Gary G. Gintner, Ph.D., LPC-S, Bezdek Candidate, Smith, S ...
21
Gary G. Gintner, Ph.D., LPC-S, Bezdek, M. T., Master’s Candidate, Smith, S. E., Master’s Candidate, & Mecholsky, S., Master’s Candidate Louisiana State University, Baton Rouge, LA
Transcript of Gary G. Gintner, Ph.D., LPC-S, Bezdek Candidate, Smith, S ...
Gary G. Gintner, Ph.D., LPC -S, Bezdek, M. T., Master’s Candidate, Smith, S. E., Master’s Candidate, & Mecholsky, S., Master’s Candidate
Louisiana State University, Baton Rouge, LA
• Why add new disorders and specifiers?
• Poor coverage
• Overuse of NOS
• Categories vs. spectrums
• Treatment response
• Issues in identifying effective treatments
Introduction
• Guiding principles:
• Evidence-based
• Feasible to implement
• Shares continuity with current manual
• Steps in the Approval Process
• DSM-5 Work Group reviews the extant data on the topic
• A rationale for the addition is provided based upon the data
• DSM-5 field trial data is reviewed
• Two outside committees review the evidence
• APA’s Board of Trustees vote (November, 2012)
Steps in Adding a New Disorder
Winners Losers
Mixed Anxiety-Depressive Disorder
Hypersexual Disorder
Attenuated Psychosis Syndrome
Alternative Model for Personality Disorders
Nonsuicidal Self-Injury
Autisms Spectrum Disorder
Social Communication Disorder
Disruptive Mood Dysregulation Disorder
Persistent Depressive Disorder
Premenstrual Dysphoric Disorder
Hoarding Disorder
Excoriation Disorder
Avoidant Restrictive Food Intake Disorder
Binge-Eating Disorder
Neurocognitive Disorders
Proposed Disorders: Winners and Losers
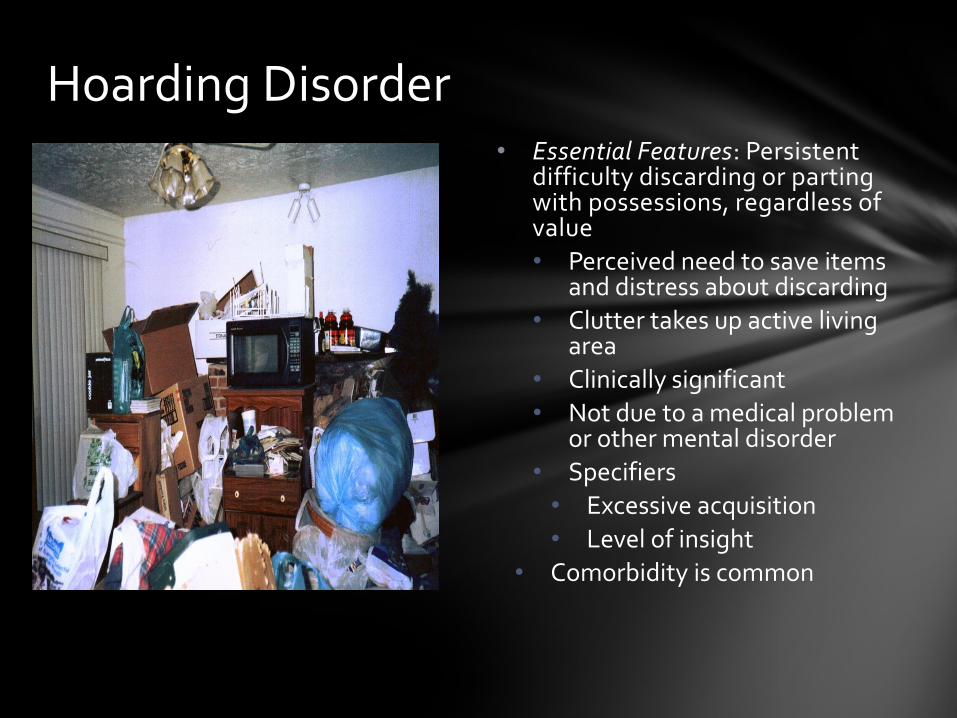
• Essential Features: Persistent difficulty discarding or parting with possessions, regardless of value
• Perceived need to save items and distress about discarding
• Clutter takes up active living area
• Clinically significant
• Not due to a medical problem or other mental disorder
• Specifiers
• Excessive acquisition
• Level of insight
• Comorbidity is common
Hoarding Disorder

• Predisposing factors
• Genetics
• Family environment and attachment issues
• Maladaptive cognitive processes
• Cognitive distortions associated with possessions
• Frequent stressful events
• Precipitating factors
• Stressful events (especially loss events)
• Chronic stress
• Perpetuating factors
• Poor insight and low motivation to change
• Behavioral avoidance
Understanding Hoarding Disorder
• Treatments that don’t work:
• Behavior therapy (exposure and response prevention)
• SSRI’s
• First line treatment: Cognitive-Behavior Therapy (CBT; Steketee & Frost, 2007)
• Psychoeducation
• Motivational interviewing, especially early
• Cognitive restructuring
• Skills training (decision making, organizing, and problem solving)
• Identifying barriers and reinforcing successive approximations
• Relapse prevention
• Other
• Practical assistance
• Home visits
• Online support
Treating Hoarding Disorder (Tolin, 2011; Muroff et al., 2013; )
• Essential feature: Recurrent episodes of binge eating in which there is a sense of lack of control • At least three ways eating is
disturbed • Not part of Anorexia or
Bulimia and no compensatory behaviors
• Severity rating based upon the number of binges per week
Binge-Eating Disorder (BED)
•Predisposing factors
• Genetics
• Environmental factors
• Demographic profile
• Precipitating factors
• Comorbid psychiatric disorders
• Concerns about body weight and shape
• Perpetuating factors
• Cognitive distortions about body weight/shape
• Metabolic syndrome
• Quality of life issues
• Obesity vs. BED
Understanding BED
•First line treatment: CBT tailored to BED
• Psychoeducation: Dieting, healthy eating and exercise
• Self-monitoring binges/urges
• Identify non-eating coping behaviors
• Cognitive restructuring for maladaptive thinking
• Relapse prevention
• Treatment of comorbid disorders
• Second line treatments
• Interpersonal Therapy
• Dialectical Behavior Therapy
• Role of medications
Treating BED (APA, 2006;Grilo et al., 2012)
• Essential feature: Severe temper outbursts with underlying persistent angry or irritable mood
• Outburst frequency: 3x or more a week
• Duration: At least 12 months
• Severity: Present in two settings and severe in at least one
• Onset: Before 10 but do not diagnose before age 6
• Rule-outs: Bipolar, ASD, ODD, CD and Intermittent Explosive Disorder
Disruptive Mood Dysregulation Disorder
• Predisposing factors
• Neurological abnormalities
• Early disruptive behavior disorders: AHDHD, ODD and CD
• Family Stress
• Precipitating
• Frustrated goal attainment
• Negative interpersonal cycles
• Perpetuating
• Comorbid anxiety and depression
• Low educational attainment
• Legal problems
• Stressful home environment
Understanding DMDD

Issues with DMDD
Was it ready for prime time?
What are the treatment implications?
• No empirically supported treatments
• Avoid bipolar medications
• Consider CBT treatments used for depression in children (Waxmonsky et al., 2012):
• Coping skills for thoughts, feelings and behavior
• Parent training
• Parent support group
• Essential feature: Depression that persists for two years or longer (one year or longer in children and adolescents)
• May include major depressive episodes
• Course specifiers:
• With pure dysthymic syndrome
• With persistent major depressive episode
• With intermittent major depressive episodes, with current episode
• With intermittent major depressive episodes, without current episode
Persistent Depressive Disorder
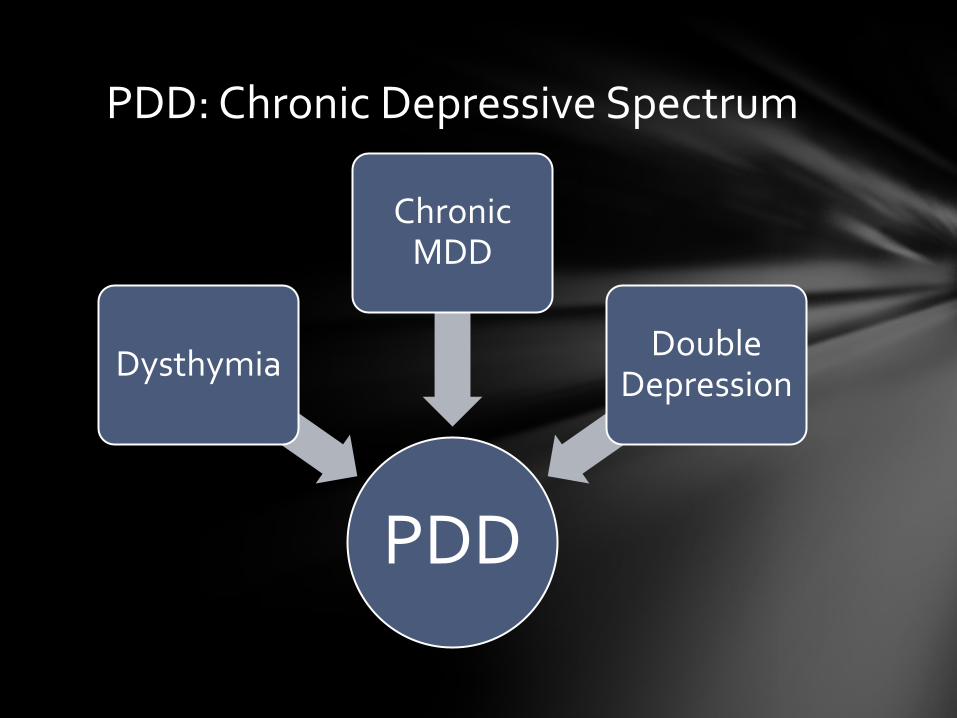
PDD
Dysthymia
Chronic MDD
Double Depression
PDD: Chronic Depressive Spectrum
• Chronic vs. non-chronic forms of depression
• Predisposing factors for PDD
• Genetics
• Early loss, separation and maladaptive parenting
• Personality traits (Negative affectivity, introversion)
• Depressogenic thinking
• Precipitating factors
• Loss event
• Stressful life events (e.g., medical condition, care-giving)
• Perpetuating
• Thinning interpersonal networks
• Chronic stress
• Comorbidity
Understanding PDD
• Treatment outcome for PDD vs. MDD
• Acute Phase Treatments
• Combination of psychotherapy plus meds are superior to either alone
• Indications for psychotherapy:
• History of childhood adversity
• Maladaptive personality traits
• Onset due to a stressful life event or interpersonal problems
• Empirically supported psychotherapies for chronic depression
• CBT
• IPT
• Continuation and Maintenance Phase
Treatment Considerations for PDD (APA, 2010; Klein & Black, 2013)
• Why note subtypes and specifiers?
• New specifiers for Bipolar Disorders and Depressive Disorder:
• With Anxious Distress
• With Mixed Features
• With Peripartum Onset
• Conduct Disorder
• With Limited Prosocial Emotions
• PTSD
• With Dissociative Symptoms
New Specifiers for Selected DSM-5 Disorders

• Sources for practice guidelines:
• National Guidelines Clearinghouse
• American Psychiatric Association
• American Academy of Child and Adolescent Psychiatry
• Keep up with the changes
Final Comments
Alexson, D., Findling, R. L., Fristad, M. A., Kowatch, R. A., Youngstrom, E. A., Horwitz, S. M., Arnold, L. E., Frazier, T. W., Ryan, N., Demeter, C., Gill, M. K., Hauser-Harrington, J. C., Depew, J., Kennedy, S. M., Gron, B. A., Rowles, B. M., & Birmaher, B. (2012). Examining the proposed disruptive mood dysregulation disorder diagnosis in children in the longitudinal assessment of manic symptoms study. Journal of Clinical Psychiatry, 73(10), 1342-1350. doi: 10.4088/JCP012m07674.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington DC: American Psychiatric Association.
American Psychiatric Association. (2010). Practice guidelines for the treatment of major depressive disorder, third edition. [Supplement]. American Journal of Psychiatry. 167(10). doi:10.1176/appi.books.9780890423387.654001
Colins, O. F., & Vermeiren, R. R. J. (2013). The usefulness of DSM-IV and DSM-5 conduct disorder subtyping in detained adolescents. The Journal of Nervous and Mental Disease, 201(9), 736-743. doi:10.1097/NMD.0b013e3182a20e94
Copeland, W. E., Angold, A., Costello, E., & Egger, H. (2013). Prevalence, comorbidity, and correlates of DSM -5 proposed disruptive mood dysregulation disorder. American Journal of Psychiatry, 170(2), 173-179.
Copeland, W. E., Shanahan, L., Egger, H., Angold, A., & Costello, E. J. (2014). Adult diagnostic and functional outcomes of DSM -5 disruptive mood dysregulation disorder. American Journal of Psychiatry, 171(6), 668-674.
Choate, L. H., & Gintner, G. G. (2011). Prenatal depression: Best practices for diagnosis and treatment. Journal of Counseling and Development,84, 373-382.
Davis, C., and J.C. Carter. (2009). Compulsive overeating as an addiction disorder: A review of theory and evidence. Appetite, 53, 1-8.
Deveney, C. M, Connolly, M. E., Haring, C. T., Bones, B. L., Reynolds, M. S., Kim, P., Pine, D. S., & Leibenluft, E. (2013). Neural mechanisms of frustration in chronically irritable children. American Journal of Psychiatry, 170(10), 1186-1194.
Gintner, G. G. (In press). DSM-5 conceptual changes: Innovations, limitations and clinical implications. The Professional Counselor.
Grilo, C. M., Masheb, R. M., & Crosby, R. D. (2012). Predictors and moderators of response to cognitive behavioral therapy and medication for the treatment of binge eating disorder. Journal of Counseling and Clinical Psychology, 80(5), 897-906. doi: 10.1037/a0027001
Guerdjikova, A. I., McElroy, S. L., Winstanley, E. L., Nelson, E. B., Mori, N., McCoy, J., Keck, P. E., & Hudson, J. I. (2012). Duloxetine in the treatment of binge eating disorder with depressive disorders: A placebo -controlled trial. International Journal of Eating Disorders, 45(2), 281-289. doi: 10.1002/eat.20946
References
Klein, D. N. & Black, S. R. (2013). Persistent depressive disorder: Dysthymia and chronic depression. In W. E. Craighead, D. J. Miklowitz, & L. W. Craighead (Eds.), Psychopathology: History, diagnosis, and empirical foundations (pp. 334- 355). Hoboken, New Jersey: John Wiley & Sons.
Margulies, D. M., Weintraub, S., Basile, J., Grover, P. J., & Carlson, G. A. (2012). Will disruptive mood dysregulation disorder reduce false diagnosis of bipolar disorder in children? Bipolar Disorders, 14, 448-496. doi: 10.1111/j.1399-5618.2012.01029.x
Mikita, N., & Stringaris, A. (2013). Mood dysregulation. European Child & Adolescent Psychiatry, 22, 11-16. doi:10.1007/s00787-012-0355-9
Muroff, J., Bratiotis, C., & Steketee, G. (2011). Treatment for hoarding behaviors: A review of the evidence. Clinical Social Work Journal, 39, 406-423. doi: 10.1007/s10615-010-0311-4
Muroff, J., Steketee, G., Bratiotis, C., & Ross, A. (2012). Group cognitive and behavioral therapy and bibliotherapy for hoarding: A pilot trial. Depression and Anxiety, 29, 597-604. doi: 10.1002/da.219253
National Institute for Clinical Excellence (NICE). (2009). Eating Disorders —Core interventions in the treatment and management of anorexia.
Rheberger, D. & Grahaam, R. (2013). The re-labelling of dysthymic disorder to persistent depressive disorder in DSM -5: Old wine in new bottles. Psychiatry, 27, 27-31.
Sharma, V., & Mazmanian, D. (2014). The DSM-5 peripartum specifier: Prospects and pitfalls. Archive of Women’s Mental Health. doi: 10.1007/s00737-013-0406-3
Steketee, G. & Frost, R. O. (2007). Compulsive hoarding and acquiring: A therapist guide . New York, NY: Oxford University Press.
Tolin, D. F. (2011). Challenges and advances in treating hoarding. Journal of Clinical Psychology: In Session, 67(5), 451-455. doi: 10.1002/jclp.20796.
Waxmonsky, J., Wymbs, F., Pariseau, M., Belin, P., Waschbusch, D., Babocsai, L., & ... Pelham, W. (2012). A novel group therapy for children with ADHD and severe mood dysregulation. Journal of Attention Disorders, XX(X), 1-15.