Genetics of Human Cancer...GENETICS OF HUMAN CANCER 235 mutation to one-half of the offspring, but...
23
Ann. Rev. Genet. 1986. 20:231-51 Copyright ©1986by Annual Reviews Inc. All rights reserved GENETICS OF HUMAN CANCER Alfred G. Knudson, Jr. Institute for Cancer Research, Fox Chase Cancer Center, Philadelphia, Pennsylvania 19111 CONTENTS INTRODUCTION ..................................................................................... 231 HEREDITARY CANCER IN MAN ............................................................... 232 Recessive Breakage andRepair Disorders ................................................... 232 Dominantly Heritable Predisposition to Cancer ............................................ 233 ONCOGENES AND ANTIONCOGENES ....................................................... 244 Role in Human Cancer .......................................................................... 244 Role in Development ............................................................................. 246 SUMMARY ............................................................................................ 247 INTRODUCTION A large body of evidence amassed from the study of the mechanisms of action of chemical carcinogens and radiation, and of chromosomal aberrations in cancer cells, supports the hypothesis that many,perhaps all, human cancers are initiated by somatic mutations. Even some cancers that seem to be of viral origin depend upon integration of all or part of a viral genome near a critical host gene and, in a broad sense, may be attributed to somatic mutation. The next step in the study of oncogenesisis to identify the genes in which these oncogenic mutations occur. So far twoclasses of such genes have beenidentified. The first, consisting of the cellular oncogenes, was discovered through the study of oncogenic retroviruses. The genes critical for the transforming properties of the acutely oncogenic retroviruses are homologous to genes present in normal ver- tebrates, and, at least in some cases, in other eukaryotesas well. Oncogenesis can also follow the activation of the normal host oncogenes by the nearby 231 0066-4197/86/1215 -0231 $02.00 www.annualreviews.org/aronline Annual Reviews Annu. Rev. Genet. 1986.20:231-251. Downloaded from arjournals.annualreviews.org by University of Minnesota- Law Library on 10/27/06. For personal use only.
Transcript of Genetics of Human Cancer...GENETICS OF HUMAN CANCER 235 mutation to one-half of the offspring, but...

Ann. Rev. Genet. 1986. 20:231-51Copyright © 1986 by Annual Reviews Inc. All rights reserved
GENETICS OF HUMAN CANCER
Alfred G. Knudson, Jr.
Institute for Cancer Research, Fox Chase Cancer Center, Philadelphia, Pennsylvania19111
CONTENTS
INTRODUCTION ..................................................................................... 231HEREDITARY CANCER IN MAN ............................................................... 232
Recessive Breakage and Repair Disorders ................................................... 232Dominantly Heritable Predisposition to Cancer ............................................ 233
ONCOGENES AND ANTIONCOGENES ....................................................... 244Role in Human Cancer .......................................................................... 244Role in Development ............................................................................. 246
SUMMARY ............................................................................................ 247
INTRODUCTION
A large body of evidence amassed from the study of the mechanisms of actionof chemical carcinogens and radiation, and of chromosomal aberrations incancer cells, supports the hypothesis that many, perhaps all, human cancersare initiated by somatic mutations. Even some cancers that seem to be of viralorigin depend upon integration of all or part of a viral genome near a criticalhost gene and, in a broad sense, may be attributed to somatic mutation. Thenext step in the study of oncogenesis is to identify the genes in which theseoncogenic mutations occur.
So far two classes of such genes have been identified. The first, consistingof the cellular oncogenes, was discovered through the study of oncogenicretroviruses. The genes critical for the transforming properties of the acutelyoncogenic retroviruses are homologous to genes present in normal ver-tebrates, and, at least in some cases, in other eukaryotes as well. Oncogenesiscan also follow the activation of the normal host oncogenes by the nearby
2310066-4197/86/1215 -0231 $02.00
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

232 KNUDSON
insertion of the promoting portion of retroviruses that do not contain their ownoncogenes. These chronic retroviruses appear to have recombined with hostoncogenes at some time in the past to generate the acute retroviruses. Normalalleles of host oncogenes undoubtedly play important roles in normal physiol-ogy and development, and can be mutated or activated by nonviral means toproduce cancer.
A second class of cancer genes has been identified through the study ofhereditary cancer, and these are the subject of this review.
HEREDITARY CANCER IN MAN
Mendelian inheritance of predisposition to cancer is well known in humans.The pattern of inheritance of such predisposition is typically dominant, butthere is an interesting group of recessively inherited disorders that have beeninformative of oncogenic processes. These conditions, which affect rates ofmutation and chromosomal breakage, are briefly discussed.
Recessive Br~eakage and Repair Disorders
Cleaver (12) discovered that cells from patients with xeroderma pigmentosum(XP) are defective for repair of DNA damage induced by ultraviolet radiation;this became the first of these conditions whose mechanism was understood.The mutation is not directly oncogenic; exposure to ultraviolet light, orperhaps some other mutagens, must occur before a tumor cell is produced.The rates of in vitro induced mutations and neoplastic transformation areincreased in XP cells (59, 60). Since more than one kind of cancer is produced(skin cancer, melanoma, and some internal cancers), several different genesmay be the targets of oncogenic damage. XP does not impart susceptibility tomutation at any particular locus; evidently a critical "cancer gene" is onlyfortuitously mutated.
Another condition, ataxia telangiectasia (AT), imparts sensitivity to killingby ionizing radiation and certain radiomimetic chemicals (72). In AT,chromosomes are susceptible to breakage and rearrangement. AT subjects arechiefly predisposed to lymphoid leukemias and lymphomas (primarily T-cellforms), suggesting that lymphoid cells are especially mutable. In clones oflymphocytes and in leukemic cells, rearrangements most often involve fourspecific bands: 7p13, 7q35, 14ql 1, and 14q32 (3). These sites have also beenreported in T-cell lymphoid neoplasms unassociated with AT. The first threesites are loci for the ~/, /3, and a chains of the T-cell receptor (34, 67); thefourth is the locus of the immunoglobulin heavy-chain gene complex. Break-age in AT does not seem limited to these sites, but translocations involvingthem have a selective growth advantage.
Two other disorders in this category are Fanconi’s anemia and Bloom’s
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

GENETICS OF HUMAN CANCER 233
syndrome (BS). Both involve excessive chromosomal breakage andrearrangement (80). Some cells from BS patients show a high rate of sister-chromatid exchange (11) and are transformed in vitro by carcinogens (83).The associated finding of homologous chromosome exchange in BS cellscould lead to genetic recombination at heterozygous loci. It has been sug-gested that BS may predispose to cancer by increasing the rate at which asecond step occurs (25, 40, 71). In this hypothesis somatic mutation producesa cell mutant at some recessive oncogenic locus, and subsequent somaticrecombination produces a homozygous tumor cell from it. This possibility isparticularly interesting because it could explain the occurrence of diverseneoplasms observed in BS patients. The first event in BS may also occur atincreased rate, as a tenfold increase in mutation rate was observed in vitro(94).
In one fascinating case study of Bloom’s syndrome, the authors describe ablack child with anomalous pigmentation of the skin (25). The prevailing skincolor was intermediate, but there were patchy areas in which darker areaswere adjacent to light areas. The anomalous areas were attributed to geneticrecombination during development, as is observed with radiation-inducedtwin spots in fruit flies heterozygous for certain mutations with integumentaryphenotypes.
Although disorders of chromosomal breakage and repair provide newinsights into oncogenic mechanisms, they do not identify genetic loci criticalfor transformation. These disorders may be regarded as diseases that pre-dispose to mutation and/or chromosomal breakage generally, with cancer astheir major outcome. On the other hand, the dominantly heritable pre-dispositions identify a class of such critical loci, or "cancer genes."
Dominantly Heritable Predisposition to Cancer
Every human cancer has been reported in both hereditary and nonhereditaryform. Almost every example of heritable cancer has a dominant pattern ofinheritance. None of these hereditary forms is common, as is expected for agenetic disorder in which some of the heterozygotes die before the end of thereproductive period. Only recurrent germinal mutations maintain such geneticconditions in a population. In the case of retinoblastoma the fraction ofheritable cases that results from germinal mutation is approximately 0.8. Theincidence of heritable cases is 2 × 10-5 births, q (gene frequency) = -5,
and/x (mutation rate) ~ 0.8 × -5, a rate that is probably average in man.The two most common hereditary conditions that predispose strongly to
cancer are neurofibromatosis (NF) and polyposis coli (PC), for which heterozygote frequencies are estimated at 3 × 10-4 and 1.2 × 10-4, respec-tively (17, 75). The great majority of cases of PC are inherited, so the fractionthat results from new mutations is probably 0.2 or less. A heterozygote
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

234 KNUDSON
frequency of 1.2 × 10-4 corresponds to q = 0.6 × 10-4. If 0.2 of cases arenew mutations,/z = 1.2 × 10-5, an average rate for loci in man. For NF thefraction of cases due to new germinal mutations is approximately 0.5, whichleads to an estimate of a high mutation rate of 8 × 10-5. This rate mightsimply be a rare rate of mutation within the normal distribution of mutationrates. On the other hand, it could reflect some unusual mechanism. NF is alsounusual with respect to somatic variation in its expression. Within one familyexpressivity may be extreme, with minimal phenotypic features in one mem-ber and hundreds of neurofibromas and cafr-au-lait spots in another member.Is it possible that some unusual agent, such as a transposable element,operates to produce both the high mutation rate and the great phenotypicvariability?
For uncommon tumors like retinoblastoma (RB), where the total incidenceof hereditary and nonhereditary cases is 5 × 10-5, the hereditary fraction canbe substantial (approximately 0.4 for RB). For common cancers (life expecta-tion greater than 10-2), the fraction can never be high. Thus, the probabilityof colon carcinoma over a lifetime is greater than 10 z, and the "common"hereditary form, polyposis coli, has an incidence not much greater than 10-4.
Although it is difficult to assess the contribution of dominantly heritablepredisposition with a low penetrance, the total contribution to cancer mortal-ity from all dominant conditions is likely no more than a few per cent.However, these dominant conditions assume a disproportional importancebecause (a) they represent a high-risk group that could benefit from identifica-tion and intervention, (b) they may involve oncogenic mechanisms operativein the nonhereditary forms of cancer, and (c) they call attention to a new classof genes.
HETEROZYGOSITY FOR RECESSIVE CANCER GENES Two cancers, RB andWilms’ tumor (WT), that exist in well-known dominantly heritable formshave been used as models for a class of cancer genes recessive in oncogenesis.The principal reasons for their use were that in these diseases most heritablecases can be distinguished from those of the nonhereditary form and that asubgroup of heritable cases with a constitutional chromosomal deletion exists,which makes localization of the gene possible. Many other cancers seemlikely to resemble these models.
Hereditary and nonhereditary forms of cancer RB is a malignant tumor thatoccurs almost exclusively in children under the age of five years. However,its cure rate has been high for much of this century, so many patients havesurvived to adulthood and reproduced. The transmission of susceptibility toRB depends strongly upon the circumstances of the survivor. Of course, theperson with a previous positive family history can be expected to transmit the
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

GENETICS OF HUMAN CANCER 235
mutation to one-half of the offspring, but most hereditary cases are newgerminal mutants with a negative family history. However, those individualsaffected in both eyes transmit the mutation as expected for a hereditary case,whereas only 10-15% of unilaterally affected persons transmit the mutation(39). These latter cases are not examples of a "milder" mutant that onlyoccasionally causes tumor; when a unilaterally affected individual does havean affected child, the latter is most often bilaterally affected. It appears thatRB has both hereditary and nonhereditary forms, the former being 35-40percent of the total.
WT is the other neoplasm involved in the definition of a new class of cancergenes. It too exists in both hereditary and nonhereditary forms (47). Bilateraltumors occur more frequently than expected among cases with a positivefamily history, but there are not enough data on the offspring of survivors ofbilateral tumors to state the reverse, that is, that bilaterality in a sporadic casesignifies a germ-line mutation, as was observed for RB.
Hereditary forms are well known for virtually all cancers, but especially forneuroblastoma (NB), pheochromocytoma (Pheo), medullary carcinoma of thyroid (MCT), brain tumors, sarcomas, leukemias and lymphomas, melano-ma, and carcinomas of skin, breast, colon, endometrium, and kidney (41,49).
Requirement for a second event For the heritable cancers it is not unusual tofind obligate carriers of the mutation who do not themselves develop thecancer. In some cases, these individuals might have developed the cancer hadthey lived longer. In others, however, the tumor appears at an early age, andgene carriers who survive past this age are no longer at risk for that particulartumor. Thus, a person unaffected by RB occasionally has an affected parentand an affected child. Even among affected gene carriers one eye may beunaffected, as noted above. Clearly, the presence of the germinal mutation isnot sufficient to cause a tumor; another event, somatic in nature, seems to benecessary.
Whether such a second event is a chance occurrence with more or lessconstant probability from case to case can be determined. If it is fortuitous,and if the number of tumors is small, the numbers of tumors in a group ofcases should have a Poisson distribution. In some bilateral cases the tumors inat least one eye are small enough to resolve and count by ophthalmoscopicexamination. A tabulation of these numbers for 66 eyes fits to a Poissondistribution, with a mean of 3 tumors (39). It was concluded that heritable arises in two steps, the first a germ-line mutation, the second a somatic event.
The frequency of second events per cell division can be estimated. Thecells derived from retinoblasts include the photoreceptor cells and the neuralcells in the retina. The former are by far the most numerous; an estimated 10s
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

236 KNUDSON
cells in the adult eye derive from retinoblasts. The number of retinoblastspresent when they begin to proliferate has been estimated for the mouse, usingan allophenic system that combined animals that were normal and those thatcarried a mutation for retinal degeneration (64). Sectors of degeneration wereobserved, the smallest being approximately one-tenth of the whole, and allsectors being whole-number multiples thereof. It was concluded that in themouse 10 cells are committed as retinoblasts per eye. If that number appliedalso to humans, then 107 cell divisions of retinoblasts would occur duringdevelopment. The frequency of the second event would be about 10-7 per celldivision, a rate compatible with somatic mutation.
Pathologic examination of RB and WT reveals no difference between theirhereditary and nonhereditary forms. Might then the genetic changes seen inthe hereditary forms also occur in the nonhereditary ones? If so, they wouldnecessarily both be somatic, the only difference being that the first eventwould be germinal in one form, and somatic in the other. This idea was testedusing a comparison of the age of appearance of first tumor in bilateral (allheritable) and sporadic unilateral (nearly all nonheritable) cases (39). The were plotted in semilog fashion: the log of the fraction of cases not yetdiagnosed vs age. The bilateral cases decline in linear fashion, as anticipatedfor a single event, following the equation y = Yo exp (-kt). The unilateralcases, on the other hand, declined in curvilinear fashion, as expected for atwo-event phenomenon.
Similar evidence was also procured for both hereditary and nonhereditaryforms of WT, NB, and Pheo (47, 48), although estimates of rates were notpossible.
Chromosomal locations of the first events The location of the inheritedmutation for ILl3 was found by studying a subgroup of deletion cases. About3% of the cases of retinoblastoma show a constitutional deletion, detectable inleukocytes, in one chromosome 13. The sizes of the deletions and thebreakpoints that define them are variable. However, a comparison of casesrevealed that only one band, 13q14, was common to all of the deletions (27,46). Subsequent detection of small intraband deletions has enabled the criticalsite to be further defined as band 13q14.1 (99).
The fact that deletions of various sizes are present in the chromosomes ofsome heritable cases immediately separates the gene responsible for RB fromthe oncogenes that are involved in some translocations of importance in theleukemias and lymphomas. The current paradigm for the latter is Burkitt’slymphoma, in which the common translocation juxtaposes the myc oncogeneon chromosome 8 to the immunoglobulin heavy-chain gene on chromosome14. This translocation results in activation of the myc oncogene by an enhanc-er on chromosome 14 (16). In these translocations the breakpoints are
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

GENETICS OF HUMAN CANCER 237
virtually the same from case to case, and the result is a positive action of anoncogene. Such an action cannot occur with RB because no consistentopportunity for a cis effect exists. It was therefore necessary to conclude thatit is the loss of a gene (or genes) that is important (42). The question arises of whether heterozygosity is responsible for this loss, with the secondevent being at another genetic site, or whether homozygosity is responsiblefor the loss, the second event being at the homologous site in the otherchromosome of the pair.
Since most heritable cases of RB do not involve a visible deletion, we mustinquire in another way whether the remaining heritable cases affect the samegene in which the deletion occurs or whether they represent mutation atanother locus. The answer depended upon the discovery of a closely linkedgene, that coding for esterase D. The deletion cases had only 50% of theexpected levels of this enzyme, showing that the deletions included both loci(89). Since even very small deletions produced this effect, close linkage wassuspected. For the study of nondeletion cases electrophoretic allelic variantsof the enzyme were used. In those pedigrees in which these variants and theretinoblastoma mutation were cosegregating no recombinants were found,and the lod score exceeded 3, indicating that the heritable forms affect thesame locus, whether by deletion or by submicroscopic change (15, 88).
WT is the second tumor for which constitutional deletions have located apredisposing gene. Miller et al (63) were the first to point out an associationbetween congenital aniridia and WT. They found that familial cases ofaniridia did not have an increased risk of WT, but sporadic cases did.Knudson & Strong (47) proposed that such cases may have resulted fromchromosomal deletion, the deleted segment including linked loci for the twoconditions. The isolated hereditary cases of each disease would be the resultof mutations confined to one locus, so hereditary aniridia without deletionwould impose no predisposition to WT. Furthermore, the deletion cases mightdie before the age of reproduction or would not reproduce even if theysurvived. The latter circumstance seemed likely, since many patients haveother congenital defects, including mental retardation.
The first case analyzed cytogenetically revealed a translocation betweenchromosomes 8 and 11, and the authors concluded that it produced a netdeletion in chromosome 8 (53). When other cases were shown to involvechromosome 1 lp13 (78), this case was reexamined and also found to have deletion at this site rather than on chromosome 8 (26). Cases with a familyhistory of WT are much rarer than those with a family history of RB, andthere has not yet been a test of linkage for homogeneity of heritable WT.
Since there are no pathological differences between the hereditary andnonhereditary forms of RB and WT, might the genetic changes be the same?It was proposed that the only difference in their pathogenesis is that in the
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

238 KNUDSON
nonhereditary forms the first event is somatic rather than germinal (39, 47).The first evidence for this idea was cytogenetic. In some patients with thenonhereditary form of RB, and whose lymphocytes showed normalkaryotypes, the tumor cells contained a deletion that included band 13q14, asobserved constitutionally in some RB individuals (4, 5, 28). It now appearsthat about 30% of tumors reveal such a deletion. One might expect that thefraction of deletions in tumor cells would be greater than the fraction ofdeletions among heritable cases (about 5%) because constitutional deletionsmight often be lethal to the host.
Other evidence on the first event in nonhereditary cases was provided bythe analysis of esterase D expression in the tumors of persons heterozygousfor the electrophoretic variants. Godbout et al (32) found that in someunilateral tumors containing two normal-appearing chromosomes 13, onlyone allele was expressed.
Cytogenetic analysis of WT reveals that in a similar fraction of cases thereis a deletion of chromosome band 1 lp13 in the tumors of patients with normalblood karyotypes (37, 85).
The first events in RB and WT involve the same loci in both the hereditaryand nonhereditary forms. This similarity-may indicate that tumor-specificdeletions found only in tumors might represent first events that have not beenfound in constitutional form because of their embryonic lethality. Thus, thereports of deletions of lp in neuroblastoma (7, 30) and 3p in small-cellcarcinoma of the lung (96) may be clues to genetic loci that play correspond-ing roles in these tumors.
There are no other situations of multiple cases of constitutional chromo-somal aberrations localizing this class of genes, but there are isolated ex-amples of interest. In one large pedigree (13), renal carcinoma was found association with a reciprocal translocation between chromosomes 3 and 8.However, the authors emphasize that the translocation was not a sufficientcondition for oncogenesis, as it may be for the somatic translocationsobserved in the leukemias and lymphomas. Of great interest is the observationthat 3p deletions can occur in the tumors of individuals with normal bloodkaryotypes (97).
One patient with familial osteosarcoma (OS) had a complex rearrangementinvolving chromosomes 13 and 14 (31). Her unaffected mother had Robertsonian translocation between these chromosomes. It was not possibleto pinpoint a band as being involved in OS. As noted below, band 13q14 hasbeen incriminated in OS because of the association of OS with RB.
Nature of the second event Because the second event in RB occurred at arate compatible with a somatic mutation, it was hypothesized to be a genomicevent at one of three locations: (a) at or near (cis) the first, inherited event; (b)
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

GENETICS OF HUMAN CANCER 239
at an unrelated site; or (c) at the corresponding site in the homologouschromosome (46). The first possibility was discarded for reasons notedabove. While the second could not be excluded, the third seemed to be themost interesting because it implies that the responsible mutation was recessivewith respect to oncogenesis. It would then represent the first example in manof a recessive mutation being expressed in heterozygous and normalhomozygous individuals.
Three kinds of gene loss were considered (42): submicroscopic mutation(including small deletions), microscopic mutation, and chromosomal loss.Homozygous loss of the normal allele could occur through any of the sixcombinations of these three abnormalities; de novo second events could resultfrom mutation, deletion, or nondisjunction. It was also proposed that somaticrecombination could account for the second event (42). This possibility wasfound attractive because of the observations on patients with Bloom’s syn-drome (BS), noted earlier (25, 40, 71). This mechanism could convert heterozygous cell into a homozygous cell by somatic recombination. There-fore, a cell that had become heterozygous for a recessive cancer gene bysomatic mutation could be expected to become homozygous at a rate muchhigher than normal. Perhaps BS revealed a mechanism that could occur atlower frequency in normal individuals. If true, the second event could resultfrom either a de novo second event or somatic recombination.
The first evidence bearing on the identification of this mechanism camefrom a study by Godbout et al (32). As noted above, these investigatorsexamined tumors for loss of heterozygosity at the esterase D locus in unilater-al cases. They also examined some bilateral cases, finding that some of themalso lost heterozygosity even though both chromosomes were present, but itcould not be concluded that homozygosity or hemizygosity had occurred atthe rb locus.
The first unequivocal evidence was provided by Benedict et al (6), whostudied lymphocytes that showed no karyotypic evidence for a deletion, butwhose level of esterase D suggested hemizygosity and an occult deletion.Examination of the tumor cells revealed no measurable esterase D and onlyone chromosome 13. The investigators concluded that both copies of thenormal allele at the rb locus had been lost, one by constitutional deletion, theother by somatic chromosomal loss.
Further evidence for the recessive hypothesis came from t~he study of DNAmarkers. Utilizing a series of restriction-fragment-length DNA polymor-phisms (RFLP) mapped to chromosome 13, Cavenee et al (9) compared bloodcells and tumor cells in patients with RB. In about half of the cases they foundthat markers heterozygous in lymphocytes were either homozygous orhemizygous in tumor cells. The change was specific for chromosome 13;heterozygous markers on other chromosomes were still heterozygous in the
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

240 KNUDSON
tumors. Occasionally the loss of heterozygosity is for loci beyond a certainpoint on 13q, with retention of heterozygosity for the marker nearest thecentromere. When this change is found in cells that retain both chromosomes13, it is reasonable to conclude that somatic recombination, with a crossoverbetween the proximal RFLP and the rb locus, has occurred. In other casesheterozygosity has been lost for all of the relevant markers. The developmentof monosomy 13 via nondisjunction can explain a few of these cases. In most,however, the tumor cells contain two chromosomes 13. Three possible mech-anisms have been proposed to account for the cases with two chromosomes 13in tumor cells (9, 20, 42, 43, 66): (a) recombination from a crossover betweenthe centromere and the most proximal RFLP locus; (b) nondisjunction fol-lowed by duplication (presumably another nondisjunction); (c) segregation two copies of the same chromosome 13 from a tetraploid intermediate. Thelast mechanism seems unlikely in view of the data at hand; one would expectto find homozygosity for some other chromosomes as well. Distinctionbetween the first two possibilities could be made if markers, either cytogenet-ic or molecular, were available for the centromere.
It was possible to demonstrate in two cases that the inherited mutation hadbeen retained in the tumor cells (10). An affected parent was heterozygous forone or more chromosome 13 RFLP. The affected parent’s alleles were foundin both the lymphocytes and the tumors, whereas the unaffected parent’salleles were found in the lymphocytes but not in the tumors.
In about half of the cases exami~’ned there is retention of heterozygosity forchromosome 13 RFLP’s in the tumor cells, so it is not possible to infer thenature of a second event. However, the a priori expectation is that in someinstances the second event would be a new local event, i.e. a mutation. Such amutation could be a point mutation, small deletion, or rearrangement, orpossibly another submicroscopic change. A suitable test of the recessivehypothesis in these cases awaits the cloning of the rb locus.
The findings described for the loss of heterozygosity apply to nonheredi-tary, as well as to hereditary, cases (9, 20), RB is clearly a homogeneousentity because the initial events leading to disease involve the loss 6f the twonormal alleles of the rb locus. The only difference between hereditary andnonhereditary forms of RB is that in the hereditary cases the first event is amutation in the germ line.
Similar results have been found for WT. Using DNA polymorphisms forgenes ki~own to be on chromosome arm 1 lp (insulin, ~-globin complex, rasoncogene, and parathyroid hormone), the investigators found thatheterozygosity was lost in about 50% of the cases, suggesting that WTemploys the same mechanisms as with RB (24, 52, 70, 77). In a subsequentreport heterozygosity for parathyroid-hormone DNA was retained in the
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

GENETICS OF HUMAN CANCER 241
tumor, while the insulin and /~-globin loci had become homozygous; thetumor contained two normal-appearing chromosomes 11 (74). These findingsconstitute evidence for a crossover between the parathyroid and wt loci.
Because osteosarcoma (OS) has been associated with RB, it has also beeninvestigated for loss of heterozygosity of markers on 13q. Some of thetumors, found in patients with or without RB, had lost heterozygosity (21,33). The association of Wilms’ tumor with the Beckwith-Wiedemann syn-drome (which also predisposes to hepatoblastoma and rhabdomyosarcoma)stimulated an investigation of these latter two tumors for loss of heterozygos-ity of 1 lp markers.~ This study discovered such a loss in some cases (51).
Similar studies have been performed on bladder cancers, using 1 lp markers(23). In 40% of the cases there was loss of heterozygosity. This importantfinding suggests that the epithelial cancers of adults may behave in a mannersimilar to that of the solid tumors of children.
There are then four regions of the human karyotype that merit investigationfor the purpose of isolating this class of cancer gene: lp, 3p, llp, and 13q.Since more than one tumor may be determined at each site, the search mayreveal clusters of genes for different tumors, or single genes with differenttissue expression.
OTHER POSSIBLE HERITABLE ONCOGENIC MUTATIONS As noted earlier,AT heterozygotes may be predisposed to cancer. This would be an instance ofdominant inheritance of predisposition by a mechanism other thanheterozygosity for an antioncogene. Still, other possibilities are conceivableincluding two that might be expected a priori. The first hypothesis concernsthe inheritance of site-specific chromosomal fragility; the second, the in-heritance of a mutation in an oncogene.
Heritable fragile sites and cancer Ataxia telangiectasia points to the in-heritance of chromosomal breakage and rearrangement as a cause of cancer,A much more common situation involves the inheritance of predisposition tobreakage at a single specific site. Seventeen of these dominantly heritablefragile sites (h-fra) are known (35, 55, 57, 98). Their band locations are 2ql 2q13, 6p23, 7pll, 8q22, 9p21, 9q32, 10q23, 10q25, llq13, 11q23, 12q13,16p12, 16q22, 17p12, 20pll, and Xq27. Ten of these sites are at, or verynear, sites involved in chromosomal aberrations found in leukemias andlymphomas (18, 35, 36, 55-57, 98) (Table 1). Genes relevant in pathogenesis of leukemia or lymphoma occur in seven of the sites. Some ofthese genes are protooncogenes whose activation may be oncogenic; theiractivation may be caused by juxtaposition to genes normally active in theaffected cell type. Other genes seem to belong to this group of activating
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

242 KNUDSON
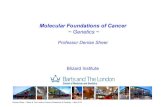
Table 1 Chromosomal sites coincident for fragility and rearrangement or dele-tion in leukemias and lymphomasa
Fragile site Aberration Disease Significant gene
6p23 t(6;9) ANLL7pll t(l;7) ANLL Proto-oncogene c-erb B8q22 t(8;21) ANLL Protooncogene c-raos9p21 t(9;11) ANLL Interferon or/31
10q25 t(10;14) NHLllql3 t(ll;14) NHL Putative protooncogene bcl-111 q23 t(9; 11) ANLL Protooncogene c-ets-112q13 t(12;14) NHL16q22 inv(l 6) ANLL Metallothionein17p12 dic(17p) ANLL Tumor antigen p53
aData compiled from references 18, 35, 36, 55, 56, 57, 98. ANLL = acute nonlymphocyticleukemia; NHL = non-Hodgkin’s lymphoma.
genes. That heritable fragile sites predispose to cancer needs to be shown.There are two reports of the association of h-fra 16q22 with multiple cases ofcancer in families (62, 82).
Inheritance of oncogene mutations If oncogene mutations produce cancerautonomously in one step in all target cells, they cannot be expected toaccount for any examples of dominant inheritance of cancer susceptibility.Such mutations should be lethal to the fetus as the target cells are formed.However, mutant oncogenes may often not have such autonomy. Thus inmany instances of in vitro transformation of normal embryonic fibroblasts,two cooperating oncogenes are necessary (54). This finding leaves open thepossibility that inheritance of an oncogene could be only predisposing andcould require a second, somatic, event for oncogenesis.
A few dominantly heritable conditions have been tested for this possibilityby transfection of DNA into NIH-3T3 cells (69). The disorders includedGardner’s syndrome, a form of polyposis coli, and neurofibromatosis, buttransformation was not observed. A negative finding in this assay does notdisprove the possibility, however.
In the family that cosegregated renal carcinoma and a t(3;8) translocation,investigation of lymphocytes reveals that the c-myc oncogene has been trans-located (19), so this family could represent an example of inherited oncogeneabnormality.
Inherited proto-oncogene abnormality that predisposes to cancer has beendemonstrated experimentally on two occasions. Both experiments dependedupon transfection of fertilized mouse eggs with a c-myc proto-oncogene thathad been fused with a promoting sequence. In one case the sequence was a
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

GENETICS OF HUMAN CANCER 243
regulatory element from the mouse mammary tumor virus, and the tumorsthat resulted were mammary carcinomas (91). In the other case the sequenceswere normal immunoglobulin enhancers, and the tumors were lymphomas(1). Predisposition to lymphoma was transmitted dominantly. Because of latent period for tumor development, of preneoplastic lesions in the lymphoidtissue, and of monoclonality of many tumors, it was concluded that in-heritance of the artificially constructed oncogenes was not sufficient foroncogenesis, but that at least one other event (presumably somatic) wasnecessary.
One condition that could be caused by an oncogene mutation is the Beck-with-Wiedemann Syndrome (BWS), a rare congenital disorder that impartspredisposition to certain tumors, especially WT, but also hepatoblastoma(HB), adrenocortical carcinoma (ACC), and rhabdomyosarcoma (RMS) Patients with this syndrome are distinct from those with heritable WT alone.The latter persons are not stigmatized in other ways, except in the aniridia-deletion syndrome; deletion of other genes accounts for aniridia and the otherdefects that may be observed. On the other hand, patients with BWS ha’:eother anomalies, especially macroglossia, omphalocele, congenital hypogly-cemia, and lesser anomalies. They are also large at birth (average weightgreater than 4 kg). Some patients have hemihypertrophy rather than sym-metrically large size. The disease has often been lethal, and there have beenfew fertile survivors, but there have been a few pedigrees that indicate that thedisease is attributable to a dominant semilethal mutation (50).
The BWS presents a clinical picture so different from that of the otherdominantly heritable conditions that it suggests the involvement of a differentkind of gene. Of interest is the observation of a constitutional cytogeneticabnormality in some patients, an abnormality different from that found in thedeletion cases of WT. A few patients have been discovered in whom there istrisomy for chromosomal band 1 lp15. This trisomy may result either fromduplication in one chromosome 11, or from translocation of the band, prob-ably in an unaffected parent, with inheritance of normal chromosomes 11along with the translocation (93, 95).
Such a finding is incompatible with a recessive mutation, but is compatiblewith an abnormality of an oncogene because those genes are known to showdosage effects. In fact, two possibly relevant genes are located distal to the wtlocus on chromosome 11, in the region of bands 1 lp14 and 1 lp15: the H-rasoncogene and the insulin-like growth factor I! (IGF11) gene. IGFII is activelyexpressed in the tumors observed in the BWS (76, 8l). Conceivably such gene might produce the growth effects observed in BWS. IGFII is of furtherinterest because its expression is greater prenatally than postnatally (2). Thisdecreased expression is consistent with the observation that the growth ofBWS patients becomes steadily more normal with age. Since oncogenesis in
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

244 KNUDSON
the BWS is still a rare event at the cellular level, it probably requires a second,somatic, event. Speculation on the nature of such an event is of limited valuebecause there are too many possibilities. For example, a second event couldlead to amplification of the germ-line mutation, it could be a mutation in adifferent oncogene that complements the germline mutation, or it might bea mutation in an antioncogene that blocks heterozygotes from regulating amutant or trisomic growth gene (44).
ONCOGENES AND ANTIONCOGENES
Role in Human Cancer
A second class of cancer genes, identified through the study of hereditarycancer, can now be added to the class of cancer genes known as oncogenes.These genes have been referred to as recessive cancer genes, recessiveoncogenes, or antioncogenes (the last name resulting from the antioncogeniceffect of the presence of one normal allele). Such recessive genes had beenanticipated from the observations of recessiveness for the cancer phenotype inhuman somatic-cell hybrids (90).
The two classes of cancer genes are different in several ways. The classicaloncogene is active; its product must be present and abnormal either instructure or in amount. The antioncogene is inactive; cancer results when nonormal copy is present. Both normal alleles can be deleted. Mutations inantioncogenes can be transmitted dominantly; mutant oncogenes have notbeen shown to be inherited.
These two classes of oncogenes have cytogenetic differences too. The bestexamples of abnormalities in oncogenes, or in their expression, that causecancers are the hematopoietic malignancies associated with chromosomaltransiocation. In Burkitt’s lymphoma the juxtaposition of immunoglobulingenes on chromosomes 14, 2, or 22 with the c-rnyc oncogene on chromosome8 leads to abnormal expression of the c-myc oncogene (16). Many suchtranslocations are known in this group of malignancies, and they may allinvolve a similar mechanism involving an activating gene and an oncogene.Yet, for the nonhematopoietic tumors whose primary defect is partiallyunderstood, the mechanism involves a deletion or submicroscopic mutation inan antioncogene. What mechanisms do the common cancers use? So far thereare too few results, but the findings on renal and bladder cancer and small-cellcarcinoma of the lung are more consistent with the mechanism involving adeletion or microscopic mutation in an antioncogene. If subsequent data oncommon cancers seem to confirm this mechanism, then the mechanism oftranslocation in hematological malignancies must be reevaluated. Perhapstranslocation is a mechanism more readily available to hematopoietic thannonhematopoietic cells in the initiation of cancer. Thus immunoglobulin and
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

GENETICS OF HUMAN CANCER 245
T-cell receptor gene rearrangements are normal phenomena in B- and T-celllineages, respectively. The enzyme recombinase, involved in the former,inserts telltale nucleotide sequences that are also found in the chromosomaltranslocations, suggesting that the translocations are errors committed by anormal mechanism of blood cells (92).
In some tumors caused by the recessive mechanism there is expression ofan oncogene. Thus in both RB and WT the oncogene N-myc is expressed atelevated levels (58, 100). In both cases the embryonic cell from which thetumor is derived shows elevated expression. IGFII illustrates this phenome-non; it is elevated in Wilms’ tumor, rhabdomyosarcoma, and hepatoblastomaand evidently in the normal counterpart embryonic cells as well (76, 81). Oneexplanation for this increased expression is that it is a feature of the targetcells and has nothing to do with the transformation process. The secondhypothesis is that the normal antioncogene is a regulator of expression of oneor more oncogenes and/or growth factors, and loss of both alleles of theantioncogene causes continued expression of such gene(s), thus leading oncogenesis. This case invokes the model of Comings (14), in which the finalcommon pathway of cancer entails oncogene expression, whether by primarychange in the oncogene or by secondary expression following loss of aregulatory gene.
As is typical of cancer, further genetic changes occur, and clones evolvewith further growth advantages. Oncogene changes can play a role in thesechanges, too (38). For example, in neuroblastoma, tumor N-myc is expressedat elevated levels. However, the gene itself may also be amplified and it is ofgreat importance that this amplification is correlated with more advancedstages of the disease (8). Amplification of the N-myc 0ncogene has also beenobserved in retinoblastoma (58). Amplification of one of the members of thefamily of myc genes is a common feature of small-cell carcinoma of the lung(68).
Other oncogene changes are also frequently observed. Thus, transfectionassays reveal that a mutated ras gene is present in some fraction of manytumors, even including some embryonic tumors (79), where the change almost certainly secondary rather than primary.
Oncogene abnormality therefore seems to be a common, perhaps evenuniversal, feature of cancer. There are several mechanisms for this phenom-enon, including activation by translocated enhance.rs, mutation, andamplification. Whether it can also result from antioncogene loss, or whether itis simply a feature of certain target cells, remains to be demonstrated.
Translocation commonly operates as the primary change in hematopoieticneoplasms. Primary antioncogene change operates in many other cancers.One might even predict that most cancers are caused by the latter mechanismand that the hematological neoplasms are uniquely caused by the oncogene-
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

246 KNUDSON
translocation mechanism. Since translocations are generally a commonfeature of cancers, this mechanism also seems to operate in extant cancercells.
Role in Development
The fact, noted above, that the N-myc oncogene is expressed in certain tissuesthat give rise to embryonal cancers suggests that this oncogene has a de-velopmental role. The N-myc oncogene is particularly expressed in the brainand kidney of the fetal and neonatal mouse (100). The c-myc gene is ex-pressed at low levels in the 3-week human embryo, but at high levels in6-10-week embryos, primarily in the germinal epithelial layers of the skinand gut (73). Differential expression of some oncogenes has also been foundduring development of the mouse (65, 84, 86).
If loss of normal alleles of antioncogenes leads to cancer, one couldimagine that these alleles play a role in growth control in development. Thetissue specificity displayed by many hereditary cancers further suggests thatthe control may be circumscribed in its tissue effects. Some of the hereditarycancers even seem to affect oncogenesis at different points within a de-velopmental system. The best example of this effect concerns tumors ofneural-crest derivatives. Separate hereditary predispositions to each ofmeningioma, neuroblastoma, pheochromocytoma, medullary carcinoma ofthe thyroid, neurofibroma, melanoma, and chemodectoma are known (45).The normal alleles of these loci are good candidates for differentiation genes.
Since antioncogenes are recessive in oncogenesis, it may be that heterozy-gotes for their mutations would not show any developmental abnormalitieseven though the genes may be important for development. On the other hand,homozygotes might be abnormal. Such individuals have not been reportedamong humans. However, there is a heritable form of renal carcinoma in rats(22). Heterozygous rats show no effect of the gene except for oncogenesis,but the homozygous state is lethal to the embryo (22; A. G. Knudson,unpublished data). Unfortunately, the cause of this lethality is unknown.
In Drosophila rnelanogaster, tumors can arise in larvae among cells thatdifferentiate into adult tissues. The best known of these tumors is caused bythe lethal giant larvae gene. Heterozygous flies are normal, but homozygousmutant flies develop neuroblastic tumors in the putative optic centers (29).These tumors are invasive and lethal. The normal alleles are functional duringdevelopment, controlling differentiation and growth of cells in the opticcenters. Differentiation fails to occur in homozygous flies, and tumors devel-op. The gene has now been cloned (61), therefore its physiology and itspossible relationship to human genes can be studied.
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

GENETICS OF HUMAN CANCER 247
SUMMARY
Study of hereditary cancer in humans has revealed new mechanisms incarcinogenesis. In particular, a new class of cancer gene, recessive in
oncogenesis, accounts for dominantly transmitted predisposition to some
cancers, and may play a primary role in the nonhereditary forms of most
cancers. Comparison of polymorphic markers in lymphocytes and tumors has
permitted the in vivo observation of somatic events that lead to geneticrecombination. The tissue specificities of these recessive cancer genes suggest
that their normal alleles, like those of oncogenes, play important roles in
normal development.
ACKNOWLEDGMENTS
Supported in part by an appropriation from the Commonwealth of Pennsyl-vania and by USPHS Grant CA-06927.
Literature Cited
1. Adams, J. M., Harris, A. W., Pinkert,C. A., Corcoran, L. M., Alexander, W.S., et al. 1985. The c-myc oncogenedriven by immunmoglobulin enhancersinduces lymphoid malignancy intransgenic mice. Nature 318:533-38
2. Adams, S. O., Nissley, S. P., Handwer-ger, S., Rechler, M. M. 1983. De-velopmental patterns of insulin-likegrowth factor-I and -11 synthesis andregulation in rat fibroblasts. Nature302:150-53
3. Aurias, A., Dutrillaux, B., Bufiot, D.,Lejeune, J. 1980. High frequencies ofinversions and translocations of chromo-somes 7 and 14 in ataxia telangiectasia.Mutat. Res. 69:369-74
4. Balaban, G., Gilbert, F., Nichols, W,,Meadows, A. T., Shields, J. 1982.Abnormalities of chromosome No. 13 inretinoblasts from individuals with nor-mal constitutional karyotypes. CancerGenet. Cytogenet. 6:213-21
5. Benedict, W. F., Banerjee, A., Mark,C., Murphree, A. L. 1983. Non-randomchromosomal changes in untreated reti-noblastomas. Cancer Genet. Cytogenet.10:311-33
6. Benedict, W. F., Murphree, A. L.,Banerjee, A., Spina, C. A., Sparkes, M.D., Sparkes, R. S. 1983. Patient with 13chromosome deletion: evidence that theretinoblastoma gene is a recessive cancergene. Science 219:973-75
7. Brodeur, G., Green, A. A., Hayes, F.A., Williams, K. J., Williams, D. L.,
Tsiatis, A. A. 1981. Cytogenetic fea-tures of human neuroblastomas and celllines. Cancer Res. 41:4678-86
8. Brodeur, G. M., Seeger, R. C.,Schwab, M., Varmus, H. E., Bishop, J.M. 1984. Amplification of N-myc in un-treated human neuroblastomas correlateswith advanced disease stage. Science224:1121-24
9. Cavenee, W. K., Dryja, T. P., Phillips,R. A,, Benedict, W. F., Godbout, R., etal. 1983. Expression of recessive allelesby chromosomal mechanisms in retino-blastoma. Nature 305:779--84
10~Cavenee, W. K., Hansen, M. F~, Nor-denskjold, M., Kock, E., Maumenee,I., et al. 1985. Genetic origin of muta-tions predisposing to retinoblastoma.Science 228:501-3
11. Chaganti, R. S., Schonberg, S., Ger-man, J. 1974. A manyfold increase insister chromatid exchanges in Bloom’ssyndrome lymphocytes. Proc. Natl.Acad, Sci. USA 71;4508-12
12. Cleaver, J. E. 1968. Defective repairreplication of DNA in xeroderma pig-mentosum. Nature 218:652-56
13. Cohen, A. J., Li, F. P., Berg, S., Mar-chetto, D. J., Tsai, S., et al. 1979.Hereditary renal-cell carcinoma associ-ated with a chromosomal translocation.N. Engl. J. Med. 30l:592-95
14. Comings, D. E. 1973. A general theoryof carcinogenesis. Proc. NatL Acad.Sci. USA 70:3324-32
15. Connolly, M. J., Payne, R. H., John-
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

248 KNUDSON
son, G., Gallic, B. L., Allerdice, P. W.,et al. 1983. Familial, EsD-linked, reti-noblastoma with reduced penetrance andvariable expressivity. Hum. Genet.65:122-2,1
16. Croce, C. M., Nowell, P. :C. 1985.Molecular basis of human B cell neopla-sia. Blood 65:1-7
17. Crowe, F. W., Schull, W. J., Neel, J.V. 1956. A Clinical, Pathological, andGenetic Study of Multiple Neurofibro-matosis. Springfield, I11: Charles C.Thomas
18. Diaz, M. O., LeBeau, M. M., Pitha, P.,Rowley, J. D. 1986. Interferon and c-ets-I genes in the translocation (9;11)(p22;q23) in human acute monocyticleukemia. Science 231:265~7
19. Drabkin, H. A., Bradley, C., Hart, I.,Bleskan, J., Li, F. P., Patterson, D.1985. Translocation of c-myc in thehereditary renal cell carcinoma associ-ated with a t(3;8)(p14.2;q24.13) chro-mosomal translocation. Proc. Natl.Acad. Sci. USA 82:6980-84
20. Dryja, T. P., Cavenee, W., White, R.,Rapaport, J. M., Peterson, R., et al.1984. Expression of recessive alleles bychromosomal mechanisms in retinoblas-toma. N. Engl. J. Med. 310:550-53
21. Dryja, T. P., Rapaport, J. M., Epstein,J., Goorin, A. M., Weichselbaum, R.,et al. 1986. Chromosome 13 homozy-gosity in osteosarcoma without retino-blastoma. Am. J. Hum. Genet. 38:59-66
22. Eker, R., Mossige, J., Johannessen, J.V., Aars, H. 1981. Hereditary renal ade-nomas and adenocarcinomas in rats.Diag. Histopathol. 4:99--110
23. Fearon, E. R., Feinberg, A. P., Hamil-ton, S. H., Vogelstein, B. 1985. Loss ofgenes on the short arm of chromosome11 in bladder cancer. Nature 318:377-
8024. Fearon, E. R., Vogelstein, B., Fein-
berg, A. P. 1984. Somatic deletion andduplication of genes on chromosome 11in Wilms’ tumours. Nature 309:176-78
25. Festa, R. S., Meadows, A. T., Boshes,R. A. 1979. Leukemia in a black childwith Bloom’s syndrome. Cancer44:1507-10
26. Francke, U., Holmes, L. B., Atkins, L.,Riccardi, V. M. 1979. Aniridia-Wilms’tumor association: evidence for specificdeletion of llp13. Cytogenet. CellGenet. 24:185-92
27. Franeke, U., Kung, F. 1976. Sporadicbilateral retinoblastoma and 13q- chro-mosomal deletion. M ed. P ediatr. Oncol.2:379-85
28. Gardner, I-I. A., Gallic, B. L., Knight,L. A., Phillips, R. A. 1982. Multiplekaryotypic changes in retinoblastomatumor cells: presence of normal chromo-some no. 13 in most tumors. CancerGenet. Cytogenet. 6:201-11
29. Gateff, E. 1978.. Malig.nant neoplasmsof genetic ongm m Drosophilamelanogaster. Science 200:1448-59
30. Gilbert, F., Feder, M., Balaban, G.,Brangman, D., Lurie, D. K., et al.1984. Human neuroblastomas andabnormalities of chromosomes 1 and 17.Cancer Res. 44:5444-49
31. Gilman, P. A., Wang, N., Fan, S.-F.,Reede, J., Khan, A., Leventhal, B. G.1985. Familial osteosarcoma associatedwith 13; 14 chromosomal rearrangement.Cancer Genet. Cytogenet. 17:123-32
32. Godbout, R., Dryja, T. P., Squire, J.,Gallie, B. L., Phillips, R. A. 1983.Somatic inactivation of genes onchromosome 13 is a common event inretinoblastoma. Nature 304:451-53
33. Hansen, M. F., Koufos, A., Gallic, B.L., Phillips, R. A., Fodstad, ~3. et al.1985. Osteosarcoma and retinoblastoma:A shared chromosomal mechanismrevealing recessive predisposition. Proc.Natl. Acad. Sci. USA 82:1-5
34. Hecht, F., Hecht, B. K.-M., Morgan,R. 1986. T-cell cancer breakpoints atgenes for T-cell receptor on chromo-somes 7 and 14. Cancer Genet.Cytogenet. 20:181-83
35. Hecht, F., Sutherland, G. R. 1984.Fragile sites and cancer breakpoints.Cancer Genet. Cytogenet. 12:179-81
36. Isobe, M., Emanuel, B. S., Givol, D.,Oren, M., Croce, C. M. 1986. Localiza-tion of gene for human p53 tumour anti-gen to band 17p13. Nature 320:84-85
37. Kaneko, Y., Egues, M. C., Rowley, J.D. 1981. Interstitial deletion of shortann of chromosome 11 limited toWilms’ tumor ceils in a patient withoutaniridia. Cancer Res. 41:4577-78
38. Klein, G., Klein, E. 1985. Evolution oftumours and the impact of molecularoncology. Nature 315:190-95
39. Knudson, A. G. 1971. Mutation andcancer: statistical study of retinoblasto-ma. Proc. Natl. Acad. Sci. USA 68:820-23
40. I(nudson, A. G. 1976. Germinal andsomatic mutations in cancer. In Proc.5th Int. Congr. Hum. Genet. MexicoCity Oct. 10-15, 1976. pp. 367-371.Amsterdam: Excerpta Medica
41. Knudson, A. G. 1977. Genetics andetiology of human cancer. Adv. Hum.Genet. 8:1-66
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

GENETICS OF HUMAN CANCER 249
42. Knudson, A. G. 1978. Retinoblastoma:a prototypic hereditary neoplasm.Semin. Oncol. 5:57-60
43. Knudson, A. G. 1983. Genetics of hu-man cancer with special reference tomodel cancers. In Biocl~emical andBiological Markers of NeoplasticTransformation, ed. P. Chandra, pp.159-70. New York: Plenum
44. Knudson, A. G. 1984. Genetic pre-disposition to cancer. Hereditas100:171-72
45. Knudson, A. G. 1985. Hereditary can-cer, oncogenes, and antioncogenes.Cancer Res. 45;1437-43
46. Knudson, A. G., Meadows, A. T.,Nichols, W. W., Hill, R. 1976. Chro-mosomal deletion and retinoblastoma.N. Engl. J. Med. 295:1120-23
47. Knudson, A. G., Strong, L. C. 1972.Mutation and cancer: a model forWilms’ tumor of the kidney. J. Natl.Cancer Inst. 48:313-24
48. Knudson, A. G., Strong, L. C. 1972.Mutation and cancer: neuroblastoma andpheochromocytoma. Am. J. Hum.Genet. 24:514-32
49. Knudson, A. G., Strong, L. C., An-derson, D. E. 1973. Heredity and cancerin man. Prog. Med. Genet. 9:113-58
50. Kosseff, A. L., Hetrmann, J., Gilbert,E. F., Viseskul, C., Lubinsky, M., Op-itz, J. M. 1976. Studies of malformationsyndromes of man XXIX: the Beckwith-Wiedemann syndrome. Clinical, genet-ic, and pathogenetic studies of 12 cases.Eur. J. Pediatr. 123:139-66
51. Koufos, A., Hansen, M. F., Copeland,N. G., Jenkins, N. A., Lampkin, B. C.,Cavenee, W. K. 1985. Loss ofheterozygosity in three embryonaltumours suggest a common pathogeneticmechanism. Nature 316:330-34
52. Koufos, A., Hansen, M. F., Lampkin,D. B., Workman, M. L., Copcland, N.t3., et al. 1984. Loss of alleles at loci onhuman chromosome 11 during genesisof Wilms’ tumour. Nature 309:170-72
53. Ladda, R., Atkins, L,, Littlefield, J.,Neurath, P., Marimuthu, K. M. 1974.Computer-assisted analysis of chromo-somal abnormalities: detection of a dele-tion in aniridia/Wilms’ tumor syndrome.Science 185:784-87
54. Land, H., Parada, L, F., Weinberg, R.A. 1983. Cellular oncogenes and multi-step carcinogenesis. Science 222:771-78
55. LeBeau, M. M. 1986. Chromosomalfragile sites and cancer-specific re-arrangements. Blood 67:849-58
56. LeBeau, M. M., Diaz, M. O., Holt-greve, H., Karin, M., Rowley, J. D,
1984. Chromosomal localization of thehuman metallothionein genes and evi-dence of their rearrangement in the inv(16) (p13q22) associated with acutemyelomonocytic leukemia. Nature313;709-11
57. LeBeau, M. M., Rowley, J. D. 1984.Heritable fragile sites in cancer. Nature308:607-8
58. Lee, W. H., Murphree, A. L., Benedict,W. F. 1984. Expression and amplifica-tion of the N-myc gene in primary retino-blastoma. Nature 309:458-60
59. Maher, V. M., Ouellette, L. M., Cur-ren, R. D., McCormick, J. J. 1976. Fre-quency of ultraviolet light-inducedmutation is higher in xeroderma pigmen-tosum variant cells than in normal hu-man cells. Nature 261:593-95
60. Maher, V. M., Rowan, L. A., Silinskas,K. C., Kateley, S. A., McCormick, J. J.1982. Frequency of UV-induced neo-plastic transformation of diploid humanfibroblasts is higher in xeroderma pig-mentosum cells than in normal cells.Proc. Natl. Acad. Sci. USA 79:2613-17
61. Mechler, B. M., McGinnis, W., Geh-ring, W. J, 1985. Molecular cloning of&thai (2) giant larvae, a recessiveoncogene of Drosophila melanogaster.EMBO J. 4:1551-57
62. Meisner, L. F., Gilbert, E., Ris, H. W.,Haverty, G. 1979. Genetic mechanismsin cancer predisposition. Report of acancer family. Cancer 43:679-89
63. Miller, R. W., Fraumeni, J. F., Man-ning, M. D. 1964. Association ofWilms’ tumor with aniridia,hemihypertrophy and other congenitalmalformations. N. Engl. J. Med.270:922-27
64. Mintz, B., Sanyal, S. 1970. Clonal ori-gin of the mouse visual retina mappedfrom genetically mosaic eyes. Genetics64:43-44
65. Miiller, R., Slamon, D. J., Tremblay, J.M., Cline, M. J., Verma, I. M, 1982.Differential expression of cellularoncogenes during pre- and postnatal de-velopment of the mouse. Nature299:640-44
66. Murphree, A. L., Benedict, W. F. 1984.Retinoblastoma: clues to human onto-genesis. Science 223:1028-33
67. Murre, C., Waldmann, R. A., Morton,C. C., Bongiovanni, K. F., Waldman,T. A., et al. 1985. Human y-chait~ genesare rearranged in leukemic T ceils andmap to the short arm of chromosome 7.Nature 316:549-52
68. Nau, M. M., Brooks, B. J., Carney, D.N., Gazdar, A. F., Battey, J. F., et al.1986. Human small-cell lung cancers
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

250 KNUDSON
show amplification and expression of theN-myc gene. Proc. Natl. Acad. Sci. USA83:1092-96
69. Ncedleman, S. W., Yuasa, Y’., Srivasta-va, S., Aaronson, S. A. 1983, Normalcells of patients with high cancer risksyndromes lack transforming activity inthe NIH/3T3 transfection assay. Science222:173-75
70. Orkin, S. H., Goldman, D. S., Sallan,S. E. 1984. Development of homozy-gosity for chromosome 1 lp markers inWilms’ tumour. Nature 309:172-74
71. Passarge, E., Bartram, C. R. 1976,Somatic recombination as possible pre-lude to malignant transformation. InCancer and Genetics, ed. D. Bergsma,12:177-80. New York: Liss
72. Paterson, M. C., Smith, P. J. 1979.Ataxia telangiectasia: an inherited hu-man disorder involving hypersensitivityto ionizing radiation and related DNA-damaging chemicals. Ann. Rev. Genet.13:291-318
73. Pfeifer-Ohlsson, S., Rydnert, J., Gous-tin, A. S., Larsson, E., Bethsholtz, C.,Ohlsson, R. 1985. Cell-type-specificpattern of myc protooncogene expressionin developing human embryos, t’roc.Natl. Acad. Sci. USA 82:5050-54
74. Raizis, A. M., Becroft, D. M., Shaw,R. L., Reeve, A. E. 1985. A mitoticrecombination in Wilms’ tumor occursbetween the parathyroid hormone lo-cus and llp13. Hum. Genet. 70:344-46
75. Reed, T. E., Neel, J. V. 1955. A geneticstudy of multiple polyposis of the colon.Am. J. Hum. Genet. 7:236-63
76. Reeve, A. E., Eccles, M. R., Wilkins,R. J., Bell, G. I., Millow, L. J. 1985.Expression of insulin-like growth factor-II transcripts in Wilms’ tumour. Nature317:258-60
77. Reeve, A. E., Housiaux, P. J., Gardner,R. J. M., Chewings, W. E., Grindley,R. M., Millow, L. J. 1984. Loss ofHarvey ras allele in sporadic Wilms’tumour. Nature 309:174-76
78. Riccardi, V. M., Sujansky, E., Smith,A. C., Francke, U. 1978. Chromosomalimbalance in the aniridia-Wilms’ tumorassociation: l lp interstitial deletion.Pediatrics 61:604-10
79. Rosson, D., Tereba, A. 1984.Transforming N-ras genes have beenidentified in three childhood rhabdo-myosarcomas and one Wilms’ tumor.Proc. Am. Assoc. Cancer Res. 25:71
80. Schroeder, T. M., German, J. 1974.Bloom’s syndrome and Fanconi’s ane-mia: demonstration of two distinctive
patterns of chromosome disruption andrearrangement. Humangenetik 25:299-306
81. Scott, J., Cowell, I., Robertson, M. E.,Priestley, L. M., Wadey, R., et al.1985. Insulin-like growth factor-II geneexpression in Wilms’ turnout andembryonic tissues. Nature 317:260-62
82. Shabtai, F., Klar, D., Schwartz, A.,Moroz, A., Halbrecht, I. 1983. Markerchromosomes in a family with high in-cidence of cancer. Cancer Genet.Cytogenet. 9:281-87
83. Shiraishi, Y., Yosida, T. H., Sandberg,A. A. 1985. Malignant transformationof Bloom syndrome B-lymphoblastoidcell lines by carcinogens. Proc. Natl.Acad. Sci, USA 82:5102-6
84. Slamon, D. J., Cline, M. J. 1984. Ex-pression of cellular oncogenes duringembryonic and fetal development of themouse. Proc. Natl. Acad. Sci. USA81:7141-45
85. Slater, R. M. 1986. The cytogenetics ofWilms’ tumor. Cancer Genet. Cytoge-net. 19:37-41
86. Sorge, L. K., Levy, B. T., Maness, P.R. 1984. pp60c~rc is developmentallyregulated in the neural retina. Cell3,6:249-57
87. Sotelo-Avila, C., Gonzales-Crussi, F.,Fowler, J. W. 1980. Complete and in-complete forms of Beckwith-Wiede-mann syndrome: their oncogenic poten-tial, J. Pediatr. 96:47-50
88. Sparkes, R. S., Murphree, A. L., Lin-gua, R. W., Sparkes, M. C., Field, L.L., et al. 1983. Gene for hereditary reti-noblastoma assigned to human chromo-some 13 by linkage to esterase D. Sci-ence 219:971-73
89. Sparkes, R. S., Sparkes, M. C., Wilson,M. G., Towner, J. W., Benedict, W. F.,et al. 1980. Regional assignment ofgenes for human esterase D and retino-blastoma to chromosome band 13q14.Science 208:1042-44
90. Stanbridge, E. J. 1976. Suppression ofmalignancy in human cells. Nature260:17-20
91. Stewart, T. A., Pattengale, P. K., Le-der, P. 1984. Spontaneous mammaryadenocarcinomas in transgenic mice thatcarry and express MTV/myc fusiongenes. Cell 38:627-37
92. Tsujimoto, Y., Gorham, J., Cossman,J., Jaffe, E., Croce, C. M. 1985. Thet(14;18) chromosome translocations in-volved in B-cell neoplasms result frommistakes in VDJ joining. Science229:1390-93
93. Turleau, C., deGrouchy, J., Chavin-
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

GENETICS OF HUMAN CANCER 251
Colin, F., Mart¢lli, H., Voyer, M.,Charlas, R. 1984. Trisomy llp15 andBeckwith-Wiedemann syndrome. A re-port of two cases. Hum. Genet. 67:219-21
94. Vijayalaxmi, Evans, H. J., Ray, J. H.,German, J. 1983. Bloom’s syndrome:evidence for an increased mutationfrequency in vivo. Science 221:851-53
95. Waziri, M., Patil, S. R., Hanson, J. W.,Bartley, J. A. 1983. Abnormality ofchromosome 11 in patients with featuresof Beckwith-Wiedemann syndrome. J.Pediat. 102:873-76
96. Whang-Peng, J., Bunn, P. A., Kao-Shan, C. S., Lee, E. C., Carney, D. N.,et al. 1982. A nonrandom chromosomalabnormality, del 3p(14-23), in human
small cell lung cancer (SCLC). CancerGenet. Cytogenet. 6:119-34
97. Yoshida, M. A., Ohyashiki, K., Ochi,H., Gibas, Z., Pontes, J. E., et al. 1986.Cytogenetic studies of tumor tissue frompatients with nonfamilial renal cell carci-noma. Cancer Res. 46:2139-47
98. Yunls, J. J. 1984. Fragile sites and pre-disposition to leukemia mid lymphoma.Cancer Genet. Cytogenet. 12:85-88
99. Yunis, J. J., Ramsay, N. 1978. Retino-blastoma and subband deletion ofchromosome 13. Am. J. Dis. Child.132:161-63
100. Zimmerman, K. A., Yancopoulos, G.D., Collum, R. G., Smith, R. K., Kohl,N. E., et al. 1986. Differential expres-sion of myc family genes during murinedevelopment. Nature 319:780-83
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.

Ann
u. R
ev. G
enet
. 198
6.20
:231
-251
. Dow
nloa
ded
from
arj
ourn
als.
annu
alre
view
s.or
gby
Uni
vers
ity o
f M
inne
sota
- L
aw L
ibra
ry o
n 10
/27/
06. F
or p
erso
nal u
se o
nly.