From personal reflection to social positioning: the development of a transformational model of...
11
© 2002 Blackwell Science Ltd Nursing Inquiry 2002; 9 (4): 239 – 249 Feature Blackwell Science, Ltd From personal reflection to social positioning: the development of a transformational model of professional education in midwifery Diane Phillips, a Rod Fawns b and Barbara Hayes c a School of Nursing, Faculty of Health and Behavourial Sciences, Deakin University, Burwood, Victoria, b Department of Science and Mathematics Education, The University of Melbourne, Parkville, Victoria, and c School of Nursing Sciences, James Cook University, Townsville, Queensland, Australia Accepted for publication 19 March 2002 PHILLIPS D, FAWNS R and HAYES B. Nursing Inquiry 2002; 9 : 239 – 249 From personal reflection to social positioning: the development of a transformational model of professional education in midwifery A transformational model of professional identity formation, anchored and globalized in workplace conversations, is advanced. Whilst the need to theorize the aims and methods of clinical education has been served by the techno-rational platform of ‘reflective practice’, this platform does not provide an adequate psychological tool to explore the dynamics of social episodes in professional learning and this led us to positioning theory. Positioning theory is one such appropriate tool in which indi- viduals metaphorically locate themselves within discursive action in everyday conversations to do with personal positioning, institutional practices and societal rhetoric. This paper develops the case for researching social episodes in clinical education through professional conversations where midwifery students, in practice settings, are encouraged to account for their moment-by-moment interactions with their preceptors/midwives and university mentors. It is our belief that the reflection elaborated by positioning theory should be considered as the new epistemology for professional education where professional conversations are key to transformative learning processes for persons and institutions. Key words: positioning theory, professional conversations, professional identity formation, reflection. REFLECTION AND COMPETENCE ‘Reflection’ as a purpose arose from a need for a new epistemology of professional practice in the mid-1980s within nursing education. Reflective practice embodied the authority of experience and executive intelligence in the emergent professions of both nursing and midwifery education. It challenged accepted functions of nurse and midwifery education that were embedded in a responsibility to repro- duce a technical class in society that could competently implement predetermined techniques to achieve predeter- mined ends. The burgeoning literature in professional education has held that there is not a universal agreement about the desired ends of professional practice; indeed, such desired ends are often the subject of dispute. The literature points also to the inappropriateness of technical rationality in the rapidly changing, flexible, complex and uncertain world of professional practice to draw emphasis upon pro- fessional knowing arising in action, demonstrated often intuitively in every skilful act. The various components of reflective practice or knowing-in-action are held to be the hallmark of the competent practitioner who is able to apprehend and respond to dynamic and unique situations. Nurses and midwives have long been fascinated by how aspirants acquire the personal and professional skills, traits, Correspondence: Diane Phillips, School of Nursing, Faculty of Health and Behavourial Sciences, Deakin University, 221 Burwood Highway, Burwood, VIC. 3125, Australia. E-mail: <[email protected]>
-
Upload
diane-phillips -
Category
Documents
-
view
212 -
download
0
Transcript of From personal reflection to social positioning: the development of a transformational model of...

© 2002 Blackwell Science Ltd
Nursing Inquiry
2002;
9
(4): 239–249
F e a t u r e
Blackwell Science, Ltd
From personal reflection to socialpositioning: the development of a
transformational model ofprofessional education in midwifery
Diane Phillips,
a
Rod Fawns
b
and Barbara Hayes
c
a
School of Nursing, Faculty of Health and Behavourial Sciences, Deakin University, Burwood, Victoria,
b
Department of Science and Mathematics Education, The University of Melbourne, Parkville, Victoria, and
c
School of Nursing Sciences, James Cook University, Townsville, Queensland, Australia
Accepted for publication 19 March 2002
PHILLIPS D, FAWNS R and HAYES B.
Nursing Inquiry
2002;
9
: 239–249
From personal reflection to social positioning: the development of a transformational model of professional education inmidwifery
A transformational model of professional identity formation, anchored and globalized in workplace conversations, is advanced.Whilst the need to theorize the aims and methods of clinical education has been served by the techno-rational platform of‘reflective practice’, this platform does not provide an adequate psychological tool to explore the dynamics of social episodesin professional learning and this led us to positioning theory. Positioning theory is one such appropriate tool in which indi-viduals metaphorically locate themselves within discursive action in everyday conversations to do with personal positioning,institutional practices and societal rhetoric. This paper develops the case for researching social episodes in clinical educationthrough professional conversations where midwifery students, in practice settings, are encouraged to account for theirmoment-by-moment interactions with their preceptors/midwives and university mentors. It is our belief that the reflectionelaborated by positioning theory should be considered as the new epistemology for professional education where professionalconversations are key to transformative learning processes for persons and institutions.
Key words:
positioning theory, professional conversations, professional identity formation, reflection.
REFLECTION AND COMPETENCE
‘Reflection’ as a purpose arose from a need for a newepistemology of professional practice in the mid-1980s withinnursing education. Reflective practice embodied the authorityof experience and executive intelligence in the emergentprofessions of both nursing and midwifery education. Itchallenged accepted functions of nurse and midwiferyeducation that were embedded in a responsibility to repro-duce a technical class in society that could competently
implement predetermined techniques to achieve predeter-mined ends. The burgeoning literature in professionaleducation has held that there is not a universal agreementabout the desired ends of professional practice; indeed, suchdesired ends are often the subject of dispute. The literaturepoints also to the inappropriateness of technical rationalityin the rapidly changing, flexible, complex and uncertainworld of professional practice to draw emphasis upon pro-fessional knowing arising in action, demonstrated oftenintuitively in every skilful act. The various componentsof reflective practice or knowing-in-action are held to bethe hallmark of the competent practitioner who is able toapprehend and respond to dynamic and unique situations.
Nurses and midwives have long been fascinated by howaspirants acquire the personal and professional skills, traits,
Correspondence: Diane Phillips, School of Nursing, Faculty of Health andBehavourial Sciences, Deakin University, 221 Burwood Highway, Burwood, VIC.3125, Australia.E-mail: <[email protected]>
NIN_145.fm Page 239 Friday, November 15, 2002 9:04 PM

D Phillips et al.
240
© 2002 Blackwell Science Ltd,
Nursing Inquiry
9
(4), 239–249
attitudes and values deemed necessary so that practitionersare judged to be both competent and accountable. Nursingand midwifery embraced the opportunities offered in reflec-tion and incorporated these opportunities in the educationof undergraduate and postgraduate students from the early1990s (Garratt 1992). The notion that reflection could alsoassist the advanced practitioner was also posed in theearly 1990s (Emden 1991; Street 1991) but was slower to beintegrated (Hayes 2000; Taylor 2000). However, as reflectionand reflective practice are inextricably tied to a late twentieth-century rediscovery of the philosophical bases of practicedisciplines, the humanising roots of professions such asmidwifery have fully embraced these notions.
Reflection has come to refer both to the aims and methodsof clinical education. It has been used to describe teachingand learning strategies, which afford tacit appreciation ofthe links between theory and practice, personal professionalidentity formation and institutional or structural transfor-mation. The concept of ‘reflection’ is, however, often usedmetaphorically for ‘thinking’ and often carries loose conno-tations of the meanings and experiences of the ‘professionalrole’. In this paper it is argued that ‘reflective practice’ doesnot provide an adequate psychological tool to explore thedynamics of social episodes in professional learning, and thatthe static and stereotyping nature of role theory is an obstacle.This paper is a plea for ‘the person’ as against ‘the role’ in thetheory of research in nursing education. Positioning theory(Davies and Harré 1990; Harré & van Langenhove 1999a)is a relatively new tool for describing not only a person’sparticipation in the world, through the analysis of the dis-cursive positioning of the person in conversational settingsand, hence, personal identity formation in nursing andmidwifery, but also the transformations that occur withininstitutional settings. This social constructivist focus on theperson, we believe, sets a new agenda for research and teachingin postgraduate midwifery education.
Within midwifery education a range of learning experi-ences have been applied that afford students opportunitiesto engage in either private (individual, on their own) or public(collective, with others) reflection. However, the literatureshows that claims for reflective practice have assumed eithera psychological model of an individual’s employment ofa potent internal dialogue or, more recently, social scienceconstructs of potent social discourses. Through the applica-tion of social constructivist models of learning to midwiferyeducation, Schön’s pragmatic model of reflective practicehas been weakened by its failure to provide an explanatorymodel or mechanism of social institutional learning. Theemphasis has moved from reflection for facilitation to reflec-tion for confirmation of competence. A dialogical research
model is needed that reflects the complexity and uncertaintyof constructive responses to modern contingencies.
POSITION VS. ROLE
Reflective practice is promoted as the foundation of profes-sional development but lacks a psycho-sociological theoryfor exploring social constructive meanings in dialogues inthe work place. Doctoral research by Phillips seeks a learningmechanism in the ordinary conversations, seen as social actsoccurring between students and their preceptors in practicesettings, which impact upon students’ personal professionalidentity formation. Positioning theory can be used to under-stand this discursive activity in terms of the psychologicallocation or position of the speakers in the storylines theybring into their conversations, developed from institutionalpractices and societal rhetoric to project their specific persona.The theory proposes that it is through the same conversa-tions that the speakers come to a sense of their own personalidentity and that the social institution of midwifery is notonly maintained but also transformed.
Positioning theory proposes the person and the conver-sation as primary social entities in the construction of socialmeaning. It is in the very nature of the discursive acts that manyphenomena, such as the duty of care, associated with profes-sional competence are to be found. This means that withinmidwifery education, students during supervised practiceengage in professional conversations with their preceptors,other midwives and health professionals and throughpositioning processes promote these conversations to ensuresituated learning.
‘Role’ has long been assumed to be important in describingprofessional behaviour, framing reflective practice andcharacterizing stages and goals in professional inductionand development. Role symbolizes the bundle of formalpredictable attributes associated with a particular socialposition, as distinct from the personal characteristics of theindividual who occupies that position.
When fine details of interpersonal interactions in clinicalplacements are examined closely, they appear more dynamicthan role theory would allow. Further, the relations betweenpeople that seem to be operating are, in a broad sense, moralas they involve moment-by-moment assignments of rightsand duties with respect to the social meanings of what peoplecan be understood to be doing.
VARIOUS DEFINITIONS OF REFLECTION
In reference to literature related to nursing/midwifery edu-cation and education in general, the prevailing assumption
NIN_145.fm Page 240 Friday, November 15, 2002 9:04 PM

From personal reflection to social positioning
© 2002 Blackwell Science Ltd,
Nursing Inquiry
9
(4), 239–249
241
is that reflection is a cognitive activity, where the developmentof practical reasoning at this intersection of individualpurposes and social action occurs. A variety of viewpointshave considered reflection as a social or political act, asopposed to it being a psychological act.
Dewey (1933) considered reflection and thinking tobe interdependent activities. Kemmis (1985, 141) describedreflection as simply ‘thinking about thinking’. In performinga specific task upon ‘reflection-in-action’ and ‘reflection-on-action’, Schön (1983, 1988) described reflection asthe process for the new graduate as ‘thinking on their feet’.The pedagogical model promoted by Shulman (1987) forthe appraisal of advanced reasoning included comprehension,transformation (preparation, representation, selection,adaptation), instructions, evaluation, reflection and newcomprehensions. Within this context, Shulman (1987, 18),concerned with the improvement of the quality of teachingthrough the appraisal of teachers’ practical reasoning,described reflection as ‘what a teacher does when he or shelooks back at the teaching and learning that has occurred,and reconstructs, re-enacts, and/or recaptures the events, theemotions, and the accomplishments’, which succinctlydescribed the cognitive processes required for learning.Mezirow and Associates (1990
)
and Mezirow (1991, 1994,1996) explained a transformational process whereby eachlearner develops opinions based on previous experiences tocreate new meaning from new experiences. Reflectionhere plays a key role in the transformation of meaning(s).This transformation theory (Mezirow 1998) is grounded inthe nature of human communication, especially with referenceto intentions, values, moral issues and feelings. In nursing andmidwifery education, recent literature draws upon reflectivepractice as an essential learning tool to promote criticalthinking, analysis, synthesis and evaluation of situatedlearning experiences that impact upon the development ofpractice (Johns and McCormack 1998; Bulman and Burns2000; Taylor 2000).
EDUCATING TACIT KNOWLEDGE
The notion of tacit knowledge has widespread currencyin modern social theory and philosophy (Polanyi 1958;Giddens 1979; Schön 1988; Bourdieu 1990). Schön (1988,1991) used the term ‘technical rationality’ to refer to an implicitproblem-solving ability that arises from the influence ofpositivist epistemology in those professions aligned withscience or applied science, such as medicine. It is understoodthat such professions have an existing body of technicalknowledge and expertise, the exactness of which defines theirprofession. Schön and others refer to tacit knowledge as
an understanding of the hidden order of rule(s) inherentwithin professional practice for everyday social action.
Schön referred to the use of this tacit knowledge as‘artistry’. The concept of tacit knowledge was introduced byPolanyi (1958, 92), who stated that it ‘exceeds the powers ofarticulation’. Previous learning and perceptions are influen-tial factors in practice, even though the individual may beat a loss to explain how this impacts upon his or her clinicaldecision-making (Schön 1983, 1988; Boud et al. 1985;Kemmis 1985).
Johns (1998, 3), a nurse academic, described professionalintuition as the manifestation of tacit knowledge, ‘a know-ing that is deeply embodied but unable to be expressedin rational ways’. Taylor (2000), Johns (1998) and Rolfe (1998),three nurse academics/practitioners, stated that ‘intuition’ isdeveloped from experiential knowledge, but not necessarilyfrom simple exposure to situations. Intuition, accordingto Benner (1984) and Benner et al. (1996), is usually experi-enced by expert practitioners; however, a nurse with 20 yearsexperience should not be assumed to be an expert. Heath(1998) took the view that nursing actions can rarely be simplyright or wrong and, further, qualified nurses may perform atdifferent levels based on their understanding of the formaltheory and experiences that contribute to reflective decision-making processes. The term ‘practical knowledge’ is embeddedin the social sciences and articulated in acts and, accordingto Giddens (1979), is similar to Polanyi’s tacit knowledge.Giddens characterized practical knowledge as primarily beingabout the internalized rules, resources and beliefs that guidesocial interactions without conscious attention being givento those rules and beliefs.
Fawns (1984) described a cycle of reflection, incorporatingself-analysis, planning, transacting and reviewing, stimulatedby conversations related to professional praxis in teaching.He encompassed three elements of Polanyi’s (1958) personalknowledge: theoretical and interdisciplinary knowing through‘skilful-tacit knowing’, ‘common-sense/social knowing’ and‘disciplinary knowing’. These forms of knowledge developin a dialogical cycle of reflective practice and active learning.Butler (1992, 234) argued that the process that leads to‘the uncovering of the self by the process of reflection musttake place prior to the formulation of the action that leadsto the Schön processes’. Butler’s analysis was grounded in aGadamerian hermeneutics (Skinner 1985).
Boud and Feletti (1991, 21) stated that the social settingfor professional praxis in reflection, which they describeas ‘problem-based learning’, is an approach to structuringthe curriculum that ‘involves confronting students withproblems from practice that provide a stimulus for learning’.Problem-based learning is consistent with adult learning
NIN_145.fm Page 241 Friday, November 15, 2002 9:04 PM

D Phillips et al.
242
© 2002 Blackwell Science Ltd,
Nursing Inquiry
9
(4), 239–249
principles such as self-directed learning, communicationskills, critical reasoning, logical and analytical approachesto problems, reasoned decision-making and self-evaluation.Although these attributes are required for problem-basedlearning, they do not constitute it. These are skills learnedin situated ‘professional’ learning, and although there is noclear definition of these skills within the context of nursing/midwifery education, critical reflection has been establishedas the highest level of reflection, with the outcome beingcognitive change. Yost et al. (2000) saw reflection as aproblem-solving process in which experienced individualsattempt to make sense of a challenging situation. This meansthat the individual concerned identifies areas of practicethat require scrutiny, determines goals for improved practiceand undertakes actions to achieve the identified goals. Theaim is therefore to modify and enhance professional practicethrough the progression of problem-solving, resulting in thereconstruction of knowledge.
In ‘problem-based learning’, as in ‘reflective practice’, thepsychological process is under-theorized as the ‘problem’ isoften being addressed. As with reflective practice, confusionmay emerge in relation to different terminology applicationsmade in curriculum planning for problem-based learning.Ross (1991) found multiple meanings in the literature.
The concept of tacit knowledge has been clearlyinfluenced by the ‘ordinary language philosophy’ of Polanyi(1958) and Ryle (1973), with the clear distinction between‘knowing how’ and ‘knowing that’. Critics such as Pleasants(1996) argued that ‘tacit knowledge’ remains an ‘occult’ entityin wide use in the explanatory schemes of different socialtheorists and is used by the ‘laity’, meaning the professionalsin his context, in celebration of the solidarity of their socialbonds.
SHIFTING THE RESEARCH FOCUS ONTO PROFESSIONAL DIALOGUE
Benner (1984), Schön (1983, 1988, 1991) and Shulman (1987,1998) are primarily concerned with the codification of thesocial, psychological and technical knowledge of professionals;Van Manen (1994), Sockett (1993) and others have placedemphasis upon the ethical dimensions of decision-makingof professionals. Professionals observed to be makingdecisions often do not attempt to articulate explicitly therationale for their actions, which according to Schön (1983,1988) is often tacit, embodied in a particular context suchas previous experiences in previous conversations and con-nected with reflection. This suggests that Schön’s reflectivepractice is not an individual or mentalistic construction,but rather a social-professional dialogue in which logical
and moral knowledge can be achieved through a process ofundefined inductive acts or habits rehearsed in discursivepractice in particular settings. This means that the mentor roleis undeveloped in the professional induction of a neophyteand where positioning theory is intrinsic in the moment-by-moment interactions that occur between a mentor and astudent leading to social constructions and learning.
POSITIONING THEORY
Positioning theory is a relatively recent development thatoriginated in the work of Hollway in 1984 (van Langenhoveand Harré 1999a). It is related to position and gender dif-ferentiation, and is underpinned by theories from socialconstructionist psychology, developed by Wittgenstein andVygotsky (Davies and Harré 1990; Gillett and Harré 1994;Howie and Peters 1996). Vygotsky, from a social psychologicalperspective, emphasized the power of discourse to influencethinking and consciousness (Hanfmann and Vakar 1962),fundamental to positioning theory. The relationship ofpositioning theory to midwifery education and practice ispresented in consideration of the possible range of humanbehaviours within personal, societal and institutional contexts.Harré and van Langenhove (1999a) described positioningtheory as a tool that can be applied to the analysis of everydayconversations conducted in clinical settings in which studentmidwives are engaged, and that may enable identities(individual and social), societal issues and culture to bedetermined.
A ‘position’ is a metaphorical concept in which an indi-vidual ‘positions’ himself/herself within three social entities
—
people, institutions and societies
—
where discursive prac-tices are conducted either privately or publicly. Moghaddam(1999, 74) explained that to apply the word ‘position’ ratherthan ‘role’ is to bring to attention the ‘dynamic and negot-iable aspects of interpersonal encounters’. Davies and Harré(1999, 37) defined ‘positioning’ as ‘the discursive processwhereby people are located in conversations as observablyand subjectively coherent participants in jointly producedstorylines. There can be interactive positioning in which whatone person says positions another’. For example, locationsfor speech-acts between students and their preceptors/midwives were considered by van Langenhove and Harré(1999a) to be the primary configuration of positioningtheory, while individual differences, such as personal agencyand autobiography, were regarded as components for thesecondary configuration. The concept of ‘position’ is mani-fested therefore by a certain set of rights, duties and obliga-tions as a speaker, whereby each episode of everyday life canbe seen as the development of a storyline (Gillet and Harré
NIN_145.fm Page 242 Friday, November 15, 2002 9:04 PM

From personal reflection to social positioning
© 2002 Blackwell Science Ltd,
Nursing Inquiry
9
(4), 239–249
243
1994; van Langenhove and Harré 1994). The literature inthis area has more recently emphasized the importance of‘local moral orders’ or obligations that are implicit in socialstructures and interactions through conversations (Gillettand Harré 1994; Davies and Harré 1999; Harré and vanLangenhove 1999a; Moghaddam 1999; van Langenhove andHarré 1999b).
Although it is acknowledged that interactive positioningcan occur, generally positions are relational. For example,when one is positioned as powerful, others may be positionedto feel powerless, or conversely, when another individualhas positioned himself/herself as confident, one may not feelconfident. Davies and Harré (1999, 37) warned that it wouldbe a mistake to assume that positioning is intentional as‘one lives one’s life in terms of the kind of person one takesoneself to be, whoever or whatever might be responsiblefor its production’. It is implied that positioning theory isdynamic and dependent upon situations in which indi-viduals find themselves and how they manage these situ-ations. In the following, van Langenhove and Harré (1999a,17) define ‘positioning’:
Positioning is thus to be understood as a procedure ofmaking determinate a psychological phenomenon for thepurpose at hand. But positions can and do change. Fluidpositionings, not fixed roles, are used by people to cope withthis situation they usually find themselves [in].
It is within discursive practices that the ‘social world’ isformed, and according to van Langenhove and Harré (1999a,15), it is ‘within conversations, [that] social acts and societalicons are generated and reproduced’. This means that socialactions can be recognized or ‘determined’ by others, whileother actions may not be understood, and are described withinthe literature as ‘indeterminate’. Clearly, individuals choosewhether or not they wish to respond to being positioned.In institutional settings, choices may not exist for individualssubjected to positioning by those who have a foremost func-tion within an organization. In essence, positioning theorydraws upon the construction on meanings that participantsmake through their conversations to incorporate position,speech-act and storyline (Harré and van Langenhove 1991;van Langenhove and Harré 1999a).
Language that is strategically used and perceived,according to Davies and Harré (1990), is a public institutionand as a consequence is the foundation upon which socialstructures and agencies are developed and understoodlocally as either the ‘social force’ or ‘illocutionary force’.Gillett and Harré (1994) argued that important componentsfor professional discourses are the joint constructionscreated by individuals to embody socio-cultural factors wheresymbols, interactions, relationships and rules are applied.
Certainly, this is applicable to midwifery education, whereinstudents work in close collaboration with midwives (as theirpreceptors) to learn about practice within the context oflegislative requirements (Nurses Board of Victoria) and thepolicies and procedures related to organizations in whichstudents are inducted into midwifery practice. The discursiveact of positioning requires reconstructing the speaker’sbiography in relation to the individual being positionedand adopting positions that may be subject to rhetorical re-descriptions. Individuals therefore construct stories (internalor external) about institutions or events that are intelligibleand, as pointed out by Harré and van Langenhove (1991),these stories have symbolic meanings and moral indexesof their agency and become, at this ontological level, ‘societalicons’. Three methods assist in the expression of personalidentity within discursive practice: agency (assuming respon-sibility), statement on the point of view, and evaluation ofa past event as a contribution to one’s biography (Howie andPeters 1996; Harré and van Langenhove 1999a).
A PSYCHOLOGICAL MODEL OF REFLECTIVE PRACTICE AND PROFESSIONAL IDENTITY
FORMATION
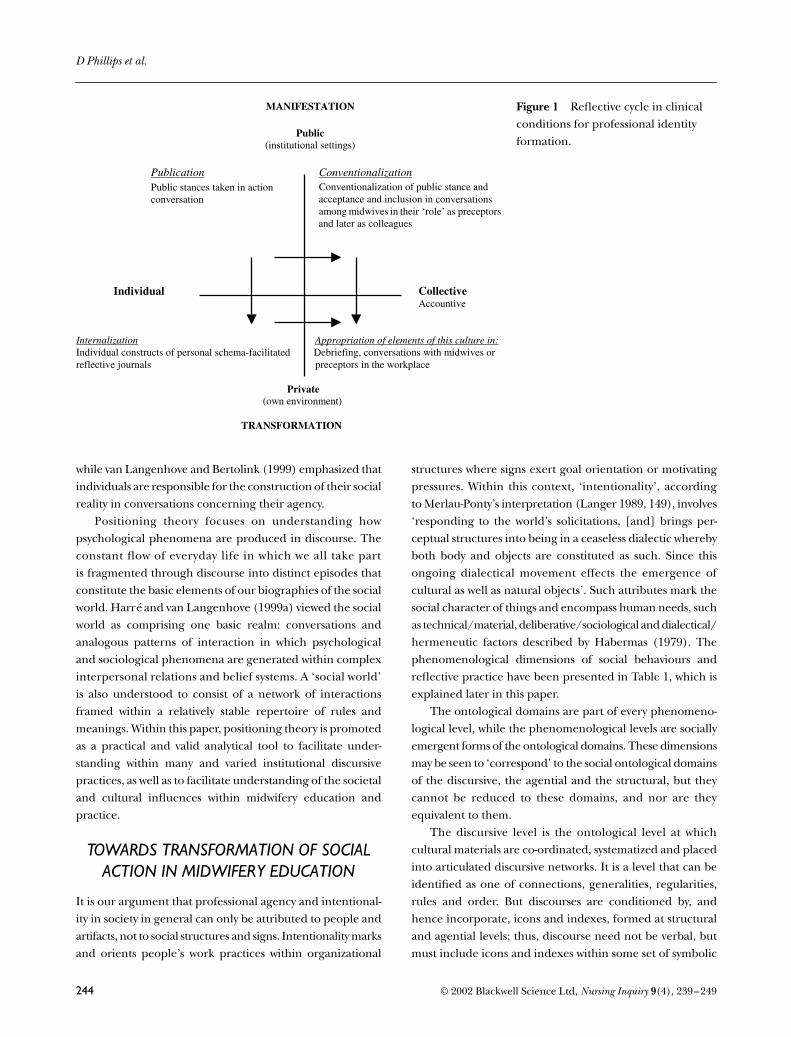
Figure 1 presents a schematic cycle of the personal andprofessional identity formation that individuals engage inand the interactions represented between the ‘public’ and‘private’ domains for reflective practice. Core elements withinsuch interactions include, for example, private or personalreflection occurring within the ‘individual’ (representingindividual thoughts), while public reflection is embodiedwithin social discourse with, for example, peers (singly or withina group), midwives or the preceptor/midwife and occurswithin the ‘collective’. These underpinning principles havedrawn upon Vygotskian theories where ‘public’ (external)and ‘private’ (internal) language may impact upon actionsthat individuals may take following discussion with others(public) or thinking (private) through a problem (Hanfmannand Vakar 1962).
SOCIAL CONSTRUCTIONIST RESEARCH
Harré and van Langenhove (1999b) described how two basicprinciples underpin social constructionism with positioning.First, what individuals do publicly and privately is intentional;secondly, what individuals are to themselves and others is aresult of interpersonal interactions developed over a lifetime.Davies and Harré (1999) referred to the ‘immanentist stance’,meaning that conversations are conducted within social rules,
NIN_145.fm Page 243 Friday, November 15, 2002 9:04 PM
D Phillips et al.
244
© 2002 Blackwell Science Ltd,
Nursing Inquiry
9
(4), 239–249
while van Langenhove and Bertolink (1999) emphasized thatindividuals are responsible for the construction of their socialreality in conversations concerning their agency.
Positioning theory focuses on understanding howpsychological phenomena are produced in discourse. Theconstant flow of everyday life in which we all take partis fragmented through discourse into distinct episodes thatconstitute the basic elements of our biographies of the socialworld. Harré and van Langenhove (1999a) viewed the socialworld as comprising one basic realm: conversations andanalogous patterns of interaction in which psychologicaland sociological phenomena are generated within complexinterpersonal relations and belief systems. A ‘social world’is also understood to consist of a network of interactionsframed within a relatively stable repertoire of rules andmeanings. Within this paper, positioning theory is promotedas a practical and valid analytical tool to facilitate under-standing within many and varied institutional discursivepractices, as well as to facilitate understanding of the societaland cultural influences within midwifery education andpractice.
TOWARDS TRANSFORMATION OF SOCIAL ACTION IN MIDWIFERY EDUCATION
It is our argument that professional agency and intentional-ity in society in general can only be attributed to people andartifacts, not to social structures and signs. Intentionality marksand orients people’s work practices within organizational
structures where signs exert goal orientation or motivatingpressures. Within this context, ‘intentionality’, accordingto Merlau-Ponty’s interpretation (Langer 1989, 149), involves‘responding to the world’s solicitations, [and] brings per-ceptual structures into being in a ceaseless dialectic wherebyboth body and objects are constituted as such. Since thisongoing dialectical movement effects the emergence ofcultural as well as natural objects’. Such attributes mark thesocial character of things and encompass human needs, suchas technical/material, deliberative/sociological and dialectical/hermeneutic factors described by Habermas (1979). Thephenomenological dimensions of social behaviours andreflective practice have been presented in Table 1, which isexplained later in this paper.
The ontological domains are part of every phenomeno-logical level, while the phenomenological levels are sociallyemergent forms of the ontological domains. These dimensionsmay be seen to ‘correspond’ to the social ontological domainsof the discursive, the agential and the structural, but theycannot be reduced to these domains, and nor are theyequivalent to them.
The discursive level is the ontological level at whichcultural materials are co-ordinated, systematized and placedinto articulated discursive networks. It is a level that can beidentified as one of connections, generalities, regularities,rules and order. But discourses are conditioned by, andhence incorporate, icons and indexes, formed at structuraland agential levels; thus, discourse need not be verbal, butmust include icons and indexes within some set of symbolic
Figure 1 Reflective cycle in clinical conditions for professional identity formation.
NIN_145.fm Page 244 Friday, November 15, 2002 9:04 PM

From personal reflection to social positioning
© 2002 Blackwell Science Ltd,
Nursing Inquiry
9
(4), 239–249
245
relations in discourse. Discourses incorporate icons and/orindexes not only for the production of knowledge but alsofor the cultural possibility of articulating discourses thatare intended to show uncertainty and dissent, insofar as theseconcerns derive from images and indicators produced ineveryday experience.
Harré and van Langenhove (1999a) described howtwo basic principles underpin social constructionism withpositioning. First, what individuals do, publicly and privately,
is intentional; second, what individuals are to themselvesand others is a result of interpersonal interactions developedover a lifetime. Social constructionism, as argued by vanLangenhove and Bertolink (1999), is crucial for socialphenomena to be considered and generated in and throughconversations and conversation-like activities. As such, discursiveprocesses are considered to be the ‘place’ where many, if notmost, of the psychological and social constructions are jointlycreated (Harré and van Langenhove 1999a).
Table 1 A transformational model for midwifery education
Ontological domains of practice
Phenomenological scopes for practice
Technical Material entities
Social Self and others
Hermeneutic Interpretations of experiences
Discourses (conversations) (quasi/internal conversations based on reflective practice)
Oral discourseDiscourse between the student and preceptor/midwife essential for the delivery of care. Written discourse The student participates in documentation procedures while providing care and maintains a clinical log that incorporates reflections about acceptable practices; questions the practice of self and others.
Illocutionary forces/intended meanings in oral discourse Psychological processes of inner speech informing written discourse and oral discourse.Power as ability to choose.
Discursive formulations, reasons, reasoning of self and others, particular and generalized othersTheories taught in the university, midwifery and nursing professionalism, power/parity, subjective/objective truth, moral/technical values, interests and cultural background. Particular critical incidents, for example in the birthing room or in culture.
SymbolsAgency (actual)
Supervised program of practice and organised experiences to facilitate professional development.Institutions or organizations.Habits/habitus in professional communities of nursing and midwifery.
Midwifery practice development is a planned process whereby students work in collaboration with their preceptors or other midwives in the provision of maternity services.
Successful discursive action enables the student to be admitted as an endorsed midwife.Discursive positioning and performance strategies. Indexes With regard to an elaboration of Benner’s stage model.For successful course completion, the student must be clinically assessed to be ‘competent’, in a range of skill-based competencies, by preceptors.
Institutions, organizations.Power as ability to act.
Structures(possibilities)
Practice development is planned according to:Nurses Board of Victoria (Code of Practice)ACMI Code of Ethics/Competencies.
Midwifery as a profession developed upon:Social positions.Social relations of production.Power domination within institutional practices.
Image schemata, base level categories: meaning structures. ICONS include:Midwifery care.Technology.Benner’s model.Feelings (membership to midwifery culture).Institutional policies and
procedures.
NIN_145.fm Page 245 Friday, November 15, 2002 9:04 PM

D Phillips et al.
246
© 2002 Blackwell Science Ltd,
Nursing Inquiry
9
(4), 239–249
In this paper, we argue that three ontological domains(discourse, agency and structures) appear in some form withineach dimension of social practice because the domains formidwifery practice only exist through human agency. Asthe phenomenological dimensions are related to the onto-logical domains, they have emergent properties and hencea degree of autonomy. The phenomenological dimensionsof practice also correlate with the three main modes ofexplaining social behaviour, delineating in what manner,to what end and with what understanding we act. Technicalexplanations focus on material realities to show how socialstructures, practices and discourses operate or, in otherwords, how they achieve their effects.
Such explanations divulge systems, structures, mech-anisms and dispositions for individuals to act in certainways and generate certain results. However, it is possiblefor agents to monitor and act upon these systems ormechanisms, facilitating or not facilitating their operation,in order to achieve or inhibit their emergent effects. Thus,emerging from technical explanations are functionalarguments, which identify the goal orientations, roles orconsequences that direct agent’s actions in social structuresand discourses, the ways they feed back into agents’ ownstates and conditions. Functional explanations in thisexpanded sense concern the reflexive motivation of agents’actions upon causal mechanisms. Such explanations donot assume that all actions are beneficial to the social systemas a whole nor even necessarily to the dominant group.Moreover, as society is a system of positioned practices (Harréand van Langenhove 1999a), midwives as social agents arenecessarily differentiated and therefore obtain differentreflexive motivations in the form of interests and differentcapacities to realize such interests, as well as intentionsto act on the basis of their given conditions, positions andresources.
However, these various reflexive motivations (interestsand intentions) can themselves become the object of reflexivemotivation: by ‘monitoring the monitoring’ of their actions,agents generate an understanding and rationale for theiractions. That is, the meanings of action influence the inten-tion to act. Thus, hermeneutic explanations have emergedfrom functional explanations and disclose how peopleand institutions, such as midwifery, act according to sociallycreated structures of meanings, including the legislativerequirements for practice. Midwifery practices not only havemethods and goals, but also significance: along with thepragmatic and interactive aspects of their activities, peopleact for symbolic ends or in symbolic ways, say for a more‘relevant’ or ‘grounded’ education, and produce meaningsin the course of their activity. The structures of meaning
themselves depend on positioned practices to motivatesocial distinction.
Taken together, the social levels and their phenomeno-logical dimensions can be represented in a grid, as shown inTable 1.
The vertical axis of Table 1 shows three levels of socialontology; the general ontological domains to which they aremost connected are indicated in parentheses. The horizontalaxis presents the phenomenological dimensions of practice,and places the modes of explanation. We attempted toindicate the sorts of social elements that occupy each gridcell (more could be added). Due to the mixed character ofall social practices, it is sometimes difficult to decide whereto place certain features of society, and the reasons behindsome of these choices cannot be fully explained here. Mostare, we believe, clear. Starting from the lower left structurescell and working counter clockwise, we find the materialstructures of society (forces of production and human bodies),including economic structure, the framework of communi-cation, and possibly family structures. Out of these materialprocesses emerge social relations and forms of power, such asdomination, subordination and exploitation in the workplace.
From both the material and sociological dynamics emergemeanings in the form of basic concepts and images, whichare principally iconic. The ‘Benner model’, for instance, isan icon of intellectual and social exchange in professionaleducation through the identification of five stages of skillacquisition. Conversely, our understanding of underlyingstructures, such as the domain for midwifery practice, dependson our ability to generate iconic models of such structures.Image schema and basic categories conjoin to form meaningstructures that act as generative principles for higher-levelforms of meaning. Due to the highly imagistic and qualitativenature of feelings, Raymond William’s ‘structures of feelings’may perhaps be placed here. These image schemata providethe basis for images of ‘self ’ and ‘other’ (Mead 1934; Woods1998) that constitute ideas of social identity and effect socialidentifications; they also organize transposable discursiveand performance strategies or norms of behaviour. Asidentity-imagery and meaning-strategies are distinguishedaccording to agents’ social positions, they are indexes ofagents’ locations in the social order; for example, of institu-tional settings (van Langenhove and Harré 1994).
With reference to the upper right cell in Table 1, identity-imagery and meaning strategies provide the most immediatesocial bases for the explicit articulation of discourses in theeducation of midwives in such forms as theories, ideologiesand clinical experiences. Such articulations depend onsymbols and have symbolic effects (among them, theirpotential claim to generality or universality). They also supply
NIN_145.fm Page 246 Friday, November 15, 2002 9:04 PM

From personal reflection to social positioning
© 2002 Blackwell Science Ltd,
Nursing Inquiry
9
(4), 239–249
247
justifications and/or rationalizations (whether real or pre-tended) for the student’s and the preceptor’s actions, whichtake the form of intended meanings (refer to the cell underthe heading ‘social’ and parallel with the heading ‘discourses’).Psychological dynamics are a significant part of intentionality,but these too are socially conditioned and social in form,as indicated by the character of thought (private) or intern-alization. Like agents and structures, workplace discoursesbetween midwives (in their function as preceptors) andstudents are connected to a specific form of power to choose,including the choice of how to interpret and express thingsthat is once again conditioned by social position.
Everyday expressions take technical material form (upperleft cell with the heading ‘discourses’), but as Bourdieu andDewey argue, the semiotic process may ultimately generatehabits, habit changes and habitus within agents. This is partof the organization and institutionalization of agents. Thus,two mentoring functions in midwifery education, that ofthe academic educator and that of the preceptor (midwife)as agents for student learning, need to be responsive to thestructural and semiotic effects incorporated within maternityservices. Midwifery also resides in the body politic, in whichprofessional development is dependent upon referrals within‘collectivities’, such as the hospital, the university and theprofessional organization. Transformation in such modes ofembodied agency can transform the material structures anddiscourses. At the centre of this account of positioned socialaction is embodied intentional agency (both individual andgroup), which provides the motivational force behind socialprocesses.
By distinguishing between the ontological and phenom-enological dimensions of social activity, we can obtainsharper insight into the issue of society’s technical concept-dependence. Bhaskar (1994) observed that society dependson these concepts, particularly at an agential level. Wherediscourses are critical for establishing identities and alliances,differences and oppositions, poststructuralist evaluationsof professional education rightly emphasize the significanceof discursive articulation and the political value of strugglesover meaning. Yet, there would be no point to these struggles,no stakes involved, were it not that the processes of formingand maintaining alliances, oppositions and organizationalarrangements, which often consume limited resources, canseldom readily be undone and ultimately reproduce ortransform the fundamental structures of society, includingstructures of power.
A transformational model of midwifery education canfill many gaps in the theory of reflective practice by adoptingan understanding of the clinical learning context that graspsboth the intransitive (internal) dimension of knowledge,
and the dialogical and dialectical nature of our mental accessto it in the transitive (external) dimension. A transformationalmodel has an obvious place in the ontology for experiencesand concepts, as it fosters a clearer understanding of themas signs. On that basis, we can rework research at the thirdontological level from the subjective to the semiotic. Thechange from the subjective to the semiotic also makes it possibleto offer a coherent analysis of the relationship betweenontological domains by adopting the concept of emergence.It is suggested that the domains of the possible, the actualand discursive, underlie a revised ontology of society, thestructure/agents dyad with a triad of structures, agents anddiscourses, each of which impact upon material and socio-logical aspects. Because reflective semiotics recognizes thepersonal and corporeal roles in the production of meaning, itgives the transformational model of midwifery educationa firmer grasp of the non-rational and non-cognitive aspectsof learning, including the roles of images, habits and embodi-ment. A transformational model of midwifery educationthereby contains a fuller theory of socially situated learning,one that incorporates the role of semiosis, and promises adeeper account of the dynamics of power.
CONCLUSION
There is a basis for our talk, a background from within whichwe make sense of our lives, a realm of knowledgeable activitythat is sustained, not simply by a practical-technical knowledge,nor by a form of theoretical-conceptual knowledge, but by athird kind of practical-moral knowledge of the non-conceptualkind. It is in this background, a sphere of human activity thatwe advocate. The context and the person must both be heldin focus in our practice and research in professional educa-tion where we face a new task of attempting to articulatethe background of our lives perspicuously, through under-standing and seeing connections. In insisting the primaryhuman reality is conversation, broadly defined as any flowof interaction through a public semiotic system (practices,gestures, speech both internal and public) positioningtheory has confronted us with problems in our academicdiscourses that will not go away. The problem of professionalknowledge and how common sense is established andsustained cannot be solved with available ‘theories’ and‘methods’. Lacking a systematic representation of its nature,interested only in what we as individual academics canpicture, we have previously failed to see the importance ofprofessional conversations; the nature of social processesinvolved in their creation and sustenance that have beeninvisible to us. It is through the promotion of professionalconversations that meaningful constructions are made from
NIN_145.fm Page 247 Friday, November 15, 2002 9:04 PM

D Phillips et al.
248
© 2002 Blackwell Science Ltd,
Nursing Inquiry
9
(4), 239–249
the language with which we clothe our perceptions andactions.
REFERENCES
Benner P, C Tanner and C Chesla. 1996.
Expertise in nursingpractice: Caring, clinical judgment, and ethics
. New York: Springer.Benner P. 1984.
From novice to expert: Excellence and power inclinical nursing practice
. Menlo Park, California: Addison-Wesley.
Bhaskar R. 1994.
Plato etc: The problems of philosophy and theirresolution
. London: Verso.Boud D and G Feletti. 1991. Part 1. What is problem-based
learning? In
The challenge of problem based learning
, edsD Boud and G Feletti, 21–2. London: Kogan Page.
Boud D, R Keogh and D Walker. 1985.
Reflection: Turningexperience into learning
. London: Kogan Page.Bourdieu P. 1990.
The logic of practice
. Stanford: StanfordUniversity Press.
Bulman C and S Burns. 2000. Students’ perspectives onreflective practice. In
Reflective practice in nursing: Thegrowth of the professional practitioner
, 2nd edn, eds S Burnsand C Bulman, 124–35. Oxford: Blackwell Science.
Butler J. 1992. Teacher professional development: AnAustralian case study.
Journal of Education for Teaching
18(3): 221–37.Davies B and R Harré. 1990. Positioning: The discursive
production of selves.
Journal for the Theory of Social Behaviour
20(1): 43–63.Davies B and R Harré. 1999. Positioning and personhood.
In
Positioning theory: Moral contexts of intentional action
,eds R Harré and L van Langenhove, 32–52. Oxford:Blackwell.
Dewey J. 1933.
How we think: A restatement of the relation of reflect-ive thinking to the educative process.
Boston: D.C. Heath.Emden C. 1991. Becoming a reflective practitioner. In
Towardsa discipline of nursing
, eds G Gray and R Pratt, 11–30.Melbourne: Churchill Livingstone.
Fawns R. 1984. The sources of theoretical principlesfor science method programs: A new setting explored.
Research in Science Education
14: 173–80.Garratt S. 1992. Reflective practice as a learning strategy.
In
Issues in Australian Nursing 3
, eds G Gray and R Pratt,213–28. Melbourne: Churchill Livingstone.
Giddens A. 1979.
Central problems in social theory: Action, structureand contradiction in social analysis
. London: Macmillan Press.Gillett G and R Harré. 1994.
The discursive mind
. ThousandOaks, California: Sage.
Habermas J. 1976.
Communication and the evolution of society.
Translated by T. McCarthy. London: Heinemann.
Hanfmann E and G Vakar. 1962.
Thought and language:L.S. Vygotsky
. Cambridge, Massachusetts: MassachusettsInstitute of Technology.
Harré R and L van Langenhove. 1991. Varieties of posi-tioning.
Journal for the Theory of Social Behaviour
21(4):393–407.
Harré R and L van Langenhove. 1999a. The dynamics of socialepisodes. In
Positioning theory: Moral contexts of intentionalaction
, eds R Harré and L van Langenhove, 1–13. Oxford:Blackwell.
Harré R and L van Langenhove. 1999b. Reflexive position-ing: Autobiography. In
Positioning theory: Moral contextsof intentional action
, eds R Harré and L van Langenhove,60–73. Oxford: Blackwell.
Hayes B. 2000. Mental health nursing: Celebrating choice
—
shaping the future beyond 2000. Proceedings of the26th International Conference, Australian and NewZealand College of Mental Health Nurses Inc.
Mentalhealth nurses for a changing world: Not just surviving, thriving
.3–7 September, Queensland, Australia.
Heath H. 1998. Reflections and patterns of knowing innursing.
Journal of Advanced Nursing
27(5): 1054–9.Howie D, and M Peters. 1996. Positioning theory: Vygotsky,
Wittgenstein and social constructionist psychology.
Journal for the Theory of Social Behaviour
26(1): 51–64.Johns C and B McCormack. 1998. Unfolding the conditions
where the transformative potential of guided reflection(clinical supervision) might flourish or flounder. In
Trans-forming nursing through reflective practice
, eds C Johnsand D Freshwater, 62–77. Oxford: Blackwell.
Johns C. 1998. Illuminating the transformative potentialof guided reflection. In
Transforming nursing throughreflective practice
, eds C Johns and D Freshwater, 78–90.Oxford: Blackwell Science.
Kemmis S. 1985. Action research and the politics of reflection.In
Reflection: Turning experience into learning
, eds D Boud,R Keogh and D Walker, 139–63. London: Kogan Page.
van Langenhove L and R Bertolink. 1999. Positioning andassessment of technology. In
Positioning theory: Moralcontexts of intentional action
, eds R Harré and L vanLangenhove, 116–26. Oxford: Blackwell.
van Langenhove L and R Harré. 1994. Cultural stereotypesand positioning theory.
Journal for the Theory of SocialBehaviour
24(4): 359–72.van Langenhove L and R Harré. 1999a. Introducing
positioning theory. In
Positioning theory: Moral contexts ofintentional action
, eds R Harré and L van Langenhove,14–31. Oxford: Blackwell.
van Langenhove L and R Harré. 1999b. Positioning as theproduction and use of stereotypes. In
Positioning theory:
NIN_145.fm Page 248 Friday, November 15, 2002 9:04 PM

From personal reflection to social positioning
© 2002 Blackwell Science Ltd,
Nursing Inquiry
9
(4), 239–249
249
Moral contexts of intentional action
, eds R Harré andL van Langenhove, 127–37. Oxford: Blackwell.
Langer MA. 1989.
Merleau-Ponty’s phenomenology of perception:A guide and commentary.
Tallahassee, Florida: The FloridaState University Press.
Mead GH. 1934.
Mind, self and society
. Chicago: University ofChicago Press.
Mezirow J and Associates. 1990.
Fostering critical reflection inadulthood: A guide to transformative and emancipatory learning
.San Francisco: Jossey-Bass.
Mezirow J. 1991.
Transformative dimensions of adult learning
.San Francisco: Jossey-Bass.
Mezirow J. 1994. Understanding transformation theory.
Adult Education Quarterly
44(4): 222–32.Mezirow J. 1996. Contemporary paradigms of learning.
AdultEducation Quarterly
46(3): 158–73.Mezirow J. 1998. On critical reflection.
Adult EducationQuarterly
48(3): 185–98.Moghaddam FM. 1999. Reflexive positioning: culture and
private discourse. In
Positioning theory: Moral contexts ofintentional action
, eds R Harré and L van Langenhove,74–86. Oxford: Blackwell.
Pleasants N. 1996. Nothing is concealed: De-centring tacitknowledge and rules from social theory.
Journal for theTheory of Social Behaviour
26(3): 233–255.Polanyi M. 1958.
Personal knowledge: Towards a post-criticalphilosophy
. London: Routledge and Kogan Paul.Rolfe G. 1998. Beyond expertise: Reflective and reflexive
nursing practice. In
Transforming nursing through reflectivepractice
, eds C Johnsand and D Freshwater, 21–31. Oxford:Blackwell Science.
Ross B. 1991. Towards a framework for problem-based
curricula. In
The challenge of problem based learning
, edsD Boud and G Feletti, 34–41. London: Kogan Page.
Ryle G. 1973.
The concept of mind
. London: Penguin Books.Schön D. 1983.
The reflective practitioner: How professionalsthink in action
. New York: Basic Books.Schön D. 1988.
Educating the reflective practitioner: Toward anew design for teaching and learning in the professions
. SanFrancisco: Jossey-Bass.
Schön D. 1991.
The reflective practitioner: How professionals thinkin action.
Aldershot: Avebury.Shulman LS. 1987. Knowledge and teaching: Foundations
of the new reform.
Harvard Educational Review
52(1):1–22.
Shulman LS. 1998. Theory, practice, and the educationof professionals (John Dewey: The Chicago years).
TheElementary School Journal
98(5): 511.Skinner Q. 1985.
The return of grand theory in the human sciences
.Cambridge: Cambridge University Press.
Sockett H. 1993.
The moral base for teacher professionalism
.New York: Columbia University.
Street A. 1991.
From image to action: Reflection in nursing practice.
Geelong, Vic: Deakin University.Taylor B. 2000.
Reflective practice: A guide for nurses andmidwives.
St. Leonard
s
, New South Wales: Allen and Allen.Van Manen M. 1994. Pedagogy, virtue, and narrative identity
in teaching.
Curriculum Inquiry
24(2): 135–170.Woods P. 1998.
Researching the art of teaching: Ethnography foreducational use
. London: Routledge.Yost DS, SM Sentner and A Forlenza-Bailey. 2000. An
examination of the construct of critical reflection:Implications for teacher education programming in the21st Century.
Journal of Teacher Education
5(1): 39.
NIN_145.fm Page 249 Friday, November 15, 2002 9:04 PM