FUNDAMENTALS OF BILLING AND CODINGeo2.commpartners.com/users/accma/downloads/handouts_060311.pdfExam...
32
6/3/2011 1 FUNDAMENTALS OF BILLING AND CODING A Basic Training Series for Billing & Coding Staff in the Medical Office ACCMA 2011 About This Manual © Copyrighted 2011, The Sage Associates, Pismo Beach, California and Practice & Liability Consultants LLC, San Francisco, California All rights reserved. All material contained in this manual is protected by copyright. Participants who receive this book as part of a workshop presented by The Sage Associates have permission to reproduce any forms contain herein, solely for their own uses within their medical practices. Any other reproduction or use of material in this book without the permission of the author is strictly prohibited. The material in this manual was written by practice management consultants. Any advice or information contained in this manual should not be construed as legal advice. When a legal question arises, consult your attorney for appropriate advice. The information presented in this manual is extracted from official government and industry 2 publications. We make every attempt to assure that information is accurate; however, no warranty or guarantee is given that this information is error-free and we accept no responsibility or liability should an error occur. CPT codes used in this manual are excerpts from the current edition of the CPT (Current Procedural Terminology) book, are not intended to be used to code from and are for instructional purposes only. It is strongly advised that all providers purchase and maintain up to date copies of CPT. CPT is copyrighted property of the American Medical Association.
Transcript of FUNDAMENTALS OF BILLING AND CODINGeo2.commpartners.com/users/accma/downloads/handouts_060311.pdfExam...

6/3/2011
1
FUNDAMENTALS OF BILLING AND CODING
A Basic Training Series for Billing & Coding Staff in the Medical Office
ACCMA 2011
About This Manual
© Copyrighted 2011, The Sage Associates, Pismo Beach, California andPractice & Liability Consultants LLC, San Francisco, California
All rights reserved. All material contained in this manual is protected by copyright. Participants who receive this book as part of a workshop presented by The Sage Associates have permission to reproduce any forms contain herein, solely for their own uses within their medical practices. Any other reproduction or use of material in this book without the permission of the author is strictly prohibited.
The material in this manual was written by practice management consultants. Any advice or information contained in this manual should not be construed as legal advice. When a legal question arises, consult your attorney for appropriate advice.
The information presented in this manual is extracted from official government and industry
2
p g ypublications. We make every attempt to assure that information is accurate; however, no warranty or guarantee is given that this information is error-free and we accept no responsibility or liability should an error occur.
CPT codes used in this manual are excerpts from the current edition of the CPT (Current Procedural Terminology) book, are not intended to be used to code from and are for instructional purposes only. It is strongly advised that all providers purchase and maintain up to date copies of CPT. CPT is copyrighted property of the American Medical Association.
6/3/2011
2
Mary Jean Sage
The Sage Associatesg897-309 Oak Park Blvd.Pismo Beach, CA 93449
Tel: (805) 904-6311F (805) 904 6313
3
Fax: (805) 904-6313www.thesageassociates.com
AgendaAgenda
•• Managing and Preventing ClaimManaging and Preventing Claim•• Managing and Preventing Claim Managing and Preventing Claim DenialsDenials
•• EOB AnalysisEOB Analysis
4
•• EOB AnalysisEOB Analysis

6/3/2011
3
Managing & PreventingManaging & PreventingClaims Denials
Let’s Look At:
•• Claim SubmissionClaim Submission
•• Insurance Follow UpInsurance Follow Up
•• EOB AnalysisEOB Analysis
6
•• Denial and Appeal ProcessDenial and Appeal Process
•• Open ClaimsOpen Claims
6/3/2011
4
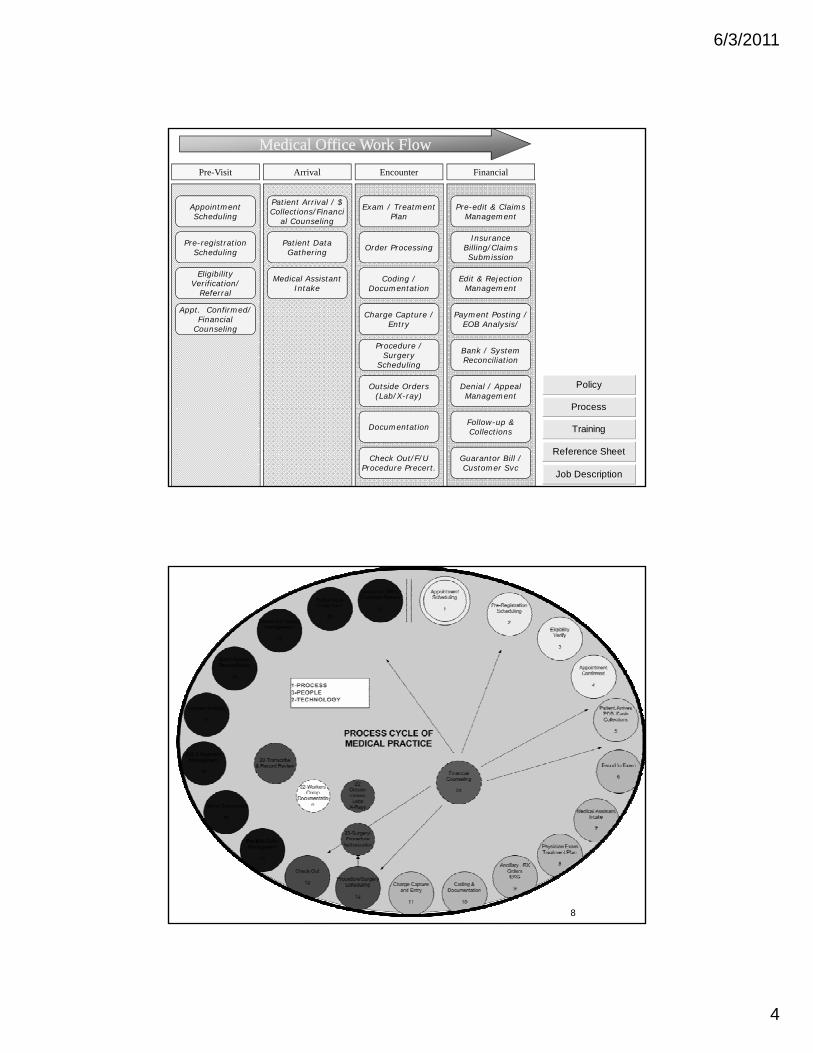
Medical Office Work FlowMedical Office Work Flow
AppointmentScheduling
Pre-registration
Patient Arrival / $ Collections/Financi
al Counseling
Patient Data
Exam / Treatment Plan
Order Processing
Pre-edit & Claims Management
Insurance Billing/Claims
Pre-Visit Arrival Encounter Financial
Scheduling
Eligibility Verification/
Referral
Appt. Confirmed/Financial
Counseling
Gathering
Medical Assistant Intake
Order Processing
Coding / Documentation
Charge Capture / Entry
Procedure / Surgery
Scheduling
Billing/Claims Submission
Edit & Rejection Management
Payment Posting / EOB Analysis/
Bank / System Reconciliation
7
Scheduling
Outside Orders (Lab/X-ray)
Documentation
Check Out/F/U Procedure Precert.
Denial / Appeal Management
Follow-up & Collections
Guarantor Bill / Customer Svc
Policy
Process
Training
Reference Sheet
Job Description
8
6/3/2011
5
9
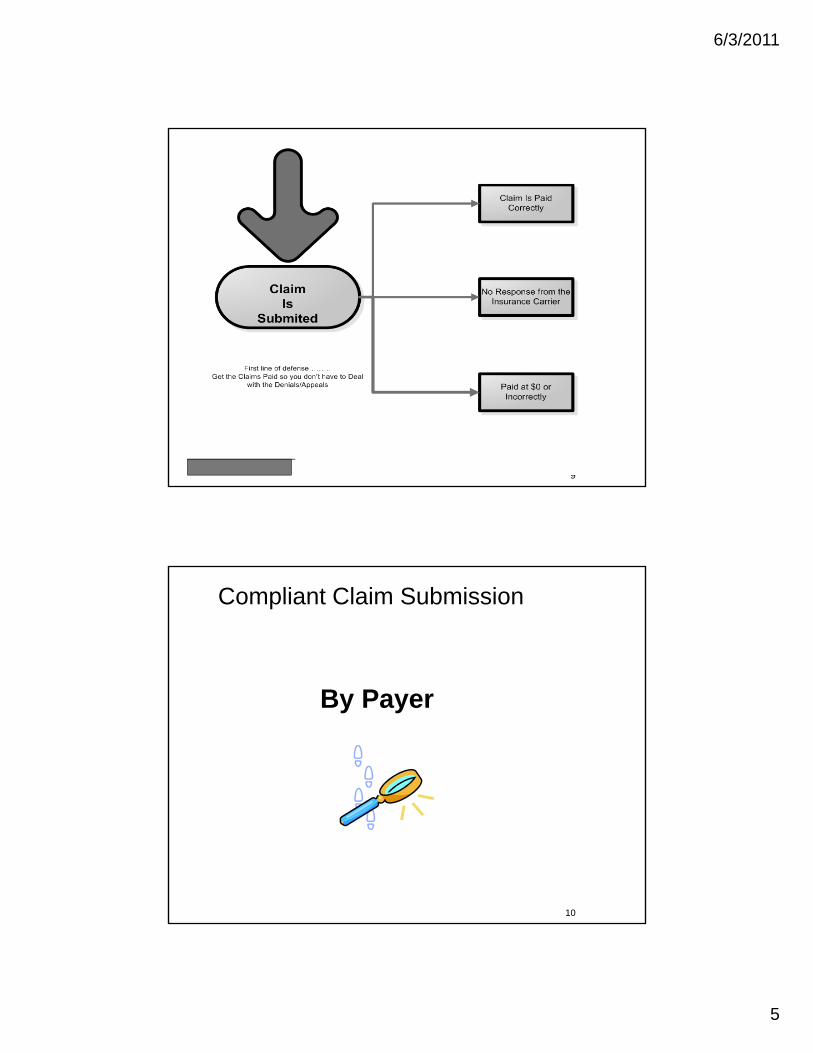
Compliant Claim Submission
By Payer
10
6/3/2011
6
Claim SubmissionClaim Submission
•• Review charges prior to releaseReview charges prior to releaseManual ReviewManual Review–– Manual ReviewManual Review
•• Scheduling StaffScheduling Staff•• Charge entry staffCharge entry staff•• Insurance followInsurance follow--up staffup staff
•• Automated review via claims scrubberAutomated review via claims scrubber
11
•• Automated review via claims scrubberAutomated review via claims scrubber
Assuring Compliant Claim Submission
• Know the requirements of EACH payer• Adhere to Billing Time Limits• Adhere to Billing Time Limits• Fill out claim correctly
– Field 1a (ID)– Fields 9 and 9D – other insurance– Field 10d
12
Field 10d– Field 11 – insurance info (a-d)
6/3/2011
7
– Fields 12 and 13• Medicare no longer requires assignment ofMedicare no longer requires assignment of
benefits signature– Fields 17 and 17B– Field 23– Fields 24E, 24G, 24J
Field 31
13
– Field 31– Field 32– Field 33
14

6/3/2011
8
Claim Submission Claim Submission
•• Ensure charges are going throughEnsure charges are going through
–– Electronic clearinghouseElectronic clearinghouse–– Direct to carrierDirect to carrier–– Be on alert for failed batchesBe on alert for failed batches
15
•• Work Error ReportsWork Error Reports–– Set Benchmarks Set Benchmarks –– ie ie all errors corrected all errors corrected
and claim resubmitted within 48 hoursand claim resubmitted within 48 hours
PaidPaid
•• Post Post meticulouslymeticulously•• UnderpaymentsUnderpayments•• UnderpaymentsUnderpayments
–– Know your allowablesKnow your allowables–– Not just $$; adjudicated as inNot just $$; adjudicated as in--network network
when it should have been outwhen it should have been out--ofof--networknetwork•• NonNon--Payments…Payments…
16
yy–– By line itemBy line item

6/3/2011
9
The Purpose of an RA / EOB
• Payments
• Adjustments– Denied Claim– Zero Payment– Reduced Payment
P lt A li d
17
– Penalty Applied– Additional Payment– Supplemental Payment
18
6/3/2011
10
Denial ManagementDenial Management
•• Top Five Reasons for Denials*Top Five Reasons for Denials*Eligibility/Patient ResponsibilityEligibility/Patient Responsibility–– Eligibility/Patient ResponsibilityEligibility/Patient Responsibility
–– Lack of Authorization/ReferralLack of Authorization/Referral–– Medical NecessityMedical Necessity–– CodingCoding–– DuplicatesDuplicates
19
*Not in order; may vary by practice and specialty*Not in order; may vary by practice and specialty
Denial ManagementDenial Management
•• Explanation of benefits (EOB)Explanation of benefits (EOB)•• By line itemBy line item•• By line itemBy line item•• Reason codeReason code
–– List: www.wpcList: www.wpc--edi.comedi.com
20
6/3/2011
11
Denial ManagementDenial Management
•• Eligibility and Patient ResponsibilityEligibility and Patient ResponsibilityF th f t dF th f t d–– Focus on the front endFocus on the front end
•• Complete, accurate information (from card)Complete, accurate information (from card)•• To avoid COB issues, ask “Do you/Does the To avoid COB issues, ask “Do you/Does the
patient have other insurance coverage?patient have other insurance coverage?
•• Verify insurance and check benefits Verify insurance and check benefits ( ti l)( ti l)
21
(optional)(optional)•• If nonIf non--covered service, and have an covered service, and have an
ABN, waiver or agreement, transfer to ABN, waiver or agreement, transfer to patientpatient
Denial ManagementDenial Management
•• Eligibility and Patient ResponsibilityEligibility and Patient ResponsibilityCheck prior (and post) insuranceCheck prior (and post) insurance–– Check prior (and post) insuranceCheck prior (and post) insurance
–– Check Medicaid eligibilityCheck Medicaid eligibility–– Check hospital registration systemCheck hospital registration system–– If no information, bill patient ASAPIf no information, bill patient ASAP
22

6/3/2011
12
Denial Management Denial Management
•• Lack of authorization/referralLack of authorization/referralCheck recordsCheck records–– Check recordsCheck records
–– Check with payerCheck with payer–– Check with referring physicians officeCheck with referring physicians office–– Check documentation for emergencyCheck documentation for emergency
23
Denial ManagementDenial Management
•• Medical NecessityMedical NecessityLet Medicare’s NCD/LCD be your guideLet Medicare’s NCD/LCD be your guide–– Let Medicare s NCD/LCD be your guideLet Medicare s NCD/LCD be your guide
•• http://www.cms.hhs.gov/mcdhttp://www.cms.hhs.gov/mcd•• Use them in your appeals with all payersUse them in your appeals with all payers
–– Know every payer’s definitionKnow every payer’s definition
24
--Cigna: Medical NecessityCigna: Medical Necessity——Medical necessity is a term used to refer to a Medical necessity is a term used to refer to a course of treatment seen as the most helpful for the specific health course of treatment seen as the most helpful for the specific health symptoms you are experiencing. The course of treatment is determined symptoms you are experiencing. The course of treatment is determined jointly by you, your health professional and CIGNA HealthCare. This jointly by you, your health professional and CIGNA HealthCare. This course of treatment strives to provide you with the best care in the most course of treatment strives to provide you with the best care in the most appropriate setting. appropriate setting.

6/3/2011
13
Denial ManagementDenial Management
•• Medical NecessityMedical NecessitySupporting documentationSupporting documentation–– Supporting documentationSupporting documentation
•• Office visit, operative report, interpretationOffice visit, operative report, interpretation•• Referring physician’s documentationReferring physician’s documentation•• Referring physician requestReferring physician request•• Medical literatureMedical literature•• Specialty society policy treatmentSpecialty society policy treatment
25
Specialty society policy treatmentSpecialty society policy treatment•• MedicareMedicare-- NCD/LCDNCD/LCD
Denial ManagementDenial Management
•• Medical NecessityMedical NecessityEvaluate payer policies: Don’t appealEvaluate payer policies: Don’t appeal oror–– Evaluate payer policies: Don t appealEvaluate payer policies: Don t appeal-- or or decide to dispute at a higher level if not decide to dispute at a higher level if not within policy guidelineswithin policy guidelines
26
6/3/2011
14
Denial ManagementDenial Management
•• CodingCodingCorrect any mistakesCorrect any mistakes–– Correct any mistakesCorrect any mistakes
•• --51 instead of a 51 instead of a --59?59?•• Overlooked a diagnosisOverlooked a diagnosis•• Incorrect linkage of diagnosis and CPT codeIncorrect linkage of diagnosis and CPT code
–– Be more specificBe more specific•• Avoid xx999 (unlisted) codesAvoid xx999 (unlisted) codes
27
•• Avoid xx999 (unlisted) codesAvoid xx999 (unlisted) codes•• Avoid “not elsewhere classified (NEC)Avoid “not elsewhere classified (NEC)•• Avoid “not elsewhere specified (NOS)Avoid “not elsewhere specified (NOS)
Denial ManagementDenial Management
•• CodingCodingReview the position of the “source ofReview the position of the “source of–– Review the position of the source of Review the position of the source of authority”authority”
•• American Medical associationAmerican Medical association–– www.amawww.ama--assn.comassn.com
•• E.g., “CPT changes: An insider’s View”, “CPT E.g., “CPT changes: An insider’s View”, “CPT
28
Assistant”, and “Modifiers Made Easy”Assistant”, and “Modifiers Made Easy”•• Current CPT and ICDCurrent CPT and ICD--9 code books9 code books
6/3/2011
15
Denial ManagementDenial Management
•• CodingCodingBundlingBundling–– BundlingBundling
•• Correct Coding InitiativeCorrect Coding Initiativehttp://www.cms.hhs.gov/NationalCorrectCodInitEd/http://www.cms.hhs.gov/NationalCorrectCodInitEd/
•• Use these in your appeals to other carriersUse these in your appeals to other carriers
29
Denial ManagementDenial Management
•• DuplicatesDuplicatesIs it really a dup?Is it really a dup?–– Is it really a dup?Is it really a dup?
–– Automatic rebillsAutomatic rebills–– Rebills as “appeals”Rebills as “appeals”–– Ignoring automatic crossoversIgnoring automatic crossovers–– StaffStaff--productive(?)productive(?)
30
–– Payer’s administrative problem; address at Payer’s administrative problem; address at a high level a high level

6/3/2011
16
Denial ManagementDenial Management
•• Source of authoritySource of authorityMedical Necessity=Medical Necessity=–– Medical Necessity=Medical Necessity=
•• MedicareMedicare•• Specialty SocietySpecialty Society
–– CPT codes= AMACPT codes= AMA–– Bundling= Medicare (CCI)Bundling= Medicare (CCI)
31
Denial ManagementDenial Management
•• Decide if a denial is Decide if a denial is inevitableinevitablePrint to paperPrint to paper–– Print to paperPrint to paper
–– Attach letter of “review requested”Attach letter of “review requested”–– Examples:Examples:
•• Certain payers (e.g., Workers Comp)Certain payers (e.g., Workers Comp)•• “Unlisted” procedure codes“Unlisted” procedure codes
–– Indicate “most like” code with pricing in letterIndicate “most like” code with pricing in letter
•• “Unspecified” diagnosis code“Unspecified” diagnosis code
32
•• Correct use of modifiersCorrect use of modifiers•• Multiple procedures or tests in one dayMultiple procedures or tests in one day•• Complex surgical caseComplex surgical case•• Other extenuating circumstancesOther extenuating circumstances
–– Automate itAutomate it

6/3/2011
17
Denial ManagementDenial Management
The Good News:The Good News:•• According to data from Medicare, According to data from Medicare,
65% or the claims carriers reviewed 65% or the claims carriers reviewed on appeal result in increased on appeal result in increased payments.payments.
•• Experts: 70 to 80% of appealedExperts: 70 to 80% of appealed
33
•• Experts: 70 to 80% of appealed Experts: 70 to 80% of appealed claims are eventually paid.claims are eventually paid.
It’s Worth Your Time!
Denial ManagementDenial Management
•• Is it “appeal” Is it “appeal” ––able?able?–– Did you code correctly?Did you code correctly?
•• CPT (procedure) and ICDCPT (procedure) and ICD--9 (diagnosis)9 (diagnosis)•• Correct use of modifier, Correct use of modifier, --59, 59, --25, 25, --5757
–– Did you code AND provide the service according to the Did you code AND provide the service according to the payer’s reimbursement guidelines?payer’s reimbursement guidelines?
–– Do you have the documentation to support your appeal?Do you have the documentation to support your appeal?
34
•• Is it worth your time?Is it worth your time?–– Dollar amount v. Staff effortDollar amount v. Staff effortIf the answer is “no” to any of these questions
then Write-It Off. Make sure to track write-off codes/reasons and run monthly report.

6/3/2011
18
Denial ManagementDenial Management
•• Call and request reconsideration over Call and request reconsideration over the telephonethe telephonethe telephonethe telephone
•• If verbal reconsideration is not an If verbal reconsideration is not an option, appeal in writingoption, appeal in writing–– Process?Process?
35
–– Address?Address?
36
6/3/2011
19
37
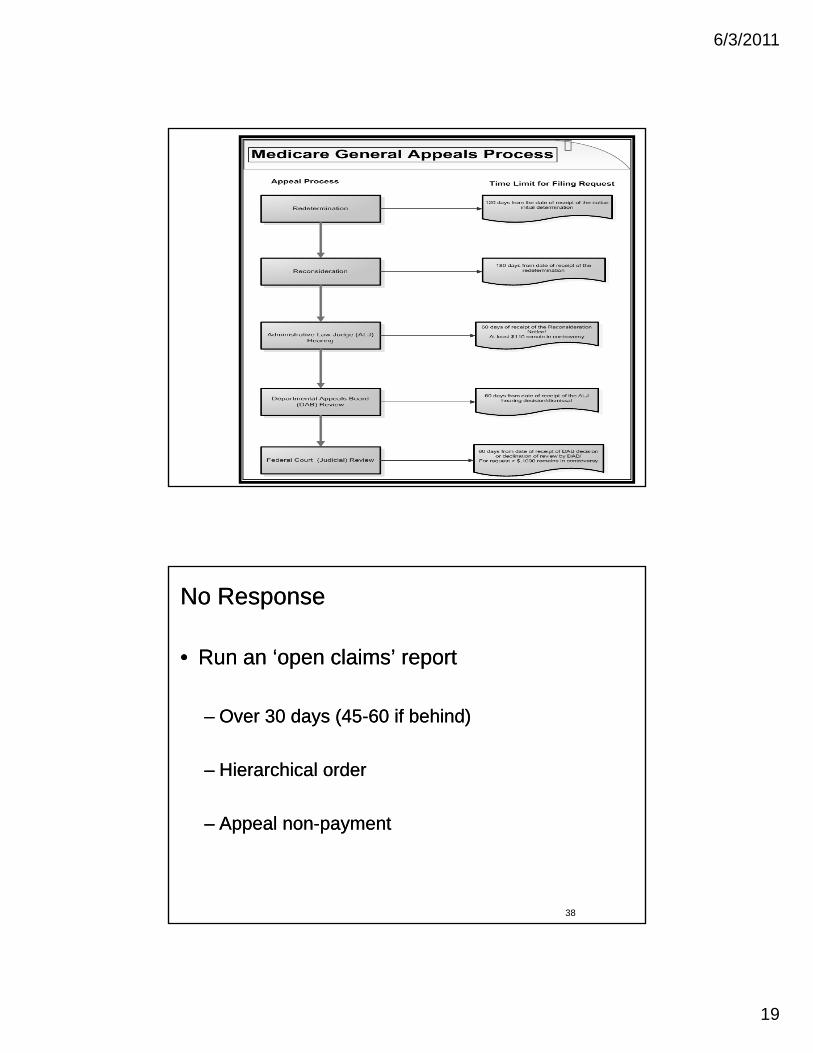
No ResponseNo Response
•• Run an ‘open claims’ reportRun an ‘open claims’ report
–– Over 30 days (45Over 30 days (45--60 if behind)60 if behind)
–– Hierarchical orderHierarchical order
38
–– Appeal nonAppeal non--paymentpayment
6/3/2011
20
Other tipsOther tips
•• “Unbilled” report (e.g., pending MCD)“Unbilled” report (e.g., pending MCD)
•• Work accounts in hierarchical orderWork accounts in hierarchical order
•• Adjustment/ WriteAdjustment/ Write--off codesoff codes
39
Account FollowAccount Follow--Up Up Performance Workload RangesPerformance Workload Ranges
•• Research correspondence * and resolve by Research correspondence * and resolve by t l h 5t l h 5 10 i / t 610 i / t 6 12/h12/htelephone: 5telephone: 5--10 min/account; 610 min/account; 6--12/hour12/hour
•• Research correspondence* and resolve by Research correspondence* and resolve by appeal: 15appeal: 15--20 min/account; 320 min/account; 3--4/hour4/hour
•• Check status of claim (telephone/online) and Check status of claim (telephone/online) and rebill: 1rebill: 1--5 min/account; 125 min/account; 12--60/hour60/hour
40
•• Assuming 1/3,1/3,1/3= 113 accounts/dayAssuming 1/3,1/3,1/3= 113 accounts/day
*Including reviewing correspondence from payer that shows denial and/or *Including reviewing correspondence from payer that shows denial and/or underpayment, identifying cause of denial or underpayment, pulling underpayment, identifying cause of denial or underpayment, pulling medical documentation and/or other support and developing a case for medical documentation and/or other support and developing a case for reconsideration of payment.reconsideration of payment.
6/3/2011
21
Payment PostingPayment Posting& EOB Analysis& EOB Analysis
41
Payment Posting & EOB Analysis ProcessPayment Posting & EOB Analysis Process
•• ERA and fund transferERA and fund transfer•• Batch mail paymentsBatch mail paymentsp yp y•• Bank deposit is prepared and reconciledBank deposit is prepared and reconciled•• Match patient, date of service and CPT codes Match patient, date of service and CPT codes
from EOB against systemfrom EOB against system•• Apply payment and contractual adjustments to Apply payment and contractual adjustments to
individual line itemindividual line item•• Post zero paymentPost zero payment
42
Post zero paymentPost zero payment•• Appeal underpayment or zero pays line itemsAppeal underpayment or zero pays line items•• Transfer balance to secondary or patient Transfer balance to secondary or patient
balancebalance•• Print statements and secondary claims Print statements and secondary claims

6/3/2011
22
EOB Information…EOB Information…
Information Routinely Found on EOB’sInformation Routinely Found on EOB’s
•• Patient NamePatient Name•• Date of ServiceDate of Service•• Physician (Service Provider)Physician (Service Provider)•• Patient Account NumberPatient Account Number•• Patient Group NumberPatient Group Number•• Subscriber (Insured)Subscriber (Insured)•• Charge AmountCharge Amount
43
Charge AmountCharge Amount•• Amount Allowed (Negotiated Rate)Amount Allowed (Negotiated Rate)•• Amount Paid (Negotiated rate minus deductible)Amount Paid (Negotiated rate minus deductible)•• Deductible, CoDeductible, Co--insurance &/or Coinsurance &/or Co--payment Amountpayment Amount•• Contractual Adjustment AmountContractual Adjustment Amount•• Patient Responsibility (Including coPatient Responsibility (Including co--pays, copays, co--ins & deductible)ins & deductible)
44
6/3/2011
23
Why audit EOBs ?Why audit EOBs ?
•• If you have not approached the denial issue If you have not approached the denial issue previous, a great starting option is to conduct previous, a great starting option is to conduct your own EOB audit as a means of measuring your own EOB audit as a means of measuring denial occurrences. denial occurrences.
•• Denials are not part of the fee that providers Denials are not part of the fee that providers
45
have contractually agreed to write off with have contractually agreed to write off with payers. Rather denials need to be accounted payers. Rather denials need to be accounted for separately, just like bad debt, refunds and for separately, just like bad debt, refunds and other adjustments to charges. other adjustments to charges.
•• An EOB audit ensures that posters are not An EOB audit ensures that posters are not manually entering denials and zeromanually entering denials and zero--dollar paid dollar paid claims as contractual allowances This postingclaims as contractual allowances This postingclaims as contractual allowances. This posting claims as contractual allowances. This posting error removes the provider’s ability to identify, error removes the provider’s ability to identify, rework, and resubmit these claim line items. It rework, and resubmit these claim line items. It is also clearly improper from a reporting is also clearly improper from a reporting perspective; it masks denials under the perspective; it masks denials under the contractual adjustment bucket. Lack ofcontractual adjustment bucket. Lack of
46
contractual adjustment bucket. Lack of contractual adjustment bucket. Lack of standards and consistency in posting of denials standards and consistency in posting of denials and zeroand zero--dollar payments causes the available dollar payments causes the available data to misrepresent the extent of denials, their data to misrepresent the extent of denials, their causes, and the amounted of unrecovered causes, and the amounted of unrecovered revenue. revenue.

6/3/2011
24
GOALS of EOB AuditGOALS of EOB Audit
•• Denials often are hidden on the explanation of payment or Denials often are hidden on the explanation of payment or remittance advice. remittance advice.
•• An EOB allows providers to establish a baseline denial rate. An EOB allows providers to establish a baseline denial rate.
•• For those starting out, the goal of an EOB audit is not For those starting out, the goal of an EOB audit is not necessarily to conduct a statistical significant sample that necessarily to conduct a statistical significant sample that definitively quantifies the extent of the denial problem within definitively quantifies the extent of the denial problem within the organization.the organization.
47
the organization. the organization.
•• You can also use it to get a handle on claim pends since You can also use it to get a handle on claim pends since these will show up as a zero dollar payment on the EOB. these will show up as a zero dollar payment on the EOB.
Two areas that are not tracked through the EOB audit Two areas that are not tracked through the EOB audit are:are:
•• Underpayments that are not zero Underpayments that are not zero dollarsdollarsdollarsdollars
•• Claims that fail to be processed by the Claims that fail to be processed by the payer either electronically (EDI payer either electronically (EDI edits/rejections) or via paper edits/rejections) or via paper
48
j ) p pj ) p pprocessing.processing.

6/3/2011
25
Silent PPOSilent PPO
Be Ware!Be Ware!
49
Be Ware!Be Ware!
What is a Silent PPO?What is a Silent PPO?
•• Silent PPOs are illegal, fraudulent schemes that every year Silent PPOs are illegal, fraudulent schemes that every year take millions of dollars out of the pockets of physicians and take millions of dollars out of the pockets of physicians and health care providers.health care providers.
•• The term Silent PPO refers to the scheme where insurers, The term Silent PPO refers to the scheme where insurers, who do not offer PPO policies, apply your contracted PPO who do not offer PPO policies, apply your contracted PPO discount rates to bills for patients who are not PPO members. discount rates to bills for patients who are not PPO members.
50
Insurers who operate Silent PPOs are typically indemnity Insurers who operate Silent PPOs are typically indemnity insurers, such as automobile insurers and workmen’s insurers, such as automobile insurers and workmen’s compensation insurers, that have no way of referring patients compensation insurers, that have no way of referring patients to you.to you.

6/3/2011
26
•• Medical providers join PPOs to increase patient volume. Medical providers join PPOs to increase patient volume. Legitimate PPOs increase patient volume by entering intoLegitimate PPOs increase patient volume by entering intoLegitimate PPOs increase patient volume by entering into Legitimate PPOs increase patient volume by entering into agreements with Payers, most often group health insurers. agreements with Payers, most often group health insurers. These group insurers offer PPO policies that contain These group insurers offer PPO policies that contain steerage mechanisms to insteerage mechanisms to in--network providers, such as network providers, such as lower colower co--payments, lower deductibles or lower premiums. payments, lower deductibles or lower premiums. Also, legitimate Payers distribute provider directories that Also, legitimate Payers distribute provider directories that identify the preferred providers in the network. These identify the preferred providers in the network. These
51
directories are given to patients when they purchase their directories are given to patients when they purchase their insurance and receive their PPO member ID cards. In insurance and receive their PPO member ID cards. In exchange for increased patient volume, providers give exchange for increased patient volume, providers give legitimate Payers steep discounts on their bills, sometimes legitimate Payers steep discounts on their bills, sometimes as much as 50% off their usual charges.as much as 50% off their usual charges.
•• That is not what happens with Silent PPOs. Under a That is not what happens with Silent PPOs. Under a Silent PPO scheme, Payers who do not offer PPO Silent PPO scheme, Payers who do not offer PPO policies obtain the database of preferred pro ider ratespolicies obtain the database of preferred pro ider ratespolicies obtain the database of preferred provider rates policies obtain the database of preferred provider rates from your PPO or from a middleman called a “discount from your PPO or from a middleman called a “discount broker.” Then they apply those discounts to your bills. You broker.” Then they apply those discounts to your bills. You get nothing in return. In fact, it’s impossible for you to get get nothing in return. In fact, it’s impossible for you to get increased patient volume from such insurers because increased patient volume from such insurers because they have no PPO policy, they provide no directories, and they have no PPO policy, they provide no directories, and they give out no PPO ID cards The patient does not eventhey give out no PPO ID cards The patient does not even
52
they give out no PPO ID cards. The patient does not even they give out no PPO ID cards. The patient does not even know the name of the PPO whose discounts were applied know the name of the PPO whose discounts were applied to the bill. As part of the Silent PPO scheme, insurers try to the bill. As part of the Silent PPO scheme, insurers try to pass off the discount as legitimate on Explanation of to pass off the discount as legitimate on Explanation of Benefit forms.Benefit forms.
6/3/2011
27
•• The result? You lose a tremendous The result? You lose a tremendous amount of moneyamount of money —— and most likelyand most likelyamount of money amount of money and, most likely, and, most likely, never discover that you have been never discover that you have been defrauded. The AMA estimates that defrauded. The AMA estimates that medical providers lose tens of millions medical providers lose tens of millions of dollars per year based on the Silent of dollars per year based on the Silent PPO hPPO h
53
PPO scheme.PPO scheme.
How a Silent PPO Scheme WorksHow a Silent PPO Scheme Works
1. Office Visit. A patient chooses to treat with a 1. Office Visit. A patient chooses to treat with a certain medical provider. The patient is not certain medical provider. The patient is not referred or steered to the provider by an insurer. referred or steered to the provider by an insurer. The primary type of insurance coverage The primary type of insurance coverage responsible to pay the bill is a form of indemnity responsible to pay the bill is a form of indemnity insurance, such as automobile insurance, worker's insurance, such as automobile insurance, worker's compensation, disability insurance or the outcompensation, disability insurance or the out--ofof--network portion of a PPO policy.network portion of a PPO policy.
54
2. The Insurance Claim. The medical provider bills 2. The Insurance Claim. The medical provider bills the insurance company based on their usual and the insurance company based on their usual and customary charge for the service provided.customary charge for the service provided.
6/3/2011
28
3. The “Re3. The “Re--pricing” of Your Bill.pricing” of Your Bill. The patient’s insurance The patient’s insurance company receives your bill and does one of two things. It company receives your bill and does one of two things. It either:either:
runs your tax ID number on your bill through a PPO discount runs your tax ID number on your bill through a PPO discount database it leased from a PPO, or database it leased from a PPO, or
provides a discount broker (also called a bill reprovides a discount broker (also called a bill re--pricing company) pricing company) with a copy of your billwith a copy of your bill
55
with a copy of your bill. with a copy of your bill.
The discount broker searches for a PPO “hit” by running your tax The discount broker searches for a PPO “hit” by running your tax ID number through its database of PPO discounts. After a ID number through its database of PPO discounts. After a successful “hit,” your bill is “resuccessful “hit,” your bill is “re--priced” based on the PPO priced” based on the PPO discounts that were accessed.discounts that were accessed.
4. The Deceptive EOB. After applying the discount, the 4. The Deceptive EOB. After applying the discount, the insurance company states on the EOB that you agreed to insurance company states on the EOB that you agreed to reduce your bill based on your contract with the PPO.reduce your bill based on your contract with the PPO.reduce your bill based on your contract with the PPO. reduce your bill based on your contract with the PPO. This is usually FALSE because your preferred provider This is usually FALSE because your preferred provider contract, if you had one with that PPO, allowed only contract, if you had one with that PPO, allowed only Payers with PPO policies or plans to access your Payers with PPO policies or plans to access your discounts. discounts.
56
5. The Write5. The Write--Off. The medical provider accepts the insurer’s Off. The medical provider accepts the insurer’s statement on the EOB and writes the discount off statement on the EOB and writes the discount off ——never knowing that the discount was invalid.never knowing that the discount was invalid.

6/3/2011
29
How to Audit Claims Payments and Recover Your MoneyHow to Audit Claims Payments and Recover Your Money
•• Step #1: Know the Contents of Your PPO Step #1: Know the Contents of Your PPO Contracts. Contracts. Examine all your PPO contracts and the Examine all your PPO contracts and the payer lists for each contract. See if there is room in payer lists for each contract. See if there is room in those contracts for payers who do not offer preferred those contracts for payers who do not offer preferred provider plans or policies to gain access to your provider plans or policies to gain access to your discounts. If the nine terms discussed above are not discounts. If the nine terms discussed above are not in your PPO contract, you’re leaving yourself open to in your PPO contract, you’re leaving yourself open to problems.problems.
57
•• Step #2: Scrutinize All EOBs With PPO Step #2: Scrutinize All EOBs With PPO Discounts. Discounts. Beware of the following red flags: (1) Beware of the following red flags: (1) the insurer taking the discount is an automobile the insurer taking the discount is an automobile insurer or a workmen’s compensation insurer; (2) insurer or a workmen’s compensation insurer; (2) failure to name the PPO whose discount was failure to name the PPO whose discount was accessed; (3) you have no PPO agreement with accessed; (3) you have no PPO agreement with the PPO indicated; (4) the PPO discount is the PPO indicated; (4) the PPO discount is indicated on the check but not on the EOB; (5) the indicated on the check but not on the EOB; (5) the PPO is identified but you terminated the contract a PPO is identified but you terminated the contract a
hil (6) th EOB billhil (6) th EOB bill i ii i
58
while ago; (6) the EOB comes on a bill rewhile ago; (6) the EOB comes on a bill re--pricing pricing company’s letterhead, rather than the insurer’s company’s letterhead, rather than the insurer’s letterhead, and references the bill reletterhead, and references the bill re--pricing pricing company’s agreement with a PPO, rather than the company’s agreement with a PPO, rather than the insurer’s agreement with the PPO.insurer’s agreement with the PPO.
6/3/2011
30
•• Step #3: CrossStep #3: Cross--check the EOB check the EOB Against Your PPO Contract for thatAgainst Your PPO Contract for thatAgainst Your PPO Contract for that Against Your PPO Contract for that PPO. PPO. Check your contract to see if the Check your contract to see if the payer is listed and what the contract payer is listed and what the contract requires. requires.
59
•• Step #4: CrossStep #4: Cross--check the EOB Against the check the EOB Against the Insurance Information You Received From the Insurance Information You Received From the Patient. Patient. When you questioned the patient at the time When you questioned the patient at the time of intake, if the patient did not mention the PPO of intake, if the patient did not mention the PPO indicated on the EOB, that should be a red flag. For indicated on the EOB, that should be a red flag. For all suspect EOBs, contact the payer and ask if they all suspect EOBs, contact the payer and ask if they offer a PPO policy or plan with inoffer a PPO policy or plan with in--network and outnetwork and out--of of network features. Also, ask if the patient bought a network features. Also, ask if the patient bought a PPO policy and whether the Payer has anPPO policy and whether the Payer has an
60
PPO policy and whether the Payer has an PPO policy and whether the Payer has an agreement with your facility to discount your bills. agreement with your facility to discount your bills. Ask for a letter confirming both of these in writing. Ask for a letter confirming both of these in writing.

6/3/2011
31
•• Step #5: Contact the PPO and the Payer to Step #5: Contact the PPO and the Payer to Discuss the Discrepancy. Discuss the Discrepancy. If the PPO participated in If the PPO participated in the illegal discount, perhaps by selling the the illegal discount, perhaps by selling the information to an improper payer, they may work with information to an improper payer, they may work with you to settle the claim with the payer. You can also you to settle the claim with the payer. You can also make an oral or written demand on the payer for make an oral or written demand on the payer for payment of the discounted amount. Don’t hold your payment of the discounted amount. Don’t hold your breath for payment.breath for payment.
61
•• Step #6: Hire an Experienced Health Care Law Step #6: Hire an Experienced Health Care Law Firm to Conduct a MiniFirm to Conduct a Mini--audit of Your EOBs and audit of Your EOBs and to Recoup Silent PPO Discounts. to Recoup Silent PPO Discounts.
62
6/3/2011
32
Questions?Questions?
63


![[Strawson P F] on Referring()](https://static.fdocuments.us/doc/165x107/577cc1931a28aba711936250/strawson-p-f-on-referring.jpg)















