GEMNet: Management of Suspected Scaphoid Fractures in the ...
32
Guidelines in Emergency Medicine Network - GEMNet Guideline for the Management of Suspected Scaphoid Fractures in the Emergency Department The College of Emergency Medicine September 2013 #6
Transcript of GEMNet: Management of Suspected Scaphoid Fractures in the ...
Guidelines in Emergency Medicine Network - GEMNet
Guideline for the
Management of Suspected
Scaphoid Fractures in the
Emergency Department
The College of Emergency Medicine
September
2013
#6

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 2

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 3
About this guideline
Running title: GEMNet guideline: Management of Suspected
Scaphoid Fractures in the Emergency Department
Version Control: First published Sept 2013
Authors: Emma Machin
Julian Blackham
Jonathan Benger
Main affiliation: Emergency Department, Bristol Royal Infirmary,
Upper Maudlin Street, Bristol, BS2 8HW
Corresponding author and address: Professor Jonathan Benger, Emergency
Department, Bristol Royal Infirmary, Upper Maudlin
Street, Bristol, BS2 8HW
E-mail: [email protected]
Published September 2013
Review September 2018

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 4
Contents
1. Executive summary p5
2. Introduction p6
3. Topic background p6
4. Scope p8
5. Methodology p8
6. Summary of recommendations p10
7. Detailed findings p12
7.1 Clinical examination p12
7.2 Imaging p14
7.3 Immobilisation p23
7.4 Follow up p24
7.5 Scaphoid fractures in children p24
8. Evidence-based flowchart p25
References p26

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 5
1. Executive summary
• The Guidelines in Emergency Medicine Network (GEMNet) exists to promote best
medical practice in a range of conditions presenting to Emergency Departments
(EDs) in the UK.
• This guideline presents a summary of the best available evidence to guide the
management of adult patients who present to the ED with a suspected scaphoid
fracture.
• The guideline has been developed following discussion amongst Emergency
Physicians to decide which topics would benefit from the development of clinical
guidelines.
• The guideline is intended for use in the ED by Emergency Physicians and is based on a
review of the best available evidence at the time of writing.
• There is no one examination finding or combination of examination findings that can
reliably exclude a scaphoid fracture. However it would be reasonable to consider this
possibility if the patient has sustained trauma compatible with scaphoid fracture and
has anatomical snuffbox or scaphoid tubercle tenderness. Such patients should
usually undergo imaging.
• Plain radiographs remain a useful first line imaging test for scaphoid fracture, however
they are insufficiently sensitive to exclude a fracture. Repeat imaging between 2 and
6 weeks increases the sensitivity, but is still not high enough to exclude a fracture.
• On the basis of currently available evidence, dual energy X-Ray absorptiometry,
macroradiography, ultrasound and intrasound vibration cannot be recommended as
useful imaging tests for a suspected scaphoid fracture.
• Bone scanning has a very high sensitivity; however it also produces a number of false
positives when compared with delayed plain radiographs. There have been few
studies of CT, but those performed demonstrate a high sensitivity for scaphoid fracture.
• MRI for patients with ongoing clinical suspicion of scaphoid fracture despite normal
initial radiographs has a very high sensitivity for detecting scaphoid fracture and other
injuries to the wrist, and is the second-line investigation of choice.
• There are no studies comparing wrist splints with or without thumb extensions to a
plaster cast for the definitive management of scaphoid fractures. Based on the
available evidence there is no benefit of a scaphoid cast over a standard “Colles”
cast.
• There is no guidance in the published literature on follow up per se. The period of
follow up is dependent on the chosen imaging modality, since once a fracture has
been excluded further follow up is not required.
• These recommendations are summarised in a clinical decision support guideline that
has been presented as a simple algorithm.
• The intention is for every GEMNet guideline to be updated and reviewed as further
evidence becomes available. The formal revision date has been set at 5 years from
publication, though the guideline is subject to continuous informal review.
GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 6
2. Introduction
2.1 Responsibility for development
This document has been developed in response to a perceived need to improve and
standardise clinical care in patients with a suspected fracture of the scaphoid bone. The
intention is to distil the best available evidence into practical advice for clinicians working
in the Emergency Department. The information is presented in the form of clinical decision
support guidelines, readily available for use in the ED.
Abbreviations used in this guideline:
ASB - Anatomic snuff box
CT – Computed tomography
ED – Emergency Department
LC – Longitudinal compression
MRI – Magnetic resonance imaging
SC – Scaphoid compression
ST - Scaphoid tubercle
3. Topic background
Scaphoid fractures are the commonest fracture of the carpal bones, comprising almost
90% of carpal fractures. They are most common in men aged between 15 and 30 years.
Middle third Scaphoid fractures usually result from extreme dorsiflexion of the wrist with
pressure over the radial side of the palm – most commonly due to a fall on an
outstretched hand. Scaphoid fractures can also be caused by a direct blow to the palm
of the hand; historically this was a “crank handle” injury, but it can also be caused by
holding a car steering wheel during a motor vehicle collision.
Generations of medical students have been told that tenderness in the anatomical snuff
box is the cardinal sign of a scaphoid fracture, and that missed scaphoid fractures are
common. The cutaneous branch of the radial nerve runs directly over the anatomical
snuff box, which means that discomfort on firm palpation of this area is common even in
the absence of injury.[1]
The published incidence of false negative initial radiographs is between 5 and 48%.[2]
Early diagnosis is commonly held to be necessary in order to avoid complications such as
non-union, pseudoarthrosis and avascular necrosis. That said, as long ago as 1969
McLaughlin and colleagues noted that fractures of the scaphoid that were not visible on

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 7
the initial radiographs were ‘class A fractures’: undisplaced fractures that are little more
than a split in the articular cartilage.[3] They stated that ‘it was abundantly clear that,
barring a reinjury, the fractures in this group would heal under almost any circumstance’.
The incidence of delayed union increases from 9% in patients where treatment is instituted
within days of fracture to 36% if treatment is delayed beyond 4 weeks. Similarly, the non-
union rate rises from 5% to 45%.[4]
A number of authors have questioned the diagnosis of ‘clinically fractured’ scaphoid.
Duncan et al. undertook a study of patients with suspected or proven scaphoid fractures
over one year in a single hospital.[5] Of the 156 patients, 42 were initially felt to have
scaphoid fractures, and 108 to have a clinical scaphoid fracture by the “casualty officer”.
They were unable to demonstrate a case of a scaphoid fracture becoming visible
radiologically after a period of observation. Leslie noted that of 222 fresh scaphoid
fractures, 98% were visible on initial radiographs, but 3% of these were missed by “casualty
officers”.[6] The remaining 2% were not visible until 2 weeks, however these were
incomplete fractures. As noted above, McLaughlin felt that incomplete fractures of this
type were stable fractures that required no immobilization.
There is great variation between hospitals in the initial management of suspected
scaphoid fractures, even amongst neighbouring hospitals.[7] In an international study of
hospital management of suspected scaphoid fractures, there was no agreement on initial
imaging, follow up period or the type of repeat imaging for ongoing clinical suspicion. The
most common second line investigation was MRI (31/105).[8]
The immobilisation of a suspected scaphoid fracture entails significant inconvenience for
patents; in many cases leaving them unable to work for prolonged periods of time (an
average of 21 days in one study).[5]
Recent Royal College of Radiology guidelines recommend plain radiology followed by CT,
MRI or nuclear medicine, but with MRI as the recommended form of secondary
imaging.[9] The current American College of Radiology guidance recommends repeat
plain radiographs at 14 days or MRI if the original radiographs are normal, with CT as a an
alternative option if MRI contra-indicated.[10]
Dorsay and colleagues reviewed the published literature as part of a cost effectiveness
study to find the positive predictive value of clinical examination.[11] They found it ranged
from 13-69%, with a weighted average of 21%. This means that four out of five patients with
a clinically suspected Scaphoid fracture turn out not to have one. They went on to look at
the negative predictive value of normal initial radiographs and noted that the range was
50-80%, with a weighted average of 74%.

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 8
4. Scope
This guideline is intended for the management of patients aged over 8 years presenting to
the Emergency Department with suspected scaphoid fracture. Scaphoid fractures are
very rare in children under 8 years of age; alternative diagnoses should therefore be
considered in this patient group.
5. Methodology
MEDLINE 1966-05/11, EMBASE 1980-05/11, CINHAL 1981-05/11 and the Cochrane Library
were searched using the strategies described below to answer a number of “three part”
questions:
5.1 Clinical examination
In a [patient with suspected scaphoid fracture] which [clinical test] is most effective
in [diagnosing a scaphoid fracture] [12]
[(SCAPHOID BONE OR scaphoid.ti.ab) AND (FRACTURES, BONE/di) AND (PHYSICAL
EXAMINATION OR (clinical ADJ test).ti.ab) OR examin$.ti)]
5.2 Imaging
In a [patient with suspected scaphoid fracture] which [imaging strategy] is most
effective in [achieving the correct diagnosis]
[(SCAPHOID BONE OR scaphoid.ti.ab) AND (FRACTURES, BONE/di) AND
(DIAGNOSTIC IMAGING/ OR MAGNETIC RESONANCE IMAGING/ OR RADIONUCLIDE
IMAGING/ OR TECHNETIUM TC 99M MEDRONATE/ OR TECHNETIUM/ OR X-RAYS/ OR
ultrasound.ti,ab OR mri.ti,ab OR (magnet$ ADJ resonan$).ti,ab OR x-ray$.ti,ab OR
(bone AND scan).ti,ab OR scint$.ti,ab)]
5.3 Immobilisation
In a [patient with a clinically suspected scaphoid fracture] is [wrist immobilisation in
a splint] better than [wrist immobilisation in a cast] for [reducing complications from
occult fractures]
[(SCAPHOID BONE OR scaphoid.ti.ab)] AND [(CASTS, SURGICAL/ OR CALCIUM
SULFATE/ OR SPLINTS/) OR (plaster AND of AND paris).ti,ab OR splint$.ti,ab OR
IMMOBILIZATION/ OR immobilisation.ti,ab OR immobilization.ti,ab OR cast$.ti,ab]
AND [FRACTURES, BONE/]

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 9
5.3 Follow up
In a [patient with a clinically suspected scaphoid fracture] is [clinical follow up] or
[further imaging] best for [excluding occult fractures]
The duration of follow up was considered in the imaging section. It was noted that
the sensitivity and timing of clinical and radiological examination determines the
duration of follow up required.
Cochrane reviews
There was one relevant Cochrane review: “Diagnosing suspected scaphoid
fractures: a systematic review and meta-analysis”.[2]
Levels of evidence and grading of recommendations
Studies included in this guideline were graded for their level of evidence according to
accepted definitions.[13]
In summary:
Level 1 evidence is derived from well-designed randomised controlled trials (RCTs),
Level 2 evidence is derived from large cohort studies or poorly designed RCTs,
Level 3 evidence is derived from small cohort studies or case-control studies, and
Level 4 evidence is derived from experimental studies, case series or case studies.
The suffix ‘a’ implies that evidence at this level is from a systematic review or meta-
analysis, whereas the suffix ‘b’ implies that the evidence is from original research.
The recommendations made have been graded according to the level of evidence upon
which they are based:
Grade A: Based upon multiple level 1a or 1b papers.
Grade B: Based upon individual level 1a or 1b papers, or multiple level 2a or 2b papers.
Grade C: Based upon individual level 2a or 2b papers, or multiple level 3a or 3b papers.
Grade D: Based upon individual level 3a or 3b papers, or level 4 papers.
Grade E: Based upon consensus guidelines or studies of expert opinion.
GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 10
6. Summary of recommendations
6.1 Clinical examination
There is no one examination or combination of examinations that can reliably exclude a
scaphoid fracture. This is based on a number of small level 3 studies which limits the
reliability of the conclusions that can be drawn. The highest probability of fracture is in
patients with ASB and ST tenderness combined with pain on LC of the thumb (sensitivity
100%; specificity 74%). ASB or ST tenderness also has a reasonable specificity and
sensitivity.
It would be reasonable to consider the possibility of a scaphoid fracture if the patient has
ASB or ST tenderness as this will pick up patients in both the above groups. These patients
should undergo imaging. [Grade C]
6.2 Imaging
A problem with all published studies is the lack of a “gold standard” imaging modality
against which reliable comparisons can be made. Plain radiographs are a useful first line
imaging technique for scaphoid fracture; however they are insufficiently sensitive to
exclude a fracture. Repeat imaging at between 2 and 6 weeks increases the sensitivity,
but is still not high enough to exclude fracture.
Dual energy X-Ray absorptiometry and macroradiography are not sensitive or specific
enough to have a role in excluding scaphoid fractures. There have been a number of
small studies looking at the role of ultrasound and intrasound vibration in the diagnosis of
scaphoid fractures. There is great variation in the sensitivity and specificity of ultrasound,
and this modality cannot be recommended on the basis of currently available evidence.
[Grade C]
Bone scanning has a very high sensitivity (100% in most studies), however it produces a
number of false positives when compared with delayed plain radiographs. It also requires
intravenous radioisotope and multiple images over a 3 hour period which is inconvenient
for patients and represents a significant workload for radiology departments. [Grade C]
There have been few studies of CT, but those performed demonstrate a high sensitivity for
scaphoid fracture. [Grade C]
In comparison studies MRI performs similarly to CT and bone scan. MRI for patients with an
ongoing clinical suspicion of scaphoid fracture despite normal initial radiographs has a
very high sensitivity for detecting scaphoid fracture and other injuries to the wrist, and is
the second-line imaging investigation of choice. [Grade C]

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 11
6.3 Immobilisation
There are no studies comparing wrist splints with or without thumb extensions to a plaster
cast for the definitive management of scaphoid fractures. Based on the available
evidence:
• There is no benefit of a scaphoid cast over a standard “Colles” cast. [Grade C]
• Immobilising the wrist in up to 20 degrees extension is better than having the
wrist immobilised in flexion [Grade D]
• There may be some benefit to immobilising a scaphoid fracture in an above
elbow cast, but the two studies in this area do not agree.
6.4 Follow up
There is no useful guidance in the literature regarding the duration of patient follow up.
The period of follow up is dependent on the chosen imaging modality, since once a
fracture has been excluded (normal MRI, CT or bone scan) further follow up is not
required.

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 12
7. Detailed findings
1. Clinical Examination
The search strategy produced 21 unique results
2. Imaging
The search strategy produced 147 unique results
3. Immobilisation
The search strategy produced 173 unique results
4. Follow up
The search strategy produced no useful results
5. Scaphoid Fractures in Children
7.1 Clinical examination
Clinical suspicion of a fractured scaphoid leads to many patients being immobilised
unnecessarily,[14] with the incidence of occult fracture being reported as low as 1.3% and
a final diagnosis of soft tissue injury being made in 88.8% of patients. Knowledge of surface
anatomy of the carpal bones is often poor.[15]
Clinical examination can be useful, but any proposed clinical test should be easy to teach
and apply. Table 1, below, summarises 9 studies looking at commonly used clinical
examination findings. The sensitivity of clinical examination tests are usually high, but the
corresponding specificity poor, limiting their use in clinical practice.
Table 1: Clinical examination findings
Study
Patient group
Incidence (and
Gold standard
used)
ASB
tenderness ST tenderness
Axial loading
of thumb*
Other
examination
findings and
combinations
Freeland [16]
246 patients
presenting
over a 10
month period
with possible
scaphoid
fracture
30 patients
eventually
shown to have
a fracture
Sensitivity
= 90%
Specificity
= 40%
Sensitivity
= 87%
Specificity =
57%
- -
Parvizi et al
[17]
215 patients
presenting
within 24 hours
of injury with a
suspected
scaphoid
fracture.
56 patients had
proven
scaphoid
fractures on
initial or repeat
plain
radiographs or
radioisotope
bone scan
Sensitivity
=100%
Specificity
= 19%
Sensitivity
=100%
Specificity =
30%
Sensitivity
=100%
Specificity
= 48%
ASB, ST and LC
Sensitivity
=100%
Specificity =
74%
Esberger [18] 99 patients
with suspected
Scaphoid
fracture,
Initial x-rays
positive = 34
patients. 10
further fractures
found on
repeat x-ray or
bone scan at 2
weeks
- - Sensitivity
= 70%
Specificity
= 22%
-

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 13
Waizenegger
et al [19]
64 patients
with suspected
scaphoid
fracture
presenting
within 3 days
of injury
52 included
patients of
whom 23 had
confirmed
scaphoid
fractures and 29
in whom
scintigraphy
excluded a
scaphoid
fracture
Day 1/Day 14
Sensitivity
= 87%/65%
Specificity
= 38%/41%
- Day 1/Day 14
Sensitivity
= 48%/9%
Specificity
= 52%/76%
Pronation/ulnar
deviation –
Day1/Day14
Sensitivity
= 82%/57%
Specificity
= 17%/45%
Grover [20] 221 patients
with suspected
scaphoid
fracture
presenting
over a 6
month period
29 patients had
proven
fractures, plain
X-rays repeated
10 days if initial
films were
normal
Sensitivity
= 100%
Specificity
= 29%
Sensitivity
= 83%
Specificity
= 51%
Sensitivity
= 100%
Specificity
= 80%
Wrist diameter
- significantly
higher in
patients with a
fracture
(p<0.05) but no
cut-off value
given
Rhemrev et al
[21]
78 patients
with suspected
clinically
scaphoid
fracture
presenting
within 48 hours
of injury and
normal initial
plain
radiography
13 patients had
definite
scaphoid
fractures
following MRI
and bone
scintigraphy
assessment
- - - Supination
strength <10%
of
contralateral
side
Sensitivity =
85% Specificity
= 59%
Extension <50%
of
contralateral
side
Sensitivity =
85% Specificity
= 59%
Unay et al [22] 187 patients
with a
suspected
scaphoid
fracture
presenting to a
single hospital
over a 1-year
period.
Initial x-rays
positive = 89. Of
remaining 98
patients, 67 had
MRI, which
showed 12
additional
scaphoid
fractures.
- - Sensitivity
= 71%
Specificity
= 35%
Pain on
thumb/index
pinch
Sensitivity =
73%
Specificity =
75%
Pain during
pronation
Sensitivity =
79%
Specificity =
58%
Wilson et al
[23]
111 patients
with clinical
scaphoid injury
but normal
initial
radiographs
29 patients had
scaphoid
fractures
confirmed on
bone
scintigraphy
- - Sensitivity
= 70%
Specificity
= 22%
-
Evenski et al
[24]
104 children
referred to
orthopedics
with high
clinical
suspicion of
scaphoid
fracture but
normal initial X-
ray
31children had
radiographically
evident
scaphoid
fracture on
follow up x-ray
Sensitivity
= 100%
Specificity
= 9%
- - Volar scaphoid
tenderness OR
5.50
Pain with radial
deviation
OR 9.75
Pain with wrist
active range
of movement
OR 5.51
* Axial loading of thumb includes tests described as Scaphoid compression or longitudinal thumb compression or thumb
telescoping or thumb compression.
GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 14
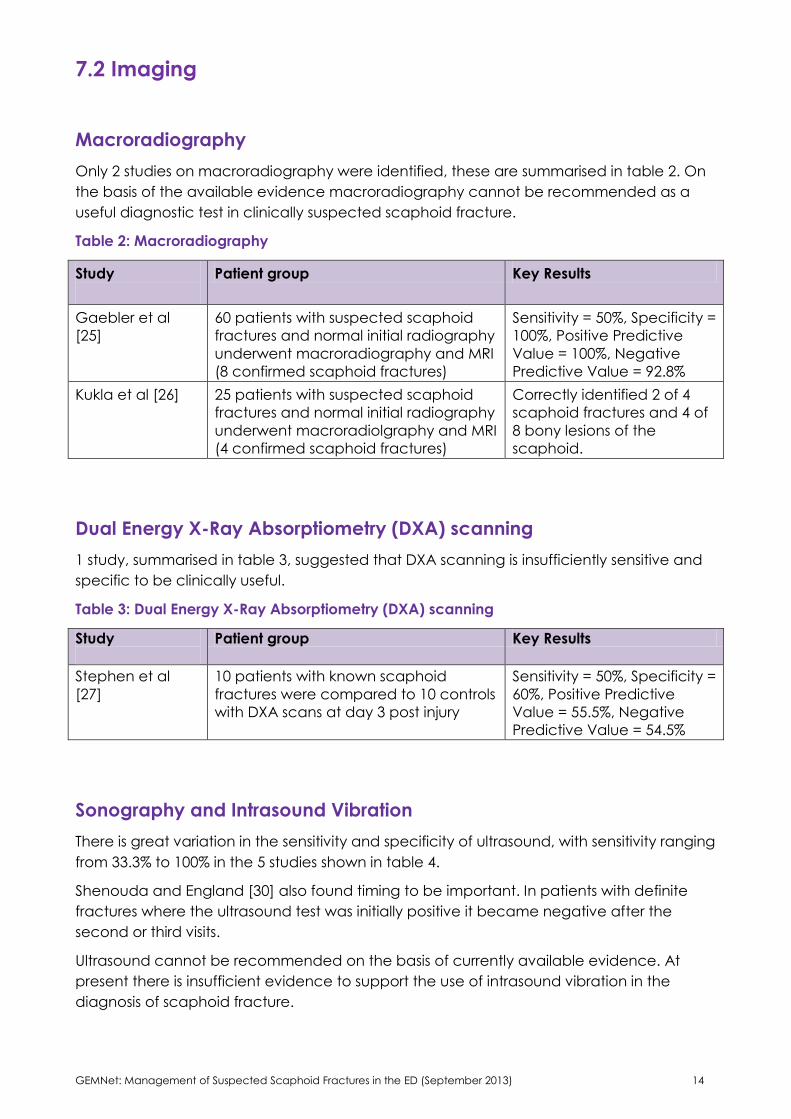
7.2 Imaging
Macroradiography
Only 2 studies on macroradiography were identified, these are summarised in table 2. On
the basis of the available evidence macroradiography cannot be recommended as a
useful diagnostic test in clinically suspected scaphoid fracture.
Table 2: Macroradiography
Study
Patient group Key Results
Gaebler et al
[25]
60 patients with suspected scaphoid
fractures and normal initial radiography
underwent macroradiography and MRI
(8 confirmed scaphoid fractures)
Sensitivity = 50%, Specificity =
100%, Positive Predictive
Value = 100%, Negative
Predictive Value = 92.8%
Kukla et al [26] 25 patients with suspected scaphoid
fractures and normal initial radiography
underwent macroradiolgraphy and MRI
(4 confirmed scaphoid fractures)
Correctly identified 2 of 4
scaphoid fractures and 4 of
8 bony lesions of the
scaphoid.
Dual Energy X-Ray Absorptiometry (DXA) scanning
1 study, summarised in table 3, suggested that DXA scanning is insufficiently sensitive and
specific to be clinically useful.
Table 3: Dual Energy X-Ray Absorptiometry (DXA) scanning
Study
Patient group Key Results
Stephen et al
[27]
10 patients with known scaphoid
fractures were compared to 10 controls
with DXA scans at day 3 post injury
Sensitivity = 50%, Specificity =
60%, Positive Predictive
Value = 55.5%, Negative
Predictive Value = 54.5%
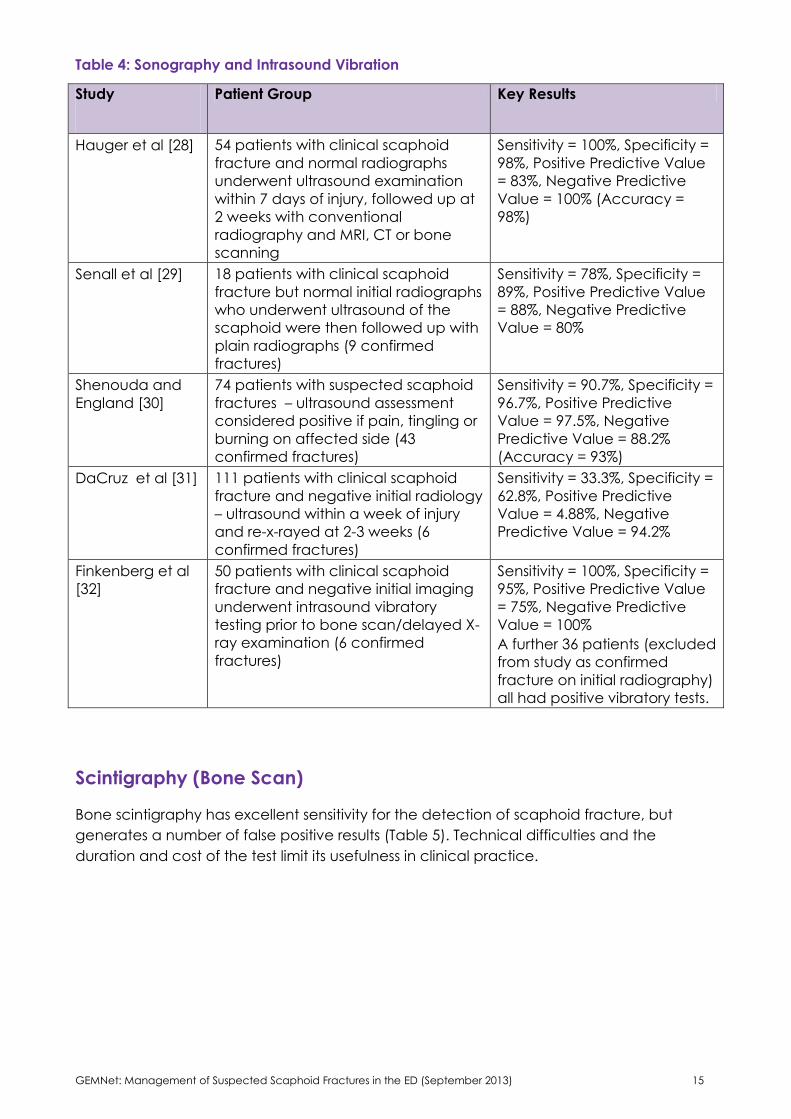
Sonography and Intrasound Vibration
There is great variation in the sensitivity and specificity of ultrasound, with sensitivity ranging
from 33.3% to 100% in the 5 studies shown in table 4.
Shenouda and England [30] also found timing to be important. In patients with definite
fractures where the ultrasound test was initially positive it became negative after the
second or third visits.
Ultrasound cannot be recommended on the basis of currently available evidence. At
present there is insufficient evidence to support the use of intrasound vibration in the
diagnosis of scaphoid fracture.
GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 15
Table 4: Sonography and Intrasound Vibration
Study
Patient Group Key Results
Hauger et al [28] 54 patients with clinical scaphoid
fracture and normal radiographs
underwent ultrasound examination
within 7 days of injury, followed up at
2 weeks with conventional
radiography and MRI, CT or bone
scanning
Sensitivity = 100%, Specificity =
98%, Positive Predictive Value
= 83%, Negative Predictive
Value = 100% (Accuracy =
98%)
Senall et al [29] 18 patients with clinical scaphoid
fracture but normal initial radiographs
who underwent ultrasound of the
scaphoid were then followed up with
plain radiographs (9 confirmed
fractures)
Sensitivity = 78%, Specificity =
89%, Positive Predictive Value
= 88%, Negative Predictive
Value = 80%
Shenouda and
England [30]
74 patients with suspected scaphoid
fractures – ultrasound assessment
considered positive if pain, tingling or
burning on affected side (43
confirmed fractures)
Sensitivity = 90.7%, Specificity =
96.7%, Positive Predictive
Value = 97.5%, Negative
Predictive Value = 88.2%
(Accuracy = 93%)
DaCruz et al [31] 111 patients with clinical scaphoid
fracture and negative initial radiology
– ultrasound within a week of injury
and re-x-rayed at 2-3 weeks (6
confirmed fractures)
Sensitivity = 33.3%, Specificity =
62.8%, Positive Predictive
Value = 4.88%, Negative
Predictive Value = 94.2%
Finkenberg et al
[32]
50 patients with clinical scaphoid
fracture and negative initial imaging
underwent intrasound vibratory
testing prior to bone scan/delayed X-
ray examination (6 confirmed
fractures)
Sensitivity = 100%, Specificity =
95%, Positive Predictive Value
= 75%, Negative Predictive
Value = 100%
A further 36 patients (excluded
from study as confirmed
fracture on initial radiography)
all had positive vibratory tests.
Scintigraphy (Bone Scan)
Bone scintigraphy has excellent sensitivity for the detection of scaphoid fracture, but
generates a number of false positive results (Table 5). Technical difficulties and the
duration and cost of the test limit its usefulness in clinical practice.

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 16
Table 5 Scintigraphy/Bone scanning
Study
Patient group Key Results
Stordahl et al
[33]
28 patients with clinically
suspected scaphoid fracture
and normal initial radiography
who underwent bone scanning
at 2 weeks post injury and
repeat x-rays at 2 and 6 weeks.
Sensitivity = 100%, Specificity = 57.89%,
Positive Predictive Value = 52.9%,
Negative Predictive Value = 100%
N.B.: 2 patients who were excluded as
had confirmed scaphoid fractures on
initial imaging both had positive bone
scans.
Waizenegger
et al [34]
84 patients with clinically
suspected scaphoid fracture
and normal initial radiology who
underwent bone scanning and
repeat radiography +/- CT
scanning (7 confirmed scaphoid
fractures)
Sensitivity = 100%, Specificity = 85%,
Positive Predictive Value = 50%,
Negative Predictive Value = 100%
N.B.: 25 patients had increased uptake
in areas of the wrist other than the
scaphoid
Akdemir et al
[35]
32 patients with suspected
carpel injury and normal
radiology underwent bone
scintigraphy at 2 weeks post
injury. (8 confirmed scaphoid
fractures)
Sensitivity = 100%, Specificity = 85%,
Positive Predictive Value = 50%,
Negative Predictive Value = 100%
N.B.: 12 patients had fractures of
bones other than the scaphoid, and
all had positive bone scans
Young et al
[36]
23 patients with suspected
scaphoid fracture and normal
initial radiology who had bone
scanning at 10-14 days post
injury and repeat radiology at 3
weeks (3 confirmed fractures)
Sensitivity = 100%, Specificity = 85%,
Positive Predictive Value = 50%,
Negative Predictive Value = 100%
N.B.: 2 patients had ‘mildly positive’
bone scans which were treated as
‘normal’ with under 3 weeks
immobilization – neither patient had a
confirmed fracture.
Jorgensen et
al [37]
50 patients with suspected
scaphoid fracture who had
plain radiographs on the day of
presentation, x-ray and bone
scan on day 10 and x-ray on
day 20 (22 confirmed fractures)
Sensitivity = 100%, Specificity = 37.04%,
Positive Predictive Value = 52.78%,
Negative Predictive Value = 100%
N.B.: 4 patients had uninterpretable
bone scans due to wet plasters and 10
of the positive bone scan patients had
fractures of bones other than the
scaphoid.
Wilson et al
[23]
111 patients with suspected
scaphoid injury but normal initial
radiology underwent bone
scanning. The first 42 patients
were re-x-rayed at 10 days.
Bone scanning used as rule out test –
those with negative bone scans had
immobilization removed and no
missed fractures were reported. 29
patients had bone scans consistent
with scaphoid fracture – 2 of whom
had positive x-rays at day 10 –
however only 42 of the 111 patients
underwent x-rays at day 10.
Bayer et al
[38]
40 patients with suspected
scaphoid fracture and initially
normal radiographs had bone
scanning at 14 days post injury
(8 confirmed scaphoid
fractures)
Sensitivity = 100%, Specificity = 85%,
Positive Predictive Value = 50%,
Negative Predictive Value = 100%
N.B.: 10 patients with positive bone
scans had wrist fractures affecting
bones other than the scaphoid

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 17
CT Scanning
2 studies, summarised in table 6, looked specifically at the use of CT scanning. Further
papers considered CT scanning in comparison to other modalities and these are discussed
later.
Table 6: CT scanning
Study
Patient group Key Results
Temple et al [39] CT and plain film images
were compared in 11
cadaver specimens with
iatrogenic fractures.
CT:
Sensitivity for detecting fracture =100%,
sensitivity for detecting if fracture
displaced >1mm =50%, specificity for
detecting if fracture displaced >1mm
=89%
Plain film:
Sensitivity for detecting fracture =99%,
Specificity for detecting if fracture
displaced >1mm =84%
Nguyen et al [40] 118 patients with clinical
scaphoid fractures and
normal or non-conclusive
initial x-rays underwent CT
scanning (26 fractures
were identified)
3 scaphoid fractures identified by CT in the
16 patients with suspicious initial
radiography
23 scaphoid fractures identified by CT in
the 102 patients with normal films
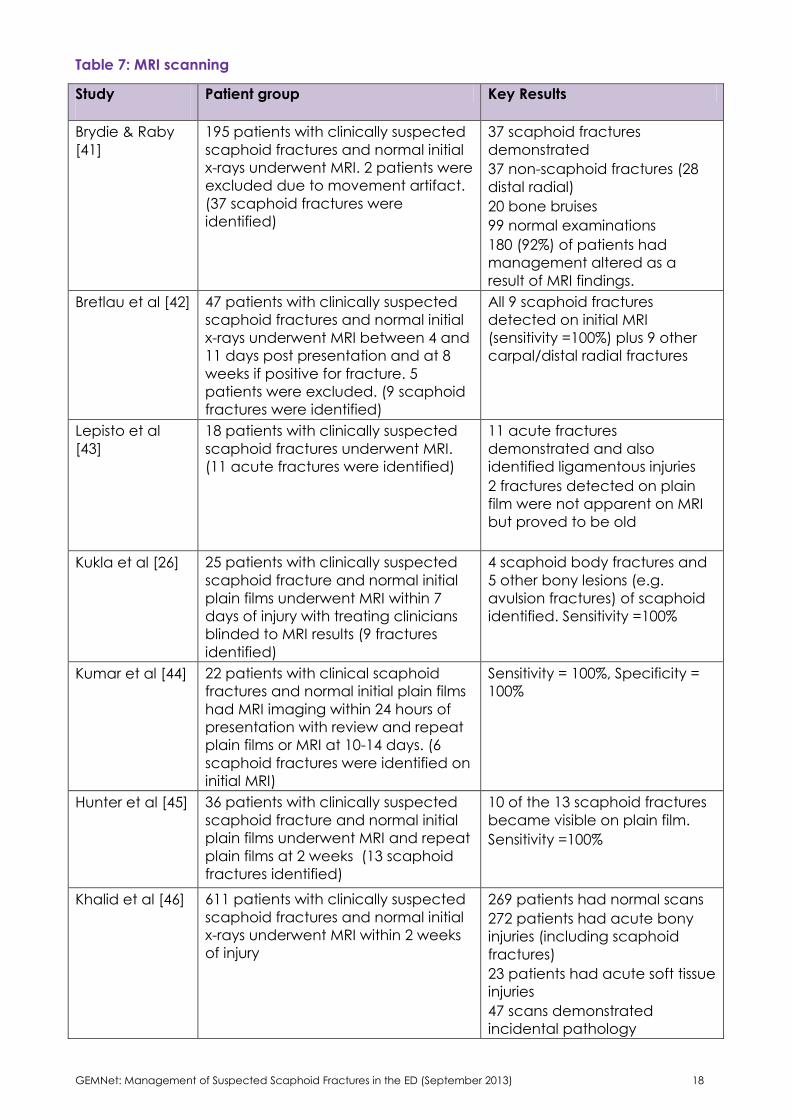
MRI
Table 7 summarises the studies looking at MRI. The sensitivity for detecting scaphoid
fractures was excellent (typically 100%) while also being able to give diagnostic
information on non-scaphoid injuries both bony and ligamentous.
GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 18
Table 7: MRI scanning
Study
Patient group Key Results
Brydie & Raby
[41]
195 patients with clinically suspected
scaphoid fractures and normal initial
x-rays underwent MRI. 2 patients were
excluded due to movement artifact.
(37 scaphoid fractures were
identified)
37 scaphoid fractures
demonstrated
37 non-scaphoid fractures (28
distal radial)
20 bone bruises
99 normal examinations
180 (92%) of patients had
management altered as a
result of MRI findings.
Bretlau et al [42] 47 patients with clinically suspected
scaphoid fractures and normal initial
x-rays underwent MRI between 4 and
11 days post presentation and at 8
weeks if positive for fracture. 5
patients were excluded. (9 scaphoid
fractures were identified)
All 9 scaphoid fractures
detected on initial MRI
(sensitivity =100%) plus 9 other
carpal/distal radial fractures
Lepisto et al
[43]
18 patients with clinically suspected
scaphoid fractures underwent MRI.
(11 acute fractures were identified)
11 acute fractures
demonstrated and also
identified ligamentous injuries
2 fractures detected on plain
film were not apparent on MRI
but proved to be old
Kukla et al [26] 25 patients with clinically suspected
scaphoid fracture and normal initial
plain films underwent MRI within 7
days of injury with treating clinicians
blinded to MRI results (9 fractures
identified)
4 scaphoid body fractures and
5 other bony lesions (e.g.
avulsion fractures) of scaphoid
identified. Sensitivity =100%
Kumar et al [44] 22 patients with clinical scaphoid
fractures and normal initial plain films
had MRI imaging within 24 hours of
presentation with review and repeat
plain films or MRI at 10-14 days. (6
scaphoid fractures were identified on
initial MRI)
Sensitivity = 100%, Specificity =
100%
Hunter et al [45] 36 patients with clinically suspected
scaphoid fracture and normal initial
plain films underwent MRI and repeat
plain films at 2 weeks (13 scaphoid
fractures identified)
10 of the 13 scaphoid fractures
became visible on plain film.
Sensitivity =100%
Khalid et al [46] 611 patients with clinically suspected
scaphoid fractures and normal initial
x-rays underwent MRI within 2 weeks
of injury
269 patients had normal scans
272 patients had acute bony
injuries (including scaphoid
fractures)
23 patients had acute soft tissue
injuries
47 scans demonstrated
incidental pathology

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 19
Comparing Bone Scan with MRI
Two studies compared scintigraphy (bone scanning) with MRI and are described in table
8.
Table 8: Bone scanning versus MRI scanning
Study
Patient group Key Results
Thorpe et al [47] Prospective study comparing bone
scan and MRI in 62 patients (3 of whom
were excluded due to inability to
tolerate MRI/degraded images) with
suspected scaphoid fracture and
normal initial radiographs. 4 scaphoid
fractures were identified.
Bone Scan
Sensitivity = 100%, Specificity
= 94.5%, Positive Predictive
Value = 57.1%, Negative
Predictive Value = 100%
MRI
Sensitivity = 100%, Specificity
= 98.18%, Positive Predictive
Value = 80%, Negative
Predictive Value = 100%
Beeres et al [48] Study comparing bone scan and MRI in
100 patients with suspected scaphoid
fracture and normal initial radiographs
with plain radiographs and examination
at 6 weeks used as gold standard
where there was disagreement
between MRI and bone scan. 20
scaphoid fractures were identified.
Bone Scan
Sensitivity = 100%, Specificity
= 90%, Positive Predictive
Value = 71%, Negative
Predictive Value = 100%
MRI
Sensitivity = 80%, Specificity =
100%, Positive Predictive
Value = 100%, Negative
Predictive Value = 95%
Comparing CT and Bone Scan
Only 1 study compared CT against bone scanning, the details of which are given in table
9.
Table 9: CT versus Bone Scan
Study
Patient group Key Results
Breederveld et al [49] Prospective study comparing
CT and bone scan with follow
up CT at 6 weeks and clinical
follow up at 8-14 months in 29
patients with suspected
scaphoid fracture and normal
initial radiographs. 9 scaphoid
fractures identified.
Bone Scan
Sensitivity = 78 %, Specificity =
90%, Positive Predictive Value =
78%, Negative Predictive Value =
90%
CT
Sensitivity = 100%, Specificity =
100%, Positive Predictive Value =
100%, Negative Predictive Value
= 100%

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 20
Comparing MRI and CT
Table 10 summarises the 2 studies comparing MRI and CT.
Table 10: CT versus MRI
Study
Patient group Key Results
Memarsadeghi
et al [50]
Prospective study comparing CT
and MRI against gold standard
of plain radiographs at 6 weeks
in 29 patients with suspected
scaphoid fracture and normal
initial radiography –
differentiated between cortical
fractures (8 fractures) and
trabecular fractures (3 fractures)
MRI – All scaphoid fractures
Sensitivity = 100%, Specificity = 100%,
Accuracy = 100%,
MRI – Cortical scaphoid fractures
Sensitivity = 38%, Specificity = 100%,
Accuracy = 55%,
CT – All scaphoid fractures
Sensitivity = 73%, Specificity = 100%,
Accuracy = 89%,
CT – Cortical scaphoid fractures
Sensitivity = 100%, Specificity = 100
%, Accuracy = 100%,
Mallee, W., et al.
2011
Prospective study comparing CT
and MRI against gold standard
of plain radiographs at 6 weeks
in 40 patients with suspected
scaphoid fracture and normal
initial radiography. 6 scaphoid
fractures identified (5 on plain
films, 1 not visible on x-ray but
seen on CT and MRI) with 5
patients lost to follow up and 1
excluded due to inadequate
imaging.
MRI – scaphoid fractures only
Sensitivity = 67 %, Specificity = 89%,
Accuracy = 85%,
CT – scaphoid fractures only
Sensitivity = 67%, Specificity = 96%,
Accuracy = 91%,
The results of the Mallee study are significantly worse than all others looking at CT and MRI.
The authors excluded all fractures visible on initial imaging, and considered a focal area of
bone oedema on MRI as diagnostic of a fracture. If the MRI criteria had been changed to
require a cortical abnormality to be visible, then it would have found 4 fractures (instead
of 7), with one false positive result (instead of 3) and three false-negative results (instead of
2). This would have given a sensitivity of 50%, specificity of 96% and accuracy of 88%.
One difficulty is the lack of a definition as to what constitutes a scaphoid fracture. MRI
findings may be a bone bruise, CT findings may be a vascular channel, and 6 week plain
radiography may not be a definitive gold standard.
Cost effectiveness studies
There have been a number of cost effectiveness studies that demonstrate that one mode
of imaging is more cost effective than another. These are shown in Table 11. However
there is great variation in the calculated costs of different types of imaging and follow up,
which makes interpretation of these data difficult. Furthermore the loss of income and
personal inconvenience associated with being unnecessarily immobilized in a cast or splint

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 21
is difficult to quantify, and will vary greatly between individuals.
Table 11: Cost effectiveness studies comparing different management strategies in
suspected Scaphoid fracture.
Study MRI Cost X-ray cost Clinic cost Bone scan
cost
Plaster cast
cost
Gooding et
al [65]
NZ$300 NZ$60 NZ$77 Not stated NZ$125
Brooks et al
[64]
AU$475 AU$28 1st AU$119
(subsequent
AU$60)
AU$295 Not stated
Saxena et al
[63]
£120 £22 £40 £70 £25
Hansen et al
[62]
€330 €88 €170 Not stated Not stated
Buul et al
[61]
Not stated €28 Not stated €164 €50
Published Reviews
Yin and colleagues used a meta-analysis to compare bone scintigraphy, MRI and CT in
the detection of clinically suspected scaphoid fractures.[2] This is also the current
Cochrane review. The main results are shown in table 12.
Table 12: Results of a meta-analysis of the diagnostic properties of commonly used tests in
suspected scaphoid fracture.[2] (Ln DOR = Natural logarithm of Diagnostic Odds Ratio)
Imaging
modality
Number of
Studies
Number of
patients
Sensitivity [95%
CI]
Specificity
[95% CI]
Ln DOR [95%CI]
Bone
Scintigraphy
15 1,102 97% [93-995] 89% [83-94%] 4.78 [4.02-5.54]
MRI 10 513 96% [91-99%] 99% [96-100%] 6.60 [5.43-7.76]
CT 6 211 93% [83-98%] 99% [96-100%] 6.11 [4.56-7.66]
The studies included in the meta-analysis were generally small, with the largest recruiting
just over 200 patients. None of the studies were randomised. Bone scintigraphy
demonstrated a statistically worse specificity than MRI (p<0.001) and CT (p=0.001),
however there was no statistically significant difference between CT and MRI. The
diagnostic odds ratio (DOR) for MRI was greater than bone scintigraphy (p=0.009), but no
other significant differences were identified in DOR.
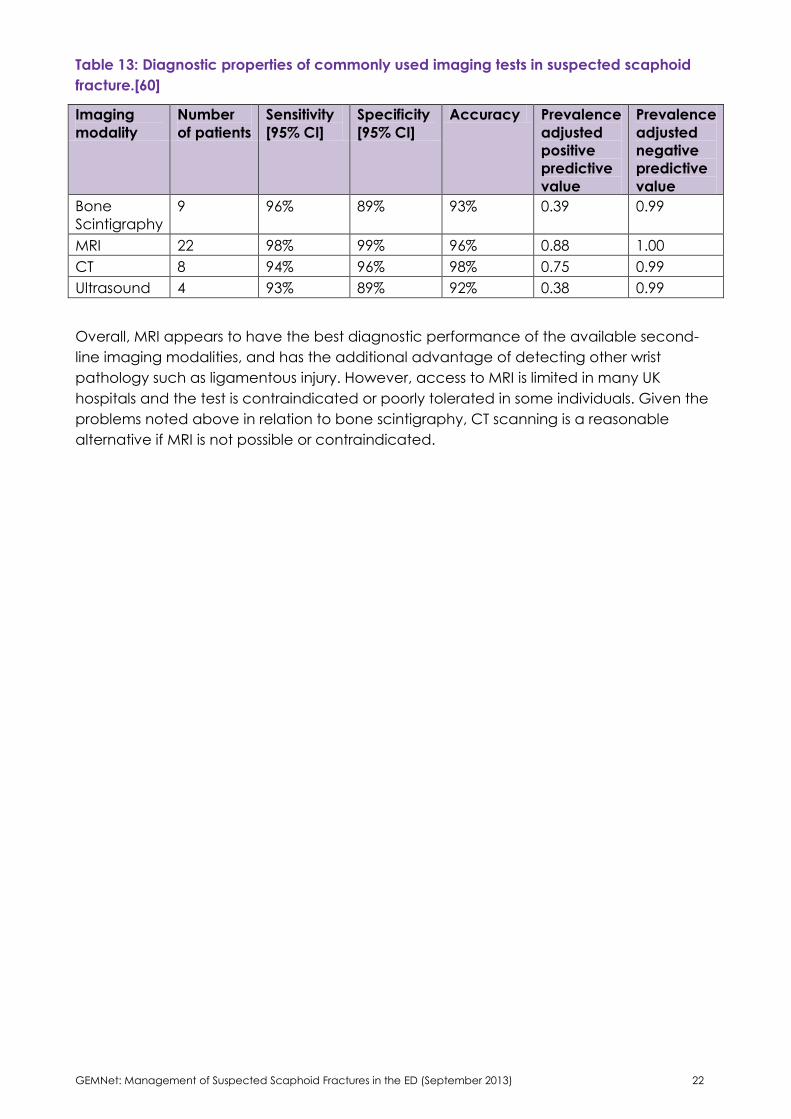
Ring and colleagues [60] also undertook a review of the literature and calculated the
diagnostic properties of bone scintigraphy, MRI, CT and ultrasound (Table 13). The high
negative predictive value is attributable to the low prevalence of scaphoid fractures.
GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 22
Table 13: Diagnostic properties of commonly used imaging tests in suspected scaphoid
fracture.[60]
Imaging
modality
Number
of patients
Sensitivity
[95% CI]
Specificity
[95% CI]
Accuracy Prevalence
adjusted
positive
predictive
value
Prevalence
adjusted
negative
predictive
value
Bone
Scintigraphy
9 96% 89% 93% 0.39 0.99
MRI 22 98% 99% 96% 0.88 1.00
CT 8 94% 96% 98% 0.75 0.99
Ultrasound 4 93% 89% 92% 0.38 0.99
Overall, MRI appears to have the best diagnostic performance of the available second-
line imaging modalities, and has the additional advantage of detecting other wrist
pathology such as ligamentous injury. However, access to MRI is limited in many UK
hospitals and the test is contraindicated or poorly tolerated in some individuals. Given the
problems noted above in relation to bone scintigraphy, CT scanning is a reasonable
alternative if MRI is not possible or contraindicated.

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 23
7.3 Immobilisation
Published research in this area is very limited (see table 14), but the available evidence
suggests that a Scaphoid cast offers no benefit over a standard “Colles” cast, and is more
disabling for the patient. There may be some benefit to immobilising a Scaphoid fracture
in an above elbow cast, but the two studies in this area do not agree.
Table 14: Immobilisation
Study Patient Group Key Results
Kaneshiro et al [52] Cadaveric study of 4
iatrogenic scaphoid fractures
immobilised with a below
elbow cast
Significant movement of scaphoid
(>1mm) with
pronation/suppination
Clay et al [53] Prospective randomized trial
comparing rate of non-union
between patients randomly
allocated to either a “Colles”
or scaphoid cast. 292 patients
were reviewed at 2, 4 and 8
weeks when the cast was
removed. If healing was in
doubt at this point, the plaster
was replaced for a further 4
weeks.
No difference in non-union rate
between the two groups, but
patients felt the scaphoid cast was
more disabling.
Hambidge et al[56] Compared rate of non-union
after immobilising the wrist in
flexion or extension in fractures
of the waist or distal pole of
the scaphoid treated in a
“Colles” cast
No difference in non-union rate,
flexion or grip strength at 6 months,
but significantly reduced extension
in patients who were immobilized
in 20 degrees of flexion rather that
20 degrees of extension
Karantana et al [55] Compared hand function with
the wrist immobilized in a
“Colles” or scaphoid cast
Scaphoid cast caused significantly
more disability than the “Colles”
cast, or no cast at all
Gellman et al [57] Compared a long thumb
spica, which included elbow
immobilization (28 fractures),
with a short thumb spica that
did not immobilise the elbow
(23 fractures)
Fractures of the proximal or middle
third of the scaphoid healed
quicker if immobilised for 6 weeks
in a long thumb spica followed by
a short thumb spica, rather than
spending the entire period of
immobilisation in a short thumb
spica. Fractures of the distal third
healed independently of splint
length
Terkelsen et al [58] 48 patients in the long cast
group and 44 in the short cast
group, all of whom were
followed up for at least 12
months.
Non-union occurred in 2 of 5
fractures in the proximal part of
the scaphoid, and 8 of 77
fractures in the waist or distal part.
There were 7 non-unions in the
long cast group and 3 in the short
cast group, but this difference was
not significant (p=0.25).

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 24
7.4 Follow up
There is no useful evidence on the duration or timing of clinical follow-up in suspected
scaphoid fracture. Once a fracture has been confirmed or excluded further management
can proceed accordingly, and therefore clinical follow-up is only required until a firm
diagnosis has been made, either on clinical grounds or through the use of additional
imaging.
Outpatient review at two weeks is a popular option, based on the assumption that an
initially occult fracture will be more readily visualized on plain X-rays taken at this stage.
However, whilst it is true that scaphoid fractures that cannot be detected on initial X-rays
may become apparent on an X-ray taken after two weeks, the published evidence
indicates that scaphoid fractures may still be diagnosed for the first time when a patient is
X-rayed at 8 weeks,[29] though the clinical significance of such injuries is unclear.
7.5 Scaphoid fractures in children
These are rare fractures; accounting for 0.34% of all children’s fractures. However
scaphoid fractures become more common as the child grows older. [59]
Evenski and colleagues performed a retrospective review of children with suspected
scaphoid fracture who presented to a single children’s emergency department over a 7
year period.[24] Of 165 wrists, 104 were included in the study (there were 103 patients,
since in one child both wrists were included). 21 had scaphoid fractures on presentation,
11 had an ipsilateral upper limb fracture and there were incomplete data for 29. Those
included were 57 boys and 46 girls with an average age of 13 years (range 5-15 years).
31(30%) children were found to have a scaphoid fracture during follow up: 14 at two
weeks, 12 at five weeks and 5 at seven weeks.

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 25
8. Evidence-based flowchart
History compatible with possible fracture
AND
Examination confirms tenderness:
Anatomical snuffbox and/or scaphoid tubercle
Plain radiographs, scaphoid views
“Colles” cast and orthopaedic
follow-up
Immobilise in “Colles” cast or wrist splint
(according to local practice) until MRI
scan.
Thumb immobilisation is not required.
(Senior medical review may be useful to
exclude alternative causes of symptoms)
MRI scan
(CT scan if MRI contra-indicated)
Discharge:
no follow-up required
No Fracture
Fracture
Fracture
No Fracture

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 26
References
1. Steenvoorde, P., C. Jacobi, A.L. van, L. van, J. Kievit, and J. Oskam, Development
of a clinical decision tool for suspected scaphoid fractures. Acta Orthopaedica
Belgica, 2006. 72(4): p. 404-10.
2. Yin, Z.G., J.B. Zhang, S.L. Kan, and X.G. Wang, Diagnosing suspected scaphoid
fractures: a systematic review and meta-analysis. Clinical Orthopaedics & Related
Research, 2010. 468(3): p. 723-34.
3. McLaughlin, H.L. and J.C. Parkes, 2nd, Fracture of the carpal navicular (Scaphoid)
bone: gradations in therapy based upon pathology. J Trauma 1969;9(4):311-9.
4. Langhoff, O. and J.L. Andersen, Consequences of late immobilization of Scaphoid
fractures. J Hand Surg Br 1988;13(1):77-9.
5. Duncan, D.S. and A.J. Thurston, Clinical fracture of the carpal Scaphoid--an
illusionary diagnosis. Journal of Hand Surgery (Edinburgh, Lothian) 1985;10(3):375-
376.
6. Leslie, I.J. and R.A. Dickson, The fractured carpal Scaphoid. Natural history and
factors influencing outcome. J Bone Joint Surg Br 1981;63-B(2):225-30.
7. Hunter, D., Diagnosis and management of Scaphoid fractures: a literature review.
Emergency Nurse 2005;13(7):22-6.
8. Groves, A.M., I. Kayani, R. Syed, B.F. Hutton, P.P. Bearcroft, A.K. Dixon, and P.J. Ell,
An international survey of hospital practice in the imaging of acute scaphoid
trauma. AJR. American Journal of Roentgenology, 2006. 187(6): p. 1453-6
9. Royal College of Radiologists, Making the best use of clinical radiology services:
referral guidelines. 7th. Ed 2011, London: Royal College of Radiologists.
10. Royal College of Radiologists, Appropriateness Criteria. 2008 [cited 2011 4/9/2011];
Available from:
http://www.acr.org/SecondaryMainMenuCategories/quality_safety/app_criteria/p
df/ExpertPanelonMusculoskeletalImaging/AcuteHandandWristTraumaDoc1.aspx
11. Dorsay, T.A., N.M. Major, and C.A. Helms, Cost-effectiveness of immediate MR
imaging versus traditional follow-up for revealing radiographically occult Scaphoid
fractures. American Journal of Roentgenology 2001;177(6):1257-63.
12. Callaghan, M. and J.R. Fowler, Clinical Tests for Scaphoid Fractures. Emergency
Medicine Journal 2011;28(4):332-334.
13. Oxford Centre for Evidence-based Medicine - Levels of Evidence (March 2009).
[cited 2011 24/05/2011]; Available from: http://www.cebm.net/?o=1025
14. Jacobsen, S., G. Hassani, D. Hansen, and O. Christensen, Suspected scaphoid
fractures. Can we avoid overkill? Acta Orthopaedica Belgica, 1995. 61(2): p. 74-8.
15. Jayasekera, N., N. Akhtar, and J.P. Compson, Physical examination of the carpal
bones by orthopaedic and accident and emergency surgeons. Journal of Hand
Surgery - British Volume 2005;30(2):204-6.
16. Freeland, P., Scaphoid tubercle tenderness: a better indicator of Scaphoid
fractures? Archives of Emergency Medicine 1989;6(1):46-50.
17. Parvizi, J., J. Wayman, P. Kelly, and C.G. Moran, Combining the clinical signs
improves diagnosis of scaphoid fractures. A prospective study with follow-up.
Journal of Hand Surgery - British Volume, 1998. 23(3): p. 324-7.

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 27
18. Esberger, D.A., What value the Scaphoid compression test? J Hand Surg Br 1994;
19(6):748-9.
19. Waizenegger, M., N.J. Barton, T.R. Davis, and M.L. Wastie, Clinical signs in scaphoid
fractures. J Hand Surg Br, 1994. 19(6): p. 743-7..
20. Grover, R., Clinical assessment of Scaphoid injuries and the detection of fractures.
Journal of Hand Surgery - British Volume 1996;21(3):341-3.
21. Rhemrev, S.J., F.J. Beeres, R.H.R. van, M. Hogervorst, and D. Ring, Clinical prediction
rule for suspected scaphoid fractures: A prospective cohort study. Injury, 2010.
41(10): p. 1026-30..
22. Unay, K., B. Gokcen, K. Ozkan, O. Poyanli, and E. Eceviz, Examination tests
predictive of bone injury in patients with clinically suspected occult scaphoid
fracture. Injury, 2009. 40(12): p. 1265-8
23. Wilson, A.W., M.H. Kurer, J.L. Peggington, D.S. Grant, and C.C. Kirk, Bone
scintigraphy in the management of X-ray-negative potential scaphoid fractures.
Arch Emerg Med, 1986. 3(4): p. 235-42.
24. Evenski, A.J., M.J. Adamczyk, R.P. Steiner, M.A. Morscher, and P.M. Riley, Clinically
suspected scaphoid fractures in children. J Pediatr Orthop, 2009. 29(4): p. 352-5.
25. Gaebler, C., C. Kukla, M.J. Breitenseher, L. Mrkonjic, F. Kainberger, and V. Vecsei,
Limited diagnostic value of macroradiography in suspected scaphoid fractures.
Acta Orthopaedica Scandinavica, 1998. 69(4): p. 401-3.
26. Kukla, C., C. Gaebler, M.J. Breitenseher, S. Trattnig, and V. Vecsei, Occult fractures
of the scaphoid. The diagnostic usefulness and indirect economic repercussions of
radiography versus magnetic resonance scanning. J Hand Surg Br, 1997. 22(6): p.
810-3.
27. Stephen, A.B., D. Pye, A.R. Lyons, J.A. Oni, and T.R. Davis, Dual energy X-ray
absorptiometry (DXA): can it detect acute scaphoid fractures? Journal of Hand
Surgery - British Volume, 2005. 30(1): p. 83-4.
28. Hauger, O., O. Bonnefoy, M. Moinard, D. Bersani, and F. Diard, Occult fractures of
the waist of the scaphoid: early diagnosis by high-spatial-resolution sonography.
AJR Am J Roentgenol, 2002. 178(5): p. 1239-45.
29. Senall, J.A., J.M. Failla, J.A. Bouffard, and M. van, Ultrasound for the early diagnosis
of clinically suspected scaphoid fracture. Journal of Hand Surgery - American
Volume, 2004. 29(3): p. 400-5.
30. Shenouda, N.A. and J.P. England, Ultrasound in the diagnosis of Scaphoid fractures.
J Hand Surg Br 1987;12(1):43-5.
31. DaCruz, D.J., R.H. Taylor, B. Savage, and G.G. Bodiwala, Ultrasound assessment of
the suspected scaphoid fracture. Archives of Emergency Medicine, 1988. 5(2): p.
97-100.
32. Finkenberg, J.G., E. Hoffer, C. Kelly, and D.M. Zinar, Diagnosis of occult scaphoid
fractures by intrasound vibration. J Hand Surg Am, 1993. 18(1): p. 4-7.
33. Stordahl, A., A. Schjoth, G. Woxholt, and H. Fjermeros, Bone scanning of fractures of
the scaphoid. J Hand Surg Br, 1984. 9(2): p. 189-90.
34. Waizenegger, M., M.L. Wastie, N.J. Barton, and T.R. Davis, Scintigraphy in the
evaluation of the "clinical" scaphoid fracture. J Hand Surg Br, 1994. 19(6): p. 750-3.
GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 28
35. Akdemir, U.O., T. Atasever, S. Sipahioglu, S. Turkolmez, C. Kazimoglu, and E. Sener,
Value of bone scintigraphy in patients with carpal trauma. Ann Nucl Med, 2004.
18(6): p. 495-9.
36. Young, M.R., J.H. Lowry, J.D. Laird, and W.R. Ferguson, 99Tcm-MDP bone scanning
of injuries of the carpal scaphoid. Injury, 1988. 19(1): p. 14-17.
37. Jorgensen, T.M., T.M., J.r.-H. Andresen, P. Thommesen, and H.H. Hansen, Scanning
and Radiology of the Carpal Scaphoid Bone. Acta Orthopaedica, 1979. 50(6): p.
663-665..
38. Bayer, L.R., A. Widding, and H. Diemer, Fifteen minutes bone scintigraphy in patients
with clinically suspected Scaphoid fracture and normal x-rays. Injury 2000; 31(4):243-
8.
39. Temple, C.L., D.C. Ross, J.D. Bennett, G.J. Garvin, G.J. King, and K.J. Faber,
Comparison of sagittal computed tomography and plain film radiography in a
scaphoid fracture model. Journal of Hand Surgery - American Volume, 2005. 30(3):
p. 534-42..
40. Nguyen, Q., S. Chaudhry, R. Sloan, I. Bhoora, and C. Willard, The clinical scaphoid
fracture: early computed tomography as a practical approach. Annals of the
Royal College of Surgeons of England, 2008. 90(6): p. 488-91.
41. Brydie, A. and N. Raby, Early MRI in the management of clinical Scaphoid fracture.
British Journal of Radiology 2003;76(905):296-300.
42. Bretlau, T., O.M. Christensen, P. Edstrom, H.S. Thomsen, and G.S. Lausten, Diagnosis
of scaphoid fracture and dedicated extremity MRI. Acta Orthopaedica, 1999.
70(5): p. 504-508.
43. Lepisto, J., K. Mattila, S. Nieminen, B. Sattler, and M. Kormano, Low field MRI and
scaphoid fracture. J Hand Surg Br, 1995. 20(4): p. 539-42.
44. Kumar, S., A. O'Connor, M. Despois, and H. Galloway, Use of early magnetic
resonance imaging in the diagnosis of occult scaphoid fractures: the CAST Study
(Canberra Area Scaphoid Trial). The New Zealand medical journal, 2005. 118(1209).
45. Hunter, J.C., E.M. Escobedo, A.J. Wilson, D.P. Hanel, G.C. Zink-Brody, and F.A. Mann,
MR imaging of clinically suspected scaphoid fractures. AJR Am J Roentgenol, 1997.
168(5): p. 1287-93.
46. Khalid, M., Z.R. Jummani, K. Kanagaraj, A. Hussain, D. Robinson, and R. Walker, Role
of MRI in the diagnosis of clinically suspected scaphoid fracture: analysis of 611
consecutive cases and literature review. Emergency Medicine Journal, 2010. 27(4):
p. 266-269.
47. Thorpe, A.P., A.D. Murray, F.W. Smith, and J. Ferguson, Clinically suspected
scaphoid fracture: a comparison of magnetic resonance imaging and bone
scintigraphy. Br J Radiol, 1996. 69(818): p. 109-13.
48. Beeres, F.J., S.J. Rhemrev, P. den, L.M. Kingma, S.A. Meylaerts, S. le, K.A. Bartlema,
J.F. Hamming, and M. Hogervorst, Early magnetic resonance imaging compared
with bone scintigraphy in suspected scaphoid fractures. Journal of Bone & Joint
Surgery - British Volume, 2008. 90(9): p. 1205-9.
49. Breederveld, R.S. and W.E. Tuinebreijer, Investigation of computed tomographic
scan concurrent criterion validity in doubtful Scaphoid fracture of the wrist. J
Trauma 2004;57(4):851-4.

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 29
50. Memarsadeghi, M., M.J. Breitenseher, C. Schaefer-Prokop, M. Weber, S. Aldrian, C.
Gabler, and M. Prokop, Occult scaphoid fractures: comparison of multidetector CT
and MR imaging--initial experience. Radiology, 2006. 240(1): p. 169-76
51. Mallee, W., et al., Comparison of CT and MRI for diagnosis of suspected Scaphoid
fractures. Journal of Bone & Joint Surgery - American Volume 2011;93(1):20-8.
52. Kaneshiro, S.A., J.M. Failla, and S. Tashman, Scaphoid fracture displacement with
forearm rotation in a short-arm thumb spica cast. Journal of Hand Surgery -
American Volume 1999;24(5):984-91.
53. Clay, N.R., J.J. Dias, P.S. Costigan, P.J. Gregg, and N.J. Barton, Need the thumb be
immobilised in scaphoid fractures? A randomised prospective trial. Journal of Bone
& Joint Surgery - British Volume, 1991. 73(5): p. 828-32.
54. Petheram, T.G., S. Garg, and J.P. Compson, Is the Scaphoid cast still alive? A survey
of current UK practice in conservative management of Scaphoid fractures. Journal
of Hand Surgery: European Volume 2009;34(2):281-2.
55. Karantana, A., M.J. Downs-Wheeler, K. Webb, C.A. Pearce, A. Johnson, and G.C.
Bannister, The effects of Scaphoid and Colles casts on hand function. J Hand Surg
Br, 2006. 31(4): p. 436-8.
56. Hambidge, J.E., V.V. Desai, P.J. Schranz, J.P. Compson, T.R. Davis, and N.J. Barton,
Acute fractures of the scaphoid. Treatment by cast immobilisation with the wrist in
flexion or extension? J Bone Joint Surg Br, 1999. 81(1): p. 91-2.
57. Gellman, H., R.J. Caputo, V. Carter, A. Aboulafia, and M. McKay, Comparison of
short and long tumb-spica casts for non-displaced fractures of the carpal scaphoid.
Journal of Bone and Joint Surgery - Series A, 1989. 71(3): p. 354-357.
58. Terkelsen, C.J. and J.r.M. Jepsen, Treatment of Scaphoid fractures with a
removable cast. Acta Orthopaedica 1988;59(4):452-453.
59. D'Arienzo, M., Scaphoid fractures in children. Journal of Hand Surgery - British
Volume 2002;27(5):424-6.
60. Ring, D. and S. Lozano-Calderon, Imaging for suspected Scaphoid fracture. Journal
of Hand Surgery - American Volume 2008;33(6):954-7.
61. Tiel-van, M.M.M., T.H. Broekhuizen, E.J.E. van, and P.M. Bossuyt, Choosing a strategy
for the diagnostic management of suspected scaphoid fracture: a cost-
effectiveness analysis. Journal of Nuclear Medicine, 1995. 36(1): p. 45-8.
62. Hansen, T.B., R.B. Petersen, J. Barckman, P. Uhre, and K. Larsen, Cost-effectiveness
of MRI in managing suspected scaphoid fractures. Journal of Hand Surgery:
European Volume, 2009. 34(5): p. 627-30.
63. Saxena, P., R. McDonald, S. Gull, and N. Hyder, Diagnostic scanning for suspected
scaphoid fractures: an economic evaluation based on cost-minimisation models.
Injury, 2003. 34(7): p. 503-11.
64. Brooks, S., F.M. Cicuttini, S. Lim, D. Taylor, S.L. Stuckey, and A.E. Wluka, Cost
effectiveness of adding magnetic resonance imaging to the usual management of
suspected scaphoid fractures. British Journal of Sports Medicine, 2005. 39(2): p. 75-9.
65. Gooding, A., M. Coates, and A. Rothwell, Cost analysis of traditional follow-up
protocol versus MRI for radiographically occult Scaphoid fractures: a pilot study for
the Accident Compensation Corporation. New Zealand Medical Journal
2004;117(1201):U1049.

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 30

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 31

GEMNet: Management of Suspected Scaphoid Fractures in the ED (September 2013) 32
The College of Emergency Medicine
7-9 Breams Buildings
London
EC4A 1DT
Tel: +44 (0)20 7400 1999
Fax: +44 (0)20 7067 1267
www.collemergencymed.ac.uk