Officer-involved deaths on rise, no officers charged since 2000

From Research to Practice:Postgraduate Training Course in Chronic Disease
Geneva 2004
Primary prevention:Primary prevention:TobaccoTobacco
Carmen AuderaCarmen AuderaTobacco Free Initiative, WHOTobacco Free Initiative, WHO--HQHQ

Today, in the world,Today, in the world,
48% of men and 12% of 48% of men and 12% of
women smokewomen smoke
1.2 billion smokers worldwide, 800 million in developing countries … and growing

Why is tobacco a public health Why is tobacco a public health problem?problem?
1. Kills and causes disesases2. Contributes to poverty3. Is a growing epidemic4. Has a negative effect on the environment

Tobacco Products: Smoking Tobacco
CigarettesCigarettes–– manufacturedmanufactured–– hand rolledhand rolled–– bidisbidis–– kretekskreteksPipesPipesCigarsCigars

Tobacco Products: Bidis or Beedis
US
Cen
ters
for D
isea
se C
ontr
ol,
Offi
ce o
n Sm
okin
g an
d H
ealth
Widely used in IndiaNow popular among young people in the USMarketed as a ‘natural cigarette’Shaped like a hand-rolled cigaretteAvailable in a variety of scents that hide the harsh taste of tobaccoUnfiltered and delivershigh yields of tar andnicotine

Tobacco Products: Kreteks (Clove cigarettes)
Made in IndonesiaMade in IndonesiaMarketed as a Marketed as a ‘‘luxury for the young and luxury for the young and trendytrendy’’Major brands include: Major brands include: –– DjarumDjarum–– GudanGudan GaramGaram–– BentoelBentoel–– SampoernaSampoerna

Tobacco Products: Cigars
Pan
Am
eric
an H
ealth
Org
aniz
atio
n
Any roll of tobacco wrapped in leaf tobacco or in Any roll of tobacco wrapped in leaf tobacco or in any substance containing tobacco any substance containing tobacco Made of airMade of air--cured tobaccocured tobaccoDelivers more CODelivers more COper gram of tobacco burned per gram of tobacco burned than a regular cigarettethan a regular cigaretteIn the 1990s cigar use becameIn the 1990s cigar use became‘‘fashionablefashionable’’ in manyin manydeveloped countriesdeveloped countries

Tobacco Products: Smokeless tobacco
Chewing tobacco– looseleaf– plug– twist
Snuff– moist– dry
RM
Dav
is, M
.D.

Per Capita Consumption of Different Forms of Tobacco in the US, 1880–1995
US Department of Agriculture, 1996
14
1880 1890 1900 1910 1920 1930 1940 1950 1960 1970 1980
Year
12
10
8
6
4
2
01990
Cigarettes
Snuff
ChewingTobacco
Pipe/Roll-your-own
Cigars
Per C
apita
Con
sum
ptio
n

1. Kills and causes disesases
It kills one in every 10 adults worldwide. In 2002 aproximately 4,83 million people died due to tobacco related diseases. It is estimated that by 2020, tobacco will be responsible for 10 million deaths per year.

Deaths in 2000 attributable to selected risk factors 2000Developed Countries - World Health Report 2002
0 500 1000 1500 2000 2500 3000
Carcinogenos ocupacionales
Lead exposure
Urban air pollution
Alcohol
Lack of physical activityInactividad fisica
Poor fruit and vegetalble intake
High body mass index
Cholesterol
Tobacco
Blood Pressure
Number of deaths (000s)

Deaths in 2000 attributable to selected risk factors 2000High mortality developping countries - World Health Report 2002
0 500 1000 1500 2000 2500 3000 3500
Vitamin A deficit
Zinc Deficit
Deficient intake of fruits andvegetables
Indoor Air Contaminants
Tobacco
Cholesterol
Unsafe water
Presion arterial
Unsafe sex
Low weight
Number of deaths (000s)

Deaths in 2000 attributable to selected risk factors 2000Low mortality developping countries - World Health Report 2002
0 500 1000 1500 2000 2500
Low weight
Urban air pollution
Physical inactivity
Indoor smoke from solid fuels
High Body mass index
Poor fruit and vegetable intake
Alcohol
Cholesterol
Tobacco
Blood Pressure
Number of deaths

It is estimated that 70% of deaths in 2020 due to tobacco will be in people from developing countries.

Percentage of total number of deaths attributable to TOBACCO use by WHO Regions, 2000
1. Kills and causes disesases
0
2
4
6
8
10
12
14
16
18
20
af rica america east med europe southeast asia
w esternpacif ic
Source: WHR, 2002

1. Kills and causes disesases
Diseases:Drug dependency- causes addiction
CancerOral, pharynx, larynx, esophagus, lung, kidney, ureter and bladder
Other chronic diseases- Stroke- Coronary heart disease- Aortic aneurysm- Atherosclerotic peripheral vascular disease- Chronic obstructive pulmonary disease (COPD

Every day about 100,000 young people around the world become addicted to tobacco
In high-income countries, 15,000 youth become addicted to tobacco every day.
In middle- and low-income countries: 84,000 youth become addicted to tobacco every day.

Risk factors as % of DALYs in high mortalitydeveloping countries
0 2 4 6 8 10 12 14 16
Colesterol
Tabaco
Presion arterial
Deficiencia Vitamina A
Deficiencia de Hierro
Deficiencia de zinc
Humo interir decarburantes solidos
Agua e higiene deficientes
Sexo no seguro
Bajo peso
Fuente:Datos obtenidos del World Health Report 2002-OMS

Risk factors as % of DALYs in low mortalitydeveloping countries
0 2 4 6 8
Agua e higiene deficientes
Deficiencia de Hierro
Humo interior de carburantes solidos
Consumo deficiente de frutas y verduras
Colesterol
Sobrepeso
Bajo peso
Tabaco
Presion arterial
Alcohol
Fuente:Datos obtenidos del World Health Report 2002-OMS
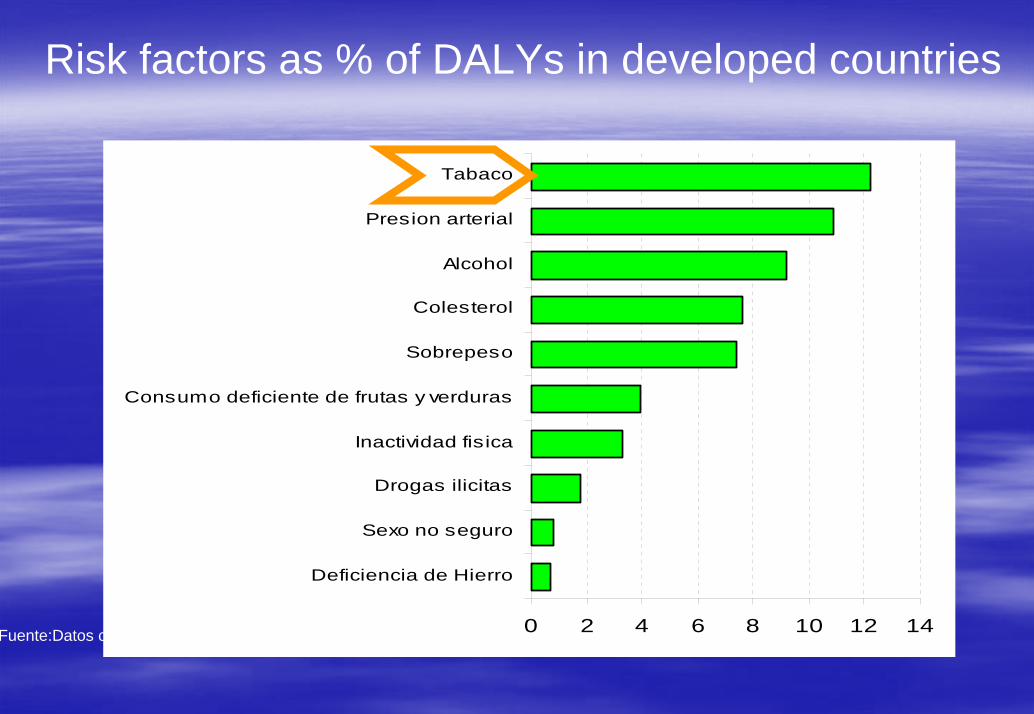
Risk factors as % of DALYs in developed countries
0 2 4 6 8 10 12 14
Deficiencia de Hierro
Sexo no seguro
Drogas ilicitas
Inactividad fisica
Consumo deficiente de frutas y verduras
Sobrepeso
Colesterol
Alcohol
Presion arterial
Tabaco
Fuente:Datos obtenidos del World Health Report 2002-OMS

Percentage of total number of DALYs attributable to TOBACCO use by WHO Regions, 2000
0
2
4
6
8
10
12
14
africa america east med europe southeast asia
westernpacific
Source: WHR, 2002

1. Kills and causes disesases
Passive Smokers
• Pasive smoker is the person exposed to second handtobacco smoke.
• There is scientificic evidence of a 30% increased risk ofsuffering lung cancer (20% in women and 30% in men) in people living or working with smokers.
• There is a 25 to 35% increased risk of suffering an acutecoronary heart disease and an increased risk ofpresenting chronic respiratory conditions

Spousal smoking and lung cancer: women (combined)
RR (95% CI) in lifelong nonsmokers – smoking vs nonsmoking spouse
0.1
1
10
Rel
ativ
e ris
k
Hackshaw et al. BMJ 315:980-88; 1997.

ETS and Coronary Heart Disease: metaETS and Coronary Heart Disease: meta--analysisanalysis
Exposure Exposure Pooled RR* Pooled RR* (95% CI)(95% CI)
ETS (smoking spouse)ETS (smoking spouse) 1.3 1.3 (1.2(1.2––1.4)1.4)
Active smoking:Active smoking:1 cig/day1 cig/day 1.41.4 (1.2(1.2––1.6)1.6)
20 cig/day 20 cig/day 1.81.8 (1.3(1.3––2.4)2.4)
** risk estimates apply to an average age at death of 65risk estimates apply to an average age at death of 65 yearsyears
Law et al., 1997.

Health effects of SHTS exposure in children
♦♦ SuddenSudden InfantInfant DeathDeath SyndromeSyndrome (SIDS)(SIDS)♦♦ AcuteAcute respiratoryrespiratory illnessesillnesses♦♦ ChronicChronic respiratoryrespiratory symptomssymptoms♦♦ AsthmaAsthma andand exacerbationexacerbation ofof asthmaasthma symptomssymptoms♦♦ ChronicChronic middlemiddle earear diseasedisease
WHO estimates that nearly 700 million, or almost half of WHO estimates that nearly 700 million, or almost half of the worldthe world’’s children, breathe air polluted by tobacco s children, breathe air polluted by tobacco smoke, particularly at home.smoke, particularly at home.

Maternal smoking and SIDS: Maternal smoking and SIDS: New Zealand caseNew Zealand case--control studycontrol study
10 *reference category for no smoking = 1
1.9
2.6
5.1
Odd
s ra
tio*
11–9 cig/day 10–19 cig/day ≥ 20 cig/day
Maternal smoking during last two weeks
DoseDose––response relationship:response relationship:Increasing maternal smoking leads to increasing Increasing maternal smoking leads to increasing frequency of SIDSfrequency of SIDS
Mitchell et al, 1991.

ETS and ARI: Shanghai cohort study
Chen et al. Int J Epidemiol 1998;17: 348– 355.With permission from Oxford University Press.
Incidence density
(per year)
1.001.00
1.001.001.00
1.00
2.30
1.141.21
2.63
1.911.33
2.96
1.551.50
4.80
1.97
1.75
0
5
10
15
20
25
30
35
40
45
Male Female <3.0 kg >3.0 kg Breast Artificial
None1–19 cigs/day≥20 cigs/day
Hospitalization for respiratory illnesses vs family cigarette consumption
• Index of exposure = paternal and other family members smoking• Significant dose–response relationship between passive smoke exposure and
hospitalizations for respiratory illness
Sex Weight Feeding

Why is tobacco a public health Why is tobacco a public health problem?problem?
1. Kills and causes disesases2. Contributes to poverty3. Is a growing epidemic4. Has a negative effect on the environment

2. Contributes to poverty
Tobacco and Poverty: A vicious circleA vicious circleThe poor are the ones The poor are the ones who smoke the mostwho smoke the mostTobacco worsens Tobacco worsens poverty among its users: poverty among its users: money spent on tobaccomoney spent on tobacco

2. Contributes to poverty
The poor are the ones who smoke the mostThe poor are the ones who smoke the most
6 4 %5 8 %
4 2 %
2 1 %
0 %
2 0 %
4 0 %
6 0 %
I l l i t e r a t e < 6 y e a r s 6 - 1 2y e a r s
> 1 2y e a r s
L e n g t h o f s c h o o l i n g
Smok
ing
prev
alen
ce
Source:Source: GajalakshmiGajalakshmi, , JhaJha et al 1997et al 1997
Smoking prevalence in Smoking prevalence in ChennaiChennai, India (, India (bidisbidis and cigarettes)and cigarettes)

2. Contributes to poverty
Eggs? Where will the money come from to buy them?”--Dhaka rickshaw puller who could feed each of his three children an egg a day if hebought eggs instead of tobacco
At individual level
•Expenditure on tobacco can be a high percentage of household income
• Loss of family income due to ill health and premature death
• Health care expenses

Tobacco use is increasing among those least able to afford it2. Contributes to poverty
In Bangladesh, the poorest citizens are twice as likely to smoke as the wealthiest citizens. (D. Efroymson et al, 2001) The price of 20 imported cigarettes could buy: 6 kg of rice in Bangladesh
Low income households with at least one smoker in Bulgaria spent 10.4% of their total income on tobacco products in 1995 (Sayginsoy Ö et al, 2000).
In China, smokers in 2716 householdssurveyed in the Minhang district reported spending 17% of household income on cigarettes (Gong LY et al. 2000)

2. Contributes to poverty
At the national level,- huge economic losses due to high health care costs
- lost productivity due to tobacco-related illnesses and premature deaths.
- Since most countries are net importers of tobacco leaf and tobacco products, they lose millions of dollars a year in precious foreign exchange.
In short, tobacco’s contributions to the economy are outweighed by its costs to households, to public health, to the environment and to national economies.

2. Contributes to poverty
Tobacco farmers make minimal profits, compared to the industry.
Tobacco farming is labour intensive and requires costly inputs such as fertilizers and pesticides. In Brazil, officials were predicting that, in 1998, 35% of tobacco growers would finish the harvest owing more money to the tobacco companies than they earned. (Campaign for Tobacco Free Kids)

Child labour is linked to tobacco production
In Brazil, 520,000 children under 18 years of age work on tobacco farms, 32% of them are younger than 14.
Children are directly exposed to a cocktail of highly toxic agro-chemicals. In addition, children who pick tobacco can end up with a type of nicotine poisoning caused by absorption of nicotine through the skin.

Why is tobacco a public health Why is tobacco a public health problem?problem?
1. Kills and causes disesases2. Contributes to poverty3. Is a growing epidemic4. Has a negative effect on the environment

Tobacco epidemic
Tobacco has been used for centuries in many societiesTobacco has been used for centuries in many societies
Tobacco industrialisationTobacco industrialisation
Economic interestsEconomic interests
Marketing strategiesMarketing strategies
Increase in prevalenceIncrease in prevalence
Tobacco epidemicTobacco epidemic

3. Is a growing epidemicAdult per capita tobacco consumption patterns
0
500
1000
1500
2000
2500
3000
3500
1970-72 1980-82 1990-92
ciga
rette
s/ye
ar p
er a
dult
Less developedDevelopedTotal
Tobacco consumption is growing world wide because of increasing consumption in developing countries

Dissemination of Smoking Behaviour and its Effects on Mortality: The four stages of the epidemic
Prevalence of adult daily smoking (%)
Smoking-relateddeaths (% of all deaths by sex)
Stage 4Stage 1 Stage 2 Stage 3
Male prevalenceMale deaths
Female prevalence
80
60
40
20
00 10 20 30 40 50 60 70 80 90 100
0
10
20
30
40
Time from start of male smoking (years)
Female deaths
Lopez, Collislaw and Piha, 1994

The epidemic is moving from The epidemic is moving from the men in developed the men in developed countries to women in countries to women in developed countries and to developed countries and to men and women in men and women in developing countries . developing countries .

Tobacco consumption prevalence in different Tobacco consumption prevalence in different countries of the worldcountries of the world
Men Women Total Year
China 53,4% 4,0% 28.9% 1998
Korea 64,8% 5,5% 35.0% 1996
India 29,4% 2,5% 16.0% 1999
Côte d’Ivoire 42,3% 1,8% 24.4% 1997
Chile 44,1% 33,6% 40,0% 2001
United Kingdom 28,0% 26,0% 27.0% 2001
United States 25,7% 21,0% 23.3% 2000
Source: Tobacco Control Country Profiles-2003

Why is tobacco a public health Why is tobacco a public health problem?problem?
1. Kills and causes disesases2. Contributes to poverty3. Is a growing epidemic4. Has a negative effect on the environment

Deforestation is related to tobacco production
4. Has a negative effect on the environment
In developing countries, wood is often used as fuel to cure tobacco leaves. An estimated 200,000 hectares (or 2,000 square kilometres) of forests and woodlands are removed each year because of tobacco farming. (Geist, 1999)

And if we are aware of all this, why do people continue to smoke?
There are two main reasons:
1.Tobacco is very addictive
• Nicotine is an addictive substance
• Cigarettes are engineered to make tobacco more addictive

Nicotine
Dopamine
Norepinephrine
Acetylcholine
Vasopressin
Serotonin
Beta-endorphin
Pleasure, appetite suppressionArousal, appetite suppression
Arousal, cognitive enhancement
Memory improvement
Mood modulation, appetite suppressionReduction of anxiety and tension

And if we are aware of all this, why do people continue to smoke?
2. The tobacco Industry

Tobacco dependence as an infectious diseaseTobacco dependence as an infectious disease
Tobacco Industry (vector) Tobacco Industry (vector)
Tobacco (Tobacco (infectios infectios agent)agent)
People (hosts) People (hosts)
Si no hubiera que mantener un negocio la epidemia del tabaquismo tendría los días contados
With all the information that we have today, if a business did not have to be maintained, the tobacco
epidemic would soon decline.

Addressing tobacco controlAddressing tobacco control
StrategiesStrategies–– Prevent people from taking up tobacco Prevent people from taking up tobacco
(primary) (primary) –– Promote smoking cessation (secondary)Promote smoking cessation (secondary)–– Protect non smokers from the exposure to Protect non smokers from the exposure to
tobacco smoke (primary)tobacco smoke (primary)–– Regulate tobacco products (risk reduction)Regulate tobacco products (risk reduction)
MeasuresMeasures–– Reduce demandReduce demand–– Reduce supplyReduce supply

Demand side measuresDemand side measuresPrice and tax measuresPrice and tax measuresComprehensive ban and restriction on tobacco Comprehensive ban and restriction on tobacco advertising promotion and sponsorship advertising promotion and sponsorship Protection from exposure to environmental Protection from exposure to environmental tobacco smoketobacco smokeEducation communication, training and public Education communication, training and public awareness awareness Packaging and labelling Packaging and labelling Tobacco dependence cessation measures Tobacco dependence cessation measures Regulation and disclosure of the contents of Regulation and disclosure of the contents of tobacco productstobacco products

Cigarette Price and Consumption in 22 Cigarette Price and Consumption in 22 European CountriesEuropean Countries
HungaryTurkey
FranceUSSR
Romania
Greece
Spain
Portugal
Italy
Netherlands
Belgium
Cz
Iceland
IrelandSwitzerland
Finland
Sweden
Denmark
Norway
GDR GFRUK
Price of 20 cigarettes (US$)
Cig
aret
tes
per a
dult
per y
ear
500
1000
2000
4000
3000
0.3 0.5 0.7 1 2 3 4 5
Townsend, 1998

Impact of Increasing Price on Smoking Among Impact of Increasing Price on Smoking Among Canadian TeenagersCanadian Teenagers
Real cigarette prices and cigarette smoking prevalence among Canadians aged 15–19 years
270
19851984 19861980 1981 1982 198919881987 199019831979
18
212427
30
15
48
39
33
42
36
45
Year
Smok
ing
prev
alen
ce (%
)
Teenage smokingReal tobacco price index 250 R
eal cigarette price index
230
210
190
170
150
130
110
901991
Health and Welfare Canada

Demand side measuresDemand side measures
Comprehensive ban on advertising and Comprehensive ban on advertising and promotionpromotion
A comprehensive advertising ban includes direct and indirect advertising and have a complete ban on:
- Advertising in all media- Advertising in all audiences- Advertising in all locations- Sponsorship or promotion for certain audiences- Sponsorship advertising events- Brand Stretching


Demand side measuresDemand side measuresSmoke free environmentsSmoke free environments
1.1. Improved health of nonImproved health of non--smokers and smokers; smokers and smokers;
2.2. A reduction in the number cigarettes smoked daily by A reduction in the number cigarettes smoked daily by smokers (often a first step to quitting);smokers (often a first step to quitting);
3.3. Increased public awareness about the seriousness of Increased public awareness about the seriousness of exposure to secondexposure to second--hand tobacco smoke; andhand tobacco smoke; and
4.4. The emergence of societies and environments where The emergence of societies and environments where nonnon--smoking is viewed as the norm. smoking is viewed as the norm.

Smoke free places
• Public places:
•public transport
•restaurantes
•bars
•cinemas
•workplaces
•Homes

Information about the effects of tobaccoDemand side measuresDemand side measures
World no World no tobaccotobacco dayday20042004

Campaigns

Strong warning labels on all Strong warning labels on all tobacco productstobacco products

Health Information reduces the demand for cigarettes
Country Time Event Immediate reduction incigarette consumption
UK 1962 1st report of the RoyalCollege of Physicians
5%
Switzerland 1966 An anti-smokingcampaign
11%
Turkey 1982 Implementation of healthwarning labels
8%
Source: Kenkel and Chen, 2000

Behavioural Behavioural –– Counselling Counselling –– Psychological supportPsychological support
PharmacologicalPharmacological–– Nicotine replacementNicotine replacement–– Antidepressants Antidepressants
Demand side measuresDemand side measuresTreatment of tobacco dependencyTreatment of tobacco dependency

NRT and cessation therapiesNRT and cessation therapies
•• NRTs double the effectiveness of cessation efforts NRTs double the effectiveness of cessation efforts and reduce individualsand reduce individuals’’ withdrawal costswithdrawal costs
•• Governments may widen access to NRT and other Governments may widen access to NRT and other cessation therapies by:cessation therapies by:
•• Reducing regulationReducing regulation•• Conducting more studies on costConducting more studies on cost--effectiveness effectiveness
(especially in low/middle income countries)(especially in low/middle income countries)•• Considering NRT subsidies for poorest smokersConsidering NRT subsidies for poorest smokers

Increasing access to Increasing access to treatmenttreatment
Quitting works for lung cancer patients% survived after diagnosed with lung cancer
0
5
10
15
20
25
30
2 years 5 years
quitsmoke
Quitting tobacco at any point in life provides both immediate benefits and substantial long-term benefits to health

Cost effectiveness of demand side measures for allregions including Europe
FromFrom mostmost toto leastleast costcost effectiveeffective::1. 1. TaxationTaxation2. 2. AdvertisingAdvertising bansbans3. 3. EducationEducation andand ComunicationComunication4. 4. CleanClean indoorindoor airair5. 5. NicotineNicotine replacementreplacement treatmenttreatment

Supply side measuresSupply side measures
–– ProhibitionProhibition–– Youth access restrictionsYouth access restrictions–– Crop substitutionCrop substitution–– Trade restrictionsTrade restrictions
–– Control SmugglingControl Smuggling
are not validatedas effectivemeasures
is the only exception and is the key supply-side measure

SmugglingSmuggling control in control in SpainSpain
0
100
200
300
400
500
600
700
800
1 2 3 4 5 60
2
4
6
8
10
12
14
excise renevue fromtobacco sales
Contraband cigarettesas percentage of totalsales
1996 1997 1998 1999 2000 2001
Smuggling was controlled in Spain without reducing the price of tobacco

Who is responsible for tobacco control?Who is responsible for tobacco control?
SocietySociety
Civil society GovernmentsUN and sister organizations

Ministry of Health
Ministry of Trade Ministry of Justice
Governmentalstructures
Parliamentothers
Ministry of Foreign Affairs Ministry of Education
Customs

Human rights groupsHealth professionals
Social justice Consumers groupsEnvironmental
Civil society Religious groupsGender groups
Tobacco control groupsPrivate companies
Others
ConclusionsConclusions• Tobacco consumption is a known risk factor for a number of
diseases
•Tobacco dependence itself is a disease
• It is a growing global epidemic
• Tobacco control measures have proven to be effective
• Tobacco Control is a multisectorial and multiprofessional task
•All the society segments should be involved