Gastro Intestinal Bleeding By: Abdulrahman Sindi ED Resident.
20
Gastro Intestinal Bleeding By: Abdulrahman Sindi ED Resident
-
Upload
brice-garrett -
Category
Documents
-
view
221 -
download
5
Transcript of Gastro Intestinal Bleeding By: Abdulrahman Sindi ED Resident.
Gastro Intestinal BleedingBy: Abdulrahman Sindi
ED Resident

Case ScenarioA 55-year-old male not known to have any
medical illness, presented to the E.D. complaining of blood in his vomitus two times this day.
HR:120
BP:95/60
RR:22
T:36.7

Is the patient stable?
What should be done for this patient?
What are initial steps in the management?
Epidemiology GI bleeding is relatively common problem
encountered in ED
The mortality rate is is approximately 10%
UGIB affects 50-150 people per 100,000 each year
Mean age of affected people with GIB is 59 years
UGIB is more common in men, whereas LGIB is more common in women
UGIB admission is more common in adults whereas LGIB admission is more common in children

Differential Considerations

Differential ConsiderationsUpper Lower
Peptic ulcer disease
diverticulosis
Gastric erosions
angiodysplasia
varices UGIB
Mallory-Weiss tear
Cancer/polyp
esophagitis Rectal disease
duodenitis IBD
Upper Lower
esophagitis Anal fissure
gastritis Infectious colitis
ulcer IBD
Esophageal varices
polyps
Mallory-Weiss tear
intussusception
Adult Children
• In children less than 2 years of age massive LGIB is most often due to Meckels diverticulum or intussusception
Rapid Assessment and Stabilization
Patients with suspected GIB who are hemodynamically unstable should be stabilized and evaluated rapidly. Undress and place cardiac and oxygen saturation
monitors. Give supplemental oxygen. 2 large bore peripheral intravenous lines. Take blood for (CBC, PT, type and screen or crossmatch). Give bolus crystalloid. Give type O, type specific or crossmatched blood. Consult the GE in UGIB or surgeon in LGIB if persistently
unstable.
History Hematemesis:: vomiting of blood that occurs in
bleeding of the esophagus, stomach, or proximal bowel (50% in UGIB).
Melena: black tarry stool that results from the presence of 150-200 ml of blood for prolonged period (70% in UGIB and 33% in LGIB).
Hematochezia:
History Hematemesis: vomiting of blood that occurs in
bleeding of the esophagus, stomach, or proximal bowel (50% in UGIB).
Melena: black tarry stool that results from the presence of 150-200 ml of blood for prolonged period (70% in UGIB and 33% in LGIB).
Hematochezia: bright red blood in the stool that mostly occurs with LGIB but can occur in UGIB (66% in LGIB and 10-15% in UGIB).
History Duration, quantity, associated symptoms,
previous history, medications, alcohol, and associated medical illness
Physical ExaminationVitals: hypotension, tachycardia or postural
change in heart rate.
General exam: general appearance, mental status, skin signs and abdomin should be assessed carefully.
Rectal exam: it’s the key to confirm the diagnosis, it does not exclude the diagnosis if negative

Ancillary Testing Occult blood test: it may have positive result 14
days after a major bleed, it has a false positive and negative results,
Clinical labs: CBC, coagulation profile, type and screen and crossmatch
ECG: should be done to all patients over 50, preexisting cardiac insult, anemia, chest pain, S.O.B., persistent
Imaging: CXR if perforation is suspected
Management Reassurance
N.G. tube and gastric lavage:Aspiration of bloody content diagnoses UGIB, but it
does not determine if it is ogoingFalse negative results are possible if if bleeding is
intermittent, in duodenal bleed, pyloric spasm.False positive occurs in nasal bleeding.The presence of bile in excludes the possibility of
UGIB.Gastric lavage is helpful to prepare for endoscopyLavage should not performed in pneumoperitoneum.
Management Anoscopy/proctosigmoidoscopy.
Endoscopy: It identifies lesion in 78% to 95% if done within 12
to 24 hours.
Angiography and tagged RBC scan:Angiography is commonly used in LGIBDetects 40% of LGIB site. It is performed ideally in active bleeding. In undetected bleeding tagged RBC scan is
performed.
Management Proton pump inhibitors
Octreotide
Vasopressin
Sengstaken-Blakmore Tube: Stops bleeding in 80% of esophageal varices. Indicated when endoscopy is not readily available and
vasopressin has not slowed the bleeding.
Surgery: Indicated in for all hemodynamically unstable with
active bleeding unresponsive to resuscitation
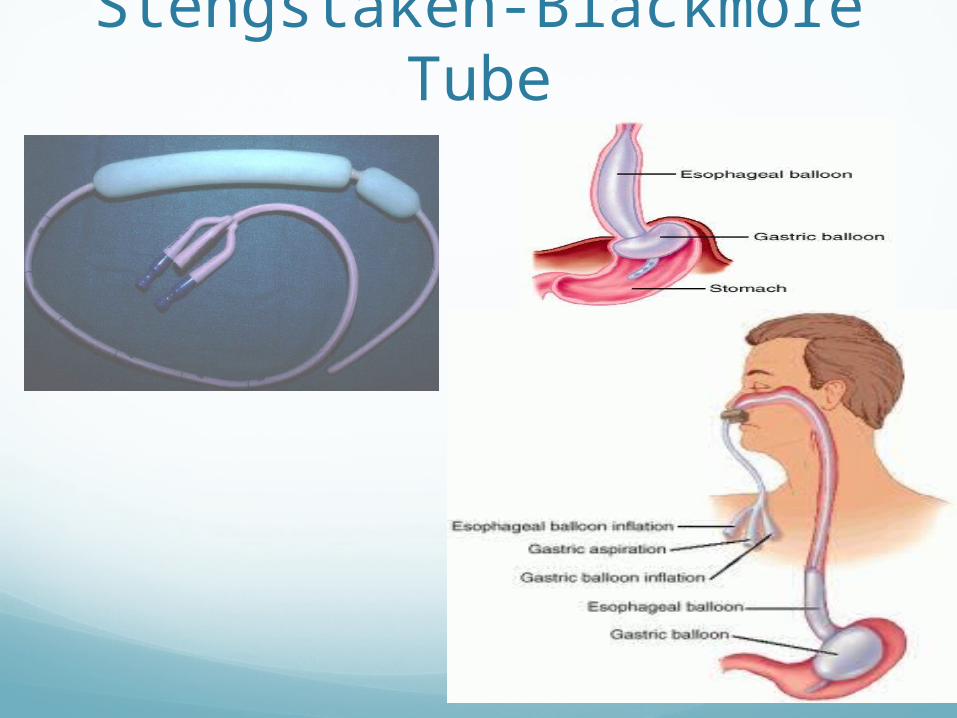
Stengstaken-Blackmore Tube

DispositionVery low criteria for GIB patients
No comorbid diseaseNormal vitalsNegative guaiac testNegative gastric aspirationNormal hemoglobin/hematocritProper understanding for signs and symptoms Immediate access to ERArranged follow up within 24 hours
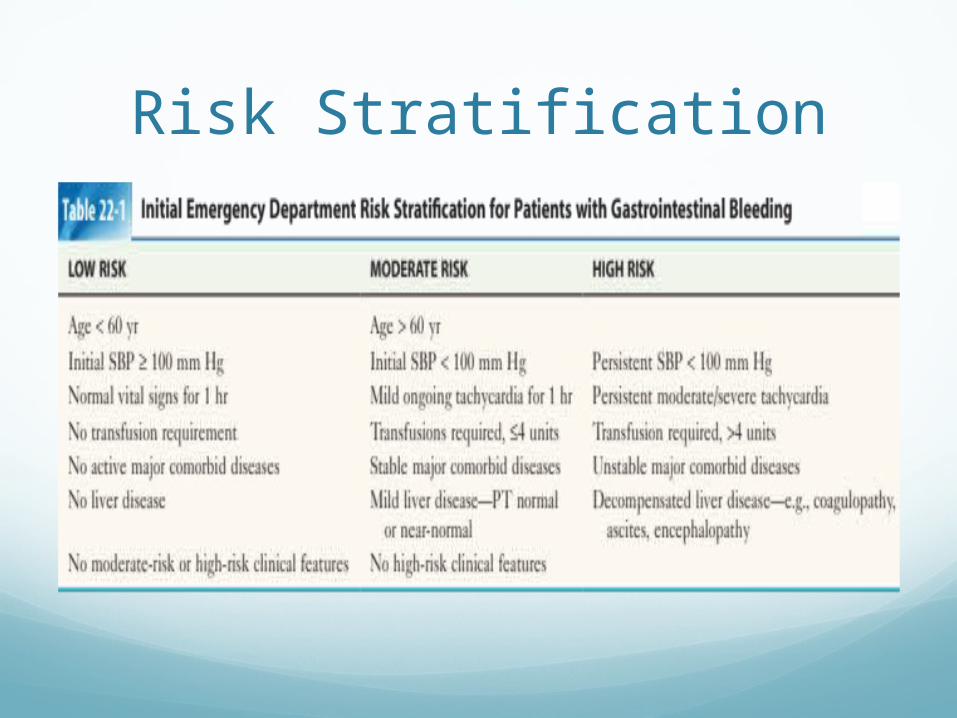
Risk Stratification
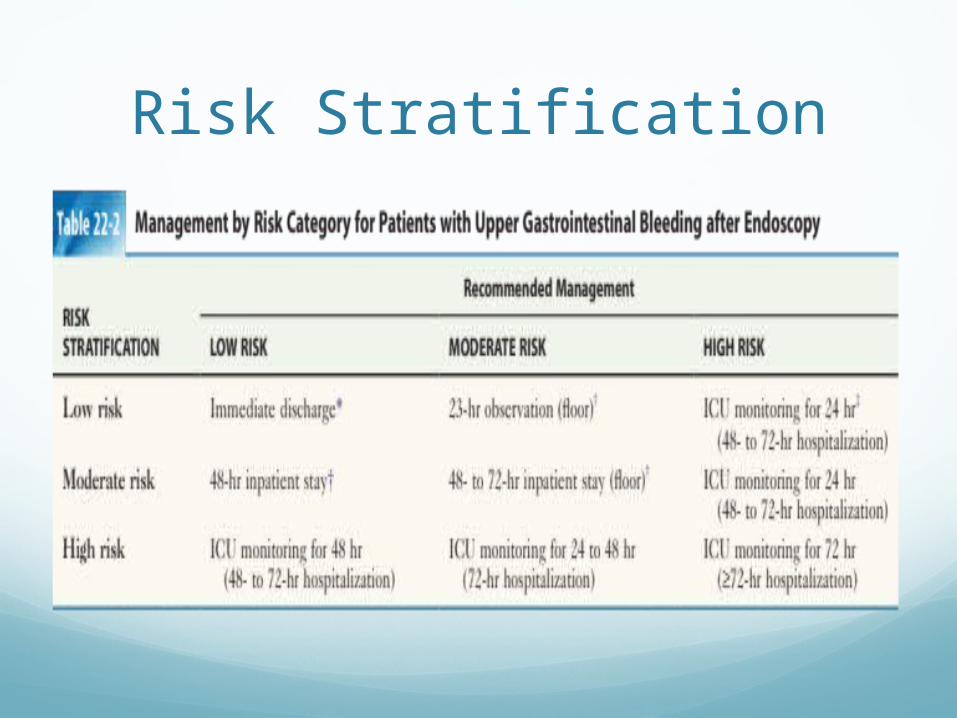
Risk Stratification
L
Thank YouBy Dr. Abdulrahman Sindi