
Functional and esthetics prosthetic rehabilitation in the ...sjod.org/eJournals/_eJournals/22_CASE...
4
42 Scientific Journal of Dentistry ● Vol. 2:1 ● Jan-Feb 2015 Scientific Journal of Dentistry (2015), 2, 42-45 CASE REPORT Functional and esthetics prosthetic rehabilitation in the elderly patient with metal ceramic crowns Fabrício Reskalla Amaral 1 , Marcelo Ferrarezi de Andrade 2 , José Roberto Cury Saad 2 , José Claudio Martins Segalla 2 , Andrea Abi Rached Dantas 2 , Élida Lúcia Assunção 3 , Sizenando de Toledo Porto Neto 2 1 Department of Odontologia, UNESP, Araraquara, Brazil, 2 Department of Restorative Odontology, UNESP, Araraquara, Brazil, 3 Department of Dentistry, PUC, Belo Horizonte, Minas Gerais, Brazil Abstract With patients increasingly seeking esthetics, advances in the dental area now offer many forms of treatment in order to achieve success. This paper aims to report a clinical case of functional and esthetic rehabilitation involving prostheses over implants and esthetics crowns on the posterior area as well as on the anterior area in an elderly patient. The results achieved were very satisfactory for both the dental surgeon and the patient. The self-esteem of the patient improved after this treatment, thus improving her interpersonal relations. Keywords Ceramic, dentistry, mouth rehabilitation Correspondence Dr. Fabrício Reskalla Amaral, Departamento de Odontologia, Rua Oscar Paulo Freire n 115/302, Cep: 36025-350 Juiz de Fora, Minas Gerais, Brazil. Email: fabricioreskalla@yahoo. com.br Received October 22, 2014; Accepted December 13, 2014 doi: 10.15713/ins.sjod.22 How to cite the article: Amaral FR, de Andrade MF, Saad JR, Segalla JC, Dantas AAR, Assunção ÉL, Neto ST. Functional and esthetics prosthetic rehabilitation in elderly patient with metal ceramic crowns. Sci J Dent 2015;2:42-45. Introduction The quest for health associated with better esthetics has become increasingly more evident. Culturally, the association of these two aspects contributed a lot for a better social life of patients. Deficiencies related to changes in color, shape, size, position, total or partial loss of the teeth can trigger damage, such as numerous physiological mastication, phonation and cause joint disorders temporomandibular, besides undeniable negative impacts to patients’ quality of life, such as low self-esteem and psychological inability. [1-7] Among the various dental treatments available in the market to rehabilitate the patient, the metal-ceramic restorations have great clinical success in the long-term, because they have excellent physical and optical characteristics derived from metallic and ceramic infrastructure. The metallic infrastructure provides high resistance and aesthetic properties, such as fluorescence, opalescence and translucency of ceramic. These esthetic properties are similar to those of tooth enamel and dentin. They are natural and widely recommended for patients who have partial or total destruction in dental crowns or large restorations. [8-12] The main positive characteristics of metal-ceramic restorations include Young’s modulus, also known as elastic modulus. It has high support stiffness, high thermal expansion coefficient, hardness supporting masticatory stress and keeping the anatomic configuration of the occlusal and interproximal, marginal integrity, high fracture toughness (about 2.3% after 7½ years), and require less removal of tooth structure to achieve the proper thickness for the prosthesis. [13-18] Another method of obtaining reliable unit (or total) is oral rehabilitation through the use of dental implants. [3,19,20] The
Transcript of Functional and esthetics prosthetic rehabilitation in the ...sjod.org/eJournals/_eJournals/22_CASE...
42 Scientific Journal of Dentistry ● Vol. 2:1 ● Jan-Feb 2015
Scientific Journal of Dentistry (2015), 2, 42-45
C A S E R E P O R T
Functional and esthetics prosthetic rehabilitation in the elderly patient with metal ceramic crownsFabrício Reskalla Amaral1, Marcelo Ferrarezi de Andrade2, José Roberto Cury Saad2, José Claudio Martins Segalla2, Andrea Abi Rached Dantas2, Élida Lúcia Assunção3, Sizenando de Toledo Porto Neto2
1Department of Odontologia, UNESP, Araraquara, Brazil, 2Department of Restorative Odontology, UNESP, Araraquara, Brazil, 3Department of Dentistry, PUC, Belo Horizonte, Minas Gerais, Brazil
AbstractWith patients increasingly seeking esthetics, advances in the dental area now offer many forms of treatment in order to achieve success. This paper aims to report a clinical case of functional and esthetic rehabilitation involving prostheses over implants and esthetics crowns on the posterior area as well as on the anterior area in an elderly patient. The results achieved were very satisfactory for both the dental surgeon and the patient. The self-esteem of the patient improved after this treatment, thus improving her interpersonal relations.
Keywords Ceramic, dentistry, mouth rehabilitation
Correspondence Dr. Fabrício Reskalla Amaral, Departamento de Odontologia, Rua Oscar Paulo Freire n 115/302, Cep: 36025-350 Juiz de Fora, Minas Gerais, Brazil. Email: [email protected]
Received October 22, 2014; Accepted December 13, 2014
doi: 10.15713/ins.sjod.22
How to cite the article: Amaral FR, de Andrade MF, Saad JR, Segalla JC, Dantas AAR, Assunção ÉL, Neto ST. Functional and esthetics prosthetic rehabilitation in elderly patient with metal ceramic crowns. Sci J Dent 2015;2:42-45.
Introduction
The quest for health associated with better esthetics has become increasingly more evident. Culturally, the association of these two aspects contributed a lot for a better social life of patients.
Deficiencies related to changes in color, shape, size, position, total or partial loss of the teeth can trigger damage, such as numerous physiological mastication, phonation and cause joint disorders temporomandibular, besides undeniable negative impacts to patients’ quality of life, such as low self-esteem and psychological inability.[1-7]
Among the various dental treatments available in the market to rehabilitate the patient, the metal-ceramic restorations have great clinical success in the long-term, because they have excellent physical and optical characteristics derived from metallic and ceramic infrastructure.
The metallic infrastructure provides high resistance and aesthetic properties, such as fluorescence, opalescence and translucency of ceramic. These esthetic properties are similar to those of tooth enamel and dentin. They are natural and widely recommended for patients who have partial or total destruction in dental crowns or large restorations.[8-12]
The main positive characteristics of metal-ceramic restorations include Young’s modulus, also known as elastic modulus. It has high support stiffness, high thermal expansion coefficient, hardness supporting masticatory stress and keeping the anatomic configuration of the occlusal and interproximal, marginal integrity, high fracture toughness (about 2.3% after 7½ years), and require less removal of tooth structure to achieve the proper thickness for the prosthesis.[13-18]
Another method of obtaining reliable unit (or total) is oral rehabilitation through the use of dental implants.[3,19,20] The
Amaral, et al. Prosthetic rehabilitation in the elderly patient
Scientific Journal of Dentistry ● Vol. 2:1 ● Jan-Feb 2015 43
rehabilitation treatment relies on implants in the maxilla or jaw and it is a widely accepted method. However, a treatment like this requires some considerations when inserted in aesthetic areas, as it needs a continuing education of professionals and proper planning of each case. It is possible to achieve rehabilitation with esthetic quality and natural gingival contour.[4,6,16,21]
The advantages and disadvantages of each rehabilitation treatment should be observed in details. It must take into account the patient’s expectations, functionality, success, perspective, and financial resources.[10,15,16,22]
Satisfying results of rehabilitation depend on a correct diagnosis and proper planning. When rehabilitating a patient, the physician must have a thorough understanding of the physiological factors that may affect the patient’s occlusion, because the natural and artificial elements must have a functional relationship and harmonious aesthetic.[14,23,24]
Among the desirable characteristics for an occlusal oral rehabilitation, it is possible to mention the incorporation of physiological occlusal vertical dimension, which will facilitate to obtain a mutually protected occlusion, transmitting the resultant of occlusal forces in the direction of the long axis of the posterior teeth. Another important point is the obtainment of bilateral contacts, simultaneous posterior elements as well as lateral and anterior guides to protect the rehabilitation.[4,9,24-26]
Articulated study models and diagnostic wax can provide important information for the diagnosis and treatment evaluation.[5,11,17,22,27,28]
Case Report
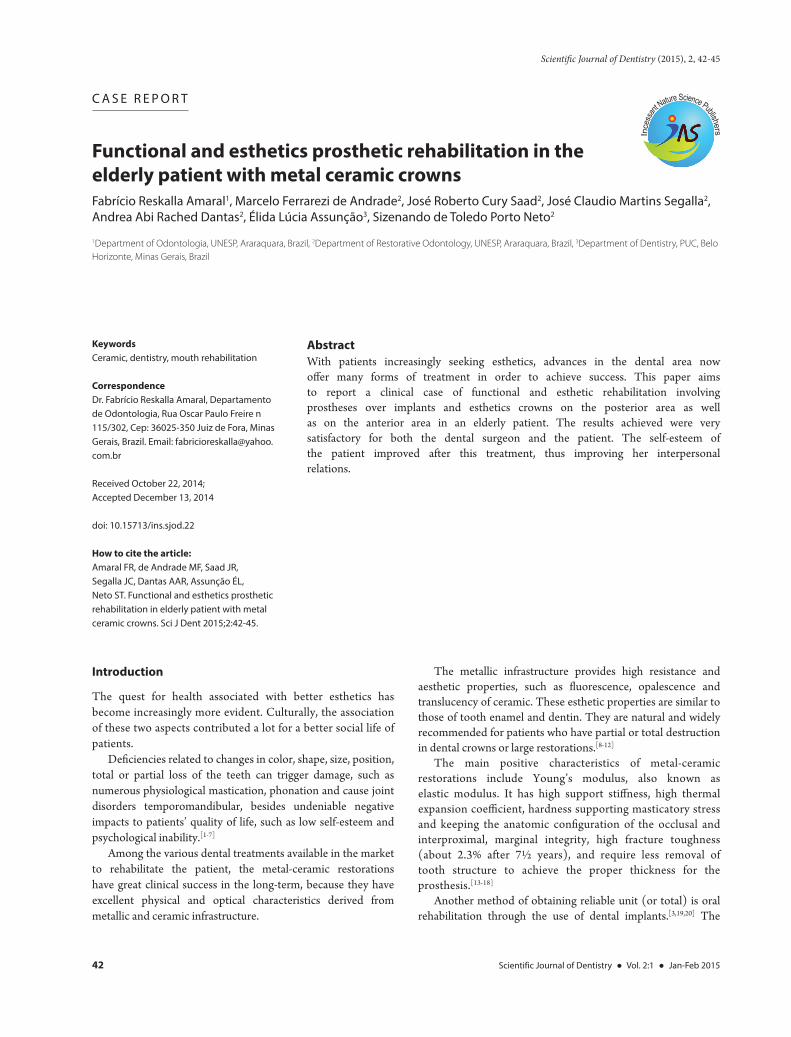
A patient, 62 years old, appeared at the dental office complaining about the absence of the elements 35, 36, 44 and 45, in which the patient was previously operated with the insertion of bone grafts without immediate loading. However, there was a need to rehabilitate the patient prosthetically because some elements had extensive and aesthetically unsatisfactory asymmetry of shape, color and placement, with occlusal and functional losses. Due to the factors outlined above, as well as by the analysis of X-ray panoramic examinations and computed tomography in the treatment plan, it was proposed a rehabilitation process with metal-ceramic crowns in the upper arch and the prosthesis on implants in the lower arch.
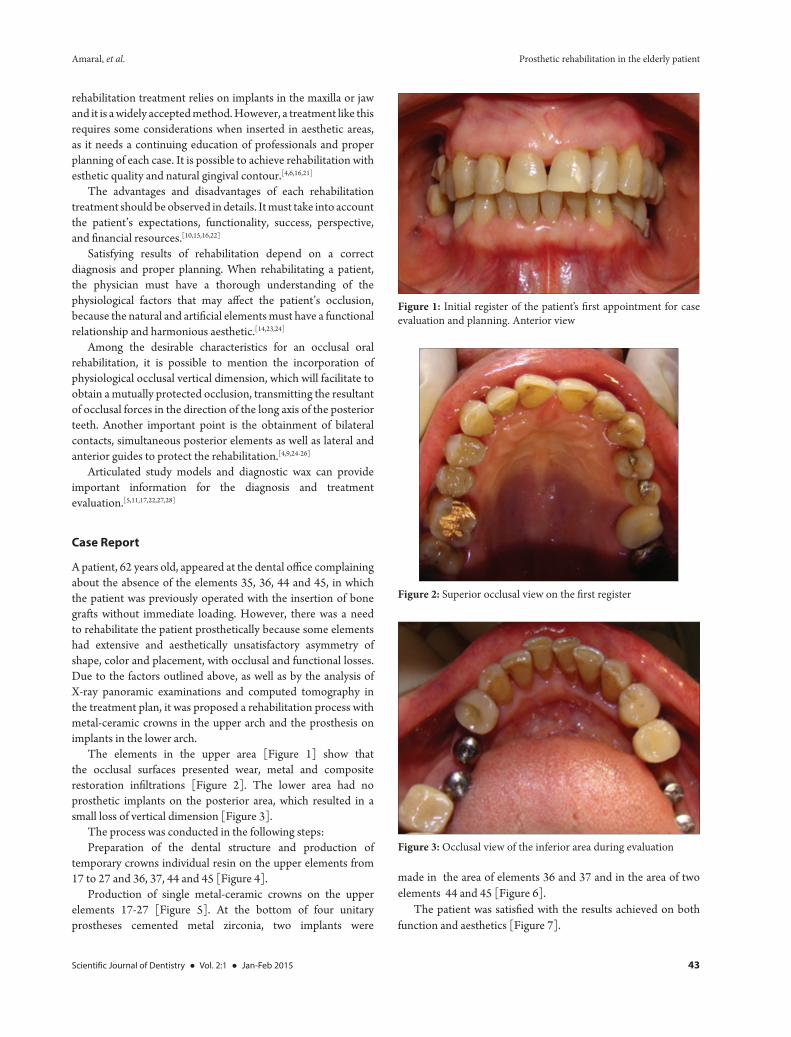
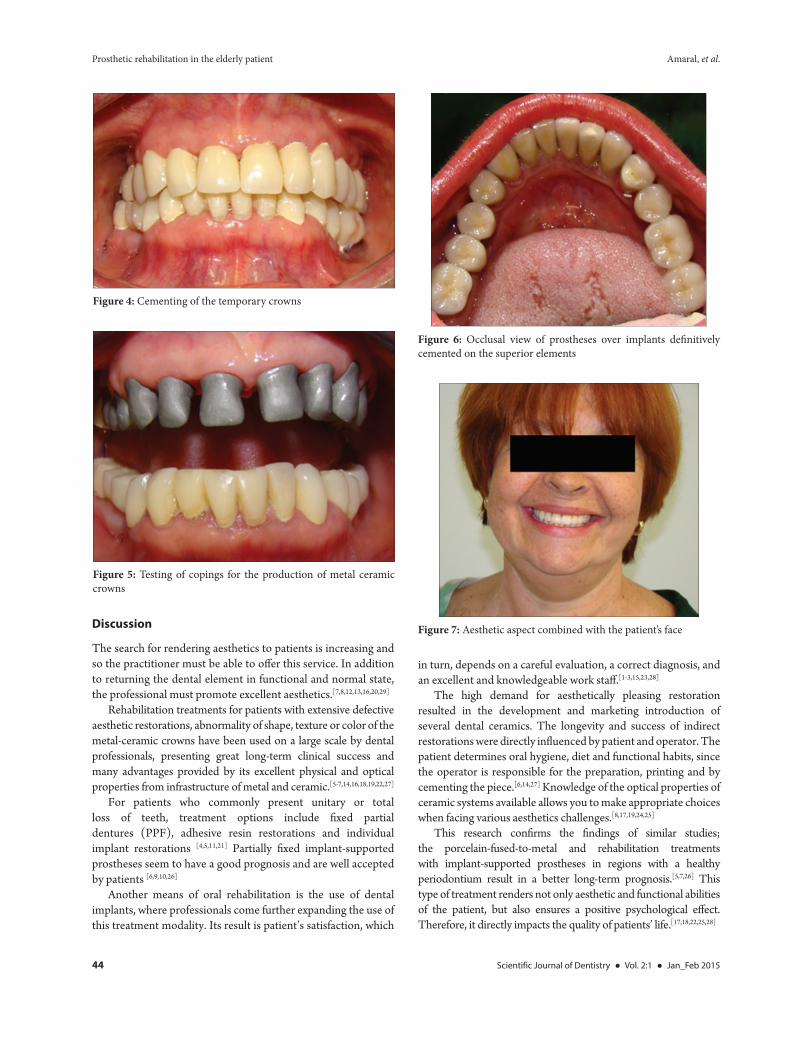
The elements in the upper area [Figure 1] show that the occlusal surfaces presented wear, metal and composite restoration infiltrations [Figure 2]. The lower area had no prosthetic implants on the posterior area, which resulted in a small loss of vertical dimension [Figure 3].
The process was conducted in the following steps:Preparation of the dental structure and production of
temporary crowns individual resin on the upper elements from 17 to 27 and 36, 37, 44 and 45 [Figure 4].
Production of single metal-ceramic crowns on the upper elements 17-27 [Figure 5]. At the bottom of four unitary prostheses cemented metal zirconia, two implants were
made in the area of elements 36 and 37 and in the area of two elements 44 and 45 [Figure 6].
The patient was satisfied with the results achieved on both function and aesthetics [Figure 7].
Figure 1: Initial register of the patient’s first appointment for case evaluation and planning. Anterior view
Figure 2: Superior occlusal view on the first register
Figure 3: Occlusal view of the inferior area during evaluation
Prosthetic rehabilitation in the elderly patient Amaral, et al.
44 Scientific Journal of Dentistry ● Vol. 2:1 ● Jan_Feb 2015
Discussion
The search for rendering aesthetics to patients is increasing and so the practitioner must be able to offer this service. In addition to returning the dental element in functional and normal state, the professional must promote excellent aesthetics.[7,8,12,13,16,20,29]
Rehabilitation treatments for patients with extensive defective aesthetic restorations, abnormality of shape, texture or color of the metal-ceramic crowns have been used on a large scale by dental professionals, presenting great long-term clinical success and many advantages provided by its excellent physical and optical properties from infrastructure of metal and ceramic.[5-7,14,16,18,19,22,27]
For patients who commonly present unitary or total loss of teeth, treatment options include fixed partial dentures (PPF), adhesive resin restorations and individual implant restorations [4,5,11,21] Partially fixed implant-supported prostheses seem to have a good prognosis and are well accepted by patients [6,9,10,26]
Another means of oral rehabilitation is the use of dental implants, where professionals come further expanding the use of this treatment modality. Its result is patient’s satisfaction, which
in turn, depends on a careful evaluation, a correct diagnosis, and an excellent and knowledgeable work staff.[1-3,15,23,28]
The high demand for aesthetically pleasing restoration resulted in the development and marketing introduction of several dental ceramics. The longevity and success of indirect restorations were directly influenced by patient and operator. The patient determines oral hygiene, diet and functional habits, since the operator is responsible for the preparation, printing and by cementing the piece.[6,14,27] Knowledge of the optical properties of ceramic systems available allows you to make appropriate choices when facing various aesthetics challenges.[8,17,19,24,25]
This research confirms the findings of similar studies; the porcelain-fused-to-metal and rehabilitation treatments with implant-supported prostheses in regions with a healthy periodontium result in a better long-term prognosis.[5,7,26] This type of treatment renders not only aesthetic and functional abilities of the patient, but also ensures a positive psychological effect. Therefore, it directly impacts the quality of patients’ life.[17,18,22,25,28]
Figure 4: Cementing of the temporary crowns
Figure 5: Testing of copings for the production of metal ceramic crowns
Figure 6: Occlusal view of prostheses over implants definitively cemented on the superior elements
Figure 7: Aesthetic aspect combined with the patient’s face

Amaral, et al. Prosthetic rehabilitation in the elderly patient
Scientific Journal of Dentistry ● Vol. 2:1 ● Jan-Feb 2015 45
Conclusion
The treatment achieved a satisfactory aesthetic and functional rehabilitation. It has provided an appropriate function for the patient’s quality of life, and the expected aesthetic result was obtained.
References
1. Morley J. The role of cosmetic dentistry in restoring a youthful appearance. J Am Dent Assoc 1999;130:1166-72.
2. Goyal MK, Goyal S, Hegde V, Balkrishana D, Narayana AI. Recreating an esthetically and functionally acceptable dentition: A multidisciplinary approach. Int J Periodontics Restorative Dent 2013;33:527-32.
3. Fradeani M. The application of all-ceramic restorations in the anterior and posterior regions. Pract Proced Aesthet Dent 2003;Suppl:13-7.
4. Anusavice KJ. Cerâmicas Odontológicas. In: Anusavice KJ, editor. Phillips, Materiais Dentários. São Paulo: Elsevier; 2005. p. 619-77.
5. Kronström M, Palmqvist S, Söderfeldt B, Vigild M. Subjective need for implant treatment among middle-aged people in Sweden and Denmark. Clin Implant Dent Relat Res 2002;4:11-5.
6. Jahangiri L, Jang S. Onlay partial denture technique for assessment of adequate occlusal vertical dimension: A clinical report. J Prosthet Dent 2002;87:1-4.
7. Johansson LA, Ekfeldt A. Implant-supported fixed partial prostheses: A retrospective study. Int J Prosthodont 2003;16:172-6.
8. Pena CE, Viotti RG, Dias WR, Santucci E, Rodrigues JA, Reis AF. Esthetic rehabilitation of anterior conoid teeth: Comprehensive approach for improved and predictable results. Eur J Esthet Dent 2009;4:210-24.
9. Rekow ED, Harsono M, Janal M, Thompson VP, Zhang G. Factorial analysis of variables influencing stress in all-ceramic crowns. Dent Mater 2006;22:125-32.
10. Zitzmann NU, Sendi P, Marinello CP. An economic evaluation of implant treatment in edentulous patients-preliminary results. Int J Prosthodont 2005;18:20-7.
11. Stanford CM. Application of oral implants to the general dental practice. J Am Dent Assoc 2005;136:1092-100.
12. Reshad M, Jivraj S. The influence of posterior occlusion when restoring anterior teeth. J Calif Dent Assoc 2008;36:567-74.
13. Weinstein AR. Esthetic applications of restorative materials and techniques in the anterior dentition. Dent Clin North Am 1993;37:391-409.
14. Eckert SE, Laney WR. Patient evaluation and prosthodontic treatment planning for osseointegrated implants. Dent Clin North Am 1989;33:599-618.
15. Gardner FM, Tillman-McCombs KW, Gaston ML, Runyan DA. In vitro failure load of metal-collar margins compared with porcelain facial margins of metal-ceramic crowns. J Prosthet Dent 1997;78:1-4.
16. Naylor WP. Essentials of metal ceramic substructure design. In: Naylor WP, editor. Introduction to Metal Ceramic Technology. Chicago: Quintessence; 1992. p. 43-64.
17. Kindberg H, Gunne J, Kronström M. Tooth- and implant-supported prostheses: A retrospective clinical follow-up up to 8 years. Int J Prosthodont 2001;14:575-81.
18. Bottino MA, Quintas AF, Miy Ashit AE, Giannini V. Estetica Em ReabilitacAo Oral Metal-Free. São Paulo: Artes Medicas; 2001.
19. Wall JG, Cipra DL. Alternative crown systems. Is the metal-ceramic crown always the restoration of choice? Dent Clin North Am 1992;36:765-82.
20. Adell R, Lekholm U, Rockler B, Brånemark PI. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg 1981;10:387-416.
21. McIntyre F. Restoring esthetics and anterior guidance in worn anterior teeth. A conservative multidisciplinary approach. J Am Dent Assoc 2000;131:1279-83.
22. Mete JJ, Dange SP, Khalikar AN, Vaidya SP. Functional and esthetic rehabilitation of mutilated dentition associated with amelogenesis imperfecta. J Indian Prosthodont Soc 2012;12:94-100.
23. Dias AH, Myashita E, Nono MC, Bottino MA. Avaliacão mecânica e microestrutural da interface ceramo-cerâmica. PGRO Post-Graduate Journal in Dentistry 2005;8(2):31-8.
24. Martin MP. Material and clinical considerations for full-coverage indirect restorations. Compend Contin Educ Dent 2012;33:2-5.
25. Cancão MY, Parque JM, Parque EJ. Full mouth rehabilitation of the patient with severely worn dentition: A case report. J Adv Prosthod 2010;2(3):106-10.
26. Santezi C, Tonetto MR, Presoto CD, Jasse FF, de Oliveira Júnior OB, de Andrade MF, et al. Anterior restorations in bleached teeth: Difficulty establishing the color after bleaching. J Contemp Dent Pract 2012;13:735-9.
27. Stanford CM. A role in geriatric dentistry for the general practice? J Am Dent Assoc 2007;138:34S-40.
28. Vargas MA, Bergeron C, Arnold AD. Cementing all-ceramic restorations recommendations for success. J Am Dent Assoc 2011;142:20S-24.
29. Cuello SJ, Pasquini CM, Bazáez FM, Oliva BC. Carillas directas con resinas compuestas: Una alternativa en operatoria dental. RCOE 2003;8:415-21.


















