FULL PAPER THERAPEUTIC RESPONSE EVALUATION ON ...
12
FULL PAPER THERAPEUTIC RESPONSE EVALUATION ON HYPERTHYROIDISM USING A FIXED DOSED OF I-131 Yulia Kurniawati, and AHS Kartamihardja Department of Nuclear Medicine, Dr. Hasan Sadikin General Hospital, Faculty of medicine Universitas Padjadjaran, Bandung, Indonesia POSTER PRESENTATION 4 th International Conference on Radiopharmaceutical Therapy New World Hotel, Ho Chi Minh City, Vietnam 28 Nov – 2 Dec 2011
Transcript of FULL PAPER THERAPEUTIC RESPONSE EVALUATION ON ...

FULL PAPER
THERAPEUTIC RESPONSE EVALUATION ON
HYPERTHYROIDISM USING A FIXED DOSED OF I-131
Yulia Kurniawati, and AHS Kartamihardja
Department of Nuclear Medicine, Dr. Hasan Sadikin General Hospital,
Faculty of medicine Universitas Padjadjaran,
Bandung, Indonesia
POSTER PRESENTATION
4th
International Conference on Radiopharmaceutical Therapy
New World Hotel, Ho Chi Minh City, Vietnam
28 Nov – 2 Dec 2011

THERAPEUTIC RESPONSE EVALUATION ON
HYPERTHYROIDISM USING A FIXED DOSED OF I-131
Yulia Kurniawati, and AHS Kartamihardja
Department of Nuclear Medicine, Dr. Hasan Sadikin General Hospital,
Faculty of Medicine Universitas Padjadjaran,
Bandung, Indonesia
Abstract
Introduction.Euthyroidism condition is the ideal expected after treatment of
hyperthyroidism, but there is still no established therapeutical method that can achieve
that condition. Radioactive iodine-131 (131
I) has been used to treat hyperthyroidism for
long time. It is clinically effective, safe, and cost-effective. However, controversy over
the optimum dose of I-131 therapy is still debatable. The aim of this study was to
evaluate the therapeutic response of a fixed dosed I-131 in hyperthyroidism patients.
Material and method. Retrospective study was carried out during January 2010 until
January of 2011. The inclusion criteria were all subjects received I-131 for the first time
with a fixed dose of 8 mCi, diffused and high uptake of Tc-99m. Theraupeutical
response was evaluated based on the patient’s clinical state and or their laboratory
finding3 months after the treatment. Theurapeutical response categorizedgood response
if thyroid hormones within normal limit and/or improvement of clinical state, when
thyroid hormones still high (above normal value ) with improvement of clinical state
was considered as partial response, no respons if there was no changes both on
laboratory finding and clinical state.
Results. There were 127 patients receiving a fixed dose I-131 therapy of 8 mCi during
January 2010 to January 2011. Forty patients did not show a routine examination on
third month.The patients were between 12 to 63 years of age. From the 87 patients,
32(36,78%) were no response, still considered in a hyperthyroid condition, 55 (63.21%)
patients have good responses, which were20 (36.36%) were hypothyroid, 21 (38.18%)
were euthyroid and 14 (25.45%) were partial responses.
Conclusion.Fixed dose I-131 therapyof 8 mCi showed good response in our hospital on
hyperthyroidism, thereforewe can considered as dose of treatment.
Introduction
Hyperthyroidism is a hypermetabolic condition with increased thyroid hormone
production.1,2
Study based on community showed that the incidence of hyperthyroidism
found more in female than male. The prevalence of hyperthyroidism was about 2 % in
female and 0,2% in male.3 A study conducted in UK involving 2.779 people with mean
age was 58 years old showed the incidence of hyperthyroid was 0,8 per 1.000 female
per year.4
The objective of hyperthyroidism treatment is to restore thyroid hormone
level to normal range or euthyroidism.5 Euthyroidism can be achieved by destroyed
thyroid tissue or inhibite synthesis and release of thyroid hormone.1 Destroying thyroid
tissue could be done by surgery or radioiodine ablation and inhibition of synthesis and
release thyroid hormone can be achieved by oral antithyroid drug.1, 2, 6, 7
Recurence hyperthyroid was observed in 34% patients treated with oral anti
thyroid drug. This is the highest among the other treatment modalities. Recurrence
hyperthyroidism after treatment by using I-131 ablation and surgery were 21% and 8%
respectively.8 I-131 now is considered to be drug of choice or second linetreatment
after oral antithyroid drugfor hyperthyroidism patients. However, the optimum dose of
I-131 therapy is still controversy. Until now there was no agreement on dose given for

hyperthyroidism. The dose of I-131 could be given as fixed dose 5-15 mCi based on
empirical study or calculated dose.7,9,10
Calculated dose usually depend on weight of
thyroid gland and I-131 uptake ability of thyroid gland.10,11
The aim of this study was to
evaluate the therapeutic response of a fixed dosed I-131 in hyperthyroidism patients.
Material and method
Retrospective study was carried out during January 2010 until January of 2011 in
Department of Nuclear Medicine, Dr. Hasan Sadikin General Hospital.
Hyperthyroidism patient with diffuse and high uptake thyroid on 99m
Tc- pertechnetate
thyroid scintigraphy were included in this study. Subject was received a single fixed
dose of 8 mCi I-131 for the first time. Therapeutical response was evaluated based on
the patient’s clinical state and or their laboratory finding 3 months after the treatment.
Theurapeutical response categorized as good response is considered if thyroid
hormones within normal limit and/or improvement of clinical state, when thyroid
hormones still high (above normal value) with improvement of clinical state was
considered as partial response, and no respons if there was no changes both on
laboratory finding and clinical state.
Results
Subjects were 127 hyperthyroid patients who received a fixed therapeutic dose of
8 mCi I-131 during period of January 2010 to January 2011 were included in this study.
Out of 127 subjects, 40 subjects were excluded in this study, since they did not show on
the day of a routine follow up 3 months after ablation. Subject who fulfill the study
procedure were 84 consist of 57 female and 27 male. The ages of subject was between
12 to 63 years old (X=36.38 yrs). Subject with history of taking antithyroid drug prior
to radioiodine ablation was 49 (58.33%) and rest of them had no history of taking
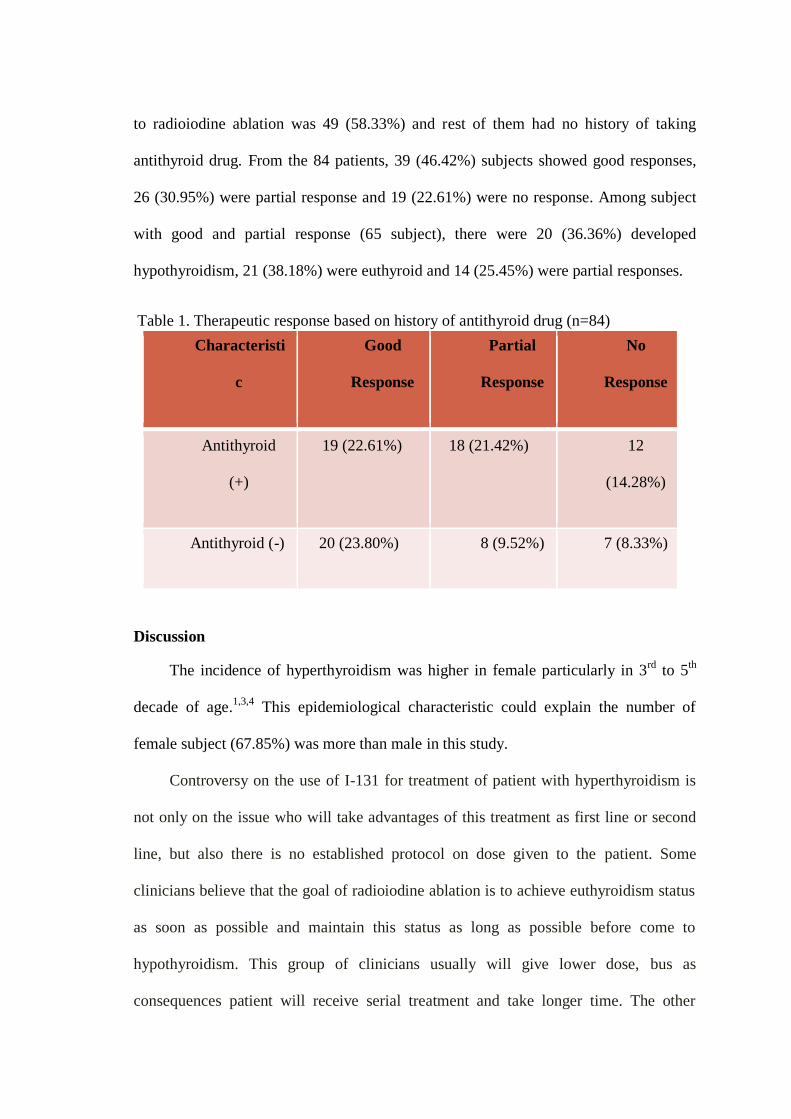
antithyroid drug. From the 84 patients, 39 (46.42%) subjects showed good responses,
26 (30.95%) were partial response and 19 (22.61%) were no response. Among subject
with good and partial response (65 subject), there were 20 (36.36%) developed
hypothyroidism, 21 (38.18%) were euthyroid and 14 (25.45%) were partial responses.
Table 1. Therapeutic response based on history of antithyroid drug (n=84)
Characteristi
c
Good
Response
Partial
Response
No
Response
Antithyroid
(+)
19 (22.61%) 18 (21.42%) 12
(14.28%)
Antithyroid (-) 20 (23.80%) 8 (9.52%) 7 (8.33%)
Discussion
The incidence of hyperthyroidism was higher in female particularly in 3rd
to 5th
decade of age.1,3,4
This epidemiological characteristic could explain the number of
female subject (67.85%) was more than male in this study.
Controversy on the use of I-131 for treatment of patient with hyperthyroidism is
not only on the issue who will take advantages of this treatment as first line or second
line, but also there is no established protocol on dose given to the patient. Some
clinicians believe that the goal of radioiodine ablation is to achieve euthyroidism status
as soon as possible and maintain this status as long as possible before come to
hypothyroidism. This group of clinicians usually will give lower dose, bus as
consequences patient will receive serial treatment and take longer time. The other

groups of clinicians believe that all hyperthyroidism patients, particularly grave’s
disease will end with hypothyroidism and the management of hypothyroidism is more
simple and less complication. Due to these reasons, the goal of radioiodine ablation is
to reach hypothyroidism status by using high dose of I-131.5,7
Theoritically, calculated dose is the best choice to treat hyperthyroid, but in fact
calculated dose applied in many department based on weight and thyroid uptatke was
not sufficient. This condition due to the effetiveness of I-131 on hyperthyroid patients
was also influenced by many factors such age, gender, ethnic and history of smoking.
Anti thyroid drug taken prior to radioiodine therapy also could interferen the efficacy of
treatment.1 Due to this situation many center of nuclear medicine used fixed dose of I-
131 ranged 8-15 mCi.1,5,12,13,14
The result from this study showed good and partial response was obseved in 55
(65.47%) subjects. Similar study was done in Bangladesh using fixed dose 8-15 mCi
and the result was 82%,15
This better results could be due to several patients were
recieved higher dose from 8 mCi. The higher the dose of I-131, the faster the
hypothyroidism achieved.1,14
This result was support by other study done in India. The
effectiveness of radioiodine ablation using fixed dose of 5 mCi was less than 59,37%
and in the dose of 10 mCi the effectiveness was 91,22%.14
From 84 subjects, 65
(77.39%) subjects showed good responses and 19 (22.61%) were no response. Among
subject with good and partial response, there were 20 (36.36%) developed
hypothyroidism, 21 (38.18%) were euthyroid and 14 (25.45%) were partial responses.
Leslie et al conclude that fixed dose regimen is simple and as effective as calculated
ones for treatment hyperthyroidism, but they still do not define the ideal fixed dose to
prescribe.11
Subject with history of taking antithyroid drug prior to radioiodine ablation was
49 (58.33%) and rest of them had no history of taking antithyroid drug.1
Although the
impact of preceding antithyroid drug on the outcome of I131
is still debatable, our data
suggest that the drug can reduces the therapeutic efficacy.
Conclusion
Fixed dose I-131 therapy of 8 mCi showed good response in 3 month follow up
for the treatment of hyperthyroidism. Anti thyroid drugs may be a factor that can
reduces efficacy of I-131 on the treatmen of hyperthyroidism.
Referrences
1. Meier. DA, Dworkin. HJ, Bender. JM. Therapy for Hyperthyroidism. In: Henkin.
RE, Bova. D, Dillehay. GL, Halama. JR, Karesh SM, Wagner RH, et al., editors.
Nuclear Medicine. 2nd ed. Pennsylvania: MOSBY elsevier; 2006. p. 1567-75
2. Cooper. DS, Greenspans. FS, Gardner. DG, Ladenson. PW. The Thyroid Gland.
Basic & Clinical Endocrinology. 7th ed. New York: McGraw-Hill; 2004. p. 209-
78.
3. Reid JR, Wheeler SF. Hyperthyroidism: diagnosis and treatment. Am Fam
Physician. 2005 Aug 15;72(4):623-30.
4. Vanderpump MP, Tunbridge WM, French JM, Appleton D, Bates D, Clark F, et al.
The incidence of thyroid disorders in the community: a twenty-year follow-up of
the Whickham Survey. Clin Endocrinol (Oxf). 1995 Jul;43(1):55-68.
5. Jones. RE, Huether. SE. Alteration of Hormonal Regulation. In: McCance. KL,
Huether. SE, editors. Pathophysiology : The biologic Basic for Disease in Adults
and Children. 5th ed. Pennsylvania: Elsevier Mosby; 2006. p. 692-4.

6. Jamerson. JL, Weetman. AP. Disorders of The Thyroid Gland. In: Kasper. DL,
Braunwald. E, Fauci. AS, Hauser. SL, Longo. DL, Jamerson. JL, editors.
Harisson's Principles of Internal Medicine. 16th ed. New York: McGraw-Hill;
2005. p. 2113-7.
7. Weetman AP. Graves' disease. N Engl J Med. 2000 Oct 26;343(17):1236-48.
8. Torring O, Tallstedt L, Wallin G, Lundell G, Ljunggren JG, Taube A, et al. Graves'
hyperthyroidism: treatment with antithyroid drugs, surgery, or radioiodine--a
prospective, randomized study. Thyroid Study Group. J Clin Endocrinol Metab.
1996 Aug;81(8):2986-93.
9. Klein I, Becker DV, Levey GS. Treatment of hyperthyroid disease. Ann Intern
Med. 1994 Aug 15;121(4):281-8.
10. Iagaru A, McDougall IR. Treatment of thyrotoxicosis. J Nucl Med. 2007
Mar;48(3):379-89
11. Leslie WD, Ward L, Salamon EA, Ludwig S, Rowe RC, Cowden EA. A
randomized comparison of radioiodine doses in Graves' hyperthyroidism. J Clin
Endocrinol Metab. 2003 Mar;88(3):978-83
12. Moore. KL, Dalley. AF. Neck. Clinically Oriented Anatomy. 5th ed. Baltimore:
Lippincott Williams & Wilkins; 2006. p. 1083-7.
13. Singer PA, Cooper DS, Levy EG, Ladenson PW, Braverman LE, Daniels G, et al.
Treatment guidelines for patients with hyperthyroidism and hypothyroidism.
Standards of Care Committee, American Thyroid Association. JAMA. 1995 Mar
8;273(10):808-12.
14. Khan S, Namgyal P, Ahmad M, Wani T. Optimizing a Single Fixed Dose of Iodine
- 131 in theTreatment of Graves' Disease: Experience From an Endemic Iodine

Deficiency Goiter Belt in the Himalayan Valley of Kashmir, India. World J Nucl
Med. 2006;5:109-14.
15. Akter R, Hossain S, Reza S, Afroz S. Outcome of Radioiodine (I-131) Therapy in
Primary Thyrotoxicosis in Young (21-40) Bangladeshi Population - A 10 years
study in 482 patient. World J Nucl Med. 2008;7(2):100-3.