Gastrointestinal tract haemorrhage and ischaemia
6
INTENSIVE CARE ANAESTHESIA AND INTENSIVE CARE MEDICINE 10:3 131 © 2008 Elsevier Ltd. All rights reserved. Gastrointestinal tract haemorrhage and ischaemia Aung Lwin Daniele C Bryden Abstract Gastrointestinal (GI) bleeding, especially acute upper gastrointestinal bleeding, is a common medical emergency. Peptic ulcer, variceal bleed- ing and bleeding from stress ulceration in critically ill patients are all associated with significant morbidity and mortality. The Rockall score should be used to identify high-risk patients who need urgent treat- ment. Adequate resuscitation is essential before attempting endoscopy, which is used to establish the diagnosis and allow effective endoscopic therapies. Terlipressin, a vasopressin analogue, is indicated in patients with suspected variceal bleeding prior to endoscopy, whereas a proton pump inhibitor infusion is recommended in patients with peptic ulcer bleeding only after endoscopic treatment. Selective mesenteric emboli- zation and surgery are reserved for patients with non-variceal bleeding refractory to therapeutic endoscopy. Transjugular intrahepatic portosys- temic shunt stenting and shunt surgery are reserved for patients with refractory variceal bleeding in an acute setting or as a bridge therapy for prevention of acute variceal bleeding before liver transplantation. In criti- cally ill patients, adequate resuscitation, cautious use of vasopressors, prophylactic use of gastric acid-suppressing agents and enteral nutrition are the cornerstones of treatment in prevention of stress ulcers. Lower GI investigations should be performed in patients with rectal bleeding after exclusion of upper GI bleeding. GI tract ischaemia plays an important role in the aetiology of stress ulcer disease and ischaemic colitis and is also a potential complication of mesenteric embolization in patients with GI bleeding refractory to therapeutic endoscopy. Keywords lower gastrointestinal haemorrhage; mesenteric ischaemia; non-variceal haemorrhage; stress ulcer disease; upper gastrointestinal haemorrhage; variceal haemorrhage Gastrointestinal haemorrhage originates from either the upper gastrointestinal tract, that is, above the ligament of Treitz (oesoph- agus, stomach or duodenum), or the lower gastrointestinal tract (usually colonic and rectal, but can be small bowel in origin). Aung Lwin, MRCP, is a Specialist Registrar in Intensive Care Medicine at Sheffield Teaching Hospitals (STH) NHS Trust, UK, and is training for a Dual CCT in Acute General Medicine and Intensive Care Medicine with the Eastern deanery. He is currently finishing his Enhanced ICM training in Sheffield. Conflicts of interest: none declared. Daniele C Bryden, FRCA, LLB (Hons), MML, is a Consultant in Intensive Care Medicine at STH. Her interests are medical education and the interplay of law and ethics with critical care practice. Conflicts of interest: none declared. An algorithm summarizing the management of gastrointesti- nal haemorrhage is given in Figure 1. Upper gastrointestinal bleeding Epidemiology and aetiology Acute upper gastrointestinal bleeding (UGIB) is a common medical emergency and accounts for 8% of medical admis- sions. 1 Based on a 1993 UK audit, the overall incidence of acute UGIB was 103 per 100,000 adults per year with a median age of 71 years. 1 A further national audit 2 in 2007 showed an overall mortality of 10% with incidence, co-morbidities and mortality significantly increased with age. Peptic ulcer and variceal bleed- ing are the major causes of severe UGIB (Table 1). Typical pre- sentations include haematemesis (vomiting of blood), melaena (passing of black tarry stools), anaemia, syncope and shock. Peptic ulcer disease: peptic ulcer bleeding accounts for approxi- mately 36% of acute UGIB. 1,2 Helicobacter pylori infection, use of non-steroidal anti-inflammatory drugs (NSAIDs), including cyclo-oxygenase 2 (COX 2) inhibitors, selective serotonin reup- take inhibitors (SSRIs) and corticosteroids are important causes of peptic ulcer disease. The incidence of peptic ulcer bleeding has not been affected despite improvements in pharmacotherapy and therapeutic procedures. This may be due to greater use of antiplatelet therapy (aspirin, clopidogrel) and anticoagulants in patients with cardiovascular disease. In patients with acute UGIB who have recent coronary artery stents, the inadvertent stopping of antiplatelet therapy can cause stent thrombosis and myocar- dial infarction. Variceal bleeding: varices are dilatations of superficial veins due to portal hypertension at the junction between the portal and sys- temic venous systems. The common sites of bleeding are distal oesophagus (oesophageal varices) and proximal stomach (gas- tric varices) but they can also be found in the rectum. Bleeding due to varices and portal hypertensive gastropathy has been an increasingly important cause of acute UGIB (from 4% to 16%). 1,2 A history of previous variceal bleed, chronic liver disease and alcoholism, and/or stigmata of chronic liver disease or portal hypertension on physical examination should raise the suspicion of variceal bleeding. The outcome of variceal bleeding depends on the severity of the underlying liver disease. Management of upper gastrointestinal bleeding Initial assessment: during and after resuscitation, the aim of initial assessment is to identify high-risk patients who require urgent investigations (endoscopy) and aggressive treatment. Fresh haematemesis suggests significant bleeding, whereas coffee ground vomitus (vomiting of black material) is more usu- ally seen in relatively minor bleeding. A prospective cohort study 3 found that age, presence of shock, co-morbidity, underlying diagnosis, major stigmata of recent haemorrhage and rebleeding are all independent predic- tors of mortality. The Rockall score (a numerical scoring system) was developed and is based on these parameters (Table 2). This scoring system has been validated for prediction of rebleeding and mortality, in variceal and non-variceal populations. 4 A gen- eral relationship exists between increasing score and increased
Transcript of Gastrointestinal tract haemorrhage and ischaemia

IntensIve care
Gastrointestinal tract haemorrhage and ischaemiaaung Lwin
Daniele c Bryden
AbstractGastrointestinal (GI) bleeding, especially acute upper gastrointestinal
bleeding, is a common medical emergency. Peptic ulcer, variceal bleed-
ing and bleeding from stress ulceration in critically ill patients are all
associated with significant morbidity and mortality. the rockall score
should be used to identify high-risk patients who need urgent treat-
ment. adequate resuscitation is essential before attempting endoscopy,
which is used to establish the diagnosis and allow effective endoscopic
therapies. terlipressin, a vasopressin analogue, is indicated in patients
with suspected variceal bleeding prior to endoscopy, whereas a proton
pump inhibitor infusion is recommended in patients with peptic ulcer
bleeding only after endoscopic treatment. selective mesenteric emboli-
zation and surgery are reserved for patients with non-variceal bleeding
refractory to therapeutic endoscopy. transjugular intrahepatic portosys-
temic shunt stenting and shunt surgery are reserved for patients with
refractory variceal bleeding in an acute setting or as a bridge therapy for
prevention of acute variceal bleeding before liver transplantation. In criti-
cally ill patients, adequate resuscitation, cautious use of vasopressors,
prophylactic use of gastric acid-suppressing agents and enteral nutrition
are the cornerstones of treatment in prevention of stress ulcers. Lower GI
investigations should be performed in patients with rectal bleeding after
exclusion of upper GI bleeding. GI tract ischaemia plays an important
role in the aetiology of stress ulcer disease and ischaemic colitis and is
also a potential complication of mesenteric embolization in patients with
GI bleeding refractory to therapeutic endoscopy.
Keywords lower gastrointestinal haemorrhage; mesenteric ischaemia;
non-variceal haemorrhage; stress ulcer disease; upper gastrointestinal
haemorrhage; variceal haemorrhage
Gastrointestinal haemorrhage originates from either the upper gastrointestinal tract, that is, above the ligament of Treitz (oesoph-agus, stomach or duodenum), or the lower gastrointestinal tract (usually colonic and rectal, but can be small bowel in origin).
Aung Lwin, MRCP, is a Specialist Registrar in Intensive Care Medicine
at Sheffield Teaching Hospitals (STH) NHS Trust, UK, and is training
for a Dual CCT in Acute General Medicine and Intensive Care Medicine
with the Eastern deanery. He is currently finishing his Enhanced ICM
training in Sheffield. Conflicts of interest: none declared.
Daniele C Bryden, FRCA, LLB (Hons), MML, is a Consultant in Intensive Care
Medicine at STH. Her interests are medical education and the interplay
of law and ethics with critical care practice. Conflicts of interest: none
declared.
anaestHesIa anD IntensIve care MeDIcIne 10:3 131
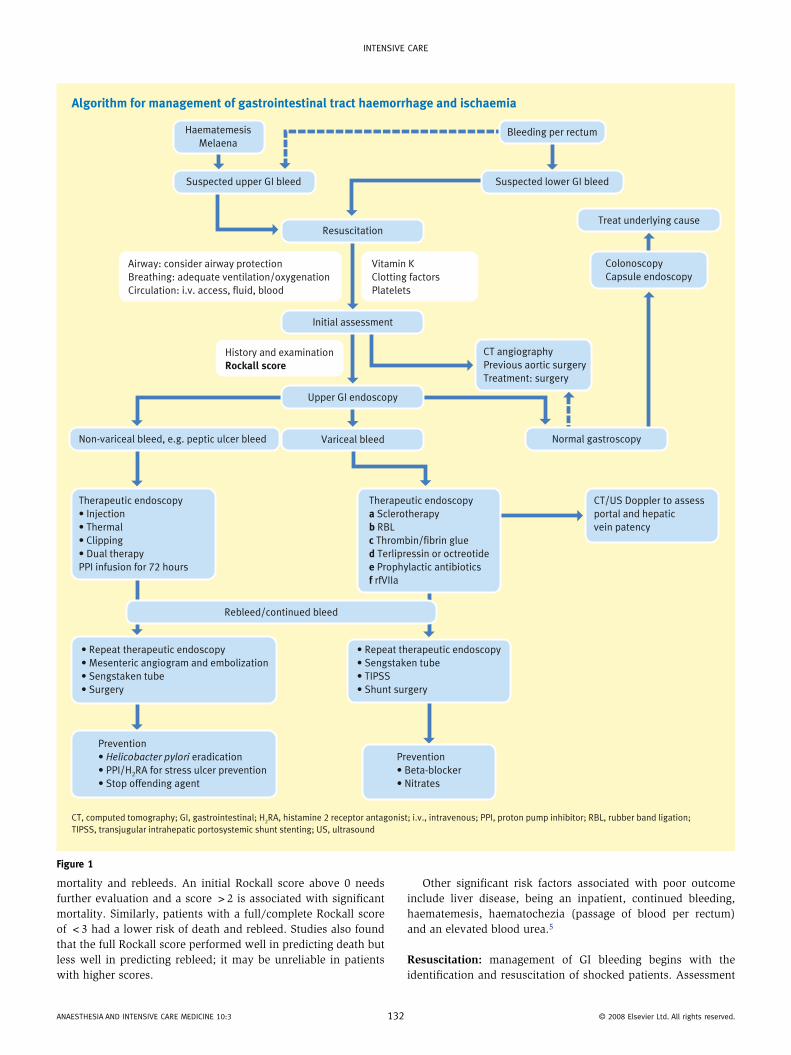
An algorithm summarizing the management of gastrointesti-nal haemorrhage is given in Figure 1.
Upper gastrointestinal bleeding
Epidemiology and aetiologyAcute upper gastrointestinal bleeding (UGIB) is a common medical emergency and accounts for 8% of medical admis-sions.1 Based on a 1993 UK audit, the overall incidence of acute UGIB was 103 per 100,000 adults per year with a median age of 71 years.1 A further national audit2 in 2007 showed an overall mortality of 10% with incidence, co-morbidities and mortality significantly increased with age. Peptic ulcer and variceal bleed-ing are the major causes of severe UGIB (Table 1). Typical pre-sentations include haematemesis (vomiting of blood), melaena (passing of black tarry stools), anaemia, syncope and shock.
Peptic ulcer disease: peptic ulcer bleeding accounts for approxi-mately 36% of acute UGIB.1,2 Helicobacter pylori infection, use of non-steroidal anti-inflammatory drugs (NSAIDs), including cyclo-oxygenase 2 (COX 2) inhibitors, selective serotonin reup-take inhibitors (SSRIs) and corticosteroids are important causes of peptic ulcer disease. The incidence of peptic ulcer bleeding has not been affected despite improvements in pharmacotherapy and therapeutic procedures. This may be due to greater use of antiplatelet therapy (aspirin, clopidogrel) and anticoagulants in patients with cardiovascular disease. In patients with acute UGIB who have recent coronary artery stents, the inadvertent stopping of antiplatelet therapy can cause stent thrombosis and myocar-dial infarction.
Variceal bleeding: varices are dilatations of superficial veins due to portal hypertension at the junction between the portal and sys-temic venous systems. The common sites of bleeding are distal oesophagus (oesophageal varices) and proximal stomach (gas-tric varices) but they can also be found in the rectum. Bleeding due to varices and portal hypertensive gastropathy has been an increasingly important cause of acute UGIB (from 4% to 16%).1,2 A history of previous variceal bleed, chronic liver disease and alcoholism, and/or stigmata of chronic liver disease or portal hypertension on physical examination should raise the suspicion of variceal bleeding. The outcome of variceal bleeding depends on the severity of the underlying liver disease.
Management of upper gastrointestinal bleedingInitial assessment: during and after resuscitation, the aim of initial assessment is to identify high-risk patients who require urgent investigations (endoscopy) and aggressive treatment.
Fresh haematemesis suggests significant bleeding, whereas coffee ground vomitus (vomiting of black material) is more usu-ally seen in relatively minor bleeding.
A prospective cohort study3 found that age, presence of shock, co-morbidity, underlying diagnosis, major stigmata of recent haemorrhage and rebleeding are all independent predic-tors of mortality. The Rockall score (a numerical scoring system) was developed and is based on these parameters (Table 2). This scoring system has been validated for prediction of rebleeding and mortality, in variceal and non-variceal populations.4 A gen-eral relationship exists between increasing score and increased
© 2008 elsevier Ltd. all rights reserved.
IntensIve care
Algorithm for management of gastrointestinal tract haemorrhage and ischaemia
CT, computed tomography; GI, gastrointestinal; H2RA, histamine 2 receptor antagonist; i.v., intravenous; PPI, proton pump inhibitor; RBL, rubber band ligation;
TIPSS, transjugular intrahepatic portosystemic shunt stenting; US, ultrasound
Haematemesis
MelaenaBleeding per rectum
Suspected upper GI bleed Suspected lower GI bleed
Resuscitation
Initial assessment
Upper GI endoscopy
Treat underlying cause
Airway: consider airway protection
Breathing: adequate ventilation/oxygenation
Circulation: i.v. access, fluid, blood
Non-variceal bleed, e.g. peptic ulcer bleed
Therapeutic endoscopy
• Injection
• Thermal
• Clipping
• Dual therapy
PPI infusion for 72 hours
• Repeat therapeutic endoscopy
• Mesenteric angiogram and embolization
• Sengstaken tube
• Surgery
Prevention
• Helicobacter pylori eradication
• PPI/H2RA for stress ulcer prevention
• Stop offending agent
Prevention
• Beta-blocker
• Nitrates
• Repeat therapeutic endoscopy
• Sengstaken tube
• TIPSS
• Shunt surgery
Therapeutic endoscopy
a Sclerotherapy
b RBL
c Thrombin/fibrin glue
d Terlipressin or octreotide
e Prophylactic antibiotics
f rfVIIa
CT/US Doppler to assess
portal and hepatic
vein patency
Variceal bleed
Rebleed/continued bleed
Normal gastroscopy
History and examination
Rockall score
CT angiography
Previous aortic surgery
Treatment: surgery
Vitamin K
Clotting factors
Platelets
Colonoscopy
Capsule endoscopy
Figure 1
mortality and rebleeds. An initial Rockall score above 0 needs further evaluation and a score >2 is associated with significant mortality. Similarly, patients with a full/complete Rockall score of <3 had a lower risk of death and rebleed. Studies also found that the full Rockall score performed well in predicting death but less well in predicting rebleed; it may be unreliable in patients with higher scores.
anaestHesIa anD IntensIve care MeDIcIne 10:3 13
Other significant risk factors associated with poor outcome include liver disease, being an inpatient, continued bleeding, haematemesis, haematochezia (passage of blood per rectum) and an elevated blood urea.5
Resuscitation: management of GI bleeding begins with the identification and resuscitation of shocked patients. Assessment
2 © 2008 elsevier Ltd. all rights reserved.

IntensIve care
and maintenance of airway patency, adequate ventilation and tissue oxygenation are essential in patients with haemorrhagic shock. High-flow supplemental oxygen should be given to shocked patients. Endotracheal intubation is indicated in patients with airway compromise. It should also be considered in all
Causes of acute upper gastrointestinal bleed
Endoscopic diagnoses Total number of patients
(n = 4137)a (n = 5004)b
Peptic ulcer 35% 36%
Malignancy 4% 4%
varices 4% 11%
Portal hypertensive
gastropathy
– 5%
Mallory–Weiss tear 5% 4%
erosive diseases 11% –
Gastritis/erosion – 22%
erosive duodenitis – 13%
Oesophagitis 10% 24%
vascular ectasia – 3%
Other 6% –
no cause found 25% 17%
aadapted with permission (www.bmj.com).1badapted with permission (www.bsg.org.uk).2
Table 1
anaestHesIa anD IntensIve care MeDIcIne 10:3 13
patients with potential airway compromise before attempting gastroscopy.
Peripheral venous access with at least two large-bore cannulae is traditionally recommended and central venous access should only be attempted by experienced staff if peripheral access is impossible.
Either colloid or crystalloid can be used for initial fluid resus-citation. Vasopressors with invasive blood pressure monitoring are indicated in patients refractory to fluid resuscitation. Terlip-ressin (a vasopressin analogue) should be given to patients with suspected variceal bleeding.
Blood of type O rhesus negative can be used in emergen-cies, but group-specific or ideally cross-matched blood is pref-erable. The current transfusion recommendation in shocked patients with acute UGIB is to maintain the haemoglobin above 10 g/dl.2
Coagulopathy must be corrected with vitamin K, clotting fac-tors or platelet transfusion depending on the nature and sever-ity of the abnormality. Consultation with a haematologist is essential.
Endoscopy: upper oesophago-gastro-duodenoscopy (OGD) is the initial investigation of choice in patients with UGIB and even in patients with suspected lower gastrointestinal bleeding. Gener-ally, it should be performed only after adequate resuscitation.
However, in a minority of patients with extreme shock and continued bleeding, urgent OGD (on-table) under general anaes-thesia is indicated with progression to laparotomy if the bleed-ing cannot be controlled. Mesenteric angiography with selective embolization of the bleeding vessel is an alternative option if the facility is available.
Rockall scoring system
Score
Variable 0 1 2 3
age <60 years 60–79 years ≥ 80 years
shock ‘no shock’;
sBP > 100 mm Hg;
pulse < 100/min
‘tachycardia’;
sBP ≥ 100 mm Hg;
pulse ≥ 100/min
‘Hypotension’;
sBP < 100 mm Hg
Initial
(clinical pre-
endoscopic)
score
co-morbidity no major
co-morbidity
cardiac failure; ischaemic
heart disease; any major
co-morbidity
renal failure;
liver failure;
disseminated
malignancy
Complete
Rockall
Score
Diagnosis Mallory–Weiss tear;
no lesion identified
and no srH
all other diagnoses Malignancy of upper GI
tract
Major srH none, or dark spot
only
Blood in upper GI tract;
adherent clot; visible or
spurting vessel
GI, gastrointestinal; sBP, systolic blood pressure; srH, stigmata of recent haemorrhage.adapted with permission (www.bmj.com).3
Table 2
3 © 2008 elsevier Ltd. all rights reserved.

IntensIve care
Early OGD (within 24 hours) is indicated in high-risk patients, initial Rockall score >2, and in patients with suspected variceal bleeding.
Repeat endoscopy within 24 hours is indicated in patients with a high risk of rebleed or when the initial endoscopy was suboptimal.
Management of specific conditionsPeptic ulcer disease:Therapeutic endoscopy. During endoscopy, bleeding can be con-trolled by injection of epinephrine or sclerosing agents, thermal therapy (cauterization), clipping or rubber band ligation. It is only indicated in high-risk lesions (active arterial bleeding, non-bleeding visible vessels and adherent clot). Combination therapy with injection and thermal treatment is superior to any therapy alone or medical therapy. Metal clipping of the bleeding vessel is an effective treatment but it can be technically difficult.Management of rebleed/continued bleeding. In patients who rebleed or continue to bleed despite endoscopic treatment, the options include repeat therapeutic endoscopy, surgery or mesenteric angiography and embolization. Close discussion between physicians, anaesthetists and surgeons is essential and the optimum management depends on the complexity of the case, local expertise and technical availability.Pharmacotherapy. The aim of acid suppression is to achieve an intragastric pH >6 to stabilize clots and prevent rebleeding. High-dose proton pump inhibitor (PPI) infusion (omeprazole, pantoprazole), 80 mg bolus followed by 8 mg/h for 72 hours after endoscopic haemostatic therapy of high-risk bleeding pep-tic ulcer, reduces rebleeding, the need for surgery and overall mortality.
Agents that may be beneficial, but for which there is insuf-ficient evidence to support their use, include high-dose PPI infu-sion prior to endoscopy, somatostatin and its analogues, and tranexamic acid (fibrinolytic inhibitor).
Secondary prevention of bleeding peptic ulcers includes avoidance of ulcerogenic agents (NSAIDs, steroids, antiplatelet agents, COX 2 inhibitors, SSRIs) if possible, Helicobacter pylori eradication and PPIs. The duration of PPI treatment depends on the underlying cause of the peptic ulcer. Long-term PPI treatment may be indicated if patients need to take ulcerogenic drugs for co-existing medical conditions.
Variceal bleeding:Therapeutic endoscopy. In patients with bleeding oesophageal varices, sclerotherapy or rubber band ligation (RBL) can achieve haemostasis. Current evidence shows RBL is superior to sclero-therapy, but it can be technically difficult. Sclerotherapy can be complicated by deep ulceration and oesophageal stricture.
In patients with bleeding gastric varices, cyanoacrylate glue and thrombin injection are options.Pharmacotherapy. Vasoactive drugs: prior to endoscopy in sus-pected patients with variceal bleeding, studies show that terlip-ressin (1–2 mg 4–8 hourly) and vapreotide (50 μg bolus followed by 50 μg/h for 5 days) significantly improved bleeding control and short-term survival, whereas somatostatin and octreotide did not.5
After endoscopic treatment of variceal bleeding, the addi-tion of vasoactive drugs (terlipressin for 48 hours, octreotide or
anaestHesIa anD IntensIve care MeDIcIne 10:3 13
high-dose somatostatin for 3–5 days) improves haemostasis but does not improve survival, which depends on the severity of the underlying liver disease.5
Antibiotics: several randomized controlled trials have shown that prophylactic antibiotics in variceal bleeds reduce mortality.6 Bac-terial infection is present in 20% of patients with cirrhosis pre-senting with variceal bleeding, and mortality is higher in infected patients. Both cephalosporins and quinolones have shown a ben-efit for prophylaxis.Recombinant factor VIIa (rfVIIa): one study demonstrated that use of rfVIIa, in addition to therapeutic endoscopy and vasoac-tive treatment, was safe and beneficial with regard to bleeding control in a subgroup of patients with advanced cirrhosis (Child–Pugh groups B and C) but did not affect mortality.7
Management of rebleed/continued variceal bleeding. In patients who rebleed or continue to bleed despite a combination of endoscopic therapy and vasoactive treatment, further endo-scopic therapy may be attempted. Tamponade with a Sengstaken tube can achieve temporary haemostasis and can be used as a bridge therapy before definitive endoscopic therapy, transjugu-lar intrahepatic portosystemic shunt stenting (TIPSS) or surgery. TIPSS and shunt surgery are very effective in controlling variceal bleeding by reducing portal hypertension but are associated with significant morbidity and mortality.
Stress ulcer (stress-related mucosal disease):Stress ulceration is a spectrum of conditions ranging from super-ficial erosion to deep ulceration of the upper gastrointestinal mucosa that occurs with extreme physiological stress.
Gut ischaemia, a consequence of profound hypotension, vaso-constriction and proinflammatory cytokines, causes (1) a reduc-tion in bicarbonate secretion, decreased GI motility and acid back-diffusion and (2) disturbances in mucosal microcirculation which impair mucosal defences. This is exacerbated by gastric acid, resulting in acute stress ulceration.
It can be asymptomatic or patients can have overt bleed-ing without haemodynamic compromise or significant bleeding which is associated with hypotension and/or a drop in haemo-globin >2 g/dl.
The incidence of clinically significant bleeding is 1–2.1%. Respiratory failure requiring mechanical ventilation for ≥48 hours and coagulopathy were two strong independent risk factors. Hypotension, sepsis, liver failure, renal failure, glucocorticoids, organ transplant and anticoagulant therapy were also identified as possible risk factors. Patients who have had major surgery, major trauma, severe burns (Curling’s ulcers), head trauma or coma (Cushing’s ulcers) and multiorgan failure also have an increased risk of stress ulceration.
Stress ulcer bleeding is associated with increased mortality and cost, and prolonged stay on an intensive care unit (ICU).Management of stress ulcer bleeding. Stress ulcer bleeding is managed as for peptic ulcer bleeding, but the emphasis of man-agement is centred on prevention of stress ulcers. Stress ulcer prevention reduces bleeding but does not reduce mortality as it is dependent on underlying conditions rather than on the bleed-ing itself.
Optimization of haemodynamic status and pharmacotherapy for gastric acid suppression are an important part of stress ulcer prevention.
4 © 2008 elsevier Ltd. all rights reserved.

IntensIve care
Intravenous ranitidine, a histamine 2 receptor antagonist (H2RA), is the first-line agent for stress ulcer prevention and has been shown to reduce clinically significantly bleeding in a large multicentre randomized controlled trial.8 Ranitidine was more efficacious than sucralfate in stress ulcer prevention but was associated with a non-significant increase in ventilator-associated pneumonia.
PPIs are increasingly used because of better acid suppression and because they are more efficacious than H2RAs in peptic ulcer disease; however, they are not currently recommended for first-line use owing to a lack of good-quality studies on their safety and efficacy in the context of stress ulcer prevention. A PPI can be used as an alternative or is usually continued if patients are already taking one prior to ICU admission.
Enteral nutrition improves blood flow to the stomach and has a mucosal-protective effect. However, as ranitidine still reduces significant bleeding from stress ulceration regardless of enteral nutritional status, the use of enteral nutrition as the only therapeutic agent for stress ulcer prevention is not currently recommended.
Lower gastrointestinal bleed
Epidemiology and aetiologyAcute lower gastrointestinal bleed (LGIB) accounts for approx-imately 25% of patients presenting with GI tract haemor-rhage in hospital, although it is a common problem in primary care.5 Major causes include diverticular disease, haemor-rhoids, inflammatory bowel disease, neoplasia, ischaemic colitis, vascular malformation (angiodysplasia) and radiation enteropathy.5
Haematochezia is the main presenting symptom of lower GI bleeding, but 15% of acute severe haematochezia originates from the upper GI tract.5 A history of weight loss, change in bowel habit, painful defaecation, obstructive bowel symptoms, known inflammatory bowel disease and radiation are clues to a correct diagnosis.5
Initial assessment and resuscitationThere is no formal scoring system in LGIB to predict poor out-come. However, current recommendations based on expert opin-ion suggest that patients aged ≥60 years or those with gross rectal bleeding, shock or significant co-morbidity and those taking aspirin or NSAIDs should be considered for admission (resuscita-tion as for UGIB).
Management of lower gastrointestinal haemorrhageAfter resuscitation, the underlying cause and site of bleeding can be determined by colonoscopy, computed tomography (CT), angiography or nuclear scintigraphy. Colonoscopic haemostatic techniques can effectively control bleeding due to diverticular disease or post-polypectomy bleeding. Mesenteric angiography with selective embolization or surgery (localized bowel resec-tion) may be required in refractory cases.
Miscellaneous causes of bleeding
Aorto-enteric fistula presents with torrential GI bleeding. It is a rare (0.2% cases) but recognized complication of aortic graft
anaestHesIa anD IntensIve care MeDIcIne 10:3 135
surgery. Patients usually present with haematochezia and nega-tive findings on endoscopy. A history of aortic aneurysm repair and abdominal scar are clues and urgent CT angiography is indicated.
Capsule endoscopy is indicated in patients with suspected small bowel bleeding who have negative OGD and colonoscopy.
Gastrointestinal tract ischaemia
GI tract ischaemia plays an important role in the aetiology of stress ulcer disease and ischaemic colitis, and is also a poten-tial complication of mesenteric embolization in patients with GI bleeding refractory to therapeutic endoscopy.
Any forms of shock can induce splanchnic hypoperfusion resulting in ischaemic and reperfusion injury. Gut mucosal permeability is increased and translocation of bacteria, endo-toxin and other mediators will lead to multi-organ dysfunction. Clinical manifestations are stress ulcer bleeding, ileus, isch-aemic hepatitis, ischaemic colitis, acalculus cholecystitis and pancreatitis.
Ischaemic colitis accounts for 19% of LGIB. Patients present with sudden onset of abdominal pain followed by haematochezia. Most cases resolve spontaneously but surgery is indicated for per-sistent symptoms or chronic ischaemic colitis with stricture. ◆
REFEREnCES
1 rockall ta, Logan rF, Devlin HB, northfield tc. Incidence of and
mortality from acute upper gastrointestinal haemorrhage in the
United Kingdom. BMJ 1995; 311: 222–6.
2 British society of Gastroenterology. UK comparative audit of upper
GI bleed and the use of blood. also available at: http://www.bsg.
org.uk/pdf_word_docs/blood_audit_report_07.pdf (accessed 2007).
3 rockall ta, Logan rF, Devlin HB, northfield tc. risk assessment
after acute upper gastrointestinal haemorrhage. Gut 1996; 38:
316–21.
4 vreeburg eM, terwee cB, snel P. validation of the rockall risk
scoring system in upper gastrointestinal bleeding. Gut 1999; 44:
331–5.
5 scottish Intercollegiate Guidelines network. Management of acute
upper and lower gastrointestinal bleeding. also available at:
http://www.sign.ac.uk/guidelines/fulltext/105/index.html (accessed
sep 2008).
6 soares-Weiser K, Brezis M, tur-Kaspa r, Leibovici L. antibiotic
prophylaxis for cirrhotic patients with gastrointestinal bleeding.
Cochrane Database Syst Rev 2002 Issue 2, art. no.: cD002907.
7 Bosch J, thabut D, Bendtsen F. recombinant factor vIIa for upper
gastrointestinal bleeding in patients with cirrhosis: a randomized,
double-blind trial. Gastroenterology 2004; 127: 1123–30.
8 cook D, Fuller H, Guyatt G. risk factors for GI bleed in critically ill
patients. N Engl J Med 1994; 330: 377–81.
FURThER REAdInG
British society of Gastroenterology. UK guidelines on the management
of variceal haemorrhage in cirrhotic patients. also available at:
http://www.bsg.org.uk/pdf_word_docs/vari_hae.pdf (accessed 2000).
© 2008 elsevier Ltd. all rights reserved.

IntensIve care
British society of Gastroenterology endoscopy committee. Guidelines
for non-variceal upper gastrointestinal haemorrhage. also
available at: http://www.bsg.org.uk/pdf_word_docs/nonvar3.pdf
(accessed 2002).
scottish Intercollegiate Guidelines network. Management of acute
upper and lower gastrointestinal bleeding. also available at:
anaestHesIa anD IntensIve care MeDIcIne 10:3
http://www.sign.ac.uk/guidelines/fulltext/105/index.html (accessed
sep 2008).
cook D, Heyland D, Marshall J. On the need for observational studies
to design and interpret randomised trials in IcU patients. a case
study in stress ulcer prophylaxis. Intensive Care Med 2001; 27:
347–54.
136 © 2008 elsevier Ltd. all rights reserved.