
General Neurology: “Mind Bending” Neurologic Conundrumsmudgroup.com/files/Rengachary.pdf ·...
67
Metropolitan Underwriting Discussion Group General Neurology: “Mind Bending” Neurologic Conundrums Dave Rengachary, MD Vice President and Medical Advisor January 26, 2015
Transcript of General Neurology: “Mind Bending” Neurologic Conundrumsmudgroup.com/files/Rengachary.pdf ·...
Metropolitan Underwriting Discussion Group
General Neurology: “Mind Bending” Neurologic Conundrums
Dave Rengachary, MDVice President and Medical AdvisorJanuary 26, 2015
Transient Ischemic Attacks (versus mimics)
2
3
“We often receive attending physician statements where we have difficulty telling whether an individual had a TIA. We already know what TIAs are and how to apply ratings for these events. We need some guidance on situations where it is not entirely certain that a person had an actual TIA or whether it might be another condition like migraine”
TIA: Previous definition
“Sudden focal neurologic deficit lasting less than 24 hours, presumed to be of vascular origin, and confined to an area of the brain or eye perfused by a specific artery”
TIA: New Definition (AHA/ASA)
“a brief episode of neurologic dysfunction caused by focal brain or retinal ischemia, without evidence of acute infarction”
Easton JD et al. Stroke. 2009; 40:228 1
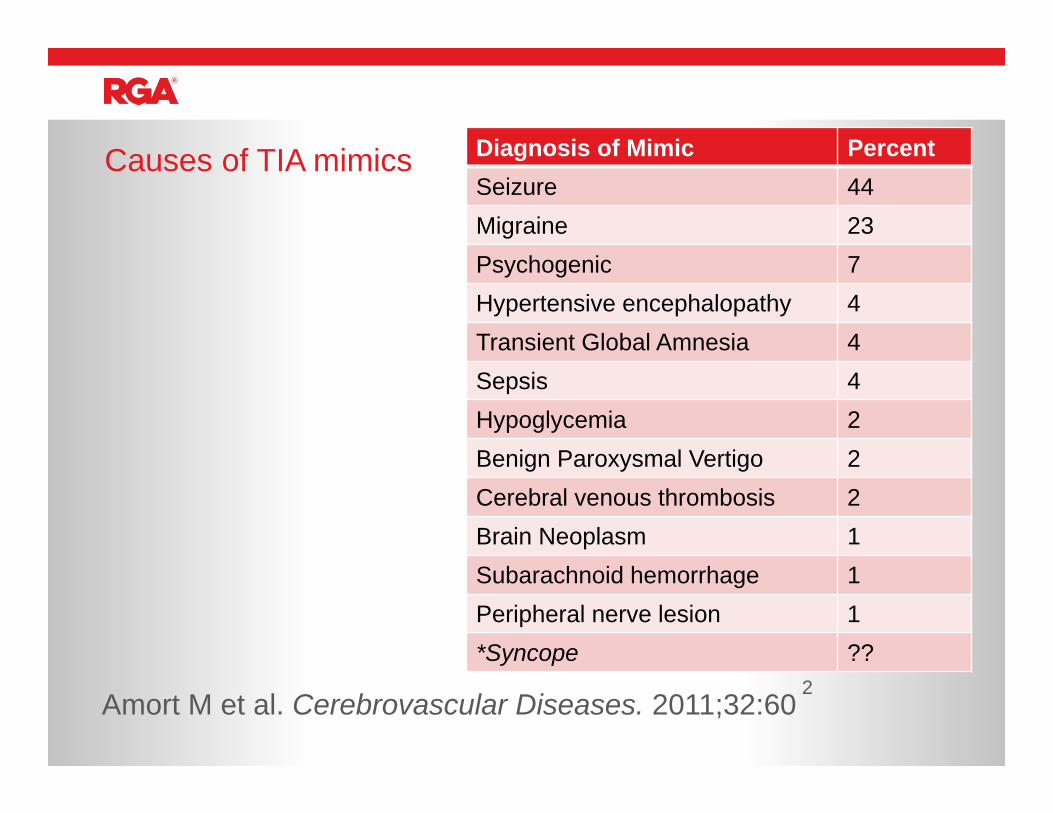
Causes of TIA mimics
Amort M et al. Cerebrovascular Diseases. 2011;32:602
Diagnosis of Mimic PercentSeizure 44Migraine 23Psychogenic 7Hypertensive encephalopathy 4Transient Global Amnesia 4Sepsis 4Hypoglycemia 2Benign Paroxysmal Vertigo 2Cerebral venous thrombosis 2Brain Neoplasm 1Subarachnoid hemorrhage 1Peripheral nerve lesion 1*Syncope ??
Symptoms Predictive of TIA mimic
• Headache - no mechanism whereby TIA should cause headache• Memory Loss (*see below!)• Blurred vision (as opposed to loss of vision or diplopia)• Syncope• Recurrent stereotyped episodes with negative workup• Symptoms that do not conform well to a single artery - generalized
symptoms with a gradual or hazy onset rather than focal sudden onset symptoms ("weak" all over”, "dizzy“)
• Lack of other vascular risk factors
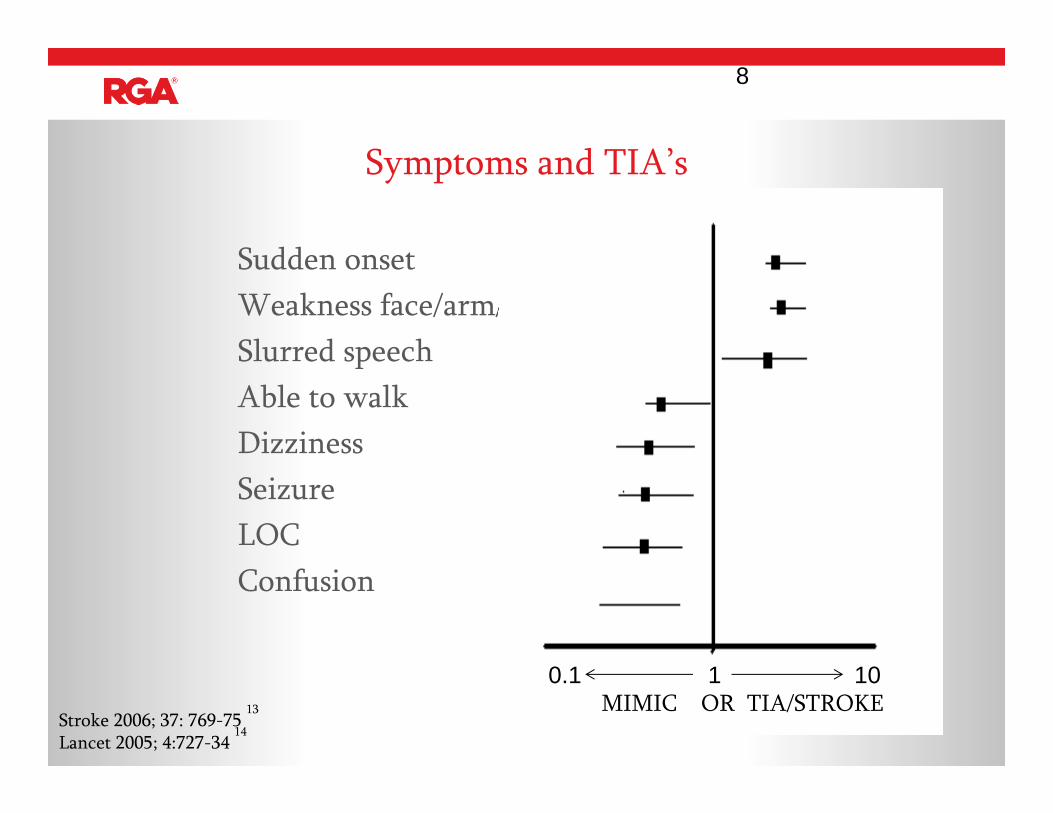
Symptoms and TIA’s
Sudden onsetWeakness face/arm/legSlurred speechAble to walkDizzinessSeizureLOCConfusion
8
0.1 1 10MIMIC OR TIA/STROKE
Stroke 2006; 37: 769-75 13
Lancet 2005; 4:727-34 14
Prognosis of TIA mimics
“ At 3 months, stroke, recurrent TIA and myocardial infarction were absent in patients with TIA mimics but occurred in 13 (5.2%), 20 (8.1%) and 3 (1.2%) TIA patients, respectively.”
Amort M et al. Cerebrovascular Diseases. 2011;32:62 1
Transient global amnesia
• One of the most interesting neurologic phenomenon – happens in entirely normal people with little medical history
• Pathogenesis unknown• Key feature is sudden and profound inability to form new memories,
repetition of questions lasting on the order of hours without focal symptoms
• Often follows exercise• Workup typically normal (MRI, ECHO, carotids, EEG)• Entirely different prognosis
• Low rate of recurrence (6%) Lower rate of stroke, myocardial infarction or deathPantoni Let al. European Journal of Neurology. 2005; 12: 350
5
Funny Spots on the Brain
“Notation is made of white matter hyperintensities – these are nonspecific findings of unlikely clinical significance. However…..
“…cannot exclude Lyme disease, vasculitis, multiple sclerosis and demyelinating variants, small vessel strokes, dementia, migrainous phenomenon, hypertensive disease, microbleeds…..”
“….clinical correlation is advised”“(please don’t sue me)”
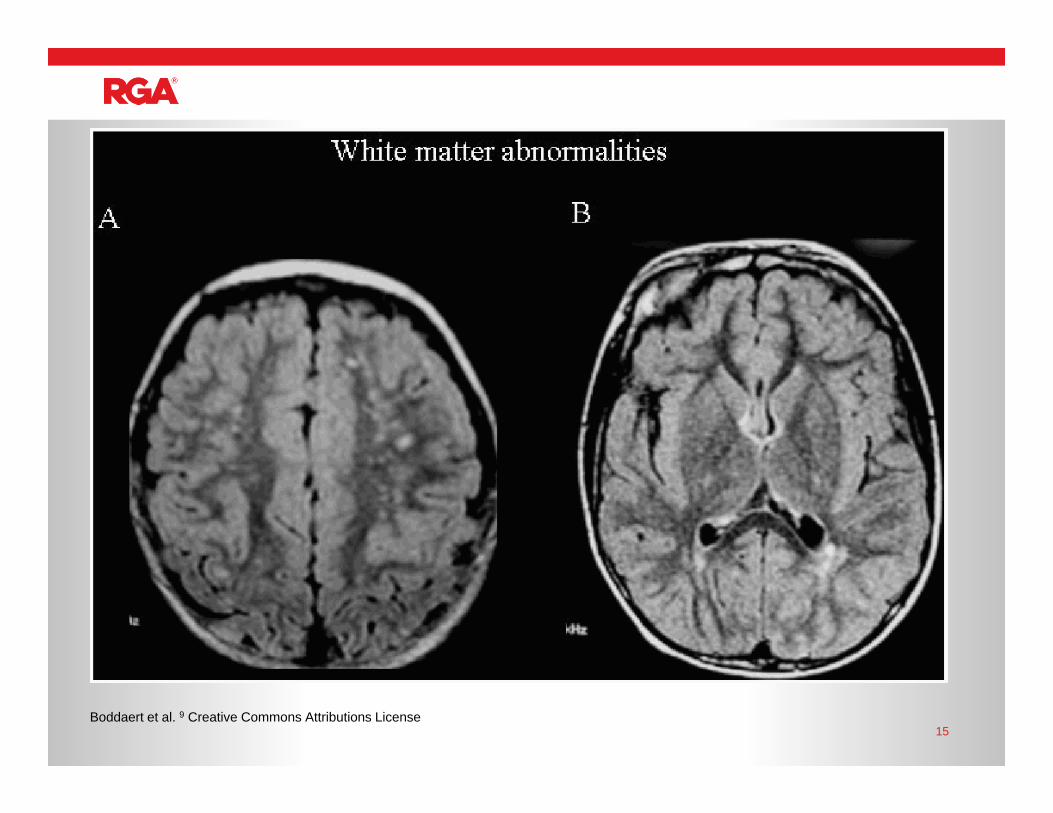
15Boddaert et al. 9 Creative Commons Attributions License
White matter hyperintensities Small vessel ischemic changes Leukoaraiosis Lacunar infarcts Microvascular Changes High Signal Intensity Areas (HSIA) Age related changes FLAIR hyperintensities Dilated Virchow-Robin Spaces UBOs (Unidentified Bright Objects)
Different names for the same game
16
Complicating matter further these and other incidental findings are quite common - NEJM article by Vernooij et al.6 found that about one in ten people in the general population had a “incidentaloma” on imaging.
Studies also vary significantly in terms of what is “counted” as a white matter change – size? Number?
White Matter Hyperintensities
17
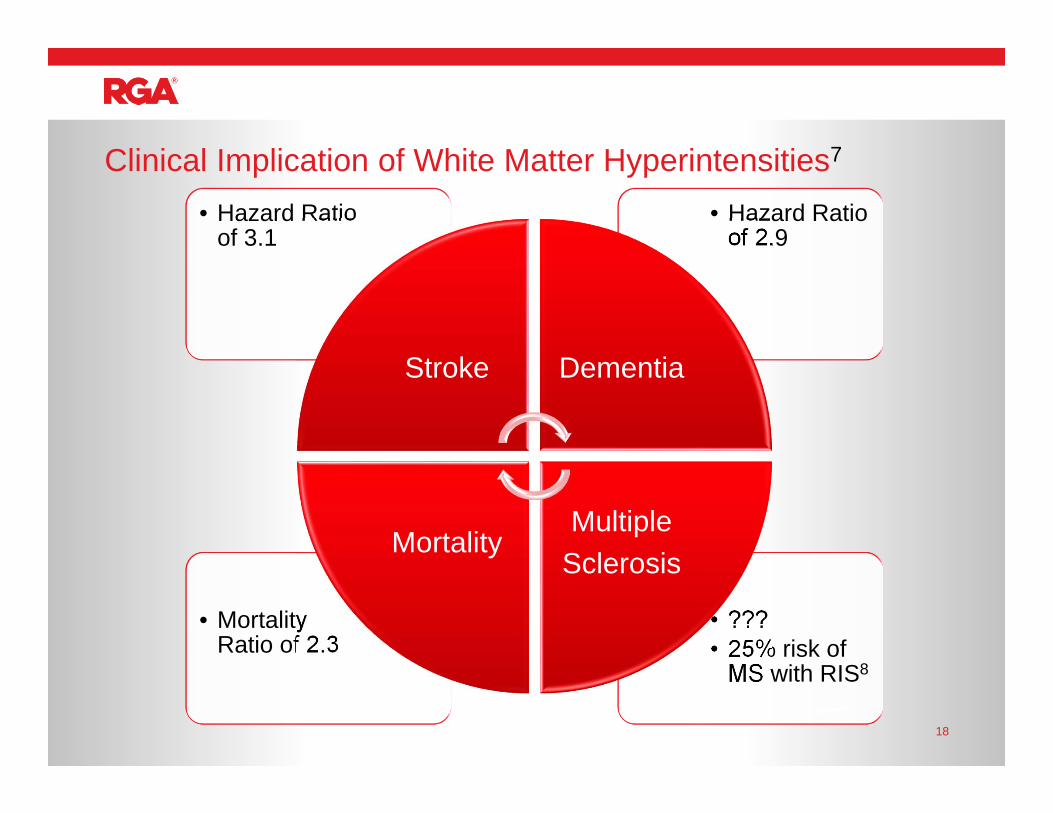
• ???• 25% risk of
MS with RIS8
• Mortality Ratio of 2.3
• Hazard Ratio of 2.9
• Hazard Ratio of 3.1
Stroke Dementia
MultipleSclerosis
Mortality
Clinical Implication of White Matter Hyperintensities7
18
Age
Symptomatic
Vascular Risk Profile
Enhancement
Location
Number
Progression (or stability)
Factors to consider and Red Flags
19
“Mild” Carotid Stenosis
We receive carotid ultrasound reports that show lesions in the range of 10-49% obstruction. How worried should we be about this degree of obstruction?
Non-stenotic carotid disease
0
50
100
150
200
250
300
350
0 10 20 30 40 50 60 70 80 90 100
Velo
city
(cm
/sec
)
Diameter Stenosis %
SystolicDiastolic
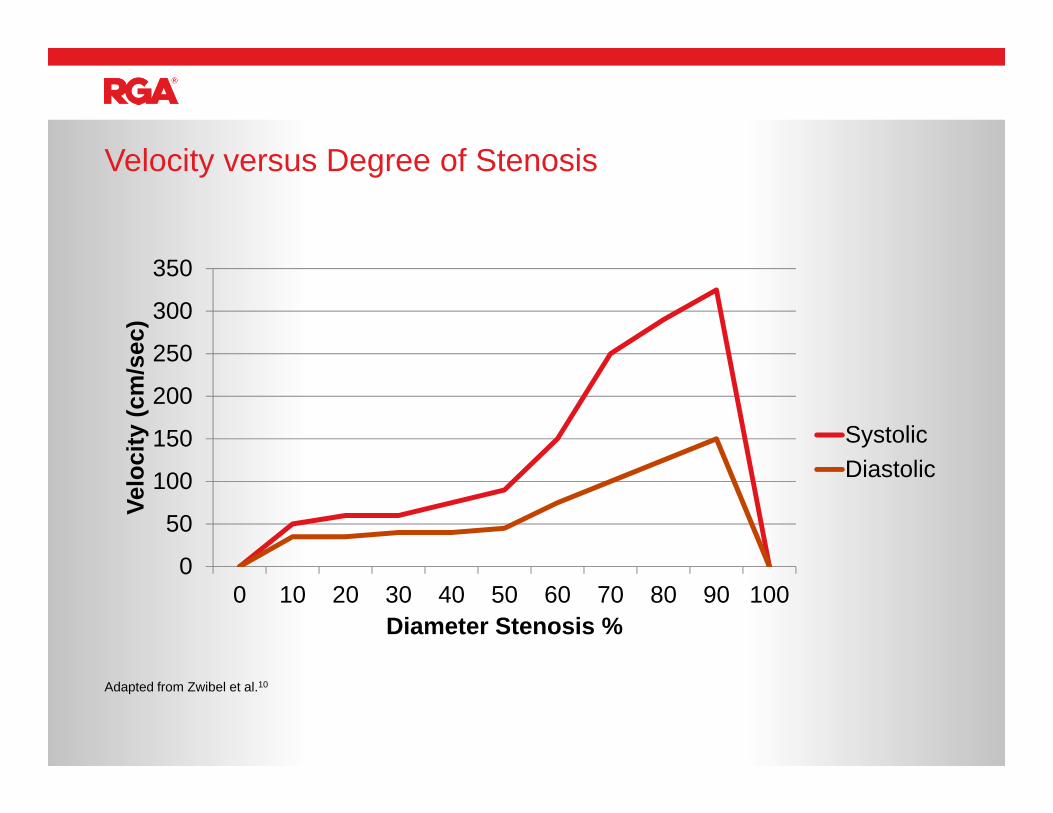
Velocity versus Degree of Stenosis
Adapted from Zwibel et al.10
• “ulceration”• “complex”• “heterogeneous”• “soft”• “intraluminal thrombus”• “plaque hemorrhage”• “Echo Lucent” (high lipid content)
Bottom line: red flags for non-stenotic carotid lesions
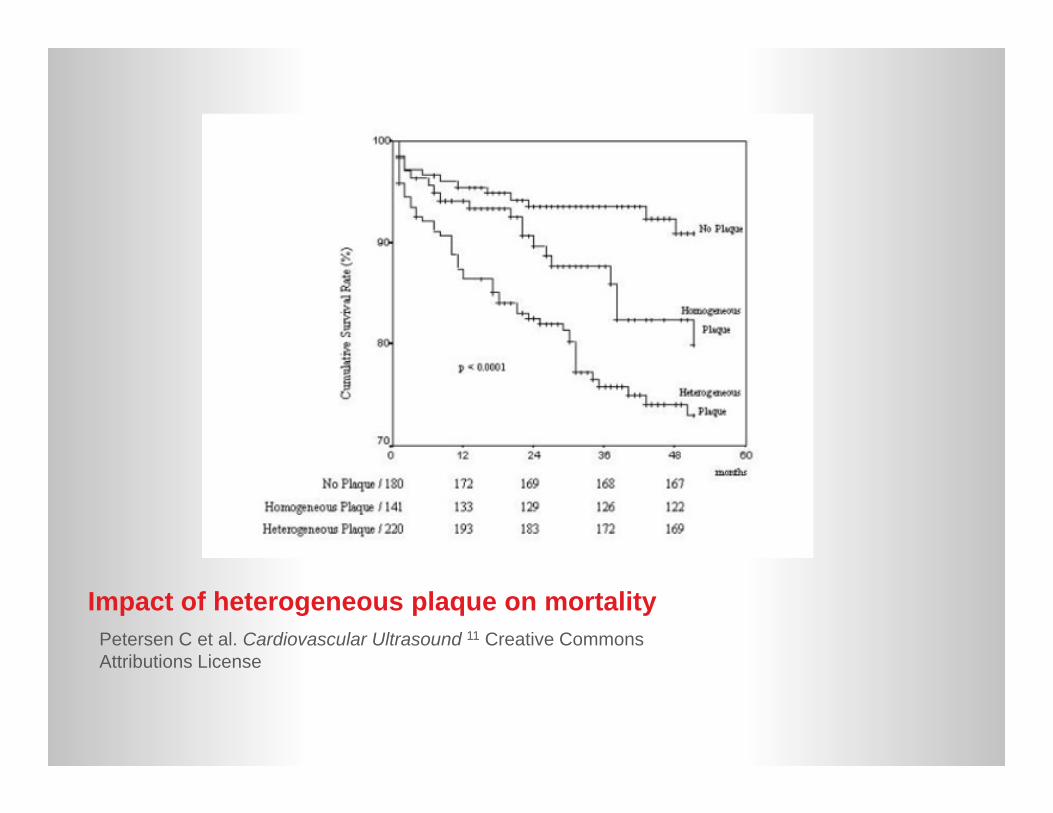
Impact of heterogeneous plaque on mortalityPetersen C et al. Cardiovascular Ultrasound 11 Creative Commons Attributions License
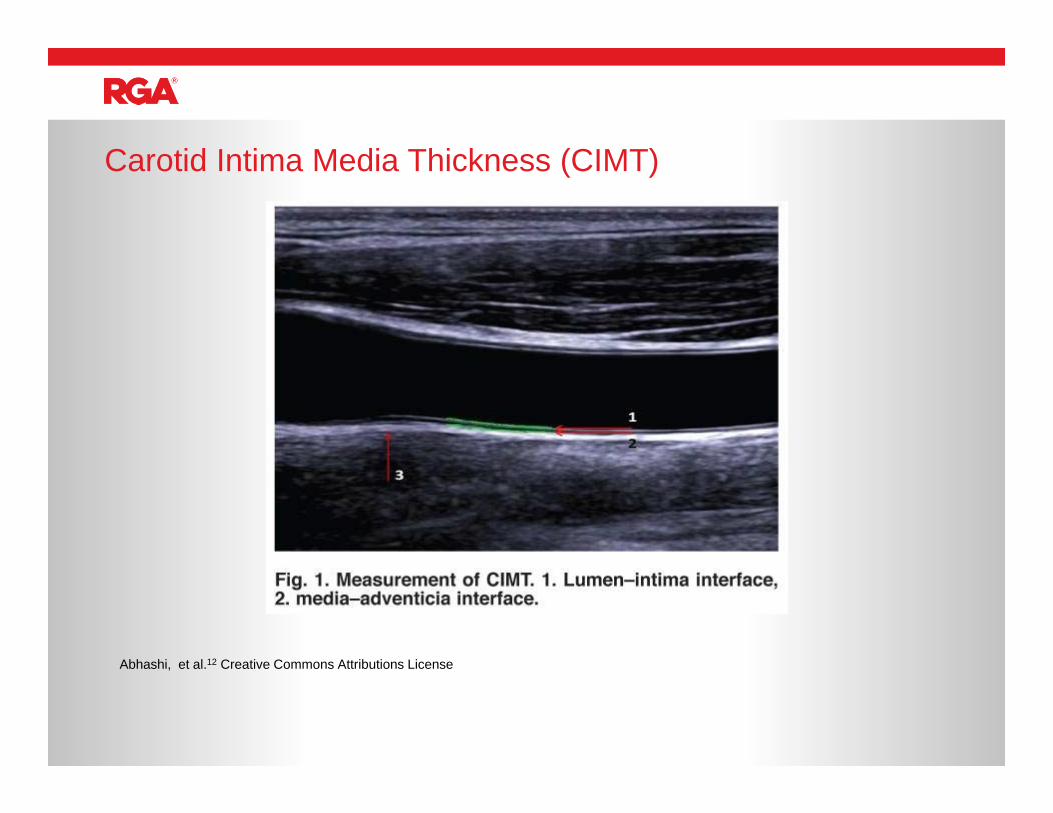
Carotid Intima Media Thickness (CIMT)
Abhashi, et al.12 Creative Commons Attributions License
Peripheral Neuropathy
It is fairly common for us to see applicants with either sensory or motor neuropathies as determined by either clinical history or EMG reports. Which ones should we worry about, and which ones are less concerning?
Peripheral neuropathy
• 23% of patients aged 70-7915
• 40% of patients over 8015
• Bottom line : isolated absence of sural nerve likely little consequence in terms of morbidity and mortality, especially in the elderly
“Normal” loss of sural nerve with aging
• Time course• “Demyelinating”• Any neuropathy that affects the arms or cranial nerves suggests a more advanced
process • Same as indicators for nerve biopsy:
o Demyelination by NCTso Asymmetry (also indicate an immune process)o Significant functional disability (e.g. foot drop/AFO)o Hereditary history (e.g. Friedreich’s ataxia, familial amyloid, certain spino-
cerebellar ataxias)o Systemic disease (vasculitis, Sjogren's, amyloid)
Peripheral neuropathy: malignant indicators
Red flag indicators in NCT/EMG reports
• "Demyelinating" or "significant slowed conduction velocities"
• "Conduction Block”• “Asymmetric”NCT• "Acute" "Fibrillations" "Positive Sharp
Waves" these latter two are indicators of an active recent process very much analogous to contrast enhancement on MRI
• MyopathyEMG
Diabetic peripheral neuropathy
• 57% of patients who died related to complications of diabetes (68% cardiovascular) had neuropathy compared to 23% of those survivors at the end of a 9 year follow up period16.
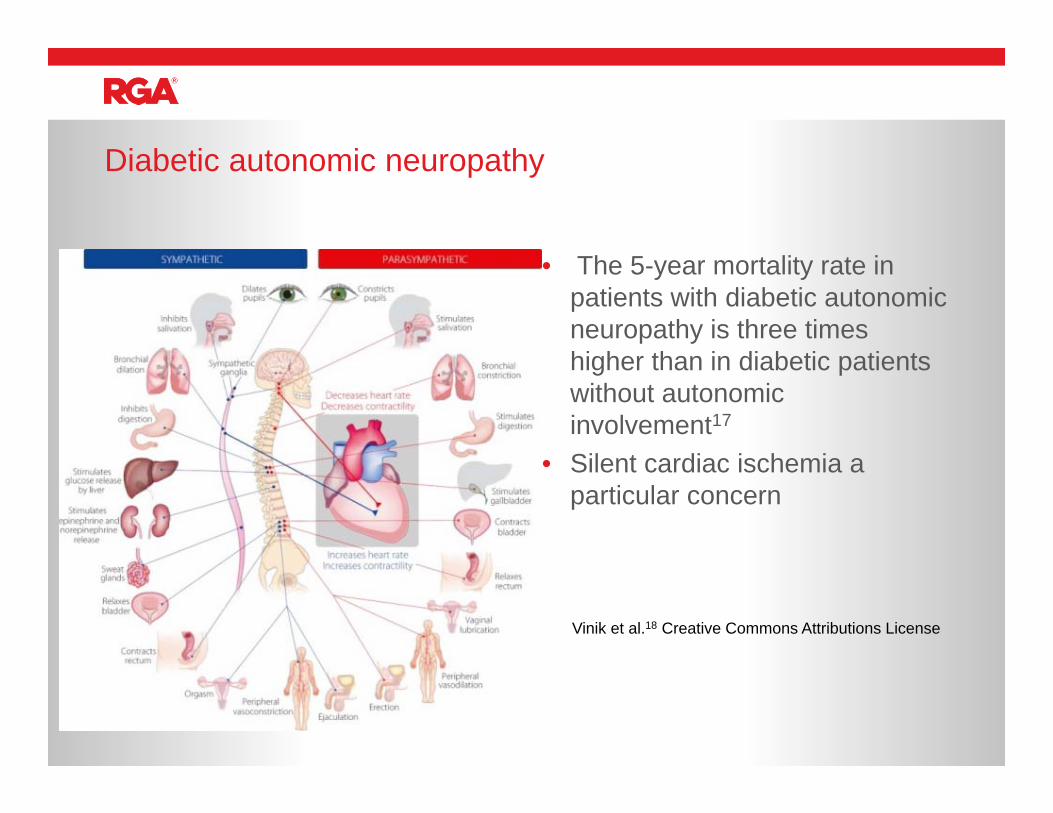
Diabetic autonomic neuropathy
• The 5-year mortality rate in patients with diabetic autonomic neuropathy is three times higher than in diabetic patients without autonomic involvement17
• Silent cardiac ischemia a particular concern
Vinik et al.18 Creative Commons Attributions License
Syrinx
“Please define a syrinx and help understand the associated mortality.”
Syrinx
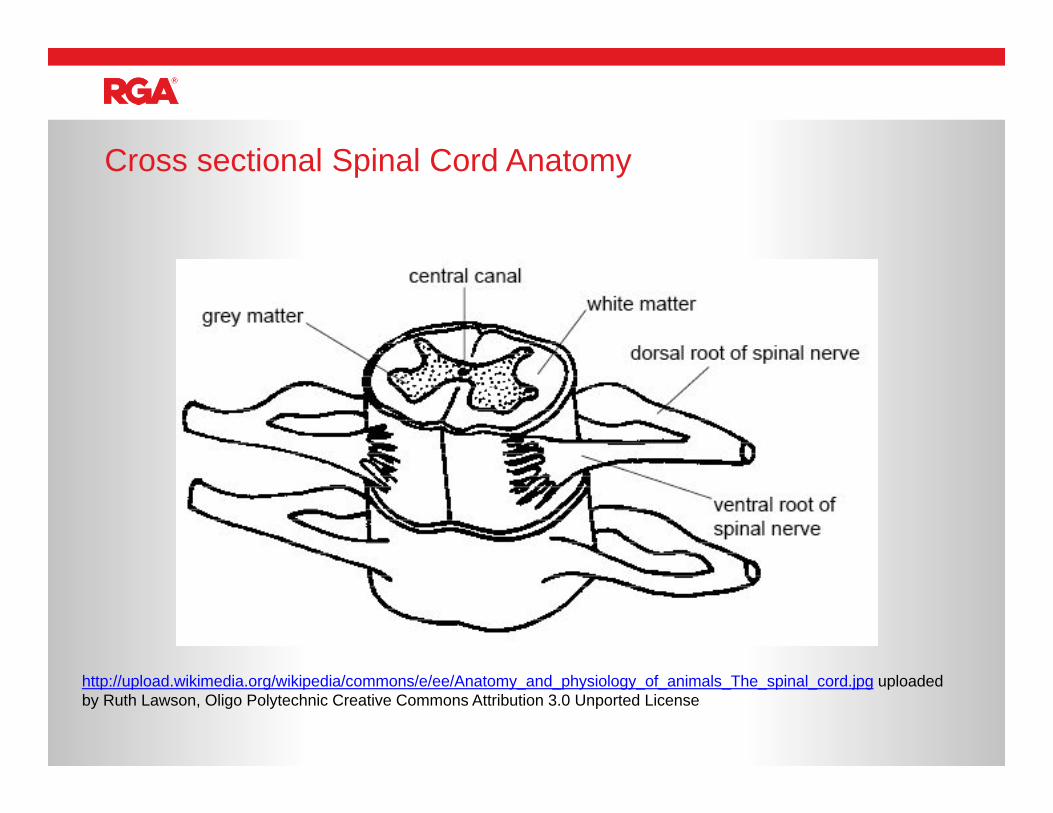
Cross sectional Spinal Cord Anatomy
http://upload.wikimedia.org/wikipedia/commons/e/ee/Anatomy_and_physiology_of_animals_The_spinal_cord.jpg uploaded by Ruth Lawson, Oligo Polytechnic Creative Commons Attribution 3.0 Unported License
Hydromyelia
Synrinx
Syringomyelia
Cape like pattern of
sensory loss
Bowel and Bladder loss
Incomplete Paraplegia
and sensory loss
Syrinx Symptoms

http://commons.wikimedia.org/wiki/File:Syringomyelia.jpg uploaded by Cyborg Ninja license CC Attribution ShareAlike 3.0
• Very often can be an incidental or equivocal finding (a slightly enlarged central canal is a normal variant)
• Overall rare condition (8.4 out of 100,000, mean age of onset is 30) with a wide variety of underlying structural conditions:
• Etiologies • Congenital
• Birth Defects (Chiari Malformations)• Tethered Spinal cord
• Acquired• Spinal cord tumors• Trauma• Hemorrhage• Meningitis• Arachnoiditis• Idiopathic
• Surgical indications and outcomes are unclear (are you treating the cause or temporizing a solution? - shunts can become clogged)
Syrinx
Good prognostic indicators• Idiopathic, asymptomatic, incidental• Localized syrinx (< 3 vertebra)
predicted stability without surgical intervention
Bad prognosticators:• Any progression (clinically or
radiographically) over time• Higher = worse - more to lose
Syrinx prognostic indicators
• 91% of 48 children with idiopathic (but not necessarily incidental) syrinxes remained asymptomatic over 2.5 years19
• In a retrospective study of small incidental syrinxes (2 mm and < 3 vertebral levels) , none of the 32 syrinxes enlarged at 32 months20
Arnold Chiari Malformations
Please review the various types of Arnold Chiari Malformations and mortality concerns with each.
Arnold Chiari Malformations
42
43http://upload.wikimedia.org/wikipedia/commons/e/e8/Brain_chrischan.jpg uploaded by Christian Linder Creative Commons Attribution Share Alike License
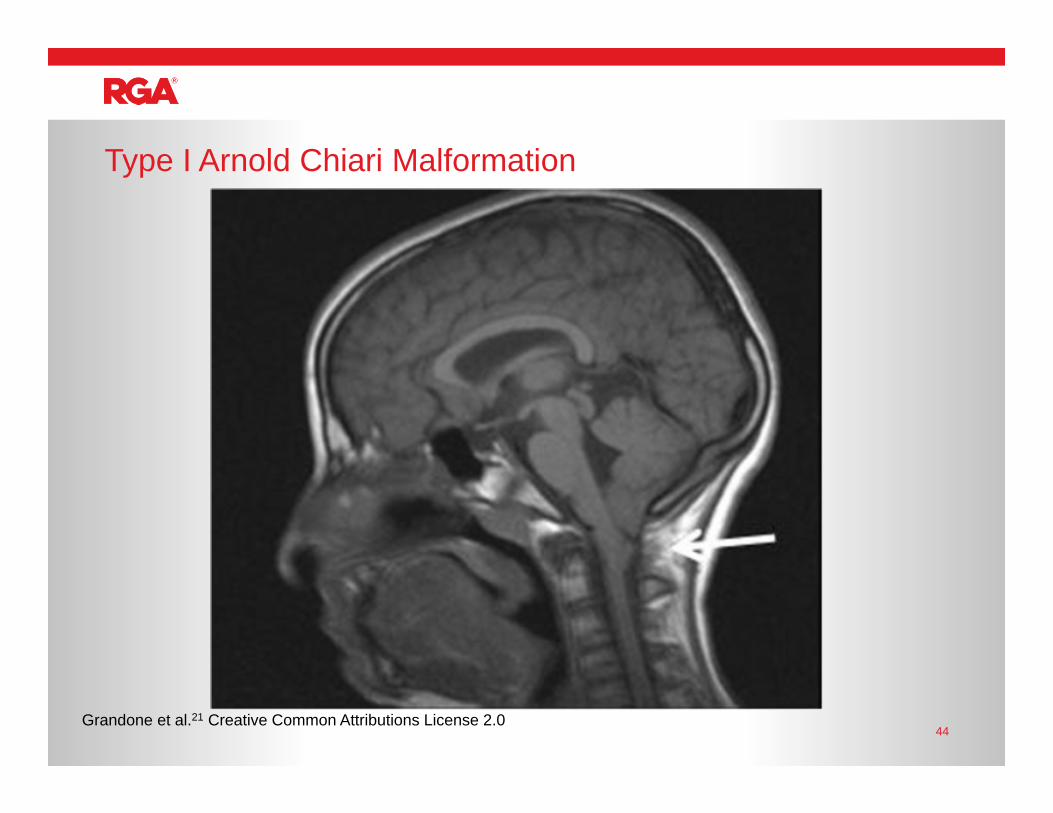
Type I Arnold Chiari Malformation
44Grandone et al.21 Creative Common Attributions License 2.0
Defined as a herniation of the cerebellum of > 5mm Typically presents in adolescents or young adults with symptoms of increased
intracranial pressure, syrinx or compression of the brainstem and cerebellum Symptoms:
Key Symptom: Headaches that increase with cough, position, pressure Visual changes / Papilledema Absent gag reflex Syncope / Dizziness Hoarseness (cranial nerve X) Muscle weakness Tinnitus Sensory deficits Dysphagia Dysarthria Ataxia • Nystagmus (vertical and downbeating)
Type I Chiari Malformation
• Major caveat is that this is much more likely to be found as an incidental or asymptomatic finding
• Around 0.8% of all MRI scans performed (or of 22,591) at Johns Hopkins.22
• Average degree of herniation 11 mm• Only one syrinx found
• Bottom line: Good Prognostic indicators:• Asymptomatic, incidental radiographic finding (including non specific headaches)• Adult Presentation• Normal Neurologic exam• Herniation <12 mm23
• No syrinx or hydrocephalus (no evidence of pressure above or below the lesion)• No radiographic progression over time
Type I Chiari malformation
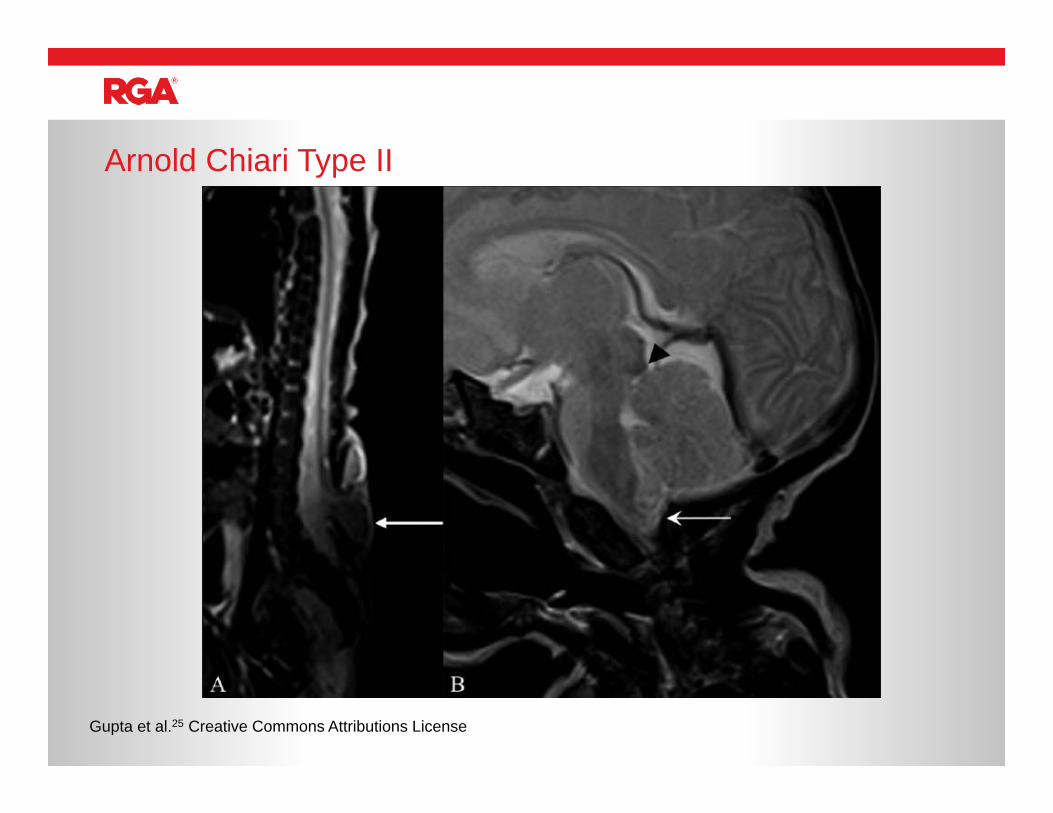
• Present in children• Portions of the brainstem and cerebellum herniate
downwards into the foramen magnum • Associated with other birth defects
• Almost always with a myelomeningocele (type of spina bifida from incomplete closure of the spinal canal)
• Absence of the cerebellar vermis• 15 % die by age 3, 33% survivors with significant
neurologic disability24
Type II Chiari malformation
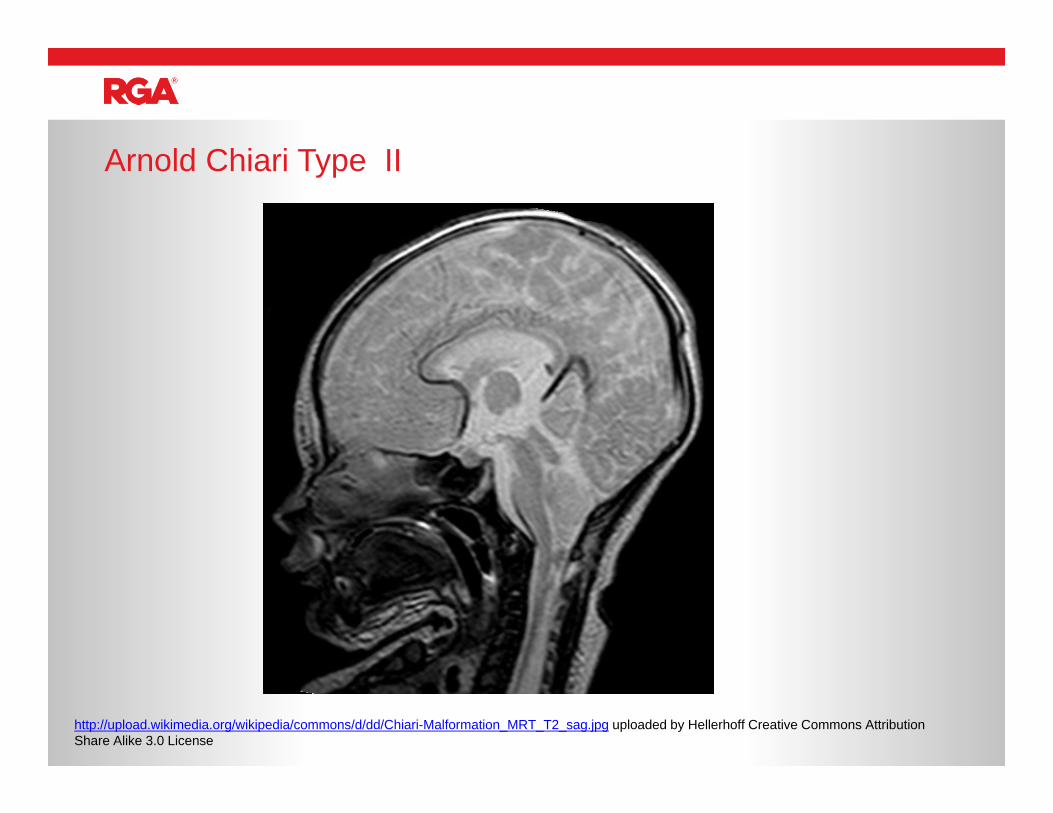
Arnold Chiari Type II
http://upload.wikimedia.org/wikipedia/commons/d/dd/Chiari-Malformation_MRT_T2_sag.jpg uploaded by Hellerhoff Creative Commons Attribution Share Alike 3.0 License
Arnold Chiari Type II
Gupta et al.25 Creative Commons Attributions License
Parkinsonism – how can we best risk stratify this disease?
Parkinson’s disease
• UPRDS (Unified Parkinson’s Rating Disease Scale)
• 42 point scale with measures of mentation, behavior, mood, activities of daily living, motor exam, dyskinesias, and complications of therapy.
• A wonderful tool, little used outside of the ivory towers.
Parkinson’s disease
• Older age of onset (variably defined as over age 57-78 years) (two Class II and one Class III studies) and rigidity/hypokinesia as a presenting symptom (two class II studies) are factors which are probably useful in predicting a more rapid rate of motor progression of PD.
• The presence of associated comorbidities (one class II study), features of PIGD (Postural Instability and Gait Disturbance (one Class II and one Class III studies) and male gender (one class II study), are factors that are possibly useful for predicting a more rapid rate of motor progression of PD.
• Tremor as the initial presentation is a factor that is possibly useful in predicting slower progression and a longer response to levodopa therapy (one Class II and one Class III studies).
• Older age of onset and initial manifestations of hypokinesia/rigidity are factors that are probably useful in predicting earlier development of cognitive declineand dementia (two Class II and one Class III studies).
• Older age of onset, dementia, and decreased dopamine responsiveness are factors that are possibly useful in predicting an increased risk for nursing home placement and shorter survival after diagnosis (one Class II study).
Prognosis in Parkinson'sAAN Practice Parameter: Diagnosis and Prognosis of PD26
• Rotterdam Study - Prospective Cohort Study between 1990-1999 with 6969 patients found mortality ratio (1.8)27
• The Sydney multicentre study of Parkinson’s disease: progression and mortality at 10 years. Mean Duration of disease 9.1 years28
• SMR 1.86• Increased mortality - Older Age/Duration of disease (SMRs increased with time)
• Women after 8 years duration disease• Admission to NH
Mortality in Parkinson's
• DATATOP Cohort (study of selegiline and alpha-tocopherol)29
• Increased mortality• Gait Dysfunction• Poor Response to Levodopa• Increased Parkinson Symmetry• Severity of Parkinsonism/Rate of Progression
• Predictors of Survival in Patients With Parkinson Disease30
• Large Retrospective Study in 138000 patients published by Washington University Movement Disorders Center
• Female hazard ratio 0.74• Asian hazard ratio 0.86• Hispanic hazard ratio 0.72• Dementia hard ratio 1.72
Mortality in Parkinson's
• Bottom Line - higher risk patients are males with dementia, higher rates of falls, less response to levodopa, and more rigid symmetric parkinsonism
Parkinson’s
Special Topics in Epilepsy
Typically a consideration for focal epilepsy resistant to two reasonable AED trials.
Anterior temporal lobectomy including mesial structures (hippocampus,) and lesionectomy are most common procedures
Success rates vary widely, but average rate of seizure freedom is 80%
Frequency of epilepsy surgery has remained fairly static (and fairly low) over the last 15 years.
Epilepsy surgery
57
Recent cohort study from 1975 to 1995 found an overall SMR of 2.0. Confirming an earlier finding, right hemispheric surgeries were associated with significant excess mortality. 31
A second study 32 found that almost all excess mortality was in those patients with seizures refractory to epilepsy surgery. Only 1 of 19 deaths occurred in those who were free of seizures. An additional study33 found that mean duration of epilepsy prior to surgery was an important prognostic factor
Bottom line, in those who are status post epilepsy surgery rate according to residual seizure frequency
Be particularly cautious with post surgical depression, not necessarily related to seizure control!
Mortality after epilepsy surgery
58
Look for evidence of non-compliance! In those with poor follow-up, breakthrough seizures are common
secondary to decreasing plasma concentrations of AEDs (esp. Lamotrigine, Oxacarbezine).
A study from 300 countries examining seizure frequency during pregnancy found stability in 64%, decrease in 6%, and increase in 18% 34
Recent AAN/AES practice parameter guidelines found no convincing evidence of increased frequency of cesarean delivery, pregnancy related bleeding (maternal Vitamin K no longer recommended), status epilepticus, seizures, or preeclampsia).
Pregnancy and Epilepsy
59
Occur in 1 every 25 children Typically at temperatures > 102 F Generalized, last less than 15 minutes Although there is a small increased risk of adult epilepsy, 95-98% do
not develop epilepsy No effect on cognitive function
Febrile Seizures
60
Complex Febrile Seizures Focal Recurrent Prolonged
Family history of febrile seizures Neurologic abnormalities Seizures at temperatures less than 101 F One mortality study on febrile seizures – SMRs were 1.0-1.9 in first
two years of life and then approaches that of general population. SMR for complex febrile seizures was 1.99. 35
Febrile Seizures – Poor Prognostic Indicators
61
1. Easton, J. Donald, Jeffrey L. Saver, Gregory W. Albers, Mark J. Alberts, Seemant Chaturvedi, Edward Feldmann, Thomas S. Hatsukami, et al. “Definition and Evaluation of Transient Ischemic Attack A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association Stroke Council; Stroke 40, no. 6 (June 1, 2009): 2276–93.
2. Amort, Margareth, Felix Fluri, Juliane Schäfer, Florian Weisskopf, Mira Katan, Annika Burow, Heiner C. Bucher, Leo H. Bonati, Philippe A. Lyrer, and Stefan T. Engelter. “Transient Ischemic Attack versus Transient Ischemic Attack Mimics: Frequency, Clinical Characteristics and Outcome.” Cerebrovascular Diseases 32, no. 1 (2011): 57–64.
3. Hand, Peter J., Joseph Kwan, Richard I. Lindley, Martin S. Dennis, and Joanna M. Wardlaw. “Distinguishing between Stroke and Mimic at the Bedside: The Brain Attack Study.” Stroke; a Journal of Cerebral Circulation 37, no. 3 (March 2006): 769–75.
4. Nor, Azlisham Mohd, John Davis, Bas Sen, Dean Shipsey, Stephen J. Louw, Alexander G. Dyker, Michelle Davis, and Gary A. Ford. “The Recognition of Stroke in the Emergency Room (ROSIER) Scale: Development and Validation of a Stroke Recognition Instrument.” Lancet Neurology 4, no. 11 (November 2005): 727–34.
5. Pantoni, L., E. Bertini, M. Lamassa, G. Pracucci, and D. Inzitari. “Clinical Features, Risk Factors, and Prognosis in Transient Global Amnesia: A Follow-up Study.” European Journal of Neurology: The Official Journal of the European Federation of Neurological Societies 12, no. 5 (May 2005): 350–56.
6. Vernooij, Meike W., M. Arfan Ikram, Hervé L. Tanghe, Arnaud J.P.E. Vincent, Albert Hofman, Gabriel P. Krestin, Wiro J. Niessen, Monique M.B. Breteler, and Aad van der Lugt. “Incidental Findings on Brain MRI in the General Population.” New England Journal of Medicine 357, no. 18 (November 1, 2007): 1821–28. doi:10.1056/NEJMoa070972.
References
7. Debette S, Markus HS. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: systematic review and metaanalysis. BMJ. 2010;341:c3666.
8. Okuda, D. T., et al. "Incidental MRI anomalies suggestive of multiple sclerosis The radiologically isolated syndrome." Neurology 72.9 (2009): 800-805.
9. Boddaert, Nathalie, Mônica Zilbovicius, Anne Philipe, Laurence Robel, Marie Bourgeois, Catherine Barthélemy, David Seidenwurm, et al. “MRI Findings in 77 Children with Non-Syndromic Autistic Disorder.” PloS One 4, no. 2 (2009): e4415.
10. Zwiebel, W J. “Duplex Sonography of the Cerebral Arteries: Efficacy, Limitations, and Indications.” American Journal of Roentgenology 158, no. 1 (January 1, 1992): 29–36. doi:10.2214/ajr.158.1.1727355.
11. Petersen, Christina, Patricia B. Peçanha, Lucia Venneri, Emilio Pasanisi, Lorenza Pratali, and Eugenio Picano. “The Impact of Carotid Plaque Presence and Morphology on Mortality Outcome in Cardiological Patients.” Cardiovascular Ultrasound 4, no. 1 (March 24, 2006):
12. Abhashi, Sejran Ahmet, Fadil Uke Kryeziu, and Feim Durak Nazreku. “Increased Carotid Intima-Media Thickness Associated with High Hs-CRP Levels Is a Predictor of Unstable Coronary Artery Disease.” Cardiovascular Journal of Africa 24, no. 7 (August 2013): 270–73.
13. Hand, Peter J., Joseph Kwan, Richard I. Lindley, Martin S. Dennis, and Joanna M. Wardlaw. “Distinguishing between Stroke and Mimic at the Bedside: The Brain Attack Study.” Stroke; a Journal of Cerebral Circulation 37, no. 3 (March 2006): 769–75.
14. Nor, Azlisham Mohd, John Davis, Bas Sen, Dean Shipsey, Stephen J. Louw, Alexander G. Dyker, Michelle Davis, and Gary A. Ford. “The Recognition of Stroke in the Emergency Room (ROSIER) Scale: Development and Validation of a Stroke Recognition Instrument.” Lancet Neurology 4, no. 11 (November 2005): 727–34.
References
15. Rivner, M. H., T. R. Swift, and K. Malik. “Influence of Age and Height on Nerve Conduction.” Muscle & Nerve 24, no. 9 (September 2001): 1134–41.
16. Forsblom, C. M., T. Sane, P. H. Groop, K. J. Tötterman, M. Kallio, C. Saloranta, L. Laasonen, et al. “Risk Factors for Mortality in Type II (non-Insulin-Dependent) Diabetes: Evidence of a Role for Neuropathy and a Protective Effect of HLA-DR4.” Diabetologia 41, no. 11 (November 1998): 1253–62
17. Vinik, A. I., and T. Erbas. “Recognizing and Treating Diabetic Autonomic Neuropathy.” Cleveland Clinic Journal of Medicine 68, no. 11 (November 2001): 928–30, 932, 934–44.
18. Vinik, Aaron I, Tomris Erbas, and Carolina M Casellini. “Diabetic Cardiac Autonomic Neuropathy, Inflammation and Cardiovascular Disease.” Journal of Diabetes Investigation 4, no. 1 (January 29, 2013): 4–18.
19. Magge, Suresh N., Matthew D. Smyth, Lance S. Governale, Liliana Goumnerova, Joseph Madsen, Becca Munro, Stephen V. Nalbach, Mark R. Proctor, R. Michael Scott, and Edward R. Smith. “Idiopathic Syrinx in the Pediatric Population: A Combined Center Experience.” Journal of Neurosurgery. Pediatrics 7, no. 1 (January 2011): 30–36.
20. Holly, Langston T., and Ulrich Batzdorf. “Slitlike Syrinx Cavities: A Persistent Central Canal.” Journal of Neurosurgery 97, no. 2 Suppl (September 2002): 161–65.
21. Marzuillo, Pierluigi, Anna Grandone, Ruggero Coppola, Domenico Cozzolino, Adalgisa Festa, Federica Messa, Caterina Luongo, Emanuele Miraglia Del Giudice, and Laura Perrone. “Novel cAMP Binding Protein-BP (CREBBP) Mutation in a Girl with Rubinstein-Taybi Syndrome, GH Deficiency, Arnold Chiari Malformation and Pituitary Hypoplasia.” BMC Medical Genetics 14 (2013): 28.
22. Meadows, Jeffery, Michael Kraut, Michael Guarnieri, Raymond I. Haroun, and Benjamin S. Carson. “Asymptomatic Chiari Type I Malformations Identified on Magnetic Resonance Imaging.” Journal of Neurosurgery 92, no. 6 (June 1, 2000): 920–26. doi:10.3171/jns.2000.92.6.0920.
References
23. Elster, A. D., and M. Y. Chen. “Chiari I Malformations: Clinical and Radiologic Reappraisal.” Radiology 183, no. 2 (May 1992): 347–53. doi:10.1148/radiology.183.2.1561334.
24. Stevenson, Kevin L. “Chiari Type II Malformation: Past, Present, and Future.” Neurosurgical Focus 16, no. 2 (February 15, 2004): E5.
25. Gupta, Mudit, Rashmi Gupta, and Ashu Seith. “Persistent Primitive Hypoglossal Artery Associated with Chiari II Malformation: Diagnosis and Clinical Implications.” The Indian Journal of Radiology & Imaging 20, no. 4 (November 2010): 258–60.
26. Suchowersky, O., S. Reich, J. Perlmutter, T. Zesiewicz, G. Gronseth, W. J. Weiner, and Quality Standards Subcommittee of the American Academy of Neurology. “Practice Parameter: Diagnosis and Prognosis of New Onset Parkinson Disease (an Evidence-Based Review): Report of the Quality Standards Subcommittee of the American Academy of Neurology.” Neurology 66, no. 7 (April 11, 2006): 968–75.
27. de Lau LL, Schipper CA, Hofman A, Koudstaal PJ, and Breteler MB. “Prognosis of Parkinson Disease: Risk of Dementia and Mortality: The Rotterdam Study.” Archives of Neurology 62, no. 8 (August 1, 2005): 1265–69.
28. Hely, Mariese A., John G. L. Morris, Wayne G. J. Reid, and Robert Trafficante. “Sydney Multicenter Study of Parkinson’s Disease: Non-L-Dopa-Responsive Problems Dominate at 15 Years.” Movement Disorders: Official Journal of the Movement Disorder Society 20, no. 2 (February 2005): 190–99.
29. Marras, C., M. P. McDermott, P. A. Rochon, C. M. Tanner, G. Naglie, A. Rudolph, A. E. Lang, and Parkinson Study Group. “Survival in Parkinson Disease: Thirteen-Year Follow-up of the DATATOP Cohort.” Neurology 64, no. 1 (January 11, 2005): 87–93.
30. Willis, Allison W., Mario Schootman, Nathan Kung, Bradley A. Evanoff, Joel. S. Perlmutter, and Brad A. Racette. “Predictors of Survival in Parkinson Disease.” Archives of Neurology 69, no. 5 (May 2012): 601–7. doi:10.1001/archneurol.2011.2370.
References
31. Seymour N. Mortality after temporal lobe epilepsy surgery. Epilepsia. 2012 Feb;53(2):267-7132. Sperling MR, Mortality after epilepsy surgery. Epilepsia. 2005;46 Suppl 11:49-53. 33. Salanova V, Markand O, Worth R. Temporal lobe epilepsy surgery: outcome, complications, and late mortality
rate in 215 patients. Epilepsia. 2002 Feb;43(2):170-4. M Baraitser. Relevance of a family history of seizures. Arch Dis Child. 1983 June; 58(6): 404–405.
34. Harden CL. Practice parameter update: management issues for women with epilepsy--focus on pregnancy (an evidence-based review): obstetrical complications and change in seizure frequency. Report of the Quality Standards Subcommittee. Neurology. 2009 Jul 14;73(2):126-32Tomson T, Battino D, Bonizzoni E et al. Collaborative EURAP Study Group 2004. EURAP: an international registry of antiepileptic drugs and pregnancy. Epilepsia 45(11), 1463-1464 (2004).
35. Vestergaard M. Death in children with febrile seizures: a population-based cohort study. Lancet. 2008 Aug 9;372(9637):457-63.
References


















