From Guidelines To Decision Support - Yale...
42
From Guidelines To Decision Support A Systematic and Replicable Approach To Guideline Knowledge Transformation Yale School of Medicine GLIDES PROJECT GuideLines Into DEcision Support sponsored by the Agency for HealthCare Research and Quality
Transcript of From Guidelines To Decision Support - Yale...

From Guidelines To Decision SupportA Systematic and Replicable Approach
To Guideline Knowledge Transformation
Yale School of Medicine
GLIDES PROJECTGuideLines Into DEcision Support
sponsored bythe Agency for HealthCare Research and Quality

Overview
• Systematic and replicable• Define clinical objectives• Markup with GEM• XML transforms• Action-types• GLIA



Define Clinical Objectives
• Teleconference involving stakeholders• Notes distilled; circulated for approval• Each objective scored
– Addressed by the selected guidelines?– IT can facilitate attainment?– Evaluable?

Goals and Specific Activities
Recognize high-risk behaviors
Screen time (TV computers) Y Y Y
Nutritional Y Y Y
Lack of exercise Y Y Y
Counseling (Energy balance: Nutrition-Activity)
Limit sugar sweetened beverages Y Y Y
Encourage fruits and vegetables Y Y Y
Breakfast daily Y Y Y
Limit fast food Y Y Y
Encourage family meals Y Y Y
Limit portion sizes Y Y Y
5210: (fruits & vegetables, max screen time, physical activity, juice intake) Y Y Y
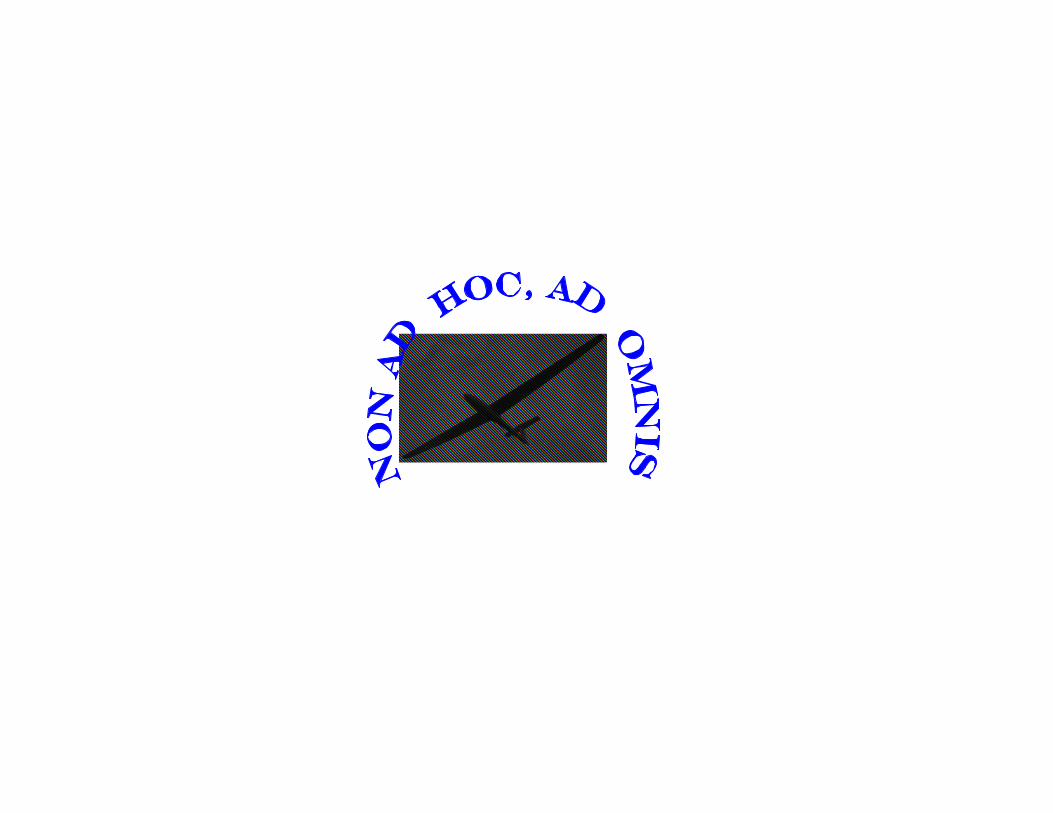
Select Relevant Guideline andRecommendations
• Manual process• .pdf documents transformed to .html
Recognize high-risk behaviors
Screen time (TV computers) Y Y Y 245 1c
Nutritional Y Y Y 179, 186 6
Lack of exercise Y Y Y 179, 186 7
Counseling (Energy balance: Nutrition-Activity)
Limit sugar sweetened beverages Y Y Y 245 1a
Encourage fruits and vegetables Y Y Y 245 1b
Breakfast daily Y Y Y 245 1d
Limit fast food Y Y Y 245 1e
Encourage family meals Y Y Y 245 1 f
Limit portion sizes Y Y Y 245 1g
5210: (fruits & vegetables, max screen time, physical activity, juice intake) Y Y Y 245 1

Markup Guideline
• GEM Cutter II– Parses guideline text into components of
the Guideline Elements Model– Create XML files– “GEMifying”
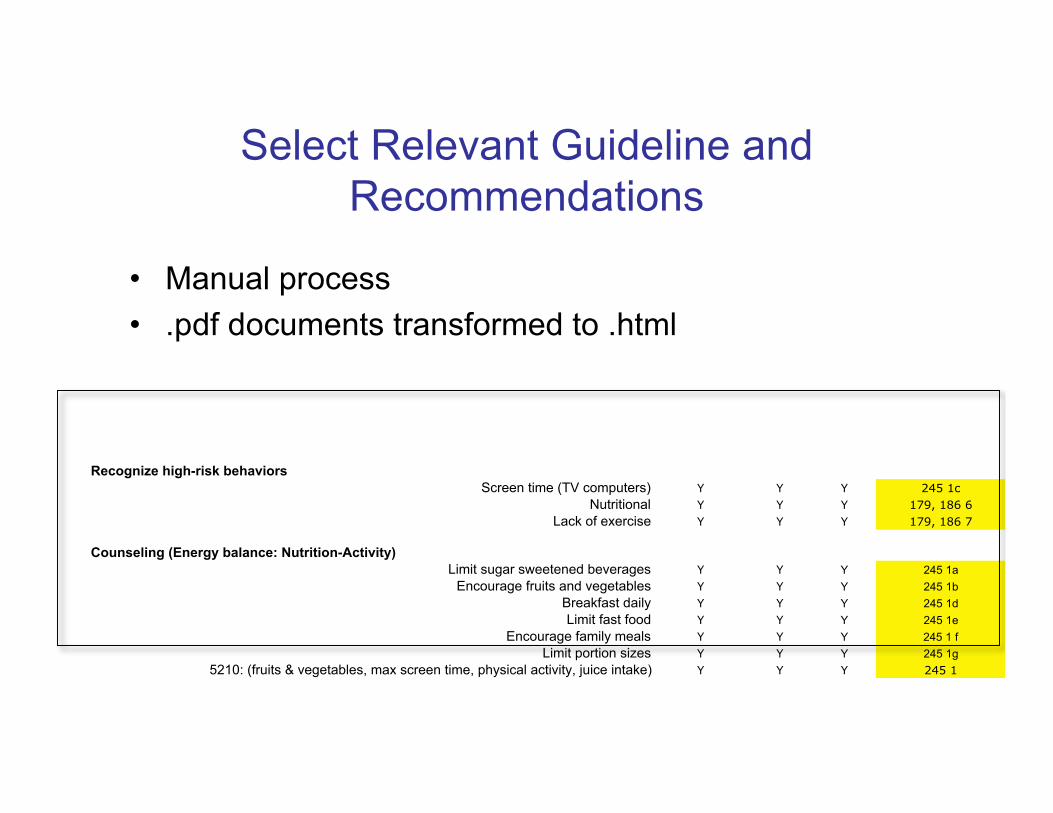
Logical Analysis withHighlighters
• UTI Recommendation 3If an infant or young child 2 months to 2 years of age
with unexplained fever is assessed as being sufficiently illto warrant immediate antimicrobial therapy, a urinespecimen should be obtained by SPA or bladdercatheterization; the diagnosis of UTI cannot beestablished by a culture of urine collected in a bag.(Strength of evidence: good) Urine obtained by SPA orurethral catheterization is unlikely to be contaminated...

XML: From a small number ofdiscrete colors to an unlimited palette
XML
• Multi-platform, Web-based, open standard
• “Tags” enclose and describe text
<inclusion.criterion>hematuria</inclusion.criterion>
• Human-readable, yet can be processed by machine
• Markup can be performed by non-programmers
• “Hot”—considerable energies invested in X-tech

• Knowledge model for guideline documents
• GEM adopted as a standard by ASTM in 2002; GEM II updated andre-standardized in 2006
• Models heterogeneous information contained in guidelines
– Multi-level hierarchy (>100 elements) indicates relationships
GEM

GEM II-Top Level


Conditional

GEM Cutter

MORO
Reuse OftenMarkup Once,

Perform Guideline Quality Appraisal
• Informal• COGS (GEM-COGS)• AGREE

GEM-COGS

Extractor: Recommendations• Executive Summary of actionable statements
that bear on clinical objectives
Recommendation5–11 Years of Age: Initiating Long-Term Control Therapy.
Conditional: 5–11 Years of Age: Initiating Long-Term Control Therapy.The Expert Panel recommends daily long-term controltherapy for children who have persistent asthmaRec_5: Cond_5
RecommendationAdjusting Therapy
Conditional: The Expert Panel recommends that, if a child is alreadytaking long-term control medication, treatment decisions arebased on the level of asthma control that has been achieved:therapy should be stepped up if necessary to achieve controlRec_6: Cond_6

EXTRACTOR: RulesHuman-readable statement logic
EXTRACTOR: Decision Variables
• Decision variables are removed from guidelinecontext and presented in a list.
• Opportunity to identify and judge vagueness,underspecification, and decidability
• Provides a comprehensive list of trigger items fordecision support activities
• Measurable starting points for evaluation

Decision Variables

EXTRACTOR Transforms (2)
• Actions• Actions (and directives) are removed from guideline
context and presented in a list• Opportunity to identify and judge underspecification,
vagueness, and executability• Comprehensive list of activities that will need to be
addressed in the design of the decision support system• Listing of potentially measurable actions

Actions

Categorize Action-types
• Test (Inquire,Examine)
• Monitor• Conclude• Prescribe• Perform Procedure
• Refer/consult• Educate/counsel• Document• Dispose• Prepare• Advocate

Action-Types in405 Recommendations
Monitor
Test
Gather Interpret Perform Dispose
Action
Conclude Prescribe
Educate
Document
Procedure
Consult
Advocate
Prepare
Essaihi A. Proc AMIA 2004

Action Distribution
Refer 5%
Dispose 4%Conclude 3%Monitor 3%Document Prepare Advocate
No Rec

Example: Application of Action-Types
• Action-type: Prescribe– Drug information– Safety alerts (allergy, drug-drug, drug-
disease, drug-lab)– Formulary check– Dosage calculation– Pharmacy transmission– Patient education– Corollary orders

Action-Types
Determine a diagnosis or clinical statusConclude
Direct a patient to another clinician for evaluationand/or treatment.
Refer /Consult
Inform the patient about means to improve/maintainhealth, or instruct on how to perform specificactivities.
Educate /Counsel
Order activities that are therapeutic in nature.Perform
Order a treatment requiring medication or durablemedical equipment.
Prescribe
Obtain or collect additional data through inquiry,laboratory testing, or other investigative procedureswhose intent is not curative.
Test
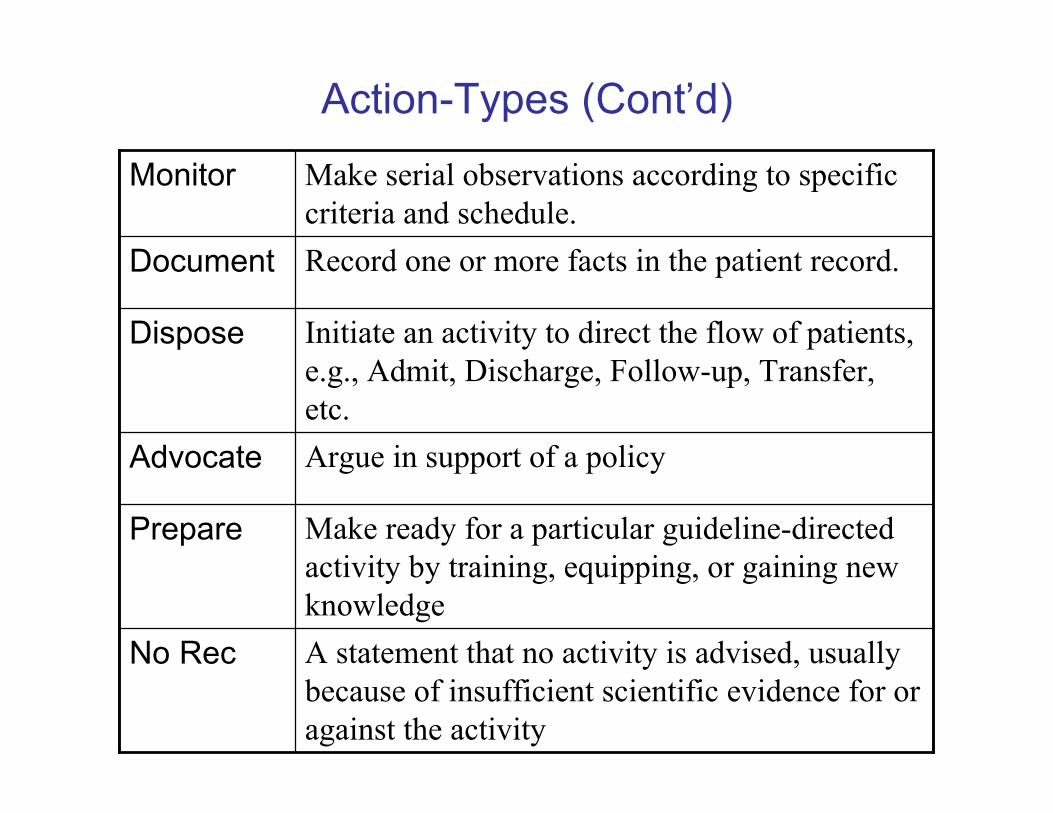
Action-Types (Cont’d)
A statement that no activity is advised, usuallybecause of insufficient scientific evidence for oragainst the activity
No Rec
Make ready for a particular guideline-directedactivity by training, equipping, or gaining newknowledge
Prepare
Argue in support of a policyAdvocate
Initiate an activity to direct the flow of patients,e.g., Admit, Discharge, Follow-up, Transfer,etc.
Dispose
Record one or more facts in the patient record.Document
Make serial observations according to specificcriteria and schedule.
Monitor

Map Recommendations toControlled Vocabulary
Recommendation Language Monitoring Signs and Symptoms of
Asthma
Codable Components Fully-Specified Concept Name Concept ID SNOMED ID CTV3 ID
Peak flow monitoring Peak expiratory flow rate monitoring (regime/therapy) 401004000 P0-00975 XaIxD
Moderate persistent asthma Moderate persistent asthma (disorder) 427295004 F-04F3F XUfiW
Severe persistent asthma Severe persistent asthma (disorder) 426656000 F-04F40 XUfiX
Severe exacerbations Exacerbation of asthma (disorder) 281239006 D2-00076 Xa1hD
Action TypeImperative: Consider long-term daily peak flow monitoring for: — Patients who have
moderate or severe persistent asthma (Evidence B). — Patients who have a history
of severe exacerbations (Evidence B).
Monitor

Identify Obstacles to Implementation
• GuideLine Implementability Appraisal• eGLIA

Identify Obstacles to Implementation
• To provide feedback to guideline authors toanticipate and address obstacles before a draftguideline is finalized
• To assist implementers in guideline selection andto target attention toward anticipated obstacles
• GLIA is available fromhttp://gem.med.yale.edu/glia

GLIA Structure
• 7 global questions relate to the guideline as a whole(e.g., Target population defined? Sequence? Internalconsistency?)
• 20 questions pertain to EACH recommendation– “No” responses indicate barriers
• 4 optional questions relate to implementability in alocal computer system
• Significance of barriers is variable

Evaluate guideline as a wholewith: GLOBALS
1) Do the organization(s) and author(s) who developedthe guideline have credibility with the intended usersof the guideline?
2) Is the patient population eligible for the guidelineclearly defined?
3) Does the guideline document suggest possiblestrategies for dissemination and implementation?
4) Is the guideline supported with tools for applicatione.g., a summary document, a quick reference guide,educational tools, patients' leaflets, online resourcesor computer software?

GLOBALS II
5) If any guideline recommendations are consideredmore important than others, does their presentationor formatting reflect this?
6) Is it clear in what sequence the recommendationsshould be applied?
7) Is the guideline internally consistent, i.e., withoutcontradictions between recommendations or betweentext recommendations and flowcharts, summaries,patient education materials, etc.?
Evaluate EACH recommendationwith respect to:
• Decidability - precisely under what circumstances to dosomething
• Executability - exactly what to do under the circumstancesdefined)
• Effect on process of care - the degree to which arecommendation impacts upon the usual workflow of a caresetting)
• Presentation and formatting - the degree to which therecommendation is easily recognizable and succinct
• Measurable outcomes - the degree to which the guidelineidentifies markers or endpoints to track the effects ofimplementation of this recommendation

GLIA Constructs (2)• Apparent validity - the degree to which a recommendation
reflects the intent of the developer and the strength ofevidence
• Novelty/innovation - the degree to which arecommendation proposes behaviors consideredunconventional by clinicians or patients
• Flexibility - the degree to which a recommendation permitsinterpretation and allows for alternatives in its execution
• Computability - the ease with which a recommendationcan be operationalized in an electronic information system