

GERD solo patologia gastro-esofagea? · asthma attacks and even pneumonia. In the case of asthma,...
77
GERD solo patologia gastro - esofagea? Prof. Giancarlo D’Ambrosio UNIVERSITÀ DI ROMA “LA SAPIENZA” Resp. UO “Chirurgia Generale ad Indirizzo Colo-Rettale” Az. Policlinico “Umberto I”, Roma
Transcript of GERD solo patologia gastro-esofagea? · asthma attacks and even pneumonia. In the case of asthma,...

GERD
solo patologia gastro-esofagea?
Prof. Giancarlo D’AmbrosioUNIVERSITÀ DI ROMA “LA SAPIENZA”
Resp. UO “Chirurgia Generale ad Indirizzo Colo-Rettale”Az. Policlinico “Umberto I”, Roma

• Gastroesophageal reflux
disease (GERD) is one
of the most frequent
benign disorders of the
upper gastrointestinal
tract.

The Montreal definition and classification of
GERD
• “a prevalent and chronic condition in which
reflux of the stomach contents into the
oesophagus causes a range of troublesome
symptoms (including heartburn, acid
regurgitation and epigastric pain) and
complications”
Vakil et al. The Montreal definition and classification of GERD: a
global evidence-based consensus. Am J Gastroenterol. 2006

GERD: epidemiology
• In developed countries, the prevalence of
gastro-oesophageal reflux disease (defined
by symptoms of heartburn, acid
regurgitation, or both, at least once a week)
is 10–20%, whereas in Asia the prevalence
is roughly less than 5%.
El-Serag H, Hill C, Jones R. Systematic review: the epidemiology of gastro-oesophageal
reflux disease in primary care, using the UK General Practice Research Database. Aliment
Pharmacol Ther 2009; 29: 470–80.
Dent J, El-Serag HB, Wallander MA, Johansson S. Epidemiology of gastro-oesophageal
reflux disease: a systematic review. Gut 2005; 54: 710–17.

GERD: epidemiology
• In the USA, this disease is the most common gastrointestinal diagnosis to prompt an outpatient clinic visit (8·9 million visits in 2009).
• The rising prevalence of gastro-oesophageal reflux disease seems to be related to the rapidly increasing prevalence of obesity.
Peery AF, Dellon ES, Lund J, et al. Burden of gastrointestinal disease in the United States:
2012 update. Gastroenterology 2012; 143: 1179–87.

GERD: epidemiology
• incidence of gastro oesophageal reflux
disease diagnosis in uk general practice
El-Serag H, Hill C, Jones R. Systematic review: the epidemiology of gastro-oesophageal
reflux disease in primary care, using the UK General Practice Research Database. Aliment
Pharmacol Ther 2009; 29: 470–80.

GERD: Pathophysiology
Dysfunction of the oesophagogastric junction
• Three components make up the
oesophagogastric junction:
– the lower oesophageal sphincter,
– the crural diaphragm,
– and the anatomical flap valve.
• This complex functions as an antireflux
barrier.


GERD: Pathophysiology
Helicobacter pylori
• Helicobacter pylori does not have an
important role in the pathogenesis of gastro-
oesophageal reflux disease. Eradication of
the microorganism does not lead to an
increased chance of development of the
disorder

Diagnostic investigations
The most important diagnostic investigations to prove
the presence of GERD are
• endoscopy
• long-term impedance pH monitoring (or pH
monitoring).

• Endoscopy can directly evaluate the
Esophago-Gastric Junction and make
biopsies in order to identificate
precancerous lesions (Barrett’s Esophagus)
Diagnostic investigations

Los Angeles classification of reflux oesophagitis
•grade A, endoscopic abnormalities are restricted to one or more mucosal
lesions with a maximum length of 5 mm.
•In grade B, one or more mucosal breaks are present, with a maximum
length of more than 5 mm but non-continuous across mucosal folds.
•In grade C, mucosal breaks are continuous between at least two
mucosal folds, but less than 75% of oesophageal circumference is
involved.
•In grade D, mucosal breaks encompass more than 75% of oesophageal
circumference
GERD: definition

Diagnostic investigations
• Manometry studies are
important prior to any
surgical procedure to
evaluate motility
disorders, especially
spastic motility disorders
or achalasia

Typical symptoms
• heartburn (pyrosis)
• regurgitation.
GERD: Signs & Symptoms

GERD: Signs & Symptoms
• Although reflux and heartburn happen
predominantly during the day, in particular
postprandially, both can also occur during
sleep.
• Nocturnal reflux is associated significantly
with severe oesophagitis and intestinal
metaplasia (Barrett’s oesophagus) and can
lead to sleep disturbance.

• Laryngopharyngeal reflux (LPR) is
implicated in the pathogenesis of various
upper airway inflammatory diseases as
sinusitis or dacryostenosis.
• 20% of the children with diagnosed LPR
showed pepsin in the tears.
Extra-oesophageal (or atypical)
symptoms

GERD: Signs & Symptoms
Extra-oesophageal (or atypical) symptoms
• Asthma
• cough
• disturbances in cardiac rhythm
• pharyngitis, sinusitis
• recurrent otitis media
• pulmonary fibrosis

GERD: Signs & Symptoms
Extra-oesophageal (or atypical) symptoms
• hoarseness
• sleep apnoea
• tooth decay
• difficulty swallowing
• foreign body sensation in the throat
• growths on the vocal cords (granulomas)

GERD & ASTHMA

Asthma causes GERD or
GERD causes asthma?
• GERD present in 30-90% of adults with asthma
• 80% of asthmatic patients shows pH-metric abnormalities
• 77% of asthmatic patients show symptoms related to reflux
• 40% of asthmatic patients suffering from esophagitis
In particular, it is unclear which of the two
disorders induce the other and “vice versa”.

GERD causes asthma?
• theory of microaspiration: the aspiration of gastricmaterial refluxed in the tracheobronchial tree causesbronchoconstriction and the onset of chronic bronchitis,asthma attacks and even pneumonia. In the case of asthma,this mechanism is deemed secondary
• theory of vagal reflex: the stimulation of receptors of theesophageal submucosa induces a reflection of the vagusnerve, which causes a deterioration of respiratory function.This mechanism, which can be demonstrated through theacid perfusion test, is the most likely to explain the onset ofchronic cough and asthma.

• Student 17 year old, non-smoker, no family history of asthma and / or atopy
• Recurrent episodes of urticaria in anamnesis
• It refers to a week sense of "tightness" in the epigastric and dyspnoea predominantly postprandial
• The physical examination of the chest is negative, except for a few hisses and groans expiratory auscultation.
• spirometry is performed
CLINICAL CASE

CLINICAL CASESpirometry revealed an obstructive ventilatory defect of medium
severity with a good response to bronchodilator.

FURTHER INQUIRIES MADE
Prick test for inhalant allergens: NegativePRIST (Total IGE) 36.3: satisfactoryECP (eosinophil cationic protein) 5:32: satisfactoryBlood count: the normCXR: negative
THERAPY PRESCRIBED: beta adrenergic bronchodilator + inhaled
corticosteroid in combination: 4.5 mcg formoterol / budesonide 160 mcg x 2 / day

• 4.5 mcg formoterol / budesonide 160 mcg x 2 / day
• Budesonide 200 mcg x 2 / day
13/09/2007Discontinued therapy to improved symptoms
After a month, reappearance of oppression in the epigastric and predominantly postprandial dyspnea, while spirometry again reveals an obstructive ventilatory defect of medium severity.
It is again prescribed bronchodilator therapy, increasing the dose of inhaled corticosteroid.

gastroenterological consulting
Persists "air hunger" in post-prandial period.This symptom disappears during therapy
•Formoterol 4.5 mcg /
•Budesonide 160 mcg x 2 / day
11/10/07

gastroenterological consulting
EGDS: gastro esophageal reflux with mild
hyperemia of the gastric mucosa and
esophageal mucosa. Hp (-)
Pantoprazole 40 mg/die

23/07/13
• Currently, the patient no longer experiences the symptoms and performs maintenance therapy with proton pump inhibitor (pantoprazole 20 mg)
• It is to check once a year.

Therapy
• Antireflux therapy (both pharmacological and surgical) leads to an improvement in asthma symptoms in 70% of cases.
• The use of anti-reflux therapy also reduces the use of drugs commonly used in asthma care: Some asthma medications promote reflux.
• The intensive treatment for GERD is indicated in asthma associated with typical symptoms of reflux, non-allergic asthma, nocturnal asthma, asthma resistant to standard treatments and asthma with onset in adulthood.

GERD and COUGH
COUGH: HIDDEN EPIDEMIC
The incidence of cough symptom is
constantly growing and the
perception of doctors is that it is
not more of a problem mainly
seasonal but a symptom that
involves them all year.

Clinical Practice Guidelines
January 2006; 129(1_suppl) Diagnosis and Management of Cough: ACCP Evidence-Based
Clinical Practice Guidelines
• 70-90% of cases seen in clinical
practice• Upper airway cough syndrome (UACS)
• GERD
• Asthma

chronic cough and GERD prevalence
GERD: three prospective studies of Irwin during 17 years
• 10% (4th cause) in 1981
• 21% (3rd cause) in 1990
• 36% (2nd cause) in 1998
Jinnai M et al, Cough 2008

CRONIC COUGH
INCREASED
TRANSDIAPHRAGMATIC
PRESSURE
GASTROESOPHAGEAL
REFLUX
REFLEX DISTAL
ESOPHAGUS
TRACHEOBRONCHIAL
RELAXATION OF THE
LES IN CONNECTION
WITH SWALLOWING
TRANSITIONAL
RELAXATION OF LES
VICIOUS CIRCLE
Cough

GERD and AF

Atrial fibrillation in healthy heart
• 45 ys, ♂, smoker, alcoholic, oveweight;• Access to E.R. for prolonged palpitations on
waking;• Acknowledgement on ECG of atrial fibrillation
at 80 / min.

Atrial fibrillation in healthy heart
Cardiology consult:
• For several months extra-systolic palpitations
mainly in the early hours of the morning;
asymptomatic for angina; Echocardiogram:
Normal systolic function of the LV and normal
size of the left atrium;
• Infusion of flecainide with restoration of sinus
rhythm within one hour;
• Home tp: flecainide 100 mg 1 tablet x2 / day +
Bisoprolol 1.25 mg 1 tablet
• Holter ECG monitoring to a month.

Atrial fibrillation in healthy heart
Arrhythmological consulting
The patient reported
• worsening of extra-systolic palpitations morning despite
antiarrhythmic tp;
• an episode of atrial fibrillation after a large meal and liquor
abuse and remembers waking up just before a sense of 'weight
in the stomach associated with heartburn ";
• Holter monitoring: "... Several supraventricular extrasystoles,
mainly distributed in the night hours of recording, repetitive
(many couples and prejudice of max 15 beats) ....";
Gastroenterological consulting -> PPI

Atrial fibrillation in healthy heart
Cardiological examination
after a month of PPI:
• disappearance palpitations
• Holter ECG monitoring: satisfactory
• suspension of antiarrhythmic therapy

Atrial fibrillation in healthy heart,
but not healthy subject1. Vagal hyperstimulation induced by acid
reflux? (It has been seen that treatment with PPI would facilitate the conversion to sinus rhythm)
2. Inflammation district left atrium in patients with esophagitis?
3. Release of pro-inflammatory substances such as interleukin-1β, interleukin-6, CRP (C-reactive protein)?
4. chronic atrial ischemia induced by the reduced coronary flow because of acid reflux?
5. autoimmune mechanisms? (Autoantibodies against myosin heavy chain)
6. genetic factors? (Currently only hypothesised)
7. mechanical or inflammatory effect (linked to distal esophagitis) left atrium by a hiatal hernia?
Linz et al. Atrial fibrillation and gastroesophageal reflux disease: the cardiogastric interaction. EUROPACE. 31 May 2016

Extra-oesophageal (or
atypical) symptoms
Pharingo-laryngitis

Extra-oesophageal (or
atypical) symptoms
Hoarseness

Extra-oesophageal (or
atypical) symptoms
Recurrent otitis media

Extra-oesophageal (or
atypical) symptoms
Pulmonary fibrosis

Extra-oesophageal (or
atypical) symptoms
Sleep Apnoea

Extra-oesophageal (or
atypical) symptoms
Tooth decay

Extra-oesophageal (or
atypical) symptoms
Difficulty swallowing

Extra-oesophageal (or
atypical) symptoms
Foreign body sensation in the throat

Extra-oesophageal (or
atypical) symptoms
Growths on the vocal cords (granulomas)

Reduce fat in the diet,
Avoid spices, mint, chocolate,
carbonated drinks, coffee, tea
Stop smoking
Avoid excessive alcohol consumption
dietary and behavioral rules
dietary and behavioral rules
Avoid those movements that increase
abdominal pressure (push-ups on the bust)
and too tight clothing
Evaluate with the treating physician:
Medications that can accentuate Symptoms
Eg. Nitrates and calcium channel blockers, anti-
inflammatory drugs..

dietary and behavioral rules
Reduce body weight
(If the patient is overweight)
Elevate the headboard of the bed by
placing 10-15 cm thick
Bedtime no earlier than 3 hours between
meals.
A walk can be helpful

Medical therapy
The goal of medical therapy in GERD is to:
• control heartburn,
• heal gastroesophageal mucosal injuries,
• improve quality of life.
EAES recommendations for the management of gastroesophageal reflux
disease Surg Endosc (2014)

Medical therapy
• normalization of pH of gastric juice through
the use of alkali salts (weak bases)
• reduction of acid production
• administration of protective agents for the
gastric mucosa (sucralfate)
• acceleration of gastric emptying

Indication for surgical therapy
• Prior to the indication for surgery or any other invasive therapy, it must be proven that patients are in need of long- term treatment of GERD.
• Patients with continuous reduced quality of life, persistent troublesome symptoms, and/or progression of disease despite adequate PPI therapy in dosage and intake should be offered laparoscopic antireflux surgery after proper diagnostic testing.
EAES recommendations for the management of gastroesophageal reflux
disease Surg Endosc (2014)

Indication for surgical therapy
• There is evidence that laparoscopic
antireflux surgery can improve quality of
life in patients with altered anatomy,
massive acid exposure, nonacid reflux,
severe reduction in quality of life, and
progressive disease with need to increase
PPI dosage over the years
EAES recommendations for the management of gastroesophageal reflux
disease Surg Endosc (2014)


Indication for surgical therapy• Several randomized trials comparing PPI therapy
with antireflux surgery have been conducted. Three
of these trials showed an advantage for surgical
therapy in outcome and cost-effectiveness after a
few years, whereas one showed an advantage for
PPI therapy after 5 years
EAES recommendations for the management
of gastroesophageal reflux disease Surg Endosc (2014)

Indication for surgical therapy
Most frequently mentioned features leading to the indication for antireflux surgery:
• Typical symptoms for GERD
• Documented symptom-reflux correlation
• Year-long reflux history
• Reduced quality of life
• Need for PPI dosage increase
• Hiatal hernia
• Documented esophagitis (in the past before PPI)
• Proven LES incompetence
• Documented acid reflux
EAES recommendations for the management of gastroesophageal reflux
disease Surg Endosc (2014)
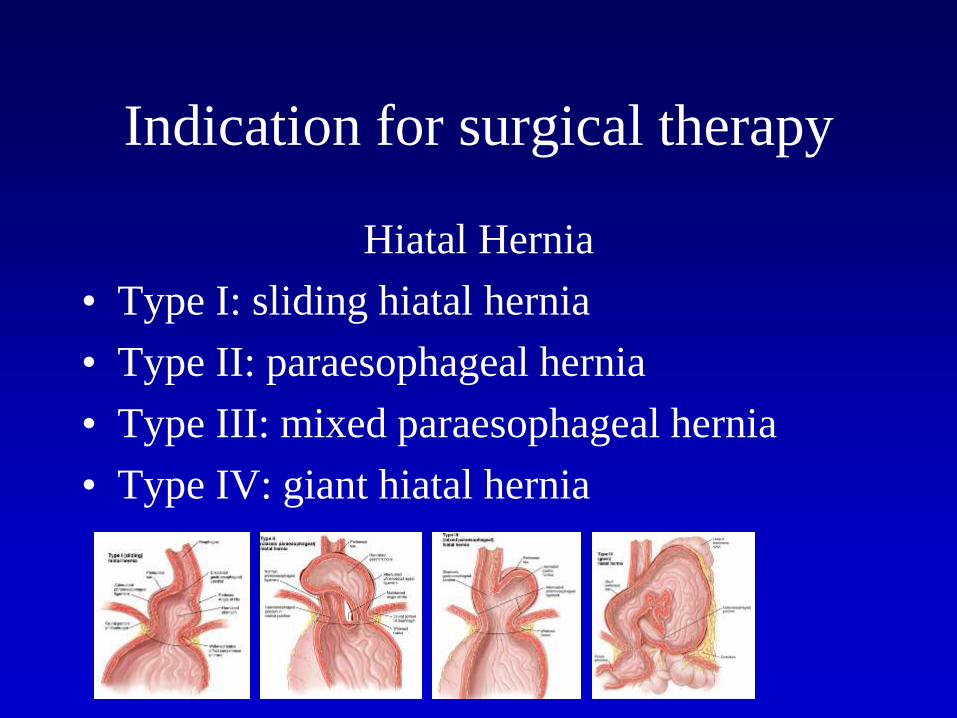
Indication for surgical therapy
Hiatal Hernia
• Type I: sliding hiatal hernia
• Type II: paraesophageal hernia
• Type III: mixed paraesophageal hernia
• Type IV: giant hiatal hernia

Indication for surgical therapy
Hiatal Hernia
• Type IV: giant hiatal hernia

Indication for surgical therapy
• Most of patients with extra-esophageal signs and symptoms benefits of medical therapy.
• Several patients with typical symptoms of GERD can benefit of surgical treatment.
• Patients with documented pathologic laryngopharyngeal reflux (LPR) and positive symptom correlation may benefit from a laparoscopic fundoplication.
EAES recommendations for the management of
gastroesophageal reflux disease. 2014

Surgical therapy
• Laparoscopic partial and total
fundoplications are currently the best
available surgical techniques to treat severe
GERD.

•TOTAL FUNDOPLICATION
• PARTIAL FUNDOPLICATION: TOUPET
FLOPPY-NISSEN
NISSEN-ROSSETTI
DOR
WHICH TECHNIQUE?

Laparoscopic surgery
of gastroesophageal reflux

Exposure of the operating region

esophagus access:
incision of pars condensa and dissection of the right pillar.

incision of the phrenoesophageal
membrane

dissection of the left pillar to the
left margin of the esophagus.

passage of retro-esophageal webbing

Exposure of the hiatus after esophageal mobilization

Rapprochement pillars of the diaphragm posteriorly
esophagus

valve passage posteriorly esophagus

Process according Nissen.
360°Process according Toupet
270°.

Robotic Dor Fundoplicatio

First the diagnosis (opponent's study)
then the strategy (tactics)
and then the victory on the field!


















