuse principles of good geriatric care into resident training for medical and surgical specialties� curricular emphasis on geriatrics for education and research for medical and surgical residents� liaison with major academies, institutions organisations and societies re educational programmes and development of
geriatric special interest groups and research awards� publications on ageing in specialist journals� inclusion of geriatric content in exams and inservice education� functional assessment, prevention of predictable disasters, identification and treatment of multiple coexisting problems,
seeking cumulative small gains in function, aggressive rehabilitation, interdisciplinary team care, careful attention to socialsupport status, guarding patients autonomy, in end of life decision making and understanding the effect of dementia onthe clinical setting
� establish enlightened specialty protocols for older patients – e.g., in prevention and treatment of urinary tract infections,delirium, depression, pressure ulcers, falls, functional decline, malnutrition and dehydration
� provision of standardised nurse-physician protocols in consultation with geriatricians implemented as usual care.
Evidence or rationale� ageing population� increasing number of frail and vulnerable older people as surgical patients� knowledge of principles of geriatric care will promote rapid recovery and maximum benefit from surgery� geriatric consultation alone is not enough� negativity towards geriatric medicine related to patients lack of self care ability and time required� rewards for geriatric care relate to patient's gratitude, improvement in function and patient's life storiesRecommendations� development of clinical geriatric research in medical surgical specialties� analysis of clinical research� opinion survey� research career development programme� care of the older patient an intrinsic part of medical/surgical medicine.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
116
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originAnderson (1986)Organisation of health care Services for the elderlyScotlandService concept, setting, staffing and other components� coordinated planning essential� older people must be given choice� seek out at risk people and organise a preventative/management programme� physical, social and mental analysis� education for older people, family, carers, public and health professionals including nurses, medical students, social
workers, paramedical staff, domestic helpers, housing wardens and residential care staff and clergy� education for town planners and architects etc� pre-retirement education and planning� responsibility held by geriatrician� older person's home is the central unit of focus� service includes social and housing focus� health care based around the GP practice with domiciliary district nurses, health visitors and social workers� social workers coordinate home help repeat admissions� GP coordinates domiciliary physiotherapy occupational therapy and podiatry� early diagnostic schemes including nurse/health visitor home visits at regular intervals for designated age groups – e.g.,
annually for over 80 years or postal surveys with routine checks for at risk people, or health protection packages fordesignated age groups
� ideally GP should assess older person at home to provide comprehensive assessment rather than just medical diagnosis� diagnoses must be treated and followed up� community nurses ensure that treatment and services are occurring� separate geriatric units or designated geriatric beds mean that older people compete for beds based on the urgency
and priority compared with other older people rather than on an age basis� these units show older admissions but shorter stays� acute admission units need to be supported by continuing care beds as an intermediate step to discharge home if
required� day hospitals and outpatients departments can shorten admissions by providing ongoing care� sheltered housing with a 24 hour warden with or without nursing cover can provide a solution to discharge "home" if
needs cannot be met by home services in the patients existing home� family unit should be preserved if possible with positive incentives for the patients return home through education and
carer support..
Evidence or rationale� increasing numbers of the very old� more men than women� rate of morbidity increases with age of population� rate of disability increases with age of population� unreported illness by older people� people happier and healthier in their own homes� illness is due to disease not age� many older people attribute symptoms to age not disease� many older people expect to be unwell� non-compliance with medications and treatment related to lack of understanding or forgetting to take medications� physiological changes with age� altered pathology in age� atypical presentation� multiple presentation unusual to find less than three diagnoses� insidious onset� geriatric care requires a whole person approach with physical, mental and social health care integrated in a continuing
care programme.�
Recommendations� none.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
117
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originSwift and Severs (1997)The challenges of service provisionEnglandService concept, setting, staffing and other componentsDevelopments� consultant led departments� academic departments in all medical schools� geriatric specialist training structure and curriculum� models of service include age-related, integrated and need-related and their variants� direct clinical responsibility of geriatrician in acute care, continuing care, rehabilitation, advisory, educative and
community care partnerships and health promotion, and a substantial "service engineering element"� multidisciplinary teams originated in geriatric medicine.Health Care Programme framework developed by Reinke USA (cited page 38 (Swift and Severs 1997))Four key elements� demography: knowledge of the characteristics and geographical distribution of the population – i.e., focus on older
people� epidemiology: knowledge of the distribution and determinants of disease in the older population� clinical research: identifying interventions that have a positive I pact on health – i.e., RCTs and pragmatic trials under "real
world conditions" and an appreciation of the organisation, quantity and quality of services required to support thesechanges
� health services research: identifying the best ways of delivering care. There has been little health services research whichis required for real life service provision focussing on the real practicalities of who will do what and when examining everystep of the delivery system providing an actual implementation strategy not just information. Need a strategy aimed atindividual and organisational decision-makers, not just clinicians. The new or experimental service must then itself beevaluated. Improvements need to be measured.
.
Evidence or rationaleCore principles for current geriatric specialty development� older people's health problems often difficult complex, multiple, recurrent, unprepossessing and seemingly unretractible
beyond the boundaries of mainstream hospital practice� cumulative disorders and multidimensional consequences� access to high quality care from ageism based on priority for diagnosis and therapy and the bed blocking burden of
intractable disability and social need inappropriate to acute hospital care perceived as inevitable with increasingchronological age
� care needs fragmented as lay between mainstream medical specialties and requiring input from social care systems� orientation towards accommodation and support rather than treatment, functional recovery and prevention� clients underestimate their own capacity for recovery� multiple episodes, recurrence, relapse and exacerbations with functional and social consequences are the rule.Outcomes� tangible and cost effective services� reduction in long-term institutional care� community resettlement after acute illness� enabling of informal and community services through prompt crisis intervention and planned support.�
Recommendations�
� access standardisation of services should reflect best practices not cost accounting or audit criteria� access must be immediate at the point of need� diagnosis, treatment, assessment and management related to needs� interdisciplinary practice across acute, continuing and rehabilitation care� specialisation of multidisciplinary team members in gerontology/geriatrics rather than generic specialisation� interdisciplinary collaborations in geriatric training� development of linkages with other specialist services following the models of integration between geriatrics and
psychiatry and geriatrics and orthopaedics – e.g., urology, urogynaecology, accident and emergency medicine, adultrehabilitation and cardiovascular medicine
� integration of health and social services through pooled funding and resources with cross-agency work patterns and jointlines of accountability
� partnerships of shared care between hospital care and GP practices� post graduate education for GPs� primary-care led services� managed care concepts� comprehensive care packages managed by the general practice� GP supervised intermediate care units, screening and prevention programmes� information systems to cope with the complexity of presentations such as problem oriented summaries and
correspondence, patient held discharge front sheets, compatible off the shelf soft ware and development of devicessuch as a patient held 'smart card'.
�

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
118
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originSwift and Severs (1997) (continued)The challenges of service provisionEnglandRecommendationsExpansion of evidence base is imperative� need to reinterpret, reapply and renegotiate principles underpinning known models of service delivery� a cross disciplinary collaborative approach to evidence based research to support both practice and service provision� need well informed evidence based and imaginative marketing strategies for public information and contract
negotiations� need funding that spans professional and functional boundaries to challenged the hospital focussed view of health care
of older people� need for research that will develop new treatments and services and research that will evaluate them� research focus on service model development and management initiatives – e.g., pathways of care, and evaluation
rather than clinical effectiveness� services should only be changed on the basis of proven management initiatives and results of experimental
developments.� require research on implementation strategies as well as the service model itself� need to consider consumer perspectives� development of robust scientific tools on which to base service development.
Publication title, author and originNg (1987)The development and organisation of medical services for the elderly in Hong KongHong KongService concept, setting, staffing and other components"Total care for the elderly"� independence, comfort and contentment in own homes� hospital accommodation for acute, continuing and long-term care� residential alternatives� prevention and health promotion programmes� early identification of at-risk older people.Service Organisation� hospital based geriatric medical service similar to other clinical disciplinesProgressive patient care through stages of care� acute assessment and treatment. Elderly patients admitted through outpatients clinics, emergency department or other
wards for initial investigations and assessment for appropriate treatment and medical and social care planning� rehabilitation includes reactivation, resocialisation and reintegration and return home with support services if required� long-term and continuing care beds in peripheral hospitals for patients requiring some nursing but minimal medical input� hospital day care a "bridge between the hospital and the community" for assessment, monitoring, procedures, tests,
treatment rehabilitation and maintenance therapy and respite day care� community nursing services continuing care and follow-up at home by community nurses.Education� gerontology and geriatrics included in all undergraduate medical, nursing and allied health programmes. aim to
encourage positive attitude, understanding of demographic and social change, physiology of ageing including physicaland psychological aspects, altered presentation of illness, common diseases, principles of rehabilitation, multidisciplinarycare and community services available.
.
Evidence or rationale� ageing population� urbanisation� vulnerable population� complex health and social needs.Recommendations� refer to future development of psychogeriatric and orthogeriatric liaison services (NB article published in 1987).

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
119
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originBrown (undated)Strategic directions for older people's health services 2001-2006Queensland, AustraliaService concept, setting, staffing and other componentsThe service environment� the service network: a complex system of relationships between acute care and long-term care with GP as a pivotal
point. Addressing the linkages can have significant benefits� health promotion and disease prevention: majority of activities are generic, some have specific relevance to older
people. Older people have been targeted and grants are available for research and development into multistrategyhealth promotion interventions and injury prevention and control
� health services: the majority of services provided to older people are generic although there are some specialist geriatricservices in major hospitals. Medicare is provided through general and specialist medical practitioners with additionalMedicare items to improve quality and range of general practitioner services available to older people
� aged care services: responsibility funding purchasing and provision of aged care and support services is dividedbetween Commonwealth and State and non-government service providers. This sharing of responsibility contributes tothe complexity of service provision, overlapping of services and responsibility and previous attempts to rationaliseresponsibility between commonwealth and State have "foundered"
� care coordination: need to reduce complexity of service provision, funding and overlapping and to improve continuity ofcare, flexibility and coordination. Attempts to simplify funding have not been successful and a trial of Team Health Carecentred around GP practices has not been evaluated. GPs are recognised as being in a unique position to identifyneeds and to make referrals. In 1996 the Commonwealth introduced new Medicare funding to reimburse GPs for a rangeof services to older people including over 75 years health assessments, payment for attendance of case and dischargeconferences and for preparation of multidisciplinary care plans. Guidelines and forms are being developed to supportGPs in these roles
� devolution of funding to local level has potential to improve service coordination and service integration.
Evidence or rationale� none.Recommendations� none.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
120
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originEvans (2000)The Oxford textbook of geriatric medicine.(Section 23.1 Services)EnglandService concept, setting, staffing and other components23.1 Principles of Care� services require comprehensive range, accessibility, coordination, continuity in content and time, with respect for patient
autonomy and the welfare of family and carers� reduced physiologic adaptability results in multiple diseases, non-specific, atypical or cryptic presentation of illness, rapid
deterioration if untreated and high incidence of complications of disease or treatment� mainstream medical services inappropriate as they can not be considered as or treated in the same way as younger
patients� require special services that allow more time, focus on function active rehabilitation, continuing care, and follow-up
across the biopsychosocial domains of health and regular review with consideration of personal and communityresources and individual objectives
� requires multidisciplinary approach including doctors, nurses, occupational therapists, physiotherapists, social workers,carers, chiropodists, clergy, dietician, pharmacist, psychogeriatrician, speech therapist and voluntary agencies.
Service design� based on principles of care� combine the best of modern health care technology and specific geriatric expertise� Services traditionally based in secondary care with referral from GPs and other doctors.Two models:� age-defined were parallel services are set up for people above and below a specified age – e.g., 65 years and an
integrated model where doctors with specialist responsibilities provide acute care with colleagues in acute medicalspecialties and are responsible for rehabilitation and community liaison work for older hospitalised people. There has beenno formal comparison of these two models
� UK geriatric services have evolved around a primary care system deployed by GPs North American specialist geriatricservices are provided through hospital and ambulatory clinics by geriatric evaluation units and visiting teams.
.
Evidence or rationaleEvidence� RCTs in USA have shown that geriatric inpatient and outpatient services are more effective than conventional care in
improving function and returning patients home. Geriatric services may also reduce mortality and health care costs� geriatric advisory services are not generally successful and geriatric services need to implement their recommendations
directly.Recommendations� none.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
121
Table 6. Descriptive overview of published specialist geriatric service models and expertopinion (continued)
Publication title, author and originLanghorne (2000)The Oxford textbook of geriatric Medicine.(Section 23.4 Stroke units)EnglandService concept, setting, staffing and other components� stroke service: a combination of inpatient, outpatient and dominciliary services for assessment, rehabilitation and
secondary prevention of stroke disease� stroke unit: system of organised impatient stroke care with multidisciplinary team of stroke specialists� acute stroke service acute admission up to one week� rehabilitation units: admission after one to two weeks post index stroke� combined acute and rehabilitation units� stroke team: a mobile team who care for patients across several wards.Service components from Stroke Units Trialists Collaboration (1996)� coordinated core multidisciplinary team of medical, nursing, physiotherapy, occupational therapy, social work and
speech therapy supported by dietician, chiropody, pharmacy and clergy� staff expertise in stoke/rehabilitation� collaborative policy� comprehensive assessment� individualised patient care� rehabilitation� staff education and research activities� weekly team conferences and ward round input� involvement and education of carers/family� between six to 30 beds� no clear trend in use of investigation or treatment protocols� no routine medical therapies proven in management of acute stroke� no clear pattern of specific medical, nursing, physiotherapy or speech therapy interventions.
.
Evidence or rationale� stroke third most common cause of death and the major cause of acquired adult disability� steep rise in incidence of stroke disease with age� historically stroke services haphazard� stroke units improve coordination and delivery of stroke care� role of stroke units has been controversial.Stroke Units Trialists Collaboration (1996 )� data from 18 trials with 3,000 patients� odds of death reduced but results not statistically robust� death rate reduction in preventable complications secondary to immobility rather than in the first one to three weeks post
index stroke� reduction in combined adverse outcome of death or institutionalisation was highly significant� stroke unit patients who died or were institutionalised were slightly reduce with a substantial increase in the number
returning home independently� no clear association of patient age, sex or stroke severity with the effectiveness of stroke unit care� acute stroke units: "appear to offer a model for improving the organisation and delivery of acute stroke care but there is
no evidence that this alone will improve patient outcomes"� rehabilitation stroke units: " appeared to improve aspects of the process and delivery of care" and "to improve patient
outcomes in terms of reducing death, disability and institutionalisation"…"there is evidence to support this model of care"� combined acute and rehabilitation stroke units - " appeared to reduce case fatality, dependency and institutionalisation"� stroke teams: lack of sufficient evidence� stroke only and mixed disability services improved stroke patient outcomes compared to conventional care in medical
wards� results comparing stroke only and mixed disability units not statistically significant.RecommendationsQuestions� which type of unit can produce the best outcomes?� can acute stroke units improve outcomes in there own right?� no clear consensus on care after discharge?� alternatives to hospital-based care unevaluated?� can mobile teams provide similar care?

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
122
SEARCH STRATEGY FOR SECTION 3
A systematic method of literature searching and selection was employed in the preparation of thisreview.
Searches were limited to English language material, there was no date restriction. The searcheswere completed on 9 May 2003.
The following databases were searched (using the search strategy outlined in Appendix 1b):
Bibliographic databases� Cinahl� Embase� Index New Zealand� Medline� PsychInfo� Science Citation Index� Social Science Citation Index
Review databases� Best Evidence� Cochrane Library� Database of Abstracts of Reviews of Effectiveness� Health Technology Assessment database� NHS Economic Evaluation database
The following professional colleges/associations were searched:
New Zealand
� New Zealand Geriatrics Society� CDHB� Elder Care Canterbury
United Kingdom
� British Geriatrics Society� British Society of Gerontology� Health Services for the Aged
Australia
� Australian Dept of Health and Ageing� Australian Society for Geriatric Medicine� Australian Association for Gerontology� Aged and Community Services Australia� Council on the Ageing� Australian Department of Health and Ageing� National Aged Care Alliance

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
123
Canada
� Health Canada� Division of Ageing and Seniors
Other International
� American Association for Geriatric Psychiatry� American Geriatrics Society� The Gerontological Society of America� The International Association of Gerontology� National Association for Geriatric Service Providers and Educators (USA)� National Institute on Ageing (USA)� National PACE Association (USA)� United Nations Program on Ageing� WHO
Search engines
� Searchnz� Google

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
124

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
125
References
Alexander, T. (1990). The elderly in acute care: a literature review. Dimensions in Health Service, 67,27-33.
Borok, G. M., Reuben, D. B., Zendle, L. J., Ershoff, D. H., Wolde-Tsadik, G., Rubenstein, L. Z.,Ambrosini, V. L., et al. (1994). Rationale and design of a multi-center randomized trial ofcomprehensive geriatric assessment consultation for hospitalized patients in an HMO. Journal of theAmerican Geriatrics Society, 42, 536-544.
Bogardus, S. T., Jr., Desai, M. M., Williams, C. S., Leo-Summers, L., Acampora, D., & Inouye, S. K.(2003). The effects of a targeted multicomponent delirium intervention on postdischarge outcomes forhospitalized older adults. American Journal of Medicine, 114, 383-390.
Boult, C., Boult, L., Morishita, L., Smith, S. L., & Kane, R. L. (1998). Outpatient geriatric evaluationand management. Journal of the American Geriatrics Society, 46, 296-302.
Cameron, I., Crotty, M., Currie, C., Finnegan, T., Gillespie, L., Gillespie, W., Handoll, H., et al.(2000). Geriatric rehabilitation following fractures in older people: A systematic review. HealthTechnology Assessment (Winchester, England), 4, 1-102.
Cameron, I. D., Handoll, H. H., Finnegan, T. P., Madhok, R., & Langhorne, P. (2003). Co-ordinatedmultidisciplinary approaches for inpatient rehabilitation of older patients with proximal femoralfractures. Cochrane Database of Systematic Reviews, 2.
Counsell, S. R., Holder, C. M., Liebenauer, L. L., Palmer, R. M., Fortinsky, R. H., Kresevic, D. M., etal. (2000). Effects of a multicomponent intervention on functional outcomes and process of care inhospitalized older patients: a randomized controlled trial of Acute Care for Elders (ACE) in acommunity hospital. Journal of the American Geriatrics Society, 48, 1572-1581.
Eng, C., Pedulla, J., Eleazer, G. P., McCann, R., & Fox, N. (1997). Program of All-inclusive Care forthe Elderly (PACE): an innovative model of integrated geriatric care and financing. Journal of theAmerican Geriatrics Society, 45, 223-232.
Evans, R. L., Connis, R. T., Hendricks, R. D., & Haselkorn, J. K. (1995). Multidisciplinaryrehabilitation versus medical care: a meta-analysis. Social Science & Medicine, 40, 1699-1706.
Forster, A., Young, J., & Langhorne, P. (2000). Medical day hospital care for the elderly versusalternative forms of care. Cochrane Database of Systematic Reviews.
Hui, E., & Woo, J. (2002). Telehealth for older patients: the Hong Kong experience. Journal ofTelemedicine and Telecare, 8 Suppl 3, 39-41.
Hyde, C. J., Robert, I. E., & Sinclair, A. J. (2000). The effects of supporting discharge from hospital tohome in older people. Age & Ageing, 29, 271-279.
Inouye, S. K., Bogardus, S. T., Jr., Charpentier, P. A., Leo-Summers, L., Acampora, D., Holford, T. R.,& Cooney, L. M., Jr. (1999). A multicomponent intervention to prevent delirium in hospitalized olderpatients. New England Journal of Medicine, 340, 669-676.
Inouye, S. K. (2000). Prevention of delirium in hospitalized older patients: risk factors and targetedintervention strategies. Annals of Medicine, 32, 257-263.
Langhorne, P., Pollock, A., Asplund, K., Berman, P., Blomstrand, C., Dennis, M., Douglas, J., et al.(2002). What are the components of effective stroke unit care? Age & Ageing, 31, 365-371.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
126
Naylor, M. D. (2002). Transitional care of older adults. Annual Review of Nursing Research, 20, 127-147.
Nikolaus, T., Specht-Leible, N., Bach, M., Oster, P., & Schlierf, G. (1999). A randomized trial ofcomprehensive geriatric assessment and home intervention in the care of hospitalized patients. Age &Ageing, 28, 543-550.
Parker, G., Bhakta, P., Katbamna, S., Lovett, C., Paisley, S., Parker, S., Phelps, K., et al. (2000). Bestplace of care for older people after acute and during subacute illness: a systematic review. Journal ofHealth Services & Research Policy, 5, 176-189.
Reuben, D. B., Borok, G. M., Wolde-Tsadik, G., Ershoff, D. H., Fishman, L. K., Ambrosini, V. L., Liu,Y., et al. (1995). A randomized trial of comprehensive geriatric assessment in the care of hospitalizedpatients. New England Journal of Medicine, 332, 1345-1350.
Rizzo, J. A., Bogardus, S. T., Jr., Leo-Summers, L., Williams, C. S., Acampora, D., & Inouye, S. K.(2001). Multicomponent targeted intervention to prevent delirium in hospitalized older patients: what isthe economic value? Medical Care, 39, 740-752.
Rubenstein, L. Z., Josephson, K. R., Wieland, G. D., English, P. A., Sayre, J. A., & Kane, R. L. (1984).Effectiveness of a geriatric evaluation unit. A randomized clinical trial. New England Journal ofMedicine, 311, 1664-1670.
Rubenstein, L. Z., Wieland, G. D., Josephson, K. R., Rosbrook, B., Sayre, J., & Kane, R. L. (1988).Improved survival for frail elderly inpatients on a geriatric evaluation unit (GEU): who benefits?Journal of Clinical Epidemiology, 41, 441-449.
Rubenstein, L. Z., Stuck, A. E., Siu, A. L., & Wieland, D. (1991). Impacts of geriatric evaluation andmanagement programs on defined outcomes: overview of the evidence. Journal of the AmericanGeriatrics Society, 39, 8S-16S; discussion 17S-18S.
Rubenstein, L. Z., Josephson, K. R., Harker, J. O., Miller, D. K., & Wieland, D. (1995). The SepulvedaGEU Study revisited: long-term outcomes, use of services, and costs. Aging (Milano), 7, 212-217.
Scott, I. (1999). Optimising care of the hospitalised elderly. A literature review and suggestions forfuture research. Australian & New Zealand Journal of Medicine, 29, 254-264.
Stuck, A. E., Siu, A. L., Wieland, G. D., Adams, J., & Rubenstein, L. Z. (1993). Comprehensivegeriatric assessment: a meta-analysis of controlled trials. Lancet, 342, 1032-1036.
Stuck, A. E., Egger, M., Hammer, A., Minder, C. E., & Beck, J. C. (2002). Home visits to preventnursing home admission and functional decline in elderly people: systematic review and meta-regression analysis. JAMA, 287, 1022-1028.
Wieland, D., Stuck, A. E., Siu, A. L., Adams, J., & Rubenstein, L. Z. (1995). Meta-analytic methodsfor health services research: An example from geriatrics. Evaluation and the Health Professions, 18,252-282.
Wieland, D., & Rubenstein, L. Z. (1996). What do we know about patient targeting in geriatricevaluation and management (GEM) programs? Aging (Milano), 8, 297-310.
Wieland, D., Lamb, V. L., Sutton, S. R., Boland, R., Clark, M., Friedman, S., Brummel-Smith, K., etal. (2000). Hospitalization in the Program of All-Inclusive Care for the Elderly (PACE): Rates,concomitants, and predictors. Journal of the American Geriatrics Society, 48, 1373-1380.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
127
Appendix 1a:Search strategy for Section 2
SEARCH STRATEGIES
Medline1 Geriatric Assessment/ (6385)2 randomized controlled trials/ or randomized controlled trial.pt. (191960)3 controlled clinical trials/ or controlled clinical trial.pt. (64455)4 program evaluation/ (17471)5 comparative study/ (1023313)6 Follow-Up Studies/ (261238)7 meta-analysis/ or meta-analysis.pt. (11206)8 (systematic$ adj3 (review$ or overview)).mp. (4771)9 or/2-8 (1421515)10 1 and 9 (1326)11 limit 10 to english (1214)12 health services for the aged/ (9170)13 exp rehabilitation/ (131232)14 12 and 13 (754)15 exp Evaluation Studies/ (445487)16 9 or 15 (1691415)17 14 and 16 (136)18 17 not 10 (113)19 hip fractures/ or femoral neck fractures/ (9225)20 rh.fs. (89570)21 (geriatric$ or elder$ or older or aged care or aged person$).ti. (69830)22 20 or 21 or 13 (259673)23 19 and 22 (1624)24 orthogeriatric$.mp. (19)25 23 or 24 (1632)26 16 and 25 (537)27 18 or 26 (648)28 limit 27 to english (520)29 28 not 11 (497)30 from 29 keep (selected references)(54)31 from 30 keep 1-54 (54)32 patient care team/ (30606)33 1 or 12 or 21 or geriatrics/ (80079)34 32 and 33 (1321)35 16 and 34 (216)36 35 not (29 or 10) (124)37 limit 36 to english (108)38 from 37 keep (selected references) (37)39 from 38 keep 1-37 (37)40 Rural Health Services/ (2623)41 Rural Health/ (13490)42 exp Telemedicine/ (5188)43 medically underserved area/ (2472)44 (rural or remote).ti. (21948)45 or/40-44 (36182)46 45 and 33 (796)47 46 and 16 (205)
WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
128
48 limit 47 to english (187)49 48 not (29 or 10 or 37) (156)50 from 49 keep (selected references)(6)51 from 50 keep 1-6 (6)
((program adj3 all-inclusive) and).mp. (45)53 (acute care adj2 elderly).mp. (68)54 52 or 53 (113)55 limit 54 to english (109)56 from 55 keep (selected references) (46)57 from 56 keep 1-46 (46)58 Acute Disease/ (123335)59 acute.ti. (195372)60 58 or 59 (242507)61 33 and 60 (2002)62 9 and 61 (445)63 limit 62 to english (356)64 63 not (10 or 29 or 37 or 49 or 55) (305)65 from 64 keep (selected references) (14)66 (subacute care or stepdown bed$ or postacute care or post-acute care or sub-acute care).mp. (760)67 66 and 33 (61)68 (day hospital or (hospital adj2 home) or home hospital or (acute adj2 home) or outreach).mp.
(6967)69 68 and 33 (685)70 67 or 69 (745)71 limit 70 to english (649)72 71 not (10 or 29 or 37 or 49 or 55 or 64) (568)73 72 and 9 (88)74 from 73 keep (selected references) (20)75 (geriatric unit or specialist geriatric or acute geriatric).mp. (353)76 ((elder$ or older or geriatric$ or aged) adj3 (unit or specialist)).tw. (924)77 75 or 76 (1012)78 9 and 77 (231)79 78 not (10 or 29 or 37 or 49 or 55 or 73 or 64) (149)80 limit 79 to english (131)81 from 80 keep (selected references)(10)82 (geriatric rehabilitation adj3 (clinic or unit)).tw. (67)83 from 82 keep (selected references)
Embase1 geriatrics/ (2391)2 (geriatric assessment or geriatric rehabilitation).tw. (693)3 elderly care/ or geriatric care/ (11807)4 (geriatric$ or elder$ or older or aged care or aged person$).ti. (43210)5 (geriatric orthopaedic or geriatric orthopedic).tw. (11)6 ((geriatric$ or elder$ or older) adj3 (clinic$ or unit$ or specialist)).tw. (4242)7 (acute geriatric$ or geriatric acute).tw. (143)8 orthogeriatric$.tw. (15)9 rural health care/ (1567)10 Rural Area/ (6521)11 (rural or remote).ti. (8110)12 (day hospital or (hospital adj2 home) or home hospital or (acute adj2 home) or outreach).tw.
(4080)13 (subacute care or stepdown bed$ or postacute care or post-acute care or sub-acute care).tw. (127)14 rehabilitation/ or functional assessment/ (21129)15 rh.fs. (27182)16 exp Hip Fracture/ (5710)17 (care team or team care or multidisciplinary team or interdisciplinary team).tw. (2659)
WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
129
18 telecommunication/ (3597)19 Randomized Controlled Trial/ (72600)20 Meta Analysis/ (15194)21 Randomization/ (5659)22 Clinical Trial/ (253999)23 EVALUATION/ or "EVALUATION AND FOLLOW UP"/ (14880)24 (systematic$ adj3 (review$ or overview)).mp. (4212)25 or/19-24 (278103)26 2 or 5 or 6 or 7 or 8 (4812)27 25 and 26 (585)28 1 or 3 or 4 (48731)29 or/9-18 (72156)30 28 and 29 and 25 (417)31 27 or 30 (937)32 limit 31 to english (855)33 from 32 keep (selected references)
Cinahl search1 Geriatric Assessment/ (1318)2 gerontologic nurse practitioners/ or gerontologic nursing/ (5184)3 (geriatric$ or elder$ or older or aged care or aged person$).ti. (19502)4 geriatric rehabilitation/ (875)5 Multidisciplinary Care Team/ (6605)6 femoral fractures/ or hip fractures/ (824)7 orthogeriatric$.mp. (6)8 (geriatric orthopaedic or geriatric orthopedic).mp. (8)9 ((elder$ or older or geriatric$) adj3 (unit or specialist or clinic)).tw. (343)10 acute geriatric.tw. (28)11 Rural Health Services/ (1077)12 Rural Health/ (981)13 Medically Underserved Area/ (113)14 TELEMEDICINE/ (815)15 (rural or remote).ti. (3663)16 Acute Disease/ (1577)17 acute.ti. (8173)18 exp Rehabilitation/ (43082)19 rh.fs. (14143)20 Health Services for the Aged/ (1871)21 Gerontologic Care/ (3725)22 exp clinical trials/ (17108)23 Comparative Studies/ (18537)24 exp Evaluation Research/ (5810)25 Meta Analysis/ (2707)26 (systematic$ adj3 (review$ or overview)).mp. (2685)27 evaluation/ or program evaluation/ (5553)28 or/22-27 (46144)29 or/11-15 (5149)30 1 or 4 or 7 or 8 or 10 (2181)31 28 and 30 (270)32 2 or 3 or 20 or 21 or 30 (26103)33 28 and 29 and 32 (34)34 5 or 6 or 16 or 17 or 18 or 19 (64436)35 32 and 34 and 28 (597)36 31 or 33 or 35 (723)37 limit 36 to english (720)38 from 37 keep (selected references)

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
130
Cross database free text search of Cinahl, Embase, Medline, Pre-Medline1 ((program$ adj2 all inclusive) and elder$).mp. (111)2 (acute care adj2 elder$).mp. (185)3 stepdown bed$.mp. (0)4 step-down bed$.mp. (5)5 (elder$ or older or geriatric$ or aged care or aged person$).tw. (333206)6 (geriatric unit or specialist geriatric or acute geriatric).mp. (653)7 (geriatric rehabilitation adj3 (clinic or unit)).tw. (167)8 "geriatric evaluation and management".tw. (152)9 ((nurse led or GP-led or general practitioner led) and (geriatric or elder$ or older or aged)).
tw. (80)10 (geriatric evaluation or geriatric management).tw. (337)11 (subacute care or sub-acute care or postacute care or post-acute care).tw. (804)12 11 and 5 (128)13 1 or 2 or 4 or 6 or 7 or 8 or 9 or 10 or 12 (1620)14 remove duplicates from 13 (1095)15 limit 14 to english (931)16 letter.pt. (756776)17 15 not 16 (910)18 from 17 keep (selected references)19 (swing bed$ or deconditioning or transitional care).tw. (1567)20 (day hospital or home hospital or "hospital at home").tw. \21 19 or 2022 5 and 2123 limit 22 to english24 remove duplicates from 2325 24 not 1526 from 26 keep (selected references)
SEARCHES FROM OTHER SOURCES
Other databases and sources without indexing were searched using combinations of words from thestrategies given above and adapted for the volume and conditions of each individual source.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
131
Appendix 1b:Search strategy for Section 3
SEARCH STRATEGIES
Medline1 Health Services for the Aged/ (9253)2 ((health adj2 service$) adj3 (elderly or aged or geriatric)).tw. (569)3 1 or 2 (9553)4 position statement$.tw. (1004)5 exp Societies, Medical/ (33594)6 organizational policy/ (9357)7 guidelines/ or practice guidelines/ (34474)8 Health Planning Guidelines/ (1627)9 Health Planning/ (17276)10 (polic$ or statement$).ti. (25619)11 Interprofessional Relations/ (26407)12 or/4-11 (139660)13 3 and 12 (613)14 limit 13 to english language (529)15 from 14 keep [SELECTED REFERENCES] (97)16 triage/ (3254)17 (3 and 16) not 13 (12)18 limit 17 to english language (12)19 from 18 keep [SELECTED REFERENCES] (2)20 og.fs. (188540)21 (3 and 20) not (13 or 18) (2303)22 limit 21 to english language (1978)23 limit 22 to review (144)24 from 23 [SELECTED REFERENCES] (23)25 15 or 19 or 24 (122)
Embase1 exp *elderly care/ (6353)2 (service$ adj3 (elderly or aged or geriatric)).tw. (910)3 1 or 2 (7020)4 position statement$.tw. (383)5 exp *health care delivery/ (66807)6 *health care planning/ (1778)7 *health care policy/ (9073)8 medical society/ (13078)9 (polic$ or statement$).ti. (10507)10 exp *practice guideline/ (4364)11 health service/ (14749)12 or/4-11 (112908)13 3 and 12 (1732)14 exp *elderly care/ (6353)15 (2 or 14) and 12 (1732)16 limit 15 to english language (1490)17 from 16 keep[SELECTED REFERENCES] (114)

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
132
Psychinfo1 elder care/ (813)2 geriatrics/ or geriatric patients/ or geriatric psychiatry/ or gerontology/ or geriatric assessment/ or
geriatric psychotherapy/ (8264)3 ((elder$ or geriatric$ or older) adj3 (servic$ or framework$ or polic$ or guideline$
statement)).tw. (2172)4 or/1-3 (10609)5 position statement$.tw. (118)6 treatment guidelines/ or treatment planning/ (1232)7 health care policy/ (1357)8 health care services/ or mental health services/ or community services/ or integrated services/ or
quality of services/ or rehabilitation/ or social services/ (28344)9 4 and 8 (1397)10 limit 9 to english language (1336)11 limit 10 to (("380 aged <age 65 yrs and older>" or "390 very old <age 85 yrs and older>") and
yr=1970-2003) (1113)12 from 11 keep [SELECTED REFERENCES] (79)
Cinahl1 Health Services for the Aged/ (1907)2 ((elderly or aged or geriatric or old$) adj3 (service$ or program$ or polic$)).mp. [mp=title, cinahl
subject headings, abstract, instrumentation] (2798)3 Gerontologic Care/ (3851)4 or/1-3 (7684)5 position statement$.tw. (993)6 og.fs. (11047)7 Health Policy/ (6563)8 exp *"Health and Welfare Planning"/ (10103)9 collaboration/ or interprofessional relations/ (7940)10 PRACTICE GUIDELINES/ (5290)11 (polic$ or statement$).ti. (7985)12 *"Health and Welfare Planning"/ (647)13 or/5-12 (44972)14 4 and 13 (925)15 limit 14 to english (922)16 from 15 keep [SELECTED REFERENCES] (64)
SEARCHES FROM OTHER SOURCES
In databases and all other sources without controlled vocabulary combinations of the index terms andadditional keywords from the above strategies, were used in the search.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
133
Appendix 2:Included studies for Section 2
RETRIEVED STUDIES INCLUDED IN REVIEW APPRAISAL
Alessi, C. A., Stuck, A. E., Aronow, H. U., Yuhas, K. E., Bula, C., Madison, R., Gold, M., et al.(1997). The process of care in preventive in-home comprehensive geriatric assessment. Journal of theAmerican Geriatrics Society, 45, 1044-1050.
Applegate, W. B., Miller, S. T., Graney, M. J., Elam, J. T., Burns, R., & Akins, D. E. (1990). Arandomized, controlled trial of a geriatric assessment unit in a community rehabilitation hospital. NewEngland Journal of Medicine, 322, 1572-1578.
Avlund, K., Jepsen, E., Vass, M., & Lundemark, H. (2002). Effects of comprehensive follow-up homevisits after hospitalization on functional ability and readmissions among old patients. A randomizedcontrolled study. Scandinavian Journal of Occupational Therapy, 9, 17-22.
Bernabei, R., Landi, F., Gambassi, G., Sgadari, A., Zuccala, G., Mor, V., Rubenstein, L. Z., &Carbonin, P. (1998). Randomised trial of impact of model of integrated care and case management forolder people living in the community. BMJ, 316, 1348-1351.
Bogardus, S. T., Jr., Desai, M. M., Williams, C. S., Leo-Summers, L., Acampora, D., & Inouye, S. K.(2003). The effects of a targeted multicomponent delirium intervention on postdischarge outcomes forhospitalized older adults. American Journal of Medicine, 114, 383-390.
Boult, C., Boult, L., Murphy, C., Ebbitt, B., Luptak, M., & Kane, R. L. (1994). A controlled trial ofoutpatient geriatric evaluation and management. Journal of the American Geriatrics Society, 42, 465-470.
Boult, C., Boult, L. B., Morishita, L., Dowd, B., Kane, R. L., & Urdangarin, C. F. (2001). Arandomized clinical trial of outpatient geriatric evaluation and management. Journal of the AmericanGeriatrics Society, 49, 351-359.
Burns, R., Nichols, L. O., Graney, M. J., & Cloar, F. T. (1995). Impact of continued geriatric outpatientmanagement on health outcomes of older veterans. Archives of Internal Medicine, 155, 1313-1318.
Burns, R., Nichols, L. O., Martindale-Adams, J., & Graney, M. J. (2000). Interdisciplinary geriatricprimary care evaluation and management: two-year outcomes. Journal of the American GeriatricsSociety, 48, 8-13.
Burch, S., Longbottom, J., McKay, M., Borland, C., & Prevost, T. (1999). A randomized controlledtrial of day hospital and day centre therapy. Clinical Rehabilitation, 13, 105-112.
Cameron, I., Crotty, M., Currie, C., Finnegan, T., Gillespie, L., Gillespie, W., Handoll, H., et al.(2000). Geriatric rehabilitation following fractures in older people: A systematic review. HealthTechnology Assessment (Winchester, England), 4, 1-102.
Cameron, I. D., Handoll, H. H., Finnegan, T. P., Madhok, R., & Langhorne, P. (2003). Co-ordinatedmultidisciplinary approaches for inpatient rehabilitation of older patients with proximal femoralfractures. Cochrane Database of Systematic Reviews, 2.
Cavalieri, T. A., Chopra, A., Gray-Miceli, D., Shreve, S., Waxman, H., & Forman, L. J. (1993).Geriatric assessment teams in nursing homes: do they work?. Journal of the American OsteopathicAssociation, 93, 1269-1272.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
134
Cohen, H. J., Feussner, J. R., Weinberger, M., Carnes, M., Hamdy, R. C., Hsieh, F., Phibbs, C., &Lavori, P. (2002). A controlled trial of inpatient and outpatient geriatric evaluation and management.New England Journal of Medicine, 346, 905-912.
Counsell, S. R., Holder, C. M., Liebenauer, L. L., Palmer, R. M., Fortinsky, R. H., Kresevic, D. M., etal. (2000). Effects of a multicomponent intervention on functional outcomes and process of care inhospitalized older patients: a randomized controlled trial of Acute Care for Elders (ACE) in acommunity hospital. Journal of the American Geriatrics Society, 48, 1572-1581.
Eagle, D. J., Guyatt, G. H., Patterson, C., Turpie, I., Sackett, B., & Singer, J. (1991). Effectiveness of ageriatric day hospital. CMAJ, 144, 699-704.
Eng, C., Pedulla, J., Eleazer, G. P., McCann, R., & Fox, N. (1997). Program of All-inclusive Care forthe Elderly (PACE): an innovative model of integrated geriatric care and financing. Journal of theAmerican Geriatrics Society, 45, 223-232.
Engelhardt, J. B., Toseland, R. W., O'Donnell, J. C., Richie, J. T., Jue, D., & Banks, S. (1996). Theeffectiveness and efficiency of outpatient geriatric evaluation and management. Journal of theAmerican Geriatrics Society, 44, 847-856.
Epstein, A. M., Hall, J. A., Fretwell, M., Feldstein, M., DeCiantis, M. L., Tognetti, J., Cutler, C., et al.(1990). Consultative geriatric assessment for ambulatory patients. A randomized trial in a healthmaintenance organization. JAMA, 263, 538-544.
Evans, R. L., Connis, R. T., Hendricks, R. D., & Haselkorn, J. K. (1995). Multidisciplinaryrehabilitation versus medical care: a meta-analysis. Social Science & Medicine, 40, 1699-1706
Fabacher, D., Josephson, K., Pietruszka, F., Linderborn, K., Morley, J. E., & Rubenstein, L. Z. (1994).An in-home preventive assessment program for independent older adults: a randomized controlled trial.Journal of the American Geriatrics Society, 42, 630-638.
Forster, A., Young, J., & Langhorne, P. (2000). Medical day hospital care for the elderly versusalternative forms of care. Cochrane Database of Systematic Reviews.
Hansen, F. R., Poulsen, H., & Sorensen, K. H. (1995). A model of regular geriatric follow-up by homevisits to selected patients discharged from a geriatric ward: a randomized controlled trial. Aging(Milano), 7, 202-206.
Hogan, D. B., MacDonald, F. A., Betts, J., Bricker, S., Ebly, E. M., Delarue, B., Fung, T. S., Harbidge,C., Hunter, M., Maxwell, C. J., & Metcalf, B. (2001). A randomized controlled trial of a community-based consultation service to prevent falls. CMAJ, 165, 537-543.
Hui, E., & Woo, J. (2002). Telehealth for older patients: the Hong Kong experience. Journal ofTelemedicine and Telecare, 8 Suppl 3, 39-41.
Hyde, C. J., Robert, I. E., & Sinclair, A. J. (2000). The effects of supporting discharge from hospital tohome in older people. Age & Ageing, 29, 271-279.
Inouye, S. K., Bogardus, S. T., Jr., Charpentier, P. A., Leo-Summers, L., Acampora, D., Holford, T. R.,& Cooney, L. M., Jr. (1999). A multicomponent intervention to prevent delirium in hospitalized olderpatients. New England Journal of Medicine, 340, 669-676.
Inouye, S. K., Bogardus, S. T., Jr., Baker, D. I., Leo-Summers, L., & Cooney, L. M., Jr. (2000). TheHospital Elder Life Program: a model of care to prevent cognitive and functional decline in olderhospitalized patients. Journal of the American Geriatrics Society, 48, 1697-1706.
Inouye, S. K. (2000). Prevention of delirium in hospitalized older patients: risk factors and targetedintervention strategies. Annals of Medicine, 32, 257-263.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
135
Karppi, P. (1995). Effects of a geriatric inpatient unit on elderly home care patients: a controlled trial.Aging (Milano), 7, 207-211.
Karppi, P., & Tilvis, R. (1995). Effectiveness of a Finnish geriatric inpatient assessment. Two-yearfollow up of a randomized clinical trial on community-dwelling patients. Scandinavian Journal ofPrimary Health Care, 13, 93-98.
Kravitz, R. L., Reuben, D. B., Davis, J. W., Mitchell, A., Hemmerling, K., Kington, R. S., & Siu, A. L.(1994). Geriatric home assessment after hospital discharge. Journal of the American Geriatrics Society,42, 1229-1234.
Landi, F., Gambassi, G., Pola, R., Tabaccanti, S., Cavinato, T., Carbonin, P., & Bernabei, R. (1999).Impact of integrated home care services on hospital use. Journal of the American Geriatrics Society,47, 1430-1434.
Langhorne, P., Pollock, A., Asplund, K., Berman, P., Blomstrand, C., Dennis, M., Douglas, J., et al.(2002). What are the components of effective stroke unit care? Age & Ageing, 31, 365-371.
Lim, W., Lambert, S., & Gray, L. (2003).Effectiveness of case management and post-acute services inolder people after hospital discharge. Medical Journal of Australia, 178, 262-266.
Malone, M., Hill, A., & Smith, G. (2002). Three-month follow up of patients discharged from ageriatric day hospital. Age and Ageing, 31, 471-475.
Melin, A. L., Hakansson, S., & Bygren, L. O. (1993). The cost-effectiveness of rehabilitation in thehome: a study of Swedish elderly. American Journal of Public Health, 83, 356-362.
Melin, A. L., Wieland, D., Harker, J. O., & Bygren, L. O. (1995). Health outcomes of post-hospital in-home team care: Secondary analysis of a Swedish trial. Journal of the American Geriatrics Society, 43,301-307.
Nikolaus, T., Specht-Leible, N., Bach, M., Oster, P., & Schlierf, G. (1999). A randomized trial ofcomprehensive geriatric assessment and home intervention in the care of hospitalized patients. Age &Ageing, 28, 543-550.
Parker, G., Bhakta, P., Katbamna, S., Lovett, C., Paisley, S., Parker, S., Phelps, K., et al. (2000). Bestplace of care for older people after acute and during subacute illness: a systematic review. Journal ofHealth Services & Research Policy, 5, 176-189.
Pitkala, K. (1998). The effectiveness of day hospital care on home care patients. Journal of theAmerican Geriatrics Society, 46, 1086-1090.
Reuben, D. B., Borok, G. M., Wolde-Tsadik, G., Ershoff, D. H., Fishman, L. K., Ambrosini, V. L., Liu,Y., et al. (1995). A randomized trial of comprehensive geriatric assessment in the care of hospitalizedpatients. New England Journal of Medicine, 332, 1345-1350.
Ritchie, C., Wieland, D., Tully, C., Rowe, J., Sims, R., & Bodner, E. (2002). Coordination andadvocacy for rural elders (CARE): a model of rural case management with veterans. Gerontologist, 42,399-405.
Rizzo, J. A., Bogardus, S. T., Jr., Leo-Summers, L., Williams, C. S., Acampora, D., & Inouye, S. K.(2001). Multicomponent targeted intervention to prevent delirium in hospitalized older patients: what isthe economic value? Medical Care, 39, 740-752.
Rockwood, K., Stadnyk, K., Carver, D., MacPherson, K. M., Beanlands, H. E., Powell, C., Stolee, P.,et al. (2000). A clinimetric evaluation of specialized geriatric care for rural dwelling, frail older people.Journal of the American Geriatrics Society, 48, 1080-1085.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
136
Rubenstein, L. Z., Josephson, K. R., Wieland, G. D., English, P. A., Sayre, J. A., & Kane, R. L. (1984).Effectiveness of a geriatric evaluation unit. A randomized clinical trial. New England Journal ofMedicine, 311, 1664-1670.
Rubenstein, L. Z., Wieland, G. D., Josephson, K. R., Rosbrook, B., Sayre, J., & Kane, R. L. (1988).Improved survival for frail elderly inpatients on a geriatric evaluation unit (GEU): who benefits?Journal of Clinical Epidemiology, 41, 441-449
Rubenstein, L. Z., Josephson, K. R., Harker, J. O., Miller, D. K., & Wieland, D. (1995). The SepulvedaGEU Study revisited: long-term outcomes, use of services, and costs. Aging (Milano), 7, 212-217.
Rubin, C. D., Sizemore, M. T., Loftis, P. A., & De Mola, N. L. (1993). A randomized, controlled trialof outpatient geriatric evaluation and management in a large public hospital. Journal of the AmericanGeriatrics Society, 41, 1023-1028.
Salgado, R., Ehrlich, F., Banks, C., Browne, E., Buckman, S., & Burraston, B. (1995). A mobilerehabilitation team program to assist patients in nursing homes rehabilitate and return to their homes.Archives of Gerontology & Geriatrics, 20, 255-261.
Saltvedt, I., Mo, E. S., Fayers, P., Kaasa, S., & Sletvold, O. (2002). Reduced mortality in treatingacutely sick, frail older patients in a geriatric evaluation and management unit. A prospectiverandomized trial. Journal of the American Geriatrics Society, 50, 792-798.
Scott, I. (1999). Optimising care of the hospitalised elderly. A literature review and suggestions forfuture research. Australian & New Zealand Journal of Medicine, 29, 254-264.
Silverman, M., Musa, D., Martin, D. C., Lave, J. R., Adams, J., & Ricci, E. M. (1995). Evaluation ofoutpatient geriatric assessment: a randomized multi-site trial. Journal of the American GeriatricsSociety, 43, 733-740.
Siu, A. L., Morishita, L., & Blaustein, J. (1994). Comprehensive geriatric assessment in a day hospital.Journal of the American Geriatrics Society, 42, 1094-1099.
Siu, A. L., Kravitz, R. L., Keeler, E., Hemmerling, K., Kington, R., Davis, J. W., Mitchell, A., et al.(1996). Postdischarge geriatric assessment of hospitalized frail elderly patients. [comment]. Archives ofInternal Medicine, 156, 76-81.
Stuck, A. E., Siu, A. L., Wieland, G. D., Adams, J., & Rubenstein, L. Z. (1993). Comprehensivegeriatric assessment: a meta-analysis of controlled trials. Lancet, 342, 1032-1036
Stuck, A. E., Aronow, H. U., Steiner, A., Alessi, C. A., Bula, C. J., Gold, M. N., Yuhas, K. E., et al.(1995). A trial of annual in-home comprehensive geriatric assessments for elderly people living in thecommunity. New England Journal of Medicine, 333, 1184-1189.
Stuck, A. E., Minder, C. E., Peter-Wuest, I., Gillmann, G., Egli, C., Kesselring, A., Leu, R., et al.(2000). A randomised trial of in-home visits for disability prevention in community-dwelling olderpeople at low and high risk for nursing home admission. Archives of Internal Medicine, 160, 977-986.
Stuck, A. E., Egger, M., Hammer, A., Minder, C. E., & Beck, J. C. (2002). Home visits to preventnursing home admission and functional decline in elderly people: systematic review and meta-regression analysis. JAMA, 287, 1022-1028.
Styrborn, K. (1995). Early discharge planning for elderly patients in acute hospitals--an interventionstudy. Scandinavian Journal of Social Medicine, 23, 273-285
Tinetti, M. E., Baker, D., Gallo, W. T., Nanda, A., Charpentier, P., & O'Leary, J. (2002). Evaluation ofrestorative care vs usual care for older adults receiving an acute episode of home care. JAMA, 287,2098-2105.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
137
Toseland, R. W., O'Donnell, J. C., Engelhardt, J. B., Hendler, S. A., Richie, J. T., & Jue, D. (1996).Outpatient geriatric evaluation and management. Results of a randomized trial. Medical Care, 34, 624-640.
Tucker, M. A., Davison, J. G., & Ogle, S. J. (1984). Day hospital rehabilitation--effectiveness and costin the elderly: a randomised controlled trial. BMJ, 289, 1209-1212.
von Sternberg, T., Hepburn, K., Cibuzar, P., Convery, L., Dokken, B., Haefemeyer, J., Rettke, S., et al.(1997). Post-hospital sub-acute care: an example of a managed care model. Journal of the AmericanGeriatrics Society, 45, 87-91.
Wieland, D., Lamb, V. L., Sutton, S. R., Boland, R., Clark, M., Friedman, S., Brummel-Smith, K., etal. (2000). Hospitalization in the Program of All-Inclusive Care for the Elderly (PACE): Rates,concomitants, and predictors. Journal of the American Geriatrics Society, 48, 1373-1380.
Williams, M. E., Williams, T. F., Zimmer, J. G., Hall, W. J., & Podgorski, C. A. (1987). How does theteam approach to outpatient geriatric evaluation compare with traditional care: a report of a randomizedcontrolled trial. Journal of the American Geriatrics Society, 35, 1071-1078.
Yeo, G., Ingram, L., Skurnick, J., & Crapo, L. (1987). Effects of a geriatric clinic on functional healthand well-being of elders. Journal of Gerontology, 42, 252-258.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
138

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
139
Appendix 3:Excluded studies from Section 2
RETRIEVED STUDIES EXCLUDED FOR REVIEW
The following studies were retrieved as full text articles but were excluded as these either did not meetthe inclusion criteria, were not specifically relevant to the topic, had inadequate descriptions ofspecialist geriatric service delivery models or were considered not to add any additional evidenceregarding the efficacy of a particular model of service.
Alexander, T. (1990). The elderly in acute care: a literature review. Dimensions in Health Service, 67,27-33.
Asplund, K., Gustafson, Y., Jacobsson, C., Bucht, G., Wahlin, A., Peterson, J., Blom, J. O., et al.(2000). Geriatric-based versus general wards for older acute medical patients: a randomizedcomparison of outcomes and use of resources. Journal of the American Geriatrics Society, 48, 1381-1388.
Beck, A., Scott, J., Williams, P., Robertson, B., Jackson, D., Gade, G., & Cowan, P. (1997). Arandomized trial of group outpatient visits for chronically ill older HMO members: the CooperativeHealth Care Clinic. Journal of the American Geriatrics Society, 45, 543-549.
Borok, G. M., Reuben, D. B., Zendle, L. J., Ershoff, D. H., Wolde-Tsadik, G., Rubenstein, L. Z.,Ambrosini, V. L., et al. (1994). Rationale and design of a multi-center randomized trial ofcomprehensive geriatric assessment consultation for hospitalized patients in an HMO. Journal of theAmerican Geriatrics Society, 42, 536-544.
Boult, C., Boult, L., Morishita, L., Smith, S. L., & Kane, R. L. (1998). Outpatient geriatric evaluationand management. Journal of the American Geriatrics Society, 46, 296-302.
Brazil, K., Bolton, C., Ulrichsen, D., & Knott, C. (1998). Substituting home care for hospitalization:the role of a quick response service for the elderly. Journal of Community Health, 23, 29-43.
Burch, S., Longbottom, J., McKay, M., Borland, C., & Prevost, T. (2000). The Huntingdon DayHospital Trial: secondary outcome measures. Clinical Rehabilitation, 14, 447-453.
Burch, S., & Borland, C. (2001). Collaboration, facilities and communities in day care services forolder people. Health & Social Care in the Community, 9, 19-30.
Burke, D. (2002). A geriatric evaluation and management programme prevented functional decline andreduced depression in high risk older adults. Evidence-Based Mental Health, 5, 9.
Byles, J. E. (2000). A thorough going over: evidence for health assessments for older persons.Australian & New Zealand Journal of Public Health, 24, 117-123.
Cameron, I. D., Lyle, D. M., & Quine, S. (1994). Cost effectiveness of accelerated rehabilitation afterproximal femoral fracture. Journal of Clinical Epidemiology, 47, 1307-1313.
Cameron, S., McKenzie, F., Warnock, L., & Farquhar, D. (2000). Impact of a nurse-ledmultidisciplinary team on an acute medical admissions unit. Health Bulletin, 58, 512-514.
Campion, E. W., Jette, A., & Berkman, B. (1983). An interdisciplinary geriatric consultation service: acontrolled trial. Journal of the American Geriatrics Society, 31, 792-796.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
140
Campbell, L. J., & Cole, K. D. (1987). Geriatric assessment teams. Clinics in Geriatric Medicine, 3,99-110.
Cefalu, C. A., Kaslow, L. D., Mims, B., & Simpson, S. (1995). Follow-up of comprehensive geriatricassessment in a family medicine residency clinic. Journal of the American Board of Family Practice, 8,263-269.
Chen, C. C., Heinemann, A. W., Granger, C. V., & Linn, R. T. (2002). Functional gains and therapyintensity during subacute rehabilitation: a study of 20 facilities. Archives of Physical Medicine &Rehabilitation, 83, 1514-1523.
Chin, J. J., Sahadevan, S., Tan, C. Y., Ho, S. C., & Choo, P. W. (2001). Critical role of functionaldecline in delayed discharge from an acute geriatric unit. Annals of the Academy of Medicine,Singapore, 30, 593-599.
Close, J., Ellis, M., Hooper, R., Glucksman, E., Jackson, S., & Swift, C. (1999). Prevention of falls inthe elderly trial (PROFET): a randomised controlled trial.[comment]. Lancet, 353, 93-97.
Cohen, H. J., Feussner, J. R., Weinberger, M., & al., e. (2002). Inpatient geriatric evaluation andmanagement did not reduce mortality but reduced functional decline. Evidence-Based Mental Health,5, 109.
Cole, M. G. (2001). The impact of geriatric post-discharge services on mental state. Age & Ageing, 30,415-418.
Collard, A. F., Bachman, S. S., & Beatrice, D. F. (1985). Acute care delivery for the geriatric patient:an innovative approach. QRB: Quality Review Bulletin, 11, 180-185.
Covinsky, K. E., Palmer, R. M., Kresevic, D. M., Kahana, E., Counsell, S. R., Fortinsky, R. H., &Landefeld, C. S. (1998). Improving functional outcomes in older patients: lessons from an acute carefor elders unit. Joint Commission Journal on Quality Improvement, 24, 63-76.
Crotty, M., Whitehead, C. H., Gray, S., & Finucane, P. M. (2002). Early discharge and homerehabilitation after hip fracture achieves functional improvements: a randomized controlled trial.Clinical Rehabilitation, 16, 406-413.
Davies, S. M. (1994). An evaluation of nurse-led team care within a rehabilitation ward for elderlypeople. Journal of Clinical Nursing, 3, 25-33.
Davies, L., Wilkinson, M., Bonner, S., Calverley, P. M., & Angus, R. M. (2000). "Hospital at home"versus hospital care in patients with exacerbations of chronic obstructive pulmonary disease:prospective randomised controlled trial. BMJ, 321, 1265-1268.
Evans, L. K., Yurkow, J., & Siegler, E. L. (1995). The CARE Program: a nurse-managed collaborativeoutpatient program to improve function of frail older people. Collaborative Assessment andRehabilitation for Elders. Journal of the American Geriatrics Society, 43, 1155-1160.
Farnworth, M. G., Kenny, P., & Shiell, A. (1994). The costs and effects of early discharge in themanagement of fractured hip.[erratum appears in Age Ageing 1995 Jul;24(4):367]. Age & Ageing, 23,190-194.
Fletcher, A. E., Jones, D. A., Bulpitt, C. J., & Tulloch, A. J. (2002). The MRC trial of assessment andmanagement of older people in the community: objectives, design and interventions. BMC HealthServices Research, 2, 21.
Fordyce, M., Bardole, D., Romer, L., Soghikian, K., & Fireman, B. (1997). Senior Team Assessmentand Referral Program--STAR. Journal of the American Board of Family Practice, 10, 398-406.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
141
Forster, A., Young, J., & Langhorne, P. (1999). Systematic review of day hospital care for elderlypeople. The Day Hospital Group. BMJ, 318, 837-841.
Fretwell, M. D., Raymond, P. M., McGarvey, S. T., Owens, N., Traines, M., Silliman, R. A., & Mor,V. (1990). The Senior Care Study. A controlled trial of a consultative/unit-based geriatric assessmentprogram in acute care. Journal of the American Geriatrics Society, 38, 1073-1081.
Fried, T. R., van Doorn, C., O'Leary, J. R., Tinetti, M. E., & Drickamer, M. A. (2000). Older person'spreferences for home vs hospital care in the treatment of acute illness. Archives of Internal Medicine,160, 1501-1506.
Germain, M., Knoeffel, F., Wieland, D., & Rubenstein, L. Z. (1995). A geriatric assessment andintervention team for hospital inpatients awaiting transfer to a geriatric unit: a randomized trial. Aging(Milano), 7, 55-60.
Gill, T. M., Baker, D. I., Gottschalk, M., Peduzzi, P. N., Allore, H., & Byers, A. (2002). A program toprevent functional decline in physically frail, elderly persons who live at home. New England Journalof Medicine, 347, 1068-1074.
Goldstein, F. C., Strasser, D. C., Woodard, J. L., & Roberts, V. J. (1997). Functional outcome ofcognitively impaired hip fracture patients on a geriatric rehabilitation unit. Journal of the AmericanGeriatrics Society, 45, 35-42.
Griffiths, P., Harris, R., Richardson, G., Hallett, N., Heard, S., & Wilson-Barnett, J. (2001).Substitution of a nursing-led inpatient unit for acute services: randomized controlled trial of outcomesand cost of nursing-led intermediate care. Age & Ageing, 30, 483-488.
Hadley, E. C. (1995). The science of the art of geriatric medicine. JAMA, 273, 1381-1383.
Harris, R. D., Henschke, P. J., Popplewell, P. Y., Radford, A. J., Bond, M. J., Turnbull, R. J., Hobbin,E. R., et al. (1991). A randomised study of outcomes in a defined group of acutely ill elderly patientsmanaged in a geriatric assessment unit or a general medical unit. Australian & New Zealand Journal ofMedicine, 21, 230-234.
Harris, D., Crilly, R. G., Stolee, P., & Ellett, F. K. (1999). Improving a system of care for elderlypersons in rural areas. Gerontologist, 39, 362-367.
Hauser, B., Robinson, J., Powers, J. S., & Laubacher, M. A. (1991). The evaluation of an intermediatecare--geriatric evaluation unit in a Veterans Administration Hospital. Southern Medical AssociationJournal, 84, 597-602.
Hebert, R., Robichaud, L., Roy, P. M., Bravo, G., & Voyer, L. (2001). Efficacy of a nurse-ledmultidimensional preventive programme for older people at risk of functional decline. A randomizedcontrolled trial. Age & Ageing, 30, 147-153.
Hendriksen, C., Lund, E., & Stromgard, E. (1984). Consequences of assessment and interventionamong elderly people: a three year randomised controlled trial. BMJ, 289, 1522-1524.
Hicks, B., Raisz, H., Segal, J., & Doherty, N. (1981). The triage experiment in coordinated care for theelderly. American Journal of Public Health, 71, 991-1003.
Hogan, D. B., & Fox, R. A. (1990). A prospective controlled trial of a geriatric consultation team in anacute-care hospital. Age & Ageing, 19, 107-113.
Hogan, D. B., Fox, R. A., Badley, B. W., & Mann, O. E. (1987). Effect of a geriatric consultationservice on management of patients in an acute care hospital. CMAJ, 136, 713-717.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
142
Husaini, B. A., Castor, R. S., Whitten-Stovall, R., Moore, S. T., Neser, W., Linn, J. G., & Griffin, D.(1990). An evaluation of a therapeutic health program for the black elderly. Journal of Health & SocialPolicy, 2, 67-85.
Huusko, T. M., Karppi, P., Avikainen, V., Kautiainen, H., & Sulkava, R. (2002). Intensive geriatricrehabilitation of hip fracture patients: a randomized, controlled trial. Acta Orthopaedica Scandinavica,73, 425-431.
Jones, J., Wilson, A., Parker, H., Wynn, A., Jagger, C., Spiers, N., & Parker, G. (1999). Economicevaluation of hospital at home versus hospital care: cost minimisation analysis of data from randomisedcontrolled trial. BMJ, 319, 1547-1550.
Kane, R. L., Homyak, P., Bershadsky, B., & Lum, Y. S. (2002). Consumer responses to the WisconsinPartnership Program for Elderly Persons: a variation on the PACE Model. Journals of GerontologySeries A-Biological Sciences & Medical Sciences, 57, M250-258.
Keeler, E. B., Robalino, D. A., Frank, J. C., Hirsch, S. H., Maly, R. C., & Reuben, D. B. (1999). Cost-effectiveness of outpatient geriatric assessment with an intervention to increase adherence. MedicalCare, 37, 1199-1206.
Kuder, L. C., Gairola, G. A., & Hamilton, C. C. (2001). Development of rural interdisciplinarygeriatrics teams. Gerontology & Geriatrics Education, 21, 65-79.
Lammers, J. E. (1992). Swing bed program in a small rural hospital: discharge outcome. SouthernMedical Journal, 85, 1184-1186.
Landi, F., Onder, G., Tua, E., Carrara, B., Zuccala, G., Gambassi, G., Carbonin, P., et al. (2001).Impact of a new assessment system, the MDS-HC, on function and hospitalization of homebound olderpeople: a controlled clinical trial. Journal of the American Geriatrics Society, 49, 1288-1293.
Leveille, S. G., Wagner, E. H., Davis, C., Grothaus, L., Wallace, J., LoGerfo, M., & Kent, D. (1998).Preventing disability and managing chronic illness in frail older adults: a randomized trial of acommunity-based partnership with primary care. Journal of the American Geriatrics Society, 46, 1191-1198.
Lightbody, E., & Baldwin, R. (2002). Inpatient geriatric evaluation and management did not reducemortality but reduced functional decline. Evidence-Based Mental Health, 5, 109.
Lightbody, E., Watkins, C., Leathley, M., Sharma, A., & Lye, M. (2002). Evaluation of a nurse-ledfalls prevention programme versus usual care: a randomized controlled trial. Age & Ageing, 31, 203-210.
Marcantonio, E. R., Flacker, J. M., Wright, R. J., & Resnick, N. M. (2001). Reducing delirium after hipfracture: a randomized trial. Journal of the American Geriatrics Society, 49, 516-522.
Martin, F., Oyewole, A., & Moloney, A. (1994). A randomized controlled trial of a high supporthospital discharge team for elderly people. Age & Ageing, 23, 228-234.
McCorkle, R., Strumpf, N. E., Nuamah, I. F., Adler, D. C., Cooley, M. E., Jepson, C., Lusk, E. J., &Torosian, M. (2000). A specialized home care intervention improves survival among older post-surgical cancer patients. Journal of the American Geriatrics Society, 48, 1707-1713.
McDowell, B. J., Silverman, M., Martin, D., Musa, D., & Keane, C. (1994). Identification andintervention for urinary incontinence by community physicians and geriatric assessment teams. Journalof the American Geriatrics Society, 42, 501-505.
Melin, A. L., & Bygren, L. O. (1992). Efficacy of the rehabilitation of elderly primary health carepatients after short-stay hospital treatment. Medical Care, 30, 1004-1015.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
143
Melin, A. L. (1995). A randomized trial of multidisciplinary in-home care for frail elderly patientsawaiting hospital discharge. Aging (Milano), 7, 247-250.
Moss, J. E., Flower, C. L., Houghton, L. M., Moss, D. L., Nielsen, D. A., & Taylor, D. M. (2002). Amultidisciplinary care coordination team improves emergency department discharge planning practice.Medical Journal of Australia, 177, 435-439.
Mykyta, L., & English, J. (2002). Geriatric assessment--lessons from personal experience. AustralianHealth Review, 25, 83-90.
Naglie, G., Tansey, C., Kirkland, J. L., Ogilvie-Harris, D. J., Detsky, A. S., Etchells, E., Tomlinson, G.,O'Rourke, K., & Goldlist, B. (2002). Interdisciplinary inpatient care for elderly people with hipfracture: a randomized controlled trial. CMAJ, 167, 25-32.
Naylor, M., Brooten, D., Jones, R., Lavizzo-Mourey, R., Mezey, M., & Pauly, M. (1994).Comprehensive discharge planning for the hospitalized elderly: A randomized clinical trial. Annals ofInternal Medicine, 120, 999-1006.
Naylor, M. D. (2002). Transitional care of older adults. Annual Review of Nursing Research, 20, 127-147.
Nikolaus, T., Specht-Leible, N., Bach, M., Wittmann-Jennewein, C., Oster, P., & Schlierf, G. (1995).Effectiveness of hospital-based geriatric evaluation and management and home intervention team(GEM-HIT). Rationale and design of a 5-year randomized trial. Zeitschrift fur Gerontologie undGeriatrie, 28, 47-53.
Parkes, J., & Shepperd, S. (2000). Discharge planning from hospital to home. Cochrane Database ofSystematic Reviews.
Payne, S., Kerr, C., Hawker, S., Hardey, M., & Powell, J. (2002). The communication of informationabout older people between health and social care practitioners. Age & Ageing, 31, 107-117.
Philbin, E. F. (1999). Comprehensive multidisciplinary programs for the management of patients withcongestive heart failure. Journal of General Internal Medicine, 14, 130-135.
Pitkala, K. H., Strandberg, T. E., & Tilvis, R. S. (2001). Is it possible to reduce polypharmacy in theelderly? A randomised, controlled trial. Drugs & Aging, 18, 143-149.
Powell, C., & Nixon, M. (1996). Caring for patients in geriatric day hospitals: guidelines on therelationship between primary care physicians and specialist/consultants. Canadian Family Physician,42, 110-5, 117.
Province, M. A., Hadley, E. C., Hornbrook, M. C., Lipsitz, L. A., Miller, J. P., Mulrow, C. D., Ory, M.G., et al. (1995). The effects of exercise on falls in elderly patients. A preplanned meta-analysis of theFICSIT Trials. Frailty and Injuries: Cooperative Studies of Intervention Techniques. JAMA, 273, 1341-1347.
Reeves, D. J., Alborz, A., Hickson, F. S., Bamford, J. M., & Gosden, T. (2000). Community provisionof hearing aids and related audiology services. Health Technology Assessment (Winchester, England),4, 1-120.
Rich, M. W., Vinson, J. M., Sperry, J. C., Shah, A. S., Spinner, L. R., Chung, M. K., & Davila-Roman,V. (1993). Prevention of readmission in elderly patients with congestive heart failure: results of aprospective, randomized pilot study. Journal of General Internal Medicine, 8, 585-590.
Richardson, G., Griffiths, P., Wilson-Barnett, J., Spilsbury, K., & Batehup, L. (2001). Economicevaluation of a nursing-led intermediate care unit. International Journal of Technology Assessment inHealth Care, 17, 442-450.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
144
Richardson, J., Law, M., Wishart, L., & Guyatt, G. (2000). The use of a simulated environment (EasyStreet) to retrain independent living skills in elderly persons: A randomized controlled trial. Journals ofGerontology Series A-Biological Sciences & Medical Sciences, 55, M578-M584.
Reid, U. V., & Ploeg, J. (2002). An outpatient geriatric evaluation and management programme wasmore effective than usual care in preventing functional decline in high risk older adults. Evidence-Based Nursing, 5, 19.
Rubenstein, L. Z., Bernabei, R., & Wieland, D. (1994). Comprehensive geriatric assessment into thebreach. Aging (Milano), 6, 1-3.
Rubenstein, L. Z., Aronow, H. U., Schloe, M., Steiner, A., Alessi, C. A., Yuhas, K. E., Gold, M., et al.(1994). A home-based geriatric assessment, follow-up and health promotion program: design, methods,and baseline findings from a 3-year randomized clinical trial. Aging (Milano), 6, 105-120.
Shepperd, S., Harwood, D., Gray, A., Vessey, M., & Morgan, P. (1998). Randomised controlled trialcomparing hospital at home care with inpatient hospital care. II: Cost minimisation analysis. BMJ, 316,1791-1796.
Shepperd, S., & Iliffe, S. (2001). Hospital at home versus in-patient hospital care. Cochrane Databaseof Systematic Reviews.
Sinoff, G., Clarfield, A. M., Bergman, H., & Beaudet, M. (1998). A two-year follow-up of geriatricconsults in the emergency department. Journal of the American Geriatrics Society, 46, 716-720.
Stevens, R. S., Potter, J. M., & Smith, M. H. (1990). Effect on a geriatric service of opening a 25-bedward on the district general hospital site: an audit. Journal of the Royal College of Physicians ofLondon, 24, 107-111
Stewart, M., Suchak, N., Scheve, A., Popat-Thakkar, V., David, E., Laquinte, J., & Gloth, F. M., 3rd(1999). The impact of a geriatrics evaluation and management unit compared to standard care in acommunity teaching hospital. Maryland Medical Journal, 48, 62-67.
Sulch, D., Evans, A., Melbourn, A., & Kalra, L. (2002). Does an integrated care pathway improveprocesses of care in stroke rehabilitation? A randomized controlled trial. Age & Ageing, 31, 175-179.
Tinetti, M. E., Baker, D. I., Gottschalk, M., Williams, C. S., Pollack, D., Garrett, P., Gill, T. M., et al.(1999). Home-based multicomponent rehabilitation program for older persons after hip fracture: arandomized trial. Archives of Physical Medicine & Rehabilitation, 80, 916-922.
Tinetti, M. E., Baker, D. I., McAvay, G., Claus, E. B., Garrett, P., Gottschalk, M., Koch, M. L., et al.(1994). A multifactorial intervention to reduce the risk of falling among elderly people living in thecommunity. New England Journal of Medicine, 331, 821-827.
Toseland, R. W., O'Donnell, J. C., Engelhardt, J. B., Richie, J., Jue, D., & Banks, S. M. (1997).Outpatient geriatric evaluation and management: is there an investment effect? Gerontologist, 37, 324-332.
Tracey, F., Taylor, I. C., & McConnell, J. G. (1998). A prospective study of the process of assessmentand care management in the discharge of elderly patients from hospital. Ulster Medical Journal, 67,36-40.
Trentini, M., Semeraro, S., Rossi, E., Giannandrea, E., Vanelli, M., Pandiani, G., Bardelli, E., et al.(1995). A multicenter randomized trial of comprehensive geriatric assessment and management:experimental design, baseline data, and six-month preliminary results. Aging (Milano), 7, 224-233.
Trentini, M., Semeraro, S., Motta, M., Italian Study Group for Geriatric, A., & Management (2001).Effectiveness of geriatric evaluation and care. One-year results of a multicenter randomized clinicaltrial. Aging (Milano), 13, 395-405

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
145
Ward, D., Severs, M., Dean, T., & Brooks, N. (2003). Care home versus hospital and own homeenvironments for rehabilitation of older people. Cochrane Protocol (updated 29 May 2001). CochraneDatabase of Systematic Reviews, 1.
Wieland, D., Stuck, A. E., Siu, A. L., Adams, J., & Rubenstein, L. Z. (1995). Meta-analytic methodsfor health services research: An example from geriatrics. Evaluation and the Health Professions, 18,252-282.
Williams, M. E., Rabiner, D. J., & Hunter, R. H. (1995). The interdisciplinary geriatric team evaluationproject. A new approach to the delivery of geriatric medicine in geographically remote locations. NorthCarolina Medical Journal, 56, 502-505.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
146

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
147
Appendix 4:Included studies for Section 3
RETRIEVED STUDIES INCLUDED IN REVIEW APPRAISAL
American Geriatrics Society (1999). Role of the geriatrician in managed care: American GeriatricSociety position statement.: American Geriatric Society. Available fromhttp://www.americangeriatrics.org Accessed on 31/03/03.
American Geriatrics Society (2000). Care management: American Geriatric Society position statement:American Geriatrics Society. Available from: http://www.americangeriatrics.org Accessed on31/03/03.
American Geriatrics Society (2002). Improving the quality of transitional care for persons withcomplex care needs: American Geriatrics Society position statement: American Geriatrics Society.Available from: http://www.americangeriatrics.org Accessed on 31/03/03.
Anderson, W. F. (1986). Organization of health care services for the elderly. Journal of the AmericanGeriatrics Society, 34, 240-244.
Anonymous (2000). A statement of principles: toward improved care of older patients in surgical andmedical specialties. Journal of the American Geriatrics Society, 48, 699-701.
Bachman, S. S., Collard, A. F., Greenberg, J. N., Fountain, E., Huebner, T. W., Kimball, B., &Melendy, K. (1987). An innovative approach to geriatric acute care delivery: The Choate-Symmesexperience. Hospital & Health Services Administration, 32, 509-520.
Boult, C., Boult, L., & Pacala, J. T. (1998). Systems of care for older populations of the future. Journalof the American Geriatrics Society, 46, 499-505.
British Geriatrics Society (1995). Acute medical care of elderly people. London: British GeriatricsSociety. Available from: http://www.bgs.org.uk Accessed on 29/04/03.
British Geriatrics Society (1997a). NHS medical services for older people: BGS compendiumdocument A2. London: British Geriatrics Society. Available from: http://ww.bgs.org.uk Accessed on22/04/03.
British Geriatrics Society (1997b). Rehabilitation of older people. BGS compendium document A4.London. Available from: http://www.bgs.org.uk. Accessed on 22/04/03.
British Geriatrics Society (1997c). Seamless care: obstacles and solutions. BGS compendium documentD1. London: British Geriatrics Society. Available from: http://www.bgs.org.uk Accessed on 29/04/03.
British Geriatrics Society (1999). Guidelines for the implementation of clinical governance in geriatricmedicine: recommendations of the British Geriatrics Society and Royal College of Physicians. London:British Geriatrics Society. Available from: http://www.bgs.org.uk Accessed on 29/04/03.
British Geriatrics Society (2000). The older patient in the accident and emergency department: a jointstatement of the British Geriatrics Society, the British Association of Accident and EmergencyMedicine, and the Royal College of Nursing: compendium document C2. London. Available from:http://www.bgs.org.uk. Accessed on 29/04/03.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
148
British Geriatrics Society (2001a). The BGS response to the National Service Framework for OlderPeople in England: delivery is the key - but we see some pitfall to be addressed! London. Availablefrom: http://www.bgs.org.uk Accessed on 22/04/03.
British Geriatrics Society (2001b). National service framework for older people in England: a shortsummary. London: British Geriatrics Society. Available from: http://www.bgs.org.uk Accessed on22/04/03.
British Geriatrics Society (2003). Standards of medical care for older people: expectations andrecommendations. BGS compendium document A3. London: British Geriatrics Society. Availablefrom: http://www.bgs.org.uk Accessed on 22/04/03.
Brown, J. Strategic directions for older people's health services 2001-2006: background paper.Brisbane: Aged and Community Care Reform Unit.
Campion, E. W. (2002). Specialized care for elderly patients. New England Journal of Medicine, 346,874.
Evans, J. (2000). Principles of care. In G. J. Evans, T. F. Williams, B. L. Beattie, J. P. Michel & G. K.Wilcock (Eds.), Oxford textbook of geriatric medicine. Oxford: Oxford University Press.
Flaherty, M. J. (1987). Health care of the elderly: the need for interprofessional cooperation. CMAJ,137, 381-383.
Grachek, M. K. (2000). Joint Commission accreditation: a framework for coordinating care for olderadults. Geriatric Nursing, 21, 326-327.
Langhorne, P. (2000). Stroke units. In G. J. Evans, A. F. Williams, A. M. Beattie, J. P. Michel & G. K.Wilcock (Eds.), Oxford textbook of geriatric medicine. Oxford: Oxford University Press.
Ng, Y. Y. (1987). The development and organization of medical services for the elderly in Hong Kong.Annals of the Academy of Medicine, Singapore, 16, 31-34.
Sainsbury, R. (1994). The effects of the health reforms on the elderly. Health Manager, 1, 13-15.
Sainsbury, R., & Wilkinson, T. J. (1999). The achievements of geriatric medicine. New ZealandMedical Journal, 112, 407-410.
Solomon, D. H., Burton, J. R., Lundebjerg, N. E., & Eisner, J. (2000). The new frontier: increasinggeriatrics expertise in surgical and medical specialties. Journal of the American Geriatrics Society, 48,702-704.
Swift, C. G., & Severs, M. P. (1997). The challenges of service provision. Age & Ageing, 26, 30-42.

WHAT IS THE EVIDENCE FOR THE EFFECTIVENESS OF SPECIALIST GERIATRIC SERVICES IN ACUTE, POST-ACUTE AND SUB-ACUTE SETTINGS?
149
Appendix 5:Excluded studies from Section 3
RETRIEVED STUDIES EXCLUDED FOR REVIEW AND REASON FOREXCLUSION
Anonymous (1999). Improving geriatric services: sources of help. Advice from the Royal College ofPhysicians Committee on Geriatrics. Journal of the Royal College of Physicians of London, 33, 152.
About organisations.
Anonymous (2001). Guideline for the prevention of falls in older persons. American Geriatrics Society,British Geriatrics Society, and American Academy of Orthopaedic Surgeons Panel on Falls Prevention.Journal of the American Geriatrics Society, 49, 664-672.
Falls prevention not service description.
Foster Alter, C. (1988). The changing structure of elderly service delivery systems. Gerontologist, 28,91-98.
Research case studies.
Reed, I. (2002). The aged care strategy 2002-2007. Older people's health services: draft forconsultation. Brisbane: Aged and Community Care Reform Unit. Available from:http://www.health.qld.gov.au/accru/aged_care Accessed on 29/04/03.
Principles of care.
Willis, M. (2002). The aged care strategy 2002-2007. Acute hospital services for older people: draft forconsultation. Brisbane: Aged and Community Care Reform Unit. Available from:http://www.health.qld.gov.au/accru/aged_care Accessed on 29/04/03.
Principles of care.


















