General Data J.O 6 years old Male Tondo Manila Mother, good CC: Fever.
37
-
Upload
roberta-erika-norris -
Category
Documents
-
view
219 -
download
1
Transcript of General Data J.O 6 years old Male Tondo Manila Mother, good CC: Fever.

General Data
J.O 6 years old Male Tondo Manila Mother, good
CC: Fever
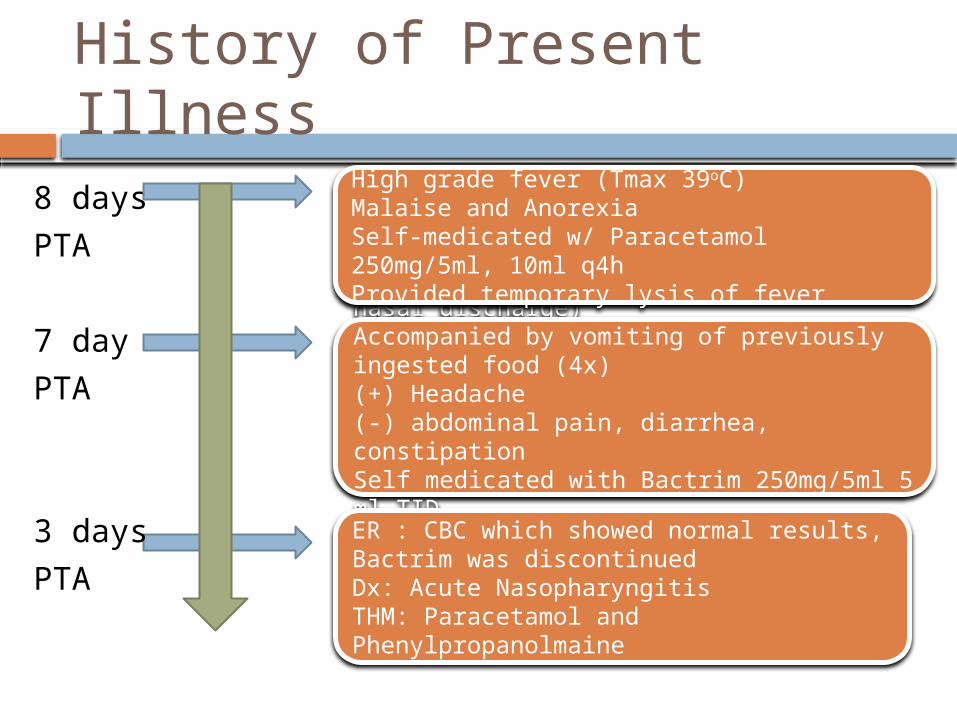
History of Present Illness
8 days
PTA
7 day
PTA
3 days
PTA
Developed prod cough & colds (clear nasal discharge)Accompanied by vomiting of previously ingested food (4x)(+) Headache(-) abdominal pain, diarrhea, constipationSelf medicated with Bactrim 250mg/5ml 5 ml TIDNo relief except vomitingER : CBC which showed normal results, Bactrim was discontinuedDx: Acute NasopharyngitisTHM: Paracetamol and Phenylpropanolmaine
High grade fever (Tmax 39oC)Malaise and AnorexiaSelf-medicated w/ Paracetamol 250mg/5ml, 10ml q4hProvided temporary lysis of fever

History of Present Illness
8 days
PTA
7 day
PTA
3 days
PTA
Few hours
PTA
Developed prod cough & colds (clear nasal discharge)Accompanied by vomiting of previously ingested food (4x)(+) Headache(-) abdominal pain, diarrhea, constipationSelf medicated with Bactrim 250mg/5ml 5 ml TIDNo relief except vomitingER : CBC which showed normal results, Bactrim was discontinuedDx: Acute NasopharyngitisTHM: Paracetamol and Phenylpropanolmaine
High grade fever (Tmax 39oC)Malaise and AnorexiaSelf-medicated w/ Paracetamol 250mg/5ml, 10ml q4hProvided temporary lysis of fever
Periumbilical painFollow up at OPD
Review of Systems
(-) weight changes (-) exanthem, (-) jaundice (-) hematuria (-) constipation or diarrhea (-) polydipsia, polyphagia, polyuria (-) gum bleeding (-) weakness
Immunizations
BCG HepB 1, 2, 3 DTP 1, 2, 3 OPV 1, 2, 3 Measles, Varicella

Past Medical History
Amebiasis at 2 years old, given Metronidazole
No previous confinements No previous illnesses

Family Profile
Member Age Sex Educational Attainment
Occupation
Health status
JF 31 M college bookkeeper
healthy
JO 26 F secretariat
housewife healthy

Family History
(+) HPN (-) respiratory, endocrine, hematologic,
infectious diseases

Developmental Milestones
At par with age Draws a person with hands and clothes Knows morning and afternoon Knows right and left sides Copies a diamond Has chums composed mainly of male
friends Grades high 70’s – low 80’s Enjoys sports

Physical Examination
Alert, ill-looking, Well-nourished, Well-hydrated BP 100/60 HR 120 RR 28 T 39.1 Ht: 75 cm Wt:
29.5kg Warm moist skin, (+) flushed skin, (-) Tourniquet
test Normocephalic, atraumatic Pink palpebral conjunctivae, anicteric sclera, Septum midline, turinates not congested, (+)
watery nasal discharge, (-) alar flaring, no tragal tenderness, retained cerumen
Moist buccal mucosa, hyperemic PPW, tonsils hyperemic but not enlarged, (-) Palatal petechiae
Physical Examination
Supple neck, no anterior masses, no CLAD Symmetrical chest expansion, No retractions,
Clear breath sounds Adynamic precordium, apex beat at 4th LICS
MCL, (-) murmurs Globular abdomen, normoactive bowel
sounds, soft, (+) Epigastric tender, (-) masses, Liver and spleen non-palpable
Pulses full and equal, (-) edema or cyanosis NE: oriented to 3 spheres, CN I-XII intact, No
tremors, MMT 5/5, No sensory deficit, DTR ++, No meningeal signs, No Babinski
Presenting Manifestation
Look for a symptom, sign or laboratory finding.. Pathognomonic of a disease Pointing to an organ or part of an organ Pointing to a group of disease Mechanism is well understood Found in the least number of diseases
UST: Pedia (2009). Guideline for History Taking, PE and Diagnosis of Pediatric Patients. 2nd ed.
Fever+ Cough
+ Abdominal Pain
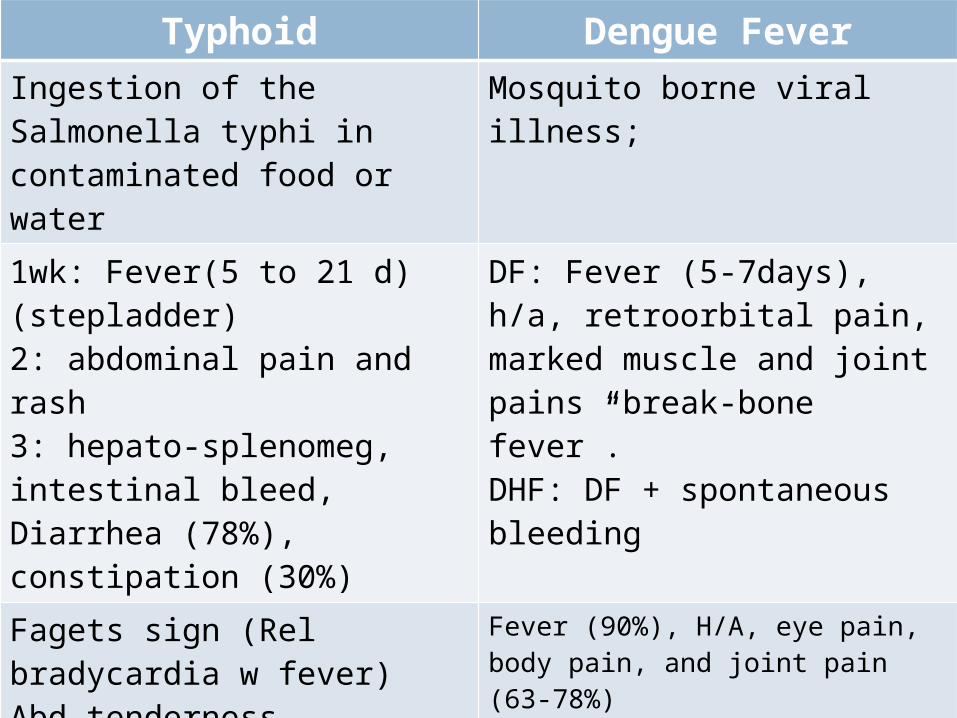
Typhoid Dengue FeverIngestion of the Salmonella typhi in contaminated food or water
Mosquito borne viral illness;
1wk: Fever(5 to 21 d) (stepladder)2: abdominal pain and rash3: hepato-splenomeg, intestinal bleed, Diarrhea (78%), constipation (30%)
DF: Fever (5-7days), h/a, retroorbital pain, marked muscle and joint pains “break-bone fever”.DHF: DF + spontaneous bleeding
Fagets sign (Rel bradycardia w fever)Abd tendernessHepatosplenomegaly
Fever (90%), H/A, eye pain, body pain, and joint pain (63-78%)Rash (50%)N/V (50%) Diarrhea (30%)Cough, sore throat and nasal congestion (1/3)
CBC: Anemia, leukopenia or cytosis, Elevated AminotranWidal TestStool CultureBone Marrow cul
Without full picture of classical DF in childrenGI and resp symptoms may predominate
ENTERIC FEVER
Enteric Fever
Aka typhoid fever Systemic febrile illness that is most
commonly caused by Salmonella typhi less frequent causes are S. paratyphi A, S.
paratyphi B (S. schottmuelleri), and S. paratyphi C (Salmonella hirschfeldii).
Non-typhoidal Salmonellae (S. enteritidis and S. typhimurium)
classically present with sustained fever, abdominal tenderness, and hepatosplenomegaly
Uptodate Medical Desktop 17.1

Epidemiology
Most often foodborne Paratyphoid fever: exposures outside the home
purchase of food from street vendors) Typhoid fever: exposure within the household
Sharing utensils, presence of a patient with typhoid, lack of soap or adequate toilet facilities
Most px to hospitals with typhoid fever are children or young adults from 5-25 years old. <5 years old nonspecific illness that is not
recognized clinically as typhoid.
Uptodate Medical Desktop 17.1Parry, C.; Dougan G; White N; Farrar J. (2002) Typhoid Fever. N Engl J Med, Vol.
347, No. 22
Microorganism
Member of the family Enterobacteriaciae Lipopolysaccharide antigens O9 and
O12, protein flagellar antigen Hd, and Polysaccharide capsule Vi (90%)
protective effect against the bactericidal action of the serum of infected patients.
Basis for one of the commercially available vaccines
Uptodate Medical Desktop 17.1Parry, C.; Dougan G; White N; Farrar J. (2002) Typhoid Fever. N Engl J Med, Vol.
347, No. 22
Pathogenesis
Ingestion of contaminated food or water Infectious dose:103 – 105 CFU
Gastrointestinal infection: survive the gastric acid barrier* adhere and invade the small intestines M cell- epithelial cells overlying the Payer’s
Patches Direct penetration into the epithelial cells
S. typhi in the lamina propria recruitment of mononuclear cells and macrophage ingested but survive
Parry, C.; Dougan G; White N; Farrar J. (2002) Typhoid Fever. N Engl J Med, Vol. 347, No. 22
Pathogenesis
Incubation phase: Some remain in SI lymphoid tissues, others drain into mesenteric lymph nodes reticuloendothelial cells of the liver and spleen Incubation period ranges 3-60 days (usually 7-14d) Survive and multiply in the mononuclear phagocytic
cells of the lymphoid follicles, liver and spleen. Bacteremic phase: bacteria released from
sequestered intracellular habitat into bloodstream induce systemic and local humoral and cellular immune responses MC sites of secondary infection: liver, spleen, bone
marrow, gallbladder and payer’s patch of the terminal ileum
Parry, C.; Dougan G; White N; Farrar J. (2002) Typhoid Fever. N Engl J Med, Vol. 347, No. 22
Pathogenesis
Chronic carrier (4%): asymptomatic carriers after acute infection persistence of Salmonellae in stool or urine for
more than one year. immunologic equilibrium- virulent bacteria
persist without causing disease but cannot be eliminated women Persons with biliary abnormalities such as gallstones Defect in the urinary tract (eg, urolithiasis, prostatic
hyperplasia) or concurrent bladder infection with Schistosoma

Clinical Manifestation
Febrile illness for 7-14d after ingestion of the causative microorganism in contaminated food or water ONSET: fever and malaise Presentation (end of the 1st week): fever,
influenza-like symptoms with chills (although rigors are rare), a dull frontal headache, malaise, anorexia, nausea, poorly localize abdominal discomfort, a dry cough, and myalgia, but with few physical signs
Relative bradycardia or pulse-temperature dissociation – not consistent
Parry, C.; Dougan G; White N; Farrar J. (2002) Typhoid Fever. N Engl J Med, Vol. 347, No. 22
Clinical Manifestation
Diarrhea – more common in children Constipation – more common in adults Bronchitic cough – common in the early stage of
the illness Rose spots on the chest, abdomen and back Arthalgia and myalgia Bacteremic seeding focal extra-intestinal
complications of the central nervous system, hepatobiliary, cardiovascular, respiratory, genitourinary, and musculoskeletal systems (uncommon)
Uptodate Medical Desktop 17.1

Clinical Manifestation
Classic Manifestation of untreated individuals: First week of illness — rising ("stepwise")
fever and bacteremia Second week — abdominal pain and rash
(rose spots, which are faint salmon colored macules on the trunk and abdomen)
Third week — hepatosplenomegaly, intestinal bleeding and perforation, related to ileocecal lymphatic hyperplasia of the Peyer's patches, may occur with secondary bacteremia and peritonitis.Uptodate Medical Desktop 17.1

Clinical and Laboratory Presentation of Typhoid Fever
Yaramis A; Yilchim I, Katar S; Ozbek M, Yakjin, Tas A, Hosoglu SInternational Pediatrics/Vol. 16/No. 4/2001 227
typical symptoms in adults such as cough, headache and constipation were uncommon, tending to occur in older children.
Common clinical signs of typhoid fever in adults such as relative bradycardia and rose spots were seldom documented
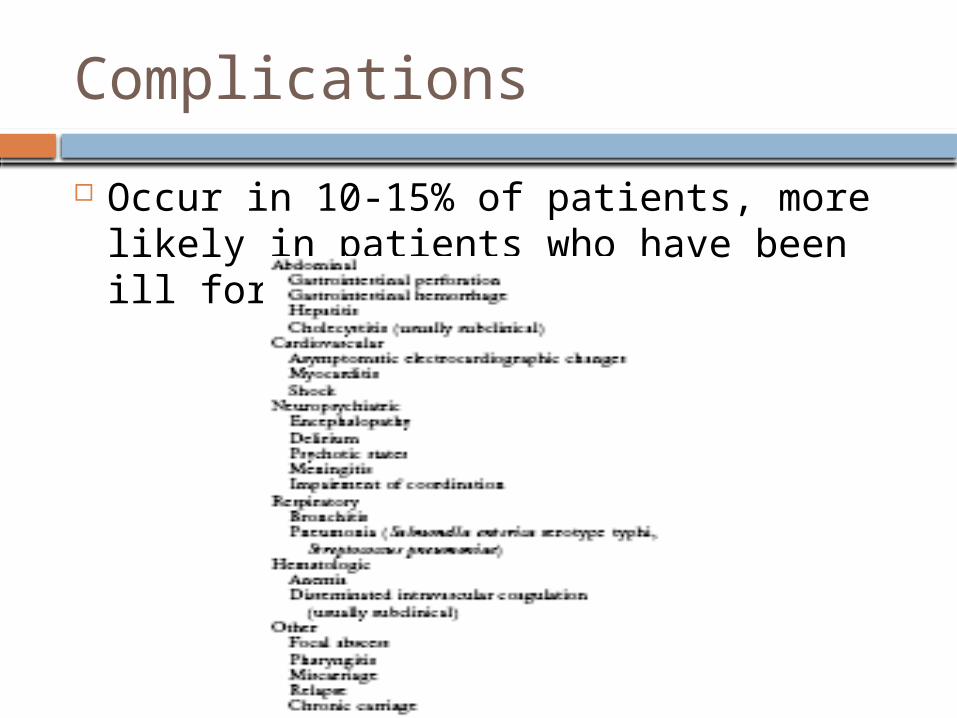
Complications
Occur in 10-15% of patients, more likely in patients who have been ill for >2 weeks.

Complications
GI bleeding, (MC): 10% Erosion of necrotic Payer’s patch through the wall
of the enteric vessel Intestinal perforation: 1-2%
Most serious comp Manifest as acute abd or increasing abdominal
pain, rising pulse, and hypotension. Typhoid encelopathy:
Often accompanies shock Commonly apathetic although arousable. Can be severely agitated, delirious, or obtunded.

Diagnosis
Diagnosis
Isolation of the microorganism Stool culture (30-40%)
often negative by the time systemic symptoms arise Blood culture (60-80%)
higher in the first week Reduced by prior use in antibiotics
Bone marrow culture (80-95%) especially useful if antibiotics therapy have already
been started Urine, rose spots and duodenal content (string
capsule) culture
Parry, C.; Dougan G; White N; Farrar J. (2002) Typhoid Fever. N Engl J Med, Vol. 347, No. 22

Diagnosis
Serologic Test: detects agglutinating antibodies to O and H antigens of S. typhi Controversial High false positive because shares antigens with
other salmonella serotypes and cross-reacting epitopes with other Enterobacteriaceae.
Laboratory Findings Anemia Leukopenia Leukocytosis (more common in children) Aminotransaminases elevated
Uptodate Medical Desktop 17.1

Mean total WBC was 7.3x103/mm3. Shift to left was found in 78%
38% anemic (Hb<12/dl), 10% thrombocytopenic (<105/mm3)
Elevated serum ALT and AST in 32% Antibiotic resistance were found as follows: (>50) levels were observed in 100 (32%)
ampicillin(17%); trimethoprim-sulfamethoxazole (5%); Ceftriaxone (4%); sulbactam-ampicillin (6%). No resistance to quinolones and chloramphenicol.
Clinical and Laboratory Presentation of Typhoid Fever
Yaramis A; Yilchim I, Katar S; Ozbek M, Yakjin, Tas A, Hosoglu SInternational Pediatrics/Vol. 16/No. 4/2001 227

Diagnosis
Confirmed Case
•Fever (T>38oC) > 3 days•Laboratory confirmed positive culture (blood, bone marrow, bowel fluid)
Probable Case
•Fever (T>38oC) > 3 days•(+) Serodiagnosis or antigen detection test•w/o isolation
Chronic Carrier
•Excretion of S. typhi in stools or urine >1 year after typhoid fever

Treatment

Treatment
60-90% are managed at home with antibiotics and bed rest.
Fluoroquinolones are the most effective drugs for the treatment of typhoid fever more rapidly effective and are associated with lower rates of
stool carriage than the traditional first-line drugs (chloramphenicol and trimethoprim–sulfamethoxazole).
Average fever-clearance time is less than four days, and the cure rates exceed 96 percent
no evidence of bone or joint toxicity, tendon rupture, or, in long-term followup, impairment of growth
Used at the maximal possible dose for a minimum of 10 to 14 days, and the patients should be carefully followed to determine whether they are excreting S. enterica serotype typhi in their feces
Parry, C.; Dougan G; White N; Farrar J. (2002) Typhoid Fever. N Engl J Med, Vol. 347, No. 22

Treatment
2nd line: 3rd gen cephalosporins (ceftriaxone, cefixime, cefotaxime, and cefoperazone) and azithromycin are also effective drugs for typhoid.
3rd line: Aztreonam and Imipenem
Chloramphenicol, amoxicillin, and trimethoprim–sulfamethoxazole remain appropriate for the treatment in areas of the world where the bacterium is still fully susceptible to these drugs and where the fluoroquinolones are not available or affordable. inexpensive, widely available, and rarely associated
with side effects.Parry, C.; Dougan G; White N; Farrar J. (2002) Typhoid Fever. N Engl J Med, Vol.
347, No. 22

Treatment

Treatment