Full Text (PDF) - cancerres.aacrjournals.orgcancerres.aacrjournals.org/content/72/3/616.full.pdf ·...
11
Molecular and Cellular Pathobiology Common Structural and Epigenetic Changes in the Genome of Castration-Resistant Prostate Cancer Terence W. Friedlander 1 , Ritu Roy 2 , Scott A. Tomlins 4 , Vy T. Ngo 3 , Yasuko Kobayashi 3 , Aruna Azameera 3 , Mark A. Rubin 6 , Kenneth J. Pienta 5 , Arul Chinnaiyan 4 , Michael M. Ittmann 7 , Charles J. Ryan 1 , and Pamela L. Paris 1,3 Abstract Progression of primary prostate cancer to castration-resistant prostate cancer (CRPC) is associated with numerous genetic and epigenetic alterations that are thought to promote survival at metastatic sites. In this study, we investigated gene copy number and CpG methylation status in CRPC to gain insight into specific pathophysiologic pathways that are active in this advanced form of prostate cancer. Our analysis defined and validated 495 genes exhibiting significant differences in CRPC in gene copy number, including gains in androgen receptor (AR) and losses of PTEN and retinoblastoma 1 (RB1). Significant copy number differences existed between tumors with or without AR gene amplification, including a common loss of AR repressors in AR- unamplified tumors. Simultaneous gene methylation and allelic deletion occurred frequently in RB1 and HSD17B2, the latter of which is involved in testosterone metabolism. Lastly, genomic DNA from most CRPC was hypermethylated compared with benign prostate tissue. Our findings establish a comprehensive methylation signature that couples epigenomic and structural analyses, thereby offering insights into the genomic alterations in CRPC that are associated with a circumvention of hormonal therapy. Genes identified in this integrated genomic study point to new drug targets in CRPC, an incurable disease state which remains the chief therapeutic challenge. Cancer Res; 72(3); 616–25. Ó2011 AACR. Introduction Despite the effectiveness of castrating therapies in slowing the growth of metastatic prostate cancer, therapeutic resis- tance eventually develops. Unchecked, metastatic castration- resistant prostate cancer (CRPC) is lethal, causing approxi- mately 30,000 annual deaths in the United States (1). Tissue from metastatic CRPC is difficult to obtain for genetic characterization because biopsies can be technically challeng- ing and are generally unnecessary for routine clinical decision making. Considerably less is therefore understood about the later acquired genetic alterations that emerge in the context of the selection pressure of an androgen-deprived milieu. To address this, rapid autopsy programs were developed to provide high-quality metastatic tissue for research (2–4). Tissue obtained from these studies has been used for genomic analysis and to create cell lines and xenograft models (2). In addition, improvements in DNA and RNA array–based tech- niques have allowed for the acquisition of high-resolution quantitative tumor genome information from small amounts of tissue. This includes the quantification of global gene copy number (CN), expression level, and gene CpG methylation status. Recent studies of metastatic CRPC have examined the variation in androgen receptor (AR) splicing (5), AR signaling (6), tumor heterogeneity (7), and has identified new targets for therapy (8). Similarly, a number of recent studies have impli- cated local androgen production by tumor cells (9–11). Geno- mic studies across different platforms, as described here, allow a more thorough investigation and yield a more complete picture of the genetic changes that occur in CRPC. In this study, 15 metastatic CRPC tumors obtained at autopsy were profiled using comprehensive high-resolution array-comparative geno- mic hybridization (aCGH) and methylation arrays to describe the most common CN aberrations in metastatic CRPC and their concordant methylation levels. Materials and Methods Clinical profile of cases Fifteen tumors were obtained from rapid autopsies of 14 patients, including 2 metastases from 1 individual carried out Authors' Affiliations: 1 Division on Genitourinary Medical Oncology, 2 Biostatistics Core, Helen Diller Family Comprehensive Cancer Center, and 3 Department of Urology, University of California, San Francisco, California; Departments of 4 Pathology and 5 Urology and Internal Medicine, University of Michigan Comprehensive Cancer Center, Ann Arbor, Michi- gan; 6 Department of Pathology, Weill Cornell Medical College, New York, New York; and 7 Department of Pathology, Baylor College of Medicine, Houston, Texas Note: Supplementary data for this article are available at Cancer Research Online (http://cancerres.aacrjournals.org/). Corresponding Author: Terence W. Friedlander, Division of Genitourinary Medical Oncology, Helen Diller Family Comprehensive Cancer Center, UCSF Box 3110, 1450 3rd Street HD384, San Francisco, CA 94143. Phone: 415-514-2559; Fax: 415-514-4987; E-mail: [email protected] doi: 10.1158/0008-5472.CAN-11-2079 Ó2011 American Association for Cancer Research. Cancer Research Cancer Res; 72(3) February 1, 2012 616 on May 13, 2018. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from Published OnlineFirst December 7, 2011; DOI: 10.1158/0008-5472.CAN-11-2079
Transcript of Full Text (PDF) - cancerres.aacrjournals.orgcancerres.aacrjournals.org/content/72/3/616.full.pdf ·...

Molecular and Cellular Pathobiology
Common Structural and Epigenetic Changes in the Genomeof Castration-Resistant Prostate Cancer
Terence W. Friedlander1, Ritu Roy2, Scott A. Tomlins4, Vy T. Ngo3, Yasuko Kobayashi3, Aruna Azameera3,Mark A. Rubin6, Kenneth J. Pienta5, Arul Chinnaiyan4, Michael M. Ittmann7, Charles J. Ryan1, andPamela L. Paris1,3
AbstractProgression of primary prostate cancer to castration-resistant prostate cancer (CRPC) is associated with
numerous genetic and epigenetic alterations that are thought to promote survival atmetastatic sites. In this study,we investigated gene copy number and CpG methylation status in CRPC to gain insight into specificpathophysiologic pathways that are active in this advanced form of prostate cancer. Our analysis defined andvalidated 495 genes exhibiting significant differences in CRPC in gene copy number, including gains in androgenreceptor (AR) and losses of PTEN and retinoblastoma 1 (RB1). Significant copy number differences existedbetween tumors with or without AR gene amplification, including a common loss of AR repressors in AR-unamplified tumors. Simultaneous gene methylation and allelic deletion occurred frequently in RB1 andHSD17B2, the latter of which is involved in testosterone metabolism. Lastly, genomic DNA from most CRPCwas hypermethylated comparedwith benign prostate tissue. Our findings establish a comprehensivemethylationsignature that couples epigenomic and structural analyses, thereby offering insights into the genomic alterationsin CRPC that are associated with a circumvention of hormonal therapy. Genes identified in this integratedgenomic study point to new drug targets in CRPC, an incurable disease state which remains the chief therapeuticchallenge. Cancer Res; 72(3); 616–25. �2011 AACR.
Introduction
Despite the effectiveness of castrating therapies in slowingthe growth of metastatic prostate cancer, therapeutic resis-tance eventually develops. Unchecked, metastatic castration-resistant prostate cancer (CRPC) is lethal, causing approxi-mately 30,000 annual deaths in the United States (1).
Tissue frommetastatic CRPC is difficult to obtain for geneticcharacterization because biopsies can be technically challeng-ing and are generally unnecessary for routine clinical decisionmaking. Considerably less is therefore understood about thelater acquired genetic alterations that emerge in the context ofthe selection pressure of an androgen-deprived milieu.
To address this, rapid autopsy programs were developedto provide high-quality metastatic tissue for research (2–4).Tissue obtained from these studies has been used for genomicanalysis and to create cell lines and xenograft models (2). Inaddition, improvements in DNA and RNA array–based tech-niques have allowed for the acquisition of high-resolutionquantitative tumor genome information from small amountsof tissue. This includes the quantification of global gene copynumber (CN), expression level, and gene CpG methylationstatus.
Recent studies of metastatic CRPC have examined thevariation in androgen receptor (AR) splicing (5), AR signaling(6), tumor heterogeneity (7), and has identified new targets fortherapy (8). Similarly, a number of recent studies have impli-cated local androgen production by tumor cells (9–11). Geno-mic studies across different platforms, as described here, allowa more thorough investigation and yield a more completepicture of the genetic changes that occur in CRPC. In this study,15 metastatic CRPC tumors obtained at autopsy were profiledusing comprehensive high-resolution array-comparative geno-mic hybridization (aCGH) and methylation arrays to describethe most common CN aberrations in metastatic CRPC andtheir concordant methylation levels.
Materials and Methods
Clinical profile of casesFifteen tumors were obtained from rapid autopsies of 14
patients, including 2 metastases from 1 individual carried out
Authors' Affiliations: 1Division on Genitourinary Medical Oncology,2Biostatistics Core, Helen Diller Family Comprehensive Cancer Center,and 3Department of Urology, University of California, San Francisco,California; Departments of 4Pathology and 5Urology and Internal Medicine,University of Michigan Comprehensive Cancer Center, Ann Arbor, Michi-gan; 6Department of Pathology, Weill Cornell Medical College, New York,New York; and 7Department of Pathology, Baylor College of Medicine,Houston, Texas
Note: Supplementary data for this article are available at Cancer ResearchOnline (http://cancerres.aacrjournals.org/).
Corresponding Author: Terence W. Friedlander, Division of GenitourinaryMedical Oncology, Helen Diller Family Comprehensive Cancer Center,UCSFBox 3110, 1450 3rdStreet HD384, San Francisco, CA 94143. Phone:415-514-2559; Fax: 415-514-4987; E-mail: [email protected]
doi: 10.1158/0008-5472.CAN-11-2079
�2011 American Association for Cancer Research.
CancerResearch
Cancer Res; 72(3) February 1, 2012616
on May 13, 2018. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2011; DOI: 10.1158/0008-5472.CAN-11-2079

from 1996–1999. Clinical characteristics have been reported(2); all had metastatic CRPC, had received hormonal therapy,and all but one had received chemotherapy.To corroborate findings from the metastatic cohort, a
separate cohort of 36 intermediate grade primary prostatetumors obtained at prostatectomy were also obtained. Patientclinical characteristics and methods used to isolate DNA havebeen reported (12). With amedian of 60.2 months follow up, 14patients had biochemical evidence of recurrent disease, where-as 22 did not.
Tissue processingThe tissue procurement procedure has been described (2).
Metastatic liver (N¼ 7) or soft-tissue (N¼ 8) lesions were usedfor genomic analysis, including 2 separate soft-tissue depositsfrom the same patient, both of which were used. A singlepathologist (MR) sectioned 15 tissue slices at 15 mm from areaswith extensive tumor involvement. DNA was extracted with aWizard Genomic DNA Isolation kit (Promega) and purified byphenol/chloroform extraction. All DNAs were of sufficientquality and quantity for genomic analysis by gel chromatog-raphy and UV-Vis spectrophotometry.
Array comparative genomic hybridizationaCGH was carried out using Human Genome microarrays
(Agilent), consisting of 244,000 60-mer oligonucleotide DNAprobes with approximately 9 kb average spatial resolution,with pooled male lymphocyte DNA (single lot, Promega) as areference sample. Labeling and microarray processing weredone according to the manufacturer's protocol using 500 ng ofgenomic DNA. After 60-hour hybridization, microarrays werescanned at 10 mm resolution using an Agilent-G25005B scan-ner. All samples passed Agilent quality control assessment.Feature-level data was abstracted with Agilent software. CNwas expressed as the log2 ratio of tumor:control DNA fluores-cence intensity.
DNA methylation profilingDNA was bisulfite converted using the EZ DNAMethylation
Kit (Zymo). DNA was then whole-genome amplified, enzymat-ically fragmented, precipitated, resuspended, and hybridizedovernight at 48�C to an array containing 27,578 locus-specificoligonucleotide primers (Illumina). After hybridization, the Cor T nucleotides were detected by fluorescent single-baseprimer extension using an Illumina BeadStation GX scanner.Data were analyzed with Genome Studio software (v2009.1;
Illumina) which assigns a quantitative measure of the meth-ylation level (b value) for each CpG site, corresponding to theratio between the fluorescence signal from the methylatedallele (C) and the sum of the fluorescence signals of themethylated (C) and unmethylated (T) alleles for that CpG site.Themethylation status for each site ranges from 0 (completelyunmethylated) to 1 (completely methylated). Conservative bvalue cutoffs of �0.8, <0.8 to >0.2, and �0.2 were used,respectively, to call a CpG locus homozygously methylated,heterozygously methylated, or unmethylated. Hierarchicalclustering of b values used the Pearson correlation as thesimilarity measure and complete linkage as the agglomeration
method and was analyzed with R software. Only probes inwhich 50% ormore of samples had nonmissing data and whichhad SD greater than the 25th percentile were used for whole-genome clustering (20,675 of 27,578), and in which not allsamples had the same methylation status (513 of 27,578) forexploration of probes differentially methylated across samples.Using methylated and unmethylated status encoded as 1 and�1, respectively, hierarchical clustering was done separatelywith Cluster and Treeview softwares (13) using Euclideandistance as the similarity measure and Ward's agglomerationmethod (14).
Validation of candidate gene copy changesA subset of samples showing AR copy gain or PTEN deletion
by aCGH were selected for validation using the TaqMan GeneCopy Number Assay (Applied Biosystems) with the UCSFGenome Core. Reference samples included pooled male lym-phocyte DNA (Promega), DNA from 2 castration-sensitiveprimary prostate tumors known to harbor normal AR andPTENCNby aCGH (unpublisheddata), andAR andPTENcopy-normal DNA (Coriell; ref. 15). The internal reference gene wasRnaseP. Tennanograms ofDNAwasusedper sample and run inquadruplicate per manufacturer's instructions. CN analysiswas done using CopyCaller software (Applied Biosystems).
Gene expressionA subset of the metastases (5 liver, 8 soft tissue) were
analyzed at the University of Michigan by Dr. Tomlins (dataavailable on Oncomine; ref. 16) on AgilentWhole-HumanGeneExpression 44K microarrays against pooled benign prostatetissue (Clontech). RNA preparation has been previouslydescribed (17). Hierarchical clustering was done using log2ratio values, Euclidean distance, and Ward's agglomerationmethod (14). Only those probes which had at least 50% ofsamples with nonmissing data were considered (466 of 507probes).
Pathway analysisThePanther libraries (18–21) were used to identify pathways
containing genes of interest. A binomial statistical tool is usedto compare classifications of multiple clusters of lists to aRefSeq-based reference list to statistically determine whetherspecific classification categories are over- or underrepresent-ed, using the Bonferroni method to adjust for multiple testing.
Statistical analysisCN data was mapped to the human genome sequence hg18
freeze and log2 intensity ratios were segmented using circularbinary segmentation to translate noisy intensity measure-ments into regions of equal CN (22). The median absolutedeviation (MAD), scaled by the factor 1.4826, of the differencebetween the observed and segmented values was used toestimate the sample-specific experimental variation. Outlierprobes were identified as those which were more than 4sample-specific MAD away from their segment value. For eachsample, a segment was declared gained or lost if the segmentvalue wasmore than 2 times the sampleMAD from themediansegment value of the autosomes. Y chromosome probes were
Structural and Epigenetic Changes in CRPC
www.aacrjournals.org Cancer Res; 72(3) February 1, 2012 617
on May 13, 2018. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2011; DOI: 10.1158/0008-5472.CAN-11-2079

excluded. Probe-wise frequency plots of CN alterations werebased on gain/loss/normal status.
Probes in which CN aberrations were significantlyassociated with one group versus another were identifiedbased on segment values with original log2 ratios for outlierprobes and using moderated t statistics as implementedin the limma package (23) in Bioconductor (24). Q valueswere computed from the nominal P values to adjust formultiple testing by controlling the false discovery rate (25). AQ value cutoff of 0.05 or less was used to declare a probe tobe significant.
For the AR gene aberration analysis all 20 probes map-ping to the AR gene had the same CN status for all samples(copy normal or amplified). These AR probes were excludedwhen carrying out probe-wise tests of association of CNwith AR and also when testing association of chromosomalarms with AR. The sample profiles were clustered usinggain, loss, and copy-normal status encoded as 1, �1, and 0,respectively. Hierarchical clustering was done as discussedabove.
To analyze the correlation between gene expression and CN,each expression probe was mapped to the closest CN probe.Only expression probes which were less than 50 kb from theclosest CN probe and in which there were 5 or more sampleswith CN aberration, identified as having absolute CN segmentvalue greater than 0.3, were considered. A Spearman correla-tion coefficient was computed for each probe. P values, cal-culated using asymptotic t approximation, identified signifi-cant correlations for a precompiled candidate list of genesinvolved in androgen and phosphatidyl-inositol-3-kinase(PI3K) signaling (Supplementary Table S1).Q values, computedto correct for multiple testing, identified significant correla-tions for noncandidate genes. P andQ values cutoffs 0.05 or lesswere, respectively, considered significant.
All analyses were done using R software in the UCSFBiostatistics Core. The aCGH andmethylationmicroarray datahave been deposited in National Center for BiotechnologyInformation Gene Expression Omnibus (ref. 26; accession no.GSE34174).
Results
Oligonucleotide aCGHOverall, 217,960 (92.8%) probes had a CN aberration (gain or
loss) in at least one of the 15 metastatic samples. Specifically,119,405 (50.84%) probes had amplification and 180,372 (76.8%)probes had deletion in 1 or more samples. The absolute log2ratio for copy change relative to the control ranged from�6.41(homozygous loss) for AK054947 on chromosome 6, to þ5.88(gain of 59 copies) for KIF4A, located 2.56 Mb downstream ofAR on chromosome X.
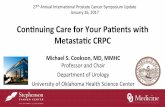
Figure 1 shows the probe-wise frequency of CN changesacross the entire genome for all metastatic samples. A fre-quency value of 66% or more (i.e., �10 of the samples) was setto identify commonly amplified or deleted probes. After fil-tering out probes in intergenic regions, 495 unique genes (79amplified and 416 deleted)met this frequency cutoff (Gene list,Supplementary Table S2).
Validation of copy number gains and lossesThe CN of 2 candidate genes, AR and PTEN, was assayed
using a TaqMan PCR assay. These genes were selected becauseboth have been shown to be amplified (AR) or deleted (PTEN)in prostate cancer, both were frequently aberrant in themetastatic aCGH analysis (AR, 73%; PTEN 87%), and both arepresent at normal CN in available controls (15). Onemetastaticsample harboring AR copy gain and one harboring PTENdeletion as determined by aCGH were selected (Fig. 2).
For the metastatic sample, the mean aCGH log2 ratio acrossall probes in the AR gene was 3.41 (range: 2.65–4.08), corre-sponding to a mean gain of 11 copies per cell. By PCR, thissample had 8 copies (range: 7.65–9.17) per cell (Fig. 2A and B).Similarly, the mean aCGH log2 ratio across all probes in thePTEN gene for the selected sample was�2.11 (range: �0.54 to�2.73), indicating deletion of one or both copies per cell. ByPCR, this sample had 0.55 copies (range: 0.54–0.6), correspond-ing to heterozygous PTEN deletion with some evidence of bothcopies being lost (Fig. 2C and D).
Correlation of copy number results with expressionOf the 495 commonly aberrant genes identified by aCGH, 318
(64%) were both represented on the expression array and hadavailable expression data. After inclusion of candidate genesinvolved in androgen and P13K signaling and correction formultiple testing for noncandidate genes, 77 genes were iden-tified which had a significant correlation of gene CN toexpression (Spearman correlation range: 0.5–0.89, Q < 0.05,Gene list, Supplementary Table S1).
We next investigated whether CN aberrations in thesecorrelated genes were present in unmatched primary tumors,and if so, whether the aberrations were associated with recur-rence after prostatectomy. A higher prevalence of CN aberra-tions was observed for the correlated genes in recurrent cases(26.8%, N ¼ 14 recurrent cases) than for nonrecurrent tumors(17%, N¼ 22 nonrecurrent cases, Fisher's exact test, P < 0.001).This comparison held for the entire 495 copy aberrant gene set,
1.0
0.8
0.6
0.4
0.2
0.0
−0.2
−0.4
−0.6
−0.8
−1.0
2
1 3 5 7
Chromosome number
9 11 13 15 17 19 21 x
4 6 8 10 12 14 16 18 20 22
Fra
cti
on
ga
ine
d o
r lo
st
of
all
sa
mp
les
Figure 1. Genome topography of lethal prostate cancer. aCGH CNfrequency plot for 15 metastatic CRPC tumors. Y-axis, fraction of thesamples altered. Horizontal black bars represent a 0.66 fraction. X-axis,probes across thegenome.Green, gains; red, losses. The vertical dashedlines represent the centromeres.
Friedlander et al.
Cancer Res; 72(3) February 1, 2012 Cancer Research618
on May 13, 2018. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2011; DOI: 10.1158/0008-5472.CAN-11-2079

with 26.1% of genes aberrant in the recurrent group comparedwith 15.5% in the nonrecurrent group (P < 0.001).The most common copy gains and losses, defined by a
frequency 66% or more occurred on 6 specific chromosomes(6, 8, 10, 13, 16, and X). Mapping of correlated genes (CN andexpression) was done to evaluate whether focused regions ofalteration could be identified for these commonly aberrantchromosomes and, in so doing, identify potential "driver"genes, whose expression correlates with their tumor genomiccopy status, from potential "passenger" genes, whose expres-sion levels do not. This proved to be most useful on chromo-some 8 (Fig. 3).
Genomics of AR amplificationBecause AR overexpression is key to CRPC growth and
because AR amplification and expression were significantlycorrelated (P ¼ 0.03), the degree of genomic AR amplificationwas investigated. AR amplification was present in 11 of 15(73%) of the metastatic samples. Across the 20 AR microarrayprobes, the average log2 ratio for copy gain was 1.7 in the
AR-amplified subset compared with 0.16 in the remaining 4samples (referred to as AR copy normal). Overall, the maxi-mum AR log2 ratio detected for a single probe was 4.08,corresponding to 17 AR gene copies per cell.
To further explore the differences between AR copy-normaland AR-amplified samples, genome topography plots wereconstructed for each subset (Fig. 4). Despite the small samplesize, it is evident that AR-amplified samples have a higheroverall frequency of amplification across their entire tumorgenome, with 66% or more of samples having copy gain inchromosomes 7q, 8q, and X. Between the 2 groups therewas nosignificant difference in arm-wise chromosomal deletions, andno single probe was found to be significantly different aftercorrection for multiple testing.
It is plausible that the AR copy-normal tumors have acti-vated the AR pathway by means other than AR amplification,thus a supervised analysis was undertaken to investigate theCN of 197 genes that regulate AR signaling (27). Retinoblas-toma 1 (RB1) and PTEN, considered to have a role in ARregulation, were deleted and underexpressed in both cohorts.
A B
C D
AR
AR
Co
py
nu
mb
er
PTEN
PTEN
Metastatic CRPC
Log2 ratio
Metastatic CRPC
Log2 ratio
Ch
rom
os
om
e 1
0C
hro
mo
so
me
X
9
8
7
6
5
4
3
2
1
0
Co
py
nu
mb
er
2
1
0
Singlefemale
germlineDNA
Singlemale
germlineDNA
Pooledmale
germlineDNA
PrimaryCSPC
MetastaticCRPC
Singlefemale
germlineDNA
Singlemale
germlineDNA
Pooledmale
germlineDNA
PrimaryCSPC
PrimaryCSPC
–3
p22.32
p15.2
p14
p12.33p12.31
p12.1p11.22
q11.22
q21.1
q21.3
q22.2
q23.1q23.31q23.33q24.2q24.32
q25.1
q25.3q26.12
p22.2p22.12
p21.3
p21.1
p11.3
p11.22
q12
q13.2
q21.1
q21.31
q21.33q22.2
q23
q25
q26.2
q27.1
q27.3
–2 –1 0 +1 +2 +3
–3 –2 –1 0 +1 +2 +3
MetastaticCRPC
Figure 2. Copy number validation with PCR. A, AR-amplification by TaqMan PCR confirms gain in a metastatic CRPC tumor. Due to location on the Xchromosome, normal males harbor only one copy of AR. CSPC (castration-sensitive prostate cancer) and germline DNA, controls. B, aCGH of same CRPCtumor profiled in A, showing focal AR amplification. C, PTEN deletion by TaqMan PCR confirms loss in a metastatic CRPC tumor. D, aCGH of same CRPCtumor profiled in C, showing focal PTEN deletion.
Structural and Epigenetic Changes in CRPC
www.aacrjournals.org Cancer Res; 72(3) February 1, 2012 619
on May 13, 2018. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2011; DOI: 10.1158/0008-5472.CAN-11-2079

Four genes were found to have discordant copy status betweenthe 2 AR groups. Amplification of the AR coactivator NCOA2was significantly associated (P¼ 0.002) with the presence of ARamplification, whereas deletion of large tumor suppressor,homolog 2 (LATS2) and pleiomorphic adenoma gene-like 1(PLAG1) were detected in 75% of AR copy-normal samples, butin none of the AR-amplified tumors. DnaJ (Hsp40) homolog,subfamily C,member 3 (DNAJC3) was found to be deleted in allAR copy-normal samples, but in only 36% of AR-amplifiedsamples.
To parse out the evolution of NCOA2 andAR amplification, acomparison of this dataset with genome-wide CN data from 36
primary prostate tumors was done. NCOA2 is amplified in 21%of primary tumorswhich subsequently recurred biochemically,compared with 9% of nonrecurrent tumors (Fisher's exact test,P¼ 0.36); ARwas not amplified in any primary prostate tumors.
Methylation signature of metastatic CRPCAverage methylation values were higher for the metastatic
samples than those reported for benign prostate tissueanalyzed on the same platform (28). The average b valuewas 0.38 (0.34–0.41) across all of the metastatic samples,compared with 0.3 for benign prostate tissue. When restrictedto CpG islands (N ¼ 20,006 probes), the average b value per
Chromosome 8
Co
py n
um
ber
: E
xp
ressio
n
co
rrela
tio
n Q
Base position
Delectedlocus #1
Delectedlocus #2
Centromere
0 20,000,000 40,000,000 60,000,000 80,000,000 100,000,000 120,000,000 140,000,000
Genes with frequent copy
gain/loss (≥66% samples)
Agilent 244K probe
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
Amplicon #1 Amplicon #2
Figure 3. Mapping of frequently copy aberrant genes. Mapping reveals 2 amplicons and 2 loci of deletion on chromosome 8. Positively correlated genes arefound above the dashed horizontal line. Correlated deleted genes: BIN3, RHOBTB2, CHMP7, LOXL2, FUT10, and RBM13. Correlated amplified genes:TERF1, RPL7, STAU2, UBE2W, COX6C, and GRHL2. X-axis, chromosome position. Y-axis, Q value for CN: expression correlation.
AR CN normal (N = 4)
AR amplified (N = 11)
1
0
–1
2
1 3 5 7 9 11 13 15 17 19 21 x
1 3 5 7 9 11 13 15 17 19 21 x
4 6 8 10 12 14 16 18 20 22
2 4 6 8 10 12 14 16 18 20 221
0
–1
Chromosome number
Fra
cti
on
Fra
cti
on
Figure 4. Genome topography ofCRPC stratified by AR copynumber (CN) status. Y-axis,fraction of the samples altered. X-axis, probes across the genome.Green, gains; red, losses. Verticaldashed lines represent thecentromeres.
Friedlander et al.
Cancer Res; 72(3) February 1, 2012 Cancer Research620
on May 13, 2018. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2011; DOI: 10.1158/0008-5472.CAN-11-2079

sample was 0.27 (0.23–0.31) compared with 0.16 for benigntissue, and for non-CpG islands (N¼ 7,572 probes), the averagemethylationwas 0.64 (0.59–0.68) comparedwith 0.58 for benigntissue.For the metastases, 9,217 probes (33.4%) were methylated in
at least one sample. The average number of methylated probesper patient was 4,744 (17.2%, range: 3,522–6,388). Of all 27,578CpG sites assayed, there were 1,361 sites (4.9%) that weremethylated across all samples, corresponding to 1,133 differentgenes (7.3% of all genes on the array, Supplementary Table S3).Hierarchical clustering was done to establish a comprehen-
sive methylation signature of metastatic CRPC. Figure 5Ashows that the majority of probes (blue) are unmethylated.After subtracting probes with identical methylation statusacross all samples, there were 513 probes which showeddifferential methylation among the samples (Fig. 5B). Twodifferent patterns of CpG methylation emerged, with themajority of samples having a mixed methylation phenotype(hyper and hypomethylated) and a subset of samples(Met29_23M, 25_46M, and 12_6M) evincing a hypomethylatedphenotype relative to the rest. This hypomethylated set did notsegregate by clinical factors (Gleason score, PSA at diagnosis,time from diagnosis to death, and type of therapy received) norby pathologic–genomic factors (metastatic site, whole-genomeCN, and AR amplification status). Three classes of genes wereunmethylated in this subset whereas methylated in more than90% of the other samples, including the homeobox genes(HOXC11, HOXD3, HOXB2, and HOXD4), 2 PI3K isoforms(PIK3CG and PIK3CD), as well as 4 kallikrein isoforms, (KL,KLK1, KLK4, and KLK5).
Integrated analysis of methylation with copy numberAn analysis was undertaken to compare the frequency of
methylation to the frequency of gene CN in the metastaticsamples and describe their interaction. Methylation occurredat a much higher rate (10.5% of all genes on the methylationarray) than common CN changes (2.1% of all genes on the CNarray). Seventy of the 416 commonly deleted genes (35%) hadconcurrent methylation in 1 or more samples. Overall 16 genesincluding the tumor suppressor RB1 were found to havemethylation and copy loss occurring together in the sametumor in 66% or more of samples.
Genes frequently structurally and epigenetically alteredwere then mapped into pathways and the overlap explored.Overall, the gene sets mapped to 3 common pathways: andro-gen biosynthesis (3 of 20 CN genes, P ¼ 0.006; 8 of 20methylation genes, P ¼ 0.004), the p53 pathway (6 of 113 CNgenes, P¼ 0.01; 24 of 113methylation genes, P¼ 0.008), and theIGF1-protein kinase B signaling cascade (4 of 89 CN genes, P¼0.035; 19 of 89 methylation genes, P ¼ 0.04).
Genomics of the androgen biosynthesis pathwayBoth theCNand themethylation gene setswere significantly
enriched for genes responsible for androgen synthesis andmetabolism. Three of 20 genes in this pathway, HSD17B2,HSDL1, and LIPF, were both simultaneously copy lost andmethylated in the promoter region. Of the gene set immedi-ately involved in testosterone synthesis, methylation of CpGsites in the gene body of both CYP17A1 and HSD17B3 wasobserved (Fig. 6). AR was unmethylated at all 11 CpG sitesinvestigated.
Genomics of p53/IGF-1/protein kinase B signalingcascade
The p53 pathway and the IGF-1/protein kinase B signalingcascade pathways share a number of similar aberrant genes,including deletion of PTEN and methylation within the genebody and promoter of multiple subcomponents of the PI3kinase as well as promoter methylation of AKT3. Two tumorsuppressors in the p53 pathway, RB1 and TNFRSF10C, werefound to be both deleted as well as exhibit promotermethylation.
Genomics and site of metastasisTo investigate whether structural, epigenetic, and/or tran-
scriptional changes play a role in determining the site ofmetastatic spread, hierarchical clustering of samples wascarried out individually for CN, methylation, and expression.Neither CN, methylation nor expression separated the samplesby metastatic site (Fig. 5 and Supplementary Fig. S1).
TMPRSS2-ERG and TMPRSS2-ETS2 mappingGenomic alterations involving TMPRSS2, ERG, and ETS2
were previously reported in 8 of these 15 samples (29). Because
Figure 5. Hierarchical clustering ofCRPC samples by methylation.A, clustering of samples bycontinuous b value. B, clustering ofsamples by categorical methylationstatus (b value�0.8 or�0.2). Probeswith identical methylation status in allsamples were excluded. X-axis,methylation array probes. Red,methylated; blue, unmethylated;white, missing data. �,hypomethylated subset.
A BMet22_62MMet24_6MMet17_18MMet20_6MMet10_36MMet26_38MMet3_81MMet18_6MMet13_21MMet6_9MMet28_41MMet28_5MMet12_6M*Met29_23M*Met25_46M*
Met28_5MMet28_41MMet6_9MMet13_21MMet26_38MMet18_6MMet17_18MMet3_81MMet20_6MMet10_36MMet24_6MMet22_62MMet29_23M*Met25_46M*Met12_6M*
Liver≤0.2 ≥0.8
β value Tissue site
0.5 Soft tissue
Structural and Epigenetic Changes in CRPC
www.aacrjournals.org Cancer Res; 72(3) February 1, 2012 621
on May 13, 2018. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2011; DOI: 10.1158/0008-5472.CAN-11-2079

these genes are found in close proximity on chromosome 21,high-resolution mapping of this locus was done to explorewhether the deletion of intergenomic DNA between TMPRSS2and ERG or ETS2 and specific breakpoints in these regionswere detectable using aCGH.
In total, genomic deletions in this region were detectable in12 of the 15 samples assessed, including the 8 detected pre-viously by FISH (Fig. 7), one which harbored only a smalldeletion in TMPRSS2, and 3 additional samples which har-bored deletion of the entire genomic segment that includedTMPRSS2, ERG, and ETS2. Most of the intergenic deletionsencompass ETS and introns 1–3 of ERG. Of note, ETS2 wasunmethylated in all samples, TMPRSS2 promoter methylationwas present in 1 sample, and ERG promoter methylation waspresent in 6 samples. No clear correlation of ERG methylationand other genomic aberrations was found. More detailedinformation about the aCGH and methylation results is inSupplementary Table S4.
Discussion
In this study, a high-resolution integrated analysis of struc-tural and epigenetic changes was done on metastatic CRPCtumors. Although small, the sample set is a rare resource forwhich whole-genome analysis can provide insight into thelethal form of prostate cancer. Multiple lines of evidencesupport the copy changes observed. First,many of the commoncopy changes observed, including AR gain and loss of PTENand RB1 are consistent with those reported in previous studies(8, 30, 31). Second, a novel PCR-based tool was used toqualitatively confirm the CN aberrations observed, showingfor the first time the feasibility and application of this specific
approach for validating genomic changes observed with large-scale arrays. Further work is needed to determine the quan-titative accuracy of this approach. Third, the gene set identifiedas commonly aberrant in these metastatic samples was morefrequently aberrant in a separate set of primary prostatetumors which recurred after surgery compared with thosethat did not recur. Lastly, mapping of the locus of deletionbetween TMPRSS2 and ETS2 was consistent with prior FISHresults in this sample set (29) and also shows the usefulness ofhigh-resolution aCGH in mapping specific intrachromosomaltranslocation breakpoints.
AR amplification was common, and AR expression corre-lated strongly with copy change (Spearman correlation 0.53,Q ¼ 0.05). When compared with AR-unamplified tumors, AR-amplified tumors were found to commonly carry coamplifica-tions of broad areas along chromosomes 7, 8, and X. Amongthese, amplification of the AR coactivator and putative onco-gene NCOA2 was significantly associated (P ¼ 0.002) with thepresence of AR amplification. NCOA2 amplification has beenreported to be amplified in 17% of metastatic tumors; in thisstudy it was amplified in 60% of samples (8). This differencecould be due to different statistical methods used to analyzeaCGH or the relatively small sample sizes in each study. It hasbeen suggested that AR and NCOA2 genes cooperate in earlyprostate cancer (32); however, it seems likely that tumors firstacquire NCOA2 amplification along with broad amplificationson chromosome 8q. Work by us and others has shown gain of8q to be a common event but AR gain rare in primary tumors(33). NCOA2-amplified tumors may then be essentially"primed" for increased androgen responsiveness, which occursonce AR becomes amplified at a later time point. An exami-nation of either metastatic castration-sensitive or newly cas-tration-resistant tumors would help further define this evolu-tion and could potentially aid in identifying patients more orless likely respond to AR-targeted therapies.
Although 4 patients in this study lacked AR amplification,they nonetheless died of metastatic CRPC. Although no singlegene was uniquely amplified in this subset, statistically signif-icant losses were observed in genes critical to the repression ofAR activity. Specifically, 3 putative tumor suppressors weredeleted including LATS2, a negative regulator of AR (34),PLAG1, a transcription factor thought to function as a repres-sor of AR transcriptional activity (35), and DNAJC3, whichcodes for the c-subunit of the HSP40 complex which preventsnuclear AR translocation (36). Loss of any of these genes ispostulated to derepress AR activity and lead to increased AR-mediated signaling, thereby potentially conferring a selectivetumor growth advantage that could occur in the absence ofAR gene amplification. These cases also raise the possibilitythat the progression of tumors without AR amplification maynevertheless be driven by aberrations of AR signaling asopposed to completely AR-independent pathways. Furtherstudy is needed to see whether this observation holds in largersample sets.
Although gene amplification and deletion have beendescribed as mechanisms of genomic change in CRPC, rela-tively little is known about CpG methylation and its effect onthe development and progression of this disease. Here, for the
Progesterone
17OH-progesterone
Legend:
Androstenedione
Testosterone
AR
CYP17A1
CYP17A1
HSD17B2 HSD17B3
CN Meth
47% 87%
CN Meth
Copy
number
Effect onexpression
+
–
+
–Methylation
47%
Deletion
Promoter
87%
CN Meth
0%73%
CN Meth CN Meth
73% 67% 100%
Amplification
Gene body
13%
Figure 6. Epigenetic and structural genomic bias toward testosteroneproduction in CRPC. CN andmethylation status of key enzymes involvedin testosterone synthesis are shown. Legend, postulated effect of copychange and methylation. The assumption that intragenic methylationincreases transcription is hypothesis generating. These findings suggestintratumoral testosterone production is favored.
Friedlander et al.
Cancer Res; 72(3) February 1, 2012 Cancer Research622
on May 13, 2018. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2011; DOI: 10.1158/0008-5472.CAN-11-2079

first time, a comprehensive methylation signature of meta-static CRPC is established (Fig. 5) using a high-resolution array.Overall, the results show that whereas the majority of probesare unmethylated, CRPC is slightly hypermethylated comparedwith benign tissue. This hypermethylation occurs at individualCpG loci, both within and outside the context of CpG islands.Whether CRPC is globally hypo- or hypermethylated relative toearlier prostate tumors is not established in this study.Although methylation signatures appeared similar for the
majority of samples, at least 3 samples (Mets 29_23, 25_46, and12_6) were hypomethylated. These tumors did not differ byclinical or pathologic characteristics nor by the CN or meth-ylation status of the DNA methyltransferase gene (DNMT).Three classes of genes were differentially methylated betweenthese 2 methylation subsets, including homeobox genes impli-cated in tumorigenesis (37), PI3K isoforms known to beinvolved in protein translation (38), as well as multiple kalli-krein isoforms, proteases implicated in tumor invasion andmetastasis, of which PSA is a member (39). Whether thesemethylation changes would influence response to therapies,including inhibitors of PI3K/AKT/mTOR and/or serve as bio-markers for response to other therapies is worthy of futureinvestigation.Hierarchical clustering by CN, expression (Supplementary
Fig. S1), and methylation (Fig. 5) was unable to establish agenomic signature of a liver or a soft-tissue metastasis. Thefinding that tumors do not cluster by tissue type is in concor-
dance with work showing that metastatic prostate tumorshave monoclonal origins (7). Although multiple genomicchanges must occur to allow a tumor cell to metastasize toa distant site, the clustering in this study implies that for ametastatic tumor, few if any specific CN or methylationchanges are needed to allow it to establish itself in liver tissuecompared with soft tissue. Whether this is true of othermetastatic sites including bone is not known. The small samplesize and large number of comparisons with whole-genomedata may miss small, consistent changes across tumors. Fur-ther study is needed in larger metastatic sets to determine thegene(s)/mechanism(s) that program a cancer cell to hone to aparticular organ.
Integrating the CN and methylation analyses, it was foundthat CpG methylation occurs more frequently for genes com-monly deleted than for those commonly amplified. The obser-vation that CN and methylation work in concert more fre-quently for genes deleted than for those amplified suggests thatgene silencing may occur through heterozygous loss of oneallele and CpG methylation of the remaining allele. Thiscooperation may be essential for inhibiting expression ofcritical tumor suppressors, such as RB1, which was bothfrequently deleted and methylated in CRPC. This points toCpG methylation as a possible therapeutic target in CRPC, forwhich there are already available hypomethylating agents (e.g.,5-azacytidine). More work fully dissecting the functional sig-nificance of the commonly observed epigenetic and structural
Figure 7. Mapping copy number status of TMPRSS2, ERG, and ETS2. Determination of probable breakpoints by aCGH on chromosome 21. Eight CRPCsamples with interstitial alterations for this locus are shown. A log2 ratio of 0 is normal CN. More detailed information is provided in Supplementary Table S4.
Structural and Epigenetic Changes in CRPC
www.aacrjournals.org Cancer Res; 72(3) February 1, 2012 623
on May 13, 2018. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2011; DOI: 10.1158/0008-5472.CAN-11-2079

changes is needed, and control tumors of earlier stage andconsistent grade will help identify which epigenetic and struc-tural changes occur early or late in the development of CRPC.
Intracrine androgen signaling is implicated in prostatecancer progression (11), and the integrated analysis heresuggests that methylation and CN changes may occur concur-rently to both promote the local production and inhibit localbreakdown of potent androgens (Fig. 6). Recent work suggeststhat promoter methylation reduces gene transcription, where-as gene body methylation increases transcription (40–42).Thus, as a hypothesis generating exercise in the absence ofexpression data for these genes, methylation of CpG sites ingene promoters was interpreted as reducing gene transcrip-tion, whereas methylation of gene body CpGs was interpretedas increasing transcription. With this interpretation, we positthat despite almost half of the metastatic tumors exhibitingheterozygous deletion of CYP17A1, a gene critical to androgensynthesis and the target of multiple inhibitors currently inclinical trials (43, 44), tumors are nonetheless able to upregu-late CYP17A1 through methylation of CpG sites in the genebody. Resistance to CYP17A1 inhibitors may be epigeneticallymediated, and this clinically suggests that resistance toCYP17A1 inhibitors could be attenuated through the use ofhypomethylating agents.
This genomic study, which to the best of our knowledgeincludes the most comprehensive methylation analysis of
metastatic CRPC, presents evidence of specific pathway bio-markers that may be useful for assessment of prognosis andstratification for therapy if validated in larger clinical studysets. Furthermore, these observations suggest that the appli-cation of agents targeting genes both structurally and epige-netically altered may delay the progression of castration-resistant disease.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Acknowledgments
The authors thank Ravi Nagarajan for assistance with methylation experi-ments, and Catherine Burke for gene mapping.
Grant Support
The work received support from UCSF REAC Career Award (P.L. Paris), UCSFFrank Landy Fund (T.W. Friedlander/C.J. Ryan), and UCSF Bernard SchwartzFund (T.W. Friedlander).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicate thisfact.
Received June 23, 2011; revised November 16, 2011; accepted November 17,2011; published OnlineFirst December 7, 2011.
References1. Jemal A, Murray T, Samuels A, Ghafoor A, Ward E, Thun MJ. Cancer
statistics, 2003. CA Cancer J Clin 2003;53:5–26.2. Rubin MA, Putzi M, Mucci N, Smith DC, Wojno K, Korenchuk S, et al.
Rapid ("warm") autopsy study for procurement of metastatic prostatecancer. Clin Cancer Res 2000;6:1038–45.
3. Roudier MP, True LD, Higano CS, Vesselle H, Ellis W, Lange P, et al.Phenotypic heterogeneity of end-stage prostate carcinomametastaticto bone. Hum Pathol 2003;34:646–53.
4. Embuscado EE, Laheru D, Ricci F, Yun KJ, deBoomWitzel S, Seigel A,et al. Immortalizing the complexity of cancer metastasis: geneticfeatures of lethal metastatic pancreatic cancer obtained from rapidautopsy. Cancer Biol Ther 2005;4:548–54.
5. Hu R, Dunn TA, Wei S, Isharwal S, Veltri RW, Humphreys E, et al.Ligand-independent androgen receptor variants derived from splicingof cryptic exons signify hormone-refractory prostate cancer. CancerRes 2009;69:16–22.
6. Tamura K, Furihata M, Tsunoda T, Ashida S, Takata R, Obara W, et al.Molecular features of hormone-refractory prostate cancer cells bygenome-widegeneexpressionprofiles.CancerRes 2007;67:5117–25.
7. Liu W, Laitinen S, Khan S, Vihinen M, Kowalski J, Yu G, et al. Copynumber analysis indicates monoclonal origin of lethal metastaticprostate cancer. Nat Med 2009;15:559–65.
8. Taylor BS, Schultz N, Hieronymus H, Gopalan A, Xiao Y, Carver BS,et al. Integrative genomic profiling of human prostate cancer. CancerCell 2010;18:11–22.
9. StanbroughM, Bubley GJ, Ross K, Golub TR, Rubin MA, Penning TM,et al. Increased expression of genes converting adrenal androgens totestosterone in androgen-independent prostate cancer. Cancer Res2006;66:2815–25.
10. Montgomery RB, Mostaghel EA, Vessella R, Hess DL, Kalhorn TF,Higano CS, et al. Maintenance of intratumoral androgens inmetastaticprostate cancer: a mechanism for castration-resistant tumor growth.Cancer Res 2008;68:4447–54.
11. Mostaghel EA, Nelson PS. Intracrine androgenmetabolism in prostatecancer progression: mechanisms of castration resistance and thera-peutic implications. Best Pract Res Clin Endocrinol Metab 2008;22:243–58.
12. Cottrell S, JungK, KristiansenG, Eltze E, SemjonowA, IttmannM, et al.Discovery and validation of 3 novel DNA methylation markers ofprostate cancer prognosis. J Urol 2007;177:1753–8.
13. Eisen MB, Spellman PT, Brown PO, Botstein D. Cluster analysis anddisplay of genome-wide expression patterns. ProcNatl Acad Sci USA1998;95:14863–8.
14. Hartigan JA. Clustering algorithms. New York; Toronto: Wiley, 1975:xiii, 351.
15. Database of Genomic Variants [database on the Internet] Toronto: TheCentre for Applied Genomics. c1999 [cited September 19th].
16. Oncomine [database on the Internet] Ann Arbor: Compendia Biosci-ence. c2007–2011 [cited November 14th].
17. Tomlins SA, Rhodes DR, Yu J, Varambally S, Mehra R, Perner S, et al.The role of SPINK1 in ETS rearrangement-negative prostate cancers.Cancer Cell 2008;13:519–28.
18. Thomas PD, Kejariwal A, Campbell MJ, Mi H, Diemer K, Guo N, et al.PANTHER: a browsable database of gene products organized bybiological function, using curated protein family and subfamily clas-sification. Nucleic Acids Res 2003;31:334–41.
19. Mi H, Dong Q, Muruganujan A, Gaudet P, Lewis S, Thomas PD.PANTHER version 7: improved phylogenetic trees, orthologs andcollaboration with the Gene Ontology Consortium. Nucleic Acids Res2010;38:D204–10.
20. Panther Classification System [database on the Internet] LosAngeles (CA): The University of Southern California. c2010 [citedOctober 7th]. Available from: http://www.pantherdb.org.
21. Thomas PD, Campbell MJ, Kejariwal A, Mi H, Karlak B, Daverman R,et al. PANTHER: a library of protein families and subfamilies indexedbyfunction. Genome Res 2003;13:2129–41.
Friedlander et al.
Cancer Res; 72(3) February 1, 2012 Cancer Research624
on May 13, 2018. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2011; DOI: 10.1158/0008-5472.CAN-11-2079

22. Olshen AB, Venkatraman ES, Lucito R, Wigler M. Circular binarysegmentation for the analysis of array-based DNA copy number data.Biostatistics 2004;5:557–72.
23. Smyth G. (ed.) Limma: linear models for microarray data. New York,NY: Springer, 2005:13–32.
24. Gentleman RC, Carey VJ, Bates DM, Bolstad B, Dettling M, Dudoit S,et al. Bioconductor: open software development for computationalbiology and bioinformatics. Genome Biol 2004;5:R80.
25. Storey J. The positive false discovery rate: a Bayesian interpretationand the q-value. Ann Stat 2003;31:2013–35.
26. Barrett T, Suzek TO, Troup DB, Wilhite SE, Ngau WC, Ledoux P, et al.NCBI GEO: mining millions of expression profiles–database and tools.Nucleic Acids Res 2005;33:D562–6.
27. Heemers HV, Tindall DJ. Androgen receptor (AR) coregulators: adiversity of functions converging on and regulating the AR transcrip-tional complex. Endocr Rev 2007;28:778–808.
28. Bibikova M, Le J, Barnes B, Saedinia-Melnyk S, Zhou L, Shen R, et al.Genome-wide DNA methylation profiling using Infinium assay. Epige-nomics 2009;1:177–200.
29. Mehra R, Tomlins SA, Yu J, Cao X, Wang L, Menon A, et al. Charac-terization of TMPRSS2-ETS gene aberrations in androgen-indepen-dent metastatic prostate cancer. Cancer Res 2008;68:3584–90.
30. Paris PL, Sridharan S, Scheffer A, Tsalenko A, Bruhn L, Collins C. Highresolution oligonucleotide CGH using DNA from archived prostatetissue. Prostate 2007;67:1447–55.
31. SaramakiOR,PorkkaKP,VessellaRL,Visakorpi T.Genetic aberrationsin prostate cancer by microarray analysis. Int J Cancer 2006;119:1322–9.
32. Lim J, Ghadessy FJ, Abdullah AA, Pinsky L, TrifiroM, Yong EL. Humanandrogen receptor mutation disrupts ternary interactions betweenligand, receptor domains, and the coactivator TIF2 (transcriptionintermediary factor 2). Mol Endocrinol 2000;14:1187–97.
33. Paris PL, Andaya A, Fridlyand J, Jain AN, Weinberg V, Kowbel D, et al.Whole genome scanning identifies genotypes associated with recur-rence and metastasis in prostate tumors. Hum Mol Genet 2004;13:1303–13.
34. Powzaniuk M, McElwee-Witmer S, Vogel RL, Hayami T, RutledgeSJ, Chen F, et al. The LATS2/KPM tumor suppressor is a negativeregulator of the androgen receptor. Mol Endocrinol 2004;18:2011–23.
35. Huang SM, Stallcup MR. Mouse Zac1, a transcriptional coactivatorand repressor for nuclear receptors. Mol Cell Biol 2000;20:1855–67.
36. Gelmann EP. Molecular biology of the androgen receptor. J Clin Oncol2002;20:3001–15.
37. Rauch T, Wang Z, Zhang X, Zhong X, Wu X, Lau SK, et al. Homeoboxgenemethylation in lung cancer studied bygenome-wide analysiswitha microarray-based methylated CpG island recovery assay. Proc NatlAcad Sci U S A 2007;104:5527–32.
38. Majumder PK, SellersWR. Akt-regulated pathways in prostate cancer.Oncogene 2005;24:7465–74.
39. Borgono CA, Diamandis EP. The emerging roles of human tissuekallikreins in cancer. Nat Rev Cancer 2004;4:876–90.
40. Costello JF, Futscher BW, Tano K, Graunke DM, Pieper RO. Gradedmethylation in the promoter and body of the O6-methylguanine DNAmethyltransferase (MGMT) gene correlates with MGMT expression inhuman glioma cells. J Biol Chem 1994;269:17228–37.
41. Maunakea AK, Nagarajan RP, Bilenky M, Ballinger TJ, D'Souza C,Fouse SD, et al. Conserved role of intragenic DNA methylation inregulating alternative promoters. Nature 2010;466:253–57.
42. Murrell A, HeesonS,BowdenL,ConstanciaM,DeanW,KelseyG, et al.An intragenic methylated region in the imprinted Igf2 gene augmentstranscription. EMBO Rep 2001;2:1101–6.
43. RyanCJ, SmithMR, FongL,Rosenberg JE, Kantoff P, RaynaudF, et al.Phase I clinical trial of the CYP17 inhibitor abiraterone acetate dem-onstrating clinical activity in patients with castration-resistant prostatecancer who received prior ketoconazole therapy. J Clin Oncol2010;28:1481–8.
44. Reid AH, Attard G, Danila DC, Oommen NB, Olmos D, Fong PC, et al.Significant and sustained antitumor activity in post-docetaxel, cas-tration-resistant prostate cancer with the CYP17 inhibitor abirateroneacetate. J Clin Oncol 2010;28:1489–95.
Structural and Epigenetic Changes in CRPC
www.aacrjournals.org Cancer Res; 72(3) February 1, 2012 625
on May 13, 2018. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2011; DOI: 10.1158/0008-5472.CAN-11-2079

2012;72:616-625. Published OnlineFirst December 7, 2011.Cancer Res Terence W. Friedlander, Ritu Roy, Scott A. Tomlins, et al. Castration-Resistant Prostate CancerCommon Structural and Epigenetic Changes in the Genome of
Updated version
10.1158/0008-5472.CAN-11-2079doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerres.aacrjournals.org/content/suppl/2011/12/07/0008-5472.CAN-11-2079.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerres.aacrjournals.org/content/72/3/616.full#ref-list-1
This article cites 39 articles, 15 of which you can access for free at:
Citing articles
http://cancerres.aacrjournals.org/content/72/3/616.full#related-urls
This article has been cited by 10 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/72/3/616To request permission to re-use all or part of this article, use this link
on May 13, 2018. © 2012 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2011; DOI: 10.1158/0008-5472.CAN-11-2079