Genetics of susceptibility to malaria related phenotypes
7
Short communication Genetics of susceptibility to malaria related phenotypes Danielle Carpenter a, *, Ingegerd Rooth b , Anna Fa ¨ rnert c , Hind Abushama a , Rupert J. Quinnell a , Marie-Anne Shaw a a Institute of Integrative and Comparative Biology, Faculty of Biological Sciences, University of Leeds, Leeds LS2 9JT, UK b Nyamisati Malaria Research, Rufiji, National Institute for Medical Research, Dar-es-Salaam, Tanzania c Unit of Infectious Diseases, Department of Medicine, Karolinska Institute, Karolinska University Hospital Solna, S-17176 Stockholm, Sweden 1. Introduction Plasmodium falciparum malaria is a major cause of mortality and morbidity, particularly in sub-Saharan Africa. Individuals living in endemic areas may be subjected to constant sub-clinical malaria infection, but only a minority develop severe disease. Variations in disease pattern are attributable to a number of different factors, both environmental and genetic, that can determine whether an exposed individual develops parasitaemia (parasites in the blood), and the risk of a parasitaemic individual developing clinical disease. Over the course of the last decade a number of studies have evaluated genetics of quantitative malaria phenotypes, such as parasite density and the frequency of malaria episodes. Complex segregation analyses have established a genetic component of susceptibility to P. falciparum blood infection level (Garcia et al., 1998a; Rihet et al., 1998; Abel et al., 1993) and to clinical infection of malaria in a mixed P. falciparum and Plasmodium vivax population (Mackinnon et al., 2000). There are a number of studies which have aimed to identify loci involved with control of blood infection level and asymptomatic malaria. Linkage studies provided evidence for linkage between blood infection levels and the 5q31–q33 region in populations from Burkina Faso (Flori et al., 2003a) and Cameroon (Garcia et al., 1998b). Two-point and multipoint analyses provided evidence of linkage between mild malaria and the MHC region (Jepson et al., 1997; Flori et al., 2003b), and TDT analysis identified associations with a number of different TNF polymorphisms with both mild malaria and parasite density (Flori et al., 2005). More recently a genome-wide linkage analysis of malaria infection and mild disease showed evidence for linkage to chromosome 10p15 (Timmann et al., 2007). In the current study, we have investigated polymorphisms within a number of candidate genes that may play a role in susceptibility to parasite density and clinical infection, in a well- studied Tanzanian population. We build on previous studies by using family-based association methods to investigate blood infection levels and clinical infection data collected over a period of 7 years. Candidate gene regions (MHC class II and III, IL1, IL10, IL4, IL13, and TCRBV) were chosen from their identification in prior case control studies and/or their potential role in the control of malaria infection. Infection, Genetics and Evolution 9 (2009) 97–103 ARTICLE INFO Article history: Received 10 April 2008 Received in revised form 18 July 2008 Accepted 16 October 2008 Available online 31 October 2008 Keywords: Plasmodium falciparum Parasite density Clinical episodes TDT Association TNF ABSTRACT Previous studies have established a genetic component for susceptibility to malaria. Here we use a pedigree based approach, and transmission disequilibrium testing (TDT), to identify immune response genes that influence susceptibility to Plasmodium falciparum malarial phenotypes (parasite density and frequency of clinical episodes) in a Tanzanian population. Evidence for association was observed between markers in the TNF gene cluster and both the malarial phenotypes. There was weaker evidence for associations between HLA-DRB1*04, HLA-DRB1*10, and loci in the TCRBV region with parasite density. There was no evidence for association with polymorphisms in the IL10 promoter, IL1 gene cluster, or from the IL4/IL13 region. ß 2008 Elsevier B.V. All rights reserved. * Corresponding author at: Institute of Genetics, School of Biology, Queens Medical Centre, University of Nottingham, Nottingham, NG7 2UH, UK. Tel.: +44 115 823 0309. E-mail address: [email protected] (D. Carpenter). Contents lists available at ScienceDirect Infection, Genetics and Evolution journal homepage: www.elsevier.com/locate/meegid 1567-1348/$ – see front matter ß 2008 Elsevier B.V. All rights reserved. doi:10.1016/j.meegid.2008.10.008
-
Upload
danielle-carpenter -
Category
Documents
-
view
213 -
download
1
Transcript of Genetics of susceptibility to malaria related phenotypes

Short communication
Genetics of susceptibility to malaria related phenotypes
Danielle Carpenter a,*, Ingegerd Rooth b, Anna Farnert c, Hind Abushama a,Rupert J. Quinnell a, Marie-Anne Shaw a
a Institute of Integrative and Comparative Biology, Faculty of Biological Sciences, University of Leeds, Leeds LS2 9JT, UKb Nyamisati Malaria Research, Rufiji, National Institute for Medical Research, Dar-es-Salaam, Tanzaniac Unit of Infectious Diseases, Department of Medicine, Karolinska Institute, Karolinska University Hospital Solna, S-17176 Stockholm, Sweden
Infection, Genetics and Evolution 9 (2009) 97–103
A R T I C L E I N F O
Article history:
Received 10 April 2008
Received in revised form 18 July 2008
Accepted 16 October 2008
Available online 31 October 2008
Keywords:
Plasmodium falciparum
Parasite density
Clinical episodes
TDT
Association
TNF
A B S T R A C T
Previous studies have established a genetic component for susceptibility to malaria. Here we use a
pedigree based approach, and transmission disequilibrium testing (TDT), to identify immune response
genes that influence susceptibility to Plasmodium falciparum malarial phenotypes (parasite density and
frequency of clinical episodes) in a Tanzanian population. Evidence for association was observed between
markers in the TNF gene cluster and both the malarial phenotypes. There was weaker evidence for
associations between HLA-DRB1*04, HLA-DRB1*10, and loci in the TCRBV region with parasite density.
There was no evidence for association with polymorphisms in the IL10 promoter, IL1 gene cluster, or from
the IL4/IL13 region.
� 2008 Elsevier B.V. All rights reserved.
Contents lists available at ScienceDirect
Infection, Genetics and Evolution
journa l homepage: www.e lsev ier .com/ locate /meegid
1. Introduction
Plasmodium falciparum malaria is a major cause of mortality andmorbidity, particularly in sub-Saharan Africa. Individuals living inendemic areas may be subjected to constant sub-clinical malariainfection, but only a minority develop severe disease. Variations indisease pattern are attributable to a number of different factors,both environmental and genetic, that can determine whether anexposed individual develops parasitaemia (parasites in the blood),and the risk of a parasitaemic individual developing clinicaldisease.
Over the course of the last decade a number of studies haveevaluated genetics of quantitative malaria phenotypes, such asparasite density and the frequency of malaria episodes. Complexsegregation analyses have established a genetic component ofsusceptibility to P. falciparum blood infection level (Garcia et al.,1998a; Rihet et al., 1998; Abel et al., 1993) and to clinicalinfection of malaria in a mixed P. falciparum and Plasmodium
* Corresponding author at: Institute of Genetics, School of Biology, Queens
Medical Centre, University of Nottingham, Nottingham, NG7 2UH, UK.
Tel.: +44 115 823 0309.
E-mail address: [email protected] (D. Carpenter).
1567-1348/$ – see front matter � 2008 Elsevier B.V. All rights reserved.
doi:10.1016/j.meegid.2008.10.008
vivax population (Mackinnon et al., 2000). There are a number ofstudies which have aimed to identify loci involved with controlof blood infection level and asymptomatic malaria. Linkagestudies provided evidence for linkage between blood infectionlevels and the 5q31–q33 region in populations from BurkinaFaso (Flori et al., 2003a) and Cameroon (Garcia et al., 1998b).Two-point and multipoint analyses provided evidence of linkagebetween mild malaria and the MHC region (Jepson et al., 1997;Flori et al., 2003b), and TDT analysis identified associations witha number of different TNF polymorphisms with both mildmalaria and parasite density (Flori et al., 2005). More recently agenome-wide linkage analysis of malaria infection and milddisease showed evidence for linkage to chromosome 10p15(Timmann et al., 2007).
In the current study, we have investigated polymorphismswithin a number of candidate genes that may play a role insusceptibility to parasite density and clinical infection, in a well-studied Tanzanian population. We build on previous studies byusing family-based association methods to investigate bloodinfection levels and clinical infection data collected over a periodof 7 years. Candidate gene regions (MHC class II and III, IL1, IL10,IL4, IL13, and TCRBV) were chosen from their identification in priorcase control studies and/or their potential role in the control ofmalaria infection.

D. Carpenter et al. / Infection, Genetics and Evolution 9 (2009) 97–10398
2. Materials and methods
2.1. Study population
The study population is from the coastal village of Nyamisati inthe Rufiji delta, Tanzania and has previously been described(Carpenter et al., 2007; Bereczky et al., 2007). The area isholoendemic for malaria, with transmission increasing duringthe two rainy seasons (April to June and November to December)(Rooth, 1992). The predominant malaria species is P. falciparum,which causes 99.5% of all recorded clinical episodes of malaria.There were no malaria control measures in the village and only alimited use of bed-nets (about 3%) during the study period. Thevillage totalled 451 individuals, when recorded in 1989, but hadincreased by 1999, predominantly due to immigration, with 1662people recorded between 1993 and 1999. HbS is the only structuralhaemoglobin variant studied in the Nyamisati population, withheterozygotes (AS) observed at a frequency of 15% in a previousstudy (Rooth, 1992).
2.2. Phenotypes
Epidemiological phenotypes were generated from: (i) nonselected ‘total’ population surveys carried out annually from 1993to 1999 in March to April, and (ii) the complete annual record ofclinical malaria episodes documented in Nyamisati between 1993and 1999 by Rooth, living in the village since 1985 (Bereczky et al.,2007).
2.2.1. Parasite density
The total population surveys provided longitudinal informationon ‘asymptomatic’ parasite densities (parasites per ml) measuredby conventional light microscopy, using Giemsa stained bloodsmears. The total numbers of individuals that were present withinNyamisati in March and April varied year by year and details of thenumbers of individuals present for the population survey andparasite density ranges are presented in Table 1. In 1996 and 1998,surveys were carried out but microscopy was not performed due totechnical problems; in 1997 only a partial survey was carried out.The majority of the 1289 individuals recorded in the populationsurveys do not have data from all years, but individuals have anaverage of 2.3 entries (range 1–5). Furthermore, a small proportion(1%) of these individuals also presented with clinical episodes atthe time of survey, when cross referenced with the clinical episoderecords for March to May. These samples were included in theanalysis as presented here, and did not impact on the overallfindings.
In order to retain as much information as possible, a strategywas used to generate a single quantitative parasite densityphenotype for genetic analysis that included data from all yearsan individual was sampled, and incorporated age and sex effects.This strategy was similar to that used by Rihet et al. (1998) andinvolved correcting each year’s log (1 + x) transformed parasitedensity data for age and sex. This was done using a general linear
Table 1Percentage of individuals positive for malaria parasites, and geometric mean
parasite density (parasites per ml) in Nyamisati by year (n = number of individuals
sampled; 95% confidence interval (CI) calculated on log-transformed data).
Year n Percentage positive Geometric mean (95% CI)
1993 524 46.6% 11.4 (8.4–15.2)
1994 775 38.5% 8.3 (6.4–10.6)
1995 712 35.8% 7.5 (5.7–9.7)
1997 126 57.1% 8.9 (5.4–14.3)
1999 848 25.9% 6.8 (5.1–9.0)
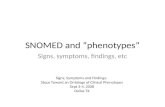
model, with age, age2 and sex as covariates. An arithmetic meanvalue was calculated for each individual from the standardizedresiduals of the age and sex corrected data over all the yearssurveyed, to generate one phenotype for use in the analysis. Fig. 1Ashows the distribution of parasite densities before and aftertransformation.
2.2.2. Clinical episodes
Cases of clinical malaria were continually recorded in Nyamisatipassively between 1993 and 1999, when the inhabitants reportedto the clinic in the event of a fever (>37.5 8C). Diagnosis of malariawas confirmed, via microscopy, by the presence of >5000 P.
falciparum parasites/ml blood. All individuals with fever andconfirmed malaria were treated with sulphadoxine-pyrimetha-mine (SP), according to national guidelines at the time. Due to theprophylactic effect of SP, multiple clinical episodes were con-sidered as recrudescences unless greater than 4 weeks apart. Therewere no recorded cases of cerebral malaria, and a low incidence ofsevere anaemia in this area (Rooth, 1992). The total number ofclinical episodes per calendar year was calculated from theserecords for each individual. A value of no clinical episodes wasgiven when an individual was not entered in the clinical records,but had been identified as present in Nyamisati, through the totalpopulation surveys. The total numbers of clinical episodes per yearare presented in Table 2. A total of 1611 individuals had data forclinical episodes, with a mean of 6.6 years data (range 1–7).
As for parasite density data, age and sex correction was carriedout prior to analysis on the log (1 + x) transformed clinical episodesdata for each year, using a general linear model with age, age2 andsex as covariates, and an arithmetic mean value was calculated foreach individual from the standardized residuals of the age and sexcorrected data over all the years. Fig. 1B shows the distribution ofclinical episodes before and after transformation.
2.3. Genotyping
To enable family based analysis, pedigrees were generated fromlocal knowledge of households by Dr Ingegerd Rooth, who workedand lived in the village as a practising clinician during, and manyyears prior, to the present study. Pedigrees were checked usinggenotype data and PEDCHECK (O’Connell and Weeks, 1998). Thereare a total of 167 extended pedigrees comprising two or moregenerations, and containing a total of 303 nuclear families and1469 individuals. There are three main pedigrees that comprise themajority of the Nyamisati population. Each extends over 140individuals and spans four generations. Blood collection took placemainly in 1999. DNA was extracted from a total of 1050 samples, ofwhich 860 samples are from related individuals and 190 fromunrelated individuals. All samples have a clinical episodesphenotype. The total number of DNA samples available for whichthere is a parasite density phenotype is 977.
DNA extraction was performed using standard phenol–chloro-form extraction from frozen packed blood cells. SNP genotypingwas performed by PCR-RFLP on all 1050 DNA samples for thefollowing polymorphisms, TNF�308, LTA�368, IL1B�511, IL10�592,IL10�1082, IL13arg130gln, BV8S3, BV24S1, BV2S1, BV15S1 and BV3S1;and the VNTRs [IL1RNVNTR and IL4VNTR] were typed by PCR andagarose gel electrophoresis as previously been described (Carpen-ter et al., 2007). HLA class II loci were typed using sequence specificoligonucleotide probes to detect polymorphisms in HLA-DQB1,HLA-DQA1 and HLA-DRB1 (Erlich, 1989). Genotype frequencies atall SNP and VNTR loci did not differ significantly from thoseexpected under Hardy–Weinberg equilibrium, with the exceptionof BV2S1. The genotyping at this locus was repeated and genotypesconfirmed.

Fig. 1. Frequency distributions for average parasite density truncated at 10,000 (A) and average number of clinical episodes phenotypes (B), (i) before and (ii) after log
transformation and correction for age and sex.
D. Carpenter et al. / Infection, Genetics and Evolution 9 (2009) 97–103 99
Known haplotypes were determined using the family data forTNF�308 and LTA�368, IL1B�511 and IL1RNVNTR, IL10�592 and IL10�1082,and between the 5 TCRBV markers BV8S3, BV24S1, BV2S1, BV15S1
and BV3S1. In contrast to the biallelic markers, a reduced number ofsamples were genotyped for HLA-DQB1, HLA-DQA1 and HLA-DRB1;239, 442 and 472, respectively, and, as such, data were too few foranalysis of the HLA class II markers as haplotypes.
2.4. Statistical analysis
Heritabilities of the parasite density and clinical episodephenotypes were calculated by variance components analysis asimplemented in SOLAR (Blangero and Almasy, 1997). The numberof relative pairs contributing to each heritability analysis wascalculated using the ‘relpairs’ command in SOLAR. The number ofrelative pairs was 3516 for parasite density and 4800 for clinical
Table 2Percentage of individuals reporting a clinical episode, and geometric mean number
of clinical episodes of malaria per person in Nyamisati by year (n = number of
individuals present in the village; 95% confidence interval (CI) calculated on log-
transformed data).
Year n Percent with
episode
Range
(all individuals)
Geometric mean
(95% CI)
1993 1388 6.6% 0–5 0.05 (0.04–0.06)
1994 1447 11.7% 0–5 0.10 (0.09–0.12)
1995 1493 15.9% 0–6 0.16 (0.14–0.18)
1996 1549 15.8% 0–8 0.16 (0.14–0.19)
1997 1574 18.5% 0–9 0.21 (0.19–0.24)
1998 1602 14.4% 0–8 0.17 (0.14–0.19)
1999 1611 12.5% 0–4 0.10 (0.09–0.11)
episodes. For the parasitaemia this included 1175 parent–offspringcomparisons, 1411 sibling, or half sibling, 303 grand-parent,grand-child, 468 avuncular or half avuncular and 68 first cousincomparisons. For the clinical episodes this included 1485 parent–offspring comparisons, 1915 sibling or half sibling, 456 grand-parent, grand-child, 656 avuncular or half avuncular and 119 firstcousin comparisons. Associations between the phenotypes andalleles or haplotypes at candidate loci were tested by a quantitativetransmission disequilibrium test (TDT) using the program QTDTversion 2.1.3 (Abecasis et al., 2000). To retain as much informationas possible all the individuals within the sample set were includedin a test for the total evidence of association. To control for anypopulation stratification, we then tested only the within-familyassociation in an orthogonal model including environmental,polygenic heritability and additive major locus variance compo-nents. For the HLA loci, to generate a single global p value per locus,a multi-allelic test was performed for both the total and within-family models. We also tested for evidence of populationstratification for each marker. To control for any non-normality,p values were confirmed by calculating empirical p values bypermutation. Uncorrected p values are presented. Linkagedisequilibrium between adjacent loci was calculated using theprogram EH (Xie and Ott, 1993) on unrelated individualsgenotyped for all loci in the haplotype.
3. Results
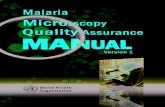
There was a significant decline in both parasite density andnumber of clinical episodes with age, as is typical for malaria(Fig. 2). Parasite density showed a gradual decline across all ages,while number of episodes declined more steeply in children and

Fig. 2. Variation in geometric mean parasite density (A) and number of clinical episodes per year (B) with age in Nyamisati during 1993–1997. For clinical episodes, age groups
with a mean of zero were plotted as a mean of 0.01 episodes per year. Key: 1993 (^), 1994 (&), 1995 (~), 1996 (~), 1997 (&), 1998 (^) and 1999 (�).
D. Carpenter et al. / Infection, Genetics and Evolution 9 (2009) 97–103100
did not vary with age in adults. For both phenotypes, there was asignificant quadratic relationship with age in all years, withnegative coefficients for age (p < 0.001) and positive coefficientsfor age2 (p � 0.001), except for the partial parasite density surveyin 1997. In contrast, there were no significant sex differences inparasite density, and a significant sex difference in number ofepisodes in only one of 7 years. Parasite densities were similaracross all years (Table 1 and Fig. 2). Clinical episodes were morevariable between years, with notably less disease in 1993.
The heritability (SE) of the parasite density phenotype was0.104 (0.052) (p = 0.011) and heritability of the clinical episodephenotype was 0.221 (0.046) (p < 0.001). Table 3 presents asummary of the quantitative transmission disequilibrium testingwhich shows limited evidence for association between phenotypesand the candidate markers, the most significant observation beingfor the MHC class III region. There was evidence for an associationwith LTA+368 and parasite density using the within-family test, witha positive association being observed with LTA+368*A (p = 0.007).There was also evidence using this model for association betweenTNF�308 and mean number of clinical episodes, with TNF�308*Abeing positively associated (p = 0.007). There were no significantobservations for these loci when modelling total evidence for
Table 3Tests for association between polymorphisms or known haplotypes and the quantitative
values for total and within-family tests of association using QTDT. Significant p values
Marker Parasite density
Total association Within-family
DQB1 n/s n/s
DQA1 n/s n/s
DRB1 0.016 n/s
TNF�308 n/s 0.066
LTA�368 n/s 0.007TNF�308–LTA+368 n/s n/s
IL1B�511 n/s n/s
IL1RNVNTR n/s n/s
IL1B�511–IL1RNVNTR n/s n/s
IL10�592 n/s n/s
IL10�1082 n/s n/s
IL10�1082–IL10�592 n/s n/s
IL13arg130gln n/s n/s
IL4VNTR n/s n/s
BV8S3 n/s n/s
BV24S1 n/s n/s
BV2S1 0.043 0.022BV15S1 n/s 0.011BV3S1 n/s n/s
TCR haplotypeBV8-24-2-15-3 0.0653 0.0043
association. When testing for population stratification there weresignificant observations for both loci [TNF�308 (p = 0.0196) andLTA+368 (p = 0.0079)] with parasite density but not with clinicalepisodes, suggesting that the appropriate test for these markers isthe within-family test. There was evidence for strong linkagedisequilibrium between TNF�308 and LTA+368 (D0 = 0.68, p = 0.001),with a greater than expected number of the two locus haplotypesTNF�308*G-LTA+368*G and TNF�308*A-LTA+368*A. Haplotype analysisgenerated no significant associations with either phenotype.
The total association test provided evidence for an associationbetween parasite density and alleles at the DRB1 locus (p = 0.016),but this was not supported when including family structure. Therewas no evidence for stratification with any of the MHC class IImarkers. More specifically, significant negative associations wereobserved for DRB1*04 (p = 0.022) and DRB1*10 (p = 0.003) withparasite density.
There was evidence for a positive association with BV2S1*A(p = 0.022) and BV15S1*G (p = 0.011) with parasite density usingthe within-family test. There was also weaker evidence from thetotal association test for BV2S1*A (p = 0.043) and parasite levels.There was no significant evidence of population stratification forBV2S1, however, there was evidence for stratification of BV15S1
phenotypes parasite density and number of clinical episodes. Values presented are p
are in bold.
Clinical episodes
association Total association Within-family association
n/s 0.056
n/s n/s
n/s n/s
n/s 0.007n/s n/s
n/s n/s
n/s n/s
n/s 0.077
n/s n/s
n/s 0.083
n/s n/s
n/s n/s
n/s n/s
n/s n/s
n/s n/s
n/s 0.097
n/s n/s
0.085 n/s
n/s n/s
n/s n/s

Table 4Within-family association tests between TCRBV haplotypes and parasite density.
Haplotype Na p value
BV8S3*C–BV24S1*G–BV2S1*T–BV15S1*G–BV3S1*C 144 n/s
BV8S3*C–BV24S1*A–BV2S1*T–BV15S1*G–BV3S1*C 135 n/s
BV8S3*C–BV24S1*A–BV2S1*T–BV15S1*G–BV3S1*T 34 0.014
BV8S3*C–BV24S1*A–BV2S1*T–BV15S1*A–BV3S1*C 33 0.004
a N = number of transmissions, defined as the number of instances where
transmission of the particular haplotype occurs and contributes to the significance
of the test.
D. Carpenter et al. / Infection, Genetics and Evolution 9 (2009) 97–103 101
with parasite density (p = 0.004). There was evidence for stronglinkage disequilibrium between the 5 TCR markers BV8S3–BV24S1–BV2S1–BV15S1–BV3S1, with a greater than expected number of thehaplotype BV8S3*C–BV24S1*G–BV2S1*T–BV15S1*G–BV3S1*C(p < 0.0001), present at a frequency of 41%. There were significantassociations between TCRBV haplotypes and parasite density(multi-allelic test, p = 0.004), with a significant negative associa-tion for the haplotypes BV8S3*C–BV24S1*A–BV2S1*T–BV15S1*A–BV3S1*C (p = 0.004) and BV8S3*C–BV24S1*A–BV2S1*T–BV15S1*G–BV3S1*T (p = 0.014) (Table 4). No significant associations weredetected between TCRBV haplotypes and clinical episodes.
There were no significant associations with either phenotypefor any of the polymorphisms within the IL1 gene cluster, the IL10
promoter and the IL4/IL13 region.
4. Discussion
This study has employed family based methods of association inthe analysis of malaria. Family based methods of analysis are notaffected by population admixture and stratification (Spielmanet al., 1993), which can confound population based methods. Inthis study we investigated the genetic control of malariasusceptibility using parasite levels and clinical episodes as ourphenotypes, effectively using all available individuals from thepopulation, in an effort to avoid problems associated with selectivebias. The incorporation of data collected over several years isdistinct from most studies of malaria, as previous genetic studieshave concentrated on single time points. It is generally acceptedthat single time point measurements of asymptomatic parasitae-mia do not provide a robust phenotype (Farnert et al., 1997).Infections studied in asymptomatic children from this region areknown to be complex, with daily changes in both parasite densityand genotypic pattern of the parasite. The use of multiple timepoints provides more information than from a single time pointand should provide a more accurate representation of anindividual’s overall susceptibility to infection, particularly forclinical episode, where complete data over 7 years were availablefor many individuals.
The heritability of the parasite density phenotype was 0.104,and for the clinical episodes was 0.221. We were unable to accountfor effects of shared exposure (household effects), which ifincluded may lower the estimate of heritability, as relatedindividuals often share households. In a previous study, theincidence of malaria episodes was shown to be lower in HbASchildren in comparison to HbAA, but mean parasite density was thesame (Rooth, 1992). Thus, the higher heritability of clinicalepisodes may reflect the involvement of haemoglobin polymorph-isms. A practical value of heritability for genetic analysis might beconsidered to be 0.2. Whilst the value for the clinical episodes isgreater than this, the low heritability of parasite density suggeststhat the sample size required to detect genes that contribute toparasite levels will be higher than for clinical episodes. Herit-abilities are not always reported in the literature with geneticanalysis studies, however, heritability of 0.08–0.21 for clinical
episodes were reported in a Sri Lankan study (Mackinnon et al.,2000), which is consistent with our observations. Heritability ofparasite density was reported as 0.16–0.24 in the Sri Lankan study(Mackinnon et al., 2000), which is greater than the value for theTanzanian population. A heritability of 0.24 was reported for mildmalaria in a Kenyan population (Mackinnon et al., 2005).
We found evidence for associations between malaria pheno-types and loci in the MHC class III region, specifically betweenLTA+368*A and parasite density and between TNF–308*A and thenumber of clinical episodes. The evidence for these associations isrelatively weak, and would not survive correction for multipletesting. This in part is, due to a lack of power, particularly with thelow heterozygosity for TNF�308. However, these findings docorroborate findings by Flori et al. (2005) also investigatingparasite density in a population in Burkina Faso, and a study inKenya by Aidoo et al. (2001) which reported an associationbetween TNF�308*A and an increase in infant mortality andmorbidity. Carriage of TNF�308*A has also been associated withsymptomatic reinfections with P. falciparum in Gabon (Meyer et al.,2002). Case control studies have previously shown a significantassociation between TNF�308*A and cerebral malaria in a Gambianpopulation (McGuire et al., 1994), and between TNF�308*A andsevere malaria in a Sri Lankan population (Wattavidanage et al.,1999). More recently other TNF promoter polymorphisms havebeen investigated and have highlighted the diverse and complexnature of this region (Knight and Kwiatkowski, 1999; Ubalee et al.,2001; Gourley et al., 2002).
Acute concentrations of TNF-a have been related to malariapathology (Ferrante et al., 1990; Kwiatkowski et al., 1990). Whilstsome early functional studies of the TNF�308 polymorphismsuggested that it may alter TNF transcription, with TNF�308*Aleading to a seven fold increase in TNF-a production (Wilson et al.,1997; Louis et al., 1998), others report no effect of the TNF�308
polymorphism on TNF-a production (Brinkman et al., 1996;Huizinga et al., 1997; Mycko et al., 1998). However, multiplepolymorphisms and the presence of strong linkage disequilibriumacross this region result in complex TNF promoter regionhaplotypes, which, when combined with the effects of differentgenetic backgrounds, will have an impact. Thus, the functionalrelevance of such SNPs is hard to examine.
The observed genetic associations may be the result of thecomplex pattern of linkage disequilibrium across the MHC class IIIregion. Significant linkage disequilibrium has been shown betweenLTA+368 and TNF�308 in this study and there is well reported linkagedisequilibrium between these genes, and across a number ofdifferent polymorphic sites (Ubalee et al., 2001; Flori et al., 2005).Hence, the associations that are described here with TNF�308*A andLTA+368*A could be influenced by the linkage disequilibriumbetween these alleles, and/or between an allele at an adjacentclass III locus.
There was weak evidence of a negative association with allelesDRB1*04 and DRB1*10 and asymptomatic parasite levels. Anassociation has previously been reported between the distributionof MHC class II haplotypes and clinical episodes in the Gambia(Bennett et al., 1993) and weak associations were observedbetween MHC class II alleles and P. falciparum specific IgEresponses in our Tanzanian population (Carpenter et al., 2007).Significant associations with different alleles at the DRB1 locushave been detected previously when severe malaria phenotypeshave been examined. Interestingly, a case control study in Gabonidentified an association between DRB1*04 and susceptibility tosevere malaria (May et al., 1999).
Whilst the MHC has received considerable attention in relationto malaria phenotypes, T cell receptor genes have not been a focusof interest (Kwiatkowski, 2005). The data presented here provide

D. Carpenter et al. / Infection, Genetics and Evolution 9 (2009) 97–103102
evidence for a positive association between parasite density andBV2S1*A and BV15S1*G, and also with the 5 locus TCRBV haplotype.These polymorphisms result in non-synonymous changes (Corne-lis et al., 1992; Wei et al., 1995), and therefore may cause afunctional alteration to the T cell repertoire. Both these poly-morphisms alter amino acids which are involved with the interfacebetween the variable regions of the TCRa and TCRb chains, andcould lead to a conformational change in the TCR, or affect theaffinity of binding to the MHC molecule.
The TCRBV region exhibits strong linkage disequilibrium asreported here and elsewhere (Subrahmanyan et al., 2001), and aparticular TCRBV haplotype has been reported at high frequencieswithin Africa [BV8S3*C–BV2S1*T–BV15S1*G–BV3S1*C] (Craddocket al., 2000). Interestingly, a study focusing on the variation infrequency of this common TCRBV haplotype in Africa supported anobservation of a North–South gradient (Donaldson et al., 2002b),where this haplotype was observed to decrease in frequencywithin Africa with distance from the North Pole. Previous studieshave speculated that the occurrence of the common African TCRBV
haplotype is due to selection by malaria, and that this haplotypemay convey protection (Donaldson et al., 2002b). However, a studyto investigate this TCRBV region in relation to severe malaria(defined as cerebral malaria, severe malarial anaemia or hypogly-caemia) in Gambians could not identify significant differences inthe TCRBV haplotype frequencies between cases and controls(Donaldson et al., 2002a). The phenotypes that are presented in thepresent study were not tested by Donaldson et al. (2002a). Wefound evidence for a negative association between parasite densityand two different TCRBV haplotypes [BV8S3*C–BV24S1*A–BV2S1*T–BV15S1*A–BV3S1*C] and [BV8S3*C–BV24S1*A–BV2S1*T–BV15S1*G–BV3S1*T] in Tanzanians, suggesting that these haplo-types themselves could be associated with resistance to malaria.Alternatively, the haplotypic associations observed could simplybe a consequence of the positive association seen with BV2S1*A inthe analysis of single loci. There was no evidence for association ofthe common TCRBV haplotype [BV8S3*C–BV2S1*T–BV15S1*G–BV3S1*C] with protection from or susceptibility to malaria.
In conclusion we have found evidence for the involvement of theMHC class III region in the genetic control of P. falciparum parasitedensity and the frequency of clinical episodes. A full understandingof complex susceptibility haplotypes spanning the TNF promoterregion will require a larger dataset to be established. Further studiesto haplotype the promoter region would certainly be of interest, notonly to identify susceptibility haplotypes, but also to better pinpointfunctionally contributing sites. We have also found evidence that theTCRBV region may play a role in malaria susceptibility. The stronglinkage disequilibrium across this region makes it difficult toidentify the specific site(s) responsible for the association, but anatural progression of this study would be to examine the peripheralTCR repertoire of the individuals in this population, in relation to theloci that have been genotyped.
Acknowledgements
The authors would like to thank Prof. Anders Bjorkman and Prof.Marita Troye-Blomberg for helpful discussion.
References
Abecasis, G.R., Cardon, L.R., Cookson, W.O.C., 2000. A general test of association forquantitative traits in nuclear families. Am. J. Hum. Genet. 66, 279–292.
Abel, L., Cot, M., Mulder, L., Carnevale, P., Feingold, J., 1993. Segregation analysisdetects a major gene controlling blood infection levels in human malaria. Am. J.Hum. Genet. 50, 1308–1317.
Aidoo, M., McElroy, P.D., Kolczak, M.S., Terlouw, D.J., ter Kuile, F.O., Nahlen, B., Lal,A.A., Udhayakumar, V., 2001. Tumour necrosis factor-alpha promoter variant 2
(TNF2) is associated with pre-term delivery, infant mortality, and malariamorbidity in Western Kenya. Genet. Epidemiol. 21, 201–211.
Bennett, S., Allen, S.J., Olerup, O., Jackson, D.J., Wheeler, J.G., Rowe, P.A., Riley, E.M.,Greenwood, B.M., 1993. Human leukocyte antigen (HLA) and malaria morbidityin a Gambian community. Trans. R. Soc. Trop. Med. Hyg. 87, 286–287.
Bereczky, S., Liljander, A., Rooth, I., Faraja, L., Granath, F., Montgomery, S.M., Farnett,A., 2007. Multiclonal asymptomatic Plasmodium falciparum infections predict areduced risk of malaria disease in a Tanzanian population. Microb. Infect. 9,103–110.
Blangero, J., Almasy, L., 1997. Multipoint oligogenic linkage analysis of quantitativetraits. Genet. Epidemiol. 14, 959–964.
Brinkman, B.M.N., Zuijdgeest, D., Kaijzel, E.L., Breedveld, F.C., Verweij, C.L., 1996.Relevance of the tumour necrosis factor alpha (TNF alpha)—308 promoterpolymorphism in the TNF alpha gene regulation. J. Inflamm. 46, 32–41.
Carpenter, D., Abushama, H., Bereczky, S., Farnert, A., Rooth, I., Troye-Blomberg, M.,Quinnell, R.J., Shaw, M.-A., 2007. Immunogenetic control of antibody respon-siveness in a malaria endemic area. Hum. Immunol. 68, 165–169.
Cornelis, F., Hashimoto, L., Loveridge, J., MacCarthy, A., Buckle, V., Julier, C., Bell, J.,1992. Identification of a CA repeat at the TCRA locus using yeast artificialchromosomes: a general method for generating highly polymorphic markers atchosen loci. Genomics 13, 820–825.
Craddock, T.P., Zumla, A.M., Ollier, W.E.R., Chintu, C.Z., Muyinda, G.P., Lancaster, F.C.,Boylston, A.W., 2000. Predominance of one T-cell antigen receptor BV haplotypein African populations. Immunogenetics 51, 231–237.
Donaldson, I., Shefta, J., Hill, A.V.S., Boylston, A., 2002a. Malaria is not responsible forthe selection of the TCRb-subunit variable gene haplotypes in The Gambia.Immunogenetics 53, 894–899.
Donaldson, I., Shefta, J., Lawson, C.A., Bushnell, J.A., Morgan, A.W., Isaacs, J.D.,Carpenter, D., Shaw, M.-A., Rooth, I., Quinnell, R.J., Zumla, A.M., Ollier, W.E.R.,Chintu, C.Z., Muyinda, G.P., Hill, A.V.S., Boylston, A.W., 2002b. Unique TCR-bsubunit variable gene haplotypes in Africa. Immunogenetics 53, 884–893.
Erlich, H.A., 1989. HLA class II gene polymorphisms: DNA typing evolution andrelationship to disease susceptibility. In: Erlich, H.A. (Ed.), PCR Technology:Principles and Applications for DNA Amplifications. Stockton Press, New York,pp. 193–208.
Farnert, A., Snounou, G., Rooth, I., Bjorkman, A., 1997. Daily dynamics of Plasmodiumfalciparum sub populations in asymptomatic children in a holoendemic area.Am. J. Trop. Med. Hyg. 56, 538–547.
Ferrante, A., Staugas, R.E.M., Rowan-Kelly, B., Bresatz, S., Kumaratilake, L.M.,Rzepczyk, C.M., Adolf, G.R., 1990. Production of tumour necrosis factors alphaand beta by human mononuclear leukocytes stimulated with mitogens, bac-teria and malaria parasites. Infect. Immun. 58, 3994–4004.
Flori, L., Delahaye, N.F., Iraqi, F.A., Hernandez-Valladares, M., Fumoux, F., Rihet, P.,2005. TNF as a malaria candidate gene: polymorphism-screening and familybased association analysis of mild malaria attack and parasitaemia in BurkinaFaso. Genes Immun. 6, 472–480.
Flori, L., Kumulugui, B., Aucan, C., Esnault, C., Traore, A.S., Fumoux, F., Rihet, P.,2003a. Linkage and association between Plasmodium falciparum blood infectionlevels and chromosome 5q31–33. Genes Immun. 4, 265–268.
Flori, L., Sawadogo, S., Esnault, C., Delahaye, F., Fumoux, F., Rihet, P., 2003b. Linkageof mild malaria to the major histocompatibility complex in families living inBurkina Faso. Hum. Mol. Genet. 12, 375–378.
Garcia, A., Cot, M., Chippaux, J.P., Ranque, S., Feingold, J., Demenais, F., Abel, L.,1998a. Genetic control of blood infection levels in human malaria: evidence fora complex genetic model. Am. J. Trop. Med. Hyg. 58, 480–488.
Garcia, A., Marquet, S., Bucheton, B., Hillaire, D., Cot, M., Fievet, N., Dessain, A.J., Abel,L., 1998b. Linkage analysis of the blood Plasmodium falciparum levels: linkage ofthe 5q31–q33 chromosome region. Am. J. Trop. Med. Hyg. 58, 705–709.
Gourley, I.S., Kurtis, J.D., Kamoun, M., Amon, J.J., Duffy, P.E., 2002. Profound bias ininteferon-g and interleukin-6 allele frequencies in Western Kenya, wheresevere malaria is common in children. J. Infect. Dis. 186, 1007–1012.
Huizinga, T.W.J., Westendorp, R.G.J., Bollen, E.L.E.M., Keijers, V., Brinkman, B.M.N.,Langermans, J.A.M., Breedveld, F.C., Verweij, C.L., van de Gaer, L., Dams, L.,Crusius, J.B., Garcia-Gonzalez, A., van Oosten, B.W., Polman, C.H., Pena, A.S.,1997. TNF-a promoter polymorphisms, production and susceptibility tomultiple sclerosis in different groups of patients. J. Neuroimmunol. 72,149–153.
Jepson, A.P., Sisay-Joof, F., Banya, W., Hassan-King, M., Frodsham, A., Bennett, S., Hill,A.V.S., Whittle, H., 1997. Genetic linkage of mild malaria to the major histo-compatibilty complex in Gambian children: study of affected sibling pairs. Br.Med. J. 315, 96–97.
Knight, J.C., Kwiatkowski, D., 1999. Inherited variability of tumor necrosis factorproduction and susceptibility to infectious disease. Proc. Assoc. Am. Phys. 111,290–298.
Kwiatkowski, D., Hill, A.V.S., Sambou, I., Twumasi, P., Castracane, J., Manogue, K.R.,Cerami, A., Brewster, D.R., Greenwood, B.M., 1990. TNF concentration in fatalcerebral, non-fatal cerebral, and uncomplicated Plasmodium falciparum malaria.Lancet 336, 1201–1204.
Kwiatkowski, D.P., 2005. How malaria has affected the human genome and whathuman genetics can teach us about malaria. Am. J. Hum. Genet. 77, 171–192.
Louis, E., Franchimont, D., Piron, A., Gevaert, Y., Schaaf-Lafontaine, N., Roland, S.,Mahieu, P., Malaise, M., de Groote, D., Louis, R., Belaiche, J., 1998. Tumournecrosis factor (TNF) gene polymorphism influences TNF-a production inlipopolysaccharide (LPS)-stimulated whole blood cell culture in healthyhumans. Clin. Exp. Immunol. 113, 401–406.

D. Carpenter et al. / Infection, Genetics and Evolution 9 (2009) 97–103 103
Mackinnon, M.J., Gunawarden, D.M., Rajakaruna, J., Weeasingha, S., Mendis, K.N.,Carter, R., 2000. Quantifying genetic and non-genetic contributions to malariainfection in a Sri Lankan population. Proc. Natl. Acad. Sci. U. S. A. 97, 12661–12666.
Mackinnon, M.J., Mwangi, T.W., Snow, R.S., Marsh, K., Williams, T.N., 2005. Herit-ability of malaria in Africa. PloS Med. 2, 1253–1259.
May, J., Meyer, C.G., Kun, J.F.J., Lell, B., Luckner, D., Dippmann, A.K., Bienzle, U.,Kremsner, P.G., 1999. HLA class II factors associated with Plasmodium falciparummerozoite surface antigen allele families. J. Infect. Dis. 179, 1045–1942.
McGuire, W., Hill, A.V.S., Allsopp, C.E.M., Greenwood, B.M., Kwiatkowski, D., 1994.Variation in the TNF-alpha promoter region associated with susceptibility tocerebral malaria. Nature 371, 508–511.
Meyer, C.G., May, J., Luty, A.J., Lell, B., Kremsner, P.G., 2002. TNF-alpha-308Aassociated with shorter intervals of Plasmodium falciparum reinfections. TissueAntigens 59, 287–292.
Mycko, M., Kowalski, W., Kwinkowski, M., Buenafe, A.C., Szymanska, B., Tronc-zynska, E., Plucienniczak, A., Selmaj, K., 1998. Multiple sclerosis: the frequencyof allelic forms of tumour necrosis factor and lymphotaxin-alpha. J. Neuroim-munol. 84, 198–206.
O’Connell, J.R., Weeks, D.E., 1998. Pedcheck: a program for identifying genotypingincompatibilities in linkage analysis. Am. J. Hum. Genet. 63, 259–266.
Rihet, P., Traore, Y., Abel, L., Aucan, C., Troare-Leroux, T., Fumoux, F., 1998. Malaria inhumans: Plasmodium falciparum blood infection levels are linked to chromo-some 5q31–q33. Am. J. Hum. Genet. 63, 498–505.
Rooth, I., 1992. Malaria morbidity and control in a Tanzanian village, Doctoralthesis. Karolinska Institutet, Stockholm.
Spielman, R.S., McGinnis, R.E., Ewens, W.J., 1993. Transmission test for linkagedisequilibrium: the insulin gene region and insulin-dependent diabetes melli-tus (IDDM). Am. J. Hum. Genet. 52, 506–516.
Subrahmanyan, L., Eberle, M.A., Clark, A.G., Kruglak, L., Nickerson, D.A., 2001.Sequence variation and linkage disequilibrium in the human T cell receptorb (TCRB) locus. Am. J. Hum. Genet. 69, 381–395.
Timmann, C., Evans, J.A., Konig, I.R., Kleensang, A., Ruschendorf, F., Lenzen, J.,Sievertsen, J., Becker, C., Enuameh, Y., Kwakye, K.O., Opoku, E., Browne,E.N.L., Zieger, A., Nurnberg, P., Horstmann, R.D., 2007. Genome-wide linkageanalysis of malaria infection intensity and mild disease. PLoS Genet. 3, 393–400.
Ubalee, R., Suzuki, F., Kikuchi, M., Tasanor, O., Wattanagoon, Y., Ruangweerayut, R.,Na-Bangchang, K., Karbwang, J., Kimura, A., Itoh, K., Kanda, T., Hirayama, K.,2001. Strong association of a tumour necrosis factor-a promoter allele withcerebral malaria in Myanmar. Tissue Antigens 58, 407–410.
Wattavidanage, J., Carter, R., Perera, K.L.R.L., Munasingha, A., Bandara, S., Mcguiness,D., Wickramasinghe, A.R., Alles, H.K., Mendis, K.N., Premawansa, S., 1999. TNFalpha*2 marks high risk of severe disease during Plasmodium falciparum malariaand other infections in Sri Lankans. Clin. Exp. Immunol. 115, 350–355.
Wei, S., Charmley, P., Birchfield, R., Concannon, I.P., 1995. Human T-cell receptorVb gene polymorphism and multiple sclerosis. Am. J. Hum. Genet. 56, 963–969.
Wilson, A.G., Symons, J.A., McDowell, T.L., McDevitt, H.O., Duff, G.W., 1997. Effects ofa polymorphism in the human tumour necrosis factor a promoter on tran-scriptional activation. Proc. Natl. Acad. Sci. U. S. A. 94, 3195–3199.
Xie, X., Ott, J., 1993. Testing linkage disequilibrium between a disease gene andmarker loci. Am. J. Hum. Genet (53, Suppl.), 1107 (abstract).