Gastroesophageal Reflux Disease (GERD) Dr. Kairu S. M.
42
Gastroesophageal Gastroesophageal Reflux Disease Reflux Disease (GERD) (GERD) Dr. Kairu S. M. Dr. Kairu S. M.
-
Upload
esmond-emery-cole -
Category
Documents
-
view
223 -
download
1
Transcript of Gastroesophageal Reflux Disease (GERD) Dr. Kairu S. M.
- Slide 1
- Slide 2
- Gastroesophageal Reflux Disease (GERD) Dr. Kairu S. M.
- Slide 3
- Gastro-oesophageal reflux disease (GORD): Abnormal reflux of gastric juice (acid and bile) into the oesophagus leading to symptoms Pathological reflux ranges from simple to erosive to Barretts Non-erosive reflux disease (NERD): Reflux disease in which erosion does not occur Heartburn: Burning retrosternal pain radiating upward due to exposure of the oesophagus to acid Oesophagitis: Endoscopically demonstrated damage to the oesophageal mucosa GERD - Definitions
- Slide 4
- Prevalence. Increased prevalence last 10 years. Increased prevalence last 10 years. Accompanied increase in adenocarcinoma lower esophagus. Accompanied increase in adenocarcinoma lower esophagus. Obesity associated with increased GERD. Obesity associated with increased GERD.
- Slide 5
- Anti Reflux Mechanism(ARM) This has both:- This has both:- (1) Anatomical. (1) Anatomical. (2) Functional. (2) Functional.
- Slide 6
- Anatomical. The lower esophageal sphincter (LES) at the OG junction consists of tonically contracted smooth muscle at approx. 8-20 mmHg above the gastric pressure. The lower esophageal sphincter (LES) at the OG junction consists of tonically contracted smooth muscle at approx. 8-20 mmHg above the gastric pressure. The outside (extrinsic) compression at the OG junction from the crural diaphragm. The outside (extrinsic) compression at the OG junction from the crural diaphragm. Sharp angle- entry of esophagus into stomach (angle of His). Sharp angle- entry of esophagus into stomach (angle of His).
- Slide 7
- Slide 8
- TLESR (Transient Lower Esophageal Sphincter Relaxations) A normal phenomenon in healthy individuals. A normal phenomenon in healthy individuals. Dominant mechanism of pathological reflux. Dominant mechanism of pathological reflux. Too frequent TLESRs. Too prolonged TLESRs.
- Slide 9
- Functional. Esophageal peristalsis that serves to clear luminal contents into the stomach. Esophageal peristalsis that serves to clear luminal contents into the stomach. Secretion and swallowing of saliva to neutralize the acid and enhance clearance. Secretion and swallowing of saliva to neutralize the acid and enhance clearance. Prompt Gastric emptying. Prompt Gastric emptying.
- Slide 10
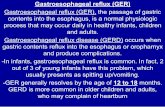
- Impaired mucosal defence salivary HCO 3 Hiatus hernia Impaired LOS (smoking, fat, alcohol) transient LOS relaxations basal tone H + Pepsin Bile and pancreatic enzymes oesophageal clearance of acid (lying flat, alcohol, coffee) acid output (smoking, coffee) intragastric pressure (obesity, lying flat) bile reflux gastric emptying (fat) Pathophysiology of GERD
- Slide 11
- Symptoms.
- Slide 12
- Heartburn and Regurgitation are the two cardinal symptoms of GERD. Heartburn and Regurgitation are the two cardinal symptoms of GERD. Others:- Others:- (1) Dysphagia-due to peptic stricture or (1) Dysphagia-due to peptic stricture or peristaltic dysfunction. peristaltic dysfunction. (2) Chest pain (NCCP). (2) Chest pain (NCCP). (3) Water brash. (3) Water brash. (4) Globus Sensation. (4) Globus Sensation. (5) Odynophagia. (5) Odynophagia.
- Slide 13
- Extra Esophageal Manifestations. 1. Asthma. 1) Microaspiration. 2) Vagal reflex activation. 2. Laryngitis. Complications of GERD. Complications of GERD. a) Bleeding. b) Stricture. c) Barrets esophagus adenocarcinoma
- Slide 14
- Role of Endoscopy in GERD. Confirm diagnosis of GERD - erosions/ulcerations. Confirm diagnosis of GERD - erosions/ulcerations. Diagnose endoscopy-negative reflux. Diagnose endoscopy-negative reflux. Exclude other causes of esophagitis/ Exclude other causes of esophagitis/ odynophagia e.g.Candida, Herpes Simplex. Diagnose complications of chronic GERD e.g Barrets esophagus, stricture, adenocarcinoma. Diagnose complications of chronic GERD e.g Barrets esophagus, stricture, adenocarcinoma.
- Slide 15
- 1.Savary-Miller classification. 1. Solitary erythematous /erosions covering one mucosal fold. 2. Solitary erythematous /erosion covering more than one mucosal folds but not circumferential. 3. Circumferential erythematous / erosions. 4. Complications Ulcers. Ulcers. Strictures. Strictures. Barretts esophagus. Barretts esophagus.
- Slide 16
- Slide 17
- Slide 18
- Grade I
- Slide 19
- Grade 1
- Slide 20
- Grade 2
- Slide 21
- Slide 22
- Slide 23
- Grade 3
- Slide 24
- Grade 4
- Slide 25
- Slide 26
- Slide 27
- Grade 4.
- Slide 28
- Modes of Treatment Proton Pump Inhibitors Proton Pump Inhibitors Longer acting PPIs. Adverse events/effects of PPIs. Potassium competitive acid blockers (PCABs) Potassium competitive acid blockers (PCABs) Motility agents. Motility agents. GABA agonists Endoscopic therapy Endoscopic therapy Full-thickness plication
- Slide 29
- The Step up Approach. PPI PPI LOW DOSE PB. LOW DOSE PB. H2RA +PROKINETIC. H2RA OTC ANTACIDS + LIFESTYLE ADVICE.
- Slide 30
- The Step Down Approach. PPI PPI LOW DOSE PB. LOW DOSE PB. H2RA +PROKINETIC. H2RA +PROKINETIC. H2RA+LIFESTYLE ADVICE. H2RA+LIFESTYLE ADVICE. OTC ANTACIDS. OTC ANTACIDS.
- Slide 31
- Long Term Therapy. Many patients, GERD a chronic relapsing problem because the underlying motor abnormalities persist. Many patients, GERD a chronic relapsing problem because the underlying motor abnormalities persist. PPIs. PPIs. Majority of patients require PPI even in low doses. Majority of patients require PPI even in low doses. Occasional patients may require high doses (double dose of PPI to control symptoms.) Occasional patients may require high doses (double dose of PPI to control symptoms.) Nocturnal acid breakthrough. Nocturnal acid breakthrough.
- Slide 32
- Surgery in GERD Nissan Fundoplication Surgery in GERD Nissan Fundoplication 40-50% have required medical treatment after surgery. 40-50% have required medical treatment after surgery. High failure rate. Mortality operator dependent. Mortality operator dependent. Morbidity / complications: ~ 10% dysphagia requiring repeated esophageal dilatation. Morbidity / complications: ~ 10% dysphagia requiring repeated esophageal dilatation.
- Slide 33
- Potential Risks of Chronic PPI Therapy Hypergastrinemia, carcinoids Hypergastrinemia, carcinoids Gastritis, intestinal metaplasia, gastric cancer Gastritis, intestinal metaplasia, gastric cancer Achlorhydria and loss of gastric sterility Achlorhydria and loss of gastric sterility Increased enteric infections, C, difficile. Increased enteric infections, C, difficile. N-nitrosamine and carcinogen risk N-nitrosamine and carcinogen risk Community =acquired pneumonia Community =acquired pneumonia Safety during pregnancy /lactation Safety during pregnancy /lactation Drug interactions. Drug interactions.
- Slide 34
- Potential Risks of Chronic PPI Therapy Hypergastrinemia, carcinoids RATS Elevated gastrin ECL cell hyperplasia ECL cell carcinoid tumors HUMANS Elevated gastrin ECL cell hyperplasia NO CARCINOID TUMORS Species specific problem (rat) Up to 8 year continuous use in patients (as of 2000)
- Slide 35
- Potential Risks of Chronic PPI Therapy Achlorhydria, N-nitrosamine generation The RISKThe REALITY Achlorhydria permits growth of bacteria that can convert nitrates to nitrites to N- nitrosamine (carcinogen) Increased UGI bacteria has been detected in PPI takers. N-nitrosamine formation is also catalyzed by acid. Data on PPI use and increased gastric N-nitrosamine remain uncertain and the cancer risk is speculative
- Slide 36
- Potential Risks of Chronic PPI Therapy Achlorhydria, enteric infection The RISK The REALITY Achlorhydria disables the gastric barrier to ingested pathogens Case-control study: Small increase in enteric infections with PPIs for 2 months. Relative risk 1.6 (Cl 1.0-2.4) PPPI use is independent risk of C. difficile diarrhea in antibiotic users. PPI use OR 2.1 (Cl 1.2-3.5) 3 AB OR 2.1 (Cl 1.3-3.4) Medical ward OR 4.1 (Cl 2.3-7.3) Only occasional cases of enteric infections in patients taking PPIs have been reported. Garcia Rodriguez LA et al. Epidemiol 1997:8:571-4, Dial S et al CMAJ 2004: 171: 33-8
- Slide 37
- Potential Risks of Chronic PPI Therapy Community acquired pneumonia The RISKThe REALITY Gastric colonization followed by reflux and aspiration of gastric contents results in pneumonia Case-control Dutch primary case database 1/1/95-12/31/2002. 364,683 Individuals 5551 1st Pneumonias PPI user risk 0.60/100 pt yrs Nested case control analysis to reduce confounding effects of indication Non-PPI user risk 0.60/100 pt yrs Adjusted OR all 1.27 (Cl 1.06-1.54) Adjusted OR PPI 1.73 (Cl 1.33-2.25) Association does not prove causation PPI takers are also more likely to smoke, drink, be obese, have GERD, and ?? (note how OR 4.08 dwindled to 1.73) Laheji RJ et al. JAMA 2004: 292: 1955-60
- Slide 38
- Potential Risks of Chronic PPI Therapy Safety during pregnancy/lactation The RISKThe REALITY Omeprazole crosses placenta, category C; Other PPIs category B A.controlled human studies no risk. B.animal studies or, adverse fetal. C.no adequate studies or, adverse fetal effects in animals at some dose. D.evidence of fetal risk: benefit > risk X.Evidence of fetal risk: benefit < risk 1992-2001 prospective controlled evaluation of PPI gestational exposures Omeprazole: 247 births 3.6% major anomalies. Lansoprazole: 50 births, 3.9% MA Pantoprazole: 48 births, 2.1% MA Controls: 787 births, 3.8%MA European Network of Teratology Information Servicesthe PPIs do not represent a major teratogenic risk in humans Diav-Citrin O et al, Aliment Pharmacol Ther 2005: 21: 269-75
- Slide 39
- PPIs: Adverse Events/Effects Clopidogrel Clopidogrel Prospective studies of platelet aggregation. Retrospepctive studies of clinical outcomes. Randomized, double-blind trail of PPI vs placebo among clopidogrel users. No difference in cardiac events, mortality No difference in cardiac events, mortality Significant reduction in GI events with PPI Significant reduction in GI events with PPI
- Slide 40
- GABA Agonist Baclofen Baclofen 40mg Baclofen 40mg Reduced TLESRs in patients with GERD Reduced esophageal acid exposure Limitations Limitations CNS side-effects mainly drowsiness. Short half-life. Van Herwaarden et al. Aliment Phar,acol Ther 2002
- Slide 41
- New motility agent (GABA Agonist) Lesogaberan Lesogaberan a peripheral acting GABA agonist. Lesogaberan a peripheral acting GABA agonist. Study showed 35% in TLESR. Study showed 35% in TLESR. A potential agent for treatment of GERD as co- therapy. A potential agent for treatment of GERD as co- therapy.
- Slide 42
- Summary PPIs remain the standard treatment for GERD. PPIs remain the standard treatment for GERD. Well established to be very safe. Well established to be very safe. Prevalence of GERD increasing with increase in lower esophageal adenocarcinoma. Prevalence of GERD increasing with increase in lower esophageal adenocarcinoma. New motility drugs in development Lesogaberan. New motility drugs in development Lesogaberan.
- Slide 43
- THE END