Six Sigma Workbook For Dummies (For Dummies (Business & Personal Finance))
Functional spine unit development
Literature review
Ed Fournier Michael Wonnacott Biokinetics and Associates Ltd. 2470 Don Reid Drive Ottawa, Ontario K1H 1E1
PWGSC Contract Number: W7701-061933/001/QCL (TA84) CSA: Robert Durocher
The scientific or technical validity of this Contract Report is entirely the responsibility of the Contractor and the contents do not necessarily have the approval or endorsement of the Department of National Defence of Canada. This document was reviewed for Controlled Goods by DRDC using the Guide to Canada’s Export Controls.
Contract Report
DRDC-RDDC-2016-C161
May 2016
© Her Majesty the Queen in Right of Canada, as represented by the Minister of National Defence, 2016
© Sa Majesté la Reine (en droit du Canada), telle que représentée par le ministre de la Défense nationale,
2016
i
Significance for Defence and Security
Vehicles subjected to IED detonation exposes the occupants to significant high rate loading in the
vertical direction. Seating systems designed to mitigate the magnitude of the forces transmitted to
the occupants have been implemented. The evaluation of these seats is carried out in full-scale
blast tests using automotive crash test dummies. The lumbar spine of these dummies were not
designed for loading in the vertical direction and consequently do not properly assess the loads
transmitted to the occupant. A new lumbar spine element is being developed such that loading
and threat of injury can be better evaluated.
ii
Abstract……….…….…….
The prevalence of lumbar spine injuries from underbody blast (UBB) has been noted to result in
debilitating long terms effects on mounted servicemen and women. The energy absorbing vehicle
seats that have been implemented do provide some protection against UBB loading but the level
of protection cannot be properly assessed using current test methods. The Hybrid III
anthropomorphic test device (ATD) used in experimental blast trials along with the Dynamic
Response Index (DRI) injury criteria for assessing lumbar spine injuries are believed to be
inadequate for assessing the various modes of dynamic loading and related injury risks.
A literature review was conducted to identify the parameters that may affect a surrogate’s ability
to assess injury. These include the effect of seating posture and increased inertial loads from
additional body borne mass on the loads applied to the lumbar spine during an UBB incident.
Biofidelic characterization of the functional spine unit was sought for the development of an
improved functional spine unit for assessing spine injury. Of principal concern is an ATD’s
ability to be correctly oriented during initial placement and have the required sensing capabilities
to monitor for combined loading conditions commensurate with the selected injury assessment
reference values.
iii
Table of contents
Significance for Defence and Security ............................................................................................. i
Abstract……….…….……. ............................................................................................................. ii
Table of contents ............................................................................................................................ iii
List of figures ................................................................................................................................. iv
List of tables .................................................................................................................................... v
1 Introduction – Problem Definition ............................................................................................ 1
2 Effects of Seating Posture ......................................................................................................... 3
3 Upper Body Mass Effects On Lumbar Injury ........................................................................... 6
4 Spine Response to Loading....................................................................................................... 8
4.1 Response to Compression Loading ............................................................................... 8
4.2 Response to Shear Loading ......................................................................................... 12
4.3 Response to Flexion-Shear Loading ............................................................................ 13
4.4 Range of Motion .......................................................................................................... 19
5 Existing Injury Criteria ........................................................................................................... 20
5.1 Eiband Injury Tolerance Curve for Vertical Acceleration .......................................... 20
5.2 Dynamic Response Index ............................................................................................ 20
5.3 Multi-axial Dynamic Response Criteria ...................................................................... 22
5.4 Lumbar Load Criterion ................................................................................................ 24
5.5 Spine Injury Criterion .................................................................................................. 25
6 Anthropomorphic Test Devices .............................................................................................. 26
6.1 Frontal Impact Dummies ............................................................................................. 26
6.1.1 Hybrid III ........................................................................................................... 26
6.1.2 THOR-M ........................................................................................................... 27
6.2 Rear Impact Dummies ................................................................................................. 28
6.2.1 RID3D ............................................................................................................... 28
A.1.1 BioRID II ........................................................................................................... 29
6.3 Side Impact Dummies ................................................................................................. 30
6.4 Other Dummies ........................................................................................................... 30
6.4.1 ADAM Dummy ................................................................................................. 30
6.4.2 WIAMan ............................................................................................................ 32
7 Surrogate Spine Development Approach................................................................................ 33
8 Summary and Conclusion ....................................................................................................... 35
References/Bibliography.... ........................................................................................................... 38
References ............................................................................................................................... 38
Bibliography ........................................................................................................................... 42
List of symbols/abbreviations/acronyms/initialisms ..................................................................... 44
iv
List of figures
Figure 1: Possible loading mechanism that may result in fracture (figure from [3]). ..................... 2
Figure 2: Mean translational displacements of lumbar spine segments under preload
conditions. ..................................................................................................................... 4
Figure 3: Mean rotational displacements of lumbar spine segments under preload conditions. ..... 5
Figure 4: Compressive force deflection curve for; (a) normal, and; (b) degenerated
intervertebral disk loaded in compression (figure from [14]). ...................................... 9
Figure 5: Probability curves for spinal injury due to compressive loading (figure from [15]). .... 10
Figure 6: Compressive stiffness of intervertebral disks by lumbar level and loading rate [16]. ... 11
Figure 7: Typical shear results for a L2-L3 motion segment (figure from [17]). .......................... 13
Figure 8: Mean flexion, extension, lateral bending and torsion response of motion segments
tested by Schultz et al [18]. Dashed lines are tests with the posterior elements
removed. ...................................................................................................................... 14
Figure 9: Mean compression, lateral, anterior and posterior shear response of motion
segments tested. Dashed lines are tests with the posterior elements removed
(figure from [19]). ....................................................................................................... 15
Figure 10: Flexion and versus bending moment at failure of lumbar motion segments (figure
from [20]). ................................................................................................................... 16
Figure 11: Typical bending moment versus time response for severe load with a 15 ms and a
5 ms pulse rise time (figure from [23]). ...................................................................... 17
Figure 12: Moment deflection curve up to the elastic limit of the FSU (figure from [25]). ......... 18
Figure 13: Eiband injury tolerance curve for vertical acceleration (figure from [32]). ................. 20
Figure 14: DRI lumped mass model of the spine (figure from [33]). ............................................ 21
Figure 15: DRI versus spinal injury rate (figure from [32]). ......................................................... 21
Figure 16: Critical point for computing BDRC (figure from [36]). .............................................. 22
Figure 17: Correlation between DRI and SIC (figure from [39]). ................................................. 25
Figure 18: Three types of Hybrid III spines are available: a) curved spine, b) pedestrian
straight spine, and c) FAA straight spine. ................................................................... 26
Figure 19: THOR spine (image from [43]). .................................................................................. 27
Figure 20: RID3D (image from [47]). ........................................................................................... 28
Figure 21: BioRID II Spine (image from [48]). ............................................................................ 29
Figure 22: ADAM Spine (image from [50]). ................................................................................ 31
Figure 23: Spine criterion – acceleration (image from [51]). ........................................................ 32
Figure 24: Spine criterion – force (image from [51]). ................................................................... 32
v
List of tables
Table 1: Reported lumbar injury from vertical loading of PMHS specimens [13]. ........................ 9
Table 2: Mechanical properties determined from the FSU compression tests [14]. ...................... 10
Table 3: Summary of average FSU stiffness [17]. ........................................................................ 11
Table 4: Summary of lumbar spine segment shear test results [17]. ............................................. 12
Table 5: Summary of lumbar motion segment loads at failure [20]. ............................................. 16
Table 6: Summary of results, combined dynamic bending and shear [22] and [23]. .................... 17
Table 7: Summary of lumbar motion segment flexion-shear test results for Neumann et
al[24]. .......................................................................................................................... 18
Table 8: Lumbar motion segment failure loads and their corresponding displacements [26]. ...... 19
Table 9: BDRC model coefficients. .............................................................................................. 23
Table 10: Dynamic response limits, DRlimit
, for use in injury risk calculations (Equation 7). ...... 24
Table 11: Recommended military lumbar load limits [37]. .......................................................... 24
Table 12: Lumbar spine response to compressive loading. .......................................................... 36
Table 13: Lumbar spine response to shear loading. ...................................................................... 37
Table 14: Lumbar spine response to flexion. ................................................................................ 37
Table 15: Lumbar spine response combined flexion and shear loading. ....................................... 37
1
1 Introduction – Problem Definition
In recent military conflicts in Iraq and Afghanistan, the incidence of lumbar spinal injuries
sustained by mounted US military personnel from underbody blast (UBB) represents 26% of the
1819 reported incidents of spinal injuries or 145 cases. For the most part, the thoracolumbar
junction from the T10 vertebra to the L3 vertebra was the most susceptible region of the spine to
injury [1]. An increase in spinal injuries was noted following the introduction of vehicles
designed to protect against underbody blast through the use of V-shaped hull design, energy
absorbing seating systems and increased ground clearance. However, this increase may be more
related to the change in the adversaries’ tactics as the conflict moved from Iraq to Afghanistan
where buried improvised explosive devices (IED) became the weapon of choice.
In Bernstock et al’s [2] review of combat related spine injuries, it was noted that amongst
Canadian Forces (CF) casualties reported at the Role 3 Multinational Medical Unit in Afghanistan
there was an 8% incidence of spine injuries of which 10.4% were from IED blast, however, there
was no mention as to the proportion of these that were sustained by mounted soldiers. From
personal discussions with DRDC, the prevalence of lumbar spine injuries from underbody blast
amongst CF personnel has been noted to result in debilitating long term effects on mounted CF
servicemen and women.
DRDC Valcartier is investigating the spinal injuries that are associated with exposure to UBB
threats. Of interest is the effect of seating posture and increased inertial loads from body armour
and torso borne equipment on the loads applied to the lumbar spine during an UBB incident. The
energy absorbing seats that have been implemented in CF armoured vehicles do provide
protection against UBB loading but the level of protection cannot be properly assessed using
current test methods. The current Hybrid III anthropomorphic test device (ATD) used in
experimental blast trials along with the Dynamic Response Index (DRI) for assessing lumbar
spine injuries, are believed to be inadequate for assessing the various modes of dynamic loading
and related injury risks. While the current method may be suitable for certain upright seating
postures for which the ATD was designed, it is not amenable to the slouched posture often
assumed by mounted crew members as it may not properly reproduce the loading for a human-
like seating posture. Furthermore, the DRI injury criterion only uses the vertical acceleration of
the pelvis in its computation of injury severity which would underestimate the loading due to
misalignment of the rotated pelvis accelerometer’s measurement axis. In this orientation, injury
is likely to involve bending and shear components in addition to the axial compressive loading of
the spine.
In their retrospective study of injured NATO and Afghan soldiers during Operation Enduring
Freedom in Afghanistan, Ragel et al [3] found that flexion-distraction fractures represented 1.8%
of all trauma admissions to the Craig Joint Theater Hospital and 38% of the reported
thoracolumbar fractures. This type of fracture to the thoracolumbar spine results from hyper-
flexion of the spine about a fulcrum. In the case of the mounted soldier, their body armour and
attached gear may act as the required fulcrum during vertical loading from the initial UBB
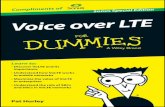
launching the vehicle in the air or from the impact as the vehicle hits the ground. Possible
loading mechanism that could result in flexion-distraction fractures are presented in Figure 1.
Scenario A involves an unbelted soldier equipped with body worn gear subject to vertical loading
who subsequently folds about the bulk of their gear as the body compresses under load.
2
Scenario B involves an unequipped soldier with lap restraint who flexes and collapses downward
during vertical loading. Finally, Scenario C involves an unequipped soldier restrained by lap and
a torso belt whose pelvis rocks forward and rotates underneath the lap belt as the legs are thrown
upwards resulting in a reverse flexion of the thoracolumbar spine. These loading mechanisms
may be further exacerbated with a poor initial seating posture.
Figure 1: Possible loading mechanism that may result in fracture (figure from [3]).
Although vertical loading is present in all three scenarios shown in Figure 1, compressive loading
of the spine is not the underlying mechanism of lumbar injury but rather hyper-flexion which is
not assessed by the Dynamic Response Index, the current injury assessment reference value used
in full scale testing to determine spinal injury outcome following UBB.
The work presented herein will support DRDC’s investigation of lumbar spine injury and the
development of a surrogate spine to realistically assess seating systems’ performance during UBB
experiments where the influence of posture and inertial effects on potential injury mechanisms
associated with non-ideal seating postures and not well known.
3
2 Effects of Seating Posture
Blast attenuating seats attempt to use energy management mechanisms to reduce the forces from
a UBB from being transmitted directly to the vehicle occupants. These attenuation mechanisms
may include, dampers, padding materials, seat belts and alternative seat mounting methods.
Regardless of a seat’s construction, its effectiveness at reducing injury is partly predicated on the
occupant being able to attain a proper seating posture. In the case of a soldier sitting in a military
vehicle this may not always be possible. With the bulk and mass of a soldier’s standard issue
personal protective equipment, obtaining a correct seating posture may be difficult to achieve and
often an out-of-position slouched seating posture may be assume. Generally, poor posture in
one’s daily activity (sitting, standing, and lifting) is detrimental to the load capacity and stability
of the spine, whether during low level loads, as evident in chronic injuries, or with acute loads
potentially leading to strains, extractions or fractures.
There is limited data available pertaining to high rate vertical loading of the spine and associated
lumbar injuries, particularly as they relate to seating posture. That being said, Liu et al [4]
investigated the effects of spinal positioning of pilots during ejection using a mathematical model
of the spine. In their review they cited earlier research that showed that 17% of ejection seat
deployment resulted in spinal fracture of which 70% of the injuries were to the thoracolumbar
spine. In their analysis they came to several conclusions related specifically to ejection seats and
injury mechanisms, the most pertinent to the current UBB study are; (a) spinal alignment at the
time of ejection determines the location and magnitude of stresses applied to the spine, and; (b)
seat back restraints reduce the normal stresses and the use of a lumbar pad can reduce anterior
stresses by placing the lumbar spine in extension.
In Latham’s [5] investigation of safe ejection speeds and accelerations, he noted that compressive
loading to the spine can only be safely tolerated if flexion of the spine can be prevented.
Otherwise, as documented in cases of inadvertent ejection-seat deployment in which the pilot was
incorrectly positioned, that compression fractions to the T11 to L2 region were likely. It was
found that correct spinal alignment could be achieved by means of a 3.8 cm (1.5 in) lumbar pad
on the seat back.
Adams et al [6] conducted testing on excised lumbar sections to evaluate the effects of posture on
the compressive strength of the specimen. The objective was to establish a range of flexion and
extension in which the lumbar spine is most resistant to compressive loads. Nineteen lumbar
spines were dissected into 29 motion segments consisting of two vertebrae and the intervening
disks and ligaments. The vertebrae were potted in dental plaster and secured to two endplates that
could be loaded in a computer controlled hydraulic materials testing machine. The endplates
could be angled relative to one another to simulate compression, bending and shear that may act
on a motion segment. The lower endplate was fixed to the hydraulic ram whereas rollers on the
upper endplate were free to roll on a bearing plate attached to a load cell. The height of the rear
roller was adjustable such that the various bending moments could be induced for a given
compressive load. The motion segments were loaded until the elastic limit was reached as
indicated by a reduction in slope of the moment versus flexion angle output graph. The results of
their tests suggest that the lumbar spine is best able to withstand compressive loading when the
motion segment is flexed within 0% to 75% of its flexion range and that the optimum stress
distribution in the disk occurs at 50% of maximum flexion, this appears to contradict Latham’s
4
conclusion that compressive loading can only be tolerated if flexion of the spine can be
prevented.
Preload of the lumbar spine can be introduced by the mass of body worn personal protective
equipment or other equipment acting to apply a compressive load on the intervertebral discs.
Additionally, postural changes that result in non-neutral spine positioning can also introduce
compressive loads from the muscle’s contraction required to maintain a stable spine. These
postural changes could be the result of slouching or raised leg position when seated. Tension in
the musculature acts only to stabilize the spine and in so doing increases the compressive loads on
the intervertebral discs. However, similarly to a neutral spine position the muscles cannot react
fast enough to effect body kinematics during an UBB.
Janevic et al [7] conducted experiments on thirteen motion segments that were mounted in a test
apparatus that used a system of cables and pneumatic cylinder to apply the loads and preloads to
the specimen. The preload was kept constant while various bending moments, shear loads and
one torsion load were applied. Four incrementally increasing loads of 40 N were applied up to a
maximum of 160 N. Similarly, an incremental moment of 4 Nm was applied up to a maximum
16.0 Nm. The sequence of test loads were introduced while a compressive preload of 0 N,
2200 N or 4400 N was applied. The results of the testing indicated that the stiffness of the lumbar
spine in bending, shear and torsion would increase when compressive loads are applied. Figure 2
and Figure 3 show the decrease in displacement (mm or deg) for the applied test loads of 80 N or
8 Nm for shear and flexion respectively.
Figure 2: Mean translational displacements of lumbar spine segments under preload conditions.
5
Figure 3: Mean rotational displacements of lumbar spine segments under preload conditions.
6
3 Upper Body Mass Effects On Lumbar Injury
To be effective, blast attenuating seats must be tuned to the mass of the occupant. If the energy
absorption mechanism is too stiff for a given occupant then the seat may not use its maximum
displacement range or ride-down thereby increasing the loads on the occupant. Conversely, if the
seat is not stiff enough it may bottom out resulting in very high loads being transmitted. To
complicate matters, a military vehicle occupant may be wearing a significant amount of extra
mass due to the protective equipment or other gear that may be worn on their person, typically on
the upper torso degrading the performance of the attenuation system.
Iluk [8][9] used LS-Dyna to evaluate blast loading on three seating configurations. The first seat
configuration employed a constant damping force set for the mass of the ATD used in a typical
STANAG 4569 test. In the second configuration, the constant damping force was proportional to
the real mass of the ATD and the third configuration the damping was proportional to the
measured mass of the ATD including any protective gear worn. The ratio of the actual strain in
the spine to the strain of the base ATD without additional mass was used to compare risk based
on DRIz calculations. For similar loading, a 40% increase in spine loads was observed for the
ATD with the increased torso borne mass while at the same time the calculated DRIz decreased
due to the lower accelerations that would be imparted to a heavier occupant. An alternative
method for computing DRIz that accounts for additional body borne mass was proposed such that
the total occupant mass should be considered in the calculation of DRIz. The rationale being a
seat designed for a 50th percentile occupant may not provide the correct damping for a 5
th
percentile occupant or for the 50th percentile subject wearing heavy ballistic armour.
In a helicopter crash, aircrew are subjected to vertical loading when hitting the ground and it has
been suggested that this loading is similar to that experienced in a surface vehicle hitting the
ground after been launched vertically from the force of a UBB event. The resulting loads on an
aircrew’s spine may be exacerbated by the extra mass of the body borne equipment. This may
include body armour and primary survival gear and other gear such as ammunition, radio, knife
and flashlight that can add between 5 kg to 30 kg of extra mass. Using a finite element model of a
50th percentile Hybrid III, Aggromito et al [10] further evaluated the effects that mass distribution
and placement of the extra items have on the resulting loads and injuries. Aggromito also
investigated whether the mass increase causes the seats to be overloaded in a crash. As indicated,
the seats are designed to absorb vertical loading by collapsing, however, if the total mass on the
seat exceeds its design specifications the seat may bottom out resulting in much higher vertical
loads on the occupant. A Hybrid III ATD with a curved spine was used in their testing although
the straight spine variant would have been preferred but was not available. The findings as they
relate to lumbar loads are summarized here:
lumbar loads increased when seat bottoming occurred, the sooner bottoming occurred the larger the lumbar loads,
equipment placed on the sides of the body produced lower lumbar loads compared to the equipment placed on the front of the torso, and;
lumbar loads increased with equipment bulk which caused the body to move forward, the more offset from the body the larger the lumbar loads.
7
Zhang et al [11] used a high-fidelity finite element model of the pelvis and lumbar spine to
evaluate the potential of lumbar injuries as it relates to the loading severity during the initial
stages of high-rate vertical loading. The effects of added torso borne mass on injury outcome
were also assessed. The lumbar FE model used was developed by Johns Hopkins University
Applied Physics Laboratory (JHU/APL) and is based on geometry obtained from the Visible
Human Project1 and scaled to the dimensions of the average US male. The input to the pelvis and
lumbar spine model was determined from FE simulations with a full body Hybrid III dummy and
applied to the ischial tuberosity. The torso and torso borne equipment were represented by a
couple of masses connected to the upper end of the lumbar spine. The results from the FE
simulations suggested that at high rate loading the added torso borne mass had little effect on the
injury outcome since under severe pelvis acceleration lumbar spine failure would occur
regardless. The extra mass may have had an effect during later stages of the loading event which
were not included in the model run times. It was noted that for lower severity pelvis loading
conditions, the added torso borne mass might have an effect on the maximum lumbar loads.
1 For more information on the Visible Human Project please see:
www.nlm.nih.gov/research/visible/visible_human.html
8
4 Spine Response to Loading
Currently, the Hybrid III antropomorphic test dummy is used in the assessment of occupant injury
during UBB full-scale test programs. However, its lumbar spine was designed for forward
flexion that is common in automotive frontal crashes but it was not intended for the vertical
loading mechanisms of an UBB environment. Additionally, because of the Hybrid III lumbar
spine’s stiffness and curvature, it is difficult to position the dummy in the blast attenuation seating
systems or to have it assume a posture that is less than ideal (i.e. slouched). A stated objective of
the current development program is to design a new functional spine unit (FSU) that could
replace the current Hybrid III spine having greater biofidelity and ability to assume more human-
like postures. In order to accomplish this, specifications for the spine’s stiffness and range of
motion must be developed. The results of a literature review seeking information related to the
mechanical characteristics of the lumbar spine are presented below. Most research reported in the
literature considered ideal loading conditions and therefore necessitates additional fundamental
research to develop lumbar tolerances for out-of-position loading. Regardless, the data that is
available can potentially be used in developing a preliminary definition of a surrogate spine’s
response to UBB loading.
4.1 Response to Compression Loading
Stemper et al [12][13] simulated the vertical loading on the spine during the catapult phase of an
aircraft ejection seat and during a helicopter crash to investigate the fracture patterns from these
high-rate loading events. A drop tower arrangement was used to apply vertical loading to post
mortem human subject (PMHS) spine segments (T12-L5). The upper end of the spine was fixed
to an upper plate such that the L2-L3 intervertebral disk was horizontal. The lower end of the
spine was attached to a bottom plate via a 6 axis load cell. An accelerometer mounted to the
bottom plate measured the input into the system. The upper torso mass was simulated with a
32 kg mass attached to the upper plate. The specimens were pre-flexed with a 5 Nm moment.
Both the upper and lower plates were independently attached to a rail system which guided the
drop assembly in a vertical orientation for impact with a foam pad. Pad materials were selected
to simulate either the loading experienced during the catapult phase of an emergency ejection or
during a helicopter crash.
Compression fractures occurring during the initial loading phase were identified as the primary
mechanism of injury. The peak forces and moments are summarized in Table 1 but there was no
indication of the magnitude at which the injuries occurred. Stemper recognized that the results
are likely dependent on other factors such as column length, curvature, bone quality, spine
orientation and state of flexion or extension when loading is applied, but these variables were not
investigated further.
9
Table 1: Reported lumbar injury from vertical loading of PMHS specimens [13].
Type Peak Axial
Force
(N)
Peak
Moment
(Nm)
Injury Description
Ejection Catapult 1 5598 98 L1- Anterior cortex fracture with endplate fracture
Ejection Catapult 2 5827 166 L1- Burst fracture with retropulsion into spinal canal
Helicopter Crash 1 7184 386 L1 and L2- Anterior compression
Helicopter Crash 2 5236 179 L3- Vertical cortical fracture with laminar fracture
L4- Mild compression fracture of the anterior cortex
Helicopter Crash 3 7821 293 L2- Anterior body fracture including cranial endplate
L2- Vertical cortical fracture of posterior wall
L3- Burst fracture with retropulsion into spinal canal
Yoganandan et al [14] conducted compression tests on 9 FSUs from 6 different donors. In four of
the specimens, the intervertebral disks of the FSU showed signs of degeneration. The specimens
were potted and installed in a servo-hydraulic material test system. A load cell in the test
apparatus’ loading head measured the axial compressive load that was applied at a rate of
2.54 mm/s normally to the mid-plane of the FSU’s intervertebral disk. A typical force deflection
curve is shown in Figure 4 for both a normal and a degenerated intervertebral joint. The
measured mechanical properties are summarized in Table 2.
Figure 4: Compressive force deflection curve for; (a) normal, and; (b) degenerated intervertebral
disk loaded in compression (figure from [14]).
10
Table 2: Mechanical properties determined from the FSU compression tests [14].
Overall Stiffness 2850 ± 293 N/mm
Load at Failure 9.02 ± 1.08 kN
Ultimate Load 11.03 ± 1.42 kN
Years later, Yoganandan et al [15] investigated the mechanism of compression related injuries of
the thoracolumbar spine seen during automotive frontal crashes. Laboratory tests comprising
vertical impact tests on spinal columns obtained from unembalmed post mortem human subject
(PMHS) were conducted.
Similar to Stemper, the lower end of the spinal section was potted and fixed to a metal plate
through a load cell. The upper end was similarly potted and fixed to an upper metal plate with
5 Nm of induced flexion. The entire assembly was dropped in guided free fall on a custom drop
tower with the bottom plate striking an impact pad, simulating the loading from a seat into the
pelvis and lumbar spine of a vehicle occupant. An accelerometer in the lower steel plate
measured the input into the system. Three drops of increasing energy levels were conducted for
each specimen; the first two drop energies were non-injurious, while the third was sufficient to
cause injury. The extent of injury was assessed using pre and post-test radiographs and CT scans.
The authors recognized that repeated impacts to the same test specimen may decrease its
tolerance levels during subsequent impacts, therefore, the results obtained are considered to be
conservative estimates of the failure loads. A logistic regression analysis indicated that a peak
compressive force of 3.7 kN is associated with a 50% probability of injury in the thoracolumbar
spine. The authors speculated that if only the lumbar spine was included in the test that the load
required to cause a 50% probability of injury would be greater than 3.7 kN, so again the results
are conservative. The logist curves for probability of injury obtained are presented in Figure 5.
Figure 5: Probability curves for spinal injury due to compressive loading (figure from [15]).
Kemper et al [16] investigated the effect of loading rate on the compressive stiffness of lumbar
intervertebral disks. Thirty-three (33) compression tests were conducted on 11 FSU obtained
11
from six fresh frozen human lumbar spines. The cranial vertebral body of the FSUs were potted
such that the mid-plane of the disk was parallel to the potting cup and attached to the test
apparatus. The caudal vertebra was lowered into the second potting cup which prevented any
moment from being introduced. The test apparatus comprised of a hydraulic material test system
with a five-axis load cell for measuring the reactionary loads and a single axis load cell for
measuring the applied impact load. Accelerometers were also placed on the impactor and the
impact plate.
The FSUs were preconditioned with 10 cycles of a 0.5 mm displacement at 0.1 m/s and then
preloaded to 88.96 N followed by a 0.5 mm and a 1.0 mm dynamic step inputs loaded at a rate of
0.1 m/s and 0.2 m/s respectively. The preload of 88.96 N was reconfirmed and the FSUs were
then loaded to failure at a rate of 1 m/s. The measured stiffness was found to be independent of
the vertebral level from which the FSU had been harvested but it increased with the rate at which
the specimen was loaded, as shown in Figure 6.
Figure 6: Compressive stiffness of intervertebral disks by lumbar level and loading rate [16].
The average stiffness for each loading rate is summarized in Table 3. The strain rates were
established using the measured disk heights.
Table 3: Summary of average FSU stiffness [17].
Loading Rate (m/s) Average Stiffness (N/mm) Strain Rate (s-1)
0.1 1835 ± 645.6 6.8 ± 1.5
0.2 2489.5 ± 474.1 13.5 ± 2.0
1.0 6551.1 ± 2017.0 72.7 ± 16.8
12
Combining his results with previous published data, Kemper proposed the relationship between
stiffness and strain rate shown in Equation (1) and the effective stiffness for the full lumbar spine
is given by Equation (2).
𝑘 = 57.328𝜀 + 2019.1 (1)
𝑘𝑒𝑓𝑓 = 1
[∑1
𝑘𝑁𝑁1 ]
; 𝑁 = 5 (2)
4.2 Response to Shear Loading
The shear strength of the lumbar spine as it relates to bone mineral density (BMD) and disk
height reduction was investigated by Skrzypiec et al [17] in laboratory experiments using 29 L2-
L3 motion segments comprised of the intervertebral disk, adjacent vertebrae, apophyseal joint and
ligaments. The motion segments were categorized into three groups: young-no-creep, young-
creep and finally old-no-creep. Creep is the reduction in disk height due to a sustained
compressive load on the disk. For these tests creep was introduce by applying a 1000 N load for
one hour prior to testing. The vertebrae were positioned in metal cups and embedded in resin.
The cups were mounted to a servo-hydraulic testing machine such that the axis of the spine was
horizontal with the anterior side facing up. The caudal vertebra was fixed to the testing machine
via a 6-axis load cell and a dead weight and cable/pulley system applied a 500 N compressive
load to the joint while fore-aft shear was introduced through a 15 mm displacement of the cranial
vertebrae. Throughout testing, the motion segment was immersed in a Ringer solution to
maintain its hydration.
The force deflection during the initial stages of shear displacement were found to be somewhat
linear in both the anterior and posterior directions, however, the stiffness was higher in the
anterior direction which is likely due to the overlapping geometry of the apophyseal joint. Not all
the segments failed within the 15 mm displacement of the cranial vertebra but failures did
typically demonstrate load-displacement curves that reached a plateau rather than failing in a
brittle manner. It was further noted that the motion segment exhibited an increase in height as the
shear displacement was applied. A summary of the results is presented in Table 4 below and
sample load-displacement curves are presented in Figure 7.
Table 4: Summary of lumbar spine segment shear test results [17].
Group Stiffness Stiffness after creep Yield Peak
Anterior (N/mm)
Posterior (N/mm)
Anterior (N/mm)
Posterior (N/mm)
Force (kN)
Disp. (mm)
Force (kN)
Disp. (mm)
Young-No-Creep 565 366 - - 1.57 4.20 3.29 13.14
Young-Creep 515 318 566 254 2.01 4.99 3.57 13.43
Old-No-Creep 480 342 - - 1.79 5.02 2.90 12.74
13
Figure 7: Typical shear results for a L2-L3 motion segment (figure from [17]).
4.3 Response to Flexion-Shear Loading
Schultz et al [18] tested 42 motion segments obtained from 24 fresh lumbar spine sections. The
cranial and caudal sections were potted in epoxy resin and secured in a cylindrical test fixture.
The caudal fixture was clamped to the test machine base while the cranial section was
unconstrained. Through a series of wire attachments to the specimen’s cranial support tube
flexion, extension and lateral moments could be applied to the motion segment. A re-
configuration of the wire connections to the specimen’s test fixture allowed for torsional loading
to be applied. Bending and torsion loads up to 20 Nm and shear loads up to 205 N were applied
to the cranial support fixture using the wire loading system. A constant 400 N compressive load,
approximating the weight of the body above L3, was applied for all the tests. The mean
responses for the testing of the different loading modes were presented graphically and are shown
in Figure 8. The tests were repeated with the posterior elements of the motion segments removed.
14
Figure 8: Mean flexion, extension, lateral bending and torsion response of motion segments
tested by Schultz et al [18]. Dashed lines are tests with the posterior elements removed.
In follow-on testing to that conducted by Schultz [18], Berkson et al [19] conducted compression
and shear tests on the same motion segment specimens using the same test machine to apply shear
and compressive loads. The results of these additional tests are shown graphically in Figure 9.
15
Figure 9: Mean compression, lateral, anterior and posterior shear response of motion segments
tested. Dashed lines are tests with the posterior elements removed (figure from [19]).
Osvalder et al [20] conducted laboratory experiments to assess the ultimate strength of the lumbar
spine in flexion. Sixteen motion segments comprising an intervertebral disk and the adjacent
vertebra were subjected to an increasing static bending and shearing load up until the point of
complete failure. The motion segment specimens were extracted from PMHS lumbar spines
(T12-L5) and consisted of L1-L2 vertebra, L2-L3 vertebra or L3-L4 vertebra. For the testing, the
cranial and caudal vertebrae were potted in metal cups. The caudal cup was rigidly attached to a
force plate for measuring the reaction loads from a moment applied to the cranial vertebra by a
vertical lever arm affixed to the upper mounting cup. Regardless of the composition of the FSU,
complete failure occurred at an applied moment of 156±11 Nm with a corresponding shear of
620±53 N and there was no correlation between the lumbar spine levels tested. None of the
specimens failed below 135 Nm in bending and 520 N in shear. Just prior to failure, the tension
in the rear portion of the motion segment was 2.8±0.2 kN. A strong correlation between the bone
mineral density (BMD) of the adjacent vertebra and the ultimate strength was noted, as was also
noted in Neumann et al’s [21] analysis of the data. Moment versus angle-of-rotation for the
cranial vertebra is shown in Figure 10. The force and moment results are summarized in Table 5.
16
Figure 10: Flexion and versus bending moment at failure of lumbar motion segments (figure from
[20]).
Table 5: Summary of lumbar motion segment loads at failure [20].
Spine Level At Failure Maximum
Bending Moment
(Nm)
Shear Force (N) Tensile Force – posterior
structure (N)
Flexion (deg) Horizontal
Displacement (mm)
L1-L2 154 ± 6 600 ± 28 2.8 ± 0.2 17.3 ± 1.0 8.5 ± 1.4
L2-L3 153 ± 5 616 ± 22 2.7 ± 0.1 21.5 ± 0.8 9.4 ± 1.5
L3-L4 161 ± 16 640 ± 80 2.9 ± 0.2 19.8 ± 0.9 10.4 ± 2.4
Osvalder et al [22] conducted additional experiments on 20 motion segments to look at their
response to combined dynamic bending and shear. L1-L2 or L3-L4 motions segments were
mounted in a test fixture with the caudal end affixed to a load and rigidly attached to the ground.
A 12 kg mass applied a preload on the end of the motion segment. A combined shear and
bending moment was applied with a 20 kg padded pendulum that struck a vertically mounted
leaver arm that was rigidly attached to the cranial vertebra. Either a moderate or severe pendulum
impact, as defined by an accelerometer on the pendulum, was applied to the specimens. A
pendulum acceleration of 5 G with a rise time of 30 ms and duration of 150 ms was considered
moderate whereas an acceleration of 12 G with a rise time of 15 ms and duration of 250 ms was
considered severe. The results of the testing are presented in Table 6 below.
Using the same test methodology, Osvalder et al [23] conducted a similar test series on 48
additional motion segments. However, in addition to the moderate and severe test conditions a
medium condition defined by an 8 G pendulum acceleration pulse was also added. The data for
all the tests from both test programs are summarized in Table 6 below. The values presented are
the maximum before a noticeable dip in the output was observed.
17
Table 6: Summary of results, combined dynamic bending and shear [22] and [23].
Impact Severity
Peak Accel.
(G)
Rise Time
(ms)
Moment (Nm) Shear Force (N)
Flexion (deg)
Horizontal Displacement
(mm)
Vertical Displacement
(mm)
Moderate 1 5 30 140 ± 20 458 ± 73 13.7 ± 2.4 6.6 ± 1.7 14.1 ± 1.4
Moderate 2 5 15 149 ± 27 466 ± 73 NA NA NA
Medium 1 8 30 160 ± 15 480 ± 65 15.4 ± 2.9 7.3 ± 1.2 15.1 ± 1.1
Medium 2 8 15 170 ± 15 503 ± 72.5 14.8 ± 1.5 7.0 ± 1.5 14.9 ± 1.8
Severe 1 12 15 183 ± 33 620 ± 94 18.8 ± 2.5 8.5 ± 3.2 18.2 ± 2.4
Severe 2 12 5 200 ± 25 663 ± 58 18.1 ± 3 7.9 ± 1.7 17.6 ± 2.5
There were indications of injury onset in all the tests that was evident by a distinct dip in the
measured force and moment response as seen in a typical bending moment response shown in
Figure 11.
Figure 11: Typical bending moment versus time response for severe load with a 15 ms and a 5 ms
pulse rise time (figure from [23]).
Neumann et al [24] determined the injury threshold of 11 motion segments loaded in combined
flexion and shear. Four spines were sectioned into motion segments comprising T12-L1, L2-L3
and L4-L5. The specimens were potted and loaded and unloaded in 20 N increments until the
first signs of injury were detected as evident by a dip of 50 N or 15 Nm in the force deflection or
moment deflection responses respectively. The load was applied in the anterior direction to a
vertical lever arm affixed to the cranial vertebra of a vertically mounted motion segment.
Permanent deformation was recorded at an applied moment of 121 Nm (SD = 10 Nm) or 486 N
shear force (SD = 38 N). Pertinent results from Neumann’s experiments are summarized in
Table 7.
18
Table 7: Summary of lumbar motion segment flexion-shear test results for Neumann et al[24].
Parameter Measured result (standard deviation)
Bending Moment (Nm) 121 (10)
Shear Force (N) 486 (38)
Horizontal Displacement (mm) 7.5 (1.4)
Vertical Displacement (mm) 16.9 (1.4)
Flexion Angle (deg) 15.8 (0.9)
Bending Stiffness (Nm/deg) 7.5 (1.6)
Shear Stiffness (N/mm) 71 (7)
Adams et al [25] conducted similar experiments to Osvalder with the exception that a
compression creep test was performed on 15 PMHS specimens to ensure the water content of the
disc lay within the physiological range. This was accomplished by applying a compressive force
of between 1000 N and 2000 N depending on the specimen’s age for a period of 2 and 3 hours.
This procedure reduced the overall height of the motion segments by 1.09±0.4 mm. The motion
segments were then flexed to failure. The elastic limit of the specimens was reached at
72.8±18.1 Nm with a rotation angle of 14.8±3.3°. Whereas previous failure of the motion
segment was identified by overt indications in the Osvalder experiments, Adams identified failure
by a slight reduction in the loading curve indicating that the elastic limit of flexion had been
reached and that at this stage of flexion only the supraspinous/interspinous ligaments are damaged
which would not have been noticed in the previous experiments. Moment versus angle-of-
rotation for a typical test is shown in Figure 12.
Figure 12: Moment deflection curve up to the elastic limit of the FSU (figure from [25]).
In her master’s thesis, Belwadi [26] investigated combined anterior shear and flexion of the
lumbar spine that may occur in a frontal automotive crash in which knee bolsters are deployed.
Knee bolsters could restrict forward motion of the pelvis allowing for a greater relative motion
between the upper and lower torso.
19
The response of 7 full cadaveric lumbar spines (T12-Sacrum) to sub-injurious
tension-compression, flexion-extension, shear, and combined loading was measured in a spine
testing machine that could apply a fixed displacement and/or rotation to the cranial end of the test
specimen. The full spine specimens were then sectioned through the L3 vertebral to obtain 11
motion segments comprising three vertebra and two discs. Each motion segment was also tested
similarly to the full sections. Failure in the combined shear-flexion mode was noted in eight of
the 155 total tests that were performed. The failure forces and moments for these tests are
summarized in Table 8.
Table 8: Lumbar motion segment failure loads and their corresponding displacements [26].
Motion Segment No Shear Flexion
Force (N) Displacement (mm) Moment (Nm) Angle (deg)
Sacrum to L4 3 1936.7 ± 554.1 10.7 ± 0.6 216.6 ± 20.8 13.1 ± 1.4
L2 to T12 5 1962.2 ± 687.4 10.5 ± 4.3 186.1 ± 97.7 15.1 ± 2.3
Average 1952.5 ± 598.2 10.6 ± 3.3 197.5 ± 76.4 14.4 ± 2.3
4.4 Range of Motion
There is limited information in the literature specific to lumbar range of motion that would be
pertinent to the development of an ATD spine. There is a plethora related to range of motion for
various daily activities and chronic back pain, however, these were specific to the modality being
investigated.
A comprehensive review of spine mobility was reported by Nyquist and King [27]. Nyquist and
Merton [28] performed experiments on six male volunteers to establish static range of motion
from T8 to the pelvis. Full range of motion with straight legs was 120° but increased to 143° when legs were flexed 90°. Dynamic range of motion was determined by Cheng et al. [29] using a test sled for accelerations up to 8 G. Range of Motion (ROM) for T12/Pelvis was determined
for both male and female subjects, and in a tensed and relaxed condition. Angles (± 1 SD) of
22.7±6.8 to 28.0±4.3 degrees were observed.
Demetropoulos et. al. [30] looked at the flexion and extension properties of cadaveric lumbar
specimens, both with and without simulated muscle tension. Without muscle tension, the flexion
results were quite variable, however, when simulated muscle tension was applied, the results
became much more coherent (96.5°±1.76).
For the most recent frontal automotive ATD development program, the THOR dummy, it was
determined that the existing information was insufficient to specify any spine kinematic response
requirements [31].
20
5 Existing Injury Criteria
5.1 Eiband Injury Tolerance Curve for Vertical Acceleration
The Eiband injury tolerance curve was proposed for assessing the risk of injury from vertical
impacts [32][33]. It suggested that under vertical loading conditions, human volunteers tolerated
acceleration levels of 10 G for 0.1 s and 15 G for 0.05 s. Adding data obtained from animal tests
the criteria was expanded to exposure limits for moderately and severely injured occupants. The
limitation of the criterion is that it did not distinguish amongst body regions and it was not
sensitive to pulse shape and or duration. The Eiband tolerance curve is shown in Figure 13.
Figure 13: Eiband injury tolerance curve for vertical acceleration (figure from [32]).
5.2 Dynamic Response Index
The Dynamic Response Index (DRI) [33] is used as a lumbar spine injury assessment reference
value for blast tests of vehicle and seating systems. The calculation for DRI is based on the
response of a lumped mass model representation of the spinal column (see Figure 14). The
criteria DRIz denotes loading in the vertical direction. The input into the model was originally
the vertical acceleration of the seat pan of an aircrew ejection seat but its use has been modified
for blast attenuation using the vertical acceleration of the ATD’s pelvis during the experimental
trials. The maximum value of the deflection response is the value of DRI which has been
correlated to experimental and operational injury data (see Figure 15).
21
Figure 14: DRI lumped mass model of the spine (figure from [33]).
Figure 15: DRI versus spinal injury rate (figure from [32]).
The equation of motion for DRI’s lumped mass model is:
Ζ̈(𝑡) = �̈� + 2 𝜁 𝜔𝑛 �̇� + 𝜔𝑛2 𝛿 (3)
Where:
Ζ̈(𝑡) is the pelvis acceleration in the vertical direction
𝛿 = 𝜉1 − 𝜉2 (when delta > 0) is the compression of the system
𝜁 =𝑐
2 𝑚 𝜔𝑛 is the damping coefficient (0.224)
𝜔𝑛 = √𝑘
𝑚 is the circular frequency (52.9 rad/s)
22
DRI is calculated with the maximum compression 𝛿𝑚𝑎𝑥, 𝜔𝑛2 and the acceleration of gravity ‘g’ is
(9.81 m/s):
𝐷𝑅𝐼𝑧 =𝜔𝑛
2 𝛿𝑚𝑎𝑥𝑔
(4)
A DRIz value of 17.7 is currently used as the pass-fail criteria in the AEP-55 test procedures [34].
Spurrier et al [35] suggests that the DRI criterion is inappropriate for use in assessing the
probability of spine injury in vehicle blast scenarios. A comparison of injuries locations amongst
aircrew during ejection, for which DRI was developed, and those of vehicle occupants subjected
to UBB showed that the location of injury varied significantly between the two events. Spine
injuries from aircraft ejection were primarily to the thoracic spine whereas injuries from UBB we
predominant in the lumbar spine, suggesting the mechanisms of injury are very different.
Furthermore, DRI is intended for assessing the probability of injury to vertical loading and is not
specific to the lumbar spine. In an UBB, the deformation of the vehicle floor pan may push up on
the occupant legs thereby rotating the pelvis and lumbar spine such that they are no longer
aligned with the direction of loading. The DRI would then underestimate the severity of the
loading.
5.3 Multi-axial Dynamic Response Criteria
The Multi-axial Dynamic Response Criteria is referred to as the Brinkley Dynamic Response
Criteria (BDRC) by the National Aeronautics and Space Administration (NASA) [36]. It is
similar to the computation of the DRI except that the BDRC is based on the response of three
lumped mass models representing the three orthogonal axes with the origin located at the critical
point and is used to calculate a general whole body injury risk. For a seated occupant the critical
point is fixed relative to the seat coordinate system and shown in Figure 16.
Figure 16: Critical point for computing BDRC (figure from [36]).
23
The equation for the BDRC lumped mass models, for each of the three orthogonal directions, is
given by Equation 5.
𝐴(𝑡) = �̈�(𝑡) + 2 𝜁 𝜔𝑛 �̇�(𝑡) + 𝜔𝑛2 𝛿(𝑡) (5)
Where:
�̈�(𝑡) is the occupants acceleration in the inertial frame
�̇�(𝑡) is the occupants relative velocity with respect to the critical point
𝛿(𝑡) is the displacement of the occupant’s body with respect to the critical point
𝜁 the damping coefficient ratio
𝜔𝑛 undamped natural frequency of the dynamic
𝐴(𝑡) is the measured acceleration, per axis, at the critical point. Rotational accelerations must be considered when computing the linear accelerations at the
critical point
The coefficients to be used in the computation of the BDRC for each of the three orthogonal axes
are presented in Table 9.
Table 9: BDRC model coefficients.
Coefficient X
displacement direction
Y
displacement direction
Z
displacement direction
X0 Y0 Z0
𝜔𝑛 56.0 62.8 58.0 58.0 47.1 52.9
𝜁 0.04 0.2 0.07 0.07 0.24 0.224
For each axis, the dynamic response is calculated according to Equation (6) and the risk of injury
(β) is obtained from Equation (7). The dynamic response limits for each axis are presented in
Table 10. The injury risk (β) is first calculated using the DRlimit
for the “low” risk and if it is less
than 1 then the value represents the risk of injury. If it is greater than 1 then the injury risk is
recalculated using the next higher DRlimit
.
𝐷𝑅 =𝜔𝑛
2 ∙ 𝛿(𝑡)
𝑔 (6)
𝛽(𝑡) = √(𝐷𝑅𝑥(𝑡)
𝐷𝑅𝑥𝑙𝑖𝑚
)
2
+ (𝐷𝑅𝑦(𝑡)
𝐷𝑅𝑦𝑙𝑖𝑚
)
2
+ (𝐷𝑅𝑧(𝑡)
𝐷𝑅𝑧𝑙𝑖𝑚
)
2
(7)
24
Table 10: Dynamic response limits, DRlimit
, for use in injury risk calculations (Equation 7).
Axis Displacement
direction
Low (
25
5.5 Spine Injury Criterion
Dosquet et al [39] proposed a spine injury criterion (SIC) that is based on the effective impulse to
the spine and is calculated by integrating the applied force to the spine over time. In an analysis
of over 200 tests on a vertical drop tower where seated Hybrid III manikins were dropped in free
fall, a correlation between SIC and DRI was obtained. It was also determined that the best
correlation was obtained if the difference between the limits of integration was 40 ms with the use
of an exponent of 1.2. The SIC equation is:
𝑆𝐼𝐶 = 𝑠𝑢𝑝𝑡1, 𝑡2 {(1
𝑡2−𝑡1∫ 𝐹𝑑𝑡
𝑡2𝑡1
)1.2
∗ (𝑡2 − 𝑡1)} with t2 – t2 = 40 ms (8)
The correlation between SIC and DRI as seen in Figure 17 is:
𝐷𝑅𝐼 = 2.39 − 2 ∗ 𝑆𝐼𝐶 (9)
Figure 17: Correlation between DRI and SIC (figure from [39]).
26
6 Anthropomorphic Test Devices
There are several anthropomorphic test devices (ATD) that are available commercially and their
suitability for UBB injury assessment is briefly discussed in the following sections.
6.1 Frontal Impact Dummies
6.1.1 Hybrid III
The Hybrid III ATD was developed by General Motors in the 1970’s to address the need for a
more biofidelic crash test dummy than was available at the time. It was adopted into the United
States’ Federal Motor Vehicle Safety Standards in 1986, and has become the worldwide standard
for use in frontal impact crashworthiness testing. Due to its extensive use, and availability, the
Hybrid III is also used in many other non-automotive applications where the use of an ATD is
required (e.g. sports equipment testing, military testing), including UBB testing. The Hybrid III’s
biofidelity in many of these applications has not been demonstrated.
The lumbar spine of the Hybrid III is a polyacrylate elastomer member which is rigidly attached
to the dummies thoracic spine and pelvis. Two steel cables run through the mid-coronal plane of
the lumbar spine, providing side support while permitting fore-aft flex.
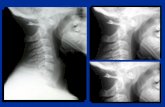
Three versions of the Hybrid III lumbar spine are produced as shown in Figure 18. The standard
version is curved to permit the dummy to be accurately placed in a seated posture within an
automotive vehicle. A straight version is also available to place the dummy in an erect stance for
use in pedestrian impact testing, as well as a Hybrid II based straight spine version designed for
aircraft seat testing which is incorporated into the FAA-Hybrid III dummy.
a) b) c)
Figure 18: Three types of Hybrid III spines are available: a) curved spine, b) pedestrian straight
spine, and c) FAA straight spine.
27
The Hybrid III instrumentation includes:
six-axis lower lumbar spine load cell, and;
tri-axial pelvis acceleration.
Injury risk functions for the spine when using the Hybrid III have centered on the use of DRIz.
Two risk curves appear in the literature, one created from operational data and another from lab
data [40]. The lab data presents a more conservative curve, so this has been used to calculate an
Injury Assessment Reference Value (IARV) of 17.7 (10% risk of AIS2+) [40][41].
ATD’s like the Hybrid III are instrumented to directly measure lumbar force. Compressive
Lumbar Load (LL) uses the load cell input to develop Peak LL (Compressive) criterion.
Attempts to create a criterion for LL have produced values of 5598 N to 6675 N by correlating
compression to DRIz, or by scaling neck IARV data [40][42].
6.1.2 THOR-M
The THOR (Test device for Human Occupant Restraint) dummy was developed by the US
Department of Transportation, National Highway Traffic Administration (NHTSA) to improve on
the biofidelity of the Hybrid III ATD2. It includes extensive instrumentation to assess the
performance of vehicle safety systems designed to mitigate injuries in frontal and frontal oblique
crashes. It is not currently used in the regulation of automotive safety systems.
The lumbar spine is comprised predominantly of metal components, however there is a short
(76 mm) butyl rubber flex joint to provide some lumbar compliance. This flex joint, like the
Hybrid III, has two steel cables running internally on the mid-coronal plane to provide lateral
stability. The lumbar spine is rigidly attached to the pelvis but an adjustable joint is provided at
the thoracolumbar joint to aid dummy positioning. The Thor spine is depicted in Figure 19.
Figure 19: THOR spine (image from [43]).
2 http://www.nhtsa.gov/Research/Biomechanics+&+Trauma/THOR+50th+Male+ATD
28
THOR’s relevant instrumentation includes:
5 axis lower thoracic (T12) load cell,
tri-axial lower thoracic (T12) acceleration, and;
tri-axial pelvis acceleration.
No injury reference values specific to the THOR were found. The limited availability of the
dummy is reflected in its restricted use in the field. FE modeling using the THOR was noted,
with Lumbar Loading Criterion being used, and the values being the same as for the Hybrid III
[44].
6.2 Rear Impact Dummies
6.2.1 RID3D
The RID3D is a rear impact dummy developed in the early 2000’s as an improvement on the
RID2 ATD. It is based on the THOR frontal impact dummy, having a THOR thorax, however,
the lumbar spine is a straight cylindrical rubber component adopted from the EUROSID-1
dummy [45] (Figure 20). It has been validated for rear impact scenarios up to 60 km/h and 15 G
[46] but no validation work has focused on impact biofidelity specific to the lumbar spine.
Figure 20: RID3D (image from [47]).
The RID3D has the same adjustment at the thoracolumbar connection as the THOR dummy. A
group of researchers used the RID3D while testing lifeboats used on oil rig platforms. These
boats are dropped from a height of 30 m, and in one case, the dummy is placed in a supine
position with the legs crouched. They noted that the RID3D was the rear impact dummy with
enough lumbar adjustment and flexibility to permit the correct seating position [46].
29
The RID3D instrumentation includes:
6 axis lower thoracic (T12-L1) load cell,
tri-axial lower thoracic (T12-L1) acceleration, and;
tri-axial pelvic acceleration
No lumbar injury assessment risk values are available for the RID3D. Rear impact dummy IARV
work is concentrated on cervical spine injuries.
A.1.1 BioRID II
The BioRID II dummy was developed at Chalmers University through the late 1990’s into the
2000’s. The key distinguishing feature of the BioRID II is the spine which consists of 24
individual articulating components representing the human vertebrae (see Figure 21). Rubber
bumpers are glued to the spine segments. Motion of the spine is constrained to the mid-sagittal
plane.
Figure 21: BioRID II Spine (image from [48]).
The researchers who used the RID3D to assess drop launched life boats also considered the
BioRID II, however, it did not have the same degree of lumbar flexibility and adjustment.
Depending on the seating configuration, the BioRID II may offer better conformance to the
seat [49].
30
The complexity of the spine also has raised concerns regarding durability, repeatability and
reproducibility [45]. This would be of particular concern when considering UBB testing.
The BioRID II instrumentation includes:
bi-axial lower thoracic (T12-L1) acceleration,
tri-axial pelvic acceleration, and;
five-axis lumbar load cell (L5).
No injury assessment values are available for the lumbar spine of the BioRID II [45].
6.3 Side Impact Dummies
Side impact dummies were considered for this review but deemed inappropriate given that the
primary direction of impact during underbody mine blasts will be in vertical or the fore-aft
direction.
6.4 Other Dummies
6.4.1 ADAM Dummy
The ADAM (Advanced Dynamic Anthropomorphic Manikin) dummy was developed for the
United States Air Force as a biofidelic test device for assessing high performance aircraft escape
systems [50]. The spine of the ADAM dummy is comprised of a helical spring and damper
system which provides movement along the axis of the spine (z-direction). A universal joint joins
the spine to the pelvis in the lumbar region permitting pitch and roll rotation (y and x axis
rotation, respectively) of the pelvis relative to the spine. Yaw rotation of the torso relative to the
pelvis is accomplished in the spine piston assembly (see Figure 22).
31
Figure 22: ADAM Spine (image from [50]).
The ADAM ATD’s instrumentation includes:
six axis lower lumbar spine load cell,
triaxial Pelvis acceleration, and;
lumbar position; yaw and pitch (potentiometer).
Raddin et al [51] have detailed various injury probability assessment criteria for the ADAM
dummy. When considering spinal injury, they are of the opinion that DRI has been successful in
predicting spinal injury. They, therefore, have not devoted much effort to developing any new
criterion and propose using DRI as the spinal injury criterion.
After making this proposal, they do suggest the possibility of using the data from the pelvic
accelerometers, and lumbar/pelvic load cell as input to two separate strain based models similar to
that which they have suggested for other regions of the body (e.g. neck). Figure 23 shows the
spine criterion for acceleration while Figure 24 shows the force-based criterion. SX, SY and SZ are
the strains caused by acceleration in the x, y and z directions, respectively. For the force-based
criterion, SA is strain in the axial direction, SM is the strain caused by the applied moment, and SS
is the shear strain. It is unclear how these would be used practically and if the research into the
required limits is available.
32
Figure 23: Spine criterion – acceleration (image from [51]).
Figure 24: Spine criterion – force (image from [51]).
6.4.2 WIAMan
The US Army, under direction of the US Army Research Development and Engineering
Command, have embarked on a project to develop a next generation ATD, designed specifically
to look at the threats experienced by soldiers. The Warrior Injury Assessment Manikin
(WIAMan) project is an extensive development program which includes looking at operational
injuries from Iraq and Afghanistan, cadaveric testing, and the development of new injury risk
curves. Within the development plan, the lumbar spine has been identified as a key area.
The program is ongoing, and there is very little information available in the public domain. A
program overview is available from Tegtmeyer [52].
33
7 Surrogate Spine Development Approach
The purpose of an ATD is to act as a human surrogate in environments that would otherwise be
harmful or deadly to a human and to provide quantitative feedback of the loads that would be
experienced by a human. Feedback of an ATD’s response is obtained by measurement
transducers that may measure any combination of acceleration, forces, moments and
displacements at any location on the ATD. For these measurements to be meaningful the ATDs
response to outside loading environments must be “biofidelic” or representative of a human’s
response. Furthermore, as a practical tool for experimentation the ATD must be durable while
providing repeatable and reproducible responses to similar input conditions.
The Hybrid III, which is widely used in vehicle blast testing, was originally designed for
automotive crash testing for which it is well suited and meets the criteria listed above. However,
for blast testing or more specifically, for vertical loading from UBB, the Hybrid III’s lumbar
spine response is believed to be inadequate for assessing the variables that may influence injury.
The approach to be followed in the development of a new surrogate lumbar spine is to model the
dynamic response and range of mobility of the human spine without necessarily duplicating the
complex vertebral geometry, connective ligaments or supporting musculature and tendons of the
human lumbar spine. The steps to be followed in the lumbar spine development are outlined
below:
Define the loading mechanism(s): In the case of UBB it is believed to be a combination of flexion-shear with an axial compressive component, predominantly
in the mid-sagittal plane.
Define dynamic response corridors: The results of the literature review, as it pertains to the loading mechanisms and modes of interest, can be used to define a
preliminary set of human response corridors for dynamic loading. The biofidelity of
a newly designed ATD lumbar spine will be assessed in comparison to these
response corridors. Ideally, fundamental research should be performed to establish
response corridors for the exact loading conditions of interest but this is costly and
may be outside the scope of the project.
Define the ROM: The neutral range of motion and degrees of freedom required for correct placement and posture within the blast mitigating systems is to be defined.
Limiting the required degrees of freedom will improve repeatability and
reproducibility.
Define injury probability criteria and thresholds: These criteria and thresholds will be used to assess the response of the ATD during UBB and to determine the
effectiveness of a countermeasure at preventing or mitigating injury.
Define FSU’s mechanical parameters:
Geometrical and body segment mass constraints
Compatibility with Hybrid III thorax and pelvis
Range of adjustability
34
Identify required instrumentation: The instrumentation requirements will principally be selected to support the calculation of the anticipated injury assessment
reference values (IARV). The IARVs are the transfer function that correlates the
response of the FSU and its injury prediction to that of a human lumbar spine.
FSU component design: The FSU will be designed and a manufacturing package assembled for the production of a prototype unit. Included will be the component
drawings, material and hardware specifications.
Prototype fabrication: A prototype FSU will be manufactured and assembled with subsequent sub-system and full Hybrid III ATD system installations.
Prototype prove-out testing: Laboratory tests of the FSU sub-system and full system installed in an ATD are to be conducted to confirm biofidelity, repeatability
and durability. The test matrix will investigate the FSU’s response to different
energy levels and pre-impact posture.
Match pair testing: Ideally final prove-out testing of the ATD can be done in direct comparison with PMHS subjects. Correlation between the ATD and PMHS can be
confirmed and the IARVs validated.
35
8 Summary and Conclusion
Vehicle designs have evolved to offer protection against underbody blast, nevertheless, an
increase in spinal injuries related to improvised explosive devices (a weapon of choice in recent
conflicts), has been observed. The prevalence of lumbar spine injuries from underbody blast
amongst CF personnel has been noted to result in debilitating long terms effects on mounted CF
servicemen and women.
A literature review has been conducted to determine the current state of knowledge pertaining to
the effect of seating posture and increased inertial loads from body borne equipment on lumbar
spine loads during a UBB incident. Biofidelity requirements such as range of motion, spine
segment stiffness and the influence of posture, which could help in the development of
specifications for a new functional spine unit for a test surrogate, were sought. The information
gained will support DRDC’s investigation of lumbar spine injuries in the CF and the development
of a surrogate spine to realistically assess seating systems’ performance during UBB experiments.
Blast attenuating seats installed in military vehicles attempt to reduce direct transmission of UBB
loads to the occupants. The effectiveness of these seats is partly influenced by the occupant’s
posture which in military vehicles is often less than ideal. The additional bulk and mass of
standard issue personal protective equipment make it difficult for a soldier to assume a correct
seating posture and often an out-of-position or slouched seating posture is all that is possible.
The postural changes that result in non-neutral spine positioning introduce compressive loads
from the muscles contraction required to maintain a stable spine. Preload of the lumbar spine can
also be introduced by the added mass of personal protective equipment acting to apply a
compressive load on the intervertebral discs. This initial muscle tension acts only to stabilize the
spine and in so doing increases the inherent compressive loads. However, the muscles cannot
react fast enough to affect body kinematics during an UBB.
There is only limited pilot ejection seat data available that relates high rate vertical loading of the
spine and with the associated injuries. The available data does suggest that spinal alignment at
the time of ejection determines the location and magnitude of stresses applied to the spine and
that loading to the spine can only be safely tolerated if flexion of the spine can be prevented. The
use of a lumbar pad was found to aid in correct spinal alignment.
In addition to the occupant’s posture, blast attenuating seats must be tuned to the mass of the
occupant to be effective. A seat may not use its maximum ride-down distance if its damping
mechanism is too stiff for the occupant. Conversely, a mechanism that is too soft may bottom out
resulting in very high loads being transmitted. That being said an occupant’s extra mass from
body borne equipment may degrade the optimum performance of a seating system. The
following observations were noted during helicopter crash tests:
lumbar loads increased when seat bottoming occurred, the sooner bottoming occurred the larger the lumbar loads,
equipment placed on the sides of the body produced lower lumbar loads compared to the equipment placed on the centre of the body, and;
36
lumbar loads increased with equipment bulk which caused the body to move forward. The more offset from the body the larger the lumbar loads.
However, numerical simulations by Zhang [11] suggested that added torso borne mass had little
effect on the injury outcome since, under severe pelvis acceleration, lumbar spine failure would
occur regardless.
The Hybrid III anthropomorphic test device (ATD) used during full scale UBB blast trials was
designed for forward flexion that is common with automotive frontal crashes. This ATD is
believed to be inadequate for UBB because it does not respond properly to the various modes of
dynamic loading that can occur during UBB. The development of a new test dummy must
include the ability for the lumbar spine to be correctly oriented during initial ATD placement and
have the required sensing capabilities to monitor for combined loading conditions commensurate
with the injury assessment reference values.
The dynamic response index which is the injury criteria used with the Hybrid III assumes
unidirectional loading therefore it may not be valid for high rate loading of UBB with possible
combined flexion, compression and shear loading. Injury risk assessment criteria and thresholds
are required for these combined loading conditions. That being said, the sophistication of a new
dummy should be limited in terms of the available range of motion and degree of freedom to
improve repeatability, reproducibility and durability while reducing acquisition and operating
costs.
Most research reported in the literature considers ideal loading conditions which necessitate the
need for additional fundamental research to develop more appropriate and specific lumbar
tolerances criteria for out-of-position occupants during UBB. Regardless, the data that is
available can potentially be used in developing or guiding the specification of a preliminary
definition for a surrogate spine’s response to UBB loading. The lumbar spine’s response to
loading reported in the literature is summarized in the Table 12 to Table 15.
Table 12: Lumbar spine response to compressive loading.
Test Description Specimen Peak Force (N) Force at Failure (N)
Peak Moment (Nm)
Stiffness (N/mm)
Stemper [12][13] Full lumbar section
5598 – 5827 na 98 – 166 na
Stemper [12][13] Full lumbar section
5236 – 7821 na 179 – 293 na
Yogonandan [14] Motion segment 11030 ± 1420 9020 ± 1080 na 2850 ± 293
Yogonandan [15] (50% probability of injury)
Full lumbar section
3700 na na
Compression 0.1 m/s loading Kemper [16] 0.2 m/s loading 1.0 m/s loading
FSU na na na 1835 ± 645.6 2489.5 ± 474.1 6551.1 ± 2017.0
37
Table 13: Lumbar spine response to shear loading.
Test Description Specimen Peak Force (N)
Force at Failure (N)
Stiffness (N/mm) (Anterior)
Stiffness (N/mm) (Posterior)
Skrzypiec [17] Young-No-Creep Young-Creep Old-No-Creep
Motion segment
3290 3570 2900
1570 2010 1790
565 566 480
366 254 342
Table 14: Lumbar spine response to flexion.
Test Description Specimen Moment at Failure (Nm)
Shear Force at Failure (N)
Tension at failure (kN)
Flex at Yield (deg)
Max Flex (deg)
Max Displ. (mm)
Osvalder [20] L1-L2 L2-L3 L3-L4
154 ± 6 153 ± 5 161 ± 16
600 ± 28 616 ± 22 640 ± 80
2.8 ± 0.2 2.7 ± 0.1 2.9 ± 0.2
na na na
17.3 ± 1.0 21.5 ± 0.8 19.8 ± 0.9
8.5 ± 1.4 9.4 ± 1.5 10.4 ± 2.4
Adams [25] Motion segment
72.8 ± 18.1 na 1129 ± 255 (comp)
14.8 ± 3.3 na na
Table 15: Lumbar spine response combined flexion and shear loading.
Test Description Specimen Moment at Failure (Nm)
Shear Force at Failure (N)
Flex at Yield (deg)
Hor. Displ. (mm)
Vert. Displ. (mm)
Bending Stiff (Nm/deg)
Shear Stiff (N/mm)
Belwadi [26] 2 disk motion segment
186.1 ± 97.7 216.6 ± 20.8
1962.2 ± 687.4 1936.7 ± 554.1
15.1 ± 2.3 13.1 ± 1.4
10.5 ± 4.3 10.7 ± 0.6
na na
12.3 16.5
186 180.9
Osvalder Moderate 1 [22][23] Moderate 2 Medium 1 Medium 2 Severe 1 Severe 2
Motion segment
140 ± 20 149 ± 27 160 ± 15 170 ± 15 183 ± 33 200 ± 25
458 ± 73 466 ± 73 480 ± 65 503 ± 72.5 620 ± 94 663 ± 58
13.7 ± 2.4 Na 15.4 ± 2.9 14.8 ± 1.5 18.8 ± 2.5 18.1 ± 3
6.6 ± 1.7 na 7.3 ± 1.2 7.0 ± 1.5 8.5 ± 3.2 7.9 ± 1.7
14.1 ± 1.4 Na 15.1 ± 1.1 14.9 ± 1.8 18.2 ± 2.4 17.6 ± 2.5
10.2 10.4 11.5 9.7 11.0
69.4 65.6 71.8 72.9 83.9
Newman [24] Motion segment
121 486 15.8 7.5 16.9 7.5 71
38
References/Bibliography....
References
[1] Possley DR, Blair JA, Freedman BA, Schoenfeld AJ, Lehman RA, “ The effect of vehicle protection on spine injuries in military conflict”, The Spine Journal 12 (2012): 843-848.
[2] Bernstock JD, Caples 2LT CM, Wagner LT SC, Kang CPT D G, Lehman LTC RA, “Characteristics of combat-related spine injuries: A review of recent literature”, Military
Medicine, Vol. 180 (May 2015): 503-512.
[3] Ragel BT, Allred D, Brevard S, Davis RT, Frank EH, “Fracture of the thoracolumbar spine sustained by soldiers in vehicles attacked by improvised explosive devices”, SPINE 34(22)
(2009): 2400-2405.
[4] Liu KY, Pontius UR, “The effects of initial spinal configuration on pilot ejection”, U.S. Army Aeromedical Research Laboratory, Report No. 74-6, (October 1973).
[5] Latham F, “A study in body ballistics: Seat ejection”, Proceedings of the Royal Society of London B: Biological Sciences, 147(926) (1957): 121-139.
[6] Adams MA, McNally DS, Chinn H, Dolan P, “The clinical biomechanics award paper 1993 Posture and the compressive strength of the lumbar spine”, Clinical Biomechanics, 9(1)
(1994): 5-14.
[7] Janevic J, Ashton‐Miller JA, Schultz AB, “Large compressive preloads decrease lumbar motion segment flexibility”, Journal of Orthopaedic Research, 1; 9(2), (1991): 228-36.
[8] Iluk A, “Influence of the additional inertial load of the torso on the mine blast injury”, In Proceedings of the International Research Council on the Biomechanics of Injury Conference
(2013), IRC-13-35: 281
[9] Iluk A, “ Estimation of spine injury risk as a function of bulletproof vest mass in case of under body blast load”, In Proceedings of the International Research Council on the
Biomechanics of Injury Conference (2014), IRC-14-88: 809-820.
[10] Aggromito D, Thomson R, Wang J, Chhor A, Chen B, Yan W, “Effect of body-borne equipment on injury of military pilots and aircrew during a simulated helicopter crash”,
International Journal of Industrial Ergonomics (2015).
[11] Zhang J, Merkle AC, Carneal CM, Armiger RS, Kraft RH, Ward EE, Roberts JC, “ Effects of torso-borne mass and loading severity on early response of the lumbar spine under hi