The Spinal Cord and Spinal Nerves Chapter 12. THE SPINAL CORD.

BRAINA JOURNAL OF NEUROLOGY
Functional neurological recovery after spinal cordinjury is impaired in patients with infectionsVieri Failli,1,* Marcel A. Kopp,1,* Christine Gericke,2,* Peter Martus,2,3 Susann Klingbeil,1,4
Benedikt Brommer,1 Ines Laginha,1 Yuying Chen,5 Michael J. DeVivo,5 Ulrich Dirnagl6 andJan M. Schwab1
1 Department of Neurology and Experimental Neurology, Clinical and Experimental Spinal Cord Injury Research (Neuroparaplegiology), Charite—
Universitatsmedizin Berlin, D-10117 Berlin, Germany
2 Institute of Biostatistics and Clinical Epidemiology, Charite—Universitatsmedizin Berlin, D-12203 Berlin, Germany
3 Department of Clinical Epidemiology and Applied Biostatistics, Eberhard Karls Universitat Tubingen, D-72070 Tubingen, Germany
4 Department of Neurology, University Hospital of Cologne, D-50937 Cologne, Germany
5 National Spinal Cord Injury Statistical Center, Department of Physical Medicine and Rehabilitation, University of Alabama at Birmingham,
Birmingham, AL 35233, USA
6 Department of Neurology and Experimental Neurology, Centre for Stroke Research Berlin, Charite—Universitatsmedizin Berlin, D-10117 Berlin,
Germany
*These authors contributed equally to this work.
Correspondence to: Prof. Jan M. Schwab, MD, PhD,
Department of Neurology and Experimental Neurology,
Clinical and Experimental Spinal Cord Injury Research (Neuroparaplegiology),
Charite—Universitatsmedizin Berlin,
Chariteplatz 1,
D-10117 Berlin, Germany
E-mail: [email protected]
Infections are a common threat to patients after spinal cord injury. Furthermore, infections might propagate neuronal death, and
consequently contribute to the restriction of neurological recovery. We investigated the association of infections (i.e. pneumonia
and/or postoperative wound infections) with functional neurological outcome after acute severe traumatic spinal cord injury. We
screened data sets of 24 762 patients enrolled in a prospective cohort study (National Spinal Cord Injury Database, Birmingham,
AL, USA). Patients were assessed according to the ASIA classification. ASIA impairment scale–classified A and B patients
recruited within 24 h post-trauma (n = 1436) were selected as being a major recruitment population for interventional trials.
Patients with documented pneumonia and/or postoperative wound infections (n = 581) were compared with control subjects
(non-documented infections, n = 855). The functional neurological outcome parameters (i) upward ASIA impairment scale con-
versions; (ii) gain of ASIA motor scores; and (iii) gain of motor and sensory levels were consecutively analysed over time up to 1
year after spinal cord injury. The group with pneumonia and/or postoperative wound infections revealed less ASIA impairment
scale upward conversions after 1 year than the control group (ASIA impairment scale A: 17.2 versus 23.9%, P = 0.03; ASIA
impairment scale B: 57.1 versus 74.7%, P = 0.009). ASIA motor score gain [median (interquartile range)] was lower in patients
with infections [ASIA impairment scale A: 8 (4–12) versus 10 (5–17), P = 0.01; ASIA impairment scale B: 19.5 (8–53.5) versus 42
(20.5–64), P = 0.03)]. Analysis of acquired motor/sensory levels supported these findings. In ASIA impairment scale A patients,
doi:10.1093/brain/aws267 Brain 2012: 135; 3238–3250 | 3238
Received February 27, 2012. Revised July 23, 2012. Accepted August 10, 2012
� The Author (2012). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved.
For Permissions, please email: [email protected]
Dow
nloaded from https://academ
ic.oup.com/brain/article/135/11/3238/272916 by guest on 31 D
ecember 2021

the gain in motor levels (21.7 versus 33.3%, P = 0.04) and sensory levels (24.4 versus 38 of 102, 37.3%, P = 0.03) was
significantly lower in the group with pneumonia and/or postoperative wound infections than in the control group. Multiple
regression analysis identified pneumonia and/or postoperative wound infections as independent risk factors for impaired ASIA
impairment scale upward conversion (odds ratio: 1.89, 95% confidence interval: 1.36–2.63, P50.0005) or lower gain in ASIA
motor score (regression coefficient: �8.21, 95% confidence interval: �12.29 to �4.14, P50.0005). Infections associated with
spinal cord injury, such as pneumonia and/or postoperative wound infections, qualify as independent risk factors for poor
neurological outcome after motor complete spinal cord injury. Infections constitute a clinically relevant target for protecting
the limited endogenous functional regeneration capacity. Upcoming interventional trials might gain in efficacy with improved
patient stratification and might benefit from complementary protection of the intrinsic recovery potential after spinal cord injury.
Keywords: intrinsic/endogenous recovery potential; poor outcome; neurological recovery
Abbreviations: ASIA = American Spinal Injury Association; AIS = ASIA impairment scale; NSCID = National Spinal Cord InjuryDatabase; SCI = spinal cord injury
IntroductionThis study investigates the hypothesis that infections restrict re-
covery of neurological function after spinal cord injury (SCI).
Infections are the leading cause of morbidity and mortality in pa-
tients after SCI. Infection rates range from 28 to 38%, leading to
a mortality rate between 4.4 and 16.7% (DeVivo et al., 1999;
Sekhon and Fehlings, 2001; Meisel et al., 2005). Several risk fac-
tors contribute to increased susceptibility of these patients to in-
fections (e.g. for pneumonia: aspiration due to drowsiness,
impaired bulbar reflexes, dysphagia and hypostasis in bedridden
patients and invasive procedures). Immobility and reduced reflex
status increase the risk of aspiration itself, but do not sufficiently
explain the increased risk of developing infections. The search for
additional underlying reasons led to the discovery of the SCI-
induced immune depression syndrome, which may pave the way
for infections. SCI-induced immune depression syndrome is a neu-
rogenically triggered secondary immune deficiency syndrome
(immune paralysis) (Riegger et al., 2003, 2007, 2009; Vega
et al., 2003; Furlan et al., 2006; Lucin et al., 2007; Held et al.,
2010; Oropallo et al., 2012). It occurs within 24 h after SCI, af-
fects the innate and adaptive immune systems irrespective of the
administration of iatrogenic methylprednisolone and shares similar
characteristics in experimental models and post-SCI patients
(monocytopenia, lymphopenia) (Riegger et al., 2003, 2009;
Vega et al., 2004; Furlan et al., 2006; Lucin et al., 2007).
Infections may pose an independent risk factor for poor out-
come, impeding an intrinsic functional neurological recovery after
ischaemic injury to the CNS (Meisel et al., 2005; Vermeij et al.,
2009). Specifically, the induction of pneumonia, a frequent infec-
tion after both stroke and SCI, has been shown to promote sec-
ondary damage in experimental ischaemic CNS injury (Meisel
et al., 2004). To date, there are no systematic data available
that evaluate the effect of infections on the clinical neurological
outcome after SCI. We analysed data from a large prospective
multicentre cohort study (Marino et al., 1999; Fawcett et al.,
2007) to learn more about the impact of paradigmatic infections
such as pneumonia and postoperative wound infections and report
the first systematic investigation of their effects on the neuro-
logical recovery of post-SCI patients.
Patients and methods
Database informationThe data sets were obtained from the National Spinal Cord Injury
Database (NSCID) at the National Spinal Cord Injury Statistical
Center, Birmingham, AL, USA. Data were collected prospectively in
25 specialized SCI care centres (Model Spinal Cord Injury Systems)
from patients whose injuries were of acute traumatic aetiology
(Richards et al., 1995; Stover et al., 1999). The procedures taken to
ensure the quality of data have been previously described (Richards
et al., 1995; Stover et al., 1999; DeVivo et al., 2002). At the SCI
centre level, a defined set of procedures and responsibilities are estab-
lished to ensure that the required data are collected prospectively by
qualified staff familiar with the definitions and guidelines as stipulated
in the NSCID data collection syllabus. The National Spinal Cord Injury
Statistical Center performs two types of periodic analysis on all data-
base variables to identify data collection problems. The first analysis
determines the number and percentage of unknown responses for
each variable from each SCI centre. The second analysis reveals the
variability in responses across the SCI centres. Extensive quality control
checks are built into the National Spinal Cord Injury Statistical Center’s
data management software (checking routines) used at each SCI
centre. Checks are performed on each record entered by an SCI
centre, and each record must pass all quality control checks before it
is merged into the NSCID. Finally, twice during a 5-year period, all SCI
centre data collectors received refresher training to ensure standar-
dized data procurement.
Data qualifying the longitudinal course of neurological recovery after
traumatic SCI have been previously reported (Marino et al., 1999) and
have been consistent with data from other databases such as the
European Multicentre Study on Spinal Cord Injury with regards to
the main end-points used for this study (Fawcett et al., 2007; Furlan
et al., 2008). The institutional review board of each model system
approved the database, and enrolment was in accordance with the
Declaration of Helsinki. All subjects were informed about the database
and its aim and gave their written informed consent.
Neurological assessmentThe neurological assessments were performed in compliance with the
International Standards for Neurological Classification of Spinal Cord
Injury/American Spinal Injury Association (ASIA) classification of SCI
Infections and recovery after SCI Brain 2012: 135; 3238–3250 | 3239
Dow
nloaded from https://academ
ic.oup.com/brain/article/135/11/3238/272916 by guest on 31 D
ecember 2021

(Marino, 2003), the validated instrument for the identification and lon-
gitudinal evaluation of SCI patients (Furlan et al., 2008). The (i) ASIA
impairment scale (AIS); (ii) ASIA motor score; and (iii) neurological
motor and sensory levels were assessed (Supplementary material).
Baseline data were obtained at admission to a model system for
acute care. The assessment points for follow-up were admission to
in-patient rehabilitation (start of rehabilitation), discharge from in-pa-
tient rehabilitation (end of rehabilitation) and first annual examination
(1 year) after SCI.
Study populationThe NSCID was screened according to the data collection syllabus
terms. The data sets of patients suffering from SCI of acute traumatic
aetiology and recruited within 24 h after injury were selected at the
database level for detailed follow-up data collection (Fig. 1). Patients
admitted later than 24 h were not assigned to follow-up documenta-
tion, and for this reason, not accessible for longitudinal outcome
evaluation. Patients were not analysed in this study if they had been
assessed with the outdated Frankel scale, which was replaced by the
AIS in 1992. Predefined eligibility criteria were applied (Fig. 1).
Exclusion criteria were as follows: (i) age 515 and 470 years;
(ii) non-infectious pulmonary complications such as pulmonary embol-
ism; (iii) complications that might be related to pulmonary embolism,
such as deep vein thrombosis; (iv) rehospitalization for unspecified
infectious and parasitic diseases during trial course; (v) missing a
neurological level for each side of the body; and (vi) missing AIS at
baseline. The AIS was also encoded as ‘missing’ if an associated injury
or cognitive impairment interfered with the performance of a complete
neurological examination. For example, patients with severe concomi-
tant traumatic brain injury or psychological disorders were excluded.
Consequently, the reliability of the early baseline assessment was
improved (Burns et al., 2003). The exclusion criteria also included
patients unavailable at the NSCID at 1 year because of death or loss
to follow-up (Fig. 1). To describe potential sources of selection bias,
differences between the selected patient population and excluded
patients were assessed (Supplementary Table 1).
For the selected patient population (AIS A–D), the rate of pneumo-
nia/postoperative wound infections during the first year after SCI was
calculated stratified for AIS. Pneumonia was defined as a state of lung
tissue inflammation of infectious aetiology with radiographic demon-
stration of parenchymal disease. Postoperative wound infections were
defined as postoperative wound infection at the site of spinal surgery
that was performed during the reporting period. Patients with AIS C
and D were excluded from outcome analysis (i) owing to the low
overall incidence of pneumonia/postoperative wound infections
(Table 1); and (ii) because potential ceiling effects on AIS conversion
and ASIA motor score apply for motor-incomplete SCI (Fawcett et al.
2007; Steeves et al. 2007). For the final ‘analysis-in population’ (AIS A
and B), the timing of the neurological assessments, as well as the
frequency and timing of pneumonia/postoperative wound infections
episode occurrence during acute care, during in-patient rehabilitation
and after discharge, was calculated. Furthermore, baseline character-
istics and clinical characteristics during follow-up were assessed.
Analysis strategyAs reported previously, it is acceptable to pool examination data when
evaluating recovery at the group level (Marino et al., 1999; Curt et al.,
2007; Fawcett et al., 2007). We compared patients with pneumonia/
postoperative wound infections and patients without documented
pneumonia/postoperative wound infections (control patients) stratified
for AIS at baseline (Fawcett et al., 2007). We grouped pneumonia and
postoperative wound infection data together because the number of
patients with postoperative wound infections was too low for statistical
evaluation as a separate group. AIS conversions were evaluated in
patients with neurological levels from C1 to S1. Conversion rates
from AIS at baseline into the different AIS grades at 1 year were
calculated and subsequently categorized into patients gaining or plat-
eauing/worsening over the first year after SCI.
In analysing ASIA motor score gain, we selected patients with motor
levels C1–C8 documented on both body sides at baseline. Patients
with cervical injury are of particular interest because most thoracic
and sacral segments are not represented in ASIA motor scoring
(Supplementary material), and thereby cannot be monitored. In add-
ition, cervical patients comprise the relevant patient population for
upcoming interventional trials focusing on the primary end-point ‘im-
proved motor recovery’ (Fawcett et al., 2007; Steeves et al., 2007).
The ASIA motor score was analysed over time at each assessment
point up to 1 year. Patients with at least one available follow-up as-
sessment were included. The differences in the total motor score from
baseline were calculated for each group at each assessment point. The
patients were differentially assigned to the groups (with or without
pneumonia/postoperative wound infections) with regards to the oc-
currence of pneumonia/postoperative wound infections before the re-
spective assessment point.
For the analysis of acquired motor or sensory levels, we selected
patients with motor or sensory levels C1–C8 at baseline. Only patients
with documented levels on both body sides were included. Motor and
sensory levels were evaluated individually. The difference between
levels at baseline and levels at 1 year was calculated for each side
of the body. Then, the mean of the side-specific level differences
was calculated for each patient. The proportion of patients gaining
more than one level at 1 year was calculated for each group and
defined as relevant improvement.
Multiple logistic or linear regression analyses were performed to
determine factors independently associated with impaired AIS conver-
sion or ASIA motor score recovery, respectively. To address the prob-
lem of missing data in the ‘analysis-in population’, ‘missing value’
analysis of baseline parameters and multiple imputation was
performed.
Finally, to evaluate an influence of the frequency, the timing and
the type of infection episodes on changes in the AIS and the ASIA
motor score, we performed subgroup analyses. To achieve sufficient
group sizes for subgroup analyses, AIS A and B patients were taken
together. Control patients were compared with patients with one epi-
sode and patients with two or more episodes of pneumonia/post-
operative wound infections. In addition, control patients were
compared with patients who first presented with a pneumonia/post-
operative wound infection episode during acute care and with patients
who first presented with pneumonia/postoperative wound infections
during rehabilitation or after discharge up to 1 year after SCI.
Furthermore, control patients were compared with patients presenting
with pneumonia, patients presenting with postoperative wound infec-
tions and patients with both types of infection (pneumonia and post-
operative wound infections).
Statistical analysisThe distribution of continuous variables was described as median and
quartiles or means and 95% limits of confidence (CI). The Mann–
Whitney test was used to compare between the groups. The
Kruskal–Wallis test was applied for multiple comparison, followed by
post tests. The �2 test was used for categorical variables. Missing value
3240 | Brain 2012: 135; 3238–3250 V. Failli et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article/135/11/3238/272916 by guest on 31 D
ecember 2021

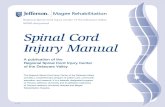
Figure 1 Patient enrolment chart. A stepwise data set selection was performed from the NSCID. In the ‘analysis-in population’ (pool of
patients for outcome analysis), groups for statistical analysis were determined with respect to characteristics of the particular outcome
parameter and the availability of data at each follow-up assessment point. We controlled for missing data–related attrition bias, applying
multiple regression models after multiple imputation. Besides applying linear and logistic regression models, we tested for interactions.
Note that total numbers differ from subgroup numbers because, for some patients, items apply several times. Pn/Wi = pneumonia and/or
postoperative wound infection.
Infections and recovery after SCI Brain 2012: 135; 3238–3250 | 3241
Dow
nloaded from https://academ
ic.oup.com/brain/article/135/11/3238/272916 by guest on 31 D
ecember 2021

analysis was performed for AIS and ASIA motor score in the
‘analysis-in population’. Logistic regression analysis was performed
using impaired AIS conversion at 1 year as a dependent variable.
Linear regression analysis was performed using ASIA motor score re-
covery at 1 year as a dependent variable. In both multiple regression
analyses, forward variable selection was applied (inclusion criterion:
P = 0.05, exclusion criterion: P = 0.10). Furthermore, interactions be-
tween AIS and pneumonia/postoperative wound infections were ana-
lysed. Goodness of fit was assessed using the Hosmer–Lemeshow test.
Multiple imputation was performed as follows: the first imputation
used the conversion or motor score differences on the first two time
points and motor score differences or conversion on the three time
points as independent variables without imputation of themselves.
Only one variable (conversion or motor score difference on third
time point) was imputed at this stage. In the second imputation, all
independent variables from the analysis were used as independent
variable and were imputed. Then the merged data set was used for
the imputation repeated five times. The final algorithm averaged the
five imputations.
With 396 versus 540 patients and an overall rate of AIS conversion
of 32% 1 year after SCI, differences of 9% could be detected with
80% power in this study. With 163 versus 173 patients and standard
deviations of 24.7 and 17.6, respectively, differences in overall motor
score recovery of 6.7 points (mean) 1 year after SCI could be detected
with 80% power.
All tests were two sided, and the level of significance was 0.05. The
power analysis was calculated with nQueryAdvisor version 6.0. All
other statistical analyses were performed with SPSS for Windows ver-
sion 19.0.
Results
Baseline characteristics and clinical dataSCI patients (n = 24 762) were incorporated in the NSCID at the
time point of the analysis (Fig. 1). Within 24 h, 10 859 patients
were admitted and assigned to complete the longitudinal
follow-up documentation. The 6339 patient data sets assessed
with the outdated Frankel scale were not considered for the
study. The study monitored for attrition bias (‘missing data’,
‘loss to follow-up’) and selection bias due to ‘exclusion criteria’.
After application of the exclusion criteria, 2089 data sets from
AIS A–D patients were selected. These patients were recruited
between 1992 and 2005 and followed up to 1 year after injury,
until 2006. The 2089 individuals included (AIS A–D) were evalu-
ated for baseline differences compared with the 2431 individuals
who were excluded (Supplementary Table 1). Descriptive data
from the selected patients were comparable with the excluded
patients in terms of gender, ethnic group and ASIA motor score
at baseline, but revealed differences in age, AIS and neurological
level. The group of excluded patients showed a higher mean age,
and rates of AIS A and cervical neurological level were slightly
higher than those in the selected patients. These differences
might be attributable to the exclusion of patients older than 70
years and to the number of patients lost from the NSCID because
of death, as severely injured patients are more likely to develop
fatal complications.
The AIS grades of included data sets were compared to assess
whether the occurrence of a documented pneumonia/postopera-
tive wound infection was dependent on the completeness of injury
(Table 1). High rates of pneumonia/postoperative wound infection
were observed in severely impaired, complete AIS A and motor
complete AIS B patients. The rate of pneumonia/postoperative
wound infections was low in the motor incomplete AIS C and D
patients.
The neurological function was evaluated in the final ‘analysis-in
population’ of 1436 AIS A and B patients (pool of patients with or
without pneumonia/postoperative wound infections, Fig. 1). From
the ‘analysis-in population’, 581 (40.5%) patients had a total of
687 documented episodes of pneumonia/postoperative wound in-
fection. Some patients developed more than one episode or type
of infection. Of those patients, 550 (94.7%) had at least one
episode of pneumonia and 45 (7.7%) had at least one episode
of postoperative wound infection. Pneumonia/postoperative
wound infection episodes were documented in 407 cases
(70.1%) during stay in acute care, in 211 cases (36.3%) during
in-patient rehabilitation and in 69 cases (11.9%) after discharge
up to 1 year post-trauma. The first presentation of infection during
in-patient rehabilitation occurred in 148 cases (25.5%), whereas
the first presentation of pneumonia/postoperative wound infection
after discharge up to 1 year occurred only in 26 cases (4.5%).
Thus, 495% of pneumonia/postoperative wound infections
occurred first during acute care and in-patient rehabilitation. The
neurological baseline assessment at admission to an SCI centre
was performed during acute care at Day 1 (0–2) after SCI
[median (interquartile range)]; the first follow-up assessment was
performed at admission to in-patient rehabilitation at Day 15
(8–25), and the second follow-up assessment was performed at
discharge from in-patient rehabilitation at Day 62 (42–98). The
final 1-year outcome was obtained at the first annual examination
365 (304–408) days after SCI (Table 2).
Next, we investigated the groups (with or without pneumonia/
postoperative wound infection) for their congruency with regards
to outcome-relevant factors (Table 3). The groups revealed similar
baseline characteristics such as age, gender and race. The rate of
penetrating injury also revealed no statistical difference between
the groups. The groups were distinct in AIS and neurological level,
or in mechanical ventilation and rehospitalization during follow-up.
In addition, there was a significant difference in enrolment period
between the groups with regards to the likelihood of developing
pneumonia/postoperative wound infection. To provide an estima-
tion of access to rehabilitation, we compared the length of stay in
in-patient rehabilitation between the groups. Patients with pneu-
monia/postoperative wound infection had a longer access to in-
Table 1 Rates of pneumonia/postoperative wound infec-tions stratified for AIS at baseline
AIS at baseline Total n Pn/Win (%)
AIS A 1098 470 (42.8)
AIS B 338 111 (32.8)
AIS C 378 83 (22.0)
AIS D 275 36 (13.1)
Pn/Wi = pneumonia and/or postoperative wound infection (up to 1 year after SCI).
3242 | Brain 2012: 135; 3238–3250 V. Failli et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article/135/11/3238/272916 by guest on 31 D
ecember 2021

patient rehabilitation of 57 (35–88) days compared with control
patients with an access time of 47 (30–78) days (P5 0.0005).
The ‘missing value’ analysis revealed no significant baseline dif-
ferences between the groups with regards to the primary outcome
parameter ‘neurological outcome’, which encompasses (i) AIS
(P = 0.51) and (ii) ASIA motor score (P = 0.21) within the
‘analysis-in population’.
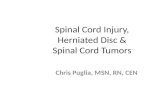
Association of pneumonia/postopera-tive wound infections with impairedneurological recoveryWe first investigated AIS conversion rates at 1 year (n = 936,
Fig. 2). Significantly lower AIS upward conversions were observed
for patients with documented pneumonia/postoperative wound
infections compared with the control group. Among AIS A pa-
tients, 56 of 326 patients (17.2%) from the pneumonia/post-
operative wound infections group converted upwards compared
with 94 of 394 (23.9%) in the control group (P = 0.03). The AIS B
pneumonia/postoperative wound infections group demonstrated
lower upward conversion rates in 40 of 70 patients (57.1%),
versus 109 of 146 (74.7%) in the control group (P = 0.009).
Consequently, AIS A and B patients in the pneumonia/postopera-
tive wound infections group are significantly more likely to plateau
as non-converters.
To determine whether pneumonia/postoperative wound infec-
tions is an independent risk factor that affects AIS conversion
(dependent variable) during 1-year follow-up, we controlled for
baseline and clinical differences between the groups using multiple
regression models. The results of the multiple logistic regression
analysis identified pneumonia/postoperative wound infections as
an independent risk factor associated with lower AIS upward con-
version, as represented by an odds ratio (OR) of 1.89 (95% CI:
1.36–2.63, P5 0.0005) in the multiple analysis (n = 931, Table 4).
Subsequently, we performed multiple imputations to calculate for
missing data. Calculation of the logistic regression analysis after
multiple imputation (n = 1428) revealed an OR of 1.47 (95% CI:
1.06–2.04, P = 0.02, Supplementary Table 2). Subgroup analysis
of the frequency of pneumonia/postoperative wound infections
revealed no statistically significant differences in the AIS conver-
sion rates between patients with a single episode and patients with
several episodes of pneumonia/postoperative wound infection
(Supplementary Fig. 1A). Evaluation of the timing of pneumo-
nia/postoperative wound infections, in particular, early occurrence
during acute care versus later onset during rehabilitation or after
discharge (Supplementary Fig. 1B), did not demonstrate a differ-
ential impact for the timing of infections on AIS conversion within
the group of patients with pneumonia/postoperative wound infec-
tions. Differential evaluation of pneumonia and postoperative
wound infections was limited to a descriptive analysis in patients
Table 3 Baseline characteristics and clinical data in the ‘analysis-in population’
Baseline characteristics Control Pn/Wi P-value
Age [median (IQR)] n = 855 [28 (21–39)] n = 581 [29 (21–40)] 0.39
Gender: [male (%)] n = 855 [688 (80.5)] n = 581 [475 (81.8)] 0.54
Ethnic group: [Caucasian (%)] n = 791 [508 (64.2)] n = 555 [370 (66.7)] 0.35
AIS A (%) 628 (73.5) 470 (80.9) 0.001
AIS B (%) 227 (26.5) 111 (19.1)
Neurological level: C1–C4 (%) 107 (12.6) 171 (29.7)
Neurological level: C5–C8 (%) 220 (25.8) 146 (25.3)
Neurological level: T1–T6 (%) 163 (19.1) 127 (22.0) 50.0005
Neurological level: T7–T12 (%) 275 (32.3) 110 (19.1)
Neurological level: L1–S1 (%) 87 (10.2) 22 (3.8)
Enrolment period: 1992–98 (%) 430 (50.3) 395 (68.0) 50.0005
Enrolment period: 1999–2005 (%) 425 (49.7) 186 (32.0)
Penetrating injury (%) n = 854 [206 (24.1)] n = 581 [128 (22.0)] 0.36
Clinical data
Spinal surgery (%) n = 855 [581 (68.0)] n = 580 [407 (70.2)] 0.37
Mechanical ventilation (%) n = 853 [123 (14.4)] n = 581 [292 (50.3)] 50.0005
Rehospitalization (%) n = 834 [216 (25.9)] n = 563 [240 (42.6)] 50.0005
Distribution of baseline characteristics and clinical characteristics as occurring during the trial course up to 1 year in the ‘analysis-in population’ is shown. For statistical
comparison between the groups (�pneumonia/postoperative wound infections), the Mann–Whitney test was used for age, and the �2 test was applied for all othervariables. Differences in patient numbers within the groups result from missing data for the respective variables. Correction of ‘baseline differences’ and ‘missing data’ wasconducted by plugging into multiple regression models and missing value analysis (Tables 4 and 5).
Table 2 Assessment points after SCI
Assessment point Days, median(IQR)
Acute care within 24 h—‘baseline’ 1 (0–2)
Admission to rehabilitation 15 (8–25)
Discharge from in-patient rehabilitation 62 (42–98)
Annual examination after SCI—‘1 year’ 365 (304–408)
Assessment points are calculated for the ‘analysis-in population’ AIS A and B(n = 1436). IQR = interquartile range.
Infections and recovery after SCI Brain 2012: 135; 3238–3250 | 3243
Dow
nloaded from https://academ
ic.oup.com/brain/article/135/11/3238/272916 by guest on 31 D
ecember 2021

with postoperative wound infection because the number of pa-
tients with postoperative wound infection was low. However, the
group of patients with pneumonia was significantly different from
control patients in terms of an impaired AIS conversion rate
(Supplementary Fig. 1C).
Next, we investigated the effect of pneumonia/postoperative
wound infections on motor recovery over time (Fig. 3). This was
done in patients with cervical lesions through a longitudinal com-
parison of differences in the total motor score from baseline at
each assessment point. A longitudinal set-up was chosen to moni-
tor (i) ‘when’ a putative alteration appeared over time; and
(ii) whether it became possible to distinguish early from late effects
on neurological outcome to track different underlying patho-
physiological mechanisms. The group with pneumonia/postopera-
tive wound infections and the control group were comparable
with regards to early outcome at the start of rehabilitation. At
the end of rehabilitation, a lower gain in motor score in the
group with pneumonia/postoperative wound infections did not
yield a statistical significance in the AIS A group. The motor re-
covery in AIS B was more compromised in the group with pneu-
monia/postoperative wound infections already at the end of
rehabilitation and resulted in a significantly lower gain in motor
score points [median (interquartile range), 8 (1.5–27.5) versus 22
(9.5–45), P = 0.001] constituting a 64% difference at that time
point. One year after SCI served as our final assessment point
for determining whether the observations were persistent and
not restricted to episodes of rehabilitation. Here, the gain in
ASIA motor score in AIS A patients with pneumonia/postoperative
wound infections was significantly lower [AIS A: 8 (4–12) versus
10 (5–17), P = 0.01], demonstrating a 20% difference. In AIS B,
the group with pneumonia/postoperative wound infections
showed a persisting impairment of motor recovery [19.5 (8–
53.5) versus 42 (20.5–64), P = 0.03], constituting a 55%
Table 4 Logistic regression analysis using AIS conversion at 1 year as dependent variable
Variable Univariate analysis Multiple analysis
OR (95% CI) P-value OR (95% CI) P-value
Age (per 10 years increase) 0.88 (0.79–0.98) 0.02
Gender (male = 1; female = 2) 0.87 (0.61–1.23) 0.43
Ethnic group (Caucasian = 0; others = 1) 1.16 (0.86–1.56) 0.33
AIS (AIS B = 0; AIS A = 1) 8.45 (6.02–11.87) 50.0005 7.72 (5.41–11.00) 50.0005
Neurological level (L1–S1 = 0; C1–C4 = 1; C5–C8 = 2;T1–T6 = 3; T7–T12 = 4)
1.53 (1.37–1.72) 50.0005 1.53 (1.35–1.74) 50.0005
Penetrating injury (no = 0; yes = 1) 2.02 (1.44–2.85) 50.0005
Pn/Wi (no = 0; yes = 1) 1.88 (1.41–2.51) 50.0005 1.89 (1.36–2.63) 50.0005
Mechanical ventilation (no = 0; yes = 1) 1.18 (0.87–1.60) 0.30
Spinal surgery (no = 0; yes = 1) 0.76 (0.56–1.02) 0.07
Rehospitalization (no = 0; yes = 1) 1.74 (1.27–2.38) 0.001
Enrolment period (1999–2005 = 0; 1992–1998 = 1) 1.25 (0.95–1.66) 0.12
Univariate and multiple logistic regression analysis in patients AIS A and B score (n = 931). The coding of the variable categories is indicated in the table. The neurologicallevel L1–S1 was encoded as 0 because patients with L1–S1 demonstrated the highest rate of AIS upward conversion, followed by high cervical (C1–C4), low cervical (C5–C8) and thoracic levels (T1–T6 and T7–T12). The analysis of interactions between the AIS and pneumonia/postoperative wound infections revealed no significance withregards to AIS conversion (P = 0.29). The multiple analysis was performed after forward variable selection (Nagelkerke’s R2 = 0.30; Hosmer–Lemeshow test, P = 0.34).Correction of confounders and baseline differences was conducted by plugging in univariate followed by multiple regression models. After univariate analysis, the cohort
was controlled for ‘neurological level’, ‘lesion severity’ (AIS), ‘age’, ‘penetrating injury’ and ‘rehospitalization’. Only AIS, neurological level and pneumonia/postoperativewound infections were approved as being independently associated with impaired AIS conversion rates, yielding statistical significance in the multiple model. Pn/Wi =pneumonia and/or postoperative wound infection.
Pn/W
i
Pn/W
i
Contro
l
Contro
l
n = 724
n = 216
AIS A
AIS BA
IS g
rade
impr
ovin
gA
IS g
rade
sta
ble
or w
orse
ning
50%
0%
50%
10%
20%
30%
40%
40%
30%
20%
10%
60%
70%
80%
80%
70%
60%
Figure 2 Pneumonia/postoperative wound infections are
associated with rates of impaired upward conversion. Motor
complete injury AIS A and AIS B patients with documented
pneumonia/postoperative wound infections had a significantly
reduced rate of upward conversions in the AIS compared with
control patients. �2 test, *P = 0.03, **P = 0.009.
3244 | Brain 2012: 135; 3238–3250 V. Failli et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article/135/11/3238/272916 by guest on 31 D
ecember 2021

reduction of the intrinsic recovery potential (Fig. 3). Thus, if
the reduced gain in motor function occurs during in-patient re-
habilitation, it persists up to 1 year and is not compensated for
later on. To determine whether pneumonia/postoperative wound
infections have an independent effect on ASIA motor-score
changes at 1 year (dependent variable), a linear regression
model was applied. The multiple linear regression analysis identi-
fied pneumonia/postoperative wound infections as an independ-
ent prognostic factor associated with a lower gain of motor score
points 1 year after SCI [regression coefficient: �8.21 (95% CI:
�12.29 to �4.14), P50.0005, Table 5]. Again, the linear regres-
sion model after multiple imputation (n = 603) confirmed this
result [regression coefficient: �4.96 (95% CI: �8.85 to �1.07),
P = 0.01, Supplementary Table 3]. Of note, in contrast to pneu-
monia/postoperative wound infections, ‘mechanical ventilation’
did not reach significance levels as a risk factor for either AIS
conversion or ASIA motor score gain (Tables 4 and 5). The sub-
group analysis of frequency, type and timing of infections was
consistent with the results of the AIS conversion analysis
(Supplementary Fig. 2A–C).
Finally, we evaluated the gain in motor and sensory levels as
secondary outcome parameters, focusing on cervical injury pa-
tients. Groups were compared for improvement of more than
one motor or sensory level (Figs 4 and 5). The most pronounced
effect was observed in AIS A patients. In the group with pneu-
monia/postoperative wound infection, the gain in motor levels
was significantly lower compared with control group [31 of 143
(21.7%) versus 39 of 117 (33.3%)]. In AIS B patients, no statis-
tically significant difference was detected. AIS A patients in the
pneumonia/postoperative wound infection group were character-
ized by significantly lower sensory level gains [33 of 135 (24.4%)
versus 38 of 102 (37.3%), P = 0.03]. AIS B patients demonstrated
no statistically significant association. The clearly smaller group
sizes compared with the AIS A group may explain the observed
discrepancy between the results of the AIS conversion or motor
score analysis. Furthermore, reaching robust significance levels in
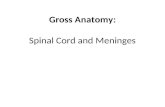
Figure 3 Pneumonia/postoperative wound infections are associated with lower gain in ASIA motor score points. Differences from
baseline (median 1 day post-SCI) in the ASIA motor score were analysed at each assessment point during 1-year follow-up in patients with
cervical lesions stratified for AIS at baseline. At start of rehabilitation (median 15 days post-SCI), no significant differences in motor
recovery were observed between patients with documented pneumonia/postoperative wound infections and control patients (AIS A and
B). AIS A patients with pneumonia/postoperative wound infections revealed a statistically significant lower recovery in the ASIA motor
score compared with control patients at 1 year. In AIS B patients, a significant impairment of motor recovery was detectable in the group
with pneumonia/postoperative wound infections at end of rehabilitation (median 62 days post-SCI) and was persistent up to 1 year.
Number of AIS A patients (control patients, pneumonia/postoperative wound infection): start of rehabilitation n = 240, n = 152; end of
rehabilitation n = 197, n = 203; and 1 year n = 113, n = 137. Number of AIS B patients (control patients, pneumonia/postoperative wound
infection): start of rehabilitation n = 101, n = 41; end of rehabilitation n = 90, n = 53; and 1 year n = 50, n = 36. Boxes are plotted as
median and interquartile range; whiskers are defined according to Tukey and outliers are indicated by dots. Mann–Whitney test,
*P = 0.03, **P = 0.01, ***P = 0.001.
Infections and recovery after SCI Brain 2012: 135; 3238–3250 | 3245
Dow
nloaded from https://academ
ic.oup.com/brain/article/135/11/3238/272916 by guest on 31 D
ecember 2021

the primary outcome parameter AIS conversions and gain of
ASIA motor scores and less pronounced in the secondary outcome
(gain of motor/sensory level) point to differences in sensitivity to
detect changes due to the immanent characteristics of the ASIA
assessments.
DiscussionTo address the impact of prevalent infections (pneumonia/post-
operative wound infection) on neurological recovery after SCI
(Marino et al., 1999), we investigated parameters of neurological
Table 5 Linear regression analysis using ASIA motor score difference from baseline at 1 year as dependent variable
Variable Univariate analysis Multiple analysis
b (95% CI) P-value b (95% CI) P-value
Age (per 10 years increase) 2.24 (0.48 to 4.00) 0.01 2.23 (0.70 to 3.75) 0.004
Gender (male = 1; female = 2) 1.09 (�4.69 to 6.86) 0.71
Ethnic group (Caucasian = 0; others = 1) �0.66 (�5.87 to 4.55) 0.80
AIS (AIS B = 0; AIS A = 1) �23.29 (�28.07 to �18.50) 50.0005 �22.21 (�26.88 to �17.54) 50.0005
Neurological level (C1–C4 = 1; C5–C8 = 2) 2.42 (�2.33 to 7.16) 0.32
Penetrating injury (no = 0; yes = 1) �7.71 (�14.58 to �0.83) 0.03
Pn/Wi (no = 0; yes = 1) �10.39 (�14.98 to �5.81) 50.0005 �8.21 (�12.29 to �4.14) 50.0005
Mechanical ventilation (no = 0; yes = 1) �9.91 (�14.56 to �5.26) 50.0005
Spinal surgery (no = 0; yes = 1) 0.96 (�4.07 to 6.62) 0.74
Rehospitalization (no = 0; yes = 1) �5.44 (�10.32 to �0.56) 0.03
Enrolment period (1999–2005 = 0;1992–1998 = 1)
�1.65 (�6.43 to 3.14) 0.50
Univariate and multiple linear regression analysis in cervical injury patients AIS A and B score (n = 336). The coding of the variable categories is indicated in the table.Interactions between AIS and pneumonia/postoperative wound infections were not significant with regards to the motor score (P = 0.39). The multiple analysis wasperformed after forward variable selection (R2 = 0.26). With the exceptions of AIS, pneumonia/postoperative wound infections and age, none of the variables that yieldedstatistical significance in the univariate model was confirmed by reaching statistical significance in the multiple model.b = unstandardized regression coefficient.
Pn/W
i
Pn/W
i
Contro
lCon
trol
AIS A
n = 260
Gai
n of
mor
e th
an o
ne m
otor
leve
l G
ain
of o
ne m
otor
leve
l or
less
50%
0%
50%
10%
20%
30%
40%
40%
30%
20%
10%
60%
70%
80%
80%
70%
60%
AIS Bn.s.
n = 87
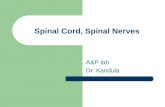
Figure 4 Effect of pneumonia/postoperative wound infection
on motor levels gained 1 year after SCI. A significantly lower
number of AIS A patients gained more than one motor level in
the group with pneumonia/postoperative wound infections
compared with control patients. In incomplete AIS B patients, no
significant differences were observed. �2 test, *P = 0.04.
Pn/W
i Pn/W
i
Contro
l Contro
l
n = 237
AIS AAIS B
n.s.n = 83
Gai
n of
mor
e th
an o
ne s
enso
ry le
vel
Gai
n of
one
sen
sory
leve
l or
less
50%
0%
50%
10%
20%
30%
40%
40%
30%
20%
10%
60%
70%
80%
80%
70%
60%
Figure 5 Effect of pneumonia/postoperative wound infections
on sensory levels gained 1 year after SCI. A significantly lower
number of AIS A patients gained more than one motor level in
the group with pneumonia/postoperative wound infections
compared with control patients. In AIS B patients, no significant
differences were observed. �2 test, *P = 0.03.
3246 | Brain 2012: 135; 3238–3250 V. Failli et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article/135/11/3238/272916 by guest on 31 D
ecember 2021

motor and sensory function (Steeves et al., 2007) in a longitudinal,
multicentre cohort study assessing data from a large prospective
database (Richards et al., 1995; Marino et al., 1999; Stover et al.,
1999; DeVivo et al., 2002). At 1 year after SCI, there were sig-
nificantly fewer upward AIS conversions, lower gains in ASIA
motor score (up to 450%) and lower sensory and motor level
gains in the group with pneumonia/postoperative wound infec-
tion. Pneumonia/postoperative wound infections were evaluated
in logistic regression or linear regression models and identified as
independent risk factors associated with AIS conversion or ASIA
motor score gain. These evaluations were confirmed after multiple
imputation for both models.
The findings for AIS conversion and ASIA motor score evalu-
ation in AIS A were consistent with those in AIS B patients. In the
motor or sensory level analysis, AIS A patients demonstrated a
significant association of pneumonia/postoperative wound infec-
tion with lower sensory or motor level gain. However, this was not
detectable and thus not significant in AIS B patients, a finding that
in a general sense is due to their clearly smaller group sizes com-
pared with AIS A. Further explanation is found in the characteris-
tics of the ASIA assessments and differences in the intrinsic
recovery pattern between AIS A and B patients. In particular,
most AIS B patients reveal partial recovery in several segments
beyond the lesion, whereas for most AIS A patients, the recovery
is restricted to few segments directly adjacent to the lesion level.
In this context, partial sensory or motor recovery might lead to AIS
conversion without necessarily influencing sensory or motor levels,
as for gain of more than one level, full recovery of function is
needed in at least one dermatome or key muscle. In parallel, par-
tial motor recovery in numerous key muscles might lead to sub-
stantial motor score improvement in AIS B patients without
necessarily influencing motor levels.
The group with pneumonia/postoperative wound infection and
the control group did not differ in the longitudinal ASIA motor
score analysis during early observation. This supports the hypoth-
esis that the difference in the observed outcome is attributable to
the pneumonia/postoperative wound infection status, and weak-
ens the alternative hypothesis that pneumonia/postoperative
wound infections just passively accumulate as ‘epiphenomena’ in
patients with more severe types of injury, who are anyhow prone
to have inferior outcomes. Another more general argument is sup-
ported by recent epidemiological studies, which report a higher
upward conversion rate in complete (AIS A) cervical injury
(33%) compared with patients with thoracic injury (18%)
(Steeves et al., 2011; Zariffa et al., 2011). This fundamentally
challenges the assumption that inferior neurological outcome is
just a passive coincidence of a higher degree of organ dysfunction
(e.g. cervical versus thoracic), and implies the relevance of ‘disease
modifying’ factors for the prognosis and evolution of functional
recovery. In conclusion, infections do not appear to be unspecific
markers for patients with SCI with poor prognosis but rather one
of the causes of inferior outcome. Infections appear as early
effectors defining the path of neurological recovery and are char-
acterized by their ability to trigger several specific pathophysio-
logical sequelae as demonstrated in experimental CNS injury
models (Schnell et al., 1997; Meisel et al., 2004; McColl et al.,
2007, 2008; Moreno et al., 2011). The underlying mechanisms by
which infections impair functional neurological recovery are likely
to be multiple.
The induction of pneumonia promotes secondary damage in
experimental ischaemic CNS injury (Meisel et al., 2004; McColl
et al., 2007). Stroke-associated infection might be an independent
risk factor for poor clinical outcome (Vermeij et al., 2009),
although there is consensus that singular interventional trials test-
ing preventive antibiotics have so far been restricted by patient
numbers too low to unequivocally prove improved outcome
(Westendorp et al., 2011). A recent meta-analysis comprising
data from 137 817 patients after acute stroke stresses the need
to prevent infections in acute stroke (Westendorp et al., 2011).
Infections, in particular, pneumonia, appear to be among the main
modifiable factors leading to early death and poor outcome in
patients treated in stroke units (Finlayson et al., 2011;
Koennecke et al., 2011).
Experimental stroke models have provided evidence that sys-
temic inflammation exacerbates the neurological deficit by trigger-
ing a chemokine and acute-phase response (McColl et al., 2007)
with induced vascular tight junction disruption and sustained
blood–brain barrier disturbance (McColl et al., 2008). These mech-
anisms are likewise relevant to SCI because ischaemia is a feature
of traumatic CNS injury. Peripheral infections also aggravate neu-
rodegeneration in experimental models and human neuropathol-
ogy as reviewed by Perry et al. (2003). For example, systemic
inflammation led to axonal damage during inflammatory CNS
disease (Moreno et al., 2011). Sustained degeneration of oligo-
dendrocytes and neurons can be observed even in the late chronic
phase after SCI, as reviewed by Bramlett and Dietrich (2007).
Consequently, the substrate for neuronal plasticity, which is con-
sidered the major effector mechanism for neurological recovery, is
reduced (Reinetenau and Schwab, 2001; Curt et al., 2008).
Preventive antibacterial treatment reduced secondary damage
and improved neurological outcome after experimental stroke
(Meisel et al., 2004). The lesional CNS inflammatory response is
exacerbated and sustained when accompanied by infection,
whether of viral (Schnell et al., 1997) or bacterial (McColl et al.,
2007, 2008) origin. Lesional inflammation can perpetuate neuro-
degeneration through multiple effector mechanisms involving cells
of innate and acquired immunity, as reviewed elsewhere
(Wyss-Coray and Mucke, 2002; Glass et al., 2010). Furthermore,
given that systemic immunological responses are triggered by in-
fections, they are likely to interfere directly or indirectly with the
capacity of the lesioned CNS for adaptive reorganization on many
levels via soluble factors (Reinetenau and Schwab, 2001; Moreno
et al., 2011) by triggering acute-phase responses (Popovich et al.,
2009).
In this study, the group with pneumonia/postoperative wound
infection and the control group did not differ in terms of known
outcome-relevant parameters associated with poor neurological
recovery, with the exception of AIS at baseline, for which the
direct comparison was stratified, and the neurological level,
which was included in the regression models. Noteworthy, pneu-
monia/postoperative wound infection is verified to be independent
of the lesion severity parameter (AIS) and lesion level. In addition,
the rates of penetrating injury and the performance of spinal sur-
gery were comparable in both groups, and patients with
Infections and recovery after SCI Brain 2012: 135; 3238–3250 | 3247
Dow
nloaded from https://academ
ic.oup.com/brain/article/135/11/3238/272916 by guest on 31 D
ecember 2021

interfering concomitant injuries or cognitive impairment were
excluded from the analysis. This suggests that the alternative hy-
pothesis according to which inferior outcome is due to (i) more
severe; (ii) higher lesions; or (iii) more generalized impairment
accompanied by infections seems less likely. Nevertheless, in the
group with pneumonia/postoperative wound infection, a higher
rate of mechanical ventilation was observed. Consequently, a
more frequent ventilation might already appear to be a predispos-
ing reason for higher infection rates that then lead to impaired
neurofunctional outcome. This explanation can be ruled out by
multiple logistic regression analysis, which yields an OR of 1.89
for impaired upward conversions for patients with pneumonia/
postoperative wound infection, whereas mechanical ventilation
itself does not impact AIS upward conversion. Furthermore, with
regards to lower ASIA motor score gain, the multiple linear regres-
sion analysis does not reveal a statistically significant relationship
for mechanical ventilation or any other established outcome-
predictive parameter such as penetrating injury, except for AIS at
admission and age, which was expected. The AIS was included as
an independent variable in both regression models because the
interactions between pneumonia/postoperative wound infections
and AIS were not significant with regards to the dependent vari-
ables. We propose that infection should be considered a novel in-
dependent factor causally linked to poor neurofunctional recovery.
This study has the limitations of a retrospectively performed
evaluation of data from a prospective database. We apply this
setting to generate new hypotheses, with the perspective of opti-
mizing clinical care in the future. We limit our analysis to pneu-
monia and wound infections. Other types of infection frequently
occurring after SCI, such as urinary tract infections, are not
encoded in the NSCID. Thus, the ‘control group’ with no docu-
mented pneumonia/postoperative wound infections might also
contain patients with other infectious complications. However,
the fact that not all infections in the control group are identified
might imply that the effects of infection are even more pro-
nounced and that the control group is thus already impaired in
terms of recovery potential. With regards to the amount of re-
habilitation received, a possible factor influencing the neurological
outcome, our analysis is restricted to the length of stay in rehabili-
tation, as data on the exact amount of rehabilitation were not
accessible for the majority of the study subjects. Nevertheless,
patients with pneumonia/postoperative wound infection had
access over a longer period to in-patient rehabilitation compared
with the control group. Infections might impede functional recov-
ery by limiting the efficacy of rehabilitation. The strengths and
limitations of the NSCID have been described previously (Stover
et al., 1999). Its main limitation is that it is not population based.
Another limitation is that the data of patients who were lost to
follow-up are missing; this might lead to bias in favour of those
patients who were successfully followed relative to the entire data-
base. Loss to follow-up as a source of attrition bias is a common
problem with any longitudinal database. The problem of missing
data within the ‘analysis-in population’ was addressed by multiple
imputation for both regression models. In our imputation analyses,
only �21 or 25% of the variability was explained by covariates,
whereas the complete case analysis explained �26 or 30% of the
variability. Thus, the observed shrinkage of differences after
imputation as compared with complete case analysis is conserva-
tive and probably not due to systematic differences between pa-
tients with complete and patients with missing data.
In conclusion, prospective trials are needed to determine pos-
sible detrimental effects on functional neurological recovery that
could result from infections that are not yet encoded by the
NSCID. Our findings might trigger the incorporation of more de-
tailed information on infectious complications in the relevant SCI
registries such as the NSCID or the European Multicentre Study on
Spinal Cord Injury. It is essential to decipher infections caused by
neurogenic syndromes such as SCI-induced immune depression
syndrome through epidemiological cohort studies to determine
their relevance to outcome and formulate new research hypoth-
eses to improve clinical neurological outcome.
The conclusion of this study identifying SCI-associated infec-
tions as an independent risk factor for poor neurological outcome
provides ‘best evidence’ available and is an essential prerequisite for
regulatory authorities to approve prospective interventional trial
protocols. Based on the reported data, the establishment of early
infection-predictive parameters identifying patients prone to infec-
tion constitutes a consequent, preventive, specific strategy verified
by a feasible time frame of opportunity. The development of
predictive diagnostic parameters (‘immunological fingerprinting’)
(e.g. Urra et al., 2009) would enable a selective preventive interven-
tional approach to protect the limited intrinsic recovery capacity after
SCI and thus improve neurological function. At present, the findings
are of particular relevance for current interventional trials to improve
outcome prediction (e.g. improved patient group stratification)
aiming at cervical lesions (Fawcett et al., 2007; Zorner et al.,
2010). Here, incident postinjury infections (pneumonia/postopera-
tive wound infections) can be confined as a ‘disease modifying’ and
possible confounding factor for effective rehabilitation in interven-
tional trials (Dobkin 2007a, b, 2009; Fouad et al., 2011).
AcknowledgementsWe would like to thank Dr. Lisa Schnell and Prof. Dr. Andreas
Meisel for valuable suggestions for the interpretation of the re-
sults. The Department of Clinical and Experimental Spinal Cord
Injury Research (Neuroparaplegiology), Department of
Experimental Neurology, Charite Universtatsmedizin Berlin, is an
Associated Member of the European Multicentre Study about
Spinal Cord Injury.
FundingThis work was supported by the German Research Council (DFG,
Research Training School, Neuroinflammation, Grant number
1258); the Berlin-Brandenburg Centre for Regenerative Therapies
(BCRT, Grant number 81717034); the International Foundation for
Research in Paraplegia, Switzerland (IFP, Grant number P102); and
Wings for Life Spinal Cord Research Foundation, Austria (Grant
Number WfL-DE-006/12). The NSCID is funded by the National
Institute on Disability and Rehabilitation Research (NIDRR, Grant
number H133A060039), U.S. Department of Education, USA.
3248 | Brain 2012: 135; 3238–3250 V. Failli et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article/135/11/3238/272916 by guest on 31 D
ecember 2021

Supplementary materialSupplementary material is available at Brain online.
ReferencesBramlett HM, Dietrich WD. Progressive damage after brain and spinal
cord injury: pathomechanisms and treatment strategies. Prog Brain Res
2007; 161: 125–41.
Burns AS, Lee BS, Ditunno JF Jr, Tessler A. Patient selection for clinical
trials: the reliability of the early spinal cord injury examination.
J Neurotrauma 2003; 20: 477–82.Curt A, Van Hedel HJ, Klaus D, Dietz V, EM-SCI Study Group. Recovery
from a spinal cord injury: significance of compensation, neural plasti-
city, and repair. J Neurotrauma 2008; 25: 677–85.
DeVivo MJ, Krause JS, Lammertse DP. Recent trends in mortality and
causes of death among persons with spinal cord injury. Arch Phys Med
Rehabil 1999; 80: 1411–19.
DeVivo MJ, Go BK, Jackson AB. Overview of the national spinal
cord injury statistical center database. J Spinal Cord Med 2002; 25:
335–8.
Dobkin BH. Confounders in rehabilitation trials of task-oriented training:
lessons from the designs of the EXCITE and SCILT multicenter trials.
Neurorehabil Neural Repair 2007a; 21: 3–13.
Dobkin BH. Curiosity and cure: translational research strategies for
neural repair-mediated rehabilitation. Dev Neurobiol 2007b; 67:
1133–47.Dobkin BH. Motor rehabilitation after stroke, traumatic brain, and spinal
cord injury: common denominators within recent clinical trials. Curr
Opin Neurol 2009; 22: 563–9.
Fawcett JW, Curt A, Steeves JD, Coleman WP, Tuszynski MH,
Lammertse D, et al. Guidelines for the conduct of clinical trials for
spinal cord injury as developed by the ICCP panel: spontaneous re-
covery after spinal cord injury and statistical power needed for thera-
peutic clinical trials. Spinal Cord 2007; 45: 190–205.
Finlayson O, Kapral M, Hall R, Asllani E, Selchen D, Saposnik G, et al.
Risk factors, inpatient care, and outcomes of pneumonia after ischemic
stroke. Neurology 2011; 77: 1338–45.
Fouad K, Krajacic A, Tetzlaff W. Spinal cord injury and plasticity: oppor-
tunities and challenges. Brain Res Bull 2011; 84: 337–42.
Furlan JC, Krassioukov AV, Fehlings MG. Hematologic abnormalities
within the first week after acute isolated traumatic cervical spinal
cord injury: a case-control cohort study. Spine 2006; 31: 2674–83.
Furlan JC, Fehlings MG, Tator CH, Davis AM. Motor and sensory as-
sessment of patients in clinical trials for pharmacological therapy of
acute spinal cord injury: psychometric properties of the ASIA
Standards. J Neurotrauma 2008; 25: 1273–301.Glass CK, Saijo K, Winner B, Marchetto MC, Gage FH. Mechanisms
underlying inflammation in neurodegeneration. Cell 2010; 140:
918–34.
Held KS, Steward O, Blanc C, Lane TE. Impaired immune responses
following spinal cord injury lead to reduced ability to control viral in-
fection. Exp Neurol 2010; 226: 242–53.
Koennecke HC, Belz W, Berfelde D, Endres M, Fitzek S, Hamilton F,
et al. Factors influencing in-hospital mortality and morbidity in patients
treated on a stroke unit. Neurology 2011; 77: 965–72.Lucin KM, Sanders VM, Jones TB, Malarkey WB, Popovich PG. Impaired
antibody synthesis after spinal cord injury is level dependent and is due
to sympathetic nervous system dysregulation. Exp Neurol 2007; 207:
75–84.
Marino RJ, Ditunno JF Jr, Donovan WH, Maynard F Jr. Neurologic re-
covery after traumatic spinal cord injury: data from the Model Spinal
Cord Injury Systems. Arch Phys Med Rehabil 1999; 80: 1391–6.
Marino RJ. International standards for neurological classification of spinal
cord injury. J Spinal Cord Med 2003; 26 (Suppl 1): S50–6.
McColl BW, Rothwell NJ, Allan SM. Systemic inflammatory stimulus po-
tentiates the acute phase and CXC chemokine responses to experi-
mental stroke and exacerbates brain damage via interleukin-1- and
neutrophil-dependent mechanisms. J Neurosci 2007; 27: 4403–12.
McColl BW, Rothwell NJ, Allan SM. Systemic inflammation alters the
kinetics of cerebrovascular tight junction disruption after experimental
stroke in mice. J Neurosci 2008; 28: 9451–62.Meisel C, Prass K, Braun J, Victorov I, Wolf T, Megow D, et al.
Preventive antibacterial treatment improves the general medical and
neurological outcome in a mouse model of stroke. Stroke 2004; 35:
2–6.
Meisel C, Schwab JM, Prass K, Meisel A, Dirnagl U. Central nervous
system injury-induced immune deficiency syndrome. Nat Rev
Neurosci 2005; 6: 775–86.
Moreno B, Jukes JP, Vergara-Irigaray N, Errea O, Villoslada P, Perry VH,
et al. Systemic inflammation induces axon injury during brain inflam-
mation. Ann Neurol 2011; 70: 932–42.
Oropallo MA, Held KS, Goenka R, Ahmad SA, O’Neill PJ, Steward O,
et al. Chronic spinal cord injury impairs primary antibody responses but
spares existing humoral immunity in mice. J Immunol 2012; 188:
5257–66.Perry VH, Newman TA, Cunningham C. The impact of systemic infection
on the progression of neurodegenerative disease. Nat Rev Neurosci
2003; 4: 103–12.
Popovich P, McTigue D. Damage control in the nervous system: be-
ware the immune system in spinal cord injury. Nat Med 2009; 15:
736–7.
Raineteau O, Schwab ME. Plasticity of motor systems after incomplete
spinal cord injury. Nat Rev Neurosci 2001; 2: 263–73.
Richards JS, Go BK, Rutt RD, Lazarus PB. The national spinal cord injury
collaborative database. In: Stover SL, DeLisa JA, Whiteneck GG, edi-
tors. Spinal cord injury: clinical outcomes from the model systems.
Gaithersburg, MD: Aspen Publishers; 1995. p. 10–20.
Riegger T, Conrad S, Schluesener HJ, Kaps HP, Badke A, Baron C, et al.
Hematologic cellular inFammatory response following human spinal
cord injury [abstract]. Acta Neuropathol 2003; 106: 392.Riegger T, Conrad S, Liu K, Schluesener HJ, Adibzahdeh M, Schwab JM.
Spinal cord injury-induced immune depression syndrome (SCI-IDS). Eur
J Neurosci 2007; 25: 1743–7.
Riegger T, Conrad S, Schluesener HJ, Kaps HP, Badke A, Baron C, et al.
Immune depression syndrome following human spinal cord injury
(SCI): a pilot study. Neuroscience 2009; 158: 1194–9.
Schnell L, Schneider R, Berman MA, Perry VH, Schwab ME. Lymphocyte
recruitment following spinal cord injury in mice is altered by prior viral
exposure. Eur J Neurosci 1997; 9: 1000–7.
Sekhon LH, Fehlings MG. Epidemiology, demographics, and patho-
physiology of acute spinal cord injury. Spine 2001; 26 (Suppl 24):
S2–12.
Steeves JD, Lammertse D, Curt A, Fawcett JW, Tuszynski MH,
Ditunno JF, et al. International Campaign for Cures of Spinal Cord
Injury Paralysis. Guidelines for the conduct of clinical trials for spinal
cord injury (SCI) as developed by the ICCP panel: clinical trial outcome
measures. Spinal Cord 2007; 45: 206–21.
Steeves JD, Lammertse D, Curt A, Fawcett JW, Tuszynski MH,
Ditunno JF, et al. Extent of spontaneous motor recovery after trau-
matic cervical sensorimotor complete spinal cord injury. Spinal Cord
2011; 49: 257–65.
Stover SL, DeVivo MJ, Go BK. History, implementation, and current
status of the National Spinal Cord Injury Database. Arch Phys Med
Rehabil 1999; 80: 1365–71.Urra X, Villamor N, Amaro S, Gomez-Choco M, Obach V, Oleaga L,
et al. Monocyte subtypes predict clinical course and prognosis in
human stroke. J Cereb Blood Flow Metab 2009; 29: 994–1002.
Vega JL, Ganea D, Jonakait GM. Acute down-regulation of antibody
production following spinal cord injury: role of systemic catechol-
amines. J Neuropathol Exp Neurol 2003; 62: 848–54.
Vermeij FH, Scholte op Reimer WJ, de Man P, van Oostenbrugge RJ,
Franke CL, de Jong G, et al. Stroke-associated infection is an
Infections and recovery after SCI Brain 2012: 135; 3238–3250 | 3249
Dow
nloaded from https://academ
ic.oup.com/brain/article/135/11/3238/272916 by guest on 31 D
ecember 2021

independent risk factor for poor outcome after acute ischemic stroke:data from the Netherlands Stroke Survey. Cerebrovasc Dis 2009; 27:
465–71.
Westendorp WF, Nederkoorn PJ, Vermeij JD, Dijkgraaf MG, van de
Beek D. Post-stroke infection: a systematic review and meta-analysis.BMC Neurol 2011; 11: 110.
Wyss-Coray T, Mucke L. Inflammation in neurodegenerative disease—a
double-edged sword. Neuron 2002; 35: 419–32.
Zariffa J, Kramer JL, Fawcett JW, Lammertse DP, Blight AR, Guest J,et al. Characterization of neurological recovery following traumatic
sensorimotor complete thoracic spinal cord injury. Spinal Cord 2011;
49: 463–71.
Zorner B, Blanckenhorn WU, Dietz V, EM-SCI Study Group, Curt A.Clinical algorithm for improved prediction of ambulation and patient
stratification after incomplete spinal cord injury. J Neurotrauma 2010;
27: 241–52.
3250 | Brain 2012: 135; 3238–3250 V. Failli et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article/135/11/3238/272916 by guest on 31 D
ecember 2021