Future comparative effectiveness studies: unanswered questions in the care of IBD patients
45
Future comparative effectiveness studies: unanswered questions in the care of IBD patients Jean-Frédéric Colombel Icahn School of Medicine at Mount Sinai New York, USA
description
Future comparative effectiveness studies: unanswered questions in the care of IBD patients. Jean- Frédéric Colombel Icahn School of Medicine at Mount Sinai New York, USA. Disclosure. J-F Colombel has served as consultant, advisory board member or speaker for or - PowerPoint PPT Presentation
Transcript of Future comparative effectiveness studies: unanswered questions in the care of IBD patients

Future comparative effectiveness studies: unanswered questions
in the care of IBD patients
Jean-Frédéric ColombelIcahn School of Medicine at Mount Sinai
New York, USA

Disclosure
J-F Colombel has served as consultant, advisory board member or speaker for or received research grants from
Abbvie, Amgen, Bristol Meyers Squibb, Celltrion, Ferring, Genentech, Giuliani SPA, Given Imaging, Janssend and Janssen, Merck & Co., Millenium Pharmaceuticals Inc., Nutrition Science Partners Ltd., Pfizer Inc. Prometheus Laboratories, Sanofi, Schering Plough Corporation, Takeda, Teva Pharmaceuticals, UCB Pharma, Vertex, Dr. August Wolff GmbH & Co.

What is comparative effectiveness research (CER) ?
• The generation and synthesis of evidence that compares the benefits andharms of alternative methods to prevent, diagnose, treat, and monitor a clinical condition, or to improve the delivery of care.
• The purpose of CER is to ‘‘assist consumers, clinicians, purchasers, and policy makers to make informed decisions that will improve health care at both the individual and population levels.’’
• Two key elements are 1) the direct comparison of effective interventions2) The application of these interventions in patients who are typical
of day-to-day clinical practice
Ratner R , et al. In: Medicine Io.ed Washington DC 2009; Sox HC, et al. Ann Interm Med 2009.

Why do we need CER in IBD ?
• Defined population
• Prescribed treatment regimen
• Follow-up regimented with schedule
• Uniform primary end-point
• Efficacy
• Heterogeneous population
• Variable treatment regimen with optimization
• Follow-up not fixed
• Variable outcomes
• Effectiveness
Clinical trials Clinical practice

Clinical trial IBD population versus real-world IBD population
31% of patients were not eligible for participationin a clinical trial of biologic therapy*
Ha C, et al. Clin Gastroenterol Hepatol 2012.
*Inclusion criteria based on those published for 9 trials of biologic therapy: ACCENT I, CLASSIC I, CHARM, PRECISE I, ENCORE, ENACT, SONIC, ACT 1, ACT 2
Retrospective study of patients with moderate-severe IBD at a US tertiary referral centre (n=206)
Reasons for exclusion in CD● Strictures or abscesses (62%)● Recent exposure or
nonresponse to anti-TNF (51%)● High-dose steroids (18%)● Comorbidities (26%)
Reasons for exclusion in UC● Current rectal therapy use (57%)● Steroid and immunomodulator
naive (45%)● Newly diagnosed (17%)● Colectomy likely (15%)
Non-eligible CD patients had a significantly lower response rate to biologics than eligible CD patients (60% vs 89%, p=0.03)

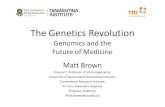
Patients with CRP 0.8 mg/dL and Lesions on Baseline Endoscopy*
22.7
41.5
50.0
0
20
40
60
80
100
AZA+ placebo IFX + placebo IFX + AZA
Perc
ent o
f pati
ents
(%)
P=.002
P=.016 P=.354
17/75 27/65 32/64
* Patients who did not enter the study extension were treated as nonresponders
The impact of CE studies: SONIC: Corticosteroid-Free Clinical Remission at Week 50
AZA=azathioprine; IFX=infliximab
Colombel JF, et al. N Engl J Med. 2010

Setting priorities for CER in IBD: results of an international provider survey, expert rand panel, and
patient focus groups
Cheifetz AS , et al. Inflam Bowel Dis 2012.

Unanswered questions…
Take-off
Flying
Landing

Unanswered questions…
Take-off

Which biologic ?

Comparing biologics agents in IBD
IFX CZADA
The anti-TNFs family

Outcomes in CD patients receiving adalimumab or infliximab therapy
Osterman M, et al. Clin Gastroenterol Hepatol 2013
Adalimumab InfliximabPersistence (%) 47 49 OR 0.98, 95% CI 0.81-1.19Surgery 6.9 5.5 HR 0.79, 95% CI 0.60-1.05Hospitalisations 15.4 11.8 HR 0.88, 95% CI 0.72-1.07
Primary outcomes at Week 26
Adalimumab InfliximabSurgery Steroids 7.2 5.6 HR 0.77, 95% CI 0.51-1.14 No steroids 6.5 5.3 HR 0.82, 95% CI 0.55-1.23Hospitalisations Steroids 17.3 13.1 HR 0.86, 95% CI 0.65-1.12 No steroids 13.5 10.7 HR 0.90, 95% CI 0.67-1.20
Primary outcomes according to baseline steroid exposure
Retrospective cohort of US Medicare data (2006–2010) from new users of adalimumab (n=871) and infliximab (n=1,459)

Vedolizumab in UC: Clinical Response, Clinical Remission, Mucosal Healing at 6 Weeks, ITT Population
25.5
5.4
24.8
47.1
16.9
40.9
0
5
10
15
20
25
30
35
40
45
50
Clinical Response Clinical Remission Mucosal Healing
PlaceboVedolizumab
%
P<0.0001
P=0.0010
D 21.711.6, 31.7
D 11.54.7, 18.3
D 16.16.4, 25.9
P=0.0010
95% CI:
Feagan B et al New Engl J Med 2013

Comparing biologics agents in IBD
IFX CZADA
Anti-Integrins
Anti-TNFs
“The key research topic in the area of IBD from the US Institute of Medicine (IOM) report is to compare the effectiveness of competing
biologic agents”

Biologic vs surgery ?

The LIRIC -trial

Combo vs mono ?

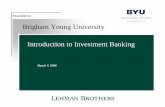
Steroid-free Remission at Week 26
Primary End Point
31
44
57
0
20
40
60
80
100
Prop
ortio
n of
Pati
ents
(%)
AZA + Placebo IFX + Placebo IFX+ AZA
P<0.001
P=0.009 P=0.022
52/170 75/169 96/169
SONIC
Steroid-free remission=CDAI <150 points
Colombel JF et al. N Engl J Med 2010

Impact of concomitant immunomodulator treatment on efficacy and safety of anti-TNF therapy in Crohn’s disease: a meta-
analysis of placebo-controlled trials using patient-level data
Results: 6 Month Clinical Remission Stratified by anti-TNF agent
CertolizumabAdalimumab
OR 0.93; (0.65-1.34) OR 0.88 (0.58-1.35) OR 1.79 (1.06-3.01)
Infliximab
Jones J et al. DDW 2013

Methotrexate with IFX vs IFX alone in CD
- Highest success rate ever observed
- At week 14 and 50 there was between the IFX group vs IFX+MTX group
- All patients on prednisone 15 to 40mg/d
55.6
76.2
57.1
77.8
01020304050607080
Week 14 Week 50
% s
ucce
ss
MTX Placebo
P = 0.83
P = 0.86
COMMIT
MTX PlaceboWeek 14 Week 50
Ster
oid-
free
rem
issio
n
Primary end-point:Failure to enter steroid-free remission at week 14 or maintain through week 50
Feagan B et al. Gastroenterology in press

Step-up vsAccelerated step-up vs
Top-down ?

Ordás I et al. Gut 2011
Conventional and evolving treatment strategies in CD

Early “top-down” therapy with azathioprine is not more effective than placebo or conventional therapy
RAPIDAZTEC
Cosnes J et al. Gastroenterology 2013;145: 758-65 Panes J et al. Gastroenterology 2013;145: 766-74

CDAI <150 AND no steroids AND no surgery
Weeks
Patie
nts (
%)
*
**
*p<0.01**p<0.05
D’Haens G, et al. Lancet 2008;371:660-7.
*
Early top-down biologic therapy vs conventional management of Crohn’s disease

Usual care vs accelerated care : REACT 1
20 practices
(1,200 pts)
20 practices
(1,200 pts)60 patientsper practice
Accelerated care
treatmentalgorithm
Usual care
Patients will be bio-naïvePrimary endpoint: Proportion in remission (HBI 4 and off steroids) at practice level 12 mo following randomization

YesEvaluate in 4 wks – remission? (HBI ≤4)
5-ASAAntibiotics
Re-evaluate in 12 wks – remission?Yes No
NoYes
Cont combo maint Rx Consider resection
Taper steroids, re-evaluate in 12 wks – remission?
Re-evaluate in 12 wks – remission?
No
Re-evaluate in 12 wks – remission?Yes No
Re-evaluate in 12 wks – remission?NoYes
Re-evaluate in 12 wks – remission?
With fistulaWithout fistula
Complex fistula
Yes
MRI, US, EUAto rule out abscess
Antibiotics/fistulotomy
Abscess present?
Yes NoDrainage/seton
+ antibioticsRe-evaluate in 4 wks – improved?
No
Yes
NoSurgical
reassessment
Yes No
Follow algorithm for activeluminal CD without fistula
Switch TNF-blockerCont combo maint Rx
Switch anti-metaboliteCont combo maint Rx
Cont combo maint Rx Increase ADA to weekly dose
ADA + AZA or MTX (steroids prn)
No maintenancetherapy
Taper steroids Add ADA + AZA or MTX
Steroids (budes vs pred based ondisease activity and location)
Active luminal CD (HBI >4)
Accelerated care therapeutic algorithm for Crohn’s disease

Unanswered questions…
Flying

Treat to mucosal healing vstreat to symptoms ?

40 patientsper practice
Step caretreatmentalgorithm
Primary endpt: risk of CD-related complications at one-year, measured at the practice level. CD-related complications include (1) CD-related hospitalizations for CD-related surgeries and non-surgical CD events (such as disease flare, bowel obstruction, excluding hospitalization for side effects of study medication), and (2) Bowel damage events not requiring hospitalization (such as symptomatic bowel obstruction, cutaneous fistula, abscess).
Enhanced care
treatmentalgorithm
15 practices(600 pts)
15 practices(600 pts)
Usual care vs enhanced care : REACT 2

Yes No
Yes
Taper GCS, re-evaluate by ileocolonoscopy in 16 wks– remission? (HBI ≤4, no large ulcers, no GCS)
No
Enhanced care algorithm
Active luminal CD (HBI >4, 1 large ulcer)
Yes
Initiate combination therapy (adalimumab + AZA or MTX) +/- GCS as required
Evaluate by ileocolonoscopy in 16 wks – remission?(HBI ≤4, no large ulcers, no GCS)
Continue combinationmaintenance therapy
Increase adalimumab to weekly dose +/- GCS as required
No
Continue combinationmaintenance therapy
Switch antimetabolite, +/- GCS as required
Re-evaluate by ileocolonoscopy in 16 wks– remission? (HBI ≤4, no large ulcers, no GCS)
Continue combinationmaintenance therapy
Switch TNF antagonist, +/- GCS as required
5-ASAAntibiotics

Treat to biomarkers vstreat to symptoms ?

Calprotectin monitoring in CD after IFX withdrawal

Prednisoneup to 8 weeks
ConventionalCDAI, steroid use
Tight controlCDAI, steroid use, high-sensitivity CRP, faecal calprotectin
Primary endpoint:Mucosal healing 48 weeks
after randomisation
Usual care vs tight control using biomarkers: CALM
Open-label, multicenter study in Europe and Canada
Evaluating two treatment algorithms in CD
Treatment intensification in both arms:1) No treatment, 2) Adalimumab every other week, 3) Adalimumab weekly, 4) Adalimumab weekly + azathioprine
Patients naïve toimmunomodulatorsand biologic therapy(n=240)
www.clinicaltrial.gov: NCT01235689

R w9 w21 w33 w45
Treatment may change at weeks 9, 21, 33 and 45 based on success criteria at weeks 8, 20, 32 and 44
At week 9, 21, 33 and 45, did subject meet all objective criteria?:– CDAI <150– HS-CRP <5mg/L– Calprotectin <250 μg/g– Off steroids starting wk 9
Flare = CDAI↑ ≥70 from BL and ≥220, pt continues as non-responder
* Flare between wks 9 + 21, ADA started
** Flare between evaluation wks, then next option
N = ADA wkly**
N = 120Prednisone8 wks
Y = No change**
Y = No change**
N = ADA EOW**
N = ADA
Y = No change*
Y = No change**
N = ADA EOW**
Y = No change**N = ADA wkly
Y = No change**N = ADA wkly
Y = ADA EOW**
N = ADA wkly + AZA
Y = No change**N = ADA EOW**
Y = No change**N = ADA wkly**
Y = No change**N = ADA wkly**
Y = No change**N = ADA wkly**
Y = ADA EOW**
Y = ADA EOW**
Y = No change**N = ADA wkly**
N = ADA wkly AZA**
Y = ADA EOW AZA**N = ADA wkly AZA**
w56
N = ADA wkly AZA**
Tight control arm

Treat to trough levels vstreat to symptoms ?

Pk of biologics: What we know already
• Drug levels of IFX and ADA are associated with outcome in Crohn’s disease
• Antibody status is not directly associated with outcome but is important in understanding reasons for loss of response (LOR) to anti-TNF
• Dose escalation can increase drug levels
• Immunomodulation can decrease antibody production
Colombel JF, et al. Inflamm Bowel Dis 2012
Date of preparation September 2013 AXHUG130882am

Randomised, single-blind, multicentre Danish study in CD (n=69)
Individualised therapy vs dose intensification in patients with CD who lose response to anti-TNF
Steenholdt C , et al. Gut 2013; gutjnl-2013-305279 [ePub ahead of print]
Co-primary clinical endpoint in intention-to-treat and per protocolpopulations. Dashed lines illustrate the predefined non-inferiority margin
0%-25%-50% 25% 50%
True difference
IFX intensificationbetter
Algorithmbetter
Per protocol
Intention-to-treat
Patients with secondary IFX failure were randomised to IFX dose intensification (5 mg/kg every 4 weeks) or interventions based on serum IFX and IFX antibody levels
Co-primary economic endpoint in per protocol populations.Data are average treatment per patient
IFXintensification
0 4 8 12
Study week
0
2
4
6
8
10
Cost
per
pati
ent,
€ m
ean
Algorithm
*
**p<0.001

Biologic Naïve Subjects with active luminal CD (N=120)
VisitsCohort 1
n=40Cohort 2
n=40Cohort 3 (control)
n=40
IFX 5 mg/kg (0,2,6 then every 8 wks) + AZA 2-2.5 mg/kg (if tolerated)
Upon Clinical Relapse and/or TL ↓: †
-1st time: IFX 7.5 mg/kg -2nd time: IFX 10mg/kg
Upon Clinical Relapse and/or TL ↓: †
-IFX 10 mg/kg
Only upon Elevated CDAI: -IFX 10 mg/kg
***
Primary endpoint: steroid-free remission between wk22 and wk54 (CDAI < 150) and endoscopic healing at wk54
Week 22
Week 14
Week 30
Week 38
Week 46
Week 54Ileocolonoscopy
Week 6Week 2Week 0
*
*
*
*
*
*
Week 12 Ileocolonoscopy/TL
18
26
34
42
50
Ileocolonoscopy at screening
Optimizing anti-TNF based on trough levels vs clinical symptoms: TAILORIX

Unanswered questions…
Landing

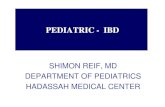
Median IFX levels, Week 8 to Week 104 combined
No need for early ‘rescue’ IFX: primary endpoint
p<0.005
0
1
10
100
Continued DiscontinuedIF
X tr
ough
leve
ls
(μg)Cum
ulat
ive
surv
ival
0 20 40 60 80 100
0.0
0.2
0.4
0.6
0.8
1.0
Time (weeks)
Log Rank (Cox): 0.735; Breslow: 0.906
ContinuedDiscontinued
Van Asche et al, Gastroenterology 2008
80 patients randomized to continue (+CON , n=40) or to interrupt (++DIS, n=40) immunomodulators (azathioprine or methotrexate) 6 months after the start of infliximab (5 mg/kg IV)
Discontinuation of Immunomodulator in Stable Remission on Combination Therapy (Infliximab Maintained)

Discontinuation of Infliximab in Stable Remission on Combination Therapy (azathioprine maintained)
STORI
• n=52 relapses/115 patients• Median follow-up 28+/- 2 months
• Median time to relapse: 16.4 months
Louis E et al. Gastroenterology. 2012;142:63-70.

Louis E et al. Gastroenterology. 2012;142:63-70.
Deleterious factors: • No previous surgery• Steroids within 12-6 months
before infliximab withdrawal• Male gender• Hemoglobin ≤14.5 g/dL, • Leukocyte count >6x109/L, • hsCRP ≥5 mg/L, • Fecal calprotectin ≥300 µg/g, • CDEIS>0• infliximab trough
≥2 mg/L
0.0
0.4
0.6
0.2
0.8
1.0
0 6 12 18 24 30
Months since infliximab withdrawal
No. deleteriousfactors
<4
4
5-6
>6
Proportion Without Relapse
Kaplan Meier time-to-relapse curves according to multivariate models and scores generated through Cox model using multiple imputations method
Predictive Model for Time to Relapse After Stopping IFX and Continuing AZA

A proSpective randomized controlled trial comParing infliximAb-antimetabolites combination therapy to anti-
metabolites monotheRapy and infliximab monothErapy in patients with Crohn’s disease in sustained steroid-free
remission on combination therapy
SPARE
CCFANycibdc

Crohn’s disease patients in steroid-free remission for 6
months and treated with infliximab and anti-
metabolites combination therapy for at least 1 year, infliximab being given at 5
mg/Kg /8 weeks for at least 6 months
Continuing the combination therapy at the same dosage
Intensification of infliximab at 10 mg/Kg/8 weeks
Judged as failure per protocol. Managment at the discretion
of the investigator
Discontinuing infliximab and continuing the anti-metabolite
at the same dosage
infliximab 5 mg/Kg infusion. If no remission at 4 weeks,
reinfusion at 10 mg/KgIf further relapse beyond one
year, the same treatment regimen is applied
If further relapse within 1 year, the same retreatment
regimen is applied and a scheduled treatment with 5
mg/Kg or 10 mg/Kg depending how the remission was recovered, is applied like
in group one
Judged as failure per protocol. Managment at the discretion
of the investigator
Discontinuing anti-metabolites and continuing infliximab at
the same dosage
Infliximab intensification like in first arm. If no remission, anti-
metabolite is restarted
Judged as failure per protocol. Managment at the discretion
of the investigator
Randomisation Relapse No remission
Timeline (weeks)
-3 0 8 16 24 32 40 48 56 64 72 80 88 96 104
Screening
Scheduled visits
Colonoscopy Small bowel MRI * *
Study end

Comparative effectiveness research in IBD
A huge opportunity
Formidable challenges• design• recruitment• funding• …